Baclofen is a medication used to treat spasticity. It is used as a central nervous system depressant and skeletal muscle relaxant. It is also used in topical creams to help with pain. Chemically it is a derivative of the neurotransmitter γ-aminobutyric acid (GABA). It is believed to work by activating (or agonizing) GABA receptors, specifically the GABAB receptors. Its beneficial effects in spasticity result from its actions in the brain and spinal cord
Description
Baclofen, USP is a muscle relaxant and antispastic.
Its chemical name is 4-amino-3-(4-chlorophenyl)-butanoic acid. The structural formula is:
Baclofen, USP is a white to off-white odorless or practically odorless crystalline powder. It is slightly soluble in water, very slightly soluble in methanol and insoluble in chloroform.
Each tablet, for oral administration, contains 10 mg or 20 mg Baclofen, USP. In addition, each tablet contains the following inactive ingredients: anhydrous lactose, colloidal silicon dioxide, dibasic calcium phosphate dihydrate, magnesium stearate, microcrystalline cellulose and sodium starch glycolate.
Baclofen – Clinical Pharmacology
The precise mechanism of action of Baclofen is not fully known. Baclofen is capable of inhibiting both monosynaptic and polysynaptic reflexes at the spinal level, possibly by hyperpolarization of afferent terminals, although actions at supraspinal sites may also occur and contribute to its clinical effect. Although Baclofen is an analog of the putative inhibitory neurotransmitter gamma-aminobutyric acid (GABA), there is no conclusive evidence that actions on GABA systems are involved in the production of its clinical effects. In studies with animals Baclofen has been shown to have general CNS depressant properties as indicated by the production of sedation with tolerance, somnolence, ataxia, and respiratory and cardiovascular depression. Baclofen is rapidly and extensively absorbed and eliminated. Absorption may be dose-dependent, being reduced with increasing doses. Baclofen is excreted primarily by the kidney in unchanged form and there is relatively large intersubject variation in absorption and/or elimination.
Baclofen is a muscle relaxer and an antispastic agent.
Baclofen is used to treat muscle symptoms caused by multiple sclerosis, including spasm, pain, and stiffness.
Baclofen is sometimes used to treat muscle spasms and other symptoms in people with injury or disease of the spinal cord.
Indication
Spasticity
Cerebral Spasticity
Spinal Spasticity
Pediatric
Spasticity
Cerebral Spasticity
Spinal Spasticity
Baclofen tablets are not indicated in the treatment of skeletal muscle spasm resulting from rheumatic disorders.The efficacy of baclofen tablets in stroke, cerebral palsy, and Parkinson’s disease has not been established and, therefore, it is not recommended for these conditions.
Important information
Do not use baclofen at a time when you need muscle tone for safe balance and movement during certain activities.
Do not stop using baclofen suddenly, or you could have unpleasant withdrawal symptoms.
Before taking this medicine
You should not use baclofen if you are allergic to it.
To make sure this medicine is safe for you, tell your doctor if you have:
kidney disease;
epilepsy or other seizure disorder;
a history of stroke or blood clots; or
if you also use a narcotic (opioid) medication.
Using baclofen during pregnancy could harm the unborn baby. In animal studies, it caused low birth weight and birth defects. However, it is not known whether these effects would occur in humans.
It is not known whether baclofen passes into breast milk or if it could harm a nursing baby. You should not breast-feed while you are using this medicine.
Using baclofen may increase your risk of developing an ovarian cyst. Talk with your doctor about your specific risk.
Baclofen is not approved for use by anyone younger than 12 years old.
How should I take baclofen?
Take baclofen exactly as prescribed by your doctor. Follow all directions on your prescription label. Your doctor may occasionally change your dose to make sure you get the best results. Do not use this medicine in larger or smaller amounts or for longer than recommended.
Call your doctor if your muscle symptoms do not improve, or if they get worse.
Do not stop using this medicine suddenly, or you could have unpleasant withdrawal symptoms such as hallucinations or a seizure. Ask your doctor how to safely stop using this medicine.
Store at room temperature away from moisture and heat.
Doses of Baclofen
Applies to the following strength(s): 10 mg ; 20 mg ; 0.05 mg/mL ; 0.5 mg/mL ; 1 mg/mL ; 2 mg/mL ; 5 mg/mL
What happens if I miss a dose?
Take the missed dose as soon as you remember. Skip the missed dose if it is almost time for your next scheduled dose. Do not take extra medicine to make up the missed dose.
What happens if I overdose?
Overdose symptoms may include muscle weakness, vomiting, drowsiness, dilated or pinpoint pupils, weak or shallow breathing, seizure, or coma.
What should I avoid while taking baclofen?
Do not use baclofen at a time when you need muscle tone for safe balance and movement during certain activities. In some situations, it may be dangerous for you to have reduced muscle tone.
Drinking alcohol with this medicine can cause side effects.
