Premature ejaculation (PE) occurs when a man experiences orgasm and expels semen soon after sexual activity and with minimal penile stimulation. It has also been called early ejaculation, rapid ejaculation, rapid climax, premature climax and (historically) ejaculatio praecox. There is no uniform cut-off defining “premature”, but a consensus of experts at the International Society for Sexual Medicine endorsed a definition of around one minute after penetration. The International Classification of Diseases (ICD-10) applies a cut-off of 15 seconds from the beginning of sexual intercourse.
Erectile dysfunction – Men who are anxious about obtaining or maintaining an erection during sexual intercourse might form a pattern of rushing to ejaculate, which can be difficult to change.
Anxiety – Many men with premature ejaculation also have problems with anxiety — either specifically about sexual performance or related to other issues.
Relationship problems – If you have had satisfying sexual relationships with other partners in which premature ejaculation happened infrequently or not at all, it’s possible that interpersonal issues between you and your current partner are contributing to the problem.
The nucleus para giganto cellulitis – of the brain has been identified as having involvement in ejaculatory control. Scientists have long suspected a genetic link to certain forms of premature ejaculation. However, studies have been inconclusive in isolated the gene responsible for Lifelong PE. Other researchers have noted that men who have premature ejaculation have a faster neurological response in the pelvic muscles
Premature ejaculation as a medical problem under evidence-based criteria generated by the International Society for Sexual Medicine in 2014 as being not the result of a nonsexual mental illness, a problem in a given relationship, or caused by medication, by the person ejaculating around a minute after penetration and before the person wants to ejaculate, occurring for a duration longer than 6 months and happening almost every time, and causing significant distress for person. These factors are identified by talking with the person, not through any diagnostic test.
The 2007 ICD-10 defined PE as ejaculating without control, and within around 15 seconds
If you’re in a long-term relationship, you may benefit from having couples therapy. During these sessions, the therapist will:
encourage couples to explore any relationship issues they have, and give them advice about resolving them
show the couple techniques that can help you “unlearn” the habit of premature ejaculation (the two most popular techniques are the “squeeze” and “stop-go” techniques)
In the squeeze technique, your partner masturbates you, but stops before the point of ejaculation and squeezes the head of your penis for between 10 to 20 seconds. They then let go and wait for another 30 seconds before resuming masturbation. This process is carried out several times before ejaculation is allowed to occur. The stop-go technique is similar, but your partner doesn’t squeeze your penis. Once you feel more confident about delaying ejaculation, you and your partner can begin to have sex, stopping and starting as required.
These techniques may sound simple, but they require lots of practice.
It acts much faster than the SSRIs mentioned above and can be used “on demand”. You’ll usually be advised to take it between one and three hours before sex, but not more than once a day. Your response to the treatment will then be reviewed after four weeks (or after six doses), and again every six months.
‘Long love’ condoms
German scientists have come up with a slightly different approach that won’t cause vaginal irritation. It’s called the ‘long love condom’ and it contains a local anesthetic (benzocaine or lidocaine) inside it. Long love condoms are now being sold in many countries, under a variety of brand names.
You put these on the head of your penis to make it less sensitive. Leave it on for about 30 minutes. It must be washed off before sex so you don’t lose your erection or cause loss of sensation for your partner.
Switching medication
There are a number of medications that can be used if it’s thought SSRIs are responsible for causing delayed ejaculation. These include:
amantadine– originally designed to treat viral infections
buproprion– usually prescribed to help people quit smoking
yohimbine – originally designed to treat erectile dysfunction
This help block some of the chemical effects of SSRIs that may contribute towards delayed ejaculation.
Alcohol and drugs
Alcohol misuse and drug use can be separate underlying causes of delayed ejaculation, so addressing these problems may help.
Pseudoephedrine
Pseudoephedrine tablets may be tried, but these will need to be prescribed “off-label”. This means the medicine shows promise in treating delayed ejaculation but it hasn’t been licensed for this particular use (pseudoephedrine is normally used as a decongestant).
In 2006, we attended a conference on sexual medicine in Vienna. One of the speakers, Dr. Mehmet Sungur, claimed good results for the cognitive behavior (CBT) method of treatment for PE. The CBT method focuses on addressing the kind of thinking that has proved unhelpful.For example, a man may believe that ‘real men’ must thrust endlessly to give a woman pleasure. Such thinking is not only damaging to the man but wrong. Most women want penetration but also derive great pleasure from love play – often preferring fondling and oral sex to intercourse.
Counseling
There are sex therapists and other specialists to deal with ejaculation and other sexual problems. You may benefit from seeing one of these professionals.
Strengthen your muscles – Weak pelvic floor muscles sometimes contribute to PE. Kegel exercises may help strengthen them. Find the right muscles to tighten by stopping your urine in midstream. Hold them tight for 3 seconds and then release them for 3 seconds. Do this 10 times, at least 3 times a day.
Kegel exercises – which aim to strengthen the pelvic floor muscles, can help men with lifelong PE.
Physio-kinesiotherapy – to achieve muscle contraction
Electrostimulation – of the perineal floor
Biofeedback –which helped them understand how to control the muscle contractions in the perineal floor
After 12 weeks of treatment, over 80 percent of the participants gained a degree of control over their ejaculation reflex. They increased the time between penetration and ejaculation by at least 60 seconds.
Substance abuse is when you take drugs that are not legal. It’s also when you use alcohol, prescription medicine, and other legal substances too much or in the wrong way. So substance abuse, also known as drug abuse, is a patterned use of a drug in which the user consumes the substance in amounts or with methods which are harmful to themselves or others, and is a form of the substance-related disorder. Widely differing definitions of drug abuse are used in public health, medical and criminal justice contexts. In some cases, criminal or anti-social behavior occurs when the person is under the influence of a drug, and long-term personality changes in individuals may occur as well. In addition to possible physical, social, and psychological harm, use of some drugs may also lead to criminal penalties,
Types of Substance Abuse
Cigarettes
A distinctive smell on the breath and clothing
Cigarettes and lighter in his or her possession
Cigarette butts outside a bedroom window or in other odd places around the home.
Alcohol
Alcoholic beverages missing from the home storage cabinet
Alcohol or mouthwash (used to cover up alcohol) breath or hangover symptoms (nausea, vomiting, or a headache), if recently used.
Marijuana
Sweet smell on clothing or bloodshot eyes, if recently used, and frequent use of eyedrops to reduce the redness
Drug paraphernalia (pipes) in his or her possession
Carelessness in grooming, increased fatigue, and changes in eating and sleeping patterns, if using regularly
Inhalants
Chemical breath, red eyes, or stains on clothing or face, if recently used
Soaked rags or empty aerosol containers in the trash
Club drugs
Skin rash similar to acne
Small bottles with liquid or powder in his or her possession
Stimulants
A persistent runny nose and nosebleeds, injection marks on arms or other parts of the body, or long periods of time without sleep
Possession of drug paraphernalia, such as syringes, spoons with smoke stains, small pieces of glass, and razor blades
LSD or other Hallucinogens
Trance-like appearance with dilated pupils, if recently used
Small squares of blotter paper (sometimes stamped with cartoon characters) or other forms of the drug in his or her possession
Heroin
Very small pupils and a drowsy or relaxed look, if recently used
Possession of injecting supplies called an outfit or rig, that may consist of a spoon or bottle cap, syringe, tourniquet, cotton, and matches
Anabolic steroids
An unpleasant breath odor
Mood changes, including increased aggression
Changes in physical appearance that can’t be attributed to expected patterns of growth and development
Possession of medicines or syringes
Other general signs
Changes in sleeping patterns
Changes in appetite or weight loss
Changes in dress
Loss of interest and motivation
Hoarseness, wheezing, or a persistent cough
Causes and Effects of Substance Abuse
While many individuals experiment with drugs and/or alcohol, there is a fine line that can be crossed that differentiates between experimentation and substance abuse. When an individual abuses a substance or substances to such a degree that it begins to negatively affect his or her life and ability to function on a daily basis, that person is likely suffering from an addiction.
According to the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders, a person who is struggling with an addiction to drugs and/or alcohol will meet some or all of the following diagnostic criteria:
The consumption of the substance occurs in larger amounts, and more often than intended
Despite a desire to end, one’s substance abuse, unsuccessful attempts have been made
A great deal of time is spent acquiring, using, and recovering from the abuse of a substance
Overpowering cravings for one’s substance of choice are present
Failure to adhere to responsibilities occur due to substance abuse
Substance abuse continues despite problems caused by the substance abuse
Activities are given up in favor of substance abuse
Substance abuse occurs in a situation where it could be dangerous
One continues to abuse substances despite knowing that it has caused problems
Tolerance to a given substance or substances develops
Withdrawal symptoms manifest when one is not able to abuse a substance
If you or someone you care about meets the criteria listed above, it is important to seek treatment. By seeking treatment for a substance abuse problem, a brighter, happier, healthier tomorrow can be achieved.
Statistics of Substance Abuse
The Substance Abuse and Mental Health Services Administration (SAMHSA) reports that as many as twenty million Americans suffer from addictions to substances, but that only fifteen percent of those individuals actually seek treatment. Additionally, research conducted by the National Institute on Drug Abuse (NIDA) states that somewhere between eighty and ninety percent of people in the United States have abused substances during their lifetimes, with alcohol, marijuana, and prescription drugs being the most frequently abused substances in today’s society.
Causes & Risk Factors for Substance Abuse
There are many reasons why a person may turn to the abuse of drugs and/or alcohol. The following are the causes and risk factors that experts in the field of addiction believe to be true in terms of what makes some individuals more susceptible to abusing substances than others
Genetic – Researchers have discovered a set of genes that can make an individual vulnerable to developing a substance abuse problem. Given this information, if a person has a first-degree relative who has struggled with substance abuse, addiction, and/or chemical dependency, that individual is at risk of also struggling with similar challenges at some point during his or her lifetime.
Environmental – In addition to genetic influences, the environment and places one spends most of his or her time can have an impact on whether or not an individual will come to abuse substances. For example, those who are exposed to substance abuse from an early age are vulnerable to also abusing substances if they lack effective coping skills and proper social support. Additionally, if an individual resides in an impoverished area, has a history of experiencing trauma, or associates him or herself with others who also abuse drugs and/or alcohol, there is a higher risk for substance abuse to occur at some point in that person’s life.
Risk Factors of Substance Abuse
Possessing an impulsive personality
Possessing a novelty-seeking temperament
Personal history of trauma
The family history of substance abuse, addiction. and/or chemical dependency
The family history of mental health concerns
Personal history of mental health concerns
Living in an impoverished area
Lacking coping skills
Having an inadequate support system
Symptoms of Substance Abuse
Each substance affects people differently, but there are some signs of addiction that are fairly universal
The onset of withdrawal symptoms after the person suddenly stops using the substance
Feeling as though he or she must consume the substance to deal with the stresses of daily life
Increased tolerance levels requiring the person to consume more of the substance to achieve the same effect
Uncharacteristic or irrational behavior such as angry or violent outbursts
Dramatic changes in appearance like weight loss, hair loss, or skin problems
Loss of interesting previously enjoyable activities
Loss of important relationships
Lying to cover up consumption patterns
Impaired performance at work, home, or school
Incessantly borrowing money or stealing money
Legal, medical, or personal problems associated with consumption of the substance
Or
Decreased involvement in activities the person used to enjoy
Trouble managing responsibilities at work, school, or home
Problems with relationships related to substance use
Increase in risk-taking behaviors
A lot of time spent seeking the substance, or dealing with its aftereffects (e.g., being hungover)
Inability to stop using the substance or change behavior, even when the problems above are present
In some cases, physical or psychological signs may be observed as well
Substance abuse can wreak havoc on a person’s life. Depending on the longevity and severity of the addiction itself, the effects that could result can be life-changing. The effects listed below are among those that may occur if a person continues to abuse substances without seeking professional help:
Some individuals who are grappling with mental health concerns turn to the abuse of drugs and/or alcohol as a means of coping with their turmoil. Additionally, there are those who only begin to suffer from mental health disorders once they start abusing substances. In either case, it is possible for a person to seek treatment for an substance abuse and be diagnosed with a mental illness at the same time. The following mental health conditions are among those that people can suffer from at the same time as a substance abuse problem:
Effects of withdrawal: The longer than an individual abuses drugs and/or alcohol, the more likely that person will be to develop a tolerance to his or her substance(s) of choice. When this occurs, it can signify that that individual has become chemically dependent on that substance(s) and will thusly experience withdrawal symptoms in the event he or she ceases his or her substance abuse. The process of withdrawing from a substance can be extremely uncomfortable and, unfortunately, trigger a person to seek out his or her substance of choice once more. The following are signs and effects of withdrawal, which also suggest that a person is in need of treatment for his or her addiction:
For many substances of abuse, there is an ever-present risk of overdose when drugs and/or alcohol are used on an ongoing basis. Depending on the substance that is being abused, the telltale warning signs of overdose can vary. If any of the following occur, it should heed as a warning that emergency medical attention is needed in order to prevent a grave outcome
If a healthcare provider suspects that you are misusing alcohol or medications, he or she will first confirm that you are dependent on a harmful substance by:
The CAGE questionnaire is often used by healthcare providers to establish whether you have a drinking problem. It has four questions:
“Have you ever felt you should cut down on your drinking?”
“Have you ever felt annoyed by criticism about your drinking?”
“Have you ever felt guilty or bad about drinking?”
“Have you ever felt the need for a drink (an “eye-opener”) in the morning to steady your nerves?”
Rational scale to assess the harm of recreational drug use
Drug
Drug class
Physical
harm
Dependence
liability
Social
harm
Total
harm
Heroin
Opioid
2.78
3.00
2.54
2.77
Cocaine
CNS stimulant
2.33
2.39
2.17
2.30
Barbiturates
CNS depressant
2.23
2.01
2.00
2.08
Methadone
Opioid
1.86
2.08
1.87
1.94
Alcohol
CNS depressant
1.40
1.93
2.21
1.85
Ketamine
Dissociative anesthetic
2.00
1.54
1.69
1.74
Benzodiazepines
Benzodiazepine
1.63
1.83
1.65
1.70
Amphetamine
CNS stimulant
1.81
1.67
1.50
1.66
Tobacco
Tobacco
1.24
2.21
1.42
1.62
Buprenorphine
Opioid
1.60
1.64
1.49
1.58
Cannabis
Cannabinoid
0.99
1.51
1.50
1.33
Solvent drugs
Inhalant
1.28
1.01
1.52
1.27
4-MTA
Designer SSRA
1.44
1.30
1.06
1.27
LSD
Psychedelic
1.13
1.23
1.32
1.23
Methylphenidate
CNS stimulant
1.32
1.25
0.97
1.18
Anabolic steroids
Anabolic steroid
1.45
0.88
1.13
1.15
GHB
Neurotransmitter
0.86
1.19
1.30
1.12
Ecstasy
Empathogenic stimulant
1.05
1.13
1.09
1.09
Alkyl nitrites
Inhalant
0.93
0.87
0.97
0.92
Khat
CNS stimulant
0.50
1.04
0.85
0.80
Treatment of Substance Abuse
When you drink alcohol with some medications, the alcohol can make the effect of the medication dangerously strong. For example, taking alcohol with pills for sleeping, pain, anxiety, or depressioncan produce harmful effects. In particular, you should avoid alcohol if you take:
If you are addicted to smoking, you have probably tried to quit many times. But another serious try is always worth it, even if you are among the very old. Quitting at any age slows the decline in lung function.
Let your healthcare provider know that you want to stop smoking. Together, you will take the following steps
Get involved in a support group or buddy system to help keep you motivated
Self-help for substance abuse and co-occurring disorders
In addition to getting professional treatment, there are plenty of self-help steps you can take to address your substance abuse and mental health issues. Remember: Getting sober is only the beginning. As well as continuing mental health treatment, your sustained recovery depends on learning healthier coping strategies and making better decisions when dealing with life’s challenges.
Recovery tip 1
Learn how to manage stress – Drug and alcohol abuse often stems from misguided attempts to manage stress. Stress is an inevitable part of life, so it’s important to have healthy coping skills so you can deal with stress without turning to alcohol or drugs. Stress management skills go a long way towards preventing relapse and keeping your symptoms at bay.
Cope with unpleasant feelings – Many people turn to alcohol or drugs to cover up painful memories and emotions such as loneliness, depression, or anxiety. You may feel like doing drugs is the only way to handle unpleasant feelings, but Help guide’s free Emotional Intelligence Toolkit can teach you how to cope with difficult emotions without falling back on your addiction.
Know your triggers and have an action plan – When you’re coping with a mental disorder as well as a substance abuse problem, it’s especially important to know signs that your illness is flaring up. Common causes include stressful events, big life changes, or unhealthy sleeping or eating patterns. At these times, having a plan in place is essential to preventing a drink or drug relapse. Who will you talk to? What do you need to do to avoid slipping?
Recovery tip 2
Make a face-to-face connection with friends and family a priority – a Positive emotional connection to those around you is the quickest way to calm your nervous system. Try to meet up regularly with people who care about you. If you don’t have anyone you feel close to, it’s never too late to meet new people and develop meaningful friendships.
Get therapy or stay involved in a support group – Your chances of staying sober improve if you are participating in a social support group like Alcoholics Anonymous or Narcotics Anonymous or if you are getting therapy.
Follow doctor’s orders –Once you are sober and you feel better, you might think you no longer need medication or treatment. But arbitrarily stopping medication or treatment is a common reason for relapse in people with co-occurring disorders. Always talk with your doctor before making any changes to your medication or treatment routine.
Make healthy lifestyle changes
Exercise regularly – Exercise is a natural way to bust stress, relieve anxiety, and improve your mood and outlook. To achieve the maximum benefit, aim for at least 30 minutes of aerobic exercise on most days.
Practice relaxation techniques – When practiced regularly, relaxation techniques such as mindfulness meditation, progressive muscle relaxation, and deep breathing can reduce symptoms of stress, anxiety, and depression, and increase feelings of relaxation and emotional well-being.
Adopt healthy eating habits – Start the day right with breakfast, and continue with frequent small meals throughout the day. Going too long without eating leads to low blood sugar, which can make you feel more stressed or anxious. Getting enough healthy fats in your diet can help to boost your mood.
To stay alcohol- or drug-free for the long term, you’ll need to build a new, meaningful life where substance abuse no longer has a place.
Develop new activities and interests – Find new hobbies, volunteer activities, or work that gives you a sense of meaning and purpose. When you’re doing things you find fulfilling, you’ll feel better about yourself and substance use will hold less appeal.
Avoid the things that trigger your urge to use – If certain people, places, or activities trigger a craving for drugs or alcohol, try to avoid them. This may mean making major changes to your social life, such as finding new things to do with your old buddies—or even giving up those friends and making new connections.
Group support for substance abuse and co-occurring disorders
As with other addictions, groups are very helpful, not only in maintaining sobriety but also as a safe place to get support and discuss challenges. Sometimes treatment programs for co-occurring disorders provide groups that continue to meet on an aftercare basis. Your doctor or treatment provider may also be able to refer you to a group for people with co-occurring disorders.
Just make sure your group is accepting of the idea of co-occurring disorders and psychiatric medication. Some people in these groups, although well-meaning, may mistake taking psychiatric medication as another form of addiction. You want a place to feel safe, not pressured.
