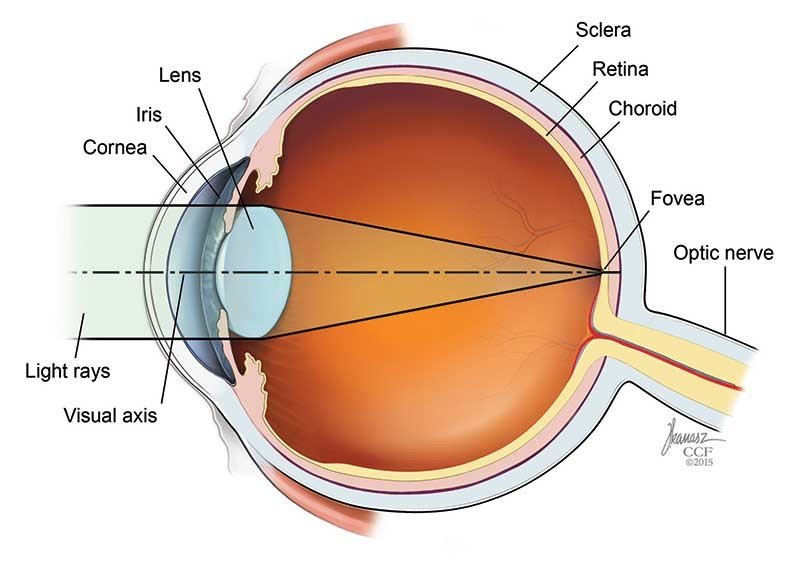
Farsightedness, also known as hyperopia, is an eye condition that causes blurry near vision. People who are farsighted have more trouble seeing things that are close up (such as when reading or using a computer) than things that are far away (such as when driving). For normal vision, light passes through the clear cornea at the front of the eye and is focused by the lens onto the surface of the retina, which is the lining of the back of the eye that contains light-sensing cells. Some people who are farsighted have eyeballs that are too short from front to back. Others have a cornea or lens that is abnormally shaped.
Far-sightedness, also known as hyperopia, is a condition of the eye in which light is focused behind, instead of on, the retina.[rx] This results in close objects appearing blurry, while far objects may appear normal.[rx] As the condition worsens, objects at all distances may be blurry.[rx] Other symptoms may include headaches and eye strain.[rx] People may also experience accommodative dysfunction, binocular dysfunction, amblyopia, and strabismus.[rx]
Types of Farsightedness
Choroid folds in high hyperopia (fluorescein angiography)
Hyperopia is typically classified according to clinical appearance, its severity, or how it relates to the eye’s accommodative status. There are three clinical categories of hyperopia.[rx]
Simple hyperopia – Occurs naturally due to biological diversity.
Pathological hyperopia – Caused by disease, trauma, or abnormal development.
Functional hyperopia – Caused by paralysis that interferes eye’s ability to accommodate.
There are also three categories severity
Low – Refractive error less than or equal to +2.00 diopters (D).
Moderate – Refractive error greater than +2.00 D up to +5.00 D.
High – Refractive error greater than +5.00 D.
Other common types of refractive errors are near-sightedness, astigmatism, and presbyopia.[rx]
Causes of Farsightedness
As hyperopia is the result of the visual image being focused behind the retina, it has two main causes
Farsightedness develops when the cornea and lens focus light behind the retina (back of the eye where images are formed) instead of on it. This problem with focusing can result from:
An eyeball that is too short (from front to back)
A flat shaped cornea (clear layer covering the front of the eye) or lens (clear disc that changes shape as it focuses)
The lens becomes less flexible after about age 40 because of changes in its proteins.
Muscles around the lens that help it change shape to focus may lose elasticity.
These age-related changes make it more difficult for your eyes to focus on close objects. You may notice that you need to hold reading material farther away to be able to see clearly enough to read.
Low converging power of eye lens because of weak action of ciliary muscles
Abnormal shape of the cornea
Far-sightedness is often present from birth, but children have a very flexible eye lens, which helps to compensate.[rx]
In rare instances hyperopia can be due to diabetes, and problems with the blood vessels in the retina.[rx]
Difficulty reading small print without holding reading material at arm’s length
Difficulty seeing objects up close
Fatigue or headache after performing tasks that require close focus, such as reading or sewing
Farsightedness and presbyopia have different causes:
Farsightedness occurs because the eye is too short and attempts to focus the image behind the retina (back of the eye). It usually is present at birth or develops in early childhood.
Presbyopia occurs because the lens becomes more rigid with age, making it di
Difficulty seeing with both eyes (binocular vision) may occur, as well as difficulty with depth perception.[rx]
You have eyestrain, including burning eyes, and aching in or around the eyes
You experience general eye discomfort or a headache after a prolonged interval of conducting close tasks, such as reading, writing, computer work or drawing
Diagnosis of Farsightedness
You may have several of the following tests during the exam:
Refraction test – Your optometrist determines your prescription for glasses, soft contact lenses or hard contact lenses with a phoropter, a device with lenses of different strengths.
Retinal exam – The optometrist uses special eye drops to dilate your pupils, then examines the inside of your eye with a lighted instrument called an ophthalmoscope.
Tonometry test – Our eye specialists measure pressure inside the eye using either a microscope and high-intensity light or an instrument that carefully touches the surface of the eye. High pressure can indicate glaucoma.
Vision acuity test – This test uses an eye chart to assess your vision sharpness.
Several methods can be used for genetic testing
Molecular genetic tests (or gene tests) study single genes or short lengths of DNA to identify variations or mutations that lead to a genetic disorder.
Chromosomal genetic tests analyze whole chromosomes or long lengths of DNA to see if there are large genetic changes, such as an extra copy of a chromosome, that cause a genetic condition.
Biochemical genetic tests study the amount or activity level of proteins; abnormalities in either can indicate changes to the DNA that result in a genetic disorder.
The American Academy of Ophthalmology (AAO) recommends the following intervals for eye exams
Before age 3 – Vision screening during regular pediatric exams
Age 3 to 19 – Vision screening every one to two years
Age 20 to 39 – Complete eye exam to evaluate vision and check for eye diseases at least once by age 29 and at least twice by age 39
Age 40 to 64
Baseline screening for eye diseases at age 40, after which your eye specialist can recommend follow-up intervals.
Vision testing each year for people who wear glasses or contact lenses
Vision testing every two to four years for people with no vision or eye conditions
Age 65 and over – Complete eye exam every one to two years to check for eye diseases and evaluate vision sharpness.
Treatment of Farsightedness
Your prescription will often contain three numbers for each of your eyes. These are:
Cyl (cylinder) – this number will show whether or not you have astigmatism (a common eye condition where your lens or cornea isn’t perfectly curved – this can cause distorted or blurred vision) in either of your eyes
Axis – describes the angle of astigmatism detailed above – if you have one
Sph (sphere) – a negative number indicates you’re shortsighted, while a positive number will show you’re long sighted (have hyperopia)
Corrective lenses
The simplest form of treatment for far-sightedness is the use of corrective lenses, eyeglasses or contact lenses.[rx][rx] Eyeglasses used to correct far-sightedness have convex lenses.
Glasses – can be an easy way to improve vision. Prescription glasses can fix refractive errors by altering the angle light rays enter the eye. Depending on your style and budget, there is an enormous selection of frames and eyeglass lenses to choose from.
Contact lenses – work under the same principles as glasses. Contact lenses differ in materials (hard and soft) and duration of use (daily disposables or extended wear). It is important to understand that contact lenses are not without risks.