This medication may impair your thinking or reactions. Be careful if you drive or do anything that requires you to be alert.
Baclofen side effects
Get emergency medical help if you have signs of an allergic reaction to baclofen: hives; difficult breathing; swelling of your face, lips, tongue, or throat.
Call your doctor at once if you have:
weak or shallow breathing;
confusion, hallucinations; or
a seizure (convulsions).
Common baclofen side effects may include:
drowsiness, dizziness, weakness, tired feeling;
headache;
sleep problems (insomnia);
nausea, constipation; or
urinating more often than usual.
What other drugs will affect baclofen?
Taking baclofen with other drugs that make you sleepy or slow your breathing can cause dangerous side effects or death. Ask your doctor before taking a sleeping pill, narcotic pain medicine, prescription cough medicine, a muscle relaxer, or medicine for anxiety, depression, or seizures.
Other drugs may interact with baclofen, including prescription and over-the-counter medicines, vitamins, and herbal products. Tell each of your health care providers about all medicines you use now and any medicine you start or stop using
In addition to its needed effects, some unwanted effects may be caused by baclofen. In the event that any of these side effects do occur, they may require medical attention.
Severity: Moderate
If any of the following side effects occur while taking baclofen, check with your doctor or nurse as soon as possible:
Less common or rare:
Bloody or dark urine
chest pain
fainting
hallucinations (seeing or hearing things that are not there)
mental depression or other mood changes
ringing or buzzing in the ears
skin rash or itching
Symptoms of overdose:
Blurred or double vision
convulsions (seizures)
muscle weakness (severe)
shortness of breath or unusually slow or troubled breathing
vomiting
Minor Side Effects
Some of the side effects that can occur with baclofen may not need medical attention. As your body adjusts to the medicine during treatment these side effects may go away. Your health care professional may also be able to tell you about ways to reduce or prevent some of these side effects. If any of the following side effects continue, are bothersome or if you have any questions about them, check with your health care professional:
More common:
Confusion
dizziness or lightheadedness
drowsiness
nausea
unusual weakness, especially muscle weakness
Less common or rare
Abdominal or stomach pain or discomfort
clumsiness, unsteadiness, trembling, or other problems with muscle control
constipation
diarrhea
difficult or painful urination or a decrease in the amount of urine
false sense of well-being
frequent urge to urinate or uncontrolled urination
a headache
loss of appetite
low blood pressure
muscle or joint pain
numbness or tingling in hands or feet
pounding heartbeat
sexual problems in males
slurred speech or other speech problems
stuffy nose
swelling of ankles
trouble in sleeping
unexplained muscle stiffness
unusual excitement
unusual tiredness
weight gain
Side Effects: Post Treatment
After you stop taking this drug, it is possible that you may still experience side effects that need medical attention. If you notice any of the following side effects check with your doctor immediately:
Convulsions (seizures)
hallucinations (seeing or hearing things that are not there)
Common (1% to 10%): Cardiac output decreased, hypotension, hypertension, diminished cardiovascular functions, peripheral edema
Rare (less than 0.1%): Arrhythmias, palpitations, chest pain
Frequency not reported: Bradycardia, orthostatic hypotension
Dermatologic
Common (1% to 10%): Rash, hyperhidrosis, urticaria/pruritus, facial edema
Uncommon (0.1% to 1%): Alopecia, diaphoresis
Frequency not reported: Rash, sweating, contact dermatitis, skin ulcer
Endocrine
Common (1% to 10%): Ovarian cysts are palpable in 4% of women treated with for up to one year.
