Treatment of Ankylosing Spondylitis (Bechterew’s disease or Marie Struempell disease as it is also known) (AS) is a chronic progressive inflammatory arthropathy or seronegative spondyloarthropathy or inflammatory form of arthritis that causes vertebrae in the spine to fuse together. This limits flexibility in the spine and may cause a person to have a hunched-forward posture. It is a form of chronic, degenerative arthritis that affects the spine and sacroiliac joints and often other joints of the body.
Ankylosing spondylitis is a chronic inflammatory rheumatic disorder that primarily affects the axial skeleton. Sacroiliitis is its hallmark, accompanied by inflammation of the entheses (points of union between tendon, ligament, or capsule and bone) and formation of syndesmophytes, leading to spinal ankylosis in later stages. The pathogenesis of AS is poorly understood. [Rx]However, immune-mediated mechanisms involving human leucocyte antigen (HLA)-B27, inflammatory cellular infiltrates, cytokines (for example, tumor necrosis factor α and interleukin 10), and genetic and environmental factors are thought to have key roles. The detection of sacroiliitis by radiography, magnetic resonance imaging, or computed tomography in the presence of clinical manifestations is diagnostic for AS, although the presence of inflammatory back pain plus at least two other typical features of spondyloarthropathy (for example, enthesitis and uveitis) is highly predictive of early AS. Non-steroidal anti-inflammatory drugs (NSAIDs) effectively relieve inflammatory symptoms and are presently first-line drug treatment.[Rx]
Treatment of Ankylosing Spondylitis
Non-Surgical Treatment
Bed rest for first 24 hours. Additional bed rest will be determined by the severity of the problem. Recent medical studies indicate that staying more active is better for back disorders than prolonged bed rest.
Use a firm mattress (place a bed board under the mattress if needed).
Massage may help. Be sure the person is well-trained or massage could cause more harm than help.
Wear a special back support device.
Other options are available depending on the degree of injury, such as surgery (if disk damaged), electrical nerve stimulation, acupuncture, special shoes, etc.
Stress reduction techniques, if needed.
Non-Prescription Pain Relievers – Naproxen, acetaminophen, and ibuprofen each reduce inflammation and pain. Though these drugs are available over-the-counter, they are potent and taking more than the recommended dose can harm health. A doctor can help with advice about the right kind of non-prescription pain reliever to take.
Cold and Heat – Applying a cold pack to the painful part of the back contracts inflamed muscle and relieves pain. This treatment helps a great deal when the disk has recently ruptured and swelling is at its greatest. A heating pad or warm pack helps with residual pain.
Continued Physical Activity – Though pain or weakness seem like good reasons to rest the back, excessive bed-rest worsens the symptoms of a slipped disc. Moving around too little allows muscles to grow weaker and prevents the body from healing. Periods of rest interspersed with periods of normal activity throughout the day keep the back muscles in shape.
Prescription Remedies – If over-the-counter drugs fail to ease slipped disc pain, the doctor will turn to prescription medications. These can include narcotics, such as hydrocodone or codeine. While they can do away with pain, narcotics are very addictive and induce a mental fogginess that can itself be dangerous. More narrowly-focused medicines designed to target damaged nerves that create chronic pain may be a better choice, as they have fewer undesirable side effects. Gabapentin and Cymbalta are two drugs that act in different ways to minimize nerve pain. These drugs are less addictive than narcotics.
Nutrition – In order to restore the disc we also are going to need to include different substances in our diet. There are a lot of supplements on the market, of course. If you wish to try them, that’s fine. I personally don’t like them. I have tried one with glucosamine and chondroitin, but I didn’t feel any different. So, if you have the opportunity to take these with the food or from more natural sources, it will be great. You can find these substances in seafood and animal cartilages and by digesting them we ensure the building blocks for the connecting tissue for our joints and spine. Also, we will need more Omega 3 fatty acids, which can be supplied from cold pressed oils, fatty fish, flax seeds, chia and many more. Vitamins from the B group are very beneficial for people with herniated discs and all kinds of issues with the peripheral nervous system. Vitamins B1, B6 and B12 nourish the nerves and help them recover from the disk accident. Usually, doctors prescribe them as a part of the treatment, but it is worth mentioning anyway.
A good massage – A massage is one of the natural methods of relieving pain. Individuals who get a massage weekly for several months stand a better chance of alleviating back pain. A good massage provides a person with many health benefits that lessen back pain. A massage triggers the release of endorphins. Endorphins aid in decreasing anxiety and relieving pain. They offer a relaxation effect by softening muscles that are injured preventing cramping.
Undertaking yoga – Yoga is an applicable strategy for keeping the level of back pain at minimal levels. Taking yoga sessions often is very an effective method of dealing with back pain. With yoga, there is a high likelihood of proper body functions. The use of pain prescriptions is also diminished. Patients suffering from back pain related issues do not have to rely on these prescriptions to manage pain. Incorporating laughter in yoga is a good way of exercising. Yoga incorporates simple yet appropriate exercises that enhance the stretching of muscles. Laughter with yoga stimulates relieving of pain. It facilitates increased uptake of oxygen, little anxiety, and production of endorphins. All these variables play an essential role in diminishing back pain.
Adjusting sleeping position – A simple sleeping mistake can immensely contribute to back pain. A poor sleeping position can cause stress and tension on the muscles contributing to back pain. Altering one’s sleeping position and adopting a style that does not exert a lot of stress on the back is a recommended tactic. Nurturing sleeping habits such as assuming a reclining position, using wedge-shaped cushions and getting adjustable beds from reputable medical institutions are easy techniques to endorse. If a reclining position does not suit an individual, the other two techniques can be embraced.
Heat therapy – Several considerations should be observed when using heat therapy. The right temperature ought to be set so as to ensure a patient does not face risks associated with too much exposure to heat. The key objective should be to ensure enough access to heat to the muscles to yield benefits for the patient. The adoption of heat therapy for easing back pain is determined by the magnitude of pain a person is experiencing. In cases where relatively low back pain is encountered, short heat therapy sessions are recommended. On the other hand, if an individual is experiencing prolonged back pain, long heat therapy sessions are the most applicable.
Taking hot baths – This is a form of heat therapy that aims at relieving back pain. It guarantees permeation of heat into the muscles leading to reduced pain. Many individuals opt for this method since they believe it achieves competent results. Hot baths initiate a fast process of blood supply to stiff neck and back muscles. When this happens, the muscles relax and stretch leading to decreased back pain. To avoid interference with one’s sleeping patterns, a hot bath should be taken several hours before retiring to bed.
Aquatic therapy – This natural technique involves physical therapy in a pool. Individuals get the best out of this therapy by relying on the resistance of water. Consistency in undertaking this therapy is what ascertains getting back pain relief. Integrating aquatic therapy in an individual’s life for the better part of the week enhances the reduction of back pain quickly.
Enlighten others – Individuals have the power to devise their own natural strategies that aid them in coping with back pain. The strategies can also be a good remedy for others going through similar circumstances. An individual can use social media platforms to equip others with important tips on how to keep back pain at bay. Further, becoming a member of associations that address back pain issues enables better communication of the knowledge gained from personal experience.
The major types of medications used to treat ankylosing spondylitis are pain-relievers and drugs aimed at stopping or slowing the progression of the disease. All of these have potentially serious side effects. Pain-relieving drugs come in two major classes:
Nonsteroidal anti-inflammatory drugs (NSAIDs) – NSAIDs including the Coxib class are the first-line drugs for ankylosing spondylitis. A recent study reported that ankylosing spondylitis is associated with the prostaglandin E receptor 4 (PTGER4) gene. This receptor is associated with bone absorption; NSAIDs inhibit prostaglandin production, thus reducing the absorption12). The mainstay of therapy in all seronegative spondyloarthropathies are anti-inflammatory drugs, which include NSAIDs such as ibuprofen, phenylbutazone, diclofenac,indomethacin,naproxen and COX-2 inhibitors, which reduce inflammation and pain. Indomethacin is a drug of choice. 2012 research showed that those with AS and elevated levels of acute phase reactants seem to benefit most from continuous treatment with NSAIDs.
Analgesics – Acetaminophen and opioid-(like) agents are often used 1) for patients who complain of pain even after administration of NSAIDs and TNF-α inhibitors or 2) when other therapeutic options are not available.
Glucocorticoids – Although local glucocorticoid injection can be considered for skeletal muscle inflammation such as enthesitis, systematic administration of steroids is not generally recommended6)
Antidepressants – such as tricyclics and serotonin and norepinephrine reuptake inhibitors have been commonly prescribed for chronic low back pain, but their benefit for nonspecific low back pain is unproven, according to a review of studies assessing their benefit.
Muscle Relaxants – If the muscles around the slipped disc experience painful spasms, a muscle relaxant such as Valium may be useful. The drawback to drugs like these is that they do not limit their power to the affected nerve. Instead, they have a generally relaxing effect and will interfere with daily activities. Such as cyclobenzaprine (Flexeril), might be prescribed to relieve the discomfort associated with muscle spasms. However, these medicines might cause confusion in older people. Depending on the level of pain, prescription pain medicines might be used in the initial period of treatment.
Steroids – If inflammation is severe, a doctor may also prescribe a steroid. Steroids, such as cortisone, reduce swelling quickly. A cortisone shot directly in the affected area will have an immediate effect on the displaced disc.
Counter-irritants – such as creams or sprays applied topically stimulate the nerves in the skin to provide feelings of warmth or cold in order to dull the sensation of pain. Topical analgesics reduce inflammation and stimulate blood flow.
Nerve Relaxant — Pregabalin or gabapentin and anti-inflammatory drugs help to relieve pain and stiffness, allowing for increased mobility and exercise. There are many common over-the-counter medicines called non-steroidal anti-inflammatory drugs (NSAIDs). They include aspirin, ibuprofen, and naproxen.
Disease-modifying anti-rheumatic drugs (DMARDs) – Although the administration of DMARDs (e.g., sulfasalazine and methotrexate) is not recommended for axial diseases such as back pain, sulfasalazine is worth considering for treatment of peripheral arthritis Rx. Disease-modifying antirheumatic drugs (DMARDs) such as sulfasalazine can be used in people with peripheral arthritis. For axial involvement, the evidence does not support sulfasalazine. Other DMARDs, such as methotrexate, did not have enough evidence to prove their effectiveness. Generally, systemic corticosteroids were not used due to lack of evidence. Local injection with a corticosteroid can be used for certain people with peripheral arthritis.
TNF-α inhibitors – In 1995, Braun and coworkersrx) isolated TNF-α from ankylosing spondylitis patients via sacroiliac arthrocentesis. Thus, it was recognized that TNF-α is an important inflammatory mediator in this disease, which dramatically facilitated the development of biological agents.
Infliximab (Remicade) – Infliximab is a chimeric monoclonal antibody against TNF-α and is the first developed biological agent, consisting of 75% of human and 25% of mouse sequences rx). This antibody directly binds to TNF-α and neutralizes it. It is administered by intravenous injections at 5 mg/kg body weight. For the first administration, the same dose of infliximab is injected twice with an interval of 2 weeks and then the drug is administered every 6 weeks. Baraliakos et al.Rx reported a drug survival rate (patients who completed 8 years of treatment) of 48% and 88% of partial remission or low disease activity after 8-year follow-up. It was also reported that the potency was similar when the treatment was interrupted for 3 years and then resumed.
Etanercept (Enbrel) – Etanercept is a soluble blocker of TNF-α. This fusion protein binds TNF-α, which hinders interactions between TNF-α and TNF-α receptor located on other cells. Etanercept is generally administered by subcutaneous injection of 25 mg twice a week Rx. Martĺn-Mola et al.Rxreported that 63% of the enrolled patients completed 5 years of etanercept administration without any serious complications, while Baraliakos reported a drug survival rate of 62%, partial remission in 31% of patients, and complete remission in 44% of patients in a 7-year follow-up study. Similar to infliximab, etanercept was effective when the medication was interrupted and then resumed; the drug survival rate was slightly higher in the etanercept group than in the infliximab group.
Adalimumab (Humira) – Like infliximab, adalimumab is a monoclonal antibody against TNF-α but its sequence is 100% human. Adalimumab is administered by subcutaneous injections of 40 mg once per 2 weeks. Sieper et al.Rx reported a drug survival rate of 65%, partial remission according to Ankylosing Spondylitis Disease Activity Score (ASDAS) in 51% of patients, and ASDAS inactive disease in 61% of patients in a 5-years follow-up study. Similar to the long-term follow-up results for infliximab, favorable outcomes of long-term follow-up were demonstrated with remission achieved after 12 weeks of administration.
Anti-tumor necrosis factor therapy —A group of medicines known as anti-tumor necrosis factor agents (anti-TNF agents or TNF inhibitors) are often effective in the treatment of AS. Examples of anti-TNF medications include infliximab, etanercept, adalimumab, certolizumab pegol, and golimumab. People who do not respond to one anti-TNF treatment may respond to another. Improvement in symptoms is common and may occur within a few weeks of starting the drugs.
Who should use anti-TNF therapy? – Not every patient with AS needs anti-TNF therapy. In general, people with the active disease in the spine who have not responded fully to NSAIDs may be candidates (see ‘How do I know how active my ankylosing spondylitis is?’ above). Your clinician may also recommend a glucocorticoid (cortisone-like drug) injection into painful or swollen joints before starting an anti-TNF drug if these areas continue to bother you despite using NSAIDs (see ‘Glucocorticoids (steroids)’ below). The decision to use anti-TNF therapy depends upon several factors that should be discussed with your clinician.
Secukinumab— Secukinumab (brand name: Cosentyx) may be an alternative treatment option for some people who do not respond adequately to anti-TNF therapy.
Glucocorticoids (steroids)— Some clinicians may also recommend a glucocorticoid injection into particularly painful or swollen joints, especially if only one or two areas are causing the most pain. In some cases, a glucocorticoid injection into the sacroiliac joint may help provide relief in patients who have sacroiliac pain that has not responded to other therapies.
Bisphosphonates – Oral bisphosphonates are commonly used for fracture prevention in ankylosing spondylitis. Bisphosphonates also have an anti-inflammatory action and may have an effect on disease activity. Intravenous pulses of the bisphosphonate pamidronate have been investigated in several studies and have produced significant clinical improvements in some but not all studies.rx
Other Medications to Stop Inflammation and Save Your Joints Biological Drugs
If NSAIDs or DMARDs do not control your AS, your doctor may prescribe drugs called biologics. These drugs aim to address the problems with your immune system. They target your body’s production of specific proteins that cause inflammation.
Biologic drugs slow your immune system to help ease AS symptoms (pain, swelling, tenderness, and stiffness) as well as inflammation. These drugs may also help protect your joints from damage.
You are at higher risk of infections like tuberculosis when you take biologics. If you have signs of an infection, such as a fever or congestion, you should tell your doctor. Your doctor will test you for tuberculosis before you start a biologic drug and while you take it. These drugs also may raise your risk of getting certain types of cancer, but this is rare.
Doctors and scientists are constantly coming up with new ways to treat diseases, and they always need patients to test the efficacy of a proposed intervention. Below, you will find a current list of trials for ankylosing spondylitis and related conditions, as well as a link to enroll. You should speak with your doctor to decide if enrolling in a clinical trial is a good option for you.
