Humerus Upper End Fracture/Proximal humeral fractures are common, particularly in the elderly. Along with proximal femoral, distal radial, and vertebral-body fractures, they are a common type of osteoporotic fracture. Women are affected two to three times as often as men [rx]. Proximal humerus and humerus fractures account for 4% to 6% and 1% to 3% of all fractures respectively in both young and elderly patients.
The proximal humerus has two necks. The anatomic neck is the old epiphyseal plate, and the surgical neck is the metaphyseal area below the humeral head. The blood supply is the anterior and posterior humeral circumflex artery with the axillary nerve as the major nerve of this region. The humeral shaft is a cylindrical bone that gradually becomes triangular distally. This bone serves as an insertion site for the pectoralis major, deltoid, and coracobrachialis and is the site of origin for the brachialis, triceps, and brachioradialis. The radial nerve is the major nerve of the humerus shaft which is seen in the spiral groove and is approximately 14 cm from the lateral epicondyle and 20 cm from the medial epicondyle. The major nerves of the distal humerus are the ulnar nerve and radial nerve. Distal humerus fractures comprise the supracondylar fractures, single condyle fractures, bi-column fractures, and coronal shear fractures. Treatment options include open reduction and internal fixation, closed reduction and percutaneous pinning, and intramedullary nailing or bracing.[rx][rx][rx]

Anatomy of Humerus Upper End Fracture
The proximal humerus includes the humeral head, greater tuberosity, lesser tuberosity, and the humeral shaft. In the sagittal plane, the humeral head has retroverted an average of 30 degrees relative to the humeral shaft [rx]. In the coronal plane, it is angled 130 to 150 degrees cephalad relative to the diaphysis. Fractures through the anatomic neck can result in significant vascular compromise to humeral head leading to avascular necrosis [rx].
In the neutral rotation, the greater tuberosity forms the lateral border of the proximal humerus. The lesser tuberosity, which sits directly anterior in this position, becomes profiled medially when the humerus is internally rotated—this creates a rounded silhouette “lightbulb sign” on radiograph. The long head of the biceps passes between the two tuberosities in the intertubercular groove, approximately 1 cm lateral to the midline of the humerus, and its relationship is an important landmark during fracture reduction [rx].
The supraspinatus muscle, innervated by the suprascapular nerve, attaches to the superior facet of the greater tuberosity with a force vector that pulls predominantly in a medial direction. The infraspinatus muscle, also innervated by the suprascapular nerve, inserts on the middle facet of the greater tuberosity. The teres minor muscle, innervated by the axillary nerve, attaches to the inferior facet. Together, these three externally rotate and yield a posteromedially directed deforming force. Therefore, if the greater tuberosity is fractured, it is displaced posteromedially. If it remains intact, and there is a surgical neck fracture, the resulting deformity is typically varus and external rotation. Anteriorly, the subscapularis, innervated by the upper and lower subscapular nerves, attaches to the lesser tuberosity, resulting in the anteromedial displacement of this osseous fragment if fractured [rx, rx]. The pectoralis major tendon insertion is an important landmark, especially during hemiarthroplasty.
The ulnar nerve arises from the medial cord of the brachial plexus and begins in the anterior compartment. It travels anterior to the medial intermuscular septum and posterior to the brachial artery. At the arcade of Struthers, approximately 8 cm from the medial epicondyle, it crosses to the posterior compartment to enter the cubital tunnel. It also provides no innervation to muscles proximal to the elbow.
The radial nerve is a terminal branch of the posterior cord of the brachial plexus. It begins in the posterior compartment and then passes through to the anterior compartment. It begins anteromedially and travels along the subscapularis proximally to join with the profound brachii at the triangular interval. About 10–14 cm from the lateral acromion, the nerve and artery travel along the posterior humerus in the spiral groove, separating the medial and lateral heads of the triceps at about the level of the deltoid tuberosity. It enters the anterior compartment through the lateral intermuscular septum approximately 10 cm from the distal articular surface, here it is tightly bound by the septum and therefore susceptible to traction injuries and radial nerve palsies [rx, rx].

