What Is Swimmer’s Shoulder?/Swimmer’s Shoulder is an umbrella term covering a range of painful shoulder overuse injuries that occur in swimmers. Because there are various parts of your shoulder that can be injured from your swimming stroke, your pain can be anything from a local pain near the shoulder joint, to a spreading pain that travels up your shoulder and neck or down into your arm. Being an overuse injury, it is caused by repeated trauma rather than a specific incident.
Swimmers have a significant potential for shoulder injuries due to the unique nature of the different strokes involved in swimming as well as the high volume of repetitions needed during training. Swimmer’s shoulder is a term that can represent numerous shoulder pathologies. These include impingement syndrome, rotator cuff tendinitis, labral injuries, instability secondary to ligamentous laxity or muscle imbalance/dysfunction, neuropathy from nerve entrapment, and anatomic variants. In order for the athlete to return to the sport in an appropriate and timely manner, the clinician must be able to differentiate between these different etiologies. [rx][rx]
Swimmer’s shoulder is the term used to describe the problem of shoulder pain in the competitive swimmer. Swimming is an unusual sport in that the shoulders and upper extremities are used for locomotion, while at the same time requiring above average shoulder flexibility and range of motion (ROM) for maximal efficiency. This is often associated with an undesirable increase in joint laxity. Furthermore, it is performed in a fluid medium, which offers more resistance to movement than air. This combination of unnatural demands can lead to a spectrum of overuse injuries seen in the swimmer’s shoulder, the most common of which is rotator cuff tendinitis.
Pathophysiology
Swimming strokes can be broken down into pull-through and recovery phases. The latissimus dorsi and the pectoralis major are the primary contributors to the propulsive forces of the swim stroke by adduction and internal rotation. The subscapularis and serratus anterior muscles also play an integral role in the freestyle stroke. [rx][rx][rx][rx][rx]The freestyle stroke can be divided into six distinct parts/phases:
-
Hand entry
-
Forward reach
-
Pull through
-
Middle pull through
-
Hand exit
-
Middle recovery
It is important for the athlete to have a properly balanced shoulder regarding muscle strength. Improper muscle balancing can cause the onset of shoulder pain. An absolute or sudden increase in training yardage and poor technique can also be associated with the onset of pain. The coaching staff can observe a dropped elbow during the recovery phase of the freestyle stroke as one of the early signs of possible injury.
Causes of Swimmer’s Shoulder
- Overtraining
- Not enough rest periods
- Poor stroke mechanics
- Poor breathing technique
- Poor flexibility or range of motion
- Decreased rotator cuff or shoulder blade (scapular muscle) strength
- Poor core strength or stability
- Decreased hip muscle strength
- Shoulder pain in swimmers includes subacromial impingement,
- Rotator cuff tendinopathy, labral pathology,
- Suprascapular nerve entrapment, or any combination thereof.
- Additionally, an injury may be accompanied or exacerbated by structural abnormalities including scapular dyskinesis, glenohumeral hyperlaxity, excess subluxation, glenohumeral internal rotation deficit (GIRD), or muscle strength imbalances.
Symptoms of Swimmer’s Shoulder
The most common swimmer’s shoulder symptoms include:
- Reduced range of motion in your shoulder compared to your other shoulder.
- Increased joint laxity than with the other shoulder.
- Reduced strength when compared with your other shoulder.
- If you’re experiencing shoulder pain while swimming, you should consult with a shoulder expert as soon as possible to avoid the problem from becoming worse stop swimming and rest your shoulder to help reduce the inflammation
- Localized pain is felt in the affected part of the shoulder
- Pain may extend to the neck and/or down the arm in some cases
- Pain worsens while resting on the affected shoulder
- Tenderness of the affected area
- Decreased range of movement
- The decrease in shoulder strength
- Increased joint laxity
Technically speaking, some common characteristics of swimmer’s shoulder are
- Bicep and supraspinatus tendon inflammation within the subacromial muscles in the back leading to shoulder impingement syndrome.
- Training errors, like overloading, overtraining and particularly poor stroke technique.
- The onset of symptoms tends to be linked with altered shoulder joint mobility, posture, muscle performance or neuromuscular control.
- Many swimmers have innate ligamentous laxity while also having multidirectional shoulder instability, or basically, more joint movement.
