Face surgery specialty involving the restoration, reconstruction, or alteration of the human body. It can be divided into two main categories: reconstructive surgery and cosmetic surgery. Reconstructive surgery includes craniofacial surgery, hand surgery, microsurgery, and the treatment of burns
Surgical Considerations and Face surgery
Anatomy of the face is essential when it comes to surgeries in the face. The face is highly vascularized and heavily innervated by nerves. The knowledge of the anatomy of the face can guide clinicians in the avoidance of damage to crucial structures in the face during surgeries and injections in the face.
A forehead lift, also known as a brow lift, is a surgical procedure that some individuals receive to decrease the appearance of wrinkles across the forehead, bridge of the nose, and between the eyes. A plastic surgeon usually performs this surgery. The procedure consists of removing segments of excess skin and fat to reduce the appearance of wrinkles.[rx]
Cheek augmentation is a cosmetic procedure that enhances the appearance of the cheeks by adding volume, removing sagginess, or removing wrinkles. The augmentation of the cheeks can be done by implantation of cheek implants or the injection of fillers to add volume to the cheeks. The addition of implants or injected fillers will increase the volume of the cheeks, usually resulting in less sagging and wrinkling of the cheeks.
Otoplasty is a surgical procedure done to correct or alter the ear. This surgery is done to improve the proportions and position of the ear to make a face appear more desirable to the patients.[rx]
Rhytidectomy is also known as a facelift. This procedure reduces the appearance of wrinkles and sagging skin from aging. In a facelift, the surgeon may remove the excess fat pad and resect excess sagging skin to create a tighter and more defined face.[rx]
Lower rhytidectomy is also known as a neck lift. This procedure targets the platysma muscle. The resection and tightening of the skin on the neck make the neck appear more desirable and hides the features of aging in some individuals.[rx]
Buccal fat removalis a procedure where the buccal fat pad is removed to create the illusion of dimpling and a more defined cheekbone.[rx]
Mentoplasty is a procedure done to enhance the appearance of the chin by implants or resection of the chin. The decision to resect or to add chin implants is decided by the patient on what would make them appear more natural or enhanced.
Blepharoplasty is a procedure done to alter the appearance of the eyelids. This procedure can reduce the appearance of bags under the eyes, eye puffiness, wrinkles due to excess skin, or reduction of excess skin that is obstructing vision.
Facial implants are done to enhance the appearance of the cheeks, chin, or jaw by the placement of implants. Implants are done to enhance and make the various regions appear fuller with less wrinkling.
Rhinoplasty is also known as a nose job. Rhinoplasties are done to alter the appearance of the nose to make it appear more proportionate to the dimensions of the face.
All of these procedures are also useful in conjunction with facial trauma repairs. In facial traumas, the surgeons operate to repair and restore the appearance of the patient’s face. Sometimes the cosmetic procedures are done as adjunctive in facial trauma repairs to optimize the surgical approach to the restoration of the face.
How Many Muscle Are Attach in Foot?/Foot Muscles acting on the foot can be divided into two distinct groups; extrinsic and intrinsic muscles. The extrinsic muscles arise from the anterior, posterior and lateral compartments of the leg. They are mainly responsible for actions such as eversion, inversion, plantarflexion and dorsiflexion of the foot.
The foot is a complex mechanical structure of the human body composed of 33 joints, 26 bones, and more than a hundred muscles, tendons, and ligaments that all work together to bear weight, allow for locomotion, and transmit force. The joints of the foot are made wherever two or more of the foot bones meet
There are 29 muscles associated with the human foot. (10 foot/ankle and 19 intrinsic) Ten of these muscles originate outside of the foot itself but cross the ankle joint to act on the ankle joint and help position the foot. The other 19 muscles are referred to as intrinsic muscles of the foot and act only within the foot. The muscles covered in this article serve various roles in gait as well as posture. These muscles are also aided by the plantar fascia, managing the mechanical vectors of the foot. The muscles of the foot influence the posture and the shape of the foot, as well as providing the ability to transmit muscle tension not only towards the ground but also towards the whole body system.
Blood Supply of Foot Muscles
The blood supply to the foot begins primarily with the popliteal artery. The popliteal artery branches off the large superficial femoral artery and gives rise to the three main branches supplying the lower leg and foot. The three branches from proximal to distal are the anterior tibial artery, peroneal artery, and posterior tibial artery. The anterior tibial artery continues distally to supply the anterior and dorsal portions of the foot. Once the anterior tibial artery passes under the extensor retinaculum, it becomes the dorsalis pedis. This artery is commonly palpated for a pedal pulse. The dorsalis pedis continues under the extensor hallucis longus and passes between it and the extensor digitorum longus. The dorsalis pedis has three lateral branches named the proximal and distal tarsal arteries and the arcuate artery, and two medial branches named the medial tarsal arteries. The arcuate artery branches at the level of the 1st tarsal-metatarsal joint and courses over the metatarsals 2 to 4 to give rise to the dorsal metatarsal arteries 2 to 4. The first dorsal metatarsal artery branches directly off the dorsalis pedis. The metatarsal branches supply the dorsal interosseous muscles of the foot. The peroneal artery supplies the muscles of the lateral leg and the posterior foot. Finally, the posterior tibial artery supplies the posterior and lateral leg as well as the plantar surface of the foot.[rx]
The venous system of the lower limbs is composed of deep veins (which run between the muscles) and superficial veins (which constitute a complex network just below the skin). The two systems are joined by transfascial valved communications that constitute a real system, that of the perforating veins. The perforating veins have the function of favouring the outflow of the blood that flows in the system superficial (about 10%) towards the deep system.
In the sole of the foot, there is a sort of sponge, consisting of a complicated intertwining of superficial and deep veins which, at each step, is emptied by compression on the ground. Thanks to this mechanism, the blood is pushed over the ankle up to the calf.
The venous system originates in the microcirculation from the arterial capillaries (afferent branch) to continue with the venous capillaries that converge in the collecting venules first and then in the collecting veins, thus constituting the initial efferent branch of venous macrocirculation.
In the anterior region the dorsal venous network of the foot through the intercapitular veins that pass through the interdigital spaces; the digital veins, joining two to two in the interdigital spaces, originate the metatarsal veins that are directed in the deep plantar venous arch, converging in the lateral plantar veins; these, after joining posteriorly with the medial plantar veins, originate the two posterior tibial veins. The anterior tibialis originate from the deep veins of the dorsal region of the foot. The medial marginal vein of the foot ascending anterior to the medial malleolus forms the internal saphenous vein or the great saphenous vein. The lateral marginal vein of the foot ascending anterior to the lateral malleolus forms the small saphenous vein.
The lymph drained from the lower limb reaches the external and common iliac lymph node chains. The fingers and the sole of the foot are rich in superficial lymphatic vessels, which gather in the medial and lateral collectors. The lymph drained deeply from the foot, concerns above all the articular area, bone and muscle and aponeurosis; the lymph gathers in the popliteal and femoral collectors.
Nerves Supply of Foot Muscles
There will be discussion regarding innervation of the various muscles in greater detail in the sections that follow. The initial nerve that gives rise to most of the innervation of the lower extremity is the sciatic nerve. The sciatic nerve makes its way out of the lumbosacral plexus and passes under the piriformis muscle before traveling distally. Around the distal third of the femur, the sciatic nerve branches to give rise to the common fibular nerve and the tibial nerve. The tibial nerve continues distally to give rise to the medial calcaneal branches, the medial sural cutaneous nerve, and the medial and lateral plantar nerves. The common peroneal nerve gives rise to two main branches, the superficial peroneal and the deep peroneal nerves. The superficial peroneal nerve primarily gives rise to cutaneous branches that receive sensory information from the skin. The deep peroneal nerve supplies motor function to many of the muscles responsible for dorsiflexion of the foot.[rx][rx]
The nerves of the foot, their branches, and their origins include [rx]
Superficial peroneal (fibular) nerve (arises from the common fibular nerve)
Deep peroneal (fibular) nerve (arising from the common fibular nerve)
Tibial nerve (arises in the popliteal fossa as a division of the sciatic nerve)
Medial plantar nerve (arises from the larger terminal branch of the tibial nerve)
Digital nerves (arise from both the medial and lateral plantar nerves)
Lateral plantar nerve (arises from the smaller terminal branch of the tibial nerve)
Inferior calcaneal nerve, also known as Baxter’s nerve (typically arises as the first branch of the lateral plantar nerve)
Medial calcaneal nerve (typically arises from the tibial nerve)
Sural nerve (typically arises from branches of both the common fibular and tibial nerves)
Saphenous nerve (arises from the femoral nerve)
The sural nerve originates from branches of both the common fibular nerve and the tibial nerve. It supplies the lateral hind and midfoot. The calcaneal branches originate from the tibial and sural nerves and sensory innervation to the skin of the heel.[rx][rx]
Sciatic
Tibial
Medial sural cutaneous
Medial calcaneal
Medial plantar
Common plantar digital nerves
Proper plantar digital nerves
Lateral plantar
Deep branch
Superficial branch
Common plantar digital nerves
Proper plantar digital nerves
Common fibular (peroneal)
Deep fibular
Lateral terminal branch
Medial terminal branch
Superficial
Medial dorsal cutaneous
Intermediate dorsal cutaneous
Sural
Lateral dorsal cutaneous
Lateral calcaneal
Muscles Attachment of Foot Muscles
The fascia plays a key role in dividing and attaching muscles in the foot. The relationship of the fascia with the muscles can be further described by the compartment they are in.
Medial compartment: The medial plantar fascia overlies the abductor hallucis, flexor hallucis brevis, and the flexor hallucis longus tendon.
Central compartment: The central plantar fascia overlies the flexor digitorum brevis, the tendon of the flexor hallucis longus, the tendons and musculature of the flexor digitorum longus, the quadratus plantae, the lumbricals, and the adductor hallucis.
Lateral compartment: The lateral plantar fascia overlies the abductor and flexor digiti minimi brevis.
Interosseous compartment: The plantar and dorsal interosseous fascias border the interosseous muscles.
Dorsal compartment: The dorsal fascia overlies the extensors hallucis brevis and extensor digitorum brevis.
To simplify the organization of the muscles, the following will break them up into those that act upon the foot and ankle and those classified as intrinsic.[rx][rx][rx]
Foot and Ankle
Peroneus Longus
The peroneus longus is one of the three muscles that span the lateral leg – peroneus may also be interchanged with fibular, referring to the lateral bone of the lower leg running deep to the peroneal muscles
Origin: The peroneus longus muscle originates on the head of the fibula and the upper half of the fibular shaft – this muscle crosses the ankle joint and courses deep into the foot and passes into a groove of the cuboid bone.
Insertion: the posterolateral aspect of the medial cuneiform bone and the lateral portion of the base of the first metatarsal
Action: The peroneus longus acts to evert the foot, plantarflex the ankle and adds support to the transverse arch of the foot
Blood Supply: Anterior tibial artery
Innervation: Superficial peroneal nerve
Peroneus Brevis
The peroneus brevis is another of the three muscles spanning the lateral leg and may also be called fibularis brevis, referring to the fibula
Origin: The peroneus brevis originates on the inferior two-thirds of the lateral fibula and courses posteriorly to the lateral malleolus of the fibula ultimately
Insertion: The styloid process of the fifth metatarsal
Action: The primary action of the peroneus brevis is to evert the foot and plantar flex the ankle
Blood Supply: Peroneal artery
Innervation: The superficial peroneal nerve innervates the peroneus brevis muscle
Peroneus Tertius
The peroneus tertius is the third and final muscle of the lateral peroneus or fibular muscles
Origin: The peroneus tertius originates from the middle fibular shaft
Insertion: The dorsal surface of the fifth metatarsal
Action: Dorsiflex, evert, and abduct the foot
Blood Supply: The peroneus tertius primarily receives its blood supply from the anterior tibial artery
Innervation: Peroneus tertius innervation comes from the deep peroneal nerve, an innervation different than its similarly named peroneal counterparts
Anterior Tibialis
The anterior tibialis is the most prominent muscle in the anterior leg and is often visible during dorsiflexion of the foot
Origin: The lateral condyle of the tibia and the proximal half to two-thirds of the tibial shaft.
Insertion: Occurs after passing under the extensor retinaculum and is on the medial and plantar surfaces of the medial cuneiform and base of the 1st metatarsal.
Action: Dorsiflex the ankle and invert the hindfoot
Blood Supply: Anterior tibial artery
Innervation: Comes from the deep peroneal nerve
Posterior Tibialis
Origin: The superior two-thirds of the medial posterior surface of the tibia
Insertion: The tendon courses distally, splitting into two at the calcaneonavicular ligament, to insert on the tuberosity of the navicular bone (superficial slip) and the plantar surfaces of the metatarsals two to four (deep slip)
Action: The posterior tibialis is the primary inverter of the foot but also adducts, plantar flexes, and aides in supination of the foot
Blood Supply: Sural, peroneal, and posterior tibial arteries
Innervation: Tibial nerve
Extensor Digitorum Longus
Origin: Lateral tibial condyle and continues distally to split into four tendons after the level of the extensor retinaculum
Insertion: Dorsum of the middle and distal phalanges
Action: Extend the second through fifth digits and dorsiflex the ankle
Blood Supply: anterior tibial artery
Innervation: deep peroneal nerve
Flexor Digitorum Longus
Origin: Posterior surface of the tibia distal to the popliteal line
Insertion: Continues distally to split into four individual tendons which insert on the plantar surfaces of the bases of the second through fifth distal phalanges
Action: Flex the digits two through five and may aid in plantar flexion of the ankle
Blood Supply: Posterior tibial artery
Innervation: Tibial nerve
Flexor Hallucis Longus
Origin: inferior two-thirds of the posterior fibula
Insertion: The plantar surface of the base of the distal phalanx of the great toe
Action: Flex the great toe but may minimally supinate and plantar flex the ankle
Blood Supply: Peroneal and posterior tibial artery
Innervation: Tibial nerve
Gastrocnemius
The gastrocnemius is the most superficial calf muscle
Origin: femoral condyles
Insertion: thick Achilles tendon inserting on the calcaneus.
Action: Plantarflex the ankle.
Blood Supply: Sural branch of the popliteal artery
Innervation: Tibial nerve
Soleus
The soleus is the deep muscle of the posterior leg and makes up most of the bulk of the calf
Origin: Upper quarter of the posterior fibula and the middle third of the posterior tibial shaft
Insertion: The soleus eventually joins the gastrocnemius to for the Achilles tendon to insert on the calcaneus
Action: The action is to plantarflex the ankle
Blood Supply: Posterior tibial, peroneal, and sural arteries
Innervation: Tibial nerve
Intrinsic
Dorsal
Extensor Digitorum Brevis
Origin: Dorsal surface of the calcaneus
Insertion: The base of the proximal phalanx of digits two through four
Action: Extend the toes
Blood Supply: Dorsalis pedis
Innervation: Deep peroneal nerve
Dorsal Interosseus
The dorsal interossei muscles (3) exist between digits two through five – the two adjacent muscles form a central tendon and act to abduct the metatarsal-phalangeal joints and innervation comes from the lateral plantar nerve
Extensor Hallucis Brevis
Origin: Dorsal surface of the calcaneus
Insertion: The base of the proximal phalanx of the great toe
Action: Extend the great toe
Blood Supply: Dorsalis pedis.
Innervation: Deep peroneal nerve
Plantar
1st layer
Abductor Hallucis
Origin: Calcaneal tuberosity
Insertion: Base of the great toe and the proximal phalanx.
Action: Abduct the great toe
Blood Supply: Medial plantar artery
Innervation: Medial plantar nerve
Flexor Digitorum Brevis
Origin: Calcaneal tuberosity
Insertion: The middle phalanx of digits two thorugh five
There are four muscles referred to as lumbricals in the foot
Origin: Flexor digitorum longus tendon
Insertion: Extensor digitorum longus tendon
Action: Flex the metatarsophalangeal joints and extend the interphalangeal joints
Blood Supply: Medial and lateral plantar arteries
Innervation: Medial and lateral plantar nerve
3rd layer
Flexor Hallucis Brevis
Origin: The cuboid and the lateral cuneiform
Insertion: Proximal phalanx of the great toe
Action: Flex the great toe
Blood Supply: Medial plantar artery
Innervation: Medial plantar nerve
Oblique and Transverse Head of Adductor Hallucis
The adductor hallucis has two heads, an oblique head, and a transverse head
Origin: The oblique head originates at the proximal ends of the metatarsals two thourgh four, and the transverse head originates via MTP ligaments of digits three through five
Insertion: inserts at the proximal phalanx of the great toe
Action: The primary action is to adduct the great toe
Blood Supply: First plantar metatarsal artery
Innervation: Deep branch of lateral plantar
Flexor Digiti Minimi Brevis
Origin: Base of the fifth metatarsal
Insertion: Proximal phalanx of the fifth metatarsal
Action: The primary action is to flex the fifth digit
Blood Supply: Lateral Plantar artery
Innervation: Lateral plantar nerve
4th layer
Plantar Interosseous
The plantar interossei (3)
Origin: medial aspect of the individual metatarsals of digits three through five
Indications/ Uses of Knee Arthroplasty /Knee arthroplasty is a reconstruction of the knee joint. It is more commonly referred to as a total knee replacement and is a very reliable procedure with predictable results. Total knee arthroplasty (TKA) is an excellent treatment option for individuals with symptomatic osteoarthritis in at least 2 of the 3 compartments of the knee and who have failed conservative treatment.[rx][rx] Additionally, partial knee arthroplasty (PKA) is an excellent treatment option for individuals with symptomatic osteoarthritis localized to 1 compartment of the knee and who have failed conservative treatment.[rx] The primary goal of either surgery is durable pain relief with the improvement of functional status.
Anatomy and Physiology of Knee Arthroplasty
The knee is a synovial hinge joint with minimal rotational motion. It is comprised of the distal femur, proximal tibia, and the patella. There are 3 separate articulations and compartments: medial femorotibial, lateral femorotibial, and patellofemoral. The stability of the knee joint is provided by the congruity of the joint as well as by the collateral ligaments. The capsule surrounds the entire joint and extends proximally into the suprapatellar pouch. Articular cartilage covers the femoral condyles, tibial plateaus, trochlear groove, and patellar facets. Menisci are interposed in the medial and lateral compartments between the femur and tibia which act to protect the articular cartilage and support the knee.
The mechanical axis of the femur, defined by a line drawn from the center of the femoral head to the center of the knee, is 3 degrees valgus to the vertical axis. The anatomic axis of the femur, defined by a line bisecting the femoral shaft, is 6 degrees valgus to the mechanical axis of the femur and 9 degrees valgus to the vertical axis.[rx] The proximal tibia is oriented to 3 degrees of varus. The varus position of the proximal tibia, along with the offset of the hip center of rotation, results in the weight-bearing surface of the tibia is parallel to the ground. The sagittal alignment of the proximal tibia is sloped posteriorly approximately 5 to 7 degrees. The asymmetry of the natural bony anatomy maintains the alignment of the joint and ligamentous tension.
Indications of Knee Arthroplasty
TKA is a well-described treatment option for patients suffering from knee pain secondary to osteoarthritis who have failed conservative treatment measures. It is a reliable procedure that provides pain relief and improves the patient’s functional status.[rx] Furthermore, the need for correction of a significant or progressive deformity at the knee with evidence of osteoarthritis can also be an indication for a TKA. A patient with persistent knee pain without radiographic evidence of knee osteoarthritis should have further workup to exclude other possible sources of their pain.
Presence of active infection elsewhere in the body
Extensor mechanism dysfunction
Medically unstable patient
Relative
Neuropathic joint
Poor overlying skin condition
Morbid obesity
Noncompliance due to major psychiatric disorder, alcohol, or drug abuse
Insufficient bone stock for reconstruction
Poor patient motivation or unrealistic expectation
Severe peripheral vascular disease
Equipment of Knee Arthroplasty
A TKA system will consist of instrumentation that helps the surgeon prepare the ends of the femur, tibia, and patella to receive an implant. The instrumentation will be specific to the brand and type of implant being used with each company and model having specific intricacies.
In general, the instrumentation will consist of:
Intramedullary femoral guide to help establish the distal femoral alignment
The distal femoral cutting guide
Femoral sizing guide
The 4-in-1 femoral cutting guide
The extramedullary or intramedullary tibial guide
The proximal tibial cutting guide
Patella sizing guide
Femoral component trial
Tibial baseplate trial
Patellar button trial
Trial plastic bearing
The final implants will come in individual sterile packages and will consist of:
Femoral component, typically made of cobalt-chrome
Tibial component, typically made of cobalt-chrome or titanium
Tibial polyethylene bearing, made of an ultra high molecular weight (UHMW) polyethylene
Patellar button, made of UHMW polyethylene
Personnel
Anesthesia team
Operating room nurse
Surgical technician
Surgical assistant
Preparation
Full medical and drug history before surgery
Appropriate pre-surgical workup, clearance, and optimization
Pre-operative radiographs of the affected knee
Pre-operative templating of the affected knee to estimate the component size
Primary TKA system of choice
Have various final implant sizes ready and available in the hospital
Have increasing prosthesis constraint options ready and available in the hospital
Have revision total knee replacement system of choice ready and available if needed
+/- antibiotic cement, surgeon preference
The Technique of Knee Arthroplasty
The goal of TKA is the same regardless of surgeon, implant, or technique. The variability in the procedure lies in the technique. Some of the variations in operative technique for TKA are listed below.
General anesthesia versus regional anesthesia
Tourniquet versus tourniquet-less surgery
Standard versus patient-specific instrumentation
Standard versus patient-specific implants
Traditional versus robotic-assisted TKA
Traditional versus navigation-assisted TKA
Traditional versus sensor-assisted TKA
Measured resection versus gap balancing
Cruciate-retaining implant versus cruciate stabilized the implant
Resurfaced versus non-resurfaced patella
Cement versus cement-less (press fit) TKA
Complications of Indications/ Uses of Knee Arthroplasty
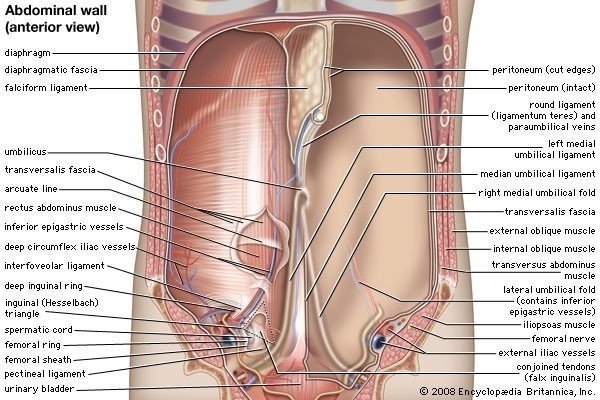
Transversus abdominis Muscle/Transversus abdominis (Transversalis muscle), so-called from the direction of its fibers, is the most internal of the flat muscles of the abdomen, being placed immediately beneath the obliquus internus. It arises, by fleshy fibers, from the lateral third of the inguinal ligament, from the anterior three-fourths of the inner lip of the iliac crest, from the inner surfaces of the cartilages of the lower six ribs, interdigitating with the diaphragm, and from the lumbodorsal fascia. The muscle ends in front in a broad aponeurosis, the lower fibers of which curve downward and medial ward, and are inserted, together with those of the Obliquus internus, into the crest of the pubis and pectineal line, forming the inguinal aponeurotic falx.
The transverse abdominal muscle (TVA), also known as the transverse abdominis, transversalis muscle and transversus abdominis muscle, is a muscle layer of the anterior and lateral (front and side) abdominal wall which is deep to (layered below) the internal oblique muscle. It is thought by most fitness instructors to be a significant component of the core.
Anatomy of Transversus Abdominis
The transverse abdominal so-called for the direction of its fibers, is the innermost of the flat muscles of the abdomen, being placed immediately beneath the internal oblique muscle.
The transverse abdominal arises as fleshy fibers, from the lateral third of the inguinal ligament, from the anterior three-fourths of the inner lip of the iliac crest, from the inner surfaces of the cartilages of the lower six ribs, interdigitating with the diaphragm, and from the thoracolumbar fascia.
It ends anteriorly in a broad aponeurosis (the Spigelian fascia), the lower fibers of which curve anteromedially (medially and downward), and are inserted, together with those of the internal oblique muscle, into the crest of the pubis and pectineal line, forming the inguinal conjoint tendon also called the aponeurotic falx. In layman’s terms, the muscle ends in the middle line of a person’s abdomen.
At A Glance Transversus Abdominis
The transversus abdominis is the deepest of the flat muscles, with transversely running fibers. Deep to this muscle is a well-formed layer of fascia, known as the transversal fascia.
Attachments – Originates from the inguinal ligament, costal cartilages 7-12, the iliac crest and thoracolumbar fascia. Inserts into the conjoint tendon, xiphoid process, linea alba and the pubic crest.
Functions – Compression of abdominal contents.
Innervation- Thoracoabdominal nerves (T7-T11), subcostal nerve (T12) and branches of the lumbar plexus.
Origin of Transversus Abdominis
Transversus abdominis originates from;
The deep surface of lower six costal cartilages
Lumbar fascia
Anterior two-thirds of the iliac crest
Lateral third of inguinal ligament
The part of transversus abdominis, which originates from the costal cartilages, interdigitate with the attachment of diaphragm from the same place.