Types of Humeral Neck Fracture
AO/OTA Classification of Distal Humerus Fractures
| Type A | Extraarticular (supracondylar fracture),80% are extension type; epicondyle | |
| Type B | Intraarticular-Single column (partial articular-isolated condylar, coronal shear, epicondyle with particular extension) | |
| Type C | Intraarticular-Both columns fractured and no portion of the joint contiguous with the shaft (complete articular) | |
| Each type further divided by degree and location of fracture comminution | ||
The AO classification divides proximal humeral fractures into three groups, A, B and C, each with subgroups, and places more emphasis on the blood supply to the articular surface. The assumption is that if either the lesser or greater tuberosity remains attached to the particular segment, then blood supply is probably adequate to avoid avascular necrosis.
Type A: extra-articular unifocal (either tuberosity +/- surgical neck of the humerus)
- A1: extra-articular unifocal fracture
- A2: extra-articular unifocal fracture with an impacted metaphyseal fracture
- A3: extra-articular unifocal fracture with a non-impacted metaphyseal fracture
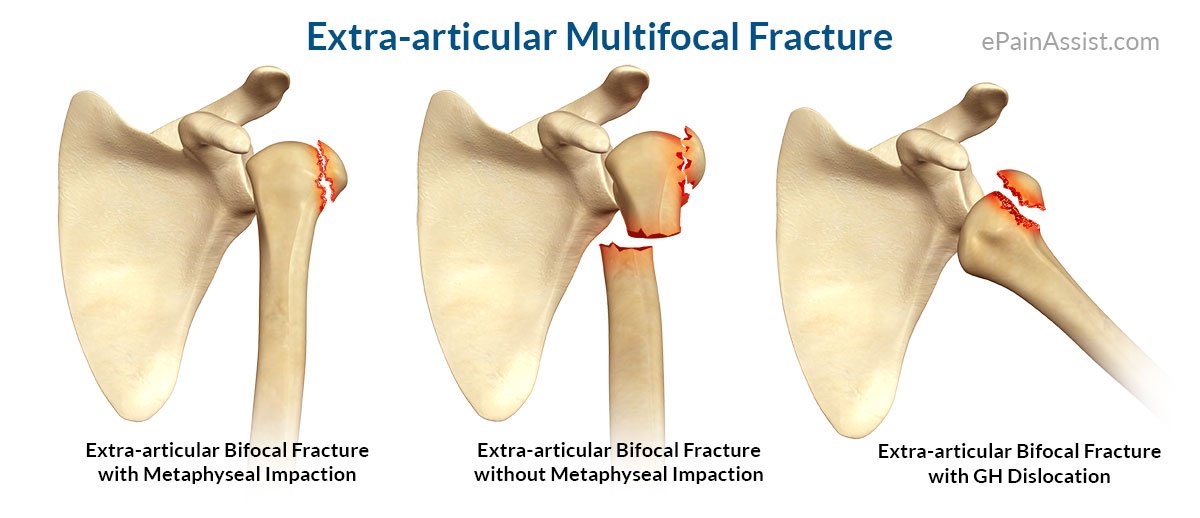
Type B: extra-articular bifocal (both tuberosities +/- surgical neck of the humerus or glenohumeral dislocation)
- B1: extra-articular bifocal fractures with impacted metaphyseal fracture
- B2: extra-articular bifocal fractures with non-impacted metaphyseal fracture
- B3: extra-articular bifocal fractures with glenohumeral joint dislocation
Type C: extra-articular (anatomical neck) but compromise the vascular supply of the particular segment
- C1: anatomical neck fracture, minimally displaced
- C2: anatomical neck fracture, displaced and impacted
- C3: anatomical neck fracture with glenohumeral joint dislocation
The risk of avascular necrosis increases from type A (very low) to type C (high risk) and thus determines treatment.