Intraocular lens exchange – is another option that a doctor may recommend to correct hyperopia in certain patients. This is a surgical procedure in which an artificial lens is implanted in place of the natural lens. Intraocular lens exchange is a common procedure for patients suffering from cataracts, while refractive or clear lens exchange refers to patients without cataract. Your doctor can recommend this if it is an option for you as well as which IOL is right for you and your refractive error. Like all surgeries though, it is not without risks.
Phakic intraocular lens (PIOL) – is an artificial lens, which is implanted in addition to the existing natural lens, and is used in refractive surgery to change the eye’s optical power. Like all surgeries though, it is not without risks.
Bifocal contact lenses
Rigid gas permeable (RGP) lenses, the latest generation of hard contact lenses
Soft lenses
Hybrid lenses, which have an RGP center surrounded by a soft lens outer ring
Eyeglasses
Bifocal with the top portion of the lens for far vision and the bottom portion for near
Progressives, which are similar to bifocals but the lens sections are blended together rather than having a distinct separation between them
Reading glasses to correct the near vision and help the person read and do other close tasks
Surgery
There are also surgical treatments for far-sightedness
Photorefractive keratectomy (PRK) – Removal of a minimal amount of the corneal surface[rx][rx]
Laser assisted in situ keratomileusis (LASIK) – Laser eye surgery to reshape the cornea, so that glasses or contact lenses are no longer needed.[rx][rx] It is another option to treat hyperopia. LASIK and PRK/LASEK both treat refractive errors. At this time, SMILE cannot treat hyperopia. Like all surgeries though, they are not without risks.
Refractive lens exchange (RLE) – A variation of cataract surgery where the natural crystalline lens is replaced with an artificial intraocular lens; the difference is the existence of abnormal ocular anatomy which causes a high refractive error.[rx]
Laser epithelial keratomileusis (LASEK) – Resembles PRK, but uses alcohol to loosen the corneal surface.[rx]
Computer vision syndrome is a group of eye and vision-related problems that result from prolonged computer, tablet, e-reader and mobile phone use. Individuals may present in pharmacies complaining of eye discomfort and vision problems, so pharmacists and pharmacy teams should be able to distinguish which factors may be at play for particular patients.
Individuals are spending more time using digital devices, which is linked to more people experiencing eye discomfort and vision problems.
Computer vision syndrome (CVS) is the combination of eye and vision problems associated with the use of computers. In modern western society the use of computers for both vocational and avocational activities is almost universal. However, CVS may have a significant impact not only on visual comfort but also occupational productivity since between 64% and 90% of computer users experience visual symptoms which may include eyestrain, headaches, ocular discomfort, dry eye, diplopia and blurred vision either at near or when looking into the distance after prolonged computer use. This paper reviews the principal ocular causes for this condition, namely oculomotor anomalies and dry eye. Accommodation and vergence responses to electronic screens appear to be similar to those found when viewing printed materials, whereas the prevalence of dry eye symptoms is greater during computer operation. The latter is probably due to a decrease in blink rate and blink amplitude, as well as increased corneal exposure resulting from the monitor frequently being positioned in primary gaze. However, the efficacy of proposed treatments to reduce symptoms of CVS is unproven. A better understanding of the physiology underlying CVS is critical to allow more accurate diagnosis and treatment. This will enable practitioners to optimize visual comfort and efficiency during computer operation.[Rx]
Common symptoms related to computer vision syndrome and its pathophysiological mechanisms
To evaluate the Chakshushya activity of both the drugs, whole importance was given to the subjective complaints as no particular objective findings have been mentioned or available for diagnosis of this disease so far. So, in this present study, routine hematological investigations, routine eye examination including intraocular pressure, visual acuity and slit lamp examination, were carried out to exclude any other ocular pathology.
Inclusion criteria
Patients between 16 and 75 years of age.
Computer users complaining of eye strain, dry eyes, blurred vision, redness, burning eyes, excessive tears, double vision, headache, glare sensitivity, fatigue, neck, shoulder and back pain.
Patients having minimum three symptoms of CVS.
Minimum 1 hour exposure to any type of VDT like desktop, laptop or both.
Minimum 1 year exposure to any type of above-mentioned VDTs.
Exclusion criteria
Patients of age below 16 years or above 75 years.
Those having symptoms due to direct physiological effects of substance (e.g., drug abuse, medication) or a general medical condition (e.g., hypothyroidism).
Patients suffering from infectious conditions of the eye like conjunctivitis, scleritis, uveitis, glaucoma, stye, blepharitis, etc.
Patients having any fundus pathology like optic atrophy, diabetic retinopathy, hypertensive retinopathy, papilledema, etc.
In 2016, The Pharmaceutical Journal joined forces with UK health company RB to gauge how commonly dry eye is seen in the pharmacy and devised an independent editorial campaign to address the learning needs of pharmacists. This culminated in the publication of a print supplement ‘Focus: Dry eye’ and the production of The Pharmacy Learning Centre, a dedicated learning resource on the treatment, and management of eye conditions in pharmacy.
The prolonged use of digital devices has contributed to an increase in ‘computer-related’ ocular symptoms, called computer vision syndrome (CVS). CVS is often linked with dry eye disease, therefore, this article aims to build on the previous work and support pharmacists in discussing how lifestyle factors, including screen and device use, are associated with dry eye symptoms.
The prolonged use of digital devices has contributed to an increase of ‘computer-related’ ocular symptoms called computer vision syndrome (CVS), also known as digital eye fatigue. Research has found that around 75% of the population working in front of a screen for 6–9 hours daily complain of some ocular discomfort. Office-based studies have shown the prevalence of CVS to be higher in women than men, but similar between contact lens and spectacle wearers.
CVS broadly relates to ocular discomfort associated with prolonged computer use, but the time spent using screens, especially handheld devices, is increasing inexorably in our day-to-day activities, and avoiding screen use is not a possibility for many people. Indeed, it is estimated that children and young adults now spend around six hours a day using screens, including the use of multiple mobile devices.
This article aims to help pharmacists and healthcare professionals to identify the causes of ocular discomfort and how they can help patients manage their symptoms effectively.
Identifying CVS
Symptoms of CVS can be divided into four categories:
Eye strain (asthenopia);
Dry or painful eyes relating to the ocular surface;
Difficulty focusing (visual blur);
Or non-ocular symptoms.
Asthenopia can be defined through non-specific symptoms such as fatigue, pain in or around the eyes, headache, or even double vision. In patients with dry eye disease (see Box 1: ‘What is dry eye disease?’), the ocular surface dries out, causing scratchy, tired, irritated eyes, which may become worse with contact lens use. Refractive errors may result in complaints of blurred vision, slow focusing, double vision or difficulty focusing for close work (presbyopia). Non-ocular symptoms include neck, back or shoulder pain. Patients with CVS quite often have a range of symptoms from more than one category, and the pharmacist or pharmacy team may need to work out which of these may be associated with the condition in order to recommend the most appropriate treatment. In some patients, symptoms of dry eye disease may be accompanied by symptoms of anxiety relating to work, or even depression.
Box 1: What is dry eye disease?
The Tear Film and Ocular Surface Society (TFOS) International Dry Eye Workshop (DEWS) II report and guidelines, published in 2017, provides the following defintion for dry eye: “Dry eye is a multifactorial disease of the ocular surface characterised by a loss of homeostasis of the tear film, and accompanied by ocular symptoms, in which tear film instability and hyperosmolarity, ocular surface inflammation and damage, and neurosensory abnormalities play aetiological roles.”
