Cervical myelopathy occurs when the spinal cord is compressed. Spinal cord compression can cause neurologic symptoms – such as pain, numbness, or difficulty walking. Your spinal cord is the conduit that enables communication between your brain and body. The spinal cord begins at the base of the brain and ends at the first lumbar vertebra (L1). Below L1, the spinal cord becomes the cauda equina; a bundle of lumbar and sacral nerves.
Anatomy of Cervical Myelopathy
Your spine is made up of 24 bones, called vertebrae, that are stacked on top of one another.
The seven small vertebrae that begin at the base of the skull and form the neck comprise the cervical spine.
Other parts of your spine include
Spinal cord and nerves. The spinal cord extends from the skull to your lower back and travels through the middle part of each stacked vertebra, called the central canal. Nerves branch out from the spinal cord through openings in the vertebrae (foramen) and carry messages between the brain and muscles.
Intervertebral disks. In between your vertebrae are flexible intervertebral disks. They act as shock absorbers when you walk or run.
Intervertebral disks are flat and round and about a half inch thick. They are made up of two components:
Annulus fibrosus. This is the tough, flexible outer ring of the disk.
Nucleus pulposus. This is the soft, jelly-like center of the disk.
Animation courtesy Visual Health Solutions, Inc
About Myelopathy
More common in adults age 50 and older
Most often affects the cervical spine (neck)
Less common in the thoracic spine (mid back)
Sometimes affects the low back (eg, severe lumbar spinal stenosis)
Usually a gradual and progressive disorder
Can develop quickly (eg, trauma, injury)
Below is a lateral MRI of a patient’s cervical spine. The red arrow points to areas where the spinal cord is compressed—cervical myelopathy.
Symptoms of Cervical Myelopathy
Neck pain and stiffness
Tingling
Numbness
Weakness
Find yourself dropping things
Hand clumsiness (eg, buttoning a shirt)
Balance problems
Difficulty walking
Tingling or numbness in the arms, fingers, or hands
Weakness in the muscles of the arms, shoulders, or hands. You may have trouble grasping and holding on to items.
Imbalance and other coordination problems. You may have trouble walking or you may fall down. With myelopathy, there is no sensation of spinning, or “vertigo.” Rather, your head and eyes feel steady, but your body feels unable to follow through with what you are trying to do.
Loss of fine motor skills. You may have difficulty with handwriting, buttoning your clothes, picking up coins, or feeding yourself.
Pain or stiffness in the neck
Possible Causes
There are many different causes of myelopathy; several are listed below.
Cervical kyphosis
Cyst or tumor
Degenerative spondylosis (spinal arthritis)
Epidural abscess, infection
Herniated disc
Inflammatory diseases (eg, Rheumatoid Arthritis)
Osteophytes (bone spurs)
Spinal Stenosis
Spondylolisthesis
Vertebral body abnormality
Diagnosis of Cervical Myelopathy
The neurological exam is non-invasive and evaluates your sensory and motor functions. Sensory functions are related to your senses, such as sight, hearing, eye movement, and touch. Motor functions are related to your gait (how you walk), balance, coordination, reflexes, the range of motion, and muscle movement.
Physical Examination
After discussing your medical history and general health, your doctor will ask you about your symptoms. He or she will conduct a thorough examination of your neck, shoulders, arms, hands, and legs, looking for:
Changes in reflexes—including the presence of hyperreflexia, a condition in which reflexes are exaggerated or overactive
Numbness and weakness in the arms, hands, and fingers
Trouble walking, loss of balance, or weakness in the legs
Atrophy—a condition in which muscles deteriorate and shrink in size
Clinical Examination
The diagnosis of CSM is primarily based on the clinical signs found on physical examination and is supported by imaging findings. According to Cook et al, selected combinations of the following clinical findings are effective in ruling out and ruling in cervical spine myelopathy. Combinations of three of five or four of five of these tests enable the post-test probability of the condition to 94–99%:
gait deviation
+ve Hoffmann’s test
inverted supinator sign
+ve Babinski test
age 45 years or older
Other clinical examination tests often used for myelopathy include
Spurling’s test
Distraction test
+ve clonus/Babinski/Hoffman’s
Hyperreflexic biceps
Hyperreflexia quadriceps
Hyperreflexia achilles
Pain constancy
L’hermitte’s sign
Romberg test
Although these tests exhibit moderate to substantial reliability among skilled clinicians, they demonstrate low sensitivity and are not appropriate for ruling out myelopathy. One method used to improve the diagnostic accuracy of clinical testing is combining tests into clusters. These often overcome the inherent weakness of stand-alone tests.
These provide images of dense structures, such as bone. An x-ray will show the alignment of the vertebrae in your neck.
Magnetic resonance imaging (MRI) scans
These studies create better images of the body’s soft tissues. An MRI can show spinal cord compression and help determine whether your symptoms are caused by damage to soft tissues—such as a bulging or herniated disk.
This MRI image shows herniated disks pressing on the spinal cord (red arrows).
Computed tomography (CT) scans – More detailed that a plain x-ray, a CT scan can show narrowing of the spinal canal and can help your doctor determine whether you have developed bone spurs in your cervical spine.
Myelogram –This is a special type of CT scan. In this procedure, a contrast dye is injected into the spinal column to make the spinal cord and nerve roots show up more clearly.
In some cases, doctors use nerve conduction studies to measure how well the cervical spinal nerves work and to help specify the site of compression. Doctors commonly use a test called a nerve conduction velocity (NCV) test. During the study, a nerve is stimulated in one place and the amount of time it takes for the message or impulse to travel to a second place is measured.
Somatosensory evoked potentials (SSEPs) or motor evoked potentials (MEPs) are used to test how the spinal cord transmits nerve signals about sensory or movement information. Your doctor will place sticky patch-like electrodes on your skin that covers a spinal nerve. The NCV test may feel uncomfortable while it is performed.
Electromyography (EMG) test is often done at the same time as the NCV test. An EMG measures the impulses in the muscles to identify damage or decay. Muscles need impulses to perform movements. Your doctor will place fine needles through your skin and into the muscles that the spinal nerve controls.
Treatment of Cervical Myelopathy
Your spine specialist may recommend spine surgery. The goals of spine surgery to treat myelopathy are: (1) remove pressure from the spinal cord, (2) prevent symptoms from becoming worse, and (3) improve your condition.
Nonsurgical Treatment
In milder cases, initial treatment for CSM may be nonsurgical. The goal of nonsurgical treatment is to decrease pain and improve the patient’s ability to perform daily activities. Nonsurgical treatment options include:
Soft cervical collar – This is a padded ring that wraps around the neck and is held in place with velcro. Your doctor may advise you to wear a soft cervical collar to allow the muscles of the neck to rest and limit neck motion. A soft collar should only be worn for a short period of time since long-term wear may decrease the strength of the muscles in your neck.
Physical therapy management of Cervical Myelopathy
Patients can be treated conservatively. Kadaňka et al. found no difference in long term outcomes (2 years after the intervention) between a patient who received conservative or surgical treatment. Even after 10 years, there were no differences found between the surgery and conservative group.F ouyas et al also confirmed these findings. The only prognostic factor in which surgery can be generally recommended is with a circumferential spinal cord compression seen on an axial MRI.
The goals of physiotherapy treatment are
pain relief
to improve function
to prevent neurological deterioration
to reverse or improve neurological deficits
Cervical myelopathy can be treated symptomatically. Possible therapies include:
Ice, heat, and other modalities – Your doctor may recommend careful use of ice, heat, massage, and other local therapies to help relieve symptoms. Applying a cold pack to the painful part of the back contracts inflamed muscle and relieves pain. This treatment helps a great deal when the disk has recently ruptured and swelling is at its greatest. A heating pad or warm pack helps with residual pain.
Cervical traction and manipulation of the thoracic spine – useful for the reduction of pain scores and level of disability in patients with mild cervical myelopathy. Other signs and symptoms, such as weakness, headache, dizziness, and hypoesthesia, can also be positively affected. Cervical traction can be combined with other treatments like electrotherapy and exercises. Joghataei et al. reported a significant increase in grip strength after 10 weeks of this combined treatment
Manual therapy techniques – used to reduce the neck pain with natural apophyseal glides and sustained natural apophyseal glides for cervical extension and rotation. Manipulation and mobilizations can be effective when they are combined with exercise therapy. When you use them without exercises, there is only poor evidence that it could be effective
Exercises – the effects of exercise therapy specifically on cervical myelopathy have not been studied, but there is evidence for exercises for mechanical neck pain. For example: stretching, strengthening exercises, active range of motion exercises, home exercise programmes.
Cervical stabilization exercises – when there is anteroposterior instability of the vertebral bodies of a degenerative nature, vertebral segment stabilization of the cervical spine can be performed with a pressure biofeedback unit (PBU),
Dynamic upper and lower limb exercises – (flexion and extension) with the use of the PBU on the neck.
Proprioceptive neuromuscular facilitation – for the upper and lower limbs.
Improve posture
Motor training programmes– may improve arm and hand functioning at a function and/or activity level in cervical spinal cord injured patients.
Mobility and proprioception exercises
Aerobic exercises
Balance training – e.g. standing on one leg with eyes open and evolving to eyes closed; standing on a stable platform and evolving to an unstable platform with a rocker board
Core stability exercises –In surgical cases, the physiotherapist still has an important role, both before and after the surgery. In the pre-operative phase, the physiotherapist needs to become thoroughly familiar with the patient’s history and about their activities of daily living that they are aiming to return to. The physiotherapist will inform the patient about the treatment program and the expectations after the surgery. There are different tests to develop a thorough picture of the patient’s baseline pre-operative status such as walking tolerance, Neck Pain and Disability Scale, the Neck Disability Index and lung function. Nomura et. al found that the maximum voluntary ventilation should significantly increase after surgery
Continued Physical Activity – Though pain or weakness seem like good reasons to rest the neck, excessive bed-rest worsens the symptoms of a slipped disc in neck. Moving around too little allows muscles to grow weaker and prevents the body from healing. Periods of rest interspersed with periods of normal activity throughout the day keep the back muscles in shape.
Physical Therapy – Physical therapists show slipped disc sufferers ways to move that do not cause pain. Occupational therapists teach skills that allow patients to return to a productive life.
Nutrition – In order to restore the disc we also are going to need to include different substances in our diet. There are a lot of supplements on the market, of course. If you wish to try them, that’s fine. I personally don’t like them. I have tried one with glucosamine and chondroitin, but I didn’t feel any different. So, if you have the opportunity to take these with the food or from more natural sources, it will be great. You can find these substances in seafood and animal cartilages and by digesting them we ensure the building blocks for the connecting tissue for our joints and spine. Also, we will need more
Omega 3 fatty acids– which can be supplied from cold pressed oils, fatty fish, flax seeds, chia and many more. Vitamins from the B group are very beneficial for people with herniated discs and all kinds of issues with the peripheral nervous system. Vitamins B1, B6 and B12 nourish the nerves and help them recover from the disk accident. Usually, doctors prescribe them as a part of the treatment, but it is worth mentioning anyway.
A good massage – A massage is one of the natural methods of relieving pain. Individuals who get a massage weekly for several months stand a better chance of alleviating neck pain. A good massage provides a person with many health benefits that lessen neck pain. A massage triggers the release of endorphins. Endorphins aid in decreasing anxiety and relieving pain. They offer a relaxation effect by softening muscles that are injured preventing cramping.
Undertaking yoga– Yoga is an applicable strategy for keeping the level of back pain at minimal levels. Taking yoga sessions often is very an effective method of dealing with neck pain. With yoga, there is a high likelihood of proper body functions. The use of pain prescriptions is also diminished. Patients suffering from neck pain related issues do not have to rely on these prescriptions to manage pain. Incorporating laughter in yoga is a good way of exercising. Yoga incorporates simple yet appropriate exercises that enhance the stretching of muscles. Laughter with yoga stimulates relieving of pain. It facilitates increased uptake of oxygen, little anxiety, and production of endorphins. All these variables play an essential role in diminishing neck pain.
Adjusting sleeping position – A simple sleeping mistake can immensely contribute to neck pain. A poor sleeping position can cause stress and tension on the muscles contributing to neck pain. Altering one’s sleeping position and adopting a style that does not exert a lot of stress on the back is a recommended tactic. Nurturing sleeping habits such as assuming a reclining position, using wedge-shaped cushions and getting adjustable beds from reputable medical institutions are easy techniques to endorse. If a reclining position does not suit an individual, the other two techniques can be embraced.
Heat therapy – Several considerations should be observed when using heat therapy. The right temperature ought to be set so as to ensure a patient does not face risks associated with too much exposure to heat. The key objective should be to ensure enough access to heat to the muscles to yield benefits for the patient. The adoption of heat therapy for easing neck pain is determined by the magnitude of pain a person is experiencing. In cases where relatively low back pain is encountered, short heat therapy sessions are recommended. On the other hand, if an individual is experiencing prolonged back pain, long heat therapy sessions are the most applicable.
Taking hot baths – This is a form of heat therapy that aims at relieving neck pain. It guarantees permeation of heat into the muscles leading to reduced pain. Many individuals opt for this method since they believe it achieves competent results. Hot baths initiate a fast process of blood supply to stiff neck muscles. When this happens, the muscles relax and stretch leading to decreased pain. To avoid interference with one’s sleeping patterns, a hot bath should be taken several hours before retiring to bed.
Aquatic therapy – This natural technique involves physical therapy in a pool. Individuals get the best out of this therapy by relying on the resistance of water. Consistency in undertaking this therapy is what ascertains getting back pain relief. Integrating aquatic therapy in an individual’s life for the better part of the week enhances the reduction of back pain quickly.
Enlighten others – Individuals have the power to devise their own natural strategies that aid them in coping with back pain. The strategies can also be a good remedy for others going through similar circumstances. An individual can use social media platforms to equip others with important tips on how to keep back pain at bay. Further, becoming a member of associations that address back pain issues enables better communication of the knowledge gained from personal experience.
Medications of Cervical Myelopathy
In some cases, medications can help improve your symptoms.
Analgesics – Prescription-strength drugs that relieve pain but not inflammation.
Antidepressants: A Drugs that block pain messages from your brain and boost the effects of endorphins (your body’s natural painkillers).
Corticosteroid injections – Your doctor will inject a steroid such as prednisone into your back or neck. Steroids make inflammation go down. However, because of side effects, they are used sparingly.
Anesthetics – Used with precision, an injection of a “nerve block” can stop the ain for a time.
Muscle Relaxants – These medications provide relief from spinal muscle spasms.
Skeletal muscle relaxers– may also be used. Their short term use has been shown to be effective in the relief of acute back pain. However, the evidence of this effect has been disputed, and these medications do have negative side-effects.
Antibiotic –to the management of bowel & bladders control and protect further infection. Infection causes should be treated with appropriate antibiotic therapy
Topical Medications – These prescription-strength creams, gels, ointments, patches, and sprays help relieve pain and inflammation through the skin.
Glucosamine & diacerine – can be used to tightening the loose tension and regenerate cartilage or inhabit the further degeneration of cartilage.
Corticosteroid – to healing the nerve inflammation and clotted blood in the joints.
Dietary supplement-to remove the general weakness & improved the health.
Amitriptyline – If pain persists for more than a month, and has not responded to the above painkillers, your GP may prescribe a medicine called amitriptyline. Amitriptyline was originally designed to treat depression, but doctors have found that a small dose is also useful in treating nerve pain. You may experience some side effects when taking amitriptyline.
Lesion debulking – is required for space-occupying lesions – eg, tumors, abscess.
If surgery cannot be performed – radiotherapy may relieve cord compression caused by malignant disease.
Radiation therapy and Chemotherapy – may have a role in treatment if the cauda equina syndrome is caused by a tumor.
Support or brace – A pelvic belt can be used to stabilize a joint that is too loose until the inflammation and pain subside.
Joint injections– Numbing injections into the sacroiliac joint are used diagnostically to help identify the cause of them but are also useful in providing immediate pain relief. Typically, an anesthetic is injected along with an anti-inflammatory medication.
Cervical epidural block – In this procedure, steroid and anesthetic medicine is injected into space next to the covering of the spinal cord (“epidural” space). This procedure is typically used for neck and/or arm pain that may be due to a cervical disk herniation, also known as radiculopathy or a “pinched nerve.”
Cervical facet joint block – In this procedure, steroid and anesthetic medicine is injected into the capsule of the facet joint. The facet joints are situated at the back of the neck and stability and movement. Arthritis may be formed and will play a part to neck pain.
Medial branch block and radiofrequency ablation – This procedure is usually done for some chronic neck pain It can be used for both diagnosis and treatment of a potentially painful joint.
Although people sometimes turn to chiropractic manipulation for neck and back pain, manipulation should never be used for spinal cord compression.
Other Treatment Options
Other treatment options – may be useful in certain patients, depending on the underlying cause of the CES
Patients with spinal neoplasms should be evaluated for chemotherapy and radiation therapy.
Weakness – Physiotherapy may be helpful if there is no inflammatory component such as that found in arachnoiditis where exercise might exacerbate the condition and cause flare-ups.
Sensory Loss – Little conventional treatment exists for sensory loss in cauda Equina syndrome, although in conditions such as Multiple Sclerosis use of vitamin B complex is considered to have potential beneficial effects.
Sore Feet – Loss of muscle tone and control over the movement of the foot may lead to foot pain. If foot drop is a notable issue, a brace to hold it in position may help. It is important; however, to attempt to maintain as much muscle tone as possible as well as the range of movement (ROM). Exercises might help.
Sexual Dysfunction –Sexual dysfunction is very hard for people to talk about at times. It might be best to pursue advice from specialists. If no physical treatment is feasible for improving function, the person and their sexual partner might pursue counseling which might help to lessen the impact of this disability on not only the person affected but their partner.
Depression– Depression is an understandable reaction to a form of debilitating illness. Antidepressant medication should be reserved for severe depression. Counseling and support are the preferred methods of managing depression. Sharing experiences may help people with Cauda equina syndrome to come to terms with the disabilities associated with Cauda Equina syndrome.
Poor Circulation – Poor circulation is a common issue in Cauda Equina syndrome. The person’s feet may be cold and turn white, then red when re-warmed (also known as, ‘Raynaud’s syndrome,) as well as chilblains. Some medications exist that can be taken, yet it is most likely best to use general measures such as avoiding getting cold feet and foot massage with warm oil to help improve the person’s circulation. Avoid extremely hot baths after the feet have been cold because it will most likely cause chilblains.
Postoperative care – includes addressing lifestyle issues (eg, obesity), and also physiotherapy and occupational therapy, depending on residual lower limb dysfunction.
Prolotherapy – the practice of injecting solutions into joints (or other areas) to cause inflammation and thereby stimulate the body’s healing response – has not been found to be effective by itself, although it may be helpful when added to another therapy.
Herbal medicines – as a whole, are poorly supported by evidence. The herbal treatments Devil’s claw and white willow may reduce the number of individuals reporting high levels of pain; however, for those taking pain relievers, this difference is not significant. Capsicum, in the form of either a gel or a plaster cast, has been found to reduce pain and increase function.
Behavioral therapy – may be useful for chronic pain. There are several types available, including operant conditioning, which uses reinforcement to reduce undesirable behaviors and increase desirable behaviors;
Cognitive behavioral therapy– which helps people identify and correct negative thinking and behavior; and respondent conditioning, which can modify an individual’s physiological response to pain. Medical providers may develop an integrated program of behavioral therapies. The evidence is inconclusive as to whether mindfulness-based stress reduction reduces chronic back pain intensity or associated disability, although it suggests that it may be useful in improving the acceptance of existing pain.
Tentative evidence supports neuroreflexotherapy (NRT) – in which small pieces of metal are placed just under the skin of the ear and back, for non-specific low back pain
Surgery of Cervical Myelopathy
If nonsurgical treatment does not relieve your symptoms, your doctor will talk with you about whether you would benefit from surgery. The majority of patients with symptoms and tests consistent with CSM are recommended to have surgery.There are several procedures that can be performed to help relieve pressure on the spinal cord. The procedure your doctor recommends will depend on many factors, including what symptoms you are experiencing and the levels of the spinal cord that are involved.
Vaginal discharge is a mixture of liquid, cells, and bacteria that lubricates and protects the vagina. This mixture is constantly produced by the cells of the vagina and cervix and it exits the body through the vaginal opening. The composition, amount, and quality of discharge vary between individuals as well as through the various stages of sexual and reproductive development. Normal vaginal discharge may have a thinner, watery consistency or a thick, sticky consistency, and may be clear or white in color. Normal vaginal discharge may be large in volume but typically does not have a strong odor, nor is it typically associated with itching or pain. While most discharge represents normal functioning of the body, some changes in discharge can reflect infection or other pathological processes
What infections cause vaginal discharge to change?
There are a number of infections that cause vaginal discharge to change or become unpleasant. Many of these infections can be caused by having sex with someone who has the infection. This graph describes a number of common vaginal infections
Yeast Infection
Is caused by having sex with an infected person? No
What does discharge look like? Thick, white, like cottage cheese
How is the infection treated? Antifungal vaginal creams or pills
Trichomoniasis (“Trick”)
Is caused by having sex with an infected person? Yes
What does discharge look like? Green, yellow, or gray in color; frothy
How is the infection treated? Antibiotics ordered by your doctor
Bacterial vaginosis (Gardnerella or BV)
Is caused by having sex with an infected person? Probably not
What does discharge look like? White discharge that smells fishy
How is the infection treated? Antibiotic pills or vaginal cream ordered by your doctor
Gonorrhea (Clap)
Is caused by having sex with an infected person? Yes
What does discharge look like? Cloudy or yellow, but often no symptoms. If not treated, the infection may spread, causing pelvic inflammatory disease with pelvic pain.
How is the infection treated? Antibiotic pills or shots ordered by your doctor
Chlamydia (Kla-mid-ee-ah)
Is caused by having sex with an infected person? Yes
What does discharge look like? Often no symptoms. If not treated, the infection may spread, causing pelvic inflammatory disease with pelvic pain.
How is the infection treated? Antibiotic pills ordered by your doctor
Causes of vaginal discharge
Non-infective
Physiological
Cervical ectopy
Foreign bodies, such as retained tampon
Vulval dermatitis
Non-sexually transmitted infection
Bacterial vaginosis
Candida infections
Sexually transmitted infection
Chlamydia trachomatis
Neisseria gonorrhoeae
Trichomonas vaginalis
Causes abnormal discharge
According to the causes of infection
Non-infective
Physiological
Cervical ectopy
Foreign bodies, such as retained tampon
Vulval dermatitis
Non-sexually transmitted infection
Bacterial vaginosis
Candida infections
Sexually transmitted infection
Chlamydia trachomatis
Neisseria gonorrhoeae
Trichomonas vaginalis
According to the overall condition
Any change in the vagina’s balance of normal bacteria can affect the smell, color, or discharge texture. These are a few of the things that can upset that balance:
Antibiotic or steroid use
Bacterial vaginosis, a bacterial infection more common in pregnant women or women who have multiple sexual partners
Birth control pills
Cervical cancer
Chlamydia or gonorrhea (STDs), sexually transmitted infections
Diabetes
Douches, scented soaps or lotions, bubble bath
Pelvic infection after surgery
Pelvic inflammatory disease (PID)
Trichomoniasis, a parasitic infection typically contracted and caused by having unprotected sex
Vaginal atrophy, the thinning and drying out of the vaginal walls during menopause
Vaginitis, irritation in or around the vagina
Yeast infections
See the chart below to learn more about what a particular type of discharge might mean.
Types of Abnormal Discharge and Their Possible Causes
Type of Discharge
What It Might Mean
Other Symptoms
Bloody or brown
Irregular menstrual cycles, or less often, cervical or endometrial cancer
Abnormal vaginal bleeding, pelvic pain
Cloudy or yellow
Gonorrhea
Bleeding between periods, urinary incontinence, pelvic pain
Frothy, yellow or greenish with a bad smell
Trichomoniasis
Pain and itching while urinating
Pink
Shedding of the uterine lining after childbirth (lochia)
Thick, white, cheesy
Yeast infection
Swelling and pain around the vulva, itching, painful sexual intercourse
White, gray, or yellow with fishy odor
Bacterial vaginosis
Itching or burning, redness and swelling of the vagina or vulva
Types of abnormal discharge and their possible causes
Any change in the balance of normal bacteria in the vagina can affect the smell, colour, or texture of the discharge. These are a few of the things that can upset the balance:
Type of Discharge
What It Might Mean
Other Symptoms
Bloody or brown
Irregular menstrual cycles, or less often, cervical or endometrial cancer
Irregular vaginal bleeding, pelvic pain
Cloudy or yellow
Gonorrhoea
Bleeding between periods, painful urination
Frothy, yellow or greenish with a bad smell
Trichomoniasis
Pain and itching while urinating
Pink
Shedding of the uterine lining after childbirth (lochia)
Thick, white, cheesy
Yeast infection
Swelling and pain around the vulva, itching, painful sexual intercourse
White, grey, or yellow with a fishy odor
Bacterial vaginosis
Itching or burning, redness and swelling of the vagina or vulva
Warning signs
In girls, a fever or a yellow or green discharge with a fishy odor (because they may have a sexually transmitted disease resulting from sexual abuse)
Severe abdominal or pelvic pain or pain, particularly if it lasts more than 2 hours
Drainage of pus, a fever, or other signs of infection in the reproductive organs
Stool in the vaginal discharge
A bloody discharge after menopause
Looks foamy or like cottage cheese
Is green, yellow, or gray in color
Causes swelling
Causes itching
In women with an abnormal discharge, certain characteristics are cause for concern
Diagnosis of Vaginal Discharge
History Ask the patient about itching, odor, the color of discharge, painful intercourse, or spotting after intercourse.
Yeast causes intense itching with a cheesy, dry discharge.
Gardnerella causes a foul-smelling, thin white discharge.
Trichomonas gives irritation and frothy white discharge.
Foreign body (lost tampon) causes a foul-smelling black discharge.
Cervicitis causes a nondescript discharge with deep dyspareunia
Chlamydia may cause a purulent vaginal discharge, post-coital spotting, and deep dyspareunia.
Gonorrhea may cause a purulent vaginal discharge and deep dyspareunia.
Cervical ectropion causes a mucous, asymptomatic discharge.
Physical Exam
Inspect carefully for the presence of lesions, foreign bodies and odor. Palpate to determine cervical tenderness.
Yeast has a thick white cottage-cheese discharge and red vulva.
Gardnerella has a foul-smelling, thin discharge.
Trichomonas has a profuse, bubbly, frothy white discharge.
Foreign body is obvious and has a terrible odor.
Cervicitis has a mucopurulent cervical discharge and the cervix is tender to touch.
Chlamydia causes a friable cervix but often has no other findings.
Gonorrhea causes a mucopurulent cervical discharge and the cervix may be tender to touch.
Cervical ectropion looks like a non-tender, fiery-red, friable button of tissue surrounding the cervical os.
Infected/Rejected IUD demonstrates a mucopurulent cervical discharge in the presence of an IUD. The uterus is mildly tender.
Chancroid appears as an ulcer with irregular margins, dirty-gray necrotic base and tenderness.
Laboratory
Obtain cultures for chlamydia, gonorrhea, and Strept. You may test the vaginal discharge in any of 4 different ways:
Test the pH. If >5.0, this suggests Gardnerella.
Mix one drop of KOH with some of the discharge on a microscope slide. The release of a bad-smelling odor confirms Gardnerella.
Examine the KOH preparation under the microscope (“Wet Mount”). Multiple strands of thread-like hyphae confirm the presence of yeast.
Mix one drop of saline with some discharge (“Wet Mount”). Under the microscope, large (bigger than WBCs), moving micro-organisms with four flagella are trichomonads. Vaginal epithelial cells studded with coccoid bacteria are “clue cells” signifying Gardnerella.
Differential diagnosis of vulvovaginal symptoms. The parameters listed here can be useful for the rapid diagnosis of vulvovaginal symptoms. It is important to differentiate aerobic vaginitis from atrophic vaginitis. The latter often presents with identical symptoms in women with estrogen deficiency (e.g., postpartum, during the lactation period, in postmenopausal women) and can usually be treated effectively with local application of estriol.
parabasal cells, elevated leukocyte count, no lactobacilli
KOH (whiff) test
positive
negative
often positive
negative
or
Combination therapies for PID (modified and based on 16, 17, 40).
Combinations of active ingredients
Dose
Length of treatment
Azithromycin – can also be used as an alternative to doxycycline (pregnancy!) to treat severe PID.* On the length of treatment: data on the length of treatment required when administering antibiotic therapies is poor and inconsistent. With the exception of single doses and the use of doxycycline to treat chlamydia (at least 14 days), the length of treatment should depend on the clinical condition (rule of thumb: intravenous antibiotic treatment should be discontinued at the earliest 24 hours after significant clinical improvement; length of treatment should be at least 7 days, usually not more than 14 days).
Mild to moderate form
1. Ceftriaxone plusdoxycycline
250 mg i. m.2 × 100 mg/day orally
single dose14 days
Alternatively
2. Amoxicillin/clavulanic acidplusdoxycycline
2–3 × 875 mg/125 mg per day orally2 × 100 mg/day orally
*14 days
Alternatively
3. Ofloxacinplus metronidazole
2 × 400 mg per day orally2 × 500 mg per day orally
*14 days
The first two regimens can be additionally combined with metronidazole to ensure effectiveness against anaerobes (combination 1) or increase effectiveness even further (combination 2). These regimens also treat potentially present BV. The use of azithromycin (off-label) is a possible alternative to doxycycline and ofloxacin, both of which are contraindicated in pregnancy; suggested azithromycin dosage: 1 × 1 g per week [rx].
Severe form
1.Ceftriaxone plusmetronidazoleplus doxycycline
1 × 2,0 g/day2 × 500 mg/day (i. v. or orally)2 × 100 mg/day, orally where possible
**14 days
Alternatively
2. Piperacillin/tazobactamplusdoxycycline
4.0 g/0.5 g every 8 hours i. v.2 × 100 mg/day, orally where possible
*At least 14 days
Alternatively 3. Meropenem
500 mg/every 8 hours i. v.
*
Treatment of Vaginal Discharge
Non Pharmacological Treatment
Ways to Ease Watery Discharge Discomfort
Methods of helping to calm the discharge are common sense, but many women will fail to do them. If the discharge is causing discomfort, consult your doctor. Otherwise, you can try the following to help ease:
Use Baby Wipes – Make use of your purse. Baby wipes are a great way to help clean the vagina and keep the area bacteria-free. These wipes shouldn’t be inserted in the vagina. Simply clean the outside of the vagina to alleviate any smells or wetness that’s causing discomfort. If possible, choose an unscented baby wipe. The fewer chemicals, the better.
Use Pads – I don’t recommend keeping a tampon in to solve watery discharge. But you can use pads to ensure that your undies stay dry. Always offers very thin pads that are comfortable and work to absorb any liquid that may be expelled. These pads don’t come with wings, and they absorb within seconds. This is a great way to stop the wet feeling that leaves you feeling self-conscious and uncomfortable throughout the day.
Change Your Underwear Often – If your underwear is getting wet fast, you’ll want to keep a fresh pair in your purse. This allows you to change your underwear as it gets wet to avoid any discomfort. You’ll also want to change your underwear to ensure that no bacteria buildup occurs. It’s not uncommon for the moist and wet environment to cause bacteria growth in the panties. And this bacterium can lead to infection, which is not fun.
Increase the “Air” – If you can, sleep naked at night without pants or underwear. Place a towel down on the bed to ensure that the bed doesn’t get wet. This airing out allows you to decrease the risk of infection and reduces irritation. An issue of bacteria imbalance will benefit from airing out. The body will sort out the bacteria imbalance on its own in most cases.
Boost Your Immune System With Natural Herbs – Watery discharge isn’t an indicator of health issues, but there’s a small risk that the discharge will transition into an infection. This happens when other symptoms are present, and the discharge will often change colors instead of staying clear.
A few natural herbs and products that can help you boost your immune system to fight off potential infection are:
Vitamin C
D-Mannose
Saraca Ashoka
Cimicifuga Racemosa
You can also try to cleanse the urinary tract with cranberry juice to stop an infection before it progresses. Again, this may be overkill, but it’s never a bad idea to help boost your immune system and clean out the reproductive system.
Watery discharge is common, and there often isn’t a cause for concern. Since the clear discharge is part of the normal menstrual cycle, it often occurs monthly without concern. If you notice a gush of discharge that can soak a tampon, consult with your doctor.
Treatment of Vaginal Discharge
In addition to specific treatment of any organism identified by culture or another test.
summarises some of the recommended treatments for individual infections.
Management of vaginal infections
Bacterial vaginosis
Metronidazole 2 g as a single oral dose, metronidazole 400-500 mg twice daily for five to seven days, intravaginal clindamycin cream (2%) once daily for seven days, or intravaginal metronidazole gel (0.75%) once daily for five days4
The infection often recurs and acidic vaginal jelly (such as Relact from Kora Healthcare) may reduce relapse rates27
Partner notification not needed
Vulvovaginal candidiasis
Vaginal imidazole preparations (such as clotrimazole, econazole, miconazole—various preparations are available including single dose ones), or fluconazole 150 mg orally8
The role of alternative treatments like tea tree oil and yoghurt containing Lactobacillus acidophilus have not been evaluated9
Oral versus vaginal treatment depends on preference
Treatment for candidiasis is available over the counter in the UK
Partner notification not needed
Chlamydia trachomatis
Doxycycline 100 mg twice daily for seven days (contraindicated in pregnancy), azithromycin 1 g orally in a single dose (WHO recommends azithromycin in pregnancy but the British National Formulary advises against its use unless no alternatives are available)13
Cefixime 400 mg as a single oral dose or ceftriaxone 250 mg intramuscularly as a single dose16
Referral to a genitourinary medical unit is encouraged because of the existence of resistant strains of the organism16
A test of cure is not routinely indicated if an appropriately sensitive antibiotic has been given, symptoms have resolved, and there is no risk of reinfection16
Partner notification required
Trichomonas vaginalis
Metronidazole 2 g orally in a single dose or metronidazole 400-500 mg twice daily for five to seven days17
Partner notification required
Readers should refer to BASHH guidelines, the British National Formulary, and local policies for full treatment options, including treatment in pregnancy
Any patient complaining of an itchy vaginal discharge should probably be treated with an antifungal agent (Monistat, Lotrimin, etc.) because of the high likelihood that yeast is present, and
Any patient complaining of a bad-smelling vaginal discharge should probably be treated with Flagyl (or another reasonable substitute) because of the high likelihood that Gardnerella is present
Ectropion, Erosion or Eversion
This harmless condition is frequently mistaken for cervicitis.
Ectropion, erosion or eversion (all synonyms) occurs when the normal squamocolumnar junction is extended outward from its; normal position at the opening of the cervix.
Grossly, the cervix has a red, friable ring of tissue around the os. Careful inspection with magnification (6-10x) will reveal that this red tissue is the normal tissue of the cervical canal, which has grown out onto the surface of the cervix.
Cervical ectropion is very common, particularly in younger women and those taking BCPs. It usually causes no symptoms and need not be treated. If it is symptomatic, producing a more or less constant, annoying, mucous discharge, cervical cauterization will usually eliminate the problem.
When faced with a fiery red button of tissue surrounding the cervical os, chlamydia culture (in high-risk populations) and Pap smear should be performed. If these are negative and the patient has no symptoms, this cervical ectropion should be ignored.
Cervicitis
Inflammation or irritation of the cervix is rarely the cause of significant morbidity. It is mainly a nuisance to the patient and a possible symptom of the underlying disease (gonorrhea, chlamydia).
Some patients with cervicitis note a purulent vaginal discharge, deep dyspareunia, and spotting after intercourse, while others may be symptom-free. The cervix is red, slightly tender, bleeds easily, and a mucopurulent cervical discharge from the os is usually seen.
A Pap smear rules out malignancy. Chlamydia culture and gonorrhea culture (for gram negative diplococci) are routinely performed.
No treatment is necessary if the patient is asymptomatic, the Pap smear is normal, and cultures are negative. Antibiotics specific to the organism are temporarily effective and may be curative. Cervical cautery may be needed to achieve a permanent cure.
Chlamydia
This sexually-transmitted disease is caused by “Chlamydia trachomatis“. It very commonly locates in the cervical canal although it can spread to the fallopian tubes where it can cause PID.
Most women harboring chlamydia will have no symptoms, but others complain of purulent vaginal discharge, deep dyspareunia, and pelvic pain. There may be no significant pelvic findings, but a friable cervix, mucopurulent cervical discharge, pain on motion of the cervix, and tenderness in the adnexa are suggestive.
The diagnosis is often made on the basis of clinical suspicion but can be confirmed with chlamydia culture. Such cultures are frequently performed routinely in high-risk populations.
Treatment is:
Recommended Regimens
Azithromycin1 g orally in a single dose OR
Doxycycline100 mg orally twice a day for 7 days.
Alternative Regimens
Erythromycin base500 mg orally four times a day for 7 days, OR
Erythromycin ethylsuccinate800 mg orally four times a day for 7 days, OR
Ofloxacin300 mg orally twice a day for 7 days, OR
Levofloxacin500 mg orally for 7 days.
Read the CDC Treatment Guidelines for Chlamydia
Foreign Body
Lost and forgotten tampons are the most common foreign body found in the vagina, although other objects are occasionally found. Women with this problem complain of a bad-smelling vaginal discharge which is brown or black in color. The foreign body can be felt on digital exam or visualized with a speculum.
As soon as you suspect or identify a lost tampon or another object in the vagina, immediately prepare a plastic bag to receive the object. As soon as it is retrieved, place it in the bag and seal the bag since the anaerobic odor from the object will be extremely penetrating and long-lasting.
Have the patient return in a few days for a follow-up examination. Normally, no other treatment is necessary, but patients who also complain of fever or demonstrate systemic signs/symptoms of illness should be evaluated for possible toxic shock syndrome, an extremely rare, but serious, complication of a retained tampon.
Gardnerella (Hemophilus, Bacterial Vaginosis)
The patient with this problem complains of a bad-smelling discharge which gets worse after sex. Cultures will show the presence of “Gardnerella Vaginalis,” the bacteria associated with this condition. While this problem is commonly called “Gardnerella,” it is probably the associated anaerobic bacteria which actually cause the bad odor and discharge.
The diagnosis is confirmed by the release of a bad odor when the discharge is mixed with KOH (“whiff test”), a vaginal pH greater than 5.0, or the presence of “clue cells” (vaginal epithelial cells studded with bacteria) in the vaginal secretions.
The treatment is
Metronidazole500 mg orally twice a day for 7 days,
Recommended Regimens (CDC 2002)
ORMetronidazole gel0.75%, one full applicator (5 g) intravaginally, once a day for 5 days,
OR
Clindamycin cream 2%, one full applicator (5 g) intravaginally at bedtime for 7 days.
Alternative Regimens (CDC 2002)
Metronidazole2 g orally in a single dose,
OR
Clindamycin300 mg orally twice a day for 7 days
OR
Clindamycin Ovules100 g intravaginally once at bedtime for 3 days.
Read the CDC Treatment Guidelines for Bacterial Vaginosis
Many (perhaps most) women harboring the gonococcus will have no symptoms, but others complain of purulent vaginal discharge, pelvic pain, and deep dyspareunia. There may be no significant pelvic findings, but mucopurulent cervical discharge, pain on motion of the cervix, and tenderness in the adnexa are all classical.
Gonorrhea
This sexually-transmitted disease is caused by a gram-negative diplococcus. The organism grows easily in the cervical canal, where it can spread to the fallopian tubes, causing PID. It may also infect the urethra, rectum or pharynx.
The diagnosis is often made on the basis of clinical suspicion but can be confirmed with chocolate agar culture or gram stain.
Treatment is: Recommended Regimens (CDC 2002)
Cefixime400 mg orally in a single dose,
OR
Ceftriaxone125 mg IM in a single dose,
OR
Ciprofloxacin500 mg orally in a single dose,
OR
Ofloxacin400 mg orally in a single dose,
OR
Levofloxacin250 mg orally in a single dose,
PLUS, IF CHLAMYDIAL INFECTION IS NOT RULED OUT
Azithromycin1 g orally in a single dose
OR
Doxycycline100 mg orally twice a day for 7 days.
Alternative Regimens (CDC 2002)
Spectinomycin2 g in a single, IM dose. Spectinomycin is expensive and must be injected; however, it has been effective in published clinical trials, curing 98.2% of uncomplicated urogenital and anorectal gonococcal infections. Spectinomycin is useful for the treatment of patients who cannot tolerate cephalosporins and quinolones.
Single-dose cephalosporinregimens (other than ceftriaxone 125 mg IM and cefixime 400 mg orally) that are safe and highly effective against uncomplicated urogenital and anorectal gonococcal infections include ceftizoxime (500 mg, administered IM), cefoxitin (2 g, administered IM with probenecid 1 g orally), and cefotaxime (500 mg, administered IM). None of the injectable cephalosporins offer any advantage over ceftriaxone.
Single-dose quinolone regimens include gatifloxacin 400 mg orally, norfloxacin 800 mg orally, and lomefloxacin 400 mg orally. These regimens appear to be safe and effective for the treatment of uncomplicated gonorrhea, but data regarding their use are limited. None of the regimens appear to offer any advantage over ciprofloxacin at a dose of 500 mg, ofloxacin at 400 mg, or levofloxacin at 250 mg.
Sexual partners also need to be treated.
Infected IUD
Sooner or later, as many as 5% of all intrauterine devices will become infected. Patients with this problem usually notice mild lower abdominal pain, sometimes have a vaginal discharge and fever, and may notice deep dyspareunia. The uterus is tender to touch and one or both adnexa may also be tender.
Treatment consists of removal of the IUD and broad-spectrum antibiotics. If the symptoms are mild and the fever low-grade, oral antibiotics (amoxicillin, cephalosporins, tetracycline, etc.) are very suitable. If the patient’s fever is high, the symptoms significant or she appears quite ill, IV antibiotics are a better choice (cefoxitin, or metronidazole plus gentamicin, or clindamycin plus gentamicin).
If an IUD is present and the patient is complaining of any type of pelvic symptom, it is wisest to remove the IUD, give antibiotics, and then worry about other possible causes for the patient’s symptoms.
IUDs can also be rejected without infection. Such patients complain of pelvic pain and possibly bleeding. On pelvic exam, the IUD is seen protruding from the cervix. It should be grasped with an instrument and gently removed. It cannot be saved and should not be pushed back inside.
PID:
Mild Gradual onset of mild bilateral pelvic pain with purulent vaginal discharge is the typical complaint. Fever <100.4 and deep dyspareunia are common.
Moderate pain on motion of the cervix and uterus with purulent or mucopurulent cervical discharge is found on examination. Gram-negative diplococci or positive chlamydia culture may or may not be present. WBC may be minimally elevated or normal.
Treatment consists of:
Regimen A (CDC 2002)
Ofloxacin400 mg orally twice a day for 14 days
OR
Levofloxacin500 mg orally once daily for 14 days
WITH or WITHOUT
Metronidazole500 mg orally twice a day for 14 days
Regimen B (CDC 2002)
Ceftriaxone250 mg IM in a single dose
OR
Cefoxitin2 g IM in a single dose and Probenecid,1 gorally administered concurrently in a single dose
OR
Other parenteral third-generation cephalosporin(e.g., ceftizoxime or cefotaxime)
PLUS
Doxycycline 100mg orally twice a day for 14 days
WITH or WITHOUT
Metronidazole 500 mg orally twice a day for 14 days.
PID: Moderate to Severe
Severe PID required a hysterectomy to cure.
With moderate to severe PID, there is a gradual onset of moderate to severe bilateral pelvic pain with purulent vaginal discharge, fever >100.4 (38.0), lassitude, and headache. Symptoms more often occur shortly after the onset or completion of menses.
Excruciating pain on movement of the cervix and uterus is characteristic of this condition. Hypoactive bowel sounds, purulent cervical discharge, and abdominal dissension are often present. Pelvic and abdominal tenderness is always bilateral except in the presence of an IUD.
Gram-negative diplococci in cervical discharge or positive chlamydia culture may or may not be present. WBC and ESR are elevated.
Treatment consists of bedrest, IV fluids, IV antibiotics, and NG suction if ileus is present. Since surgery may be required, transfer to a definitive surgical facility should be considered.
Parenteral Regimen A (CDC 2002)
Cefotetan2 g IV every 12 hours
OR
Cefoxitin2 g IV every 6 hours
PLUS
Doxycycline100 mg orally or IV every 12 hours.
Parenteral Regimen B (CDC 2002)
Clindamycin900 mg IV every 8 hours
PLUS
Gentamicin loading dose IV or IM (2mg/kg of body weight) followed by a maintenance dose (1.5mg/kg) every 8 hours. Single daily dosing may be substituted.
Alternative Parenteral Regimens (CDC 2002)
Ofloxacin400 mg IV every 12 hours
OR
Levofloxacin500 mg IV once daily
WITH or WITHOUT
Metronidazole500 mg IV every 8 hours
OR
Ampicillin/Sulbactam3 g IV every 6 hours
PLUS
Doxycycline100 mg orally or IV every 12 hours.
Trichomonas
This microorganism, with its four flagella to propel it, is not a normal inhabitant of the vagina. When present, it causes a profuse, frothy white or greenish vaginal discharge.
When the discharge is suspended in normal saline and examined under the microscope, the typical movement of these large organisms (larger than white blood cells) is obvious. Itching may be present, but this is inconsistent. Trichomonas is transmitted sexually and you may wish to treat the sexual partner, particularly if this is a recurrent trichomonad infection.
Recommended Regimen (CDC 2002)
Metronidazole2 g orally in a single dose.
Alternative Regimen (CDC 2002)
Metronidazole500 mg twice a day for 7 days.
Yeast (Monilia, Thrush)
Vaginal yeast infections are common, monilial overgrowths in the vagina and vulvar areas, characterized by itching, dryness, and a thick, cottage-cheese appearing vaginal discharge. The vulva may be reddened and irritated to the point of tenderness.
Yeast thrives in damp, hot environments and women in such circumstances are predisposed toward these infections. Women who take broad-spectrum antibiotics are also predisposed towards these infections because of loss of the normal vaginal bacterial flora.
Yeast organisms are normally present in most vaginas, but in small numbers. A yeast infection, then, is not merely the presence of yeast, but the concentration of yeast in such large numbers as to cause the typical symptoms of itching, burning, and discharge. Likewise, a “cure” doesn’t mean the eradication of all yeast organisms from the vagina. Even if eradicated, they would soon be back because that is where they normally live. A cure means that the concentration of yeast has been restored to normal and symptoms have resolved.
The diagnosis is often made by history alone and enhanced by the classical appearance of a dry, cheesy vaginal discharge. It can be confirmed by microscopic visualization of clusters of thread-like, branching Monilia organisms when the discharge is mixed with KOH.
Recommended Regimens (CDC 2002)
Intravaginal Agents
Butoconazole2% cream 5 g intravaginally for 3 days,
OR
Butoconazole2% cream 5 g (Butaconazole1-sustained release), single intravaginal application,
OR
Clotrimazole1% cream 5 g intravaginally for 7–14 days,
OR
Clotrimazole100 mg vaginal tablet for 7 days,
OR
Clotrimazole 100 mg vaginal tablet, two tablets for 3 days,
OR
Clotrimazole 500 mg vaginal tablet, one tablet in a single application,
OR
Miconazole2% cream 5 g intravaginally for 7 days,
OR
Miconazole100 mg vaginal suppository, one suppository for 7 days,
OR
Miconazole200 mg vaginal suppository, one suppository for 3 days,
OR
Nystatin 100,000-unit vaginal tablet, one tablet for 14 days,
OR
Tioconazole6.5% ointment 5 g intravaginally in a single application,
OR
Terconazole0.4% cream 5 g intravaginally for 7 days,
OR
Terconazole0.8% cream 5 g intravaginally for 3 days,
OR
Terconazole80 mg vaginal suppository, one suppository for 3 days.
Oral Agent:
Fluconazole150 mg oral tablet, one tablet in single dose.
Reoccurrences are common and can be treated the same as for initial infections. For chronic recurrences, many patients find the use of a single applicator of Monistat 7 at the onset of itching will abort the attack completely. Sexual partners need not be treated unless they are symptomatic.
How to keep your vagina healthy
Maintaining a healthy vagina does not require a lot of effort, but is something you need to do. In order to protect the vagina and prevent the risk of infection, stick to the following guidelines:
Keep it clean and dry
Wear cotton underwear.
Never douche – this removes natural vaginal bacteria.
Always practice safe sex
Eat a healthy diet, especially when taking antibiotics and increase your intake of yogurt with live and active cultures.
Avoid feminine hygiene products in the genital area
Use pads and not tampons.
Keep your blood sugar levels under good control if you have diabetes.
Home Remedies
1. Tea Tree Oil
If you use scented wipes and vaginal deodorants, it’s time to throw them in the trash bin. These products can disrupt the vagina’s pH balance and induce infection and foul odor. To get rid of odors, use natural tea tree oil diluted in water as a vaginal wash.
You Will Need
A few drops of tea tree oil
A cup of water
What You Have To Do
1. Mix three to four drops of tea tree oil in water and use this to rinse the vaginal area.
2. You can also dip a tampon in olive oil, pour two to three drops of tea tree oil on it, and insert the tampon. Leave it in for an hour.
How Often You Should Do This
Wash with the tea tree oil water daily or several times a week. As for the ‘tampon and oil’ treatment, you can repeat it several times a week.
Why This Works
Tea tree oil is both antibacterial and antifungal, and thus will curb the infection while fighting the odor .
Caution
Always do a test patch on your forearm as tea tree oil might not suit everybody.
2. Baking Soda
If you thought baking soda finds its use only in cakes and bread recipes, you are wrong. You will be surprised to see how this tested method helps you to get rid of vaginal odor quickly.
You Will Need
1/2 cup of baking soda
What You Have To Do
1. Add baking soda to your bath and soak your lower body in it for 20-30 minutes.
2. You can also add a teaspoon of baking soda in a glass of warm water and gulp it down.
Why This Works
The vaginal odor intensifies when the pH level of the body goes awry. Baking soda helps bring your pH levels back to normal, thus controlling the excess of bacteria and fungi. This treats the infection and eliminates the crotch odor instantly. You can also use baking soda water as a vaginal wash.
3. Pineapple
This amazing fruit is said to be beneficial for your vaginal health and odor.
You Will Need
Pineapple or pineapple juice
What You Have To Do
Include raw pineapple and pineapple juice in your regular diet.
How Often You Should Do This
You can drink one to two glasses of fresh pineapple juice every day for a few days.
Why This Works
The strong smell of pineapple improves the odor of your vaginal secretions.
4. Hydrogen Peroxide For Bacterial Vaginosis
Hydrogen peroxide is a multipurpose chemical that can be used to treat bacterial vaginosis and remove bad vaginal odor. It is one of the most effective feminine odor remedies.
You Will Need
3% hydrogen peroxide
1 tampon
Water
What You Have To Do
1. Mix equal parts of hydrogen peroxide and water.
2. Dip a tampon in this mixture and insert it into the vagina. Leave it in for not more than 30 minutes.
How Often You Should Do This
You can repeat this every few hours until the foul odor subsides.
Why This Works
The natural disinfecting properties of hydrogen peroxide kill the bad bacteria in the vagina. This leads to an increase in the number of the good bacteria that are naturally present there. Many studies have been conducted, and they all prove the infection-treating capabilities of hydrogen peroxide .
5. Vitamin C With Rose Hips
Rose hips are the seeds of the rose plant, and they contain high levels of vitamin C. Rose hips, by themselves, or in combination with a vitamin C tablet can be used to get rid of vaginal odor.
You Will Need
Vitamin C tablet
Rose hips
1 tampon
What You Have To Do
Insert the tablet with rose hips into the vagina. You can keep it there with the help of a tampon.
How Often You Should Do This
Repeat this every day till the fishy smell from the vaginal discharge goes away.
Why This Works
Vitamin C is an immunity booster and helps remove harmful toxins from the body. The tablet, when used in combination with rose hips, is an effective and safe method to treat bacterial vaginosis, one of the major causes of foul odor in the vagina area . An efficacy study conducted in 2013 also showed that using vitamin C tablets for six days a month for six months can reduce the recurrence of this infection
Who knew betel leaves (paan) could be used to cure the smelly discharge problem? Read on to find out how.
You Will Need
A few betel leaves
Tampon
What You Have To Do
1. Tear the leaves into small pieces and boil them. Simmer for about 10 minutes.
2. Cool the decoction until it reaches lukewarm temperature.
3. Dip the tampon in this liquid and insert it into the vagina.
4. Keep it there for 15 minutes. Remove and discard.
How Often You Should Do This
Repeat this daily for one week. You could also drink this decoction twice a day or use the water as a vaginal wash.
Why This Works
The extract of betel leaves is used in ointments for its antibacterial properties. It also acts as an astringent.
7. Vinegar
Vinegar, especially ACV, is yet another potent remedy that is fail-proof when it comes to fighting vaginal odor.