Study Title
Description
Link
A Study to Evaluate the Efficacy and Safety of Ustekinumab in the Treatment of A … Show More
A Study Treating Participants With Early Axial Spondyloarthritis (axSpA) Taking … Show More
Condition: Axial Spondyloarthritis Intervention: Biological: Adalimumab; Other: Standard of Care (SOC) Sponsor: AbbVie; Improvement by Movement GmbH, Germany; Hannover Medical School; IST GmbH, Germany Recruiting – verified October 2016
An Efficacy and Safety Study of Ustekinumab in Participants With Active Nonradio … Show More
Condition: Nonradiographic Axial Spondylitis, Ankylosing Intervention: Drug: Group 1: Placebo; Drug: Group 2: Ustekinumab 45 mg; Drug: Group 3: Ustekinumab 90 m
Physical therapy
Though physical therapy remedies have been scarcely documented, some therapeutic exercises are used to help manage lower back, neck, knee, and shoulder pain. Some therapeutic exercises include
Moderate-to-high impact exercises like jogging are generally not recommended or recommended with restrictions due to the jarring of affected vertebrae that can worsen pain and stiffness in some with AS.
Physical therapy and education – The most important component of non-drug treatments of ankylosing spondylitis is the education of patients and regular exercise. Although home exercise is known to be effective, group physical therapy under appropriate supervision is more efficient than individual exercise6). It is important to educate patients that proper exercise not only alleviates pain but also relaxes the joints so that daily life activities are not affected.
Stretching – Stretching helps build flexibility and may reduce pain. Consider adding the spine stretch or the low-back rotation stretch to your daily routine.
Heat therapy – Apply a hot water bottle or heating pad to the affected area to reduce stiffness and pain. You may also use moist or dry heat. A warm bath may also help, especially before exercise. Don’t use heat therapy without consulting your doctor if you have diabetes, deep vein thrombosis, vascular disease, an open wound, or a skin condition such as dermatitis.
Cold therapy – Applying an ice pack, cold gel pack, or a bag of frozen vegetables to painful joints can help reduce swelling. After exercise, cold therapy may help reduce inflammation. Don’t apply ice for more than 20 minutes at a time. Don’t use cold therapy without consulting your doctor if you have circulation problems.
Acupuncture – Acupuncture is an ancient remedy for pain. It involves inserting thin needles into specific points in your skin. This is thought to activate your body’s pain-relieving hormones. Some people report acupuncture relieves AS pain.
Massage therapy – Massage helps you relax. It may also help you feel more flexible or “loose” so that you can exercise or stretch. Massage may cause pain at tender points around your spine. If this happens, avoid those areas and only use light massage techniques until the pain improves.
Movement – The more you sit, the stiffer you’re likely to feel. Get up, move around, and stretch regularly. If you have a desk job, take a “get up and move” break every hour.
Exercise – Gentle exercise programs such as yoga and Pilates are great for AS because they incorporate stretching. Swimming may also be beneficial because it’s easy on your joints. Strengthening exercises with weights can help build muscle, which supports joints affected by AS.
Alexander Technique – AS often leaves you hunched over. Practicing good posture is critical. The Alexander Technique teaches you to be aware of your posture throughout your day. It also teaches you how to correct poor posture and may be helpful for people with AS.
TENS Therapy – TENS stands for transcutaneous electrical nerve stimulation. This therapy uses electrical current to stimulate nerves through the body for pain control. Electrodes are usually applied at the pain site and connected to a TENS machine. It’s thought that when TENS stimulates nerves, it overrides pain signals. The TENS technique is usually taught by a physical therapist and may be continued at home.
Stop smoking – Smokers, especially men, are at risk for greater spine damage from AS than non-smokers. Quitting smoking not only helps reduce AS damage but also improves your overall health.
Physiotherapy – In spondylosis (spinal osteoarthritis), your spinal joints don’t move as well as they used to because of age-related changes in your spine, similar to arthritis. This can make it very painful to move because of decreased mobility within the spine itself. Your doctor may recommend physical therapy as part of your treatment plan because a physical therapist can help you maintain and increase mobility, learn ways to reduce pain, strengthen your spinal muscles so that they better support your spine, and stretch muscles that may be increasing nerve compression in your spine.
Physical therapy involves three main components: education, passive treatments, and active treatments. A physical therapist uses passive treatments to relax you and your body and to decrease acute pain or inflammation. They’re called passive because you don’t have to actively participate. If you’re experiencing acute pain, you’ll most likely start with passive treatments as your body heals and/or adjusts to the pain. However, the goal of physical therapy is to get into active treatments. These are therapeutic exercises that strengthen your body so that your spine has better support.
Passive Treatments for Ankylosing Spondylitis
Your physical therapist may give you passive treatments such as:
Deep Tissue Massage – This technique targets spasms and chronic muscle tension that perhaps builds up through daily life stress. You could also have spasms or muscle tension because of strains or sprains. The therapist uses direct pressure and friction to try to release the tension in your soft tissues (ligaments, tendons, muscles).
Hot and Cold Therapies – Your physical therapist will alternate between hot and cold therapies. By using heat, the physical therapist seeks to get more blood to the target area because an increased blood flow brings more oxygen and nutrients to that area. Blood is also needed to remove waste byproducts created by muscle spasms, and it also helps to heal. Cold therapy, also called cryotherapy, slows circulation, helping to reduce inflammation, muscle spasms, and pain. You may have a cold pack placed upon the target area, or even be given an ice massage. Another cryotherapy option is a spray called fluoromethane that cools the tissues. After cold therapy, your therapist may work with you to stretch the affected muscles.
Electrical stimulation – This can be performed within the clinic and if extremely successful, a TENS unit can be issued to a patient for home use. E-stim stimulates your muscles through variable (but safe) intensities of electrical current. It helps to reduce muscle spasms, and it may increase your body’s production of endorphins, your natural pain killers. It may also drive out inflammation, bring in healing properties, relax, and re-educate the muscles involved. The e-stim unit in the clinic is of a professional standard; the equipment is relatively large. However, a smaller machine for at “at home” use is also available. Electrical stimulation is a helpful therapy.
Yoga – Yoga is a great natural pain reliever for ankylosing spondylitis,” Ostrowski says. “You need to start with very basic poses and be patient, but if you work with an instructor who can modify the yoga positions for you, you can really benefit from this form of exercise.” A review of studies published in January 2016 in the Journal of Orthopedics & Rheumatology examined the impact of yoga on low back pain and found that it was safe and can help reduce both disability and pain.
Omega-3 fats and inflammation – Foods that contain omega-3 fats have been found to help reduce the inflammation associated with some forms of arthritis. These effects are modest compared with medication.
Omega-3 fats have few side effects and may have other health benefits, such as reduced heart disease. Foods rich in omega-3 fats include
fish – the oily fish such as salmon and sardines have greater amounts of omega-3 fats
linseeds and linseed (flaxseed) oil
canola (rapeseed) oil
walnuts
foods fortified with omega-3, such as margarine and eggs
some fish oil supplements.
Potassium Rich Foods
Potassium is known to decrease inflammation if it is present in the body in adequate amounts. Foods that contain potassium in high amounts are bananas, almonds, apricots, and broccoli.
Vitamin D – You must correct the vitamin D deficiency in your body if you are suffering from ankylosis. Bones need Vitamin D in greater amounts when they are affected by a disease.
Home Remedies For Ankylosing Spondylitis
Use Ginger, Black Pepper or any good digestive with your meals. It will help detoxify your body.
1 tablespoonful of Turmeric should be consumed once every day, after boiling it in milk for half an hour.
Constipation must be avoided at all costs. Constipation may increase pain in Ankylosing spondylitis.
Herbs have divine healing powers and they have the ability to cure any disease of the root. They were gifted to us by God when he created life. So believe in God if you want to get rid of your problems!
Ayurvedic herbs are unique natural remedies for Ankylosing spondylitis. Ayurvedic principles are different in many ways From modern medicine for example – Drinking water From a copper pan after keeping it overnight is also very useful in Rheumatoid arthritis and Ankylosing spondylitis.
Consuming castor oil at night with milk or alone is a very useful herbal remedy for arthritis, especially rheumatoid arthritis and ankylosing spondylitis.
Improve your nutrition as the first step. It plays an important role to fight diseases. When nothing works, nutrition works a lot!
Use herbal juices like Aloe vera juice (Kumari Saar) and Amla Juice ( Amla Saar) in routine. Amla is the richest source of natural Vitamin C. Vitamin C improves the natural immunity of the body. 100 gm of Amla juice contains 30 times more vitamin C than 100 gm of oranges.
Homeopathic treatment for Ankylosing Spondylitis
Homeopathy treats the person as a whole. A Remedy is selected after full individualizing examination and case analysis which includes a medical history of the patient, physical and mental constitution etc.
Phosphorus – The rigidity of nape of the neck. Pressure on shoulders. Swelling of the neck. Engorgement of axillary glands and of those of nape of the neck and of the neck. Paralyzes sensation in the upper sacrum and lower lumbar vertebrae. Contusive pain in loins and back (as if the back were broken), especially after having been seated a long time Sensitiveness of spinous processes of dorsal vertebrae to pressure.
Silicea –The stiffness of nape, with a headache. Swelling of glands of nape, in the neck, and under the axillae (with suppuration), sometimes with indurations…Stitches between the hips.Coccyx painful, as after a long carriage ride.- Stinging in os coccyx on rising, painful to pressure. -Scabby elevation on the coccyx, above fissure of nates- Inflammatory abscess in the lumbar region (on the psoas muscle).- Weakness and paralytic stiffness in back, loins, and nape.
Aurum Metallicum – Serious or advanced rheumatism with marked stiffness. Rheumatism with stiffness or spasms of the chest wall. Severe spasm or tearing pains. Pains also described as “paralytic.” An important remedy in ankylosing spondylitis. Wandering arthritis; moving spot to spot from one week to next. Worse: Night. Morning in bed. Hip pain worse rising from a seat or from walking.
Sulfur – The stiffness of the neck, in nape, with a paralytic, sprained pain. A child cannot hold head up neck muscles so weak. Tetters on nape. Swelling and inflammation of glands of nape and of the neck. Swelling and suppuration of axillary glands. Cracking in vertebrae of the neck, especially on bending backward.
Maintain a healthy weight– If you are overweight or obese, the extra load on your joints may be exacerbating your symptoms, especially if your affected joints include those of the hip, knee or spine. There is also a clear link between being overweight and an increased risk of developing osteoarthritis.
Dietary recommendations for ankylosing spondylitis
General dietary recommendations for a person with ankylosing spondylitis:
eat a well-balanced diet, including fruit and vegetables, protein foods, dairy, cereals, and grains. This will help to maintain general good health and a healthy weight
avoid crash dieting or fasting
increase dietary calcium to reduce the risk of osteoporosis in later life
drink plenty of non-alcoholic fluids, especially water
keep your weight within the normal range. Excess body weight increases stress on joints, especially weight-bearing joints like knees and hips.
What can the athlete do?
Keep themselves fit and healthy
Maintain an optimum weight to place as little strain on the spine as possible
Have a good diet
Maintain a good posture and mobility
Avoid sudden twisting and turning movements
Use a heat pack or warm bath to reduce pain and stiffness
Exercise such as swimming can be great for ankylosing spondylitis as it places very little strain on the spine and joints.
Other exercises for mobility and back strength can also be beneficial.
Symptoms, Diagnosis of Lumbago is a common disorder involving the muscles, nerves, and bones of the back. Pain can vary from a dull constant ache to a sudden sharp feeling. Low back pain may be classified by duration as acute (pain lasting less than 6 weeks), sub-chronic (6 to 12 weeks), or chronic (more than 12 weeks). The condition may be further classified by the underlying cause as either mechanical, non-mechanical, or referred pain. The symptoms of low back pain usually improve within a few weeks from the time they start, with 40-90% of people completely better by six weeks.
Acute low-back pain without sciatica, with some spread of discomfort to the region of the sacroiliac joint, to the outer part of the buttock as well as to the lateral and the back part of the thigh, is a unifying symptom of a very common clinical syndrome whose exact underlying cause remains often uncertain. Most patients fall then into the category of non-specific low-back pain. Probably the pathogenesis is not uniform, and the pain can arise from a variety of structures (muscles, ligament, spine). Pain which persists after 3 to 4 days should warn the clinician that a serious pathological condition may be present which requires a new approach to diagnosis and treatment.
Anatomy of the Low Back/Lumbago
The lumbar spine consists of five vertebrae (L1–L5). The complex anatomy of the lumbar spine is a combination of these strong vertebrae, linked by joint capsules, ligaments, tendons, and muscles, with extensive innervation. The spine is designed to be strong since it has to protect the spinal cord and spinal nerve roots. At the same time, it is highly flexible, providing for mobility in many different planes.
The mobility of the vertebral column is provided by the symphyseal joints between the vertebral bodies, with an IVD in between. The facet joints are located between and behind adjacent vertebrae, contributing to spine stability. They are found at every spinal level and provide about 20% of the torsional (twisting) stability in the neck and low back segments 26. Ligaments aid in joint stability during rest and movement, preventing injury from hyperextension and hyperflexion. The three main ligaments are the anterior longitudinal ligament (ALL), posterior longitudinal ligament (PLL), and ligamentum flavum (LF). The canal is bordered by vertebral bodies and discs anteriorly and by laminae and LF posteriorly. Both the ALL and PLL run the entire length of the spine, anteriorly and posteriorly, respectively. Laterally, spinal nerves and vessels come out from the intervertebral foramen. Beneath each lumbar vertebra, there is the corresponding foramen, from which spinal nerve roots exit. For example, the L1 neural foramina are located just below the L1 vertebra, from where the L1 nerve root exits.
IVDs are located between vertebrae. They are compressible structures able to distribute compressive loads through osmotic pressurization. In the IVD, the annulus fibrosus (AF), a concentric ring structure of organized lamellar collagen, surrounds the proteoglycan-rich inner nucleus pulposus (NP). Discs are avascular in adulthood, except for the periphery. At birth, the human disc has some vascular supply but these vessels soon recede, leaving the disc with little direct blood supply in the healthy adult 27. Hence, metabolic support of much of the IVD is dependent on the cartilaginous endplates adjacent to the vertebral body. A meningeal branch of the spinal nerve, better known as the recurrent sinuvertebral nerve, innervates the area around the disc space 28.
The lumbar spine is governed by four functional groups of muscles, split into extensors, flexors, lateral flexors, and rotators. The lumbar vertebrae are vascularized by lumbar arteries that originate in the aorta. Spinal branches of the lumbar arteries enter the intervertebral foramen at each level, dividing themselves into smaller anterior and posterior branches 29. The venous drainage parallels the arterial supply 30.