There are two types of dry eye disease, which can occur individually or in combination:
Evaporative dry eye is associated with an insufficient oily layer in the tear film, which can occur when the meibomian glands are damaged. Around 80% of patients with dry eye disease are affected by this type;
Aqueous deficient dry eye, on the other hand, occurs when the lacrimal glands do not produce enough of the watery component of tears to maintain a healthy eye surface.
Differentiating the causes of CVS
Pharmacists may be the first point of contact for someone who is complaining of dry or tired eyes, therefore, they need to distinguish which factors might be at play for particular patients and if screen use is one of the root causes.
Does the patient have difficulty focusing on the screen?
Refractive errors resulting from uncorrected long-sight (hyperopia), astigmatism or presbyopia may add to visual stress on the eye. While actual eyesight may be reasonable, correction of relatively small refractive errors can significantly reduce eye fatigue and other CVS symptoms.
In particular, older people may have glasses for distance correction and/or reading glasses, but computer screens are at an intermediate distance, so neither lens enables comfortable focus. Consequently, the patient is uncomfortable in trying to accommodate (pull focus back) to see the screen clearly, or over-corrects by leaning forward to read the screen comfortably.
Similarly, early middle-aged people (in their 40s) may struggle with prolonged reading, owing to presbyopia, and may need some “plus” lens correction. Patients with dry eye may also complain of blurred vision; however, unlike refractive error, this will usually improve with a blink.
Does the patient have double vision or need to close one eye to read comfortably?
Looking at objects close up (particularly handheld devices) stimulates convergence of the eyes, and difficulties with binocular vision can sometimes result in double vision, eye strain, fatigue and headaches. These symptoms are mostly transient because they ease after resting the eyes away from a digital device, and they are not a problem when looking into the distance.
Intermittent double vision (diplopia) may be caused by convergence insufficiency, where the eyes do not converge as well as they should. This is associated with some medical conditions (e.g. Parkinson’s disease), but is not uncommon in the general population. More rarely, convergence excess can cause difficulties with binocular vision, but this usually occurs in children. Some adults have a latent squint, and sustained close work can also cause them to be symptomatic.
Do the patient’s eyes feel dry, tired and scratchy with initial good vision that blurs, which is helped by a blink?
Dry eyes may be described as gritty or sore with eye redness. Many aspects of computer use can predispose a person to dry eye disease, as well as having a reduced tear film, which may be because of too little water (aqueous deficiency) or increased evaporation because of a poor-quality tear film (evaporative dry eye) — see Box 1. For example, the tear film is replenished after every blink and studies have shown the blink rate to significantly reduce during long, concentrated hours on digital devices.
Furthermore, the environment (hot, dry air being circulated in sealed offices) adds to dry eye symptoms. Some studies suggest a strong correlation between ocular surface disease symptom scores and the frequency and severity of CVS episodes.
The impact of dry eye discomfort can be greater among contact lens wearers because a well-functioning tear film plays a vital role in good lens fitting and movement. Older contact lens wearers tend to be most symptomatic as tear production generally decreases with age. Pharmacists should consider additional factors when advising contact lens wearers on treatments for dry eye, see ‘Treatments for dry eye disease’, later.
Does the patient have neck/backache when using the computer?
Work stress and environmental working conditions may cause a person to adopt a posture in front of their screen to see better, while causing neck and back strain. The symptoms may present as neck, back or shoulder ache with transient headaches after long hours of computer use. Studies have shown optimal seating arrangements with a carefully considered distance from the screen, and altering image size to provide a more comfortable working environment, reduces symptoms of CVS(Figure 1: ‘Computer vision syndrome — the environment’).
Figure 1: Computer vision syndrome — the environment
Screen time – individuals using screens should be told the 20:20:20 rule (i.e. every 20 minutes take a 20-second break and focus on an object 20 feet away).
Lighting, glare and screen configuration – abnormally bright or dim lighting, large windows or overhead lighting can form a washout effect on digital screens. The screen should also be positioned 35–40 inches from the eyes and display unit, where the center of the screen should be placed 5–6 inches below eye level.
Airflow – air conditioning, with hot, dry air can cause dry eye symptoms to be worse, particularly in offices with no openable windows and with high airflow.
Ocular features – persistent dry eye, blurred and double vision requiresreferrall to an optometrist.
Treatments and recommendations for CVS
The pharmacist can advise patients suffering symptoms of CVS in modifying the environment where screen use is a problem (usually at work), and on the specific causes identified.
Take regular breaks
To ease symptoms of fatigue, everyone using screens should be advised to follow the 20:20:20 rule, whereby every 20 minutes, individuals should take a 20-second break and focus on an object 20 feet away.
If the patient sounds like they have dry eye symptoms, while recommending the 20:20:20 rule, healthcare professionals may suggest to add blinking 20 times or advice to instill lubricating eye drops during these breaks.
No one should continuously use a screen for hours at a time without frequent breaks. It may be worth recommending to patients to set an alarm every 20 minutes to remind them to take eye breaks.
Refer to an optometrist (blurred vision)
If difficulty in focusing is a problem, patients should be advised of the Health and Safety Executive guidance (i.e. that employers have to provide an eye test if an employee habitually uses display screen equipment as a significant part of their normal day-to-day work).
This is a full eyesight test by an optometrist (or a doctor), and if glasses are particularly required for screen use, the employer should pay for them. Optometrists will be able to prescribe appropriate strength glasses for the patient’s preferred working distance.
Refer to an orthoptist (double vision)
Convergence insufficiency symptoms can be eased with exercises: the patient should hold a small target at 50cm and slowly bring it towards the face, while trying to maintain single and focused vision. When the image splits into double, the object is moved away and the exercise is repeated.
These exercises should be performed several times each day, with the aim of reducing the distance of the object before it splits into double vision.
Referral to optometric or orthoptic care usually results in the patient being prescribed simple convergence exercises, and others such as stereogram cards to train their eye muscles at home, and sometimes glasses with a prism incorporated to make reading easier.
This can be treated with artificial tears and ocular lubricants. Hydroxypropyl methylcellulose (hypromellose) was the most commonly recommended ocular lubricant in 2015.
However, a more viscous product such as carbomer 980 may be helpful for CVS patients because it can increase the time that moisture is retained.
Moderate-to-severe forms may require prescribed topical anti-inflammatory medications (e.g. ciclosporin, non-steroidal anti-inflammatory eye drops or corticosteroid eye drops). Sodium hyaluronate is often recommended for treatment of more advanced dry eye disease.
Evaporative dry eye
Around 80% of patients with dry eye disease are affected by evaporative dry eye, making this the most prevalent form of the disease. The oily layer of the tear film is significantly reduced; this could be secondary to untreated anterior blepharitis or meibomian gland dysfunction.
Ocular lubricants may be provided to ease symptoms. Further evidence is required to determine whether any of the tear film formulations available for evaporative dry eye are superior when compared with one another.
Administration
Treatments for dry eye disease are available in a range of formulations, including sprays, drops, gels and ointments. The proposed mechanism of action for newer lipid-containing artificial tear products involves stabilising the superficial lipid layer, thereby reducing tear film evaporation.
These products may be particularly useful in patients with evaporative dry eye disease, caused by either environmental conditions or secondary to meibomian gland dysfunction. Furthermore, some liposomal sprays have been shown to improve ocular comfort, increase the lipid layer thickness and promote tear film stability, particularly those containing soy lecithin.