Gastrointestinal
Very common (10% or more): Nausea (especially at start of therapy) (up to 11%)
Common (1% to 10%): Dry mouth, GI disorder/disturbance, constipation, diarrhea, retching, vomiting, increased salivation
Uncommon (0.1% to 1%): Dysphagia, dehydration, ileus, decreased taste sensation
Rare (less than 0.1%): Colicky abdominal pain, anorexia
Frequency not reported: GI hemorrhage
Genitourinary
Very common (10% or more): Urinary retention (up to 12%)
Common (1% to 10%): Urinary incontinence, urination impaired, sexual dysfunction, urinary frequency, enuresis, dysuria
Rare (less than 0.1%): Erectile dysfunction
Frequency not reported: Dysuria, abnormal ejaculation, oliguria, vaginitis
Hematologic
Frequency not reported: Leukocytosis, petechial rash
Hepatic
Rare (less than 0.1%): Disorders of hepatic function (e.g., increased AST)
Immunologic
Common (1% to 10%): Pneumonia
Uncommon (0.1% to 1%): Septicemia
Metabolic
Common (1% to 10%): Decreased appetite
Frequency not reported: Blood glucose increased
Musculoskeletal
Very common (10% or more): Hypotonia (up to 52%), lower extremity weakness (up to 15%), disturbances of gait and balance
Common (1% to 10%): Muscular weakness, myalgia, upper extremity weakness, back pain, muscular hypertonia
Nervous system
Very common (10% or more): Somnolence (up to 28%), drowsiness (up to 18%), headache (up to 16%), seizures (especially on discontinuation of therapy) (up to 15%), sedation, dizziness (up to 12%)
Common (1% to 10%): Fatigue, ataxia, tremor, lightheadedness, lassitude, exhaustion, numbness/itching/tingling, slurred speech, lethargy, hypertonia, paresthesia
Rare (less than 0.1%): Dysarthria, dysgeusia, syncope, dyskinesia, coma, potentially life-threatening withdrawal symptoms (as a result of sudden interruption of drug delivery)
Other
Common (1% to 10%): Tinnitus, pain, asthenia
Uncommon (0.1% to 1%): Accidental injury, weight loss
Very rare (less than 0.01%): Hypothermia
Frequency not reported: Drug withdrawal syndrome
Uncommon (0.1% to 1%): Subdural hemorrhage, accidental injury, weight loss
Ocular
Common (1% to 10%): Nystagmus, visual impairment, accommodation disorder, blurred vision, double vision, amblyopia
Psychiatric
Common (1% to 10%): Confusional state, hallucination, depression, insomnia, euphoric mood, nightmare, personality changes
Uncommon (0.1% to 1%): Memory loss/impairment, suicidal ideation, attempted suicide
Rare (less than 0.1%): Excitement
Renal
Very rare (less than 0.01%): Kidney calculus
Respiratory
Common (1% to 10%): Respiratory depression, hypoventilation, dyspnea, bradypnea, feeling of pressure in the chest…
Vitamin B12 deficiency, also known as cobalamin deficiency, is the medical condition of low blood levels of vitamin B12. In mild deficiency, a person may feel tired and have a reduced number of red blood cells (anemia). In moderate deficiency, there may be inflammation of the tongue and the beginning of neurological problems including abnormal sensations such as pins and needles, while severe deficiency may include reduced heart function and greater neurological problems. Neurological problems may include changes in reflexes, poor muscle function, memory problems, decreased taste, and in extreme cases psychosis. Sometimes temporary infertility may also occur. In young children, symptoms include poor growth, poor development, and difficulties with movement. Without early treatment, some of the changes may be permanent.
Vitamin B12 (Cobalamin) is a water-soluble vitamin that is derived from animal products such as red meat, dairy, and eggs. Intrinsic factor is a glycoprotein that is produced by parietal cells in the stomach and necessary for the absorption of B12 in the terminal ileum. Once absorbed, B12 is used as a cofactor for enzymes that are involved in the synthesis of DNA, fatty acids, and myelin. As a result, a B12 deficiency can lead to hematologic and neurologic symptoms. B12 is stored in excess in the liver; however, in cases in which B12 cannot be absorbed for a prolonged period (e.g., dietary insufficiency, malabsorption, lack of intrinsic factor), hepatic stores are depleted, and deficiency occurs.[rx][rx][rx]
Causes of Vitamin B12 Deficiency
Vitamin B12 deficiency has 3 primary etiologies:
Autoimmune – Pernicious anemia is an autoimmune condition in which antibodies to intrinsic factor are produced. Anti-intrinsic factor antibodies bind to and inhibit the effects of intrinsic factor, resulting in an inability of B12 to be absorbed by the terminal ileum.
Malabsorption–Parietal cells in the stomach produce intrinsic factor; therefore, any patient with a history of gastric bypass surgery may be at risk for developing a B12 deficiency because their new alimentary pathway bypasses the site of intrinsic factor production. In patients with normal intrinsic factor production, any damage to the terminal ileum, such as surgical resection due to Crohn disease, will impair the absorption of B12 and lead to a deficiency. Other damage to the small intestine, such as inflammation from Celiac disease or infection with the tapeworm Diphyllobothrium latum, may also result in a B12 deficiency.
Dietary Insufficiency – Vitamin B12 is stored in excess in the liver; however, patients who have followed a strict vegan diet for approximately three years may develop a B12 deficiency from a lack of dietary intake.
Inadequate dietary intake of vitamin B12 –Vitamin B12 occurs in animal products (eggs, meat, milk) and in some edible algae. B12 isolated from bacterial cultures is also added to many fortified foods, and available as a dietary supplement. Vegans, and to a lesser degree vegetarian, may also be at risk for B12 deficiency due to inadequate dietary intake of B12, if they do not supplement. Children are at a higher risk for B12 deficiency due to inadequate dietary intake, as they have fewer vitamin stores and a relatively larger vitamin need per calorie of food intake.
Selective impaired absorption of vitamin B12 due to intrinsic factor deficiency – This may be caused by the loss of gastric parietal cells in chronic atrophic gastritis (in which case, the resulting megaloblastic anemia takes the name of “pernicious anemia”), or may result from wide surgical resection of stomach (for any reason), or from rare hereditary causes of impaired synthesis of intrinsic factor. B12 deficiency is more common in the elderly because gastric intrinsic factor, necessary for absorption of the vitamin, is deficient, due to atrophic gastritis.