- However, due to the nature of swimming, all swimmers can develop imbalances in the muscle where the internal rotators and adductors of the arm over-develop. This can leave a weakness of the scapular stabilizers and external rotators, unfortunately, because they’re not being used as much.
Diagnosis of Swimmer’s Shoulder
- Physical examination is the first step in the process of diagnosis
- X-rays and other imagining techniques may be needed to assess the changes in the structure of the joint
- The doctor may check for any change in the pattern of swimming stroke
- The presence of ‘lazy elbow’ where the elbow on the affected side cannot be lifted to the normal height out of the water.
Shoulder Apprehension Test
- Place the shoulder in maximum abduction and external rotation (90-90 position) and apply an anteriorly-directed force to the shoulder from behind. To be positive, it must elicit a feeling of apprehension or instability. Generally, the only discomfort is seen in swimmers rather apprehension or sense of instability.
Load and Shift Test
- With the patient seated, stabilize the scapula to the thorax with one hand, while the other hand is placed across the posterior glenohumeral joint line and humeral head, and the webspace across the patient’s acromion. The index finger should the over the anterior GH joint line.
- Load and shift of the humeral head across the stabilized scapula in an anteromedial direction to assess anterior stability, and in a posterolateral direction to assess posterior instability is done. Normal motion anteriorly is half of the distance of the humeral head, more movement is considered to be a sign of glenohumeral joint laxity.
Strength Assessment of Rotator Cuff
Subscapularis
- Internal rotation movement against resistance
- Lift-off test
- Shoulder in internal rotation with the back of the patient’s hand against the small of the back.
- The patient attempts to lift the hand away from the back against the examiner’s resistance.
Infraspinatus, teres minor
- External Rotation against resistance [shoulder in the neutral position at the side and the elbow flexed to 90°.
Supraspinatus
- Resisted shoulder elevation with the arms extended, internally rotated, and positioned in the scapular plane (approximately 30-45° anterior to the coronal plane).
- If weak, retest the supraspinatus in the same arm position except with the arms externally rotated (ie, thumbs pointing upwards).
Sulcus Sign [Assessment of Joint Laxity]
The arm is pulled inferiorly and gap or sulcus is looked between the humeral head and lateral edge of the acromion. This indicates the inferior subluxation of the humeral head.
- Grade 1 – Less than 1 fingerbreadth (< 1 cm)
- Grade 2 – One fingerbreadth (1-2 cm)
- Grade 3 – Greater than 1 fingerbreadth (> 2 cm)
Compare to the opposite shoulder (should be similar). If not then consider unilateral traumatic injury. In addition, check for generalized ligamentous laxity.
Tests for Labral Tear
- A labral tear is suggested by a painful click that is noted during the recovery phase of an overhand stroke. Often, this click can be reproduced during the exam.
O’Brien test for Labral Tear [SLAP Lesion]
- A downward force is applied with the extent in the forward flexed position, adducted 15° toward the midline, with the shoulder in the maximal internal rotation (thumb pointing down). A pain that occurs in this position and relieved when external rotation is done suggests a SLAP lesion.
Positive Neer impingement test
If a subacromial injection relieves pain associated with passive forward flexion >90°
- Positive Hawkins test – positive if internal rotation and passive forward flexion to 90° causes pain
- Jobe test – pain with resisted pronation and forward flexion to 90° indicates supraspinatus pathology
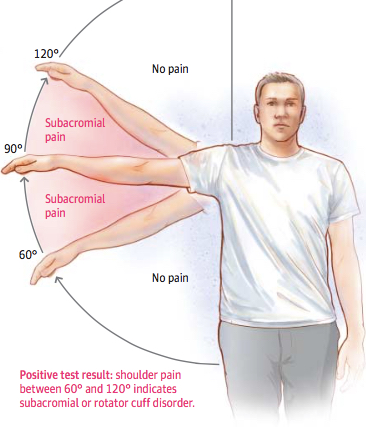
- Painful Arc Test – pain with the arm abducted in the scapular plane from 60° to 120°
- Yocum Test – positive if pain reproduced with elbow elevation while ipsilateral hand placed on the contralateral shoulder. sensitive but nonspecific
- Internal Impingement test – positive if the pain is elicited with the abduction and external rotation of the shoulder
- Take medical history, with emphasis on pain, sleep disturbance, loss of function and treatments.
- Perform a physical examination, documenting the range of motion, strength and shoulder impingement signs.