Patients should be advised of the various products, their potential modes of action and administration methods, to allow them to make an informed decision. Liposomal sprays may be beneficial for patients with reduced dexterity, who may also struggle with administering drops or for use in situations where administering drops may be less convenient.
In addition, patients should be advised on appropriate lid hygiene, such as applying heat to the eyelids (either with a face cloth dipped in hot water or with commercial microwaveable eye masks), followed by lid massage with the face cloth, or cleansing the lid margins with lid-specific scrubs or cooled boiled water and a cotton bud.
Dosage
Many patients only apply treatments when they are symptomatic. This sporadic use of treatment will provide temporary symptomatic relief, but will not improve long-term ocular health. Although manufacturers’ instructions should usually be followed, four times daily dosage is generally considered necessary for symptomatic improvement.
Further recommendations of dry eye treatments can be found in Evans and Madden.
Modify the environment
Lighting and glare
Abnormally bright or dim lighting from desk lamps, large windows or overhead lighting can form a washout effect on digital screens: a discomfort glare. After long hours of a glare effect, the patient can experience fatigue and musculoskeletal problems (from constantly changing posture in an attempt to see the screen better).
Screen filters were popular with old-style computer monitors, but the brightness of modern LED screens can be easily adjusted. Spectacle coatings, such as an anti-reflective coating, are commonly advised to eliminate surface reflection. However, the evidence base to support their effectiveness is fairly limited.
Airflow
Air conditioning with hot, dry air can cause dry eye symptoms to worsen, particularly in offices with no openable windows and with a high airflow. It may be beneficial for patients to consider where they sit in an office, use humidifiers or open the window, if possible, and reduce airflow. Lubricant eye drops applied 3–4 times a day can help replenish the tear film for long hours in front of a computer screen.
Screen and seating configuration
The recommended screen positioning is a distance of 35–40 inches from the eyes and display unit where the centre of the screen should be placed 5–6 inches below eye level. Patients with postural problems can arrange an occupational health assessment at their workplace for proper seating posture advice and set-up.
Blue light
Blue light is the shortest wavelength in the visible spectrum and carries the highest amount of energy per photon. In theory, blue light has the ability to cause photochemical damages to the retina, which may result in damage to cells in the retina and cause premature death of the cells (apoptosis). Screens, particularly LED screens, emit blue light; however, the eye filters much of this light out.
Light damage is, in part, related to the brightness of the light, and modern screens emit very little light (hence no after-image) — the sun and blue-white LED bulbs emit much more blue light. Blue light filters will reduce glare so they may help some patients; however, there is no evidence that they are needed.
Blue light suppresses the brain’s release of the hormone melatonin, a sleep-inducing hormone. Sleep patterns help regulate the body’s circadian rhythm, which is required to moderate the natural clock function on individual organs and control wakefulness. Consequently, pharmacists and healthcare professionals should advise patients to switch off all screens at least an hour before going to bed, to allow a better quality of sleep.
Lumbar disc herniation is a common condition that frequently affects the spine in young and middle-aged patients.1,5,11 The lumbar intervertebral disc is a complex structure composed of collagen, proteoglycans, and sparse fibrochondrocytic cells that serve to dissipate forces exerted on the spine. As part of the normal aging process, the disc fibrochondrocytes can undergo senescence, and proteoglycan production diminishes. This leads to a loss of hydration and disc collapse, which increases strain on the fibers of the annulus fibrosus surrounding the disc. Tears and fissures in the annulus can result, facilitating a herniation of disc material, should sufficient forces be placed on the disc. Alternatively, a large biomechanical force placed on a healthy, normal disc may lead to extrusion of disc material in the setting of catastrophic failure of the annular fibers.5
Spinal disc herniation also is known as a slipped disc, is a medical condition affecting the spine in which a tear in the outer, fibrous ring of an intervertebral disc allows the soft, central portion to bulge out beyond the damaged outer rings. Disc herniation is usually due to age-related degeneration of the outer ring, known as the anulus fibrosus, although trauma, lifting injuries, or straining have been implicated as well. Tears are almost always postero-lateral (on the back of the sides) owing to the presence of the posterior longitudinal ligament in the spinal canal .This tear in the disc ring may result in the release of chemicals causing inflammation, which may directly cause severe pain even in the absence of nerve rootcompression.
Anatomy of Spinal Disc Herniation
Herniated = from “hernia,” a part of the body that bulges out through an abnormal opening Disc = the disk-shaped cushions between the bones of the spine
The vertebral column (also called the spinal column orbackbone) is made up of 33 bones known as vertebra (plural, vertebrae). Each vertebra is separated from the adjacent vertebrae by intervertebral discs, a spongy but strong connective tissue. The intervertebral discs, along with ligaments and facet joints, connect the individual vertebrae to help maintain the spine’s normal alignment and curvature while also permitting movement.
The image at left shows the entire spinal column from beside and from the front. The bones of the spinal column are orange in color, and the intervertebral discs are white.
In the center of the spinal column there is an open channel called the spinal canal. The spinal cord and spinal nerves are located in the spinal canal, where they are surrounded by spinal fluid and protected by the strong spinal column. On each side of the spine, small openings between adjacent vertebrae called foramina (singular, foramen) allow nerve roots to enter and exit the spinal canal.
The spine is divided into the following distinct regions:
Cervicalspine – consists of seven vertebrae in the neck. These vertebrae are small and allow for the mobile nature of the neck.
Thoracic spine – consists of 12 vertebrae in the upper and mid-back. These are larger and stronger than the cervical vertebrae. Each thoracic vertebra is attached to a rib on either side. This provides significant stiffness and strength to the thoracic portion of the spine.
Lumbar spine – usually consists of five vertebrae in the lower back, but may vary between four and six. These vertebrae are the largest because they withstand the greatest amount of force in the spine. The lumbar spine is also more mobile than the thoracic spine. Because of these factors, the lumbar spine is the most frequently affected by degenerative conditions, spinal stenosis, and herniated discs.
Sacrococcygeal – the very lowest portion of the spine. The sacrococcygeal region consists of one single bone, made of fused vertebrae in the sacrum (five vertebrae) and coccyx (four vertebrae). It attaches to the pelvis on either side. In a small number of people, there may be a disc between the first and second sacral vertebrae. Alternatively, the fifth vertebra in the lumbar (lower) spine may occasionally be fused to the sacrum, leaving only 4 lumbar vertebrae.
A herniated disc occurs when the fibrous outer portion of the disc ruptures or tears, and the jelly-like core squeezes out. When the herniated disc compresses a nearby nerve, as in the image below, the result can be a pinched nerve. A pinched nerve may cause pain, numbness, tingling or weakness in the arms or legs. The substance that makes up the disc’s jelly-like core can also inflame and irritate the nerve, causing additional pain.
Prolapse of intervertebral disc closeup 3d image. (c) alexmit/Big Stock
A bulging disc occurs when the outer wall of the disc weakens but doesn’t rupture, and “bulges” outward. A herniated disc may actually begin as a bulging disc whose outer wall is then ruptured by a great amount of pressure.
Disc herniation can occur in the cervical, thoracic, or lumbar spine. The location of the pain depends on the location of the herniated disc. If the herniation occurs in the neck, for example, it can cause pain that radiates into the shoulder and arm; if it occurs in the lower back, the pain produced can radiate down into the hip and leg. Depending on the location, it can damage the spinal cord.