Insertion of Transversus Abdominis
Transversus abdominis is inserted into:
Xiphoid process
Linea alba
Symphysis pubis
The lowest tendinous fibers of transversus joint similar fibers from the internal oblique to form the conjoint tendon, which is fixed to the pubic crest and the pectineal line.
It should be appreciated that the posterior border of external oblique muscle is free, while the same borders of the internal oblique and transversus abdominis are attached to the lumbar vertebrae through the lumbar fascia.
Blood Supply of Transversus Abdominis
It receives its blood supply from;
Lower posterior intercostal and subcostal arteries
Superior and inferior epigastric arteries
Superficial and deep circumflex arteries
Posterior lumbar arteries
Nerve Supply to Transversus Abdominis
It is innervated by the branches of the following nerves.
Lower five intercostal nerves
Subcostal nerve
Iliohypogastric nerve
Ilioinguinal nerve
The lower five intercostal and subcostal nerves represent the lower six thoracic spinal nerves while the iliohypogastric and ilioinguinal nerves represent the first lumbar spinal nerve.
Functions of Transversus Abdominis
The main function of transversus abdominis is the maintenance of an abdominal tone. It also plays a significant role in increasing intra-abdominal pressure.
The transverse abdominal helps to compress the ribs and viscera, providing thoracic and pelvic stability. This is explained further here. The transverse abdominal also helps a pregnant woman to deliver her child.
Without a stable spine, one aided by proper contraction of the TVA, the nervous system fails to recruit the muscles in the extremities efficiently, and functional movements cannot be properly performed.[rx] The transverse abdominal and the segmental stabilizers (e.g. the multifidi) of the spine have evolved to work in tandem.
While it is true that the TVA is vital to back and core health, the muscle also has the effect of pulling in what would otherwise be a protruding abdomen (hence its nickname, the “corset muscle”). Training the rectus abdominal muscles alone will not and can not give one a “flat” belly; this effect is achieved only through training the TVA.[rx]
Thus to the extent that traditional abdominal exercises (e.g. crunches) or more advanced abdominal exercises tend to “flatten” the belly, this is owed to the tangential training of the TVA inherent in such exercises. Recently the transverse abdominal has become the subject of debate between Biokineticists, kinesiologists, strength trainers, and physical therapists. The two positions on the muscle are (1) that the muscle is effective and capable of bracing the human core during extremely heavy lifts and (2) that it is not. Specifically, one recent systematic review has found that the baseline dysfunction of TVA cannot predict the clinical outcomes of low back pain.[rx]
Best Exercise For Transversus Abdominis
Do 15 of each of these exercises (or, for the plank, five 10-second holds with minimal rest in between), then repeat for two to three sets total. If that’s too much, try 10 reps–or work your way up to 20 for an extra challenge.
1. Dead Bug — 15 reps
“This exercise is a great way to really focus on that hollow hold or the pelvic tilt and get those abs engaged correctly,” says Lefkowith.
Lie on your back with your feet in the air and knees bent 90 degrees. Raise your arms in the air so that your hands are directly above your shoulders.
Slowly extend your right leg in front of you and your left arm above your head, keeping your lower back pressed against the floor.
Return to the starting position. Repeat on the other side.
Do 15 reps.
2. Forearm Plank — 5 10-second holds
“These are a great way to learn to properly engage your core especially if you focus on shorter, more intense holds,” says Lefkowith.
Start with your forearms and knees on the ground, shoulder-width apart. Elbows should be stacked underneath the shoulders, your forearms straight in front of you on the ground.
Lift your knees off the ground and push your feet back to bring your body to full extension, so your body creates one long line.
Keep your core tight and your hips lifted, and keep your neck in line with your spine.
Hold for 10 seconds, take a brief break then repeat four more times.
3. Bird Dog Crunch — 15 reps
“These work on core stability and they activate the glutes as you work your abs,” says Lefkowith.
Start on your hands and knees in a tabletop position with your wrists above your shoulders and your knees below your hips.
Inhale and extend your right arm forward and left leg back, maintaining a flat back and square hips.
Squeeze your abs and exhale as you draw your right elbow to your left knee.
Extend back out to start. Don’t forget to do both sides.
Do 15 reps.
Isolated abs exercises can help with activating your whole core before a workout, but your abs should also be working during larger movements. Don’t forget to stay engaged during compound moves that work your core along with other muscle groups, says Lefkowith—think goblet squats, dumbbell thrusters, and deadlifts.
How is tumor lysis syndrome diagnosed?/Tumor lysis syndrome (TLS) is characterized by a massive tumor cell death leading to the development of metabolic derangements and target organ dysfunction? TLS can occur as a result of cancer treatment or spontaneously. Blood cancers constitute the vast majority of TLS cases because of the sensitivity to therapy and rapid division rates.
Tumor lysis syndrome (TLS) is a potentially life-threatening condition that occurs in oncologic and hematologic patients with large tumor burden, either due to cytotoxic therapy or, less commonly, spontaneously because of massive tumor cell lysis. TLS is clinically characterized by acute renal failure, hyperuricemia, hyperkalemia, hyperphosphatemia, and hypocalcemia. While limited options are available for treating TLS, identifying patients at high risk for developing TLS and prevention in high-risk patients remain an important aspect in the treatment of cancer patients. In general, treatment of TLS consists of intensive hydration, stimulation of diuresis, and, more specifically, in the use of allopurinol and rasburicase.
Tumor lysis syndrome (TLS) describes the pathological sequela of the rapid lysis of tumor cells. The shift of potassium, phosphorus, and nucleic acid material into the extracellular space can rapidly overcome existing homeostatic mechanisms, leading to acute kidney failure, arrhythmia, and death. TLS is the most common oncologic emergency, and although commonly seen in the context of initial chemotherapeutic treatment of hematologic malignancies, increasing recognition is being paid to the occurrence of spontaneous TLS and TLS secondary to treatment of bulky solid tumors.[rx,rx]
Tumor lysis syndrome is a group of metabolic abnormalities that can occur as a complication during the treatment of cancer,[rx] where large amounts of tumor cells are killed off (lysed) at the same time by the treatment, releasing their contents into the bloodstream. This occurs most commonly after the treatment of lymphomas and leukemias. In oncology and hematology, this is a potentially fatal complication, and patients at increased risk for TLS should be closely monitored before, during, and after their course of chemotherapy.
Pathophysiology
The pathophysiology of tumor lysis syndrome is complicated. Tumor lysis syndrome is caused by the massive release of intracellular ions such as potassium, phosphorus, and nucleic acids that have been metabolized to uric acid. The main organ is responsible for the excretions of these substances in the kidney. When the compensatory response of the kidney is exhausted as a result of the massive release of intracellular ions, uric acid obstructive uropathy develops which can then progress to acute kidney injury.
Molecules called nucleotides comprise DNA. These nucleotides are units made of a phosphate group, a sugar group, and a nitrogen base. The nitrogen base is adenine, thymine, guanine or cytosine. Adenine and guanine are purines while thymine and cytosine are pyrimidines. Ribonucleic acid, however, is made up of a ribose sugar and a nitrogen base adenine, thymine, and uracil.
The metabolism of the purines adenine and guanine in a stepwise process leads to the production of xanthine. Adenine is metabolized to hypoxanthine whereas guanine is metabolized to xanthine. Xanthine is then further metabolized into uric acid in a reaction that is catalyzed by xanthine oxidase. Most mammals have the enzyme urate oxidase that can transform uric acid to allantoin which is a more soluble substance that can be easily excreted by the kidney. Human beings lack this enzyme.
Due to the rapid turnover of tumor cells, there is an overwhelming production of uric acid which then crystallizes in the renal tubules causing obstructive uropathy from and decreased glomerular filtration rate. In rat models, urate nephropathy causes an increase in both proximal and distal tubule pressure. Peritubular capillary pressure and vascular resistance also increase. Uric acid scavenges nitric oxide which is a potent vasodilator. The scavenging of nitric oxide produces vasoconstriction and kidney ischemia. Uric acid is also a potential pro-inflammatory agent and can cause the release of other cytokine-like tumor necrosis factor-alpha, protein I. These cytokines attract white blood cells and facilitate further injury to the kidney.
Electrolyte Imbalance
Hyperkalemia – The concentration of potassium within the cell is about 120 to 130 meq/L. The lysis of tumorous cells leads to a massive release of intracellular potassium. The excess potassium is usually taken up by the liver and skeletal muscle. The rest is excreted via the gastrointestinal system or the kidney. The obstructive uropathy from uric acid salts can limit the excretion of potassium. Sometimes the hyperkalemia from the solid tumor can reach a potentially life-threatening level. The risk of hyperkalemia is cardiac arrest from arrhythmia.
Hyperphosphatemia – Hyperphosphatemia is another electrolyte imbalance associated with tumor lysis syndrome. The nucleic acid has a phosphate group, and the breakdown of the tumorous cell will lead to the release of a significant amount of phosphorus into the bloodstream. Most of the phosphorus is really excreted. This ability of the kidney to handle a high load of phosphorus is inhibited by acute kidney injury or chronic kidney disease. Hyperphosphatemia is less common in spontaneous tumor lysis syndrome than those induced by chemotherapy. It leads to the chelation of calcium causing hypocalcemia. Deposition of calcium and phosphorus salts in the kidney and soft tissues can also occur.
Hypocalcemia – Hypocalcemia in tumor lysis syndrome is mostly secondary to the chelation of phosphorus. This condition is more potentially life-threatening than hyperphosphatemia. Possible complications from hypocalcemia include arrhythmia, tetany, seizure, and death. The calcium level might still be relatively low even after the normalization of the phosphorus level because of a deficiency of 1, 25 Vitamin D.
Causes of Tumor Lysis Syndrome
Tumor lysis syndrome is most common in patients diagnosed with leukemia who have a very high white blood cell (WBC) count. It can also be seen in high-grade lymphomas especially after the initiation of aggressive chemotherapy. Other solid tumors that can cause tumor lysis syndrome are hepatoblastoma or neuroblastoma. [rx][rx]There are reports of tumor lysis syndrome occurring spontaneously before the initiation of chemotherapy.
An international panel of experts has stratified tumors based on the risk of developing tumor lysis syndrome.
High-Risk Tumors
Advanced Burkitt lymphoma
Advanced leukemia
Early-stage Burkitt lymphoma or leukemia with elevated lactate dehydrogenase
Acute lymphocytic leukemia with WBC count greater than 100,000/microliters, or if the baseline increase of lactate dehydrogenase is twice the upper limit of normal
Diffuse large B-cell lymphoma and bulky disease with an elevated baseline lactate dehydrogenase of twice the upper limit of normal
Acute myeloid leukemia with WBC count greater than or equal to 10,000/microliters
Intermediate-Risk Tumors
Acute myeloid leukemia with WBC count between 25,000 and 100,000/microliters
Acute lymphocytic leukemia with WBC less than 100,000/microL and lactate dehydrogenase of less than twice the upper limit of normal
Diffuse large B-cell lymphoma with a baseline increase in lactate dehydrogenase of twice ULN but the non-bulky disease
Early-stage Burkitt lymphoma or leukemia with a lactate dehydrogenase of less than twice the upper limit of normal
Low-Risk Tumors
Solid cancers
Multiple myelomas
Indolent lymphomas
Chronic lymphocytic leukemia
Chronic myeloid leukemia
Acute myelogenous leukemia with a WBC count less than 25,000/microliters and a lactate dehydrogenase elevated to less than twice the upper limit of normal
There are case reports of tumor lysis syndrome associated with the administration of steroids, biological immunomodulators, and monoclonal antibodies. Agents are associated with the development of tumor lysis syndrome include:
Thalidomide
Bortezomib
Hydroxyurea
Paclitaxel
Fludarabine
Etoposide
Zoledronic acid
In rare instances, tumor lysis syndrome has been observed in patients under general anesthesia undergoing surgery. Other rare occurrences of tumor lysis syndrome are seen in pregnancy or high fever.
High-Risk Tumors
Acute lymphocytic leukemia (5.2% to 23%)
Acute myeloid leukemia with a WBC count greater than 75,000 (18 %)
B-cell acute lymphoblastic leukemia (26.4%)
Burkitt lymphoma (14.9%)
Intermediate-Risk Tumors
Acute myeloid leukemia with WBC count between 25,000 and 50,000 (6%)
Diffuse large B-cell lymphoma (6%)
Low-risk Tumors
Acute myeloid leukemia with WBC count less than 25,000 (1%)
Chronic lymphocytic leukemia (0.33%)
Chronic myelogenous leukemia (Case reports)
A solid tumor (Case reports)
Tumor lysis syndrome is most commonly associated with the initiation of cytotoxic chemotherapy. However, there are case reports of tumor lysis syndrome precipitated by radiation therapy, including the use of thalidomide, dexamethasone therapy, and the use of newer chemotherapeutic agents like rituximab and bortezomib.
[stextbox id=’custom’]
Risk Factors for Tumor Lysis Syndrome.
Category of Risk Factor
Risk Factor
Comments
Cancer mass
Bulky tumor or extensive metastasis
The larger the cancer mass or the higher the number of cells that will lyse with treatment, the higher the risk of clinical tumor lysis syndrome.
Organ infiltration by cancer cells
Hepatomegaly, splenomegaly, and nephromegaly generally represent tumor infiltration into these organs, and therefore a larger tumor burden than that of patients without these findings.
Bone marrow involvement
Healthy adults have 1.4 kg of bone marrow. A marrow that has been replaced by leukemic cells contains a cancer mass greater than 1 kg and therefore represents bulky disease.
Renal infiltration or outflow-tract obstruction
Cancers that infiltrate the kidney or obstruct urine flow predispose to nephropathy from other causes, such as the tumor lysis syndrome.
Cell lysis potential
The high rate of proliferation of cancer cells
Lactate dehydrogenase level is a surrogate for tumor proliferation. The higher the level, the greater the risk of the tumor lysis syndrome.
Cancer-cell sensitivity to anticancer therapy
Cancers that are inherently more sensitive to therapy have a higher rate of cell lysis and a greater risk of tumor lysis syndrome than the other cancers.
The intensity of initial anticancer therapy
The higher the intensity of initial therapy, the greater the rate of cancer-cell lysis and the risk of the tumor lysis syndrome. For example, some protocols for acute lymphoblastic leukemia begin with a week of prednisone monotherapy, and others begin with a combination of a glucocorticoid, vincristine, asparaginase, and daunorubicin. A patient treated on the latter protocol would have a higher risk of tumor lysis syndrome.
Features on patient presentation
Nephropathy before a diagnosis of cancer
A patient with preexisting nephropathy from hypertension, diabetes, gout, or other causes has a greater risk for acute kidney injury and the tumor lysis syndrome.
Dehydration or volume depletion
Dehydration decreases the rate of urine flow through renal tubules and increases the level of solutes (e.g., phosphorus, uric acid) that can crystallize and cause nephropathy.
Acidic urine
Uric acid has a lower solubility in acidic urine and therefore crystallizes more rapidly. A patient who presents with acidic urine and hyperuricemia usually already has uric acid crystals or microcrystals in the renal tubules.
Hypotension
Hypotension decreases urine flow and increases the level of solutes that can crystallize. Hypotension can also independently cause acute kidney injury.
Exposure to nephrotoxins
Vancomycin, aminoglycosides, contrast agents for diagnostic imaging and other potential nephrotoxins increase the risk of acute kidney injury from the lysis of cancer cells.
Supportive care
Inadequate hydration
Initial boluses of normal saline until the patient is euvolemic followed by infusion of suitable intravenous fluids at two times the maintenance rate (about 180 ml/hr in an adult who can tolerate hyperhydration) increases the rate of urine flow through renal tubules, decreases the level of solutes that can crystallize and cause acute kidney injury, and decreases the time that those solutes remain in the tubules so that even if microcrystals form they may not have time to aggregate into clinically important crystals before removal by the high flow of urine.
Exogenous potassium
Unless the patient has severe hypokalemia or dysrhythmia from hypokalemia, potassium should not be included in the intravenous fluids, and potassium (from food or medications) should be minimized until the risk period for the tumor lysis syndrome has passed.
Exogenous phosphate
Restricting dietary phosphate and adding a phosphate binder reduce the exogenous load of phosphate so that the kidneys need only excrete the endogenous load of phosphate released by cancer-cell lysis.
Delayed uric acid removal
Allopurinol prevents the formation of new uric acid by inhibiting xanthine oxidase and preventing the conversion of xanthine to uric acid. It does not remove existing uric acid and does increase urinary excretion of xanthine, which can crystallize and cause nephropathy. Rasburicase is an enzyme that rapidly removes uric acid by converting it to allantoin, which is highly soluble and readily excreted in the urine. The longer the uric acid level remains high, the greater the risk of crystal formation and acute kidney injury.
[/stextbox]
Symptoms of Tumor Lysis Syndrome
Hyperkalemia – Potassium is mainly an intracellular ion. High turnover of tumor cells leads to a spill of potassium into the blood. Symptoms usually do not manifest until levels are high (> 7 mmol/L) [normal 3.5–5.0 mmol/L] and they include
cardiac conduction abnormalities (can be fatal)
severe muscle weakness or paralysis
Hyperphosphatemia – Like potassium, phosphates are also predominantly intracellular. Hyperphosphatemia causes acute kidney failure in tumor lysis syndrome, because of deposition of calcium phosphate crystals in the kidney parenchyma.
Hypocalcemia – Because of the hyperphosphatemia, calcium is precipitated to form calcium phosphate, leading to hypocalcemia. Symptoms of hypocalcemia include (but are not limited to):
Tetany
Sudden mental incapacity, including emotional lability
Parkinsonian (extrapyramidal) movement disorders
Papilledema
Myopathy
Hyperuricemia[rx] and hyperuricosuria. Massive cell death and nuclear breakdown generate large quantities of nucleic acids. Of these, the purines (adenine and guanine) are converted to uric acid via the purine degradation pathway and excreted in the urine. However, at the high concentrations of uric acid generated by tumor lysis, uric acid is apt to precipitate as monosodium urate crystals.
Acute uric acid nephropathy (AUAN) – due to hyperuricosuria has been a dominant cause of acute kidney failure but with the advent of effective treatments for hyperuricosuria, AUAN has become a less common cause than hyperphosphatemia. Two common conditions related to excess uric acid, gout and uric acid nephrolithiasis, are not features of tumor lysis syndrome.
Pretreatment spontaneous tumor lysis syndrome. This entity is associated with acute kidney failure due to uric acid nephropathy prior to the institution of chemotherapy and is largely associated with lymphoma and leukemia. The important distinction between this syndrome and the post-chemotherapy syndrome is that spontaneous TLS is not associated with hyperphosphatemia.
One suggestion for the reason for this is that the high cell turnover rate leads to high uric acid levels through nucleobase turnover but the tumor reuses the released phosphate for the growth of new tumor cells. In post-chemotherapy TLS, tumor cells are destroyed and no new tumor cells are being synthesized
TLS is most common during cytotoxic treatment of hematologic neoplasms.[rx]
Dark urine reduced urine output or flank pain
Lack of appetite and fatigue
Numbness, seizures, or hallucinations
Muscle cramps and spasms
Heart palpitations symptoms are generally nonspecific and can include:
Kidney failure and death can occur, especially if TLS is left untreated.
TLS is diagnosed based on blood tests, along with signs and symptoms. Its onset may be subtle, with only a few abnormal laboratory values, but it can also present with frank kidney and organ failure.
Nausea with or without vomiting
Diagnosis of Tumor Lysis Syndrome
[stextbox id=’warning’]
Cairo-Bishop grading of clinical tumor lysis syndrome for adults
Variable
Grade 0
Grade I
Grade II
Grade III
Grade IV
GradeV
Creatinine
None
1.5 times ULN. The rise in creatinine is not attributable to the chemotherapeutic agent(s)
> 1.5-3.0 times ULN. The rise in creatinine is not attributable to the chemotherapeutic agent(s)
> 3.0-6.0 times ULN. The rise in creatinine is not attributable to the chemotherapeutic agent(s)
> 6.0 times ULN. The rise in creatinine is not attributable to the chemotherapeutic agent(s)
Death
Cardiac arrhythmia
None
Intervention not indicated
Nonurgent medical intervention indicated. Cardiac arrhythmias not attributable to the chemotherapeutic agent(s)
Symptomatic and incompletely controlled medically or controlled with a device (e.g., defibrillator). Cardiac arrhythmias not attributable to the chemotherapeutic agent(s)
Life-threatening (e.g., arrhythmia associated with HF, hypotension, syncope, shock). Cardiac arrhythmias not attributable to the chemotherapeutic agent(s)
Death
Seizures
None
–
One brief, generalized seizure; seizure(s) well controlled by anticonvulsants or infrequent focal motor seizures not interfering with ADL
Seizure in which consciousness is altered; poorly controlled seizure disorder; with breakthrough generalized seizures despite medical intervention
Seizure of any kind which is prolonged, repetitive or difficult to control (e.g., status epilepticus, intractable epilepsy)
TLS should be suspected in patients with large tumor burden who develop acute kidney failure along with hyperuricemia (> 15 mg/dL) or hyperphosphatemia (> 8 mg/dL). (Most other acute kidney failure occurs with uric acid < 12 mg/dL and phosphate < 6 mg/dL). Acute uric acid nephropathy is associated with little or no urine output. The urinalysis may show uric acid crystals or amorphous urates. The hypersecretion of uric acid can be detected with a high urine uric acid – creatinine ratio > 1.0, compared to a value of 0.6–0.7 for most other causes of acute kidney failure.
[/stextbox]
Cairo-Bishop definition
In 2004, Cairo and Bishop defined a classification system for tumor lysis syndrome.[rx]
Laboratory tumor lysis syndrome: abnormality in two or more of the following, occurring within three days before or seven days after chemotherapy.
uric acid > 8 mg/dL or 25% increase
potassium > 6 meq/L or 25% increase
phosphate > 4.5 mg/dL or 25% increase
calcium < 7 mg/dL or 25% decrease
Clinical tumor lysis syndrome: laboratory tumor lysis syndrome plus one or more of the following:
increased serum creatinine (1.5 times upper limit of normal)
cardiac arrhythmia or sudden death
seizure
A grading scale (0–5) is used depending on the presence of lab TLS, serum creatinine, arrhythmias, or seizures.
Howard definition
In 2011, Howard proposed a refinement of the standard Cairo-Bishop definition of TLS accounting for 2 limitations:[11]
Two or more electrolyte laboratory abnormalities must be present simultaneously to be considered related to TLS. In fact, some patients may present with one abnormality, but later another one may develop that is unrelated to the TLS (e.g., hypocalcemia associated with sepsis).
A 25% change from baseline should not be considered a criterion since such increases are rarely clinically important unless the value is already outside the normal range.
Moreover, any symptomatic hypocalcemia should constitute clinical TLS.
History
The history and physical examination of patients with tumor lysis syndrome should be focused on the primary causes of the tumor lysis.
Time of onset of malignancy should be elicited with attention to the presence of constitutional symptoms like weight loss or anorexia. Presence of respiratory symptoms dyspnea, orthopnea, and tachypnea can be a sign of airway compression from a primary tumor.
Urinary symptoms such as dysuria, flank pain, and hematuria
Signs and symptoms that can be associated with hypocalcemia include nausea, vomiting, seizure, tetanic spasm, and change in mental status.
Other clinical manifestations of tumor lysis syndrome include, but are not limited to, syncopal attack, palpitation lethargy, pitting edema, facial edema, abdominal distention, and other sign of fluid overload.
Physical Examination
The physical examination should focus on the electrolyte abnormalities that are associated with tumor lysis syndrome. The physical findings associated with these abnormalities are listed below.
Muffled heart sound from pericarditis secondary to uremia
Joint pain
Renal colicky pain
Calcium phosphate crystal deposits in the skin
Pruritis
Gangrene
The signs and symptoms of tumor lysis syndrome can develop spontaneously or about 72 hours after the initiation of chemotherapy.
Evaluation
Tumor lysis syndrome is diagnosed based on criteria that were developed by Cairo and Bishop.[rx][rx] The criteria established by Cairo and Bishop have several limitations. The most crucial drawback is that the definition of tumor lysis syndrome based on this criterion requires the initiation of chemotherapy.
However, in clinical practice, tumor lysis syndrome can develop spontaneously without the initiation of chemotherapy. The second limitation is the use of creatinine level greater than 1.5 the upper limit for age and gender.
This is not standard as a patient with CKD (Chronic Kidney Disease) will have elevated creatine in the absence of AKI. The Cairo-Bishop criteria also factor the severity of tumor lysis syndrome based on the severity of illness from grade 0 (asymptomatic) to 4 (death).
Laboratory Diagnosis of Tumor Lysis Syndrome
Requires 2 or more of the following criteria achieved in the same 24-hour period from 3 days before to 7 days after chemotherapy initiation:
Uric acid 25% increase from baseline or greater than or equal to 8.0 mg/dL
Potassium 25% increase from baseline or greater than or equal to 6.0 mEq/L
Phosphorus 25% increase from baseline or greater than or equal to 0.5 mg/dL (greater than or equal to 6.5 mg/dL in children)
Calcium 25% decrease from baseline or less than or equal to 7.0 mg/dL
Clinical Diagnosis of Tumor Lysis Syndrome
Laboratory tumor lysis syndrome plus 1 or more of the following:
Creatinine greater than 1.5 times the upper limit of normal of an age-adjusted reference range
Seizure
Cardiac arrhythmia or sudden death
Other origins of AKI should be excluded. In the evaluation of tumor lysis syndrome, the following studies are necessary:
Imaging
X-Ray and CT scan of the chest to evaluate the presence of mediastinal mass and the presence of a concomitant pleural effusion
CT scan and an ultrasound of the abdomen and retroperitoneal structure if the mass lesion is located in the abdomen or retroperitoneum. Care must be taken with intravenous (IV) contrast because of the presence of AKI in tumor lysis syndrome.