Milch Classification of Single Column Condyle Fractures
| Milch Type I | Lateral trochlear ridge intact | |
| Milch Type II | Fracture through the lateral trochlear ridge |
Jupiter Classification of Two-Column Distal Humerus Fractures
| High-T | Transverse fx proximal to or at upper olecranon fossa |
| Low-T | Transverse fx just proximal to trochlea (common) |
| Y | Oblique fx line through both columns with distal vertical fx line |
| H | Trochlea is a free fragment (risk of AVN) |
| Medial lambda | Proximal fx line exists medially |
| Lateral lambda | Proximal fx line exists laterally |
| Multiplane T | T type with an additional fracture in the coronal plane |
The Gartland classification is a system of categorizing supracondylar humerus fractures, clinically useful as it predicts the likelihood of associated neurovascular injuries, such as anterior interosseous nerve neurapraxia or brachial artery disruption.
| Type | Description[rx] |
|---|---|
| I | Non-displaced |
| II | Angulated with intact posterior cortex |
| IIA | Angulation |
| IIB | Angulation with rotation |
| III | Complete displacement but have periosteal (medial/lateral) contact |
| IIIA | The medial periosteal hinge is intact. Distal fragment goes posteromedially |
| IIIB | Lateral periosteal hinge intact. Distal fragment goes posterolaterally |
| IV | Periostial disruption with instability in both flexion and extension |
The classification has been variably adapted by multiple authors. What is presented below is what will probably be understood by most surgeons and radiologists and consists of four major groupings, based on the number of displaced parts?
One-part fracture
No fragments meet the criteria for displacement; a fracture with no fragments considered displaced is defined as a one-part fracture regardless of the actual number of fracture lines or their location.
- fracture lines involve 1-4 parts
- none of the parts are displaced (i.e <1cm and <45 degrees)
These undisplaced/minimally displaced fractures account for ~70-80% of all proximal humeral fractures and are almost always treated conservatively.
Two-part fracture
One segment is displaced, which may be the greater tuberosity, lesser tuberosity, or articular segment at the level of the anatomic neck or surgical neck.
- fracture lines involve 2-4 parts
- one part is displaced (i.e >1cm or >45 degrees)
Four possible types of two-part fractures exist (one for each part):
- surgical neck: most common
- greater tuberosity
- frequently seen in the setting of anterior shoulder dislocation
- a lower threshold of displacement (> 5mm) has been proposed
- anatomical neck
- lesser tuberosity: uncommon
These fractures account for approximately 20% of proximal humeral fractures.
Three-part fracture
With a three-part fracture, one tuberosity is displaced and the surgical neck fracture is displaced. The remaining tuberosity is attached, which produces a rotational deformity.
- fracture lines involve 3-4 parts
- two parts are displaced (i.e >1cm or >45 degrees)
Two three-part fracture patterns are encountered:
- greater tuberosity and shaft are displaced with respect to the lesser tuberosity and articular surface which remain together
- most common three-part pattern
- lesser tuberosity and shaft are displaced with respect to the greater tuberosity and articular surface which remain together
These fractures account for approximately 5% of proximal humeral fractures.
Four-part fracture
All four segments (both tuberosities, the articular surface, and the shaft) meet criteria for displacement. The articular segment typically is laterally displaced and out of contact with the glenoid [rx]. This is a severe injury and carries a high risk of avascular necrosis.
- fracture lines involve more than 4 parts
- three parts are displaced (i.e., >1 cm or >45 degrees) with respect to the 4th
These fractures are uncommon (<1% of proximal humeral fractures).
This pattern has poor non-operative results, and as the articular surface is no longer attached to any parts of the humerus which are attached to soft tissues, it has a high incidence of osteonecrosis.
Valgus-Impacted Four-Part Fractures
Neer added this pattern [rx] as a separate category in 2002 [rx]. In this situation, the head is rotated into a valgus posture and driven down between the tuberosities, which splay out to accommodate the head. Unlike in the classic four-part fracture, the articular surface maintains contact with the glenoid, and is not laterally displaced. This four-part fracture warranted its own category because the prognosis and treatment for this injury are different than those for the classic four-part fracture [rx, rx].