{kind=link}
X-rays
- X-rays are performed to rule out bony causes of shoulder pain like a stress fracture or lesion or loose body. X-rays should be obtained if the pain persists after 6 weeks of rest and rehabilitation.
- The desirable x-rays are anteroposterior (AP) y-scapular or outlet view and axillary view of the shoulder.
Magnetic Resonance Imaging
- MRI is able to tell about rotator cuff pathology and status of the bones, ligaments, and other tendons in the shoulder.
- But in most of cases, the MRI is normal or in some cases may demonstrate some increased signal in the substance of the supraspinatus tendon. Fluid in the subacromial bursa may signify bursitis. MRI arthrogram with intraarticular gadolinium is able to depict labral tear.
Diagnostic Subacromial Injection
- Subacromial injection of an anesthetics agent like lignocaine can be used for diagnosis. Immediate relief of pain following the injection suggests an injury of the rotator cuff and/or the overlying bursa. Intra-articular injection providing relief, on the other hand, suggests intraarticular pathology.
Treatment of Swimmer’s Shoulder
Swimmers Shoulder Treatment Options
- Rest is important to allow the joint to heal
- Application of ice packs may be recommended to reduce pain and inflammation
- Sling or shoulder tape may give adequate support
- Physiotherapy sessions may be recommended to improve strength and flexibility
- Early Injury Treatment
- Avoid the HARM Factors
- Acupuncture and Dry Needling
- Sub-Acute Soft Tissue Injury Treatment
- Core Exercises
- Scapular Stabilisation Exercises
- Shoulder Exercises
- Biomechanical Analysis
- Proprioception & Balance Exercises
- Medications
- Posture Correction
- Soft Tissue Massage
- Brace or Support
- Dry Needling
- Electrotherapy & Local Modalities
- Heat Packs
- Joint Mobilisation Techniques
- Kinesiology Tape
- Neurodynamics
- Prehabilitation
- Scapulohumeral Rhythm Exercises
- Strength Exercises
- Stretching Exercises
- Supportive Taping & Strapping
- TENS Machine
- Video Analysis
- Yoga
Immediate Treatment
Identifying the involved tendons or muscles, the severity or stage of the problem and receiving proper diagnosis will result in the most efficient treatment. A proper plan of treatment includes:
- Applying ice – Apply directly to the shoulder after training for around 20 minutes.
- Use anti-inflammatory medications – Use for a few days after the injury to reduce inflammation.
- Rest – This might mean total rest with no swimming for about 24 to 48 hours depending on the severity. Or, you may be able to swim, but decrease yardage while you avoid butterfly, backstroke or kicking only with your arms at your side. Wait a few days until you’re free of pain before you resume swim training.
Medication
Your doctor may prescribe anti-inflammation pills. These could form a very important part of the treatment.
- Analgesics – Prescription-strength drugs that relieve pain but not inflammation.
- Antidepressants – A Drug that blocks pain messages from your brain and boosts the effects of exorphins (your body’s natural painkillers).
- Medication – Common pain remedies such as aspirin, acetaminophen, ibuprofen, and naproxen can offer short-term relief. All are available in low doses without a prescription. Other medications, including muscle relaxants and anti-seizure medications, treat aspects of spinal stenoses, such as muscle spasms and damaged nerves.
- Corticosteroid injections – Your doctor will inject a steroid such as prednisone into your back or neck. Steroids make the inflammation go down. However, because of side effects, they are used sparingly.
- Manual Therapy – Your physical therapist may use manual techniques, such as gentle joint movements, soft-tissue massage, and shoulder stretches to get your shoulder moving properly so that the tendons and bursa avoid impingement.
- Range-of-Motion Exercises – You will learn exercises and stretches to help your shoulder and shoulder blade move properly, so you can return to reaching and lifting without pain.
- Mobility and stretching – Stretches can be done on a daily basis assuming there is no pain. Stretching must be done regularly and continued throughout the rehabilitation process. Below are some important stretches would be performed in order to encourage a full range of motion and improved posture.
Get professional passive care. This might include things like
- Interferential current
- Ultrasound
- Trigger point work
- Cross friction tendon massage
- Adjustments to your neck or shoulder
- Post-isometric relaxation of the muscles involved
Do rehabilitation exercises
- These will strengthen your weak muscles (particularly your external shoulder rotators). You perform these exercises with minimal weights (three to five pounds) and perform them in an extremely controlled, specific manner. Perform these exercises a few times a week if you’ve ever had problems with your shoulders. Typically, it’s said that for each day you swim on a bad shoulder, you’ll require one day of rehab.