Impaired absorption of vitamin B12 – in the setting of more generalized malabsorption or maldigestion syndrome. This includes any form due to structural damage or wide surgical resection of the terminal ileum (the principal site of vitamin B12 absorption).
Forms of achlorhydria – (including that artificially induced by drugs such as proton pump inhibitors and histamine 2 receptor antagonists) can cause B12 malabsorption from foods, since acid is needed to split B12 from food proteins and salivary binding proteins. This process is thought to be the most common cause of low B12 in the elderly, who often have some degree of achlorhydria without being formally low in intrinsic factor. This process does not affect the absorption of small amounts of B12 in supplements such as multivitamins since it is not bound to proteins, as is the B12 in foods.
Surgical removal of the small bowel – (for example in Crohn’s disease) such that the patient presents with short bowel syndrome and is unable to absorb vitamin B12. This can be treated with regular injections of vitamin B12.
Long-term use of ranitidine hydrochloride may contribute to a deficiency of vitamin B12.
Untreated celiac disease may also cause impaired absorption of this vitamin, probably due to damage to the small bowel mucosa. In some people, vitamin B12 deficiency may persist despite treatment with a gluten-free diet and require supplementation.
Some bariatric surgical procedures, especially those that involve removal of part of the stomach, such as Roux-en-Y gastric bypass surgery. (Procedures such as the adjustable gastric band type do not appear to affect B12metabolism significantly).
Bacterial overgrowth within portions of the small intestine, such as may occur in blind loop syndrome, (a condition due to a loop forming in the intestine) may result in increased consumption of intestinal vitamin B12 by these bacteria.
The diabetes medication metformin may interfere with B12 dietary absorption.
A genetic disorder, transcobalamin II deficiency can be a cause.
Alcoholism – if a “diet” of excessive alcohol intake is substituted for a diet adequate in sources of B12.
Nitrous oxide exposure, and recreational use.
Infection with the Diphyllobothrium latum tapeworm
Chronic exposure to toxigenic molds and mycotoxins found in water damaged buildings.
Increased needs by the body due to AIDS, or hemolysis the breakdown of red blood cells.
Can Calcium Supplements Protect Against PPI-Induced Vitamin B12 Deficiency?
Vitamin B12 is a member of the water-soluble B-vitamin family and therefore is an essential nutrient that must be acquired from the diet [rx]. Vitamin B12 belongs to a class of naturally occurring colbalt-containing compounds known as cobalamins, which contain a planar corrin ring that binds a single colbalt atom. Colbalt is the functional part of vitamin B12, which serves as an enzyme cofactor for two vitamin B12-dependent, enzyme-catalyzed reactions in mammals.
Patients taking acid reducers long term are at greater risk for hypochlorhydria-induced vitamin B12 malabsorption.
Both proton pump inhibitors (PPIs) and histamine-2 receptor antagonists (H2RAs) can block the activity of intrinsic factor. However, the risk is widely inconsistent across studies due to variable samples and confounding designs.
Atrophic gastritis, Crohn’s disease, celiac disease, total or partial gastrectomy, gastric surgery, pancreatectomy, pancreatitis, and ileal resection can also cause vitamin B12 malabsorption. Calcium supplementation may reverse the effect of hypoparathyroidism and metformin-induced vitamin B12 malabsorption.
The Journal of Nutrition Health and Aging recently published a study that shows calcium supplements temper gastric acid inhibitor-induced vitamin B12 malabsorption. This retrospective cross-sectional study collected data from the Quebecois Geriatric Assessment Unit inpatients discharged from January 2008 through March 2012.
Enrolled patients received scheduled H2RA or PPI therapy upon admission. The researchers excluded patients with missing records and hospital stays shorter than 5 days. The prevalence of vitamin B12 deficiency in this cohort (41.3%) was similar to that seen in other studies enrolling patients in rehabilitation units.
Previous studies have shown that calcium chelators decrease intestinal vitamin B12 absorption. No research has shown that PPIs or H2RAs have chelating actions, but PPIs limit absorption of calcium carbonate, the most commonly used calcium supplement.
Quite by accident, the researchers found that patients taking PPIs (but not H2RAS) without concomitant calcium supplements were more likely to have vitamin B12 deficiency than those taking PPIs plus calcium. This indicated that calcium modifies the effect of PPIs significantly.
In the study, calcium supplements protected patients from the effect of gastric acid reducers. Inconsistent prevalence of calcium supplement co-administration between studies can explain the variable risk of vitamin B12 absorption.
The researchers concluded that calcium supplements reduce the vitamin B12 malabsorption effect of gastric acid reducers. They believe future studies should consider calcium supplement co-administration to be a confounder in the risk of vitamin B12 malabsorption.
up date May2017
HealthDay Reporter
(HealthDay News) — People who take certain acid-reflux medications might have an increased risk of vitamin B-12 deficiency, according to new research.