Helping a loved one with a substance abuse and mental health problem
Helping a loved one with both a substance abuse and a mental health problem can be a roller coaster. Resistance to treatment is common and the road to recovery can be long.
The best way to help someone is to accept what you can and cannot do. You cannot force someone to remain sober, nor can you make someone take their medication or keep appointments. What you can do is make positive choices for yourself, encourage your loved one to get help, and offer your support while making sure you don’t lose yourself in the process.
Seek support – Dealing with a loved one’s mental illness and substance abuse can be painful and isolating. Make sure you’re getting the emotional support you need to cope. Talk to someone you trust about what you’re going through. It can also help to get your own therapy or join a support group.
Set boundaries – Be realistic about the amount of care you’re able to provide without feeling overwhelmed and resentful. Set limits on disruptive behaviors and stick to them. Letting the co-occurring disorders take over your life isn’t healthy for you or your loved one.
Educate yourself – Learn all you can about your loved one’s mental health problem, as well as substance abuse treatment and recovery. The more you understand what your loved one is going through, the better able you’ll be to support recovery.
Panic disorder is an anxiety disorder characterized by reoccurring unexpected panic attacks. Panic attacks are sudden periods of intense fear that may include palpitations, sweating, shaking, shortness of breath, numbness, or a feeling that something really bad is going to happen. The maximum degree of symptoms occurs within minutes. There may be ongoing worries about having further attacks and avoidance of places where attacks have occurred in the past.
Types of Panic Disorder
Not only can panic attacks vary in intensity and duration, but they can also differ according to what prompted the attack. The DSM-5 lists two separate and distinct types of panic attacks
Expected panic attacks – These panic attacks are anticipated when one is subjected to specific cues or panic triggers. For instance, a person who has a fear of enclosed spaces (claustrophobia) may expect to have panic attacks when in an elevator or other cramped areas. A person who has a fear of flying (aerophobia) may predictably have a panic attack when boarding a plane, at the time of take-off, or at some time during the flight.
Unexpected Panic Attacks – These panic attacks occur suddenly without any obvious cause or indication. When an unexpected panic attack occurs, the person can be completely relaxed before symptoms develop. This type of panic attack does not accompany any conscious internal cues, such as having fearful thoughts, feelings of intense dread and anxiety, or uncomfortable physical sensations. Unexpected attacks also do not occur with external cues, such as specific phobias or being exposed to a frightening event or situation.
Causes of Panic Disorder
Panic disorder is associated with
Stressful life events –Graduating from college, getting married, having a first child, moving, and getting divorced are major life changes that can induce feelings of intense worry and apprehension.
Genetics – Like many other mood disorders, anxiety does tend to run in families, and having a parent with panic disorder can put you at higher risk for the condition.
At the doctor’s office or emergency department, you can expect the doctor to take a thorough history and perform a thorough physical examination.
In particular, the doctor will be concerned with the person’s past medical history, past history of any mental illness, and any surgery the person may have had. In addition to exploring whether the person suffers from any other mental illness, the practitioner often explores whether the panic attack sufferer has a specific anxiety disorder in addition to or instead of panic disorder, like post traumatic stress disorder , phobias, obsessive compulsive disorder, or generalized anxiety disorder.
The doctor likely will inquire about medications the person is taking or has recently taken and in what dosage.
The health-care professional will usually ask about any specific life stress the person may be experiencing.
The doctor will inquire about whether panic or anxiety illnesses “run in the family” and about any recent use of alcohol or other drugs by the person. During the evaluation for an illness is not the time to be untruthful about drug or alcohol habits because both of these factors are critical in the evaluation.
Also, the doctor is likely to inquire about caffeine intake and any over-the-counter or herbal medicines taken.
A physical exam will generally consist of a head-to-toe check of all the vital organ systems. The doctor will listen to the heart and lungs and may perform a brief neurologic exam designed to make sure the brain is functioning properly.
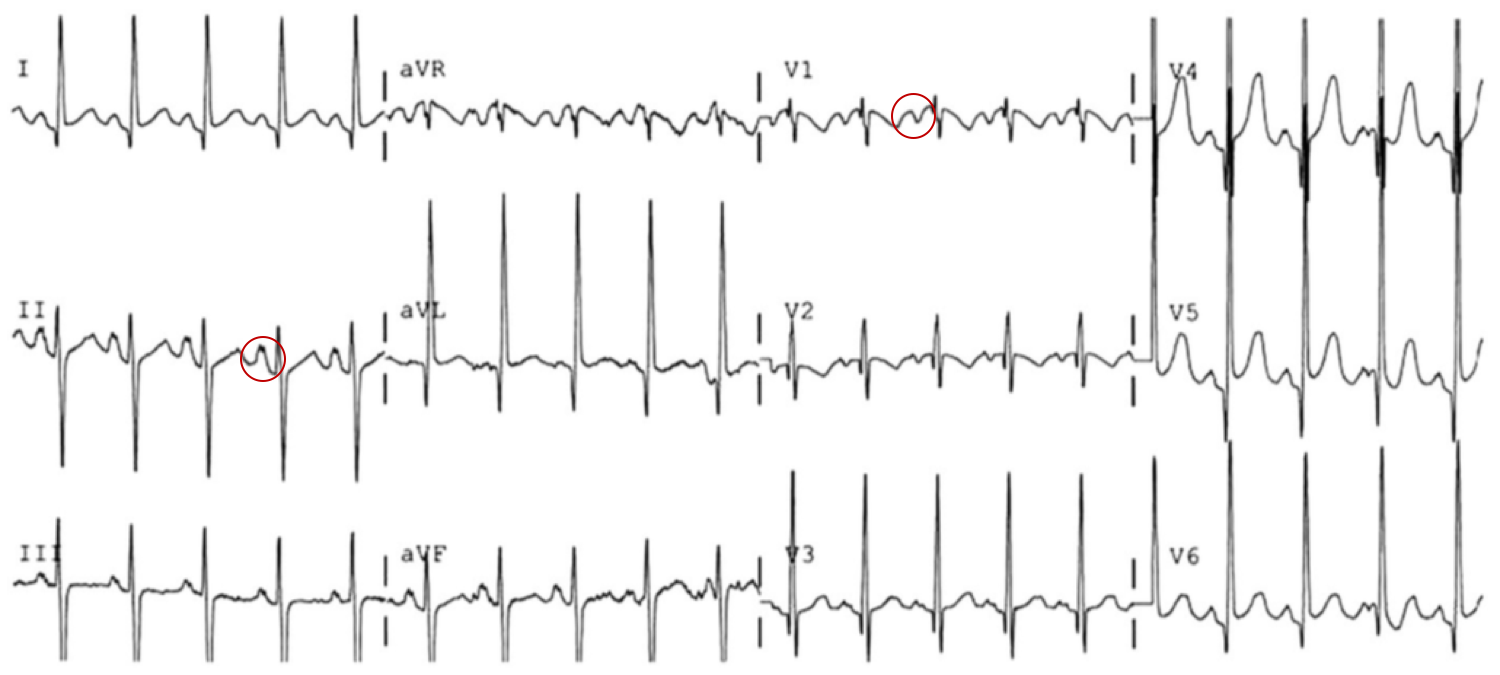
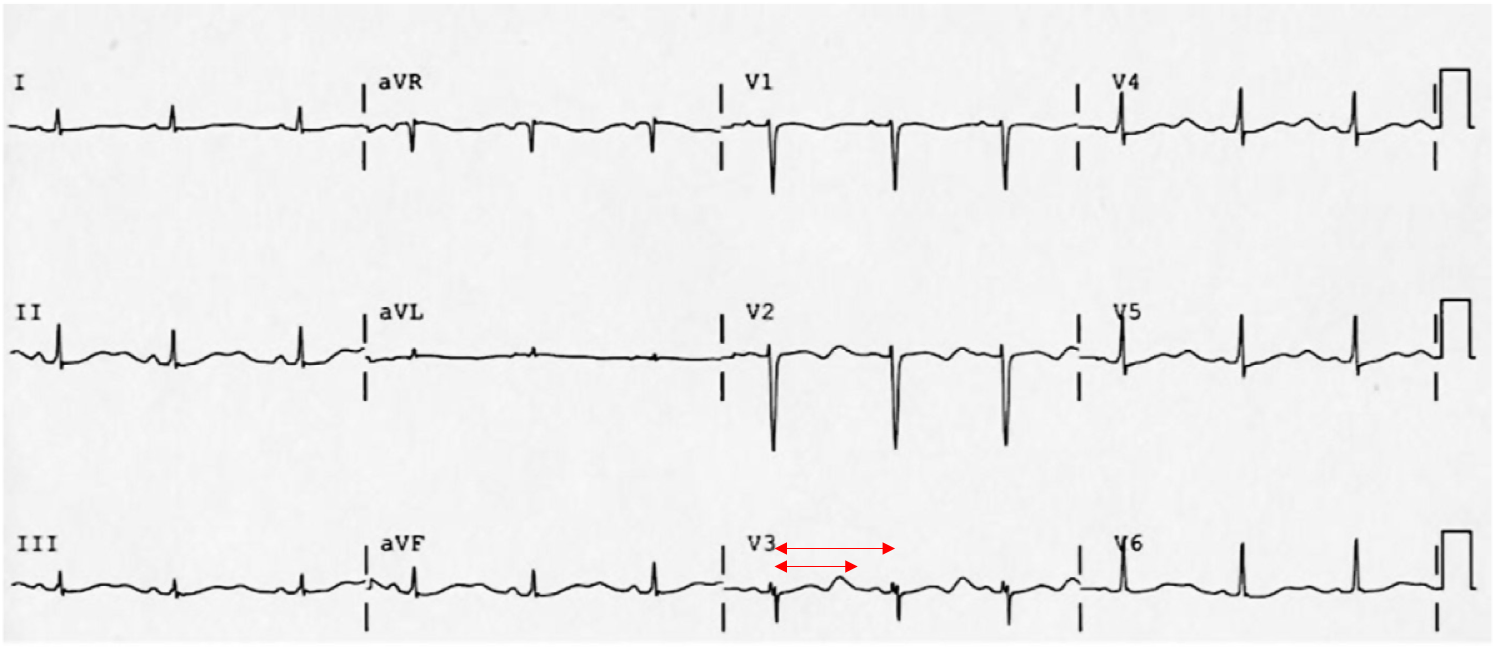
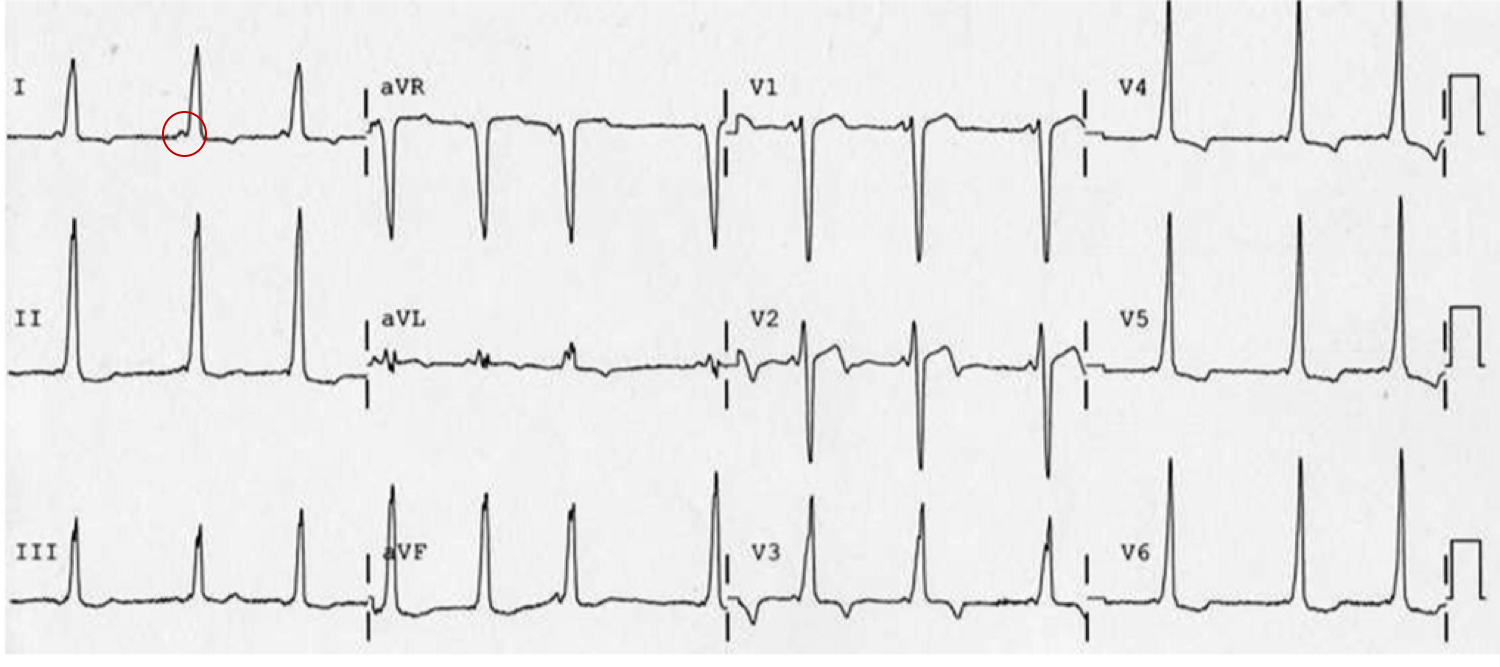
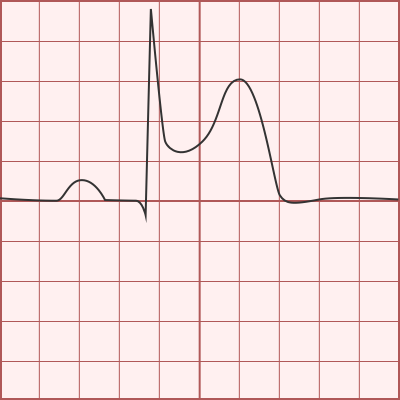
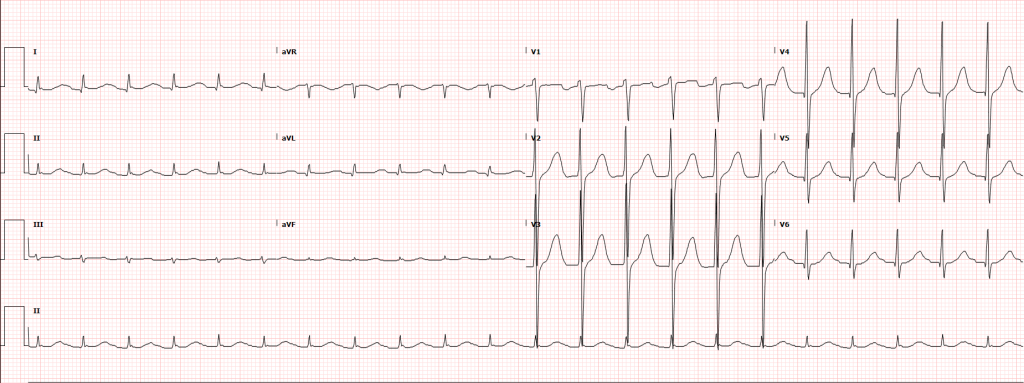
The doctor will use his or her best judgment regarding the necessity of ordering tests. Given the nature of the symptoms in a panic attack, the person will usually receive an ECG or heart tracing.
Should the doctor feel concerned that the symptoms might be caused by a medical disorder, blood tests, urine tests, drug screens, and even X-rays or CT scans might be ordered.
If the person has a family history of seizures or symptoms that are not typical for a panic attack, a neurologist may be asked to evaluate the person. There is some overlap between the symptoms of a panic attack and what is known as “partial seizures.” Distinguishing between the two is important because the treatment for each is quite different. A neurologist, if consulted, will order an EEG(electroencephalogram) to check for seizure activity in the brain. This is a painless test but does require some time to complete (typically overnight)
Treatment of Panic Disorder
Psychotherapy – All the effective psychotherapies for PTSD focus on the traumatic experience – or experiences – rather than your past life. You cannot change or forget what has happened. You can learn to think differently about it, about the world, and about your life.
EMDR (Eye Movement Desensitisation & Reprocessing) – This is a technique which uses eye movements to help the brain to process flashbacks and to make sense of the traumatic experience. It may sound odd, but it has been shown to work.
Group therapy – This involves meeting with a group of other people who have been through the same, or a similar traumatic event. It can be easier to talk about what happened if you are with other people who have been through a similar experience.
Exposure therapy for panic disorder – allows you to experience the physical sensations of panic in a safe and controlled environment, giving you the opportunity to learn healthier ways of coping. You may be asked to hyperventilate, shake your head from side to side, or hold your breath. These different exercises cause sensations similar to the symptoms of panic. With each exposure, you become less afraid of these internal bodily sensations and feel a greater sense of control over your panic.
Exposure therapy for panic disorder with agoraphobia– includes exposure to the situations you fear and avoid is also included in treatment. As in exposure therapy for specific phobias, you face the feared situation until the panic begins to go away. Through this experience, you learn that the situation isn’t harmful and that you have control over your emotions.
Medication – SSRI antidepressant tablets may help to reduce the strength of PTSD symptoms and relieve any depression that is also present. They will need to be prescribed by a doctor.
Prazosin – If symptoms include insomnia with recurrent nightmares, a drug called prazosin (Minipress) may help. Although not specifically FDA approved for panic disorder treatment, prazosin may reduce or suppress nightmares in many people with panic disorder
Benzodiazepines –Benzodiazepines are not recommended for the treatment of panic disorder due to a lack of evidence of benefit and risk of worsening panic disorder symptoms. Some authors believe that the use of benzodiazepines is contraindicated for acute stress, as this group of drugs promotes dissociation and ulterior revivals. Nevertheless, some use benzodiazepines with caution for short-term anxiety and insomnia. While benzodiazepines can alleviate acute anxiety, there is no consistent evidence that they can stop the development of panic disorder.
Glucocorticoids –Glucocorticoids may be useful for short-term therapy to protect against neurodegeneration caused by the extended stress response that characterizes panic disorder but long-term use may actually promote neurodegeneration.
Exercise, sport and physical activity– Physical activity can influence people’s psychological and physical health. The U.S. National Center for panic disorder recommends moderate exercise as a way to distract from disturbing emotions, build self-esteem and increase feelings of being in control again. They recommend a discussion with a doctor before starting an exercise program.
Cognitive Processing Therapy (CPT) – where you learn skills to understand how trauma changed your thoughts and feelings. Changing how you think about the trauma can change how you feel.
Prolonged Exposure (PE)– where you talk about your trauma repeatedly until memories are no longer upsetting. This will help you get more control over your thoughts and feelings about the trauma. You also go to places or do things that are safe, but that you have been staying away from because they remind you of the trauma.
Body-focused therapies – These don’t help PTSD directly, but can help to control your distress and hyperarousal, the feeling of being ‘on guard’ all the time. These include physiotherapy and osteopathy, but also complementary therapies such as massage, acupuncture, reflexology, yoga, meditation and tai chi. They can help you to develop ways of relaxing and managing stress.