You Will Need
1 cup of white vinegar or apple cider vinegar
What You Have To Do
1. Mix the vinegar in your bathtub with water and soak in it for 20 minutes.
2. You can also mix two tablespoons of vinegar in 8 oz of water and drink it.
How Often You Should Do This
Soak in vinegar water once daily till the foul smell discharge is treated. Drink vinegar water twice daily.
Why This Works
Vinegar gets rid of the toxins that cause the fishy vaginal odor. It is acidic in nature and is loaded with antibacterial properties that will help kill the odor-causing germs .
Caution
Some people are allergic to vinegar. Step into the bathtub lightly, and if you experience a burning sensation, step out immediately and wash the area
8. Garlic
Many may question the potency of garlic in treating odor, but thanks to its own pungent smell, it works amazingly. Believe us when we say that this is certainly one of the best-known home remedies to kill overpowering vaginal odor.
You Will Need
A garlic clove
A cheesecloth
String
What You Have To Do
1. Peel the fresh garlic clove, and wrap it in a cheesecloth.
2. Attach a small string to it. Insert it into the vagina and leave it there overnight.
3. Remove it in the morning with the help of the string.
How Often You Should Do This
Do it once overnight. The pungent vaginal odor should be gone by the morning. You can repeat if the infection and the bad odor is still there.
Why This Works
Garlic has been used since ancient times to treat infections. Various studies have proved that it has antibacterial activity against a wide range of bacteria .
9. Chlorophyll
Do you remember reading about chlorophyll that plants use to make their own food with the use of sunlight and water? Yes, that very chlorophyll can work wonders in reducing the vaginal smell.
You Will Need
Liquid chlorophyll or chlorophyll tablets
What You Have To Do
1. Drink one tablespoon of chlorophyll diluted with 8 oz of water, and you will never have to visit the doctor to get rid of vaginal odor.
2. You can take one tablet in the night and one in the morning if you cannot find the liquid version in the pharmacy.
How Often You Should Do This
Drink or take the tablet twice a day till the fishy smell from the vagina is gone.
Why This Works
Liquid chlorophyll works as a good deodorant and helps reduce the strong and unpleasant odor . It is easily available with most pharmacists.
10. Yogurt
Yogurt might not be your favorite food, but it can help diminish and reduce vaginal odor considerably. Simply have two cups of unsweetened yogurt a day, preferably with meals, to restore the normal pH of the vagina.
You Will Need
1-2 teaspoons of yogurt
1 tampon
What You Have To Do
1. Dip the tampon in the yogurt and gently insert it into your vagina.
2. Let it be there for an hour or two. Remove and rinse the area.
Alternatively, if you suffer from a very strong vaginal odor, you can also dip cotton pads in the yogurt and gently rub them on the vagina.
How Often You Should Do This
You can repeat the cotton pads method three to four times a day. The tampon method will help you to eliminate the vaginal odor overnight.
Why This Works
A strong vaginal odor is an indication of a yeast infection. The bacteria in yogurt can help fight the infection and reduce the odor as well. It brings the vaginal pH back to normal, and the lactobacillus bacteria present in it will help treat the infection. This is a natural and effective method to remove the fishy smell from your vagina (
11. Herbal Capsules
An alkaline vaginal pH leads to bacterial growth and foul smell. Therefore, it is important to maintain an acidic vaginal pH. One of the best ways to maintain acidic vaginal pH is by consuming homemade herbal capsules for two consecutive weeks.
Here is how to prepare the herbal capsule:
You Will Need
Comfrey root powder – 2 tablespoons
Myrrh gum powder – 2 tablespoons
Slippery elm bark – 2 tablespoons
Goldenseal root powder – 4 tablespoons
Echinacea root powder – 2 tablespoons
Yellow dock root powder – 2 tablespoons
Gelatin capsules – size 00
What You Have To Do
1. Mix all the herbal powders.
2. Fill the size 00 capsules with a teaspoon (~700 mg) of the herbal powder mix.
3. Store in a safe and cool place.
4. Take two capsules thrice a day.
How Often You Should Do This
Take six capsules per day for one or two weeks.
Why This Works
These homemade herbal capsules have antibacterial, antifungal, and antiviral properties, which will help boost your overall health and prevent microbial growth in the vaginal area.
12. Alum
Aluminium potassium sulfate is known as alum. It is widely used to clean water tanks, as a traditional aftershave ointment, and in pickles. Alum is mixed with water to kill bacteria and eliminate body odor or vaginal odor. If the vaginal odor is due to excessive white discharge, alum can be helpful in preventing the odor.
Here is how to use alum to prevent vaginal odor.
You Will Need
Water
Alum
What You Have To Do
1. Mix half a teaspoon of alum with a glass of water and drink it twice a day. This will help manage excess white discharge and vaginal odor.
2. Soak an alum stick in water and rub it gently near the mouth of the vagina. Alum sticks are available in the market. Do this once or twice daily until you get the desired results.
2. Mix one-fourth tablespoon of alum powder in a liter of water and wash your vagina with this water.
How Often You Should Do This
Drink alum water twice a day. Wash your vagina with alum water daily for two weeks.
Why This Works
Alum arrests bacterial growth by preventing bacterial adhesion to the vaginal wall, which is one of the reasons for vaginal odor.
13. Gooseberry (Amla)
One the of the best and effective herbal home remedies to get rid of vaginal odor is to eat gooseberry or amla every day until you get the desired results. Gooseberry has a lot of antioxidants and has anti-inflammatory and antibacterial properties.
You Will Need
2 gooseberries
½ teaspoon roasted cumin powder
A pinch of salt
1 glass water
What You Have To Do
1. Use a mortar and pestle to grind the gooseberries.
2. In a glass of water, add the gooseberry paste, roasted cumin powder, and a pinch of salt. Stir well before drinking. Do this for two weeks.
3. You can also slice a gooseberry, add salt to it and let it dry in the sun for two days. Eat two or three pieces of the dried gooseberry per day for a week.
4. Cut a gooseberry in half and put it in a glass of water and refrigerate it overnight. In the morning, add a little salt and roasted cumin powder and sip this water throughout the day. Do this for two weeks.
5. Juice the gooseberries and consume two tablespoons of the juice first thing in the morning every alternate day for two weeks.
How Often You Should Do This
Follow any of the above mentioned methods for atleast two weeks for effective results.
Why This Works
The juice of the gooseberry contains vitamin C while cumin aids digestion and improves immunity. Both the ingredients help to boost immunity and kill bacterial growth .
14. Neem
Neem leaves (Indian lilac) and neem bark have antimicrobial properties. Neem leaves have been used for ages to cure many skin diseases, smallpox, gut parasites, and wounds. Since vaginal odor can also be due to bacterial overgrowth, neem leaves can be used to treat vaginal odor effectively.
You Will Need
10 neem leaves
1 inch neem bark
1 liter water
What You Have To Do
Wash the neem leaves thoroughly and add them in water. Boil the water until the quantity reduces to half. Use this water to wash your vagina daily. Do this for at least one week.
1. Wash the neem leaves thoroughly and let them soak in water overnight. Use this water to wash your vagina.
2. Wash the neem leaves thoroughly and grind them using a mortar and pestle. Do not add water. Take the neem paste and use your palm to make five small “neem balls”. Gulp one neem ball every morning. Wash it down with water.
3. Put the neem bark in the water and boil it till the water reduces to half. Drink this water the first thing in the morning.
How Often You Should Do This
Wash your vagina with neem water twice daily for two weeks. Drink neem water every morning for two weeks.
Why This Works
Since neem leaves and bark have antimicrobial properties, a daily dose of this herbal medicine will help prevent microbial growth and clean your system from within
15. Fenugreek
The leaves and seeds of fenugreek are both beneficial for women. It helps to maintain hormonal balance, reduces abdominal fat, improves digestion, reduces blood sugar levels, and reduces menstrual cramps . To use fenugreek to eliminate vaginal odor, follow these steps:
You Will Need
1 teaspoon fenugreek seeds
1 liter water
What You Have To Do
1. Boil the fenugreek seeds in water until the quantity of water reduces to half. Cool it and drink it before breakfast every day.
2. Soak the fenugreek seeds in water overnight. Drink it the first thing in the morning every day.
How Often You Should Do This
For best results, drink fenugreek water for two weeks.
Why This Works
Fenugreek water has a subtle bitter-sweet taste. Apart from providing the body with vitamins and minerals, it also aids weight loss. Less fat in the body would lead to less sweat, which is one of the causes of foul vaginal odor.
16. Cranberry
You might be aware that cranberry juice is highly effective in treating urinary tract infection (UTI). Cranberries have antimicrobial and anti-inflammatory properties. Hence, they will help reduce the foul odor of your vagina.
You Will Need
1 cup fresh cranberries
1 liter water
What You Have To Do
1. Soak the cranberries in the water overnight. Sip this water all throughout the day. This will help to flush out toxins and prevent bacterial infections.
2. Blend or juice the cranberries and drink the juice without removing the pulp. Remove the pulp if you have Irritable Bowel Disease.
How Often You Should Do This
Drink a glass of cranberry juice every day to eliminate vaginal odor.
Why This Works
Cranberries are highly effective against bacteria that affect the vagina and urinary tract. Cranberries prevent the adhesion of the bacteria on the vaginal wall, therefore preventing bacterial growth.
17. Turmeric
Turmeric has antimicrobial, anti-inflammatory, and antioxidant properties. It is one of the best home remedies to treat microbial infections and wounds .
Here is how to use turmeric to eliminate vaginal odor.
You Will Need
1 inch turmeric root or 1 teaspoon turmeric powder
1 glass milk
What You Have To Do
1. Wash the turmeric root thoroughly. Peel it and chew on it the first thing in the morning.
2. Add turmeric powder to a glass of warm milk and drink it before going to bed.
3. Wash the turmeric root thoroughly. Peel it and boil it in a liter of water until the quantity of water reduces to half. Use this water to wash your vagina.
How Often You Should Do This
Wash your vagina with this water twice a week.
Why This Works
Turmeric, if consumed in the raw and natural form, helps to kill bacteria and boost immunity. You will see a visible difference in your skin and your vaginal odor.
18. Citrus Fruits
Citrus fruits, such as oranges, grapefruit, sweet lime, lemon, grapes, etc., are excellent sources of vitamin C that boosts immunity. It helps the body to fight against bacterial growth in the vagina. Therefore, eating citrus fruits or drinking fresh citrus fruit juices will help to get rid of vaginal odor.
You Will Need
½ cup green grapes
1 sweet lime or orange
1 liter water
What You Have To Do
1. Eat the citrus fruits.
2. Slice the fruits and toss them into a jar containing a liter of water. Let them soak overnight. Sip this water all throughout the day.
3. Juice the citrus fruits and drink.
How Often You Should Do This
Eat citrus fruits or drink juices daily to eliminate vaginal odor.
Why This Works
Citrus fruit juice or detox water will help to maintain the body’s pH balance and prevent microbial infection and itching in the vagina.
19. Seeds & Nuts
Nuts and seeds have a good amount of vitamin E, which prevents vaginal dryness and itching. Pumpkin seeds and almonds are rich in zinc, which helps to prevent vaginal dryness, itching, bacterial growth and odor. Other nuts, such as walnuts, flax seeds (rich in omega-3-fatty acid and polyestrogen), hazelnuts, and sunflower seeds, are also helpful in regulating the menstrual cycle and preventing vaginal dryness and hormone imbalance .
You Will Need
4 almonds
2 hazelnuts
1 tablespoon flax seed powder
1 cup milk
What You Have To Do
1. Soak the almond seeds in water for four hours.
2. Peel the skin of the almonds and toss into the blender.
3. Toss in the hazelnuts.
4. Pour the milk and give it a spin.
5. Pour out the milk into a cup.
6. Add the flaxseed powder and stir well.
Why This Works
Nuts and milk will help strengthen your bones, improve brain function, scavenge oxygen radicals, and boost immunity.
20. Guava Leaves
Guava leaves contain tannins, antioxidants, antibacterial, and anti-proactive properties. Guava leaves have been used to treat wounds and prevent microbial infections. Here is how to use guava leaves to treat foul vaginal odor.
You Will Need
4-5 guava leaves
1 liter water
What You Have To Do
Throw in the guava leaves into the water and boil the water until it reduces to half.
How Often You Should Do This
Drink this before breakfast every alternate day for two weeks.
Why This Works
Guava leaves have antimicrobial properties that make them one of the best herbal remedies to treat vaginal odor .
21. Lavender Oil
This sweet smelling and mood uplifting oil will help to reduce vaginal itching and irritation. Here is how to use it.
You Will Need
2 drops lavender oil
1 drop mint oil
What You Have To Do
1. Add the oils to your bath water and soak your body in the water for at least 10 minutes.
2. Add the oils to a liter of water and store in a bottle. Refrigerate it. Use cotton to dab this solution on the mouth of your vagina and vaginal area.
How Often You Should Do This
Do this every alternate day for a couple of weeks.
Why This Works
The aroma of this oil will make you feel rejuvenated, smell good all the day long, and curb the problem of vaginal odor.
22. Use Boric Acid
To prevent bacterial growth and vaginal itching, it is important to maintain an acidic pH in the vagina. Lactobacillus (the good bacteria) helps to maintain the acidic pH levels in the vagina. However, menstrual blood and semen increase the pH levels and make it favorable for bacterial growth. Using boric acid, a mild antiseptic, will help to lower the pH levels and prevent bacterial vaginosis,
Here is how to use boric acid to get rid of vaginal odor.
You Will Need
Boric Acid
Gelatin capsules – size “00”
What You Have To Do
1. Fill the gelatin capsules with boric acid and keep them safe in an airtight container. Store it in a cool and dry place.
2. Insert one boric acid filled capsule into your vagina. Keep it overnight.
How Often You Should Do This
Use these capsules for three consecutive nights if you have bacterial vaginosis (use increased amount of boric acid). After that, use these capsules twice a week.
Caution: Do not swallow the boric acid capsules. Make sure you label the container properly. Also, do not try this method if you are pregnant or trying to conceive. Keep the boric acid capsule container away from children.
Why Does My Vagina Smell?
Normally, the vagina consists of the perfect combination of healthy bacteria that maintain the pH in that region. When this balance is altered due to the different reasons listed above like other bacteria and yeast, there is a change in this pH. The number of healthy bacteria goes down, and the other unhealthy bacteria and yeast grow. These cause a change in the vaginal discharge’s color and consistency and also result in the foul smell in your private parts.
Vaginal Odor After Intercourse
It is seen in many women that right after intercourse, they experience a change in their vaginal discharge accompanied by a foul smell. This is because most bacterial and fungal infections are spread through sex . Having vaginal, oral, or anal sex, or any sexual contact involving touching fluids of an infected person can make you contract the infection. These infections cause rashes, abnormal vaginal discharge, and that peculiar fishy smell from your vagina . Wash your vaginal area with cold or lukewarm water before and after having sex. This will prevent any unwanted bacterial growth, itching, and yeast infections. You may also encourage your partner to do so as well.
Vaginal Odor During Pregnancy
Vaginal odor that results due to infections can cause severe complications during pregnancy . If you are planning to get pregnant, it is advisable to get tested for any vaginal infections and treat it as soon as possible.
Extra care needs to be taken during the course of your pregnancy to avoid contracting any infections that result in alterations in your normal vaginal discharge and smell. Consult your doctor in case you notice any strong foul odor.
How To Make Your Vagina Smell Good Fast
It makes sense to pay attention to what you eat and strike off food that triggers the bad odor. Sweet food that contains a lot of sugar or foods rich in yeast can often cause vaginal odor. You should avoid them to reduce the yeast infection, and, in turn, reduce the vaginal odor. Several vegetables like kale and celery and fruits like pineapple and cranberry are said to make your vagina smell good.
Also, remember, panty liners, pads, or any other such lining held in close contact with your private parts can lead to the production of yeast or bacteria, giving way to foul vaginal smell. Avoid the use or limit the use of liners and pads, unless absolutely necessary. The idea is to stay natural and play it safe by visiting your doctor regularly.
Drink Enough Water Daily
Water helps to maintain body’s temperature and cell integrity and flush out the harmful toxins. Dehydration is one of the causes of foul vaginal odor. Therefore, you need to stay hydrated. The amount of water you need to drink will depend on your height, weight, and activity levels. You will require more water if you are highly active.
Avoid Bathing In Hot Water
Hot water kills the body’s natural bacteria. The prolonged use of hot water for bathing will lead to vaginal odor. Take cold water baths or use lukewarm water to bathe. You can also add essential oils, rose petals, or camphor to your bath water.
Avoid High Yeast And Sugar Foods
High yeast and high sugar foods can lead to vaginal odor. Avoid eating bread, cakes, pastries, sweets, alcohol, donuts, etc. Nibble on dark chocolate when you crave for something sweet.
Eat Veggies And Fruits Every Day
Fruits and veggies are loaded with nutrients that help to fight a lot of health problems, including bacterial and yeast infections, heart disease, etc. Eat at least three servings of veggies and two servings of fruits to avoid foul vaginal odor. You can also make smoothies with vegetables or fruits for breakfast. Avoid spicy food and starchy veggies.
Stop Using Soaps And Fragrances
Soaps and fragrances contain chemicals that affect the pH balance of the vagina, which leads to bacterial growth. These chemicals also kill the natural bacteria present in the vaginal area. Therefore, to eliminate vaginal odor, avoid using soaps or fragrances in the vaginal area. Also, do not use water sprays or douches to wash your vaginal area. Water sprays or douches wash away the natural bacteria, leading to vaginal odor.
Wipe The Toilet Seat
The surface of toilet seats is a good place for many pathogenic bacteria. Therefore, always wipe the toilet seat, even if it looks clean, before sitting down on it. Do not flush while sitting on the seat. Be very careful while using public toilets.
Avoid Too Much Oil Or Meat During Periods
Vaginal odor during periods can be avoided by avoiding meat and a lot of oil in your food for the first three days of your period. Consume green leafy veggies, vegetable soup, smoothies, fresh fruits, fresh fruit juices, and fruit detox water. This will help prevent bacterial growth and any extra oil secretion through sweat glands, flush out toxins from the body, and maintain the pH balance.
Say Yes To Soft Panty Liners
Using uncomfortable pads or panty liners can cause vaginal irritation and itching. This may kill the natural vaginal bacteria and help in the growth of harmful bacteria. Switch to a panty liner that is soft and more comfortable for you. This will prevent the growth of harmful bacteria and eliminate vaginal odor.
Change Panty Liners Frequently
Panty liners should be changed after every three to four hours. Using a panty liner for more than four hours will aid bacterial growth, which can lead to foul odor. Also, try not to use tampons as they aid bacterial growth and cause itching and vaginal discomfort.
Change Underwear After Exercising
Sweaty, dark, and covered areas are ideal for bacterial growth. Therefore, change your underwear after exercising. It will help prevent itching, irritation, and foul odor.
Wash Your Underwear Regularly In Warm Water
Make sure to wash your underwear regularly in warm water. Soak your underwear in warm detergent water for 10 minutes before switching the washer on. This will help wash away any bacteria in your underwear. Also, dry your underwear properly before wearing it again.
Shed The Thigh Fat
Extra thigh fat causes extra sweat as the thighs constantly touch each other. This leads to bacterial growth and vaginal odor. Exercise regularly to shed a few pounds from the thigh area to completely eliminate vaginal itching and odor.
Check Your Hormones
Women who are undergoing hormonal changes or suffering from hormonal imbalance may have vaginal secretions that have a foul or fishy odor. Check with your gynecologist to know how these hormonal imbalances can be treated or the underlying reason for vaginal secretions. Use an antibacterial and antifungal powder on your inner thighs to get rid of vaginal odor temporarily.
Play It Safe
Always have safe sex if you suffer from foul vaginal odor. Safe sex will limit bacterial growth and also keep you away from harmful diseases.
Change Your Panties Twice A Day
One of the best ways to get rid of vaginal odor is to change panties twice a day or every 12 hours. Also, wear cotton panties rather than silk or satin. You may wear silk or satin panties, but do not wear them for longer hours. Satin and silk entrap sweat and urine, which leads to bacterial growth, and hence the foul smell. Change to a more comfortable cotton panty before going to sleep every night. Also, buy panties of different types so that the bacteria doesn’t get a favorable condition to grow
Ankylosing Spondylitis (Bechterew’s disease or Marie Struempell disease as it is also known) is a form of chronic, degenerative arthritis that affects the spine and sacroiliac joints and often other joints of the body.
Ankylosing spondylitis is a chronic inflammatory rheumatic disorder that primarily affects the axial skeleton. Sacroiliitis is its hallmark, accompanied by inflammation of the entheses (points of union between tendon, ligament, or capsule and bone) and formation of syndesmophytes, leading to spinal ankylosis in later stages. The pathogenesis of AS is poorly understood. [Rx]However, immune-mediated mechanisms involving human leucocyte antigen (HLA)-B27, inflammatory cellular infiltrates, cytokines (for example, tumor necrosis factor α and interleukin 10), and genetic and environmental factors are thought to have key roles. The detection of sacroiliitis by radiography, magnetic resonance imaging, or computed tomography in the presence of clinical manifestations is diagnostic for AS, although the presence of inflammatory back pain plus at least two other typical features of spondyloarthropathy (for example, enthesitis and uveitis) is highly predictive of early AS. Non-steroidal anti-inflammatory drugs (NSAIDs) effectively relieve inflammatory symptoms and are presently first-line drug treatment.[Rx]
What is Ankylosing Spondylitis?
Ankylosing Spondylitis (Bechterew’s disease or Marie Struempell disease as it is also known) is a form of chronic, degenerative arthritis that affects the spine and sacroiliac joints and often other joints of the body. The cause is currently unknown although there is a hereditary factor.
The word ankylosing means fusion and the word spondylitis means inflammation of the joints of the spine. Inflammation within the spine and sacroiliac joints develops which also triggers the development of bony growths which often fuse the vertebrae causing pain and stiffness. Ankylosing Spondylitis is one of a group of arthritis conditions known as spondoarthritides, including psoriatic, colitic and reactive arthritis. AS can occur in isolation or in conjunction with any of these conditions, as well as crohns disease, psoriasis and osteoporosis.
No two cases of AS are exactly the same. Variations occur in the distribution of pain, stiffness, inflammation and in the length of flare-ups and course of the disease. In some cases the disease becomes less active and pain may cease altogether.
Anatomy of Ankylosing Spondylitis
Ankylosing spondylitis is a systemic disease, meaning it can affect the entire body in some people. It can cause fever, loss of appetite, and fatigue, and it can damage other organs besides the joints, such as the lungs, heart, and eyes. Most often though, only the low back is involved.
The eye is the most common organ affected by ankylosing spondylitis. Eye inflammation (iritis) occurs from time to time in one-fourth of people with ankylosing spondylitis. Iritis results in a red, painful eye that also leads to photophobia, increased pain when looking at a bright light. It is a potentially serious condition requiring medical attention by an ophthalmologist. Luckily, it rarely causes blindness but it can affect vision while the inflammation is present.
Less frequently, ankylosing spondylitis may be associated with a scaly skin condition called psoriasis. In rare cases, typically when the ankylosing spondylitis has been present for many years, ankylosing spondylitis may cause problems with the heart or lungs. It can affect the large vessel called the aorta that moves blood from the heart into the body. Ankylosing spondylitis can cause inflammation where the heart and aorta connect leading to possible enlargement of the aorta.
Symptoms similar to that seen in ankylosing spondylitis may also may occur along with such conditions as psoriasis, inflammatory bowel disease, or Reiter’s syndrome. It is thought that bowel inflammation is somehow tied to the development of ankylosing spondylitis and this is the reason that people with inflammatory bowel disease, i.e. Crohn’s disease or ulcerative colitis are at an increased risk of the illness.
Causes of Ankylosing Spondylitis
www.rxharun.com
The exact cause of ankylosing spondylitis is unclear. It is thought to be an autoimmune disease – where the body’s own immune system attacks the body’s tissues causing inflammation and tissue damage.
Genetic (inherited) factors appear to influence development of AS. Approximately 90% of people diagnosed with AS have a gene called HLA-B27. However only about 10 – 15% of people with the gene will go on to develop AS. Approximately one in five individuals with AS also has a relative with the condition.
The information cited below is not binding. Each case should be adjudicated on the evidence provided and its own merits.
Idiopathic – The precise etiology is unclear.
Genetic – Although the precise cause of Ankylosing Spondylitis is unknown, there is a strong genetic component, i.e. HLA-B27. Significant physical traum – aggravation only Significant physical trauma will produce aggravation only in the site that is affected by significant physical trauma. For significant physical trauma to produce aggravation of Ankylosing Spondylitis, the following should be evident: Significant physical trauma must occur to an area of the body where Ankylosing Spondylitis is active; Increased signs/symptoms of Ankylosing Spondylitis must be present on a continuous or recurrent basis for at least 6 months. Significant physical trauma is a discrete injury that causes, within 24 hours of the injury being sustained, the development of acute symptoms and signs for which medical attention would normally or reasonably be sought.
The cause of ankylosing spondylitis (AS) is unknown – It’s likely that genes (passed from parents to children) and the environment both play a role. The main gene associated with the risk for AS is called HLA-B27. Having the gene doesn’t mean you will get AS. Fewer than 1 of 20 people with HLA-B27 gets AS. Scientists recently discovered two more genes (IL23R and ERAP1) that, along with HLA-B27, make it more likely you will get AS.
Inability to obtain appropriate clinical management. Medical Conditions Which Are To Be Included In Entitlement / Assessment
Peripheral arthritis due to ankylosing spondylitis
Enthesitis
Common Medical Conditions Which May Result In Whole Or In Part From Ankylosing Spondylitis
Restrictive lung disease
Cauda equina syndrome
Post-traumatic intervertebral fractures (the C5-C6 or C6-C7 level is the most commonly involved site)
Osteoporosis
Uveitis
Aortic regurgitation
Cardiac conduction abnormalities
Atlantoaxial subluxation
IgA nephropathy
Anatomy and Physiology of Ankylosing Spondylitis
Ankylosing Spondylitis has distinct pathological changes at the enthesis, i.e. the area in which a ligament or joint capsule attaches to bone.
The inflammatory component of this disease causes bony erosions at the enthesis. The body seeks to repair these erosions, and this repair activity results in ossification at these sites. It is this inflammation-repair process that is the basis for many of the findings in Ankylosing Spondylitis.
Ankylosing Spondylitis is usually diagnosed during the second to fourth decade of life. It is more common in first degree relatives of those with Ankylosing Spondylitis. While a strong affiliation with the HLA-B27 antigen supports a genetic predisposition, the evidence suggests that other factors also play a role in susceptibility to Ankylosing Spondylitis. The HLA-B27 antigen is a generic maker found in 8% of North Americans of European (white) heritage. Of those who are HLA-B27 positive, the actual risk of developing Ankylosing Spondylitis is estimated to be 1 to 2 %. Only 20% of HLA-B27 positive first degree relatives of individuals with Ankylosing Spondylitis and who are positive for HLA-B27 will develop the disease.
Symptoms of Ankylosing Spondylitis
General symptoms-
Difficulty bending the spine
Pain in the hips and difficulty walking- dull diffuse type of pain
Pain in the heels and soles of the feet- pain in worse in morning and night and better after a warm shower
Bent-over posture
Straightening of the normal curvature of the spine
Fever- In the early stages of disease, there may be mild fever, loss of appetite and general discomfort
Loss of appetite, weight loss
Fatigue, decreased energy
Eye swelling, redness and pain
Sensitivity to light
Difficulty taking a deep breath (because expanding the chest is difficult and painful)
Heart failure
Pain and stiffness. Constant pain and stiffness in the low back, buttocks, and hips that continue for more than three months. Back pain from ankylosing spondylitis is inflammatory in nature
The stiffness is often worst in the morning and after you have been inactive for a while
Bone fusion resulting in a rigid spine. These changes may be mild or severe, and may lead to a stooped-over posture
Pain in ligaments and tendons.
According to the Web Md
Symptoms of ankylosing spondylitis may initially be limited to lower back or joint aching, which is often just put down to ‘aches and pains’ and ‘growing pains’ in young people. Symptoms come and go and will usually progress to include the following:
Stiffness and pain in the morning affecting the sacroiliac joint area and spine.
Aching in the lower back which can disrupt sleep.
Pain radiating down the legs and into the groin.
Pain is worse during and after rest e.g. in the mornings.
Exercise eases the pain and stiffness.
Aches and pains in the buttocks, neck, shoulders, hips and upper back.
Symptoms may flare up and then disappear.
Severe cases may cause feelings of illness, weight loss and fatigue.
Back pain relieved by movement and exercise
Difficulty bending the spine
Pain in the hips and difficulty walking
Pain in the heels and soles of the feet
Bent-over posture
Straightening of the normal curvature of the spine
Fever
Loss of appetite, weight loss
Fatigue, decreased energy
Eye swelling, redness and pain
Sensitivity to light
Difficulty taking a deep breath (because expanding the chest is difficult and painful)
Diagnosis of Ankylosing Spondylitis
Early diagnosis of AS is important if fusion of the joints and permanent stiffening of the spine are to be avoided. It can be difficult to diagnose in the early stages as symptoms may be attributed to more common causes of back pain. A doctor will evaluate the following when diagnosing the condition:
These diagnostic criteria include:
Inflammatory back pain
Chronic, inflammatory back pain is defined when at least four out of five of the following parameters are present: (1) Age of onset below 40 years old, (2) insidious onset, (3) improvement with exercise, (4) no improvement with rest, and (5) pain at night (with improvement upon getting up)
A full medical history, including any family history of AS
Discussion of current symptoms including a history of back pain
The age of the patient when the pain started
Physical assessment
Past history of inflammation in the joints, heels, or tendon-bone attachments
Family history for axial spondyloarthritis
Positive for the biomarker HLA-B27
Good response to treatment with nonsteroidal anti-inflammatory drugs (NSAIDs)
Signs of elevated inflammation (C-reactive protein and erythrocyte sedimentation rate)
Manifestation of psoriasis, inflammatory bowel disease, or inflammation of the eye (uveitis)
If these criteria still do not give a compelling diagnosis magnetic resonance imaging (MRI) may be useful. MRI can show inflammation of the sacroiliac joint.
Radiographic features
The earliest changes in the sacroiliac joints demonstrable by plain x–ray shows erosions and sclerosis.
Progression of the erosions leads to pseudo-widening of the joint space and bony ankylosis.
X-ray spine can reveal squaring of vertebrae with spine ossification with fibrous band run longitudinally called syndesmophyte while producing bamboo spine appearance.
A drawback of X-ray diagnosis is the signs and symptoms of AS have usually been established as long as 8–10 years prior to X-ray-evident changes occurring on a plain film X-ray, which means a delay of as long as 10 years before adequate therapies can be introduced. Options for earlier diagnosis are tomography and MRI of the sacroiliac joints, but the reliability of these tests is still unclear.
Blood tests – which may show the presence of the HLA-B27gene, a raised ESR (erythrocyte sedimentation rate) and a reactive protein which indicates inflammation
Bamboo spine-Bamboo spine is a radiographic feature seen in ankylosing spondylitis that occurs as a result of vertebral body fusion. It is often accompanied by fusion of the posterior vertebral elements as well and resembles a bamboo stem…therefore the term bamboo spine.
In order for a diagnosis of AS to be made, a referral to a rheumatologist – who specialises in treating arthritis – may be recommended.
Treatment of Ankylosing Spondylitis
Non-Surgical Treatment
Bed rest for first 24 hours. Additional bed rest will be determined by the severity of the problem. Recent medical studies indicate that staying more active is better for back disorders than prolonged bed rest.
Use a firm mattress (place a bed board under the mattress if needed).
Massage may help. Be sure the person is well-trained or massage could cause more harm than help.
Wear a special back support device.
Other options are available depending on the degree of injury, such as surgery (if disk damaged), electrical nerve stimulation, acupuncture, special shoes, etc.
Stress reduction techniques, if needed.
Non-Prescription Pain Relievers – Naproxen, acetaminophen, and ibuprofen each reduce inflammation and pain. Though these drugs are available over-the-counter, they are potent and taking more than the recommended dose can harm health. A doctor can help with advice about the right kind of non-prescription pain reliever to take.
Cold and Heat – Applying a cold pack to the painful part of the back contracts inflamed muscle and relieves pain. This treatment helps a great deal when the disk has recently ruptured and swelling is at its greatest. A heating pad or warm pack helps with residual pain.
Continued Physical Activity – Though pain or weakness seem like good reasons to rest the back, excessive bed-rest worsens the symptoms of a slipped disc. Moving around too little allows muscles to grow weaker and prevents the body from healing. Periods of rest interspersed with periods of normal activity throughout the day keep the back muscles in shape.
Prescription Remedies – If over-the-counter drugs fail to ease slipped disc pain, the doctor will turn to prescription medications. These can include narcotics, such as hydrocodone or codeine. While they can do away with pain, narcotics are very addictive and induce a mental fogginess that can itself be dangerous. More narrowly-focused medicines designed to target damaged nerves that create chronic pain may be a better choice, as they have fewer undesirable side effects. Gabapentin and Cymbalta are two drugs that act in different ways to minimize nerve pain. These drugs are less addictive than narcotics.
Nutrition – In order to restore the disc we also are going to need to include different substances in our diet. There are a lot of supplements on the market, of course. If you wish to try them, that’s fine. I personally don’t like them. I have tried one with glucosamine and chondroitin, but I didn’t feel any different. So, if you have the opportunity to take these with the food or from more natural sources, it will be great. You can find these substances in seafood and animal cartilages and by digesting them we ensure the building blocks for the connecting tissue for our joints and spine. Also, we will need more Omega 3 fatty acids, which can be supplied from cold pressed oils, fatty fish, flax seeds, chia and many more. Vitamins from the B group are very beneficial for people with herniated discs and all kinds of issues with the peripheral nervous system. Vitamins B1, B6 and B12 nourish the nerves and help them recover from the disk accident. Usually, doctors prescribe them as a part of the treatment, but it is worth mentioning anyway.
A good massage – A massage is one of the natural methods of relieving pain. Individuals who get a massage weekly for several months stand a better chance of alleviating back pain. A good massage provides a person with many health benefits that lessen back pain. A massage triggers the release of endorphins. Endorphins aid in decreasing anxiety and relieving pain. They offer a relaxation effect by softening muscles that are injured preventing cramping.
Undertaking yoga – Yoga is an applicable strategy for keeping the level of back pain at minimal levels. Taking yoga sessions often is very an effective method of dealing with back pain. With yoga, there is a high likelihood of proper body functions. The use of pain prescriptions is also diminished. Patients suffering from back pain related issues do not have to rely on these prescriptions to manage pain. Incorporating laughter in yoga is a good way of exercising. Yoga incorporates simple yet appropriate exercises that enhance the stretching of muscles. Laughter with yoga stimulates relieving of pain. It facilitates increased uptake of oxygen, little anxiety, and production of endorphins. All these variables play an essential role in diminishing back pain.
Adjusting sleeping position – A simple sleeping mistake can immensely contribute to back pain. A poor sleeping position can cause stress and tension on the muscles contributing to back pain. Altering one’s sleeping position and adopting a style that does not exert a lot of stress on the back is a recommended tactic. Nurturing sleeping habits such as assuming a reclining position, using wedge-shaped cushions and getting adjustable beds from reputable medical institutions are easy techniques to endorse. If a reclining position does not suit an individual, the other two techniques can be embraced.
Heat therapy – Several considerations should be observed when using heat therapy. The right temperature ought to be set so as to ensure a patient does not face risks associated with too much exposure to heat. The key objective should be to ensure enough access to heat to the muscles to yield benefits for the patient. The adoption of heat therapy for easing back pain is determined by the magnitude of pain a person is experiencing. In cases where relatively low back pain is encountered, short heat therapy sessions are recommended. On the other hand, if an individual is experiencing prolonged back pain, long heat therapy sessions are the most applicable.
Taking hot baths – This is a form of heat therapy that aims at relieving back pain. It guarantees permeation of heat into the muscles leading to reduced pain. Many individuals opt for this method since they believe it achieves competent results. Hot baths initiate a fast process of blood supply to stiff neck and back muscles. When this happens, the muscles relax and stretch leading to decreased back pain. To avoid interference with one’s sleeping patterns, a hot bath should be taken several hours before retiring to bed.
Aquatic therapy – This natural technique involves physical therapy in a pool. Individuals get the best out of this therapy by relying on the resistance of water. Consistency in undertaking this therapy is what ascertains getting back pain relief. Integrating aquatic therapy in an individual’s life for the better part of the week enhances the reduction of back pain quickly.
Enlighten others – Individuals have the power to devise their own natural strategies that aid them in coping with back pain. The strategies can also be a good remedy for others going through similar circumstances. An individual can use social media platforms to equip others with important tips on how to keep back pain at bay. Further, becoming a member of associations that address back pain issues enables better communication of the knowledge gained from personal experience.
The major types of medications used to treat ankylosing spondylitis are pain-relievers and drugs aimed at stopping or slowing the progression of the disease. All of these have potentially serious side effects. Pain-relieving drugs come in two major classes:
Nonsteroidal anti-inflammatory drugs (NSAIDs) – These drugs relieve pain and swelling. Aspirin, ibuprofen, and naproxen are examples of NSAIDs. NSAIDs including the Coxib class are the first-line drugs for ankylosing spondylitis. A recent study reported that ankylosing spondylitis is associated with the prostaglandin E receptor 4 (PTGER4) gene. This receptor is associated with bone absorption; NSAIDs inhibit prostaglandin production, thus reducing the absorption[rx]. The mainstay of therapy in all seronegative spondyloarthropathies are anti-inflammatory drugs, which include NSAIDs such as ibuprofen, phenylbutazone, diclofenac,indomethacin,naproxen and COX-2 inhibitors, which reduce inflammation and pain. Indomethacin is a drug of choice. 2012 research showed that those with AS and elevated levels of acute phase reactants seem to benefit most from continuous treatment with NSAIDs.
Corticosteroids – These strong drugs are similar to the cortisone made by your body. They fight pain and swelling.
Analgesics – Acetaminophen and opioid-(like) agents are often used 1) for patients who complain of pain even after administration of NSAIDs and TNF-α inhibitors or 2) when other therapeutic options are not available.
Glucocorticoids – Although local glucocorticoid injection can be considered for skeletal muscle inflammation such as enthesitis, systematic administration of steroids is not generally recommended6)
Antidepressants – such as tricyclics and serotonin and norepinephrine reuptake inhibitors have been commonly prescribed for chronic low back pain, but their benefit for nonspecific low back pain is unproven, according to a review of studies assessing their benefit.
Glucosamine & Diacerein – can be used to tightening the loose tension and regenerate cartilage or inhabit the further degeneration of cartilage.
Corticosteroid- to healing the nerve inflammation and clotted blood in the joints.
Dietary supplement-to remove the general weakness & improved the health.
Muscle Relaxants – If the muscles around the slipped disc experience painful spasms, a muscle relaxant such as Valium may be useful. The drawback to drugs like these is that they do not limit their power to the affected nerve. Instead, they have a generally relaxing effect and will interfere with daily activities. Such as cyclobenzaprine (Flexeril), might be prescribed to relieve the discomfort associated with muscle spasms. However, these medicines might cause confusion in older people. Depending on the level of pain, prescription pain medicines might be used in the initial period of treatment.
Steroids – If inflammation is severe, a doctor may also prescribe a steroid. Steroids, such as cortisone, reduce swelling quickly. A cortisone shot directly in the affected area will have an immediate effect on the displaced disc.
Counter-irritants – such as creams or sprays applied topically stimulate the nerves in the skin to provide feelings of warmth or cold in order to dull the sensation of pain. Topical analgesics reduce inflammation and stimulate blood flow.
Nerve Relaxant — Pregabalin or gabapentin and anti-inflammatory drugs help to relieve pain and stiffness, allowing for increased mobility and exercise. There are many common over-the-counter medicines called non-steroidal anti-inflammatory drugs (NSAIDs). They include aspirin, ibuprofen, and naproxen.
Disease-modifying antirheumatic drugs (DMARDs) – These drugs work in different ways to reduce pain and swelling in AS. Although the administration of DMARDs (e.g., sulfasalazine and methotrexate) is not recommended for axial diseases such as back pain, sulfasalazine is worth considering for treatment of peripheral arthritis [Rx]. Disease-modifying antirheumatic drugs (DMARDs) such as sulfasalazine can be used in people with peripheral arthritis. For axial involvement, the evidence does not support sulfasalazine.Other DMARDs, such as methotrexate, did not have enough evidence to prove their effectiveness. Generally, systemic corticosteroids were not used due to lack of evidence. Local injection with a corticosteroid can be used for certain people with peripheral arthritis.
TNF-α inhibitors – In 1995, Braun and coworkers[rx] isolated TNF-α from ankylosing spondylitis patients via sacroiliac arthrocentesis. Thus, it was recognized that TNF-α is an important inflammatory mediator in this disease, which dramatically facilitated the development of biological agents.
Infliximab (Remicade) – Infliximab is a chimeric monoclonal antibody against TNF-α and is the first developed biological agent, consisting of 75% of human and 25% of mouse sequences[ rx]. This antibody directly binds to TNF-α and neutralizes it. It is administered by intravenous injections at 5 mg/kg body weight. For the first administration, the same dose of infliximab is injected twice with an interval of 2 weeks and then the drug is administered every 6 weeks. Baraliakos et al.[Rx] reported a drug survival rate (patients who completed 8 years of treatment) of 48% and 88% of partial remission or low disease activity after 8-year follow-up. It was also reported that the potency was similar when the treatment was interrupted for 3 years and then resumed.
Etanercept (Enbrel) – Etanercept is a soluble blocker of TNF-α. This fusion protein binds TNF-α, which hinders interactions between TNF-α and TNF-α receptor located on other cells. Etanercept is generally administered by subcutaneous injection of 25 mg twice a week [Rx]. Martĺn-Mola et al.[Rx]reported that 63% of the enrolled patients completed 5 years of etanercept administration without any serious complications, while Baraliakos reported a drug survival rate of 62%, partial remission in 31% of patients, and complete remission in 44% of patients in a 7-year follow-up study. Similar to infliximab, etanercept was effective when the medication was interrupted and then resumed; the drug survival rate was slightly higher in the etanercept group than in the infliximab group.
Adalimumab (Humira) – Like infliximab, adalimumab is a monoclonal antibody against TNF-α but its sequence is 100% human. Adalimumab is administered by subcutaneous injections of 40 mg once per 2 weeks. Sieper et al.[Rx] reported a drug survival rate of 65%, partial remission according to Ankylosing Spondylitis Disease Activity Score (ASDAS) in 51% of patients, and ASDAS inactive disease in 61% of patients in a 5-years follow-up study. Similar to the long-term follow-up results for infliximab, favorable outcomes of long-term follow-up were demonstrated with remission achieved after 12 weeks of administration.
Anti-tumor necrosis factor therapy —A group of medicines known as anti-tumor necrosis factor agents (anti-TNF agents or TNF inhibitors) are often effective in the treatment of AS. Examples of anti-TNF medications include infliximab, etanercept, adalimumab, certolizumab pegol, and golimumab. People who do not respond to one anti-TNF treatment may respond to another. Improvement in symptoms is common and may occur within a few weeks of starting the drugs.
Who should use anti-TNF therapy? – Not every patient with AS needs anti-TNF therapy. In general, people with the active disease in the spine who have not responded fully to NSAIDs may be candidates (see ‘How do I know how active my ankylosing spondylitis is?’ above). Your clinician may also recommend a glucocorticoid (cortisone-like drug) injection into painful or swollen joints before starting an anti-TNF drug if these areas continue to bother you despite using NSAIDs (see ‘Glucocorticoids (steroids)’ below). The decision to use anti-TNF therapy depends upon several factors that should be discussed with your clinician.
Secukinumab— Secukinumab (brand name: Cosentyx) may be an alternative treatment option for some people who do not respond adequately to anti-TNF therapy.
Glucocorticoids (steroids)— Some clinicians may also recommend a glucocorticoid injection into particularly painful or swollen joints, especially if only one or two areas are causing the most pain. In some cases, a glucocorticoid injection into the sacroiliac joint may help provide relief in patients who have sacroiliac pain that has not responded to other therapies.
Bisphosphonates – Oral bisphosphonates are commonly used for fracture prevention in ankylosing spondylitis. Bisphosphonates also have an anti-inflammatory action and may have an effect on disease activity. Intravenous pulses of the bisphosphonate pamidronate have been investigated in several studies and have produced significant clinical improvements in some but not all studies.[rx]
Other Medications to Stop Inflammation and Save Your Joints: Biological Drugs
If NSAIDs or DMARDs do not control your AS, your doctor may prescribe drugs called biologics. These drugs aim to address the problems with your immune system. They target your body’s production of specific proteins that cause inflammation.
Biologic drugs slow your immune system to help ease AS symptoms (pain, swelling, tenderness, and stiffness) as well as inflammation. These drugs may also help protect your joints from damage.
You are at higher risk of infections like tuberculosis when you take biologics. If you have signs of an infection, such as a fever or congestion, you should tell your doctor. Your doctor will test you for tuberculosis before you start a biologic drug and while you take it. These drugs also may raise your risk of getting certain types of cancer, but this is rare.
Doctors and scientists are constantly coming up with new ways to treat diseases, and they always need patients to test the efficacy of a proposed intervention. Below, you will find a current list of trials for ankylosing spondylitis and related conditions, as well as a link to enroll. You should speak with your doctor to decide if enrolling in a clinical trial is a good option for you.
Study Title
Description
Link
A Study to Evaluate the Efficacy and Safety of Ustekinumab in the Treatment of A … Show More
A Study Treating Participants With Early Axial Spondyloarthritis (axSpA) Taking … Show More
Condition: Axial Spondyloarthritis Intervention: Biological: Adalimumab; Other: Standard of Care (SOC)
Sponsor: AbbVie; Improvement by Movement GmbH, Germany; Hannover Medical School; IST GmbH, Germany Recruiting – verified October 2016
An Efficacy and Safety Study of Ustekinumab in Participants With Active Nonradio … Show More
Condition: Nonradiographic Axial Spondylitis, Ankylosing Intervention: Drug: Group 1: Placebo; Drug: Group 2: Ustekinumab 45 mg; Drug: Group 3: Ustekinumab 90 m
[/dropshadowbox]
Physical therapy
Though physical therapy remedies have been scarcely documented, some therapeutic exercises are used to help manage lower back, neck, knee, and shoulder pain. Some therapeutic exercises include
Moderate-to-high impact exercises like jogging are generally not recommended or recommended with restrictions due to the jarring of affected vertebrae that can worsen pain and stiffness in some with AS.
Physical therapy and education – The most important component of non-drug treatments of ankylosing spondylitis is the education of patients and regular exercise. Although home exercise is known to be effective, group physical therapy under appropriate supervision is more efficient than individual exercise6). It is important to educate patients that proper exercise not only alleviates pain but also relaxes the joints so that daily life activities are not affected.
Stretching – Stretching helps build flexibility and may reduce pain. Consider adding the spine stretch or the low-back rotation stretch to your daily routine.
Heat therapy – Apply a hot water bottle or heating pad to the affected area to reduce stiffness and pain. You may also use moist or dry heat. A warm bath may also help, especially before exercise. Don’t use heat therapy without consulting your doctor if you have diabetes, deep vein thrombosis, vascular disease, an open wound, or a skin condition such as dermatitis.
Cold therapy – Applying an ice pack, cold gel pack, or a bag of frozen vegetables to painful joints can help reduce swelling. After exercise, cold therapy may help reduce inflammation. Don’t apply ice for more than 20 minutes at a time. Don’t use cold therapy without consulting your doctor if you have circulation problems.
Acupuncture – Acupuncture is an ancient remedy for pain. It involves inserting thin needles into specific points in your skin. This is thought to activate your body’s pain-relieving hormones. Some people report acupuncture relieves AS pain.
Massage therapy – Massage helps you relax. It may also help you feel more flexible or “loose” so that you can exercise or stretch. Massage may cause pain at tender points around your spine. If this happens, avoid those areas and only use light massage techniques until the pain improves.
Movement – The more you sit, the stiffer you’re likely to feel. Get up, move around, and stretch regularly. If you have a desk job, take a “get up and move” break every hour.
Exercise – Gentle exercise programs such as yoga and Pilates are great for AS because they incorporate stretching. Swimming may also be beneficial because it’s easy on your joints. Strengthening exercises with weights can help build muscle, which supports joints affected by AS.
Alexander Technique – AS often leaves you hunched over. Practicing good posture is critical. The Alexander Technique teaches you to be aware of your posture throughout your day. It also teaches you how to correct poor posture and may be helpful for people with AS.
TENS Therapy – TENS stands for transcutaneous electrical nerve stimulation. This therapy uses electrical current to stimulate nerves through the body for pain control. Electrodes are usually applied at the pain site and connected to a TENS machine. It’s thought that when TENS stimulates nerves, it overrides pain signals. The TENS technique is usually taught by a physical therapist and may be continued at home.
Stop smoking – Smokers, especially men, are at risk for greater spine damage from AS than non-smokers. Quitting smoking not only helps reduce AS damage but also improves your overall health.
Physiotherapy – In spondylosis (spinal osteoarthritis), your spinal joints don’t move as well as they used to because of age-related changes in your spine, similar to arthritis. This can make it very painful to move because of decreased mobility within the spine itself. Your doctor may recommend physical therapy as part of your treatment plan because a physical therapist can help you maintain and increase mobility, learn ways to reduce pain, strengthen your spinal muscles so that they better support your spine, and stretch muscles that may be increasing nerve compression in your spine.
Physical therapy involves three main components: education, passive treatments, and active treatments. A physical therapist uses passive treatments to relax you and your body and to decrease acute pain or inflammation. They’re called passive because you don’t have to actively participate. If you’re experiencing acute pain, you’ll most likely start with passive treatments as your body heals and/or adjusts to the pain. However, the goal of physical therapy is to get into active treatments. These are therapeutic exercises that strengthen your body so that your spine has better support.
Passive Treatments for Ankylosing Spondylitis
Your physical therapist may give you passive treatments such as:
Deep Tissue Massage – This technique targets spasms and chronic muscle tension that perhaps builds up through daily life stress. You could also have spasms or muscle tension because of strains or sprains. The therapist uses direct pressure and friction to try to release the tension in your soft tissues (ligaments, tendons, muscles).
Hot and Cold Therapies – Your physical therapist will alternate between hot and cold therapies. By using heat, the physical therapist seeks to get more blood to the target area because an increased blood flow brings more oxygen and nutrients to that area. Blood is also needed to remove waste byproducts created by muscle spasms, and it also helps to heal. Cold therapy, also called cryotherapy, slows circulation, helping to reduce inflammation, muscle spasms, and pain. You may have a cold pack placed upon the target area, or even be given an ice massage. Another cryotherapy option is a spray called fluoromethane that cools the tissues. After cold therapy, your therapist may work with you to stretch the affected muscles.
Electrical stimulation – This can be performed within the clinic and if extremely successful, a TENS unit can be issued to a patient for home use. E-stim stimulates your muscles through variable (but safe) intensities of electrical current. It helps to reduce muscle spasms, and it may increase your body’s production of endorphins, your natural pain killers. It may also drive out inflammation, bring in healing properties, relax, and re-educate the muscles involved. The e-stim unit in the clinic is of a professional standard; the equipment is relatively large. However, a smaller machine for at “at home” use is also available. Electrical stimulation is a helpful therapy.
Yoga – Yoga is a great natural pain reliever for ankylosing spondylitis,” Ostrowski says. “You need to start with very basic poses and be patient, but if you work with an instructor who can modify the yoga positions for you, you can really benefit from this form of exercise.” A review of studies published in January 2016 in the Journal of Orthopedics & Rheumatology examined the impact of yoga on low back pain and found that it was safe and can help reduce both disability and pain.
Omega-3 fats and inflammation – Foods that contain omega-3 fats have been found to help reduce the inflammation associated with some forms of arthritis. These effects are modest compared with medication.
Omega-3 fats have few side effects and may have other health benefits, such as reduced heart disease. Foods rich in omega-3 fats include
fish – the oily fish such as salmon and sardines have greater amounts of omega-3 fats
linseeds and linseed (flaxseed) oil
canola (rapeseed) oil
walnuts
foods fortified with omega-3, such as margarine and eggs
some fish oil supplements.
Potassium Rich Foods
Potassium is known to decrease inflammation if it is present in the body in adequate amounts. Foods that contain potassium in high amounts are bananas, almonds, apricots, and broccoli.
Vitamin D – You must correct the vitamin D deficiency in your body if you are suffering from ankylosis. Bones need Vitamin D in greater amounts when they are affected by a disease.
Home Remedies For Ankylosing Spondylitis
Use Ginger, Black Pepper or any good digestive with your meals. It will help detoxify your body.
1 tablespoonful of Turmeric should be consumed once every day, after boiling it in milk for half an hour.
Constipation must be avoided at all costs. Constipation may increase pain in Ankylosing spondylitis.