Taking proton pump inhibitors (PPIs) to ease the symptoms of excess stomach acid for more than two years was linked to a 65 percent increase in the risk of vitamin B-12 deficiency. Commonly used PPI brands include Prilosec, Nexium and Prevacid.
Researchers also found that using acid-suppressing drugs called histamine-2 receptor antagonists — also known as H2 blockers — for two years was associated with a 25 percent increase in the risk of B-12 deficiency. Common brands include Tagamet, Pepcid and Zantac.
“This study raises the question of whether or not people who are on long-term acid suppression need to be tested for vitamin B-12 deficiency,” said study author Dr. Douglas Corley, a research scientist and gastroenterologist at Kaiser Permanente’s division of research in Oakland, Calif.
Corley said, however, that these findings should be confirmed by another study. “It’s hard to make a general clinical recommendation based on one study, even if it is a large study,” he said.
Vitamin B-12 is an important nutrient that helps keep blood and nerve cells healthy, according to the U.S. Office of Dietary Supplements (ODS). It can be found naturally in meat, fish, poultry, eggs, milk and other dairy products. According to the ODS, between 1.5 percent and 15 percent of Americans are deficient in B-12.
Although most people get enough B-12 from their diet, some have trouble absorbing the vitamin efficiently. A deficiency of B-12 can cause tiredness, weakness, constipation and a loss of appetite. A more serious deficiency can cause balance problems, memory difficulties and nerve problems, such as numbness and tingling in the hands or feet.
Stomach acid is helpful in the absorption of B-12, Corley said, so it makes sense that taking medications that reduce the amount of stomach acid would decrease vitamin B-12 absorption.
More than 150 million prescriptions were written for PPIs in 2012, according to background information included in the study. Both types of medications also are available in lower doses over the counter.
Corley and his colleagues reviewed data on nearly 26,000 people who had been diagnosed with a vitamin B-12 deficiency and compared them to almost 185,000 people who didn’t have a deficiency.
While 12 percent of people with a vitamin B-12 deficiency had taken PPIs for more than two years, 7.2 percent of those without a deficiency had taken the medications long-term.
Of those with a deficiency, 4.2 percent took an H2 blocker for two years or longer, while 3.2 percent of those without a deficiency took the drugs for two years or more.
The risk of developing a vitamin B-12 deficiency was 65 percent higher for the long-term PPI users and 25 percent higher for those taking H2 blockers, according to the study.
People who took higher doses were more likely to develop a vitamin B-12 deficiency. People who took an average of 1.5 PPI pills per day had almost double the risk of developing a deficiency compared to those who averaged 0.75 pills per day, the study found.
Women had a greater risk of deficiency than men, and people younger than 30 taking these medications had a greater risk of developing a deficiency than older people, according to the study.
The risk of vitamin B-12 deficiency decreases when you stop taking the medications, but doesn’t disappear completely, Corley said.
The study’s findings were published in the Dec. 11 issue of the Journal of the American Medical Association. Although the study found an association between taking acid-reflux drugs long-term and having a higher risk of a B-12 deficiency, it didn’t establish a cause-and-effect relationship.
If you’re taking acid-suppressing medications, Corley said, “our study doesn’t recommend stopping those medications, but you should take them at the lowest effective dose.” And people shouldn’t start taking vitamin B-12 supplements on their own, but should discuss it with their doctor, he said.
One expert had concerns about how frequently acid-suppressing drugs are used.
“This study found an adverse effect associated with taking these drugs,” said Victoria Richards, an associate professor of medical sciences at the Frank H. Netter M.D. School of Medicine at Quinnipiac University, in Hamden, Conn. “It’s also concerning that these drugs are used at such a high rate. Why do so many people have the need to suppress acid so much?”
The bottom line, Richards said, is that if you are having any symptoms of vitamin B-12 deficiency and you’ve been taking these medications, talk to your doctor about whether you should be tested for a deficiency. Tell your doctor if you’ve been taking over-the-counter acid-suppressing medications, so your doctor can properly evaluate your risk.
Interactions with: Vitamin B12 (Cobalamin)
If you are currently being treated with any of the following medications, you should not use vitamin B12 supplements without first talking to your health care provider.
Medications that reduce levels of B12 in the body include:
Anticonvulsants — include phenytoin (Dilantin), phenobarbital, primidone (Mysoline)
Bile acid sequestrants — used to lower cholesterol; include colestipol (Colestid), cholestyramine (Questran), and colsevelam (Welchol)
H2 blockers — used to reduce stomach acid; include cimetidine (Tagamet), famotidine (Pepcid AC), ranitidine (Zantac)
Metformin (Glucophage) — medication taken for diabetes
Proton pump inhibitors — used to reduce stomach acid; include esomeprazole (Nexium), lansprazole (Prevacid), omeprazole (Prilosec), rabeprazole (Aciphex)
Antibiotics, Tetracycline:Vitamin B12 should not be taken at the same time as tetracycline because it interferes with the absorption and effectiveness of this medication. Vitamin B12 should be taken at different times of the day from tetracycline. (All vitamin B complex supplements act in this way and should be taken at different times from tetracycline.)