Electrocardiography (ECG)
ECG is part of the workup for patients with tumor lysis syndrome to check for findings associated with hyperkalemia and hypocalcemia. Hyperkalemia is a potential cause of fatal arrhythmia in tumor lysis syndrome.
Complete Blood Count (CBC)
CBC helps in the diagnosis of malignancy associated with tumor lysis syndrome. The hallmark of most malignancy is leukocytosis with anemia and thrombocytopenia.
Comprehensive Metabolic Panel (CMP)
The metabolic derangement associated with tumor lysis syndrome is hyperkalemia, hypocalcemia, hyperphosphatemia, and hyperuricemia. Blood urea nitrogen (BUN), creatinine, and lactate dehydrogenase are also elevated in tumor lysis syndrome. CMP must be monitored between two to three times daily before and after initiation of therapy. Elevated laboratory value might be indicative of the beginning of tumor lysis syndrome.
Urine Analysis
Precipitation of uric acid salt can cause obstructive uropathy. In the treatment of tumor lysis syndrome, Alkalinisation of urine with sodium bicarbonate is the standard of care. Frequent urine analysis with an assessment of urine pH, specific gravity and output are mandatory.
Differential Diagnosis
Tumor lysis syndrome should be differentiated from other clinical conditions that can cause
Hyperkalemia
Hyperphosphatemia
Hyperuricemia
The differential diagnosis of each electrolyte abnormalities are listed below:
Hyperkalemia
Hypocalcemia
Metabolic acidosis
Congenital adrenal hyperplasia
Toxicity from digitalis
Acute tubular necrosis
Electrical burn
Head trauma
Rhabdomyolysis
Thermal burns
Hyperphosphatemia
Monoclonal gammopathy
Waldenstrom macroglobulinemia
Multiple Myeloma
Other differentials to be considered in hyperphosphatemia include:
Pseudohypoparathyroidism
Rhabdomyolysis
Vitamin D intoxication
Oral saline laxative (Phospho-soda) abuse
Pseudohyperphosphatemia
Hyperuricemia
Hyperparathyroidism
Hypothyroidism
Nephrolithiasis
Alcoholic ketoacidosis
Diabetic ketoacidosis
Gout
Pseudogout
Type 1 a glycogen storage disease
Hemolytic anemia
Hodgkins lymphoma
Uric acid nephropathy
Treatment of Tumor Lysis Syndrome
Electrolytes imbalances
Hyperkalemia – Intravenous calcium gluconate may be given to stabilize cardiac membranes for severe hyperkalemia or for electrocardiogram changes. For temporary serum reductions in potassium levels, intravenous insulin with dextrose or a high dose of inhaled beta-agonists may be used. Oral sodium polystyrene resin, i.e. kayexalate, is recommended for definitive treatment of hyperkalemia. If these measures are insufficient or for severe metabolic derangements, renal replacement therapy should be considered with the consultation of nephrology.
Hyperphosphatemia – Aggressive intravenous fluid resuscitation with the maintenance of high urine output and oral phosphate binders such as sevelamer may be sufficient to improve phosphate levels. Hemodialysis may be required for severe hyperphosphatemia not controlled by these methods.
Hypocalcemia – Hypocalcemia will correct without specific intervention as phosphate levels normalize. With the exception of severe symptomatic hypocalcemia, intravenous calcium gluconate can be considered, however, it is otherwise not recommended due to elevated risk of calcium-phosphate precipitation.
Rapid Expansion of Intravascular Volume
Treatment of tumor lysis syndrome starts with rapid volume expansion. It is recommended to use crystalloids in volume expansion as this will help to increase the glomerular filtration rate (GFR) quickly. Improved GFR helps with the excretion of solutes associated with tumor lysis syndrome. The drawback to this is that the kidney functions should still be intact. Intravenous fluid should be initiated 48 hours before the start of chemotherapy and should be continued for 48 hours after chemotherapy. Hydration with about 3 to 3.5 liters/m2 per day or 4 to 5 liters per day might be needed to provide adequate hydration. This will provide a urine output of about 3 liters per day[rx][rx][rx]
Medications
Allopurinol
This is a structural isomer of hypoxanthine. Xanthine oxidase converts allopurinol to oxypurinol. This is the active metabolite, and it is excreted primarily by the kidney. CKD or AKI impair the elimination of oxypurinol. The level of xanthine in the urine and serum can be elevated after the administration of allopurinol because of the inhibition of the conversion of xanthine to uric acid. Xanthine by itself has limited solubility and can crystallize in the renal tubules making the obstructive uropathy associated with tumor lysis syndrome worse.
Allopurinol can decrease the production of uric acid in tumor lysis syndrome but is ineffective in the treatment of hyperuricemia associated with tumor lysis syndrome. Allopurinol is a very useful agent to prevent the development of tumor lysis syndrome.
The use of allopurinol is associated with the development of skin rash, eosinophilia, and acute hepatitis. The combination of these symptoms is called allopurinol hypersensitivity syndrome. In the treatment of tumor lysis syndrome, clinicians should be aware of a potential drug to drug interaction with azathioprine, immunosuppressive drug use in patients with solid organ transplant and autoimmune disorder.
Recombinant Urate Oxidase
A recombinant version of urate oxidase is a drug that is used to treat hyperuricemia in patients with leukemia, lymphoma, and solid tumor who are undergoing chemotherapy.
It is derived from Aspergillus by recombinant technology. The drug’s mechanism of action is the catalyzes of uric acid to allantoin, carbon dioxide, and hydrogen peroxide.
Hydrogen peroxide is a potent oxidizing agent and can cause severe methemoglobinemia or hemolytic anemia in patients with glucose 6 phosphate dehydrogenase G6PD deficiency. The Food and Drug Administration approved recombinant urate oxidase in 2009 This medication can be administered intramuscularly. It can also be given intravenously at doses of between 50 to 100 U/kg per day.
Sodium Bicarbonate for Urine Alkalinisation
The normal urine is acidic with a pH of about 5. The solubility of uric acid in urine is increased about 10-fold with the alkalinization of urine. This can be achieved by adding about 40 to 50 mEq/liter of sodium bicarbonate to the fluid use for hydration in tumor lysis syndrome.
The risk of alkalinization of the urine is a decrease in the level of ionized calcium as there is less bonding of calcium to albumin. This can worsen the hypocalcemia associated with tumor lysis syndrome leading o arrhythmia or tetany. That apart, the alkalinization of urine can favor the precipitation of calcium and phosphate salts in the kidney tubules thus making AKI in tumor lysis syndrome worse.
Therefore, alkalinization of urine with sodium bicarbonate is only advisable if rasburicase is not readily available. Even with that, the level of calcium should be serially monitored.
Calcium
Calcium chloride and calcium gluconate can be administered parenterally to treat hypocalcemia. In tumor lysis syndrome hypocalcemia is secondary to hyperphosphatemia; therefore, administration of calcium can potentiate the deposition of calcium phosphate crystals in soft tissues and the kidney making AKI worse. This might sometimes necessitate the use of hemodialysis.
Hemodialysis
This is an option that is available to use in a dire situation if the level of potassium and phosphorus is too high in the face of tumor lysis syndrome associated AKI. In tumor lysis syndrome, there is an ongoing liberation of intracellular ions. If intermittent hemodialysis is utilized for extracorporeal clearance, rebound hyperkalemia or hyperphosphatemia might develop. Because of this, continuous renal replacement therapy is the best modality for solute removal. This is done with a high flow rate for the dialysate or replacement fluid*-+. For life-threatening hyperkalemia, early hemodialysis is recommended. For severe hyperphosphatemcnvmb, is, continuous renal replacement therapy might also be the best treatment modality.
Febuxostat
This medication is also a xanthine oxidase inhibitor that is relatively new to the market. It is more expensive than allopurinol. It does not cause the hypersensitivity reaction that is associated with allopurinol.
In the clinical trial, the Febuxostat for Tumor Lysis Syndrome Prevention in Hematologic Malignancies (FLORENCE), febuxostat provides better control of hyperuricemia of tumor lysis syndrome with a good safety profile and preservation of renal functions.
Alkalinization of urine
Alkalinization of urine was historically recommended in the management of TLS due to the possibility that it may increase the solubility of uric acid in urine. However, recent increasing evidence suggests that urine alkalinization is associated with increased precipitation of calcium phosphate in the renal tubules, particularly in patients with hyperphosphatemia. Therefore, alkalinization of the urine is not recommended in TLS prophylaxis and therapy anymore.[rx]
Allopurinol
Allopurinol is available as oral and intravenous formulations and prevents the conversion of hypoxanthine to xanthine and xanthine to uric acid. The renal clearance of hypoxanthine and xanthine are ten times higher than that of uric acid. Allopurinol has several drug-drug interactions, especially with 6-mercaptopurine, thiazide diuretics, azathioprine, cyclosporine, cyclophosphamide, and amoxicillin. It is necessary to adjust the dose or monitor serum levels of these drugs. The drug should be discontinued in case of skin rash due to the possibility of severe hypersensitivity reactions. Indeed, the dose of allopurinol needs to be adjusted in case of renal insufficiency.
Rasburicase
In most mammals, but not in humans, uric acid is oxidized to allantoin using the enzyme urate oxidase. In humans, uric acid is the end product of purine metabolism. Allantoin is ten times more soluble than uric acid and is easily excreted in the urine.[rx] Obtained from Aspergillus flavus, a nonrecombinant urate oxidase has been available since 1968.
Hyperkalemia may cause serious cardiac arrhythmias; therefore, potassium should be withheld from hydration fluid. Patients with potassium levels ≥6 mmol/L should be closely monitored and immediate measures should be taken (infusion of calcium gluconate, therapy with β-adrenergic agonists, and intravenous infusion of insulin and glucose).
Treating hyperphosphatemia is difficult, especially if accompanied by AKI. Oral phosphate binders are less effective, and their oral administration could be difficult in these patients. Significant hyperphosphatemia is treated best with renal replacement therapy.
Renal replacement therapy in TLS should be considered for patients with persistent hyperkalemia despite adequate therapy, severe acidosis, and volume overload unresponsive to diuretic therapy.
Volume Expansion
Once TLS has developed, efforts should be made to re-establish normal concentrations of extracellular solutes. Provided that there has not been a complete loss of kidney function, volume expansion, with a goal of increasing kidney excretion of these solutes, is the bedrock of TLS therapy.[rx,rx]
In addition to augmenting potassium, phosphate, and uric acid excretion, a robust urine flow rate will decrease the calcium-phosphate product in the renal tubules, decreasing the risk of crystal formation and micro-obstruction. As we discuss above, we agree with current consensus statements suggesting a target fluid intake of 3 L per day, barring contraindications.
Diuretics
Although the use of diuretics to enhance urinary flow rate may be expected to decrease the risk of tubular calcium-phosphate precipitation, this practice has not been studied. Furthermore, the hemodynamic changes associated with diuretic use may further compromise kidney function in this population.[rx] Barring clinically important volume overload, we do not routinely use diuretics in the care of patients with TLS.
[stextbox id=’grey’]
Recommendations for the prevention and treatment of tumor lysis syndrome
Low-risk disease
Intermediate-risk disease
High-risk disease
Diagnostic measures
• No specific measures
• Daily monitoring of laboratory abnormalities before and during the first 7 days of anticancer therapy
• At least twice daily monitoring of laboratory abnormalities before and during the first 7 days of anticancer therapy
Preventive measures
• Moderate hydration is recommended
• Vigorous hydration
• Keep urinary output >100 mL/h
• Treatment with allopurinol or febuxostat should be started at least 24 hours before initiation of anticancer therapy and should be continued till normalization of uric acid levels and signs of large tumor burden are absent
• Vigorous hydration
• Keep urinary output >100 mL/h
• Single-dose 6 mg of rasburicase. Repeat doses as necessary. In the case of contraindication treatment with febuxostat
Treatment of established tumor lysis syndrome
• Admission to intensive care unit with continuous cardiac monitoring and monitoring of laboratory abnormalities every 4–6 hours
• Early nephrology consultation to estimate the indications for renal replacement therapy
What Are The Benefits of Devil’s Claw/Harpagophytum also called grapple plant, wood spider and most commonly devil’s claw is a genus of plants in the sesame family, native to southern Africa. Plants of the genus owe their common name “devil’s claw” to the peculiar appearance of their hooked fruit. Several species of North American plants in genus Proboscidea and certain species of Pisonia are however also known by this name. Devil’s claw’s tuberous roots are used in folk medicine to reduce pain.
Devil’s Claw, is a genus of tuberiferous xerophytic plants native to southern Africa. Some of the taxa are appreciated for their medicinal effects and have been traditionally used to relieve symptoms of inflammation. The objectives of this pilot study were to investigate the antioxidant capacity and the content of total phenols, verbascoside, is verbascoside, and selected iridoids, as well as to investigate the capacity of various Harpagophytum taxa in suppressing respiratory burst in terms of reactive oxygen species produced by human neutrophils challenged with phorbol myristate acetate (PMA), opsonisedStaphylococcus aureus, and Fusobacterium nucleatum.
Indications of Devil’s Claw
Devil’s Claw was completely ineffective in reducing edema of the rat hindfoot induced by either lambda-carrageenan or Mycobacterium butyricum. At concentrations of up to 1 x 10(5) microgram/ml, Devil’s Claw was also ineffective as an in-vitro inhibitor of prostaglandin synthetase. These results indicate that Devil’s Claw lacks the anti-inflammatory properties possessed by all antiarthritic drugs of the nonsteroidal, anti-inflammatory analgesic type.
Preparations of the plant or its extracts, such as harpagoside – [rx] are presumed to have used in folk medicine and phytotherapy as an anti-inflammatory herbal drug or dietary supplement.[rx] Although there is no accepted clinical evidence of its efficacy and bioavailability, limited effects were noted for treating lower back pain and osteoarthritis.[rx] A Cochrane review of clinical research noted that devil’s claw seems to reduce low back pain more than placebo, although evidence was of moderate quality at best.[rx]
Back pain – Taking devil’s claw by mouth seems to reduce low-back pain. Devil’s claw seems to work about as well as some non-steroidal anti-inflammatory drugs (NSAIDs).
Osteoarthritis – Taking devil’s claw alone or along with nonsteroidal anti-inflammatory drugs (NSAIDs) seems to help decrease osteoarthritis-related pain. Some evidence suggests that devil’s claw works about as well as diacerein (a slow-acting drug for osteoarthritis that is not available in the U.S.) for improving osteoarthritis pain in the hip and knee after 16 weeks of treatment. Some people taking devil’s claw seem to be able to lower the dose of NSAIDs they need for pain relief.
Rheumatoid arthritis (RA) – Early research suggests that taking devil’s claw extract by mouth might not improve RA.
Do not use with antiarrhythmic, chronotropic, or inotropic medicines. Because of the bitterness of the preparation and consequent increase in gastric secretion, devil’s claw is contraindicated in patients with gastric or duodenal ulcers.
Pregnancy/Lactation
Documented oxytocic adverse effects. Avoid use.
Dosage of Devil’s Claw
The following doses have been studied in scientific research:
For osteoarthritis – 2-2.6 grams of devil’s claw extract has been taken in up to three divided doses daily for up to 4 months. A specific combination product providing 600 mg of devil’s claw, 400 mg of turmeric, and 300 mg of bromelain has been taken 2-3 three times daily for up to 2 months.
For back pain – 0.6-2.4 grams of devil’s claw extract has been taken daily, usually in divided doses, for up to 1 year.
Side Effects and Interactions of Devil’s Claw
Devil’s claw appears to be safe when taken in doses up to 2,610 mg daily, though long-term effects have not been investigated [rx].
Reported side effects are mild, the most common being diarrhea. Rarer adverse effects include allergic reactions, headache and coughing (30Trusted Source).
Heart problems, high blood pressure, low blood pressure – Since devil’s claw can affect heart rate, heartbeat, and blood pressure, it might harm people with disorders of the heart and circulatory system. If you have one of these conditions, talk with your healthcare provider before starting devil’s claw.
Heart disorders – Studies have indicated that devil’s claw can affect heart rate, heartbeat and blood pressure.
Diabetes – Devil’s claw may reduce blood sugar levels and intensify the effects of diabetes medications.
Gallstones – Use of devil’s claw may increase the formation of bile and make problems worse for those with gallstones.
Stomach ulcers – Production of acid in the stomach can increase with the use of devil’s claw, which may aggravate peptic ulcers.
NSAIDs – Devil’s claw may slow the absorption of popular NSAIDs, such as Motrin, Celebrex, Feldene and Voltaren.
Blood thinners – Devil’s claw may enhance the effects of Coumadin (also known as warfarin), which may lead to increased bleeding and bruising.
Stomach acid reducers – Devil’s claw may decrease the effects of stomach acid reducers, such as Pepcid, Zantac, Prilosec, and Prevacid.
This is not an all-inclusive list of medication interactions. To be on the safe side, always discuss your use of supplements with your doctor.
What Are The Advantages of Taking Vitamin B Complex/B vitamins are a class of water-soluble vitamins that play important roles in cell metabolism? Though these vitamins share similar names, they are chemically distinct compounds which often coexist in the same foods. In general, dietary supplements containing all eight are referred to as a vitamin B complex. Individual B vitamin supplements are referred to by the specific number or name of each vitamin. Individual B vitamin supplements are referred to by the specific number or name of each vitamin – B1 = thiamine, B2 = riboflavin, B3 = niacin, etc. Some are better known by name than number niacin, pantothenic acid, biotin, and folate.
The recommended daily amount of each Vitamin B Complex/B vitamins
[stextbox id=’info’]
For women and men, the recommended daily intake (RDI) for B vitamins are as follows
Women
Men
B1 (Thiamine)
1.1 mg
1.2 mg
B2 (Riboflavin)
1.1 mg
1.3 mg
B3 (Niacin)
14 mg
16 mg
B5 (Pantothenic acid)
5 mg (RDI not established; Adequate Intake, or AI, provided)
5 mg (AI)
B6 (Pyridoxine)
1.3 mg
1.3 mg
B7 (Biotin)
30 mcg (AI)
30 mcg (AI)
B9 (Folate)
400 mcg
400 mcg
B12 (Cobalamin)
2.4 mcg
2.4 mcg
Older adults and women who are pregnant require higher amounts of B vitamins. Your doctor can provide dosage information tailored to your individual needs.
[/stextbox]
Types of Vitamin B Complex/B vitamins
Thiamine (Vitamin B1)
Thiamine is a coenzyme in the pentose phosphate pathway, which is a necessary step in the synthesis of fatty acids, steroids, nucleic acids and the aromatic amino acid precursors to a range of neurotransmitters and other bioactive compounds essential for brain function [rx].
Thiamine plays a neuro-modulatory role in the acetylcholine neurotransmitter system, distinct from its actions as a cofactor during metabolic processes [rx] and contributes to the structure and function of cellular membranes, including neurons and neuroglia [35].
Riboflavin (Vitamin B2)
The two flavoprotein coenzymes derived from riboflavin, FMN and FAD are crucial rates limiting factors in most cellular enzymatic processes. As an example, they are crucial for the synthesis, conversion, and recycling of niacin, folate and vitamin B6, and for the synthesis of all heme proteins, including hemoglobin, nitric oxide synthases, P450 enzymes, and proteins involved in electron transfer and oxygen transport and storage [rx].
The flavoproteins are also co-factors in the metabolism of essential fatty acids in brain lipids [rx], the absorption and utilization of iron [rx], and the regulation of thyroid hormones [rx].
Dysregulation of any of these processes by riboflavin deficiency would be associated with its own broad negative consequences for brain function. Riboflavin derivatives also have direct antioxidant properties and increase endogenous antioxidant status as essential cofactors in the glutathione redox cycle [rx].
Niacin (Vitamin B3)
A vast array of processes and enzymes involved in every aspect of peripheral and brain cell function are dependent on niacin derived nucleotides such as nicotinamide adenine dinucleotide (NAD) and NAD phosphate (NADP). Beyond energy production, these include oxidative reactions, antioxidant protection, DNA metabolism and repair, cellular signaling events (via intracellular calcium), and the conversion of folate to its tetrahydrofolate derivative [rx].
Niacin also binds agonistically at two G protein receptors, the high-affinity Niacin receptor 1 (NIACR1), responsible for the skin flush associated with high intake of niacin, and the low-affinity NIACR2. Niacin receptors are distributed both peripherally in immune cells and adipose tissue, and throughout the brain. Currently established roles include modulation of inflammatory cascades [rx,rx] and anti-atherogenic lipolysis in adipose tissue [rx,rx].
NIACR1 receptor populations have been shown to be down-regulated in the anterior cingulate cortex of schizophrenia sufferers [rx] and upregulated in the substantia nigra of Parkinson’s disease sufferers, (a group that have low niacin levels generally) with levels correlating with poorer sleep architecture in this group [rx]. A recent case study demonstrated that 250 mg niacin administration modulated peripheral immune cell NIACR1 expression and attenuated the disturbed sleep architecture associated with Parkinson’s disease [rx].
Pantothenic Acid (Vitamin B5)
This vitamin is a substrate for the synthesis of the ubiquitous coenzyme A (CoA). Beyond its role in oxidative metabolism, CoA contributes to the structure and function of brain cells via its involvement in the synthesis of cholesterol, amino acids, phospholipids, and fatty acids. Of particular relevance, pantothenic acid, via CoA, is also involved in the synthesis of multiple neurotransmitters and steroid hormones [rx].
Vitamin B6 (Pyridoxine, Pyridoxal, Pyridoxamine)
Beyond its role as a necessary cofactor in the folate cycle (see above and folate section below), the role of vitamin B6 in amino acid metabolism makes it a rate-limiting cofactor in the synthesis of neurotransmitters such as dopamine, serotonin, γ-aminobutyric acid (GABA), noradrenaline and the hormone melatonin.
The synthesis of these neurotransmitters is differentially sensitive to vitamin B6 levels, with even mild deficiency resulting in preferential down-regulation of GABA and serotonin synthesis, leading to the removal of inhibition of neural activity by GABA and disordered sleep, behavior, and cardiovascular function and a loss of hypothalamus-pituitary control of hormone excretion.
Vitamin B6 also has a direct effect on immune function and gene transcription/expression [rx] and plays a role in brain glucose regulation [rx].
More broadly, levels of pyridoxal-5′-phosphate are associated with increased functional indices and biomarkers of inflammation, and levels of pyridoxal-5′-phosphate are down-regulated as a function of more severe inflammation [rx,rx], potentially as a consequence of pyridoxal-5′-phosphate’s role either in the metabolism of tryptophan or in one-carbon metabolism [rx]. This role is particularly pertinent as inflammatory processes contribute to the etiology of numerous pathological states including dementia and cognitive decline [rx].
Biotin (Vitamin B7)
The brain is particularly sensitive to the delivery and metabolism of glucose. Biotin plays a key role in glucose metabolism and hemostasis, including regulation of hepatic glucose uptake, gluconeogenesis (and lipogenesis), insulin receptor transcription and pancreatic β-cell function [rx].
Frank deficiency in biotin is rarely reported, although lower circulating levels of biotin have been reported in those suffering glucoregulatory dysfunction, for instance, Type II diabetes, alongside an inverse relationship between fasting plasma glucose and biotin levels [rx].
Folate (Vitamin B9) and Vitamin B12 (Cobalamin)
The functions of these two vitamins are inextricably linked due to their complementary roles in the “folate” and “methionine” cycles. Indeed, a deficiency in vitamin B12 results in a functional folate deficiency, as folate becomes trapped in the form of methyltetrahydrofolate [rx,rx].
An actual or functional folate deficiency, with an attendant reduction in purine/pyrimidine synthesis and genomic and non-genomic methylation reactions in brain tissue, leads to decreased DNA stability and repair and gene expression/transcription, which could hamper neuronal differentiation and repair, promote hippocampal atrophy, demyelination and compromise the integrity of membrane phospholipids impairing the propagation of action potentials [rx].
Folate related downregulation of the synthesis of proteins and the nucleotides required for DNA/RNA synthesis has ramifications for rapidly dividing tissue in particular and therefore underlies the fetal developmental disorders and megaloblastic anemia (alongside aspects of neuronal dysfunction), associated with either folate or vitamin B12 deficiency [rx,rx,rx].
The efficient functioning of the folate cycle is also necessary for the synthesis and regeneration of tetrahydrobiopterin, an essential cofactor for the enzymes that convert amino acids to both monoamine neurotransmitters (serotonin, melatonin, dopamine, noradrenaline, adrenaline), and nitric oxide [rx,rx]
Functions of Vitamin B Complex/B vitamins
[stextbox id=’info’]
Vitamin
Name
Structure
Molecular Function
Vitamin B1
thiamine
Thiamine plays a central role in the release of energy from carbohydrates. It is involved in RNA and DNA production, as well as nerve function. Its active form is a coenzyme called thiamine pyrophosphate (TPP), which takes part in the conversion of pyruvate to acetyl coenzyme A in metabolism.
Vitamin B2
riboflavin
Riboflavin is involved in release of energy in the electron transport chain, the citric acid cycle, as well as the catabolism of fatty acids (beta oxidation)..