Typically, the end of the spinal cord forms the conus medullaris within the lumbar spinal canal at the lower margin of the L2 vertebra 31. All lumbar spinal nerve roots stem from the connection between the dorsal or posterior (somatic sensory) root from the posterolateral aspect of the spinal cord and the ventral or anterior (somatic motor) root from the anterolateral aspect of the cord 31. The roots then flow down through the spinal canal, developing into the cauda equina, before exiting as a single pair of spinal nerves at their respective intervertebral foramina. Cell bodies of the motor nerve fibers can be found in the ventral or anterior horns of the spinal cord, whereas those of the sensory nerve fibers are in the dorsal root ganglion (DRG) at each level. One or more recurrent meningeal branches, known as the sinuvertebral nerves, run out from the lumbar spinal nerves. The sinuvertebral nerve, or Luschka’s nerve, is a recurrent branch created from the merging of the grey ramus communicans (GRC) with a small branch coming from the proximal end of the anterior primary ramus of the spinal nerve. This polisegmentary mixed nerve directly re-enters the spinal canal and gives off ascending and descending anastomosing branches comprising both somatic and autonomic fibers for the posterolateral annulus, the posterior vertebral body and the periostium, and the ventral meninges 32, 33. The sinuvertebral nerves connect with branches from radicular levels both above and below the point of entry, in addition to the contralateral side, meaning that localizing pain from involvement of these nerves is challenging 34. Also, the facet joints receive two-level innervation comprising somatic and autonomic components. The former convey a well-defined local pain, while the autonomic afferents transmit referred pain.
www.rxharun.com
Causes of Lumbago /Backache
The human back is composed of a complex structure of muscles, ligaments, tendons, disks and bones – the segments of our spine are cushioned with cartilage-like pads called disks. Problems with any of these components can lead to back pain. In some cases of back pain, its cause is never found.
Problems with the spine such as osteoporosis can lead to back pain.
Strain – the most common causes of back pain are:
Strained muscles
Strained ligaments
A muscle spasm
Things that can lead to strains or spasms include:
Lifting something improperly
Lifting something that is too heavy
The result of an abrupt and awkward movement
Structural problems –
Sprains and strains – account for most acute back pain. Sprains are caused by overstretching or tearing ligaments, and strains are tears in tendon or muscle. Both can occur from twisting or lifting something improperly, lifting something too heavy, or overstretching. Such movements may also trigger spasms in back muscles, which can also be painful.
Intervertebral disc degeneration – is one of the most common mechanical causes of low back pain, and it occurs when the usually rubbery discs lose integrity as a normal process of aging. In a healthy back, intervertebral discs provide height and allow bending, flexion, and torsion of the lower back. As the discs deteriorate, they lose their cushioning ability.
Herniated or ruptured discs – can occur when the intervertebral discs become compressed and bulge outward (herniation) or rupture, causing low back pain.
Radiculopathy – is a condition caused by compression, inflammation and/or injury to a spinal nerve root. Pressure on the nerve root results in pain, numbness, or a tingling sensation that travels or radiates to other areas of the body that are served by that nerve. Radiculopathy may occur when spinal stenosis or a herniated or ruptured disc compresses the nerve root.
Sciatica – is a form of radiculopathy caused by compression of the sciatic nerve, the large nerve that travels through the buttocks and extends down the back of the leg. This compression causes shock-like or burning low back pain combined with pain through the buttocks and down one leg, occasionally reaching the foot. In the most extreme cases, when the nerve is pinched between the disc and the adjacent bone, the symptoms may involve not only pain, but numbness and muscle weakness in the leg because of interrupted nerve signaling. The condition may also be caused by a tumor or cyst that presses on the sciatic nerve or its roots.
Spondylolisthesis – is a condition in which a vertebra of the lower spine slips out of place, pinching the nerves exiting the spinal column.
A traumatic injury – such as from playing sports, car accidents, or a fall can injure tendons, ligaments or muscle resulting in low back pain. Traumatic injury may also cause the spine to become overly compressed, which in turn can cause an intervertebral disc to rupture or herniate, exerting pressure on any of the nerves rooted to the spinal cord. When spinal nerves become compressed and irritated, back pain and sciatica may result.
Ruptured disks – each vertebra in our spine is cushioned by disks. If the disk ruptures there will be more pressure on a nerve, resulting in back pain.
Bulging disks – in much the same way as ruptured disks, a bulging disk can result in more pressure on a nerve.
Sciatica – a sharp and shooting pain that travels through the buttock and down the back of the leg, caused by a bulging or herniated disk pressing on a nerve.
Arthritis – patients with osteoarthritis commonly experience problems with the joints in the hips, lower back, knees and hands. In some cases spinal stenosis can develop, which is the term used to describe when the space around the spinal cord narrows.
Abnormal curvature of the spine – if the spine curves in an unusual way the patient is more likely to experience back pain. An example is a scoliosis, a condition in which the spine curves to the side.
Osteoporosis– bones, including the vertebrae of the spine, become brittle and porous, making compression fractures more likely.
Spinal stenosis – is a narrowing of the spinal column that puts pressure on the spinal cord and nerves that can cause pain or numbness with walking and over time leads to leg weakness and sensory loss.
Skeletal irregularities – include scoliosis, a curvature of the spine that does not usually cause pain until middle age; lordosis, an abnormally accentuated arch in the lower back; and other congenital anomalies of the spine.
Abdominal aortic aneurysms – occur when the large blood vessel that supplies blood to the abdomen, pelvis, and legs becomes abnormally enlarged. Back pain can be a sign that an aneurysm is becoming larger and that the risk of rupture should be assessed.
Kidney stones – can cause sharp pain in the lower back, usually on one side.
Below are some other causes of back pain
Cauda equina syndrome – the cauda equine is a bundle of spinal nerve roots that arise from the lower end of the spinal cord. People with cauda equine syndrome feel a dull pain in the lower back and upper buttocks, as well as analgesia (lack of feeling) in the buttocks, genitalia, and thigh. There are sometimes bowel and bladder function disturbances.
Cancer of the spine – a tumor located on the spine may press against a nerve, resulting in back pain.
Infection of the spine – if the patient has an elevated body temperature (fever) as well as a tender warm area on the back, it could be caused by an infection of the spine.
Other infections – pelvic inflammatory disease (females), bladder, or kidney infections may also lead to back pain.
Endometriosis – is the buildup of uterine tissue in places outside the uterus.
Fibromyalgia – a chronic pain syndrome involving widespread muscle pain and fatigue.
Sleep disorders – individuals with sleep disorders are more likely to experience back pain, compared to others.
Shingles – an infection that can affect the nerves may lead to back pain, depending on the nerves affected.
Bad mattress – if a mattress does not support specific parts of the body and keep the spine straight, there is a greater risk of developing back pain.
Everyday activities or poor posture
Back pain can also be the result of some everyday activity or poor posture. Examples include:
Adopting a very hunched sitting position when using computers can result in increased back and shoulder problems over time.
Bending awkwardly
Pushing something
Pulling something
Carrying something
Lifting something
Standing for long periods
Bending down for long periods
Twisting
Coughing
Sneezing
Muscle tension
Over-stretching
Straining the neck forward, such as when driving or using a computer
Long driving sessions without a break, even when not hunched
Exertion or lifting.
Severe blow or fall.
Back disorders.
Infections.
Ruptured lumbar disk.
Nerve dysfunction.
Osteoporosis.
Spondylosis (hardening and stiffening of the spinal column).
The main symptom of back pain is, as the name suggests, an ache or pain anywhere on
Pain in the back, and sometimes all the way down to the buttocks and legs. Some back issues can cause pain in other parts of the body, depending on the nerves affected.
In most cases, signs, and symptoms clear up on their own within a short period. If any of the following signs or symptoms accompany back pain, people should see their doctor:
Pain. It may be continuous, or only occur when you are in a certain position. The pain may be aggravated by coughing or sneezing, bending or twisting.
Patients who have been taking steroids for a few months
Drug abusers
Patients with cancer
Patients who have had cancer
Patients with depressed immune systems
Stiffness.
According to the British National Health Service (NHS), the following groups of people should seek medical advice if they experience back pain:
Weight loss
Elevated body temperature (fever)
Inflammation (swelling) on the back
Persistent back pain – lying down or resting does not help
Pain down the legs
Pain reaches below the knees
A recent injury, blow or trauma to your back
Urinary incontinence – you pee unintentionally (even small amounts)
Difficulty urinating – passing urine is hard
Fecal incontinence – you lose your bowel control (you poo unintentionally)
Numbness around the genitals
Numbness around the anus
Numbness around the buttocks
dull ache,
numbness,
tingling,
sharp pain,
pulsating pain,
pain with movement of the spine,
pins and needles sensation,
muscle spasm,
tenderness,
sciatica with shooting pain down one or both lower extremities
People aged less than 20 and more than 55 years
Additionally, people who experience pain symptoms after a major trauma (such as a car accident) are advised to see a doctor. If low back pain interferes with daily activities, mobility, sleep, or if there are other troubling symptoms, medical attention should be sought.
Risk increases with
Biomechanical risk factors.
Sedentary occupations.
Gardening and other yard work.
Sports and exercise participation, especially if infrequent.
Obesity.
Preventive measures
Exercises to strengthen lower back muscles.
Learn how to lift heavy objects.
Sit properly.
Back support in bed.
Lose weight, if obese.
Choose proper footwear.
Wear special back support devices.
Red flag conditions indicating possible underlying spinal pathology or nerve root problemsw9
Red flags
Onset age < 20 or > 55 years
Non-mechanical pain (unrelated to time or activity)
Thoracic pain
Previous history of carcinoma, steroids, HIV
Feeling unwell
Weight loss
Widespread neurological symptoms
Structural spinal deformity
Indicators for nerve root problems
Unilateral leg pain > low back pain
Radiates to foot or toes
Numbness and paraesthesia in the same distribution
Straight leg raising test induces more leg pain
Localized neurology (limited to one nerve root)
Diagnosis of Lumbago /Backache
Suspected disk, nerve, tendon, and other problems – X-rays or some other imaging scan, such as a CT (computerized tomography) or MRI (magnetic resonance imaging) scan may be used to get a better view of the state of the soft tissues in the patient’s back.
X-rays – can show the alignment of the bones and whether the patient has arthritis or broken bones. They are not ideal for detecting problems with muscles, the spinal cord, nerves or disks.
MRI or CT scans – these are good for revealing herniated disks or problems with tissue, tendons, nerves, ligaments, blood vessels, muscles, and bones.
Bone scan – a bone scan may be used for detecting bone tumors or compression fractures caused by brittle bones (osteoporosis). The patient receives an injection of a tracer (a radioactive substance) into a vein. The tracer collects in the bones and helps the doctor detect bone problems with the aid of a special camera.
Electromyography or EMG – the electrical impulses produced by nerves in response to muscles is measured. This study can confirm nerve compression which may occur with a herniated disk or spinal stenosis (narrowing of the spinal canal).
Types of low back pain associated with physical findings of no clear pathoanatomical significance
Syndrome
Findings
Assessment/Plan
Facet syndrome
History and physical examination:
local and pseudoradicular symptoms and signs
pain on movement
facet tenderness
pain on reclination
positive injection test
joint dysfunction on manual diagnosis
Radiological findings (not indicated on intial evaluation):
differentiation from high-grade or activated spondylarthrosis (possibly, juxtaforaminal cyst) or
Causes Symptoms of Backache is a common disorder involving the muscles, nerves, and bones of the back. Pain can vary from a dull constant ache to a sudden sharp feeling. Low back pain may be classified by duration as acute (pain lasting less than 6 weeks), sub-chronic (6 to 12 weeks), or chronic (more than 12 weeks). The condition may be further classified by the underlying cause as either mechanical, non-mechanical, or referred pain. The symptoms of low back pain usually improve within a few weeks from the time they start, with 40-90% of people completely better by six weeks.
Acute low-back pain without sciatica, with some spread of discomfort to the region of the sacroiliac joint, to the outer part of the buttock as well as to the lateral and the back part of the thigh, is a unifying symptom of a very common clinical syndrome whose exact underlying cause remains often uncertain. Most patients fall then into the category of non-specific low-back pain. Probably the pathogenesis is not uniform, and the pain can arise from a variety of structures (muscles, ligament, spine). Pain which persists after 3 to 4 days should warn the clinician that a serious pathological condition may be present which requires a new approach to diagnosis and treatment.
Pain in the lower part of the back is commonly referred to as Lumbago. It can be defined as mild to severe pain or discomfort in the area of the lower back. The pain can be acute (sudden and severe) or chronic if it has lasted more than three months.
Most people will experience lumbago at some point in their life. It is one of the most common reasons people miss work and visit the doctor. It can occur at any age but is a particular problem in younger people whose work involves physical effort and much later in life, in the elderly.
www.rxharun.com
Anatomy of the Low Back / Backache
The lumbar spine consists of five vertebrae (L1–L5). The complex anatomy of the lumbar spine is a combination of these strong vertebrae, linked by joint capsules, ligaments, tendons, and muscles, with extensive innervation. The spine is designed to be strong, since it has to protect the spinal cord and spinal nerve roots. At the same time, it is highly flexible, providing for mobility in many different planes.
The mobility of the vertebral column is provided by the symphyseal joints between the vertebral bodies, with an IVD in between. The facet joints are located between and behind adjacent vertebrae, contributing to spine stability. They are found at every spinal level and provide about 20% of the torsional (twisting) stability in the neck and low back segments [rx]. Ligaments aid in joint stability during rest and movement, preventing injury from hyperextension and hyperflexion. The three main ligaments are the anterior longitudinal ligament (ALL), posterior longitudinal ligament (PLL), and ligamentum flavum (LF). The canal is bordered by vertebral bodies and discs anteriorly and by laminae and LF posteriorly. Both the ALL and PLL run the entire length of the spine, anteriorly and posteriorly, respectively. Laterally, spinal nerves and vessels come out from the intervertebral foramen. Beneath each lumbar vertebra, there is the corresponding foramen, from which spinal nerve roots exit. For example, the L1 neural foramina are located just below the L1 vertebra, from where the L1 nerve root exits.
IVDs are located between vertebrae. They are compressible structures able to distribute compressive loads through osmotic pressurization. In the IVD, the annulus fibrosus (AF), a concentric ring structure of organized lamellar collagen, surrounds the proteoglycan-rich inner nucleus pulposus (NP). Discs are avascular in adulthood, except for the periphery. At birth, the human disc has some vascular supply but these vessels soon recede, leaving the disc with little direct blood supply in the healthy adult [rx]. Hence, metabolic support of much of the IVD is dependent on the cartilaginous endplates adjacent to the vertebral body. A meningeal branch of the spinal nerve, better known as the recurrent sinuvertebral nerve, innervates the area around the disc space [rx].
The lumbar spine is governed by four functional groups of muscles, split into extensors, flexors, lateral flexors, and rotators. The lumbar vertebrae are vascularized by lumbar arteries that originate in the aorta. Spinal branches of the lumbar arteries enter the intervertebral foramen at each level, dividing themselves into smaller anterior and posterior branches [rx]. The venous drainage parallels the arterial supply [rx].