In addition, long-term use of antibiotics can deplete vitamin B levels in the body, particularly B2, B9, B12, and vitamin H (biotin), which is considered part of the B complex vitamins.
Sadness / depression is a disease that can break the very being of a person.Though about 350 million people all around the world suffer from depression, it still has not been recognized as a serious mental illness in many parts of the world. It’s symptoms are subtle and effects fatal, thus pushing many patients to the brink of death before it is diagnosed. Who knows, even your spouse could be silently suffering from it while you are too caught up with life to notice. Do not wait until it’s too late-here are 7 signs that could tell if your partner is depressed.
The Need To Be Alone of sadness
Has your loved one recently turned anti-social? When a person is depressed, they yearn to stay isolated. If your partner used to have a lot of friends and suddenly wants nothing to do with them, it could be because he or she is mentally unwell. Other symptoms include cancelling social events at the last minute, boycotting family events, avoiding direct conversations, and developing a pessimistic attitude.
Loss of Interest In Things They Once Loved
When going through depression, people slowly develop an aversion towards all the things they one used to enjoy.They could even end up avoiding their spouses as well as children. This could have serious consequences on relationships. If your partner suddenly starts to show disinterest in you or your children, make it a point to find out the reason behind it.
Difficulty To Focus
Depression is known to mess with the cognitive ability of a person. Depressed people tend to lose focus from time to time and have difficulty in remembering stuff. They may also keep tuning in and out of conversations, without knowing what’s really happening around them. If left untreated, this symptom can cause serious cognitive impairment.
The Constant Feeling That They Are Worthless
Depression makes the patients feel like they are never good enough. Depressed people are constantly haunted by a host of negative feelings and self-doubt. This can also be accompanied by guilt, hopelessness, and disappointment. This symptom is the major factor that pushes people towards self harm and suicide.
Since depressed people have a hard time holding on to their senses and emotions, there is a chance they will turn to alcohol and drugs for consolation. Substance abuse happens because the person is trying to numb out their mental and physical pain. This is a dangerous, and at times fatal symptom of depression as it could lead to addiction as well as the death of a patient.
Sudden weight loss is a prominent symptom of depression. If you notice your partner develop an aversion towards food- even the dishes they used to love- depression could be creeping in. While going through depression, the lack of a balanced diet leads to unusual and abrupt weight loss, accompanied by fatigue and exhaustion.
Though depressed people tend to be exhausted all the time, it does not mean they get a lot of sleep. In fact, it’s exactly the opposite. If your partner keeps turning and tossing in bed night after night for no particular reason, it could be because they are disturbed by countless negative thoughts which keep them awake all night long.
References
NIMH. May 2016. Archived from the original on 5 August 2016. Retrieved 31 July 2016.
Sleeping disorder or somnipathy is a medical disorder of the sleep patterns of a person or animal. Some sleep disorders are serious enough to interfere with normal physical, mental, social and emotional functioning. Polysomnography and actigraphy are tests commonly ordered for some sleep disorders
Some sleep disorders are serious enough to interfere with normal physical, mental, social and emotional functioning. Polysomnography and actigraphy are tests commonly ordered for some sleep disorders.
Disruptions in sleep can be caused by a variety of issues, from teeth grinding (bruxism) to night terrors. When a person suffers from difficulty falling asleep and/or staying asleep with no obvious cause, it is referred to as insomnia.
Sleep disorders are broadly classified into dyssomnias, parasomnias, circadian rhythm sleep disorders involving the timing of sleep, and other disorders including ones caused by medical or psychological conditions and sleeping sickness.
Chemical Messenger: How Hormones Help Us Sleeping
The activities we do during the day – from having a fight with a partner to using our iPhones at night – also affect our hormone levels and, in turn, our quality of sleep. Jan Faukner/Shutterstock
When it comes to motives for getting a good night’s sleep we don’t usually think about our body’s hormones. But sleep allows many of our hormones to replenish so we have the optimal energy, immunity, appetite and coping ability to face the day’s highs and lows.
The activities we do during the day – from having a fight with a partner, using our iPhones at night, running in a race, to travelling overseas – also affect our hormone levels and, in turn, our quality of sleep.
For both men and women, changes in our levels of sex hormones can affect how well we sleep. These differences also change with age.
Understanding the connections between hormones and sleep may help improve your own sleep and well-being.
What are hormones?