Interoceptive techniques – Interoceptive exposure is sometimes used for panic disorder. People’s interoceptive triggers of anxiety are evaluated one-by-one before conducting interoceptive exposures, such as addressing palpitation sensitivity via light exercise. Though this practice is used in 12-20% of cases
Self-help tips for panic attacks – No matter how powerless or out of control you may feel about your panic attacks, it’s important to know that there are many things you can do to help yourself. The following self-help techniques can make a big difference to helping you overcome panic:
Learn about panic and anxiety – Simply knowing more about panic can go a long way towards relieving your distress. Read up on anxiety, panic disorder, and the fight-or-flight response experienced during a panic attack. You’ll learn that the sensations and feelings you have when you panic are normal and that you aren’t going crazy.
Avoid smoking, alcohol, and caffeine – These can all provoke panic attacks in people who are susceptible. If you need help to kick the cigarette habit, see How to Quit Smoking. Also, be careful with medications that contain stimulants, such as diet pills and non-drowsy cold medications.
Learn how to control your breathing – Hyperventilation brings on many sensations (such as lightheadedness and tightness of the chest) that occur during a panic attack. Deep breathing, on the other hand, can relieve the symptoms of panic. By learning to control your breathing, you can calm yourself down when you begin to feel anxious. And if you know how to control your breathing, you’re also less likely to create the very sensations that you’re afraid of.
Practice relaxation techniques – When practiced regularly, activities such as yoga, meditation, and progressive muscle relaxation strengthen the body’s relaxation response—the opposite of the stress response involved in anxiety and panic. And not only do these relaxation practices promote relaxation, but they also increase feelings of joy and equanimity.
Connect face-to-face with family and friends –Symptoms of anxiety can become worse when you feel isolated, so reach out to people who care about you on a regular basis. If you feel that you don’t have anyone to turn to, explore ways to meet new people and build supportive friendships.
Exercise regularly – Exercise is a natural anxiety reliever so try to get moving for at least 30 minutes on most days (three 10-minute sessions is just as good). Rhythmic aerobic exercise that requires moving both your arms and legs—like walking, running, swimming, or dancing—can be especially effective.
Get enough restful sleep – Insufficient or poor quality sleep can make anxiety worse, so try to get seven to nine hours of restful sleep a night. If sleeping well is a problem for you, these tips to getting a good night’s sleep can help.
Post traumatic stress disorder (PTSD) is a mental disorder that can develop after a person is exposed to a traumatic event, such as sexual assault, warfare, traffic collisions, or other threats on a person’s life. Symptoms may include disturbing thoughts, feelings, or dreams related to the events, mental or physical distress to trauma-related cues, attempts to avoid trauma-related cues, alterations in how a person thinks and feels, and an increase in the fight-or-flight response. These symptoms last for more than a month after the event. Young children are less likely to show distress but instead may express their memories through play. A person with PTSD is at a higher risk for suicide and intentional self-harm.
Types of Post Traumatic Stress Disorder
Are there different types of PTSD
Delayed-onset PTSD– if your symptoms emerge more than six months after experiencing trauma, this might be described as ‘delayed PTSD’ or ‘delayed-onset PTSD’.
Complex PTSD – if you experienced trauma at an early age or it lasted for a long time, you might be given a diagnosis of ‘complex PTSD’.
Birth trauma – PTSD that develops after a traumatic experience of childbirth is also known as ‘birth trauma’.
Causes of Post Traumatic Stress Disorder
Genetic –Anxiety disorders tend to run in families. People who have first-degree relatives who struggle with anxiety disorders are at a greater risk for developing the disorder themselves. While not a definitive cause for PTSD, it does make a person more vulnerable to developing the disorder after a traumatic event.
Brain Structures– It’s believed that certain areas of the brain that regulate emotions and fear are different than those who do not develop PTSD after a traumatic event.
Environmental – Those who have a history of trauma and stress are more likely to develop PTSD than those who do not have a similar history. Also, children who grow up in families where addiction is present are at greater risk for developing a post-traumatic stress disorder.
Psychological – People who struggle with certain types of mental illness, notably anxiety and depression, are at a higher risk of developing a post-traumatic stress disorder.
Violent personal assaults, such as sexual assault, mugging or robbery
Prolonged sexual abuse, violence or severe neglect
Witnessing violent deaths
Military combat
Being held hostage
Natural disasters, such as severe floods, earthquakes or tsunamis
A diagnosis of a life-threatening condition
An unexpected severe injury or death of a close family member or friend
Effects of Post Traumatic Stress Disorder
The effects of PTSD touch every area of an individual’s life leaving virtually nothing unscathed. The longer that PTSD exists without treatment, the greater the effects of PTSD on a person’s life. The most common effects of post-traumatic stress disorder may include:
PTSD can be particularly difficult to diagnose because numerous factors can lead to over-reporting (e.g., disability) and under-reporting (e.g., avoidance) symptoms, dysfunction, and distress.
Screening and assessment
A number of screening instruments are used for screening adults for PTSD, such as the PTSD Checklist for DSM-5 (PCL-5) and the Primary Care PTSD Screen for DSM-5(PC-PTSD-5).
There are also several screening and assessment instruments for use with children and adolescents. These include the Child PTSD Symptom Scale (CPSS), Child Trauma Screening Questionnaire, and UCLA Posttraumatic Stress Disorder Reaction Index for DSM-IV.
Diagnostic and statistical manual
PTSD was classified as an anxiety disorder in the DSM-IV but has since been reclassified as a “trauma- and stressor-related disorder” in the DSM-5. The DSM-5 diagnostic criteria for PTSD include four symptom clusters: re-experiencing, avoidance, negative alterations in cognition/mood, and alterations in arousal and reactivity.
International classification of diseases
The International Classification of Diseases and Related Health Problems 10 (ICD-10) classifies PTSD under “Reaction to severe stress, and adjustment disorders.”The ICD-10 criteria for PTSD include re-experiencing, avoidance, and either increased reactivity or inability to recall certain details related to the event.
Differential diagnosis of Post Traumatic Stress Disorder
A diagnosis of PTSD requires that the person has been exposed to an extreme stressor such as one that is life-threatening. Any stressor can result in a diagnosis of adjustment disorder and it is an appropriate diagnosis for a stressor and a symptom pattern that does not meet the criteria for PTSD, for example a partner being fired, or a spouse leaving. If any of the symptom pattern is present before the stressor, another diagnosis is required, such as brief psychotic disorder or major depressive disorder. Other differential diagnoses are schizophrenia or other disorders with psychotic features such as Psychotic disorders due to a general medical condition.
The symptom pattern for acute stress disorder must occur and be resolved within four weeks of the trauma. If it lasts longer, and the symptom pattern fits that characteristic of PTSD, the diagnosis may be changed.
Treatment of Post Traumatic Stress Disorder
Trauma-focused cognitive-behavioral therapy – involves gradually “exposing” yourself to feelings and situations that remind you of the trauma, and replacing distorted and irrational thoughts about the trauma with a more balanced picture.
Family therapy – can help your loved ones understand what you’re going through and help the family work through relationship problems.
EMDR (Eye Movement Desensitization and Reprocessing) – incorporates elements of cognitive-behavioral therapy with eye movements or other forms of rhythmic, left-right stimulation, such as hand taps or sounds. These techniques work by “unfreezing” the brain’s information processing system, which is interrupted in times of extreme stress.CBT can help you change these ‘extreme’ ways of thinking, which can also help you to feel better and to behave differently.
Psychotherapy – All the effective psychotherapies for PTSD focus on the traumatic experience – or experiences – rather than your past life. You cannot change or forget what has happened. You can learn to think differently about it, about the world, and about your life.
EMDR (Eye Movement Desensitisation & Reprocessing) – This is a technique which uses eye movements to help the brain to process flashbacks and to make sense of the traumatic experience. It may sound odd, but it has been shown to work.
Group therapy –This involves meeting with a group of other people who have been through the same, or a similar traumatic event. It can be easier to talk about what happened if you are with other people who have been through a similar experience.
Medication – SSRI antidepressant tablets may help to reduce the strength of PTSD symptoms and relieve any depression that is also present. They will need to be prescribed by a doctor.
Prazosin – If symptoms include insomnia with recurrent nightmares, a drug called prazosin (Minipress) may help. Although not specifically FDA approved for PTSD treatment, prazosin may reduce or suppress nightmares in many people with PTSD.
Benzodiazepines –Benzodiazepines are not recommended for the treatment of PTSD due to a lack of evidence of benefit and risk of worsening PTSD symptoms. Some authors believe that the use of benzodiazepines is contraindicated for acute stress, as this group of drugs promotes dissociation and ulterior revivals. Nevertheless, some use benzodiazepines with caution for short-term anxiety and insomnia. While benzodiazepines can alleviate acute anxiety, there is no consistent evidence that they can stop the development of PTSD and may actually increase the risk of developing PTSD 2–5 times.
Glucocorticoids –Glucocorticoids may be useful for short-term therapy to protect against neurodegeneration caused by the extended stress response that characterizes PTSD, but long-term use may actually promote neurodegeneration.
Cannabinoids –Evidence as of 2017 is insufficient to determine if medical cannabis useful for PTSD. Despite the uncertain evidence, use of cannabis or derived products is widespread among U.S. veterans with PTSD. The cannabinoid nabilone is sometimes used off-label for nightmares in PTSD. Although some short-term benefit was shown, adverse effects are common and it has not been adequately studied to determine efficacy. Additionally, there are other treatments with stronger efficacy and less risks (e.g., psychotherapy, serotonergic antidepressants, adrenergic inhibitors). The use of medical marijuana for PTSD is controversial, with only a handful of states permitting its use for that purpose.
Exercise, sport and physical activity– Physical activity can influence people’s psychological and physical health. The U.S. National Center for PTSD recommends moderate exercise as a way to distract from disturbing emotions, build self-esteem and increase feelings of being in control again. They recommend a discussion with a doctor before starting an exercise program.
Play therapy for children – Play is thought to help children link their inner thoughts with their outer world, connecting real experiences with abstract thought. Repetitive play can also be one way a child relives traumatic events, and that can be a symptom of trauma in a child or young person. Although it is commonly used, there have not been enough studies comparing outcomes in groups of children receiving and not receiving play therapy, so the effects of play therapy are not yet understood.
Military programs – Many veterans of the wars in Iraq and Afghanistan have faced significant physical, emotional, and relational disruptions. In response, the United States Marine Corps has instituted programs to assist them in re-adjusting to civilian life, especially in their relationships with spouses and loved ones, to help them communicate better and understand what the other has gone through. Walter Reed Army Institute of Research (WRAIR) developed the Battlemind program to assist service members to avoid or ameliorate PTSD and related problems. Wounded Warrior Project partnered with the US Department of Veterans Affairs to create Warrior Care Network, a national health system of PTSD treatment centers
Cognitive Processing Therapy (CPT) – where you learn skills to understand how trauma changed your thoughts and feelings. Changing how you think about the trauma can change how you feel.
Prolonged Exposure (PE) – where you talk about your trauma repeatedly until memories are no longer upsetting. This will help you get more control over your thoughts and feelings about the trauma. You also go to places or do things that are safe, but that you have been staying away from because they remind you of the trauma.
Body-focused therapies –These don’t help PTSD directly, but can help to control your distress and hyperarousal, the feeling of being ‘on guard’ all the time. These include physiotherapy and osteopathy, but also complementary therapies such as massage, acupuncture, reflexology, yoga, meditation and tai chi. They can help you to develop ways of relaxing and managing stress.
The way of best works –At present, there is evidence that EMDR, Cognitive Behavioural Therapy, behavior therapy, and antidepressants are all effective. There is not enough information for us to show that one of these treatments is better than another. There is not yet any evidence that other forms of psychotherapy or counseling are helpful for PTSD.
Getting better – Try to start doing the normal things of life that have nothing to do with your past experiences of trauma. This could include finding friends, getting a job, doing regular exercise, learning relaxation techniques, developing a hobby or having pets. This helps you slowly to trust the world around you.
Lack of trust in other people– and the world in general – is central to complex PTSD. Treatment often needs to be longer to allow you to develop a secure relationship with a therapist – to experience that it is possible to trust someone in this world without being hurt or abused. The work will often happen in 3 stages:
Stabilization – learn how to understand and control your distress and emotional cutting-off, or ‘dissociation’. This can involve ‘grounding’ techniques to help you to stay in the present – concentrating on ordinary physical feelings to remind you that you are living in the present, not the abusive and traumatic past.start to ‘disconnect’ your physical symptoms of fear and anxiety from the memories and emotions that produce them, making them less frightening. Start to be able to tolerate day-to-day life without experiencing anxiety or flashbacks.
Trauma-focussed Therapy – EMDR or Cognitive Behavioural Therapy can help you to remember your traumatic experiences with less distress and more control. Other psychotherapies, including psychodynamic psychotherapy, can also be helpful. Care needs to be taken in complex PTSD because these treatments can make the situation worse if not used properly.
Reintegration – You begin to develop a new life for yourself. You become able to use your skills or learn new ones and to make satisfying relationships in the real world. Medication can be used if you feel too distressed or unsafe, or if psychotherapy is not possible. It can include both antidepressants and antipsychotic medication – but not usually tranquillisers or sleeping tablets.
Exercise, sport and physical activity – Physical activity can influence people’s psychological and physical health. The U.S. National Center for PTSD recommends moderate exercise as a way to distract from disturbing emotions, build self-esteem and increase feelings of being in control again. They recommend a discussion with a doctor before starting an exercise program.
Play therapy for children – Play is thought to help children link their inner thoughts with their outer world, connecting real experiences with abstract thought. Repetitive play can also be one way a child relives traumatic events, and that can be a symptom of trauma in a child or young person. Although it is commonly used, there have not been enough studies comparing outcomes in groups of children receiving and not receiving play therapy, so the effects of play therapy are not yet understood.
For friends, relatives & colleagues
Do …….
watch out for any changes in behaviour – poor performance at work, lateness, taking sick leave, minor accidents
watch for anger, irritability, depression, lack of interest, lack of concentration
take time to allow a trauma survivor to tell their story
ask general questions
let them talk, don’t interrupt the flow or come back with your own experiences.
Don’t …….
tell a survivor you know how they feel – you don’t
tell a survivor they’re lucky to be alive – it doesn’t feel like that to them
minimise their experience – “it’s not that bad, surely …
suggest that they just need to “pull themselves together.
Risk Factors and Resilience Factors for PTSD
Some factors that increase risk for PTSD include:
Living through dangerous events and traumas
Getting hurt
Seeing another person hurt, or seeing a dead body
Childhood trauma
Feeling horror, helplessness, or extreme fear
Having little or no social support after the event
Dealing with extra stress after the event, such as loss of a loved one, pain and injury, or loss of a job or home
Having a history of mental illness or substance abuse
Seeking out support from other people, such as friends and family
Finding a support group after a traumatic event
Learning to feel good about one’s own actions in the face of danger
Having a positive coping strategy, or a way of getting through the bad event and learning from it
Being able to act and respond effectively despite feeling fear
Researchers are studying the importance of these and other risk and resilience factors, including genetics and neurobiology.
As well as many of the symptoms of PTSD described above, you may find that you:
feel shame and guilt
have a sense of numbness, a lack of feelings in your body
can’t enjoy anything
control your emotions by using street drugs, alcohol, or by harming yourself
cut yourself off from what is going on around you (dissociation)
have physical symptoms caused by your distress
find that you can’t put your emotions into words
want to kill yourself
take risks and do things on the ‘spur of the moment’.
It is worse if
it happens at an early age – the earlier the age, the worse the trauma
it is caused by a parent or other care giver
the trauma is severe
the trauma goes on for a long time
you are isolated
you are still in touch with the abuser and/or threats to your safety.
Support to prevent furthers PTSD
If stress and other problems caused by a traumatic event affect your life, see your doctor or mental health professional. You can also take these actions as you continue with treatment for post-traumatic stress disorder:
Follow your treatment plan – Although it may take a while to feel benefits from therapy or medications, treatment can be effective, and most people do recover. Remind yourself that it takes time. Following your treatment plan and routinely communicating with your mental health professional will help move you forward.
Learn about PTSD – This knowledge can help you understand what you’re feeling, and then you can develop coping strategies to help you respond effectively.
Take care of yourself – Get enough rest, eat a healthy diet, exercise and take time to relax. Try to reduce or avoid caffeine and nicotine, which can worsen anxiety.
Don’t self-medicate – Turning to alcohol or drugs to numb your feelings isn’t healthy, even though it may be a tempting way to cope. It can lead to more problems down the road, interfere with effective treatments and prevent real healing.
Break the cycle – When you feel anxious, take a brisk walk or jump into a hobby to re-focus.
Stay connected – Spend time with supportive and caring people — family, friends, faith leaders or others. You don’t have to talk about what happened if you don’t want to. Just sharing time with loved ones can offer healing and comfort.
Consider a support group – Ask your mental health professional for help finding a support group, or contact veterans’ organizations or your community’s social services system. Or look for local support groups in an online directory.
Remember that you can’t change someone. However, you can
Learn about PTSD – This can help you understand what your loved one is going through.
Recognize that avoidance and withdrawal are part of the disorder – If your loved one resists your help, allow space and let your loved one know that you’re available when he or she is ready to accept your help.
Offer to attend medical appointments – If your loved one is willing, attending appointments can help you understand and assist with treatment.
Be willing to listen – Let your loved one know you’re willing to listen, but you understand if he or she doesn’t want to talk. Try not to force your loved one to talk about the trauma until he or she is ready.
Encourage participation – Plan opportunities for activities with family and friends. Celebrate good events.
Make your own health a priority – Take care of yourself by eating healthy, being physically active and getting enough rest. Take time alone or with friends, doing activities that help you recharge.
Seek help if you need it – If you have difficulty coping, talk with your doctor. He or she may refer you to a therapist who can help you work through your stress.
Stay safe – Plan a safe place for yourself and your children if your loved one becomes violent or abusive.
CBT (Cognitive Behavioral Therapy) is a short-term form of behavioral treatment that helps people problem-solve and see the relationship between beliefs, thoughts, and feelings, and subsequent behavior patterns and actions. Through CBT, people learn that their perceptions directly influence their responses to specific situations. In other words, a person’s thought process informs his or her behaviors and actions. Cognitive behavioral therapy is not a distinct treatment technique; rather, it is a general term which refers to a group of therapies that have certain similarities in therapeutic methodology.
Types of Cognitive Behavioral Therapy
CBT takes place over a couple of sessions that can last up to 12 accumulated hours by design. This technique was first implemented and developed on soldiers overseas in active duty by David M. Rudd to prevent suicide.
Breakdown of treatment
Orientation
Commitment to treatment
Crisis response and safety planning
Means restriction
Survival kit
Reasons for living card
Model of suicidality
Treatment journal
Lessons learned
Skill focus
Skill development worksheets
Coping cards
Demonstration
Practice
Skill refinement
Relapse prevention
Skill generalization
Skill refinement
The principle of Cognitive Behavioral Therapy
CBT is based on several core principles, including
People suffering from psychological problems can learn better ways of coping with them, thereby relieving their symptoms and becoming more effective in their lives.
CBT treatment usually involves efforts to change thinking patterns. These strategies might include
Learning to recognize one’s distortions in thinking that are creating problems, and then to reevaluate them in light of reality.
Gaining a better understanding of the behavior and motivation of others.