Modify your swimming training
- It’s often said hand paddles aren’t good for your shoulders. But, Zoomers and other types of fins keep your body elevated in the water; therefore, they might help if you begin experiencing small problems with your shoulders during your workout. Ask the coach or a friend to check your body and arm position. They may even want to videotape you so you can take a look and the coach can discuss the stroke mechanics with you.
Shoulder Stretching and Dynamic Warm-Up
- The shoulder is the most frequently stretched joint among swimmers. To date, swimmers have adopted stretches that target the static stabilizers of the GHJ. In the past, static stretches and pre-race rituals (i.e., ballistic windmill motion) were utilized in hopes of preventing injury [rx].
- Recent research on swimmer’s flexibility suggests there is no indication that extraordinary shoulder joint motion or flexibility is necessary to achieve a fast, efficient stroke [rx, rx]. In addition, there is no evidence that static stretching immediately before activity will reduce muscle injury rates [rx, rx].
- Many swimmers are generally flexible and possess loose connective tissue (general joint laxity) [rx]. Because of their inherent laxity, swimmers should emphasize preserving the overall stability of the shoulder and less time on general static stretches [rx].
- Instead, a dynamic warm-up has been found to produce short-term and long-term performance enhancements in power, agility, strength, muscle endurance, and anaerobic capacity [rx, rx, rx, rx].
- A dynamic warm-up tends to include some form of dynamic stretching, agility, and plyometric activities and specific motor pattern movements [rx]. Demonstrates dynamic warm-up which is specifically designed for the swimming population. Swimmers should employ a steady pace with each activity and avoid ballistic type motions.
Focused Strengthening Exercises
- Dryland training has been an important part of strengthening programs among swimmers at different ages and skill levels. The main focus of these training programs seems to be the spine and core strengthening [rx]. Strength deficits can play an important role in fatigue development.
- The majority of swimmers demonstrated signs of scapular dyskinesis in the course of a 100-min swimming session [rx]. Through EMG analysis of the painful shoulder, discovered muscle activity of the serratus anterior is significantly depressed through the important pull-through phase in swimmers with shoulder pain [rx].
- Revealed in the course of a swim season the internal rotators of competitive swimmers become proportionally stronger when compared to their antagonists, increasing muscle imbalance, and the risk of an injury process [rx, rx].
- Fatigue may lead to a short-term decrease in acromiohumeral distance [rx]. As a result, a dryland program focusing on the shoulder external rotators and the scapular stabilizers would be of benefit and should be recommended as routine prophylactic measures [rx]. Strengthening internal rotators should be de-emphasized.
Rehabilitations of Swimmer’s Shoulder
Phase 1- Pain Relief and Anti-inflammatory Tip
As with most soft tissue injuries the initial treatment is RICE – Rest, Ice, Compression and Elevation.
- In the early phase, you’ll most likely be unable to fully lift your arm or sleep comfortably. You should stop doing the movement or activity that provoked the shoulder pain in the first place and avoid doing anything that causes pain in your shoulder.
- You may need to wear a sling or have your shoulder taped to provide pain relief. In some cases, it may mean that you need to sleep relatively upright or with pillow support.
- Ice is a simple and effective modality to reduce your pain and swelling. Apply for 20-30 minutes every 2 to 4 hours during the initial phase, or when you notice that your injury is warm or hot.
- Anti-inflammatory medication (if tolerated) and natural substances (eg arnica) may help reduce your pain and swelling. However, it is best to avoid anti-inflammatory drugs during the initial 48 to 72 hours when they may encourage additional bleeding. Most people can tolerate paracetamol as pain-reducing medication. As you improve, supportive taping will help to both support the injured soft tissue and reduce excessive swelling.
Your osteopath will utilize a range of pain relief techniques including joint mobilizations and massage to assist you during this painful phase.
Phase 2- Regain Full Range of Motion
- If you protect your injured rotator cuff structures appropriately the injured tissues will heal. Inflammed structures eg (tendonitis, bursitis) will settle when protected from additional damage.
- Symptoms related to swimmers’ shoulders may take several weeks to improve. During this time it is important to create an environment that allows you to return to normal use quickly and prevent a recurrence.
- It is important to lengthen and orientate your healing scar tissue via joint mobilizations, massage, shoulder muscle stretches and light active-assisted and active exercises.
