Cervical spondylosis is a generalized disease process affecting all levels of the cervical spine. Cervical spondylosis encompasses a sequence of degenerative changes in the intervertebral discs, osteophytosis of the vertebral bodies, hypertrophy of the facets and laminal arches, and ligamentous and segmental instability. The natural history of cervical spondylosis is associated with the aging process. Senescent and pathologic processes are thus morphologically indistinguishable. Clinical manifestations of cervical spondylosis may arise when morphologic sequelae are superimposed on a developmentally narrow spinal canal. The two clinical syndromes of spondylotic radiculopathy and myelopathy are distinct, yet they may overlap.[rx]
Cervical spondylosis is a term that encompasses a wide range of progressive degenerative changes that affect all the components of the cervical spine (i.e., intervertebral discs, facet joints, joints of Luschka, ligaments Flava, and laminae). It is a natural process of aging and presents in the majority of people after the fifth decade of life.[rx]
Causes of Cervical Spondylosis
A clinical syndrome caused by compression on the spinal cord that is characterized by
clumsiness in hands
gait imbalance
degenerative cervical spondylosis (CSM)
compression usually caused by anterior degenerative changes (osteophytes, disc osteophyte complex)
degenerative spondylolisthesis and hypertrophy of ligamentum flavum may contribute
the most common cause of cervical myelopathy
Congenital stenosis
Symptoms usually begin when congenital narrowing combined with spondylotic degenerative changes in older patients
OPLL
tumor
epidural abscess
trauma
cervical kyphosis
Neurologic injury
mechanism of injury can be
direct cord compression
ischemic injury secondary to compression of the anterior spinal artery
tandem stenosis occurs in the lumbar and cervical spine in ~20% of patients
tends to be slowly progressive and rarely improves with nonoperative modalities
progression characterized by steplike deterioration with periods of stable symptoms
early recognition and treatment prior to spinal cord damage is critical for good clinical outcomes
Risk Factors for Cervical Spondylosis
The lists below are the factors that you will have a higher risk of getting neck pain and cervical spondylosis:
Genetics – if your family has a history of neck pain
Smoking – clearly linked to increased neck pain
Occupation – jobs with lots of neck motion and overhead work
Mental health issues – depression/anxiety
Injuries/trauma – car wreck or on-the-job injury
“Red flag” features and the conditions they may suggest
Malignancy, infection, or inflammation
Fever, night sweats
Unexpected weight loss
History of inflammatory arthritis, malignancy, infection, tuberculosis, HIV infection, drug dependency, or immunosuppression
Excruciating pain
Intractable night pain
Cervical lymphadenopathy
Exquisite tenderness over a vertebral body
Myelopathy
Gait disturbance or clumsy hands, or both
Objective neurological deficit—upper motor neuron signs in the legs and lower motor neuron signs in the arms
Sudden onset in a young patient suggests disc prolapse
Other
History of severe osteoporosis
History of neck surgery
Drop attacks, especially when moving the neck, suggest vascular disease
Intractable or increasing pain
Symptoms of Cervical spondylosis
The pain can be from minor to major and it becomes worse when looking up or down for a long period of time, such example is reading a book or driving. To improve the pain, most people tend to takes rest or even lay down. The pain usually becomes worse in the morning and at the end of the day.
Symptoms of cervical spondylosis include
Neck stiffness and pain
Numbness and weakness in the upper limbs
Difficulty in walking, losing balance, or weakness in limbs
Difficulty in turning the head fully or bending the neck, which may hinder drive
Muscle spasms in neck and shoulders
Headaches
Grinding and popping feeling in the neck when rotating the head
Loss of bladder and bowel control.
Axial neck pain (oftentimes absent)
Occipital headache common
Extremity paresthesias
Diffuse non-dermatomal numbness and tingling
Weakness and clumsiness
Weakness and decreased manual dexterity (dropping object, difficulty manipulating fine objects)
Gait instability patient feels “unstable” on feet
Weakness walking up and downstairs
Gait changes are the most important clinical predictor
Urinary retention rare and only appear late in disease progression, not very useful in diagnosis due to the high prevalence of urinary conditions in this patient population
Cervical pain aggravated by movement
Referred pain (occiput, between the shoulder blades, upper limbs)
Retro-orbital or temporal pain (from C1 to C2)
Cervical stiffness—reversible or irreversible
Vague numbness, tingling, or weakness in upper limbs
Dizziness or vertigo
Poor balance
Rarely, syncope triggers a migraine pseudo-angina
Poorly localized tenderness
Limited range of movement (forward flexion, backward extension, lateral flexion, and rotation to both sides)
Minor neurological changes like inverted supinator jerks (unless complicated by myelopathy or radiculopathy)
Diagnosis of Cervical Spondylosis
Classically, symptomatic cervical spondylosis presents as one or more of the following three primary clinical syndromes
Axial neck pain
Commonly complain of stiffness and pain in the cervical spine that is most severe in the upright position and relieved with bed rest when removing the load from the neck
Neck motion, especially in hyperextension and side-bending, typically increases the pain
In upper and lower cervical spine disease, patients may report radiating pain into the back of the ear or occiput versus radiating pain into the superior trapezius or periscapular musculature, respectively
Occasionally, patients can present with atypical symptoms of cervical angina such as jaw pain or chest pain.
Cervical radiculopathy
Radicular symptoms usually follow a myotomal distribution depending on the nerve root(s) involved and can present as unilateral or bilateral neck pain, arm pain, scapular pain, paresthesia, and arm or hand weakness
Pain is exacerbated by head tilt toward the affected side or by hyperextension and side-bending toward the affected side.
Cervical myelopathy
Typically has an insidious onset with or without neck pain (frequently absent)
Can initially present with hand weakness and clumsiness, resulting in the inability to complete tasks requiring fine motor coordination (e.g., buttoning a shirt, tying shoelaces, picking up small objects)
Frequent reports of gait instability and unexplained falls
Urinary symptoms (i.e., incontinence) are rare and typically appear late in disease progression
Physical exam of Cervical spondylosis
Other non-specific neck pain lesions—acute neck strain, postural neck ache, or whiplash
Fibromyalgia – and psychogenic neck pain
Mechanical lesions – disc prolapse or diffuse idiopathic skeletal hyperostosis
Inflammatory disease – rheumatoid arthritis, ankylosing spondylitis, or polymyalgia rheumatica
Metabolic diseases – Paget’s disease, osteoporosis, gout, or pseudo-gout
Infections – osteomyelitis or tuberculosis
Malignancy – primary tumors, secondary deposits, or myeloma
lower extremity weakness is more concerning finding
finger escape sign when the patient holds fingers extended and adducted, the small finger spontaneously abducts due to the weakness of intrinsic muscle grip and release test normally a patient can make a fist and release 20 times in 10 seconds. myelopathic patients may struggle to do this
Upper motor neuron signs
Hoffman’s sign (quick flexion of both the thumb and index finger when the middle fingernail is snapped)
Inverted radial reflex (flexion of the fingers in response to the brachioradialis reflex)
Pathological clonus
Babinski sign
Sensory dysfunction
Glove-like sensory loss in hands
Proprioceptive dysfunction
Proprioception dysfunction
due to dorsal column involvement
occurs in advanced disease
associated with a poor prognosis
Decreased pain sensation
pinprick testing should be done to look for a global decrease in sensation or dermatomal changes
due to the involvement of lateral spinothalamic tract
vibratory changes are usually only found in the severe case of long-standing myelopathy
Assessment tools
Lhermitte sign
Romberg test
9-Hole peg test
Grip and release test (observe a decreasing number of cycles)
Timed gait, 30-m walking test
Tandem gait
Upper motor neuron signs (spasticity)
Hyperreflexia – may be absent when there is concomitant peripheral nerve disease (cervical or lumbar nerve root compression, spinal stenosis, diabetes)
Hoffmann’s sign – snapping patients distal phalanx of the middle finger leads to spontaneous flexion of other fingers
Sustained clonus
> three beats defined as sustained clonus
sustained clonus has poor sensitivity (~13%) but high specificity (~100%) for cervical myelopathy
Babinski test
considered positive with the extension of the great toe
Gait and balance
toe-to-heel walk patient has difficulty performing
Romberg test patient stands with arms held forward and eyes closed loss of balance consistent with posterior column dysfunction
provocative tests: Lhermitte Sign >test is positive when extreme cervical flexion leads to electric shock-like sensations that radiate down the spine and into the extremities
Motor dysfunction
Upper extremities
0
Unable to move hands
1
Unable to eat with a spoon but able to move hands
2
Unable to button shirt but able to eat with a spoon
3
Able to button shirt with great difficulty
4
Able to button shirt with slight difficulty
Lower extremities
0
Complete loss of motor & sensory function
1
Sensory preservation without the ability to move legs
2
Able to move legs but unable to walk
3
Able to walk on a flat floor with a walking aid (cane or crutch)
4
Able to walk up- &/or downstairs w/aid of a handrail
5
Moderate-to-significant lack of stability but able to walk up &/or downstairs without a handrail
6
Mild lack of stability but able to walk unaided with smooth reciprocation
recommended views cervical AP, lateral, oblique, flexion, and extension views
general findings degenerative changes of uncovertebral and facet joints
osteophyte formation
disc space narrowing
decreased sagittal diameter
cord compression occurs with canal diameter is < 13mm
lateral radiograph important to look for the diameter of the spinal canal
a Pavlov ratio of less than 0.8 suggests a congenitally narrow spinal canal predisposing to stenosis and cord compression
Sagittal alignment
C2 to C7 alignment determined by tangential lines on the posterior edge of the C2 and C7 body on lateral radiographs in neutral position
Local kyphosis angle the angle between the lines drawn at the posterior margin of most cranial and caudal vertebral bodies forming the maximum local kyphosis
Oblique radiograph important to look for foraminal stenosis which often caused by uncovertebral joint arthrosis
Flexion and extension views important to look for angular or translational instability look for compensatory subluxation above or below the spondylotic/stiff segment
Sensitivity/specificity changes often do not correlate with symptoms 70% of patients by 70 yrs of age will have degenerative changes seen on plain x -rays
X-ray
Plain radiographs are an appropriate initial imaging study for neck and upper extremity pain in the absence of “red flag” symptoms. However, degenerative changes seen on imaging often poorly correlate with the presence of neck pain.[rx]
Common radiographic findings include osteophyte formation, disc space narrowing, endplate sclerosis, degenerative changes of uncovertebral and facet joints, and calcified/ossified soft tissues. AP, lateral, and oblique views of the spine are adequate to evaluate for foraminal stenosis, sagittal alignment, and size of the spinal canal.