Typically, the end of the spinal cord forms the conus medullaris within the lumbar spinal canal at the lower margin of the L2 vertebra [rx]. All lumbar spinal nerve roots stem from the connection between the dorsal or posterior (somatic sensory) root from the posterolateral aspect of the spinal cord and the ventral or anterior (somatic motor) root from the anterolateral aspect of the cord [rx. The roots then flow down through the spinal canal, developing into the cauda equina, before exiting as a single pair of spinal nerves at their respective intervertebral foramina. Cell bodies of the motor nerve fibers can be found in the ventral or anterior horns of the spinal cord, whereas those of the sensory nerve fibers are in the dorsal root ganglion (DRG) at each level. One or more recurrent meningeal branches, known as the sinuvertebral nerves, run out from the lumbar spinal nerves. The sinuvertebral nerve, or Luschka’s nerve, is a recurrent branch created from the merging of the grey ramus communicans (GRC) with a small branch coming from the proximal end of the anterior primary ramus of the spinal nerve. This polisegmentary mixed nerve directly re-enters the spinal canal and gives off ascending and descending anastomosing branches comprising both somatic and autonomic fibers for the posterolateral annulus, the posterior vertebral body and the periosteum, and the ventral meninges [rx], [rx]. The sinuvertebral nerves connect with branches from radicular levels both above and below the point of entry, in addition to the contralateral side, meaning that localizing pain from involvement of these nerves is challenging [rx]. Also, the facet joints receive two-level innervation comprising somatic and autonomic components. The former convey a well-defined local pain, while the autonomic afferents transmit referred pain.
www.rxharun.com
Causes of Lumbago /Backache
The human back is composed of a complex structure of muscles, ligaments, tendons, disks and bones – the segments of our spine are cushioned with cartilage-like pads called disks. Problems with any of these components can lead to back pain. In some cases of back pain, its cause is never found.
Problems with the spine such as osteoporosis can lead to back pain.
Strain – the most common causes of back pain are:
Strained muscles
Strained ligaments
A muscle spasm
Things that can lead to strains or spasms include:
Lifting something improperly
Lifting something that is too heavy
The result of an abrupt and awkward movement
Structural problems –
Sprains and strains – account for most acute back pain. Sprains are caused by overstretching or tearing ligaments, and strains are tears in tendon or muscle. Both can occur from twisting or lifting something improperly, lifting something too heavy, or overstretching. Such movements may also trigger spasms in back muscles, which can also be painful.
Intervertebral disc degeneration – is one of the most common mechanical causes of low back pain, and it occurs when the usually rubbery discs lose integrity as a normal process of aging. In a healthy back, intervertebral discs provide height and allow bending, flexion, and torsion of the lower back. As the discs deteriorate, they lose their cushioning ability.
Herniated or ruptured discs – can occur when the intervertebral discs become compressed and bulge outward (herniation) or rupture, causing low back pain.
Radiculopathy – is a condition caused by compression, inflammation and/or injury to a spinal nerve root. Pressure on the nerve root results in pain, numbness, or a tingling sensation that travels or radiates to other areas of the body that are served by that nerve. Radiculopathy may occur when spinal stenosis or a herniated or ruptured disc compresses the nerve root.
Sciatica – is a form of radiculopathy caused by compression of the sciatic nerve, the large nerve that travels through the buttocks and extends down the back of the leg. This compression causes shock-like or burning low back pain combined with pain through the buttocks and down one leg, occasionally reaching the foot. In the most extreme cases, when the nerve is pinched between the disc and the adjacent bone, the symptoms may involve not only pain, but numbness and muscle weakness in the leg because of interrupted nerve signaling. The condition may also be caused by a tumor or cyst that presses on the sciatic nerve or its roots.
Spondylolisthesis – is a condition in which a vertebra of the lower spine slips out of place, pinching the nerves exiting the spinal column.
A traumatic injury – such as from playing sports, car accidents, or a fall can injure tendons, ligaments or muscle resulting in low back pain. Traumatic injury may also cause the spine to become overly compressed, which in turn can cause an intervertebral disc to rupture or herniate, exerting pressure on any of the nerves rooted to the spinal cord. When spinal nerves become compressed and irritated, back pain and sciatica may result.
Ruptured disks – each vertebra in our spine is cushioned by disks. If the disk ruptures there will be more pressure on a nerve, resulting in back pain.
Bulging disks – in much the same way as ruptured disks, a bulging disk can result in more pressure on a nerve.
Sciatica– a sharp and shooting pain that travels through the buttock and down the back of the leg, caused by a bulging or herniated disk pressing on a nerve.
Arthritis – patients with osteoarthritis commonly experience problems with the joints in the hips, lower back, knees and hands. In some cases, spinal stenosis can develop, which is the term used to describe when the space around the spinal cord narrows.
Abnormal curvature of the spine – if the spine curves in an unusual way the patient is more likely to experience back pain. An example is scoliosis, a condition in which the spine curves to the side.
Osteoporosis– bones, including the vertebrae of the spine, become brittle and porous, making compression fractures more likely.
Spinal stenosis – is a narrowing of the spinal column that puts pressure on the spinal cord and nerves that can cause pain or numbness with walking and over time leads to leg weakness and sensory loss.
Skeletal irregularities – include scoliosis, a curvature of the spine that does not usually cause pain until middle age; lordosis, an abnormally accentuated arch in the lower back; and other congenital anomalies of the spine.
Abdominal aortic aneurysms – occur when the large blood vessel that supplies blood to the abdomen, pelvis, and legs becomes abnormally enlarged. Back pain can be a sign that an aneurysm is becoming larger and that the risk of rupture should be assessed.
Kidney stones – can cause sharp pain in the lower back, usually on one side.
Below are some other causes of back pain
Cauda equina syndrome – the cauda equine is a bundle of spinal nerve roots that arise from the lower end of the spinal cord. People with cauda equine syndrome feel a dull pain in the lower back and upper buttocks, as well as analgesia (lack of feeling) in the buttocks, genitalia, and thigh. There are sometimes bowel and bladder function disturbances.
Cancer of the spine – a tumor located on the spine may press against a nerve, resulting in back pain.
Infection of the spine – if the patient has an elevated body temperature (fever) as well as a tender warm area on the back, it could be caused by an infection of the spine.
Other infections – pelvic inflammatory disease (females), bladder, or kidney infections may also lead to back pain.
Endometriosis – is the buildup of uterine tissue in places outside the uterus.
Fibromyalgia – a chronic pain syndrome involving widespread muscle pain and fatigue.
Sleep disorders – individuals with sleep disorders are more likely to experience back pain, compared to others.
Shingles – an infection that can affect the nerves may lead to back pain, depending on the nerves affected.
Bad mattress – if a mattress does not support specific parts of the body and keep the spine straight, there is a greater risk of developing back pain.
Everyday activities or poor posture
Back pain can also be the result of some everyday activity or poor posture. Examples include:
Adopting a very hunched sitting position when using computers can result in increased back and shoulder problems over time.
Bending awkwardly
Pushing something
Pulling something
Carrying something
Lifting something
Standing for long periods
Bending down for long periods
Twisting
Coughing
Sneezing
Muscle tension
Over-stretching
Straining the neck forward, such as when driving or using a computer
Long driving sessions without a break, even when not hunched
Exertion or lifting.
Severe blow or fall.
Back disorders.
Infections.
Ruptured lumbar disk.
Nerve dysfunction.
Osteoporosis.
Spondylosis (hardening and stiffening of the spinal column).
The main symptom of back pain is, as the name suggests, an ache or pain anywhere on
Pain in the back, and sometimes all the way down to the buttocks and legs. Some back issuescan cause pain in other parts of the body, depending on the nerves affected.
In most cases, signs, and symptoms clear up on their own within a short period.If any of the following signs or symptoms accompany a back pain, people should see their doctor:
Pain. It may be continuous, or only occur when you are in a certain position. The pain may be aggravated by coughing or sneezing, bending or twisting.
Patients who have been taking steroids for a few months
Drug abusers
Patients with cancer
Patients who have had cancer
Patients with depressed immune systems
Stiffness.
According to the British National Health Service (NHS), the following groups of people should seek medical advice if they experience back pain:
Weight loss
Elevated body temperature (fever)
Inflammation (swelling) on the back
Persistent back pain – lying down or resting does not help
Pain down the legs
Pain reaches below the knees
A recent injury, blow or trauma to your back
Urinary incontinence – you pee unintentionally (even small amounts)
Difficulty urinating – passing urine is hard
Fecal incontinence – you lose your bowel control (you poo unintentionally)
Numbness around the genitals
Numbness around the anus
Numbness around the buttocks
dull ache,
numbness,
tingling,
sharp pain,
pulsating pain,
pain with movement of the spine,
pins and needles sensation,
muscle spasm,
tenderness,
sciatica with shooting pain down one or both lower extremities
People aged less than 20 and more than 55 years
Additionally, people who experience pain symptoms after a major trauma (such as a car accident) are advised to see a doctor. If low back pain interferes with daily activities, mobility, sleep, or if there are other troubling symptoms, medical attention should be sought.
Risk increases with
Biomechanical risk factors.
Sedentary occupations.
Gardening and other yard work.
Sports and exercise participation, especially if infrequent.
Obesity.
Preventive measures
Exercises to strengthen lower back muscles.
Learn how to lift heavy objects.
Sit properly.
Back support in bed.
Lose weight, if obese.
Choose proper footwear.
Wear special back support devices.
Red flag conditions indicating possible underlying spinal pathology or nerve root problemsw9
Red flags
Onset age < 20 or > 55 years
Non-mechanical pain (unrelated to time or activity)
Thoracic pain
Previous history of carcinoma, steroids, HIV
Feeling unwell
Weight loss
Widespread neurological symptoms
Structural spinal deformity
Indicators for nerve root problems
Unilateral leg pain > low back pain
Radiates to foot or toes
Numbness and paraesthesia in the same distribution
Straight leg raising test induces more leg pain
Localized neurology (limited to one nerve root)
Diagnosis of Lumbago /Backache
Suspected disk, nerve, tendon, and other problems – X-rays or some other imaging scan, such as a CT (computerized tomography) or MRI (magnetic resonance imaging) scan may be used to get a better view of the state of the soft tissues in the patient’s back.
X-rays – can show the alignment of the bones and whether the patient has arthritis or broken bones. They are not ideal for detecting problems with muscles, the spinal cord, nerves or disks.
MRI or CT scans – these are good for revealing herniated disks or problems with tissue, tendons, nerves, ligaments, blood vessels, muscles and bones.
Bone scan – a bone scan may be used for detecting bone tumors or compression fractures caused by brittle bones (osteoporosis). The patient receives an injection of a tracer (a radioactive substance) into a vein. The tracer collects in the bones and helps the doctor detect bone problems with the aid of a special camera.
Electromyography or EMG – the electrical impulses produced by nerves in response to muscles is measured. This study can confirm nerve compression which may occur with a herniated disk or spinal stenosis (narrowing of the spinal canal).
[stextbox id=’info’]
Types of low back pain associated with physical findings of no clear pathoanatomical significance
Syndrome
Findings
Assessment/Plan
Facet syndrome
History and physical examination:
local and pseudoradicular symptoms and signs
pain on movement
facet tenderness
pain on reclination
positive injection test
joint dysfunction on manual diagnosis
Radiological findings (not indicated on intial evaluation):
differentiation from high-grade or activated spondylarthrosis (possibly, juxtaforaminal cyst) or
Treatment of Backache is a common disorder involving the muscles, nerves, and bones of the back. Pain can vary from a dull constant ache to a sudden sharp feeling. Low back pain may be classified by duration as acute (pain lasting less than 6 weeks), sub-chronic (6 to 12 weeks), or chronic (more than 12 weeks). The condition may be further classified by the underlying cause as either mechanical, non-mechanical, or referred pain. The symptoms of low back pain usually improve within a few weeks from the time they start, with 40-90% of people completely better by six weeks.
Acute low-back pain without sciatica, with some spread of discomfort to the region of the sacroiliac joint, to the outer part of the buttock as well as to the lateral and the back part of the thigh, is a unifying symptom of a very common clinical syndrome whose exact underlying cause remains often uncertain. Most patients fall then into the category of non-specific low-back pain. Probably the pathogenesis is not uniform, and the pain can arise from a variety of structures (muscles, ligament, spine). Pain which persists after 3 to 4 days should warn the clinician that a serious pathological condition may be present which requires a new approach to diagnosis and treatment.
Treatment of Lumbago /Backache
General measures
Bed rest for first 24 hours. Additional bed rest will be determined by the severity of the problem. Recent medical studies indicate that staying more active is better for back disorders than prolonged bed rest.
Use a firm mattress (place a bed board under the mattress if needed).
An ice pack or cold massage or heat applied to the affected area with a heating pad or hot water bottle.
Physical therapy.
Massage may help. Be sure the person is well-trained or massage could cause more harm than help.
Wear a special back support device.
Other options are available depending on the degree of injury, such as surgery (if disk damaged), electrical nerve stimulation, acupuncture, special shoes, etc.
Stress reduction techniques, if needed.
Non-Prescription Pain Relievers – Naproxen, acetaminophen, and ibuprofen each reduce inflammation and pain. Though these drugs are available over-the-counter, they are potent and taking more than the recommended dose can harm health. A doctor can help with advice about the right kind of non-prescription pain reliever to take.
Cold and Heat – Applying a cold pack to the painful part of the back contracts inflamed muscle and relieves pain. This treatment helps a great deal when the disk has recently ruptured and swelling is at its greatest. A heating pad or warm pack helps with residual pain.
Continued Physical Activity – Though pain or weakness seem like good reasons to rest the back, excessive bed-rest worsens the symptoms of a slipped disc. Moving around too little allows muscles to grow weaker and prevents the body from healing. Periods of rest interspersed with periods of normal activity throughout the day keep the back muscles in shape.
Prescription Remedies – If over-the-counter drugs fail to ease slipped disc pain, the doctor will turn to prescription medications. These can include narcotics, such as hydrocodone or codeine. While they can do away with pain, narcotics are very addictive and induce a mental fogginess that can itself be dangerous. More narrowly-focused medicines designed to target damaged nerves that create chronic pain may be a better choice, as they have fewer undesirable side effects. Gabapentin and Cymbalta are two drugs that act in different ways to minimize nerve pain. These drugs are less addictive than narcotics.
Physical Therapy – Physical therapists show slipped disc sufferers ways to move that do not cause pain. Occupational therapists teach skills that allow patients to return to a productive life.
Nutrition – In order to restore the disc we also are going to need to include different substances in our diet. There are a lot of supplements on the market, of course. If you wish to try them, that’s fine. I personally don’t like them. I have tried one with glucosamine and chondroitin, but I didn’t feel any different. So, if you have the opportunity to take these with the food or from more natural sources, it will be great. You can find these substances in sea food and animal cartilages and by digesting them we ensure the building blocks for the connecting tissue for our joints and spine. Also we will need more Omega 3 fatty acids, which can be supplied from cold pressed oils, fatty fish, flax seeds, chia and many more. Vitamins from the B group are very beneficial for people with herniated discs and all kinds of issues with the peripheral nervous system. Vitamins B1, B6 and B12 nourish the nerves and help them recover from the disk accident. Usually doctors prescribe them as a part of the treatment, but it is worth mentioning anyway.