Causes of Humerus Upper End Fracture
Humerus fractures usually occur after physical trauma, falls, excess physical stress, or pathological conditions. Falls that produce humerus fractures among the elderly are usually accompanied by a preexisting risk factor for bone fractures, such as osteoporosis, a low bone density, or vitamin B deficiency.[rx]
- Proximal humerus fractures – most often occur among elderly people with osteoporosis who fall on an outstretched arm.[rx] Less frequently, proximal fractures occur from motor vehicle accidents, gunshots, and violent muscle contractions from an electric shock or seizure.[rx]
- A stress fracture of the proximal – and shaft regions can occur after an excessive amount of throwing, such as pitching in baseball.[rx]
- Sudden forceful fall down
- Road traffic accident
- Falls – Falling onto an outstretched hand is one of the most common causes of a broken clavicle.
- Sports injuries – Many Scapular fractures occur during contact sports or sports in which you might fall onto an outstretched hand — such as in-line skating or snowboarding.
- Motor vehicle crashes – Motor vehicle crashes can cause wrist bones to break, sometimes into many pieces, and often require surgical repair.
- Have osteoporosis – a disease that weakens your bones
- Eave low muscle mass or poor muscle strength – or lack agility and have poor balance (these conditions make you more likely to fall)
- Walk or do other activities in snow or on the ice – or do activities that require a lot of forwarding momenta, such as in-line skating and skiing
- Wave an inadequate – intake of calcium or vitamin D
- Football or soccer – especially on artificial turf
In younger patients, proximal humeral fractures are usually caused by high-energy trauma, such as traffic accidents or sporting accidents. In older patients, the most common cause is a fall onto the outstretched arm from a standing position, which is a type of low-energy trauma [rx, rx]
Symptoms of Humerus Upper End Fracture
- Typical signs and symptoms include pain, swelling, bruising, and limited range of motion at the shoulder. Deformity may be present in severe fractures, however, a musculature may cause absence of deformity on inspection.[rx]
- Numbness over the outside part of the upper arm and deltoid muscle weakness may indicate axillary nerve injury.[rx]
- Symptoms from poor blood circulation in the arm are uncommon due to collateral circulation in the arm.[rx]
Diagnosis of Humerus Upper End Fracture
Typically, the patient holds the injured arm in a protective posture close to the chest. Pain, swelling, hematoma, and tenderness of the proximal portion of the humerus may indicate the presence of a fracture. The perfusion and sensorimotor function of the limb should be tested in the periphery. The functioning of the axillary nerve should be tested as well.
Radiographs
- Recommended views
-
- obtain AP and lateral of humerus and elbow
- include the entire length of humerus and forearm
-
Obtain wrist radiographs if elbow injury present or distal tenderness on exam
- oblique radiographs may assist in surgical planning
- traction radiographs may assist in surgical planning specifically evaluate if there is continuity of the trochlear fragment to medial epicondylar fragment, this can influence hardware choice
CT
- often obtained for surgical planning
- especially helpful when shear fractures of the capitellum and trochlea are suspected
- 3D CT scan improves the intraobserver and interobserver reliability of several classification systems
MRI
- usually not indicated in acute injury
Treatment of Humerus Upper End Fracture
Non-Pharmacological
- Immobilization – in either a sling or a Velpeau bandage, with early gentle range of motion exercises. Some fractures may reduce with gravity alone as the patient resumes ambulating, but for some fractures, the closed reduction may improve the deformity and the amount of bony contact.
- In the acute setting – pain control can be difficult for patients. Resting in a supine position allows the arm to extend at the fracture site, and leads to pain and discomfort. Placing the injured extremity in a sling and having the patient rest in an upright or semi-reclining position with some bolsters behind the arm can help to reduce the pain. Patients may also find it more comfortable to sleep sitting in a reclining position when they are at home. Patients and caregivers should be advised that prolonged immobilization can be detrimental to the outcome.
- The range of Motion Exercises – Due to their limited movement following a proximal humerus fracture, individuals lose their range of shoulder motion and may develop stiffness of the shoulder joint. Your physical therapist will assess your shoulder motion compared to expected normal motion and the motion of shoulder of your noninjured arm, and lead you through a program of motion exercises to restore shoulder function.