Vitamin B3
niacin
Niacin is composed of two structures: nicotinic acid and nicotinamide. There are two co-enzyme forms of niacin: nicotinamide adenine dinucleotide (NAD) and nicotinamide adenine dinucleotide phosphate (NADP). Both play an important role in energy transfer reactions in the metabolism of glucose, fat and alcohol.NAD carries hydrogens and their electrons during metabolic reactions, including the pathway from the citric acid cycle to the electron transport chain. NADP is a coenzyme in lipid and nucleic acid synthesis.
Vitamin B5
pantothenic acid
Pantothenic acid is involved in the oxidation of fatty acids and carbohydrates. Coenzyme A, which can be synthesised from pantothenic acid, is involved in the synthesis of amino acids, fatty acids, ketone bodies, cholesterol,[5] phospholipids, steroid hormones, neurotransmitters (such as acetylcholine), and antibodies.[6]
Vitamin B6
pyridoxine, pyridoxal, pyridoxamine
The active form pyridoxal 5′-phosphate (PLP) (depicted) serves as a cofactor in many enzyme reactions mainly in amino acid metabolism including biosynthesis of neurotransmitters.
Vitamin B7
biotin
Biotin plays a key role in the metabolism of lipids, proteins and carbohydrates. It is a critical co-enzyme of four carboxylases: acetyl CoA carboxylase, which is involved in the synthesis of fatty acids from acetate; pyruvate CoA carboxylase, involved in gluconeogenesis; β-methylcrotonyl CoA carboxylase, involved in the metabolism of leucine; and propionyl CoA carboxylase, which is involved in the metabolism of energy, amino acids and cholesterol.
Vitamin B9
folate
Folate acts as a co-enzyme in the form of tetrahydrofolate (THF), which is involved in the transfer of single-carbon units in the metabolism of nucleic acids and amino acids. THF is involved in pyrimidine nucleotide synthesis, so is needed for normal cell division, especially during pregnancy and infancy, which are times of rapid growth. Folate also aids in erythropoiesis, the production of red blood cells.
Vitamin B12
cobalamin
Vitamin B12 is involved in the cellular metabolism of carbohydrates, proteins and lipids. It is essential in the production of blood cells in bone marrow, and for nerve sheaths and proteins. Vitamin B12 functions as a co-enzyme in intermediary metabolism for the methionine synthase reaction with methylcobalamin, and the methylmalonyl CoA mutase reaction with adenosylcobalamin
[/stextbox]
Deficiency Symptoms of Vitamin B Complex/B vitamins
Several named vitamin deficiency diseases may result from the lack of sufficient B vitamins. Deficiencies of other B vitamins result in symptoms that are not part of a named deficiency disease.
[stextbox id=’warning’]
Vitamin
Name
Deficiency effects
Vitamin B1
thiamine
Deficiency causes beriberi. Symptoms of this disease of the nervous system include weight loss, emotional disturbances, Wernicke encephalopathy (impaired sensory perception), weakness and pain in the limbs, periods of irregular heartbeat, and edema (swelling of bodily tissues). Heart failure and death may occur in advanced cases. Chronic thiamin deficiency can also cause alcoholic Korsakoff syndrome, irreversible dementia characterized by amnesia and compensatory confabulation.
Vitamin B2
riboflavin
Main article: Riboflavin § Deficiency
Deficiency causes ariboflavinosis. Symptoms may include cheilosis (cracks in the lips), high sensitivity to sunlight, angular cheilitis, glossitis (inflammation of the tongue), seborrheic dermatitis or pseudo-syphilis (particularly affecting the scrotum or labia majora and the mouth), pharyngitis (sore throat), hyperemia, and edema of the pharyngeal and oral mucosa.
Vitamin B3
niacin
Deficiency, along with a deficiency of tryptophan causes pellagra. Symptoms include aggression, dermatitis, insomnia, weakness, mental confusion, and diarrhea. In advanced cases, pellagra may lead to dementia and death (the 3(+1) D’s: dermatitis, diarrhea, dementia, and death).
Vitamin B5
pantothenic acid
Deficiency can result in acne and paresthesia, although it is uncommon.
Deficiency does not typically cause symptoms in adults but may lead to impaired growth and neurological disorders in infants. Multiple carboxylase deficiency, an inborn error of metabolism, can lead to biotin deficiency even when dietary biotin intake is normal.
Vitamin B9
folic acid
Deficiency results in macrocytic anemia, and elevated levels of homocysteine. Deficiency in pregnant women can lead to birth defects.
Vitamin B12
cobalamin
Deficiency results in macrocytic anemia, elevated methylmalonic acid and homocysteine, peripheral neuropathy, memory loss, and other cognitive deficits. It is most likely to occur among elderly people, as absorption through the gut declines with age; the autoimmune disease pernicious anemia is another common cause. It can also cause symptoms of mania and psychosis. In rare extreme cases, paralysis can result.
The B vitamins: nomenclature, dietary sources, coenzyme forms (roles), symptoms of deficiency, and risk factors (over and above low consumption).
Vitamin
Generally Known as
Good Dietary Sources
RDA 1(mg)
UL 2
Principal Bioactive Coenzymes (and Principal Coenzyme Role [rx])
Symptoms of Deficiency
Brain Specific Symptoms of Deficiency
Specific Risk Factors for Deficiency
B1
Thiamin(e)
Cereals (esp. whole grain), brown rice, green vegetables, potatoes, pasta, liver, pork, eggs
1.2/1.1
–
Thiamine pyrophosphate (Generation of leaving group potential)
Mild deficiency: general fatigue/weakness gastro-intestinal symptoms [rx].
Deficiency: “Beri-beri”— Peripheral nerve damage and cardiovascular dysfunction leading to: pain, impaired sensory perception; swelling, weakness and pain in the limbs; shortness of breath, irregular heart rate, heart failure [rx]
Mild deficiency: irritability, emotional disturbances, confusion, disturbed sleep, memory loss [rx].
Deficiency: Wernicke-Korsakoff syndrome (neurodegeneration, within the medial thalamus and cerebellum). Ataxia, abnormal motor function and eye movement, amnesia, apathy, confabulation [rx]
1 Recommended Daily Allowance; 2 Upper limit—Food and Nutrition Board, Institute of Medicine, USA estimated “adequate intake” due to lack of data required to arrive at an RDA; 3 more prevalent for vitamin B12 deficiency; 4more prevalent for folate deficiency.
[/stextbox]
Health Benefit of Vitamin B Complex/B vitamins
Thiamine (B1)
Vitamin B1, also known as thiamine, ensures that the body can produce new, healthy cells. It has also been reported to possess anti-stress properties, in addition to the ability to boost your immune system when it’s low. Vitamin B1 is also essential for the breakdown of simple carbohydrates.
Thiamine (Vitamin B1) Foods
Vitamin B2, also known as riboflavin, helps to get rid of particles in the body which can damage our cells. B2 has also been linked with the potential prevention of early aging, in addition to the ability to reduce your risk of heart disease.
Furthermore, B2 is essential for the production of red blood cells and hemoglobin, which is responsible for ensuring that the rest of your body’s cells receive the oxygen that they require. There have also been studies [1] that suggest that vitamin B2 can help in overcoming migraines, however, the results are not conclusive.
Riboflavin (Vitamin B2) Foods
Almonds, rice, eggs, milk, yoghurt, spinach, soy and sprouts.
Niacin (B3)
One of the main roles of vitamin B3, also known as niacin, is to increase the levels of high-density lipoproteins (HDL) in the blood. These are the ‘good cholesterol’. The higher your HDL levels are, the lower your overall cholesterol ratio is. This means you are seen as being at a lower risk of developing cardiovascular diseases (CVD).
Several studies have also shown that vitamin B3 may be able to treat skin conditions such as acne.
Niacin (Vitamin B3) Foods:
Milk, eggs, beans, green vegetables and red meat.
Pantothenic Acid (B5)
Vitamin B5, also known as pantothenic acid, can be found in many foods in small quantities. Its main responsibilities include breaking down fats and carbohydrates for energy, and the production of important hormones such as testosterone.
There have been studies [4] that show that vitamin B5 can have a positive effect on skin, reducing the signs of ageing and improving blemishes, redness and spots.
Pantothenic Acid (Vitamin B5) Foods
Eggs, meat, yogurt, beans, and legumes.
Pyridoxine (B6)
Pyridoxine, also known as vitamin B6, has several different qualities. Firstly, it works to regulate blood levels of homocysteine, which is an amino acid associated with heart disease. It also helps to body to produce hormones such as serotonin and melatonin, as well as norepinephrine. These are our sleep and stress hormones that alter mood and energy levels.
There have also been a number of studies [5] that suggest that vitamin B6 can improve the condition of patients suffering from arthritis.
Pyridoxine (Vitamin B6) Foods
Seeds, rice, salmon, tuna, turkey and chicken.
Biotin (B7)
Vitamin B7 (biotin), also known as the beauty vitamin, has several benefits in relation to appearance, as it has been linked with improving the appearance of skin, hair, and nails.
There have also been studies [6] that suggest that vitamin B7 can help to control blood glucose levels, suggesting that supplementation can be beneficial for those who suffer from diabetes. Biotin may also be beneficial during pregnancy to support the normal growth of the baby.
Biotin (Vitamin B7) Foods
Most commonly found in meats, such as chicken and pork, although it can also be found in egg yolks, potatoes and nuts.
Folate (B9)
Folate, also known as vitamin B9, has several key benefits. It has been linked [7] to the prevention of memory loss, as well as improving depression. It has also been strongly linked with the prevention of birth defects in babies.
B9 can be found in a synthetic form, folic acid, which is often added to foods such as cereals to fortify them. It can also be bought in supplement form.
Folic Acid (Vitamin B9) Foods
Can be consumed naturally through green leafy vegetables, asparagus, root vegetables, milk, wheat, beans and salmon.
Cobalamin (B12)
The main role of vitamin B12 is to aid the other B vitamins in completing their roles. It works with folate to produce red blood cells, as well as to produce haemoglobin.
Vitamin B12 is only found in animal products, which means the vegans and vegetarians are at risk of being deficient. It may be necessary to supplement with vitamin B12 if you do not consume many animal products.
Cobalamin (Vitamin B12) Foods
Vitamin B12 most commonly found in fish, pork, beef, dairy and eggs.
Mood
B-complex vitamins have been known since the 1940s as antistress nutrients. Many of the vitamins have direct effects on mood and perception. For example, vitamin B1 supplements improve overall mood; high doses of vitamin B3 (in combination with vitamin C) have been used successfully to treat recent-onset schizophrenia. Vitamin B6 is needed to make serotonin, a neurotransmitter with antidepressant benefits.
Blood sugar.
Biotin and vitamin B1 stand out for their roles in maintaining normal blood sugar levels. Your body needs biotin to make insulin, a hormone that controls blood sugar levels. In addition, biotin regulates genes involved in the metabolism of glucose, amino acids, and fatty acids. Large amounts of biotin can lower triglyceride levels, and a combination of biotin and chromium picolinate has been shown to lower blood sugar levels. Vitamin B1 (100 mg, three times daily) has been shown to lower levels of microalbuminuria (protein in urine) in people with type 2 diabetes.
Cognitive function.
Approximately one-third of seniors suffer from atrophic gastritis, a condition that interferes with vitamin B12 absorption. Studies have found that vitamin B12 deficiency can mimic Alzheimer’s disease and other types of dementia. In these cases, taking vitamin B12 can restore cognitive function. Other B-complex vitamins, including niacin and folic acid, may be helpful in combination with vitamin B12.
Macular degeneration.
Researchers reported in the February 2009 issue of Archives of Internal Medicine that large supplemental amounts of B-complex vitamins led to a 35 percent lower incidence risk of age-related macular degeneration in women over the course of seven years.
Balancing Stress
The B vitamins are vital cofactors for specific enzymes involved in the production of adrenal hormones. These hormones regulate many processes in your body as well as help you to adapt to stress and cope with anxiety.
Your adrenal response to stress causes the metabolism of your cells to speed up, increasing the number of nutrients needed, which can lead to deficiencies. According to research, chronic stress depletes vitamin B6, so supplementing to maintain healthy levels could be of help therapeutically.
Bending and Stretching
Research has indicated that Vitamin B3 may have anti-inflammatory properties that could offer protection against arthritic symptoms and the need for pharmaceutical anti-inflammatory drugs.
Additionally, vitamin B5 may be of help to sufferers of Rheumatoid Arthritis, as these individuals have been found to have lower levels of this B vitamin in their blood than healthy people.
Scientists discovered that the lower the levels of B5, the more extreme the symptoms were. Further studies have shown that vitamin B5 may improve the morning stiffness and pain associated with rheumatoid arthritis.
Brighter Vision
Over time eye health can deteriorate leaving some people with short-sightedness and others with cataracts or age-related macular degeneration (AMD), which can lead to blindness. Fortunately, vitamin B2 (Riboflavin) works in tandem with other nutrients to help maintain normal clear vision.
Animal trials show that rats fed riboflavin deficient diets have developed cataracts and other studies have led some researchers to conclude that riboflavin deficiency may also contribute to night blindness.
Pregnant or Breastfeeding Women
During pregnancy, the demand for B vitamins, particularly B12 and folate, grows to support fetal development.
In women who are pregnant or breastfeeding, especially those who follow vegetarian or vegan diets, supplementing with a B-complex vitamin is crucial.
B12 or folate deficiency in pregnant or breastfeeding women can lead to severe neurological damage or birth defects in the fetus or infant .
Cardiovascular disease
Low levels of folic acid (and sometimes low B6 and B12 levels) lead to increases in blood levels of homocysteine, a chemical that damages blood vessel walls and sets the stage for cholesterol deposits.
Recently, researchers at the University of Southern California gave subjects high-dose B-complex vitamins or placebos daily for three years. Those taking the vitamins had significantly less thickening of their blood vessel walls, according to an article in Stroke.
Related Compounds
Many of the following substances have been referred to as vitamins as they were once believed to be vitamins. They are no longer considered as such, and the numbers that were assigned to them now form the “gaps” in the true series of B-complex vitamins described above (e.g., there is no vitamin B4). Some of them, though not essential to humans, are essential in the diets of other organisms; others have no known nutritional value and may even be toxic under certain conditions.
Vitamin B4 – can refer to the distinct chemicals choline, adenine, or carnitine.[rx][rx] Choline is synthesized by the human body, but not sufficient to maintain good health, and is now considered an essential dietary nutrient.[rx] Adenine is a nucleobase synthesized by the human body.[rx] Carnitine is an essential dietary nutrient for certain worms, but not for humans.[rx]
Vitamin B8 – adenosine monophosphate (AMP), also known as adenylic acid.[rx] Vitamin B8 may also refer to inositol.[rx]
Vitamin B10 – para-aminobenzoic acid (PABA or PABA), a chemical component of the folate molecule produced by plants and bacteria, and found in many foods.[rx][rx] It is best known as a UV-blocking sunscreen applied to the skin and is sometimes taken orally for certain medical conditions.[rx][rx]
Vitamin B11 – pteryl-hepta-glutamic acid (PHGA; chick growth factor). Vitamin Bc-conjugate was also found to be identical to PHGA.
Vitamin B14 – cell proliferant, anti-anemia, rat growth factor, and antitumor pterin phosphate named by Earl R. Norris. Isolated from human urine at 0.33ppm (later in the blood), but later abandoned by him as further evidence did not confirm this. He also claimed this was not xanthopterin.
Vitamin B15 – pangamic acid,[rx] also known as pangamate. Promoted in various forms as a dietary supplement and drug; considered unsafe and subject to seizure by the US Food and Drug Administration.[rx]
Vitamin B16 – dimethylglycine (DMG)[rx] is synthesized by the human body from choline.
Vitamin B17 – the pseudoscientific name for the poisonous compound amygdalin, also known as the equally pseudoscientific name “nitrilosides” despite the fact that it is a single compound. Amygdalin can be found in various plants but is most commonly extracted from apricot pits and other similar fruit kernels. Amygdalin is hydrolyzed by various intestinal enzymes to form, among other things, hydrogen cyanide, which is toxic to human beings when exposed to a high enough dosage. Some proponents claim that amygdalin is effective in cancer treatment and prevention, despite its toxicity and a severe lack of scientific evidence.[rx]
Dengue Fever Symptoms/Dengue fever also known as breakbone fever is a mosquito-borne infectious tropical disease caused by the dengue virus. Symptoms include fever, headache, muscle, and joint pains, and a characteristic skin rash that is similar to measles. In a small proportion of cases, the disease develops into life-threatening dengue hemorrhagic fever, which results in bleeding, thrombocytopenia, and leakage of blood plasma, or into dengue shock syndrome, in which dangerously low blood pressure occurs. Treatment of acute dengue fever is supportive, with either oral or intravenous rehydration for mild or moderate disease and use of intravenous fluids and blood transfusion for more severe cases. Along with attempts to eliminate the mosquito vector, work is ongoing to develop a vaccine and medications targeted directly at the virus.
Dengue is an acute febrile illness characterized by severe muscle and joint pain, rash, malaise, and lymphadenopathy. The severity of the musculoskeletal complaints gave rise to the sobriquet breakbone fever.
Dengue virus (DENV) belongs to the family Flaviviridae, genus Flavivirus, and is transmitted to humans by Aedes mosquitoes, mainly Aedes aegypti. Based on neutralization assay data, four serotypes (DENV-1, DENV-2, DENV-3, and DENV-4) can be distinguished. DENV infection is a major cause of disease in tropical and subtropical areas, with an estimated 50 million infections occurring each year and more than 2.5 billion people being at risk of infection [rx].
Types of Dengue Fever
The WHO classifies DF into two groups
Uncomplicated and severe.[rx,rx] Severe cases are linked to excessive hemorrhage, organ impairment, or severe plasma escape, and the remaining cases are considered uncomplicated.[rx]
According to the 1997 classification, dengue can be divided into an undifferentiated fever, DF, and DHF.[rx] DHF was further subdivided into grades I–IV.
Grade I: Only mild bruising or a positive tourniquet test
Grade II: Spontaneous bleeding into the skin and elsewhere
Grade III: Clinical sign of shock
Grade IV: Severe shock – feeble pulse, and blood pressure cannot be recorded.[rx]
Symptoms can appear up to 7 days after being bitten by the mosquito that carries the virus.
They include:
Aching muscles and joints
Body rash that can disappear and then reappear
High fever
Intense headache
Pain behind the eyes
Vomiting and feeling nauseous
Symptoms usually disappear after a week, and mild dengue rarely involves serious or fatal complications.
Dengue Hemorrhagic Fever
At first, symptoms of DHF may be mild, but they gradually worsen within a few days. As well as mild dengue symptoms, there may be signs of internal bleeding. DHF is frequently seen during secondary dengue infection. However, in infants, it may also occur during a primary infection due to maternally attained dengue antibodies.[rx] The proposed diagnostic criteria for DHF include:[rx]
Clinical parameters Acute-onset febrile phase – high-grade fever lasting from 2 days to 1 week. Hemorrhagic episodes (at least one of the following forms): Petechiae, purpura, ecchymosis, epistaxis, gingival and mucosal bleeding, GIT or injection site, hematemesis and/or Malena
A person with Dengue hemorrhagic fever may experience
Bleeding from the mouth, gums, or nose
Clammy skin
Damage to lymph and blood vessels
Internal bleeding, which can lead to black vomit and feces, or stools
A lower number of platelets in the blood
Sensitive stomach
Small blood spots under the skin
Weak pulse
Without prompt treatment, DHF can be fatal.
Dengue Shock Syndrome
DSS is a severe form of dengue. It can be fatal.
Apart from symptoms of mild dengue fever, the person may experience:
Intense stomach pain
Disorientation
Sudden hypotension, or a fast drop in blood pressure
Heavy bleeding
Regular vomiting
Blood vessels leaking fluid
Without treatment, this can result in death.
Criteria for Dengue Include
Probable dengue – The patient lives in or has traveled to a dengue-endemic area. Symptoms include fever and two of the following: nausea, vomiting, rash, myalgias, arthralgias, rash, positive tourniquet test, or leukopenia.
Warning Signs of Dengue – Abdominal pain, persistent vomiting, clinical fluid accumulation such as ascites or pleural effusion, mucosal bleeding, lethargy, liver enlargement greater than 2 cm, increase in hematocrit, and thrombocytopenia.
Severe Dengue – Dengue fever with severe plasma leakage, hemorrhage, organ dysfunction including transaminitis greater than 1000 international units per liter, impaired consciousness, myocardial dysfunction, and pulmonary dysfunction.
Dengue shock syndrome clinical warnings – Symptoms include rapidly rising hematocrit, intense abdominal pain, persistent vomiting, and narrowed or absent blood pressure.
The virus antigen can be detected by ELISA, polymerase chain reaction, or isolation of the virus from body fluids. Serology will reveal a marked increase in immunoglobulins. It is vital to assess pregnant patients with dengue as the symptoms may be very similar to preeclampsia.
Mechanism of Dengue Fever
When a mosquito carrying dengue virus bites a person, the virus enters the skin together with the mosquito’s saliva. It binds to and enters white blood cells, and reproduces inside the cells while they move throughout the body. The white blood cells respond by producing a number of signaling proteins, such as cytokines and interferons, which are responsible for many of the symptoms, such as the fever, the flu-like symptoms, and the severe pains. In severe infection, the virus production inside the body is greatly increased, and many more organs (such as the liver and the bone marrow) can be affected. Fluid from the bloodstream leaks through the wall of small blood vessels into body cavities due to capillary permeability. As a result, less blood circulates in the blood vessels, and the blood pressure becomes so low that it cannot supply sufficient blood to vital organs. Furthermore, dysfunction of the bone marrow due to infection of the stromal cells leads to reduced numbers of platelets, which are necessary for effective blood clotting; this increases the risk of bleeding, the other major complication of dengue fever.[rx]
Transmission
The Aedes aegypti mosquito is the primary vector of dengue. The virus is transmitted to humans through the bites of infected female mosquitoes. After virus incubation for 4–10 days, an infected mosquito is capable of transmitting the virus for the rest of its life.
Infected symptomatic or asymptomatic humans are the main carriers and multipliers of the virus, serving as a source of the virus for uninfected mosquitoes. Patients who are already infected with the dengue virus can transmit the infection (for 4–5 days; maximum 12) via Aedes mosquitoes after their first symptoms appear.
The Aedes aegypti mosquito lives in urban habitats and breeds mostly in man-made containers. Unlike other mosquitoes Ae. aegypti is a day-time feeder; its peak biting periods are early in the morning and in the evening before dusk. Female Ae. aegypti bites multiple people during each feeding period. Aedes eggs can remain dry for over a year in their breeding habitat and hatch when in contact with water.
Aedes albopictus, a secondary dengue vector in Asia, has spread to North America and more than 25 countries in the European Region, largely due to the international trade in used tires (a breeding habitat) and other goods (e.g. lucky bamboo). Ae. albopictus is highly adaptive and, therefore, can survive in cooler temperate regions of Europe. Its spread is due to its tolerance to temperatures below freezing, hibernation, and ability to shelter in microhabitats.[rx]
Through Mosquito Bites
Aedes aegypti mosquito.
Dengue viruses are spread to people through the bites of infected Aedes species mosquitoes (Ae. aegypti or Ae. albopictus). These are the same types of mosquitoes that spread Zika and chikungunya viruses.
These mosquitoes typically lay eggs near standing water in containers that hold water, like buckets, bowls, animal dishes, flower pots, and vases.
These mosquitoes prefer to bite people and live both indoors and outdoors near people.
Mosquitoes that spread dengue, chikungunya, and Zika bite during the day and night.
Mosquitoes become infected when they bite a person infected with the virus. Infected mosquitoes can then spread the virus to other people through bites.
Aedes albopictus mosquito.
From mother to child
A pregnant woman already infected with dengue can pass the virus to her fetus during pregnancy or around the time of birth.
To date, there has been one documented report of dengue spread through breast milk. Because of the benefits of breastfeeding, mothers are encouraged to breastfeed even in areas with risk of dengue.
Causes of Dengue Fever
[stextbox id=’info’]
Summary of soluble factors that are or are likely to be associated with the development of DHF/DSS
Soluble factor
Biological function in relation to pathogenesis
Thrombin
Thrombin is thought to act near the site at which it is produced. Thrombin converts circulating fibrinogen to fibrin and triggers platelet activation, which results in platelet aggregation. Thrombin activates EC and increases EC permeability, leading to plasma leakage and edema formation. Thrombin is chemotactic for monocytes and is mitogenic for lymphocytes and mesenchymal cells. Activated platelets release several soluble factors with inflammatory, antimicrobial, and immune modulating activity, such as MMP-9, which enhances EC permeability. Activated platelets also secrete soluble CD40 ligand, which can induce EC to produce reactive oxygen species, adhesion molecules, chemokines, and TF. Thrombin also inhibits IL-12 production by mononuclear cells.
C3a and C5a
C3a activates platelets and enhances their activation and adhesion properties. C5a enhances blood thrombogenicity by upregulating TF and PAI-1 expression on various cell types. C5a stimulates monocytes to produce IL-1, IL-6, IL-8, and TNF-α. Activation of these complement factors is enhanced by thrombin, which cleaves C3 and C5 to C3a/b and C5a/b, respectively. Activated platelets are also involved in C3 cleavage, which induces activation of the classical complement pathway.