The Torg-Pavlov ratio is obtainable by comparing the sagittal diameter of the spinal canal to the sagittal diameter of the vertebral body. The normal value is 1.0, with a ratio of <0.8 indicating cervical stenosis. Flexion and extension views also merit consideration if there is a concern for ligamentous instability.
MRI
MRI is a study of choice to evaluate the degree of the spinal cord and nerve root compression effacement of CSF indicates functional stenosis
Signal changes on T1-weighted images correlate with a poorer prognosis following surgical decompression spinal cord signal changes
Seen as bright signal on T2 images (myelomalacia) compression ratio of < 0.4 carries poor prognosis CR = smallest AP diameter of cord / largest transverse diameter of the cord
Sensitivity/specificity has a high rate of false-positive (28% greater than 40 will have findings of HNP or foraminal stenosis)
CT without contrast can provide complementary information with an MRI and is more useful to evaluate OPLL and osteophytes
CT myelography more invasive than an MRI but gives excellent information regarding degrees of spinal cord compression
Useful in patients that cannot have an MRI (pacemaker), or have artifact (local hardware)
Contrast is given via C1-C2 puncture and allowed to diffuse caudally, or given via a lumbar puncture and allowed to diffuse proximally by putting the patient in Trendelenburg position.
Computed tomography (CT)
CT provides a good definition of bony structures and is more sensitive than plain radiographs in assessing intervertebral foraminal stenosis in the setting of uncovertebral or facet hypertrophy. However, it is less sensitive than MRI for the evaluation of soft tissues and nerve root compression.
CT myelogram
CT is most useful when combined with the injection of intrathecal contrast (myelography) to better evaluate the location and amount of neural compression. It is more invasive than an MRI but can be a consideration in patients who have a contraindication to MRI (e.g., pacemaker) or have an artifact from the hardware.
Discogram
Provocative discography is rarely necessary for cervical spondylosis. It is useful for the evaluation of patients who are experiencing cervical discogenic pain or have multiple herniations in which surgery is a strong possibility. However, the diagnostic procedure remains controversial as it may accelerate the degeneration of normal discs.[rx]
Electromyogram (EMG)
EMG can be useful in supplementing neuroimaging findings in the diagnosis of cervical radiculopathy. It is especially valuable in differentiating nerve root compression from other possible concomitant neurologic conditions, including peripheral neuropathies, entrapment neuropathies, brachial plexopathies, myopathies, and motor neuron diseases.
Nerve conduction studies high false-negative rate may be useful to distinguish peripheral from the central process (ALS)
Normal aging mild symptoms of myelopathy often confused with a “normal aging” process
Stroke
Movement disorders
Vitamin B12 deficiency
Amyotrophic lateral sclerosis (ALS)
Multiple sclerosis
Treatment of Cervical spondylosis
Nonoperative
Observation, NSAIDs, therapy, and lifestyle modifications
indications of mild disease with no functional impairment
the function is a more important determinant for surgery than physical exam finding
patients who are poor candidates for surgery
modalities medications (NSAIDS, gabapentin)
immobilization (hard collar in slight flexion)
physical therapy for neck strengthening, balance, and gait training
traction and chiropractic modalities are not likely to benefit and do have some risks
be sure to watch patients carefully for progression
outcomes improved nonoperative outcomes associated with patients with larger transverse area of the spinal cord (>70mm2)
some studies have shown improvement with immobilization in patients with very mild symptoms
Operative
surgical decompression, restoration of lordosis, stabilization
indications significant functional impairment AND 1-2 level disease lordotic, neutral or kyphotic alignment
techniques appropriate procedure depends on cervical alignment number of stenotic levels
medical conditions (e.g., goiter)
location of compression
anterior cervical diskectomy/corpectomy and fusion
posterior laminectomy and fusion
posterior laminoplasty
combined anterior and posterior procedure
cervical disk arthroplasty
outcomes prospective studies show improvement in overall pain, function, and neurologic symptoms with operative treatment early recognition and treatment prior to spinal cord damage is critical for good clinical outcomes
Goals
optimal surgical treatment depends on the individual. Things to consider include
number of stenotic levels
sagittal alignment of the spine
the degree of existing motion and desire to maintain
medical comorbidities (eg, dysphasia)
simplified treatment algorithm
Anterior Decompression and Fusion (ACDF) alone
Indications
the mainstay of treatment in most patients with single or two level disease
fixed cervical kyphosis of > 10 degrees anterior procedure can correct kyphosis
compression arising from 2 or fewer disc segments
pathology is anterior (OPLL, soft discs, disc osteophyte complexes)
Approach
uses Smith-Robinson anterior approach
Decompression of corpectomy and strut graft may be required for multilevel spondylosis two level corpectomies tend to be biomechanically vulnerable (preferable to combine single-level corpectomy with adjacent level diskectomy)
7% to 20% rates of graft dislodgement with cervical corpectomy with associated severe complications, including death, reported.
fixation anterior plating functions to increase fusion rates and preserve the position of the interbody cage or strut graft
pros & cons advantages compared to posterior approach lower infection rate blood loss less postoperative pain disadvantages avoid in patients with poor swallowing function
Laminectomy with posterior fusion
multilevel compression with kyphosis of < 10 degrees,> 13 degrees of fixed kyphosis is a contraindication for a posterior procedure
in the flexible kyphotic spine, posterior decompression and fusion may be indicated if kyphotic deformity can be corrected prior to instrumentation
Contraindications
fixed kyphosis of > 10 degrees is a contraindication to posterior decompression
will not adequately decompress spinal cord as it is “bowstringing” anterior
Pros & cons
fusion may improve neck pain associated with degenerative facets
not effective in patients with > 10 degrees fixed kyphosis
Laminoplasty
gaining in popularity
useful when maintaining motion is desired
avoids complications of fusion so may be indicated in patients at high risk of pseudoarthrosis
Contraindications
cervical kyphosis > 13 degrees is a contraindication to posterior decompression will not adequately decompress spinal cord as it is “bowstringing” anterior
severe axial neck pain is a relative contraindication and these patients should be fused
Technique
the volume of the canal is expanded by hinged-door laminoplasty followed by fusion usually performed from C3 to C7
open door technique hinges created unilaterally at the junction of lateral mass and lamina and opening on opposite side opening held open by bone, suture anchors, or special plates
French door technique hinge created bilaterally and the opening created midline
Pros & cons advantages
lower complication rate than multilevel anterior decompression especially in patients with OPLL a motion-preserving technique pseudoarthrosis not a concern in patients with poor healing potential (diabetes, chronic steroid users) can be combined with a subsequent anterior procedure
allows for decompression of multilevel stenotic myelopathy without compromising stability and motion (avoids postlaminectomy kyphosis)
Disadvantages
higher average blood loss than anterior procedures
postoperative neck pain
still associated with loss of motion outcomes equivalent to multilevel anterior decompression and fusion
Combined anterior and posterior surgery multilevel stenosis in the rigid kyphotic spine
multi-level anterior cervical corpectomies
postlaminectomy kyphosis
Laminectomy alone
indications rarely indicated due to risk of post laminectomy kyphosis
pros & cons progressive kyphosis 11 to 47% incidence if laminectomy performed alone without fusion
Surgical Infection
higher rate of surgical infection with posterior approach than anterior approach
Pseudoarthrosis incidence 12% for single level fusions, 30% for multilevel fusions treatment
treat with either posterior wiring or plating or repeat anterior decompression and plating if patient has symptoms of radiculopathy
Postoperative C5 palsy
reported to occur in ~ 4.6% of patients after surgery for cervical compression myelopathy
no significant differences between patients undergoing anterior decompression and fusion and posterior laminoplasty
occurs immediately postop to weeks following surgery
Mechanism
mechanism is controversial
in laminectomy patients, it is thought to be caused by tethering of nerve root with dorsal migration of spinal cord following removal of posterior elements
Prognosis
patients with postoperative C5 palsy generally have a good prognosis for functional recovery, but recovery takes time
Recurrent laryngeal nerve injury approach in the past it has been postulated that the RLN is more vulnerable to injury on the right due to a more aberrant pathway recent studies have shown there is not an increased injury rate with a right sided approach
treatment if you have a postoperative RLN palsy, watch over time
if not improved over 6 weeks, then ENT consult to scope patient and inject Teflon
if you are performing revision anterior cervical surgery, and there is any suspicion of an RLN from the first operation, obtain ENT consult to establish prior injury
if a patient has prior RLN nerve injury, perform revision surgery on the same as the prior injury/approach to prevent a bilateral RLN injury
Hardware failure and migration 7-20% with two-level anterior corpectomies two-level corpectomies should be stabilized from behind
Postlaminectomy kyphosis treat with anterior/posterior procedure
In a 2019 cohort study by El-Yahochouchi et al., the overall incidence of immediate and delayed adverse events following an epidural steroid injection was 2.4% and 4.9%, respectively.[rx] Complications include:
Lumbar disc herniation is a common condition that frequently affects the spine in young and middle-aged patients.1,5,11 The lumbar intervertebral disc is a complex structure composed of collagen, proteoglycans, and sparse fibrochondrocytic cells that serve to dissipate forces exerted on the spine. As part of the normal aging process, the disc fibrochondrocytes can undergo senescence, and proteoglycan production diminishes. This leads to a loss of hydration and disc collapse, which increases strain on the fibers of the annulus fibrosus surrounding the disc. Tears and fissures in the annulus can result, facilitating a herniation of disc material, should sufficient forces be placed on the disc. Alternatively, a large biomechanical force placed on a healthy, normal disc may lead to extrusion of disc material in the setting of catastrophic failure of the annular fibers.5
Spinal disc herniation also is known as a slipped disc, is a medical condition affecting the spine in which a tear in the outer, fibrous ring of an intervertebral disc allows the soft, central portion to bulge out beyond the damaged outer rings. Disc herniation is usually due to age-related degeneration of the outer ring, known as the anulus fibrosus, although trauma, lifting injuries, or straining have been implicated as well. Tears are almost always postero-lateral (on the back of the sides) owing to the presence of the posterior longitudinal ligament in the spinal canal .This tear in the disc ring may result in the release of chemicals causing inflammation, which may directly cause severe pain even in the absence of nerve rootcompression.