Herbs have divine healing powers and they have the ability to cure any disease of the root. They were gifted to us by God when he created life. So believe in God if you want to get rid of your problems!
Ayurvedic herbs are unique natural remedies for Ankylosing spondylitis. Ayurvedic principles are different in many ways From modern medicine for example – Drinking water From a copper pan after keeping it overnight is also very useful in Rheumatoid arthritis and Ankylosing spondylitis.
Consuming castor oil at night with milk or alone is a very useful herbal remedy for arthritis, especially rheumatoid arthritis and ankylosing spondylitis.
Improve your nutrition as the first step. It plays an important role to fight diseases. When nothing works, nutrition works a lot !
Use herbal juices like Aloe vera juice (Kumari Saar) and Amla Juice ( Amla Saar) in routine. Amla is the richest source of natural Vitamin C. Vitamin C improves the natural immunity of the body. 100 gm of Amla juice contains 30 times more vitamin C than 100 gm of oranges.
Homeopathic treatment for Ankylosing Spondylitis
Homeopathy treats the person as a whole. A Remedy is selected after full individualizing examination and case analysis which includes a medical history of the patient, physical and mental constitution etc.
Phosphorus – The rigidity of nape of the neck. Pressure on shoulders. Swelling of the neck. Engorgement of axillary glands and of those of nape of the neck and of the neck. Paralyzes sensation in the upper sacrum and lower lumbar vertebrae. Contusive pain in loins and back (as if the back were broken), especially after having been seated a long time Sensitiveness of spinous processes of dorsal vertebrae to pressure.
Silicea –The stiffness of nape, with a headache. Swelling of glands of nape, in the neck, and under the axillae (with suppuration), sometimes with indurations…Stitches between the hips.Coccyx painful, as after a long carriage ride.- Stinging in os coccyx on rising, painful to pressure. -Scabby elevation on the coccyx, above fissure of nates- Inflammatory abscess in the lumbar region (on the psoas muscle).- Weakness and paralytic stiffness in back, loins, and nape.
Aurum Metallicum – Serious or advanced rheumatism with marked stiffness. Rheumatism with stiffness or spasms of the chest wall. Severe spasm or tearing pains. Pains also described as “paralytic.” An important remedy in ankylosing spondylitis. Wandering arthritis; moving spot to spot from one week to next. Worse: Night. Morning in bed. Hip pain worse rising from a seat or from walking.
Sulfur – The stiffness of the neck, in nape, with a paralytic, sprained pain. A child cannot hold head up neck muscles so weak. Tetters on nape. Swelling and inflammation of glands of nape and of the neck. Swelling and suppuration of axillary glands. Cracking in vertebrae of the neck, especially on bending backward.
Maintain a healthy weight– If you are overweight or obese, the extra load on your joints may be exacerbating your symptoms, especially if your affected joints include those of the hip, knee or spine. There is also a clear link between being overweight and an increased risk of developing osteoarthritis.
Early studies of anti–tumor necrosis factor (TNF)-alpha therapy over 2 years showed no structural progression of ankylosing spondylitis (AS) on radiography. However, more recent data indicated that a strong relationship exists between disease activity and structural progression . If you have inactive disease, it’s a relatively flat line, but if you have very high disease activity, there’s a very striking relationship between disease activity and the Ankylosing Spondylitis Disease Activity Score,” said Dr. Elewaut of the department of rheumatology at Ghent (Belgium) University Hospital. “We were missing something in the early clinical studies of anti-TNF alpha agent, and there are a few explanations as to why.”
Antioxidants are compounds that inhibit oxidation. Oxidation is a chemical reaction that can produce free radicals, thereby leading to chain reactions that may damage the cells of organisms. Antioxidants such as thiols or ascorbic acid (vitamin C) terminate these chain reactions. To balance the oxidative state, plants and animals maintain complex systems of overlapping antioxidants, such as glutathione and enzymes (e.g., catalase and superoxide dismutase), produced internally, or the dietary antioxidants vitamin A, vitamin C, and vitamin E.
Antioxidants neutralize free radicals produced by various environmental insults such as ultraviolet radiation, cigarette smoke and air pollutants, thereby preventing cellular damage. The role of oxidative stress and antioxidants is known in diseases like obesity, atherosclerosis, and Alzheimer’s disease. Herein we discuss the effects of oxidative stress on the skin and role of antioxidants in dermatology.
Vitamin include in Antioxidants
Some compounds contribute to antioxidant defense by chelating transition metals and preventing them from catalyzing the production of free radicals in the cell. Particularly important is the ability to sequester iron, which is the function of iron-binding proteins such as transferrin and ferritin. Selenium and zinc are commonly referred to as antioxidant nutrients, but these chemical elements have no antioxidant action themselves and are instead required for the activity of some antioxidant enzymes, as is discussed below.
Antioxidant
Solubility
Concentration in human serum (μM)
Concentration in liver tissue (μmol/kg)
Ascorbic acid (vitamin C)
Water
50–60
260 (human)
Glutathione
Water
4
6,400 (human)
Lipoic acid
Water
0.1–0.7
4–5 (rat)
Uric acid
Water
200–400
1,600 (human)
Carotenes
Lipid
β-carotene: 0.5–1retinol (vitamin A): 1–3
5 (human, total carotenoids)
α-Tocopherol (vitamin E)
Lipid
10–40
50 (human)
Ubiquinol (coenzyme Q)
Lipid
5
200 (human)
Uric acid
Uric acid has the highest concentration of any blood antioxidants and provides over half of the total antioxidant capacity of human serum. Uric acid’s antioxidant activities are also complex, given that it does not react with some oxidants, such as superoxide, but does act against peroxynitrite, peroxides, and hypochlorous acid.
Concerns over elevated UA’s contribution to gout must be considered as one of many risk factors. By itself, UA-related risk of gout at high levels (415–530 μmol/L) is only 0.5% per year with an increase to 4.5% per year at UA supersaturation levels (535+ μmol/L). Many of these aforementioned studies determined UA’s antioxidant actions within normal physiological levels, and some found an antioxidant activity at levels as high as 285 μmol/L.
Vitamin C
Ascorbic acid or “vitamin C” is a monosaccharide oxidation-reduction (redox) catalyst found in both animals and plants. As one of the enzymes needed to make ascorbic acid has been lost by mutation during primate evolution, humans must obtain it from the diet; it is, therefore, a vitamin. Most other animals are able to produce this compound in their bodies and do not require it in their diets.
Ascorbic acid is required for the conversion of the procollagen to collagen by oxidizing proline residues to hydroxyproline. In other cells, it is maintained in its reduced form by reaction with glutathione, which can be catalysed by protein disulfide isomerase and glutaredoxins. Ascorbic acid is a redox catalyst which can reduce, and thereby neutralize, reactive oxygen species such as hydrogen peroxide. In addition to its direct antioxidant effects, ascorbic acid is also a substrate for the redox enzyme ascorbate peroxidase, a function that is particularly important in stress resistance in plants. Ascorbic acid is present at high levels in all parts of plants and can reach concentrations of 20 millimolar in chloroplasts.
Glutathione
The free radical mechanism of lipid peroxidation. Glutathione is a cysteine-containing peptide found in most forms of aerobic life. It is not required in the diet and is instead synthesized in cells from its constituent amino acids. Glutathione has antioxidant properties since the thiol group in its cysteine moiety is a reducing agent and can be reversibly oxidized and reduced.
In cells, glutathione is maintained in the reduced form by the enzyme glutathione reductase and in turn reduces other metabolites and enzyme systems, such as ascorbate in the glutathione-ascorbate cycle, glutathione peroxidases, and glutaredoxins, as well as reacting directly with oxidants. Due to its high concentration and its central role in maintaining the cell’s redox state, glutathione is one of the most important cellular antioxidants. In some organisms, glutathione is replaced by other thiols, such as by mycothiol in the Actinomycetes, bacillithiol in some Gram-positive bacteria, or by trypanothione in the Kinetoplastids.
Vitamin E
Vitamin E is the collective name for a set of eight related tocopherols and tocotrienols, which are fat-soluble vitamins with antioxidant properties. Of these, α-tocopherol has been most studied as it has the highest bioavailability, with the body preferentially absorbing and metabolizing this form.
It has been claimed that the α-tocopherol form is the most important lipid-soluble antioxidant and that it protects membranes from oxidation by reacting with lipid radicals produced in the lipid peroxidation chain reaction. This removes the free radical intermediates and prevents the propagation reaction from continuing. This reaction produces oxidised α-tocopheroxyl radicals that can be recycled back to the active reduced form through reduction by other antioxidants, such as ascorbate, retinol or ubiquinol.
This is in line with findings showing that α-tocopherol, but not water-soluble antioxidants, efficiently protects glutathione peroxidase 4 (GPX4)-deficient cells from cell death. GPx4 is the only known enzyme that efficiently reduces lipid-hydroperoxides within biological membranes.
Beta-carotene
Beta-carotene is a fat soluble member of the carotenoids which are considered provitamins because they can be converted to active vitamin A. Beta-carotene is converted to retinol, which is essential for vision. It is a strong antioxidant and is the best quencher of singlet oxygen. However, beta-carotene supplement in doses of 20mg daily for 5-8 years has been associated with an increased risk of lung and prostate cancer and increased total mortality in cigarette smokers (rx). Beta-carotene 20-30mg daily in smokers may also increase cardiovascular mortality by 12% to 26% (rx). These adverse effects do not appear to occur in people who eat foods high in beta-carotene content. Beta-carotene is present in many fruits, grains, oil and vegetables (carrots, green plants, squash, spinach) (rx).
Lycopene
Lycopene, a carotenoid, possesses antioxidant and antiproliferative properties in animal and in vitro studies on breast, prostate and lung cell lines, although anticancer activity in humans remains controversial (rx, rx,). Lycopene has been found to be very protective, particularly for prostate cancer (rx). Several prospective cohort studies have found associations between high intake of lycopene and reduced incidence of prostate cancer, though not all studies have produced consistent results (rx). The major dietary source of lycopene is tomatoes, with the lycopene in cooked tomatoes, tomato juice and tomato sauce included, being more bioavailable than that in raw tomatoes (rx).
Selenium (Se)
Se is a trace mineral found in soil, water, vegetables (garlic, onion, grains, nuts, soybean), seafood, meat, liver, yeast (rx). It forms the active site of several antioxidant enzymes including glutathione peroxidase. At low dose, health benefits of Se are antioxidant, anti-carcinogenic and immunomodulator (rx). Selenium is also necessary for the thyroid function (rx). Exceeding the Tolerable Upper Intake Level of 400 μg Se/day can lead to selenosis which is a selenium poisoning characterized by gastrointestinal disorders, hair and nail loss, cirrhosis, pulmonary edema and death (rx).
Selenium deficiency can occur in patients on total parenteral nutrition (TPN) and in patients with gastrointestinal disorders. In certain China areas with Se poor soil, people have developed a fatal cardiomyopathy called Keshan disease which was cured with Se supplement (rx). The role of Se in cancer prevention has been the subject of recent study and debate. Results from clinical and cohort studies about cancer prevention, especially lung, colorectal, and prostate cancers are mixed (rx, rx).
Flavonoids
Flavonoids are polyphenolic compounds which are present in most plants. According to chemical structure, over 4000 flavonoids have been identified and classified into flavanols, flavanones, flavones, isoflavones, catechins, anthocyanins, proanthocyanidins. Beneficial effects of flavonoids on human health mainly reside in their potent antioxidant activity (rx).
They have been reported to prevent or delay a number of chronic and degenerative ailments such as cancer, cardiovascular diseases, arthritis, aging, cataract, memory loss, stroke, Alzheimer’s disease, inflammation, infection. Every plant contains a unique combination of flavonoids, which is why different herbs, all rich in these substances, have very different effects on the body (rx). The main natural sources of flavonoids include green tea, grapes (red wine), apple, cocoa (chocolate), ginkgo biloba, soybean, Curcuma, berries, onion, broccoli, etc.
For example, green tea is a rich source of flavonoids, especially flavonols (catechins) and quercetin. Catechin levels are 4-6 times greater in green tea than in black tea. Many health benefits of green tea reside in its antioxidant, anticarcinogenic, antihypercholesterolemic, antibacterial (dental caries), anti-inflammatory activities (rx).
Omega-3 and omega-6 fatty acids.
They are essential long-chain polyunsaturated fatty acids because the human body cannot synthesize them. Therefore, they are only derived from food. Omega-3 fatty acids can be found in fat fish (salmon, tuna, halibut, sardines, pollock), krill, algae, walnut, nut oils and flaxseed. However, certain big fishes like tilefish, shark, swordfish are to be avoided because of their high mercury levels (rx).
There are three major dietary types of omega-3 fatty acids: eicosapentaenoic acid (EPA), docosahexaenoic acid (DHA) and alpha-linolenic acid (ALA). EPA and DHA are abundant in fish and are directly used by the body; while ALA is found in nuts and has to be converted to DHA and EPA by the body. Dietary sources of omega-6 fatty acids (linoleic acid) include vegetable oils, nuts, cereals, eggs, poultry. It is important to maintain an appropriate balance of omega-3s and omega-6s in the diet, as these two substances work together to promote health (rx, rx).
Benefits of Antioxidants
Antioxidants come up frequently in discussions about good health and preventing diseases. These powerful substances, which mostly come from the fresh fruits and vegetables we eat, prohibit (and in some cases even prevent), the oxidation of other molecules in the body. The benefits of antioxidants are very important to good health, because if free radicals are left unchallenged, they can cause a wide range of illnesses and chronic diseases.
Antioxidants and Free Radicals
The human body naturally produces free radicals and the antioxidants to counteract their damaging effects. However, in most cases, free radicals far outnumber the naturally occurring antioxidants. In order to maintain the balance, a continual supply of external sources of antioxidants is necessary in order to obtain the maximum benefits of antioxidants. Antioxidants benefit the body by neutralizing and removing the free radicalsfrom the bloodstream.
Different Antioxidants Benefit Different Parts of the Body
There are a wide range of antioxidants found in nature, and because they are so varied, different antioxidants provide benefits to different parts of the body. For example, beta-carotene (and other carotenoids) is very beneficial to eye health; lycopene is beneficial for helping maintain prostate health; flavonoids are especially beneficial for heart health; and proanthocyanidins are beneficial for urinary tract health.
Antioxidants and Skin Health Benefits
When skin is exposed to high levels of ultraviolet light, photo-oxidative damage is induced by the formation of different types of reactive species of oxygen, including singlet oxygen, superoxide radicals, and peroxide radicals. These forms of reactive oxygen damage cellular lipids, proteins, and DNA, and they are considered to be the primary contributors to erythema (sunburn), premature aging of the skin, photodermatoses, and skin cancers.
Astaxanthin, followed by beta-carotene combined with vitamin E has been shown to be one of the most powerful antioxidant combinations for helping protect the skin from reactive species of oxygen.
Antioxidants and Immune System Support
Singlet oxygen can compromise the immune system because it has the ability to catalyze the production of free radicals. Astaxanthin and Spirulina have been shown to enhance both the non-specific and specific immune system and to protect cell membranes and cellular DNA from mutation.
Astaxanthin is the single most powerful quencher of singlet oxygen and is up to ten times stronger than other carotenoids (including beta-carotene), and up to 500 times stronger than alpha tocopherol (Vitamin E), while Spirulina has a variety of antioxidants and other substances that are beneficial in boosting immunity.
Additional Ways Antioxidants Help Benefit One’s Health
Increasing one’s antioxidant intake is essential for optimum health, especially in today’s polluted world. Because the body just can’t keep up with antioxidant production, a good amount of these vitamins, minerals, phytochemicals, and enzymes must come from one’s daily diet. Boosting your antioxidant intake can help provide added protection for the body against:
Antioxidant Supplementation and Diabetic Kidney Disease
www.rxharun.com
Diabetes’ propensity to cause metabolic derangement is directly responsible for a looming epidemic of diabetic kidney disease (DKD). And left unchecked, DKD can progress to end-stage kidney disease (ESKD).
About 50% of all those with ESKD developed it after a diabetes diagnoses. ESKD’s progression is associated with an increased risk of cardiovascular events and hospitalizations, and those complications escalate in patients who need chronic renal replacement therapy by dialysis or kidney transplant.
A team of researchers from Italy has published a review and meta-analysis in the journal PLOS ONEthat examines use of chronic antioxidant supplementation as a tool to retard kidney disease progression in patients who have diabetes.
The authors looked at many studies that used various antioxidants in an attempt to slow DKD. They found multiple randomized controlled trials but had difficulty comparing and contrasting the results due to varying sample sizes, study designs, and outcome measures.
One area in which there was considerable diversity was the definition of kidney disease progression to end stage. Some studies defined this point as a need for chronic dialysis or kidney transplant, but other studies used surrogate endpoints such as changes in urinary albumin excretion or renal function.
Overall, the researchers concluded that studies have shown that the use of antioxidants can reduce albuminuria. This finding is encouraging because pathological urinary albumin excretion is an early sign of DKD. In this meta-analysis, the researchers found that antioxidant supplementation was associated with significant reductions in albumin excretion.
Studies employed many antioxidants including vitamin C, vitamin E, zinc, and silymarin. Several studies used oxidants in combination. Evidence was strongest for vitamin E in doses ranging from 480 mg to 1200 mg daily.
Most studies indicated that participants reported no significant adverse events, though a few studies did not seem to examine adverse events systematically.
www.rxharun.com
The authors reported that additional studies are needed to determine which oxidants and at what dose) are most likely to slow DKD progression. They also indicated the need for better definitions of outcomes.
Workhorse Vitamin: A Primer on Vitamin B12
Vitamin B12 (cobalamin) is a workhorse vitamin. It helps keep nerve and blood cells healthy, make DNA, and prevent megaloblastic anemia. Cobalamin is different from other vitamins because it is not plant-sourced, but is found naturally in a wide variety of animal products such as meat, fish, eggs, and dairy.
The July 2017 issue of Nature Reviews Disease Primers includes a disease primer that discusses the epidemiology, mechanism/pathophysiology, diagnosis/screening, prevention, and management of vitamin B12 deficiency.
B12 status varies through the lifetime, creating a need to consider patient factors when interpreting diagnostic biomarkers of B12 status. Inadequate intake, impaired absorption, chemical inactivation, or inherited B12 transport or metabolism impairment may lead to deficiency. Diagnosis is critical because B12 deficiency can be life-threatening.
Clinical B12 deficiency with hematological and neurological manifestations is relatively uncommon. On the other hand, 2.5-26% of the general population has subclinical deficiency and it’s unclear if these people will progress to deficiency or continue to have low but stable B12 levels.
B12 deficiency’s signs and symptoms are weakness, constipation, numbness and tingling in the hands and feet, confusion, poor memory, and mouth or tongue soreness. Vitamin B12 deficiency can affect individuals at any age, but vegans and elders are at increased risk. It is often difficult to diagnose elderly patients because its typical clinical manifestations are absent or are confused with dementia.
Increased consumption of animal products and fortified foods may prevent B12 deficiency, as will oral or parenteral B12 supplementation. Initially, higher doses are required to replete B12 stores in the body.
Hematologic abnormalities respond to B12 treatment in about 5 days and completely recover in 4 to 6 weeks. Neurological abnormalities are slower to correct. B12 deficiency not due to nutritional deficiency may require lifelong treatment.
Erectile dysfunction (ED)also known as impotence is a type of sexual dysfunction characterized by the inability to develop or maintain an erection of the penis during sexual activity. Erectile dysfunction can have psychological consequences as it can be tied to relationship difficulties and self-image.
Erectile dysfunction (ED) is defined as the persistent inability to attain and maintain an erection that is sufficient to permit satisfactory sexual performance (rx). The current pharmaco-therapeutic research in ED focuses on underlying endothelial dysfunction as the root cause for ED and introduction of phosphodiesterase type 5 inhibitors to potentiate nitric oxide (NO) action and cavernosal smooth muscle vasodilation, has revolutionized modern ED treatment over the past two decades (Rx). In contrast to Western Medicine, the traditional and complementary medicine (TCM) aims at restoration and better overall bodily regulation with medicine to invigorate qi (energy) in vital organs such as kidney, spleen, and liver; to enhance physical fitness, increase sexual drive, stabilize the mind and improve the overall situation resulting in natural and harmonious sexual life (rx).
Types of Erectile Dysfunction
There are two different types of premature ejaculation
Primary (lifelong)
Secondary (acquired)
Algorithm for the diagnosis and treatment of erectile dysfunction.
Types of ED and associated causes*
Classification
Causes
Psychogenic
Physical and mental health problems
Psychological trauma
Relationship problems/partner dissatisfaction
Family/social pressures
Depression
Organic
Neurologic
Central nervous system—spinal cord injury, multiple sclerosis, stroke
*The below causes are often characteristic of the following classifications, however it should be remembered that ED etiology is often “mixed”
Pathophysiology of Erectile Dysfunction
ED may result from organic causes (e.g., vascular, neurogenic, hormonal, anatomic, drug-induced), psychological causes, or a combination of both. A normal sexual erectile response results from the interaction between neurotransmitter, biochemical, and vascular smooth muscle responses initiated by parasympathetic and sympathetic neuronal triggers that integrate physiologic stimuli of the penis with sexual perception and desire. Nitric oxide produced from endothelial cells after parasympathetic stimuli triggers a molecular cascade that results in smooth muscle relaxation and arterial influx of blood into the corpus cavernosum. This is followed by compression of venous return, which produces an erection.
The major risk factors for the development of erectile dysfunction
Causes of Erectile Dysfunction
Erectile dysfunction (ED) can have many causes, such as certain medical conditions, medications and stress. It’s important to identify the cause of erectile dysfunction and treat any underlying conditions.
Erections
When a man becomes sexually excited (aroused), his brain sends signals to the nerves in his penis. The nerves increase the blood flow to the penis, causing the tissue to expand and harden. Anything that interferes with the nervous system or the blood circulation could lead to erectile dysfunction. Anything that affects the level of sexual desire (libido) can also cause erectile dysfunction because a reduced libido makes it more difficult for the brain to trigger an erection. Psychological conditions, such as depression, can reduce libido, as can changes in hormone levels (chemicals produced by the body).
Causes
a. Psychological causes
Starting with feelings of sexual excitement, a number of things can interfere and cause or worsen erectile dysfunction like:
Relationship problems due to stress, poor communication or other concerns
b. Physical causes
The majority of these cases are secondary to diseases and disorders. These physical causes can further be classified into.
Diseases and disorders that cause erectile dysfunction are:
Heart disease
Atherosclerosis
High blood pressure
Diabetes (It is one of the major causes. 35-50% men with diabetes experience ED)
Obesity or overweight
Metabolic syndrome
Parkinson’s disease
Multiple sclerosis
Low testosterone
Peyronie’s disease (development of scar tissue inside the penis)
There are four main types of health conditions that can cause physical problems resulting in erectile dysfunction. These are:
conditions affecting the flow of blood to your penis – vasculogenic
conditions affecting your nervous system, which is made up of your brain, nerves and spinal cord – neurogenic
conditions affecting your hormone levels – hormonal
conditions affecting the physical structure of your penis – anatomical
Injuries and surgery
Penis injuries or surgical treatment of the penis, pelvis or surrounding areas can sometimes lead to erectile dysfunction. Erectile dysfunction is also thought to occur in up to 15-25% of people who experience a severe head injury.
Vasculogenic conditions
Examples of vasculogenic conditions that cause erectile dysfunction include:
Cardiovascular disease – a disease of the heart or blood vessels, such as atherosclerosis (hardening of the arteries)
High blood pressure – (hypertension)
Diabetes – a condition caused by high blood sugar levels. This can affect both the blood supply and the nerve endings in your penis, so it is also a neurogenic condition
Erectile dysfunction is strongly associated with cardiovascular disease. For this reason, it may be one of the first causes your GP considers when making a diagnosis and planning your treatment.
Neurogenic conditions
Examples of neurogenic conditions that cause erectile dysfunction include:
Multiple sclerosis – a condition that affects the body’s actions, such as movement and balance
Parkinson’s disease – a condition that affects the way that the brain coordinates body movements, including walking, talking and writing
A spinal injury or disorder
A stroke – a serious condition that occurs when the blood supply to the brain is interrupted
Hormonal Conditions
Examples of hormonal conditions that cause erectile dysfunction include:
Hypogonadism – a condition that affects the production of the male sex hormone, testosterone, causing abnormally low levels
An overactive thyroid gland (hyperthyroidism) – where too much thyroid hormone is produced
An underactive thyroid gland (hypothyroidism) – where not enough thyroid hormone is produced
Cushing’s syndrome – a condition that affects the production of a hormone called cortisol
Anatomical Conditions
Peyronie’s disease, which affects the tissue of the penis, is an example of an anatomical condition that can cause erectile dysfunction.
Medicine
In some men, certain medicines can cause erectile dysfunction, including:
Diuretics – these increase the production of urine and are often used to treat high blood pressure (hypertension), heart failure and kidney disease
Antihypertensives – such as beta-blockers, that are used to treat high blood pressure
Fibrates – medicines used to lower cholesterol levels
Antipsychotics – used to treat some mental health conditions, such as schizophrenia
Antidepressants – used to treat depression and some types of pain
Corticosteroids – medication that contains steroids, which are a type of hormone
H2-antagonists – medicines used to treat stomach ulcers
Anticonvulsants – used to treat epilepsy
Antihistamines – used to treat allergic health conditions, such as hay fever
Anti-androgens – medication that suppresses androgens (male sex hormones)
Cytotoxics – medication used in chemotherapy to prevent cancer cells from dividing and growing
Speak to your GP if you are concerned that a prescribed medicine is causing erectile dysfunction. Alternative medication may be available. However, it is important never to stop taking a prescribed medicine unless you are advised to do so by a qualified healthcare professional who is responsible for your care.
Psychological Causes
Possible psychological causes of erectile dysfunction include:
Depression – feelings of extreme sadness that last for a long time
Anxiety – a feeling of unease, such as worry or fear
Erectile dysfunction can often have both physical and psychological causes. For example, if you have diabetes, it may be difficult for you to get an erection, which may cause you to become anxious about the situation. The combination of diabetes and anxiety may lead to an episode of erectile dysfunction. There are many emotional issues that may also affect your physical ability to get or maintain an erection. These include:
Relationship problems
Lack of sexual knowledge
Past sexual problems
Past sexual abuse
Being in a new relationship
Other Causes
Certain medications (like for depression or high blood pressure)
Tobacco use
Alcoholism and other forms of substance abuse such as cocaine and heroin
Treatments for prostate cancer or enlarged prostate using hormones and allopathic drugs
Surgeries or injuries that affect the pelvic area or spinal cord
Lifestyle problems like obesity as mentioned above
Other possible causes of erectile dysfunction include:
Excessive alcohol intake
Tiredness
Using illegal drugs, such as cannabis, heroin or cocaine
Cycling
Men who cycle for more than three hours per week may be recommended to try a period without cycling to see if this helps to improve erectile dysfunction. Riding in the correct position with a properly fitted seat may also help to prevent regular cycling from leading to erectile dysfunction.
Psychological causes – (e.g. depression, anxiety, and stress involving the workplace) used to be considered some time ago as the most common reason for ED [Rx], especially in young men, but are now thought to be the primary factor in only a few cases. However, secondary psychological problems are expected in all cases associated with ED.
Vasculogenic – The most common single cause, due to low blood inflow (e.g. large vessel atherosclerosis). The incidence of ED in atheromatous aortoiliac and peripheral vascular disease is about 50%. On the other side, increased outflow, also known as a venous leak or venogenic ED, may be responsible. The venous outflow regulatory mechanism depends on the completeness of trabecular smooth muscle relaxation and the expandability of the erectile tissue, defined as the ability to achieve maximal corporal volumes at low intracavernosal pressures. Arteriogenic and venogenic ED can also coexist in the same patient.
Diabetes mellitus – is a common cause of organic ED, up to 75% of diabetic patients accusing poor erections. It is hypothesized that cavernosal artery insufficiency, corporal venoocclusive dysfunction, and/or autonomic neuropathy are the major organic pathophysiologic mechanisms leading to persistent erectile impairment in men with diabetes mellitus.
Endocrinologic disorders– are responsible for fewer than 5% of instances of ED. The etiologic significance of the hypothalamic-pituitary-testicular axis in ED is unclear. Their effect on libido and sexual behavior is well established, but the effect of androgens on normal erectile physiology is poorly understood. It has been proved that testosterone enhances sexual interest, increases the frequency of sexual acts, and increases the frequency of nocturnal erections but has little or no effect on fantasy-induced or visually stimulated erections [rx].
Hypogonadotropic hypogonadism is rare, its main characteristic being the delayed puberty;
Hypogonadotropic hypogonadism – (Klinefelter’s syndrome, surgical orchiectomy) may decrease libido while potency may persist.
Late-onset hypogonadism – may lead to ED by decreasing the hormonal levels in a patient who previously had a normal androgenic function.
Hyperprolactinemia – (pituitary adenoma, craniopharyngioma, drugs) is associated with low or low– normal levels of serum testosterone, its effects on erectile function appear to be centrally mediated. Hyperthyroidism is commonly associated with diminished libido and, less frequently with ED, while ED associated with hypothyroid states has been reported and may be secondary to associated low levels of testosterone secretion and elevated levels of prolactin.
Renal failure – Approximately 50% of dialysis-dependent uremic patients suffer from ED, but improvement after transplantation occurs in many patients mostly because of reversal of the anemia associated with chronic renal failure and improvement in uremic neuropathy. In this case, the psychogenic etiology cannot be neglected
Neurogenic – It is estimated that 10–19% of the organic ED are neurogenic [rx]. The main causes are:
intracerebral (Parkinson’s Disease, cerebrovascular disease–especially efferent pathways from the medial preoptic area may be affected in addition to higher cortical functions, affecting sexual response; other causes are: stroke, encephalitis, or temporal lobe epilepsy)
spinal cord (trauma – psychogenic erections are not possible in patients with complete lesions above T12; up to 75% of patients with multiple sclerosis have sexual disfunction; myelodysplasia).
peripheral nerves are also affected in alcoholic neuropathy, diabetic neuropathy (most common cause), after surgery (radical pelvic surgery), and trauma.
Trauma– pelvic fractures with the ruptured posterior urethra. The damage to the neurovascular bundle or to the internal pudendal or common penile artery at the time of injury is predominantly responsible for most of the ED seen following these injuries. Perineal trauma, considered as a ‘hidden’ cause of ED, is often considered to be psychogenic, but neurovascular lesions may occur. Bicycle accidents and extensive bicycle riding account for a significant portion of these blunt perineal injuries, most of them during childhood.
Penile diseases – vascular lesions in priapism, Peyronie’s disease, or other traumatic lesions of tunica albuginea or congenital deformities, can cause ED.
Malignant diseases – lower abdomen or pelvic organ malignancies may cause organic ED. However, in the vast majority of malignancies, the psychogenic etymology is considered the most important
Iatrogenic – consists in aortic or peripheral vascular surgery, renal transplantation (especially if second contralateral transplantation is performed with end–to–end hypogastric artery anastomosis), perineal irradiation (leads to fibrosis of cavernosal erectile tissue), cavernosal spongiosis shunts performed for the emergency treatment of priapism, abdominal perineal resection of the rectum, radical prostatectomy or cystoprostatectomy (the incidence of ED can be lowered to 40%–60% if nerve sparring techniques are used), transurethral sphincterotomy (should avoid incision at the 3 o’clock and 9 o’clock positions to prevent thermal injury to the cavernosal arteries). Other procedures may cause psychogenic ED.
Symptoms of Erectile Dysfunction
Symptoms of erectile dysfunction
Psychogenic
Sudden onset
Intermittent function (variability, situational)
Loss of sustaining capability
Excellent nocturnal erection
Response to phosphodiesterase type 5 inhibitors is likely to be excellent
Organic
Gradual onset
Often progressive
Consistently poor response
Erection better in standing position than lying down (in the presence of venous lear
Diagnosis of Erectile Dysfunction
Criteria Involved in Diagnoses
Ejaculatory Latency Time [ELT]
Ejaculatory Latency Time measure the time it takes for ejaculation to occur after penetration
For men with female partners, this Ejaculatory Latency Time is called Intravaginal Ejaculatory Latency Time [IELT], which measures the time it takes for ejaculation to occur after vaginal penetration.
With Premature Ejaculation, ejaculation tends to occur just on or before penetration or within 1 or 2 minutes after penetration
A man’s time to ejaculate varies throughout his life and can be influenced by various factors, such as; levels of excitement, levels of anxiety, a new partner, new sexual activity/position, level of sexual experience, the length of time from the last ejaculation, the extent of foreplay, relationship/intimacy issues.
Ejaculatory CONTROL
It is important to remember that the problem with Premature Ejaculation is more about control than duration. So it is about how much-perceived control does a man has over his ejaculation.
Men with Premature Ejaculation tend to have an inability to delay ejaculation associated with a lack of control.
The dissatisfaction of Self and/or Partner
Premature Ejaculation has negative affective consequences to either 1 or both partners. Examples of those consequences are distress, bother, frustration, sadness, anxiety, sexual dissatisfaction, etc.
Withdrawn from Partner
Premature Ejaculation can result in avoidance of intimacy/affection, sexual intimacy, and intercourse. A useful and simple way to distinguish between physiological and psychological impotence is to determine whether the patient ever has an erection. If never, the problem is likely to be physiological; if sometimes (however rarely), it could be physiological or psychological. The current diagnostic and statistical manual of mental diseases (DSM-IV) has included a listing for impotence.
Penile nerves function – Tests such as the bulbocavernosus reflex test are used to determine if there is sufficient nerve sensation in the penis. The physician squeezes the glans (head) of the penis, which immediately causes the anus to contract if nerve function is normal. A physician measures the latency between squeeze and contraction by observing the anal sphincter or by feeling it with a gloved finger inserted past the anus.
Nocturnal penile tumescence (NPT) – It is normal for a man to have five to six erections during sleep, especially during rapid eye movement (REM). Their absence may indicate a problem with nerve function or blood supply in the penis. There are two methods for measuring changes in penile rigidity and circumference during nocturnal erection: snap gauge and strain gauge. A significant proportion of men who have no sexual dysfunction nonetheless do not have regular nocturnal erections.
Penile biothesiometry – This test uses electromagnetic vibration to evaluate sensitivity and nerve function in the glans and shaft of the penis.
Dynamic infusion cavernosometry (DICC) – a technique in which fluid is pumped into the penis at a known rate and pressure. It gives a measurement of the vascular pressure in the corpus cavernosum during an erection.
Corpus cavernosometry – Cavernosography measurement of the vascular pressure in the corpus cavernosum. Saline is infused under pressure into the corpus cavernosum with a butterfly needle, and the flow rate needed to maintain an erection indicates the degree of venous leakage. The leaking veins responsible may be visualized by infusing a mixture of saline and x-ray contrast medium and performing a cavernosogram.In Digital Subtraction Angiography (DSA), the images are acquired digitally.
Magnetic resonance angiography (MRA) –This is similar to magnetic resonance imaging. Magnetic resonance angiography uses magnetic fields and radio waves to provide detailed images of the blood vessels. Doctors may inject a “contrast agent” into the patient’s bloodstream that causes vascular tissues to stand out against other tissues. The contrast agent provides for enhanced information regarding blood supply and vascular anomalies.
Specialized testing
Endocrinological tests
There is still controversy on the ideal endocrine workup for men with ED. A morning total testosterone or bioavailable testosterone is logical in men with decreased sexual interest, delayed ejaculation, reductions in ejaculate volume, failure of PDE5-inhibitor treatment, and men with ED and diabetes.
Free testosterone measurements have significant intra-assay variability which limits their clinical utility in Canada and is not recommended. Bioavailable testosterone is clinically useful and recommended, but is not available in all areas of Canada. This form of testing generally allows us to measure the sacral reflex arc, an indirect measure of perineal neural integrity, and has limited clinical availability and utility.
Duplex ultrasonography
Drawbacks of intracavernosal injection include a degree of invasiveness and ultimately a subjective evaluation of penile rigidity by the assessor. Duplex ultrasound, on the other hand, is noninvasive and provides a quantitative component to the evaluation of blood flow.
In this test, high-resolution ultrasonography and color-pulsed Doppler is used. Flow velocities are measured at the penis base, before and after vasodilator injections. In a normal Doppler study, the filling phase has characteristically high waveforms during systole and diastole.[rx]
Penile angiography
Penile angiography is a third-line study used for the evaluation of the penile vasculature. It is typically reserved for young patients with ED related to a traumatic arterial injury, or in patients with penile compression injury being considered for revascularization surgery.[rx]
In this test, the internal pudendal artery is selectively cannulated, and then radiographic contrast is injected for visualization of the internal pudendal and penile arteries. Penile vascular anatomic variations exist, making it difficult for the angiographer to determine congenital from acquired abnormalities and limiting the utility of this modality.
However, there is promise in that penile angiography could potentially serve as a diagnostic and therapeutic option in select patients. Some argue that in men with evidence of penile arterial insufficiency who have failed pharmacotherapy, contemporary endovascular treatment options may have utility.[rx] At this time, however, supportive literature is limited to case reports or small nonrandomized clinical trials.
Penile magnetic resonance imaging
Several investigational vascular studies are underway. Penile magnetic resonance imaging (MRI) has promise in detailing penile anatomy and microcirculation. The use of MRI during the work-up of prostate cancer has recently become more popular. Given the proximity of the genitals, penile anatomy and vasculature are often depicted on these imaging studies. Vargas et al.[rx] evaluated 50 prostate cancer patients who underwent an MRI pelvis for staging prior to prostatectomy.
Treatment of Erectile Dysfunction
Non-surgical therapy includes
Psychological therapy – especially sex therapy is recommended for patients with evidence of psychogenic ED and no detectable organic cause. A short course (4 to 12 weeks) of sex therapy should be prescribed. Family planning may also help fighting ED if the cause is somehow interconnected [ rx].
Lifestyle changes – when ED is linked with obesity, initial stages of diabetes mellitus, etc. There is some evidence that ED may spontaneously subside if the general health status of the patient improves.
Medication Change – if ED is caused by medications.
Herbal or vitamin supplements – are being used for centuries in treating ED, and they still have some role. Although some studies suggest that there is a high rate of placebo responders, herbal supplements are clinically proved to improve sexual function [rx].
Pelvic floor – exercises may reduce ED, although there is only limited evidence supporting that theory [rx].
Hormonal therapy – more specific testosterone replacement, is proved as very effective if the cause of ED is the low level of testosterone. Some authors suggest that the testosterone level should be checked in all patients presenting for ED [rx]. However, if low testosterone is diagnosed, further testing is necessary to rule out a metabolic syndrome. Nowadays, testosterone is available in several presentations, including patches, gels, pellet, oral pills, and buccal agents. The literature suggests that the results are similar, regardless of the way of administration. The only major issue seems to be the correct indication for testosterone suppression.
Recent evolutions developed a preparation of dihydrotestosterone, promising better results in hypogonadal men with a propensity to gynecomastia or boys with constitutionally delayed puberty [rx].
Dehydroepiandrosterone – has a controversial role in improving the treatment of ED, although some data may suggest improvement of sexual function in treated men [rx].
Human Chorionic Gonadotropin proved effective when administered to aged men with testosterone levels in the lower range of normal. The results included a decrease in fat mass, an increase in body mass, and no effect on muscle strength [rx].
Pharmacological
First-Line Therapy, are non-invasive treatments, which include:
PDE5 inhibitors, such as Viagra, Cialis, and Levitra
Androgen/Testosterone Replacement Therapy
External Devices, such as rubber rings and vacuum devices
Lifestyle modifications
Counseling/Sex Therapy
Second-Line Therapy, are injectable treatments, which include:
Penile Injection Therapy, such as Caverject
Third-Line Therapy, are surgical treatments, which include:
Penile Prosthesis
Vascular Surgery
It is important that all men receiving treatment for erectile dysfunction are supported with counseling.
Outcomes of oral PDE5 inhibitors should be characterized/stratified based on serum testosterone levels.
Additional research also is needed to characterize, in greater detail, the adverse events associated with the use of ED therapies such as their duration.
The effect of lifestyle modification on PDE5 inhibitor use should be clarified.
The cohort of patients who should not be sexually active with or without PDE5 inhibitors should be identified.
PDE11 is present in the anterior pituitary and the testes. While studies, to date, have demonstrated no effect on spermatogenesis when PDE5 inhibitors are administered daily for 6 months in healthy individuals, further assessment of the effect of PDE5 inhibitors that cross-react with PDE11 in patients with abnormal spermatogenesis is needed.
The applicability of PDE5 inhibitors after radical prostatectomy needs to be characterized.
Whether vasoactive intracavernous therapy will cause improvement in spontaneous erectile function needs to be clarified.
The role of testosterone therapy in men with sexual dysfunction with low, borderline normal, and normal testosterone levels should be better defined.
Additional randomized controlled trials of various herbal therapies are needed.
Additional prospective patient-partner satisfaction studies are needed using standardized questionnaires both pre-and post-penile prostheses implantation.
The role of prophylactic antibiotics in penile prostheses implantation and the use of impregnated prostheses needs to be studied further.
The efficacy and safety of combining pharmacotherapies and/or mechanical therapies such as oral and intrapenile vasoconstrictive therapies, PDE5 inhibitors and prostheses, or vacuum constriction and vasoconstriction devices should be explored.
Additional research also is needed to evaluate the efficacy and safety of arterial reconstruction in the treatment of ED.
No randomized controlled trial to date has addressed the particular efficacy of drugs in the management of venous-occlusive ED or defined those patients thought to have veno- occlusive dysfunction who would benefit from the surgical application.
Cost-effectiveness analyses of the fixed and unfixed costs involved with the various ED treatment modalities need to be undertaken.
Vacuum pumps
A vacuum pump consists of a clear plastic tube that is connected to a pump, which is either hand or battery operated. You place your penis in the tube and pump out all of the air. This creates a vacuum that causes the blood to fill your penis, making it erect. You then place a rubber ring around the base of your penis to keep the blood in place, allowing you to maintain an erection for around 30 minutes.
It may take several attempts to learn how to use the pump correctly, but they are usually effective. After using a vacuum pump, nine out of 10 men are able to have sex, regardless of the cause of their ED.
Alprostadil
If your erectile dysfunction doesn’t respond to treatment, or you are unable or unwilling to use PDE-5 inhibitors or a vacuum pump, you may be given a medicine called alprostadil. This is a synthetic (man-made) hormone that helps to stimulate blood flow to the penis.
Alprostadil is available as
an injection directly into your penis – this is called an intracavernosal injection
a small pellet placed inside your urethra (the tube that carries urine from your bladder to the tip of your penis) – this is called urethral application
You may be trained to correctly inject or insert alprostadil. If your partner is pregnant, use a condom during sex if you are inserting alprostadil into your urethra. Alprostadil will usually produce an erection after five to 15 minutes. How long the erection lasts will depend on the dose.
In men who did not respond to PDE-5 inhibitors, alprostadil injections were successful in 85 out of 100 men. Alprostadil inserted into the urethra is successful for up to two-thirds of men.
Hormone therapy
If a hormonal condition is causing erectile dysfunction, you may be referred to an endocrinologist (who specializes in the treatment of hormonal conditions). Hormones are chemicals produced by the body. Many hormonal conditions can be treated using injections of synthetic (man-made) hormones to restore normal hormone levels.
Testosterone
There is considerable controversy about the importance of androgens in the initiation and maintenance of erectile function, and this subject has been extensively reviewed (some of the more recent reviews include). [rx–rx] Recent studies suggest it plays a permissive role in Erectile Function.
Without adequate androgen levels expression of NOS and PDE-5 genes are altered.[rx] However, the overall consensus appears to be that testosterone plays more of a role in sexual desire, rather than a direct physiological role in ED.[rx] Therefore testosterone levels are more likely to be related to psychogenic rather than organic erectile health.
Sphingosine-1-phosphate
Sphingosine-1-phosphate (S1P) is a biologically active sphingolipid that is generated upon cell activation from membrane phospholipids as part of the sphingomyelin cycle.[rx,rx] It is stored in red blood cells and in platelets.[rx] S1P acts on five types of G-protein-coupled receptors termed S1P1-S1P5 (originally termed EDG (endothelial differentiation genes)).
Intracavernous Injection
Although long known and used since the initial demonstration of Brindley in 1983, it is in constant evolution and development. Most commonly used are papaverine (alkaloid isolated from opium), phentolamine and alprostadil (widely known as Caverject). Some authors report good results when using a combination of two or three agents [rx].
Intraurethral Therapy
Proved effective in treating ED during the last decades. The MUSE device, containing alprostadil, is the only FDA approved treatment.
Vacuum Erection Device (VED)
It is one of the most common choices of noninvasive therapy for ED. It consists of a cylindrical component and a suction device that the patient places around the penis to create negative pressure and achieve an erection. Maintenance of erection is then accomplished with an elastic constriction ring placed at the base of the penis. Patients with significant peripheral vascular disease, those receiving anticoagulants, and diabetics are generally not good candidates for the VED.
Vacuum Constriction and Erection Devices
The vacuum device is approved by the USA Food and Drug Administration (FDA) for the treatment of ED since 1982. Vacuum therapy (VT) works by creating a negative pressure environment around the penis through the use of cylindrical housing attached to a pump mechanism, which can be manually-operated or battery-operated.
The vacuum draws mixed arterial and venous blood into the corporal bodies and distends the corporal sinusoids to create an erected penis. If a pre-loaded constriction band is applied over the base of the penis to prevent the outflow of blood and maintain tumescence for intercourse, it is considered a vacuum constriction device (VCD). It is recommended that the constriction band be removed within 30 mins to return the penis to its flaccid state, as prolonged application of the constriction band can compromise both arterial and venous blood flow (rx).
Penile Vibratory Stimulation (PVS)
The penile vibratory stimulator is a battery operated device with oscillating discs that can provide excitation of afferent penile nerves at various regulated frequency and amplitudes. PVS has been utilized to activate the ejaculatory reflex for patients with spinal cord injury above T10 seeking to collect retrogradely ejaculated semen infertility treatment (rx).
The Viberect is a vibratory stimulation handheld device approved by the FDA for the treatment of ED. It is clamp-shaped with two oscillating discs facing each other near the tips, and the glans penis is placed between the two oscillating discs to receive concurrent dorsal and ventral stimulation at adjustable frequencies and amplitudes.
The use of shock wave therapy has revolutionized the treatment of many aspects of medicine. High-intensity extracorporeal shockwave therapy has been used for the treatment of nephrotic-urolithiasis while medium intensity shockwave therapy is used by orthopedic surgeons to treat joint pain as well as tendinitis. Low-intensity shockwaves therapy was first noted to improve ischemia-induced myocardial dysfunction in animal studies when low-intensity shockwaves were applied to porcine myocardium (Rx).
Papaverine
Papaverine is an opium alkaloid that acts as a non-specific PDEi that increases intracellular cAMP and cGMP leading to corporal smooth muscle relaxation (rx). Intracavernosal papaverine injection was the first clinically effective pharmacological therapy for ED and led to a full erection in at least half of the patients in early studies (rx,rx).
Alprostadil/Prostaglandin E1
Alprostadil is a potent vasodilator and smooth muscle relaxant identical to the naturally occurring PGE1. PGE1 binds with specific receptors on smooth muscle cells and activates intracellular adenylate cyclase to produce cAMP, which in turn induces tissue relaxation through a second messenger system (rx).
PGE1 is the only FDA approved form of intracavernosal therapy and is available commercially as EDEX, or Caverject. Its efficacy was demonstrated in several clinical trials where the rate of responders ranged from 40% to 80% (rx,rx). The most common adverse event is penile pain, which is not related to the injection of the medication itself. In men with prolonged use the pain is usually self-limited (rx).
Vasoactive Intestinal Peptide (VIP)
VIP is a neurotransmitter with regulatory actions on blood flow, secretion, and muscle tone with intracorporal adenylate cyclase activation and smooth muscle relaxation. VIP has been shown to elevate cAMP intracellular concentrations without affecting cGMP levels. However, when VIP is given alone it may not induce erection and requires combination with phentolamine or papaverine for it to be effective (rx).
Common associated adverse effects were facial flushing and headache. VIP in combination with phentolamine is currently being used in the UK and Europe and is seeking regulatory approval for use in the United States.
Phentolamine
Phentolamine blocks postsynaptic adrenergic α1 receptors preventing smooth muscle contraction. However, it also may interfere with prejunctional α2 receptors, which may counteract the process (rx). Consequently, this may be a reason phentolamine is not prescribed as monotherapy, and frequently is combined with papaverine, alprostadil or VIP.
Intraurethral Suppository
The use of IUS involves the placement of a prostaglandin E1-loaded pellet within the urethra before sexual intercourse. After insertion of the pellet, the patient should massage that area of the penis to help disperse the medication. The drug is absorbed through the urethra into the corpora cavernosa and increases the intracellular levels of cyclic AMP (cAMP), leading to decreased intracellular Ca2+ levels, increased smooth muscle relaxation and tumescence[rx].
Intracavernosal Injection
ICI involves the use of vasoactive substances injected directly into the corpora cavernosa via a small needle. These vasoactive agents include prostaglandin E1, papaverine and phentolamine (and sometimes atropine), which work alone or in combination to elicit an erection.
Prostaglandin E1 has been approved by the FDA as a single-agent ICI for erectile dysfunction and increases cAMP levels. Papaverine is a nonspecific phosphodiesterase inhibitor that leads to increased levels of cAMP and cGMP.
Transurethral Therapies
While limited in its utility, transurethral alprostadil (prostaglandin E1 (PGE1)) is a reasonable first-line or combination ED therapy. First brought to market in 1994 and marketed as Medicated Urethral System for Erection, transurethral alprostadil has shown limited efficacy, with response rates of 27–53 % when compared with 66–96 % for intracavernosal injected alprostadil [rx].
In addition, the formulation requires placement into the penile urethra, with penile pain in 25–43 % of patients. However, combination therapy with sildenafil has been shown to salvage the effects of MUSE® in nonresponders [rx] and is also beneficial in men whose penile nerves have been compromised as it bypasses the need for intact neurological pathways for erection.
Penile Prosthesis Implant
Penile prosthesis implant remains the most effective and permanent treatment for ED. Penile prosthesis implants can be broadly divided into malleable and inflatable prostheses (rx). A malleable penile prosthesis, also known as a semi-rigid prosthesis, does not allow for a (physiological) flaccid state of the penis.
The patient can bend the prosthesis upwards for sexual intercourse and downwards for concealment. Although the angle of prosthesis concealment has improved with recent devices, however, due to the constant rigid state of the penis, they are still less comfortable compared to their inflatable counterparts, are more likely to cause social embarrassment, and associated with a higher risk of implant erosions (rx).
Low-Intensity Shockwave Therapy
Extracorporeal low-intensity shockwave therapy (LIST) to the penis has recently emerged as a novel and promising treatment modality for ED. LIST has been previously used to treat a wide variety of urological and non-urological conditions [rx]. The mechanism of action for this treatment consists of sending acoustic waves that generate pressure impulses, which can treat patients with kidney stones, tendinitis, and peripheral vascular disease [rx].
For the treatment of ED [rx], it is hypothesized that LIST causes cell membrane microtrauma and mechanical stress, which causes an upregulation of angiogenic factors such as vascular endothelial growth factor (VEGF), NO synthase, and von Willebrand factor, which increase angiogenesis and vascularization of tissues [rx]. As such, it is postulated that LIST increases blood flow and endothelial function and results in an improvement in erectile function.
Regenerative Medicine
Following the breakthrough in ED treatment using PDE5-inhibitors, Western medicine has now moved on to a new frontier of regenerative medicine, with stem cell and gene therapy leading the way (rx). There is a practical need for novel therapy as a significant portion of diabetic or post-prostatectomy ED patients do not respond to oral pharmacotherapy.
To date, stem cells derived from different sites including adipose tissue-derived stem cells, bone marrow mesenchymal stem cells, and muscle-derived stem cells have been investigated using animal models for ED, to study their effects on neural, vascular, endothelial, or smooth muscle regeneration (rx,rx).
Gene Therapy
Gene therapy is a potential therapeutic option that is another area of investigation for the treatment of ED. Genetic material can be easily injected into the penis, which is advantageous as this direct-injection avoids potential systemic complications. Furthermore, the effects of gene therapy are more prolonged in the penis because of a slow turnover rate of the tunica albuginea [rx].
In the first human trial, Melman et al.administered a single-dose cavernosal injection of maxi-K, a ‘naked’ DNA plasmid carrying the human cDNA encoding the gene for the alpha subunit of the human smooth muscle Maxi-K channel [rx].
Stem Cell Transplant
Stem cell therapy is a new treatment option that offers the potential to reverse the underlying causes of ED and reduce patient reliance on the transitory effects of PDE5-I medications. It has been studied in several animal models in subjects who poorly respond to PDE5-Is (cavernous nerve injury and DM).