C4b
C4b binds to protein S and thereby inhibit the anticoagulant properties of activated protein C-protein S complexes.
IL-1
IL-1β is a major mediator of platelet-induced activation of EC, causing enhanced chemokine release and upregulation of VCAM-1. VCAM-1 promotes adhesion of monocytes to the endothelium. IL-1 increases the expression of TF on EC and suppresses the cell surface anticoagulant activity of EC. Depending on its concentration, it may upregulate TNF-α production or downregulate TNF-receptors. IL-1 stimulates the hypothalamus and, as a consequence, the pituitary gland to produce anti-inflammatory mediators such as endorphins, melanocyte-stimulating hormone, and adrenocorticotropic hormone.
IL-6
Together with other proinflammatory cytokines, IL-6 potentiates the coagulation cascade. It can downregulate the production of TNF-α and TNF receptors. IL-6, together with IL-1, is a potent inducer of fever.
IL-8
IL-8 is a chemokine that is abundantly produced by monocytes, EC, and hepatocytes. EC damage in the liver may elevate systemic concentrations. Activation of the coagulation system results in increased expression of IL-6 and IL-8 by monocytes, while the APC-PS anticoagulation pathway downregulates production of IL-8 by EC.
IL-10
IL-10 is produced by monocytes and regulatory T helper cells and may cause platelet decay. Thrombin can stimulate IL-10 production by monocytes. The cytokine downregulates the inflammatory response and creates a proviral survival milieu. IL-10 promotes OAS by inhibiting the development of effector T cells to new epitopes. IL-10 also inhibits the expression of TF and inhibits fibrinolysis.
TNF-α
TNF-α in a potent activator of EC and enhances capillary permeability. TNF-α upregulates expression of TF on monocytes and EC and downregulates the expression of thrombomodulin on EC. It also activates the fibrinolysis system. TNF-α enhances expression of NO and mediates activation-induced death of T cells, and it has therefore been implicated in peripheral T-cell deletion.
TGF-β
TGF-β may act as a proinflammatory or anti-inflammatory cytokine, depending on its concentration. Early in infection, low levels of TGF-β may trigger the secretion of IL-1 and TNF-α. However, later in infection, the cytokine inhibits the Th1 response and enhances the production of Th2 cytokines such as IL-10. TGF-β increases expression of TF on EC and upregulates expression and release of PAI-1.
NO
NO has a multifaceted role in inflammatory reactions. It enhances the vasodilatation and formation of edema. It upregulates TNF-α production in monocytes. At low concentrations, it protects cells from apoptosis, while at high concentrations it induces apoptosis. NO downregulates expression of MHC class II and suppresses the expansion of Th1 cells. Maintenance of the EC barrier requires a basal level of NO. Both a lack of NO and high NO levels destabilize EC junctions.
VEGF
VEGF is a key driver of vascular permeability. It reduces EC occludins, claudins, and VE-cadherin content, all of which are components of EC junctions. Upon activation, VEGF stimulates expression of ICAM-1, VCAM-1, and E-selectin in EC.
[/stextbox]
Symptoms of Dengue Fever
Symptoms of Dengue Fever patient. Illustration about diagram for health check up.
[stextbox id=’info’]
Characteristics of concurrent malaria and dengue infection.
Characteristics
Malaria infection
Dengue infection
Concurrent infection
Mode of transmission
Mosquito-borne (Anopheles)
Mosquito-borne (Aedes)
Mosquito-borne (Anopheles + Aedes)
Fever
Acute febrile illness (chronic in some cases)
Acute febrile illness
Acute febrile illness
Myalgia
Detectable
Common
Common
Shock
Possible
Possible
Possible
Blood parasite
Positive
Negative
Positive
Atypical lymphocytosis
Usually negative
Usually positive
Usually positive
Hemoconcentration
Usually negative
Usually positive
Usually positive
Thrombocytopenia
Usually negative
Usually positive
Usually positive
Bleeding
Rare
Possible
Possible
Hemolysis
Possible
Rare
Rare
Tourniquet test
Usually negative
Usually positive
Usually positive
Treatment
Antimalarial drug
Fluid therapy
Antimalarial drug with fluid therapy
[/stextbox]
According to the WHO 2011 case definition [rx], dengue infection is suspected in a patient with high fever and two of the following signs or symptoms:
Mild bleeding (such a nose bleed, bleeding gums, or easy bruising)
UF cannot be diagnosed clinically and the diagnosis is based on serology or virology.
DF is considered to be a mild disease because death is rarely reported, but massive bleeding may be associated with DF.
DHF – clinical presentations during the febrile phase are similar to those in DF. The distinct feature of DHF is the increase in vascular permeability (plasma leakage) that differentiates DHF from DF. The plasma leakage is selective leakage into the pleural and peritoneal cavities that results in pleural effusion and ascites.
DSS – presentations are the same as those in DHF but the plasma leakage is so severe that the patient develops shock.
UD – most of the unusual cases are DHF cases with prolonged shock or DHF inpatients with co-morbidities or DHF together with other infections [rx].
[stextbox id=’alert’]
World Health Organization criteria for dengue fever, dengue hemorrhagic fever, and dengue shock syndrome
DF
DHF*
DSS
An acute febrile illness with ≥2 of the following manifestations:
All of the following must be present:
All 4 criteria for DHF must be met, plus evidence of circulatory failure manifested by:
Fever or history of acute fever, lasting 2-7 d
Headache
Bleeding, evidenced by at least one of the following:
Rapid and weak pulse,
Retro-orbital pain
and
Myalgia
Positive tourniquet test result†
Narrow pulse pressure
Arthralgia
Petechiae, ecchymoses, or purpura
or
Rash
Bleeding from the mucosa, GI tract, injection sites, or other locations
Hypotension for age (systolic pressure < 80 mm Hg for those < age 5 y, or <90 mm Hg for those > age 5 y)
Hemorrhagic manifestations
Leukopenia
Hematemesis or melena
AND
Thrombocytopenia (≤ 100,000 cells/mm3)
Cold clammy skin and restlessness
Supportive serology
OR
Evidence of plasma leakage caused by increased vascular permeability, manifested by at least one of the following:
The occurrence at the same location and time as other confirmed cases of DF
Laboratory criteria
Increase in hematocrit ≥ 20% above average for age, sex, and population
Isolation of dengue virus ≥ 4-Fold change in antibody titers
The decrease in hematocrit after volume-replacement treatment ≥ 20% of baseline
Demonstration of dengue virus antigen
Detection of dengue virus genomic sequence
Signs of plasma leakage such as pleural effusion, ascites, and hypoproteinemia
Grade I: fever and nonspecific constitutional symptoms; only hemorrhagic manifestation is a positive tourniquet test and/or easy bruising.
Grade II: same as grade I but includes spontaneous bleeding.
Grade III: Circulatory failure manifested by a rapid, weak pulse and narrowing of the pulse pressure or hypotension.
Grade IV: Profound shock with undetectable blood pressure or pulse. Grades III and IV define DSS.
Tourniquet test is performed by inflating a blood pressure cuff on the upper aspect of arm to a point midway between systolic and diastolic pressures for 5 minutes. The test result is positive when ≥ 20 petechiae/2.5 cm2 are observed.
[/stextbox]
Diagnosis of Dengue Fever
Laboratory diagnosis of a dengue virus infection
Confirmed dengue infection
Virus isolation
Genome detection
Antigen detection
IgM or IgG seroconversion
Probable dengue infection
IgM positive
Elevated IgG titer (that is, 1,280 or greater by haemagglutination inhibition test)
[stextbox id=’custom’]
Differential diagnosis of classic dengue fever–associated flushing erythema
Disease
Presenting symptoms
Exanthem
Timing from symptoms to rash
Distinguishing features
Chikungunya fever
Fever, arthralgia, myalgia, HA, ± vomiting, diarrhea
Flushing erythema on the face and upper aspect of the chest.[rx]
24 h
Asia, Africa, Indian Ocean
Sandfly fever
Fever, HA, malaise, retro-orbital pain
Flushing scarlatiniform erythema on face and neck. Very rare reports of subsequent rash (urticaria, erythema-multiforme, morbilliform). Lack of later rash helps distinguish from dengue fever.[rx]
Initially on neck/chest. The rapid development of 1- to 2-mm papules on the erythematous background (sandpaper). Linear petechiae (Pastia’s lines) in the skin folds. Subsequent membranous desquamation of palms/soles. White, then red, strawberry tongue.[rx]
12-48 h
ASO titer positive, leukocytosis
Toxic shock syndrome
Fever, hypotension
Generalized erythroderma or scarlatiniform rash. Erythema/edema of palms/soles. Strawberry tongue, conjunctival injection. Desquamation of palms/soles 1-2 wk after disease onset.[rx]
Polymorphic, including flushing macular erythema, nonpruritic erythematous plaques, erythema marginatum, pustules. Perineal involvement. Strawberry tongue, conjunctival hyperemia. Edema, erythema, then desquamation of palms/soles.[rx]
Concomitant
± Cardiac abnormalities
Erythema infectiosum (parvovirus B19)
Fever, HA, rhinorrhea
Initial macular fiery erythema of cheeks with circumoral pallor. In 1-4 d, morbilliform reticulated eruption on extremities (spares palms/soles); recurring stage (rash on exposure to trigger).[rx]
1-2 d
Arthritis in 80% of adults
ASO, Antistreptolysin O; HA, headache; LAD, lymphadenopathy.
[/stextbox]
Test / Differential diagnosis
[stextbox id=’info’]
Differential diagnosis of classic dengue fever–associated morbilliform eruption
Disease
Presenting symptoms
Exanthem
Timing from symptoms to rash
Distinguishing features
Infectious mononucleosis (EBV, CMV)
Fever, malaise, pharyngitis, LAD
Polymorphic, including generalized macular erythema ± petechiae, urticaria, scarlatiniform, erythema multiforme-like. The rash is rare (3%-10%).[rx,rx] Eyelid edema. Pinhead petechiae at the junction of the soft/hard palate (Forschheimer’s spots).
Within first week of illness
Roseola infantum (HHV 6)
Fever, LAD ± convulsions
Mostly discrete pink macules, occasional papules. Often starts on the back. The fully developed rash usually involves the trunk, nape of the neck, proximal limbs ± scalp. Rare for face involvement. Total duration 24-72 h. Nonpruritic. Not followed by desquamation or pigment change.[rx]
As fever subsides
Age 6-36 mo; reactivation in immunocompromised hosts; associated with DRESS syndrome (controversial)rx]
Measles
Fever, cough, coryza
Initial erythematous papules on the face; within 1-2 d, spreads to the trunk. Small bright red spots with blue-white center on buccal mucosa–often appear at the beginning stage of exanthem (Koplick spots).[rx]
1-7 d
Rubella
Fever, eye pain, LAD
Initial “brilliant” generalized erythema on face, which fades within 24 h. Then, pale rose-pink macules appear on face and scalp that spread down trunk and extremities. Macules coalesce on the lower aspect of back/buttocks. Forschheimer’s spots.[rx]
2-5 d
Enterovirus
Fever ± pharyngitis
Polymorphic, including diffuse macular or morbilliform eruption. ±Vesicles, petechiae, purpura.[rx]
Varies
Associated with myocarditis
Secondary syphilis
Fever, HA, pharyngitis, myalgia, weight loss, LAD
Polymorphic: macules/papules/psoriasiform papules. Often diffuse discrete red to red-brown papules involving palms and soles. ±Condyloma lata. ±Moth-eaten alopecia.[rx]
Weeks to months after the initial chance
Serology for RPR or VDRL
Typhoid fever
Fever, vomiting, diarrhea, HA
Rose spots: 2- to 4-mm pink grouped papules on the trunk or generalized erythema “erythema typos.”[rx]
2-4 wk
Rose spot cultures may be Salmonella typhi+
Chikungunya fever
Fever, arthralgia, myalgia, HA, LAD, vomiting, diarrhea
Erythematous macules and papules on the trunk and extremities with islands of sparing. ±Petechiae. Face spared. Burning sensation in pinna.[rx]
3-5 d
Asia, Africa, Indian Ocean
West Nile virus
Fever, seizures, ascending flaccid paralysis
Ill-defined erythematous-to-pink macules on the trunk, and proximal extremities with pruritus and dysesthesia. Spares face palms, soles, mucous membranes. Resolve without scaling.[rxx]
Pruritic morbilliform eruption. Initially discrete, then confluent. Starts on the face spread to trunk and extremities. Favors neck, chest, back, flanks, inner aspect of thighs and arms. Does not desquamate.[rx]
4 d, but varies
Sub-Saharan Africa
Mayaro virus
Fever, HA, myalgia, arthralgia
Erythematous macules and papules with some areas of confluence. Extremities and trunk[rx] ± hand involvement. Relative sparing of the face. Rash more common in children (89%) than adults (53%).[rx]
As fever subsides
South America
Sindbis virus
Fever, fatigue, arthralgia/arthritis
Generalized morbilliform eruption. Reports of vesicles on pressure points (palms/soles).[rx]
3-4 d
Europe, Africa, Asia, Australia
Ross River disease
Fever, fatigue, arthralgia/arthritis
Most commonly maculopapular on trunk and limbs. ± Palm/sole/face/scalp involvement. Reports of vesicular or purpuric. The rash seen in about 50% of affected persons.[rx]
3-4 d
Australia, Papua New Guinea, Fiji, Samoa
Leptospirosis
Acute phase: fever, HA, myalgia, pharyngitis.
Immune phase: organ failure
Acute phase: generalized morbilliform rash, most prominent on the trunk.[rx]
Immune phase: hemorrhage, bleeding, jaundice.
Jaundice with history of water exposure differentiates from dengue fever.[rx]
Concomitant
History of exposure to fresh water
Acute retroviral syndrome (HIV)
Fever, fatigue, HA, pharyngitis, myalgias, LAD
Macules and papules on the trunk and upper arms.[rx] ±Palms and soles.
Concomitant
CMV, Cytomegalovirus; DRESS, drug reaction with eosinophilia and systemic symptoms; EBV, Epstein-Barr virus; HA, headache; HHV, human herpesvirus; LAD, lymphadenopathy; RPR, rapid plasma reagin; VDRL, Venereal Disease Research Laboratory test.
[/stextbox]
Baby Mice
Although all four dengue serotypes were initially isolated from human serum by using baby mice (rx, rx, rx), this method is very time-consuming, slow, and expensive. Moreover, because of the low sensitivity of the method, many wild-type viruses cannot be isolated with baby mice.
Those that are isolated frequently require numerous passages to adapt the viruses to growth in mice. This method is no longer recommended for the isolation of dengue viruses, but some laboratories continue to use it (rx). One advantage of using baby mice, however, is that other arboviruses that cause dengue-like illness may be isolated with this system.
Mammalian Cell Culture
Mammalian cell cultures have many of the same disadvantages as baby mice for isolation of dengue viruses—they are expensive, slow, and insensitive (rx, rx, rx, rx).
As with isolation systems that use baby mice, viruses that are isolated frequently require many passages before a consistent cytopathic effect can be observed in the infected cultures. Although the use of this method continues in some laboratories, it is not recommended (rx, rx).
Mosquito Inoculation
Mosquito inoculation is the most sensitive method for dengue virus isolation (rx, rx). Isolation rates of up to 100% of serologically confirmed dengue infections are not uncommon, and this is the only method sensitive enough for routine successful virologic confirmation of fatal DHF and DSS cases (rx, rx, rx, rx). Moreover, there are many endemic dengue virus strains that can be recovered only by this method (rx, rx, rx).
Mosquito Cell Culture
Mosquito cell cultures are the most recent addition to dengue virus isolation methodology (rx, rx, rx, rx, rx). Three cell lines of comparable sensitivity are most frequently used (rx). The first cell line developed, and still the most widely used is the C6/36 clone of A. albopictus cells (76).
The use of these cell lines has provided a rapid, sensitive, and economical method for dengue virus isolation. Moreover, many serum specimens can be processed easily, making the method ideal for routine virologic surveillance (rx).
Hybridization Probes
The hybridization probe method detects viral nucleic acids with cloned hybridization probes (rx, rx). Probes with variable specificity ranging from dengue complex to serotype-specific can be constructed depending on the genome sequences used. The method is rapid and relatively simple and can be used on human clinical samples as well as fixed autopsy tissues.
Unfortunately, hybridization probes have not been widely used or evaluated in the diagnostic laboratory. Preliminary data suggest that this method is less sensitive than RT-PCR, but like PCR, the outcome of the test is not influenced by the presence of neutralizing antibodies or other inhibitory substances.
Even so, the difficulties of working with RNA and the technical expertise required to obtain reproducible results make this method more suitable as a research tool than as a routine diagnostic test (rx, rx, rx).
Immunohistochemistry
A major problem in dengue laboratory diagnosis has been confirmation of fatal cases. In most instances, only a single serum sample is obtained and serologic testing is therefore of limited value. Also, most patients die at the time of or slightly after defervescence, when virus isolation is difficult.
With new methods of immunohistochemistry, it is now possible to detect dengue viral antigen in a variety of tissues (rx, rx).
Although immunofluorescence tests were used in the past, newer methods involving enzyme conjugates such as peroxidase and phosphatase in conjunction with either polyclonal or monoclonal antibodies are greatly improved (rx). Because tissues can be fresh or fixed, autopsies should be performed in all cases of suspected DHF with a fatal outcome (rx, rx).
MAC-ELISA
The Armed Forces Research Institute of Medical Sciences (AFRIMS) developed an IgM antibody-capture enzyme-linked immunosorbent assay (MAC-ELISA) for dengue in regions where dengue and Japanese encephalitis virus co-circulate[rx[. Today, many groups have developed their own in-house MAC-ELISAs. Dengue-specific IgM in the test serum is detected by first capturing all IgM using human-specific IgM bound to a solid phase.
IgG ELISA
An ELISA for dengue-specific IgG detection can be used to confirm a dengue infection in paired sera. It is also widely used to classify primary or secondary infections[rx,rx,rx,rx]. Some protocols use serum dilutions to titer dengue-specific IgG[rx] and others use the ratio of IgM to IgG[rx,rx].
The assay uses the same dengue antigens as MAC-ELISA and it correlates with results from the haemagglutination inhibition assay.
IgM: IgG ratio
A dengue virus E and M protein-specific IgM – IgG ratio can be used to distinguish primary from secondary dengue virus infections. IgM capture and IgG capture ELISAs are the most common assays for this purpose. According to this method, a dengue infection is defined as a primary infection if the IgM:IgG OD ratio is greater than 1.2 (using patient sera at 1:100 dilution) or 1.4 (using patient sera at 1:20 dilution), or as a secondary infection if the ratio is less than 1.2 or 1.4 (rxrx,rx).
Nucleic Acid Amplification Tests
Many nucleic acid amplification tests (NAATs) have been developed for the diagnosis of dengue infection. Some techniques are quantitative and others can be used for serotyping. However, none has been commercialized to date and quality assurance materials are not widely available to ensure the quality of the results.
Treatment of Dengue Fever
For milder forms, treatment includes
Preventing dehydration – A high fever and vomiting can dehydrate the body. The person should drink clean water, ideally bottled rather than tap water. Rehydration salts can also help replace fluids and minerals.
Painkillers, such as Tylenol or paracetamol – These can help lower fever and ease the pain.
Non-steroidal anti-inflammatory drugs (NSAIDs) – such as aspirin or ibuprofen, are not advised, as they can increase the risk of internal bleeding.
More severe forms of dengue fever may need
Intravenous (IV) fluid supplementation, or drip, if the person cannot take fluids by mouth
Blood transfusion, for patients with severe dehydration
WHO guidelines summarize the following principles of fluid therapy [rx]
Oral fluid supplementation must be as plentiful as possible. However, intravenous fluid administration is mandatory in cases of shock, severe vomiting, and prostration (cases where the patient is unable to take fluids orally)
Crystalloids form the first-line choice of intravenous fluid (0.9% saline)
Hypotensive states that are unresponsive to boluses of intravenous crystalloids, colloids (e.g., dextran) form the second-line measures
If the patient remains in the critical phase with low platelet counts, there should be a serious concern for bleeding. Suspected cases of bleeding are best managed by transfusion of fresh whole blood.
The management of patients with dengue infections depends on the phase of illness, i.e. febrile phase, critical/ leakage phase and convalescence phase, as follows:
1. Febrile Phase [rx–rx] (Early diagnosis of dengue infection )
Clinical sign
High fever with positive Tourniquet test + leukopenia (WBC ≤ 5,000 cells/mm3) – positive predictive value 70–83% [rx, rx]
Rapid Diagnostic Test
NS1Ag test during the febrile phase (first five days of fever): sensitivity 60–70%, specificity >99%
PCR – good sensitivity and specificity but expensive and not available in most places
ELISA- IgM, IgG test – not suitable for early diagnosis because the antibody significantly rises after day 5 of fever
(Management)
Reduction of high fever: paracetamol only, tepid sponge
Promote oral feeding: soft diet, milk, fruit juice, oral rehydration solution (ORS). Avoid IV fluid if there is no vomiting and moderate/ severe dehydration
Follow up CBC every day
Advise to come back to the hospital ASAP when there is no clinical improvement despite a lack of fever, severe abdominal pain/ vomiting, bleeding, restless/irritable, drowsy, refusal to eat or drink (some patients may be thirsty), urine not passed for 4–6 hours
2. Critical/ Leakage phase: (Early detection of plasma leakage/ shock)
Thrombocytopenia, i.e. platelet count ≤ 100,000 cells/mm3, is the best indicator for plasma leakage: Platelet count between 50,000 and 100,000 cells/mm3 – beginning of plasma leakage (about half of DF patients have thrombocytopenia at this level), platelet count < 50,000 cells/mm3 – DHF is most likely and usually indicates that plasma leakage has occurred, probably for 24 hours.
Admit patients with thrombocytopenia and poor appetite/ poor clinical conditions. Consider admitting high-risk patients: infants, obese patients, patients with prolonged shock (grade IV), bleeding, encephalopathy, underlying diseases, pregnancy.
Detection of pleural effusion and ascites by a physical examination in the early leakage phase or even at the time of shock is very difficult. Chest film – right lateral decubitus technique, ultrasonography or serum albumin ≤ 3.5 gm% are the alternative ways to detect plasma leakage.
(Proper IV fluid management during the critical period)
Isotonic salt solution in the critical period, e.g. 5% dextrose in normal saline solution (NSS), 5% Ringer Acetate, 5% Ringer-Lactate. The 5% dextrose in NSS is preferable because the severe cases needing admission are those with poor appetite, nausea/ vomiting, and abdominal pain.
The total amount of fluid needed during the critical period of 24–48 hours is estimated to be maintenance + 5% deficit (M+5%D), including oral and IV fluids. In DSS patients the duration of IV fluid may be 24–36 hours and in non-shock DHF 48–60 hours.
The rate of IV fluid should be adjusted according to clinical vital signs (BP, pulse, respiratory rate, temperature), hematocrit (Hct) and urine output (0.5 ml/kg/hr)
The rate of IV fluid for shock patients (DHF grade III) is shown in Figure [rx]. The IV fluid resuscitation for DHF grade III is less than that recommended for other kinds of shock, i.e. only 10 ml/kg/hr, not 20 ml/kg/hr or over. A larger amount of IV fluid is needed for DHF grade IV, but the rate should be reduced to 10 ml/kg/hr as soon as the blood pressure is restored.
The rate of IV fluid for non-shock patients (DHF grade I and II) is shown in Figure [rx]. The administration should begin at a slower rate if leakage is in the earlier stage, i.e. platelet count is between 50,000 and 100,000 cells/mm3. The rate of IV should be more rapid when the leakage has continued for some time, i.e. platelet count < 50,000 cells/mm3.
If the clinical response is not good (re-shock, unstable vital signs, inability to reduce the rate of IV fluid) investigate and correct the following laboratory data:
A – Acidosis – blood gas (capillary or venous), if present, check liver and renal functions. Correct acidosis when blood pH is < 7.35 and HCO3 < 15 mEq/L.
B – Bleeding – Hct: if high, dextran is indicated, if low or not rising, consider blood transfusion and consider giving vitamin K1 intravenously.
C – iCa and other electrolytes – Na, K. Give gluconate 1 ml/kg/dose diluted twice with IV fluid and IV push slowly. The maximum dose is 10 ml/dose.
S – Blood sugar
Colloidal solution – only plasma expander that has an osmolarity higher than that of plasma is recommended, e.g. 10% Dextran-40 in NSS. A bolus dose of 10 ml/kg/hr in children or 500 ml/hr in adults is recommended, and this will usually bring the Hct down to 10 points in cases with signs of fluid overload or persistently high Hct.
In cases with significant bleeding, i.e. > 6–8 ml/kg ideal body weight in children or 300 ml in adult, blood transfusion is recommended as soon as possible. The amount to transfuse is equal to the estimated amount. If it is impossible to estimate (concealed internal bleeding), transfuse 10 ml/kg of fresh whole blood (FWB) or 5 ml/kg of packed red cells (PRC) in children to raise Hct by 5 points. In adults, transfuse 1 unit of FWB or PRC.
Platelets are indicated in cases with significant bleeding. If the patient already has signs of fluid overload, however, do not give platelets because this will cause fluid overload (possibly acute pulmonary edema). Platelet transfusion is only adjunct therapy, no specific treatment. There is no platelet prophylaxis in children, no matter how low the platelet count. Clinicians may consider prophylactic platelet transfusion in adults with underlying hypertension or heart disease and a platelet count < 10,000 cells/mm3.