Using problem-solving skills to cope with difficult situations.
Learning to develop a greater sense of confidence is one’s own abilities.
CBT treatment also usually involves efforts to change behavioral patterns. These strategies might include
Facing one’s fears instead of avoiding them.
Using role-playing to prepare for potentially problematic interactions with others.
Learning to calm one’s mind and relax one’s body.
How you prepare for Cognitive Behavioral Therapy
You might decide on your own that you want to try cognitive behavioral therapy. Or a doctor or someone else may suggest therapy to you. Here’s how to get started:
Find a therapist – You can get a referral from a doctor, health insurance plan, friend or other trusted source. Many employers offer counseling services or referrals through employee assistance programs (EAPs). Or you can find a therapist on your own — for instance, through a local or state psychological association or by searching the Internet.
Understand the costs – If you have health insurance, find out what coverage it offers for psychotherapy. Some health plans cover only a certain number of therapy sessions a year. Also, talk to your therapist about fees and payment options.
Review your concerns – Before your first appointment, think about what issues you’d like to work on. While you can also sort this out with your therapist, having some sense in advance may provide a starting point.
Steps in CBT
The basic steps in a cognitive-behavioral assessment include
Step 1: Identity critical behaviors step 2: Determine whether critical behaviors are excesses or deficits
Step 3: Evaluate critical behaviors for frequency, duration, or intensity (obtain a baseline)
Step 4: If excess, attempt to decrease the frequency, duration, or intensity of behaviors; if deficits, attempt to increase behaviors
CBT typically includes these steps
Identify troubling situations or conditions in your life – These may include such issues as a medical condition, divorce, grief, anger, or symptoms of mental illness. You and your therapist may spend some time deciding what problems and goals you want to focus on.
Become aware of your thoughts, emotions, and beliefs about these problems – Once you’ve identified the problems to work on, your therapist will encourage you to share your thoughts about them. This may include observing what you tell yourself about an experience (self-talk), your interpretation of the meaning of a situation, and your beliefs about yourself, other people and events. Your therapist may suggest that you keep a journal of your thoughts.
Identify negative or inaccurate thinking – To help you recognize patterns of thinking and behavior that may be contributing to your problem, your therapist may ask you to pay attention to your physical, emotional and behavioral responses in different situations.
Reshape negative or inaccurate thinking – Your therapist will likely encourage you to ask yourself whether your view of a situation is based on fact or on an inaccurate perception of what’s going on. This step can be difficult. You may have long-standing ways of thinking about your life and yourself. With practice, helpful thinking and behavior patterns will become a habit and won’t take as much effort.
Length of therapy
CBT is generally considered short-term therapy — about 10 to 20 sessions. You and your therapist can discuss how many sessions may be right for you. Factors to consider include:
Type of disorder or situation
The severity of your symptoms
How long you’ve had your symptoms or have been dealing with your situation
How quickly you make progress
How much stress you’re experiencing
How much support you receive from family members and other people
CBT combines cognitive therapy and behavior therapy
CBT focuses on changing unhelpful or unhealthy thoughts and behaviors. It is a combination of two therapies: ‘cognitive therapy’ and ‘behavior therapy’. The basis of both these techniques is that healthy thoughts lead to healthy feelings and behaviors.
Cognitive therapy – The aim of cognitive therapy is to change the way the person thinks about the issue that’s causing concern. Negative thoughts cause self-destructive feelings and behaviors. For example, someone who thinks they are unworthy of love or respect may feel withdrawn in social situations and behave shyly. Cognitive therapy challenges those thoughts and provides the person with healthier strategies. Many techniques are available. One technique involves asking the person to come up with evidence to ‘prove’ that they are unlovable. This may include prompting the person to acknowledge the family and friends who love and respect them. This evidence helps the person to realize that their belief is false. This is called ‘cognitive restructuring’. The person learns to identify and challenge negative thoughts, and replace them with more realistic and positive thoughts.
Behavior therapy – The aim of behavior therapy is to teach the person techniques or skills to alter their behavior. For example, a person who behaves shyly at a party may have negative thoughts and feelings about themselves. They may also lack social skills. Behavior therapy teaches the person more helpful behaviors. For example, they may be taught conversational skills that they practice in therapy and in social situations. Negative thoughts and feelings reduce as the person discovers they can enjoy themselves in social situations.
Treatment with CBT
The details of treatment will vary according to the person’s problem. However, CBT typically includes the following:
Assessment – this may include filling out questionnaires to help you describe your particular problem and pinpoint distressing symptoms. You will be asked to complete forms from time to time so that you and your therapist can plot your progress and identify problems or symptoms that need extra attention
Personal education – your therapist provides written materials (such as brochures or books) to help you learn more about your particular problem. The saying ‘knowledge is power’ is a cornerstone of CBT. A good understanding of your particular psychological problem will help you to dismiss unfounded fears, which will help to ease your anxiety and other negative feelings
Goal setting – your therapist helps you to draw up a list of goals you wish to achieve from therapy (for example, you may want to overcome your shyness in social settings). You and your therapist work out practical strategies to help fulfill these goals
The practice of strategies – you practice your new strategies with the therapist. For example, you may role-play difficult social situations or realistic self-talk (how you talk to yourself in your head) to replace unhealthy or negative self-talk
Homework – you will be expected to actively participate in your own therapy – for example, the therapist may ask you to keep a diary – and you are encouraged to use the practical strategies during the course of your daily life and report the results to the therapist.
Graded Exposure – Exposure is a cognitive behavioral therapy exercise designed to reduce anxiety and fear through repeated contact with what is feared. This has been to shown to be among the most effective treatments for any psychological problem. The underlying theory has to do with avoidance of things that we fear resulting in increased fear and anxiety. By systematically approaching what you might normally avoid, a significant and lasting reduction in anxiety takes place.
Successive Approximation – Successive approximation is a cognitive behavioral therapy exercise that helps people tackle difficult or overwhelming goals. By systematically breaking large tasks into smaller steps, or by performing a task similar to the goal, but less difficult, people are able to gain mastery over the skills needed to achieve the larger goal.
Mindfulness Meditation – Mindfulness meditation is a cognitive behavioral therapy exercise that helps people disengage from harmful ruminating or obsessing by learning to connect to the present moment. Mindfulness comes from Buddhist meditation and is the subject of a significant amount of new research on the effective treatment of psychological problems.
Skills Training – Skills Training is a cognitive behavioral therapy exercise to help remedy skills deficits, and works through modeling, direct instruction, and role-plays. The most common subjects of skills training are social skills training, assertiveness training, and communication training.
Problem Solving – Problem Solving is a cognitive behavioral therapy exercise to help people take an active role in finding solutions to problems. Chronic mood problems or repeated disappointment can result in people taking a passive role when difficult situations arise. By teaching people effective problem-solving strategies, they are able to regain control and make the best of difficult situations.
Relaxation Breathing Training – Relaxation training is a cognitive behavioral therapy exercise designed to help people reduce physiological symptoms of anxiety, such as shortness of breath, rapid heart rate, dizziness, etc. By reducing the body’s anxious arousal, people are able to think more clearly, thus increasing feelings of comfort and further decreasing anxiety symptoms.
Origins of Cognitive Behavior Therapy
The idea for developing this form of psychotherapy took root when Aaron Beck began to notice that his patients with depression often verbalized thoughts that were lacking in validity and noted characteristic “cognitive distortions” in their thinking. His empirical observations led him to start viewing depression not so much as a mood disorder but as a cognitive disorder. Based on his clinical observations and empirical findings, Beck outlined a new cognitive theory of depression. He published Cognitive Therapy for Depression (Beck, Rush, Shaw, and Emery, 1979) after having published a study that evaluated and demonstrated the efficacy of cognitive therapy. The combination of a detailed treatment protocol manual with outcome research was an innovation in psychotherapy practice that had only previously been attempted by behavior therapists in treating discrete behavioral problems. By accomplishing the same feat with a more complex set of clinical interventions that included cognitive, emotional, and behavioral components, Beck pioneered a model for what psychologists many years later defined as an “empirically validated psychological treatment.”
Other clinicians and researchers became interested and began developing CBT treatment protocols and evaluating their efficacy. Specific treatment protocols were developed for some psychiatric disorders. As behavioral strategies were incorporated, the term cognitive therapy changed to cognitive behavior therapy. Today CBT is the most extensively researched of all psychotherapies with several evidence-based treatment protocols.
Cognitive Model
CBT is based on a straightforward, common-sense model of the relationships among cognition, emotion, and behavior.[rx][rx][rx][rx]
Three aspects of cognition are emphasized:
Automatic thoughts
Cognitive distortions
Underlying beliefs or schemas
Automatic Thoughts
An individual’s immediate, unpremeditated interpretations of events are referred to as automatic thoughts. Automatic thoughts shape both the individual’s emotions and their actions in response to events. For example, a friend may cross you in the hallway and not say hello to you. If you were to have an automatic thought of “he hates me,” or “I have done something to anger him,” it is likely to impact your mood and cause you to feel upset and also to behave in an avoidant manner when you see him next. On the other hand, if you had the automatic thought, “he is in a hurry,” you would not be too concerned, and you would not be avoidant when you were to see him next.
CBT is based on the observation that dysfunctional automatic thoughts that are exaggerated, distorted, mistaken, or unrealistic in other ways, play a significant role in psychopathology.
Cognitive Distortions
Errors in logic are quite prevalent in patients with psychological disorders. They lead individuals to erroneous conclusions. Below are some cognitive distortions that are commonly seen in individuals with psychopathology:
Dichotomous thinking – Things are seen regarding two mutually exclusive categories with no shades of gray in between
Overgeneralization – Taking isolated cases and using them to make wide generalizations
Selective abstraction – Focusing exclusively on certain, usually negative or upsetting, aspects of something while ignoring the rest
Disqualifying the positive – Positive experiences that conflict with the individual’s negative views are discounted
Mind reading – Assuming the thoughts and intentions of others
Fortune telling – Predicting how things will turn out before they happen
Minimization – Positive characteristics or experiences are treated as real but insignificant
Catastrophizing – Focusing on the worst possible outcome, however unlikely, or thinking that a situation is unbearable or impossible when it is just uncomfortable
Emotional reasoning – Making decisions and arguments based on how you feel rather than objective reality
“Should” statements – Concentrating on what you think “should” or “ought to be” rather than the actual situation you are faced with or having rigid rules which you always apply no matter the circumstances
Personalization, blame, or attribution – Assuming you are completely or directly responsible for a negative outcome. When applied to others consistently, the blame is the distortion
Underlying Beliefs
Underlying beliefs shape the perception and interpretation of events. Belief systems or schemas take shape as we go through life experiences. They are defined as templates or rules for information processing that underlie the most superficial layer of automatic thoughts. Beliefs are understood at two levels in CBT:
Core Beliefs
The central ideas about self and the world
The most fundamental level of belief
They are global, rigid, and overgeneralized
Examples of dysfunctional core beliefs
“I am unlovable.”
“I am inadequate.”
“The world is a hostile and dangerous place.”
Intermediate Beliefs
Consist of assumptions, attitudes, and rules
Influenced in their development by the core beliefs
Examples of dysfunctional intermediate beliefs
“To be accepted, I should always please others.”
“I should be excellent at everything I do to be considered adequate.”
“It is best to have as little as possible to do with people.”
Schizophrenia is a mental disorder characterized by abnormal social behavior and failure to understand reality. Common symptoms include false beliefs, unclear or confused thinking, hearing voices that others do not, reduced social engagement and emotional expression, and a lack of motivation. People with schizophrenia often have additional mental health problems such as anxiety,depressive, or substance-use disorders. Symptoms typically come on gradually, begin in young adulthood, and last a long time.
Subtypes of Schizophrenia
With the publication of DSM-5, the APA removed all sub-classifications of schizophrenia. The five sub-classifications included in DSM-IV-TR were
Paranoid type – Delusions or auditory hallucinations are present, but thought disorder, disorganized behavior, or affective flattening are not. Delusions are persecutory and/or grandiose, but in addition to these, other themes such as jealousy, religiosity, or somatization may also be present.
Disorganized type – Named hebephrenic schizophrenia in the ICD. Where thought disorder and flat affect are present together.
Catatonic type – The subject may be almost immobile or exhibit agitated, purposeless movement. Symptoms can include catatonic stupor and waxy flexibility.
Undifferentiated type – Psychotic symptoms are present but the criteria for paranoid, disorganized, or catatonic types have not been met.
Residual type – Where positive symptoms are present at a low intensity only.
The ICD-10 defines additional subtypes
Post-schizophrenic depression – A depressive episode arising in the aftermath of a schizophrenic illness where some low-level schizophrenic symptoms may still be present.
Simple schizophrenia – Insidious and progressive development of prominent negative symptoms with no history of psychotic episodes.
Other schizophrenia – include cenesthopathic schizophrenia and schizophreniform disorder NOS.
Causes of Schizophrenia
While the causes of schizophrenia are not fully known, it seems to result from a complex interaction between genetic and environmental factors.
Genetic causes – While schizophrenia runs in families, about 60% of schizophrenics have no family members with the disorder. Furthermore, individuals who are genetically predisposed to schizophrenia don’t always develop the disease, which shows that biology is not destiny.
Environment – Exposure to viruses or malnutrition before birth, particularly in the first and second trimesters has been shown to increase the risk of schizophrenia. Inflammation or autoimmune diseases can also lead to increased immune system
Brain chemistry – Problems with certain brain chemicals, including neurotransmitters called dopamine and glutamate, may contribute to schizophrenia. Neurotransmitters allow brain cells to communicate with each other. Networks of neurons are likely involved as well.
Substance use – Some studies have suggested that taking mind-altering drugs during teen years and young adulthood can increase the risk of schizophrenia. A growing body of evidence indicates that smoking marijuana increases the risk of psychotic incidents and the risk of ongoing psychotic experiences. The younger and more frequent the use, the greater the risk. Another study has found that smoking marijuana led to earlier onset of schizophrenia and often preceded the manifestation of the illness.
Environmental Causes
Studies suggest that inherited genes make a person vulnerable to schizophrenia and then environmental factors act on this vulnerability to trigger the disorder.
More and more research is pointing to stress, either during pregnancy or at a later stage of development, as a major environmental factor. Stress-inducing factors could include:
Prenatal exposure to a viral infection
Low oxygen levels during birth (from prolonged labor or premature birth
In addition to abnormal brain chemistry, abnormalities in brain structure may also play a role in schizophrenia. However, it is highly unlikely that schizophrenia is the result of any one problem in any one region of the brain
Behaviors that are early warning signs of schizophrenia include
Hearing or seeing something that isn’t there
A constant feeling of being watched
The peculiar or nonsensical way of speaking or writing
Anyone who experiences several of these symptoms for more than two weeks should seek help immediately.
Symptoms of Schizophrenia
Positive major symptomsare disturbances that are “added” to the person’s personality.
Delusions – the patient displays false beliefs, which can take many forms, such as delusions of persecution, or delusions of grandeur. They may feel others are attempting to control them remotely. Or, they may think they have extraordinary powers and abilities.
Thought disorder – the person may jump from one subject to another for no logical reason. The speaker may be hard to follow or erratic.
Disordered thinking and speech –moving from one topic to another, in a nonsensical fashion. Individuals may also make up their own words or sounds, rhyme in a way that doesn’t make sense or repeats words and ideas.
Disorganized behavior –this can range from having problems with routine behaviors like hygiene or choosing appropriate clothing for the weather, to unprovoked outbursts, too impulsive and uninhibited actions. A person may also have movements that seem anxious, agitated, tense or constant without any apparent reason.
Negative symptoms – these refer to elements that are taken away from the individual. For example, the absence of facial expressions or lack of motivation.
Cognitive symptoms– these affect the person’s thought processes. They may be positive or negative symptoms, for example, poor concentration is a negative symptom.
Emotional symptoms – these are usually negative symptoms, such as blunted emotions.
Other symptoms may include
Lack of motivation (avolition) – the patient loses their drive. Everyday actions, such as washing and cooking, are neglected.
Social withdrawal – when a patient with schizophrenia withdraws socially, it is often because they believe somebody is going to harm them.
Unawareness of illness– as the hallucinations and delusions seem so real for patients, many of them may not believe they are ill. They may refuse to take medication for fear of side effects, or for fear that the medication may be poison, for example.
Cognitive difficulties – the patient’s ability to concentrate, recall things, plan ahead, and to organize their life are affected. Communication becomes more difficult.
Negative symptoms are capabilities that are “lost” from the person’s personality.
Social withdrawal
Extreme apathy (lack of interest or enthusiasm)
Lack of drive or initiative
Emotional flatness
Diagnosis of Schizophrenia
Determining a diagnosis of schizophrenia may include
Physical exam – This may be done to help rule out other problems that could be causing symptoms and to check for any related complications.
Tests and screenings – These may include tests that help rule out conditions with similar symptoms, and screening for alcohol and drugs. The doctor may also request imaging studies, such as an MRI or CT scan.
Psychiatric evaluation – A doctor or mental health professional checks mental status by observing appearance and demeanor and asking about thoughts, moods, delusions, hallucinations,substance use, and potential for violence or suicide. This also includes a discussion of family and personal history.
Diagnostic criteria for schizophrenia – A doctor or mental health professional may use the criteria in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), published by the American Psychiatric Association.
Schizophrenia requires long-term treatment.Most people with schizophrenia need to continue treatment even when they’re feeling better to prevent new episodes and stay symptom-free. Treatment can change over time, though, so your doctor may be able to lower the dosage or change medication as your symptoms improve.
Therapy – can help you improve coping and life skills, manage stress, address relationship issues, and improve communication. Group therapy can also connect you to others who are in a similar situation and gain valuable insight into how they’ve overcome challenges.
The 7 keys to self-help
Seek social support – Not only are friends and family vital to helping you get the right treatment and keeping your symptoms under control, regularly connecting with others face-to-face is the most effective way to calm your nervous system and relieve stress. Stay involved with others by continuing your work or education-or if that’s not possible, consider volunteering, joining a schizophrenia support group, or taking a class or joining a club to spend time with people who have common interests. As well as keeping you socially connected, it can help you feel good about yourself.
Manage stress – High levels of stress are believed to trigger schizophrenic episodes by increasing the body’s production of the hormone cortisol. As well as staying socially connected, there are plenty of steps you can take to reduce your stress levels, including relaxation techniques such as meditation, yoga, or deep breathing.
Get regular exercise – As well as all the emotional and physical benefits, exercise may help reduce symptoms of schizophrenia, improve your focus and energy, and help you feel calmer. Aim for 30 minutes of activity on most days or if it’s easier three 10-minute sessions. Try rhythmic exercise that engages both your arms and legs, such as walking, running, swimming or dancing.
Get plenty of sleep – When you’re on medication, you most likely need even more sleep than the standard 8 hours. Many people with schizophrenia have trouble with sleep, but getting regular exercise and avoiding caffeine can help.
Relaxation Techniques – Accessing the Relaxation Response
Avoid alcohol, drugs, and nicotine – Substance abuse complicates schizophrenia treatment and worsens symptoms. Even smoking cigarettes can interfere with the effectiveness of some schizophrenia medications. If you have a substance abuse problem, seek help.
Eat regular, nutritious meals – to avoid symptoms exacerbated by changes in blood sugar levels. Omega-3 fatty acids from fatty fish, fish oil, walnuts, and flaxseeds can help improve focus, banish fatigue, and balance your moods.