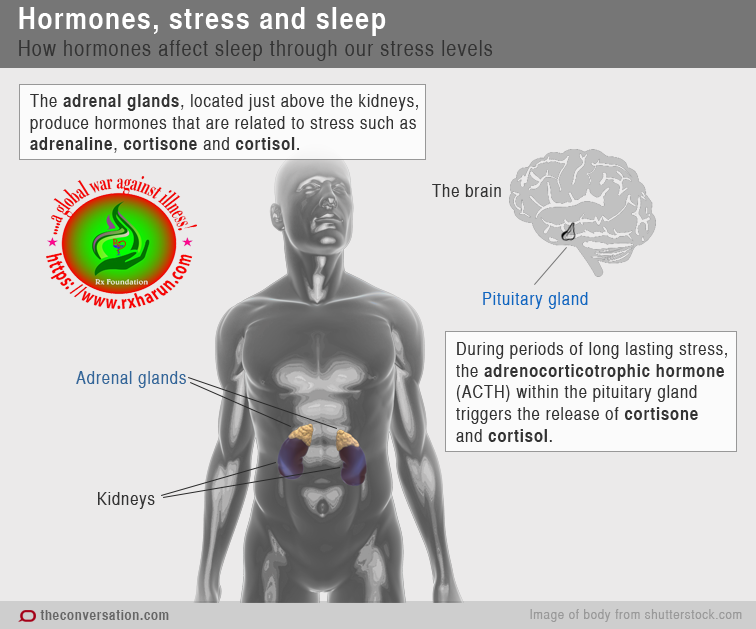
Our body’s hormones are like chemical messages in the bloodstream which cause a change in a particular cell or organ and surrounding tissues. The hormone adrenaline, for example, is produced by the adrenal glands (on top of the kidneys) and helps prepare the body’s “fight or flight” response during times of stress.
Hormones control many of the body’s processes, including growth, development, reproduction, responding to stress, metabolism and energy balance.
Hormones are linked with sleep in a number of ways.
Hormones affect sleeping through our stress levels
Some hormones, such as adrenaline, make us feel more alert and prepared for action. This then makes it hard for us to go to sleep. To prevent this effect it’s best to do relaxing activities before bedtime, rather than stressful work tasks or intense exercise.
When stress is long lasting, adrenocorticotrophic hormone within the pituitary gland (attached to the base of the brain) triggers the release of cortisone and cortisol from the adrenal glands.
Levels of adrenocorticotrophic hormone tend be higher in people with insomnia than in good sleepers. This suggests that excessive arousal and ongoing stressors contribute to the insomnia.
Elite athletes can have difficulty getting to sleep because they tend to have high levels of cortisol throughout the day, including in the evening.
Hormones released during sleep boost our immune system and make us hungry
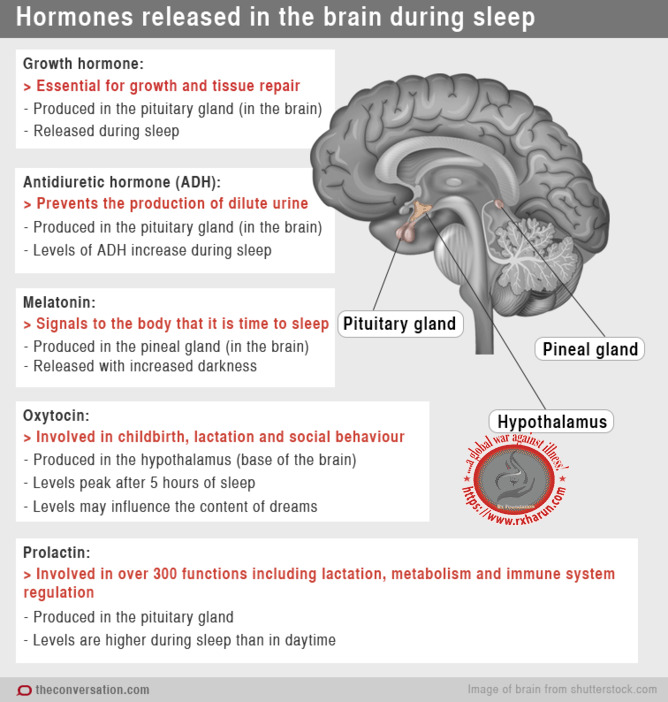
Sleep is a time when several of the body’s hormones are released into the bloodstream. These include growth hormone, which is essential for growth and tissue repair, including in adults.