Stem cell regenerative therapy is based on the rationale that stem cells can differentiate into a wide variety of cells including endothelial cells, Schwann cells, smooth muscle cells, and neurons [rx]. In ED research, three types of stem cells are commonly used: adipose tissue-derived stem cells, bone marrow-derived stem cells, and muscle-derived stem cells.
Surgery
Surgery for erectile dysfunction is usually only recommended if all other treatment methods have failed. It may also be considered in
younger men who have experienced a serious injury to their pelvic area – for example, in a car accident
men with a significant anatomical problem with their penis
Surgical techniques used in the treatment of ED aim to restore erection by means of the intracavernous prosthesis or to cure other causes that led to ED.
Penile prostheses – are represented by several constructive models: semirigid rod, positionable, two-piece inflatable or three pieces inflatable. Although the cost and high invasiveness of the procedure may reduce its expansion in the general population, the results are generally better, in terms of erection, personal and partner satisfaction. Future evolutions will most likely try to improve the long term mechanical reliability [rx].
Vascular surgery – for ED became widespread at the end of the 1980s, but the poor long term results have somehow compromised the initial enthusiasm. The American Urological Association Guidelines still considers this type of intervention as experimental, due to the lack of consistent data and standardized procedures [rx]. The main procedures used today are penile revascularization and penile venous surgery recommended only for selected patients and offering fair long– term results.
Penile Revascularization Surgery – Approaches to penile revascularization include repair of arterial stenosis and penile venous ligation, depending on the ED etiology. Neither of these approaches, however, has a substantial evidence base, with only grade D recommendations offered in the absence of prospective, randomized studies (reviewed in [rx]). However, the consensus at this time is that penile revascularization can be offered to nonsmoking, nondiabetic men <55 years old with isolated arterial stenoses without generalized vascular disease. A consensus for penile venous ligation has not been reached, given the absence of evidentiary support.
Penile implants
Penile implants are a type of surgery that may be considered. These can be:
semi-rigid implants – which may be suitable for older men who do not have sex regularly
inflatable implants – which consist of two or three parts that can be inflated to give a more natural erection
Penile implants are not usually available on the NHS and inflatable implants may be very expensive. However, around three-quarters of men report being satisfied with the results of this type of surgery.
Psychological treatments
If your erectile dysfunction has an underlying psychological cause then you may benefit from a type of treatment called sensate focus. If conditions such as anxiety or depression are causing your erectile dysfunction, you may benefit from counseling (a talking therapy).
Sensate focus
Sensate focus is a type of sex therapy that you and your partner complete together. It starts with you both agreeing not to have sex for a number of weeks or months. During this time, you can still touch each other, but not in the genital area (or a woman’s breasts). The idea is to explore your bodies knowing that you will not have sex.
After the agreed period of time has passed, you can gradually begin touching each other’s genital areas. You can also begin to use your mouth to touch your partner, for example, licking or kissing, them. This can build up to include penetrative sex. You can find out more about sensate focus from the College of Sexual and Relationship Therapists (COSRT).
Psychosexual Counseling
Psychosexual counseling is a form of relationship therapy where you and your partner can discuss any sexual or emotional issues that may be contributing to your erectile dysfunction. By talking about the issues, you may be able to reduce any anxiety that you have and overcome your erectile dysfunction.
The counselors can also provide you with some practical advice about sex, such as how to make effective use of other treatments for erectile dysfunction to improve your sex life. For information and advice about sexual arousal, read about good sex. Psychosexual counseling may take time to work and the results achieved have been mixed.
Cognitive-behavioral therapy (CBT)
Cognitive-behavioral therapy (CBT) is another form of counseling that may be useful if you have erectile dysfunction. CBT is based on the principle that the way you feel is partly dependent on the way you think about things. CBT helps you realize that your problems are often created by your mindset. It is not the situation itself that is making you unhappy, but how you think about it and react to it.
Your CBT therapist can help you to identify any unhelpful or unrealistic thoughts that may be contributing to your erectile dysfunction – for example, to do with:
your self-esteem (the way you feel about yourself)
your sexuality
your personal relationships
Your CBT therapist will be able to help you to adopt more realistic and helpful thoughts about these issues.
Pelvic floor muscle exercises
Some studies have suggested that, in a few cases, it may be beneficial to exercise your pelvic floor muscles. These are a group of muscles around the underside of the bladder and rectum, as well as at the base of the penis. Pelvic floor muscle exercise involves strengthening and training the muscles used to control the anus (back passage) and urinate. If your GP feels this type of exercise could be beneficial, then you may want to discuss it with a physiotherapist to learn it correctly. By strengthening and training these muscles, you may be able to reduce the symptoms of erectile dysfunction.
Complementary therapies
Some complementary therapies, such as acupuncture, have claimed to treat erectile dysfunction. However, there is little evidence they are useful. In some cases, they may even include ingredients that could interact with other medications and cause side effects. Always speak to your GP before using any complementary therapies. Counseling may be required if the underlying cause of your erectile dysfunction is psychological
Natural Treatments
www.rxharun.com
You are having problems with erectile dysfunction.
You want to fix these problems naturally.
“Naturally,” means not taking any pills that are advertised in commercials along with a couple holding hands in a bathtub on the beach – what is that anyway? We’re talking about Viagra, Cialis, Levitra, and similar pills.
Fun fact about Viagra: Viagra has saved the lives of many tigers. Asian poachers harvest tiger bones and sell them for use in medicines. One function of tiger bones in medicine is curing erectile dysfunction. Since Viagra was invented, tigers have been less used for this issue. Now that you’ve learned something today, let’s get into some natural erectile dysfunction cures that don’t require taking pills.
Raise Your Testosterone
www.rxharun.com
This is VITAL to increasing your sex drive. You may be thinking, “My sex drive is strong, I just can’t fulfill the wishes caused by my sex drive.” Although normal testosterone levels are not required to maintain a normal erection, if testosterone levels dip low enough, they could be the cause of your erectile dysfunction.
You will notice as you read on in this article, that many of the natural cures for erectile dysfunction are also ways to raise your testosterone levels naturally. To read more on naturally increasing your testosterone levels, check out the TestShock program.
Exercise for Erections
www.rxharun.com
Exercise gets the blood flow moving, which is clearly important for getting blood into your nether regions. Exercise is a good way to prevent the onset of erectile dysfunction, but can also reverse the effects after you are experiencing the symptoms. It is advised to walk – not run – to get the blood flow moving.
Running lowers your testosterone levels and can raise cortisol levels and stress on your body. Weight lifting is a good way to get the blood flow moving while also raising your testosterone levels naturally. Also, moving your pelvic regions around your penis is a great way to increase continence. According to this study, doing Kegel exercises can help with erectile dysfunction.
Eat for Erections
Maintaining a healthy and balanced diet is important in reversing the effects of your erectile dysfunction. A diet rich in fruit, veggies, grains, and fish can help with the symptoms. (3)
Both exercise and diet have been proven important for preventing erectile dysfunction because studies show that a man with a 42-inch waist is 50 percent more likely to have erectile dysfunction than a man with a 32-inch waist. (4)
Stay on the Same Sleep Schedule
In a study published by Brain research in 2011, results showed that men who do not have a consistent sleep schedule have problems maintaining normal or high testosterone levels. The results also showed that hormonal depletion is a cause of sexual dysfunction.
If you do not have a bedtime, then you need to get one. Go to sleep and wake up at the same time on a consistent basis. The amount of quality sleep you get is important as well. Not sure whether or not you are getting enough sleep? A good way to know is to simply stop using an alarm.
Do a week or two of testing where you can find the amount of sleep you need so that you can wake up without an alarm every morning. This is when you know you got enough sleep in the night.
Quit Smoking
www.rxharun
Erectile dysfunction can be a result of vascular disease. The process occurs when the blood that is supposed to go to the penis is restricted due to narrowing arteries.
Not only smoking tobacco but also smokeless tobacco, can narrow the arteries and restrict the blood vessels necessary to get an erection. If you smoke, this is possibly the cause of your erectile dysfunction. If the dysfunction is bothering you, consider quitting the habit to get your erections back.
Stop Drinking So Much
www.rxharun.com
Everyone who has heard the term “Whiskey Dick” knows that alcohol can cause temporary sexual dysfunction. But alcohol is a powerful depressant and high exposure to alcohol can result in full-blown erectile dysfunction. (3)
To add to the concerns, alcohol does a great job at lowering testosterone levels. So maybe cut back on the drinks if you feel this may be the cause of your erectile dysfunction.
Check Your Medications
www.rxharun.com
Erectile dysfunction can be a common side effect of certain medications. Medications that have been known to cause erectile dysfunction are medications for high blood pressure, antidepressants, diuretics, beta-blockers, heart medications, cholesterol medications, antipsychotic drugs, hormone drugs, corticosteroids, chemotherapy, and medications for male pattern baldness.
Look up your specific medication or ask your doctor if your erectile dysfunction could be a result of the medication you are taking.
Acupuncture
www.rxharun.com
Acupuncture can be used to cure erectile dysfunction.
According to this study, acupuncture can improve the quality of your erection and it cured erectile dysfunction in 39% of its participants. In TCM, the meridian system is thought to represent a path through which the life energy qi flows and as discussed in the earlier section, the “Jing” (kidney) qi plays an important role in penile erection.
Acupuncture helps to correct the imbalances to relieve physical symptoms by stimulating various meridian points. The Shensu (BL23), Zusanli (ST36) and Neiguan (PC6) points represent important acupoints for penis stimulation and thus has a positive homeostatic effect on the autonomic nervous system, and potentially modulate NO release (rx,rx).
Ingest These Natural Remedies
www.rxharun.com
There are plenty of non-pill natural remedies you can ingest in order to cure your erectile dysfunction. Taking high doses of L-Arginine has been known to widen the blood vessels in the penis which can stimulate the blood flow and cure erectile dysfunction.
Yohimbe taken from the bark of an African tree has been known to cure erectile dysfunction. BEWARE the side effects of Yohimbe are riskier than previously mentioned remedies. This should not be used without a doctor’s supervision.
Two more untested natural remedies are ginkgo and horny goat weed. Gingko can help to increase blood flow to the penis but has no proof that it cures erectile dysfunction. Horny goat weed has been known to increase sexual performance but has not been formally tested for humans.
Drink These Juices – Pomegranate, Watermelon
www.rxharun.com
There are two juices that you can drink to help with erectile dysfunction: Watermelon and Pomegranate. A component of watermelon called citrulline, when eaten in high amounts, can increase blood flow to the penis. Although no proof exists that pomegranate juice helps with erectile dysfunction, results of a 2007 study testing the relationship were promising.
Herbal Products
Yohimbine
Yohimbine is an indole alkaloid derived from the bark of the African Yohimbe tree (rx). Yohimbine has been noted to treat fatigue, depression, diabetes, and sexual dysfunction. A meta-analysis of seven placebo-controlled trials (rx) deemed yohimbine superior to placebo for the treatment of ED with rare adverse events.
The proposed mechanism of action (rx) is via the inhibition of central alpha-2-adrenergic receptors, decreasing central inhibition of arousal, and increasing penile nerve stimulation resulting in increased NO. Common side effects include a headache, sweating, agitation, hypertension, and insomnia. Contraindications include patients on tricyclic antidepressants, anti-hypertensives, and central nervous system stimulants.
Ginseng
Ginseng is the most common ingredient among top-selling supplements for men’s sexual health (rx). The English word ginseng derives from the Chinese term tension. Ren means “person” and she means “plant root”. This plant has been named in this manner as its roots resemble the lower limbs of a human, Traditionally, ginseng has been used to restore and enhance the normal well-being of the body.
The effects are due to ginseng’s reactions with the central nervous system, metabolism, immune function, and cardiovascular system. The principal active compounds are triterpene saponins known as ginsenosides. Animal studies have suggested that specific ginsenosides may be responsible for ginseng-mediated effects on copulatory behavior (rx). Ginsenoside induces smooth muscle relaxation by hyperpolarizing the smooth muscle membrane via activation of large-conductance KCa channels (rx).
Tribulus Terrestris
Tribulus Terrestris is a dicotyledonous herbal plant of the Zygophyllaceae family, used to increase serum testosterone levels, which has only been shown in animal studies (rx). A prospective, randomized, double-blind study of 30 men showed that Tribulus Terrestris was not more effective than placebo on improving IIEF scores or serum total testosterone (rx). Two accounts of hepato-nephrotoxicity have been reported in young men who ingested high doses of this herbal medication (rx,rx).
Horny Goat Weed (Epimedium spp)
The Epimedium plant is a flowering perennial found throughout Asia and parts of the Mediterranean. Horny Goat Weed’s active ingredient is icariin, a flavonol glycoside, and reputed to improve cardiovascular function, hormone regulation, modulation of immunological function, and antitumor activity (rx).
Icariin has also been shown to have a PDE5i effect. Animal studies have been carried out showing improvements in penile hemodynamic parameters. There is one report of tachyarrhythmia and hypomania with the use of this herb (rx).
Tongkat Ali (Eurycoma longifolia Jack)
Tongkat Ali is a well-known herb in Malaysia and Singapore and is commonly used especially by the Malay ethnic group for treating diseases and enhancing general health and sexual health (rx). It is a flowering plant of the family Simaroubaceae.
Quassinoids isolated from Tongkat Ali has been reputed to be anti-tumor, anti-malarial, anti-amoebic, and anti-inflammatory. Its leaves are used for washing itches, its fruits for the treatment of dysentery, its bark used as a vermifuge, the taproots used for the treatment of hypertension, and the root bark for treatment of diarrhea and fever.
The roots extracts are used for sexual dysfunction, aging, malaria, cancer, diabetes, anxiety, aches, constipation, exercise recovery, fever, increased energy, increased strength, leukemia, osteoporosis, stress, and syphilis. Animal studies done on middle age sex rats showed enhancement of the sexual qualities in terms of hesitation time among middle-aged rats (rx).
Ginkgo Biloba
Ginkgo Biloba is promoted to treat conditions ranging from hypertension to Alzheimer’s dementia. There is evidence that shows an improvement of memory enhancements in the geriatric population (rx), improvement in terms of cognitive function via an effect on cerebral vasculature (rx), improvement of claudication distance, and cutaneous ulcers in patients with peripheral vascular disease (rx).
Ginkgo Biloba extract is proposed to induce NO in endothelial cells and thus causing relaxation of vascular smooth muscles. Animal studies have reported relaxation of rabbit corpus cavernosal smooth muscle cells with the use of Ginkgo Biloba (rx). Adverse effects include headaches, major bleeding (in a patient who is taking warfarin concurrently), and seizures with reported fatality (rx).
Physical Exercise
Low levels of physical exercise can be associated with ejaculatory and erectile disorders. And higher levels of physical exercise have been shown to improve erectile function in hypogonadal men undergoing testosterone replacement therapy (rx). There are, however, no proven physical exercises that can improve erections directly.
Jelqing Exercise
Jelqing is a penile massage technique of ancient Arabic origin (rx). Men who practice jelqing will stretch their penises while in a semi-erected state and repeatedly milk their penises from base to glans, with their thumb and index finger touching to form an “OK” hand sign around their penile shaft.
This massage can be done daily with the aim to achieve greater penile length and harder erections. Unwanted side effects of bruising, pain, and fibrosis had been reported. No studies have been done to evaluate the efficacy of jelqing objectively.
Qigong
Qigong is a form of breathing exercise commonly practiced in Asia to maintain health (rx). In a cross-sectional population-based comparison study in Taiwan, individuals practicing Qigong demonstrate higher SF-36 scores in the domains of physical functioning, role limitations due to physical problems, bodily pain, general health, and vitality (rx). Techniques to concentrate the energy or qi in the pelvis or genitals are regularly practiced, but the effects of Qigong on ED have not been studied.
Homeopathy Medicines for Erectile Dysfunction
These are some of the many homeopathic remedies which cater to relieve ED specifically.
Agnus castus – This remedy may be helpful if problems with impotence develop after a man has led a life of intense and frequent sexual activity for many years. A cold sensation felt in the genitals is a strong indication for the Agnus castus. People who need this remedy are often very anxious about their health and loss of abilities and may have problems with memory and concentration.
Argentum nitricum – This remedy may be helpful if a man’s erection fails when sexual intercourse is attempted, especially if thinking about the problem makes it worse. People who need this remedy are often nervous and imaginative. A person who needs Argentum nitricum is usually warm-blooded, with cravings for both sweets and salt.
Caladium – This remedy may be helpful to a man whose genitals are completely limp, despite having sexual interest. Nocturnal emissions can occur without an erection, even if dreams are not sex-related. A person who needs this remedy often craves tobacco.
Causticum – This remedy may be indicated if physical pleasure during sex has diminished and sexual urges are reduced. The person feels tired and weak and may experience memory loss, with a compulsive need to check things (to see that doors are locked, etc.) Prostate problems may be associated with impotence, and urine may be lost when the person coughs or sneezes.
Lycopodium – commonly called club moss, is a wonderful homeopathic remedy.
People who need this remedy may have problems with erections because of worry, and can also be troubled by memory loss. They often lack self-confidence (though some may overcompensate by acting egoistically). People who need this remedy often have digestive problems with gas and bloating, and an energy slump in the late afternoon and evening.
Selenium metallicum – Selenium is a nutrient needed by humans in micro amounts. It is widely distributed in nature. Brazilian nuts, sea-foods, yeast, whole grains are all excellent sources of selenium. A homeopathic remedy is highly potent and has a wide curative spectrum for disorders like impotency, chronic fatigue syndrome, sterility, depression, etc.
This remedy is often helpful to men who have diminished sexual ability, especially if the problem starts after a fever or exhausting illness. The person feels weak and exhausted, but interest is usually still present. Erection is slow, insufficient, weak, and has involuntary seminal emissions. Unusual hair-loss (body hair or eyebrows) can also suggest a need for Selenium.
Staphysagria – Staphysagria is a homeopathic remedy made from the seeds of the Delphinium Staphisagria, which has lovely purple-blue flowers, and in its raw form is highly poisonous, historically used to kill vermin. The homeopathic remedy, through its preparation, is no longer toxic yet remains extremely powerful.
Stretching is a form of physical exercise in which a specific muscle or tendon (or muscle group) is deliberately flexed or stretched in order to improve the muscle’s felt elasticity and achieve comfortable muscle tone. The result is a feeling of increased muscle control, flexibility, and range of motion. Stretching is also used therapeutically to alleviate cramps.
Stretching is a common activity used by athletes, older adults, rehabilitation patients, and anyone participating in a fitness program. While the benefits of stretching are known, controversy remains about the best type of stretching for a particular goal or outcome. The purpose of this clinical commentary is to discuss the current concepts of muscle stretching interventions and summarize the evidence related to stretching as used in both exercise and rehabilitation.
Increasing flexibility through stretching is one of the basic tenets of physical fitness. It is common for athletes to stretch before (for warming up) and after exercise in an attempt to reduce the risk of injury and increase performance, though these practices are not always based on scientific evidence of effectiveness.
Stretching before playing
A series of exercise routines you can do to help reduce any pain, including tension, stiffness, and soreness.
These exercises from physiotherapist and BackCare expert Nick Sinfield help to stretch, strengthen and mobilize the lower back.
When starting out, go gently to get used to the movements and work out how far you can go into each position without feeling pain. Aim to do this routine at least once a day if the pain allows. You can complement this routine with walking, cycling and water-based activities.
You are advised to seek medical advice before starting these back pain exercises, and to stop immediately if you feel any pain.
Stretching exercises should form an integral part of any conditioning program. Performed consistnetly, the stretching exercises below can help to do the following…
Increase the range of motion about a joint reducing the risk of muscle and tendon tears during competitive activity.
Relieve muscle tightness and stiffness.
Improve postural imbalances and help to reduce chronic back pain.
Increase localized blood flow to the muscles being stretched.
Possibly relieve muscle soreness after intense physical activity and help to reduce the severity of DOMS (dleayed Onset Muscle Sorness).
STRETCHING EXERCISES
Stretches for the side of neck
Sit or stand with arms hanging loosely at sides
Turn head to one side, then the other
Hold for 5 seconds, each side
Repeat 1 to 3 times
Stretches side of the neck
Sit or stand with arms hanging loosely at sides
Tilt head sideways, first one side then the other
Hold for 5 seconds
Repeat 1-3 times
Stretches back of the neck
Sit or stand with arms hanging loosely at sides
Gently tilt head forward to stretch back of the neck
Hold 5 seconds
Repeat 1-3 times
Stretches side of shoulder and back of the upper arm
Stand or sit and place right hand on left shoulder
With left hand, pull right elbow across chest toward left shoulder and hold 10 to 15 seconds
Pull elbow behind head gently as you slowly lean to side until a mild stretch is felt
Hold 10 to 15 sec
Repeat on another side
Stretches middle back
Stand with hands on hips
Gently twist torso at the waist until a stretch is felt
Hold 10 to 15 sec
Repeat on another side
Keep knees slightly flexed
Stretches ankles
Stand and hold onto something for balance
Lift right foot and rotate foot and ankle 8 to 10 times clockwise, then 8 to 10 times counterclockwise.
Repeat on another side
(Note: can also be done sitting)
Stretches calf
Stand a little way from the wall and lean on it with forearms, head resting on hands
Place right foot in front of you, leg bent left leg straight behind you
Slowly move hips forward until you feel stretch in the calf of left leg
Keep left heel flat and toes pointed straight ahead
Hold easy stretch 10 to 20 seconds
Do not bounce
Repeat on another side
Do not hold breath
Stretches front on the thigh (quadriceps)
Stand a little away from the wall and place left hand on the wall for support
Standing straight, grasp the top of the left foot with right hand
Pull heel toward buttock
hold 10 to 20 sec
Repeat on another side
Relaxes hamstrings stretch calves, Achilles, and ankles
Stand with feet shoulder-width apart
Keep heels flat, toes pointed straight ahead
Assume bent knee position (quarter squat)
Hold 30 sec
Stretches inner thigh, groin
Stand with feet pointed straight ahead, a little more than shoulder-width apart
Bend right knee slightly and move left hip downward toward right knee
Hold 10 to 15 seconds
Repeat on another side
If necessary, hold on to something (chair, etc.) for balance
Stretches side of hip, hamstrings
Sit on the floor with right leg straight out in front
Bend left leg, cross left foot over, place outside right knee
Pull left knee across body toward the opposite shoulder
Hold 10 to 20 seconds
Repeat on another side
Breathe easily
Stretches lower back, side of hip, and neck
Sit on the floor with left leg straight out in front
Bend right leg, cross right foot over, place outside left knee
Bend left elbow and rest it outside right knee
Place right hand behind hips on the floor
Turn head over right shoulder, rotate upper body right
Hold 10 to 15 seconds
Repeat on another side
Breathe in slowly
Stretches back of the leg and lower back
Sit on the floor, legs straight out at sides
Bend left leg in at the knee
Slowly bend forward from hips toward the foot of straight leg until you feel a slight stretch
Do no dip head forward at the start of a stretch
Hold this developmental stretch 10 to 20 seconds
Repeat on other side
Foot of straight leg upright, ankles and toes relaxed
Use a towel if you cannot easily reach your feet
Stretches shoulders, arms, hands, feet, and ankles
Lie on floor, extend arms overhead, keep legs straight
Reach arms and legs in opposite directions
Stretch 5 sec, relax
Bottom to heels stretching
A series of exercise routines you can do to help reduce any lower back pain (occasionally referred to as low back pain), including tension, stiffness and soreness.
These exercises from physiotherapist and BackCare expert Nick Sinfield help to stretch, strengthen and mobilize the lower back.
When starting out, go gently to get used to the movements and work out how far you can go into each position without feeling pain.
Aim to do this routine at least once a day if the pain allows. You can complement this routine with walking, cycling, and water-based activities.
You are advised to seek medical advice before starting these back pain exercises and to stop immediately if you feel any pain.
Bottom to heels stretch
Stretches and mobilizes the spine
Start position: Kneel on all fours, with your knees under hips and hands under shoulders. Don’t over-arch your lower back. Keep your neck long, your shoulders back and don’t lock your elbows.
Action: Slowly take your bottom backward, maintaining the natural curve in the spine. Hold the stretch for one deep breath and return to the starting position.
Repeat 8 to 10 times.
Tips:
Avoid sitting back on your heels if you have a knee problem.
Ensure correct positioning with the help of a mirror.
Only stretch as far as feels comfortable.
Knee rolls
Stretches and mobilises the spine
Start position: Lie on your back. Place a small flat cushion or book under your head. Keep your knees bent and together. Keep your upper body relaxed and your chin gently tucked in.
Action: Roll your knees to one side, followed by your pelvis, keeping both shoulders on the floor. Hold the stretch for one deep breath and return to the starting position.
Repeat 8 to 10 times, alternating sides.
Tips:
Only move as far as feels comfortable.
Place a pillow between your knees for comfort.
Back extensions
Stretches and mobilizes the spine backward
Start position: Lie on your stomach, and prop yourself on your elbows, lengthening your spine. Keep your shoulders back and neck long.
Action: Keeping your neck long, arch your back up by pushing down on your hands. You should feel a gentle stretch in the stomach muscles as you arch backward. Breathe and hold for 5 to 10 seconds. Return to the starting position.
Repeat 8 to 10 times.
Tips:
Don’t bend your neck backwards.
Keep your hips grounded.
Deep abdominal strengthening
Strengthens the deep supporting muscles around the spine
Start position: Lie on your back. Place a small, flat cushion or book under your head. Bend your knees and keep your feet straight and hip-width apart. Keep your upper body relaxed and your chin gently tucked in.
Action: As you breathe out, draw up the muscles of your pelvis and lower abdominals, as though you were doing up an imaginary zip along your stomach. Hold this gentle contraction while breathing from your abdomen for 5 to 10 breaths, and relax.
Repeat 5 times.
Tips:
This is a slow, gentle tightening of the lower abdominal region. Don’t pull these muscles in using more than 25% of your maximum strength.
Make sure you don’t tense up through the neck, shoulders or legs.
Pelvic Tilts
Stretches and strengthens the lower back
Start position: Lie on your back. Place a small, flat cushion or book under your head. Bend your knees and keep your feet straight and hip-width apart. Keep your upper body relaxed and your chin gently tucked in.
Action: Gently flatten your low back into the floor and contract your stomach muscles. Now tilt your pelvis towards your heels until you feel a gentle arch in your lower back, feeling your back muscles contracting and return to the starting position.
Repeat 10 to 15 times, tilting your pelvis back and forth in a slow rocking motion.
Tips:
Keep your deep abdominals working throughout.
Don’t press down through the neck, shoulders or feet.
Modification Place one hand on your stomach and the other under your lower back to feel the correct muscles working
Torticollis is involuntary tonic contractions or intermittent spasms of neck muscles causing the neck to turn from its usual position. It can be present at birth (congenital), inherited or develop as a result of damage to the nervous system or muscles. Torticollis with recurrent, but transient contraction of the muscles of the neck and especially of the sternocleidomastoid, is called spasmodic torticollis.
Torticollis refers to a twisting of the head and neck caused by a shortened sternocleidomastoid muscle, tipping the head toward the shortened muscle, while rotating the chin in the opposite direction. Torticollis is seen at all ages, from newborns to adults. It can be congenital or postnatally acquired. In this review, we offer a new classification of torticollis, based on its dynamic qualities and pathogenesis. All torticollis can be classified as either nonparoxysmal (nondynamic) or paroxysmal (dynamic). Causes of nonparoxysmal torticollis include congenital muscular; osseous; central nervous system/peripheral nervous system; ocular; and nonmuscular, soft tissue. Causes of paroxysmal torticollis are benign paroxysmal; spasmodic (cervical dystonia); Sandifer syndrome; drugs; increased intracranial pressure; and conversion disorder. The description, epidemiology, clinical presentation, evaluation, treatment, and prognosis of the most clinically significant types of torticollis follow.
Alternative Names
Spasmodic torticollis; Wry neck; Loxia; Cervical Dystonia. Synonyms are “intermittent torticollis”, “cervical dystonia” or “idiopathic cervical dystonia”, depending on the cause.
Types of torticollis
Aetiological Types of Torticollis
Torticollis classifies into several types:
Congenital torticollis – During gestation or birth, trauma can occur that causes edema in the muscle, which can generate congenital fibrosis of the sternocleidomastoid muscle, causing a shortening of the fibers of this muscle.
Congenital muscular torticollis –The cause of congenital muscular torticollis is unclear. Birth trauma or intrauterine malposition is considered to be the cause of damage to the sternocleidomastoid muscle in the neck. Other alterations to the muscle tissue arise from repetitive microtrauma within the womb or a sudden change in the calcium concentration in the body which causes a prolonged period of muscle contraction.
Dermatogenic pain – When there is an injury to the skin of the neck, and it shortens, this can lead to a limitation in movement, usually occurring in cases of burns or scars.
Ocular torticollis – This refers to the paralysis of muscles involved with the inclination and rotation of the head (compensation) from the involvement of the oblique extraocular muscles.
Rheumatological torticollis – This variant is secondary to various rheumatologic diseases.
Torcicolo vestibular – Inner ear responsible for the balance, involving the labyrinth of the inner ear.
Neurogenic tormentor – This results from any neurological disorder or accident, such as stroke or trauma.
Spasmodic torticollis (dystonia) – this is the most common cause of neck rigidity. This type results from increased muscle tone. The most common triggering factors include emotional stress, physical overload or sudden movement.
Experimental models of torticollis show that torticollis can result from both local factors and central nervous system disorders.[rx][rx][rx][rx]
Temporary torticollis
This type of wry neck usually disappears after one or two days. It can be due to:
Swollen lymph nodes
Ear infection and cold
an injury to your head and neck that causes swelling
Fixed torticollis – Fixed torticollis is also called acute torticollis or permanent torticollis. It’s usually due to a problem with the muscular or bony structure.
Muscular torticollis – This is the most common type of fixed torticollis. It results from scarring or tight muscles on one side of the neck.
Klippel-Feil syndrome – This is a rare, congenital form of wry neck. It occurs when the bones in your baby’s neck form incorrectly, notably due to two neck vertebrae being fused together. Children born with this condition may have difficulty with hearing and vision.
Cervical dystonia – This rare disorder is sometimes referred to as spasmodic torticollis. It causes neck muscles to contract in spasms. If you have cervical dystonia, your head twists or turns painfully to one side. It may also tilt forward or backward. Cervical dystonia sometimes goes away without treatment. However, there’s a risk of recurrence.
Acquired torticollis
Noncongenital muscular torticollis may result from scarring or disease of cervical vertebrae, adenitis, tonsillitis, rheumatism, enlarged cervical glands, retropharyngeal abscess, or cerebellar tumors. It may be spasmodic (clonic) or permanent (tonic). The latter type may be due to Pott’s Disease (tuberculosis of the spine).
Spasmodic torticollis – A self-limiting spontaneously occurring form of torticollis with one or more painful neck muscles is by far the most common (‘stiff neck’) and will pass spontaneously in 1–4 weeks. Usually, the sternocleidomastoid muscle or the trapezius muscle is involved. Sometimes draughts, colds, or unusual postures are implicated; however, in many cases, no clear cause is found. These episodes are commonly seen by physicians.
Tumors of the skull base (posterior fossa tumors) can compress the nerve supply to the neck and cause torticollis, and these problems must be treated surgically.
Infections in the posterior pharynx can irritate the nerves supplying the neck muscles and cause torticollis, and these infections may be treated with antibiotics if they are not too severe but could require surgical debridement in intractable cases.
Ear infections and surgical removal of the adenoids can cause an entity known as Grisel’s syndrome, a subluxation of the upper cervical joints, mostly the atlantoaxial joint, due to inflammatory laxity of the ligaments caused by an infection. This bridge must either be broken through manipulation of the neck or, surgically resected.
The use of certain drugs, such as antipsychotics, can cause torticollis.
Antiemetics – Neuroleptic Class – Phenothiazines
There are many other rare causes of torticollis. A very rare cause of acquired torticollis is fibrodysplasia ossificans progressiva (FOP), the hallmark of which is malformed great toes.
Trochlear torticollis
Torticollis may be unrelated to the sternocleidomastoid muscle, instead caused by damage to the trochlear nerve (fourth cranial nerve), which supplies the superior oblique muscle of the eye. The superior oblique muscle is involved in depression, abduction, and intorsion of the eye. When the trochlear nerve is damaged, the eye is extorted because the superior oblique is not functioning.
Synostosis of a hemicoronal or hemilambdoid suture associated at least with synostosis of another suture of the cranial vault
Category IV
Synostosis of a hemicoronal or hemilambdoid suture associated at least with synostosis of another suture of the cranial vault, with cranial base involving malformation (prolapse, asymmetry)
Category V
Secondary or consequent to metabolic disorders, blood disease (sick-cell anaemia, thalassaemia, polycythaemia vera, vitamin D deficiency, mucopolysaccharidosis)
Deformation/non synostotic plagiocephaly
Category VI
Secondary forms without craniosynostosis, consequent on extrinsic factors or brain anomalies; cranial base involving malformations (prolapse or asymmetry) without craniosynostosis, congenital torticollis
Causes of Torticollis
Because there are different types of torticollis, it is important to know the root cause so that your child can get the proper care and treatment as quickly as possible.
Causes of congenital muscular torticollis
For children with congenital muscular torticollis, the most common form of pediatric torticollis, the sternocleidomastoid (SCM) muscle becomes shortened and contracted. The SCM muscle runs along each side of the neck and controls how the head moves — side to side, and up and down.
There are a few common reasons why the SCM muscle may have become contracted and cause your child’s head to tilt to one side:
The way your baby was positioned in the womb before birth
Abnormal development of the SCM muscle
Trauma or damage to the muscle during birth
congenital bony abnormalities of the upper cervical spine, with subluxation (abnormal rotation) of the C1 vertebrae over the C2 vertebrae in the cervical spine (the part of the spine that encompasses the neck).
congenital bony abnormalities of the upper cervical spine, which are most often associated with other congenital skeletal anomalies, such as:
shortened neck
short limbs (arms and legs)
dwarfism
congenital webs of skin running along the side of the neck
Klippel-Feil syndrome, a rare birth defect that causes some of the neck vertebrae to fuse together
achondroplasia, a bone growth disorder
multiple epiphyseal dysplasias, a disease that affects the development of bone and cartilage in the long bones of the arms and legs
Morquio’s syndrome, an inherited metabolic disorder that prevents the body from breaking down sugar molecules
Causes of acquired torticollis
For children who have acquired torticollis, the causes vary widely and range in severity from benign (not serious) to very serious. Some causes of acquired torticollis include:
a mild (usually viral) infection.
Infection
Head and neck (URTI, otitis media, mastoiditis, cervical adenitis, retropharyngeal abscess)
Respiratory and soft-tissue infections of the neck
Abnormalities in the cervical spine (such as atlantoaxial subluxation)
Vision problems (called ocular torticollis)
Abnormal reaction to certain medications (called a dystonic reaction)
Spasmus nutans (a usually benign condition that causes head bobbing along with uncontrolled eye movements)
Sandifer syndrome (a rare condition combining gastroesophageal reflux with spasms in the neck)
Sleeping in an awkward position
Neck muscle injury at birth
Burn injury
Any injury that causes heavy scarring and skin or muscle shrinkage
Neck muscle spasm
Atlantoaxial rotary fixation > Trauma and ligamentous laxity (eg as part of underlying disorders)
Pharyngeal infection (Grisel syndrome)
Inflammation eg: Juvenile idiopathic arthritis
Neoplasm >CNS tumors & Bone tumors
Dystonic syndromes (idiopathic spasmodic torticollis, drug reactions)
Ocular dysfunction
Torticollis may also be a secondary condition that results from the following
Slipped facets (two small joints on the side of the spine)
Herniated disk
Viral or bacterial infection
There are three distinct varieties of Spasmodic Torticollis
Tonic, in which the head turns to one side,
Clonic, which involves the shaking of the head, and
Mixed which involves both turning and shaking. The turning of the head is generally considered to fall into one of four categories
Rotational, in which the head turns to one side or the other
Laterocollis in which the head is pulled toward the shoulder
Retrocollis in which the head is pulled to the back, or
Anterocollis in which the head is pulled forward.
Symptoms of Torticollis
Symptoms of congenital muscular torticollis
The child has a limited range of motion in the head and neck.
The head tilts to one side while the chin tilts to the other.
A small, pea-sized lump (or “pseudo tumor”) is sometimes found on the sternocleidomastoid (SCM) muscle.
Asymmetries of the head and face, indicating plagiocephaly, may also be present.
Musculoskeletal problems, such as hip dysplasia, are sometimes present.
Symptoms of acquired torticollis
There is a limited range of motion in the head and neck.
The head tilts to one side while the chin tilts to the other.
With a condition called benign paroxysmal torticollis, there may be recurrent episodes, or “attacks,” of head tilting; often these attacks are accompanied by other symptoms, such as vomiting, irritability and/or drowsiness.
Additional symptoms vary according to the cause of the torticollis.
In addition, children who develop painful torticollis at the same time as a fever that is caused by an infection in the pharynx (cavity behind the nose, mouth, and larynx) or retropharyngeal space (the area behind the pharynx) need to see a doctor immediately. If left untreated, these complications can lead to a rare disorder called Grisel’s syndrome.
Time course – (Uncomplicated acute torticollis should resolve within 7 – 10 days without complication.)
Awkward position pre-symptoms, particularly if recent symptoms.
Medications associated with acute dystonic reactions e.g. metoclopramide.
Neuro – a headache, strabismus, diplopia
Examination
Assess for midline tenderness, general neck palpation and attempt active ROM.
Congenital muscular: palpate for sternocleidomastoid pseudotumor, head shape (plagiocephaly), hip examination.
Location of tenderness may assist with diagnosis, however deep pathology (eg: infection) may have no external signs.
Neurologic examination.
Eye examination
ENT examination including lymph nodes
In reviewing the history of present illness, identifying the characteristics of the torticollis is vital to determine an etiology. Important aspects include:
Symptoms associated with torticollis (vomiting, fever or signs of infection, gait disturbances, balance problems, associated headaches, and vision changes)
Emotional state
Personal and family context when torticollis occurs in the neonatal period (birth details, the course of the neonatal period, known pathology such as chromosomal alterations, systemic disease, visceral or skeletal malformations, muscle fibrosis, strabismus
Acute or chronic duration
Underlying associated pathologic medical conditions
Permanent versus transient or paroxysmal symptoms
Recent changes in medication
Age of onset of the initial episode
The age of onset of torticollis makes it possible to immediately distinguish between congenital torticollis (present at birth or during the neonatal period) from acquired torticollis, which would present later in life
Events leading up to the episode of torticollis (such as recent trauma
Determining if the torticollis is painful or non-painful is crucial
Pain present may be bony, central, muscular, or from previous radiation
The physical exam is also important in diagnosing torticollis. Areas of focus include[rx][rx][rx]:
The patient’s posture
Constant or intermittent head tilt
Presence of any limitation of movement as well as any relieving factors
Bony or muscular tenderness to palpation
The diagnosis of torticollis is straightforward in the typical form with lateral tilt and contralateral neck rotation, but if the patient presents in spine immobilization by EMS, a rigid form of the head, the inclination or rotation of the head may be isolated.[rx][rx][rx]
Differential diagnosis of torticollis
Non-osseous:
Muscular
Ocular (muscle palsy)
Neurogenic tumours:
Cerebellar
Spinal cord
Syndromal:
Sandifer syndrome (torticollis and gastro-oesophageal reflux)
Spasmodic
Neurological (brachial plexus injury)
Osseous:
Congenital cervical spine malformations:
Occipitocervical invagination,
Atlas malformation
Klippel–Feil syndrome
Rotatory fixation (C1–C2):
Trauma
Respiratory tract infection
Cervical adenitis
Investigation
Consider
Cervical Spine xray – particularly if there is cervical spine tenderness, severe pain, persistent symptoms (≥1 week), limitation ROM.
Ultrasound – if a mass is palpated or collection suspected. May also be helpful to confirm the fibrous SCM in congenital muscular torticollis.
CT neck and/or the brain if
Associated neurology symptoms,
Severe pain
Bone anomaly suspected clinically or abnormal cervical xray.
There is suspicion of a retropharyngeal abscess.
X-ray of the neck
CT scan of the neck
Electromyogram (EMG) to see which muscles are most affected
MRI of the brain
Blood tests to look for medical conditions that are linked to torticollis
Depending on the presentation, consultation with, General Medicine, Orthopaedics, ENT, Ophthalmology or Neurology will help with decisions about imaging.
Selected Differential Diagnosis of Torticollis in Infants
CONDITION
CHARACTERISTICS
Benign, paroxysmal torticollis
Recurrent episodes of head tilting, usually accompanied by vomiting, pallor, irritability, ataxia, and drowsiness
Congenital muscular torticollis
Tightness and thickening of the sternocleido-mastoid muscle, with or without a muscle tumor
Neurogenic torticollis
An acute episode of torticollis that usually occurs in older children with neurologic abnormalities
Osseous torticollis
Congenital cervical spine malformations
Postural torticollis
No tightness or tumor of the sternocleidomastoid muscle
Treatment of Torticollis
Acute management
Management depends on the suspected cause:
Stabilization may be required.
Infectious cause: appropriate antibiotic therapy e.g. iv Timentin. Refer to ENT if a retropharyngeal or parapharyngeal abscess is suspected.
Atlantoaxial rotatory fixation: Rest, use of an Aspen collar.
Injury or congenital bony cause: refer Orthopaedics.
Congenital muscular torticollis – refer to community physiotherapy for education and stretching exercises. Severe cases persistent greater than 12 months warrant a surgical opinion.
Conservative approaches are usually employed initially among all patients. These include:
Passive stretching and positioning – This treatment option is used among infants and children wherein there are no chronic spasms in the muscles. The aim of this treatment is to stretch the shortened neck muscles in younger children. This treatment often corrects the tilted neck when it is started within 3 months of birth. For adults, stretching exercises can be passively or actively done with the assistance of physical therapy.
Use of neck braces – Neck braces may also be used among patients to support the neck and promote the normal anatomic position of the cervical spine and prevent further lateral flexion contracture.
Traction – Traction is also employed to some patients to create a tension that will pull the head to the opposite side. Traction is carefully used to prevent nerve damages on the neck as a result of too heavyweight or incorrect positioning of the traction device.
Application of heat and massage
For temporary relief of neck pain, heat application and massage help relax the spastic muscles for pain relief.
Medication use
Dystonic reactions: Benztropine
Analgesia or anti-inflammatory medications may be effective.
Heat packs and massage may provide symptomatic relief in cases of wry neck.
Diazepam can be effective with some cases of spasm of the SCM…
Taking medicines such as baclofen to reduce neck muscle contractions.
Injecting botulinum.
Trigger point injections to relieve pain at a particular point.
Surgery of the spine might be needed when the torticollis is due to dislocated vertebrae. In some cases, surgery involves destroying some of the nerves in the neck muscles or using brain stimulation.
Physiotherapy
Physiotherapy is a first-line treatment and is warranted in all infants with CMT with or without positional plagiocephaly. One evidence-based clinical practice guideline on physical therapy management in CMT has been published.
The majority of published studies use a combination of physiotherapy and home programme completed by the carers. Evidence has shown full recovery in 70% of subjects by 12 months of age, with 7% requiring surgery. Education of carers to use their daily routines of carrying, positioning, and feeding to accomplish the desired postures is important.
In addition to massage and myofascial release performed by physiotherapists, physiotherapy and a home programme can include the following:
Gentle stretching using carrying and play techniques to promote active neck rotation towards the affected side and discourage tilting of the head towards the affected side.
Turning the head of the infant while sleeping supine to encourage rotation to the non-favored side.
Encouraging head rotation to the side of the affected muscle by arranging the environment with visually stimulating items on that side or changing the crib orientation if necessary.
Strengthening the contralateral neck muscles by carrying the infant with his/her body tilted to the affected side, practicing assisted rolling to the contralateral side, or side-lying on the affected side (these activities use the head righting response to strengthen the weak contralateral side).
Alternating carrying and feeding positions.
Encouraging mid-line head position in infant carriers with the use of rolled towels.
Prone time to play several times a day (newborns often tolerate a more inclined position). This position also facilitates bilateral sternocleidomastoid (SCM) elongation.
Complementary or Supportive Treatments are Available for Cervical Dystonia or Spasmodic Torticollis?
Below is a mention of some of the supportive or complementary treatments for cervical dystonia or spasmodic torticollis
Cranial molding orthosis – This is used for moderate to severe plagiocephaly, which is often associated with CMT. As the skull grows the fastest and is most malleable in the first year of life, the optimal response is obtained if used between 4 and 12 months of age. The orthosis is worn 23 hours a day, and treatment duration is usually 3 to 4 months. It is then adjusted upon receipt every 2 to 3 weeks. Use of a cranial molding orthosis can indirectly improve head position in CMT as it provides asymmetric surface when lying supine, thus removing the gravitational forces that promote turning of the head toward the flattened occiput. Evidence shows a statistically significant improvement in infants treated with a molding orthosis. Evidence One systematic review showed considerable evidence that molding therapy may reduce skull asymmetry more effectively than repositioning therapy.
OnabotulinumtoxinA (botulinum toxin type A) – Injections are performed in children with CMT who are unresponsive to physical therapy and a home program. They may also help avoid the need for surgical release and can be repeated in 3 months if deficits persist. OnabotulinumtoxinA, a neurotoxin derived from the bacteria Clostridium botulinum, produces a protein that inhibits release of acetylcholine and results in localized reduction in muscle activity. The goal is to temporarily weaken the affected SCM or upper trapezius muscle, resulting in an easier and more successful stretching program as well as an improved ability to strengthen the contralateral neck musculature. It has been shown to be safe and effective in the treatment of cervical dystonia in adults and has been used safely in children with limb spasticity for many years.
Acupuncture for Cervical Dystonia or Spasmodic Torticollis
Acupuncture is the traditional Chinese alternate therapy of medication where the principles of medicine are based on the anatomy, pathology, and physiology of the body. It is a natural way of stimulating the nerves present in the skin. It also stimulates the muscles and tissues with various effects. Acupressure therapy of medication can replace the botox injections treatment used for cervical dystonia or spasmodic torticollis to a great extent. It has effectively treated cervical dystonia or spasmodic torticollis and is recommended worldwide. It reduces the side effects of Botox and is an entirely an organic procedure.
Reflexology for Cervical Dystonia or Spasmodic Torticollis
This is another supportive treatment of cervical dystonia or spasmodic torticollis where the feet and hands are pressurized. The pressure creates an effect in the entire body. The patient is made to felt certain tension in the limbs which brings a pleasant relief. This therapy is also used in general pain, anxiety or depression commonly seen in cervical dystonia or spasmodic torticollis.
Hypnosis for Cervical Dystonia or Spasmodic Torticollis
This is a psychological therapy which brings certain positive changes to the mind as well as the body of the patient. The therapist hypnotizes the patient and offers her deep relaxation. The inner focus of the patient is thus enhanced and the pain is reduced effectively. Other pain, anxiety or depression can also be treated with this mental exercise. Several successful cases of cervical dystonia or spasmodic torticollishave been registered under hypnosis. People are becoming more aware of this therapy with the number of successful cases around the world.
Meditation or Autogenic Training as a Complementary Therapy for Cervical Dystonia Or Spasmodic Torticollis
Autogenic training is a highly structured type of meditation and is a greatly accepted therapy. This is a natural way of healing the mind and body by utilizing the process of meditation. This is the way to keep you calm and balanced over any situation. Meditation is recommended for all sorts of physical and mental illness. Meditation is an effective complementary therapy in treating cervical dystonia or spasmodic torticollis naturally.
Craniosacral Therapy for Cervical Dystonia or Spasmodic Torticollis
This is one “hands-on” therapy tested on cervical dystonia or spasmodic torticollis patients for quicker posture correction. This procedure of releasing the body tension can be simultaneously carried with the medical treatment. This is a great way of muscle relaxation as well as pain release.
Wear a Neck Brace – If the neck ache is both chronic and severe, where even small movements result in waves of pain, then invest in a neck brace. The brace will help support your neck and let the muscles heal unimpeded.
What is Botox Injection Treatment for Cervical Dystonia or Spasmodic Torticollis – Botulinum toxin injection or Botox injection is used under strict medical surveillance by a dystonia nurse, doctor or a physiotherapist. Botox injection is only delivered at the hospital and is injected at the muscle spasm. This is measured by using an Electromyography Machine. Speak to your doctor about the Botox injection dose required for your cervical dystonia or spasmodic torticollis. They can suggest you the best depending on the seriousness of your cervical dystonia or spasmodic torticollis. The botox treatment continues to take its effect from 4 to 7 days of injecting. It may even take some more time for some people. This is an effective medication in most cases. The Botox effect remains in the body for a period of over 4 months. It may be longer for some people. It is good to consult the doctor once every 12 weeks.
Graded Neck Exercises for Cervical Dystonia or Spasmodic Torticollis – Graded neck exercises are a “step by step” formulation of the head movement towards its rectification. It is a gradual physical procedure to bring back the lost balance of the neck in cervical dystonia or spasmodic torticollis.
The exercises of the neck have been graded into two main ways.
First way – The head is made to move very gradually in all the directions.
Second way – The head is tilted to a particular direction as a target to rectify the misbalance.
Head Passive Movement for Cervical Dystonia or Spasmodic Torticollis – Take help of your family member, nurse or care taker to move your head to a particular direction. Then again ask the helper to try move your head to all the directions. This exercise is particularly for those who cannot move their head at all by their own. The force used by the helper should be moderate and regular. No extra force should be inserted with an objective to get a better result. However, it can have reverse effects if so done.
Head Active Movement for Cervical Dystonia or Spasmodic Torticollis – This is for the ones who can move the head on their own. The simple task of all direction head movement has to be carried out regularly. The task can be better performed in front of a mirror. It enhances the techniques as well as the moral of the patient. The movements will be gentle and without any excessive force. The movement should be established in all the directions. However, if there is any pain felt in any particular area, it should be taken care of and reported to the doctor. A gentle movement of the head is good for the quick correction of the problem. The mirror effect is for the confidence upliftment in the patient. As she finds her in a successful position in moving the neck and witnesses it, the moral is naturally boosted.
Body and Head Straight Movement for Cervical Dystonia or Spasmodic Torticollis – It is very important to keep the head straight. Many of the cervical dystonia or spasmodic torticolli ssufferers are so depressed with the extreme pain of the disorder that they do not even know the inclination of their head. The straight inclination of the head is very much required for a quick recovery. Use a mirror to inspect the inclination of the head. Check your chin to be in a position which is parallel to the floor. Touch your chin by yourself and adjust the position by your own. Practice this exercise as many times a day you can. This is effective in gradually correcting the posture of the neck and it tends to gain more balance. Regular practice will bring faster changes in the body.
Correct Posture During Sitting – It is necessary to maintain a correct posture as you sit down. Stand straight from your chair and try to maintain the body balance as you proceed towards sitting again. Pull back your head to maintain the posture of the neck. Tuck your chin backward as your neck falls down. The SCM (sternocleidomastoid) muscles thus get a chance to relax. You can practice this posture making in front of a mirror when no one is around. If you are sitting for a long time somewhere, you can practice doing the same mechanism. The chin tucking exercise is one of the most beneficial exercises in cervical dystonia or spasmodic torticollis. More patients have got back the confidence of social dining due to the effects of this exercise. This has been effective from saving the person from the extreme pain during this phase. The confidence is highly uplifted after the successful accomplishment of the physical performance.
A regular work out is necessary for better results. It assures the head to be free from getting frozen.
Ayurvedic cure for Neck pain
Ayurveda is one of the ancient form of treatment which has immense results only till the disease is limited between 4th stage. Well, as it the case of spine problem then mostly physical exercise is involved but following are some of the herbal remedies for neck pain cure-
www.rxharun.com
Aromatherapy
Studies show that some essential oils of some fragrant herbs heal a lot in the case of neck pain or any kind of inflammation. Like rosemary oil; it soothes the blood flow and creates warmth when massaged over the affected area.
Herbal ingredients
Herbal cure
There are many herbs which are meant to cure pains and inflammation. Like, you can use ginger and turmeric combine to cure neck pain. Hot cow’s milk with a pinch of turmeric powder heals a lot in cervical pain. Many other herbs like chamomile, Valerian, jatamansi, skullcap etc are the herbs which combat tension-related pain.
Massaging and acupressure therapy-
Massage for cervical pain
In the case of muscle related ailments, massaging techniques really works; it makes you feel relaxed and combats the pains. Same in the case of acupressure, when you press the special points related it becomes an effective-healer.
Just below the hair portion; back side of neck press the points below the skull. It will cure the neck pain with a great ease. Use mustard oil or any herbal; oil and massage the shoulders, neck portion and massage the head too. This will give an immense relief.
Yoga therapy for Neck pain
Yoga for neck pain
Now, lets move towards one of the best and obvious cure for neck pain or ay kind f inflammation. It is called Yoga; it is a simple physical activity which has hidden many therapies in it. Following are 3 yoga poses which are meant for neck pain cure. So, lets proceed-
Gomukhasana
Gomukhasana Yoga pose
Gomukhasana also known as Cow pose is one of the best poses for neck pain. In this your whole body is concentrated; the breathing is normal in this and you should carry it according to your capability; exertion of power can even increase the symptoms. Its regular practice tones up your whole body and keeps cervical pain at bay.