- Strengthening Exercises – The muscles of the shoulder and upper back work together to allow for normal upper-body motion. Based on the way the shoulder joint is designed (a ball-and-socket joint, like a golf ball on a golf tee), there are many directions in which the shoulder may move. Therefore, the balanced strength of all the upper body muscles is crucial to make sure that the shoulder joint is protected and efficient with its movements. When there is a fracture to the proximal humerus (near the “ball” segment of the joint), the muscles around the shoulder girdle weaken, as they are not being used normally; this process is called “atrophy.” There are many exercises that can be done to strengthen the muscles around the shoulder so that each muscle is able to properly perform its job. Often, building strength after a fracture can take weeks to months due to atrophy. Your physical therapist will help you develop a strengthening program that is safe and comprehensive.
- Manual Therapy – Physical therapists are trained in manual (hands-on) therapy. When appropriate, based on the stage of healing at your fracture site, your physical therapist will gently move your shoulder joint and surrounding muscles as needed to improve their motion, flexibility, and strength. These techniques can target areas that are difficult to treat on your own.
- Modalities – Your physical therapist may recommend therapeutic modalities, such as ice and heat to aid in pain management.
- Functional Training – Whether you work in a factory, are a mother of a young child, work as a secretary, or are an older adult, the ways in which you perform your normal daily activities are important. Improper movement patterns after a fracture may come back to haunt you, as they may lead to future secondary injuries. Physical therapists are experts in assessing movement quality. Your physical therapist will be able to point out and correct faulty movements, so you are able to regain use of and maintain, a pain-free shoulder.
- Physiotherapy – which can be self-directed or in a formal setting, depending on the patient’s wishes and abilities, should begin no later than two weeks after the injury [rx, rx]. Initially, pendulum exercises will allow for a range of motion without placing weight-bearing stress on the fracture. After the patient is more comfortable, finger crawl exercises along a vertical surface can help with an overhead range of motion.
Medications
Medication can be prescribed to ease the pain.
- Antibiotic – Cefuroxime or Azithromycin, or Flucloxacillin or any others cephalosporin/quinolone antibiotic must be used to prevent infection or clotted blood remove to prevent furthers swelling and edema. Antibiotics and tetanus vaccination may be used if the bone breaks through the skin creating an open fracture.[rx]
- Antidepressants – A drugs that block pain messages from your brain and boost the effects of endorphins (your body’s natural painkillers).
- Muscle Relaxants – These medications provide relief from associated muscle spasms.
- Neuropathic Agents – Drugs(pregabalin & gabapentin) that address neuropathic or nerve-related pain. This includes burning, numbness, and tingling.
- Opioids – Also known as narcotics, these medications are intense pain relievers that should only be used under a doctor’s careful supervision.
- Topical Medications – These prescription-strength creams, gels, ointments, patches, and sprays help relieve pain and inflammation through the skin.
- NSAIDs – Prescription-strength drugs that reduce both pain and inflammation. Pain medicines and anti-inflammatory drugs help to relieve pain and stiffness, allowing for increased mobility and exercise. There are many common over-the-counter medicines called non-steroidal anti-inflammatory drugs (NSAIDs). They include and Ketorolac, Aceclofenac, naproxen
- Calcium & vitamin D3 – to improve bones health and healing fracture.
- Glucosamine & Diacerein, Chondroitin sulfate – can be used to tightening the loose tension, cartilage, ligament, and cartilage, ligament regenerate cartilage or inhabit the further degeneration of cartilage, ligament
- Corticosteroid- to healing the nerve inflammation and clotted blood in the joints.
- Dietary supplement – to remove general weakness & improved health.
- Cough Medication – Specially Cough expectorant syrup to elevate breathing problem or remove the lung congestion.
Surgery
- Closed reduction with percutaneous pinning (CRPP)
- Open reduction with internal fixation (ORIF)
- Intramedullary rod fixation
- Shoulder arthroplasty
- Reverse shoulder arthroplasty
Suture Fixation
- This technique has been described as a method to treat proximal humerus fractures and avoid the complications associated with implant placement and arthroplasty [rx, rx]. Using this method, nonabsorbable sutures are passed through the rotator cuff tissue and/or the bone fragments, in order to obtain and maintain the reduction.
- This technique avoids extensive soft tissue stripping and the risk of symptomatic implants. It also preserves the bone stock of the proximal humerus, which may allow for future procedures.