Family psycho-education and support – In addition to educating family members about the symptoms, course, and treatment of schizophrenia, this form of treatment consists of providing the family with supportive therapy, problem-solving skills, and access to ongoing community supports, including care providers during times of crises. When this intervention is consistently provided for at least several months, it has been found to decrease the relapse rate for the person with schizophrenia and improve social and emotional outcomes. Also, the burden that family members experience as a result of having a loved one with schizophrenia is less, family members tend to be more knowledgeable about the disorder and feel more supported by the professionals involved, and family relationships are improved.
Assertive community treatment (ACT) – This intervention consists of members of the person’s treatment team meeting with that individual on a daily basis, in community settings (for example, home, work, or other places the person with schizophrenia frequents) rather than in an office or hospital setting. The treatment team is made up of a variety of professionals. For example, a psychiatrist, nurse, case manager, employment counselor, and substance-abuse counselor often make up an ACT team. Over the long term, ACT tends to be successful in reducing how often people with schizophrenia are psychiatrically hospitalized or become homeless.
Substance abuse treatment – Providing medical and psychosocial interventions that address substance abuse should be an integral part of treatment as about 50% of individuals with schizophrenia suffer from some kind of substance abuse or dependence.
Social skills training – Also called illness management and recovery programming, social-skills training involves teaching clients ways to handle social situations appropriately. It may be conducted as part of individual or group psychotherapy and often involves the person scripting (thinking through or role-playing) situations that occur in social settings in order to prepare for those situations when they actually occur. This treatment type has been found to help people with schizophrenia resist using drugs of abuse, as well as improve their relationships with health care professionals and with people at work.
Supported employment – This intervention provides supports like a job coach (someone who periodically or consistently counsels the client in the workplace), as well as instruction on constructing a résumé, interviewing for jobs, and education and support for employers to hire individuals with chronic mental illness. Supported employment has been found to help schizophrenia sufferers secure and maintain employment, earn more money, and increase the number of hours they are able to work.
Cognitive behavioral therapy (CBT) – CBT is a reality-based intervention that focuses on helping a client understand and change patterns that tend to interfere with his or her ability to interact with others and otherwise function. Except for people who are actively psychotic, CBT has been found to help individuals with schizophrenia decrease symptoms and improve their ability to function socially. This intervention can be done either individually or in group therapy.
Group therapy – Group therapy is usually supportive and expressive, in that participants are encouraged in their efforts to care for themselves and otherwise engage in healthy, appropriate behaviors in the community.
Weight management – Educating people with schizophrenia about weight gain and related health problems that can be a side effect of some antipsychotic and other psychiatric medications have been found to be helpful in resulting in a modest weight loss. That is also true when schizophrenia sufferers are provided with behavioral interventions to help with weight loss.
Edema also spelled oedema or edema, is an abnormal accumulation of fluid in the interstitium, located beneath the skin and in the cavities of the body, which can cause severe pain. Clinically, edema manifests as swelling. The amount of interstitial fluid is determined by the balance of fluid homeostasis; and the increased secretion of fluid into the interstitium. The word is from meaning “swelling. An edema will occur in specific organs as part of inflammations, tendonitis or pancreatitis, for instance.Certain organs develop edema through tissue-specific mechanisms. Examples of edema in specific organs
Classification according to the organ position
Cerebral edema is extracellular fluid accumulation in the brain. It can occur in toxic or abnormal metabolic states and conditions such as systemic lupus or reduced oxygen at high altitudes. It causes drowsiness or loss of consciousness, leading to brain herniation and death.
Pulmonary edema occurs when the pressure in blood vessels in the lung is raised because of obstruction to the removal of blood via the pulmonary veins. This is usually due to failure of the left ventricle of the heart. It can also occur in altitude sickness or on inhalation of toxic chemicals. Pulmonary edema produces shortness of breath. Pleural effusions may occur when fluid also accumulates in the pleural cavity.
Edema may also be found in the corner of the eye with glaucoma, severe conjunctivitis or keratitis or after surgery. Sufferers may perceive colored haloes around bright lights.
Edema surrounding the eyes is called periorbital edema or eye puffiness. The periorbital tissues are most noticeably swollen immediately after waking, perhaps as a result of the gravitational redistribution of fluid in the horizontal position.
Common appearances of cutaneous edema are observed with mosquito bites, spider bites, bee stings (wheal and flare), and skin contact with certain plants such as Poison Ivy or Western Poison Oak, the latter of which are termed contact dermatitides.
Another cutaneous form of edema is myxedema, which is caused by increased deposition of connective tissue. In myxedema (and a variety of other rarer conditions) edema is caused by an increased tendency of the tissue to hold water within its extracellular space. In myxedema, this is because of an increase in hydrophilic carbohydrate-rich molecules (perhaps mostly hyaluronan) deposited in the tissue matrix. Edema forms more easily independent areas in the elderly (sitting in chairs at home or on airplanes) and this is not well understood. Estrogens alter body weight in part through changes in tissue water content. There may be a variety of poorly understood situations in which transfer of water from tissue matrix to lymphatics is impaired because of changes in the hydrophilicity of the tissue or failure of the ‘wicking’ function of terminal lymphatic capillaries.
In lymphedema abnormal removal of interstitial fluid is caused by the failure of the lymphatic system. This may be due to obstruction from, for example, pressure from cancer or enlarged lymph nodes, destruction of lymph vessels by radiotherapy, or infiltration of the lymphatics by infection (such as elephantiasis). It is most commonly due to a failure of the pumping action of muscles due to immobility, most strikingly in conditions such as multiple sclerosis, or paraplegia. It has been suggested that the edema that occurs in some people following the use of aspirin-like cyclo-oxygenase inhibitors such as ibuprofen or indomethacin may be due to inhibition of lymph heart action.
Hydrops fetalis is a condition of the fetus characterized by an accumulation of fluid, or edema, in at least two fetal compartments.
Lower Extremity Edema
51-year-old male with a history of HTN, DM and chronic alcohol abuse presenting with lower extremity swelling. He notes one month of progressive, bilateral lower extremity swelling, in the past two weeks associated with increasing pain and redness and is now no longer able to ambulate due to pain. He denies fevers/chills, chest pain or shortness of breath. He also denies orthopnea and paroxysmal nocturnal dyspnea. He states that he has not had these symptoms prior to one month ago. On review of systems, he denies nausea/vomiting, abdominal pain, and changes in bowel or urinary habits. He has a history of GI bleeding (unknown treatment) but denies hematemesis, hematochezia or melena. He has previously experienced alcohol withdrawal, which manifested as tremors, but no hallucinations or seizures
Types of Edema
Peripheral edema –This usually affects the legs, feet, and ankles, but it can also happen in the arms. It could be a sign of problems with your circulatory system, lymph nodes, or kidneys.
Pedal edema –This happens when fluid gathers in your feet and lower legs. It’s more common if you’re older or pregnant. It can make it harder to move around in part because you may not have as much feeling in your feet
Lymphedema –This swelling in the arms and legs is most often caused by damage to your lymph nodes, tissues that help filter germs and waste from your body. The damage may be the result of cancer treatments like surgery and radiation. Cancer itself can also block lymph nodes and lead to fluid buildup.
Pulmonary edema – When fluid collects in the air sacs in your lungs, you have pulmonary edema. That makes it hard for you to breathe, and it’s worse when you lie down. You may have a fast heartbeat, feel suffocated, and cough up a foamy spittle, sometimes with blood.
Cerebral edema –This is a very serious condition in which fluid builds up in the brain. It can happen if you hit your head hard if a blood vessel gets blocked or bursts or you have a tumor or an allergic reaction.
Macular edema – This happens when fluid builds up in a part of your eye called the macula, which is in the center of the retina, the light-sensitive tissue at the back of the eye. It happens when damaged blood vessels in the retina leak fluid into the area.
Physical Exam
VS:
T
37.6
HR
86
RR
16
BP
128/84
O2
99% RA
Gen:
Adult, non-obese male, lying in bed. Tremors noted in upper extremities.
HEENT:
PERRL, EOMI, no scleral icterus. Mucous membranes moist.
CV:
RRR, normal S1/S2, no additional heart sounds, JVP 3cm above sternal angle at 30°.
Lungs:
CTAB, no crackles.
Abd:
Soft, non-distended, with normoactive bowel sounds. Liver edge palpated 1cm below costal margin at mid-clavicular line, non-tender. No rebound/guarding.
Ext:
Warm, well-perfused with 2+ distal pulses (PT, DP). 3+ pitting edema symmetric in bilateral lower extremities to knee. Erythema and warmth bilaterally extending from ankles to mid-shin. Mild tenderness to palpation. No pain with passive dorsiflexion. 3x3cm shallow ulceration below medial malleolus on right lower extremity without underlying fluctuance or expression of purulent material. No venous varicosities noted. Decreased sensation to light touch below knee bilaterally.
Rectal:
Normal rectal tone, brown stool, guaiac negative.
Neuro:
Alert and oriented, CN II-XII intact, gait intact, normal FTN/RAM.
Labs/Studies
CBC: 7.4/13.1/39/180
Creatinine: 0.84
Albumin: 4.3
BNP: 28
Imaging
Venous Lower Extremity Ultrasound
No DVT.
Pulsatile flow in bilateral EIV (external iliac veins) suggestive of elevated right heart pressure.
Assessment/Plan
51M with HTN, DM, EtOH abuse presenting with lower extremity edema. Chronic bilateral lower extremity edema likely secondary to chronic venous insufficiency perhaps related to OSA given ultrasound findings of pulsatile flow in EIV’s. Doubt systemic cause: no evidence of heart failure on exam and normal BNP, no stigmata of cirrhosis and normal albumin, normal creatinine. Also, no evidence of DVT on ultrasound though bilateral DVT unlikely. Bilateral cellulitis also unlikely as the patient is afebrile without leukocytosis, however the patient was started on antibiotics including ceftriaxone and TMP/SMX given erythema, warmth and tenderness to palpation. The patient received benzodiazepines which eased withdrawal symptoms and he was admitted for continued treatment.
Mechanisms of Lower Extremity Edema
Differential Diagnosis of Lower Extremity Edema
Evaluation
History
Duration: acute (<72h) vs. chronic
Pain: DVT, CRPS, less severe in venous insufficiency
Systemic Disease
Cardiac: orthopnea, PND
Renal: proteinuria
Hepatic: jaundice, ascites
Malignancy: lymphedema
Improvement with elevation/recumbency: venous insufficiency
OSA: snoring, daytime somnolence
Medications: B-blocker, CCB, hormones, NSAID’s
Physical Exam
Distribution: unilateral, bilateral, generalized
Quality: pitting, non-pitting
TTP: DVT, cellulitis
Varicose veins: venous insufficiency
Kaposi-Stemmer: inability to pinch dorsum of foot at base of 2nd toe (lymphedema)
Electrolytes Abnormalities means the abnormal function of body fluid that plays a vital role in maintaining homeostasis within the body. They help to regulate heart and neurological function, fluid balance, oxygen delivery, acid-base balance and much more. Electrolyte imbalances can develop by the following mechanisms: excessive ingestion; diminished elimination of an electrolyte; diminished ingestion or excessive elimination of an electrolyte. The most serious electrolyte disturbances involve abnormalities in the levels of sodium, potassium or calcium. Other electrolyte imbalances are less common and often occur in conjunction with major electrolyte changes. Chronic laxative abuse or severe diarrhea or vomiting (gastroenteritis) can lead to electrolyte disturbances along with dehydration. People suffering from bulimia or anorexia nervosa are at especially high risk for an electrolyte imbalance.
Electrolyte Abnormalities
Routine laboratory studies are common in the intensive care unit; abnormalities are even more common. Typically these studies include a chemistry panel (Chem 10). The differential diagnoses of the most frequent and clinically relevant electrolyte abnormalities are detailed below.
Differential Diagnosis and Evaluation of Hyponatremia
Differential Diagnosis and Evaluation of Hypernatremia
Differential Diagnosis and Evaluation of Hypokalemia
Differential Diagnosis of Hyperkalemia
Differential Diagnosis of Hypo and Hypercalcemia
Differential Diagnosis of Hypo and Hypermagnesemia
Differential Diagnosis of Hypo and Hyperphosphatemia
Hyponatremia
62M with a history of hepatitis C cirrhosis complicated by hepatocellular carcinoma s/p radiofrequency ablation presenting after referral from hepatology clinic for hyponatremia. One week ago, the patient developed abdominal distension and shortness of breath that resolved after large-volume paracentesis and was started on furosemide 40mg p.o. daily and aldactone 100mg p.o. daily.
After initiating diuretics, the patient noted worsening lower extremity edema, and increased thirst/fluid intake.
He reports two days of fatigue and intermittent confusion supported by family members who reported slowed speech. He otherwise denies abdominal pain, distension, nausea/vomiting, diarrhea/constipation, chest pain or shortness of breath. In the ED, the patient received 1L NS bolus.
PMH:
Hepatitis C cirrhosis c/b HCC s/p RFA
Rheumatoid arthritis, well-controlled without medications
PSH:
None
FH:
Non-contributory.
SHx:
Lives with partner, denies current or prior t/e/d abuse
HepC contracted from blood transfusions
Meds:
Furosemide 40mg p.o. daily
Spironolactone 100mg p.o. daily
Rifaximin 550mg p.o. b.i.d.
Allergies
NKDA
Physical Exam
VS:
T
98.2
HR
80
RR
14
BP
95/70
O2
98% RA
Vent:
PRVC, VT 320, RR 35, PEEP 6, FiO2 95%
Gen:
Elderly female in no acute distress, alert and answering questions appropriately.
HEENT:
NC/AT, PERRL, EOMI, no scleral icterus, MMM.
CV:
RRR, normal S1/S2, no murmurs. JVP 8cm.
Lungs:
Faint basilar crackles on bilateral lung bases.
Abd:
Normoactive bowel sounds, non-distended, non-tender, without rebound/guarding.
Ext:
2+ pitting edema in lower extremities to knees bilaterally. 2+ peripheral pulses, warm and well perfused.
Neuro:
AAOx3. CN II-XII intact. No asterixis. Normal gait. Normal FTN/RAM.
Labs/Studies
BMP (admission): 112/5.6/88/22/28/1.1/97
BMP (+10h): 118/5.4/93/23/26/1.0/133
sOsm: 264
Urine: Na <20, K 26, Osm 453
BNP: 40
AST/ALT/AP/TB/Alb: 74/57/91/2.4/2.2
Assessment/Plan
62M hx HepC cirrhosis, newly decompensated with e/o decompensation (new-onset ascites) and hyponatremia.
# hyponatremia: Sodium 114, likely chronic, patient currently asymptomatic without concerning findings on neurological exam. Clinical findings suggestive of hypervolemic hyponatremia 2/2 decompensated cirrhosis resulting in decreased effective arterial blood volume and volume retention. However, the recent initiation of diuretics, mild AKI and early response to isotonic fluids in the ED suggests possible hypovolemic component.
1L fluid restriction
q.4.h. sodium check, goal increase of 8mEq per 24h
hold diuretics
# hyperkalemia: Potassium 5.6, asymptomatic, AKI vs. medication-induced (aldactone). Continue monitoring.
# AKI: Elevated creatinine 1.1 from baseline 0.7. Likely pre-renal given recent initiation of diuretics. Consider hepatorenal syndrome given decompensated cirrhosis. Follow-up repeat creatinine after 1L NS bolus in ED.
# hepatitis C: decompensated with new-onset ascites. No e/o encephalopathy, continue home rifaximin.
Physiology of Hyponatremia
Differential Diagnosis of Hyponatremia
Evaluation of Hyponatremia
Identification of onset (acute vs. chronic)
Presence of symptoms (HA, nausea, confusion, seizures)
Assessment of volume status (edema, JVD, skin turgor, postural BP)
Medical history (cardiac, liver, renal disease), drug history
Hyperglycemic Crises
Blurred vision, numbness
HPI:
56 year-old male with a history of DM, questionable HTN presenting with blurred vision, numbness of fingertips/toes for 2wks. Associated symptoms include dry mouth, polydipsia/polyuria. He states that these symptoms coincide with elevated measurements of blood glucose at home (>500). He ran out of his diabetes medication (metformin) 8mo ago but states his BG was typically between 100-200 with diet/exercise until 2wks ago. He reports recent dietary indiscretions on a trip to Las Vegas.
He denies fevers/chills, CP/SOB, cough, abdominal pain, N/V, or dysuria.
PMH:
DM II
HTN
PSH:
None
FH:
Several maternal family members with DM.
SHx:
No tobacco/drug use
5-6 alcoholic drinks/wk
Meds:
Metformin 500mg p.o. b.i.d.
Allergies:
NKDA
Physical Exam
VS:
T 37.8 HR 60 RR 14 BP 165/90 O2 99% RA
Gen:
Well-appearing, no acute distress, obese
HEENT:
PERRL, EOMI, optic discs sharp b/l, no abnormalities visualized
CV:
RRR, normal S1/S2, no M/R/G, no additional heart sounds
Lungs:
CTAB, no wheezes/crackles
Abd:
+BS, soft, NT/ND, no rebound/guarding
Ext:
Warm, well-perfused, 2+ pulses, no clubbing/cyanosis/edema
Neuro:
AAOx3, CN II-XII intact
Labs/Studies
BMP: 135/3.8/102/24/18/1.1/378
CBC: 7.4/14.1/42.0/403
UA: + glucose, – ketones
Assessment/Plan
56M, hx DM with poor medication adherence presenting with vision changes and stocking/glove paresthesias for 2wks after reported dietary indiscretion found to be hyperglycemic. DKA/HHS unlikely given stable vital signs, normal metabolic panel with exception of isolated hyperglycemia (slight hyponatremia likely related to osmotic effect of elevated serum glucose). Also, no evidence of concerning precipitates for hyperglycemic crisis (no CP/SOB, no F/C, no cough, no abdominal pain, no change in mental status). Patient was discharged home with education on importance of medication adherence, refill of metformin, and follow-up with primary care physician for further management of DM and possible hypertension.
Evaluation of hyperglycemic crises in patients with diabetes
DKA: Short course (<24h), N/V, diffuse abdominal pain, Kussmaul respirations
HHS: Longer course (days/weeks), altered mental status (lethargy, coma, seizure)
Admission Laboratory Data of Patients with HHS vs. DKA
DKA
HHS
Glucose (mg/dl)
616
930
pH
7.12
7.30
3-β-hydroxybutyrate (mmol/l)
9.1
1.0
Serum osmolality
323
380
Delta gap (AG-12)
17
11
Na (mEq/l)
134
149
K (mEq/l)
4.5
3.9
Bicarbonate (mEq/l)
9
18
Delirium, ID
A 70 year-old female with a PMH of HTN, DM, hyperlipidemia and stage I breast cancer s/p lumpectomy with sentinel LN biopsy several years ago presented for elective surgery complicated by post-operative bleeding. She is now 4 days post-op and was found to be confused, somnolent and occasionally agitated.
HPI:
The patient could not be interviewed.
PE:
VS: Stable and within normal limits
General: unremarkable except for crackles in bilateral lung bases
MSE: only arouses to sternal rub and becomes agitated, moving all four extremities spontaneously and symmetrically.