Steps for Gomukhasana
Kneel down on ground or Yoga mat; your upper body should be straight and looking forward.
Now take left hand from down side and right hand from shoulder side. Hold tight both the hands so that your body is straightened.
This time you should be inhaling and exhaling in normal. Stay on the pose for 30 seconds to 1 minute.
Repeat this 4-5 times.
Bhujangasana-
Bhujangasana-pose
The word is derived from the Sanskrit word ‘Bhujang’ which means ‘a snake’. In this, your body gets into the pose of a rise-hood snake. It is a very important pose which helps a lot to keep away disorders and ailments. For cervical pain, it is one of the compulsory poses.
Steps for Bhujangasana
Firstly, lie down on the floor from the belly side. Your hands should be pressed on the floor as it will become a support to raise your abdomen part.
Now, while inhaling using your hands as support raise your abdomen part.
Stay on the pose for few seconds as per your capacity.
While exhaling comes back to the floor. Repeat this for 3-4 times.
Dhanurasana
Dhanurasana pose
This word is derived from a Hindi-Sanskrit word ‘Dhanur’ which means ‘bow’. In this your body tends to be like a semi-circle or a bow. It tones up your whole body and is very beneficial. This should be regularly practiced for a toned-up and a healthy body.
Steps for Dhanurasana-
Lie down on the floor; on a yoga mat. Your feet should be apart and your arms by the sides of the body.
Fold your knees and hold your ankles.
While inhaling, lift your chest up and pull your legs upwards.
Look front with a smile on your face. Do not overstretched your body as it can cause damage.
Stay on the pose for few seconds and while exhaling comes downwards. Repeat this for 3-4 times.
So, these were the complete description of Neck pain and its cure with home remedies.
Homeopathic Treatment
Homeopathic remedies are non-toxic natural medicines safe for everyone including infants and pregnant or nursing women. You may use 6X, 30X, 6C or 30C potencies.
Lachnanthes – Spasmodic torticollis with pain and stiffness drew to the right side as if dislocated when moved. Wryneck to the right side. Top remedy.
Belladonna – Throbbing pain, stiff neck, and the right shoulder. Pain in nape of the neck as if it would break. Neck worse on the left side.
Causticum – Dull pain in nape of the neck caused by cold dry wind. The stiff neck on rising from a chair and hard to move the head. Muscle atrophy and raw burning pain. Neck worse on the right side. Worse 3 – 4 pm; better from the warmth of bed.
Cicuta virosa – Twitching and spasms on bending of head backward. From severe neck and spinal trauma or head injuries. Back arches. Epileptic-type seizures.
Cimicifuga – Muscular pains of the neck and shoulders. Feels like a black cloud overhead. Stiff neck, sensitive, worse pain or pressure which causes nausea.
Lycopodium – Neck is a much usually right side but can be left-sided. Pain and stiffness. All symptoms worse 4 to 8 pm. Throbbing or pulsating pain. The tension in the nape of the neck. One side of neck stiff and swollen or emaciated.
Phosphorus – Neck worse on the left side. Sensitive, stiff, lipoma (non-cancerous fatty benign tumor) on neck, cramping, burning.
Rhus tox – Stiffness and pain on movement, but better upon continued motion. Worse in cold weather or dampness. From injury, over lifting or overuse.
Bell’s palsy is an idiopathic, acute, unilateral paresis or paralysis of the face in a pattern consistent with peripheral facial nerve dysfunction, and may be partial or complete, occurring with equal frequency on the right and left sides of the face. There is evidence that Bell’s palsy is caused by herpes viruses. Additional symptoms of Bell’s palsy may include mild pain in or behind the ear, oropharyngeal or facial numbness, impaired tolerance to ordinary levels of noise, and disturbing taste on the anterior part of the tongue. Severe pain is more suggestive of herpes zoster virus infection (shingles) and possible progression to a Ramsay Hunt syndrome, but another cause should be carefully excluded. Up to 30% of people with acute peripheral facial palsy will not have Bell’s palsy; other causes may include stroke, tumor, trauma, middle ear disease, and Lyme disease.
Bell’s palsy is an unexplained episode of facial muscle weakness or paralysis that begins suddenly and worsens over three to five days. This condition results from damage to the 7th (facial) cranial nerve, and pain and discomfort usually occur on one side of the face or head.
Bell’s palsy is the most common peripheral paralysis of the seventh cranial nerve with an onset that is rapid and unilateral. The diagnosis is one of exclusion and most often made on a physical exam. The facial nerve has both an intracranial, intratemporal, and extratemporal course as its branches. The facial nerve has a motor and parasympathetic function as well as taste to the anterior two-thirds of the tongue. It also controls salivary and lacrimal glands. The motor function of the peripheral facial nerve controls the upper and lower facial muscles. As a result, the diagnosis of Bell’s palsy requires special attention to forehead muscle strength. If forehead strength is preserved, a central cause of weakness should be considered. Although the utility of antivirals has been called into question, treatment is medical with most sources recommending a combination of corticosteroids and antiviral medication.[rx][rx][rx]
The Others Names of Bell’s palsy
Antoni’s Palsy
Facial Nerve Palsy
Facial Paralysis
Idiopathic Facial Palsy
Refrigeration Palsy
Idiopathic peripheral facial palsy; Cranial mononeuropathy – Bell palsy
Causes of Bell’s palsy
Bell’s palsy is an acute form of cranial neuropathy. This means that it involves damage to a single nerve, in this case, the seventh cranial, or facial, nerve. This is the nerve that controls the movement of muscles of facial expression. The cause is unknown, but it affects between 1 in 5,000 and 1 in 1,000 people, according to various estimates. In 75% of cases, the palsy is preceded by an upper respiratory infection. The condition has also been associated with head injuries, heart attacks, and hypertension.
What other causes of facial weakness are there?
Ramsay-Hunt Syndrome – Viral infection with the chickenpox virus, herpes zoster, which is shingles of the facial nerve. There is usually significant pain and a rash in the ear. Other cranial nerves may be affected leading to hearing loss balance disturbance and numbness.
Skull fractures involving the temporal bone – the bone that contains the middle ear. The facial nerve travels through this bone on its way to the facial muscles and so maybe damaged usually with significant trauma to the head.
High neck injuries, particularly a stab wound to the upper neck.
Tumors anywhere along the course of the facial nerve, which includes the base of the skull, the ear, and the parotid gland just in front of the ear. These will usually present with a gradual loss of weakness to distinguish them from Bell’s palsy
Middle ear disease, especially cholesteatoma.
Damage to the facial nerve during ear surgery.
Loss of power in one side of the face can be a symptom of a stroke but there will be other features present, such as loss of power in a limb, which points to the correct diagnosis.
Clinical features of Bell’s palsy
Weakness or paralysis of the upper and lower facial muscles of the affected side
Drooping of ipsilateral eyelids
Inability to close the eye completely
Dry eye due to inability to close eyes completely
Excessive tearing of the eye (epiphora)
Drooping of the corner of the mouth
Ipsilateral impaired/loss of taste sensation
Difficulty with eating due to ipsilateral muscle weakness causing food to be trapped on the affected side of the mouth
Dribbling of saliva
The altered sensation on the affected side of the face
Pain in or behind the ear
Increased sensitivity to sound (hyperacusis) on the affected side if stapedius muscle is involved
upper motor neuron lesion – based on innervation, absence of forehead wrinkling is a reliable way of differentiating Bell’s palsy from an upper motor neuron lesion
herpes zoster oticus (Ramsay Hunt syndrome)
rarer causes including otitis media, HIV infection, sarcoidosis, autoimmune disorders or tumors of the parotid gland.
Symptoms of Bell’s palsy
Sometimes, you may have a cold shortly before the symptoms of Bell palsy begin.
Symptoms most often start suddenly but may take 2 to 3 days to show up. They do not become more severe after that.
Many people feel discomfort behind the ear before weakness is noticed. The face feels stiff or pulled to one side, and may look different. Other signs can include:
Twitching
Weakness
Paralysis on one side of the face
Problems smiling or making facial expressions
Difficulty closing your eye
Drooling due to a lack of control over the facial muscles
Difficulty closing one eye
Difficulty eating and drinking; food falls out of one side of the mouth
Drooling due to lack of control over the muscles of the face
Drooping of the face, such as the eyelid or corner of the mouth
Problems smiling, grimacing, or making facial expressions
Twitching or weakness of the muscles in the face
Bell’s palsy symptoms may come on suddenly or develop over a few days. Initial symptoms may include
Pain behind the ear that is followed by weakness and paralysis of the face
Ringing sound in the ears
Slight fever
Slight hearing impairment
A slight increase in sensitivity to sound on the affected side.
Symptoms of full-blown Bell’s palsy may include
Facial weakness or paralysis (look for smooth forehead and problems smiling)—most often on one side
Numbness just before the weakness starts
Drooping corner of the mouth
Drooling
Decreased tearing
Inability to close an eye, which can lead to
Dry, red eyes
Ulcers forming on the eye
Infection
Problems with taste
Sound sensitivity in one ear
Earache
Slurred speech
Late symptoms can occur 3-4 months after or second-time onset of Bell’s palsy and can include
Muscle weakness or paralysis
Facial Droop
Impossible or difficult to blink
Difficulty speaking
Difficulty eating and drinking
Nose runs
The nose is constantly stuffed
Difficulty breathing out of nostril on the affected side
Nostril collapse on the affected side
Forehead wrinkles disappear
Sensitivity to sound
Excess or reduced salivation
Facial swelling
Drooling
Diminished or distorted taste
Pain behind ear
Long-lasting tightening of the facial muscles
Tearing from the eye during eating
Diagnosis of Bell’s Palsy
The neurologist may recommend certain diagnostic tests, depending on the patient’s symptoms, medical history and physical examination.
Frequently the neurologist will recommend electrodiagnostic testing to measure the electrical activity of muscles and nerves. If necessary, the neurologist may also recommend a nerve biopsy, a spinal tap or magnetic resonance imaging (MRI). However, for some patients with longstanding neuropathy, the cause may not be found in spite of extensive tests and examinations.
Blood tests
Blood tests are commonly employed to check for vitamin deficiencies, toxic elements and evidence of an abnormal immune response.
Depending on your individual situation, your doctor may request certain laboratory tests to identify potentially treatable causes for neuropathy. These include tests for:
Vitamin B12 and folate levels
Thyroid, liver, and kidney functions
Vasculitis evaluation
Oral glucose tolerance test
Antibodies to nerve components (e.g., anti-MAG antibody)
Antibodies related to celiac disease
Lyme disease
HIV/AIDS
Hepatitis C and B
Tear problems > Decreased tear production & Recent cold or influenza
Hearing test—to see if nerve damage involves the hearing nerve, inner ear, or hearing mechanism
Balance test—to see if balance nerves are involved
Lumbar puncture —a test of the cerebrospinal fluid (CSF) from the lower back; to rule out meningitis , autoimmune disorders, or cancer spreading from a tumor
Tear test—measures the eye’s ability to produce tears
CT scan —a type of x-ray that uses a computer to make pictures of structures inside the head to see if there is an infection, tumor, bone fracture , or other problem in the area of the facial nerve
MRI scan —a test that uses magnetic waves to make pictures of structures inside the head to see if there is an infection, tumor, bone fracture, or other problem in the area of the facial nerve
Electrodiagnostic test
Differential Diagnosis for Facial Nerve Palsy
The nerve excitability test – determines the excitation threshold by recording the minimum electrical stimulus required to produce visible muscle contraction. A difference greater than 3.5 mA between affected and unaffected sides is considered to be significant in terms of poorer outcomes. Measuring the peak-to-peak amplitude of the evoked compound action potential of the involved side compared to the normal side has prognostic importance. If there is a 90% or greater reduction in the amplitude of the affected side, the prognosis is poor.[rx]
Currently the trigeminal blink reflex – is the only test to measure the intracranial pathway of the facial nerve and also a useful test to study various post paralysis sequelae such as synkinesis and hemifacial spasms. With the recovery of facial function, the ipsilateral R1 latency becomes less prolonged and the amount of initial prolongation of this response correlates with greater loss of facial motor function.
Gadolinium contrast magnetic resonance (MRI) – study reveals enhancement of internal acoustic meatal segment on the affected side; however, this is a non-specific finding. MRI should not be done routinely and should be the investigation to look for other possible causes for acute facial paralysis especially if there is little or no recovery of function.
Treatment of Bell’s palsy
Often, no treatment is needed. Symptoms often begin to improve right away. But, it may take weeks or even months for the muscles to get stronger.
Your provider may give you lubricating eye drops or eye ointments to keep the surface of the eye moist if you can’t close it completely. You may need to wear an eye patch while you sleep.
Sometimes, medicines may be used, but it isn’t known how much they help. If medicines are used, they are started right away. Common medicines are:
Corticosteroids, which may reduce swelling around the facial nerve
Drugs such as valacyclovir to fight the virus that may be causing Bell palsy
Surgery to relieve pressure on the nerve (decompression surgery) has not been shown to benefit most people with Bell palsy.
Your healthcare provider will prescribe other treatments for your condition based on the severity of your symptoms and your health history. Other treatment options include:
Antiviral medicine, such as acyclovir
Analgesics or moist heat to relieve pain
Electrical stimulation
Relaxation techniques – Relaxing by using techniquessuch as meditation and yoga may relieve muscle tension and chronic pain.
Acupuncture – Placing thin needles into a specific point in your skin helps stimulate nerves and muscles, which may offer some relief.
Biofeedback training – By teaching you to use your thoughts to control your body, you may help gain better control over your facial muscles.
Botulinum Toxin (Botox) Injections – These injections give you the option to treat the unaffected or the affected side of your face. These injections can help your facial muscles to relax to reduce unwanted muscle movements. They can also reduce muscle activity in the unaffected side of your face to maintain a balance. Botox injections may also help treat tears when eating and to keep you from winking an eye when smiling, eating, or laughing.
Vitamin therapy – Vitamins B-12, B-6, and zinc may help nerve growth.
Prednisolone – The rationale for the use of corticosteroids in the acute phase of Bell’s palsy is that inflammation and edema of the facial nerve are implicated in causing Bell’s palsy and corticosteroids have a potent anti-inflammatory action which should minimize nerve damage and thereby improve the outcome. Randomized, double-blind, placebo-controlled trials have provided compelling evidence that treatment with prednisolone improves outcomes in patients with Bell’s palsy and shortens the time to complete recovery.[Rx–Rx]
Prednisolone – should be used in all patients with facial palsy of less than 72 h duration who do not have contraindications to steroid therapy. The prednisolone dose used was 60 mg per day for 5 days then reduced by 10 mg per day (for a total treatment time of 10 days)[Rx] and 50 mg per day (in two divided doses) for 10 days.[Rx] The reported adverse rates were low. Treatment with prednisolone is likely to be cost-effective.[Rx]
Antiviral Agents – The rationale for the use of antiviral agents is the evidence that the inflammation of the facial nerve in Bell’s palsy might be related to the herpes simplex virus (HSV). In an autopsy study, latent HSV type-1 has been isolated from the majority of the geniculate ganglia samples.[Rx] HSV-1 genome was detected in 79% of facial nerve endoneurial fluid in patients with Bell’s palsy, but not in the controls.[Rx] However, the benefit of acyclovir or valacyclovir, either as single agents or in combination with prednisolone in Bell’s palsy has not been definitively established.[Rx–Rx,Rx, Rx] Thus with the available evidence acyclovir or valacyclovir should not be routine and treatment with acyclovir is highly unlikely to be considered cost-effective.[Rx]
Physical Therapy – In Bell’s palsy various physical therapies, such as exercise, biofeedback, laser, electrotherapy, massage, and thermotherapy are used to hasten recovery. However, the evidence for the efficacy of any of these therapies is lacking. Cochrane systemic review of the efficacy of physical therapies, electrostimulation, and exercises, on the outcome of Bell’s palsy, concluded that there was no significant benefit or harm from any of these physical therapies for Bell’s palsy. There was limited evidence that improvement began earlier in the exercise group.[Rx] Another systematic review examined the effects of facial exercises associated either with mirror or electromyogram biofeedback with respect to complications of delayed recovery in Bell’s palsy and concluded that because of the small number of randomized controlled trials, it was not possible to analyze if the exercises, were effective.[Rx] However, the possibility that facial exercise reduces time to recover and sequelae need confirming with good-quality randomized controlled trials.[Rx]
Combination therapy – A randomized controlled trial found that at nine months of diagnosis, the facial function had recovered in 94.4% of patients who took prednisolone alone, 85.4% of those who took aciclovir alone, and 92.7% of those who received both. There were no serious adverse effects in any group. The study concluded that early treatment with prednisolone alone increases the likelihood of complete recovery and there was no additional benefit of treatment with aciclovir alone or combining with prednisolone.7However, a systematic review also found that treatment with prednisolone reduced the chances of incomplete recovery but using an antiviral drug had an additional benefit.14
Hyperbaric oxygen – may improve the time to recovery and the proportion of people who make a full recovery compared with corticosteroids; however, the evidence for this is weak. We don’t know whether facial nerve decompression surgery is beneficial in Bell’s palsy.
Facial retraining – may improve recovery of facial motor function scores including stiffness and lip mobility, and may reduce the risk of motor synkinesis in Bell’s palsy, but the evidence is too weak to draw conclusions.
The efficacy of acupuncture – remains unknown because the available studies are of low quality (poor primary study design or inadequate reporting practices).[Rx] There is very tentative evidence for hyperbaric oxygen therapy in severe disease.[Rx]
Physiotherapy
During the earliest stages of Bells palsy, when muscles are completely flaccid, it is advisable to limit therapy to:
Moist heat (to ease soreness and reduce swelling)
Massage (also to ease soreness, plus to provide a degree of motion & stimulation to the muscles and increase circulation)
Mental exercises (to retain the “memory” of facial motions)
A special form of physiotherapy called facial retraining can also help minimize the asymmetrical appearance of the face that occurs when one side is weakened. Examples of facial retraining exercises can include but are not limited to
Sniffle. Wrinkle’s nose. Flared nostrils.
Curl upper lip up and raise and protruding upper lip.
Compress lips together. Pucker lips & attempt to whistle.
Smile without showing teeth; then smile showing teeth.
Try moving your lips into a small smile slowly. Then gently pucker slowly using equal strength from both sides.
Draw the angle of the mouth upward so as to deepen the furrow from the side of the nose to the side of the mouth.
Harden (wrinkle) the chin; “stick out” the chin (like a boxer).
Using your index finger and thumb pull the corners of your lips toward the center. Slowly and smoothly push out and up into a smile. Continue the movement up to the cheekbone. Use firm pressure.
Placing 4 fingertips on the eyebrow rub using a firm stroke up to the hairline. Return downward to the eyebrow. Do the same type of massage in a circular motion on your cheeks and chin, and outward to your ear.
Try to close the eye slowly and gently, without letting your mouth pull up or your eyebrow moves downward.
Raise eyebrows and hold for 10 -15 seconds (watch out for synkinesis – hold the brow at a point before the corner of your mouth starts to move or your cheek tries to help). Wrinkle forehead.
Frown and draw eyebrows downward.
Gently wink with one eye and then the other to the best of your ability.
Open eyes widely, but without involving your eyebrow. Stop if you see any inappropriate muscle actions.
Bell’s palsy develops rapidly, with symptoms ‘peaking’ within 48 hours of their onset in many patients, and maximal by 5 days overall. Patients often mistakenly believe they have had a stroke, because of the facial paralysis. In the majority of cases (60-80%), the condition gradually disappears completely within weeks to months. In some, there may be slight residual paralysis that is barely noticeable to others. Unfortunately, some people are left with complications of the condition, which include:
Obvious residual paralysis (e.g. asymmetrical smile, drooling of liquids, inability to close eye, abnormal blinking, tear pooling)
Dry eye
Affected taste
Distorted nerve functions (e.g. tear production with eating, blinking when opening mouth).
In 7-10% of people, Bell’s palsy will recur.
Hyperacusis (distorted hearing) and associated diseases such as diabetes are associated with a poor outcome. Factors that increase the likelihood of better outcome include:
Young age
Incomplete paralysis at the outset
Recovery of taste within 1 week
Early recovery (within 10-21 days).
The use of facial massage, neuromuscular retraining (e.g. using a mirror to practice the use of facial muscles), acupressure, or acupuncture may help enhance the recovery process.
How can you care for yourself at home?
Facial exercises – As the nerve in your face begins to work again, doing simple exercises—such as tightening and relaxing your facial muscles—may make those muscles stronger and help you recover more quickly. Massaging your forehead, cheeks, and lips with oil or cream may also help.
Eye care – If you can’t blink or close your eye fully, your eye may become dry. A dry eye can lead to sores and serious vision problems. To help protect the eye and keep it moist:
Use your finger to close and open your eyelid often throughout the day.
Use eye drops (“artificial tears”) or ointment. Those that contain methylcellulose are a good choice and don’t require a prescription. You may want to use drops during the day and ointment at night while you sleep. Ask your doctor how often to use the drops.
Wear an eye patch while you sleep, and wear glasses or goggles the rest of the time.
Mouth care – If you have no feeling and little saliva on one side of your tongue, food may get stuck there, leading to gum disease or tooth decay. Brush and floss your teeth often and well to help prevent these problems. To prevent swallowing problems, eat slowly, and chew your food well. Eating soft, smooth foods, such as yogurt, may also help.
Surgery of Bell’s Palsy
Nerve repair or nerve grafts – Facial nerve regeneration occurs at a rate of one millimeter per day. If a nerve has been cut or removed, the direct microscopic repair is the best option.
Nerve transposition – Often the tongue nerve (hypoglossal nerve) or the other facial nerve can be connected to the existing facial nerve. For example, the patient can then train themselves to move their face by moving their tongue.
Muscle transposition or sling procedures – The temporalis muscle or masseter muscle (some of the only muscles on the face not supplied by the facial nerve), can be moved down and connected to the corner of the mouth to allow movement of the face.
Muscle transfers – Free muscles from the leg (gracilis) can be used to provide both muscle bulk
Home Remedies for Bell’s Palsy
You can improve your chances of recovering faster by taking medications. It is also important to protect your eye if you cannot close your eyelids. Here are some treatment options for quick recovery:
www .rxharun.com
Eye Protection
You can always damage your eye if your eyelids do not close properly. It may also lead to dryness. Your doctor will give you goggles or an eye pad for protection along with eye drops to keep your eye moist. There is also an option of taping the lower and upper lid together to keep your eye closed while you are sleeping.
2.
rx
Try Heat Compress
Apply soaked warm washcloth on face at least 3 times a day to find some comfort. The heat will help to relax facial muscles and prevent atrophy.
3. Massage with Olive Oil
www.rxharun.com
Regular massage with olive oil can increase blood circulation, which will help to improve your paralysis by stimulating damaged nerve. Start with your lower face. Place your thumb and index finger on each corner of your mouth, then push your lips forward and repeat for about 15 times. Next, massage your forehead and around your eyebrows. After that, move to your cheeks. Remember to apply some pressure to massage in a circular motion. Each part of the face shall be massaged for at least 2-3 minutes.
4. Try Castor Oil
www.rxharun.com
Castor oil helps because it’s effective in dealing with swelling, repairing damaged nerve and strengthening facial muscles. To do that, apply a cotton cloth that has been soaked in heated castor oil on the face for at least 3 times a day. For better result, you can use something such as flannel to retain the heat.
5. Eat Some Celery
www.rxharun.com
The vitamins and minerals in celery are beneficial for nerve health and can help to repair damaged nerve. In addition, celery can also boost your immune system. Eat celery, leaves and stick, raw several times a day.
6.
www.rxharun.com
Have Some Ginger and Turmeric
The anti-inflammatory properties in ginger and turmeric are very effective in relieving Bell’s palsy symptoms. You can either add them to your food while cooking or take their supplements.
7. Take Vitamin Supplements
www.rxharun.com
Vitamins such as vitamin B-12, B-6, and zinc can greatly speed up Bell’s palsy recovery. Vitamin B-12 is helpful for neurological conditions while vitamin B-6 helps nerve growth. Vitamin B-1 also helps with its thiamine in treating never inflammation. However, consult your doctor for proper doses before taking them.
Ayurvedic Treatment for Bell’s Palsy
Brahmi Capsules
Brahmi capsules of Planet Ayurveda are packed with pure extract of the best quality Brahmi. Brahmi is known as Bacopa monnieri scientifically.
Pack Size: 1 Bottle 60 Capsules
Dosage: 1 capsule twice daily with plain water after meals
Ashwagandha Capsules
Ashwagandha capsules of Planet Ayurveda are packed with pure extract of the best quality Ashwagandha. Ashwagandha is Withania somnifera scientifically.
Pack Size: 1 Bottle 60 Capsules
Dosage: 1 capsule twice daily with plain water after meals
Curcumin Capsules
Curcumin capsules of Planet Ayurveda are packed with a standardized extract of Curcumin, an active compound of turmeric.
Pack Size: 1 Bottle 60 Capsules
Dosage: 1 capsule twice daily with plain water after meals
Chandraprabha Vati
Chandraprabha Vati is a classical natural formulation, a blend of many ingredients that are explained in ayurvedic texts. Some of them are Vacha (Acorus calamus), Mustak (Ciprus rotundus), Pippali (Piper longum), Maricha (Piper nigrum), Haridra (Curcuma longa), Vidanga (Emblica ribes), etc.
Overall Chandraprabha Vati maintains healthy body functions.
Pack Size: 1 Bottle of 120 Tablets
Dosage: 2 tablets twice daily with plain water after meals
Nirgundi Oil
Nirgundi oil contains Nirgundi (Vitex Segundo) with other ingredients like Haridra (Curcuma longa), Manjista (Rubia cordifolia), Kalahari (Dichrostachys cinerea).
Pack Size: 1 Bottle 100ml
Dosage: for external use. Apply on the affected area once to twice daily and massage gently.
Bell’s Palsy (Homeopathy)
Aconitum napellus
When one side of a person’s face becomes paralyzed, especially after being exposed to wind or cold air, this remedy may be helpful. A feeling of fear and agitation and a sudden onset of symptoms are strong indications for Aconitum napellus.
Agaricus
This remedy may be indicated in Bell’s palsy when the facial muscles on one side are stiff, and grimacing or twitching occurs in other parts of the face. People who need this remedy are often excitable, with senses that are over acute. Many people who need this remedy have deep anxiety about their health.
Cadmium sulphur atom
Facial paralysis (usually left-sided) that starts after exposure to wind, and is accompanied by chilliness or overwhelming weakness, suggests a need for this remedy. The person’s mouth may look distorted, and completely closing one of the eyes often is impossible.
Causticum
This remedy can be helpful when facial paralysis has developed gradually (most often on the right side). Opening and closing the mouth can be difficult, and the person may accidentally bite the tongue or the inside of the cheek. The person may be weak but restless and tends to feel best when keeping warm.
Cocculus
One-sided facial paralysis, with pain or tension, felt in the other cheek, especially when opening the mouth, suggests a need for this remedy. Weakness, dizziness, or numbness are other indications. The person may feel worse from lack of sleep or from being emotionally upset.
Nux vomica
One-sided facial paralysis (more often on the left) in a person who is irritable, impatient, and hypersensitive to odors, sounds, and light may indicate a need for this remedy. Cramping and constricting feelings may be felt, and problems may be worse from the cold.
Platina (also called Platinum)
This remedy may be indicated for painless paralysis of the face, with facial distortion that raises one eyebrow or creates a “haughty” look. The person may also experience numbness in the lips and cheeks, or other body parts
Complications
Due to the complexity of our facial muscles and their function, a number of problems can arise following the prolonged experience of having Bell’s palsy
Contracture – Shortening of the facial muscles over time may make the affected side of the face appear to be slightly ‘lifted’ in comparison to the unaffected side, and the affected eye may appear smaller than the unaffected eye. The fold between the outer edge of the nostril and the corner of the mouth may seem deeper due to the increased contraction of cheek muscles on that side.
Crocodile tears – This means that the affected eye waters involuntarily, particularly whilst eating. This is due to faulty ‘re-wiring’ of the nerves during the recovery phase.
Lagophthalmos – This is an inability to close the affected eye, which if prolonged may result in eye dryness and/or corneal ulceration. (This complication can be assisted/prevented by the use of artificial tears and taping the eye down at night.) In rare cases, the vision may be permanently damaged if care is not taken.
Synkinesis – This means that when intentionally trying to move one part of the face, another part automatically moves. For example, on smiling the eye on the affected side automatically closes. Similarly, on raising the eyebrows or closing the eyes, involuntary contraction of the cheek or neck muscles occurs. Find out more about synkinesis.
People with persistent symptoms of Bell’s palsy may experience psychological problems including stress, anxiety, depression and low self-esteem
altered sense of taste
facial pain, pain in or behind the ear (in fewer than 50% of cases)
no tears in one eye
sensitivity to noise on the affected side
There’s none of the confusion, language difficulty, or crushing headache that’s commonly seen in stroke victims. You may have some trouble talking, but it’s purely muscular, whereas stroke victims have difficulty finding the words they need.
Usually, the symptoms appear at once. Occasionally, they worsen over a few days. Steady, progressive paralysis over several weeks is not a sign of Bell’s palsy.
The most serious complication seen in Bell’s palsy is permanent mild facial paralysis. This is found in a minority of cases. Overall, about 80% to 90% recover completely over weeks to months, and most of the rest improve.
Another complication is increased risk of stroke. Stroke prevention and follow-up is recommended.
Incomplete recovery is more likely in people who
are over age 55
feel pain other than ear pain
have weakness/paralysis on both sides of the face – this occurs in 1% of cases
show a lack of tears
People who don’t recover completely may be left with one or more of the following symptoms
abnormal blink
asymmetrical smile
buccinator paralysis (food caught in cheek of paralyzed side)
corneal damage
drooling of liquids from corner of paralyzed mouth
dry eye
excessive perspiration
frozen muscle in the nostril area
hyperacusis (perceiving sounds as unusually loud)
impaired taste
impaired speech
synkinesis
Summary of topics and recommendations
Treatment
Severity
Recommendation
Strength
Confidence in effect estimate
Corticosteroids
Any severity
We recommend the use of corticosteroids for all patients with Bell palsy.
Strong
Moderate
Antivirals
Any severity
We recommend against antiviral treatment alone.
Strong
Moderate
Corticosteroids + antivirals
Mild to moderate paresis
We suggest against the addition of antivirals to corticosteroids for patients with mild to moderate severity.
Weak
Moderate
Severe to complete paresis
We suggest the combined use of antivirals and corticosteroids in patients with severe to complete paresis.
Weak
Moderate
Exercise physiotherapy
Acute; any severity
We make no recommendation regarding the use of exercise physiotherapy for acute Bell palsy of any severity.
Not applicable
Very low
Chronic
We suggest exercise physiotherapy for patients with persistent weakness.
Weak
Very low
Electrostimulation
Acute; any severity
We suggest against the use of electrostimulation.
Weak
Very low
Surgical decompression
Severe to complete paresis
We suggest against the routine use of surgical decompression.
Weak
Very low
Eye-protective measures for incomplete eye closure
Any severity, with incomplete eye closure
We recommend the routine use of eye-protective measures for patients with incomplete eye closure.
Strong
Very low
Referral to specialist
Progressive cases
We recommend referral to a specialist for patients with no improvement or progressive weakness.
Strong
Very low
Work-up for neoplasm
Progressive cases
We recommend imaging to rule out neoplasms or alternative diagnoses for patients with no improvement or progressive weakness.
PLID (Prolapse lumbar intervertebral disc) is one of the most common, chronic lumbar vertebral column diseases of elderly people leading to back pain, low back pain, sciatica, quadra equines syndromes, radicular pain, and subsequently neurological deficit due to nerve root compression that leads to radiating pain up to whole lower limb. [rx,rx,rx] The lumbar intervertebral disc is a complex structure composed of collagen, proteoglycans, glycosaminoglycan, and sparse fibrochondrocytic cells that serve to dissipate forces exerted on the spine. As part of the normal aging process, the disc fibrochondrocytes can undergo senescence, and proteoglycan production diminishes. This leads to a loss of hydration and disc collapse, which increases strain on the fibers of the annulus fibrosus surrounding the disc. Tears and fissures in the annulus can result, facilitating a herniation of disc material, should sufficient forces be placed on the disc. Alternatively, a large biomechanical force placed on a healthy, normal disc may lead to extrusion of disc material in the setting of the catastrophic failure of the annular fibers.[Rx]
PLID (Prolapse lumbar intervertebral disc), also known as a slipped disc, is a medical condiververtibral dissection affecting the spine in which a tear in the outer, fibrous ring of an intervertebral disallows the soft, central portion to bulge out beyond the damaged outer rings. Rarely bowel or bladder control is lost, and if this occurs, seek medical attention at once. A common cause of lower back and leg pain is a lumbar ruptured disc or herniated disc. Symptoms of a herniated disc may include dull or sharp pain, muscle spasm or cramping, sciatica, and leg weakness or loss of leg function. Sneezing, coughing, or bending usually intensify the pain.
Sciatica is a symptom frequently associated with a lumbar herniated disc. Pressure on one or several nerves that contribute to the sciatic nerve can cause pain, burning, tingling, and numbness that extends from the buttock into the leg and sometimes into the foot. Usually, one side (left or right) is affected.
Anatomy of PLID
First, a brief overview of spinal anatomy so that you can better understand how a lumbar herniated disc can cause lower back pain and leg pain, and PLID.
In between each of the 5 lumbar vertebrae (bones) is a disc—a tough fibrous shock-absorbing pad. Endplates line the ends of each vertebra and help hold individual discs in place. Every disc has a tire-like outer band (annulus fibrosus) that encases a gel-like substance (nucleus pulposus).
Disc herniation occurs when the annulus fibrous breaks open or cracks, allowing the nucleus pulposus to escape. This is called a herniated nucleus pulposus or herniated disc, although you may have also heard it called a ruptured disc or a bulging disc.
When a disc herniates, it can press on the spinal cord or spinal nerves. All along your spine, nerves are branching off from the spinal cord and traveling to various parts of your body (to help you feel and move). The nerves pass through small passageways between the vertebrae and discs, so if a herniated disc presses into that passageway, it can compress (or “pinch”) the nerve. That can lead to the pain associated with herniated discs.
The lumbar disc is a fibrocartilaginous structure that is seated between two vertebral body endplates. It is composed of an internal gelatinous nucleus pulposus and an external fibrous annulus fibrosus. The primary function of the lumbar disc is shock absorption. Two longitudinal ligaments lie anterior and posterior to the vertebral body. The anterior longitudinal ligament resists lumbar extension, translation, and rotation. The posterior longitudinal ligament resists lumbar flexion. The segmental ligaments include the ligamentum flavum, which is perforated when performing a lumbar puncture. The remaining segmental ligaments include the supraspinous and interspinous ligaments which lie between the spinous processes and resist lumbar flexion.[rx][rx]
(In the illustration below, you can see a close-up look at a herniated disc pressing on a spinal nerve.)
This article on lumbar herniated discs will cover the symptoms, causes, and (most importantly) treatments.
Physiology of Anatomy of Spine
Complete intervertebral disc anatomy and biomechanics and disc composition. Each disc is made up of 3 main components. These components include the nucleus pulposus (NP), the annulus fibrosis (AF) and the cartilaginous endplates (CEP)[rx] The cartilaginous endplates are composed of a small amount of hyaline cartilage that is located between the vertebral endplate and the NP.[rx] It is made up of water, type II collagen, chondrocyte-like cells, and proteoglycans (sulfated glycosaminoglycans). These constituents help the NP to be elastic, allow it to be flexible under stress, and resist compression.[rx] The high amount of sulfated glycosaminoglycans gives the nucleus pulposus a high charge density which causes the NP to absorb water and swell, which gives it the ability to act like both a solid and a liquid in mechanical situations.[rx]
The annulus fibrosis
The annulus fibrosus is the type I collagen surrounding the nucleus pulposus in approximately 15-20 layers. Together, the annulus fibrosis and nucleus pulposus form the intervertebral disc between adjacent vertebrae. The annulus fibrosus runs obliquely between edges of adjacent vertebrae, connecting the inferior endplate of the superior vertebra with the superior endplate of the inferior vertebra. The directions of the layers of the annulus fibrosus alternate which adds to the strength of the annulus fibrosus. Near the central region, the annulus fibrosus blends with the nucleus pulposus. The posterolateral aspect of the annulus fibrosus has a greater content of vertically oriented fibers leading to relative focal weakness at the posterolateral aspect.
Composed of type I collagen, water, and proteoglycans
Characterized by extensibility and tensile strength
High collagen / low proteoglycan ratio (low % dry weight of proteoglycans)
Asymptomatic Annular Tear – If the annular tear or fissure is identified incidentally, then no treatment is warranted. Such annular fissures may resolve spontaneously over time and are frequently due to the stresses applied to the spine and causes PLID. It is posited that some asymptomatic annular tears may become symptomatic with time, but there is currently no definitive evidence that the treatment of asymptomatic annular tears provides any benefit or prevents any future issues.[rx]
Symptomatic Annular Tear without Disc Protrusion or Herniation – An annular fissure or tear can be symptomatic without disc protrusion or herniation. It is suspected that local inflammatory reactions from the annulus fibrosus tear or fissure lead to irritation of adjacent nerve fibers or traversing nerve roots.[rx]
Nucleus pulposus
The nucleus pulposus is composed of water, type II collagen, chondrocyte-like cells, and proteoglycans. This unique composite allows the NP to be elastic, flexible under stress forces and to absorb compression.[rx] The composition of the AF is mainly concentric layers of collagen type I fibers,[rx] forming a fibrous tissue with helical disposition surrounding the NP, this structure is denser in the anterior part and is attached to the vertebral body by Sharpey fibers.
Composed of type II collagen, water, and proteoglycans
Characterized by compressibility
Low collagen / high proteoglycan ratio (high % dry weight of proteoglycans)
Proteoglycans interact with water and resist compression
A hydrated gel due to high polysaccharide content and high water content (88%)
Nerve Root Anatomy of PLID
Lumbosacral Nerve Root and innervation Anatomy
L1 nerve root – Exits between L1 and L2 foramina, innervates iliopsoas muscle, sensory distribution, upper third thigh, assessed with the cremasteric reflex (male).
L2 nerve root – Exits between L2 and L3 foramina, innervates iliopsoas muscle, hip adductor, and quadriceps, sensory distribution, middle third thigh, no reflex.
L3 nerve root – Exits between L3 and L4 foramina, innervates iliopsoas muscle, hip adductor, and quadriceps, sensory distribution, lower third thigh, no reflex.
L4 nerve root – Exits between L4 and L5 foramina, innervates quadriceps and tibialis anterior, sensory distribution, anterior knee, medial side of the leg, assessed with patellar reflex.
L5 nerve root – Exits between L5 and S1 foramina, innervates extensor hallucis longus, extensor digitorum longus, and brevis, and gluteus medius, sensory distribution: anterior leg, lateral leg, and dorsum of the foot, no reflex.
S1 nerve root – Exits between S1 and S2 foramina, innervates gastrocnemius, soleus, and gluteus maximus, sensitive distribution, posterior thigh, plantar region, assessed with Achilles reflex.
The key difference between the cervical and lumbar spine is Pedicle/nerve root mismatch
Cervical spine C6 nerve root travels under C5 pedicle (mismatch)
Lumbar spine L5 nerve root travels under L5 pedicle (match)
Extra C8 nerve root (no C8 pedicle) allows the transition
Horizontal (cervical) vs. vertical (lumbar) anatomy of nerve root
Because of the vertical anatomy of the lumbar nerve root, a paracentral and foraminal disc will affect different nerve roots
Because of the horizontal anatomy of the cervical nerve root, a central and foraminal disc will affect the same nerve root
Location
Central Prolapse
Often associated with back pain only
May present with cauda equina syndrome which is a surgical emergency
Posterolateral (paracentral)
Most common (90-95%)
PLL is weakest here
Affects the traversing/descending/lower nerve root
At L4/5 affects the L5 nerve root
Foraminal (far lateral, extraforaminal)
Less common (5-10%)
Affects exiting/upper nerve root
At L4/5 affects the L4 nerve root
L5 at the L5/S1 level, a disc herniation far laterally into the left/right neural foramen would compress the L5 nerve, resulting in weakness of hip abduction muscles, ankle dorsiflexion (anterior tibialis muscle) and/or extension of the great toe (extensor hallucis longus muscle).
S1 at the L5/S1 level, a disc herniation centrally into the canal would compress the S1 nerve, resulting in weakness of ankle plantar flexion (gastrocnemius muscle).
Axillary
Can affect both exiting and descending nerve roots
A disc herniation at the L5/S1 level can have two overlapping presentations
Anatomic
Protrusion > eccentric bulging with an intact annulus
Extrusion > disc material herniates through the annulus but remains continuous with disc space sequestered fragment (free)disc material herniates through the annulus and is no longer continuous with disc space. Axial back pain (low back pain)
This may be discogenic or mechanical in nature
Disc herniation material (i.e., herniated nucleus pulposus, HNP)
Varying degrees of HNP are recognized, from disc protrusion (annulus remains intact), extrusion (annular compromise, but herniated material remains continuous with disc space), to sequestered (free) fragments.
HNP material predictably is resorbed over time, with the sequestered fragment demonstrating the highest degree of resorption potential
In general, 90% of patients will have an asymptomatic improvement in radicular symptoms within 3 months following nonoperative protocols alone.
Hypertrophy/expansion of degenerative tissues
Common sources include ligamentum flavum and the facet joint. The facet joint itself undergoes degenerative changes (just like any other joint in the body), and synovial hypertrophy and/or associated cysts can compromise surrounding nerve roots.
Types of PLID
According to the position of the spinal disc herniation are 4 types
Herniation may develop suddenly or gradually over weeks or months. The 4 stages of a PLID are
2) Prolapse – The form or position of the disc changes with some slight impingement into the spinal canal and/or spinal nerves. This stage is also called a bulging disc or a protruding disc.
3) Extrusion – The gel-like nucleus pulposus breaks through the tire-like wall (annulus fibrosus) but remains within the disc.
4) Sequestration or Sequestered Disc – The nucleus pulposus breaks through the annulus fibrosus and can then go outside the intervertebral disc.
Causes of PLID
Piriformis syndrome – This develops when the piriformis muscle, a small muscle that lies deep in the buttocks, becomes tight or spasms, which can put pressure on and irritate the sciatic nerve & causes PLID.
Spinal stenosis – This condition results from the narrowing of the spinal canal with pressure on the nerves.
Spondylolisthesis – This is a slippage of one vertebra so that it is out of line with the one above it, narrowing the opening through which the nerve exits.
Cauda equina syndrome – A rare but serious condition that affects the nerves in the lower part of the spinal cord; it requires immediate medical attention. Cauda equina syndrome may permanently damage the nervous system and even lead to paralysis.
Bony growths (osteophytes) – Osteophytes are bony lumps (bone spurs) that grow on the bones of the spine or around the joints. They often form next to joints affected by osteoarthritis, a condition that causes joints to become painful and stiff.
Bone spurs– are bony outgrowths on the edges of joints. Bone spurs form where cartilage is worn away (for example in arthritis) and bone is rubbing on bone. In an effort to protect the body, new bone forms on the edge of joints. This is called a bone spur. Bone spurs are not painful in themselves, but unfortunately, the bone spurs can rub on nearby bone or nerves, causing problems. In the spine, bone spurs can intrude into space normally reserved for the nerves, thus causing sciatica.
Sudden injury or accident – Some unexpected traumatic events, such as a car accident, can lead to sciatica. Injuries sustained and new scar tissue can place stress on the sciatic nerve.
Pregnancy – During pregnancy, pain in the back of the thighs spurred by shifts in the pelvic region can be misdiagnosed as sciatica. However, there are situations in which the sciatic nerve is actually being pressed as a result of these changes. Speak to your doctor if you think you are suffering from sciatica or pelvic groin pain.
Tumors – within the spine may compress the root of the sciatic nerve.
Males in their 30s and 40s are most prone to cauda equina syndrome caused by disk herniation.
Most cases of sciatica syndrome caused by disk involve large particles of disk material that have completely separated from the normal disk and compress the nerves (extruded disk herniation). In most cases, the disk material takes up at least one-third of the canal diameter.
Spinal stenosis is any narrowing of the normal front-to-back distance (diameter) of the spinal canal.
Narrowing of the spinal canal can be caused by a developmental abnormality or degenerative process.
The abnormal forward slip of one vertebral body on another is called spondylolisthesis. Severe cases can cause a narrowing of the spinal canal and lead to sciatica syndrome
Tumors (Neoplasms)
Sciatica syndrome can be caused by isolated tumors (primary neoplasms) or from tumors that have spread to the spine from other parts of the body (metastatic spinal neoplasms). Metastatic spine tumors are most commonly from the prostate or lung in males and from the lung and breast in females.
Loss of feeling in the legs (sensory loss) and loss of bowel or bladder control (sphincter dysfunction) are also common.
Inflammatory Conditions
Both acute and chronic form may be seen in long-standing ankylosing spondylitis (2nd-5th decades; average 35 years)
Long-lasting inflammatory conditions of the spine, including Paget disease and ankylosing spondylitis, can cause a narrowing of the spinal canal and lead to sciatica syndrome.
Poorly positioned screws placed in the spine can compress and injure nerves and cause sciatica syndrome.
Continuous spinal anesthesia has been linked to cases of sciatica syndrome.
Lumbar puncture (spinal tap) can cause a collection of blood in the spinal canal (spontaneous spinal epidural hematoma) in patients receiving medication to thin the blood (anticoagulation therapy). This collection of blood can compress the nerves and cause sciatica syndrome.
Loss of Sensation– Those affected may experience numbness or tingling in their perineum
Loss of Reflexes – A person’s knee and ankle reflexes might be diminished, along with anal and bulbocavernosus abilities.
Sensory Loss – Sensory loss may range from, ‘pins and needles,‘ to complete numbness. It might affect a person’s bowel, bladder, and genitalia Bladder, Bowel and
Associate clinical feature is
Approximate area of “saddle anesthesia” seen from behind (yellow highlight)
Saddle anesthesia i.e., anesthesia or paraesthesia involving S3 to S5 dermatomes, including the perineum, external genitalia, and anus; or more descriptively, numbness or “pins-and-needles” sensations of the groin and inner thighs which would contact a saddle when riding a horse.
Detrusor weaknesses causing urinary retention and post-void residual incontinence as assessed by bladder scanning the patient after the patient has urinated.
Sciatica type pain on one side or both sides, although pain may be wholly absent
Your doctor may ask about medical history in which you answer questions about your health, symptoms, and activity. Previous disease condition, fracture, lifestyle, geographical location, food habit, and acute and chronic disease, drug addictions, occupation of the patient. In the lumbar spine, a herniated disc can present with symptoms including sensory and motor abnormalities limited to a specific myotome. History in these patients should include chief complaints, the onset of symptoms, where the pain starts and radiates. History should include if there is any past treatment history.
Pain history for PLID is-
Duration – How long the pain is present?
Onset – How did it start?
Progress – What happened afterward?
Site – Where do you feel the pain, point it out with a single finger?
Character – What is the nature of pain? Is it throbbing, pricking, or burning type of pain?
The intensity of pain – What is the severity of pain at present, at rest, and during activity? How severe was the worst pain you experienced?
Temporal factors – Continuous or intermittent, diurnal variation.
Is the pain continuous or intermittent?
If intermittent, how long does each episode last?
If intermittent, is it colicky in nature?
Is there any relation between the severity of pain and the time of day?
Is there any sleep disturbance due to pain?
Aggravating factors.
Is it aggravated by activity? Suggestive of mechanical pain.
Is it aggravated when getting up in the morning? If yes, how long does the increased pain last? Morning stiffness is present if the pain lasts for more than one hour. Morning stiffness is suggestive of inflammatory spondyloarthropathy.
Is it aggravated by walking? Suggestive of vascular or neurogenic claudication.
Is it aggravated by standing? Suggestive of neurogenic claudication.
Relieving factors.
Is it relieved by activity? Suggestive of inflammatory spondyloarthropathy.
Is it relieved by rest? Suggestive of mechanical pain.
If aggravated by walking, is it relieved by standing? Suggestive of vascular claudication.
If aggravated by standing and walking, is it relieved by sitting down or stooping forwards? Suggestive of neurogenic claudication.
Manual palpation Test
Palpation was conducted on the left side-lying position with pressure applied only to the onset of pain (P1).
The presence of generalized hyperalgesia made it difficult to establish a comparable finding day.
Physical exam
A physical exam to assess your strength – reflexes, sensation, stability, alignment, and motion.
A careful neurological examination can help in localizing the level of the compression. The sensory loss, weakness, pain location, and reflex loss associated with the different levels are described in Table 2.
L1 Nerve – pain and sensory loss are common in the inguinal region. Hip flexion weakness is rare, and no stretch reflex is affected.
L2-L3-L4 Nerves – back pain radiating into the anterior thigh and medial lower leg; sensory loss to the anterior thigh and sometimes medial lower leg; hip flexion and adduction weakness, knee extension weakness; decreased patellar reflex.
L5 Nerve – back, radiating into buttock, lateral thigh, lateral calf and dorsum foot, great toe; sensory loss on the lateral calf, dorsum of the foot, webspace between first and second toe; weakness on hip abduction, knee flexion, foot dorsiflexion, toe extension and flexion, foot inversion and eversion; decreased semitendinosus/semimembranosus reflex.
S1 Nerve – back, radiating into buttock, lateral or posterior thigh, posterior calf, lateral or plantar foot; sensory loss on the posterior calf, lateral or plantar aspect of foot; weakness on hip extension, knee flexion, plantar flexion of the foot; Achilles tendon; Medial buttock, perineal, and perianal region; weakness may be minimal, with urinary and fecal incontinence as well as sexual dysfunction.
S2-S4 Nerves – sacral or buttock pain radiating into the posterior aspect of the leg or the perineum; sensory deficit on the medial buttock, perineal, and perianal region; absent bulbocavernosus, anal wink reflex.
Motor exam
Ankle dorsiflexion (L4 or L5)
Test by having the patient walk on heels
EHL weakness (L5)
Manual testing
Hip abduction weakness (L5)
Have the patient lie on the side on the exam table and abduct leg against resistance
The Straight Leg Raise (SLR) test is a neurodynamic test. SLR is a neural tension test that can be used to rule in or out neural tissue involvement as a result of a space-occupying lesion, often a lumbar disc herniation. It is one of the most common neurological tests of the lower limb.
A tension sign for L5 and S1 nerve root
Can be done sitting or supine
Reproduces pain and paresthesia in the leg at 30-70 degrees hip flexion
Sensitivity/specificity most important and predictive physical finding for identifying who is a good candidate for surgery.
Contralateral SLR
Crossed straight leg raise is less sensitive but more specific. Radicular pain in the affected leg when the contralateral asymptomatic leg is similarly raised constitutes a positive crossed straight-leg raise (X-SLR) test.
League sign
SLR aggravated by forced ankle dorsiflexion. Lasegue sign or straight leg raising test (SLRT) is a neurodynamic exam to assess nerve root irritation in the lumbosacral area.[rx] It is an integral element to the neurological exam for patients presenting with low back pain with or without radicular pain. The other less commonly used name is the Lazarevic sign.
Kernig test
Pain reproduced with neck flexion, hip flexion, and leg extension. Kernig’s sign is a test used in physical examination to look for evidence of irritation of the meninges. The test involves flexing the thighs at the hip, and the knees, at 90-degree angles, and assessing whether the subsequent extension of the knee is painful (leading to resistance), in which case it is deemed positive.
Naffziger test
A maneuverused to identifycompression of nerveroots in thecervicalspine,based on exacerbation of painandparaesthesias of thehandandfingers,whentheexaminerexertspressure on thescalenusanteriormuscles in patientswithscalenusanteriorsyndrome. (for nerve root compression) increase or aggravation of pain or sensory disturbance over the distribution of the involved nerve root upon manual compression of the jugular veins bilaterally confirms the presence of an extruded intervertebral disk or other mass.
Pain reproduced by coughing, which is instigated by lying patient supine and applying pressure on the neck veins Milgram test
Pain reproduced with straight leg elevation for 30 seconds in the supine position
Gait analysis
Trendelenburg gait due to gluteus medius weakness which is innervated by L5.
Quadrant Test
Position of patient – Standing
Position of examiner – Standing behind the patient
Procedure – Keep one hand over the patient’s contralateral shoulder and apply axial pressure. Ask the patient to hyperextend, rotate and laterally flex to the contralateral side.
Interpretation – Provocative pain is taken as a sign of lumbar instability.
Use – Used if pain cannot be produced by forwarding flexion, lateral flexion etc.
Adams Forward Bending Test
Position of patient – Standing with feet together, knee extended.
Position of examiner – Standing behind the patient first then in front of the patient.