Symptoms of Spinal Disc Herniation
A cervical herniated disc may put pressure on a cervical spinal nerve and can cause symptoms like pain, pins and needles, numbness or weakness in the neck, shoulders, or arms. A large disc herniation in the cervical spine may compress the spinal cord within the spinal canal and cause numbness, stiffness, and weakness in the legs and possibly some difficulty with bowel and bladder control.
A thoracic herniated disc may cause pain in the mid back around the level of the disc herniation. If the disc herniation compresses a thoracic spinal nerve as it travels through the foramen, then pain or numbness may travel around the rib cage from the back to the front of the chest or upper abdomen. A large disc herniation in the thoracic spine may compress the spinal cord within the spinal canal and cause numbness, stiffness and weakness in the legs and possibly some difficulty with bowel and bladder control.
A lumbar herniated disc may cause the following symptoms:
Intermittent or continuous back pain (this may be made worse by movement, coughing, sneezing, or standing for long periods of time)
Spasm of the back muscles
Sciatica — pain that starts near the back or buttock and travels down the leg to the calf or into the foot.
Muscle weakness in the legs
Numbness in the leg or foot
Decreased reflexes at the knee or ankle
Changes in bladder or bowel function
Difficulty walking
Incoordination
The symptoms of disc disease may resemble other conditions or medical problems. Always consult a doctor for a diagnosis.
Causes and Risk Factors
Herniated discs can often be the result of degenerative disc disease. As people age, the intervertebral discs lose their water content and ability to cushion the vertebrae. As a result, the discs are not as flexible. Furthermore, the fibrous outer portion of the disc is more likely to rupture or tear.
Acute disc herniations can occur in young, healthy people as a result of an injury or tear to the outer layer of the disc (called the annulus fibrosis) that allows the central, jelly-like portion of the disc (called thenucleus pulposis) to herniate into the spinal canal or foramen.
Tests and Diagnosis of Spinal Disc Herniation
Physical examination
The straight leg raise may be positive, as this finding has low specificity; however, it has high sensitivity. Thus the finding of a negative SLR sign is important in helping to “rule out” the possibility of a lower lumbar disc herniation. A variation is to lift the leg while the patient is sitting.[32] However, this reduces the sensitivity of the test.[33]
Imaging
Projection radiography (X-ray imaging) – Although traditional plain X-rays are limited in their ability to image soft tissues such as discs, muscles, and nerves, they are still used to confirm or exclude other possibilities such as tumors, infections, fractures, etc. In spite of these limitations, X-ray can still play a relatively inexpensive role in confirming the suspicion of the presence of a herniated disc. If a suspicion is thus strengthened, other methods may be used to provide final confirmation.
Computed tomography scan (CT or CAT scan) – A diagnostic image created after a computer reads x-rays. It can show the shape and size of the spinal canal, its contents, and the structures around it, including soft tissues. However, visual confirmation of a disc herniation can be difficult with a CT.
Magnetic resonance imaging (MRI) without contrast – A diagnostic test that produces three-dimensional images of body structures using powerful magnets and computer technology. It can show the spinal cord, nerve roots, and surrounding areas, as well as enlargement, degeneration, and tumors. It shows soft tissues better than CAT scans. An MRI performed with a high magnetic field strength usually provides the most conclusive evidence for diagnosis of a disc herniation. T2-weighted images allow for clear visualization of protruded disc material in the spinal canal.
Myelogram An x-ray of the spinal canal following injection of a contrast material into the surrounding cerebrospinal fluid spaces. By revealing displacement of the contrast material, it can show the presence of structures that can cause pressure on the spinal cord or nerves, such as herniated discs, tumors, or bone spurs. Because myelography involves the injection of foreign substances, MRI scans are now preferred for most patients. Myelograms still provide excellent outlines of space-occupying lesions, especially when combined with CT scanning (CT myelography).
Electromyogram and nerve conduction studies (EMG/NCS) – These tests measure the electrical impulse along nerve roots, peripheral nerves, and muscle tissue. This will indicate whether there is ongoing nerve damage, if the nerves are in a state of healing from a past injury, or whether there is another site of nerve compression. EMG/NCS studies are typically used to pinpoint the sources of nerve dysfunction distal to the spine.
Computerized tomography (CT) scan – a series of X-rays, assembled by a computer into 3-dimensional images of the body’s structures
Myelography – a procedure that involves injecting a liquid dye into the spinal column followed by a series of X-rays and a computerized tomography (CT) scan. This procedure may provide useful images that reveal the indentations of the spinal fluid sac caused by bulging or herniated discs, or bone spurs that might be pressing on the spinal cord or nerves.
Electromyography (EMG) – tests the electrical activity of a nerve root to help determine the cause of pain.
The presence and severity of myelopathy can be evaluated by means of transcranial magnetic stimulation (TMS), a neurophysiological method that allows the measurement of the time required for a neural impulse to cross the pyramidal tracts, starting from the cerebral cortex and ending at the anterior horn cells of the cervical, thoracic or lumbar spinal cord. This measurement is called Central Conduction Time (CCT). TMS can aid physicians to:
determine whether myelopathy exists
identify the level of the spinal cord where myelopathy is located. This is especially useful in cases where more that two lesions may be responsible for the clinical symptoms and signs, such as in patients with two or more cervical disc hernias[34]
follow-up the progression of myelopathy in time, for example before and after cervical spine surgery
TMS can also help in the differential diagnosis of different causes of pyramidal tract damage.[35]
Since a herniated disc may cause similar symptoms to other degenerative spinal conditions, a surgeon may order a variety of diagnostic procedures to rule out other possible conditions.
Treatment of Spinal Disc Herniation
Before discussing surgery as an option, the surgeon may initiate the following nonoperative treatments. Specific treatment for lumbar disk disease will be determined by your health care provider based on
Your age, overall health, and medical history
Extent of the condition
Type of condition
Your tolerance for specific medications, procedures, or therapies
Expectations for the course of the condition
Your opinion or preference
Typically, conservative therapy is the first line of treatment to manage lumbar disk disease. This may include a combination of the following:
Bed rest
Patient education on proper body mechanics (to help decrease the chance of worsening pain or damage to the disk)
Physical therapy, which may include ultrasound, massage, conditioning, and exercise
Weight control
Use of a lumbosacral back support
Medications of Spinal Disc Herniation
Analgesics: Prescription-strength drugs that relieve pain but not inflammation.
Antidepressants: A Drugs that block pain messages from your brain and boost the effects of eorphins (your body’s natural painkillers).
Corticosteroids: Also known as oral steroids, these medications reduce inflammation.
Muscle Relaxants: These medications provide relief from spinal muscle spasms.
Neuropathic Agents: Drugs(pregabalin & gabapentine) that address neuropathic—or nerve-related—pain. This includes burning, numbness, and tingling.
Opoids : Also known as narcotics, these medications are intense pain relievers that should only be used under a doctor’s careful supervision.
Topical Medications: These prescription-strength creams, gels, ointments, patches, and sprays help relieve pain and inflammation through the skin.
NSAIDs: Prescription-strength drugs that reduce both pain and inflammation.Pain medicines and anti-inflammatory drugs help to relieve pain and stiffness, allowing for increased mobility and exercise. There are many common over-the-counter medicines called non-steroidal anti-inflammatory drugs (NSAIDs). They include aspirin, ibuprofen (Motrin, Advil), and naproxen (Naprosyn, Aleve).
Calcium & vitamin D3, to improve bones health and healing fracture.
Glucosamaine & diacerine ,can be used to tightening the loose tenson and regenerate cartilage or inhabit the further degeneration of cartilage.
Corticosteroid to healing the nerve inflamation and clotted blood in the joints.