Reflexes: corneal and gag reflexes present, suppresses eye movements with head turn, deep tendon reflexes 3+ throughout UE/LE bilaterally.
Assessment
70 year-old woman with a history of HTN, DM, hyperlipidemia and breast cancer presents with worsening confusion, somnolence and occasional agitation four days after surgery. The combination of significantly altered consciousness and absence of focal neurological findings, all in the setting of a complicated surgical course suggest delirium.
Differential Diagnosis of Altered Mental Status
Levels of consciousness
There are different levels of consciousness, they are named in the diagram below but are better described by the characteristics observed.
Hematology/haematology is the branch of medicine concerned with the study of the cause, prognosis, treatment, and prevention of diseases related to blood. It involves treating diseases that affect the production of blood and its components, such as blood cells, hemoglobin, blood proteins, bone marrow, platelets, blood vessels, spleen, and the mechanism of coagulation. Such diseases might include hemophilia, blood clots, other bleeding disorders and blood cancers such as leukemia, multiple myeloma, and lymphoma. The laboratory work that goes into the study of blood is frequently performed by a medical technologist or medical laboratory scientist. Many hematologists work as hematologist-oncologists, also providing medical treatment for all types of cancer. The term is from the Greek αἷμα, haima meaning “blood,” and -λoγία meaning study.
Types of Hematology
Myeloid
Hemoglobinopathies (congenital abnormality of the hemoglobin molecule or of the rate of hemoglobin synthesis)
Sickle-cell disease
Thalassemia
Methemoglobinemia
Anemias (lack of red blood cells or hemoglobin)
Iron deficiency anemia
Megaloblastic anemia
Vitamin B12 deficiency
Pernicious anemia
Folate deficiency
Hemolytic anemias (destruction of red blood cells)
Immune mediated hemolytic anemia (direct Coombs test is positive)
Autoimmune hemolytic anemia
Warm antibody autoimmune hemolytic anemia
Idiopathic
Systemic lupus erythematosus (SLE)
Evans’ syndrome (antiplatelet antibodies and hemolytic antibodies)
Cold autoimmune hemolytic anemia
Cold agglutinin disease
Paroxysmal cold hemoglobinuria (rare)
Infectious mononucleosis
Alloimmune hemolytic anemia
Hemolytic disease of the newborn (HDN)
Rh disease (Rh D)
ABO hemolytic disease of the newborn
Anti-Kell hemolytic disease of the newborn
Rhesus c hemolytic disease of the newborn
Rhesus E hemolytic disease of the newborn
Other blood group incompatibility (RhC, Rhe, Kid, Duffy, MN, P and others)
Drug induced immune mediated hemolytic anemia
Penicillin (high dose)
Methyldopa
Hemoglobinopathies (where these is an unstable or crystalline hemoglobin)
Paroxysmal nocturnal hemoglobinuria (rare acquired clonal disorder of red blood cell surface proteins)
Direct physical damage to RBCs
Microangiopathic hemolytic anemia
Secondary to artificial heart valve(s)
Aplastic anemia
Fanconi anemia
Diamond-Blackfan anemia (inherited pure red cell aplasia)
Acquired pure red cell aplasia
Decreased numbers of cells
Myelodysplastic syndrome
Myelofibrosis
Neutropenia (decrease in the number of neutrophils)
Agranulocytosis
Glanzmann’s thrombasthenia
Thrombocytopenia (decrease in the number of platelets)
Idiopathic thrombocytopenic purpura (ITP)
Thrombotic thrombocytopenic purpura (TTP)
Heparin-induced thrombocytopenia (HIT)
Myeloproliferative disorders (Increased numbers of cells)
Polycythemia vera (increase in the number of cells in general)
Erythrocytosis (increase in the number of red blood cells)
Leukocytosis (increase in the number of white blood cells)
Thrombocytosis (increase in the number of platelets)
Myeloproliferative disorder
Coagulopathies (disorders of bleeding and coagulation)
Thrombocytosis
Recurrent thrombosis
Disseminated intravascular coagulation
Disorders of clotting proteins
Hemophilia
Hemophilia A
Hemophilia B (also known as Christmas disease)
Hemophilia C
Von Willebrand disease
Disseminated intravascular coagulation
Protein S deficiency
Antiphospholipid syndrome
Disorders of platelets
Thrombocytopenia
Glanzmann’s thrombasthenia
Wiskott-Aldrich syndrome
Hematological malignancies
Hematological malignancies
Lymphomas
Hodgkin’s disease
Non-Hodgkin’s lymphoma {includes the next five entries}
Burkitt’s lymphoma
Anaplastic large cell lymphoma
Splenic marginal zone lymphoma
Hepatosplenic T-cell lymphoma
Angioimmunoblastic T-cell lymphoma (AILT)
Myelomas
Multiple myeloma
Waldenström macroglobulinemia
Plasmacytoma
Leukemias increased WBC
Acute lymphocytic leukemia (ALL)
Chronic lymphocytic leukemia (CLL){now included in theCLL/SCLL type NHL}
Acute myelogenous leukemia (AML)
Chronic Idiopathic Myelofibrosis (MF)
Chronic myelogenous leukemia (CML)
T-cell prolymphocytic leukemia (T-PLL)
B-cell prolymphocytic leukemia (B-PLL)
Chronic neutrophilic leukemia (CNL)
Hairy cell leukemia (HCL)
T-cell large granular lymphocyte leukemia (T-LGL)
Aggressive NK-cell leukemia
Miscellaneous
Hemochromatosis
Asplenia
Hypersplenism
Gaucher’s disease
Monoclonal gammopathy of undetermined significance
Hemophagocytic lymphohistiocytosis
Tempi syndrome
Hematological changes secondary to non-hematological disorders
Anemia of chronic disease
Infectious mononucleosis
AIDS
Malaria
Leishmaniasis
Blood
Venous blood
Venipuncture
Hematopoiesis
Blood tests
Cord blood
Red blood cells
Erythropoiesis
Erythropoietin
Iron metabolism
Hemoglobin
Glycolysis
Pentose phosphate pathway
White blood cells
Platelets
Reticuloendothelial system
Bone marrow
Spleen
Liver
Lymphatic system
Blood transfusion
Blood plasma
Blood bank
Blood donors
Blood groups
Hemostasis
Coagulation
Vitamin K
Complement system
Immunoglobulins
(abnormality of the hemoglobin molecule or of the rate of hemoglobin synthesis)
Anemias (lack of red blood cells or hemoglobin)
Hematological malignancies
Coagulopathies (disorders of bleeding and coagulation)
Sickle Cell Anemia
Thalassemia
Evaluation
A 27 year-old male with sickle cell disease (HbSC) on hydroxurea and with a history of 2-3 hospitalizations per year for vaso-occlusive pain crises manifested by arthralgias and back pain presents to the emergency department with 3 days of worsening joint pain affecting his entire body but predominantly his knees and lower back. He is familiar with this pain and attempted therapy at home with ibuprofen, then hydrocodone-acetaminophen, and finally hydromorphone without improvement and presented to the emergency department.
On review of systems, he denied chest pain, cough, or shortness of breath. He has some periumbilical abdominal pain but tolerated normal oral intake on the day of presentation without vomiting nor changes in bowel habits. He otherwise denied fevers, peripheral numbness/weakness, urinary or fecal incontinence or retention. He similarly denies trauma, weight loss, night sweats, or intravenous drug use.
Objectively, the patient’s vital signs were normal and he was well-appearing. Mucous membranes were moist and skin turgor was normal. There were no appreciable joint effusions, warmth, nor limitation to active/passive range of motion of any joints. His back had no midline tenderness to palpation or percussion, normal range of motion in all axes and extremity sensation and strength testing were normal. Abdominal and genitourinary examinations were normal. The patient had preserved perineal sensation to light touch and normal rectal tone – a core temperature was obtained which was also normal.
Peripheral access was established and a parenteral dose of hydromorphone equivalent to his home oral dose was administered (0.015mg/kg). Repeat dosing was required at 15 minutes due to persistent pain scale of 10. Diphenhydramine and acetaminophen were also administered, for potential opioid-sparing effects, recognizing the limited evidence to support these relatively benign adjuncts.
Laboratory studies were notable for anemia (though stable compared to baseline measures), appropriate reticulocyte count, no evidence of hemolysis and with normal electrolytes and renal function.
A thorough history and examination did not identify a critical precipitant for the patient’s symptoms which were presumed to be secondary to a vaso-occlusive pain crisis. On reassessment, the patient’s pain was improved and an oral dose of hydromorphone was administered with continued observation and serial reassessments for two hours thereafter. The patient’s hematologist was available for follow-up the subsequent morning and the patient was discharged home.
Pharmacokinetics of Commonly-Used Opiate Analgesics
MEDICATION
ROUTE
ONSET
PEAK
DURATION
Morphine
IV
5-10min
20min
3-5h
IM
15-30min
30-60min
PO
30min
1h
Oxycodone
PO
10-15min
30-60min
3-6h
Hydrocodone
PO
10-20min
4-8h
Fentanyl
IV
<1min
2-5min
30-60min
Hydromorphone
IV
5min
10-20min
3-4h
PO
15-30min
30-60min
Codeine
PO
30-60min
60-90min
4-6h
Algorithm for the Evaluation and Management of Sickle Cell Crises
Chronic: anorexia, nausea/vomiting, constipation, fatigue, memory loss
Acute: CNS (lethargy, somnolence)
Findings
Calcium: >13.0mg/dL
ECG: QT shortening
Treatment
Mild: IVF
Severe: IVF, loop diuretics, bisophosphanate (pamidronate 90mg IV infused over 4 hours), consider calcitriol, consider hemodialysis if cannot tolerate fluids or unlikely to respond to diuretics
70M with a history of dementia presenting with 3 days of fatigue. The patient was unable to provide detailed history, however family members reported worsening fatigue with the patient requiring assistance with ambulation for several days. The patient was referred from an outside clinic after point-of-care hemoglobin of 6.7. No reported history of anemia, and no history suggestive of obvious external bleeding.
Vital signs stable, tachycardia and tachypnea noted with minimal exertion but saturating well on ambient air and in no acute distress. Examination notable for conjunctival pallor without scleral icterus, systolic flow murmur, brown stool guaiac negative.
CBC with hemoglobin of 7.5 , MCV 80.3 , RDW 22.4 , no leukocytosis and normal platelets. Also noted was an alkaline phosphatase of 828 , normal total and direct bilirubin, and undetectable serum troponin. Chest x-ray showed a possible pleural-based mass.
The patient was transfused two units of PRBC’s and admitted for further evaluation. CT chest/abdomen/pelvis revealed sternal and rib-based pleural soft-tissue mass, prostate mass, pelvic and retroperitoneal lymphadenopathy as well as extensive bony metastatic disease consistent with primary prostate cancer with diffused metastasis. Serum PSA was 2,087 . Iron studies suggested anemia of chronic disease. Reticulocytes were not obtained but may have suggested inadequate production index given extensive bony metastases and possible associated myelosuppression. The patient was symptomatically improved after transfusion and discharged with outpatient follow-up for discussions regarding possible biopsy and treatment.
Images
Areas of pleural thickening. Possible pleural based mass in left mid lung.
ct_chest_anemia_01
CT Chest: Lung Window
Rib-based pleural soft tissue masses.
Large 5.6 x 4.4cm anterior sternal soft-tissue mass.
ct_bone_anemia_01
CT Body: Bone Window
Extensive bony metastatic disease.
Prostate mass, large pelvic and retroperitoneal lymphadenopathy.
Consistent with primary prostate cancer with diffuse metastasis.
Algorithm for the Evaluation of Anemia
Lymphadenopathy Applied: Lymphoma
27 year-old female with no medical history presenting with neck swelling. She describes one month of progressive enlargement of a left-sided neck mass, and in the past two weeks has noted a new right-sided neck mass. This has been associated with worsening dysphagia to solids, describing a sensation of food lodging in the mid-chest and requiring liquids for passage – she attributes her recent 10lb weight loss to this. She also reports a non-productive cough for the past two weeks and generalized fatigue. She otherwise denies fevers, night sweats, chest pain, shortness of breath, nausea/vomiting, or changes in bowel/urinary habits. She has no known sick contacts or TB exposure risk factors. She has no medical history, no prior surgeries, does not take any medications and denies tobacco, alcohol or drug use.
Physical Exam
VS:
T
38.4
HR
98
RR
14
BP
108/68
O2
99% RA
Gen:
Well-appearing young female, in no acute distress.
HEENT:
PERRL, EOMI, MMM without lesions. There is a 2x3cm firm, non-tender, mobile left supraclavicular lymph node, as well as two 1x1cm firm, non-tender lymph nodes in the left and right anterior cervical chains.
CV:
RRR, normal S1/S2, no murmurs. No JVD.
Lungs:
Clear to auscultation bilaterally. There is a transition to bronchial breath sounds along the trachea inferior to the sternal angle with normal tracheal sounds superiorly.
Abd:
Soft, non-tender without organomegaly.
Ext:
Warm and well-perfused with normal peripheral pulses. No axillary or inguinal lymphadenopathy.
Neuro:
Alert and oriented, responding appropriately to questions. PERRL, EOMI, facial sensation symmetric, facial muscles symmetric, hearing grossly normal, palate rises symmetrically, tongue movements normal without fasciculation, SCM/trapezius normal. Normal FTN, RAM. Gait intact. Peripheral sensation and motor grossly normal.
Imaging
CT Chest – Axial
Anterior mediastinal mass with a wide differential – likely represents lymphoma or germ cell tumor. Less likely thymic or thyroid origin.
CT Chest – Sagittal
Anterior mediastinal mass with a wide differential – likely represents lymphoma or germ cell tumor. Less likely thymic or thyroid origin.
Assessment/Plan
27F with no PMH presenting with progressive localized lymphadenopathy. Resultant dysphagia, cervical and supraclavicular distribution as well as abnormal tracheal sounds concerning for mediastinal involvement. The patient is currently stable without evidence of airway compromise. ACT of the chest was obtained to evaluate for thoracic malignancy, which showed a large anterior mediastinal mass concerning lymphoma or germ cell tumor. The location of the mass likely explains the patient’s dysphagia due to compression of the esophagus, as well as the abnormal pulmonary exam with compression potentially irritating the trachea and triggering her non-productive cough. The patienthe t was admitted for further workup.
Lymphadenopathy Applied – Lymphoma
This case applies the differential diagnosis of lymphadenopathy. The most abnormal finding on examination was non-tender, left supraclavicular lymphadenopathy. The duration of symptoms and lack of tenderness is concerning for malignancy, and the left supraclavicular location suggests a thoracic or intra-abdominal source.
Hypocalcemia / Diabetic Ketoacidosis . Hypercalcemia also spelled Hypercalcaemia is a high calcium (Ca2+) level in the blood serum. Those with a mild increase that has developed slowly typically have no symptoms. In those with greater levels or rapid onset, symptoms may include abdominal pain, bone pain, confusion, depression, weakness, kidney stones, or an abnormal heart rhythm including cardiac arrest.
Diabetic ketoacidosis (DKA) is a potentially life-threatening complication of diabetes mellitus. Signs and symptoms may include vomiting, abdominal pain, deep gasping breathing, increased urination, weakness, confusion, and occasionally loss of consciousness. A person’s breath may develop a specific smell. Onset of symptoms is usually rapid. In some cases people may not realize they previously had diabetes.
DKA happens most often in those with type 1 diabetes, but can also occur in those with other types of diabetes under certain circumstances. Triggers may include infection, not taking insulin correctly, stroke, and certain medications such as steroids.[1] DKA results from a shortage of insulin; in response the body switches to burning fatty acids which produces acidic ketone bodies. DKA is typically diagnosed when testing finds high blood sugar, low blood pH, and ketoacids in either the blood or urine.
Most cases are due to primary hyperparathyroidism or cancer. Other causes include sarcoidosis, tuberculosis, Paget disease, multiple endocrine neoplasia (MEN), vitamin D toxicity, familial hypocalciuric hypercalcaemia, and certain medications such as lithium and hydrochlorothiazide. Diagnosis should generally include either a corrected calcium or ionized calcium level and be confirmed after a week. Specific changes, such as a shortened QT interval, may be seen on an electrocardiogram
Hypocalcemia also spelled hypocalcaemia is low calcium levels in the blood serum. The normal range is 2.1–2.6 mmol/l (8.8–10.7 mg/dl, 4.3–5.2 mEq/l) with levels less than 2.1 mmol/l defined as hypocalcemia. Mildly low levels that develop slowly often have no symptoms. Otherwise symptoms may include numbness, muscle spasms, seizures, confusion, or cardiac arrest.
Common causes include hypoparathyroidism and vitamin D deficiency. Others causes include kidney failure, pancreatitis, calcium channel blocker overdose, rhabdomyolysis, tumor lysis syndrome, and medications such as bisphosphonates. Diagnosis should generally be confirmed with a corrected calcium or ionized calcium level. Specific changes may be seen on an electrocardiogram (ECG)
Calcium Homeostasis
Fraction
15% bound to anions (phosphate, lactate, citrate)
40% bound to albumin
45% free (regulated by PTH, Vit-D)
Conditions causing changes in total calcium (without affecting ionized calcium)
Low albumin causes hypocalcemia. Corrected = measured + [0.8 x (4-albumin)]
Elevated albumin causes hypercalcemia
Multiple myeloma causes hypercalcemia
Conditions causing changes in ionized calcium (without affecting total calcium)
Alkalemia causes increased ionized calcium binding to albumin and decreases ionized calcium levels
Hyperphosphatemia causes increased ionized calcium binding to phosphate and decreases ionized calcium levels
Hyperparathyroidism causes decreased ionized calcium binding to albumin and increases ionized calcium levels
Causes of Hypocalcemia
Eating disorders
Prolonged vomiting (e.g. with a viral illness)
Exposure to mercury, including infantile acrodynia
Excessive dietary magnesium, as with supplementation.
Excessive dietary zinc, as with supplementation (causes rapid hypocalcemia).
Prolonged use of medications/laxatives containing magnesium
Chelation therapy for metal exposure, particularly EDTA
Osteoporosis treatment or preventive agents, such as bisphosphonates and denosumab.
Agents for the treatment of hypercalcemia, such as Calcitonin.
Chronic kidney failure
Absent active vitamin D
Decreased dietary intake
Decreased sun exposure
Defective Vitamin D metabolism
Anticonvulsant therapy
Vitamin-D dependent rickets, type I
Ineffective active vitamin D
Intestinal malabsorption
Vitamin-D dependent rickets, type II
Pseudohypoparathyroidism
Severe acute hyperphosphataemia
Tumour lysis syndrome
Acute kidney failure
Rhabdomyolysis (initial stage)
Exposure to hydrofluoric acid which can be fatal if 2.5% of skin is exposed
Petechiae which appear as on-off spots, then later become confluent, and appear as purpura(larger bruised areas, usually in dependent regions of the body).
Oral, perioral and acral paresthesias, tingling or ‘pins and needles’ sensation in and around the mouth and lips, and in the extremities of the hands and feet. This is often the earliest symptom of hypocalcaemia.
Carpopedal and generalized tetany (unrelieved and strong contractions of the hands, and in the large muscles of the rest of the body) are seen.