A good massage – A massage is one of the natural methods of relieving pain. Individuals who get a massage weekly for several months stand a better chance of alleviating back pain. A good massage provides a person with many health benefits that lessen back pain. A massage triggers the release of endorphins. Endorphins aid in decreasing anxiety and relieving pain. They offer a relaxation effect by softening muscles that are injured preventing cramping.
Undertaking yoga – Yoga is an applicable strategy of keeping the level of back pain at minimal levels. Taking yoga sessions often is very an effective method of dealing with back pain. With yoga, there is a high likelihood of proper body functions. The use of pain prescriptions is also diminished. Patients suffering from back pain related issues do not have to rely on these prescriptions to manage pain. Incorporating laughter in yoga is a good way of exercising. Yoga incorporates simple yet appropriate exercises that enhance stretching of muscles. Laughter with yoga stimulates relieving of pain. It facilitates increased uptake of oxygen, little anxiety and production of endorphins. All these variables play an essential role in diminishing back pain.
Adjusting sleeping position – A simple sleeping mistake can immensely contribute to back pain. A poor sleeping position can cause stress and tension on the muscles contributing to back pain. Altering one’s sleeping position and adopting a style that does not exert a lot of stress on the back is a recommended tactic. Nurturing sleeping habits such as assuming a reclining position, using wedge-shaped cushions and getting adjustable beds from reputable medical institutions are easy techniques to endorse. If a reclining position does not suit an individual, the other two techniques can be embraced.
Heat therapy – Several considerations should be observed when using heat therapy. The right temperature ought to be set so as to ensure a patient does not face risks associated with too much exposure to heat. The key objective should be to ensure enough access of heat to the muscles to yield benefits for the patient. The adoption of heat therapy for easing back pain is determined by the magnitude of pain a person is experiencing. In cases where relatively low back pain is encountered, short heat therapy sessions are recommended. On the other hand, if an individual is experiencing prolonged back pain, long heat therapy sessions are the most applicable.
Taking hot baths – This is a form of heat therapy that aims at relieving back pain. It guarantees permeation of heat into the muscles leading to reduced pain. Many individuals opt for this method since they believe it achieves competent results. Hot baths initiate a fast process of blood supply to stiff neck and back muscles. When this happens, the muscles relax and stretch leading to decreased back pain. To avoid interference with one’s sleeping patterns, a hot bath should be taken several hours before retiring to bed.
Aquatic therapy – This natural technique involves physical therapy in a pool. Individuals get the best out of this therapy by relying on the resistance of water. Consistency in undertaking this therapy is what ascertains getting back pain relief. Integrating aquatic therapy in an individual’s life for the better part of the week enhances reduction of back pain quickly.
Enlighten others – Individuals have the power to devise their own natural strategies that aid them in coping with back pain. The strategies can also be a good remedy for others going through similar circumstances. An individual can use social media platforms to equip others with important tips on how to keep back pain at bay. Further, becoming a member of associations that address back pain issues enables better communication of the knowledge gained from personal experience.
Medications
A wide range of medications are used to treat acute and chronic low back pain. Some are available over the counter (OTC); others require a physician’s prescription. Certain drugs, even those available OTC, may be unsafe during pregnancy, may interact with other medications, cause side effects, or lead to serious adverse effects such as liver damage or gastrointestinal ulcers and bleeding. Consultation with a health care provider is advised before use. The following are the main types of medications used for low back pain:
Analgesic medications – are those specifically designed to relieve pain. They include OTC acetaminophen and aspirin, as well as prescription opioids such as codeine, oxycodone, hydrocodone, and morphine. Opioids should be used only for a short period of time and under a physician’s supervision. People can develop a tolerance to opioids and require increasingly higher dosages to achieve the same effect. Opioids can also be addictive. Their side effects can include drowsiness, constipation, decreased reaction time, and impaired judgment. Some specialists are concerned that chronic use of opioids is detrimental to people with back pain because they can aggravate depression, leading to a worsening of the pain.
Nonsteroidal anti-inflammatory drugs(NSAIDS) – relieve pain and inflammation and include OTC formulations (ibuprofen, ketoprofen, and naproxen sodium). Several others, including a type of NSAID called COX-2 inhibitors, are available only by prescription. Long-term use of NSAIDs has been associated with stomach irritation, ulcers, heartburn, diarrhea, fluid retention, and in rare cases, kidney dysfunction and cardiovascular disease. The longer a person uses NSAIDs the more likely they are to develop side effects. Many other drugs cannot be taken at the same time a person is treated with NSAIDs because they alter the way the body processes or eliminates other medications.
Anticonvulsants—drugs primarily used to treat seizures—may be useful in treating people with radiculopathy and radicular pain.
Antidepressants – such as tricyclics and serotonin and norepinephrine reuptake inhibitors have been commonly prescribed for chronic low back pain, but their benefit for nonspecific low back pain is unproven, according to a review of studies assessing their benefit.
Muscle Relaxants – If the muscles around the slipped disc experience painful spasms, a muscle relaxant such as Valium may be useful. The drawback to drugs like these is that they do not limit their power to the affected nerve. Instead, they have a generally relaxing effect and will interfere with daily activities.
Such as cyclobenzaprine (Flexeril), might be prescribed to relieve the discomfort associated with muscle spasms. However, these medicines might cause confusion in older people. Depending on the level of pain, prescription pain medicines might be used in the initial period of treatment.
Steroids – If inflammation is severe, a doctor may also prescribe a steroid. Steroids, such as cortisone, reduce swelling quickly. A cortisone shot directly in the affected area will have an immediate effect on the displaced disc.
Counter-irritants – such as creams or sprays applied topically stimulate the nerves in the skin to provide feelings of warmth or cold in order to dull the sensation of pain. Topical analgesics reduce inflammation and stimulate blood flow.
Nerve Ralaxant — Pregabalin or gabapentin and anti-inflammatory drugs help to relieve pain and stiffness, allowing for increased mobility and exercise. There are many common over-the-counter medicines called non-steroidal anti-inflammatory drugs (NSAIDs). They include aspirin, ibuprofen (Motrin, Advil), and naproxen (Naprosyn, Aleve).
Spinal manipulation and spinal mobilization – Are approaches in which professionally licensed specialists (doctors of chiropractic care) use their hands to mobilize, adjust, massage, or stimulate the spine and the surrounding tissues. Manipulation involves a rapid movement over which the individual has no control; mobilization involves slower adjustment movements. The techniques have been shown to provide small to moderate short-term benefits in people with chronic low back pain. Evidence supporting their use for acute or subacute low back pain is generally of low quality. Neither technique is appropriate when a person has an underlying medical cause for the back pain such as osteoporosis, spinal cord compression, or arthritis.
Traction – Involves the use of weights and pulleys to apply constant or intermittent force to gradually “pull” the skeletal structure into better alignment. Some people experience pain relief while in traction, but that relief is usually temporary. Once traction is released the back pain tends to return. There is no evidence that traction provides any longterm benefits for people with low back pain.
Spinal injections — An injection of a cortisone-like anti-inflammatory medicine into the lower back might help reduce swelling and inflammation of the nerve roots, allowing for increased mobility.
Biofeedback – It is used to treat many acute pain problems, most notably back pain and headache. The therapy involves the attachment of electrodes to the skin and the use of an electromyography machine that allows people to become aware of and selfregulate their breathing, muscle tension, heart rate, and skin temperature. People regulate their response to pain by using relaxation techniques. Biofeedback is often used in combination with other treatment methods, generally without side effects. The evidence is lacking that biofeedback provides a clear benefit for low back pain.
Nerve block therapies – Aim to relieve chronic pain by blocking nerve conduction from specific areas of the body. Nerve block approaches range from injections of local anesthetics, botulinum toxin, or steroids into affected soft tissues or joints to more complex nerve root blocks and spinal cord stimulation. When extreme pain is involved, low doses of drugs may be administered by catheter directly into the spinal cord. The success of a nerve block approach depends on the ability of a practitioner to locate and inject precisely the correct nerve. Chronic use of steroid injections may lead to increased functional impairment.
Surgery Lumbago /Backache
When other therapies fail, surgery may be considered an option to relieve pain caused by serious musculoskeletal injuries or nerve compression. It may be months following surgery before the patient is fully healed, and he or she may suffer permanent loss of flexibility.
Vertebroplasty and kyphoplasty – are minimally invasive treatments to repair compression fractures of the vertebrae caused by osteoporosis. Vertebroplasty uses three-dimensional imaging to assist in guiding a fine needle through the skin into the vertebral body, the largest part of the vertebrae. A glue-like bone cement is then injected into the vertebral body space, which quickly hardens to stabilize and strengthen the bone and provide pain relief. In kyphoplasty, prior to injecting the bone cement, a special balloon is inserted and gently inflated to restore height to the vertebral structure and reduce spinal deformity.
Spinal laminectomy – (also known as spinal decompression) is performed when spinal stenosis causes a narrowing of the spinal canal that causes pain, numbness, or weakness. During the procedure, the lamina or bony walls of the vertebrae, along with any bone spurs, are removed. The aim of the procedure is to open up the spinal column to remove pressure on the nerves.
Discectomy or microdiscectomy – may be recommended to remove a disc, in cases where it has herniated and presses on a nerve root or the spinal cord, which may cause intense and enduring pain. Microdiscectomy is similar to a conventional discectomy; however, this procedure involves removing the herniated disc through a much smaller incision in the back and a more rapid recovery. Laminectomy and discectomy are frequently performed together and the combination is one of the more common ways to remove pressure on a nerve root from a herniated disc or bone spur.
Foraminotomy – is an operation that “cleans out” or enlarges the bony hole (foramen) where a nerve root exits the spinal canal. Bulging discs or joints thickened with age can cause narrowing of the space through which the spinal nerve exits and can press on the nerve, resulting in pain, numbness, and weakness in an arm or leg. Small pieces of bone over the nerve are removed through a small slit, allowing the surgeon to cut away the blockage and relieve pressure on the nerve.
Intradiscal electrothermal therapy (IDET) – is a treatment for discs that are cracked or bulging as a result of degenerative disc disease. The procedure involves inserting a catheter through a small incision at the site of the disc in the back. A special wire is passed through the catheter and an electrical current is applied to heat the disc, which helps strengthen the collagen fibers of the disc wall, reducing the bulging and the related irritation of the spinal nerve. IDET is of questionable benefit.
Nucleoplasty also called plasma disc decompression (PDD) – is a type of laser surgery that uses radiofrequency energy to treat people with low back pain associated with mildly herniated discs. Under x-ray guidance, a needle is inserted into the disc. A plasma laser device is then inserted into the needle and the tip is heated to 40-70 degrees Celsius, creating a field that vaporizes the tissue in the disc, reducing its size and relieving pressure on the nerves. Several channels may be made depending on how tissue needs to be removed to decompress the disc and nerve root.
Radiofrequency denervation – is a procedure using electrical impulses to interrupt nerve conduction (including the conduction of pain signals). Using x-ray guidance, a needle is inserted into a target area of nerves and a local anesthetic is introduced as a way of confirming the involvement of the nerves in the person’s back pain. Next, the region is heated, resulting in localized destruction of the target nerves. Pain relief associated with the technique is temporary and the evidence supporting this technique is limited.
Spinal fusion – is used to strengthen the spine and prevent painful movements in people with degenerative disc disease or spondylolisthesis (following laminectomy). The spinal disc between two or more vertebrae is removed and the adjacent vertebrae are “fused” by bone grafts and/or metal devices secured by screws. The fusion can be performed through the abdomen, a procedure known as an anterior lumbar interbody fusion, or through the back, called posterior fusion. Spinal fusion may result in some loss of flexibility in the spine and requires a long recovery period to allow the bone grafts to grow and fuse the vertebrae together. Spinal fusion has been associated with an acceleration of disc degeneration at adjacent levels of the spine.
Artificial disc replacement – is considered an alternative to spinal fusion for the treatment of people with severely damaged discs. The procedure involves removal of the disc and its replacement by a synthetic disc that helps restore height and movement between the vertebrae.
Other Rx of Lumbago /Backache
Chiropractic Care
Sixty percent of people with sciatica who didn’t get relief from other therapies and then tried spinal manipulation experienced the same degree of pain relief as patients who eventually had surgery, found a 2010 study in the Journal of Manipulative and Physiological Therapeutics. The 120 people in the study saw a chiropractor about 3 times a week for 4 weeks and then continued weekly visits, tapering off treatment as they felt better. In people who responded to chiropractic care, benefits lasted up to a year. “Spinal manipulation may create a response in the nervous system that relieves pain and restores normal mobility to the injured area,” says study researcher Gordon McMorland, DC, of National Spine Care in Calgary, Alberta. “It also reduces inflammation, creating an environment that promotes the body’s natural healing mechanisms.”
Acupuncture
You can get relief as soon as the first session, though it takes about 12 sessions to see improvement,” says Jingduan Yang, MD, assistant professor at the Jefferson Myrna Brind Center of Integrative Medicine at Thomas Jefferson University. A small study in the Journal of Traditional Chinese Medicine found that of 30 people with sciatica, 17 got complete relief and 10 saw symptoms improve with warming acupuncture, in which the needles are heated.
Yoga
A study in the journal Pain reported that people with chronic back pain who practiced Iyengar yoga for 16 weeks saw pain reduced by 64% and disability by 77%. Although yoga’s effects on sciatica are less clear, gentle forms may be beneficial. By strengthening muscles and improving flexibility, a yoga practice can help sciatica sufferers “move and function better so they don’t fall into a posture that aggravates sciatica,” says James W. Carson, Ph.D., a psychologist at the Comprehensive Pain Center at Oregon Health & Science University. For extra grip and stability, try these grip socks from Natural Fitness.
Massage
Don’t expect a chilled-out spa massage if you have sciatica. In this instance, trigger-point therapy is best, says Jeff Smoot, vice president of the American Massage Therapy Association. The sciatic nerve sits underneath a muscle called the piriformis, which is located beneath the glutes. “When the piriformis muscle gets tight, it pinches the sciatic nerve, causing tingling and numbness down into the leg,” says Smoot. He applies pressure to irritated and inflamed areas, or trigger points, in the piriformis muscle, as well as in muscles in the lower back and glutes. Typically, Smoot schedules treatments 7 to 10 days apart. If patients don’t see progress by the fourth visit, “they need to try another form of therapy,” he says.
Shiatsu,
Also known as finger pressure therapy, is a type of massage where pressure is applied along energy lines in the body. The shiatsu therapist applies pressure with his/her fingers, thumbs and elbows.
Topical Preparations
St. John’s wort oil, a liniment, is “one of my favorites for nerve pain,” says Tieraona Low Dog, MD, director of the fellowship at the Arizona Center for Integrative Medicine. Apply the anti-inflammatory oil two or three times a day where there’s pain. Another option: an OTC cayenne pepper plaster or cream; capsaicin, found in chiles, hinders the release of pain-causing compounds from nerves. For severe cases, Low Dog uses the prescription chile patch Qutenza, designed for shingles pain. “One application is effective for weeks,” says Low Dog.