- Researchers have concluded that osteopathic treatment will improve your range of motion quicker and, in the long-term, improve your functional outcome.
- In most cases, you will also have developed short or long-term protective tightness of your joint capsule (usually posterior) and some compensatory muscles. These structures need to be stretched to allow normal movement.
- Signs that you have full soft tissue extensibility include being able to move your shoulder through a full range of motion. In the early stage, this may need to be passively helped (by someone else) eg. your osteopath. As you improve you will be able to do this under your own muscle power.
Phase 3- Restore Scapular Control
Your shoulder blade (scapula) is the base of your shoulder and arm movements.
- Normal shoulder blade-shoulder movement – known as scapulohumeral rhythm is required for a pain-free and powerful shoulder function. Alteration of this movement pattern results in impingement and subsequent injury.
- Researchers have identified poor scapulohumeral rhythm as a major cause of rotator cuff impingement. Any deficiencies will be an important component of your rehabilitation. Plus, they have identified scapular stabilization exercises as a key ingredient for successful rehabilitation.
Phase 4- Restore Normal Neck Scapulo-Thoracic Shoulder Function
It may be difficult to comprehend, but your neck and upper back (thoracic spine) are very important in the rehabilitation of shoulder pain and injury.
- Neck or spine dysfunction can not only refer pain directly to your shoulder, but it can affect a nerve’s electrical energy, causing weakness and altered movement patterns.
- Plus, painful spinal structures from poor posture or injury do not provide your shoulder or scapular muscles with a solid pain-free base to act upon.
- In most cases, especially chronic shoulders, some treatment directed at your neck or upper back will be required to ease your pain, improve your shoulder movement and stop the pain or injury returning.
Phase 5- Restore Rotator Cuff Strength
- It may seem odd that you don’t attempt to restore the strength of your rotator cuff until a later stage in the rehabilitation. However, if a structure is injured we need to provide nature with an opportunity to undertake primary healing before we load the structures with anti-gravity and resistance exercises.
- Having said that, researchers have discovered the importance of strengthening the rotator cuff muscles with a successful rehabilitation program. These exercises need to be progressed in both load and position to accommodate for which specific rotator cuff tendons are injured and whether or not you have a secondary condition such as bursitis.
Phase 6 – Restore Technique, Speed, Power, and Agility
Swimming requires repetitive arm actions, which place enormous forces on your body (contractile and non-contractile).
- In order to prevent a recurrence as you return to swimming, your osteopath will guide you with exercises to address these important components of rehabilitation to both prevent a recurrence and improve your sporting performance.
- Depending on what your training or competitive program entails, a speed, agility, technique correction, and power program will be customized to prepare you for swimming-specific training.
Phase 7 – Return to Swimming
- Depending on the demands of your swimming season, you will require individual exercises and a progressed training regime to enable a safe and injury-free return to swimming.
- Your osteopath will discuss your goals, time frames and training schedules with you to optimize you for a complete return to swimming.
- The perfect outcome will have you performing at full speed, power, agility and function with the added knowledge that a thorough rehabilitation program has minimized your chance of future injury.
Prevention
Tips for Improving Stroke Mechanics
It’s important to gradually increase the intensity and length of swims to avoid overtraining. Allow the body proper rest periods between competitions and training sessions.
Below we’ve outlined the swim stroke techniques for each stroke to help prevent common swimming injuries.
Freestyle stroke
- When breathing, keep the head in line with the body to avoid neck pain or numbness and tingling in the arms.
- Rotate the body toward the breathing side to avoid turning the neck too far and over-reaching with the arms.
- Breathe equally to both sides to prevent excess stress on one side of the neck.
Backstroke
- Weak muscles in the front of the neck will tire more quickly than strong ones, resulting in neck soreness with increased laps.
- Swimmers just starting to swim this stroke should gradually increase both distance and intensity.
- Rotating the body properly with each stroke also will help decrease stress on the neck and shoulders.
Breaststroke
- Keep the head in line with the body to avoid increased stress on the neck.
- Strong thigh and hip muscles will make for a stronger kick and a faster swim.
- Leg strength will also help decrease the stress and strain placed on the knees as swimming distance increases.
Butterfly
- The proper timing of this stroke decreases the possibility of the neck, shoulder, or back pain.
- Focusing on a strong kick and upper body will aid in body position, as well as breathing.
References