Plate Fixation
- Operative fixation of the proximal humerus has evolved over the years. Development of locking technology, as well as a site-specific implant, has helped overcome some of the problems initially seen with operative fixation. Locking screws have improved the fixation of the head and soft metaphyseal, and often osteoporotic bone, frequently associated with these patients [rx].
- The number of proximal screw options and trajectories attempts to maximize the fixation in the head of the humerus. Conventional plating may still be used in the case of a young patient with good bone quality, or for the treatment of simple two-part greater tuberosity fractures. Successful treatment with either plating technique relies on bone quality, as well as the accuracy of reduction and humeral head viability [rx, rx, rx, rx].
Intramedullary nail
- The use of an intramedullary device has been advocated by some as an alternative to plate and screw fixation [rx–rx]. This technique is thought to be less invasive to the surrounding soft tissues.
- There has been concern regarding the disruption of the rotator cuff and injury to the footprint of the supraspinatus, but meticulous attention to dissection and repair of the supraspinatus tendon; establishing a starting point on the superior articular surface rather than the footprint of the tendon; and minimizing nail prominence, can decrease the chances of postoperative shoulder pain [rx, rx].
- Although the intramedullary nail fixation has been reported for two-part, three-part and fourpart proximal humerus fractures, currently the most appropriate patient is one that presents with a two-part surgical neck fracture [rx, rx].
Surgical Approaches
- The deltopectoral approach to the proximal humerus has been the most widely used approach for operative fixation of proximal humerus fractures. Alternative approaches have been used to allow for improved access and ease of implant positioning [rx–rx]. Both the superior subacromial approach and the extended anterolateral acromial approach use a deltoid-splitting interval while protecting the axillary nerve to access the fracture site. These approaches decrease the amount of soft tissue dissection and retraction that often necessary with a standard deltopectoral approach and improve access to the lateral and posterior regions of the proximal humerus.
Augmentation
- Structural and biologic augmentations have been used in the treatment of proximal humerus fractures to improve the rate of healing and decrease the chance of displacement. The use of autograft, allograft, cement, or bone substitutes can help to fill voids in the metaphyseal area as well as provide structure or biologic support to the fracture [rx, rx].
- Endosteal fibular strut allografts have also been used to provide stability to the fracture especially in cases where there is a loss of the posterior medial calcar support and subsequent varus deformity [rx].
Arthroplasty
- The role of arthroplasty for the treatment of proximal humerus fractures has fluctuated over time. Neer initially recommended the use of humeral head replacement for complex three-part and four-part fractures [rx].
- Using conventional plating techniques, the incidence of nonunion and avascular necrosis of the humeral head was high for these types of injuries. But with the development of site-specific plates and locking plate technology, the fixation of proximal humerus fractures has improved and the role of arthroplasty for acute fractures has diminished.
- Humeral head replacement may still have a role in fractures that are associated with multi fragmentary humeral head cleavage, un reconstructable humeral head, or humeral head devoid of any soft tissue rendering it avascular. Shoulder arthroplasty can also be used in the cases of delayed presentation or as a salvage procedure following failed operative fixation. The role of hemiarthroplasty in the elderly has also changed, as the functional results have been poorer than expected [rx].
Complications of Humerus Upper End Fracture
There are risks associated with any type of surgery. These include:
- Nonunion (1-5%)
- Infection (~4.8%)
- Pneumothorax
- Adhesive capsulitis
- 4% in the surgical group develop adhesive capsulitis requiring surgical intervention
- Bleeding
- Problems with wound healing
- Blood clots
- Damage to blood vessels or nerves
- Reaction to anesthesia
- Hardware prominence
- Malunion with cosmetic deformity
- Restriction of ROM
- The difficulty with bone healing
- Lung injury
- Hardware irritation
- Fracture comminution (Z deformity)
- Fracture displacement
- Increased fatigue with overhead activities
- Dissatisfaction with appearance
- The difficulty with shoulder straps, backpacks and the like
- ~30% of patient request plate removal
- Superior plates associated with increased irritation
- Superior plates associated with increased risk of subclavian artery or vein penetration.
References