Procedure – Rule out limb length discrepancy. Ask the patient to bend forwards at the waist till the back is in the horizontal plane. Palms should be held together.
Interpretation – If there is a rib or loin hump present, then there is structural scoliosis with rotation.
Use – To differentiate between structural and non-structural scoliosis.
Validity of test – For a patient with 40 structural scolioses, the test has a sensitivity of 0.83 and a specificity of 0.99.
Additional manual test for nerve root compression
Crossed SLRT – AKA well-leg raising test or Fajersztajn sign. When the contralateral leg is lifted, the patient experiences pain on the affected side. [rx][rx]This test is more specific than ipsilateral SLRT. It becomes positive, usually in severe compression and centrally located prolapse. Fajersztajn believed that this sign is due to disc prolapse in the axilla of the root.[rx]
Reverse SLRT – AKA femoral stretch or Ely test. While the patient is in a prone position, the leg is lifted off the table with both hip and knee joints extended. Some authors may allow knee flexion. This maneuver may reproduce radicular pain in the case of upper lumbar radiculopathy, far lateral lumbar disc, or femoral neuropathy. The pain will present in the femoral nerve distribution on the side of the lesion.[rx]
Braggart test – AKA Sciatic stretch test or Flip test. While raising the leg, the foot is held in a dorsiflexed position so that the sciatic nerve is stretched more, thereby increasing the intensity of pain or making it possible to elicit the sign early.[rx][rx]
Reverse flip test – While raising the leg, the foot is held in a plantar-flexed position; this will lessen the pain. But if the patient is complaining of an increase in pain, it can suggest malingering.[rx]
Bowstring sign – Also known as the popliteal compression test or posterior tibial nerve stretch sign. The patient can be examined in sitting or in a supine position. The examiner flexes the knee and applies pressure on the popliteal fossa, evoking sciatica. Some examiners do it after SLRT by flexing the knee to relieve the buttock pain. The pain would be reproduced by a quick snap on the posterior tibial nerve in the popliteal fossa.[rx]
Less frequently used nerve root irritation tests For PLID
For the sake of completion, other tests and signs of nerve root tension or irritation are discussed succinctly below
Sitting SLRT (Bechterew test) – the patient is made to sit at the edge of a table with both hip and knee flexed, then made to extend the knee joint or elevate the extended knee, which reproduces the radicular pain. They may be able to extend each leg alone, but extending both together causes radicular pain.[rx]
Distracted SLRT – the sitting SLRT is performed without the patient’s awareness. The patient is distracted as if the surgeon is examining the foot or pulsation, and slowly, the examiner extends the knee. If the patient is experiencing true radiculopathy, the same pain will be reproduced. Otherwise, we can assume that the patient may be malingering.
Neri’s sign – while bending forward, the patient flexes the knee to avoid stretching the nerve.[rx]
The buckling sign[rx] – the patient may flex the knee during SLRT to avoid sciatic nerve tension.
Sicard sign – passive dorsiflexion of ipsilateral great toe just at the angle of SLRT will produce more pain.
Kraus-Weber test – the patient may be able to do a sit-up with the knees flexed but not extended.
Minor sign – the patient may rise from a seated position by supporting himself/herself on the unaffected side, bending forward, and placing one hand on the affected side of the back.
Bonnet phenomenon – the pain may be more severe or elicited sooner if the test is carried out with the thigh and leg in a position of adduction and internal rotation.[rx]
Provocative Tests In A Spinal Examination and PLID
Shoulder Abduction (Relief) sign – Active abduction of symptomatic arm achieved by patient placing their ipsilateral hand on their head. A positive test results in relief (or reduction) of cervical radicular symptoms.
Neck Distraction test– Active distractive force is applied by the examiner while grasping the patient’s head under the occiput and chin. A positive test results in relief (or reduction) of cervical radicular symptoms.
L’hermitte’s sign– Examiner passively flexes patient’s cervical spine. A positive test result is an electric shock-like sensation down the spine or extremities.
Hoffman’s sign – Passive snapping flexion of distal phalanx of patient’s middle finger. A positive test results in flexion-adduction of the ipsilateral thumb and index finger.
Adson’s test – Patient is instructed to inspire with chin elevated, and head rotated to the affected side. A positive test results in obliteration of radial pulse.
The Spurling test – is designed to reproduce symptoms by compression of the affected nerve root. The cervical extension is used to induce/reproduce posterior bulging of the intervertebral disk. Rotation of the head causes narrowing of the neuroforamina in the cervical spine. Finally, axial compression is applied to amplify these effects with the aim of exaggerating the preexisting nerve root compression.
The prone instability test – The patient starts by standing on one end of the examination couch. While continuing to stand on the foot end of the couch, the patient lowers his / her torso onto the couch. The patient can hold onto the couch’s sides for support. The examiner then palpates the lower lumbar spine to elicit tenderness. The patient then holds onto the couch and lifts his / her feet off the ground tensing the paraspinal muscles. Less pain and tenderness on repeat palpation of the lower lumbar spine, while the feet are off the floor, is considered positive. [rx]
Prone Plank/Bridge – The patient is prone and elevates his / her entire body off the couch/mat on forearms and tips of toes. The body should be parallel to the couch/mat. With adequate muscle strength, men should maintain this position for 124 +/- 72s and Women for 83 +/- 63s.[rx]
Supine Bridge – The patient is supine and flexes the hip and knee to keep the feet flat on the couch/mat. The arms are flexed to position the hands beside the ears. The lower part of the torso and pelvis is lifted off the couch/mat, to maintain the trunk and the thigh in a straight line. With adequate muscle strength, men should maintain this position for 188 +/- 45s and Women for 152 +/- 30s. [rx]
Clinical Tests For Instability for PLID
Aberrant movement on flexion-extension – The standard examination involves documenting the range of movement. The quantitative range of movement may not be as significant as the qualitative range of movement. The important feature of spinal instability is the aberrant motion that occurs when flexing and extending the spine. A catch, a painful arc, supporting the arms on the thighs, or a reversal of the lumbopelvic rhythm when standing from the flexed posture indicates instability.[rx]
Passive lumbar extension test – The subject lies on the examination couch. The examiner passively lifts the lower limbs to a height of 30 cm from the coach while maintaining the knee in extension and applying gentle traction on the legs. A positive test is recorded if the patient complains of “pain in the lower back region” or complains of “heaviness in the lower back” or complains that, “the lower back is coming off.” These experiences should return to normal when the leg returned to the couch. The passive lumbar extension test has the highest combined sensitivity and specificity and may be comparable to radiological findings to identify lumbosacral structural instability.[rx]
The prone instability test – The patient stands at the foot end of the examination couch. The patient then lowers his/her upper body to rest on the examination couch. The iliac crest should rest on the edge of the examination couch. The patient holds the sides of the examination couch for increased stability. In the first part of the test, the feet of the patient is resting on the ground. The examiner with the heel of his/her hand creates a small posterior to anterior trust at each segment of the lumbar spine. Pain, if experienced by the patient, is recorded. In the second part of the test, the patient is asked to lift the feet of the floor and steady himself /herself by holding onto the sides of the examination couch. The examiner again repeats the posterior to anterior trust with the heel of his/her hand at each lumbar segment. The test is positive if the pain created in the initial part of the test subsides when the extensor muscles of the spine are tensed by lifting the feet of the floor.[rx]
Clinical Tests For Endurance in PLID
Sorensen test – The legs of the patient are strapped onto a low platform, which is only 25 cms above the floor. The upper end of the iliac crest is aligned to the edge of the table. The upper torso rests on the floor. At the commencement of the test, the patient extends the spine and lifts the upper torso off the floor with the arms crossed across the chest, and is asked to maintain the horizontal position. The record of the time, the patient can maintain this position is documented. Normative values: Men 146 +/- 51. Women 189 +/- 60.[rx]
Prone isometric chest raise – The patient lies prone on the examination couch with a pad underneath the abdomen and the arms along the sides. The patient is instructed to lift the upper trunk about 30 degrees from the table while keeping the neck flexed, and the intention is to hold the sternum of the surface of the couch. The clinician records the maximum time that the patient can hold this position. [rx]Normative values: Men 40 +/- 9. Women 52 +/- 18.[rx]
Prone double straight leg raise – The patient lies prone on the examination couch with the hips extended and the hands underneath the forehead. The arms are perpendicular to the body. The patient is then requested to lift both the legs off the couch until the knee is cleared off the couch. The patient should maintain normal breathing during the entire test procedure. The examiner can monitor the knee clearance by sliding a hand under the knee. The clinician records the maximum time that the patient can hold this position. Normative values: Men 38 +/- 6. Women 35 +/- 5. The prone double straight leg raise has shown to have great sensitivity and specificity. [rx]
Supine static chest raise – The patient lies supine on the couch with the legs extended. The hands are placed on the temples with the elbows pointing to the ceiling. The patient is then instructed to lift the head, the arms and the upper trunk of the couch. The patient should maintain normal breathing during the entire test procedure. The clinician records the maximum time that the patient can hold this position. Normative values: Men 43 +/- 9. Women 32 +/- 5. [rx]
Supine double straight leg raise – The patient lies supine with the legs extended, and the arms crossed in front of the chest. The pelvis is tilted forward to increase the lumbar lordosis. The patient is then requested to lift both the legs of the floor for 30 degrees while maintaining normal breathing during the entire test procedure. To monitor the pelvic tilt, the examiner can place one hand under the lumbar spine. The clinician records the maximum time that the patient can hold this position. Normative values: Men 28 +/- 4. Women 28 +/- 4. [rx]
Flexor endurance test – The patient is supine on the couch with the upper part of the body propped up on a support. The support is at an angle of 60 degrees. The legs are flexed so that the knee is at a 90-degree angle with the foot flat on the couch. The toes and feet are strapped to the couch to provide a counterbalance. In a modified procedure, the examiner sits on the edge of the couch and over the toes of the patient to provide a counterbalance. The arms are crossed across the chest towards the opposite shoulder. The support is moved back by 10 cms, and the patient is instructed to maintain the original position. The clinician records the maximum time that the patient can hold this position. Normal values: Men 144 +/- 76, Women 149 +/- 99 in normal subjects.[rx]
Prone Plank/Bridge – The patient lies prone on a mat. Initially, the patient lifts his / her upper torso off the mat and steadies on the elbows and forearms. The elbow is directly below the shoulder, and the forearms are straight with hands in front of the elbow. The patient then lifts the pelvis off the mat. The body is now supported on the elbow/forearm and the tips of the toes. The patient maintains a rigid horizontal position parallel to the floor. The clinician records the maximum time that the patient can hold this position. Normative values: Men 124 +/- 72s, Women 83 +/- 63s.[rx]
Supine Bridge – The patient lies supine with the legs flexed so that the knee is at a 90-degree angle, and the foot is flat on the couch but not touching each other. The elbows are bent, and the hands are placed on the ears. The patient then lifts the pelvis so that the shoulders, hips, and knees are in a straight line. A rigid position is maintained, and the clinician records the maximum time that the patient can hold this position. Normative values: Men 188 +/- 45s, Women 152 +/- 30s.[rx]
Side Plank/Bridge – The patient lies on the side on a mat. The upper part of the body is lifted off the mat and supported on the elbow of the arm below. The opposite (upper) arm crosses across the chest onto the lower shoulder. The top foot is positioned in front of the lower foot. The patient is then instructed to lift the pelvis off the floor and to maintain the trunk and the legs in a straight line. A rigid position is maintained, and the clinician records the maximum time that the patient can hold this position. Normative values: Men 95 +/- 35s, Women 74 +/- 33s.[rx]
Waddell Signs for PLID Include
Superficial tenderness – The patient’s skin over a wide area of the lumbar skin is tender to light touch or pinch.
Non-anatomical tenderness – The patient experiences deep tenderness over a wide area that is not localized to one structure and crosses over non-anatomical boundaries.
Axial loading – Downward pressure on the top of the patient’s head elicits lumbar pain.
Acetabular rotation – Lumbar pain is elicited while the provider passively and simultaneously externally rotates the patient’s shoulder and pelvis together in the same plane as the patient stands. It is considered a positive test if pain occurs within the first 30 degrees of rotation.
Distracted straight leg raises discrepancy – The patient complains of pain during a straight leg raise during formal testing, such as when supine, but does not on distraction when the examiner extends the knee with the patient in a seated position.
Regional sensory disturbance –The patient experiences decreased sensation fitting a stocking-like distribution rather than a dermatomal pattern.
Regional weakness – Weakness, cogwheeling, or the giving way of many muscle groups that are not explained on a neuroanatomical basis.
Overreaction – A disproportionate and exaggerated painful response to a stimulus that is not reproduced when the same provocation is given later. These responses can include verbalization, facial expression, muscle tension, or tremor.[trx],[rx]
Observation of posture and function for Diagnosis of PLID
In standing her shoulders lumbar paraspinal muscles – It is shunted to the left side, her back was extended and pelvis anteriorly tilted, and there was visible hyper-tonicity of the lumbar paraspinal muscles weakness in PLID.
This shunted antalgic posture – is commonly referred to as a lumber list. Observation of a lumber list, unfortunately, is a test lacking in reliability (Clare, Adams, & Maher, 2003). Maitland (2005), however, teaches us that if a person presents with an observable postural deformity in PLID, they are going to be more challenging to get better. In Sally’s case, she had a contralateral list (shoulders listed to the opposite side of back/leg pain), which is thought to respond more favorably to treatment than an ipsilateral list.
Kyphosis-lordosis posture– Head held forwards, neck hyperextended, thoracic spine in long kyphosis, lumbar spine lordotic, pelvis tilted anteriorly, hips flexed, and knees hyperextended.
Swayback posture– Head held forwards, neck hyperextended, thoracic spine in long kyphosis, lumbar spine flattened or slightly flexed, pelvis tilted posteriorly, hips hyperextended, knees hyperextended and ankle in neutral.
Military type posture– Head neutral, neck straight, thoracic spine neutral or flattened, lumbar spine hyperextended, pelvis tilted anteriorly, knees hyperextended and ankles slightly plantarflexed.
Flatback posture– Head held forwards, neck slightly extended, upper thoracic spine flexed, lower thoracic spine and lumbar spine flattened, pelvis tilted posteriorly, hips extended, knees hyperextended with plantarflexed ankles or knee flexed with the ankle in dorsiflexion.
Femoral stretch test – While lying face down, your doctor will flex each knee to determine if you feel pain in your thigh. If you do, this indicates nerve compression in your lumbar spine.
Schober test – This test examines the range of motion in your lumbar spine. During this test, you will bend over, as if you are trying to touch your toes.
Trendelenburg test – This test can identify weakness in the muscles that support the hip. In this test, you’ll stand straight on one leg for 30 seconds. Your doctor will observe if your pelvis stays level.
In my experience antalgic postures – are very important to detect because they indicate a protective position; a mechanism which the body is adopting (often subconsciously) in the acute phase of injury to protect the injury, and if the antalgic posture is not carefully examined and carefully corrected, it can make the patient a lot worse.
Movement tests – Tests that assess the spine’s range of motion may include bending the neck or torso forward, backward, or to the side. Additionally, if raising one leg in front of the body worsens leg pain, it can indicate a lumbar herniated disc (straight leg raise test).
Muscle strength – A neurological exam may be conducted to assess muscle strength and determine if a nerve root is compressed by a herniated disc. A muscle strength test may include holding the arms or legs out to the side or front of the body to check for tremors, muscle atrophy, or other abnormal movements.
Reflex test – Nerve root irritation can dampen reflexes in the arms or legs. A reflex test involves tapping specific areas with a reflex hammer. If there is little or no reaction, it may indicate a compressed nerve root in the spine.
Active range of movement
Lumbar flexion P2 (right-sided low back pain) R`(upper thigh).
Extension P2 (right buttock and leg pain) R` (vertical).
Other movements were not assessed on day 1 due to severity and irritability.
Neurological examination
Weak single leg calf raises (SLCR) and was only able to perform three assisted raises to 50% range. Gr 5 strength of right leg SLCR x5 repetitions.
No other myotomal weakness was detected.
The S1 reflex on the right side was absent, with other lower limb reflexes being preserved.
No sensory changes were noted.
Neurodynamic Examination
The straight leg raise test (SLR) was positive in reproducing Sally’s posterior thigh pain and limited at 20 degrees on the right side.
Her left SLR was limited by hamstring tightness at 50 degrees.
The research suggests the SLR reliable re-assessment asterisks for patient progress. It has been shown to be 91% sensitive and 26% specificity in detecting lumbar disc pathology.D Neville et al. (2020) found that more than an 11-degree discrepancy in hip flexion range between sides was a clinically significant result. Compared to MRI, the SLR test has poor diagnostic accuracy and therefore is often used in conjunction with such imaging.
[stextbox id=’info’]
Location of Pain and Motor Deficits in Association with Nerve Root Involvement at Each Lumbar Disc Level
DISC LEVEL
LOCATION OF PAIN
MOTOR DEFICIT
T12-L1
Pain in the inguinal region and medial thigh
None
L1-2
Pain in the anterior and medial aspect of the upper thigh
Slight weakness in quadriceps; slightly diminished suprapatellar reflex
L2-3
Pain in the anterolateral thigh
Weakened quadriceps; diminished patellar or suprapatellar reflex
L3-4
Pain in the posterolateral thigh and anterior tibial area
Weakened quadriceps; diminished patellar reflex
L4-5
Pain in the dorsum of the foot
Extensor weakness of big toe and foot
L5-S1
Pain in the lateral aspect of the foot
Diminished or absent Achilles reflex
[/stextbox]
Diagnosis For Straight Leg Raise Test (SLR Test)
Straight leg raise
Medical diagnostics
Straight Leg test sometimes used to help diagnose a lumbar herniated disc
A Cross-sectional study by Boyd and Villa (2012) examined normal asymmetries between limbs in healthy, asymptomatic individuals during SLR testing and the relationship of various demographic characteristics. The authors concluded that the overall range of motion during SLR was related to sex, weight, BMI and activity level, which is likely reflected in the high variability documented.
We can be 95% confident that inter-limb differences during SLR neurodynamic testing fall below 11 degrees in 90% of the general population of healthy individuals. In addition, inter-limb differences were not affected by demographic factors and thus may be a more valuable comparison for test interpretation.
Rabin et al. have shown the sensitivity of the SLR test to be.
Deville et al. found the specificity to be.
A systematic review of the Clinical utility of SLR by Scaia V, Baxter D, and Cook C (2012) investigated the diagnostic accuracy of a finding of pain during the straight leg raise test for lumbar disc herniation, lumbar radiculopathy, and/or sciatica.
The authors concluded that Variability in reference standard may partly explain the inconsistencies in the diagnostic accuracy findings.
Further, pain that is not specific to lumbar radiculopathies, such as that associated with hamstring tightness, may also lead to false positives for the SLR; and may inflate the sensitivity of the test.
Lab Test For Diagnosis of PLID
A doctor can diagnose cauda’s low back pain or PLID. Here’s what you may need to confirm a diagnosis
Elevated ESR– could indicate infection, malignancy, chronic disease, inflammation, trauma, or tissue ischemia.
Elevated CRP– levels are associated with infection.
RBS –To diagnosis, diabetes and it related health problem, burning sensation etc
Rheumatoid factor and anti-CCP – cyclic citrullinated peptide antibodies test should be increased if there is clinical abnormality for PLID or right and left side back pain are found.
A serum uric acid level – It is often considered by clinicians and doctors when PLID is suspected, but it is not a reliable and dangerous condition of your kidney as it may be spuriously elevated or high in acute inflammatory conditions or acutely during an attack or not.
Serologicstudies – There are no blood tests used to specifically support the diagnosis of nerve compression, demyelination but the use of these tests may be necessary for medical conditions that can either increase nerve compression or can decrease their symptoms. Some of the most frequently find conditions include diabetes and hypothyroidism. The assessment of a patient’s fasting blood glucose, hemoglobin A1c, or thyroid function tests may be helpful in the general management of the patient. Other conditions that could mimic nerve compression include deficiency of vitamin B12 or folate, vasculitides, and fibromyalgia.
Synovial fluid analysis – A joint arthrocentesis or the system of aspiration of synovial fluid with blood and synovial fluid analysis that are mandatory if an infection is suspected or dangerous. Such as the patients should also be started properly treatment by using empiric antibiotic therapy as soon as possible if the synovial fluid sample is obtained from the lumber joint. The fluid analysis or any kinds of abnormalities is also helpful in diagnosing crystal formation with osteophyte and steroid-induced arthritis. The degree of the high elevation of synovial fluid are founded by WBC count can be useful in differentiating inflammatory abnormality or from non-inflammatory causes of right and left side neck pain.
Imaging Test For PLID
X-rays – can show the alignment of the bones and whether the patient has arthritis or broken bones. They are not ideal for detecting problems with muscles, the spinal cord, nerves, or disks.
Computed Tomography (CT) scan – is a noninvasive test that uses an X-ray beam and a computer to make 2-dimensional images of your spine. It may or may not be performed with a dye (contrast agent) injected into your bloodstream. This test is especially useful for confirming which bulging disc is damage and is good for revealing herniated disks or problems with tissue, tendons, nerves, ligaments, blood vessels, muscles, and bones.
Bone scan– a bone scan may be used for detecting bone tumors or compression fractures caused by brittle bones (osteoporosis). The patient receives an injection of a tracer (a radioactive substance) into a vein. The tracer collects in the bones and helps the doctor detect bone problems with the aid of a special camera.
Magnetic Resonance Imaging (MRI) scan – is a noninvasive test that uses a magnetic field and radiofrequency waves to give a detailed view of the soft tissues of your spine with a bulging disc. Unlike an X-ray, nerves and discs are clearly visible. It may or may not be performed with a dye (contrast agent) injected into your bloodstream. An MRI can detect which disc is damaged and if there is any nerve compression. It can also detect bony overgrowth, spinal cord tumors, or abscesses.
A myelogram – is a specialized X-ray where dye is injected into the spinal canal through a spinal tap. An X-ray fluoroscope then records the images formed by the dye. The dye used in a myelogram shows up white on the X-ray, allowing the doctor to view the spinal cord and canal, PLID, a bulging disc in detail. Myelograms can show a nerve being pinched and a bulging disc by a herniated disc, bony overgrowth, spinal cord tumors, and abscesses.
Electromyography (EMG) & Nerve Conduction Studies (NCS) – EMG tests measure the electrical activity of your muscles. Small needles are placed in your muscles, and the results are recorded on a special machine. NCS is similar, but it measures how well your nerves pass an electrical signal from one end of the nerve to another. These tests can detect nerve damage and muscle weakness and a bulging disc and PLID. [rx][rx]
Discogram – A discogram may be recommended to confirm which bulging disc and PLID is painful if surgical treatment is considered. In this test, the radiographic dye is injected into the disc to recreate disc pain from the dye’s added pressure. It is useful for the evaluation of patients who are experiencing cervical discogenic pain or have multiple herniations in which surgery is a strong possibility. However, the diagnostic procedure remains controversial as it may accelerate the degeneration of normal discs.[rx]
CT myelogram – CT is most useful when combined with the injection of intrathecal contrast (myelography) to better evaluate the location and amount of neural compression. It is more invasive than an MRI but can be a consideration in patients who have a contraindication to MRI (e.g., pacemaker) or have an artifact from the hardware.
Cerebrospinal fluid analysis– is a useful test if there is a suspected neoplasm or infectious cause or radiculopathy symptoms. The recommendation for a lumbar puncture is in the case of a patient with negative or nondiagnostic neuroimaging, without known primary cancer, who has progressive neurological symptoms and has failed to improve promptly.[rx]
Bone scintigraphy – with single-photon emission computed tomography (SPECT) is more sensitive in detecting facet joint lesions and allows more accurate anatomical localization. A recent study suggested that SPECT could help to identify patients with low back pain, PLID who would benefit from facet joint injections [rx].
Foraminal nerve root entrapment test – is best visualized on T1-weighted MRI where the high contrast between fat tissue and the nerve root sheath is of great help. Usually, a combination of hypertrophic degenerative facets with osteophytes spurs posteriorly, and vertebral osteophytes and PLID/or disc herniation anteriorly diminish the anteroposterior diameter of the foramen. Foraminal height is lessened by degenerative disc disease and subsequent disc height loss. Whenever the normal rounded (oval) appearance of the nerve root sheath is lost in combination with loss of the surrounding fat tissue, nerve root compression should be considered.
Urodynamic studies – may be required to monitor the recovery of bladder function following decompression surgery.
Electrodiagnostic studies – Electromyography and nerve conduction test studies help to localize the nerve problem involved as well as where along the course of the nerve it is affected. Additionally, testing can serve as a baseline for comparison with the future during the course of treatment. It is important to note that normal electrodiagnostic studies do not identify disease, and clinical correlation should include the patient’s history and physical examination findings.[rx]
In most cases of low back pain, medical consensus advises not seeking an exact diagnosis but instead beginning to treat the pain. This assumes that there is no reason to expect that the person has an underlying problem. In most cases, the pain goes away naturally after a few weeks. Typically, people who do seek diagnosis through imaging are not likely to have a better outcome than those who wait for the condition to resolve.
Treatment of PLID
Non-surgical
Rest – It is important that the patient take proper rest and sleep and avoid any activities which will further aggravate the disc bulge and its symptoms. Many minor disc bulges can heal on their own with rest and other conservative treatments.
Cervical Pillow – It is important to use the right pillow to give your neck the right type of support for healing from a cervical and lumbar disc bulge and also to improve the quality of sleep. Specific treatment for lumbar disk disease will be determined by your health care provider based on
Your age, overall health, and medical history
The extent of the condition
Type of condition
Your tolerance for specific medications, procedures, or therapies
Expectations for the course of the condition
Your opinion or preference
Typically, conservative therapy is the first line of treatment to manage lumbar disk disease. Approach for Treating and Reversing a Disc Bulge about half of the disc bulges heal within six months and only about 10% of the disc bulges require surgery. So, the good news is that conservative treatment for a disc bulge helps in treating as well as reversing the disc bulges.
Ice & Moist Heat Application – Ice application where the ice is wrapped in a towel or an ice pack for about 20 minutes to the affected region, thrice a day, helps in relieving the symptoms of a disc bulge. Heat application in the later stages of treatment also provides the same benefit.
Hot Bath – Taking a hot bath or shower also helps in dulling the pain from a disc bulge. Epsom salts or essential oils can be added to a hot bath. They will help in soothing the inflamed region.
Traction – traction is the best essential treatment for bulging discs, pinched nerves, radiating pain management. It can be done in a manual and dynamic way to relieves pain in bulging discs.
Massage therapy – may give short-term pain relief, but not functional improvement, for those with acute lower back pain. It may also give short-term pain relief and functional improvement for those with long-term (chronic) and sub-acute lower back pain, but this benefit does not appear to be sustained after 6 months of treatment. There does not appear to be any serious adverse effects associated with massage.
Heating and cooling – This includes the use of hot packs and heating patches, a hot bath, going to the sauna or using an infrared lamp. Heat can also help relax tense muscles. Cold packs, like cold wraps or gel packs, are also used to help soothe irritated nerves.
Acupuncture– may provide some relief for back pain. However, further research with stronger evidence needs to be done.
Spinal manipulation – is a widely-used method of treating back pain, although there is no evidence of long-term benefits.
Back school – is an intervention that consists of both education and physical exercises. A 2016 Cochrane review found the evidence concerning back school to be very low quality and was not able to make generalizations as to whether the back school is effective or not.
Patient education – on proper body mechanics (to help decrease the chance of worsening pain or damage to the disk)
Hot tub therapy – is a tried-and-true method of relieving stress, relaxing muscles, and experiencing renewal through warm water immersion. It is an ancient practice. People have been enjoying warm water immersion for centuries. Ancient Egyptians, Greeks, and Romans, for example, built palaces around natural hot springs.
Physical therapy – which may include ultrasound, massage, conditioning, and exercise. The goal of physical therapy is to help you return to full activity as soon as possible and prevent re-injury. Physical therapists can instruct you on proper posture, lifting, and walking techniques, and they’ll work with you to strengthen your lower back, leg, and stomach muscles. They’ll also encourage you to stretch and increase the flexibility of your spine and legs. Exercise and strengthening exercises are key elements to your treatment and should become part of your life-long fitness.
Over the Door Traction – This is a very effective treatment for a disc bulge. It helps in relieving muscle spasms and pain. Typically a 5 to 10-pound weight is used and it is important that patients do this under medical guidance.
Weight control – By keto diet or maintaining or changing the food habit to reduce the weight not any movement during the time of acute pain.
Use of lumbosacral back support – It is helpful for back support during any travels or everyday natural movement. It also helps to straighten the lumbar spine.
Holistic therapies – Some patients find acupuncture, acupressure, nutrition/diet changes, meditation, and biofeedback helpful in managing pain as well as improving overall health.
Braces – For patients with chronic back pain, PLID, or a deformity in the spine, the doctor may recommend wearing a brace to provide support. Back braces can help to maintain proper posture, limit strenuous movement, and realign the spine to provide relief from pain.
Reiki – Reiki is a Japanese treatment that aims to relieve pain by using specific hand placements.
Moxibustion – This method is used to heat specific points on the body by placing heated needles or glowing sticks made of mugwort (“Moxa”) close to those points.
Pilates – A total body workout in which strengthening the deep core muscles is key.
Tai chi – Originally an Asian martial art, tai chi is now practiced with slow, flowing movements. It can improve your balance and coordination skills, strengthen your muscles, and is said to help you relax your body and mind.
Going on walks – Initial research suggests that going on a walk or brisk walking (Nordic walking) can help relieve back pain if done regularly – for instance, every two days for 30 to 60 minutes.
Alexander Technique – The Alexander Technique is a taught self-care discipline that enables an individual to recognize, understand, and avoid habits adversely affecting muscle tone, coordination, and spinal functioning. Priority is given to habits that affect freedom of poise of the head and neck and that lead to stiffening and shortening of the spine, often causing or aggravating the pain.
Eat Nutritiously During Your Recovery – All bones and tissues in the body need certain nutrients in order to heal properly and in a timely manner. Eating a nutritious and balanced diet that includes lots of minerals and vitamins are proven to help heal back pain of all types. Therefore focus on eating lots of fresh produce (fruits and veggies), whole grains, lean meats, and fish to give your body the building blocks needed to properly healing PLID. In addition, drink plenty of purified water, milk, and other dairy-based beverages to augment what you eat.
In bulging disc needs ample minerals (calcium, phosphorus, magnesium, boron) and protein to become strong and healthy again.
Excellent sources of minerals/protein include dairy products, tofu, beans, broccoli, nuts and seeds, sardines, and salmon.
Important vitamins that are needed for bone healing include vitamin C (needed to make collagen), vitamin D (crucial for mineral absorption), and vitamin K (binds calcium to bones and triggers collagen formation).
Conversely, don’t consume food or drink that is known to impair bone/tissue healing, such as alcoholic beverages, sodas, most fast food items, and foods made with lots of refined sugars and preservatives.
Medications
Analgesics – It is basically paracetamol with prescription-strength drugs that relieve pain but not inflammation.
Calcium & vitamin D3 – To improve bone health and healing fracture. As a general rule, men and women age 50 and older should consume 1,200 milligrams of calcium a day, and 600 international units of vitamin D a day.
Glucosamine & Diacerein, Chondroitin sulfate – can be used to tightening the loose tendon, cartilage, ligament, and cartilage, ligament regenerates cartilage or inhabits the further degeneration of cartilage, ligament. The dosage of glucosamine is 15oo mg per day in divided dosage and chondroitin sulfate approximately 500mg per day in different dosages may be taken.[rx]
Vitamin B1, B6, and B12 – It is essential for neuropathic pain management, pernicious anemia, with vitamin b complex deficiency pain, paresthesia, numbness, itching with diabetic neuropathy pain, myalgia, etc.
Dietary supplement – A dietary supplement is a manufactured product intended to supplement one’s diet by taking a pill, capsule, tablet, powder, suspension, or liquid to remove general weakness & improved health.[rx] A supplement can provide micronutrients either extracted from plants, seafood sources that are synthetic in order to increase the quantity of their consumption PLID. The class of nutrient compounds includes all kinds of vitamins, minerals, fiber, fatty acids, and amino acids.
Antidepressants – A drug that blocks pain messages from your brain and boosts the effects of endorphins (your body’s natural painkillers).
Corticosteroid – to healing the nerve inflammation and clotted blood in the joints. Steroids may be prescribed to reduce the swelling and inflammation of the nerves. They are taken orally (as a Medrol dose pack) in a tapering dosage over a five-day period. It has the advantage of providing almost immediate pain relief within a 24-hour period.
Topical Medications – These prescription-strength creams, gels, ointments, patches, and sprays help relieve pain and inflammation through the skin.
Triamcinolone acetonide Injection with local anesthesia – In lumbar epidural analgesia, the medication is injected into what is known as the epidural space (“epidural injection”). The epidural space surrounds the spinal cord and the spinal fluid in the spinal canal. This is also where the nerve roots are located. During this treatment, the spine is monitored using computer tomography or C- arms electromyography to make sure that the injection is placed at exactly the right spot.[rx]
Chemonucleolysis and chymopapain – Chemonucleolysis is a technique that is now rarely used. It attempts to decrease the volume of disc herniation by reducing the amount of material contained within the nucleus pulposus by injecting the enzyme chymopapain. Some scientific, systematic review of a lumbar discectomy with percutaneous treatments identified three RCTs that compared chymopapain with other placebo injections and reported that symptom relief was greater in the group that received chymopapain.[rx]
Collagenase Injection – Collagenase injections provide an invasive treatment derived from Clostridium histolyticum. The injection is a form of the enzyme is a metalloprotease that lyses in collagen (sparing Type IV collagen which is needed in the basement membrane of blood vessels and nerves). Treatment typically consists of 0.25 mL for contracture muscle into the spinal cord and 0.20 mL are injected in the PLID rehabilitation stage to prevent contractures delivered subcutaneously directly into the spinal cord with a needle. The affected area is manipulated under local anesthesia at 24 to 48 hours after injection. Collagenase injections have been shown to effectively result in a 75% in post-operative back muscle contracture reduction with a 35% recurrence rate. Complications of injections include edema, swelling skin tearing, tendon rupture, complex regional pain syndrome, and pulley rupture, etc.[rx]
Steroid injections – The procedure is performed under x-ray fluoroscopy and involves an injection of corticosteroids and a numbing agent into the epidural space of the spine. The medicine is delivered next to the painful area to reduce the swelling and inflammation of the nerves. About 50% of patients will notice relief after an epidural injection, although the results tend to be temporary. Repeat injections may be given to achieve the full effect. Duration of pain relief varies, lasting for weeks or years. Injections are done in conjunction with physical therapy and/or a home exercise program.
Caution: individuals with diabetes and those who may be predisposed to diabetes should note that prolonged use of corticosteroids can make it difficult to regulate insulin levels.
Surgical Treatment
There are a number of surgical procedures performed on the lumbar spine, especially for degenerative, infective, and traumatic spinal conditions. A few of them are:
When these conservative measures fail, surgery for the removal of a herniated disk may be recommended. Surgery is done under general anesthesia. An incision is placed in the lower back over the area where the disk is herniated. Some bone from the back of the spine may be removed to gain access to the area where the disk is located. Typically, the herniated part of the disk and any extra loose pieces of a disk is removed from the disk space.
Microdiscectomy – for a herniated disc, a minimally invasive procedure in which the herniated portion of the disc is removed.
Artificial disc replacement – for degenerative disc disease and herniated discs is a minimally invasive procedure that replaces a damaged disc with a specialized implant that mimics the normal function of the disc, maintaining mobility.
Spinal fusion– fusion for degenerative disc disease, in which the disc space is fused together to remove motion at the spinal segment. Spinal fusion involves setting up a bone graft, as well as possible implanted instruments, to facilitate bone growth across the facet joints. Fusion occurs after the surgery.
Open Back Surgery – Traditionally, bulging discs are treated with an open back procedure, meaning the surgeon makes a large incision into the skin and cuts muscle and surrounding tissue to gain access to the problematic disc. This traditional surgical option is invasive, requires overnight hospitalization, general anesthesia, and requires a lengthy recovery coupled with strong pain medication.
Endoscopic Surgery – Fortunately, you have a second option with endoscopic spine surgery. Thanks to the advancement of surgical technology a bulged disc surgery can be performed using endoscopic procedures, meaning the surgeon makes a small incision to insert special surgical tools. During an endoscopic bulging disc operation, the surgeon uses a tiny camera to visualize and gain access to your damaged disc. This minimally invasive new approach offers shorter recovery, easier rehabilitation, and a much higher success rate than open back or neck surgery. A local anesthetic is all that is usually required.
Percutaneous Endoscopic Discectomy – With the increasing use of endoscopic surgical techniques in spinal surgery, PED was introduced to the treatment of pediatric LDH [Rx]. Two relevant articles published by Mayer et al. [Rx] (4 cases) and Lee et al (46 cases) were obtained from the literature search. PED was associated with a short-term success rate of 91.3 and 100% respectively, without complications such as leakage of CSF, nerve root injury, interspace infection, etc. The long-term follow-up is yet to be reported. Their recommended indications of PED for pediatric LDH include
(1) failure of 6 weeks of conservative treatment;
(2) a comparatively intact disc;
(3) subligamentous protruded or extruded disc. The minimally invasive nature of PED means less surgical trauma and shorter hospital stay. Its success, however, requires a correct selection of patients and the surgeon being able to master the surgical procedure.
Open Discectomy – Discectomy remains the most used surgical procedure for LDH in children and adolescents as well as in adults. It is generally agreed in the literature that posterior discectomy with partial laminotomy is indicated for posterolateral disc herniation, whereas hemilaminectomy or laminectomy is required in cases of central disc herniation. There were also reports of successful use of extraperitoneal anterolateral discectomy on a centrally protruded disc [Rx].
Others Treatment
Intradiscal therapy
Although there are various forms of intradiscal therapy available for adult LDH, similar reports on children and adolescents are comparatively sparse. According to the literature, chemonucleolysis was the only form of intradiscal therapy reported being used on children and adolescents.
Although FDA approval for chymopapain use in humans has long been withdrawn, it is still being manufactured and in clinical use in Korea, Canada, Australia, UK, and three states in the US [rx]. In comparison with surgery, chemonucleolysis is advantageous in that it is associated with less trauma and post-operative adhesion, shorter hospital stay, earlier remobilization, and lower cost.
Sixty percent of people with sciatica who didn’t get relief from other therapies and then tried spinal manipulation experienced the same degree of pain relief as patients who eventually had surgery, found a 2010 study in the Journal of Manipulative and Physiological Therapeutics.
The 120 people in the study saw a chiropractor about 3 times a week for 4 weeks and then continued weekly visits, tapering off treatment as they felt better.
In people who responded to chiropractic care, benefits lasted up to a year. “spinal manipulations may create a response in the nervous system that relieves pain and restores normal mobility to the injured area,” says study researcher Gordon McMorland, DC, of National Spine Care in Calgary, Alberta. “It also reduces inflammation, creating an environment that promotes the body’s natural healing mechanisms.
You can get relief as soon as the first session, though it takes about 12 sessions to see improvement,” says Jingduan Yang, MD, assistant professor at the Jefferson Myrna Brind Center of Integrative Medicine at Thomas Jefferson University. A small study in the Journal of Traditional Chinese Medicine found that of 30 people with sciatica, 17 got complete relief and 10 saw symptoms improve with warming acupuncture, in which the needles are heated.
An ancient Indian practice that aims to improve your body awareness and health. Yoga typically involves getting into various positions or carrying out certain sequences of movements that aim to promote strength and flexibility, body awareness, and a good posture.
A study in the journal Pain reported that people with chronic back pain who practiced Iyengar yoga for 16 weeks saw pain reduced by 64% and disability by 77%. Although yoga’s effects on sciatica are less clear, gentle forms may be beneficial. By strengthening muscles and improving flexibility, a yoga practice can help sciatica sufferers “move and function better so they don’t fall into a posture that aggravates sciatica.
Massage
Don’t expect a chilled-out spa massage if you have sciatica. In this instance, trigger-point therapy is best, says Jeff Smoot, vice president of the American Massage Therapy Association. The sciatic nerve sits underneath a muscle called the piriformis, which is located beneath the glutes.
When the piriformis muscle gets tight, it pinches the sciatic nerve, causing tingling and numbness down into the leg, says Smoot. He applies pressure to irritated and inflamed areas, or trigger points, in the piriformis muscle, as well as in muscles in the lower back and glutes. Typically, Smoot schedules treatments 7 to 10 days apart. If patients don’t see progress by the fourth visit, they need to try another form of therapy, he says.
Topical Preparations
St. John’s wort oil, a liniment, is “one of my favorites for nerve pain, says Tieraona Low Dog, MD, director of the fellowship at the Arizona Center for Integrative Medicine. Apply the anti-inflammatory oil two or three times a day where there’s pain. Another option: an OTC cayenne pepper plaster or cream; capsaicin, found in chiles, hinders the release of pain-causing compounds from nerves. For severe cases, Low Dog uses the prescription chile patch Qutenza, designed for shingles pain. “One application is effective for weeks,” says Low Dog.
Ice or Heat
Because the sciatic nerve is buried deep within the buttock and leg, ice or heat on the surface of the body won’t ease that inner inflammation. But the time-honored treatments can act as counterirritants—that is, “they give your body other input in the painful area, and that brings the pain down a notch,” says Ruppert. Apply an ice pack or a heating pad as needed for 15 minutes.
Devil’s Claw
The herbal medication devil’s claw is “quite a potent anti-inflammatory, working like ibuprofen and similar drugs to inhibit substances that drive inflammation,” says Low Dog. She generally starts patients on 1,500 to 2,000 mg twice a day. Look for a brand that has a standardized extract of roughly 50 mg of harpagoside, the active compound. Safety reviews show that the supplement is well tolerated by most people but should be avoided by patients with peptic ulcers or on blood-thinning medications.
Physiotherapy in PLID
In stages, 1&2 of PLID physiotherapy must be applied to cure PLID. In the case of stages 3&4, physiotherapy can’t apply due to avoiding another case of foot drop.
Physiotherapy for a lumbar disc bulge
Physiotherapy treatment for a lumbar disc bulge is vital to ensure an optimal outcome and may comprise:
Soft tissue massage
Electrotherapy (e.g. ultrasound)
Lumbar taping
The use of a back brace
Mobilization
Traction
The use of a lumbar roll for sitting
Dry needling
Exercises to push the disc back ‘in’ and to improve strength, core stability, and flexibility
Education
Activity modification advice
biomechanical correction
Ergonomic advice
Clinical Pilates
Hydrotherapy
A functional restoration program
A gradual return to activity program
Physical therapy often plays a major role in herniated disc recovery. Its methods not only offer immediate pain relief, but also teach you how to condition your body to prevent further injury.
There are a variety of physical therapy techniques. Passive treatments relax your body and include deep tissue massage, hot and cold therapy, electrical stimulation (eg, TENS), and hydrotherapy.
Your physical therapy program will usually begin with passive treatments. But once your body heals, you will start active treatments that strengthen your body and prevent further pain. Your physical therapist will work with you to develop a plan that best suits you.
Passive Physical Treatments for Herniated Discs
Deep Tissue Massage – There are more than 100 types of massage, but a deep tissue massage is an ideal option if you have a herniated disc because it uses a great deal of pressure to relieve deep muscle tension and spasms, which develop to prevent muscle motion at the affected area.
Hot and Cold Therapy – Both hot and cold therapies offer their own set of benefits, and your physical therapist may alternate between them to get the best results. Your physical therapist may use heat to increase blood flow to the target area. Blood helps heal the area by delivering extra oxygen and nutrients. Blood also removes waste byproducts from muscle spasms. Conversely, cold therapy (also called cryotherapy) slows circulation. This reduces inflammation, muscle spasms, and pain. Your physical therapist may place an ice pack on the target area, give you an ice massage, or even use a spray known as fluoromethane to cool inflamed tissues.
Hydrotherapy – As the name suggests, hydrotherapy involves water. As a passive treatment, hydrotherapy may involve simply sitting in a whirlpool bath or warm shower. Hydrotherapy gently relieves pain and relaxes muscles.
Transcutaneous electrical nerve stimulation (TENS): A TENS machine uses an electrical current to stimulate your muscles. It sounds intense, but it really isn’t painful. Electrodes taped to your skin send a tiny electrical current to key points on the nerve pathway. TENS reduces muscle spasms and is generally believed to trigger the release of endorphins, which are your body’s natural painkillers.
Traction – The goal of traction is to reduce the effects of gravity on the spine. By gently pulling apart the bones, the intent is to reduce the disc herniation. The analogy is much like a flat tire “disappearing” when you put a jack under the car and take the pressure off the tire. It can be performed in the cervical or lumbar spine.
Active Treatments You May Try in Physical Therapy – Active treatments help address flexibility, posture, strength, core stability, and joint movement. An exercise program may also be prescribed to achieve optimal results. This will not only curb recurrent pain but will also benefit your overall health. Your physical therapist will work with you to develop a program based on your specific diagnosis and health history.
Core stability – Many people don’t realize how important a strong core is to their spinal health. Your core (abdominal) muscles help your back muscles support your spine. When your core muscles are weak, it puts extra pressure on your back muscles. Your physical therapist may teach you to core stabilizing exercises to strengthen your back.
Flexibility – Learning proper stretching and flexibility techniques will prepare you for aerobic and strength exercises. Flexibility helps your body move easier by warding off stiffness.
Hydrotherapy – In contrast to simply sitting in a hot tub or bath like its passive counterpart, active hydrotherapy may involve water aerobics to help condition your body without unnecessary stress.
Muscle-strengthening – Strong muscles are a great support system for your spine and better handle pain.
Your physical therapist will teach you ways to condition and strengthen your back to help prevent future pain. You may learn self-care principles so you understand how to best treat your symptoms. The ultimate goal is for you to develop the knowledge to maintain a pain-free lifestyle.
It’s essential that you learn how to exercise and condition your back after the formal physical therapy ends. If you don’t implement the lessons you learned during physical therapy, you won’t enjoy its long-term results. By taking care of your back on your own, you may prevent further herniated disc pain.
Reversal Treatment of PLID with Physical Therapy
The patient’s posture, standing, and sitting positions are also examined. The soft tissues surrounding the spine are also examined to look for abnormal temperature, texture, and tenderness for detecting any irritation, inflammation, and muscle spasms. Physical therapy combines therapeutic exercises, pain control techniques, massage therapy, and functional training practices, which help the patient by:
Physical therapy helps in easing the disc bulge to revert back to its normal position and in alleviating the inflammation and pain.
Physical therapy helps in increasing the blood circulation, oxygen, and nutrients to the spine.
Physical therapy helps in gently pushing the disc bulge back into its normal position in the spinal canal thus tries to reverse the process of the disc bulge.
Physical therapy strengthens the back and abdominal muscles, which provide enhanced support to the spine along with increasing spinal flexibility and strength.
The stretching and strengthening exercises of physical therapy helps in improving the spinal range of motion, flexibility, and strength.
Egoscue is a type of postural therapy, which is a series of gentle and targeted exercises that help in correcting musculoskeletal dysfunctions and other compensations that increase the risk of spinal injuries.
Physical therapy also helps in strengthening the back muscles which helps in preventing future injuries.
Physical therapy also helps in developing and maintaining a good posture.
Techniques of Physical Therapy for Treating and Reversing a Disc Bulge in PLID
Some of the common physical therapy techniques for relieving and reversing a disc bulge consist of:
A traction machine is used to apply traction to the spine which gently pulls on the muscles and joints and helps in easing the disc bulge back into its normal place.
Joint mobilization can be achieved by applying varying degrees of pressure to the spinal joints.
Electrical stimulation can also be used for relieving muscle spasms and pinched nerves.
The ultrasound device is used for sending high-frequency sound waves to the affected region. This helps in increasing blood flow, oxygen, and nutrients to the affected disc region and helps in relieving the symptoms of a disc bulge.
Infrared light therapy is another beneficial and effective treatment for treating the symptoms of a disc bulge. Daily use of an infrared heating pad for half an hour helps in relieving back pain for several hours without using any medication. Ordinary heating pads only heat the skin’s surface, whereas infrared heating pads penetrate deep into the tissues and are safe to use as it carries no risk of burns, skin drying, etc.
Far infrared (FIR) therapy is invisible to the naked eye and these rays can penetrate deep into the human body and improve the blood circulation in the affected region. This results in immediate pain relief along with boosting the healing process of a disc bulge.
Stretching exercises help in relieving and reversing the disc bulge along with increased strength and flexibility of the spine.
Proper posture of the body should be used for daily activities, such as bending, washing, and taking out the garbage.
It is also important to rest and avoid any physical activity which aggravates the condition.
Soft tissue massage also helps in relieving the symptoms of a disc bulge. Massage helps in relaxing the tight muscles, increasing blood circulation, and also increasing the production of endorphins. However, the use of massage therapy in the treatment of disc bulges or other disc problems is controversial and should be used with caution after a doctor’s approval.
Acupuncture is an alternative therapy that uses tiny needles that unleash the natural flow of energy in the body. Acupuncture helps in relieving the symptoms of a disc bulge.
Therapeutic massage along with heating packs applied to the affected region help in easing the stiffness and inflammation from a disc bulge. It is important to be careful when using heat applications. Heat should be avoided in the acute phase of an injury.
Spinal Decompression Therapy for Reversing a Disc Bulge in the Lower Back
For naturally healing or reversing a disc bulge, the space between the vertebrae needs to be increased. This encourages the bulged disc to revert back to its normal position. Increasing the intervertebral space also helps in rehydrating the disc, which in turn encourages the natural healing process of the affected spinal region along with decreasing any lower back pain, as the pain occurs as a result of nerve compression leading to inflammation of the lower back.
If the pressure is relieved by increasing the intervertebral space, then the pain also gets relieved. Spinal decompression is the name of the process, which helps you achieve this without any medication or surgery and allows the body to naturally heal on its own.
Different body positions affect the type of pressure exerted on our spinal discs. When a person is sitting, there is about 50% of increased pressure on the back compared to when standing in the right posture.
When a person is lying down, there is still around 25% of the standing body pressure on the spine because of the ligaments and muscles that support our back. Gravity decompression is done at an angle where about 60% of our body weight stretches the spine and its vertebrae decrease the pressure on the discs to almost a nil.
Spinal decompression can be done by 2 methods
Inversion Therapy
An inversion table can be used for spinal decompression and it helps in bringing great pain relief in many patients in less than a minute of its use. The long-term benefits of Inversion Therapy are that it helps in the relaxation of the back muscles, elongation of the spine so that there is more space for the discs to reverse back to their normal position.
It is important that the discs have adequate space to naturally rehydrate, realign and heal. This will help in shock absorption, spine flexibility, and improved posture.
Nubax Trio
This is a portable traction device and it is a very good alternative to inversion tables. It is equally effective in decompressing the spine as an inversion table and is smaller and more portable. The patient needs about 5 minutes of treatment daily on a Nubax Trio where the patient has to lean over this device and relax.
Chiropractic Spinal Adjustments for Treating and Reversing a Disc Bulge
This is an alternative therapy where a chiropractor determines the type of disc bulge the patient has and helps in diagnosing the underlying cause. After this, the chiropractor performs targeted spinal adjustments, which will help the realignment of the spinal discs and reversing the disc bulge.
Some of the chiropractic adjustments include flexion-distraction, physiotherapy, muscle stimulation, at-home exercises, stretches, and other treatments. Chiropractic adjustments help in relieving the symptoms of a disc bulge, such as neck stiffness, sciatica, and chronic low back pain.
The range of motion exercises helps in improving the range of motion of the neck and spine along with strengthening the spinal muscles and preventing the development of stiffness in the spine.
Best Exercises For PLID
Our spinal cord is supported by a number of muscles. Relevant exercises help relieve the pain and reduce the symptoms. Muscle exercises of those muscles associated with the affected area are necessary. Patients must know the region that has a slipped disc and then opt for exercises related to that muscle. The list of best exercises for the slipped disc are mentioned as follows:
Abdominal Isometrics – It can be performed either on the floor, mat, or bed. This exercise involves moving your lower back towards the surface at which you are performing this exercise. Leg movement must be reduced in this exercise and stomach muscles must be made active. This reduces pain in the lower back because of the attachment of abdominal muscles to the lower side of the vertebral column. Ten repetitions are effective.
Crunches – Lie on a flat surface with knees bent. Cross your arm under your head, raise your head and chest in such a manner that your rib cage curl interiorly towards your backbone. Perform this exercise slowly and gradually. In the beginning, perform fewer crunches and repeat it daily and increase the number of turns as you gain strength.
Lower back extension – Lie in an upside-down position, raise your upper body with the help of an elbow and hold up yourself in an elevated position for a short span of time, and then slowly lower down. Please make sure that during this exercise you do not raise your pelvis girdle (hip region).
Bilateral knee to the chest – Lay down on a flat surface and draw your knee towards your abdominal region, repeat it 5 times, and then switch leg. You can also increase the number of turns each time you repeat it.
