Selumetinib – Shrinks Tumors, Provides Clinical Benefit NF1
Selumetinib/Findings from a phase 2 clinical trial show that the [...]
Selumetinib/Findings from a phase 2 clinical trial show that the [...]
Arenaviruses are enveloped viruses (about 120 nm diameter) with a [...]
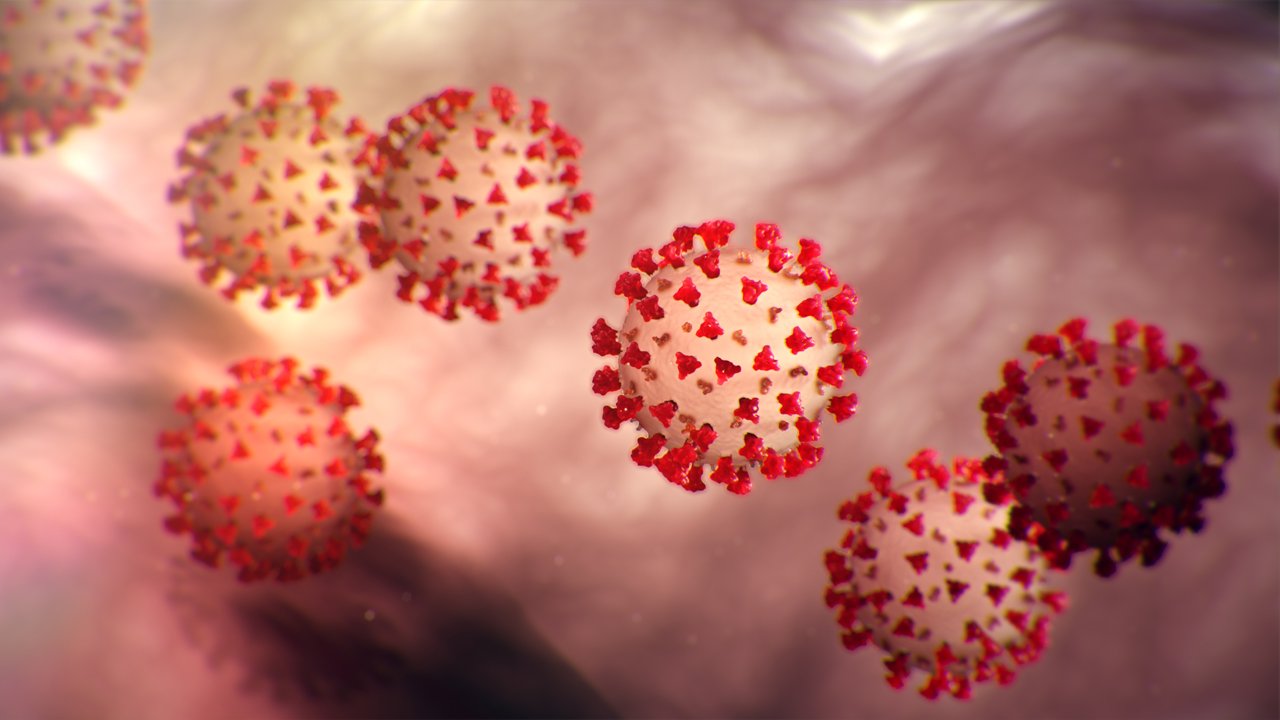
Latest Update of Coronavirus/Coronavirus (CoV) are a large family of viruses [...]
Stem Cell Therapies /Researchers hope stem cells will one day [...]
What Are The Most Common Side Effects of Antibiotics/Antibiotics also called [...]
Lyme disease is the most common tick-borne disease in the [...]
Asthma Latest Research is a chronic lung disease that inflames and [...]
Tiemonium Methylsulfate is a synthetic antispasmodic agent. Tiemonium strengthens calcium [...]
Nitazoxanide is a synthetic benzamide with antiprotozoal activity. Nitazoxanide exerts its antiprotozoal activity by interfering [...]
Metronidazole is a synthetic nitroimidazole derivative with antiprotozoal and antibacterial activities. Although its [...]
Medication/Drugs is any substance (other than food that provides nutritional support) that, when inhaled, injected, smoked, consumed, absorbed via [...]
Antidiabetes drugs is used in diabetes treat diabetes mellitus by lowering glucose levels in the [...]
We Inspire with our business services
through the agency’s dream to strive for
the excellence.
© Avada Studio • All rights reserved.
Powered by WordPress