Anatomy of Spinal Disc Herniation
Herniated = from “hernia,” a part of the body that bulges out through an abnormal opening Disc = the disk-shaped cushions between the bones of the spine
The vertebral column (also called the spinal column orbackbone) is made up of 33 bones known as vertebra (plural, vertebrae). Each vertebra is separated from the adjacent vertebrae by intervertebral discs, a spongy but strong connective tissue. The intervertebral discs, along with ligaments and facet joints, connect the individual vertebrae to help maintain the spine’s normal alignment and curvature while also permitting movement.
The image at left shows the entire spinal column from beside and from the front. The bones of the spinal column are orange in color, and the intervertebral discs are white.
In the center of the spinal column there is an open channel called the spinal canal. The spinal cord and spinal nerves are located in the spinal canal, where they are surrounded by spinal fluid and protected by the strong spinal column. On each side of the spine, small openings between adjacent vertebrae called foramina (singular, foramen) allow nerve roots to enter and exit the spinal canal.
The spine is divided into the following distinct regions:
Cervicalspine – consists of seven vertebrae in the neck. These vertebrae are small and allow for the mobile nature of the neck.
Thoracic spine – consists of 12 vertebrae in the upper and mid-back. These are larger and stronger than the cervical vertebrae. Each thoracic vertebra is attached to a rib on either side. This provides significant stiffness and strength to the thoracic portion of the spine.
Lumbar spine – usually consists of five vertebrae in the lower back, but may vary between four and six. These vertebrae are the largest because they withstand the greatest amount of force in the spine. The lumbar spine is also more mobile than the thoracic spine. Because of these factors, the lumbar spine is the most frequently affected by degenerative conditions, spinal stenosis, and herniated discs.
Sacrococcygeal – the very lowest portion of the spine. The sacrococcygeal region consists of one single bone, made of fused vertebrae in the sacrum (five vertebrae) and coccyx (four vertebrae). It attaches to the pelvis on either side. In a small number of people, there may be a disc between the first and second sacral vertebrae. Alternatively, the fifth vertebra in the lumbar (lower) spine may occasionally be fused to the sacrum, leaving only 4 lumbar vertebrae.
A herniated disc occurs when the fibrous outer portion of the disc ruptures or tears, and the jelly-like core squeezes out. When the herniated disc compresses a nearby nerve, as in the image below, the result can be a pinched nerve. A pinched nerve may cause pain, numbness, tingling or weakness in the arms or legs. The substance that makes up the disc’s jelly-like core can also inflame and irritate the nerve, causing additional pain.
Prolapse of intervertebral disc closeup 3d image. (c) alexmit/Big Stock
A bulging disc occurs when the outer wall of the disc weakens but doesn’t rupture, and “bulges” outward. A herniated disc may actually begin as a bulging disc whose outer wall is then ruptured by a great amount of pressure.
Disc herniation can occur in the cervical, thoracic, or lumbar spine. The location of the pain depends on the location of the herniated disc. If the herniation occurs in the neck, for example, it can cause pain that radiates into the shoulder and arm; if it occurs in the lower back, the pain produced can radiate down into the hip and leg. Depending on the location, it can damage the spinal cord.
Symptoms of Spinal Disc Herniation
A cervical herniated disc may put pressure on a cervical spinal nerve and can cause symptoms like pain, pins and needles, numbness or weakness in the neck, shoulders, or arms. A large disc herniation in the cervical spine may compress the spinal cord within the spinal canal and cause numbness, stiffness, and weakness in the legs and possibly some difficulty with bowel and bladder control.
A thoracic herniated disc may cause pain in the mid back around the level of the disc herniation. If the disc herniation compresses a thoracic spinal nerve as it travels through the foramen, then pain or numbness may travel around the rib cage from the back to the front of the chest or upper abdomen. A large disc herniation in the thoracic spine may compress the spinal cord within the spinal canal and cause numbness, stiffness and weakness in the legs and possibly some difficulty with bowel and bladder control.
A lumbar herniated disc may cause the following symptoms:
Intermittent or continuous back pain (this may be made worse by movement, coughing, sneezing, or standing for long periods of time)
Spasm of the back muscles
Sciatica — pain that starts near the back or buttock and travels down the leg to the calf or into the foot.
Muscle weakness in the legs
Numbness in the leg or foot
Decreased reflexes at the knee or ankle
Changes in bladder or bowel function
Difficulty walking
Incoordination
The symptoms of disc disease may resemble other conditions or medical problems. Always consult a doctor for a diagnosis.
Causes and Risk Factors
Herniated discs can often be the result of degenerative disc disease. As people age, the intervertebral discs lose their water content and ability to cushion the vertebrae. As a result, the discs are not as flexible. Furthermore, the fibrous outer portion of the disc is more likely to rupture or tear.
Acute disc herniations can occur in young, healthy people as a result of an injury or tear to the outer layer of the disc (called the annulus fibrosis) that allows the central, jelly-like portion of the disc (called thenucleus pulposis) to herniate into the spinal canal or foramen.
Tests and Diagnosis of Spinal Disc Herniation
Physical examination
The straight leg raise may be positive, as this finding has low specificity; however, it has high sensitivity. Thus the finding of a negative SLR sign is important in helping to “rule out” the possibility of a lower lumbar disc herniation. A variation is to lift the leg while the patient is sitting.[32] However, this reduces the sensitivity of the test.[33]
Imaging
Projection radiography (X-ray imaging) – Although traditional plain X-rays are limited in their ability to image soft tissues such as discs, muscles, and nerves, they are still used to confirm or exclude other possibilities such as tumors, infections, fractures, etc. In spite of these limitations, X-ray can still play a relatively inexpensive role in confirming the suspicion of the presence of a herniated disc. If a suspicion is thus strengthened, other methods may be used to provide final confirmation.
Computed tomography scan (CT or CAT scan) – A diagnostic image created after a computer reads x-rays. It can show the shape and size of the spinal canal, its contents, and the structures around it, including soft tissues. However, visual confirmation of a disc herniation can be difficult with a CT.
Magnetic resonance imaging (MRI) without contrast – A diagnostic test that produces three-dimensional images of body structures using powerful magnets and computer technology. It can show the spinal cord, nerve roots, and surrounding areas, as well as enlargement, degeneration, and tumors. It shows soft tissues better than CAT scans. An MRI performed with a high magnetic field strength usually provides the most conclusive evidence for diagnosis of a disc herniation. T2-weighted images allow for clear visualization of protruded disc material in the spinal canal.
Myelogram An x-ray of the spinal canal following injection of a contrast material into the surrounding cerebrospinal fluid spaces. By revealing displacement of the contrast material, it can show the presence of structures that can cause pressure on the spinal cord or nerves, such as herniated discs, tumors, or bone spurs. Because myelography involves the injection of foreign substances, MRI scans are now preferred for most patients. Myelograms still provide excellent outlines of space-occupying lesions, especially when combined with CT scanning (CT myelography).
Electromyogram and nerve conduction studies (EMG/NCS) – These tests measure the electrical impulse along nerve roots, peripheral nerves, and muscle tissue. This will indicate whether there is ongoing nerve damage, if the nerves are in a state of healing from a past injury, or whether there is another site of nerve compression. EMG/NCS studies are typically used to pinpoint the sources of nerve dysfunction distal to the spine.
