Ablative Nerve Block – Indications, Contraindications
Ablative Nerve Block/Ablation is the destruction (also called ablation) of nerves is a [...]
Ablative Nerve Block/Ablation is the destruction (also called ablation) of nerves is a [...]
Water-cooled radiofrequency (WCRF) ablation uses a specialized needle that is heated [...]
Pulsed Radiofrequency (PRF) Ablation /Ablation is the destruction (also called ablation) [...]
Conventional Continuous Radiofrequency (CRF) Ablation/Ablation is the destruction (also called ablation) [...]
Ablation is the destruction (also called ablation) of nerves is a method that [...]
Charlie horse is a popular colloquial term used for painful [...]
Meningitis Symptoms/Meningitis is inflammation of the meninges covering the brain. [...]
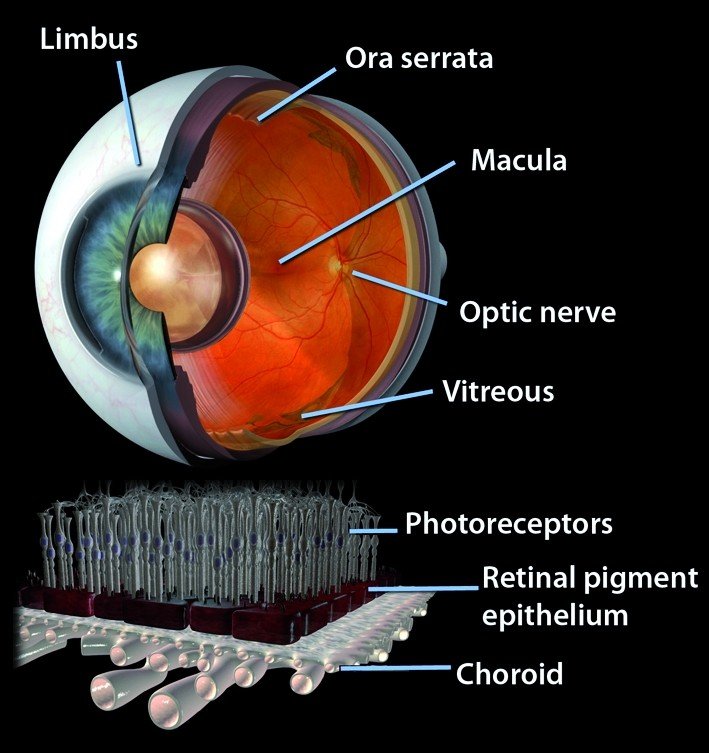
Retinal detachment (RD), defined as the separation of the neurosensory [...]
Treatment of Meningitis/Meningitis is inflammation of the meninges covering the [...]
Parasitic Meningitis/Meningitis is inflammation of the meninges covering the brain. [...]
Fungal Meningitis/Meningitis is inflammation of the meninges covering the brain. [...]
Viral Meningitis, Causes, Symptoms, Treatment/Meningitis is inflammation of the meninges [...]
We Inspire with our business services
through the agency’s dream to strive for
the excellence.
© Avada Studio • All rights reserved.
Powered by WordPress