Plasma has almost no role in the management of acute DHF in the critical phase.
The steroid has no role in the management of DSS.
At the children’s hospital, Bangkok, DHF/DSS patients were treated with NSS (100%), Dextran-40 (20–25%), blood transfusion (10–15%) and platelet transfusion (0.4%) [rx].
3. Convalescence phase
Stop IV fluid when there are signs of recovery: convalescence rash, itching, increase in appetite or > 30 hours after shock and > 60 hours after plasma leakage. Sinus bradycardia may be observed in some patients.
Patients who have massive ascites and pleural effusion may need diuretic during this period of reabsorption of extravasated plasma into the circulation.
Some patients may not regain their appetite in this period. This may be due to diuresis and loss of potassium in the urine. A potassium supplement may be necessary in this phase. Fruit (bananas, oranges) and fruit juice are rich in potassium and are preferred by most patients.
In adults, the convalescence period may extend for 2–4 weeks with fatigue.
The most common complication in DHF/DSS management is fluid overload, which may lead to heart failure, acute pulmonary edema or even death if not managed properly and timely.
Steps in the management of fluid overload
Early detection of signs and symptoms of fluid overload.Early signs of fluid overload: puffy eyelids, tachypnea, distended abdomen with abdominal discomfort. Late signs of fluid overload = indication for diuretic (furosemide 1 mg/kg/dose)* : Cough, respiratory distress (dyspnea/ orthopnea), very tense abdomen, wide pulse pressure (some may have narrowing of pulse pressure), strong and bounding pulse, hypertension (reabsorption phase), abnormal lung signs (crepitation, rhonchi, wheezing). A urinary catheter should be inserted in every patient with late signs of fluid overload.
Know the status of the patient: time after shock or time after plasma leakage. If the patients are still in the leakage phase, dextran bolus is recommended 15–30 minutes before administering furosemide.
Status of the patient at that time: shock or non-shock. If the patients are in shock state, dextran bolus is recommended for 15–30 minutes before administer furosemide.
Assessment and correct associated complications: bleeding, electrolyte/metabolic/acid-base disturbance, liver/renal failure?
Clinicians are urged to measure the vital signs four times at 15-minute intervals after furosemide administration because furosemide acts for less than 1 hour.
Most cases of encephalopathy are observed in DHF patients during or after the critical phase, but it may occur early in the febrile phase. Few cases are found among DF patients. The presentations include behavior change (aggression, violence, vulgar language), consciousness change (irritation, agitation, confusion, hallucinations, coma) and convulsion.
More than half of DHF patients who present with encephalopathy are cases of prolonged shock and liver/renal failure. The other common causes are hyponatremia, hypoglycemia, and hypocalcemia. Intracranial bleeding, although quite rare, is usually found in DSS patients with prolonged shock and multi-organ failure and occurs very late, i.e. > 3 days aftershock.
Management of dengue encephalopathy is generally the same as that of hepatic encephalopathy, as follows:
Maintain adequate airway oxygenation with oxygen therapy. Intubation may be necessary for patients who are in respiratory failure or semi-coma/ coma.
Prevent/ reduce ICP by the following measures
Give minimal IV fluid to maintain adequate intravascular volume, ideally, the total IV fluid should not exceed 80% maintenance
Switch to colloidal solution earlier if Hct continues to rise or a large volume of IV is needed in cases with severe plasma leakage.
Administer diuretic if indicated in cases with signs and symptoms of fluid overload
Consider steroids to reduce ICP. Dexamethasone 0.5 mg/kg/day IV every 6–8 hours is recommended.
Hyperventilation?
Decrease ammonia production: Give lactulose 5–10 ml every 6 hours for induction of osmotic diarrhea. Local antibiotics to eliminate bowel flora. This is not necessary if systemic antibiotics are given.
Maintain blood sugar level > 60 mg%. Recommend a glucose infusion rate between 4–6 mg/kg/hour.
Correct acid-base and electrolyte balance, e.g. correct hypo/hypernatremia, hypo/hyperkalemia, hypocalcemia, and acidosis.
Vitamin K1 IV administration: 3 mg for < 1 year old, 5 mg for < 5 years old and 10 mg for > 5 years old and adults.
Anti-convulsants should be given for control of seizures; phenobarbital, Dilantin and diazepam IV as indicated
Transfuse blood, preferably fresh packed red cells as indicated. Other blood components such as platelets and fresh frozen plasma should not be given because the fluid overload may cause increased ICP.
Empiric antibiotic therapy may be indicated if suspected superimposed bacterial infections occur.
H2-blockers or proton pump inhibitor may be given to alleviate gastrointestinal bleeding.
Avoid unnecessary drugs because most drugs have to be metabolized by the liver.
Consider plasmapheresis or hemodialysis or renal replacement therapy in cases of clinical deterioration.
Medicine that may be used
Polyoxotungstates and sulfated polysaccharides – show some potential as viral inhibitors. They impair flavivirus adsorption and entry into host cells in vitro, apparently by binding to the cell surface [rx, rx]. Sulfated galactomannans protected mice from lethal YFV infection when inoculated simultaneously with the virus [rx]
Ivermectin – a broadly used antihelmintic drug, displays specific inhibitory unwinding activity against helicases from several flaviviruses, including YFV, DENV, and WNV with the half maximal inhibitory concentration (IC50) values in the submicromolar range [rx]. Preliminary studies indicate higher binding efficiency with YFV than with DENV. Nevertheless, disappointingly, Ivermectin did not protect hamsters against infection with YFV. Structure-based optimization may result in analogs exerting potent activity against flaviviruses both in vitro and in vivo.
Doxorubicin – is an antineoplastic antibiotic obtained from Streptomyces peucetius. This antibiotic exhibits in vitro antiviral activity against the YFV17D vaccine strain and the DENV-2 NGC strain. Doxorubicin proved to be cytotoxic in uninfected host cells. However, a novel derivative of doxorubicin, SA-17, showed excellent antiviral activity against DENV and markedly reduced cytopathogenicity [rx]. The dose-dependent anti-DENV activity was confirmed using a dengue reporter virus.
Flaviviral inhibitory activity – has also been observed with plant extracts. Boesenbergia rotunda (L.) Mansf. Kulturpfl. (BR) is a common spice belonging to a member of the ginger family (Zingiberaceae)? Some of the BR compounds, such as flavonoids and chalcones, have been shown to be pharmaceutically active. The chalcone, cardamon, isolated from BR, was recently reported to exhibit appreciable anti-HIV-1 protease inhibition [rx]. Moreover, inhibitory activity by six compounds isolated from BR has also been demonstrated on DENV-2 virus NS3 protease activity.
[stextbox id=’info’]
Current status of dengue vaccine development
No
Strategy
Developer (s)
Current status
1
Live attenuated yellow fever 17D/DENV chimeric vaccine
Sanofi-Pasteur
Phase 3 trials with a tetravalent formulation in DENV endemic countries
2
PDK cell-passaged, live attenuated vaccine
WRAIR/GSK
Phase 2 trials with a tetravalent formulation in endemic countries
3
Live attenuated DENV Delta-30 mutation and intertypic DENV chimeric vaccines
NIH/Johns Hopkins
Phase 1/2 trials with monovalent formulations completed; tetravalent
phase 1 initiated
4
Dengue prM-E DNA vaccine
NMRC
Phase 1 with monovalent vaccine completed
5
Recombinant 80 % E subunit antigen vaccine
Hawaii Biotech/Merck
Phase 1 with monovalent vaccine initiated
6
Purified inactivated vaccine
WRAIR
Phase 1 with monovalent vaccine initiated
7
Live attenuated chimeric DENV vaccine
CDC
Phase 1 with monovalent vaccine initiated
Abbreviations: PDK, primary dog kidney cells; WRAIR, Walter Reed Army Institute of Research; GSK, GlaxoSmithKline Biologicals; NIH, National Institutes of Health; prM-E, membrane-envelope; NMRC, Naval Medical Research Center; CDC, Centers of Disease Control and Prevention
Selected dengue vaccine candidates
Vaccine approach
Developer
Status
Live attenuated tetravalent chimeric YF–DEN vaccine
Sanofi Pasteur
Phase II
Live attenuated tetravalent viral isolate vaccine
WRAIR and GSK
Phase II
Live attenuated chimeric DEN2–DEN vaccine
CDC and Inviragen
Phase I
Recombinant E subunit vaccine
Merck
Phase I
Live attenuated tetravalent vaccine comprising 3′ deletion mutations and DEN–DEN chimeras
US NIH LID and NIAID
Phase I
Subunit recombinant antigen (domain III) vaccine
IPK/CIGB
Preclinical
Live attenuated chimeric YF–DEN vaccine
Oswaldo Cruz Foundation
Preclinical
Tetravalent DNA vaccine
US NMRC and GenPhar
Preclinical
Purified inactivated tetravalent vaccine
WRAIR and GSK
Preclinical
[/stextbox]
Complications
Liver injury
Cardiomyopathy
Pneumonia
Orchitis
Oophoritis
Seizures
Encephalopathy
Encephalitis
Prevention
Travelers can protect themselves by preventing mosquito bites.
Prevent mosquito bites
Cover exposed skin by wearing long-sleeved shirts, long pants, and hats.
Use an appropriate insect repellent as directed.
Higher percentages of active ingredient provide longer protection. Use products with the following active ingredients
DEET – (Products containing DEET include Off!, Cutter, Sawyer, and Ultrathon)
Picaridin – (also known as KBR 3023, Bayrepel, and icaridin products containing picaridin include Cutter Advanced, Skin So Soft Bug Guard Plus, and Autan [outside the US])
Oil of lemon eucalyptus (OLE) or PMD – (Products containing OLE include Repel and Off! Botanicals)
IR3535 – (Products containing IR3535 include Skin So Soft Bug Guard Plus Expedition and SkinSmart)
Always follow product directions and reapply as directed
If you are also using sunscreen, apply sunscreen first and insect repellent second.
Follow package directions when applying repellent on children. Avoid applying repellent to their hands, eyes, and mouth.
Use permethrin-treated clothing and gear (such as boots, pants, socks, and tents). You can buy pre-treated clothing and gear or treat them yourself
Treated clothing remains protective after multiple piles of washing. See the product information to find out how long the protection will last.
If treating items yourself, follow the product instructions carefully.
Do not use permethrin directly on the skin.
Stay and sleep in screened or air-conditioned rooms.
Use a bed net if the area where you are sleeping is exposed to the outdoors.
Advocacy, social mobilization and legislation to ensure that public health bodies and communities are strengthened;
Collaboration between the health and other sectors (public and private);
An integrated approach to disease control to maximize the use of resources;
Evidence-based decision making to ensure any interventions are targeted appropriately; and
Capacity-building to ensure an adequate response to the local situation.
If you are bitten by mosquitoes
Avoid scratching mosquito bites.
Apply hydrocortisone cream or calamine lotion to reduce itching.
If you feel sick and think you may have dengue
Talk to your doctor or nurse if you feel seriously ill, especially if you have a fever.
Tell them about your travel.
For more information about medical care abroad, see Getting Health Care Abroad and a list of International Joint Commission-accredited facilities.
Use acetaminophen. Do not take pain relievers that contain aspirin and ibuprofen (Advil), it may lead to a greater tendency to bleed.
Get lots of rest, and drink plenty of liquids.
Avoid spreading the disease by preventing more mosquito bites.
Mosquito repellents – Use a repellent with at least 10 percent concentration of diethyltoluamide (DEET), or a higher concentration for longer lengths of exposure. Avoid using DEET on young children.
Mosquito traps and nets – Nets treated with insecticide are more effective, otherwise, the mosquito can bite through the net if the person is standing next to it. The insecticide will kill mosquitoes and other insects, and it will repel insects from entering the room.
Door and window screens – Structural barriers, such as screens or netting, can keep mosquitos out.
Avoid scents – Heavily scented soaps and perfumes may attract mosquitos.
Camping gear – Treat clothes, shoes, and camping gear with permethrin or purchase clothes that have been pretreated.
Timing – Try to avoid being outside at dawn, dusk, and early evening.
Stagnant water – The Aedes mosquito breeds in clean, stagnant water. Checking for and removing stagnant water can help reduce the risk.
To reduce the risk of mosquitoes breeding in stagnant water
Turn buckets and watering cans over and store them under shelter so that water cannot accumulate
Remove excess water from plant pot plates
Scrub containers to remove mosquito eggs
Loosen soil from potted plants, to prevent puddles forming on the surface
Make sure scupper drains are not blocked and do not place potted plants and other objects over them
Use non-perforated gully traps, install anti-mosquito valves, and cover any traps that are rarely used
Do not place receptacles under an air-conditioning unit
Change the water in flower vases every second day and scrub and rinse the inside of the vase
Prevent leaves from blocking anything that may result in the accumulation of puddles or stagnant water
Prevention and Control According to WHO
At present, the main method to control or prevent the transmission of the dengue virus is to combat vector mosquitoes through:
Preventing mosquitoes from accessing egg-laying habitats by environmental management and modification;
Disposing of solid waste properly and removing artificial man-made habitats;
Covering, emptying and cleaning of domestic water storage containers on a weekly basis;
Applying appropriate insecticides to water storage outdoor containers;
Using of personal household protection measures, such as window screens, long-sleeved clothes, repellents, insecticide-treated materials, coils and vaporizers (These measures have to be observed during the day both at home and place of work since the mosquito bites during the day);
Improving community participation and mobilization for sustained vector control;
Applying insecticides as space spraying during outbreaks as one of the emergency vector-control measures;
Active monitoring and surveillance of vectors should be carried out to determine the effectiveness of control interventions.
Careful clinical detection and management of dengue patients can significantly reduce mortality rates from severe dengue.
WHO Response
WHO responds to dengue in the following ways:
Supports countries in the confirmation of outbreaks through its collaborating network of laboratories;
Provides technical support and guidance to countries for the effective management of dengue outbreaks;
Supports countries to improve their reporting systems and capture the true burden of the disease;
Provides training on clinical management, diagnosis and vector control at the regional level with some of its collaborating centers;
Formulates evidence-based strategies and policies;
Develops new tools, including insecticide products and application technologies;
Gathers official records of dengue and severe dengue from over 100 Member States; and
Publishes guidelines and handbooks for surveillance, case management, diagnosis, dengue prevention and control for the Member States.
What Happens If You Don’t Get Enough Vitamin B2/Riboflavin is an essential human nutrient that is a heat-stable and water-soluble flavin belonging to the vitamin B family? Riboflavin is a precursor of the coenzymes flavin mononucleotide (FMN) and flavin adenine dinucleotide (FAD). These coenzymes are of vital importance in normal tissue respiration, pyridoxine activation, tryptophan to niacin conversion, fat, carbohydrate, and protein metabolism, and glutathione reductase-mediated detoxification. Riboflavin may also be involved in maintaining erythrocyte integrity. This vitamin is essential for healthy skin, nails, and hair.
Riboflavin is d-Ribitol in which the hydroxy group at position 5 is substituted by a 7,8-dimethyl-2,4-dioxo-3,4-dihydrobenzo[g]pteridin-10(2H)-aryl moiety. It is a nutritional factor found in milk, eggs, malted barley, liver, kidney, heart, and leafy vegetables, but the richest natural source is yeast. The free form occurs only in the retina of the eye, in whey, and in urine; its principal forms in tissues and cells are as flavin mononucleotide and flavin adenine dinucleotide. It has a role as a photosensitizing agent, a metabolite, a B vitamin, a food coloring, an Escherichia coli metabolite, and a mouse metabolite. It is conjugate acid of riboflavin(1-).
Riboflavin is yellow and naturally fluorescent when exposed to ultraviolet light. Moreover, ultraviolet and visible light can rapidly inactivate riboflavin and its derivatives. Because of this sensitivity, lengthy light therapy to treat jaundice in newborns or skin disorders can lead to riboflavin deficiency. The risk of riboflavin loss from exposure to light is the reason why milk is not typically stored in a glass container
Deficiency Symptoms of Riboflavin/vitamin B2
Riboflavin deficiency is also known as ariboflavinosis.
Primary riboflavin deficiency happens when the person’s diet is poor in vitamin B2
Secondary riboflavin deficiency happens for another reason, maybe because the intestines cannot absorb the vitamin properly, or the body cannot use it, or because it is being excreted too rapidly
Angular cheilitis, or cracks at the corners of the mouth
Riboflavin deficiency (also called ariboflavinosis) results in stomatitis including painful red tongue with a sore throat, chapped and fissured lips (cheilosis), and inflammation of the corners of the mouth (angular stomatitis). There can be oily scaly skin rashes on the scrotum, vulva, philtrum of the lip, or the nasolabial folds. The eyes can become itchy, watery, bloodshot and sensitive to light. Due to interference with iron absorption, even mild to moderate riboflavin deficiency results in an anemia with normal cell size and normal hemoglobin content (i.e. normochromic normocytic anemia). This is distinct from anemia caused by a deficiency of folic acid (B9) or cyanocobalamin (B12), which causes anemia with large blood cells (megaloblastic anemia). Deficiency of riboflavin during pregnancy can result in birth defects including congenital heart defects and limb deformities.
The stomatitis symptoms are similar to those seen in pellagra, which is caused by niacin (B3) deficiency. Therefore, riboflavin deficiency is sometimes called “pellagra sine pellagra” (pellagra without pellagra), because it causes stomatitis but not widespread peripheral skin lesions characteristic of niacin deficiency. Riboflavin deficiency prolongs recovery from malaria, despite preventing the growth of Plasmodium (the malaria parasite).
Daily Requirement of Riboflavin/vitamin B2
Intake recommendations for riboflavin and other nutrients are provided in the Dietary Reference Intakes (DRIs) developed by the Food and Nutrition Board (FNB) at the Institute of Medicine of the National Academies. DRI is the general term for a set of reference values used for planning and assessing nutrient intakes of healthy people. These values, which vary by age and sex, include:
Recommended Dietary Allowance (RDA) – Average daily level of intake sufficient to meet the nutrient requirements of nearly all (97%–98%) healthy individuals; often used to plan nutritionally adequate diets for individuals.
Adequate Intake (AI) – Intake at this level is assumed to ensure nutritional adequacy; established when evidence is insufficient to develop an RDA.
Estimated Average Requirement (EAR) – Average daily level of intake estimated to meet the requirements of 50% of healthy individuals; usually used to assess the nutrient intakes of groups of people and to plan nutritionally adequate diets for them; can also be used to assess the nutrient intakes of individuals.
Tolerable Upper Intake Level (UL): Maximum daily intake unlikely to cause adverse health effects.
Table 1 lists the current RDA for riboflavin. For infants from birth to 12 months, the FNB established an AI for riboflavin that is equivalent to the mean intake of riboflavin in healthy, breastfed infants.
[stextbox id=’info’]
Recommended Dietary Allowances (RDAs) for Riboflavin
Age
Male
Female
Pregnancy
Lactation
Birth to 6 months*
0.3 mg
0.3 mg
7–12 months*
0.4 mg
0.4 mg
1–3 years
0.5 mg
0.5 mg
4–8 years
0.6 mg
0.6 mg
9–13 years
0.9 mg
0.9 mg
14–18 years
1.3 mg
1.0 mg
1.4 mg
1.6 mg
19-50 years
1.3 mg
1.1 mg
1.4 mg
1.6 mg
51+ years
1.3 mg
1.1 mg
About 95% of riboflavin in the form of FAD or FMN from food is bioavailable up to a maximum of about 27 mg of riboflavin per meal or dose. The bioavailability of free riboflavin is similar to that of FAD and FMN. Because riboflavin is soluble in water, about twice as much riboflavin content is lost in cooking water when foods are boiled as when they are prepared in other ways, such as by steaming or microwaving.
Selected Food Sources of Riboflavin
Food
Milligrams
(mg) per
serving
Percent
DV*
Beef liver, pan fried, 3 ounces
2.9
171
Breakfast cereals, fortified with 100% of the DV for riboflavin, 1 serving
1.7
100
Oats, instant, fortified, cooked with water, 1 cup
1.1
65
Yogurt, plain, fat free, 1 cup
0.6
35
Milk, 2% fat, 1 cup
0.5
29
Beef, tenderloin steak, boneless, trimmed of fat, grilled, 3 ounces
Bagel, plain, enriched, 1 medium (3½”–4” diameter)
0.2
12
Salmon, pink, canned, 3 ounces
0.2
12
Spinach, raw, 1 cup
0.1
6
Apple, with skin, 1 large
0.1
6
Kidney beans, canned, 1 cup
0.1
6
Macaroni, elbow shaped, whole wheat, cooked, 1 cup
0.1
6
Bread, whole wheat, 1 slice
0.1
6
Cod, Atlantic, cooked, dry heat, 3 ounces
0.1
6
Sunflower seeds, toasted, 1 ounce
0.1
6
Tomatoes, crushed, canned, ½ cup
0.1
6
Rice, white, enriched, long grain, cooked, ½ cup
0.1
6
Rice, brown, long grain, cooked, ½ cup
0
0
DV = Daily Value. DVs were developed by the U.S. Food and Drug Administration (FDA) to help consumers compare the nutrient contents of products within the context of a total diet. The DV for riboflavin is 1.7 mg for adults and children age 4 and older. Foods providing 20% or more of the DV are considered to be high sources of a nutrient.
The U.S. Department of Agriculture’s (USDA’s) National Nutrient Database for Standard Reference website lists the nutrient content of many foods and provides a comprehensive list of foods containing riboflavin arranged by nutrient content and food name.
[/stextbox]
Natural Food Source
[stextbox id=’info’]
United States
Age group (years)
RDA for riboflavin (mg/d)
Tolerable upper intake level
Infants 0–6 months
0.3*
ND
Infants 6–12 months
0.4*
1–3
0.5
4–8
0.6
9–13
0.9
Females 14–18
1.0
Males 14–18
1.3
Females 19+
1.1
Males 19+
1.3
Pregnant females 14–50
1.4
Lactating females 14–50
1.6
European Food Safety Authority
Age group (years)
Adequate Intake of riboflavin (mg/d)
Tolerable upper limit
7–11 months
0.4
ND
1–3
0.6
4–6
0.7
7–10
1.0
11–14
1.4
15–17
1.6
18+
Australia and New Zealand
Age group (years)
Adequate Intake of riboflavin (mg/d)
Upper level of intake
0–6 months
0.3*
ND
7–12 months
0.4*
1–3
0.5
4–8
0.6
9–13
0.9
Females 14–70
1.1
Males 14–70
1.3
Females >70
1.3
Males >70
1.6
Pregnant females 14–50
1.4
Lactating females 14–50
1.6
* Adequate intake for infants, no RDA/RDI yet established
[/stextbox]
Uses & Health Benefit
Prevent riboflavin deficiency and to treat ariboflavinosis – Whenever possible, poor dietary habits should be corrected, and many clinicians recommend administration of multivitamin preparations containing riboflavin in patients with vitamin deficiencies since poor dietary habits often result in concurrent deficiencies.
Riboflavin – may be useful in treating microcytic anemia that occurs in patients with a familial metabolic disease associated with splenomegaly and glutathione reductase deficiency. Although riboflavin has not been shown by well-controlled trials to have any therapeutic value, the drug also has been used for the management of acne, congenital methemoglobinemia, muscle cramps, and burning feet syndrome.
People undergoing hemodialysis – or peritoneal dialysis and those with severe malabsorption are likely to require extra riboflavin. Women who are carrying more than one fetus or breastfeeding more than one infant are also likely to require more riboflavin. It is possible that individuals who are ordinarily extremely physically active may also have increased needs for riboflavin.
Preventing and treating low riboflavin levels (riboflavin deficiency) – In adults and children who have too little riboflavin in their body, taking riboflavin by mouth can increase levels of riboflavin in the body.
Cataracts – People who eat more riboflavin as part of their diet seem to have a lower risk of developing cataracts. Also, taking supplements containing riboflavin plus niacin seems to help prevent cataracts.
High amounts of homocysteine in the blood (hyperhomocysteinemia) – Taking riboflavin by mouth for 12 weeks decrease levels of homocysteine by up to 40% in some people. Also, taking riboflavin along with folic acid and pyridoxine seems to lower homocysteine levels by 26% in people with high homocysteine levels caused by drugs that are used to prevent seizures.
Migraine headaches – Taking high-dose riboflavin by mouth seems to reduce the number of migraine headache attacks, by about 2 attacks per month. Taking riboflavin in combination with other vitamin and minerals seems to also reduce the amount of pain experienced during a migraine.
Possibly Ineffective for
Stomach cancer – Taking riboflavin along with niacin does help prevent gastric cancer.
Malnutrition caused by too little protein in the diet (kwashiorkor) – Some research suggests that taking riboflavin, vitamin E, selenium, and N-acetyl cysteine by mouth does not reduce fluid, increase height or weight, or decrease infections in children at risk for kwashiorkor.
Lung cancer -Taking riboflavin by mouth along with niacin does not help prevent lung cancer.
Malaria – Taking riboflavin along with iron, thiamine, and vitamin C by mouth does not reduce the number or seriousness of malaria infections in children at risk of being exposed to malaria.
High blood pressure during pregnancy (pre-eclampsia) – In women that are 4 months pregnant, starting to take riboflavin by mouth does reduce the risk of pre-eclampsia during pregnancy.
Early research shows that taking riboflavin by mouth might be helpful for treating lactic acidosis caused by drugs called nucleoside analog reverse transcriptase inhibitors (NRTIs) in patients with acquired immunodeficiency syndrome (AIDS).