Computerized tomography (CT) scan – a series of X-rays, assembled by a computer into 3-dimensional images of the body’s structures
Myelography – a procedure that involves injecting a liquid dye into the spinal column followed by a series of X-rays and a computerized tomography (CT) scan. This procedure may provide useful images that reveal the indentations of the spinal fluid sac caused by bulging or herniated discs, or bone spurs that might be pressing on the spinal cord or nerves.
Electromyography (EMG) – tests the electrical activity of a nerve root to help determine the cause of pain.
The presence and severity of myelopathy can be evaluated by means of transcranial magnetic stimulation (TMS), a neurophysiological method that allows the measurement of the time required for a neural impulse to cross the pyramidal tracts, starting from the cerebral cortex and ending at the anterior horn cells of the cervical, thoracic or lumbar spinal cord. This measurement is called Central Conduction Time (CCT). TMS can aid physicians to:
determine whether myelopathy exists
identify the level of the spinal cord where myelopathy is located. This is especially useful in cases where more that two lesions may be responsible for the clinical symptoms and signs, such as in patients with two or more cervical disc hernias[34]
follow-up the progression of myelopathy in time, for example before and after cervical spine surgery
TMS can also help in the differential diagnosis of different causes of pyramidal tract damage.[35]
Since a herniated disc may cause similar symptoms to other degenerative spinal conditions, a surgeon may order a variety of diagnostic procedures to rule out other possible conditions.
Treatment of Spinal Disc Herniation
Before discussing surgery as an option, the surgeon may initiate the following nonoperative treatments. Specific treatment for lumbar disk disease will be determined by your health care provider based on
Your age, overall health, and medical history
Extent of the condition
Type of condition
Your tolerance for specific medications, procedures, or therapies
Expectations for the course of the condition
Your opinion or preference
Typically, conservative therapy is the first line of treatment to manage lumbar disk disease. This may include a combination of the following:
Bed rest
Patient education on proper body mechanics (to help decrease the chance of worsening pain or damage to the disk)
Physical therapy, which may include ultrasound, massage, conditioning, and exercise
Weight control
Use of a lumbosacral back support
Medications of Spinal Disc Herniation
Analgesics: Prescription-strength drugs that relieve pain but not inflammation.
Antidepressants: A Drugs that block pain messages from your brain and boost the effects of eorphins (your body’s natural painkillers).
Corticosteroids: Also known as oral steroids, these medications reduce inflammation.
Muscle Relaxants: These medications provide relief from spinal muscle spasms.
Neuropathic Agents: Drugs(pregabalin & gabapentine) that address neuropathic—or nerve-related—pain. This includes burning, numbness, and tingling.
Opoids : Also known as narcotics, these medications are intense pain relievers that should only be used under a doctor’s careful supervision.
Topical Medications: These prescription-strength creams, gels, ointments, patches, and sprays help relieve pain and inflammation through the skin.
NSAIDs: Prescription-strength drugs that reduce both pain and inflammation.Pain medicines and anti-inflammatory drugs help to relieve pain and stiffness, allowing for increased mobility and exercise. There are many common over-the-counter medicines called non-steroidal anti-inflammatory drugs (NSAIDs). They include aspirin, ibuprofen (Motrin, Advil), and naproxen (Naprosyn, Aleve).
Calcium & vitamin D3, to improve bones health and healing fracture.
Glucosamaine & diacerine ,can be used to tightening the loose tenson and regenerate cartilage or inhabit the further degeneration of cartilage.
Corticosteroid to healing the nerve inflamation and clotted blood in the joints.
Diatery suppliment to remove the general weakness & improved the health.
There is little evidence to suggest that drug treatments are effective in treating herniated disc.
NSAIDs and cytokine inhibitors don’t seem to improve symptoms of sciatica caused by disc herniation.
We found no evidence examining the effectiveness of analgesics, antidepressants, or muscle relaxants in people with a herniated disc.
We found no evidence of sufficient quality to judge the effectiveness of epidural injections of corticosteroids.
With regard to non-drug treatments, spinal manipulation seems to be more effective at relieving local or radiating pain in people with acute back pain and sciatica with disc protrusion compared with sham manipulation, although concerns exist regarding possible further herniation from spinal manipulation in people who are surgical candidates.
Neither bed rest nor traction seems effective in treating people with sciatica caused by disc herniation.
We found insufficient evidence about advice to stay active, acupuncture, massage, exercise, heat, or ice to judge their efficacy in treating people with herniated disc.
About 10% of people have sufficient pain after 6 weeks for surgery to become a consideration.
Both standard discectomy and microdiscectomy seem to increase self-reported improvement to a similar extent.
We found insufficient evidence judging the effectiveness of automated percutaneous discectomy,laser discectomy, or percutaneous disc decompression.
Surgical Treatment of Spinal Disc Herniation
When these conservative measures fail, surgery for removal of a herniated disk may be recommended. Surgery is done under general anesthesia. An incision is placed in the lower back over the area where the disk is herniated. Some bone from the back of the spine may be removed to gain access to the area where the disk is located. Typically, the herniated part of the disk and any extra loose pieces of disk are removed from the disk space.
Surgical treatment for a herniated disc will be based on the following
The history, severity and duration of pain
Whether or not the patient has received previous treatments for disc disorders and how effective the treatments were
Whether or not there is any evidence of neurologic damage such as sensory loss, weakness, impaired coordination, or bowel or bladder problems
Surgery for patients with disc disorders of the spine is usually recommended for those patients who do not find relief with non-operative treatment over a period of 6-12 weeks. Surgery is also recommended in patients who have a neurologic deficit (numbness, weakness or reduced function due to pressure on the spinal cord or nerves). Early intervention in those cases is best in order to maximize the likelihood of neurologic recovery.
Your surgeon may perform the following surgical procedures:
Microdiscectomy: A procedure that uses a microscope and microsurgical tools to remove the portion of the disc that is pressing against the nerve, relieving the pressure caused by a herniated disc. Microdiscectomy is frequently performed for herniated discs in the certical, thoracic, and lumbosacral spine. This procedure is performed under general anesthesia through a small skin incision over the spine. The muscles of the spine are gently elevated or spread apart to expose a small segment of the spine. A small amount of the back part of the spine, called the lamina and facet joint, is trimmed under high magnification of the microscope to provide safe access to the spinal canal. Using microsurgical techniques, our neurosurgeons identify and remove the herniated piece of the disc while protecting the compressed nerve. Most patients may go home either on the day of surgery or the next morning.
Anterior (from the front) or lateral (from the side) surgical approaches may be required for large or calcified thoracic disc herniations that cause spinal cord compression.
Anterior Cervical Discectomy and Fusion (ACDF): a procedure that involves the removal of the herniated disc in the cervical spine through the front of the neck. A fusion surgery may be required to make the spine stable after the discectomy.
After surgery, restrictions may be placed on the patient’s activities for several weeks while healing is taking place to prevent another disk herniation from occurring. Your surgeon will discuss any restrictions with you.
Others Treatment of Spinal Disc Herniation
Chiropractic Care
Sixty percent of people with sciatica who didn’t get relief from other therapies and then tried spinal manipulation experienced the same degree of pain relief as patients who eventually had surgery, found a 2010 study in the Journal of Manipulative and Physiological Therapeutics. The 120 people in the study saw a chiropractor about 3 times a week for 4 weeks, and then continued weekly visits, tapering off treatment as they felt better. In people who responded to chiropractic care, benefits lasted up to a year. “Spinal manipulation may create a response in the nervous system that relieves pain and restores normal mobility to the injured area,” says study researcher Gordon McMorland, DC, of National Spine Care in Calgary, Alberta. “It also reduces inflammation, creating an environment that promotes the body’s natural healing mechanisms.”
Acupuncture
“You can get relief as soon as the first session, though it takes about 12 sessions to see improvement,” says Jingduan Yang, MD, assistant professor at the Jefferson Myrna Brind Center of Integrative Medicine at Thomas Jefferson University. A small study in the Journal of Traditional Chinese Medicine found that of 30 people with sciatica, 17 got complete relief and 10 saw symptoms improve with warming acupuncture, in which the needles are heated.
Yoga
A study in the journal Pain reported that people with chronic back pain who practiced Iyengar yoga for 16 weeks saw pain reduced by 64% and disability by 77%. Although yoga’s effects on sciatica are less clear, gentle forms may be beneficial. By strengthening muscles and improving flexibility, a yoga practice can help sciatica sufferers “move and function better so they don’t fall into a posture that aggravates sciatica,” says James W. Carson, PhD, a psychologist at the Comprehensive Pain Center at Oregon Health & Science University. For extra grip and stability, try these grip socks from Natural Fitness.
Massage
Don’t expect a chilled-out spa massage if you have sciatica. In this instance, trigger-point therapy is best, says Jeff Smoot, vice president of the American Massage Therapy Association. The sciatic nerve sits underneath a muscle called the piriformis, which is located beneath the glutes. “When the piriformis muscle gets tight, it pinches the sciatic nerve, causing tingling and numbness down into the leg,” says Smoot. He applies pressure to irritated and inflamed areas, or trigger points, in the piriformis muscle, as well as in muscles in the lower back and glutes. Typically, Smoot schedules treatments 7 to 10 days apart. If patients don’t see progress by the fourth visit, “they need to try another form of therapy,” he says.