Ice or Heat
Because the sciatic nerve is buried deep within the buttock and leg, ice or heat on the surface of the body won’t ease that inner inflammation. But the timehonored treatments can act as counterirritants—that is, “they give your body other input in the painful area, and that brings the pain down a notch,” says Ruppert. Apply an ice pack or a heating pad as needed for 15 minutes.
Devil’s Claw
The herbal medication devil’s claw is “quite a potent anti-inflammatory, working like ibuprofen and similar drugs to inhibit substances that drive inflammation,” says Low Dog. She generally starts patients on 1,500 to 2,000 mg twice a day. Look for a brand that has a standardized extract of roughly 50 mg of harpagoside, the active compound. Safety reviews show that the supplement is well tolerated by most people but should be avoided by patients with peptic ulcers or on blood-thinning medications.
Pain Relievers and Muscle Relaxants
Taking a nonsteroidal anti-inflammatory drug, either OTC (like ibuprofen) or Rx, can ease the distress. Because painful muscle spasms may also accompany a disk herniation, doctors sometimes prescribe muscle relaxants or pain-reducing tricyclic antidepressants. A caveat: “These won’t help with the pain caused by pressure on the sciatic nerve,” says A. Nick Shamie, MD, a spokesperson for the American Academy of Orthopaedic Surgeon.
Epidural Steroid Injections
People whose pain doesn’t lessen within about a month and who aren’t helped by other therapies may find their pain remedied by an x-ray-guided injection of steroid into the lower back near the sciatic nerve, says Raj Rao, MD, a spokesperson for the AAOS. “The hope is to reduce inflammation within that nerve branch,” explains Rao. Because of concerns about side effects, such as loss of bone density, the epidural shots are limited to three a year.
CBT (cognitive behavioral therapy)
CBT can help patients manage chronic back pain. The therapy is based on the principle that the way a person feels is, in part, dependent on the way they think about things.
People who can be taught to train themselves to react in a different way to pain may experience less perceived pain. CBT may use relaxation techniques as well as strategies to maintain a positive attitude. Studies have found that patients with CBT tend to become more active and do exercise, resulting in a lower risk of back pain recurrence.
Exercise and Physical Therapy
Moving is usually the last thing people dogged by sciatica want to do, but it’s important to be physically active. “Lying in bed makes it more likely that the pain will last longer,” says Ruppert. “Exercise increases blood flow to the disk and the nerve, helping to get rid of the chemicals causing the inflammation.” Take 15- to 20-minute walks. If that hurts too much, give swimming or water aerobics a try; there’s not as much pressure on the back when you’re in the water, says Ruppert. It may also be worth seeing a physical therapist, who can prescribe stretching exercises to restore flexibility to the back or moves that strengthen core muscles, helping to stabilize the spine and reduce the likelihood of a similar injury.
Here are six exercises for Lumbago /Backache
Pigeon pose
Pigeon Pose is a common yoga pose. It works to broadly open the hips. There are multiple versions of this stretch. The first is a starting version of the pigeon pose, known as the reclining pigeon pose. If you are just starting your treatment, you should try the reclining pose first. Once you can do the reclining version without pain, work with your physical therapist on the sitting and forward versions.
Reclining pose
While on the back, bring your right leg up to a right angle and grasp it with both hands behind the thigh, locking your fingers.
Take your left leg and place your ankle against the knee. Hold the position for a moment before changing legs. This helps stretch the tiny piriformis muscle, which sometimes becomes inflamed and presses against the sciatic nerve causing pain.
Repeat by switching sides and doing the same exercise with the other leg.
Sitting pose
Sit on the floor with your legs stretched out straight in front of you. Then bend your right leg, putting your right ankle on top of the left knee.
Lean forward and allow your upper body to lean toward your thigh. Hold for 15 to 30 seconds and then switch sides. This stretches the glutes and lower back.
Forward pose
Kneel on the floor on all fours.
Pick up your right leg and move it forward so that your lower leg is on the ground, horizontal to the body. Your right foot should be in front of your right knee while your right knee stays to the right.
Stretch the left leg out all the way behind you on the floor, with the top of the foot on the ground and toes pointing back.
Shift your body weight gradually from your arms to your legs so that your legs are supporting your weight. Sit up straight with your hands on either side of your legs.
Take a deep breath. While exhaling, lean your upper body forward over your lower leg. Support your weight with your arms as much as possible.
Knee to opposite shoulder
This simple stretch helps relieve sciatica pain by loosening your gluteal and piriformis muscles, which can become inflamed and press against the sciatic nerve.
Lie on your back with your legs extended outward and your feet flexed upward.
Clasp your hands around your knee and gently pull your right leg across your body toward your left shoulder. Hold it there for 30 seconds and then push your knee so your leg returns to its starting position.
Repeat for a total of 3 reps, and then switch legs. Remember to only pull your knee as far as it will comfortably go. You should feel a relieving stretch in your muscle, not pain.
Sitting spinal stretch
Sciatica pain is triggered when vertebrae in the spine compress. This stretch helps create space in the spine to relieve pressure from the sciatic nerve.
Sit on the ground with your legs extended straight out with your feet flexed upward.
Bend your right knee and place your foot flat on the floor on the outside of your opposite knee.
Place your left elbow on the outside of your right knee to help you gently turn your body toward the right. Hold for 30 seconds and repeat three times, then perform this stretch with your left leg bent and body turned to the left side.
Standing hamstring stretch
This stretch can help ease pain and tightness in the hamstring caused by sciatica.
Place your right foot on an elevated surface at or below your hip level. This could be a chair, ottoman, or step on a staircase. Flex your foot so your toes and leg are straight. If your knee tends to hyperextend, keep a slight bend in it.
Bend your body forward slightly toward your foot. The further you go, the deeper the stretch. Do not push so far that you feel pain.
Release the hip of your raised leg downward as opposed to it lifting up. If you need help easing your hip down, loop a yoga strap or long exercise band over your right thigh and under your left foot. Hold for at least 30 seconds, and then repeat on the other side.
Exercise with care
Kovacs emphasizes that you should not assume that you will be able to be as flexible as the exercises ideally call for. “Don’t think that because of what you see on YouTube or TV that you can get into these positions,” he said. “Most people who demonstrate the exercises have great flexibility and have been doing it for years. If you have any kind of pain, you should stop.”
Corina Martinez, a physical therapist at Duke Sports Medicine Center and a member of the American Medical Society for Sports Medicine, says that there is no one-size-fits-all exercise for people suffering from sciatic nerve pain. “Do you feel better when you bring your knees to the chest, or when they extend back a little more? If one feels better, that is the treatment you want to pursue.”
Martinez says that anyone experiencing even mild sciatic nerve pain symptoms for more than a month should see a doctor or physical therapist. They may find relief with an in-home exercise program tailored specifically to how their pain presents itself.
What complications are associated with
Chronic (ongoing and lasting) pain is a complication of untreated sciatica. If the “pinched nerve” is seriously injured, chronic muscle weakness, such as a “drop foot,” might occur.
What is the outlook for people with
Sciatic pain usually goes away with time and rest. Most people with sciatica (80 percent to 90 percent) will get better without surgery. About half of affected individuals recover from an episode within six weeks.
Can sciatica be prevented?
Some sources of sciatica are not preventable, such as degenerative disc disease, back strain due to pregnancy, and accidental falls.
Although it might not be possible to prevent all cases of sciatica, you can take steps to protect your back and reduce your risk.
Practice proper lifting techniques. Lift with your back straight, bringing yourself up with your hips and legs, and holding the object close to your chest. Use this technique for lifting everything, no matter how light.
Avoid/ stop cigarette smoking, which promotes disc degeneration.
Exercise regularly to strengthen the muscles of your back and abdomen, which work to
support your spine.
Use good posture when sitting, standing, and sleeping. Good posture helps to relieve the pressure on your lower back.
Avoid sitting for long periods.
Preventing Lumbago /Backache
Steps to lower the risk of developing back pain consist mainly of addressing some of the risk factors.
Exercise – regular exercise helps build strength as well as keeping your body weight down. Experts say that low-impact aerobic activities are best; activities that do not strain or jerk the back. Before starting any exercise program, talk to a health care professional.
There are two main types of exercise that people can do to reduce the risk of back pain:
Core-strengthening exercises– exercises that work the abdominal and back muscles, helping to strengthen muscles that protect the back.
Flexibility – exercises aimed at improving flexibility in your core, including your spine, hips, and upper legs, may help too.
Smoking – a significantly higher percentage of smokers have back pain incidences compared to non-smokers of the same age, height and weight.
Body weight – the amount of weight people carry, as well as where they carry it, affects the risk of developing back pain. The difference in back pain risk between obese and normal-weight individuals is considerable. People who carry their weight in the abdominal area versus the buttocks and hip area are also at greater risk.
Posture when standing – make sure you have a neutral pelvic position. Stand upright, head facing forward, back straight, and balance your weight evenly on both feet – keep your legs straight and your head in line with your spine.
If you regularly use a computer, it is important to ensure that you have a chair with good back support and adopt a good posture and head position.
Posture when sitting – a good seat should have good back support, arm rests and a swivel base (for working). When sitting try to keep your knees and hips level and keep your feet flat on the floor – if you can’t, use a footstool. You should ideally be able to sit upright with support in the small of your back. If you are using a keyboard, make sure your elbows are at right-angles and that your forearms are horizontal.
Lifting things – the secret for protecting your back when lifting things is to think “legs not back”. In other words, use your legs to do the lifting, more than your back.
Keep your back as straight as you can, keeping your feet apart with one leg slightly forward so you can maintain balance. Bend only at the knees, hold the weight close to your body, and straighten the legs while changing the position of your back as little as possible.
Bending your back initially is unavoidable, but when you bend your back try not to stoop or squat, and be sure to tighten your stomach muscles so that your pelvis is pulled in. Most important, do not straighten your legs before lifting; otherwise you will be using your back for most of the work.
Do not lift and twist at the same time. If something is particularly heavy, see if you can lift it with someone else. While you are lifting keep looking straight ahead, not up nor down, so that the back of your neck is like a continuous straight line from your spine.
Moving things – remember that it is better for your back to push things across the floor, using your leg strength, rather than pulling them.
Shoes – flat shoes place less of a strain on the back.
Driving – it is important to have proper support for your back. Make sure the wing mirrors are properly positioned so you do not need to twist. The pedals should be squarely in front of your feet. If you are on a long journey, have plenty of breaks – get out of the car and walk around.
Your bed – you should have a mattress that keeps you spine straight, while at the same time supporting the weight of your shoulders and buttocks. Use a pillow, but not one that forces your neck into a steep angle.
Home Remedies for Lumbago /Backache
Ice and Heat
Ice works wonders on lower back pain. Wrap some ice cubes in a plastic bag to prepare an ice pack. Then cover it with a towel and apply it on the painful area for 20 minutes. Repeat the same process several times a day. Then after 48 hours, you can switch to heat method. Dip a towel in warm water. Flatten and fold it on to the affected area. Place heating pad on it with a plastic cover between towel and heating pad. Leave it for 20 minutes. Do it several times a day. It reduces swelling and relaxes the nerves that are responsible for sending pain signals to the brain.
Rest
Get sufficient rest. Don’t exhaust yourself physically and mentally. When sleeping, keep changing your positions. When you lie on back, put a pillow under your knees. Similarly, if you lie on your side, draw your knees near your chest and keep a pillow between your knees.
Right Posture
Your sitting and standing posture are very important to keep back pain at bay. One should not be in bending position for long time whether sitting or standing. Sitting on the edge of the chair and slouching should be avoided. The angle of the chair in office should be 110 degree.
Lemon Juice
Lemon juice is an effective home remedy for back pain. Drink lemon juice twice a day for better results.
Poppy Seeds
Prepare a mixture of poppy seeds and rock candy by grinding together 100 gm of each. Take this mixture twice a day with a glass of milk. You will get relief from back pain.
Massage with Olive Oil
Massage with olive oil to reduce stress by relaxing tensed muscles. It also helps release stiffness in joints and relieves upper back pain.
Stretching
Stretching is the easiest back pain treatment. If your job demands sitting or standing for long hours, just take a break of 5 minutes every hour and walk or simply stretch your body to avoid back pain.
Wheat
Wheat has pain minimizing component in it. Mix cuscus grass and coriander with overnight soaked wheat. Add 1 cup of milk and bring it to boil. Consume this mixture twice a day
Garlic
Eat 2-3 garlic cloves on an empty stomach every morning to get relief from back pain. You can also use garlic oil. Massage your back with this oil, cover it with warm blanket and lie on your back. Bathe using warm water after 20 minutes. This is a wonderful home remedy to treat back pain.
Ginger
The anti-inflammatory properties of ginger make it an ideal home remedy to get rid of back pain. Add ½ teaspoon of black peppercorns, ½ teaspoon of cloves and 1 teaspoon of ginger powder in a cup of boiling water to prepare herbal tea. Drink it 2-3 times a day.
Alternatively, grate some ginger to prepare a paste. Apply it on the affected area. Then massage with eucalyptus oil.
Put thin ginger slices in a pan of boiling water. Simmer it for 10-15 minutes. Strain and allow it to cool down at room temperature. Add honey to sweeten it. Drink it twice or thrice a day.
Milk
Since milk is a great source of calcium, it is extremely beneficial for strong bones and preventing back pain. People of every age group should consume milk. For quick relief, add a few drops of honey and a pinch of turmeric in the milk.
Epsom Salt
A natural healer, epsom salt reduces swelling in back. It contains magnesium and sulfate which help muscles function properly, thus, provide relief from pain. Add 2 cups of Epsom salt to a tub of warm water. Let it soak for 30 minute. Take bath with this water.
Rice
Rice is easily available in every household. It’s an effective home remedy for back pain. Put 1 cup uncooked rice in a thick sock and place it in the microwave for ½ – 1 minute. Now apply it onto the back.
Oats
Mash cooked whole oats with vinegar. Apply it on the back when hot. It soothes the aching back.
Potatoes
Mash the peeled and boiled potatoes. Let them cool and then apply on back. You will experience relief from back pain.
Coconut Oil
Take some coconut oil. Mix camphor in it and boil for 5-7 minutes. Allow it to cool. Store it in a bottle. Massage with this oil two times a day to cure back pain.
Capsaicin Cream
Capsaicin is an important ingredient of chilies. Apply capsaicin cream on the back. It will reduce the production of chemicals that transmit signals of pain to your brain.
Herbal Remedies for Lumbago /Backache
Willow Bark
White willow tree’s bark is considered an excellent herbal remedy for treating back pain. It has pain-relieving properties same as aspirin. So it will help reduce your back pain.
Basil Leaves
Basil leaves are very famous for their medicinal benefits. They aid in curing lower back pain. Boil 10-12 fresh basil leaves in a cup of water until it becomes half. Add a pinch of salt to it. Drink it once or twice a day depending on the severity of your pain.
Herbal Oils
Herbal oils like almond oil, eucalyptus oil, coconut oil or olive oil are very effective in alleviating back pain. Massage with warm oils on the painful area to relax the nerves causing pain.
Chamomile
Take some chamomile flowers. Steep them in a cup of boiling water for 15-20 minutes. Drink it 2-3 times a day. It will relax the tense muscles, thereby cure backache.