Latent tetany
Trousseau sign of latent tetany (eliciting carpal spasm by inflating the blood pressure cuff and maintaining the cuff pressure above systolic)
Chvostek’s sign (tapping of the inferior portion of the cheekbone will produce facial spasms)
Tendon reflexes are hyperactive
Life-threatening complications
Laryngospasm
Cardiac arrhythmias
Effects on cardiac output
Negative chronotropic effect, or a decrease in heart rate.
Negative inotropic effect, or a decrease in contractility
ECG changes include the following
Intermittent QT prolongation, or intermittent prolongation of the QTc (corrected QT interval) on the EKG (electrocardiogram) is noted. The implications of intermittent QTc prolongation predisposes to life-threatening cardiac electrical instability (and this is therefore a more critical condition than constant QTc prolongation). This type of electrical instability puts the patient at high risk of torsades de pointes, a specific type of ventricular tachycardia which appears on an EKG (or ECG) as something which looks a bit like a sine wave with a regularly increasing and decreasing amplitude. (Torsades de pointes can cause death, unless the patient can be medically or electrically cardioverted and returned to a normal cardiac rhythm.)
Management
Severe (symptomatic, QT prolongation)
Calcium gluconate 1-2g IV in 50mL of D5W over 10-20min followed by slow infusion of additional 2g over 2 hours.
Asymptomatic
Calcium gluconate 1g PO q6hCalcitriol 0.2mcg PO BID
Diabetic Ketoacidosis
Algorithm for the Management of Diabetic Ketoacidosis
Endocrine Emergencies
HPI
30 year-old female with a history of autoimmune polyglandular syndrome (adrenal, thyroid and endocrine pancreatic insufficiency), polysubstance use, brought to the emergency department by ambulance with reported chief complaint of fever. On presentation, the patient reported fever for one day, associated with cough. She was lethargic and confused, answering yes/no questions but unable to provide detailed history. She states that she has been taking her home medications as prescribed, which include hydrocortisone, fludrocortisone, synthroid and insulin. No collateral information was immediately available.
Additional history was obtained from chart review upon discharge. The patient was hospitalized two weeks prior with pneumonia and discharged after two days. For 2-3 days prior to presentation, she reported the following symptoms to family members: nausea/vomiting, cough, decreased oral intake, fevers, and palpitations – she did not take her home medications during this time.
Physical Exam
VS:
T
38.6
HR
112
RR
18
BP
149/82
O2
90% RA
Gen:
Alert, fatigued, slow responses.
HEENT:
No meningeal irritation, dry mucous membranes.
Pulmonary:
Tachypnea, inspiratory wheezing and faint crackles at left and right inferior lung fields, appreciated anteriorly as well.
Neuro:
Alert, oriented to self, situation, not month/year. PERRL, EOMI, facial muscles symmetric, tongue protrudes midline without fasciculation. Peripheral sensation grossly intact to light touch and moves all extremities on command.
Labs
VBG: alkalemia, primary respiratory
CBC: no leukocytosis, normal differential, normocytic anemia
The patient’s evaluation in the emergency department was concerning for severe sepsis secondary to suspected pulmonary source (given association of fever with cough, hypoxia and abnormal chest imaging findings). The patient had persistent alteration in mental status concerning for CNS infection. While preparing for lumbar puncture, cardiac monitoring revealed sustained polymorphic ventricular tachycardia without appreciable pulse. CPR was initiated, amiodarone 150mg IV push administered and at first pulse check a perfusing sinus rhythm was noted with immediate recovery of prior baseline mental status. Amiodarone load was continued and additional potassium sulfate (PO and IV) was administered. Review of telemetry monitoring revealed preceding 30-45 minutes of non-sustained ventricular tachycardia. The patient had two more episodes of sustained ventricular tachycardia requiring defibrillation. The patient was admitted to the medical intensive care unit for continued management.
#Sustained Ventricular Tachycardia
Initially attributed to critical hypokalemia and hypomagnesemia. However, after appropriate repletion serial ECG’s continued to demonstrate prolonged QT interval (possibly acquired secondary to medications, later review revealed multiple promotility agents for treatment of gastroparesis which could contribute to QT-prolongation including erythromycin and metoclopramide, also associated with endocrinopathies). Early echocardiography demonstrated global hypokinesis with estimated EF 30-35%. This was initially attributed to severe sepsis, as well as recurrent defibrillation. However, cardiac CT after resolution of acute illness showed persistent depressed ejection fraction, no evidence of coronary atherosclerosis. The presence of non-ischemic cardiomyopathy (may be attributable to chronic endocrine dysfunction or prior history of methamphetamine abuse) associated with malignant dysrhythmias warranted ICD placement for secondary prevention which the patient was scheduled to receive.
#Severe Sepsis
Attributed to pulmonary source given CT findings, healthcare associated and covered broadly. Mental status gradually improved and returned to baseline. CT head was negative, lumbar puncture deferred.
#Hypokalemia
Unclear etiology. Adrenal insufficiency commonly associated with hyperkalemia and no history of surreptitious fludrocortisone use. Possibly secondary to GI losses. Improved with repletion.
#Autoimmune Polyglandular Syndrome
Started on stress-dose steroids in emergency department. Transiently developed DKA which was reversed appropriately and hydrocortisone was tapered to home regimen. Home levothyroxine was resumed.
Hypotension: refractory to volume resuscitation and pressors
Bradypnea: with hypercapnia and hypoxia
Hyponatremia
Management
Airway protection
Fluid resuscitation
Thyroid hormone replacement
Young, otherwise healthy patients: T3 10ug IV q4h
Elderly, cardiac compromise: 300ug IV x1
Hydrocortisone: 50-100mg IV q6-8h
Treat precipitating illness
Interpretation of Thyroid Function Tests
CONDITION
TSH
T4
None
Normal
Normal
Hyperthyroidism
Low
High
Hypothyroidism
High
Low
Subclinical hyperthyroidism
Low
Normal
Subclinical hypothyroidism
High
Normal
Sick euthyroid
Low
Low
Endocrine Emergencies: Adrenal Insufficiency
Either primary due to adrenal gland failure (often secondary to autoimmune destruction), or secondary most often due to exogenous glucocorticoid administration (usually requiring more than 30mg/day for > 3wks).
Ventricular arrhythmias (exacerbated with digoxin use)
Treatment
Maximum rate 10-20mEq/h with ECG monitoring
If malignant ventricular arrhythmias or arrest imminent, consider more rapid administration (10mEq over 5 minutes)
Critical Hypomagnesemia
Causes
GI, renal losses
Thyroid dysfunction
Treatment
1-2g IV over 5-60 minutes or IVP for Torsades
Conclusion
Unfortunately, this patient’s comprehensive clinical picture does not fit neatly into a particular category of endocrinologic pathology. Her underlying autoimmune disorder manifests both primary adrenal and thyroid dysfunction. Components of the patient’s presentation are suggestive of critical hypothyroidism (myxedema coma) including alteration in mental status, QT-prolongation and hyponatremia as well as possible precipitant of pneumonia. However, despite elevated TSH, the patient’s free T4 level was within normal range. Also absent was hypoventilation (the patient was appropriately tachypneic for degree of hypoxia and with resultant respiratory alkalosis) or bradycardia/hypothermia.
Similarly, adrenal insufficiency is typically associated with hyperkalemia, whereas our patient had critical hypokalemia that was determined to be at least a contributory factor to her ventricular dysrhythmia. The etiology of the patient’s hypokalemia remained unexplained.
Hyperglycemic Crises
Blurred vision, numbness
HPI
56 year-old male with a history of DM, questionable HTN presenting with blurred vision, numbness of fingertips/toes for 2wks. Associated symptoms include dry mouth, polydipsia/polyuria. He states that these symptoms coincide with elevated measurements of blood glucose at home (>500). He ran out of his diabetes medication (metformin) 8mo ago but states his BG was typically between 100-200 with diet/exercise until 2wks ago. He reports recent dietary indiscretions on a trip to Las Vegas.
He denies fevers/chills, CP/SOB, cough, abdominal pain, N/V, or dysuria.
PMH:
DM II
HTN
PSH:
None
FH:
Several maternal family members with DM.
SHx:
No tobacco/drug use
5-6 alcoholic drinks/wk
Meds:
Metformin 500mg p.o. b.i.d.
Allergies:
NKDA
Physical Exam
VS:
T 37.8 HR 60 RR 14 BP 165/90 O2 99% RA
Gen:
Well-appearing, no acute distress, obese
HEENT:
PERRL, EOMI, optic discs sharp b/l, no abnormalities visualized
CV:
RRR, normal S1/S2, no M/R/G, no additional heart sounds
Lungs:
CTAB, no wheezes/crackles
Abd:
+BS, soft, NT/ND, no rebound/guarding
Ext:
Warm, well-perfused, 2+ pulses, no clubbing/cyanosis/edema
Neuro:
AAOx3, CN II-XII intact
Labs/Studies
BMP: 135/3.8/102/24/18/1.1/378
CBC: 7.4/14.1/42.0/403
UA: + glucose, – ketones
Assessment/Plan
56M, hx DM with poor medication adherence presenting with vision changes and stocking/glove paresthesias for 2wks after reported dietary indiscretion found to be hyperglycemic. DKA/HHS unlikely given stable vital signs, normal metabolic panel with exception of isolated hyperglycemia (slight hyponatremia likely related to osmotic effect of elevated serum glucose). Also, no evidence of concerning precipitates for hyperglycemic crisis (no CP/SOB, no F/C, no cough, no abdominal pain, no change in mental status). Patient was discharged home with education on importance of medication adherence, refill of metformin, and follow-up with primary care physician for further management of DM and possible hypertension.
Evaluation of hyperglycemic crises in patients with diabetes
DKA: Short course (<24h), N/V, diffuse abdominal pain, Kussmaul respirations
HHS: Longer course (days/weeks), altered mental status (lethargy, coma, seizure)
Admission Laboratory Data of Patients with HHS vs. DKA
DKA
HHS
Glucose (mg/dl)
616
930
pH
7.12
7.30
3-β-hydroxybutyrate (mmol/l)
9.1
1.0
Serum osmolality
323
380
Delta gap (AG-12)
17
11
Na (mEq/l)
134
149
K (mEq/l)
4.5
3.9
Bicarbonate (mEq/l)
9
18
Delirium
A 70 year-old female with a PMH of HTN, DM, hyperlipidemia and stage I breast cancer s/p lumpectomy with sentinel LN biopsy several years ago presented for elective surgery complicated by post-operative bleeding. She is now 4 days post-op and was found to be confused, somnolent and occasionally agitated.
HPI
The patient could not be interviewed.
PE
VS: Stable and within normal limits
General: unremarkable except for crackles in bilateral lung bases
MSE: only arouses to sternal rub and becomes agitated, moving all four extremities spontaneously and symmetrically.
Reflexes: corneal and gag reflexes present, suppresses eye movements with head turn, deep tendon reflexes 3+ throughout UE/LE bilaterally.
Assessment
70 year-old woman with a history of HTN, DM, hyperlipidemia and breast cancer presents with worsening confusion, somnolence and occasional agitation four days after surgery. The combination of significantly altered consciousness and absence of focal neurological findings, all in the setting of a complicated surgical course suggest delirium.
Differential Diagnosis of Altered Mental Status
Levels of consciousness
There are different levels of consciousness, they are named in the diagram below but are better described by the characteristics observed.
Epileptic seizure also known as an epileptic fit is a brief episode of signs or symptoms due to abnormal excessive or synchronous neuronal activity in the brain. The outward effect can vary from uncontrolled jerking movement (tonic-clonic seizure) to as subtle as a momentary loss of awareness (absence seizure). Diseases of the brain characterized by an enduring predisposition to generate epileptic seizures are collectively called epilepsy
Differences between seizure & Epilepsy
Seizure
Pathologic neuronal activation leading to abnormal function
Epilepsy
Recurrent unprovoked seizures
Types
Cause
Primary: Unprovoked
Secondary: Provoked, caused by trauma, illness, intoxication, metabolic disturbances, etc.
Effect on mentation
Generalized: involvement of both hemispheres with associated loss of consciousness (tonic-clonic, absence, atonic, myoclonic)
Focal: Involving single hemisphere with the preserved level of consciousness.
Status epilepticus
Witnessed convulsions lasting >5min
Recurrent seizure without recovery from a postictal period
Furthers classification of seizures
Tonic-clonic (or grand mal) seizures – These are the most noticeable. When you have this type, your body stiffens, jerks, and shakes, and you lose consciousness. Sometimes you lose control of your bladder or bowels. They usually last 1 to 3 minutes. That can lead to breathing problems or make you bite your tongue or cheek
Clonic seizures – Your muscles have spasms, which often make your face, neck, and arm muscles jerk rhythmically. They may last several minutes.
Tonic seizures – The muscles in your arms, legs, or trunk tense up. These usually last less than 20 seconds and often happen when you’re asleep. But if you’re standing up at the time, you can lose your balance and fall. These are more common in people who have a type of epilepsy known as Lennox-Gastaut syndrome, though people with other types can have them, too.
Atonic seizures – Your muscles suddenly go limp, and your head may lean forward. If you’re holding something, you might drop it, and if you’re standing, you might fall. These usually last less than 15 seconds, but some people have several in a row. Because of the risk of falling, people who tend to have atonic seizures may need to wear something like a helmet to protect their heads.
Myoclonic seizures – Your muscles suddenly jerk as if you’ve been shocked. They may start in the same part of the brain as an atonic seizure, and some people have both myoclonic and atonic seizures.
Absence (or petit mal) seizures – You seem disconnected from others around you and don’t respond to them. You may stare blankly into space, and your eyes might roll back in your head. They usually last only a few seconds, and you may not remember having one. They’re most common in children under 14.
Focal Seizures can ber break these into three groups
Simple focal seizures – They change how your senses read the world around you: They can make you smell or taste something strange, and may make your fingers, arms, or legs twitch. You also might see flashes of light or feel dizzy. You’re not likely to lose consciousness, but you might feel sweaty or nauseated.
Complex focal seizures – These usually happen in the part of your brain that controls emotion and memory. You may lose consciousness but still look like you’re awake, or you may do things like gag, smack your lips, laugh, or cry. It may take several minutes for someone who’s having a complex focal seizure to come out of it.
Secondary generalized seizures – These start in one part of your brain and spread to the nerve cells on both sides. They can cause some of the same physical symptoms as a generalized seizure, like convulsions or muscle slackness.
Causes
Different causes of seizures are common in certain age groups.
Seizures in babies are most commonly caused by hypoxic ischemic encephalopathy, central nervous system (CNS) infections, trauma, congenital CNS abnormalities, and metabolic disorders.
The most frequent cause of seizures in children is febrile seizures, which happen in 2–5% of children between the ages of six months and five years.
During childhood, well-defined epilepsy syndromes are generally seen.
In adolescence and young adulthood, non-compliance with the medication regimen and sleep deprivation are potential triggers.
Pregnancy and labor and childbirth, and the post-partum, or post-natal period (after birth) can be at-risk times, especially if there are certain complications like pre-eclampsia.
During adulthood, the likely causes are alcohol-related, strokes, trauma, CNS infections, and brain tumors.
In older adults, cerebrovascular disease is a very common cause. Other causes are CNS tumors, head trauma, and other degenerative diseases that are common in the older age group, such as dementia.
Symptoms
For generalized onset seizures
Motor symptoms may include sustained rhythmical jerking movements (clonic), muscles becoming weak or limp (atonic), muscles becoming tense or rigid (tonic), brief muscle twitching (myoclonus), or epileptic spasms (body flexes and extends repeatedly).
Non-motor symptoms are usually called absence seizures. These can be typical or atypical absence seizures (staring spells). Absence seizures can also have brief twitches (myoclonus) that can affect a specific part of the body or just the eyelids.
For focal onset seizures
Motor symptoms – may also include jerking (clonic), muscles becoming limp or weak (atonic), tense or rigid muscles (tonic), brief muscle twitching (myoclonus), or epileptic spasms. There may also be automatisms or repeated automatic movements, like clapping or rubbing of hands, lip-smacking or chewing, or running.
Non-motor symptoms – Examples of symptoms that don’t affect movement could be changes in sensation, emotions, thinking or cognition, autonomic functions (such as gastrointestinal sensations, waves of heat or cold, goosebumps, heart racing, etc.), or lack of movement (called behavior arrest).
For unknown onset seizures
Motor seizures – are described as either tonic-clonic or epileptic spasms.
Non-motor seizures – usually include a behavior arrest. This means that movement stops – the person may just stare and not make any other movements.
Diagnosis
Physical Exam
VS:
T 98.4 HR 67 RR 17 BP 116/67 O2 98% RA
Gen:
Well-appearing, no acute distress
HEENT:
PERRL, MMM, no lesions, discs sharp b/l
CV:
RRR, normal S1/S2, no M/R/G
Lungs:
CTAB, no crackles/wheezing, no focal consolidation
Abd:
+BS, soft, NT/ND, no hepatosplenomegaly
GU:
Testes descended b/l, no masses, non-tender
Ext:
Warm, well-perfused, no rashes/ecchymoses
Neuro:
AAOx4, CN II-XII intact, OS 20/40 OD 20/70, normal visual fields to confrontation, no dysmetria/dysdiadochokinesia, normal gait
Electrocardiography (ECG or EKG) is the process of recording the electrical activity of the heart over a period of time using electrodes placed on the skin. These electrodes detect the tiny electrical changes on the skin that arise from the heart muscle’s electrophysiologic pattern of depolarizing and repolarizing during each heartbeat. It is a very commonly performed cardiology test.
In a conventional 12-lead ECG, ten electrodes are placed on the patient’s limbs and on the surface of the chest. The overall magnitude of the heart’s electrical potential is then measured from twelve different angles (“leads”) and is recorded over a period of time (usually ten seconds). In this way, the overall magnitude and direction of the heart’s electrical depolarization are captured at each moment throughout the cardiac cycle. The graph of voltage versus time produced by this noninvasive medical procedure is an electrocardiogram.
Medical Uses
A 12-lead ECG of a 26-year-old male with an incomplete RBBB
The overall goal of performing electrocardiography is to obtain information about the structure and function of the heart. Medical uses for this information are varied and generally relate to having a need for knowledge of the structure and/or function. Some indications for performing electrocardiography include:
Suspected myocardial infarction (heart attack) or new chest pain
Suspected pulmonary embolism or new shortness of breath
A third heart sound, fourth heart sound, a cardiac murmur or other findings to suggest structural heart disease
Perceived cardiac dysrhythmias either by pulse or palpitations
Monitoring of known cardiac dysrhythmias
Chest pain
Atypical chest pain
Epigastric pain
Back, neck, jaw or arm pain without chest pain
Palpitations
Syncope or near syncope
Pulmonary edema
Exertional dyspnea
Weakness
Diaphoresis unexplained by ambient temperature
Feel of anxiety or impending doom
Suspected diabetic ketoacidosis
Fainting or collapse
Seizures
Monitoring the effects of a heart medication (e.g. drug-induced QT prolongation)
Assessing the severity of electrolyte abnormalities, such as hyperkalemia
Hypertrophic cardiomyopathy screening in adolescents as part of a sports physical out of concern for sudden cardiac death (varies by country)
Perioperative monitoring in which any form of anesthesia is involved (e.g. monitored anesthesia care, general anesthesia); typically both intraoperative and postoperative
As a part of a pre-operative assessment sometime before a surgical procedure (especially for those with known cardiovascular disease or who are undergoing invasive or cardiac, vascular or pulmonary procedures, or who will receive general anesthesia)
Cardiac stress testing
Computed tomography angiography (CTA) and Magnetic resonance angiography (MRA) of the heart (ECG is used to “gate” the scanning so that the anatomical position of the heart is steady)
Biotelemetry of patients for any of the above reasons and such monitoring can include internal and external defibrillators and pacemakers
Diagnosis
Numerous diagnoses and findings can be made based upon electrocardiography, and many are discussed above. Overall, the diagnoses are made based on the patterns. For example, an “irregularly irregular” QRS complex without P waves is the hallmark of atrial fibrillation; however, other findings can be present as well, such as a bundle branch block that alters the shape of the QRS complexes. ECGs can be interpreted in isolation but should be applied – like all diagnostic tests – in the context of the patient. For example, an observation of peaked T waves is not sufficient to diagnose hyperkalemia; such a diagnosis should be verified by measuring the blood potassium level. Conversely, a discovery of hyperkalemia should be followed by an ECG for manifestations such as peaked T waves, widened QRS complexes, and loss of P waves. The following is an organized list of possible ECG-based diagnoses.