Topical Preparations
St. John’s wort oil, a liniment, is “one of my favorites for nerve pain,” says Tieraona Low Dog, MD, director of the fellowship at the Arizona Center for Integrative Medicine. Apply the anti-inflammatory oil two or three times a day where there’s pain. Another option: an OTC cayenne pepper plaster or cream; capsaicin, found in chiles, hinders the release of pain-causing compounds from nerves. For severe cases, Low Dog uses the prescription chile patch Qutenza, designed for shingles pain. “One application is effective for weeks,” says Low Dog.
Ice or Heat
Because the sciatic nerve is buried deep within the buttock and leg, ice or heat on the surface of the body won’t ease that inner inflammation. But the timehonored treatments can act as counterirritants—that is, “they give your body other input in the painful area, and that brings the pain down a notch,” says Ruppert. Apply an ice pack or a heating pad as needed for 15 minutes.
Devil’s Claw
The herbal medication devil’s claw is “quite a potent anti-inflammatory, working like ibuprofen and similar drugs to inhibit substances that drive inflammation,” says Low Dog. She generally starts patients on 1,500 to 2,000 mg twice a day. Look for a brand that has a standardized extract of roughly 50 mg of harpagoside, the active compound. Safety reviews show that the supplement is well tolerated by most people but should be avoided by patients with peptic ulcers or on blood-thinning medications.
Epidural Steroid Injections
People whose pain doesn’t lessen within about a month and who aren’t helped by other therapies may find their pain remedied by an x-ray-guided injection of steroid into the lower back near the sciatic nerve, says Raj Rao, MD, a spokesperson for the AAOS. “The hope is to reduce inflammation within that nerve branch,” explains Rao. Because of concerns about side effects, such as loss of bone density, the epidural shots are limited to three a year.
Physiotherapy in Harniated Disc
In stage 1&2 of harniated disc physiotherapy must applied to cure harniated hisc .In case of stage 3&4 ,physiotherapy can’t applied due to adoining the another case of foot drop.
In accordance of NIH journal
Physiotherapy for a lumbar disc bulge
Physiotherapy treatment for a lumbar disc bulge is vital to ensure an optimal outcome and may comprise:
soft tissue massage
electrotherapy (e.g. ultrasound)
lumbar taping
the use of a back brace
mobilization
traction
the use of a lumbar roll for sitting
dry needling
exercises to push the disc back ‘in’ and to improve strength, core stability and flexibility
education
activity modification advice
biomechanical correction
ergonomic advice
clinical Pilates
hydrotherapy
a functional restoration program
a gradual return to activity program
Physical therapy often plays a major role in herniated disc recovery. Its methods not only offer immediate pain relief, but they also teach you how to condition your body to prevent further injury.
There are a variety of physical therapy techniques. Passive treatments relax your body and include deep tissue massage, hot and cold therapy, electrical stimulation (eg, TENS), and hydrotherapy.
Your physical therapy program will usually begin with passive treatments. But once your body heals, you will start active treatments that strengthen your body and prevent further pain. Your physical therapist will work with you to develop a plan that best suits you.
Passive Physical Treatments for Herniated Discs
Deep Tissue Massage
There are more than 100 types of massage, but deep tissue massage is an ideal option if you have a herniated disc because it uses a great deal of pressure to relieve deep muscle tension and spasms, which develop to prevent muscle motion at the affected area.
Hot and Cold Therapy
Both hot and cold therapies offer their own set of benefits, and your physical therapist may alternate between them to get the best results.Your physical therapist may use heat to increase blood flow to the target area. Blood helps heal the area by delivering extra oxygen and nutrients. Blood also removes waste byproducts from muscle spasms.Conversely, cold therapy (also called cryotherapy) slows circulation. This reduces inflammation, muscle spasms and pain. Your physical therapist may place an ice pack on the target area, give you an ice massage, or even use a spray known as fluoromethane to cool inflamed tissues.
Hydrotherapy
As the name suggests, hydrotherapy involves water. As a passive treatment, hydrotherapy may involve simply sitting in a whirlpool bath or warm shower. Hydrotherapy gently relieves pain and relaxes muscles.
A TENS machine uses an electrical current to stimulate your muscles. It sounds intense, but it really isn’t painful. Electrodes taped to your skin send a tiny electrical current to key points on the nerve pathway. TENS reduces muscle spasms and is generally believed to trigger the release of endorphins, which are your body’s natural pain killers.
Traction
The goal of traction is to reduce the effects of gravity on the spine. By gently pulling apart the bones, the intent is to reduce the disc herniation. The analogy is much like a flat tire “disappearing” when you put a jack under the car and take pressure off the tire. It can be performed in the cervical or lumbar spine.
Active Treatments You May Try in Physical Therapy
Active treatments help address flexibility, posture, strength, core stability, and joint movement. An exercise program may also be prescribed to achieve optimal results. This will not only curb recurrent pain but will also benefit your overall health. Your physical therapist will work with you to develop a program based on your specific diagnosis and health history.
Core stability
Many people don’t realize how important a strong core is to their spinal health. Your core (abdominal) muscles help your back muscles support your spine. When your core muscles are weak, it puts extra pressure on your back muscles. Your physical therapist may teach you core stabilizing exercises to strengthen your back.
Flexibility
Learning proper stretching and flexibility techniques will prepare you for aerobic and strength exercises. Flexibility helps your body move easier by warding off stiffness.
Hydrotherapy
In contrast to simply sitting in a hot tub or bath like its passive counterpart, active hydrotherapy may involve water aerobics to help condition your body without unnecessary stress.
Muscle strengthening
Strong muscles are a great support system for your spine and better handle pain.
Your physical therapist will teach you ways to condition and strengthen your back to help prevent future pain. You may learn self-care principles so you understand how to best treat your symptoms. The ultimate goal is for you to develop the knowledge to maintain a pain-free lifestyle.
It’s essential that you learn how to exercise and condition your back after the formal physical therapy ends. If you don’t implement the lessons you learned during physical therapy, you won’t enjoy its long-term results. By taking care of your back on your own, you may prevent further herniated disc pain
8 Best Exercises For Slipped Disc In Lower Back
Our spinal cord is supported by a number of muscles. Relevant exercises help relieve the pain and reduce the symptoms. Muscle exercises of those muscles associated with the affected area is necessary. Patients must know the region that has a slipped disc and then opt for exercises related to that muscle. The list of best exercises for the slipped disc are mentioned as follows:
Abdominal Isometrics – It can be performed either on floor, mat or bed. This exercise involves moving your lower back towards the surface at which you are performing this exercise. Leg movement must be reduced in this exercise and stomach muscles must be made active. This reduces pain in lower back because of the attachment of abdominal muscles to the lower side of the vertebral column. Ten repetitions are effective.
Crunches – Lie on a flat surface with knees bent. Cross your arm under your head, raise your head and chest in such a manner that your rib cage curl interiorly towards your backbone. Perform this exercise slowly and gradually. In the beginning, perform fewer crunches and repeat it daily and increase the number of turns as you gain strength.
Lower back extension – Lie in an upside down position, raise your upper body with the help of elbow and hold up yourself in an elevated position for a short span of time and then slowly lower down. Please make sure that during this exercise you do not raise your pelvis girdle (hip region).
Bilateral knee to the chest – Lay down on a flat surface and draw your knee towards your abdominal region, repeat it 5 times and then switch leg. You can also increase the number of turns each time you repeat it.
Iso-hip flexion – Lay down over a flat surface and draw your knees towards your chest region in a 90 degree position with your stomach. Place your hands over your knees and then exert your hand pressure to lower your knee. Then utilize the knee pressure to resist the downward movement of your legs, in all both movements should just exert pressure and allow no movements. This position should be maintained for few seconds and then lowered slowly and gradually.
Air bike – Sit on a chair with your chest and shoulders supported. Align your knees and feet together and then bring them towards your body and perform a pedaling motion in air then repeat the same motion while moving your knees farther away from body. Follow ten repetitions each time and increase its number as you gain strengths
Ham string stretch: Lie on a flat surface with your knees bend, place your hands under your knees and then slightly pull your leg towards your chest, repeat it with other leg. This exercise must involve a stretch over lower thigh muscle
Lumbar roll: Lie on a flat surface with your knee bent and your feet lying on the floor then move your legs together towards the right side and then towards your left side. Repeating these movements 5 times on each side.
The above mentioned best exercises for slipped disc can be followed but if pain increases or muscle pain is persisting then quit these exercises right away. These exercises not only help in reducing the pain but they also activate efficient muscle movement. Along with these exercise tips, proper body postures must be also maintained to prevent further disc damages.
Home Remady for Herniated Disc/Slip Disc
Consciousnes
Incase of PLID home remedies are not special treatment just only home practice & creating public awareness. All should be done in PLID stage 1&2
Walking
Walking every day keeps muscle disorders away. Walking can also help to prevent herniated disc. Walk on a flat road for 20 minutes as many times as you can in a day. Take longer steps as it will help you to keep away the pain of herniated disc. Do not give strain to yourself as it might increase the pain.
Rest
www.rxharun.com
Rest is essential for patients suffering from herniated disc. Take short rest periods from time to time. When you are sleeping make sure you don’t stay in the same position for a long time. Do not sleep on your stomach. Also, take care of the mattress you are sleeping on. Don’t let it be too soft and spongy. Buy a mattress that has good surface area and is soft in nature.