Note: – Pregnant ladies and those allergic to chamomile flowers should first consult doctor before taking this.
Ginger
Though more studies are needed, says Dr. Kiefer, ginger extract may help with joint and muscle pain because it contains phytochemicals, which help stop inflammation. Few side effects have been linked to ginger when taken in small doses.
Feverfew
Feverfew has been used for centuries to treat headaches, stomachaches, and toothaches. Nowadays it’s also used for migraines and rheumatoid arthritis. More studies are required to confirm whether feverfew is actually effective, but the herb may be worth trying since it hasn’t been associated with serious side effects. Mild side effects include canker sores and irritation of the tongue and lips. Pregnant women should avoid this remedy.
Turmeric
This spice has been used to relieve arthritis pain and heartburn, and to reduce inflammation. It’s unclear how turmeric works against pain or inflammation, but its activity may be due to a chemical called curcumin, which has anti-inflammatory properties. Turmeric is usually safe to use, but high doses or long-term use may cause indigestion. Also, people with gallbladder disease should avoid using turmeric.
Homeopathic Medicines for Lumbago /Backache
Rhus Tox
Rhus Tox tops the list of Homeopathic medicines for back pain. I have seen magnificent results in back pain from use of Rhus Tox. Rhus Tox is indicated for both upper and lower back pain, especially where the back pain is accompanied by intense stiffness. The back pain that arises from muscle strain also recovers wonderfully well with Rhus Tox. Persons suffering from back pain as a result of exertion or lifting heavy weights have found complete relief when prescribed Rhus Tox, making it one of the most reliable Homeopathic medicines for back pain. A prominent symptom to look out for while prescribing Rhus Tox is that the back pain gets worse with rest, while walking or hard pressure bring relief from pain.
Bryonia
In my clinical practice, Bryonia has shown marvellous results in lower back pain that worsens with the slightest of motion. Apart from motion, this pain also gets worse with standing or from turning in the bed, a key sign that Bryonia will work best. The pain may be accompanied by marked stiffness in such cases, for which Bryonia would rate among the best Homeopathic medicines for back pain. Lying down and taking rest brings relief from pain.
Aesculus
Aesculus is one of the most effective Homeopathic medicines for lower back pain that gets worse from stooping. In this case, the pain is most marked in the sacrum and hip region. The lower back feels as if it would break. Stiffness in the lower back is also intense. Aesculus is also one of the best Homeopathic medicines for back pain which gets worse when rising from a sitting position. Here it takes the person repeated efforts to rise from a chair or another sitting position.
Kali Carb
I would rank Kali Carb as one of the top grade Homeopathic medicines for back pain that arises after childbirth. The most prominent symptoms indicative of Kali Carb as the best suited Homeopathic medicines for back pain in such instances are stiffness and weakness in the lower back. The pain is very severe, with a feeling that the back might break. The back pain makes it difficult to walk. Women feel the need to lie down to get relief from the pain which may radiate to the upper back or down to the thigh and hips. Where these symptoms exist, Kali Carb comes highly recommended as one of the best Homeopathic medicines for back pain. Apart from post-partum backache, Kali Carb is also useful for backache in women before or during menses and after a miscarriage.
Cobaltum
Cobaltum ranks on top of the list of Homeopathic medicines for back pain that worsens from sitting. In such cases, the person feels better while walking or lying down. The back pain may radiate down the legs and feet in some cases, but the person will surely feel a weakness in the legs, a sure sign that Cobaltum will provide sustained relief.
Colocynth & Magnesium Phos
I have successfully treated several cases of back pain radiating down the legs and/or feet with two main Homeopathic medicines. These top rated Homeopathic medicines for back pain are Colocynth and Magnesium Phos. Among these, Colocynth is most effective Homeopathic medicine for back pain when the lower back pain radiates to the left leg and foot. Magnesium Phos brings relief when the lower back pain radiates down the right leg. The pain, in both the cases, can be of a shooting, cramping or tearing nature. However, both the medicines have proven their ability to bring lasting relief from pain and established themselves as the best Homeopathic medicines for back pain.
Cimicifuga & Kalmia
Two highly recommended Homeopathic medicines for back pain in the cervical region are Cimicifuga and Kalmia. I have seen remarkable results with use of Cimicifuga in cervical back pain accompanied by stiffness, contraction and sensitiveness in the neck. If pressure worsens the neck pain, Cimicifuga will offer effective treatment. However, in cases where the cervical pain radiates down the arm or hands, Kalmia has proved to be one of the most helpful Homeopathic medicines for back pain treatment. Persons feeling a weakness, numbness or tingling sensation in the arms and hands along with neck pain also recover fully well with use of Homeopathic medicine Kalmia.
Ruta & Hypericum
Ruta and Hypericum are highly suitable Homeopathic medicines for back pain resulting from injury. Ruta is prescribed for a back that is sore and bruised from injury. The pain is most marked over the sacrum and coccyx region. The injured person may feel a weakness in the lower back. Where such symptoms are noted, Ruta is the most prominent among Homeopathic medicines for back pain and has shown effective results. Homeopathic medicine Hypericum is recommended when pain from the tailbone radiates up the spine and down the limbs after injury. The pain is very sharp and intense. Motion, walking and stooping all make the pain worse. The spine is very tender and sensitive to touch in such cases where Hypericum has shown best results.
Backache is a common disorder involving the muscles, nerves, and bones of the back. Pain can vary from a dull constant ache to a sudden sharp feeling. Low back pain may be classified by duration as acute (pain lasting less than 6 weeks), sub-chronic (6 to 12 weeks), or chronic (more than 12 weeks). The condition may be further classified by the underlying cause as either mechanical, non-mechanical, or referred pain. The symptoms of low back pain usually improve within a few weeks from the time they start, with 40-90% of people completely better by six weeks.
Acute low-back pain without sciatica, with some spread of discomfort to the region of the sacroiliac joint, to the outer part of the buttock as well as to the lateral and the back part of the thigh, is a unifying symptom of a very common clinical syndrome whose exact underlying cause remains often uncertain. Most patients fall then into the category of non-specific low-back pain. Probably the pathogenesis is not uniform, and the pain can arise from a variety of structures (muscles, ligament, spine). Pain which persists after 3 to 4 days should warn the clinician that a serious pathological condition may be present which requires a new approach to diagnosis and treatment.
Pain in the lower part of the back is commonly referred to as Lumbago. It can be defined as mild to severe pain or discomfort in the area of the lower back. The pain can be acute (sudden and severe) or chronic if it has lasted more than three months.
Most people will experience lumbago at some point in their life. It is one of the most common reasons people miss work and visit the doctor. It can occur at any age but is a particular problem in younger people whose work involves physical effort and much later in life, in the elderly.
Anatomy Backache
The lumbar spine consists of five vertebrae (L1–L5). The complex anatomy of the lumbar spine is a combination of these strong vertebrae, linked by joint capsules, ligaments, tendons, and muscles, with extensive innervation. The spine is designed to be strong, since it has to protect the spinal cord and spinal nerve roots. At the same time, it is highly flexible, providing for mobility in many different planes.
The mobility of the vertebral column is provided by the symphyseal joints between the vertebral bodies, with an IVD in between. The facet joints are located between and behind adjacent vertebrae, contributing to spine stability. They are found at every spinal level and provide about 20% of the torsional (twisting) stability in the neck and low back segments [rx]. Ligaments aid in joint stability during rest and movement, preventing injury from hyperextension and hyperflexion. The three main ligaments are the anterior longitudinal ligament (ALL), posterior longitudinal ligament (PLL), and ligamentum flavum (LF). The canal is bordered by vertebral bodies and discs anteriorly and by laminae and LF posteriorly. Both the ALL and PLL run the entire length of the spine, anteriorly and posteriorly, respectively. Laterally, spinal nerves and vessels come out from the intervertebral foramen. Beneath each lumbar vertebra, there is the corresponding foramen, from which spinal nerve roots exit. For example, the L1 neural foramina are located just below the L1 vertebra, from where the L1 nerve root exits.
IVDs are located between vertebrae. They are compressible structures able to distribute compressive loads through osmotic pressurization. In the IVD, the annulus fibrosus (AF), a concentric ring structure of organized lamellar collagen, surrounds the proteoglycan-rich inner nucleus pulposus (NP). Discs are avascular in adulthood, except for the periphery. At birth, the human disc has some vascular supply but these vessels soon recede, leaving the disc with little direct blood supply in the healthy adult [rx]. Hence, metabolic support of much of the IVD is dependent on the cartilaginous endplates adjacent to the vertebral body. A meningeal branch of the spinal nerve, better known as the recurrent sinuvertebral nerve, innervates the area around the disc space [rx].
The lumbar spine is governed by four functional groups of muscles, split into extensors, flexors, lateral flexors, and rotators. The lumbar vertebrae are vascularized by lumbar arteries that originate in the aorta. Spinal branches of the lumbar arteries enter the intervertebral foramen at each level, dividing themselves into smaller anterior and posterior branches [rx]. The venous drainage parallels the arterial supply [rx].
Typically, the end of the spinal cord forms the conus medullaris within the lumbar spinal canal at the lower margin of the L2 vertebra [rx]. All lumbar spinal nerve roots stem from the connection between the dorsal or posterior (somatic sensory) root from the posterolateral aspect of the spinal cord and the ventral or anterior (somatic motor) root from the anterolateral aspect of the cord [rx]. The roots then flow down through the spinal canal, developing into the cauda equina, before exiting as a single pair of spinal nerves at their respective intervertebral foramina. Cell bodies of the motor nerve fibers can be found in the ventral or anterior horns of the spinal cord, whereas those of the sensory nerve fibers are in the dorsal root ganglion (DRG) at each level. One or more recurrent meningeal branches, known as the sinuvertebral nerves, run out from the lumbar spinal nerves. The sinuvertebral nerve, or Luschka’s nerve, is a recurrent branch created from the merging of the grey ramus communicans (GRC) with a small branch coming from the proximal end of the anterior primary ramus of the spinal nerve. This polisegmentary mixed nerve directly re-enters the spinal canal and gives off ascending and descending anastomosing branches comprising both somatic and autonomic fibers for the posterolateral annulus, the posterior vertebral body and the periostium, and the ventral meninges [rx, rx]. The sinuvertebral nerves connect with branches from radicular levels both above and below the point of entry, in addition to the contralateral side, meaning that localizing pain from involvement of these nerves is challenging [rx]. Also, the facet joints receive two-level innervation comprising somatic and autonomic components. The former convey a well-defined local pain, while the autonomic afferents transmit referred pain.
www.rxharun.com
Causes of Backache
The human back is composed of a complex structure of muscles, ligaments, tendons, disks and bones – the segments of our spine are cushioned with cartilage-like pads called disks. Problems with any of these components can lead to back pain. In some cases of back pain, its cause is never found.
Problems with the spine such as osteoporosis can lead to back pain.
Strain – the most common causes of back pain are:
Strained muscles
Strained ligaments
A muscle spasm
Things that can lead to strains or spasms include:
Lifting something improperly
Lifting something that is too heavy
The result of an abrupt and awkward movement
Structural problems –
Sprains and strains – account for most acute back pain. Sprains are caused by overstretching or tearing ligaments, and strains are tears in tendon or muscle. Both can occur from twisting or lifting something improperly, lifting something too heavy, or overstretching. Such movements may also trigger spasms in back muscles, which can also be painful.
Intervertebral disc degeneration – is one of the most common mechanical causes of low back pain, and it occurs when the usually rubbery discs lose integrity as a normal process of aging. In a healthy back, intervertebral discs provide height and allow bending, flexion, and torsion of the lower back. As the discs deteriorate, they lose their cushioning ability.
Herniated or ruptured discs – can occur when the intervertebral discs become compressed and bulge outward (herniation) or rupture, causing low back pain.
Radiculopathy – is a condition caused by compression, inflammation and/or injury to a spinal nerve root. Pressure on the nerve root results in pain, numbness, or a tingling sensation that travels or radiates to other areas of the body that are served by that nerve. Radiculopathy may occur when spinal stenosis or a herniated or ruptured disc compresses the nerve root.
Sciatica – is a form of radiculopathy caused by compression of the sciatic nerve, the large nerve that travels through the buttocks and extends down the back of the leg. This compression causes shock-like or burning low back pain combined with pain through the buttocks and down one leg, occasionally reaching the foot. In the most extreme cases, when the nerve is pinched between the disc and the adjacent bone, the symptoms may involve not only pain, but numbness and muscle weakness in the leg because of interrupted nerve signaling. The condition may also be caused by a tumor or cyst that presses on the sciatic nerve or its roots.
Spondylolisthesis – is a condition in which a vertebra of the lower spine slips out of place, pinching the nerves exiting the spinal column.
A traumatic injury – such as from playing sports, car accidents, or a fall can injure tendons, ligaments or muscle resulting in low back pain. Traumatic injury may also cause the spine to become overly compressed, which in turn can cause an intervertebral disc to rupture or herniate, exerting pressure on any of the nerves rooted to the spinal cord. When spinal nerves become compressed and irritated, back pain and sciatica may result.
Ruptured disks – each vertebra in our spine is cushioned by disks. If the disk ruptures there will be more pressure on a nerve, resulting in back pain.
Bulging disks – in much the same way as ruptured disks, a bulging disk can result in more pressure on a nerve.
Sciatica – a sharp and shooting pain that travels through the buttock and down the back of the leg, caused by a bulging or herniated disk pressing on a nerve.
Arthritis – patients with osteoarthritis commonly experience problems with the joints in the hips, lower back, knees and hands. In some cases spinal stenosis can develop, which is the term used to describe when the space around the spinal cord narrows.
Abnormal curvature of the spine – if the spine curves in an unusual way the patient is more likely to experience back pain. An example is a scoliosis, a condition in which the spine curves to the side.
Osteoporosis– bones, including the vertebrae of the spine, become brittle and porous, making compression fractures more likely.
Spinal stenosis – is a narrowing of the spinal column that puts pressure on the spinal cord and nerves that can cause pain or numbness with walking and over time leads to leg weakness and sensory loss.
Skeletal irregularities – include scoliosis, a curvature of the spine that does not usually cause pain until middle age; lordosis, an abnormally accentuated arch in the lower back; and other congenital anomalies of the spine.
Abdominal aortic aneurysms – occur when the large blood vessel that supplies blood to the abdomen, pelvis, and legs becomes abnormally enlarged. Back pain can be a sign that an aneurysm is becoming larger and that the risk of rupture should be assessed.
Kidney stones – can cause sharp pain in the lower back, usually on one side.
Below are some other causes of back pain
Cauda equina syndrome – the cauda equine is a bundle of spinal nerve roots that arise from the lower end of the spinal cord. People with cauda equine syndrome feel a dull pain in the lower back and upper buttocks, as well as analgesia (lack of feeling) in the buttocks, genitalia, and thigh. There are sometimes bowel and bladder function disturbances.
Cancer of the spine – a tumor located on the spine may press against a nerve, resulting in back pain.
Infection of the spine – if the patient has an elevated body temperature (fever) as well as a tender warm area on the back, it could be caused by an infection of the spine.
Other infections – pelvic inflammatory disease (females), bladder, or kidney infections may also lead to back pain.