Increasing intake of riboflavin from dietary and supplement sources, along with thiamine, folic acid, and vitamin B12, might decrease the risk of developing cervical cancer.
Research on the effects of riboflavin for preventing esophageal cancer is conflicting. Some research shows that taking riboflavin by mouth may decrease the risk of getting esophageal cancer, while other research shows that it has no effect.
Early research shows that taking riboflavin by mouth in certain patients at higher risk of high blood pressure due to genetic differences may lower blood pressure when used in addition to prescribed blood pressure medications.
Early research shows that taking riboflavin and niacin by mouth might reduce the risk of liver cancer in people less than 55 years old. However, it does not seem to reduce the risk of liver cancer in older people.
Early research shows that taking riboflavin by mouth for 6 months does not improve disability in patients with multiple sclerosis.
Early research shows that low levels of riboflavin in the blood are linked with an increased risk of oral leukoplakia. However, taking riboflavin supplements by mouth for 20 months does not seem to prevent or treat oral leukoplakia.
Early research shows that taking riboflavin, iron, and folic acid by mouth does not increase iron levels in pregnant women more than taking just iron and folic acid.
Early research shows that taking riboflavin by mouth for 8 weeks increases iron levels in people with low iron levels due to sickle cell disease.
Early research shows that taking riboflavin and niacin by mouth does not prevent stroke-related death in people at risk for stroke.
Acne.
Aging.
Boosting the immune system.
Canker sores.
Maintaining healthy skin and hair.
Memory loss including Alzheimer’s disease.
Muscle cramps.
[stextbox id=’warning’]
Drug Warnings
Riboflavin may cause urine to have a more yellow color than normal, especially if large doses are taken. This is to be expected and is no cause for alarm. Usually, however, riboflavin does not cause any side effects.
Signs and Symptoms of Thiamine (Vitamin B1) Deficiency/Thiamine is a vitamin found in food and manufactured as a dietary supplement and medication. Food sources of thiamine include whole grains, legumes, and some meats and fish. Grain processing removes much of the thiamine content, so in many countries, cereals and flours are enriched with thiamine. Supplements and medications are available to treat and prevent thiamine deficiency and disorders that result from it, including beriberi and Wernicke encephalopathy. Other uses include the treatment of maple syrup urine disease and Leigh syndrome. They are typically taken by mouth, but may also be given by intravenous or intramuscular injection.
Thiamine also is known as thiamin or vitamin B1, is a vitamin found in food, and manufactured as a dietary supplement and medication.[rx][rx]Food sources of thiamine include whole grains, legumes, and some meats and fish.[rx] Grain processing removes much of the thiamine content, so in many countries, cereals and flours are enriched with thiamine.[rx][rx] Supplements and medications are available to treat and prevent thiamine deficiency and disorders that result from it, including beriberi and Wernicke encephalopathy.[rx] Other uses include the treatment of maple syrup urine disease and Leigh syndrome.[rx] They are typically taken by mouth, but may also be given by intravenous or intramuscular injection.[rx][rx]
Recommended Intakes of Vitamin B1 / Thiamine
Intake recommendations for thiamin and other nutrients are provided in the Dietary Reference Intakes (DRIs) developed by the Food and Nutrition Board (FNB) at the Institute of Medicine of the National Academies (formerly National Academy of Sciences). DRI is the general term for a set of reference values used for planning and assessing nutrient intakes of healthy people. These values, which vary by age and sex, include:
Recommended Dietary Allowance (RDA) – Average daily level of intake sufficient to meet the nutrient requirements of nearly all (97%–98%) healthy individuals; often used to plan nutritionally adequate diets for individuals.
Adequate Intake (AI) – Intake at this level is assumed to ensure nutritional adequacy; established when evidence is insufficient to develop an RDA.
Estimated Average Requirement (EAR) – Average daily level of intake estimated to meet the requirements of 50% of healthy individuals; usually used to assess the nutrient intakes of groups of people and to plan nutritionally adequate diets for them; can also be used to assess the nutrient intakes of individuals.
Tolerable Upper Intake Level (UL) – Maximum daily intake unlikely to cause adverse health effects.
Table 1 lists the current RDA for thiamin. For infants from birth to 12 months, the FNB established an AI for thiamin that is equivalent to the mean intake of thiamin in healthy, breastfed infants.
[stextbox id=’info’]
Recommended Dietary Allowances (RDAs) for Thiamin
Age
Male
Female
Pregnancy
Lactation
Birth to 6 months*
0.2 mg
0.2 mg
7–12 months*
0.3 mg
0.3 mg
1–3 years
0.5 mg
0.5 mg
4–8 years
0.6 mg
0.6 mg
9–13 years
0.9 mg
0.9 mg
14–18 years
1.2 mg
1.0 mg
1.4 mg
1.4 mg
19-50 years
1.2 mg
1.1 mg
1.4 mg
1.4 mg
51+ years
1.2 mg
1.1 mg
*AI
United States
Age group
RDA (mg/day)
Tolerable upper intake level
Infants 0–6 months
0.2*
ND
Infants 6–12 months
0.3*
1–3 years
0.5
4–8 years
0.6
9–13 years
0.9
Females 14–18 years
1.0
Males 14+ years
1.2
Females 19+ years
1.1
Pregnant/lactating females 14–50
1.4
* Adequate intake for infants, as an RDA has yet to be established
European Food Safety Authority
Age group
Adequate Intake (mg/MJ)
Tolerable upper limit
All persons 7 months+
0.1
ND
[/stextbox]
Deficiency Symptoms of Vitamin B1 / Thiamine
Beriberi
Symptoms of beriberi include weight loss, emotional disturbances, impaired sensory perception, weakness and pain in the limbs, and periods of irregular heart rate. Edema (swelling of bodily tissues) is common. It may increase the amount of lactic acid and pyruvic acid within the blood. In advanced cases, the disease may cause high-output cardiac failure and death.
Symptoms may occur concurrently with those of Wernicke’s encephalopathy, a primarily neurological thiamine-deficiency related condition.
Beriberi is divided into four categories as follows. The first three are historical and the fourth, gastrointestinal beriberi, was recognized in 2004:
Dry beriberi – especially affects the peripheral nervous system.
Wet beriberi – especially affects the cardiovascular system and other bodily systems.
Infantile beriberi – affects the babies of malnourished mothers.
Gastrointestinal beriberi – affects the digestive system and other bodily systems.
Dry beriberi
Dry beriberi causes wasting and partial paralysis resulting from damaged peripheral nerves. It is also referred to as endemic neuritis. It is characterized by:
Difficulty in walking
Tingling or loss of sensation (numbness) in hands and feet
Loss of tendon reflexes
Loss of muscle function or paralysis of the lower legs
Mental confusion/speech difficulties
Pain
Involuntary eye movements (nystagmus)
Vomiting
A selective impairment of the large proprioceptive sensory fibers without motor impairment can occur and present as prominent sensory ataxia, which is a loss of balance and coordination due to loss of the proprioceptive inputs from the periphery and loss of position sense.
Brain disease
Wernicke’s encephalopathy is the most frequently encountered manifestation of thiamine deficiency in Western society, though it may also occur in patients with impaired nutrition from other causes, such as gastrointestinal disease, those with HIV/AIDS, and with the injudicious administration of parenteral glucose or hyperalimentation without adequate B-vitamin supplementation. This is a striking neuro-psychiatric disorder characterized by paralysis of eye movements, abnormal stance and gait, and markedly deranged mental function.
Korsakoff’s syndrome is, in general, considered to occur with the deterioration of brain function in patients initially diagnosed with WE. This is an amnestic-confabulatory syndrome characterized by retrograde and anterograde amnesia, impairment of conceptual functions, and decreased spontaneity and initiative.
Alcoholics may have thiamine deficiency because of the following:
Inadequate nutritional intake – Alcoholics tend to intake less than the recommended amount of thiamine.
Decreased uptake of thiamine from the GI tract – Active transport of thiamine into enterocytes is disturbed during acute alcohol exposure.
Liver thiamine stores – are reduced due to hepatic steatosis or fibrosis.
Impaired thiamine utilization – Magnesium, which is required for the binding of thiamine to thiamine-using enzymes within the cell, is also deficient due to chronic alcohol consumption. The inefficient utilization of any thiamine that does reach the cells will further exacerbate the thiamine deficiency.
Ethanol per se inhibits thiamine – transport in the gastrointestinal system and blocks phosphorylation of thiamine to its cofactor form (ThDP).
Following improved nutrition and the removal of alcohol consumption, some impairments linked with thiamine deficiency are reversed, in particular poor brain functionality, although in more severe cases, Wernicke–Korsakoff syndrome leaves permanent damage.
Wet beriberi
Wet beriberi affects the heart and circulatory system. It is sometimes fatal, as it causes a combination of heart failure and weakening of the capillary walls, which causes the peripheral tissues to become edematous. Wet beriberi is characterized by:
Increased heart rate
Vasodilation leading to decreased systemic vascular resistance, and high output heart failure
Elevated jugular venous pressure
Dyspnea (shortness of breath) on exertion
Paroxysmal nocturnal dyspnea
Peripheral edema (swelling of lower legs)
Dilated cardiomyopathy
Gastrointestinal beriberi
Gastrointestinal beriberi causes abdominal pain. Gastrointestinal beriberi is characterized by:
Infantile beriberi usually occurs between two and six months of age in children whose mothers have inadequate thiamine intake. It may present as either wet or dry beriberi.
In the acute form, the baby develops dyspnea and cyanosis and soon dies of heart failure. These symptoms may be described in infantile beriberi:
Hoarseness, where the child makes moves to moan but emits no sound or just faint moans caused by nerve paralysis
Weight loss, becoming thinner and then marasmic as the disease progresses
Alterations of the cardiovascular system, especially tachycardia (rapid heart rate)
Convulsions occasionally observed in the terminal stages
Food Source of Vitamin B1 / Thiamine
[stextbox id=’info’]
Selected Food Sources of Thiamin
Food
Milligrams
(mg) per
serving
Percent
DV*
Breakfast cereals, fortified with 100% of the DV for thiamin, 1 serving
1.5
100
Rice, white, long grain, enriched, parboiled, ½ cup
1.4
73
Egg noodles, enriched, cooked, 1 cup
0.5
33
Pork chop, bone-in, broiled, 3 ounces
0.4
27
Trout, cooked, dry heat, 3 ounces
0.4
27
Black beans, boiled, ½ cup
0.4
27
English muffin, plain, enriched, 1 muffin
0.3
20
Mussels, blue, cooked, moist heat, 3 ounces
0.3
20
Tuna, Bluefin, cooked, dry heat, 3 ounces
0.2
13
Macaroni, whole wheat, cooked, 1 cup
0.2
13
Acorn squash, cubed, baked, ½ cup
0.2
13
Rice, brown, long grain, not enriched, cooked, ½ cup
0.1
7
Bread, whole wheat, 1 slice
0.1
7
Orange juice, prepared from concentrate, 1 cup
0.1
7
Sunflower seeds, toasted, 1 ounce
0.1
7
Beef steak, bottom round, trimmed of fat, braised, 3 ounces
0.1
7
Yogurt, plain, low fat, 1 cup
0.1
7
Oatmeal, regular and quick, unenriched, cooked with water, ½ cup
0.1
7
Corn, yellow, boiled, 1 medium ear
0.1
7
Milk, 2%, 1 cup
0.1
7
Barley, pearled, cooked, 1 cup
0.1
7
Cheddar cheese, 1½ ounces
0
0
Chicken, meat and skin, roasted, 3 ounces
0
0
Apple, sliced, 1 cup
0
0
*DV = Daily Value. DVs were developed by the U.S. Food and Drug Administration (FDA) to help consumers compare the nutrient contents of products within the context of a total diet. The DV for thiamin is 1.5 mg for adults and children age 4 and older. Foods providing 20% or more of the DV are considered to be high sources of a nutrient.
The U.S. Department of Agriculture’s (USDA’s) Nutrient Database website lists the nutrient content of many foods and provides a comprehensive list of foods containing thiamin arranged by nutrient content and by food name.
[/stextbox]
Uses & Health Benefit of Vitamin B1 / Thiamine
Effective for
Metabolic disorders – Taking thiamine by mouth helps correct metabolic disorders associated with genetic diseases, including Leigh’s disease, maple syrup urine disease, and others.
Thiamine deficiency – Taking thiamine by mouth helps prevent and treat thiamine deficiency.
Brain disorder due to thiamine deficiency (Wernicke-Korsakoff syndrome) – Thiamine helps decrease the risk and symptoms of a specific brain disorder called Wernicke-Korsakoff syndrome (WKS). This brain disorder is related to low levels of thiamine (thiamine deficiency) and is often seen in alcoholics. Between 30% and 80% of alcoholics are believed to have thiamine deficiency. Giving thiamine shots seems to help decrease the risk of developing WKS and decrease symptoms of WKS during alcohol withdrawal.
Cataracts – High thiamine intake as part of the diet is associated with a reduced risk of developing cataracts.
Kidney disease in people with diabetes – Early research shows that taking high-dose thiamine (100 mg three times daily) for 3 months decreases the amount of albumin in the urine in people with type 2 diabetes. Albumin in the urine is an indication of kidney damage.
Painful menstruation (dysmenorrhea) – Early research suggests that taking thiamine for 90 days stops pain associated with menstruation in girls 12-21 years-old.
Repelling mosquitos. Some research shows that taking B vitamins, including thiamine, does not help repel mosquitos.
Insufficient Evidence for
Athletic performance – Some research suggests that taking thiamine together with pantethine and pantothenic acid (vitamin B5) does not improve muscle strength or endurance in athletes.
Preventing cervical cancer – Some research suggests that increasing intake of thiamine from dietary and supplement sources, along with another folic acid, riboflavin, and vitamin B12, might decrease the risk of precancerous spots on the cervix.
Vitamin B1 For Skin Brightness/Thiamine is a vitamin found in food and manufactured as a dietary supplement and medication. Food sources of thiamine include whole grains, legumes, and some meats and fish. Grain processing removes much of the thiamine content, so in many countries, cereals and flours are enriched with thiamine. Supplements and medications are available to treat and prevent thiamine deficiency and disorders that result from it, including beriberi and Wernicke encephalopathy. Other uses include the treatment of maple syrup urine disease and Leigh syndrome. They are typically taken by mouth, but may also be given by intravenous or intramuscular injection.
Thiamine also is known as thiamin or vitamin B1, is a vitamin found in food, and manufactured as a dietary supplement and medication.[rx][rx]Food sources of thiamine include whole grains, legumes, and some meats and fish.[rx] Grain processing removes much of the thiamine content, so in many countries, cereals and flours are enriched with thiamine.[rx][rx] Supplements and medications are available to treat and prevent thiamine deficiency and disorders that result from it, including beriberi and Wernicke encephalopathy.[rx] Other uses include the treatment of maple syrup urine disease and Leigh syndrome.[rx] They are typically taken by mouth, but may also be given by intravenous or intramuscular injection.[rx][rx]
Recommended Intakes of Vitamin B1 / Thiamine
Intake recommendations for thiamin and other nutrients are provided in the Dietary Reference Intakes (DRIs) developed by the Food and Nutrition Board (FNB) at the Institute of Medicine of the National Academies (formerly National Academy of Sciences). DRI is the general term for a set of reference values used for planning and assessing nutrient intakes of healthy people. These values, which vary by age and sex, include:
Recommended Dietary Allowance (RDA) – Average daily level of intake sufficient to meet the nutrient requirements of nearly all (97%–98%) healthy individuals; often used to plan nutritionally adequate diets for individuals.
Adequate Intake (AI) – Intake at this level is assumed to ensure nutritional adequacy; established when evidence is insufficient to develop an RDA.
Estimated Average Requirement (EAR) – Average daily level of intake estimated to meet the requirements of 50% of healthy individuals; usually used to assess the nutrient intakes of groups of people and to plan nutritionally adequate diets for them; can also be used to assess the nutrient intakes of individuals.
Tolerable Upper Intake Level (UL) – Maximum daily intake unlikely to cause adverse health effects.
Table 1 lists the current RDA for thiamin. For infants from birth to 12 months, the FNB established an AI for thiamin that is equivalent to the mean intake of thiamin in healthy, breastfed infants.
[stextbox id=’info’]
Recommended Dietary Allowances (RDAs) for Thiamin
Age
Male
Female
Pregnancy
Lactation
Birth to 6 months*
0.2 mg
0.2 mg
7–12 months*
0.3 mg
0.3 mg
1–3 years
0.5 mg
0.5 mg
4–8 years
0.6 mg
0.6 mg
9–13 years
0.9 mg
0.9 mg
14–18 years
1.2 mg
1.0 mg
1.4 mg
1.4 mg
19-50 years
1.2 mg
1.1 mg
1.4 mg
1.4 mg
51+ years
1.2 mg
1.1 mg
*AI
United States
Age group
RDA (mg/day)
Tolerable upper intake level
Infants 0–6 months
0.2*
ND
Infants 6–12 months
0.3*
1–3 years
0.5
4–8 years
0.6
9–13 years
0.9
Females 14–18 years
1.0
Males 14+ years
1.2
Females 19+ years
1.1
Pregnant/lactating females 14–50
1.4
* Adequate intake for infants, as an RDA has yet to be established
European Food Safety Authority
Age group
Adequate Intake (mg/MJ)
Tolerable upper limit
All persons 7 months+
0.1
ND
[/stextbox]
Deficiency Symptoms of Vitamin B1 / Thiamine
Beriberi
Symptoms of beriberi include weight loss, emotional disturbances, impaired sensory perception, weakness and pain in the limbs, and periods of irregular heart rate. Edema (swelling of bodily tissues) is common. It may increase the amount of lactic acid and pyruvic acid within the blood. In advanced cases, the disease may cause high-output cardiac failure and death.
Symptoms may occur concurrently with those of Wernicke’s encephalopathy, a primarily neurological thiamine-deficiency related condition.
Beriberi is divided into four categories as follows. The first three are historical and the fourth, gastrointestinal beriberi, was recognized in 2004:
Dry beriberi – especially affects the peripheral nervous system.
Wet beriberi – especially affects the cardiovascular system and other bodily systems.
Infantile beriberi – affects the babies of malnourished mothers.
Gastrointestinal beriberi – affects the digestive system and other bodily systems.
Dry beriberi
Dry beriberi causes wasting and partial paralysis resulting from damaged peripheral nerves. It is also referred to as endemic neuritis. It is characterized by:
Difficulty in walking
Tingling or loss of sensation (numbness) in hands and feet
Loss of tendon reflexes
Loss of muscle function or paralysis of the lower legs
Mental confusion/speech difficulties
Pain
Involuntary eye movements (nystagmus)
Vomiting
A selective impairment of the large proprioceptive sensory fibers without motor impairment can occur and present as prominent sensory ataxia, which is a loss of balance and coordination due to loss of the proprioceptive inputs from the periphery and loss of position sense.
Brain Disease
Wernicke’s encephalopathy is the most frequently encountered manifestation of thiamine deficiency in Western society, though it may also occur in patients with impaired nutrition from other causes, such as gastrointestinal disease, those with HIV/AIDS, and with the injudicious administration of parenteral glucose or hyperalimentation without adequate B-vitamin supplementation. This is a striking neuro-psychiatric disorder characterized by paralysis of eye movements, abnormal stance and gait, and markedly deranged mental function.
Korsakoff’s syndrome is, in general, considered to occur with the deterioration of brain function in patients initially diagnosed with WE. This is an amnestic-confabulatory syndrome characterized by retrograde and anterograde amnesia, impairment of conceptual functions, and decreased spontaneity and initiative.
Alcoholics may have thiamine deficiency because of the following
Inadequate nutritional intake – Alcoholics tend to intake less than the recommended amount of thiamine.
Decreased uptake of thiamine from the GI tract – Active transport of thiamine into enterocytes is disturbed during acute alcohol exposure.
Liver thiamine stores – are reduced due to hepatic steatosis or fibrosis.
Impaired thiamine utilization – Magnesium, which is required for the binding of thiamine to thiamine-using enzymes within the cell, is also deficient due to chronic alcohol consumption. The inefficient utilization of any thiamine that does reach the cells will further exacerbate the thiamine deficiency.
Ethanol per se inhibits thiamine – transport in the gastrointestinal system and blocks phosphorylation of thiamine to its cofactor form (GDP).
Following improved nutrition and the removal of alcohol consumption, some impairments linked with thiamine deficiency are reversed, in particular poor brain functionality, although in more severe cases, Wernicke–Korsakoff syndrome leaves permanent damage.
Wet beriberi
Wet beriberi affects the heart and circulatory system. It is sometimes fatal, as it causes a combination of heart failure and weakening of the capillary walls, which causes the peripheral tissues to become edematous. Wet beriberi is characterized by:
Increased heart rate
Vasodilation leading to decreased systemic vascular resistance, and high output heart failure
Elevated jugular venous pressure
Dyspnea (shortness of breath) on exertion
Paroxysmal nocturnal dyspnea
Peripheral edema (swelling of lower legs)
Dilated cardiomyopathy
Gastrointestinal beriberi
Gastrointestinal beriberi causes abdominal pain. Gastrointestinal beriberi is characterized by:
Infantile beriberi usually occurs between two and six months of age in children whose mothers have inadequate thiamine intake. It may present as either wet or dry beriberi.
In the acute form, the baby develops dyspnea and cyanosis and soon dies of heart failure. These symptoms may be described in infantile beriberi:
Hoarseness, where the child makes moves to moan but emits no sound or just faint moans caused by nerve paralysis
Weight loss, becoming thinner and then marasmic as the disease progresses
Alterations of the cardiovascular system, especially tachycardia (rapid heart rate)
Convulsions occasionally observed in the terminal stages
Food Source of Vitamin B1 / Thiamine
[stextbox id=’info’]
Selected Food Sources of Thiamin
Food
Milligrams
(mg) per
serving
Percent
DV*
Breakfast cereals, fortified with 100% of the DV for thiamin, 1 serving
1.5
100
Rice, white, long grain, enriched, parboiled, ½ cup
1.4
73
Egg noodles, enriched, cooked, 1 cup
0.5
33
Pork chop, bone-in, broiled, 3 ounces
0.4
27
Trout, cooked, dry heat, 3 ounces
0.4
27
Black beans, boiled, ½ cup
0.4
27
English muffin, plain, enriched, 1 muffin
0.3
20
Mussels, blue, cooked, moist heat, 3 ounces
0.3
20
Tuna, Bluefin, cooked, dry heat, 3 ounces
0.2
13
Macaroni, whole wheat, cooked, 1 cup
0.2
13
Acorn squash, cubed, baked, ½ cup
0.2
13
Rice, brown, long-grain, not enriched, cooked, ½ cup
0.1
7
Bread, whole wheat, 1 slice
0.1
7
Orange juice, prepared from concentrate, 1 cup
0.1
7
Sunflower seeds, toasted, 1 ounce
0.1
7
Beefsteak, bottom round, trimmed of fat, braised, 3 ounces
0.1
7
Yogurt, plain, low fat, 1 cup
0.1
7
Oatmeal, regular and quick, unenriched, cooked with water, ½ cup
0.1
7
Corn, yellow, boiled, 1 medium ear
0.1
7
Milk, 2%, 1 cup
0.1
7
Barley, pearled, cooked, 1 cup
0.1
7
Cheddar cheese, 1½ ounces
0
0
Chicken, meat, and skin, roasted, 3 ounces
0
0
Apple, sliced, 1 cup
0
0
*DV = Daily Value. DVs were developed by the U.S. Food and Drug Administration (FDA) to help consumers compare the nutrient contents of products within the context of a total diet. The DV for thiamin is 1.5 mg for adults and children age 4 and older. Foods providing 20% or more of the DV are considered to be high sources of a nutrient.
The U.S. Department of Agriculture’s (USDA’s) Nutrient Database website lists the nutrient content of many foods and provides a comprehensive list of foods containing thiamin arranged by nutrient content and by food name.
[/stextbox]
Uses & Health Benefit of Vitamin B1 / Thiamine
Effective for
Metabolic disorders – Taking thiamine by mouth helps correct metabolic disorders associated with genetic diseases, including Leigh’s disease, maple syrup urine disease, and others.
Thiamine deficiency – Taking thiamine by mouth helps prevent and treat thiamine deficiency.
Brain disorder due to thiamine deficiency (Wernicke-Korsakoff syndrome) – Thiamine helps decrease the risk and symptoms of a specific brain disorder called Wernicke-Korsakoff syndrome (WKS). This brain disorder is related to low levels of thiamine (thiamine deficiency) and is often seen in alcoholics. Between 30% and 80% of alcoholics are believed to have thiamine deficiency. Giving thiamine shots seems to help decrease the risk of developing WKS and decrease symptoms of WKS during alcohol withdrawal.
Cataracts – High thiamine intake as part of the diet is associated with a reduced risk of developing cataracts.
Kidney disease in people with diabetes – Early research shows that taking high-dose thiamine (100 mg three times daily) for 3 months decreases the amount of albumin in the urine in people with type 2 diabetes. Albumin in the urine is an indication of kidney damage.
Painful menstruation (dysmenorrhea) – Early research suggests that taking thiamine for 90 days stops pain associated with menstruation in girls 12-21 years-old.
Repelling mosquitos. Some research shows that taking B vitamins, including thiamine, does not help repel mosquitos.