Physiotherapy And Yoga( only home practice)
Physiotherapy is a very cheap and good way of getting rid of herniated disc from itself. Therapists will teach your proper exercises and stretches which will improve the disc shape to a great extent.
You will notice good differences while performing daily chores after just 4-5 sessions of therapy.
Physiotherapy also promotes faster healing of the disorder.
Turmeric
Turmeric contains curcumin which is a very good anti-oxidant and anti-inflammatory agent. This is why it stops the gel-like fluid inside the discs from coming out and bulge. It also shows antihistamine properties which help to reduce pain because of slowed blood circulation to the area of pain.
Dimethyl Sulfoxide (DMSO)
Dimethyl sulfoxide is a derivative from sulphur which has antioxidant properties as well as the organic sulphur present in it helps in the growth of new cells and detoxification of the body. The growth of new cells helps to replace the old cells of the discs and prevent the fluid from leaking outside.
Massage With Essential Oils
Massage with essential oils on the full body, especially on the spine and lower back regions, will help in good blood circulation and promote the growth of new cells. It will help relieve pain and promote better absorption of oxygen and nutrients. Essential oils will also regenerate the cells of the disc and hence stop the disc from getting slipped.
Acupressure And Acupuncture
In both techniques, pressure is used for relieving the pain from the swelled area. In acupressure fingers, tips and elbow are used and acupuncture needles are used. But this should be done with the help of an experienced practitioner and not alone.
This is not recommended for patients having high blood pressure and for women who are pregnant.
TENS
TENS stands for Transcutaneous Electrical Nerve Stimulation and this is one of the best remedies for herniated disc at home. This treatment uses low voltage electric current which is applied to the affected area and helps the body to release endorphin which decreases the pain.
Cayenne Pepper
It is a very effective ingredient for the treatment of herniated disc.You can drink its tea or make a paste of the pepper using water and apply on the affected area.
Diet
Diet is necessary to keep away all types of bad conditions that might affect you.Drink a lot of water and eat a balanced diet. Take excess of fibres and proteins. During this condition, you should avoid dairy products and red meat. Also, avoid fat-free foods.
Epsom Salt
Epsom salt is one of the widely used natural painkiller and anti-inflammatory agent.
You can use this by adding 3-4 cups of salt in a hot water bath. Stay inside the bath for 15 minutes. It will help you achieve maximum relaxation.
Do not use this remedy if you are diabetic or pregnant. If you are on any type of medication consult your doctor before bathing in Epsom salt.
Horsetail
Horsetail is a herb which has high quantities of minerals in it. It nourishes our tissues and has the ability to heal broken bones and torn ligaments.
All you need to do is add some horsetail leaves to half a litre of water. Boil on low heat till the water quantity reduces to half its quantity. Cool the solution and filter it off. You can drink 5 ml of the solution thrice a day.It will heal herniated disc very fast.
California Poppy
California poppy is anti-inflammatory and analgesic in nature. This is what makes it a good treatment for herniated disc.
You can tear the leaves of California poppy into small pieces and make a paste out of it using water. Use little hot water so that when you apply the paste on the affected area it is still warm.
White Willow Bark
White willow bark is used for reducing the discomfort of herniated discs. The chemical structure of this drugs shows a marked similarity to aspirin hence acts as an analgesic but doesn’t irritate your gut. It is also astringent and anti-inflammatory in nature.
This herb might react with drugs hence do consult your doctor if you are on any kind of medication.
Comfrey Leaves
Comfrey leaves have power to heal bones and connective tissues of the body.All you need to do is take some fresh leaves and add it to cold water. Let it remain undisturbed for around 12 hours. After 12 hours heat the above solution and filter it. Add the filtrate to bath water and take a bath in it 2 times a day.Do not consume it orally because it contains hepatic-toxin alkaloids.
Boswellia
Boswellia is a naturally occurring painkiller which is a very effective remedy for herniated disc.
All you can do is make a decoction of Boswellia and consume it 2 times a day to reduce pain and discomfort associated with herniated discs.
Boswellia is an organic painkiller that effectively treats the problem of herniated disc. It is also an herbal cure for osteoarthritis.
Omega-3 Fatty Acids
Omega-3 Fatty acids are helpful in decreasing the inflammation and pain experienced due to herniated disc disorder. This acid forms collagen which is used by the broken discs for repairing itself.
Eat foods that are high in this kind of fats like fish, almonds, sprouts and walnuts.
Colchicine
Colchicine is an active amino-alkaloid found in the plant of Kurchi or autumn crocus. This powder is obtained by crushing the seeds of the plant. It has anti-inflammatory properties which are effective against the slipped disc.
Make a paste with kurchi powder and honey and consume it once a day.
You can also make tea out of the powder or mix the powder in milk and have it once or twice a day.
Burdock
Burdock contains a lot of anti-oxidants which is helpful to detoxify the body and remove all kinds of harmful substances and decrease the pain and inflammation in your body. It also treats arthritis.
Burdock can be consumed as a decoction once or twice a day.
Passionflower
Passionflower is helpful for slipped discs because the essential oils present is antispasmodic in nature. It reduces pain and inflammation.
You can massage with passionflower essential oil or take capsules made from it, however, do consult your doctor before taking capsules.
Additional Tips
If you are overweight, try to lose some pounds.
Exercise every day.
Lift things in a proper way, as guided by a therapist. Do not lift heavy weights.
Stop smoking and drinking.
Always make sure you are in the right posture whatever activity you may be doing.
Wear flat and soft shoes. Avoid heels.
Walk and move around cautiously.
Slipped discs can be really painful but with the right treatment and precautions you can become as fit as you were before. So start taking home remedies and consult a doctor whenever you feel any kind of severe pain.
Women’s Health Tips for Heart/Looking for the path toward a healthier you? It’s not hard to find. The journey begins with some simple tweaks to your lifestyle. The right diet, exercise, and stress-relief plan all play a big role.All you ladies looking to stay healthy inside and out then read further.
Follow a heart-healthy diet
Try whole wheat bread, whole wheat pasta, brown rice.
Eat a lot of fruits and veggies
Eat lean proteins like fish, poultry, beans, and legumes
Cut down on salt, sugar, processed food and saturated fats.
Exercise regularly
Excersing regularly boosts your heart health, builds muscles and wards off health problems. Regular exercise offers incredible benefits for your body and mind.
Lose weight
Shedding pounds helps you lower the risk of heart disease, type 2 diabetes, and cancer.
This means you’ll have to increase your exercise and improve your diet by avoiding everyday items that contain heavy sugar and salt, like coffee, soda, or salad dressing.
Cut down stress
Stress is not only taking a toll on your mentality but also affects you physically. Over time, your body and heart could really suffer from built-up stress. To relieve some stress try these simple tips like yoga, exercise, deep breathing, a massage, healthy eating and talking to someone you trust or a counselor
Your health is extremely important to make it a priority! It’s not that hard to improve your body, mind, and soul. You just have to be mindful and put forward a concentrated effort. Do it for yourself and your future.
Follow a Heart-Healthy Diet
There’s an easy recipe if your goal is to keep away problems like heart disease and strokes.
Eat more fruits and veggies.
Choose whole grains. Try brown rice instead of white. Switch to whole wheat pasta.
Choose lean proteins like poultry, fish, beans, and legumes.
Cut down on processed foods, sugar, salt, and saturated fat.
When eating healthy, flexibility often works best, says Joyce Meng, MD, assistant professor at the Pat and Jim Calhoun Cardiology Center at UConn Health. If you like to follow a strict diet plan, go for it. If not, it’s OK. “Find what works for you.”
Looking for the path toward a healthier you? It’s not hard to find. The journey begins with some simple tweaks to your lifestyle. The right diet, exercise, and stress-relief plan all play a big role.
There’s an easy recipe if your goal is to keep away problems like heart disease and strokes.
• Eat more fruits and veggies.
• Choose whole grains. Try brown rice instead of white. Switch to whole wheat pasta.
• Choose lean proteins like poultry, fish, beans, and legumes.
• Cut down on processed foods, sugar, salt, and saturated fat.
• Move your body: Engage in daily exercise.
• Regular exercise offers incredible benefits for your body and mind.
• Exercise boosts your heart health, builds muscle and bone strength, and wards off health problems.Not only does exercise keep the body young, but it also keeps the mind vital and promotes emotional well-being. the powerful effect of exercise on many of the bio markers of ageing, including muscle mass, strength, aerobic capacity, bone density, and cholesterol.
• Focus on weight
• When you shed pounds you’ll lower your risk of heart disease, type 2 diabetes, and cancer.
• Aim for a slow, steady drop. Try to lose 1-2 pounds a week by being active and eating better.
• Drink clean water
• Get a filtration system for your drinking water. Fluoride is not good for your body.
• Meditate
• Set some time aside each day to rest your mind.
• Take time for restful sleep.
• Sleep is regenerative for your body. The more sleep you get the better you will perform the next day.
• Cut Down Your stress
To relieve stress, try:
• Deep breathing
• Meditation
• Yoga
• Massage
• Exercise
• Healthy eating
• Talking to a friend, family member, or professional counselor
If the article is helpful, please Click to Star Icon and Rate This
Post!