Diatery suppliment to remove the general weakness & improved the health.
There is little evidence to suggest that drug treatments are effective in treating herniated disc.
NSAIDs and cytokine inhibitors don’t seem to improve symptoms of sciatica caused by disc herniation.
We found no evidence examining the effectiveness of analgesics, antidepressants, or muscle relaxants in people with a herniated disc.
We found no evidence of sufficient quality to judge the effectiveness of epidural injections of corticosteroids.
With regard to non-drug treatments, spinal manipulation seems to be more effective at relieving local or radiating pain in people with acute back pain and sciatica with disc protrusion compared with sham manipulation, although concerns exist regarding possible further herniation from spinal manipulation in people who are surgical candidates.
Neither bed rest nor traction seems effective in treating people with sciatica caused by disc herniation.
We found insufficient evidence about advice to stay active, acupuncture, massage, exercise, heat, or ice to judge their efficacy in treating people with herniated disc.
About 10% of people have sufficient pain after 6 weeks for surgery to become a consideration.
Both standard discectomy and microdiscectomy seem to increase self-reported improvement to a similar extent.
We found insufficient evidence judging the effectiveness of automated percutaneous discectomy,laser discectomy, or percutaneous disc decompression.
Surgical Treatment of Spinal Disc Herniation
When these conservative measures fail, surgery for removal of a herniated disk may be recommended. Surgery is done under general anesthesia. An incision is placed in the lower back over the area where the disk is herniated. Some bone from the back of the spine may be removed to gain access to the area where the disk is located. Typically, the herniated part of the disk and any extra loose pieces of disk are removed from the disk space.
Surgical treatment for a herniated disc will be based on the following
The history, severity and duration of pain
Whether or not the patient has received previous treatments for disc disorders and how effective the treatments were
Whether or not there is any evidence of neurologic damage such as sensory loss, weakness, impaired coordination, or bowel or bladder problems
Surgery for patients with disc disorders of the spine is usually recommended for those patients who do not find relief with non-operative treatment over a period of 6-12 weeks. Surgery is also recommended in patients who have a neurologic deficit (numbness, weakness or reduced function due to pressure on the spinal cord or nerves). Early intervention in those cases is best in order to maximize the likelihood of neurologic recovery.
Your surgeon may perform the following surgical procedures:
Microdiscectomy: A procedure that uses a microscope and microsurgical tools to remove the portion of the disc that is pressing against the nerve, relieving the pressure caused by a herniated disc. Microdiscectomy is frequently performed for herniated discs in the certical, thoracic, and lumbosacral spine. This procedure is performed under general anesthesia through a small skin incision over the spine. The muscles of the spine are gently elevated or spread apart to expose a small segment of the spine. A small amount of the back part of the spine, called the lamina and facet joint, is trimmed under high magnification of the microscope to provide safe access to the spinal canal. Using microsurgical techniques, our neurosurgeons identify and remove the herniated piece of the disc while protecting the compressed nerve. Most patients may go home either on the day of surgery or the next morning.
Anterior (from the front) or lateral (from the side) surgical approaches may be required for large or calcified thoracic disc herniations that cause spinal cord compression.
Anterior Cervical Discectomy and Fusion (ACDF): a procedure that involves the removal of the herniated disc in the cervical spine through the front of the neck. A fusion surgery may be required to make the spine stable after the discectomy.
After surgery, restrictions may be placed on the patient’s activities for several weeks while healing is taking place to prevent another disk herniation from occurring. Your surgeon will discuss any restrictions with you.
Others Treatment of Spinal Disc Herniation
Chiropractic Care
Sixty percent of people with sciatica who didn’t get relief from other therapies and then tried spinal manipulation experienced the same degree of pain relief as patients who eventually had surgery, found a 2010 study in the Journal of Manipulative and Physiological Therapeutics. The 120 people in the study saw a chiropractor about 3 times a week for 4 weeks, and then continued weekly visits, tapering off treatment as they felt better. In people who responded to chiropractic care, benefits lasted up to a year. “Spinal manipulation may create a response in the nervous system that relieves pain and restores normal mobility to the injured area,” says study researcher Gordon McMorland, DC, of National Spine Care in Calgary, Alberta. “It also reduces inflammation, creating an environment that promotes the body’s natural healing mechanisms.”
Acupuncture
“You can get relief as soon as the first session, though it takes about 12 sessions to see improvement,” says Jingduan Yang, MD, assistant professor at the Jefferson Myrna Brind Center of Integrative Medicine at Thomas Jefferson University. A small study in the Journal of Traditional Chinese Medicine found that of 30 people with sciatica, 17 got complete relief and 10 saw symptoms improve with warming acupuncture, in which the needles are heated.
Yoga
A study in the journal Pain reported that people with chronic back pain who practiced Iyengar yoga for 16 weeks saw pain reduced by 64% and disability by 77%. Although yoga’s effects on sciatica are less clear, gentle forms may be beneficial. By strengthening muscles and improving flexibility, a yoga practice can help sciatica sufferers “move and function better so they don’t fall into a posture that aggravates sciatica,” says James W. Carson, PhD, a psychologist at the Comprehensive Pain Center at Oregon Health & Science University. For extra grip and stability, try these grip socks from Natural Fitness.
Massage
Don’t expect a chilled-out spa massage if you have sciatica. In this instance, trigger-point therapy is best, says Jeff Smoot, vice president of the American Massage Therapy Association. The sciatic nerve sits underneath a muscle called the piriformis, which is located beneath the glutes. “When the piriformis muscle gets tight, it pinches the sciatic nerve, causing tingling and numbness down into the leg,” says Smoot. He applies pressure to irritated and inflamed areas, or trigger points, in the piriformis muscle, as well as in muscles in the lower back and glutes. Typically, Smoot schedules treatments 7 to 10 days apart. If patients don’t see progress by the fourth visit, “they need to try another form of therapy,” he says.
Topical Preparations
St. John’s wort oil, a liniment, is “one of my favorites for nerve pain,” says Tieraona Low Dog, MD, director of the fellowship at the Arizona Center for Integrative Medicine. Apply the anti-inflammatory oil two or three times a day where there’s pain. Another option: an OTC cayenne pepper plaster or cream; capsaicin, found in chiles, hinders the release of pain-causing compounds from nerves. For severe cases, Low Dog uses the prescription chile patch Qutenza, designed for shingles pain. “One application is effective for weeks,” says Low Dog.
Ice or Heat
Because the sciatic nerve is buried deep within the buttock and leg, ice or heat on the surface of the body won’t ease that inner inflammation. But the timehonored treatments can act as counterirritants—that is, “they give your body other input in the painful area, and that brings the pain down a notch,” says Ruppert. Apply an ice pack or a heating pad as needed for 15 minutes.
Devil’s Claw
The herbal medication devil’s claw is “quite a potent anti-inflammatory, working like ibuprofen and similar drugs to inhibit substances that drive inflammation,” says Low Dog. She generally starts patients on 1,500 to 2,000 mg twice a day. Look for a brand that has a standardized extract of roughly 50 mg of harpagoside, the active compound. Safety reviews show that the supplement is well tolerated by most people but should be avoided by patients with peptic ulcers or on blood-thinning medications.
Epidural Steroid Injections
People whose pain doesn’t lessen within about a month and who aren’t helped by other therapies may find their pain remedied by an x-ray-guided injection of steroid into the lower back near the sciatic nerve, says Raj Rao, MD, a spokesperson for the AAOS. “The hope is to reduce inflammation within that nerve branch,” explains Rao. Because of concerns about side effects, such as loss of bone density, the epidural shots are limited to three a year.