Insufficient Evidence for
Athletic performance – Some research suggests that taking thiamine together with pantethine and pantothenic acid (vitamin B5) does not improve muscle strength or endurance in athletes.
Preventing cervical cancer – Some research suggests that increasing intake of thiamine from dietary and supplement sources, along with another folic acid, riboflavin, and vitamin B12, might decrease the risk of precancerous spots on the cervix.
Confusion Diagnosis/Confusion is a common neuropsychiatric syndrome in the elderly. The DSM-IV-TR defines delirium as a “disturbance of consciousness and a change in cognition that develop ois a common neuropsychiatric syndrome in the elderly. The DSM-IV-TR defines delirium as a “disturbance of consciousness and a change in cognition that develop over a short period of time. The syndrome includes fluctuations in consciousness over the course of the day, a reduced ability to focus, sustain and shift attention, and evidence that the disturbance is caused by the direct physiological consequence of a medical condition [rx].
In general, the prevalence of delirium is dependent on several factors, including the patient population, care setting, the method of study and diversity of antecedent events. The prevalence of delirium in the community is 1–2%, but increases in the setting of general hospital admissions to 6–56% [rx], with the higher prevalence associated with increased age [rx] and increased severity of medical illness [rx].
Pathophysiology
Alcohol acts as central nervous system depressant. It enhances the effect of inhibitory neurotransmitters while down-regulating excitatory neurotransmitters. Alcohol interacts with GABA receptors, chloride ion receptor acting as an inhibitory neurotransmitter, via several mechanisms to enhance its activity. Over time, through prolonged alcohol exposure, there is a decrease in GABA activity and alteration in the type of GABA receptor and function. Abrupt cessation of alcohol causes a decrease in the inhibitory actions of GABA neurotransmitter resulting in overactivity of the central nervous system.
Alcohol also inhibits the action of NMDA receptor by acting as a receptor antagonist. It inhibits the action of glutamate, which is an excitatory amino acid. Prolonged alcohol abuse results in receptor up-regulation. Abrupt discontinuation of alcohol causes an increase in the action of glutamate, resulting in profound excitatory action. This may have a clinical manifestation of sympathetic overdrive, such as agitation, tremors, tachycardia, and hypertension.
Certain individuals are more vulnerable to suffer from withdrawal symptoms than others. Though the etiology remains unclear, there is a correlation between the duration of alcohol exposure and withdrawal symptoms.[rx][rx]
Types of Confusion
There are three types of delirium
Hypoactive – meaning that the person acts sleepy or withdrawn
Hyperactive – meaning that a person is agitated
Mixed – meaning that a person alternates between these two types
Delirium subtypes have been defined based on the presence (hyperactive) or absence (hypoactive) of psychomotor agitation, perceptual disturbances, and/or changes in level of consciousness.[rx] Often both subtypes are present concurrently (mixed).[rx–rx]
Causes of Confusion
Mental confusion can result from chronic organic brain pathologies, such as dementia, as well.
Neuroinflammation – Patients who develop delirium have shown an elevated PCR and Cortisol, although IL-8 is prevalent among patients in and out of ICU. The cytokines activate the endothelium and the coagulation cascade, which predisposes to microvascular thrombosis and blood flow dysfunction. The neuroinflammation leads to infiltrate cytokines and leukocytes to the hematoencephalic barrier and then in the central nervous system in which produce ischemia and neuronal apoptosis.
Cholinergic Deficiency Hypothesis – Acetylcholine is a very important neurotransmitter in attention and consciousness. It is known, acetylcholine acts as a modulator in sensory and cognitive input so, an impairment in the route leads to develop symptoms of hypoactive or hyperactive delirium, including inattention, disorganized thinking, and perceptual disturbances. Cholinergic pathways project from basal forebrain and pontomesencephalon to interneurons in the striatum and finally targets throughout the cortex.
Neurotransmitter Imbalance – The dopamine excess contributes to hyperactive delirium and is related to decreased acetylcholine. The dopaminergic and cholinergic pathways overlap in the brain, this explains why dopamine receptors impact acetylcholine levels and explain the clinical manifestations of delirium, including hyperactive and hypoactive forms. The imbalance between neurotransmitter and cholinergic pathway may result in delirium.
Chronic Stress – Activates the sympathetic nervous system and de hypothalamus-hypophysis-suprarenal glands axis, which elevate the cytokines levels and results in chronic hypercortisolism that can cause an alteration in the hippocampus function. Cortisol is the main hormone in response to stress and has deleterious effects among 5HT 1A receptors. The association between this receptors and delirium is not conclusive. High cortisol levels produce a reduction in GABA release and impairment in neuronal energy bombs.
Medications (for example, sedative hypnotics, narcotics, anticholinergic drugs, corticosteroids, polypharmacy, withdrawal of alcohol or other drugs)
Acute neurological diseases (for example, acute stroke [usually right parietal], intracranial hemorrhage, meningitis, enkephalitis)
Intercurrent illness (for example, infections, iatrogenic complications, severe acute illness, anemia, dehydration, poor nutritional status, fracture or trauma, HIV infection)
Metabolic derangement
Surgery
Environment (for example, admission to an intensive care unit)
Pain
Emotional distress
Sustained sleep deprivation
Nonmodifiable risk factors
Dementia or cognitive impairment
Advancing age (>65 years)
History of delirium, stroke, neurological disease, falls or gait disorder
Multiple comorbidities
Male sex
Chronic renal or hepatic disease
Predisposing Factors
The most important predisposing factors are listed below:[rx]
Functional dependence (e.g., requiring assistance for self-care or mobility)
Dehydration/malnutrition
Drugs and drug-dependence
Alcohol dependence
Precipitating Factors
Acute confusional state caused by alcohol withdrawal, also known as delirium tremens. Any acute factors that affect neurotransmitter, neuroendocrine, or neuroinflammatory pathways can precipitate an episode of delirium in a vulnerable brain.[rx] Clinical environments can also precipitate delirium.[rx] Some of the most common precipitating factors are listed below
Severe drop in blood pressure, relative to the patient’s normal blood pressure (orthostatic hypotension) resulting in inadequate blood flow to the brain (cerebral hypoperfusion)
Stroke/transient ischemic attack
Intracranial bleeding
Meningitis, encephalitis
Concurrent Illness
Infections – especially respiratory (e.g. pneumonia) and urinary tract infections
In surgery of cardiac, orthopedic, prolonged cardiopulmonary bypass, thoracic surgeries
Symptoms of Confusion
Inattention – As a required symptom to diagnose delirium, this is characterized by distractibility and an inability to shift and/or sustain attention.[rx]
Memory impairment – Memory impairment is linked to inattention, especially reduced formation of new long-term memory where higher degrees of attention is more necessary than for short-term memory. Since older memories are retained without need of concentration, previously formed long-term memories (i.e. those formed before the onset of delirium) are usually preserved in all but the most severe cases of delirium.
Disorientation – As another symptom of confusion, and usually a more severe one, this describes the loss of awareness of the surroundings, environment and context in which the person exists. One may be disoriented to time, place, or self.
Disorganized thinking – Disorganized thinking is usually noticed with speech that makes limited sense with apparent irrelevancies, and can involve poverty of speech, loose associations, perseveration, tangentiality, and other signs of a formal thought disorder.
Language disturbances – Anomic aphasia, paraphasia, impaired comprehension, agraphia, and word-finding difficulties all involve impairment of linguistic information processing.
Sleep changes – Sleep disturbances in delirium reflect disturbed circadian rhythm regulation, typically involving fragmented sleep or even sleep-wake cycle reversal (i.e. active at night, sleeping during the day) and often preceding the onset of a delirium episode
Psychotic symptoms – Symptoms of psychosis include suspiciousness, overvalued ideation and frank delusions. Delusions are typically poorly formed and less stereotyped than in schizophrenia or Alzheimer’s disease. They usually relate to persecutory themes of impending danger or threat in the immediate environment (e.g. being poisoned by nurses).
Mood lability – Distortions to perceived or communicated emotional states as well as fluctuating emotional states can manifest in a delirious person (e.g. rapid changes between terror, sadness and joking).[rx]
Motor activity changes: Delirium has been commonly classified into psychomotor subtypes of hypoactive, hyperactive, and mixed,[rx] though studies are inconsistent as to the prevalence of these subtypes.[rx] Hypoactive cases are prone to non-detection or misdiagnosis as depression.
Hyperactive symptoms include hyper-vigilance, restlessness, fast or loud speech, irritability, combativeness, impatience, swearing, singing, laughing, uncooperativeness, euphoria, anger, wandering, easy startling, fast motor responses, distractibility, tangentiality, nightmares, and persistent thoughts (hyperactive sub-typing is defined with at least three of the above).[rx]
Hypoactive symptoms include unawareness, decreased alertness, sparse or slow speech, lethargy, slowed movements, staring, and apathy (hypoactive sub-typing is defined with at least four of the above).[rx]
Having trouble solving problems or doing tasks that used to be easy for you.
Not knowing where you are or not recognizing family members or familiar items.
Firmly held but false beliefs (delusions).
Seeing, hearing, feeling, smelling, or tasting things that are not really there (hallucinations or illusions).
Unfounded suspicions that others are after you or want to harm you (paranoia).
Diagnosis of Confusion
Another symptom of confusion is an immense difficulty attempting to solve problems or accomplish tasks that were previously easy to perform. People suffering from confusion will also find it hard to recognize members of their own family, and even familiar objects.
Physical Examination
Examination, particularly in patients who are not fully cooperative, should focus on the following
Vital signs
Hydration status
Potential foci for infection
Skin and head and neck
Neurologic examination
Findings can suggest a cause, as with the following
Fever, meningismus, or Kernig and Brudzinski signs suggest CNS infection.
Tremor and myoclonus suggest uremia, liver failure, drug intoxication, or certain electrolyte disorders (eg, hypocalcemia, hypomagnesemia).
Ophthalmoplegia and ataxia suggest Wernicke-Korsakoff syndrome.
Focal neurologic abnormalities (eg, cranial nerve palsies, motor or sensory deficits) or papilledema suggests a structural CNS disorder.
Scalp or facial lacerations, bruising, swelling, and other signs of head trauma suggest traumatic brain injury.
A – Disturbance in consciousness with reduced ability to focus, sustain or shift attention.
B – A change in cognition or the development of a perceptual disturbance that is not better accounted for by a preexisting, established or evolving dementia.
C – The disturbance develops over a short period of time and tends to fluctuate over the course of the day.
D – There is evidence from history, physical examination, or laboratory findings that the disturbance is caused by the direct physiological consequences of a general medical condition.
CLINICAL SUBTYPES:
HYPERACTIVE – agitation, restlessness, with hallucinations and /or delusions
HYPOACTIVE – lethargic, difficult to arouse, minimal speech, psychomotor retardation
MIXED – symptoms of both hyperactive and hypoactive delirium
[/dropshadowbox]
The Confusion Assessment Method (CAM) Diagnostic Algorithm.
General diagnostic criteria
(A) Disturbance of consciousness (that is, reduced clarity of awareness of the environment) with reduced ability to focus, sustain, or shift attention
(B) A change in cognition (such as memory deficit, disorientation, language disturbance) or the development of a perceptual disturbance that is not better accounted for by a pre-existing, established, or evolving dementia
(C) The disturbance develops over a short period of time (usually hours to days) and tends to fluctuate during the course of the day
For delirium due to a general medical condition
(D) Evidence from the history, physical examination, or laboratory findings indicates that the disturbance is caused by the direct physiological consequences of a general medical condition
For substance intoxication delirium
(D) Evidence from the history, physical examination, or laboratory findings indicates that of either (1) the symptoms in Criteria A and B developed during substance intoxication, or (2) medication use is etiologically related to the disturbance
For substance withdrawal delirium
(D) History, physical examination, or laboratory findings indicate that the symptoms in Criteria A and B developed during, or shortly after, a withdrawal syndrome
For delirium due to multiple etiologies
(D) History, physical examination, or laboratory findings indicate that the delirium has more than one etiology (for example, more than one etiological general medical condition, a general medical condition plus substance intoxication or medication side effect)
Most widely used screening test for the presence of delirium; a four-item instrument based on
DSM-III-R delirium criteria, requires the presence of acute onset and fluctuating course,
inattention, and disorganized thinking or loss of consciousness
Delirium is diagnosed when patients demonstrate an acute change in mental status or fluctuating
changes in mental status, inattention measured with either an auditory or a visual test, and either
disorganized thinking or an altered level of consciousness. Importantly, the CAM–ICU can only be
administered if the patient is arousable in response to a voice without the need for physical
stimulation
16-item scale, including 13 severity items and 3 diagnostic items. Severity scores range from 0 to
39, with higher scores indicating more-severe delirium; delirium typically involves scores ≥15
points
A structured interview detects the presence or absence of seven DSM-III criteria for delirium;
delirium is said to be present if disorientation, perceptual disturbance or disturbance of
consciousness have presented within the past 24h
Nine scaled items divided into three subscales: subscale I, information processing (score range
0–14 points), evaluates components of cognitive status; subscale II, behavior (score range 0–10
points), evaluates observed behavior and performance ability; subscale III, performance (score
range 0–16 points), assesses vital function (that is, vital signs, oxygen saturation level and urinary
incontinence). Total scores can range from 0 (minimal function) to 30 (normal function). Delirium
is present if the score is ≤ 24 points
Bedside screening tool for delirium in the intensive care unit setting; eight-item checklist based on
DSM-IV® criteria, items scored as 1 (present) or 0 (absent); a score ≥ 4 points indicates delirium
Can be used with patients unable to speak or write; assesses orientation, attention, memory,
comprehension and vigilance, primarily with visual and auditory modalities. Each individual domain
is scored 0–6 in two-point increments, except for comprehension, which is scored in single-point
increments. Total scores range from 0 to 30, with higher scores indicating better cognitive function
Abbreviations: CAM, Confusion Assessment Method; CAM–ICU, Confusion Assessment Method–Intensive Care Unit; Drs-r98, Delirium Rating Scale; DSI, Delirium Symptom Interview; DSM, Diagnostic and Statistical Manual of Mental Disorders (American Psychiatric Association, Arlington, VA); ICDSC, Intensive Care Delirium Screening Checklist; MDAS, Memorial Delirium Assessment Scale.
[/dropshadowbox]
Laboratory testing – Blood and/or urine tests may be performed to determine the cause of the person’s delirium. Delirium may be the first manifestation of a severe infection or sepsis, so additional tests to identify infection may be done. A chest x-ray is often required to exclude pneumonia.
Brain imaging tests – If the cause of a person’s delirium cannot be determined based upon the history, physical examination, and laboratory testing, a computed tomography (CT) scan or magnetic resonance imaging (MRI) scan of the head may be recommended. This test can help to determine if an abnormal growth, bleeding, infection, or inflammation is present in the brain.
Lumbar puncture – During a lumbar puncture, or spinal tap, a clinician uses a needle to remove a sample of spinal fluid from the area around the spinal cord in the low back. Several tests are done on the fluid to determine if an infection (such as meningitis or encephalitis) could be causing delirium, and if so, which antibiotic treatment is best. Lumbar puncture is not recommended for every person with delirium. It may be performed if other tests are unable to determine the cause, or if there are other signs of central nervous system infection.
EEG testing – Electroencephalography (EEG) measures the electrical activity in the brain. It may be performed in a person with delirium to search for abnormal electrical activity that is commonly associated with seizures and epilepsy. It is not recommended for all people with delirium, but it may be performed if other tests are unable to determine the cause.
Differential Diagnosis
The differential diagnosis for DT includes the following
Sepsis
Uremia
Stroke
Meningitis
Encephalitis
Wernicke encephalopathy
Neuroleptic malignant syndrome
Pheochromocytoma
Drug toxicity such as with amphetamine, hallucinogen, cocaine, heroin, and PCP
Electrolyte abnormalities such as hypocalcemia and hypomagnesemia
Thyrotoxicosis
Cerebral hemorrhage
Cerebral embolism
Toxic ingestion or exposures (ethylene glycol)
Acute liver failure
Diabetic ketoacidosis
Brain abscess
Hypoglycemia
Treatment of Confusion
Any confusion that follows a trauma to the head, or immediately succeeding unconsciousness is a cause for serious concern. Even if the symptoms of confusion appear gradually over time, a person should consult a specialist for appropriate diagnosis and treatment.
There is no specific treatment for delirium. Instead, treatment focuses on several basic principles:
Avoid factors known to cause or aggravate delirium, such as certain medications
Identify and treat the underlying illness
Provide supportive and restorative care
Control dangerous and disruptive behaviors to avoid harm to the patient or others
In people with a first episode of delirium, the initial treatment is often provided in a hospital setting. This allows the health care provider to monitor the patient, begin treatment of the underlying problem, and develop a long-term care plan with the patient and/or family.
Supportive care –The goal of supportive care is to maintain the patient’s health, prevent additional complications, and avoid those factors that can aggravate delirium. This includes:
Making sure – the person gets enough to eat and drink (or providing nutrition through an IV, if needed)
Treating pain and avoiding discomfort – including avoiding constipation
Minimizing the use of restraints and bladder catheters – which can be uncomfortable, particularly to confused patients
Encouraging movement – (getting out of bed in order to walk) with necessary assistance to avoid falls
Having someone – help during meals and having the person sit upright to minimize the risk of inhaling food, drinks, and or saliva, which can lead to pneumonia
Maintaining – a regular night-day/sleep-wake cycle when possible and avoiding sleep deprivation, and maintaining a reassuring and familiar environment with one or two visiting family members or familiar objects pictures from home
Avoiding overstimulation – (eg, multiple visitors, loud noise), which can worsen delirium, but also avoiding understimulation (darkened room, complete silence)
Making hearing – aids and eyeglasses available at the hospital if the patient uses these at home
Managing behaviors – Some people with delirium have disruptive behaviors, potentially causing them to harm themselves or others. The person may say or do things that are obscene or offensive, but such behaviors do not reflect the person’s true beliefs. The person may also be at risk for falling, wandering off, or inadvertently removing intravenous lines.
Sitter – Allowing a family member or other caregiver to stay with the patient at the bedside may help to manage the patient’s behavior. This person can provide reassurance, answer questions, reorient the patient, and notify staff if the person needs assistance. In some cases, the hospital is able to provide a sitter if a family member is unavailable. However, a familiar and trusted family member or friend can provide additional reassurance to the patient.
Restraints – The use of restraints (to tie a person to their bed or chair) is almost never appropriate, as restraints can increase agitation and create additional problems by preventing the person from moving around as needed. Preventing movement also potentially allows skin sores (called pressure ulcers) to develop from sitting or lying in the same position for long periods. The use of restraints has not been shown to prevent harmful falls among hospitalized patients.
Medications— Medications to control difficult behavior are only to be considered as a last resort, if the patient’s agitation is so extreme as to be a potential source of harm. Some classes of drugs, especially sedatives such as lorazepam and diazepam, can build up in the bloodstream and cause the person to become more confused. Antipsychotic medications, such as haloperidol, may be considered, but only in small doses and for short periods of time. If necessary, these medications should be stopped frequently, with direction or approval by the physician, so that the patient can be reevaluated. Antipsychotic medications are not recommended for long-term treatment.
0.1 to 0.2 mg/kg loading dose repeated every 30 min until symptom control, then 25% of the total dose needed to control symptoms as a continuous infusion
SC/IM: 30 min
IV: 15 min
2 hr
Continuous infusion
240 mg/day
215 mg/kg
Phenobarbital
PO/PR: Start with 30–120 mg/day in two to three divided doses; SC/IV: 10–30 mg/kg loading dose, then 20–100 mg/hr continuous infusion
Did not show improvement in condition;
treatment limited by adverse effects[rx]
Cholinesterase inhibitors
Donepezil
5 mg QD
Nausea, vomiting, diarrhea
No randomized, controlled studies have been
conducted; some case studies have indicated
promise[rx–rx]
Prophylactic therapies (potential)
Antipsychotics
Haloperidol
0.5–1 mg PO or IM; can
repeat every 4h (PO) or
every 60 min (IM)
Extrapyramidal syndrome,
prolonged QT interval
Use in surgical cases may reduce delirium
incidence;[rx] needs to be confirmed in additional
studies
Cholinesterase inhibitors
Donepezil
5 mg QD
Nausea, vomiting, diarrhea
Prevention studies have not demonstrated
efficacy[rx,rx]
Antipsychotics are the most widely used drugs for the treatment of delirium-related agitation but can have marked adverse effects.
Benzodiazepines should be reserved for treatment of drug withdrawal, diffuse Lewy body disease, or as second-line treatment following failure of antipsychotics.
Not currently accepted clinical therapies
Abbreviations: BID, twice daily; IM, intramuscularly; PO, per os (by mouth); QD, once daily.
[/dropshadowbox]
First-Generation Antipsychotics
For the first-line treatment of a potentially reversible, hyperactive delirium, evidence supports, and published guidelines recommend, the use of first-generation antipsychotics, e.g., haloperidol and chlorpromazine. (These guidelines do not distinguish potentially reversible from irreversible delirium, nor do they address the principal underlying diagnosis and comorbidities, prognosis, functional status, goals of care, or irreversible delirium.)[rx,rx,rx,rx]
Second-Generation Antipsychotics
No evidence currently exists for improved efficacy with atypical (second or third generation) antipsychotics.[rx,rx–rx]These medications are often more expensive and have fewer routes of administration.[rx] Existing treatment guidelines suggest starting with first-generation antipsychotics.[rx]
Alpha-2 agonists
Alpha-2 agonist medication uses have been shown to be effective in decreasing the incidence of delirium in critically ill patients. These agents cause minimal respiratory depression and help in maintaining a low heart rate. Therefore, they facilitate minimal hemodynamic fluctuations and lower energy expenditure that might result in global cerebral insult.[rx] Further, alpha-2 agonists may inhibit the release and production of neurotoxic glutamate, thereby having a neuroprotective effect.[rx]
Opioids
Likewise, opioids have no role in the treatment of agitation or delirium. These are analgesics with no anti-agitation actions. Sedation is a side effect of opioids (not a therapeutic effect), and is not reliable from patient to patient or opioid to opioid. Care should be taken to differentiate pain-related behaviors from delirium-induced behaviors.
Benzodiazepines
These function as sedatives, anxiolytics – skeletal muscle relaxants, amnestics, and potent antiepileptics. Using the titration technique[rx] discussed above, the minimum benzodiazepine dose needed to rapidly and safely relieve symptoms can be established. The dose of a benzodiazepine typically needed to control the symptoms of delirium is far below their median lethal dosages.[rx,rx]
Olanzapine an atypical antipsychotic – has also been tested as a prophylactic agent to prevent postoperative delirium. 495 elderly patients undergoing elective knee or hip replacement were either assigned to a placebo arm or a treatment arm of 10mg of oral olanzapine. The treatment group had a significantly decreased incidence of delirium, but those patients who did suffer delirium had a longer, more severe course [rx].
Donepezil – a cholinesterase inhibitor FDA-approved for the treatment of Alzheimer’s disease, has also been tried as a prophylactic agent for delirium. Eighty patients were randomized to receive donepezil 14 days prior to and 14 days after surgery. There was no significant difference in the two groups [rx].
Nonpharmacological Approaches
Following are example of environmental interventions
Engage patients in mentally stimulating activities to help them with disordered thinking
Provide orienting and familiar materials to help patients know the time and date, where they are, and which staff are working with them.
Ensure all individuals identify themselves each time they encounter the patient, even if the encounters are minutes apart.
Minimize the number of people interacting with the patient and the quantity of stimulation the patient receives, e.g., television or loud music
Use family or volunteers as constant companions to help reassure and reorient a delirious patient. Encourage staff to sit with the patient while they do their documentation
Provide adequate soft lighting so patients can see without being overstimulated by bright lights.
Manage fall risks.
Provide warm milk, massage, warm blankets, and use relaxation tapes to optimize sleep hygiene and minimize sleep disturbances.
Ensure patients use their glasses, hearing aids, etc., to optimize orientation, decrease confusion, and promote better communication.
Ensure patients have good nutrition and an effective bowel and bladder management strategy.
Monitor fluid intake. Rehydrate with oral fluids containing salt, e.g., soups, sport drinks, red vegetable juices. When necessary, infuse fluids subcutaneously rather than intravenously.[rx–rx]
Use physical restraints only as a last resort to temporarily ensure the safety of both staff and a severely agitated and not redirectable patient,[rx,rx] and only until less restrictive interventions are possible.
Provide education and support to help family members cope with what they are witnessing.[rx]
Complications
Seizures
Disorientation
Hypertension
Hyperthermia
Altered mental status
Global confusion
Arrhythmias
Aspiration pneumonitis
Respiratory failure
Death
To prevent relapse, the patient should be referred to alcoholic anonymous and other support groups.
Cognitive behavior therapy may help some patients prevent relapse
A referral to a psychiatrist to assess for depression and anxiety may help abstain from alcohol.
These tips may help
Provide a reassuring environment for the patient, such as a quiet, well-lit room with familiar people and objects. It may also help to place a clock and wall calendar where a patient can see it.
Talk with the doctor, nurse, or another member of the health care team about a patient’s hallucinations or unusual behaviors. The health care team can help you learn what to expect and how to manage these symptoms.
Ask about stopping or switching medications that may worsen a patient’s mental confusion. Also, ask if there are other, untreated medical conditions that may be the cause of delirium.
In some cases, giving antipsychotic medications helps control the symptoms of delirium. Although these drugs can have side effects, most can be managed well.