Sympathetic nerves run on the front surface of the spinal column and not in the spinal canal with the nerves that provide sensation and strength to your legs. The sympathetic nerves are part of the autonomic nervous system, which basically controls functions such as blood flow and temperature regulation to the arms and legs, sweating, heart rate, digestion, and blood pressure.
sympathetic nerves syatem:
What are the sympathetic nerves and why are sympathetic blocks helpful?
Nervous SystemThe autonomic nervous system is responsible for controlling bodily functions that you do not think about or have direct control over. However, there is a connection between the central nervous system (that you have control over) and the autonomic nervous system. Regulation of the connection can become altered, usually secondary to an injury. When regulation of the sympathetic nervous system is altered, various pain states can occur including complex regional pain syndrome, also known as Reflex Sympathetic Dystrophy(RSD).
What is a sympathetic block and why is it helpful?
A sympathetic nerve block involves injecting numbing medicine around the sympathetic nerves in the low back or neck. By doing this, the sympathetic nervous system in that area is temporarily ‘switched’ off in hopes of reducing or eliminating pain. If pain is substantially improved after the block, then a diagnosis of sympathetically mediated pain is established. The therapeutic effects of the anesthetic can occur, at times, longer than would be normally expected. The goal is to reset the sympathetic tone to a normal state of regulation. If the initial block is successful, then additional blocks may be repeated if the pain continues to sequentially diminish.
What will happen to me during the procedure?
An IV will be started for safety, and so relaxation medicine can be given if needed. After lying on an x-ray table, the skin over the area to be injected will be well cleansed. Next, the physician will numb a small area of skin with numbing medicine (anesthetic) which stings for a few seconds. The physician will use x-ray guidance to direct a needle to the sympathetic plexus of nerves. The physician will then inject contrast dye to confirm that the medicine only goes over the targeted sympathetic nerves. Once this occurs, numbing medicine (anesthetic) will then be slowly injected.
What should I do and expect after the procedure?
20-30 minutes after the procedure you will move the affected area to try to provoke your usual pain. You may or may not obtain improvement in the first few hours after the injection depending upon if the sympathetic nerves are carrying your pain signals. You may notice increased warmth in the affected extremity for 4-18 hours after the block. If the sympathetic nerves in the neck are injected (stellate ganglion), you will also notice a slight drooping of the eyelid and redness of the eye for several hours. This is normal, and will resolve over 4-18 hours. You should report your remaining pain (if any) and record the relief you experience during the next week on a “pain diaryâ we will provide. *Mail or fax the completed pain diary back one week after the injection so that your treating physician can be informed of your results and plan future tests and/or treatment if needed.
www.rxharun.com
You may notice a slight increase in your pain lasting for several days as the numbing medicine wears off. You might also experience mild pain at the injection site for several days. Ice will typically be more helpful than heat in the first 2-3 days after the injection. You may take your regular medicines after the procedure, but try to limit your pain medicines the first 4-6 hours after the procedure so that the diagnostic information obtained is accurate.
On the day of the injection, you should not drive and should avoid any strenuous activities. On the day after the procedure, you may return to your regular activities. If your pain is improved from this procedure, start your regular exercise/activities in moderation. Even if you are significantly improved, gradually increase your activities over 1-2 weeks to avoid recurrence of your pain.
Unless specified otherwise in the boxes, the source is: Moore, Keith L.; Agur, A. M. R. (2002). Essential Clinical Anatomy (2nd ed.). Lippincott Williams & Wilkins. p. 199. ISBN978-0-7817-5940-3.
änig, Wilfrid (2006). The integrative action of the autonomic nervous system : neurobiology of homeostasis. Cambridge: UK. pp. 132–135. ISBN9780521845182.
Robert Ornstein (1992). The Evolution of Consciousness: of Darwin, Freud, and Cranial Fire: The Origins of the Way We Think. New York: Simon & Schuster. ISBN0-671-79224-5.
বিশ্ব ভালবাসা দিবস” বা ”ভ্যালেন্টাইনস ডে”-এর পটভূমি
বিশ্ব ভালবাসা দিবস” বা ”ভ্যালেন্টাইনস ডে”-এর পটভূমি
১৪ ই ফেব্রুয়ারি সারাবিশ্বে বেশ পরিচিত একটি নাম “বিশ্ব ভালবাসা দিবস” বা ”ভ্যালেন্টাইনস ডে”। একজন ভালোবাসা প্রেমী ও সচেতন মানুষ হিসাবে ”ভ্যালেন্টাইনস ডে” কি? এর পেছনের লুকানো ইতিহাস আসলে কি? আমি মনে করি একজন সচেতন মানুষ কোন কাজ করার আগেই সে কাজটি সম্পর্কে অন্ততঃপক্ষে সেটা জানার চেষ্টা করবেন। ”ভ্যালেন্টাইনস ডে” সম্পর্কে এখন বোধহয় পরিস্কার ধারনা থাকা অপরিহার্য হয়ে দেখাদিয়েছে।
ভ্যালেন্টাইনস ডে যেভাবে আসলঃ
প্রথমঃ রোমের সম্রাট দ্বিতীয় ক্লডিয়াস-এর আমলের ধর্মযাজক সেন্ট ভ্যালেনটাইন ছিলেন শিশুপ্রেমিক, সামাজিক ও সদালাপী এবং খৃষ্টধর্ম প্রচারক। আর রোম সম্রাট ছিলেন বিভিন্ন দেব-দেবীর পূজায় বিশ্বাসী। ঐ সম্রাটের পক্ষ থেকে তাকে দেব-দেবীর পূজা করতে বলা হলে ভ্যালেন্টাইন তা অস্বীকার করায় তাকে কারারুদ্ধ করা হয়। সম্রাটের বারবার খৃষ্টধর্ম ত্যাগের আজ্ঞা প্রত্যাখ্যান করলে ২৭০ খৃস্টাব্দের ১৪ ফেব্রুয়ারি রাষ্ট্রীয় আদেশ লঙ্ঘনের দায়ে ভ্যালেন্টাইনকে মৃত্যুদন্ড প্রদান করেন।
দ্বিতীয়ঃ সেন্ট ভ্যালেন্টাইন কারারুদ্ধ হওয়ার পর প্রেমাসক্ত যুবক-যুবতীদের অনেকেই প্রতিদিন তাকে কারাগারে দেখতে আসত এবং ফুল উপহার দিত। তারা বিভিন্ন উদ্দীপনামূলক কথা বলে সেন্ট ভ্যালেন্টাইনকে উদ্দীপ্ত রাখত। এক কারারক্ষীর এক অন্ধ মেয়েও ভ্যালেন্টাইনকে দেখতে যেত। অনেকক্ষণ ধরে তারা দু’জন প্রাণ খুলে কথা বলত। এক সময় ভ্যালেন্টাইন তার প্রেমে পড়ে যায়। সেন্ট ভ্যালেন্টাইনের আধ্যাত্মিক চিকিৎসায় অন্ধ মেয়েটি দৃষ্টিশক্তি ফিরে পায়। ভ্যালেন্টাইনের ভালবাসা ও তার প্রতি দেশের যুবক-যুবতীদের ভালবাসার কথা সম্রাটের কানে গেলে তিনি ক্ষিপ্ত হয়ে ২৬৯ খৃষ্টাব্দের ১৪ ফেব্রুয়ারি তাকে মৃত্যুদন্ড দেন।
