Preparing Your Spa Experience at Home
Preparing Your Spa Experience at Home/Sometimes it feels as though [...]
Preparing Your Spa Experience at Home/Sometimes it feels as though [...]
How a Swim Spa Can Help You Live a Healthier [...]
Swimming spa is a multifunctional machine that combines the best [...]
What movement does the pectoralis major perform?/Pectoralis major is the [...]
How To Strength of The Pectoralis Muscle?/Pectoralis major is the [...]
How can I strengthen my breast muscles/ Pectoralis Major/Pectoralis major [...]
What Exercise Strengthens Pectoralis Major/Pectoralis major is the superior most [...]
Can you walk with a Jumper's the knee?/Jumper's the knee [...]
Prepatellar Bursitis is a condition where the bursa in the [...]
Swimmer’s shoulder is an umbrella term covering a range of [...]
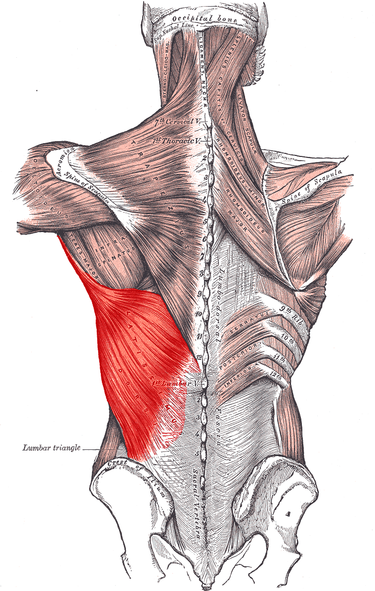
Latissimus Dorsi Muscle Pain/Latissimus Dorsi Muscle is a broad, flat [...]
Treatment Rehabilitation of Triceps Tendon Rupture/Triceps Tendon Tear is a large, [...]
We Inspire with our business services
through the agency’s dream to strive for
the excellence.
© Avada Studio • All rights reserved.
Powered by WordPress