Iso-hip flexion – Lay down over a flat surface and draw your knees towards your chest region in a 90-degree position with your stomach. Place your hands over your knees and then exert your hand pressure to lower your knee. Then utilize the knee pressure to resist the downward movement of your legs, in all both movements should just exert pressure and allow no movements. This position should be maintained for a few seconds and then lowered slowly and gradually.
Air bike – Sit on a chair with your chest and shoulders supported. Align your knees and feet together and then bring them towards your body and perform a pedaling motion in the air then repeat the same motion while moving your knees farther away from the body. Follow ten repetitions each time and increase its number as you gain strength.
Hamstring stretch – Lie on a flat surface with your knees bent, place your hands under your knees and then slightly pull your leg towards your chest, repeat it with another leg. This exercise must involve a stretch over the lower thigh muscle.
Lumbar roll – Lie on a flat surface with your knee bent and your feet lying on the floor then move your legs together towards the right side and then towards your left side. Repeating these movements 5 times on each side.
The above-mentioned best exercises for the slipped disc can be followed but if pain increases or muscle pain is persisting then quit these exercises right away. These exercises not only help in reducing the pain but also activate efficient muscle movement. Along with these exercise tips, proper body postures must be also maintained to prevent further disc damages.
Home Remady for Herniated Disc/Slip Disc
Positioning Yoga( only home practice)
Physiotherapy is a very cheap and good way of getting rid of a herniated disc itself. Therapists will teach you proper exercises and stretches which will improve the disc shape to a great extent. You will notice good differences while performing daily chores after just 4-5 sessions of therapy.
Turmeric
Turmeric contains curcumin which is a very good anti-oxidant and anti-inflammatory agent. This is why it stops the gel-like fluid inside the discs from coming out and bulge. It also shows antihistamine properties which help to reduce pain because of slowed blood circulation to the area of pain.
Dimethyl Sulfoxide (DMSO)
Dimethyl sulfoxide is a derivative from sulfur which has antioxidant properties as well as the organic sulfur present in it helps in the growth of new cells and detoxification of the body. The growth of new cells helps to replace the old cells of the discs and prevent the fluid from leaking outside.
Massage With Essential Oils
Massage with essential oils on the full-body, especially on the spine and lower back regions, will help in good blood circulation and promote the growth of new cells. It will help relieve pain and promote better absorption of oxygen and nutrients. Essential oils will also regenerate the cells of the disc and hence stop the disc from getting slipped.
Acupressure
In both techniques, pressure is used for relieving the pain from the swelled area. In acupressure fingers, hips and elbows are used and acupuncture needles are used. But this should be done with the help of an experienced practitioner and not alone. This is not recommended for patients having high blood pressure and for women who are pregnant.
TENS
TENS stands for Transcutaneous Electrical Nerve Stimulation and this is one of the best remedies for a herniated disc at home. This treatment uses a low voltage electric current which is applied to the affected area and helps the body to release endorphin which decreases the pain.
Cayenne Pepper
It is a very effective ingredient for the treatment of herniated discs. You can drink its tea or make a paste of the pepper using water and apply it to the affected area.
Diet
Diet is necessary to keep away all types of bad conditions that might affect you. Drink a lot of water and eat a balanced diet. Take excess of fibers and proteins. During this condition, you should avoid dairy products and red meat. Also, avoid fat-free foods.
Epsom Salt
Epsom salt is one of the widely used natural painkillers and anti-inflammatory agents. You can use this by adding 3-4 cups of salt in a hot water bath. Stay inside the bath for 15 minutes. It will help you achieve maximum relaxation. Do not use this remedy if you are diabetic or pregnant. If you are on any type of medication consult your doctor before bathing in Epsom salt.
Horsetail
Horsetail is a herb that has high quantities of minerals in it. It nourishes our tissues and has the ability to heal broken bones and torn ligaments. All you need to do is add some horsetail leaves to half a liter of water. Boil on low heat till the water quantity reduces to half its quantity. Cool the solution and filter it off. You can drink 5 ml of the solution thrice a day. It will heal herniated disc very fast.
California Poppy
California poppy is anti-inflammatory and analgesic in nature. This is what makes it a good treatment for a herniated disc. You can tear the leaves of the California poppy into small pieces and make a paste out of it using water. Use little hot water so that when you apply the paste to the affected area it is still warm.
White Willow Bark
White willow bark is used for reducing the discomfort of herniated discs. The chemical structure of these drugs shows a marked similarity to aspirin hence acts as an analgesic but doesn’t irritate your gut. It is also astringent and anti-inflammatory in nature. This herb might react with drugs hence do consult your doctor if you are on any kind of medication.
Comfrey Leaves
Comfrey leaves have the power to heal bones and connective tissues of the body. All you need to do is take some fresh leaves and add them to cold water. Let it remain undisturbed for around 12 hours. After 12 hours heat the above solution and filter it. Add the filtrate to bathwater and take a bath in it 2 times a day. Do not consume it orally because it contains hepatic-toxin alkaloids.
Boswellia
Boswellia is a naturally occurring painkiller that is a very effective remedy for a herniated disc. All you can do is make a decoction of Boswellia and consume it 2 times a day to reduce pain and discomfort associated with herniated discs. Boswellia is an organic painkiller that effectively treats the problem of a herniated disc. It is also an herbal cure for osteoarthritis.
Omega-3 Fatty Acids
Omega-3 Fatty acids are helpful in decreasing the inflammation and pain experienced due to herniated disc disorder. This acid forms the collagen which is used by the broken discs for repairing itself. Eat foods that are high in this kind of fat like fish, almonds, sprouts, and walnuts.
Colchicine
Colchicine is an active amino-alkaloid found in the plant of Kurchi or autumn crocus. This powder is obtained by crushing the seeds of the plant. It has anti-inflammatory properties that are effective against the slipped disc. Make a paste with kurchi powder and honey and consume it once a day. You can also make tea out of the powder or mix the powder in milk and have it once or twice a day.
Burdock
Burdock contains a lot of anti-oxidants which is helpful to detoxify the body and remove all kinds of harmful substances and decrease the pain and inflammation in your body. It also treats arthritis. Burdock can be consumed as a decoction once or twice a day.
Passionflower
Passionflower is helpful for slipped discs because the essential oils present is antispasmodic in nature. It reduces pain and inflammation. You can massage with passionflower essential oil or take capsules made from it, however, do consult your doctor before taking capsules.
Homeopathy For PLID & Back Pain
Primary Remedies
Aesculus – Pain in the very low back (the sacral or sacroiliac areas) that feels worse when standing up from a sitting position, and worse from stooping, may be eased with this remedy. Aesculus is especially indicated for people with low back pain who also have a tendency toward venous congestion and hemorrhoids.
Arnica montana – This remedy relieves lower back aches and stiffness from overexertion or minor trauma.
Bryonia – This remedy is indicated when back pain is worse from even the slightest motion. Changing position, coughing, turning, or walking may bring on sharp, excruciating pain. This remedy can be helpful for back pain after injury and backaches during illness.
Calcarea carbonica – This is often useful for low back pain and muscle weakness, especially in a person who is chilly, flabby or overweight, and easily tired by exertion. Chronic low back pain and muscle weakness may lead to inflammation and soreness that are aggravated by dampness and cold.
Calcarea phosphorica – Stiffness and soreness of the spinal muscles and joints, especially in the neck and upper back, may be relieved by this remedy. The person feels worse from drafts and cold, as well as from exertion. Aching in the bones and feelings of weariness and dissatisfaction are often seen in people who need this remedy.
Natrum muriaticum – Back pain that improves from lying on something hard or pressing a hard object (such as a block or book) against the painful area suggests a need for this remedy. The person often seems reserved or formal but has strong emotions that are kept from others. Back pain from suppressed emotions, especially hurt or anger may respond to Natrum muriaticum.
Nux vomica – This remedy is indicated for muscle cramps or constricting pains in the back. Discomfort is made worse by cold and relieved by warmth. The pain usually is worse at night, and the person may have to sit up in bed to turn over. Backache is also worse during constipation, and the pain is aggravated when the person feels the urge to move the bowels.
Rhus Toxicodendron – This remedy can be useful for pain in the neck and shoulders as well as the lower back when the pain is worse on initial movement and improves with continued motion. Even though in pain, the person finds it hard to lie down or stay still for very long, and often restlessly paces about. Aching and stiffness are aggravated in cold damp weather and relieved by warm applications, baths or showers, and massage.
Sulfur – This remedy is often indicated when a person with back pain has a slouching posture. The back is weak and the person feels much worse from standing up for any length of time. Pain is also worse from stooping. Warmth may aggravate the pain and inflammation.
Other Remedies
Cimicifuga (also called Actaea racemosa) – Severe aching and stiffness in the upper back and neck, as well as the lower back—with pains that extend down the thighs or across the hips — may be eased with this remedy. It is often helpful for back pain during menstrual periods, with cramping, heaviness, and soreness. A person who needs this remedy typically is talkative and energetic, becoming agitated or depressed when ill.
Dulcamara – If back pain sets in during cold damp weather, along with catching a cold, or after getting wet and chilled, this remedy may be indicated. Stiffness and chills can be felt in the back, and pain is usually worse from stooping.
Ignatia – Back pains related to emotional upsets—especially grief—will often respond to this remedy. The muscles of the lower back may spasm, and twitches, drawing pains, and cramps often occur in other areas.
Kali carbonicum – Kali Carbonicum is a homeopathic medicine for lower back pain with the feeling that the knees are going to give in.
Hypericum perforatum – This homeopathic remedy relieves lower back pain with sharp throbbing pain.
Ruta graveolens – This is used to relieve lower back pain caused or worsened by staying immobile.
Additional Tips
If you are overweight, try to lose some pounds.
Exercise every day.
Lift things in a proper way, as guided by a therapist. Do not lift heavyweights.
Stop smoking and drinking.
Always make sure you are in the right posture whatever activity you may be doing.
Wear flat and soft shoes. Avoid heels.
Walk and move around cautiously.
Slipped discs can be really painful but with the right treatment and precautions, you can become as fit as you were before. So start taking home remedies and consult a doctor whenever you feel any kind of severe pain.
Carpal tunnel syndrome (CTS) is a common median nerve compression syndrome and the most common peripheral mononeuropathy. The clinical syndrome is diagnosed by history and physical examination. Electrodiagnostic testing is the objective method used to measure median nerve dysfunction at the wrist and confirm the clinical diagnosis of CTS. Neuromuscular ultrasound imaging of the carpal tunnel provides supportive diagnostic information by revealing pathologic nerve swelling in CTS, and other anatomic anomalies that compress the median nerve. These tests cannot be used to make the diagnosis in the absence of history that includes CTS symptom criteria and excludes other causes.
Carpal tunnel syndrome is a painful disorder of the hand caused by pressure on nerves that run through the wrist. Symptoms include numbness, pins and needles, and pain (particularly at night). Anything that causes swelling inside the wrist can cause carpal tunnel syndrome, including repetitive hand movements, pregnancy, and arthritis. Possible treatments include rest, splinting, cortisone injections, and surgery.
Anatomy of Carpal Tunnel Syndrome
The carpal tunnel is composed of a bony canal, consisting of carpal bones, the roof of which is the fibrous but rigid transverse carpal ligament. The carpal tunnel contains the nine flexor tendons and the median [rx], which enters the tunnel in the midline or slightly radial to it [rx]. Atypical presentations could be explained by anatomical variations in the median nerve itself [rx].
Sensory branches from the median nerve supply the 3 radial digits and the radial half fourth digit – hence why CTS symptoms are felt in these fingers. The palmar sensory cutaneous branch of the median nerve supplies the cutaneous skin of the palm, and arises, on average, 6 cm proximal to the transverse carpal ligament (TLC). Therefore, the palm is generally not affected in CTS [rx].
The carpal tunnel is a narrow passageway in the wrist, which opens into the hand. It is surrounded by the bones of the wrist (underneath) and the transverse carpal ligament (across the top). The median nerve runs through the carpal tunnel and gives feeling to the thumb, forefinger, middle finger, and half of the ring finger.
Flexor tendons run through the carpal tunnel into the hand. These tendons are covered by a smooth membrane called the tenosynovium and allow hand movement. Any thickening from inflamed tendons or other causes of swelling can reduce the amount of space inside the carpal tunnel. If left unchecked, the median nerve is squashed against the transverse carpal ligament until the nerve cannot function properly. Numbness and pain are the results. It can affect one or both hands.
The muscles of the thumb are also serviced by the median nerve. A person with advanced carpal tunnel syndrome may find they cannot properly use or move their thumb anymore and may find it difficult to grasp an object.
Causes of Carpal Tunnel Syndrome
In some cases, the cause cannot be found. Sometimes there is a combination of factors such as
Pregnancy– the hormones associated with pregnancy cause general fluid retention, which can compress the nerve. Carpal tunnel syndrome triggered by pregnancy usually goes away soon after birth
Wrist fractures – bone fragments can irritate the tenosynovium or reduce the amount of space in the carpal tunnel
Congenital factors – some people have a smaller carpal tunnel than others
Overuse injury – the tendons in the carpal tunnel can become irritated and inflamed by awkward postures or repetitive hand movements.
*According to the American Academy of Neurology’s guidelines
Conditions that may be confused with carpal tunnel syndrome
Cervical radiculopathy (especially C6/7)—look for local neck pain on movement and neurological signs outside the territory of the distal median nerve
Ulnar neuropathy—this can also produce nocturnal paraesthesias; the distribution will usually be to the medial side of the hand.
Raynaud’s phenomenon—this should be recognizable from a history of symptoms related to cold exposure
Vibration white finger—suspect this if the patient uses vibrating hand tools at work
Osteoarthritis of the metacarpophalangeal joint of the thumb—this can produce a spurious appearance of thenar wasting but not true weakness or sensory deficit
Tendonitis—specific tests may help in diagnosis, such as Finkelstein’s test for De Quervain’s tenosynovitis
Generalized peripheral neuropathies—these should be recognized from the wider distribution of symptoms and reflex changes
Motor neuron disease—this can present with wasting in one hand but does not produce sensory symptoms
Syringomyelia—features such as prominent loss of temperature sensation in the hands should give a clue
Multiple sclerosis—this should be recognized from the presence of neurological abnormalities disseminated in location and time
Cervical radiculopathy – especially C6 or C7 radiculopathy, which commonly results in numbness of the thumb, index finger, or middle finger. Sensory symptoms or signs above the wrist, unilateral radicular pain exacerbated by neck movements, segmental weakness in the arm and forearm, or myotatic reflex asymmetry favors radiculopathy.
Neurogenic thoracic outlet syndrome – which frequently is associated with thenar atrophy. However, the pain and sensory manifestations in neurogenic thoracic outlet syndrome are in a C8/T1 distribution (ring and little fingers and medial aspect of the forearm).
Peripheral polyneuropathy – which may be associated with hand numbness. However, there are often sensory manifestations and motor weakness in the legs. Also, there usually is hyporeflexia or areflexia, especially at the ankles.
High median mononeuropathy – including the pronator syndrome, and compression at the ligament of Struthers in the distal arm. Both are rare syndromes and usually are associated with weakness of the long finger flexors.
Cervical myelopathy– In this condition, the numbness is not restricted to the median nerve, and there are frequently other pyramidal manifestations.
Risk factors of Carpal Tunnel Syndrome
Some people are at higher risk of developing carpal tunnel syndrome, including
People who use their hands repetitively in their day-to-day activities, such as typists or assembly line workers.
Symptoms of Carpal Tunnel Syndrome
Abnormal sensations – Parts of the hand feel numb or may tingle (also called “pins and needles”). Usually, the thumb and the middle three fingers are affected (these appear red in the illustration). Your hand falling asleep at night could be a typical early sign of carpal tunnel syndrome.
Pain in your fingers – Sometimes the entire hand might also hurt, or the pain may radiate into your arm.
The little finger and half of the ring finger are unaffected.
Standard symptoms of carpal tunnel syndrome*
Dull, aching discomfort in the hand, forearm, or upper arm
Paraesthesias in the hand
Weakness or clumsiness of the hand
Dry skin, swelling, or color changes in the hand
The occurrence of any of the above in the median distribution
Provocation of symptoms by sleep
Provocation of symptoms by sustained hand or arm positions
Provocation of symptoms by repetitive actions of the hand or wrist
Mitigation of symptoms by changing hand posture or shaking the wrist
Diagnosis of Carpal Tunnel Syndrome
Physical Assessment Tests for Carpal Tunnel Syndrome
The best of these include the carpal compression test. This is done by applying firm pressure directly over the carpal tunnel for 30 seconds. The test is positive when paresthesias, pain, or other symptoms are reproduced.
Flick Signal – One important and simple test of carpal tunnel is the “flick” signal. The patient is asked, “What do you do when your symptoms are worse?” If the patient responds with a motion that resembles shaking a thermometer, the doctor can strongly suspect carpal tunnel.
Testing for Thumb Weakness – Two questions are useful in determining thumb weakness, Can the thumb rise up from the plane of the palm? Can the thumb stretch so that its pad rests on the little finger pad?
Phalen’s Test – In Phalen’s test, the patient rests the elbows on a table and lets the wrists dangle with fingers pointing down and the backs of the hands pressed together. If symptoms develop within a minute, CTS is indicated. (If the test lasts for more than a minute, even patients without CTS may develop symptoms.) This test may be particularly important in determining the severity of CTS and assessing the results of treatment.
Tinel’s Sign – In the Tinel’s sign test, the doctor taps over the median nerve to produce a tingling or mild shock sensation.
Pressure Provocation Test – The doctor presses over the carpal tunnel for 30 seconds to produce tingling or shock in the median nerve.
Tourniquet Test – This test uses an inflatable cuff that applies pressure over the median nerve to produce tingling or small shocks.
Hand Elevation Test – The patient raises his or her hand overhead for 2 minutes to produce symptoms of CTS. The test was has been proven to be accurate and may provide useful information when combined with the Tinel’s and Phalen’s tests.
The reverse Phalen’s, or ‘prayer test,’ – is done by having the patient extend both of their wrists by placing palmar surfaces of both hands together for 1 minute (as if praying). Again a positive test is with the reproduction of symptoms.
The reverses prayer Test – is performed by having the patient fully flex their wrists by placing dorsal surfaces of both hands for one minute. A positive test is when symptoms (numbness, tingling, pain) are reproduced.
The square sign test – is an evaluation to determine the risk of developing carpal tunnel syndrome. The test is positive if the ratio of the thickness of the wrist divided by the width of the wrist is great than 0.7.
Imaging Test
X-rays – X-rays of the affected extremity at the elbow and wrist should be obtained to rule out any osseous deformity that may cause nerve entrapment, as well as cervical spine radiographs that may reveal sources of radiculopathy or first rib involvement. Finally, a chest x-ray should be obtained to rule out compression of the medial chord by an apical lung or Pancoast tumor, particularly in a patient with a positive history for smoking.
Plain radiographs – May be useful during instances where there is a history of trauma, or there is suspicion of a fracture. It can also help to identify cases of osteoarthritis, bony prominences or osteophytes, and the presence of orthopedic hardware that could compress nerves.
Ultrasound – of the nerve at the elbow and wrist can be used to measure the size of the radial nerve compared to controls, as well as to identify a thrombosis of the radial artery that can lead to ulnar nerve symptoms originating in Guyon’s canal.[rx]
Electrodiagnostic studies – Electromyography and nerve conduction studies help to localize the nerve involved as well as where along the course of the nerve it is affected. Additionally, testing can serve as a baseline for comparison with future studies during the course of treatment. It is important to note that normal electrodiagnostic studies do not rule out disease, and clinical correlation should include the patient’s history and physical examination findings.
Magnetic Resonance Imaging (MRI) – Can be useful in the identification of ganglion cysts, synovial or muscular hypertrophy, edema, vascular disease, as well as nerve changes. The cross-sectional area and space available for the nerve can also be measured and compared to accepted normal values.
Nerve ultrasonography – The use of nerve ultrasonography has increased recently. It can measure the cross-sectional area and the longitudinal diameter of the nerve. It can also identify compressive lesions. Ultrasound may also evaluate the presence of local edema. Additionally, ultrasound may help distinguish between different causes of wrist pain that can include tendonitis or osteoarthritis.
Serologicstudies – There are no blood tests used to specifically support the diagnosis of nerve compression, but the use of these tests may be necessary for medical conditions that can either promote nerve compression or can mimic their symptoms. Some of the most frequently encountered conditions include diabetes and hypothyroidism. The assessment of a patient’s fasting blood glucose, hemoglobin A1c, or thyroid function tests may be helpful in the general management of the patient. Other conditions that could mimic nerve compression include deficiency of vitamin B12 or folate, vasculitides, and fibromyalgia.
Electromyography – is also commonly used in the diagnosis of compression neuropathy with muscle denervation. Compressive neuropathies result in increased distal latency and decreased conduction velocity. Thus in patients with cubital tunnel syndrome, one is likely to identify a slowing of conduction in the ulnar nerve segment crossing the elbow.[rx][rx]
Both ultrasonic scanning (USS) – and magnetic resonance imaging (MRI) have sensitivity and specificity over 80% in diagnosis. MRI and USS are also helpful to identify other causes of compression, which may not be picked up on plain radiograph films such as soft tissue swelling and lesions such as neuroma, ganglions, aneurysms, etc.[rx]
Electromyographic and nerve conduction velocity – studies are used to evaluate the ulnar nerve pathology and to rule out other diagnoses.[rx][rx]
Electrodiagnostic tests – analyze the electric waves of nerves and muscles. These tests can help detect median nerve compression in the carpal tunnel.
Electrodiagnostic tests – should be used if clinical or provocative tests are positive and the patient is considering surgery. These tests are the best methods for confirming a diagnosis of CTS. Doctors who perform these tests should be certified by the American Board of Electrodiagnostic Medicine, which uses rigorous standards in qualifying doctors. Specific electrodiagnostic tests called nerve conduction studies and electromyography, are the most common ones performed. Nerve conduction tests can also detect other problems that cause CTS symptoms, such as pinched nerves in the neck or elbow, or thoracic outlet syndrome.
Nerve Conduction Studies – To perform nerve conduction studies, surface electrodes are first fastened to the hand and wrist. Small electric shocks are then applied to the nerves in the fingers, wrist, and forearm to measure how fast a signal travels through the nerves that control movement and sensation. Nerve conduction tests are fairly accurate when done on patients with more clear-cut symptoms of carpal tunnel syndrome. They are less accurate in identifying mild CTS, however. Patients should be sure their practitioners perform tests that compare a number of internal responses, not just the responses of muscles located in the palm at the base of the thumb. They should also make sure the tests measure responses on the second or third fingers.
Electromyography – To perform electromyography, a thin, sterile wire electrode is inserted briefly into a muscle, and the electrical activity is displayed on a viewing screen. Electromyography can be painful and is less accurate than nerve conduction. Some experts question whether it adds any valuable diagnostic information. They suggest that its use is limited to unusual cases, or when other tests indicate that the condition is aggressive and may increase the risk for rapid, significant injury.
Portable electrodiagnostic testing – Portable electronic devices are being evaluated for measuring nerve conductivity. They are relatively quick and easy to use on a large scale in an industrial facility. However, these devices have not been not well studied in clinical trials.
Limitations
Electrodiagnostic studies are not well standardized, and certain conditions can skew the results of either test:
Women and the elderly normally have slower conduction times than younger adult men.
A diagnosis of carpal tunnel syndrome may follow testing the affected hand for numbness, tingling, weakness or pain in specific areas. Muscle and nerve conduction tests may also help affirm or rule out carpal tunnel syndrome.
Treatment of Carpal Tunnel Syndrome
The improvements last for more than 6 months. Even among patients with mild CTS, there is a high risk of relapse. Some researchers are reporting better results when specific exercises for carpal tunnel syndrome are added to the program of treatments.
Ice – Ice may help with acute pain. Some patients have reported that alternating warm and cold soaks is beneficial. (If hot applications relieve pain, most likely the problem is not caused by CTS but by another condition that produces similar symptoms.)
Limiting Movement – If possible, the patient should avoid activities at work or home that may aggravate the syndrome. The affected hand and wrist should be rested for 2 – 6 weeks. This allows the swollen, inflamed tissues to shrink and relieves pressure on the median nerve. If the injury is work-related, the worker should ask to see if other jobs are available that will not involve the same hand or wrist actions. Few studies have been conducted on ergonomically designed furniture or equipment, or on frequent rest breaks. However, it is reasonable to ask for these if other work is not available.
Physiotherapy – It is one of the most common and effective non-pharmacological treatments in the world. It has a variety of treatment modules to erase acute and chronic pain. It is especially helpful in muscle spasticity, spasms related to carpal tunnel syndrome. Inflammatory and noninflammatory pain is treated by ultrasound, MRI, Shortwave, microwave, wax therapy, IRR, laser therapy, interferential current therapy, iontophoresis. Some studies have reported good outcomes with physiotherapy regimes of stretching and strengthening, with more favorable results than rest and reduced activity at short-term follow-up.[rx]
Deep transverse friction massage – It is a special type of massage technique called transverse friction massage is often used to treat carpal tunnel syndrome patients. It is applied to the tendons and the muscles, using the tips of one or two fingers to heal carpal tunnel syndrome.
Transcutaneous electrical nerve stimulation (TENS) – It is called TENS devices that help to transfer electrical impulses that are helpful for the treatment of carpal tunnel syndrome to the nervous system through the skin. These are supposed to keep the pain signals from reaching the brain by blocking pain message signals.
Extracorporeal shockwave therapy (ESWT) – It is a physiotherapy device that generates shock or pressure waves that are transferred to the tissue through the skin for healing carpal tunnel syndrome. This is assumed that to improve the circulation of blood in the tissue and speed up the healing process
Wrist Splints – Wrist splints can keep the wrist from bending. They are not as beneficial as surgery for patients with moderate-to-severe CTS, but they appear to be helpful in specific patients, such as those with mild-to-moderate nighttime symptoms that have lasted for less than a year. Typically the splint is worn at night or during sports. The splint is used for several weeks or months, depending on the severity of the problem, and it may be combined with hand and finger exercises. Benefits may last even after the patient stops wearing the splint.
Ultrasound – Ultrasound uses high-frequency sound waves directed toward the inflamed area. The sound waves are converted into heat in the deep tissues of the hand, opening the blood vessels and allowing oxygen to be delivered to the injured tissue. Ultrasound is often performed along with nerve and tendon exercises. Ultrasound treatment appears to be effective in the short term, but its long-term benefit remains unknown.
Yoga – Very limited evidence suggests that yoga practice may provide some benefit for patients with carpal tunnel syndrome. Yoga postures are designed to stretch, strengthen, and balance upper body joints.
General Exercise Program – Some experts have reported that people who are physically fit, including athletes, joggers, and swimmers, have a lower risk for cumulative trauma disorders. Although there is no evidence that exercise can directly improve CTS, a regular exercise regimen using a combination of aerobic and resistance training techniques strengthens the muscles in the shoulders, arms, and back; helps reduce weight, and improves overall health and well-being.
Low-Level Laser Therapy – Some investigators are working with low-level laser therapy (LLLT), which generates extremely pure light in a single wavelength. The procedure is painless. However, two trials comparing laser therapy to conservative treatment or a placebo laser treatment found no real benefit from this therapy.
Alternative Therapies – Many alternative therapies are offered to people with carpal tunnel syndrome and other repetitive stress disorders. Few of these therapies have any proven benefit, however. People should learn how alternative therapies may interact with other medications they are taking, or impact other medical conditions they have, and they should check with their doctor before trying any of these therapies.
Acupuncture – Acupuncture is often used to relieve CTS symptoms. Although the treatment looks promising for symptom relief, there isn’t enough solid research at this point to recommend it for CTS. More studies are needed to evaluate its benefit.
Chiropractic Therapies – Chiropractic techniques may be helpful for some people whose problems are caused by pinched nerves. There is little evidence, however, to support the use of chiropractic therapies for carpal tunnel syndrome.
Magnets – Magnets are a popular but unproven therapy for pain relief.
Medication
Over-the-counter drugs – In special circumstances, various medications can reduce the pain, the pain and swelling associated with carpal tunnel syndrome. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as aspirin, ibuprofen, naproxen, aceclofenac, and other nonprescription pain relievers, may provide some short-term relief from discomfort.
Prescription medicines – The corticosteroids (such as prednisone) or the drug lidocaine can be injected directly into the wrist to healing and remove overpressure in the median nerve or taken by mouth (in the case of prednisone) to relieve pressure on the median nerve in people with mild or intermittent symptoms.
Vitamin B1, B6, and B12 – It is essential for neuropathic pain management, pernicious anemia, tennis elbow, with vitamin b complex deficiency pain, paresthesia, numbness, itching with diabetic neuropathy pain, myalgia, etc. A side effect may be nausea- vomiting, abdominal pain, cramping
Nerve relaxant – It is basically used to reduce neuropathic pain, inflammation, nerve root entrapment, myalgia, neuralgia, and fibromyalgia, and carpal tunnel syndrome. Your doctor may prescribe gabapentin, pregabalin, vitamin B1, B6, B12, etc. Major side effects are abdominal pain, nausea- vomiting.
Lidoderm patches – It is a prescription medicine that is used to reduce pain, swelling, tenderness, paresthesia, itching, numbness, and carpal tunnel syndrome. It has the anesthetic power that is helpful in carpal tunnel syndrome.
Corticosteroid Injections – Corticosteroids (also called steroids) reduce inflammation. If restricting activities and using painkillers are unsuccessful, the doctor may inject a corticosteroid into the carpal tunnel. In CTS, steroid injections (such as cortisone or prednisolone) shrink the swollen tissues and relieve pressure on the nerve. There is good evidence that they offer short-term symptom relief in a majority of CTS patients. However, in about half of cases, symptoms return within 12 months. Generally, a second injection does not provide any added benefit. Another concern with the use of these injections in moderate or severe diseases is that nerve damage may occur even while symptoms are improving. Most doctors limit steroid injections to about three per year because they can cause complications, such as weakened or ruptured tendons, nerve irritation, or more widespread side effects.
Low-Dose Oral Corticosteroids – A short course (1 – 2 weeks) of oral corticosteroid medicines may provide relief for some people, but the relief does not usually last. Long-term use of these medications can cause serious side effects.
Botulinum toxin type A – Intracarpal injections of botulinum toxin type A (Botox) have not been well studied.
Surgery
Carpal tunnel release surgery is among the most common surgeries performed in the United States. In various trials, 70 – 90% of patients who underwent surgery were free from nighttime pain afterward. Studies have found that surgery provides a greater benefit over the long term compared with splinting or anti-inflammatory drugs plus hand therapy.
Candidates for Surgery
Although evidence strongly suggests that surgery is more effective than conservative approaches (at least in patients with moderate-to-severe CTS), the decision about whether to have surgery to correct CTS and when to have it, is not always clear. Electrodiagnostic and other tests used to confirm CTS are not always perfect or useful in determining the best candidates for surgery.
As a result, surgery does not cure all patients. A number of experts believe that release surgery is performed too often. Some recommend a full trial of conservative treatment (such as splints, anti-inflammatory agents, and physical therapy) before choosing surgery. Others warn that CTS is often progressive and will worsen over time without surgery and that surgery is better than splints and conservative measures for pain relief in cases where carpal tunnel syndrome is likely to present.
Factors that may increase the chances of a successful surgery
Having surgery performed within 3 years of being diagnosed with the disorder
Being in good general health
Having very slow nerve conduction results, but also having reasonably good muscle strength before surgery
Having symptoms that are worse at night than during the day
Factors that may reduce the chances for success
Having very severe symptoms before surgery, such as:
Symptoms that have been present for more than 10 months
Being over 50 years old
Performing heavy manual labor, particularly working with vibrating tools. Only slightly more than half of people who use vibrating hand-held tools are symptom-free 3 years after a CTS operation.
Patients who are on hemodialysis have good initial success, but the condition deteriorates in about half of these patients after around a year and a half.
Patients with diabetes and high blood pressure may be more likely to require a second operation.
Standard Release Surgical Procedures
CTS surgery can be performed through a standard open release, a mini-open technique, or endoscopy. There is no clear evidence to suggest that one surgical technique is much better than another over the long term.
Open Release Surgery – Traditionally, surgery for CTS has involved an open surgical procedure performed in an outpatient facility. In this procedure, the carpal ligament is cut free (released) from the median nerve. This relieves pressure on the median nerve. The surgery is straightforward. In treating carpal tunnel syndrome, surgery may be required to release the compressed median nerve. The open release procedure involves simply cutting the transverse carpal ligament.
The Mini-Open Approach – In recent years, more surgeons have adopted a “mini” open also called short-incision procedure. This surgery requires only a 1-inch incision, but it still allows a direct view of the area (unlike endoscopy, which is viewed on a monitor). The mini-open approach seems to reduce recovery time, pain, and recurrence rate compared to an open approach. However, over the long term, there doesn’t seem to be any significant difference between the mini-open approach and the standard open release.
Endoscopy.
Endoscopy for carpal tunnel syndrome is a less invasive procedure than standard open release.
A surgeon makes one or two 1/2-inch incisions in the wrist and palm and inserts one or two endoscopes (pencil-thin tubes).
The surgeon then inserts a tiny camera and a knife through the lighted tubes.
While looking at the underside of the carpal ligament on a screen, the surgeon cuts the ligament to free the compressed median nerve.
Patients who have endoscopic surgery report less pain than those who have the open release procedure, and they return to normal activities in about half the time. Nevertheless, at this time the best evidence available does not show any significant long-term advantages of endoscopy over open release in terms of muscle, grip strength, or dexterity. The endoscopic approach may even carry a slightly higher risk of pain afterward. This may be due to a more limited view of the hand with endoscopy. (In the open release procedure, the surgeon has a full view of the structures in the hand.) Because of this reduced visibility, there are more concerns about irreversible nerve injury with endoscopic carpal tunnel release than with open carpal tunnel release. However, larger studies have shown an extremely low number of complications when the procedure is performed by experienced physicians.
Recovery after Surgery
Timing of Recovery
For some patients, release surgery relieves symptoms of numbness and tingling immediately.
People who have the operation on both hands will need someone to help them at home for about 2 weeks.
Returning to strenuous work right after surgery may cause the symptoms to return. Patients who work in strenuous jobs generally stay out of work for at least a month and often much longer, depending upon the type of surgery and the severity of the condition. Recovery time appears to be faster with endoscopy or a mini-open release than with open release.
People who perform light office work will return to work much sooner, although possibly with some limitations.
Immediately after surgery, patients usually experience a decline in grip strength and dexterity. Studies have reported a wide range of recovery in this area. The scar may remain tender for up to a year.
Peak improvement (the best level of improvement a patient can reach) may take a long time (up to 10 months).
Physical Therapy. Physical therapy following surgery has not been shown to speed up recovery or affect the final outcome of CTS surgery.
Complications and Long-Term Outcome
Treatment failure and complication rates of CTS surgery vary.
Complications after surgery may include the following:
Loss of some wrist strength is a complication that affects 10 – 30% of patients. Some patients who have jobs requiring significant hand and wrist strength may not be able to perform them after surgery. These workers may also have problems in other parts of the upper body, including the elbows and shoulders. These problems do not go away with surgery and can persist. Studies indicate that 10 – 15% of patients change jobs after a CTS operation.
If pain and symptoms return, the release procedure may be repeated.
Reasons for procedure failure include
Incomplete release of the ligament
Extensive scarring
Recurrence of the disorder due to underlying medical conditions
Patients who had open release surgery appear more likely to require repeat operations compared with those who have had endoscopic surgery.
Immediately after surgery for carpal tunnel syndrome
You should exercise your hand and wrist as soon as possible, following your doctor’s advice.
Self-care after surgery for carpal tunnel syndrome
Follow your doctor’s advice, but general suggestions include:
If you go home within a day or two of surgery, you will probably need some help around the house.
Continue your medication as ordered by your doctor.
Cold packs applied at regular intervals can help reduce post-operative swelling.
Rest the hand as much as you can for at least four weeks following surgery.
Long-term outlook after surgery for carpal tunnel syndrome
Your symptoms should ease dramatically after surgery. However, pain around the surgery site may linger for some months. See your doctor if you are concerned about the amount of pain or discomfort. If you have non-absorbable sutures, your doctor will need to remove these about two weeks after the operation. If you have any increased swelling, redness or heat, see your doctor immediately, since these symptoms could indicate infection.
Exercises for Carpal Tunnel Syndrome
Wrists
Exercise 1
Make a loose right fist, palm up, and use your left hand to press gently down against the clenched hand.
Resist the force with the closed right hand for 5 seconds. Be sure to keep your wrist straight.
Turn your right fist palm down, and press the knuckles against the left open palm for 5 seconds.
Finally, turn your right palm so the thumb-side of the fist is up, and press down again for 5 seconds.
Repeat with your left hand.
Exercise 2
Hold one hand straight up shoulder-high with your fingers together and palm facing outward. (The position looks like a shoulder-high salute.)
With the other hand, bend the hand you are exercising backward with the fingers still held together and hold for 5 seconds.
Spread your fingers and thumb open while your hand is still bent back and hold for 5 seconds.
Repeat five times with each hand.
Exercise 3 (Wrist Circle)
Hold your second and third fingers up, and close the others.
Draw five clockwise circles in the air with the two fingertips.
Draw five more counterclockwise circles.
Repeat with your other hand.
Fingers and Hand
Exercise 1
Clench the fingers of one hand into a tight fist.
Release, fanning out your fingers.
Do this five times. Repeat with the other hand.
Exercise 2
To exercise your thumb, bend it against the palm beneath the little finger, and hold for 5 seconds.
Spread the fingers apart, palm up, and hold for 5 seconds.
Repeat five to 10 times with each hand.
Exercise 3
Gently pull your thumb out and back and hold for 5 seconds.
Repeat five to 10 times with each hand.
Forearms (stretching these muscles will reduce tension in the wrist)
Place your hands together in front of your chest, fingers pointed upward in a prayer-like position.
Keeping your palms flat together, raise your elbows to stretch your forearm muscles.
Stretch for 10 seconds.
Gently shake your hands limp for a few seconds to loosen them.
Repeat frequently when your hands or arms tire from activity.
Neck and Shoulders
Exercise 1
Sit upright and place your right hand on top of your left shoulder.
Hold that shoulder down, and slowly tip your head down toward the right.
Keep your face pointed forward, or even turned slightly toward the right.
Hold this stretch gently for 5 seconds.
Repeat on the other side.
Exercise 2
Stand in a relaxed position with your arms at your sides.
Shrug your shoulders up, then squeeze your shoulders back, then stretch your shoulders down, and then press them forward.
Frozen shoulder is an extremely painful and debilitating condition leading to stiffness and disability. It typically occurs in the fifth and sixth decades of life, thus affecting individuals of working age. The disability resulting from this condition has a considerable economic impact on affected individuals and society.
Frozen shoulder can be either primary (idiopathic) or secondary. Secondary frozen shoulder is defined as that associated with trauma; rotator cuff disease and impingement; cardiovascular disease; hemiparesis; or diabetes (although some classify this in diabetics as primary frozen shoulder). The incidence of frozen shoulder in people with diabetes is reported to be 10% to 36%, and these tend not to respond as well to treatment as in nondiabetics.1
Adhesive capsulitis (also known as frozen shoulder) is a painful and disabling disorder of unclear cause in which the shoulder capsule, the connective tissue surrounding the glenohumeral joint of the shoulder, becomes inflamed and stiff, greatly restricting motion and causing chronic pain. Pain is usually constant, worse at night, and with cold weather. Certain movements or bumps can provoke episodes of tremendous pain and cramping. The condition is thought to be caused by injury or trauma to the area and may have an autoimmune component.
Frozen shoulder, also known as adhesive capsulitis, is a common condition in which the articular shoulder capsule (a sac of ligaments surrounding the joint) swells and stiffens, restricting its mobility. It typically affects only one shoulder, but one in five cases affect both.
Stage of Frozen Shoulder
The normal course of a frozen shoulder has been described as having three stages
Clinical Stages
Painful
Gradual onset of diffuse pain (6 wks to 9 mos)
Stiff
Decreased ROM affecting activities of daily living (4 to 9 mos or more)
Thawing
Gradual return of motion (5 to 26 mos)
Arthroscopic Stages
Stage 1
Patchy, fibrinous synovitis
Stage 2
Capsular contraction and fibrinous adhesions
Stage 3
Increasing contraction, synovitis resolving
Stage 4
Severe contraction
Three phases of clinical presentation
Painful freezing phase
Duration 10-36 weeks. Pain and stiffness around the shoulder with no history of injury. A nagging constant pain is worse at night, with little response to non-steroidal anti-inflammatory drugs
Adhesive phase
Occurs at 4-12 months. The pain gradually subsides but stiffness remains. Pain is apparent only at the extremes of movement. Gross reduction of glenohumeral movements, with near total obliteration of external rotation
Resolution phase
Takes 12-42 months. Follows the adhesive phase with spontaneous improvement in the range of movement. Mean duration from onset of frozen shoulder to the greatest resolution is over 30 months
Anatomy of Frozen Shoulder
The term “frozen shoulder” is often used incorrectly for arthritis, even though the two conditions are unrelated. Frozen shoulder refers specifically to the shoulder joint, while arthritis may refer to other/multiple joints.
The shoulder has a spheroidal joint (ball – and – socket joint), in which the round part of one bone fits into the concavity of another. The proximal humerus (round head of the upper arm bone) fits into the socket of the scapula (shoulder blade). Frozen shoulder is thought to cause the formation of scar tissue in the shoulder, which makes the shoulder joint’s capsule (not to be confused with the rotator cuff) thicken and tighten, leaving less room for movement.
The humerus is the upper arm bone. This is the “ball” of the shoulder’s “ball and socket” joint. The scapula is the flat, triangular bone commonly called the shoulder blade. Prominent areas of the scapula serve as attachment points for many muscles and ligaments.
The glenoid is the shallow “socket” on the side of the scapula that receives the ‘ball’ of the humerus. Together they form the “ball and socket” arrangement of the shoulder.
The scapular spine is a horizontal ridge along the back of the scapula that divides the scapula into upper and lower regions.
The acromion is the end of the scapular spine. It projects up to form the top of the shoulder.
The coracoid process is a projection towards the front of the scapula and is an attachment site for several muscles and ligaments.
The clavicle is the collarbone. Although it appears to be straight, it actually forms an S-shape when seen from above.
The thorax or rib cage is an anchor for several muscles and ligaments. Although the ribs do not physically attach to the scapula, the thorax stabilizes and maintains proper positioning of the scapula so that the arm can function to its fullest capacity.
The modern English words “adhesive capsulitis” are derived from the Latin words adhaerens meaning “sticking to” and capsule meaning “little container” and the Greek word itis meaning “inflammation”.
Additionally, there are four bone junctions or joints:
The glenohumeral joint is the main joint of the shoulder. Here, the glenoid on the scapula and the head of the humerus come together. The fairly flat socket of the glenoid surrounds only 20% – 30% of the humeral head. Because of its poor fit, this joint relies heavily on the surrounding soft tissue for support. The labrum, a ring of fibrocartilage tissue, attaches to the glenoid and deepens the socket to encircle more of the humerus.
The acromioclavicular joint, or AC joint, is the bony point on the top of the shoulder. It stabilizes the scapula to the chest, by connecting the acromion on the scapula to the clavicle, or “collarbone”. A thick disk of fibrocartilage acts as a shock absorber between the two bones. The surrounding capsule and ligaments give this joint great stability.
The sternoclavicular joint, or SC joint, connects the other end of the clavicle to the sternum, or “breastbone”. Like the AC joint, this joint contains a fibrocartilage disk that helps the bones achieve a better fit. It also gets excellent support from its joint capsule and surrounding ligaments.
The scapulothoracic articulation is the area where the scapula, embedded in muscle, glides over the thoracic rib cage. The surrounding muscles and ligaments keep the scapula properly positioned so that the arm can move correctly.
Cartilage
There are two types of cartilage in the shoulder
Articular cartilage is the shiny white coating that covers the end of the humeral head and lines the inside surface of the glenoid. It has two purposes:
To provide a smooth, slick surface for easy movement
To be a shock absorber and protect the underlying bone
Fibrocartilage – is the thick tissue that forms the disks of the AC and SC joints and the labrum, the ring that deepens the glenoid. Fibrocartilage has three roles:
To act as a cushion in shock absorption
To help stabilize the joint by improving the fit of the bones
To act as a spacer and improve contact between the articular cartilage surfaces
Ligaments
The shoulder relies heavily on ligaments for support. Ligaments attach bone to bone and provide the “static” stability in a joint. Ligaments will alternately become tight and loose with normal motion. They keep the joint within the normal limits of movement.
The glenohumeral ligaments attach in layers from the glenoid labrum to form the joint capsule around the head of the humerus.
The coracoacromial arch is the group of ligaments that spans the bony projections of the coracoid process and the acromion.
The coracoclavicular ligaments and the acromioclavicular ligament provide most of the support for the AC joint.
Muscles and Tendons
Muscles and tendons work together in the shoulder to provide the “dynamic” stability of the shoulder.
There are four muscle groups in the shoulder:
The rotator cuff muscles are the subscapularis, the supraspinatus, the infraspinatus, and the teres minor. They are the primary stabilizers that hold the “ball” of the humerus to the glenoid “socket”. The socket is too shallow to offer much security for the humerus. These four muscles form a “cuff” around the humeral head, securing it firmly in the socket. As its name implies, this group of muscles also rotates the arm. The rotator cuff protects the glenohumeral joint from dislocation, allowing the large muscles that control the shoulder to power the arm with great mobility.
The biceps tendon complex also helps keep the humeral head in the glenoid and helps raise the arm.
The scapulothoracic muscles attach the scapula to the thorax. Their main function is to stabilize the scapula to allow for proper shoulder motion.
The superficial muscles of the shoulder are the large, powerful outer layer of muscles that are important to the overall function of the shoulder. This group includes the deltoid muscle, which covers the rotator cuff muscles.
Causes of Frozen Shoulder
Age & Gender – Frozen shoulder most commonly affects patients between the ages of 40 to 60 years old. It is twice more common in women than in men.
Endocrine (Hormonal) Disorders – Patients with diabetes are at particular risk for developing frozen shoulder. People with other endocrine abnormalities, such as thyroid problems, may also be predisposed to developing frozen shoulder.
Shoulder Trauma or Surgery – Patients who sustain a shoulder injury, or undergo shoulder surgery or vaccinations in the shoulder muscle can develop frozen shoulder. When injury or surgery is followed by prolonged joint immobilization such as putting the shoulder in a sling, the risk of developing frozen shoulder is highest.
Other Systemic Conditions – Several systemic conditions such as heart disease and Parkinson’s disease have also been associated with an increased risk of developing frozen shoulder.
Psychosomatic overlay – It is also hypothesized that some patients also develop frozen shoulder due to severe stress causing a psychosomatic reaction, especially if they feel emotionally restricted and pressured or “frozen” in the decision-making process.
The cause of frozen shoulder is not fully understood and in some cases is unidentifiable. However, most people with frozen shoulder have suffered from immobility as a result of a recent injury or fracture. The condition is common in people with diabetes.
Common risk factors for frozen shoulder are
You’re more likely to suffer from frozen shoulder if you’re female and over 40 years of age.
Age – being over 40 years of age.
Gender – 70% of people with frozen shoulder are women.
Recent surgery or arm fracture – immobility of recovery may cause the shoulder capsule to stiffen.
Diabetes – two to four times more likely to develop frozen shoulder for unknown reasons; symptoms may be more severe.
Having suffered a stroke.
Hyperthyroidism (overactive thyroid).
Hypothyroidism (underactive thyroid).
Cardiovascular disease (heart disease).
Parkinson’s disease.
Symptoms of Frozen Shoulder
Early symptoms of frozen shoulder
A feeling of pain and tightness in the shoulder area.
A feeling of tightness especially when putting the arm up and back, as you would do if you were throwing a ball overarm.
Pain on the back of the wrist. (This specifically relates to frozen shoulder caused by subscapularis trigger points.)
Dull, aching Pain
Sleep disturbance and deprivation
Severe sharp pain with rapid movement (eg. trying to catch mobile phone)
The difficulty with activities of daily living (eg. dressing, driving and personal care)
Lack of movement in all directions
As time goes on, the symptoms will worsen although the pain may be reduced.
The typical symptoms are a pain, stiffness, and limitation in the range of movement of one of your shoulders. The symptoms typically have three phases
Phase one – the ‘freezing’, painful phase. This typically lasts 2-9 months. The first symptom is usually a pain. Stiffness and limitation in movement then also gradually build up. The pain is typically worse at night and when you lie on your affected side.
Phase two – the ‘frozen’, stiff (or adhesive) phase. This typically lasts 4-12 months. The pain gradually eases but stiffness and limitation in movement remain and can become worse. All movements of your shoulder are affected. However, the movement most severely affected is usually a rotation of the arm outwards. The muscles around the shoulder may waste a bit as they are not used.
Phase three – the ‘thawing’, recovery phase. This typically lasts between one and three years. The pain and stiffness gradually go and movement gradually returns to normal, or near normal.
Symptoms often interfere with everyday tasks such as driving, dressing, or sleeping. Even scratching your back, or putting your hand in a rear pocket, may become impossible. Work may be affected in some cases.
Diagnosis of Frozen Shoulder
The following outcome measures have been used in studies researching adhesive capsulitis.
Shoulder Pain and Disability Index (SPADI)
Disability of the Arm, Shoulder and Hand scale (DASH)
American Shoulder and Elbow Surgeons Standardized Shoulder Assessment Form (ASES)
Simple Shoulder Test (SST)
Penn Shoulder Scale (PSS)
NPRS
VAS
SF-36
Hand to neck
Shoulder flexion + abduction + ER
Similar to ADLs such as combing hair, putting on a necklace
Hand to scapula
Shoulder extension + adduction + IR
Similar to ADLs such fitting a bra, putting on a jacket, getting into the back pocket
Hand to opposite scapula
Shoulder flexion + horizontal adduction
These tests require appropriate elbow, scapulothoracic, and thoracic mobility and these areas should be cleared of pathology first. If a patient is unable to complete the motion, other structures outside of the shoulder joint may be the limiting factor.
Imaging
X-ray – X-rays can help to ensure the shoulder joint appears normal, with no evidence of traumatic injury or arthritic changes.
MRI – This powerful diagnostic tool can sometimes show inflammation, but this test is better at ruling out other problems, rather than looking for a frozen shoulder. If an MRI is conducted, an injection of contrast fluid into the shoulder joint prior to the MRI is necessary. Results indicating a scarred capsule would designate frozen shoulder.
Ultrasound– can show the state of the rotator cuff tendons. Intact tendons in the setting of severe restriction in movement suggest frozen shoulder.
Arthrogram – may be used with an MRI to provide further information about structures in the shoulder. A dye is injected into the shoulder and images are obtained. The dye creates a contrast on the image, making the specific location of adhesions and the reduced space typical of frozen shoulder more visible.
Treatment of Frozen Shoulder
The aim of treatment for frozen shoulder is to alleviate pain and preserve mobility and flexibility in the shoulder. However, recovery may be slow, as symptoms tend to persist for several years.
Corticosteroid injection – Based on best available evidence, corticosteroid injection has mainly short-term benefit with a single injection. There appears to be added benefit with providing physiotherapy promptly following steroid injection compared to home exercise alone and physiotherapy alone. There is insufficient evidence to conclude with reasonable certainty in what clinical situations steroid injection, with or without physiotherapy, is most likely to be effective for treatment of frozen shoulder.
Sodium hyaluronate injection – A small number of diverse studies, all of which may have a high risk of bias, provide insufficient evidence to make conclusions about the effectiveness of sodium hyaluronate in the treatment of frozen shoulder
Physiotherapy/physical therapy – Primary studies comparing different types of physiotherapy/physical therapies support the use of various techniques to provide short- to medium-term benefit. Some interventions in current use that were investigated include therapeutic ultrasound end-range mobilization,28 short-wave diathermies plus stretching29 and high-grade mobilization therapy.30These interventions should be stage of disease and response-dependent. Based on best available evidence, there may be benefit from short-wave diathermy plus stretching and high-grade mobilization techniques in patients who have already had physiotherapy or a steroid injection. There is insufficient evidence to make conclusions on the best mode of physiotherapy for frozen shoulder
Acupuncture – The role of acupuncture in the treatment of frozen shoulder is not clear. Available evidence does not demonstrate a clear benefit.
Treatment options for frozen shoulder include Painkillers – relieve symptoms of pain. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, are over – the – counter (OTC, no prescription required) painkillers and may reduce inflammation of the shoulder in addition to alleviating mild pain. Acetaminophen (paracetamol, Tylenol) is recommended for extended use. Prescription painkillers, such as codeine (an opiate-based painkiller) may also reduce pain. Not all painkillers are suitable for every patient; be sure to review options with your doctor.
Exercise – frequent, gentle exercise can prevent and even reverse stiffness in the shoulder.
Alternating between hot and cold compression packs can help with frozen shoulder
Hot or cold compression packs – help to reduce pain and swelling. It is often helpful to alternate between the two.