Rhythm disturbances/arrhythmias:
Atrial fibrillation & atrial flutter without rapid ventricular response
T-wave inversion: Symmetric, compared to TWI associated with repolarization abnormalities
ST-elevation: Unlike J-point elevation, ST-segment merges with T-wave
Q-waves
Duration > 0.04s
Amplitude > 1/3 R-wave
Normal in aVR
Coronary Artery Territories
DISTRIBUTION
CORONARY ARTERY
LEADS
RECIPROCAL CHANGES
1. Inferior
RCA, PDA
II, III, aVF
Anterior, Lateral
2. Lateral
LCx
I, aVL, V5, V6
Inferior
3. Anterior
LAD
V1-V6
Inferior
4. Posterior
RCA
Posterior
Anterior (esp. V1)
ECG Guide: Pediatrics
ECG Standard
Full standard: no adjustment
Half-standard: commensurate reduction in amplitude (usually 50%)
Mixed: reduction in amplitude of precordial leads
Atrial Abnormalities
Right Atrial Abnormality (P pulmonale)
Peaked P-wave in II (>3mm from 0-6mo or >2.5mm >6mo)
Causes: right atrial volume overload, ASD, Ebstein, Fontan
Left Atrial Abnormality (P mitrale)
Wide, notched P-wave in II or biphasic in V1
Causes: MS, MR
Axis
Anatomical dominance of right ventricle until approximately 6mo
RAD normal
eRAD suggests AV canal defect
T-waves
1st week of life: Upright
Adolescent: Inverted
Adult: Upright
Ventricular Hypertrophy
Right Ventricular Hypertrophy
R-wave height >98% for age in lead V1
S-wave depth >98% for age in lead V6
T-wave abnormality (ex. upright in childhood)
Causes: pHTN, PS, ToF
Left Ventricular Hypertrophy
R-wave height >98% for age in lead V6
S-wave depth >98% for age in lead V1
Adult-pattern R-wave progression in newborn (no large R-waves and small S-waves in right precordial leads)
Left-axis deviation
Causes: AS, coarctation, VSD, PDA
Examples
Normal Neonatal ECG
2mo old
RAD
Inverted T-waves (normal)
Tall R-waves in V1-V3
Extreme Axis Deviation
Neonate with Down syndrome
Isoelectric in I, Negative in aVF negative in II mean QRS vector -87°
Extreme RAD suggestive of AV canal defect
LVH:
Unrepaired Coarctation
Deep S-wave in V1 (>98%)
Tall R-wave in V6 (>98%)
RVH:
10 year-old boy with pulmonary Hypertension
RAD after expected age for normal RAD
Tall R-waves in V1 (>98%)
Deep S-wave in V6 (>98%)
STEMI
ALCAPA (anomalous origin of the left coronary artery from the pulmonary artery): coronary artery arises anomalously from the pulmonary artery; as pulmonary arterial pressure falls during the first 6 months of infancy, prograde flow through the left coronary artery ceases and may even reverse.
HLHS (hypoplastic left heart syndrome): coronary arteries are perfused from a hypoplastic, narrow aorta that is susceptible to flow disruption
Orthotopic heart transplant with allograft vasculopathy
Kawasaki: coronary artery aneurysm with subsequent thrombosis
Benign early repolarization
14 year-old male
Concave ST-segment elevation
Left Atrial Abnormality:
9mo female with mitral insufficiency
Broad biphasic P-wave in V1
Tall, notched P-wave in II
Prolonged QT interval
18-year-old female
Familial long QT syndrome and a history of cardiac arrest
WPW:
Delta wave, shortened PR interval
ECG Guide: Part II
STEMI
ST-segment elevation ≥ 1mm in two contiguous leads
: ≥ 2mm V2-V3
: ≥ 1.5mm V2-V3
Posterior STEMI
ST-segment depression V1-V3 Posterior ECG
ST-segment elevation ≥ 0.5mm in V7-V9
Sgarbossa Criteria
Evaluation for STEMI in LBBB or paced rhythm
Normal: ST-segment discordant with QRS
QRS associated with ST-segment depression
QRS associated with (commensurate) ST-segment elevation
Score ≥ 3 98% specific for MI
Elevation
Concordant ST-segment elevation ≥ 1mm in any lead (5 points)
Depression
Concordant ST-segment depression ≥ 1mm in V1-V3 (3 points)
Discordant Elevation
Discordant ST-segment elevation ≥ 5mm in any lead (2 points)
Modified Sgarbossa Criteria
ST:S ratio ≥ 0.25 in any lead
Presence of any criterion is positive
Other Causes of ST-segment Elevation
Benign Early Repolarization
Concave ST-segment elevation
Notch at J-point
Asymmetric T-waves (steeper descent)
Pericarditis
Diffuse ST-segment elevation (except aVR)
PR-segment depression
Ratio: ST-elevation to T-wave amplitude ≥ 0.25 in V6 suggests pericarditis
LVH Strain
ST-segment elevation in V1-V3 in the setting of LVH
LV Aneurysm
Q-waves with ST-segment elevation in precordial leads
Ischemia and Prior Infarcts
Wellens: Type A
Suggestive of proximal LAD lesion
Wellens: Type B
Q-waves
≥ 40ms duration
Depth ≥ 25% of R-wave height
Syncope
ARVD
Epsilon wave
Brugada Syndrome: Type 1
Type 1: Coved ST-segment elevation
Brugada Syndrome: Type 2
Type 2: Saddle-back ST-segment elevation
HCM
Deep, narrow Q-waves
Wolff-Parkinson-White
Shortened PR-interval
Delta-wave
Other
Atrial Abnormalities
Normal
RAA: P-wave amplitude > 2.5mm in inferior leads
LAA: P-wave duration increased (terminal negative portion >0.04s), amplitude of terminal negative component >1mm below isoelectric line in V1
Left Bundle Branch Block
QRS duration > 0.12s (3 boxes)
Broad or notched R-wave with prolonged upstroke in I, aVL, V5, V6
Associated ST-segment depression and T-wave inversion
Reciprocal changes in V1, V2 (deep S-wave)
Possible LAD
Right Bundle Branch Block
QRS duration > 0.12s (3 boxes)
RSR’ in V1, V2
Reciprocal changes in I, aVL, V5, V6 (deep S-wave)
Axes
All ECG tracings are available for free, licensed (along with all content on this site) under Creative Commons Attribution-ShareAlike 4.0 International Public License.
Bradycardia
Brief H&P
A 38 year-old male with no medical history presents to the emergency department with abdominal pain. He had one episode each of non-bloody emesis followed by watery, non-bloody diarrhea and cited several sick contacts at home with similar symptoms. Vital signs were notable for bradycardia with a heart rate ranging from 38-46bpm though he was normotensive. The examination including abdominal examination was benign. A 12-lead electrocardiogram was obtained which demonstrated sinus bradycardia. The patient was asymptomatic during episodes of bradycardia and his heart rate responded appropriately during activity and on further history reported that he was an endurance athlete and runs multiple marathons each year. He was discharged after symptomatic improvement with anti-emetics.
Bradycardia
Definition: heart rate <60bpm
Sinus rhythm: upright P-wave in I, II, aV; inverted P-wave in aVR
Electrocardiographic Findings
Sinus bradycardia
Potentially asymptomatic and present in healthy individuals
Tachy-brady syndrome (sinus bradycardia/arrest interspersed with SVT)
Atrioventricular block
1st degree: PR prolongation, rarely symptomatic
2nd degree: Intermittent interruption of conduction of atrial impulses to ventricles
Type 1: progressive PR prolongation leading to interrupted conduction
Type 2: fixed PR interval with interrupted conduction
3rd degree: atrioventricular dissociation
Slow atrial fibrillation
Irregular RR interval without recognizable P-wave
Epidemiology
Analysis of 277 patients presenting to the emergency department with “compromising” bradycardia.
Symptoms
Syncope (33%)
Dizziness (22%)
Angina (17%)
Dyspnea/Heart Failure (11%)
ECG
High-grade AV block (48%)
Sinus bradycardia (17%)
Sinus arrest (15%)
Slow atrial fibrillation (14%)
Cause
Primary (49%)
Drug (21%)
Ischemia/Infarction (14%)
Pacemaker failure (6%)
Intoxication (6%)
Electrolyte disorder (4%)
Important Historical Features
Fever/travel
Chest pain
Cold intolerance, weight gain
Headache, AMS, trauma
Abdominal pain/distension
Medication changes
Important Examination Findings
Perfusion (temperature, capillary refill)
Presence of fistula or hemodialysis catheter
Existing device (malfunction)
Workup
ECG
Continuous telemetry monitoring
Labs
Potassium
Digoxin level
TFT
Infection titers (RPR, Lyme)
Cardiac enzymes
Management
Unstable
Airway
Atropine 0.5mg IV q3-5min (maximum 3mg)
Dopamine/epinephrine infusion
Temporary pacemaker (transcutaneous, transvenous) with blood-pressure preserving sedation
Admission and evaluation for permanent pacemaker placement
Stable (outpatient evaluation)
Event monitor
Stress test (chronotropic incompetence)
Algorithm for the Evaluation and Management of Bradycardia
Wellens Syndrome
Case Presentation
49M with a history of hypertension who presented to his primary physician for routine follow-up and was referred to the ED for an abnormal ECG. He denied chest pain, shortness of breath, or any limitation to baseline exercise tolerance. His vital signs were notable for systolic hypertension and his examination was unremarkable. A chest x-ray showed no acute cardiopulmonary findings. His initial ECG demonstrated a biphasic T-wave in V2 and deep, symmetric T-wave inversions in V3-V6. His initial serum troponin was markedly elevated at 3.499. He was admitted and urgent coronary angiography revealed proximal LAD stenosis (70%), mid-LAD stenosis (85%) and 1st right posterolateral stenosis (85%) which were stented. He was discharged on post-procedure day one and has remained asymptomatic at outpatient follow-up.
Presentation ECG
Biphasic T-wave in V2, deep and symmetric T-wave inversions in V3-V4
Post-Catheterization ECG
Resolution of biphasic T-wave and T-wave inversions
Presentation ECG
Post-Catheterization ECG
History
Initially described in 1982 where a subset of patients who did poorly with medical management of “impending myocardial infarction” (essentialy unstable angina) were found to have characteristic ECG changes. These patients were noted to be at increased risk for extensive anterior wall myocardial infarctions due to proximal LAD stenosis.
Criteria
History of chest pain
Normal or slightly-elevated cardiac enzymes
No precordial Q-waves
Isoelectric or <1mm ST-segment elevation
Pattern present in pain-free state
Type A (25%): Biphasic T-wave in V2/V3
Type B (75%): Deep, symmetrically inverted T-waves in V2/V3
Clinical Significance
Wellens Syndrome (or LAD coronary T-wave syndrome) represents a “pre-infarction” stage of coronary artery disease manifested by critical LAD stenosis. The natural history includes progression to extensive anterior wall myocardial infarction, often associated with severe left ventricular systolic dysfunction, cardiogenic shock and death. These changes may be mistaken for “non-specific” T-wave changes (which in the presence of a non-concerning history and typically non-elevated cardiac markers) may lead providers to inappropriate dispositions such a stress testing which is contraindicated. Recognition of this pattern and its appropriate management (urgent coronary angiography) is critical.
Case Summary
The case presented above is atypical. The patient had no history of chest pain and cardiac enzymes were significantly elevated – two features which are uncommon in Wellens Syndrome. However, the patient’s elevated cardiac biomarkers led to admission and angiography with identification of the characteristic proximal LAD stenosis (and other disease).
Nonsustained Ventricular Tachycardia
Case 1
64M with a history of HFrEF (LVEF 20-25%), CAD, AICD (unknown indication), COPD, CKD III presenting with gradual onset shortness of breath, progressive bilateral lower extremity edema.
Examination consistent with severe acute decompensated heart failure presumed secondary to left ventricular dysfunction.
Telemetry monitoring with multiple episodes of nonsustained ventricular tachycardia.
In the ED, the patient developed worsening respiratory failure despite initiation of therapy, requiring endotracheal intubation. Continuous cardiac monitoring revealed persistent salvos of NSVT, progressing to slow ventricular tachycardia without device intervention.
Device interrogation revealed multiple events, 3 shocks, several ATP’s over the recorded period.
Evaluation and Management:
NSVT with known (severe) ischemic heart disease
For repetitive monomorphic ventricular tachycardia: amiodarone, beta-blockade (if tolerated), procainamide (IIA, C)
ECG’s
ECG 1
Non-specific IVCD, LAA, VPC
ECG 2
VT initiated by fusion complex
ECG 1
ECG 2
Case 2
31F with the autoimmune polyglandular syndrome (adrenal, thyroid and endocrine pancreatic insufficiency), presenting with fever and cough.
Evaluation consistent with sepsis presumed secondary to the pulmonary source.
Telemetry monitoring initially with ventricular bigeminy, then nonsustained ventricular tachycardia.
In the ED, the patient developed pulseless ventricular tachycardia – apparently polymorphic. Chest compressions and epinephrine produced the return of spontaneous circulation with recovery to baseline neurologic function.
ECG revealed prolonged QTc and chemistry panel notable for critical hypokalemia/hypomagnesemia.
Evaluation and Management:
NSVT progressing to VT
Initially attributed to electrolyte disturbances. However, serial ECG’s continued to show prolonged QTc (possibly acquired, home medications included metoclopramide and erythromycin). Early echocardiography demonstrated global hypokinesis with EF 30-35% attributed to severe sepsis and recurrent defibrillation. Cardiac CT after resolution of acute illness showed persistently depressed ejection fraction without coronary atherosclerosis. The presence of NICM associated with malignant dysrhythmias warranted ICD placement.
Cardioversion for hemodynamic compromise (I, B), B-blockade (I, B), amiodarone if no LQTS (I, C), urgent angiography if ischemia not excluded (I, C)1
Correction of electrolyte abnormalities (specifically hypokalemia) may decrease progression to VF.
ECG’s
ECG 1
Ventricular bigeminy
ECG 2
Long-QT
VT on Telemetry
Non-sustained ventricular tachycardia noted on telemetry monitoring
ECG 1
ECG 2
VT on Telemetry
> 3-5 consecutive beats originating below the AV node
Rate > 100bpm
Duration <30s
Epidemiology
Occurs in 0-4% of ambulatory patients
Increased frequency in males and with increasing age
In some patients, NSVT is associated with an increased risk of sustained tachyarrhythmias and sudden cardiac death. In others it is of little prognostic significance.
Evaluation
In all patients:History: including arrhythmogenic medications/substances, pertinent family historyPhysical examinationECG/CXRTTEIn selected patients exercisetesting advancedimaging (CT/C-MR)Electrophysiologic studiesGenetic testing
NSVT in the absence of structural heart disease
NSVT in Idiopathic Ventricular Tachycardia
Ventricular outflow arrhythmias:
RVOT: 70-80%, LBBB pattern
LVOT: 20-30%, RBBB pattern
Mechanism:
Adrenergically mediated
Occur during exercise, resolve as heart-rate increases, recur during recovery
Management:
Exclude arrhythmogenic right ventricular cardiomyopathy (imaging, myocardial biopsy)
If symptomatic, beta-blockade, ± IC anti-arrhythmic, CCB (verapamil) for ILVT
Fibrosis, fibro-fatty replacement of myocardium in RVIT/RVOT/RV apex
May occur with only subtle structural abnormalities of the right ventricle
LBBB morphology
Management
Anti-arrhythmias of limited utility
Catheter ablation, ICD backup
Prognosis
Increased risk SCD
NSVT with apparent structural heart disease1
Hypertension and LVH
Mechanism
Stretch-induced abnormal automaticity
Fibrotic tissue
Presence of NSVT correlates with the degree of hypertrophy and subendocardial fibrosis
Management
Evaluation for ischemic heart disease
Aggressive medical management of hypertension (including beta-blockade)
Prognosis
Unclear
Valvular Disease
Mechanism
High incidence in AS, severe MR (25%)
Mechanical stress from dysfunctional valvular apparatus
Management
Beta-blockade if symptomatic
Prognosis
No evidence that NSVT is an independent predictor of SCD.
Ischemic Heart Disease9-14
Mechanism
Monomorphic VT associated with re-entry at the borders of ventricular scars
Ischemia induces polymorphic NSVT/VF
Management
Revascularization, beta-blockade, statin, ACE/ARB
MADIT I, MUSTT: ICD for ICM LVEF <40%, NSVT, EPS inducible VT
MADIT II, SCD-HeFT: ICD for moderate-to-severe LV dysfunction irrespective of NSVT or EPS findings
Prognosis
NSTEMI with NSVT >48h after admission 2x risk SCD (MERLIN-TIMI 36)
STEMI with NSVT common, not as predictive of ACM or SCD as LVEF (CARISMA)
NSVT <24h after admission for NSTEMI/STEMI not of prognostic significance.
Hypertrophic Cardiomyopathy
Mechanism
Genetic myocardial disease
Myocyte disarray, fibrosis, ischemia result in arrhythmogenic substrate
Management
Restriction of physical activity
(NSVT, LV thickness, FH SCD, syncope, abnormal BP response to exercise)
Beta-blockade, anti-arrhythmic for symptoms
Prognosis
Increased risk SCD (1% annual)
Other Conditions
Non-ischemic dilated cardiomyopathy
Giant-cell myocarditis
Repaired TOF
Amyloidosis
Sarcoidosis
Chagas cardiomyopathy
Algorithm for the Evaluation of NSVT
Low Voltage ECG
Definition
QRS in limb leads <5mm
QRS in precordial leads <10mm
General Causes
Fluid, fat or air attenuating signal
Myocardial infiltration
Loss of viable myocardium
Example
Low Voltage ECG
ECG of patient with pericardial effusion
Baseline ECG
Old ECG from same patient
Low Voltage ECG
Baseline ECG
Differential Diagnosis of Low Voltage ECG
ECG Guide
The format of this article is atypical for the structure and concept of the website – but it’s always been about learning. Here is a simplified guide to ECG interpretation with a focus on the aspects I find more challenging to understand or recall.