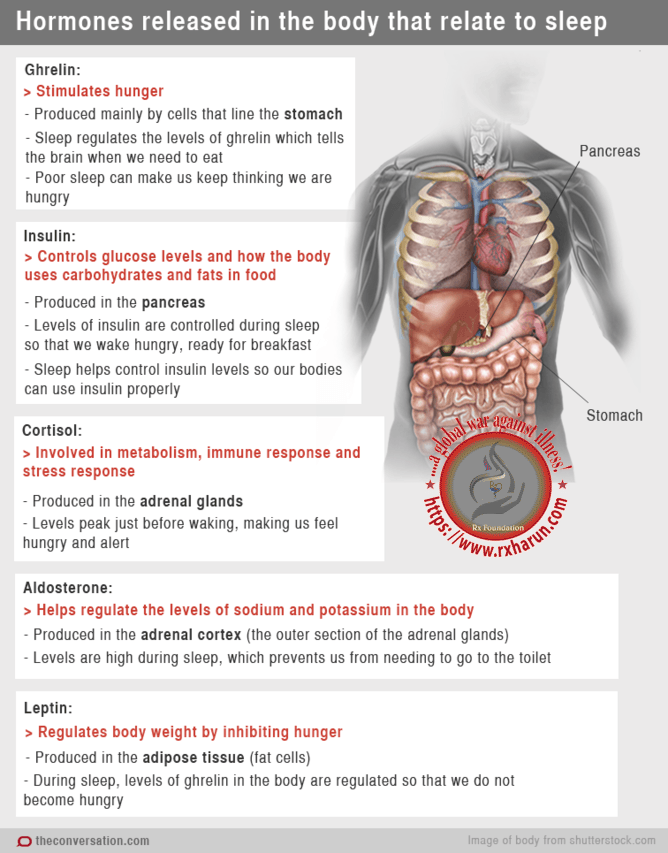
Sleep helps to balance our appetite by maintaining optimal levels of the hormones ghrelin and leptin. So, when we get less sleep than normal we may feel an urge to eat more.
Sleep also controls levels of the hormones insulin and cortisol so that we wake up hungry, prompting us to eat breakfast, and we are prepared for facing daytime stress.
If we get less sleep than normal our levels of prolactin may get out of balance and we can end up with a weakened immune system, difficulty concentrating and carbohydrate cravings during the day.
Hormones stop us from having to get up in the night to go to the bathroom
Changes in hormonal levels during sleep, including higher levels of aldosterone and antidiuretic hormone, prevent us from needing to go to the toilet. In children, while the hormonal system is still developing, bedwetting may be partly influenced by low levels of antidiuretic hormone.
Hormones make us feel sleeping at night
Hormone levels also influence the timing of when we feel sleepy and awake – our body clock or sleep-wake cycle. The hormone melatonin is released with darkness and tells our body it’s time to sleep. This is why being around too much bright light before bed can affect our sleep as it can stop the release of melatonin. It’s also why it can be hard for night-time shift workers to sleep during the day.
While artificial melatonin is available, taking the wrong dosage and at the wrong time of day can make things worse, so it’s best used with the guidance of a medical doctor.
Hormones give us a wake-up call in the morning
Levels of the hormone cortisol dip at bedtime and increase during the night, peaking just before waking. This acts like a wake-up signal, turning on our appetite and energy.
When we travel long distances our body’s sleep-wake cycle takes a while to adjust. So increased cortisol levels and hunger may occur at inappropriate times of the day.
For women, changes in sex hormones affect sleep
The relationship between hormones and the sleep-wake cycle in women is further influenced by the menstrual cycle. Just before a woman’s period, hormonal changes, including the sudden drop in levels of progesterone, affect the body’s temperature control, which in turn can reduce the amount of “REM” sleep. This is the stage of sleep when most of our dreams occur.
For women with severe premenstrual symptoms reduced levels of melatonin before bedtime just before their menstrual period can cause poor sleep, including night-time awakenings or daytime sleepiness.
Changes in hormone levels also contribute to sleeping difficulties during pregnancy. Increased progesterone levels can cause daytime sleepiness, particularly in the first trimester. High levels of oestrogen and progesterone during pregnancy can also cause nasal swelling and lead to snoring.
During menopause, low levels of oestrogen may contribute to sleeping difficulties. Changes in hormone levels mean that body temperature is less stable and there may be increases in adrenaline levels, both of which can affect sleep.
The loss of oestrogen causes body fat to move more to the stomach area, which increases the chances of women having snoring and sleep apnoea.
For men, testosterone levels affect sleep
For men, levels of testosterone are highest during sleep and require at least three hours of sleep to reach this peak. Low levels of testosterone in men, which can occur with sleep deprivation, ageing and physical problems, have been associated with a reduction in sleep efficiency and changes to the stages of sleep men experience.
Testosterone can be taken as a drug but abuse of it can lead to other sleep problems.
Hormones influence our dreams
Finally, as we sleep, our hormones, including levels of oxytocin and cortisol, may influence the content of our dreams.
By doing things to promote good sleep, such as reducing stress, engaging in relaxing evening routines before bed, going to bed and getting up at regular times, or seeking professional help for sleeping difficulties, we can facilitate the replenishing activities of our hormones that help us make the most of our day and optimise our well-being.
This article is part of an occasional series, Chemical Messengers, on hormones and the body. Stay tuned for other articles on hunger, mood and sexual desire.