তৃতীয়ঃ খৃষ্টীয় ইতিহাস মতে, ২৬৯ খৃষ্টাব্দের কথা। সাম্রাজ্যবাদী, রক্তপিপাষু রোমান সম্রাট ক্লডিয়াসের দরকার এক বিশাল সৈন্যবাহিণীর। এক সময় তার সেনাবাহিনীতে সেনা সংকট দেখা দেয়। কিন্তু কেউ তার সেনাবাহিনীতে যোগ দিতে রাজি নয়। সম্রাট লক্ষ্য করলেন যে, অবিবাহিত যুবকরা যুদ্ধের কঠিন মুহূর্তে অত্যধিক ধৈর্যশীল হয়। ফলে তিনি যুবকদের বিবাহ কিংবা যুগলবন্দী হওয়ার উপর নিষেধাজ্ঞা জারী করেন। যাতে তারা সেনাবাহিনীতে যোগ দিতে অনীহা প্রকাশ না করে। তার এ ঘোষণায় দেশের যুবক-যুবতীরা ক্ষেপে যায়। যুবক সেন্ট ভ্যালেন্টাইন নামের এক ধর্মযাজকও সম্রাটের এ নিষেধাজ্ঞা কিছুতেই মেনে নিতে পারেননি। প্রথমে তিনি সেন্ট মারিয়াসকে ভালবেসে বিয়ের মাধ্যমে রাজার আজ্ঞাকে প্রত্যাখ্যান করেন এবং তার গীর্জায় গোপনে বিয়ে পড়ানোর কাজও চালাতে থাকেন। একটি রুমে বর-বধূ বসিয়ে মোমবাতির স্বল্প আলোয় ভ্যালেন্টাইন ফিস ফিস করে বিয়ের মন্ত্র পড়াতেন। কিন্তু এ বিষয়টি এক সময়ে সম্রাট ক্লডিয়াসের কানে গেলে সেন্ট ভ্যালেন্টাইনকে গ্রেফতারের নির্দেশ দেন। ২৭০ খৃষ্টাব্দের ১৪ ফেব্রুয়ারি সৈন্যরা ভ্যালেন্টাইনকে হাত-পা বেঁধে টেনে-হিঁচড়ে সম্রাটের সামনে হাজির করলে তিনি তাকে হত্যার আদেশ দেন।
চতুর্থঃ আরেকটি খৃষ্টীয় ইতিহাস মতে, গোটা ইউরোপে যখন খৃষ্টান ধর্মের জয়জয়কার, তখনও ঘটা করে পালিত হতো রোমীয় একটি রীতি। মধ্য ফেব্রুয়ারিতে গ্রামের সকল যুবকরা সমস্ত মেয়েদের নাম চিরকুটে লিখে একটি পাত্রে বা বাক্সে জমা করত। অতঃপর ঐ বাক্স হতে প্রত্যেক যুবক একটি করে চিরকুট তুলত, যার হাতে যে মেয়ের নাম উঠত, সে পূর্ণবৎসর ঐ মেয়ের প্রেমে মগ্ন থাকত। আর তাকে চিঠি লিখত, এ বলে ‘প্রতিমা মাতার নামে তোমার প্রতি এ পত্র প্রেরণ করছি।’ বৎসর শেষে এ সম্পর্ক নবায়ন বা পরিবর্তন করা হতো। এ রীতিটি কয়েকজন পাদ্রীর গোচরীভূত হলে তারা একে সমূলে উৎপাটন করা অসম্ভব ভেবে শুধু নাম পাল্টে দিয়ে একে খৃষ্টান ধর্মায়ণ করে দেয় এবং ঘোষণা করে এখন থেকে এ পত্রগুলো ‘সেন্ট ভ্যালেনটাইন’-এর নামে প্রেরণ করতে হবে। কারণ এটা খৃষ্টান নিদর্শন, যাতে এটা কালক্রমে খৃষ্টান ধর্মের সাথে সম্পৃক্ত হয়ে যায়।
পঞ্চমঃ অন্য আরেকটি মতে, প্রাচীন রোমে দেবতাদের রাণী জুনোর সম্মানে ১৪ ফেব্রুয়ারি ছুটি পালন করা হতো। রোমানরা বিশ্বাস করত যে, জুনোর ইশারা-ইঙ্গিত ছাড়া কোন বিয়ে সফল হয় না। ছুটির পরদিন ১৫ ফেব্রুয়ারি লুপারকালিয়া ভোজ উৎসবে হাজারও তরুণের মেলায় র্যাফেল ড্র’র মাধ্যমে সঙ্গী বাছাই প্রক্রিয়া চলত। এ উৎসবে উপস্থিত তরুণীরা তাদের নামাংকিত কাগজের সি¬প জনসম্মুখে রাখা একটি বড় পাত্রে ফেলত। সেখান থেকে যুবকের তোলা সি¬পের তরুণীকে কাছে ডেকে নিত। কখনও এ জুটি সারা বছরের জন্য স্থায়ী হত এবং ভালবাসার সিঁড়ি বেয়ে বিয়েতে গড়াতো।
ঐ দিনের শোক গাঁথায় আজকের এই “ভ্যালেন্টাইন ডে”।
বাংলাদেশে ভ্যালেন্টাইনস ডে যেভাবে আসলঃ
১৯৯৩ সালের দিকে বাংলাদেশে বিশ্ব ভালবাসা দিবসের আর্বিভাব ঘঠে। যায় যায় দিন পত্রিকার সম্পাদক শফিক রেহমান। তিনি পড়াশোনা করেছেন লন্ডনে। পাশ্চাত্যের ছোঁয়া নিয়ে দেশে এসে লন্ডনী সংস্কৃতির প্র্যাকটিস শুরু করেন। তিনি প্রথম যায় যায় দিন পত্রিকার মাধ্যমে বিশ্ব ভালবাসা দিবস বাংলাদেশীদের কাছে তুলে ধরেন। তেজগাঁওয়ে তার পত্রিকা অফিসে কেউ চাকরী নিতে গেলে না কি সাথে তার গার্লফ্রেন্ডকে নিয়ে যেতে হতো। প্রেমের যুগললবন্দী কপোত-কপোতীকে দেখে ওনি না কি খুব খুশী হতেন। অভিধা প্রথম ব্যবহার করেন শফিক রেহমান। এজন্য শফিক রেহমানকে বাংলাদেশে ভালবাসা দিবসের জনক বলা হয়।
সুত্রঃপ্রথম আলো ব্লগ
আমার কিছু কথাঃআগামীকাল ভালোবাসা দিবস।শুধু বাঙ্গালীরা নয় সমগ্র পৃথিবীবাসী ভাসবে নতুন এক প্রেমের জোয়ারে, হাজার কোটি টাকা হয়ত খরচ হবে প্রিয়জনকে বিভিন্ন ধরনের অসাধারণ গিফট কিনে দিতে গিয়ে, এ যেন এক তুমুল প্রতিযোগিতা কে তার প্রিয়জনের কাছে নিজেকে কত বেশি আলাদাভাবে উপস্থাপন করতে পারে……তবুও আমি আজ কিছু কথা বলতে চাই,আমাকে বলার সুযোগ দিতেই হবে…………আপনি হয়ত আপনার কাছের মানুষগুলোকে ভালোবেসে হাজার হাজার টাকার গিফট কিনে দেবেন,কিন্তু একটু আপনার আশেপাশে খোঁজ নিয়ে দেখবেন যে হয়ত এই দিনে একটি শিশু মায়ের বুকের দুধ খাওয়ার জন্য অঝরে কাদছে,কিন্তু তার অসহায় দরিদ্র মা-বাবা তাকে কিছুই দিতে পারছে না,হয়ত একটি শিশু স্কুলে তার নতুন বছর শুরু করেছে,কিন্তু টাকার অভাবে হয়ত সে কোন নতুন জামা পরে স্কুলে যেতে পারছে না,চাইলে হয়ত এমন হাজার হাজার উদাহারন দেওয়া সম্ভব হবে,কিন্তু আপনার নিজের যদি একটু উপলব্ধি হয় যে আমার প্রিয় মানুষটিকে হাজার টাকা দিয়ে কোন উপহার না দিয়ে তার থেকে অল্প কিছু টাকা কোন দরিদ্র শিশুকে দেওয়া হয় তাহলে তার ঐ হাসিটার মত আনন্দ মনে হয় পৃথিবীতে আর কোথাও খুজে পাওয়া যাবে না,তাই আসুন না এবার ভ্যালেন্টাইনটা না হয় একটু অন্যভাবেই করলাম….
If the article is helpful, please Click to Star Icon and Rate This
Post!
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Proin ut odio tellus. Maecenas consectetur adipiscing elit Lorem ipsum dolor sit amet, consectetur adipiscing elit. Proin ut odio tellus.
If the article is helpful, please Click to Star Icon and Rate This
Post!
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Proin ut odio tellus. Maecenas consectetur adipiscing elit Lorem ipsum dolor sit amet, consectetur adipiscing elit. Proin ut odio tellus.
If the article is helpful, please Click to Star Icon and Rate This
Post!
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Proin ut odio tellus. Maecenas consectetur adipiscing elit Lorem ipsum dolor sit amet, consectetur adipiscing elit. Proin ut odio tellus.
If the article is helpful, please Click to Star Icon and Rate This
Post!
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Proin ut odio tellus. Maecenas consectetur adipiscing elit Lorem ipsum dolor sit amet, consectetur adipiscing elit. Proin ut odio tellus.
If the article is helpful, please Click to Star Icon and Rate This
Post!
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Proin ut odio tellus. Maecenas consectetur adipiscing elit Lorem ipsum dolor sit amet, consectetur adipiscing elit. Proin ut odio tellus.
If the article is helpful, please Click to Star Icon and Rate This
Post!
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Proin ut odio tellus. Maecenas consectetur adipiscing elit Lorem ipsum dolor sit amet, consectetur adipiscing elit. Proin ut odio tellus.
If the article is helpful, please Click to Star Icon and Rate This
Post!
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Proin ut odio tellus. Maecenas consectetur adipiscing elit Lorem ipsum dolor sit amet, consectetur adipiscing elit. Proin ut odio tellus.
If the article is helpful, please Click to Star Icon and Rate This
Post!



































































{kind=link}
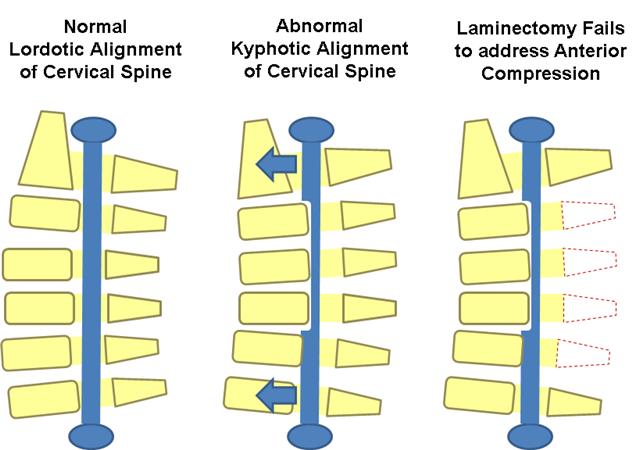{kind=link}
{kind=link}