Physiotherapy in Harniated Disc
In stage 1&2 of harniated disc physiotherapy must applied to cure harniated hisc .In case of stage 3&4 ,physiotherapy can’t applied due to adoining the another case of foot drop.
In accordance of NIH journal
Physiotherapy for a lumbar disc bulge
Physiotherapy treatment for a lumbar disc bulge is vital to ensure an optimal outcome and may comprise:
soft tissue massage
electrotherapy (e.g. ultrasound)
lumbar taping
the use of a back brace
mobilization
traction
the use of a lumbar roll for sitting
dry needling
exercises to push the disc back ‘in’ and to improve strength, core stability and flexibility
education
activity modification advice
biomechanical correction
ergonomic advice
clinical Pilates
hydrotherapy
a functional restoration program
a gradual return to activity program
Physical therapy often plays a major role in herniated disc recovery. Its methods not only offer immediate pain relief, but they also teach you how to condition your body to prevent further injury.
There are a variety of physical therapy techniques. Passive treatments relax your body and include deep tissue massage, hot and cold therapy, electrical stimulation (eg, TENS), and hydrotherapy.
Your physical therapy program will usually begin with passive treatments. But once your body heals, you will start active treatments that strengthen your body and prevent further pain. Your physical therapist will work with you to develop a plan that best suits you.
Passive Physical Treatments for Herniated Discs
Deep Tissue Massage
There are more than 100 types of massage, but deep tissue massage is an ideal option if you have a herniated disc because it uses a great deal of pressure to relieve deep muscle tension and spasms, which develop to prevent muscle motion at the affected area.
Hot and Cold Therapy
Both hot and cold therapies offer their own set of benefits, and your physical therapist may alternate between them to get the best results.Your physical therapist may use heat to increase blood flow to the target area. Blood helps heal the area by delivering extra oxygen and nutrients. Blood also removes waste byproducts from muscle spasms.Conversely, cold therapy (also called cryotherapy) slows circulation. This reduces inflammation, muscle spasms and pain. Your physical therapist may place an ice pack on the target area, give you an ice massage, or even use a spray known as fluoromethane to cool inflamed tissues.
Hydrotherapy
As the name suggests, hydrotherapy involves water. As a passive treatment, hydrotherapy may involve simply sitting in a whirlpool bath or warm shower. Hydrotherapy gently relieves pain and relaxes muscles.
A TENS machine uses an electrical current to stimulate your muscles. It sounds intense, but it really isn’t painful. Electrodes taped to your skin send a tiny electrical current to key points on the nerve pathway. TENS reduces muscle spasms and is generally believed to trigger the release of endorphins, which are your body’s natural pain killers.
Traction
The goal of traction is to reduce the effects of gravity on the spine. By gently pulling apart the bones, the intent is to reduce the disc herniation. The analogy is much like a flat tire “disappearing” when you put a jack under the car and take pressure off the tire. It can be performed in the cervical or lumbar spine.
Active Treatments You May Try in Physical Therapy
Active treatments help address flexibility, posture, strength, core stability, and joint movement. An exercise program may also be prescribed to achieve optimal results. This will not only curb recurrent pain but will also benefit your overall health. Your physical therapist will work with you to develop a program based on your specific diagnosis and health history.
Core stability
Many people don’t realize how important a strong core is to their spinal health. Your core (abdominal) muscles help your back muscles support your spine. When your core muscles are weak, it puts extra pressure on your back muscles. Your physical therapist may teach you core stabilizing exercises to strengthen your back.
Flexibility
Learning proper stretching and flexibility techniques will prepare you for aerobic and strength exercises. Flexibility helps your body move easier by warding off stiffness.
Hydrotherapy
In contrast to simply sitting in a hot tub or bath like its passive counterpart, active hydrotherapy may involve water aerobics to help condition your body without unnecessary stress.
Muscle strengthening
Strong muscles are a great support system for your spine and better handle pain.
Your physical therapist will teach you ways to condition and strengthen your back to help prevent future pain. You may learn self-care principles so you understand how to best treat your symptoms. The ultimate goal is for you to develop the knowledge to maintain a pain-free lifestyle.
It’s essential that you learn how to exercise and condition your back after the formal physical therapy ends. If you don’t implement the lessons you learned during physical therapy, you won’t enjoy its long-term results. By taking care of your back on your own, you may prevent further herniated disc pain
8 Best Exercises For Slipped Disc In Lower Back
Our spinal cord is supported by a number of muscles. Relevant exercises help relieve the pain and reduce the symptoms. Muscle exercises of those muscles associated with the affected area is necessary. Patients must know the region that has a slipped disc and then opt for exercises related to that muscle. The list of best exercises for the slipped disc are mentioned as follows:
Abdominal Isometrics – It can be performed either on floor, mat or bed. This exercise involves moving your lower back towards the surface at which you are performing this exercise. Leg movement must be reduced in this exercise and stomach muscles must be made active. This reduces pain in lower back because of the attachment of abdominal muscles to the lower side of the vertebral column. Ten repetitions are effective.
Crunches – Lie on a flat surface with knees bent. Cross your arm under your head, raise your head and chest in such a manner that your rib cage curl interiorly towards your backbone. Perform this exercise slowly and gradually. In the beginning, perform fewer crunches and repeat it daily and increase the number of turns as you gain strength.
Lower back extension – Lie in an upside down position, raise your upper body with the help of elbow and hold up yourself in an elevated position for a short span of time and then slowly lower down. Please make sure that during this exercise you do not raise your pelvis girdle (hip region).
Bilateral knee to the chest – Lay down on a flat surface and draw your knee towards your abdominal region, repeat it 5 times and then switch leg. You can also increase the number of turns each time you repeat it.
Iso-hip flexion – Lay down over a flat surface and draw your knees towards your chest region in a 90 degree position with your stomach. Place your hands over your knees and then exert your hand pressure to lower your knee. Then utilize the knee pressure to resist the downward movement of your legs, in all both movements should just exert pressure and allow no movements. This position should be maintained for few seconds and then lowered slowly and gradually.
Air bike – Sit on a chair with your chest and shoulders supported. Align your knees and feet together and then bring them towards your body and perform a pedaling motion in air then repeat the same motion while moving your knees farther away from body. Follow ten repetitions each time and increase its number as you gain strengths
Ham string stretch: Lie on a flat surface with your knees bend, place your hands under your knees and then slightly pull your leg towards your chest, repeat it with other leg. This exercise must involve a stretch over lower thigh muscle
Lumbar roll: Lie on a flat surface with your knee bent and your feet lying on the floor then move your legs together towards the right side and then towards your left side. Repeating these movements 5 times on each side.
The above mentioned best exercises for slipped disc can be followed but if pain increases or muscle pain is persisting then quit these exercises right away. These exercises not only help in reducing the pain but they also activate efficient muscle movement. Along with these exercise tips, proper body postures must be also maintained to prevent further disc damages.
Home Remady for Herniated Disc/Slip Disc
Consciousnes
Incase of PLID home remedies are not special treatment just only home practice & creating public awareness. All should be done in PLID stage 1&2
Walking
Walking every day keeps muscle disorders away. Walking can also help to prevent herniated disc. Walk on a flat road for 20 minutes as many times as you can in a day. Take longer steps as it will help you to keep away the pain of herniated disc. Do not give strain to yourself as it might increase the pain.