Transcutaneous electrical nerve stimulation (TENS) – numbs the nerve endings in the spinal cord that control pain and sends small pulses of electricity from the TENS machine to electrodes (small electric pads) that are applied to the skin on the affected shoulder.
Physical therapy (UK: physiotherapy) – can teach you exercises to maintain as much mobility and flexibility as possible without straining the shoulder or causing too much pain.
Physiotherapy for Frozen Shoulder
Your physical therapist’s overall goal is to restore your movement, so you can perform your daily activities. Once the evaluation process has identified the stage of your condition, your physical therapist will create an individualized exercise program tailored to your specific needs. Exercise has been found to be most effective for those who are in stage 2 or higher. Your treatment may include:
Stages 1 and 2
Exercises and manual therapy – Your physical therapist will help you maintain as much range of motion as possible and will help reduce your pain. Your therapist may use a combination of range-of-motion exercises and manual therapy (hands-on) techniques to maintain shoulder movement.
Modalities – Your physical therapist may use heat and ice treatments (modalities) to help relax the muscles prior to other forms of treatment.
Home-exercise program – Your physical therapist will give you a gentle home-exercise program designed to help reduce your loss of motion. Your therapist will warn you that being overly aggressive with stretching in this stage may make your shoulder pain worse. Your physical therapist will match your treatment activities and intensity to your symptoms, and educate you on the appropriate use of the affected arm. Your therapist will carefully monitor your progress to ensure a safe healing procedure is followed.
Pain medication – Sometimes, conservative care cannot reduce the pain of adhesive capsulitis. In that case, your physical therapist may refer you for an injection of a safe anti-inflammatory and pain-relieving medication. Research has shown that although these injections don’t provide longer-term benefits for a range of motion and don’t shorten the duration of the condition, they do offer short-term pain reduction.
Stage 3
The focus of treatment during phase 3 is on the return of motion. Treatment may include:
Stretching techniques – Your physical therapist may introduce more intense stretching techniques to encourage greater movement and flexibility.
Manual therapy – Your physical therapist may take your manual therapy to a higher level, encouraging the muscles and tissues to loosen up.
Strengthening exercises – You may begin strengthening exercises targeting the shoulder area as well as your core muscles. Your home-exercise program will change to include these exercises.
Stage 4
In the final stage, your physical therapist will focus on the return of “normal” shoulder body mechanics and your return to normal, every day, pain-free activities. Your treatment may include:
Stretching techniques – The stretching techniques in this stage will be similar to previous ones you’ve learned but will focus on the specific directions and positions that are limited for you.
Manual therapy – Your physical therapist may perform manual therapy techniques in very specific positions and ranges that are problematic for you. They will focus on eliminating the last of your limitations.
Strength training – Your physical therapist will prescribe specific strengthening exercises related to any weakness that you may have to help you perform your work or recreational tasks.
Return to work or sport – Your physical therapist will address movements and tasks that are required in your daily and recreational life.
Rehabilitation program
The exercises and other treatment methods are dependent on which phase of rehabilitation the patient is at. We recommend seeking professional advice before attempting any rehabilitation.
Phase 1 – Freezing
This phase is usually the most painful phase of treatment and movement becomes gradually more and more difficult. The aim of the following treatments and exercises is to help control pain and maintain movement in the shoulder joint.
NSAID’s (nonsteroidal anti-inflammatory drugs) e.g. Ibuprofen may help reduce inflammation and pain although will be of less value in later phases of treatment. Check with a doctor before taking medication and do not take ibuprofen if you have asthma.
Electrotherapy modalities such as ultrasound, TENS and laser treatment may all help reduce pain and inflammation.
Exercises should be done as long as they can be performed pain-free. Mobility exercises such as the pendulum and assisted shoulder exercises using a pole can help maintain shoulder mobility. See adhesive capsulitis exercises for more detailed information.
Shoulder stretching exercises for the muscles at the front and back of the shoulder can be done also to attempt to maintain as much movement as possible. Strengthening exercises are unlikely to be possible at this stage due to pain.
Phase 2 – Frozen
During the frozen phase of treatment is where there is the least movement in the shoulder, but on the plus side, pain tends to have reduced. This phase should be about trying to maintain strength and as much mobility as possible.
Mobility exercises such as pendulums and wand exercises should be continued. Stretching exercises for the chest muscles and muscles at the back of the shoulder should also be maintained.
Strengthening exercises can be performed to maintain muscle strength. Isometric or static contractions are exercises needing no joint movement and can be done without worrying about movement in the shoulder. Try to maintain good posture by working the upper back muscles. Poor posture could be a contributing factor in frozen shoulder helping to cause it or prevent healing.
A therapist may be able to help by performing some more advanced mobilizations on the shoulder to increase the range of movement at the shoulder joint. This is especially beneficial to patients who have very limited movement in the shoulder.
Phase 3 – Thawing
The final phase of treatment and rehab is where movement starts to return to the shoulder. This phase is all about getting the shoulder back to normal as quickly as possible by regaining full movement and strength. After a few months with little movement, the shoulder will be considerably weakened so strengthening exercises are important.
Mobility exercises and stretches can become more aggressive, but should still be within the boundaries of pain. Aim to restore full mobility in the shoulder joint.
Strengthening exercises can progress from isometric or static contractions to exercises using a resistance band, then eventually free weights or weight machines.
Work the affected shoulder first, do as many reps as you can and then do the same number on the unaffected shoulder. This will help avoid a muscle imbalance.
Include rotator cuff exercises in treatment as well as posture exercises and exercises for the deltoid and chest muscles too. The shoulder joint is a complicated joint and correct biomechanical function between the shoulder joint and shoulder blade is important as other shoulder injuries may follow if the joint is not fully rehabilitated.
Making the correct diagnosis is crucial, and will ensure an efficient and optimum treatment for the patient.
Features of importance are;
Hand dominance
Occupation and level of activity or sports
Location, radiation, and the onset of pain
Duration of symptoms (see phases of disease in the Definition earlier above)
The global reduction in the range of motion with a capsular pattern, defined as disproportionately severe loss of passive external rotation in the affected shoulder with arm by the side, over other movements.
History of diabetes, cardiovascular disease or other associations.
Normal X-rays in two planes to rule out mechanical glenohumeral incongruity such as arthritis, avascular necrosis or dislocation of the shoulder, which produce a similar clinical picture.
Red flags for the shoulder
Acute severe shoulder pain needs a proper and competent diagnosis. Any shoulder ‘red flags’ identified during primary care assessment needs urgent secondary care referral.
A suspected infected joint needs same day urgent referral.
An unreduced dislocation needs same day urgent referral.
Suspected malignancy or tumor needs urgent referral following the local 2-week cancer referral pathway.
An acute cuff tear as a result of a traumatic event needs an urgent referral and ideally should be seen in the next available outpatient clinic.
Suspected inflammatory oligo or poly-arthritis or systemic inflammatory disease should be considered as a ‘rheumatological red flag’ and local rheumatology referral pathways should be followed.
Treatment in primary care/community triage services
Pain relief
The aims of treatment are:
Improving range of motion
Reducing the duration of symptoms
Return to normal activitiesTreatment depends on the phase of the disease, severity of symptoms and degree of restriction of work, domestic and leisure activities.
Corticosteroid injection
Domestic exercise programme
Supervised physiotherapy/manual therapyFollowing interventions are suitable for primary care:
This is a painful and debilitating condition, where the pain is often severe, mimicking malignant disease (e.g. night pain). The onset of stiffness may be rapid and cause the significant functional deficit, typically in individuals of working age. Treatment should be tailored to individual patient needs depending on response and severity of symptoms.
Beware of red flags such as tumor, infection, unreduced dislocation or inflammatory polyarthritis.
Overall, a step-up approach may be adopted in terms of degree of treatment invasiveness. Some patients may have particular treatment preferences based on their needs and referral to secondary care may need to be considered early in such circumstances. Shared decision-making is particularly important for this condition.
A proportion of patients with frozen shoulder will respond to conservative treatment, and the response needs to be monitored. The most frequent indications for invasive treatments are persistent and severe functional restrictions that are resistant to conservative measures.
Symptoms usually of up to 3 months with the failure of conservative treatment measures may trigger a referral to secondary care for consideration of more invasive treatment. The severity of symptoms may necessitate earlier referral; it would not be appropriate to persist with ineffective treatment measures and delay referral of patients who experience severe pain and restriction.
Shared decision-making is important, and individual patients’ needs are different. Failure of initial treatment to control pain, if the degree of stiffness causes considerable functional compromise, or if there is any doubt about the diagnosis, prompt referral to secondary care is indicated.
Physiotherapy rehabilitation is usually for 6 weeks unless patients are unable to tolerate the exercises, or physiotherapists identify a reason for earlier referral to secondary care. If there is a patient improvement in the first 6 weeks of physiotherapy, then a further 6 weeks of therapy is justified.
Treatment timelines should include primary care and intermediate care time. Intermediate care should not delay appropriate referral to secondary care.
Secondary care
In a UK study of patterns of referral of shoulder conditions, 22% of patients were referred to secondary care up to 3 years following initial presentation, although most referrals occurred within 3 months.16 There is little evidence available on referral patterns for frozen shoulder specifically.
Confirm diagnosis with history and examination.
Obtain imaging with plain radiographs to rule out mechanical glenohumeral incongruences such as arthritis, avascular necrosis or dislocation.
Counsel patient fully regarding operative and non-operative options.
Ensure the multidisciplinary approach to care with the availability of specialist shoulder physiotherapists and shoulder surgeons.
The most commonly used secondary care interventions are
Manipulation under anesthesia (MUA)
Arthroscopic capsular release (ACR)
Distension arthrogram (DA) or hydrosilylation
Physiotherapy and corticosteroid injection, usually to supplement any of the above interventions
If symptoms fail to resolve with conservative treatment, then MUA, DA or ACR may be considered. This choice depends mainly on expertise and clinician preference.
MUA is performed under general anesthesia where the arm is manipulated to ‘tear’ the contracted shoulder capsule in a controlled fashion, thus restoring external rotation and other movements. This is supplemented with corticosteroid injection for pain relief and with physiotherapy to maintain range of motion post MUA.
ACR involves arthroscopic surgery under general anesthesia. The contracted capsule is released in a controlled fashion using arthroscopic instruments, frequently with radiofrequency ablation. The most prominent contracture occurs anteriorly and release of this improves the external rotation. The inferior capsule may be released with arthroscopic instruments, or with a controlled MUA.
DA is a procedure where the shoulder capsule is injected with saline and local anesthetic under pressure to distend and disrupt the capsule. This procedure is usually performed by an interventional radiologist and does not require general anesthesia. It is performed under fluoroscopy or ultrasound guidance and a radio-opaque dye may be used to confirm the accuracy of placement of the injected fluid. Both DA and ACR are supplemented with post-procedural physiotherapy to maintain range of motion in the affected shoulder.
It would be expected that surgical units performing ACR or MUA
Ensure patients undergo an appropriate pre-operative assessment to ensure fitness for surgery and to confirm discharge planning.
Perform surgery or MUA inappropriately resourced and staffed units.
Both procedures are typically performed as daycare or 23-hour admission (depending on the time of the day the procedure takes place) unless clinical or social circumstances dictate otherwise.
Standard postoperative care should involve the prompt start of physiotherapy and pain relief as required.
Physiotherapy services vary across the country, although up to 12 weeks of physiotherapy are typically required to maintain range of motion in the treated shoulder.
Up to three outpatient follow-up appointments may be needed, depending on progress.
Outcome metrics
Length of stay – day case (23 hours) and overnight.
Re-admission rate within 90 days.
Patient-reported outcome measure (PROM) pre-procedure, and 12 months post-procedure.
Infection/other adverse events.
Research and audit
In partnership with Centre for Reviews and Dissemination in York, BESS members were commissioned to conduct an evidence synthesis on the frozen shoulder by the National Institute for Health Research Health Technology Assessment (NIHR-HTA) Program. This report titled ‘Management of frozen shoulder: a systematic review and cost-effectiveness analysis’ has now been published, and forms a key reference document that summarises current evidence, and areas for future research on this topic.17
A recent survey of health professionals in the UK has found that the professional groups (general practitioners, a general practitioner with a special interest, physiotherapists, orthopedic surgeons) had different views on the most appropriate treatment pathway for the frozen shoulder.18. There was, however, a consensus that treatment should depend on the phase of the disease and a step-up approach would be appropriate.
In addition, a scoping review identified that most previous reviews have concentrated on one particular intervention and there is a general paucity of good primary research on frozen shoulder.19
Members of BESS involved in the above evidence syntheses are currently designing an interventional trial for frozen shoulder investigating commonly used interventions for management in secondary care.
A validated clinical score, preferably a PROM, should be used pre-operatively and the following treatment.
Acceptable scores include the Shoulder Pain and Disability Index (SPADI), Disability of Arm, Shoulder, and Hand (DASH) and the Oxford Shoulder Score (OSS). The disability subscale of the SPADI has been used by several published reports for this condition. Other measures such as EQ 5D may be used for economic analysis.
Scores should be captured pre-operatively and 1 year following intervention, which allows longitudinal analysis to determine the sustenance of treatment effect and consequences of any treatment-related adverse events.
Patient public clinician information
Patient and public information – ensure all available information is provided regarding the benefits and risks of all treatment options
Clinician information – ensure access to available evidence.
Surgery
Margery for frozen shoulder is typically offered during “Stage 2: Frozen.” The goal of surgery is to stretch and release the stiffened joint capsule. The most common methods include manipulation under anesthesia and shoulder arthroscopy.
Manipulation under anesthesia – During this procedure, you are put to sleep. Your doctor will force your shoulder to move which causes the capsule and scar tissue to stretch or tear. This releases the tightening and increases the range of motion.
Shoulder arthroscopy – In this procedure, your doctor will cut through tight portions of the joint capsule. This is done using pencil-sized instruments inserted through small incisions around your shoulder.
Home Exercises
Stiff or frozen shoulders are usually uncomfortable, even if the degree of stiffness is not great. That’s the bad news. The good news is that most stiff shoulders can be managed successfully by a simple exercise program conducted by the patient in the home.
Getting the shoulder moving
It is basically a question of gently and progressively getting the shoulder moving again. This program is the safest of all treatments for frozen shoulders. Although months of these specific exercises may be required, persistence almost always pays off. Even if arthritis is present, this program may help preserve and even improve the shoulder’s range and comfort. Before beginning these exercises you should consult with your physician.
There are two components to the home program for stiff shoulders. The first is a series of stretching exercises and the second relates to regular participation in a fitness program.
Your opposite arm is a great therapist for your stiff shoulder. Your “therapist arm” is always available to apply a gentle stretch in any direction of tightness. Each of these gentle stretches needs to be held up to a count of 100.
Stretching Exercises for the Frozen or Stiff Shoulder
The basic program includes the exercises illustrated below. Click any image below to enlarge and view in our photo gallery.
Fig. 1 – Getting the arm up while lying downFig. 2 – Getting the arm up overhead while sitting down.Fig. 3 – Getting the arm to externally rotate while lying down.Fig. 4 – Getting the arm to externally rotate while standing.Fig. 5 – Getting the arm up the back.Fig. 6 – Getting the arm across the body.
Lumbar disc herniation is a common condition that frequently affects the spine in young and middle-aged patients.1,5,11 The lumbar intervertebral disc is a complex structure composed of collagen, proteoglycans, and sparse fibrochondrocytic cells that serve to dissipate forces exerted on the spine. As part of the normal aging process, the disc fibrochondrocytes can undergo senescence, and proteoglycan production diminishes. This leads to a loss of hydration and disc collapse, which increases strain on the fibers of the annulus fibrosus surrounding the disc. Tears and fissures in the annulus can result, facilitating a herniation of disc material, should sufficient forces be placed on the disc. Alternatively, a large biomechanical force placed on a healthy, normal disc may lead to extrusion of disc material in the setting of catastrophic failure of the annular fibers.5
Spinal disc herniation also is known as a slipped disc, is a medical condition affecting the spine in which a tear in the outer, fibrous ring of an intervertebral disc allows the soft, central portion to bulge out beyond the damaged outer rings. Disc herniation is usually due to age-related degeneration of the outer ring, known as the anulus fibrosus, although trauma, lifting injuries, or straining have been implicated as well. Tears are almost always postero-lateral (on the back of the sides) owing to the presence of the posterior longitudinal ligament in the spinal canal .This tear in the disc ring may result in the release of chemicals causing inflammation, which may directly cause severe pain even in the absence of nerve rootcompression.
Anatomy of Spinal Disc Herniation
Herniated = from “hernia,” a part of the body that bulges out through an abnormal opening Disc = the disk-shaped cushions between the bones of the spine
The vertebral column (also called the spinal column orbackbone) is made up of 33 bones known as vertebra (plural, vertebrae). Each vertebra is separated from the adjacent vertebrae by intervertebral discs, a spongy but strong connective tissue. The intervertebral discs, along with ligaments and facet joints, connect the individual vertebrae to help maintain the spine’s normal alignment and curvature while also permitting movement.
The image at left shows the entire spinal column from beside and from the front. The bones of the spinal column are orange in color, and the intervertebral discs are white.
In the center of the spinal column there is an open channel called the spinal canal. The spinal cord and spinal nerves are located in the spinal canal, where they are surrounded by spinal fluid and protected by the strong spinal column. On each side of the spine, small openings between adjacent vertebrae called foramina (singular, foramen) allow nerve roots to enter and exit the spinal canal.
The spine is divided into the following distinct regions:
Cervicalspine – consists of seven vertebrae in the neck. These vertebrae are small and allow for the mobile nature of the neck.
Thoracic spine – consists of 12 vertebrae in the upper and mid-back. These are larger and stronger than the cervical vertebrae. Each thoracic vertebra is attached to a rib on either side. This provides significant stiffness and strength to the thoracic portion of the spine.
Lumbar spine – usually consists of five vertebrae in the lower back, but may vary between four and six. These vertebrae are the largest because they withstand the greatest amount of force in the spine. The lumbar spine is also more mobile than the thoracic spine. Because of these factors, the lumbar spine is the most frequently affected by degenerative conditions, spinal stenosis, and herniated discs.
Sacrococcygeal – the very lowest portion of the spine. The sacrococcygeal region consists of one single bone, made of fused vertebrae in the sacrum (five vertebrae) and coccyx (four vertebrae). It attaches to the pelvis on either side. In a small number of people, there may be a disc between the first and second sacral vertebrae. Alternatively, the fifth vertebra in the lumbar (lower) spine may occasionally be fused to the sacrum, leaving only 4 lumbar vertebrae.
A herniated disc occurs when the fibrous outer portion of the disc ruptures or tears, and the jelly-like core squeezes out. When the herniated disc compresses a nearby nerve, as in the image below, the result can be a pinched nerve. A pinched nerve may cause pain, numbness, tingling or weakness in the arms or legs. The substance that makes up the disc’s jelly-like core can also inflame and irritate the nerve, causing additional pain.
Prolapse of intervertebral disc closeup 3d image. (c) alexmit/Big Stock
A bulging disc occurs when the outer wall of the disc weakens but doesn’t rupture, and “bulges” outward. A herniated disc may actually begin as a bulging disc whose outer wall is then ruptured by a great amount of pressure.
Disc herniation can occur in the cervical, thoracic, or lumbar spine. The location of the pain depends on the location of the herniated disc. If the herniation occurs in the neck, for example, it can cause pain that radiates into the shoulder and arm; if it occurs in the lower back, the pain produced can radiate down into the hip and leg. Depending on the location, it can damage the spinal cord.
Symptoms of Spinal Disc Herniation
A cervical herniated disc may put pressure on a cervical spinal nerve and can cause symptoms like pain, pins and needles, numbness or weakness in the neck, shoulders, or arms. A large disc herniation in the cervical spine may compress the spinal cord within the spinal canal and cause numbness, stiffness, and weakness in the legs and possibly some difficulty with bowel and bladder control.
A thoracic herniated disc may cause pain in the mid back around the level of the disc herniation. If the disc herniation compresses a thoracic spinal nerve as it travels through the foramen, then pain or numbness may travel around the rib cage from the back to the front of the chest or upper abdomen. A large disc herniation in the thoracic spine may compress the spinal cord within the spinal canal and cause numbness, stiffness and weakness in the legs and possibly some difficulty with bowel and bladder control.
A lumbar herniated disc may cause the following symptoms:
Intermittent or continuous back pain (this may be made worse by movement, coughing, sneezing, or standing for long periods of time)
Spasm of the back muscles
Sciatica — pain that starts near the back or buttock and travels down the leg to the calf or into the foot.
Muscle weakness in the legs
Numbness in the leg or foot
Decreased reflexes at the knee or ankle
Changes in bladder or bowel function
Difficulty walking
Incoordination
The symptoms of disc disease may resemble other conditions or medical problems. Always consult a doctor for a diagnosis.
Causes and Risk Factors
Herniated discs can often be the result of degenerative disc disease. As people age, the intervertebral discs lose their water content and ability to cushion the vertebrae. As a result, the discs are not as flexible. Furthermore, the fibrous outer portion of the disc is more likely to rupture or tear.
Acute disc herniations can occur in young, healthy people as a result of an injury or tear to the outer layer of the disc (called the annulus fibrosis) that allows the central, jelly-like portion of the disc (called thenucleus pulposis) to herniate into the spinal canal or foramen.
Tests and Diagnosis of Spinal Disc Herniation
Physical examination
The straight leg raise may be positive, as this finding has low specificity; however, it has high sensitivity. Thus the finding of a negative SLR sign is important in helping to “rule out” the possibility of a lower lumbar disc herniation. A variation is to lift the leg while the patient is sitting.[32] However, this reduces the sensitivity of the test.[33]
Imaging
Projection radiography (X-ray imaging) – Although traditional plain X-rays are limited in their ability to image soft tissues such as discs, muscles, and nerves, they are still used to confirm or exclude other possibilities such as tumors, infections, fractures, etc. In spite of these limitations, X-ray can still play a relatively inexpensive role in confirming the suspicion of the presence of a herniated disc. If a suspicion is thus strengthened, other methods may be used to provide final confirmation.
Computed tomography scan (CT or CAT scan) – A diagnostic image created after a computer reads x-rays. It can show the shape and size of the spinal canal, its contents, and the structures around it, including soft tissues. However, visual confirmation of a disc herniation can be difficult with a CT.
Magnetic resonance imaging (MRI) without contrast – A diagnostic test that produces three-dimensional images of body structures using powerful magnets and computer technology. It can show the spinal cord, nerve roots, and surrounding areas, as well as enlargement, degeneration, and tumors. It shows soft tissues better than CAT scans. An MRI performed with a high magnetic field strength usually provides the most conclusive evidence for diagnosis of a disc herniation. T2-weighted images allow for clear visualization of protruded disc material in the spinal canal.
Myelogram An x-ray of the spinal canal following injection of a contrast material into the surrounding cerebrospinal fluid spaces. By revealing displacement of the contrast material, it can show the presence of structures that can cause pressure on the spinal cord or nerves, such as herniated discs, tumors, or bone spurs. Because myelography involves the injection of foreign substances, MRI scans are now preferred for most patients. Myelograms still provide excellent outlines of space-occupying lesions, especially when combined with CT scanning (CT myelography).
Electromyogram and nerve conduction studies (EMG/NCS) – These tests measure the electrical impulse along nerve roots, peripheral nerves, and muscle tissue. This will indicate whether there is ongoing nerve damage, if the nerves are in a state of healing from a past injury, or whether there is another site of nerve compression. EMG/NCS studies are typically used to pinpoint the sources of nerve dysfunction distal to the spine.
Computerized tomography (CT) scan – a series of X-rays, assembled by a computer into 3-dimensional images of the body’s structures
Myelography – a procedure that involves injecting a liquid dye into the spinal column followed by a series of X-rays and a computerized tomography (CT) scan. This procedure may provide useful images that reveal the indentations of the spinal fluid sac caused by bulging or herniated discs, or bone spurs that might be pressing on the spinal cord or nerves.
Electromyography (EMG) – tests the electrical activity of a nerve root to help determine the cause of pain.
The presence and severity of myelopathy can be evaluated by means of transcranial magnetic stimulation (TMS), a neurophysiological method that allows the measurement of the time required for a neural impulse to cross the pyramidal tracts, starting from the cerebral cortex and ending at the anterior horn cells of the cervical, thoracic or lumbar spinal cord. This measurement is called Central Conduction Time (CCT). TMS can aid physicians to:
determine whether myelopathy exists
identify the level of the spinal cord where myelopathy is located. This is especially useful in cases where more that two lesions may be responsible for the clinical symptoms and signs, such as in patients with two or more cervical disc hernias[34]
follow-up the progression of myelopathy in time, for example before and after cervical spine surgery
TMS can also help in the differential diagnosis of different causes of pyramidal tract damage.[35]
Since a herniated disc may cause similar symptoms to other degenerative spinal conditions, a surgeon may order a variety of diagnostic procedures to rule out other possible conditions.
Treatment of Spinal Disc Herniation
Before discussing surgery as an option, the surgeon may initiate the following nonoperative treatments. Specific treatment for lumbar disk disease will be determined by your health care provider based on
Your age, overall health, and medical history
Extent of the condition
Type of condition
Your tolerance for specific medications, procedures, or therapies
Expectations for the course of the condition
Your opinion or preference
Typically, conservative therapy is the first line of treatment to manage lumbar disk disease. This may include a combination of the following:
Bed rest
Patient education on proper body mechanics (to help decrease the chance of worsening pain or damage to the disk)
Physical therapy, which may include ultrasound, massage, conditioning, and exercise
Weight control
Use of a lumbosacral back support
Medications of Spinal Disc Herniation
Analgesics: Prescription-strength drugs that relieve pain but not inflammation.
Antidepressants: A Drugs that block pain messages from your brain and boost the effects of eorphins (your body’s natural painkillers).
Corticosteroids: Also known as oral steroids, these medications reduce inflammation.
Muscle Relaxants: These medications provide relief from spinal muscle spasms.
Neuropathic Agents: Drugs(pregabalin & gabapentine) that address neuropathic—or nerve-related—pain. This includes burning, numbness, and tingling.
Opoids : Also known as narcotics, these medications are intense pain relievers that should only be used under a doctor’s careful supervision.
Topical Medications: These prescription-strength creams, gels, ointments, patches, and sprays help relieve pain and inflammation through the skin.
NSAIDs: Prescription-strength drugs that reduce both pain and inflammation.Pain medicines and anti-inflammatory drugs help to relieve pain and stiffness, allowing for increased mobility and exercise. There are many common over-the-counter medicines called non-steroidal anti-inflammatory drugs (NSAIDs). They include aspirin, ibuprofen (Motrin, Advil), and naproxen (Naprosyn, Aleve).
Calcium & vitamin D3, to improve bones health and healing fracture.
Glucosamaine & diacerine ,can be used to tightening the loose tenson and regenerate cartilage or inhabit the further degeneration of cartilage.
Corticosteroid to healing the nerve inflamation and clotted blood in the joints.
Diatery suppliment to remove the general weakness & improved the health.
There is little evidence to suggest that drug treatments are effective in treating herniated disc.
NSAIDs and cytokine inhibitors don’t seem to improve symptoms of sciatica caused by disc herniation.
We found no evidence examining the effectiveness of analgesics, antidepressants, or muscle relaxants in people with a herniated disc.
We found no evidence of sufficient quality to judge the effectiveness of epidural injections of corticosteroids.
With regard to non-drug treatments, spinal manipulation seems to be more effective at relieving local or radiating pain in people with acute back pain and sciatica with disc protrusion compared with sham manipulation, although concerns exist regarding possible further herniation from spinal manipulation in people who are surgical candidates.
Neither bed rest nor traction seems effective in treating people with sciatica caused by disc herniation.
We found insufficient evidence about advice to stay active, acupuncture, massage, exercise, heat, or ice to judge their efficacy in treating people with herniated disc.
About 10% of people have sufficient pain after 6 weeks for surgery to become a consideration.
Both standard discectomy and microdiscectomy seem to increase self-reported improvement to a similar extent.
We found insufficient evidence judging the effectiveness of automated percutaneous discectomy,laser discectomy, or percutaneous disc decompression.
Surgical Treatment of Spinal Disc Herniation
When these conservative measures fail, surgery for removal of a herniated disk may be recommended. Surgery is done under general anesthesia. An incision is placed in the lower back over the area where the disk is herniated. Some bone from the back of the spine may be removed to gain access to the area where the disk is located. Typically, the herniated part of the disk and any extra loose pieces of disk are removed from the disk space.
Surgical treatment for a herniated disc will be based on the following
The history, severity and duration of pain
Whether or not the patient has received previous treatments for disc disorders and how effective the treatments were
Whether or not there is any evidence of neurologic damage such as sensory loss, weakness, impaired coordination, or bowel or bladder problems
Surgery for patients with disc disorders of the spine is usually recommended for those patients who do not find relief with non-operative treatment over a period of 6-12 weeks. Surgery is also recommended in patients who have a neurologic deficit (numbness, weakness or reduced function due to pressure on the spinal cord or nerves). Early intervention in those cases is best in order to maximize the likelihood of neurologic recovery.
Your surgeon may perform the following surgical procedures:
Microdiscectomy: A procedure that uses a microscope and microsurgical tools to remove the portion of the disc that is pressing against the nerve, relieving the pressure caused by a herniated disc. Microdiscectomy is frequently performed for herniated discs in the certical, thoracic, and lumbosacral spine. This procedure is performed under general anesthesia through a small skin incision over the spine. The muscles of the spine are gently elevated or spread apart to expose a small segment of the spine. A small amount of the back part of the spine, called the lamina and facet joint, is trimmed under high magnification of the microscope to provide safe access to the spinal canal. Using microsurgical techniques, our neurosurgeons identify and remove the herniated piece of the disc while protecting the compressed nerve. Most patients may go home either on the day of surgery or the next morning.
Anterior (from the front) or lateral (from the side) surgical approaches may be required for large or calcified thoracic disc herniations that cause spinal cord compression.
Anterior Cervical Discectomy and Fusion (ACDF): a procedure that involves the removal of the herniated disc in the cervical spine through the front of the neck. A fusion surgery may be required to make the spine stable after the discectomy.
After surgery, restrictions may be placed on the patient’s activities for several weeks while healing is taking place to prevent another disk herniation from occurring. Your surgeon will discuss any restrictions with you.
Others Treatment of Spinal Disc Herniation
Chiropractic Care
Sixty percent of people with sciatica who didn’t get relief from other therapies and then tried spinal manipulation experienced the same degree of pain relief as patients who eventually had surgery, found a 2010 study in the Journal of Manipulative and Physiological Therapeutics. The 120 people in the study saw a chiropractor about 3 times a week for 4 weeks, and then continued weekly visits, tapering off treatment as they felt better. In people who responded to chiropractic care, benefits lasted up to a year. “Spinal manipulation may create a response in the nervous system that relieves pain and restores normal mobility to the injured area,” says study researcher Gordon McMorland, DC, of National Spine Care in Calgary, Alberta. “It also reduces inflammation, creating an environment that promotes the body’s natural healing mechanisms.”
Acupuncture
“You can get relief as soon as the first session, though it takes about 12 sessions to see improvement,” says Jingduan Yang, MD, assistant professor at the Jefferson Myrna Brind Center of Integrative Medicine at Thomas Jefferson University. A small study in the Journal of Traditional Chinese Medicine found that of 30 people with sciatica, 17 got complete relief and 10 saw symptoms improve with warming acupuncture, in which the needles are heated.
Yoga
A study in the journal Pain reported that people with chronic back pain who practiced Iyengar yoga for 16 weeks saw pain reduced by 64% and disability by 77%. Although yoga’s effects on sciatica are less clear, gentle forms may be beneficial. By strengthening muscles and improving flexibility, a yoga practice can help sciatica sufferers “move and function better so they don’t fall into a posture that aggravates sciatica,” says James W. Carson, PhD, a psychologist at the Comprehensive Pain Center at Oregon Health & Science University. For extra grip and stability, try these grip socks from Natural Fitness.
Massage
Don’t expect a chilled-out spa massage if you have sciatica. In this instance, trigger-point therapy is best, says Jeff Smoot, vice president of the American Massage Therapy Association. The sciatic nerve sits underneath a muscle called the piriformis, which is located beneath the glutes. “When the piriformis muscle gets tight, it pinches the sciatic nerve, causing tingling and numbness down into the leg,” says Smoot. He applies pressure to irritated and inflamed areas, or trigger points, in the piriformis muscle, as well as in muscles in the lower back and glutes. Typically, Smoot schedules treatments 7 to 10 days apart. If patients don’t see progress by the fourth visit, “they need to try another form of therapy,” he says.
Topical Preparations
St. John’s wort oil, a liniment, is “one of my favorites for nerve pain,” says Tieraona Low Dog, MD, director of the fellowship at the Arizona Center for Integrative Medicine. Apply the anti-inflammatory oil two or three times a day where there’s pain. Another option: an OTC cayenne pepper plaster or cream; capsaicin, found in chiles, hinders the release of pain-causing compounds from nerves. For severe cases, Low Dog uses the prescription chile patch Qutenza, designed for shingles pain. “One application is effective for weeks,” says Low Dog.
Ice or Heat
Because the sciatic nerve is buried deep within the buttock and leg, ice or heat on the surface of the body won’t ease that inner inflammation. But the timehonored treatments can act as counterirritants—that is, “they give your body other input in the painful area, and that brings the pain down a notch,” says Ruppert. Apply an ice pack or a heating pad as needed for 15 minutes.
Devil’s Claw
The herbal medication devil’s claw is “quite a potent anti-inflammatory, working like ibuprofen and similar drugs to inhibit substances that drive inflammation,” says Low Dog. She generally starts patients on 1,500 to 2,000 mg twice a day. Look for a brand that has a standardized extract of roughly 50 mg of harpagoside, the active compound. Safety reviews show that the supplement is well tolerated by most people but should be avoided by patients with peptic ulcers or on blood-thinning medications.
Epidural Steroid Injections
People whose pain doesn’t lessen within about a month and who aren’t helped by other therapies may find their pain remedied by an x-ray-guided injection of steroid into the lower back near the sciatic nerve, says Raj Rao, MD, a spokesperson for the AAOS. “The hope is to reduce inflammation within that nerve branch,” explains Rao. Because of concerns about side effects, such as loss of bone density, the epidural shots are limited to three a year.
Physiotherapy in Harniated Disc
In stage 1&2 of harniated disc physiotherapy must applied to cure harniated hisc .In case of stage 3&4 ,physiotherapy can’t applied due to adoining the another case of foot drop.
In accordance of NIH journal
Physiotherapy for a lumbar disc bulge
Physiotherapy treatment for a lumbar disc bulge is vital to ensure an optimal outcome and may comprise:
soft tissue massage
electrotherapy (e.g. ultrasound)
lumbar taping
the use of a back brace
mobilization
traction
the use of a lumbar roll for sitting
dry needling
exercises to push the disc back ‘in’ and to improve strength, core stability and flexibility
education
activity modification advice
biomechanical correction
ergonomic advice
clinical Pilates
hydrotherapy
a functional restoration program
a gradual return to activity program
Physical therapy often plays a major role in herniated disc recovery. Its methods not only offer immediate pain relief, but they also teach you how to condition your body to prevent further injury.
There are a variety of physical therapy techniques. Passive treatments relax your body and include deep tissue massage, hot and cold therapy, electrical stimulation (eg, TENS), and hydrotherapy.
Your physical therapy program will usually begin with passive treatments. But once your body heals, you will start active treatments that strengthen your body and prevent further pain. Your physical therapist will work with you to develop a plan that best suits you.
Passive Physical Treatments for Herniated Discs
Deep Tissue Massage
There are more than 100 types of massage, but deep tissue massage is an ideal option if you have a herniated disc because it uses a great deal of pressure to relieve deep muscle tension and spasms, which develop to prevent muscle motion at the affected area.
Hot and Cold Therapy
Both hot and cold therapies offer their own set of benefits, and your physical therapist may alternate between them to get the best results.Your physical therapist may use heat to increase blood flow to the target area. Blood helps heal the area by delivering extra oxygen and nutrients. Blood also removes waste byproducts from muscle spasms.Conversely, cold therapy (also called cryotherapy) slows circulation. This reduces inflammation, muscle spasms and pain. Your physical therapist may place an ice pack on the target area, give you an ice massage, or even use a spray known as fluoromethane to cool inflamed tissues.
Hydrotherapy
As the name suggests, hydrotherapy involves water. As a passive treatment, hydrotherapy may involve simply sitting in a whirlpool bath or warm shower. Hydrotherapy gently relieves pain and relaxes muscles.
A TENS machine uses an electrical current to stimulate your muscles. It sounds intense, but it really isn’t painful. Electrodes taped to your skin send a tiny electrical current to key points on the nerve pathway. TENS reduces muscle spasms and is generally believed to trigger the release of endorphins, which are your body’s natural pain killers.
Traction
The goal of traction is to reduce the effects of gravity on the spine. By gently pulling apart the bones, the intent is to reduce the disc herniation. The analogy is much like a flat tire “disappearing” when you put a jack under the car and take pressure off the tire. It can be performed in the cervical or lumbar spine.
Active Treatments You May Try in Physical Therapy
Active treatments help address flexibility, posture, strength, core stability, and joint movement. An exercise program may also be prescribed to achieve optimal results. This will not only curb recurrent pain but will also benefit your overall health. Your physical therapist will work with you to develop a program based on your specific diagnosis and health history.
Core stability
Many people don’t realize how important a strong core is to their spinal health. Your core (abdominal) muscles help your back muscles support your spine. When your core muscles are weak, it puts extra pressure on your back muscles. Your physical therapist may teach you core stabilizing exercises to strengthen your back.
Flexibility
Learning proper stretching and flexibility techniques will prepare you for aerobic and strength exercises. Flexibility helps your body move easier by warding off stiffness.
Hydrotherapy
In contrast to simply sitting in a hot tub or bath like its passive counterpart, active hydrotherapy may involve water aerobics to help condition your body without unnecessary stress.
Muscle strengthening
Strong muscles are a great support system for your spine and better handle pain.
Your physical therapist will teach you ways to condition and strengthen your back to help prevent future pain. You may learn self-care principles so you understand how to best treat your symptoms. The ultimate goal is for you to develop the knowledge to maintain a pain-free lifestyle.
It’s essential that you learn how to exercise and condition your back after the formal physical therapy ends. If you don’t implement the lessons you learned during physical therapy, you won’t enjoy its long-term results. By taking care of your back on your own, you may prevent further herniated disc pain
8 Best Exercises For Slipped Disc In Lower Back
Our spinal cord is supported by a number of muscles. Relevant exercises help relieve the pain and reduce the symptoms. Muscle exercises of those muscles associated with the affected area is necessary. Patients must know the region that has a slipped disc and then opt for exercises related to that muscle. The list of best exercises for the slipped disc are mentioned as follows:
Abdominal Isometrics – It can be performed either on floor, mat or bed. This exercise involves moving your lower back towards the surface at which you are performing this exercise. Leg movement must be reduced in this exercise and stomach muscles must be made active. This reduces pain in lower back because of the attachment of abdominal muscles to the lower side of the vertebral column. Ten repetitions are effective.
Crunches – Lie on a flat surface with knees bent. Cross your arm under your head, raise your head and chest in such a manner that your rib cage curl interiorly towards your backbone. Perform this exercise slowly and gradually. In the beginning, perform fewer crunches and repeat it daily and increase the number of turns as you gain strength.
Lower back extension – Lie in an upside down position, raise your upper body with the help of elbow and hold up yourself in an elevated position for a short span of time and then slowly lower down. Please make sure that during this exercise you do not raise your pelvis girdle (hip region).
Bilateral knee to the chest – Lay down on a flat surface and draw your knee towards your abdominal region, repeat it 5 times and then switch leg. You can also increase the number of turns each time you repeat it.
Iso-hip flexion – Lay down over a flat surface and draw your knees towards your chest region in a 90 degree position with your stomach. Place your hands over your knees and then exert your hand pressure to lower your knee. Then utilize the knee pressure to resist the downward movement of your legs, in all both movements should just exert pressure and allow no movements. This position should be maintained for few seconds and then lowered slowly and gradually.
Air bike – Sit on a chair with your chest and shoulders supported. Align your knees and feet together and then bring them towards your body and perform a pedaling motion in air then repeat the same motion while moving your knees farther away from body. Follow ten repetitions each time and increase its number as you gain strengths
Ham string stretch: Lie on a flat surface with your knees bend, place your hands under your knees and then slightly pull your leg towards your chest, repeat it with other leg. This exercise must involve a stretch over lower thigh muscle
Lumbar roll: Lie on a flat surface with your knee bent and your feet lying on the floor then move your legs together towards the right side and then towards your left side. Repeating these movements 5 times on each side.
The above mentioned best exercises for slipped disc can be followed but if pain increases or muscle pain is persisting then quit these exercises right away. These exercises not only help in reducing the pain but they also activate efficient muscle movement. Along with these exercise tips, proper body postures must be also maintained to prevent further disc damages.
Home Remady for Herniated Disc/Slip Disc
Consciousnes
Incase of PLID home remedies are not special treatment just only home practice & creating public awareness. All should be done in PLID stage 1&2
Walking
Walking every day keeps muscle disorders away. Walking can also help to prevent herniated disc. Walk on a flat road for 20 minutes as many times as you can in a day. Take longer steps as it will help you to keep away the pain of herniated disc. Do not give strain to yourself as it might increase the pain.
Rest
www.rxharun.com
Rest is essential for patients suffering from herniated disc. Take short rest periods from time to time. When you are sleeping make sure you don’t stay in the same position for a long time. Do not sleep on your stomach. Also, take care of the mattress you are sleeping on. Don’t let it be too soft and spongy. Buy a mattress that has good surface area and is soft in nature.
Physiotherapy And Yoga( only home practice)
Physiotherapy is a very cheap and good way of getting rid of herniated disc from itself. Therapists will teach your proper exercises and stretches which will improve the disc shape to a great extent.
You will notice good differences while performing daily chores after just 4-5 sessions of therapy.
Physiotherapy also promotes faster healing of the disorder.
Turmeric
Turmeric contains curcumin which is a very good anti-oxidant and anti-inflammatory agent. This is why it stops the gel-like fluid inside the discs from coming out and bulge. It also shows antihistamine properties which help to reduce pain because of slowed blood circulation to the area of pain.
Dimethyl Sulfoxide (DMSO)
Dimethyl sulfoxide is a derivative from sulphur which has antioxidant properties as well as the organic sulphur present in it helps in the growth of new cells and detoxification of the body. The growth of new cells helps to replace the old cells of the discs and prevent the fluid from leaking outside.
Massage With Essential Oils
Massage with essential oils on the full body, especially on the spine and lower back regions, will help in good blood circulation and promote the growth of new cells. It will help relieve pain and promote better absorption of oxygen and nutrients. Essential oils will also regenerate the cells of the disc and hence stop the disc from getting slipped.
Acupressure And Acupuncture
In both techniques, pressure is used for relieving the pain from the swelled area. In acupressure fingers, tips and elbow are used and acupuncture needles are used. But this should be done with the help of an experienced practitioner and not alone.
This is not recommended for patients having high blood pressure and for women who are pregnant.
TENS
TENS stands for Transcutaneous Electrical Nerve Stimulation and this is one of the best remedies for herniated disc at home. This treatment uses low voltage electric current which is applied to the affected area and helps the body to release endorphin which decreases the pain.
Cayenne Pepper
It is a very effective ingredient for the treatment of herniated disc.You can drink its tea or make a paste of the pepper using water and apply on the affected area.
Diet
Diet is necessary to keep away all types of bad conditions that might affect you.Drink a lot of water and eat a balanced diet. Take excess of fibres and proteins. During this condition, you should avoid dairy products and red meat. Also, avoid fat-free foods.
Epsom Salt
Epsom salt is one of the widely used natural painkiller and anti-inflammatory agent.
You can use this by adding 3-4 cups of salt in a hot water bath. Stay inside the bath for 15 minutes. It will help you achieve maximum relaxation.
Do not use this remedy if you are diabetic or pregnant. If you are on any type of medication consult your doctor before bathing in Epsom salt.
Horsetail
Horsetail is a herb which has high quantities of minerals in it. It nourishes our tissues and has the ability to heal broken bones and torn ligaments.
All you need to do is add some horsetail leaves to half a litre of water. Boil on low heat till the water quantity reduces to half its quantity. Cool the solution and filter it off. You can drink 5 ml of the solution thrice a day.It will heal herniated disc very fast.
California Poppy
California poppy is anti-inflammatory and analgesic in nature. This is what makes it a good treatment for herniated disc.
You can tear the leaves of California poppy into small pieces and make a paste out of it using water. Use little hot water so that when you apply the paste on the affected area it is still warm.
White Willow Bark
White willow bark is used for reducing the discomfort of herniated discs. The chemical structure of this drugs shows a marked similarity to aspirin hence acts as an analgesic but doesn’t irritate your gut. It is also astringent and anti-inflammatory in nature.
This herb might react with drugs hence do consult your doctor if you are on any kind of medication.
Comfrey Leaves
Comfrey leaves have power to heal bones and connective tissues of the body.All you need to do is take some fresh leaves and add it to cold water. Let it remain undisturbed for around 12 hours. After 12 hours heat the above solution and filter it. Add the filtrate to bath water and take a bath in it 2 times a day.Do not consume it orally because it contains hepatic-toxin alkaloids.
Boswellia
Boswellia is a naturally occurring painkiller which is a very effective remedy for herniated disc.
All you can do is make a decoction of Boswellia and consume it 2 times a day to reduce pain and discomfort associated with herniated discs.
Boswellia is an organic painkiller that effectively treats the problem of herniated disc. It is also an herbal cure for osteoarthritis.
Omega-3 Fatty Acids
Omega-3 Fatty acids are helpful in decreasing the inflammation and pain experienced due to herniated disc disorder. This acid forms collagen which is used by the broken discs for repairing itself.
Eat foods that are high in this kind of fats like fish, almonds, sprouts and walnuts.
Colchicine
Colchicine is an active amino-alkaloid found in the plant of Kurchi or autumn crocus. This powder is obtained by crushing the seeds of the plant. It has anti-inflammatory properties which are effective against the slipped disc.
Make a paste with kurchi powder and honey and consume it once a day.
You can also make tea out of the powder or mix the powder in milk and have it once or twice a day.
Burdock
Burdock contains a lot of anti-oxidants which is helpful to detoxify the body and remove all kinds of harmful substances and decrease the pain and inflammation in your body. It also treats arthritis.
Burdock can be consumed as a decoction once or twice a day.
Passionflower
Passionflower is helpful for slipped discs because the essential oils present is antispasmodic in nature. It reduces pain and inflammation.
You can massage with passionflower essential oil or take capsules made from it, however, do consult your doctor before taking capsules.
Additional Tips
If you are overweight, try to lose some pounds.
Exercise every day.
Lift things in a proper way, as guided by a therapist. Do not lift heavy weights.
Stop smoking and drinking.
Always make sure you are in the right posture whatever activity you may be doing.
Wear flat and soft shoes. Avoid heels.
Walk and move around cautiously.
Slipped discs can be really painful but with the right treatment and precautions you can become as fit as you were before. So start taking home remedies and consult a doctor whenever you feel any kind of severe pain.





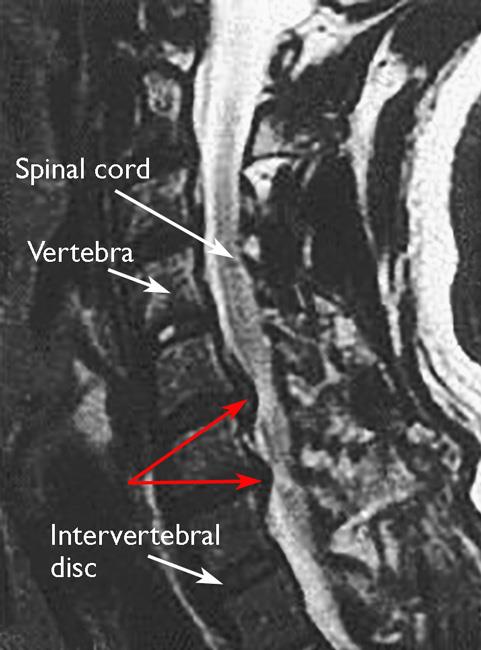











")















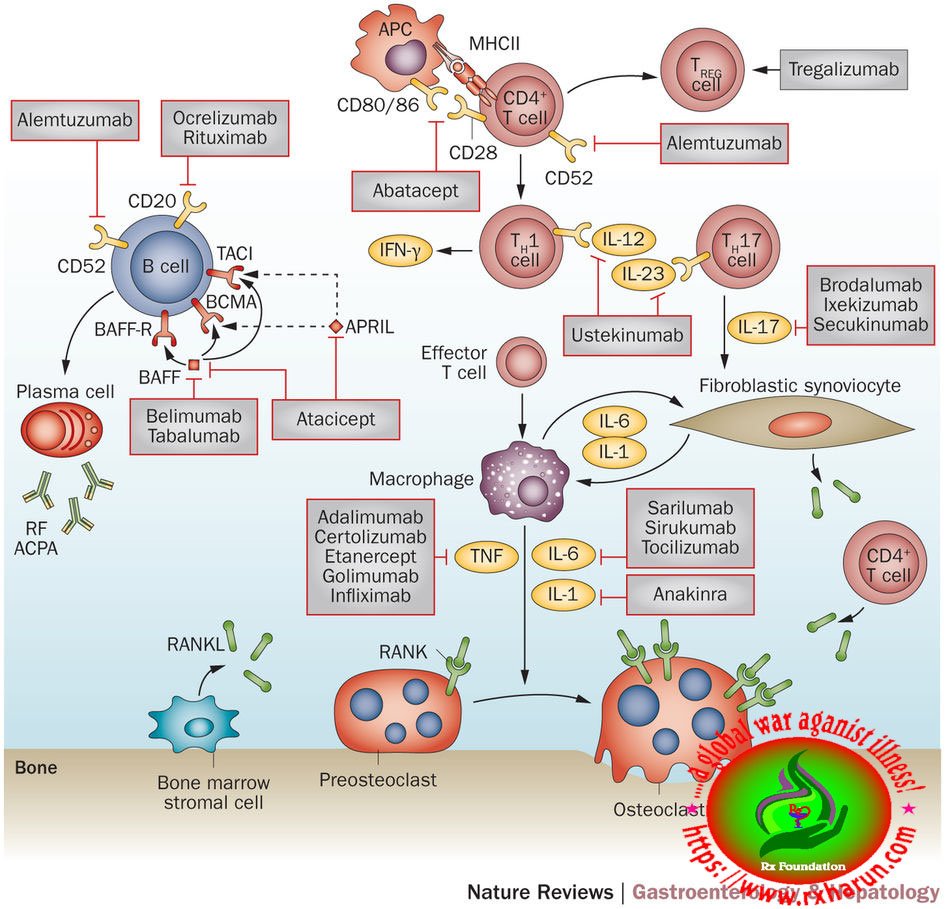

















































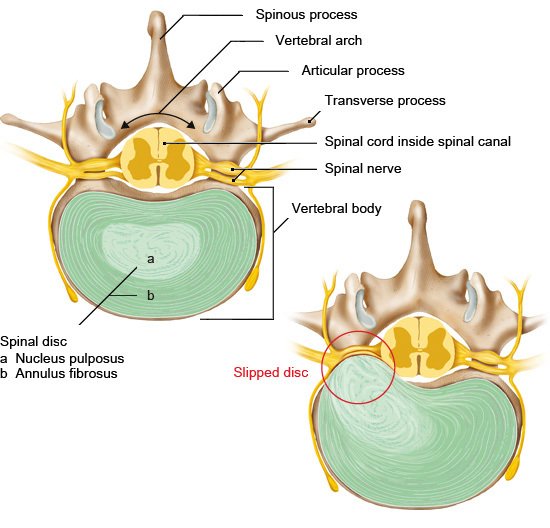








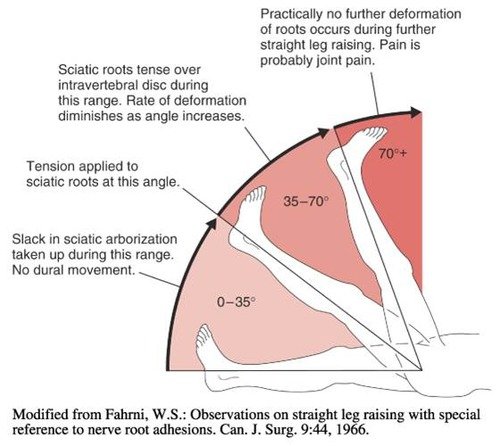



 Massage
Massage





