Rest
www.rxharun.com
Rest is essential for patients suffering from herniated disc. Take short rest periods from time to time. When you are sleeping make sure you don’t stay in the same position for a long time. Do not sleep on your stomach. Also, take care of the mattress you are sleeping on. Don’t let it be too soft and spongy. Buy a mattress that has good surface area and is soft in nature.
Physiotherapy And Yoga( only home practice)
Physiotherapy is a very cheap and good way of getting rid of herniated disc from itself. Therapists will teach your proper exercises and stretches which will improve the disc shape to a great extent.
You will notice good differences while performing daily chores after just 4-5 sessions of therapy.
Physiotherapy also promotes faster healing of the disorder.
Turmeric
Turmeric contains curcumin which is a very good anti-oxidant and anti-inflammatory agent. This is why it stops the gel-like fluid inside the discs from coming out and bulge. It also shows antihistamine properties which help to reduce pain because of slowed blood circulation to the area of pain.
Dimethyl Sulfoxide (DMSO)
Dimethyl sulfoxide is a derivative from sulphur which has antioxidant properties as well as the organic sulphur present in it helps in the growth of new cells and detoxification of the body. The growth of new cells helps to replace the old cells of the discs and prevent the fluid from leaking outside.
Massage With Essential Oils
Massage with essential oils on the full body, especially on the spine and lower back regions, will help in good blood circulation and promote the growth of new cells. It will help relieve pain and promote better absorption of oxygen and nutrients. Essential oils will also regenerate the cells of the disc and hence stop the disc from getting slipped.
Acupressure And Acupuncture
In both techniques, pressure is used for relieving the pain from the swelled area. In acupressure fingers, tips and elbow are used and acupuncture needles are used. But this should be done with the help of an experienced practitioner and not alone.
This is not recommended for patients having high blood pressure and for women who are pregnant.
TENS
TENS stands for Transcutaneous Electrical Nerve Stimulation and this is one of the best remedies for herniated disc at home. This treatment uses low voltage electric current which is applied to the affected area and helps the body to release endorphin which decreases the pain.
Cayenne Pepper
It is a very effective ingredient for the treatment of herniated disc.You can drink its tea or make a paste of the pepper using water and apply on the affected area.
Diet
Diet is necessary to keep away all types of bad conditions that might affect you.Drink a lot of water and eat a balanced diet. Take excess of fibres and proteins. During this condition, you should avoid dairy products and red meat. Also, avoid fat-free foods.
Epsom Salt
Epsom salt is one of the widely used natural painkiller and anti-inflammatory agent.
You can use this by adding 3-4 cups of salt in a hot water bath. Stay inside the bath for 15 minutes. It will help you achieve maximum relaxation.
Do not use this remedy if you are diabetic or pregnant. If you are on any type of medication consult your doctor before bathing in Epsom salt.
Horsetail
Horsetail is a herb which has high quantities of minerals in it. It nourishes our tissues and has the ability to heal broken bones and torn ligaments.
All you need to do is add some horsetail leaves to half a litre of water. Boil on low heat till the water quantity reduces to half its quantity. Cool the solution and filter it off. You can drink 5 ml of the solution thrice a day.It will heal herniated disc very fast.
California Poppy
California poppy is anti-inflammatory and analgesic in nature. This is what makes it a good treatment for herniated disc.
You can tear the leaves of California poppy into small pieces and make a paste out of it using water. Use little hot water so that when you apply the paste on the affected area it is still warm.
White Willow Bark
White willow bark is used for reducing the discomfort of herniated discs. The chemical structure of this drugs shows a marked similarity to aspirin hence acts as an analgesic but doesn’t irritate your gut. It is also astringent and anti-inflammatory in nature.
This herb might react with drugs hence do consult your doctor if you are on any kind of medication.
Comfrey Leaves
Comfrey leaves have power to heal bones and connective tissues of the body.All you need to do is take some fresh leaves and add it to cold water. Let it remain undisturbed for around 12 hours. After 12 hours heat the above solution and filter it. Add the filtrate to bath water and take a bath in it 2 times a day.Do not consume it orally because it contains hepatic-toxin alkaloids.
Boswellia
Boswellia is a naturally occurring painkiller which is a very effective remedy for herniated disc.
All you can do is make a decoction of Boswellia and consume it 2 times a day to reduce pain and discomfort associated with herniated discs.
Boswellia is an organic painkiller that effectively treats the problem of herniated disc. It is also an herbal cure for osteoarthritis.
Omega-3 Fatty Acids
Omega-3 Fatty acids are helpful in decreasing the inflammation and pain experienced due to herniated disc disorder. This acid forms collagen which is used by the broken discs for repairing itself.
Eat foods that are high in this kind of fats like fish, almonds, sprouts and walnuts.
Colchicine
Colchicine is an active amino-alkaloid found in the plant of Kurchi or autumn crocus. This powder is obtained by crushing the seeds of the plant. It has anti-inflammatory properties which are effective against the slipped disc.
Make a paste with kurchi powder and honey and consume it once a day.
You can also make tea out of the powder or mix the powder in milk and have it once or twice a day.
Burdock
Burdock contains a lot of anti-oxidants which is helpful to detoxify the body and remove all kinds of harmful substances and decrease the pain and inflammation in your body. It also treats arthritis.
Burdock can be consumed as a decoction once or twice a day.
Passionflower
Passionflower is helpful for slipped discs because the essential oils present is antispasmodic in nature. It reduces pain and inflammation.
You can massage with passionflower essential oil or take capsules made from it, however, do consult your doctor before taking capsules.
Additional Tips
If you are overweight, try to lose some pounds.
Exercise every day.
Lift things in a proper way, as guided by a therapist. Do not lift heavy weights.
Stop smoking and drinking.
Always make sure you are in the right posture whatever activity you may be doing.
Wear flat and soft shoes. Avoid heels.
Walk and move around cautiously.
Slipped discs can be really painful but with the right treatment and precautions you can become as fit as you were before. So start taking home remedies and consult a doctor whenever you feel any kind of severe pain.



 Hyperopia Symptoms, Diagnosis, Treatment
Hyperopia Symptoms, Diagnosis, Treatment
 Hyperopia Causes, Symptoms, Treatment
Hyperopia Causes, Symptoms, Treatment
 Astigmatism, Causes, Symptoms, Diagnosis, Treatment
Astigmatism, Causes, Symptoms, Diagnosis, Treatment
 Astigmatism Symptoms, Diagnosis, Treatment
Astigmatism Symptoms, Diagnosis, Treatment
 Astigmatism Types, Symptoms, Diagnosis, Treatment
Astigmatism Types, Symptoms, Diagnosis, Treatment
 Amblyopia, Causes, Symptoms, Diagnosis, Treatment
Amblyopia, Causes, Symptoms, Diagnosis, Treatment
 Lazy Eye, Causes, Symptoms, Diagnosis, Treatment
Lazy Eye, Causes, Symptoms, Diagnosis, Treatment
 Amblyopia Symptoms, Diagnosis, Treatment
Amblyopia Symptoms, Diagnosis, Treatment
 Astigmatism Diagnosis, Treatment, Prevention
Astigmatism Diagnosis, Treatment, Prevention
 Astigmatism Causes, Symptoms, Treatment
Astigmatism Causes, Symptoms, Treatment
 Astigmatism Treatment, Causes, Symptoms
Astigmatism Treatment, Causes, Symptoms
 Amblyopia Causes, Symptoms, Treatment
Amblyopia Causes, Symptoms, Treatment





