Endometriosis – is the buildup of uterine tissue in places outside the uterus.
Fibromyalgia – a chronic pain syndrome involving widespread muscle pain and fatigue.
Sleep disorders – individuals with sleep disorders are more likely to experience back pain, compared to others.
Shingles – an infection that can affect the nerves may lead to back pain, depending on the nerves affected.
Bad mattress – if a mattress does not support specific parts of the body and keep the spine straight, there is a greater risk of developing back pain.
Everyday activities or poor posture
Back pain can also be the result of some everyday activity or poor posture. Examples include:
Adopting a very hunched sitting position when using computers can result in increased back and shoulder problems over time.
Bending awkwardly
Pushing something
Pulling something
Carrying something
Lifting something
Standing for long periods
Bending down for long periods
Twisting
Coughing
Sneezing
Muscle tension
Over-stretching
Straining the neck forward, such as when driving or using a computer
Long driving sessions without a break, even when not hunched
Exertion or lifting.
Severe blow or fall.
Back disorders.
Infections.
Ruptured lumbar disk.
Nerve dysfunction.
Osteoporosis.
Spondylosis (hardening and stiffening of the spinal column).
The main symptom of back pain is, as the name suggests, an ache or pain anywhere on
Pain in the back, and sometimes all the way down to the buttocks and legs. Some back issuescan cause pain in other parts of the body, depending on the nerves affected.
In most cases, signs, and symptoms clear up on their own within a short period.If any of the following signs or symptoms accompany a back pain, people should see their doctor:
Pain. It may be continuous, or only occur when you are in a certain position. The pain may be aggravated by coughing or sneezing, bending or twisting.
Patients who have been taking steroids for a few months
Drug abusers
Patients with cancer
Patients who have had cancer
Patients with depressed immune systems
Stiffness.
According to the British National Health Service (NHS), the following groups of people should seek medical advice if they experience back pain:
Weight loss
Elevated body temperature (fever)
Inflammation (swelling) on the back
Persistent back pain – lying down or resting does not help
Pain down the legs
Pain reaches below the knees
A recent injury, blow or trauma to your back
Urinary incontinence – you pee unintentionally (even small amounts)
Difficulty urinating – passing urine is hard
Fecal incontinence – you lose your bowel control (you poo unintentionally)
Numbness around the genitals
Numbness around the anus
Numbness around the buttocks
dull ache,
numbness,
tingling,
sharp pain,
pulsating pain,
pain with movement of the spine,
pins and needles sensation,
muscle spasm,
tenderness,
sciatica with shooting pain down one or both lower extremities
People aged less than 20 and more than 55 years
Additionally, people who experience pain symptoms after a major trauma (such as a car accident) are advised to see a doctor. If low back pain interferes with daily activities, mobility, sleep, or if there are other troubling symptoms, medical attention should be sought.
Risk increases with
Biomechanical risk factors.
Sedentary occupations.
Gardening and other yard work.
Sports and exercise participation, especially if infrequent.
Obesity.
Preventive measures
Exercises to strengthen lower back muscles.
Learn how to lift heavy objects.
Sit properly.
Back support in bed.
Lose weight, if obese.
Choose proper footwear.
Wear special back support devices.
Red flag conditions indicating possible underlying spinal pathology or nerve root problemsw9
Red flags
Onset age < 20 or > 55 years
Non-mechanical pain (unrelated to time or activity)
Thoracic pain
Previous history of carcinoma, steroids, HIV
Feeling unwell
Weight loss
Widespread neurological symptoms
Structural spinal deformity
Indicators for nerve root problems
Unilateral leg pain > low back pain
Radiates to foot or toes
Numbness and paraesthesia in same distribution
Straight leg raising test induces more leg pain
Localised neurology (limited to one nerve root)
Diagnosis of Backache
Suspected disk, nerve, tendon, and other problems – X-rays or some other imaging scan, such as a CT (computerized tomography) or MRI (magnetic resonance imaging) scan may be used to get a better view of the state of the soft tissues in the patient’s back.
X-rays – can show the alignment of the bones and whether the patient has arthritis or broken bones. They are not ideal for detecting problems with muscles, the spinal cord, nerves or disks.
MRI or CT scans – these are good for revealing herniated disks or problems with tissue, tendons, nerves, ligaments, blood vessels, muscles and bones.
Bone scan – a bone scan may be used for detecting bone tumors or compression fractures caused by brittle bones (osteoporosis). The patient receives an injection of a tracer (a radioactive substance) into a vein. The tracer collects in the bones and helps the doctor detect bone problems with the aid of a special camera.
Electromyography or EMG – the electrical impulses produced by nerves in response to muscles is measured. This study can confirm nerve compression which may occur with a herniated disk or spinal stenosis (narrowing of the spinal canal).
Treatment of Backache
General measures
Bed rest for first 24 hours. Additional bed rest will be determined by the severity of the problem. Recent medical studies indicate that staying more active is better for back disorders than prolonged bed rest.
Use a firm mattress (place a bed board under the mattress if needed).
An ice pack or cold massage or heat applied to the affected area with a heating pad or hot water bottle.
Physical therapy.
Massage may help. Be sure the person is well-trained or massage could cause more harm than help.
Wear a special back support device.
Other options are available depending on the degree of injury, such as surgery (if disk damaged), electrical nerve stimulation, acupuncture, special shoes, etc.
Stress reduction techniques, if needed.
Non-Prescription Pain Relievers – Naproxen, acetaminophen, and ibuprofen each reduce inflammation and pain. Though these drugs are available over-the-counter, they are potent and taking more than the recommended dose can harm health. A doctor can help with advice about the right kind of non-prescription pain reliever to take.
Cold and Heat – Applying a cold pack to the painful part of the back contracts inflamed muscle and relieves pain. This treatment helps a great deal when the disk has recently ruptured and swelling is at its greatest. A heating pad or warm pack helps with residual pain.
Continued Physical Activity – Though pain or weakness seem like good reasons to rest the back, excessive bed-rest worsens the symptoms of a slipped disc. Moving around too little allows muscles to grow weaker and prevents the body from healing. Periods of rest interspersed with periods of normal activity throughout the day keep the back muscles in shape.
Prescription Remedies – If over-the-counter drugs fail to ease slipped disc pain, the doctor will turn to prescription medications. These can include narcotics, such as hydrocodone or codeine. While they can do away with pain, narcotics are very addictive and induce a mental fogginess that can itself be dangerous. More narrowly-focused medicines designed to target damaged nerves that create chronic pain may be a better choice, as they have fewer undesirable side effects. Gabapentin and Cymbalta are two drugs that act in different ways to minimize nerve pain. These drugs are less addictive than narcotics.
Physical Therapy – Physical therapists show slipped disc sufferers ways to move that do not cause pain. Occupational therapists teach skills that allow patients to return to a productive life.
Nutrition – In order to restore the disc we also are going to need to include different substances in our diet. There are a lot of supplements on the market, of course. If you wish to try them, that’s fine. I personally don’t like them. I have tried one with glucosamine and chondroitin, but I didn’t feel any different. So, if you have the opportunity to take these with the food or from more natural sources, it will be great. You can find these substances in seafood and animal cartilages and by digesting them we ensure the building blocks for the connecting tissue for our joints and spine. Also, we will need more Omega 3 fatty acids, which can be supplied from cold-pressed oils, fatty fish, flax seeds, chia, and many more. Vitamins from the B group are very beneficial for people with herniated discs and all kinds of issues with the peripheral nervous system. Vitamins B1, B6, and B12 nourish the nerves and help them recover from the disk accident. Usually, doctors prescribe them as a part of the treatment, but it is worth mentioning anyway.
A good massage – A massage is one of the natural methods of relieving pain. Individuals who get a massage weekly for several months stand a better chance of alleviating back pain. A good massage provides a person with many health benefits that lessen back pain. A massage triggers the release of endorphins. Endorphins aid in decreasing anxiety and relieving pain. They offer a relaxation effect by softening muscles that are injured preventing cramping.
Undertaking yoga – Yoga is an applicable strategy of keeping the level of back pain at minimal levels. Taking yoga sessions often is a very effective method of dealing with back pain. With yoga, there is a high likelihood of proper body functions. The use of pain prescriptions is also diminished. Patients suffering from back pain related issues do not have to rely on these prescriptions to manage pain. Incorporating laughter in yoga is a good way of exercising. Yoga incorporates simple yet appropriate exercises that enhance the stretching of muscles. Laughter with yoga stimulates relieving of pain. It facilitates increased uptake of oxygen, little anxiety and production of endorphins. All these variables play an essential role in diminishing back pain.
Adjusting sleeping position – A simple sleeping mistake can immensely contribute to back pain. A poor sleeping position can cause stress and tension on the muscles contributing to back pain. Altering one’s sleeping position and adopting a style that does not exert a lot of stress on the back is a recommended tactic. Nurturing sleeping habits such as assuming a reclining position, using wedge-shaped cushions, and getting adjustable beds from reputable medical institutions are easy techniques to endorse. If a reclining position does not suit an individual, the other two techniques can be embraced.
Heat therapy – Several considerations should be observed when using heat therapy. The right temperature ought to be set so as to ensure a patient does not face risks associated with too much exposure to heat. The key objective should be to ensure enough access to heat to the muscles to yield benefits for the patient. The adoption of heat therapy for easing back pain is determined by the magnitude of pain a person is experiencing. In cases where relatively low back pain is encountered, short heat therapy sessions are recommended. On the other hand, if an individual is experiencing prolonged back pain, long heat therapy sessions are the most applicable.
Taking hot baths – This is a form of heat therapy that aims at relieving back pain. It guarantees the permeation of heat into the muscles leading to reduced pain. Many individuals opt for this method since they believe it achieves competent results. Hot baths initiate a fast process of blood supply to stiff neck and back muscles. When this happens, the muscles relax and stretch leading to decreased back pain. To avoid interference with one’s sleeping patterns, a hot bath should be taken several hours before retiring to bed.
Aquatic therapy – This natural technique involves physical therapy in a pool. Individuals get the best out of this therapy by relying on the resistance of water. Consistency in undertaking this therapy is what ascertains getting back pain relief. Integrating aquatic therapy in an individual’s life for the better part of the week enhances reduction of back pain quickly.
Enlighten others – Individuals have the power to devise their own natural strategies that aid them in coping with back pain. The strategies can also be a good remedy for others going through similar circumstances. An individual can use social media platforms to equip others with important tips on how to keep back pain at bay. Further, becoming a member of associations that address back pain issues enables better communication of the knowledge gained from personal experience.
Medications
Analgesic medications – are those specifically designed to relieve pain. They include OTC acetaminophen and aspirin, as well as prescription opioids such as codeine, oxycodone, hydrocodone, and morphine. Opioids should be used only for a short period of time and under a physician’s supervision. People can develop a tolerance to opioids and require increasingly higher dosages to achieve the same effect. Opioids can also be addictive. Their side effects can include drowsiness, constipation, decreased reaction time, and impaired judgment. Some specialists are concerned that chronic use of opioids is detrimental to people with back pain because they can aggravate depression, leading to a worsening of the pain.
Nonsteroidal anti-inflammatory drugs(NSAIDS) – relieve pain and inflammation and include OTC formulations (ibuprofen, ketoprofen, and naproxen sodium). Several others, including a type of NSAID called COX-2 inhibitors, are available only by prescription. Long-term use of NSAIDs has been associated with stomach irritation, ulcers, heartburn, diarrhea, fluid retention, and in rare cases, kidney dysfunction and cardiovascular disease. The longer a person uses NSAIDs the more likely they are to develop side effects. Many other drugs cannot be taken at the same time a person is treated with NSAIDs because they alter the way the body processes or eliminates other medications.
Anticonvulsants—drugs primarily used to treat seizures—may be useful in treating people with radiculopathy and radicular pain.
Antidepressants – such as tricyclics and serotonin and norepinephrine reuptake inhibitors have been commonly prescribed for chronic low back pain, but their benefit for nonspecific low back pain is unproven, according to a review of studies assessing their benefit.
Muscle Relaxants – If the muscles around the slipped disc experience painful spasms, a muscle relaxant such as Valium may be useful. The drawback to drugs like these is that they do not limit their power to the affected nerve. Instead, they have a generally relaxing effect and will interfere with daily activities.
As cyclobenzaprine (Flexeril) – which might be prescribed to relieve the discomfort associated with muscle spasms. However, these medicines might cause confusion in older people. Depending on the level of pain, prescription pain medicines might be used in the initial period of treatment.
Steroids – If inflammation is severe, a doctor may also prescribe a steroid. Steroids, such as cortisone, reduce swelling quickly. A cortisone shot directly in the affected area will have an immediate effect on the displaced disc.
Counter-irritants – such as creams or sprays applied topically stimulate the nerves in the skin to provide feelings of warmth or cold in order to dull the sensation of pain. Topical analgesics reduce inflammation and stimulate blood flow.
Nerve Relaxant — Pregabalin or gabapentin and anti-inflammatory drugs help to relieve pain and stiffness, allowing for increased mobility and exercise. There are many common over-the-counter medicines called non-steroidal anti-inflammatory drugs (NSAIDs). They include aspirin, ibuprofen (Motrin, Advil), and naproxen (Naprosyn, Aleve).
Spinal manipulation and spinal mobilization – Are approaches in which professionally licensed specialists (doctors of chiropractic care) use their hands to mobilize, adjust, massage, or stimulate the spine and the surrounding tissues. Manipulation involves a rapid movement over which the individual has no control; mobilization involves slower adjustment movements. The techniques have been shown to provide small to moderate short-term benefits in people with chronic low back pain. Evidence supporting their use for acute or subacute low back pain is generally of low quality. Neither technique is appropriate when a person has an underlying medical cause for the back pain such as osteoporosis, spinal cord compression, or arthritis.
Traction – involves the use of weights and pulleys to apply constant or intermittent force to gradually “pull” the skeletal structure into better alignment. Some people experience pain relief while in traction, but that relief is usually temporary. Once traction is released the back pain tends to return. There is no evidence that traction provides any long-term benefits for people with low back pain.
Spinal injections — An injection of a cortisone-like anti-inflammatory medicine into the lower back might help reduce swelling and inflammation of the nerve roots, allowing for increased mobility.
Biofeedback – It is used to treat many acute pain problems, most notably back pain and headache. The therapy involves the attachment of electrodes to the skin and the use of an electromyography machine that allows people to become aware of and self-regulate their breathing, muscle tension, heart rate, and skin temperature. People regulate their response to pain by using relaxation techniques. Biofeedback is often used in combination with other treatment methods, generally without side effects. The evidence is lacking that biofeedback provides a clear benefit for low back pain.
Nerve block therapies – aim to relieve chronic pain by blocking nerve conduction from specific areas of the body. Nerve block approaches range from injections of local anesthetics, botulinum toxin, or steroids into affected soft tissues or joints to more complex nerve root blocks and spinal cord stimulation. When extreme pain is involved, low doses of drugs may be administered by catheter directly into the spinal cord. The success of a nerve block approach depends on the ability of a practitioner to locate and inject precisely the correct nerve. Chronic use of steroid injections may lead to increased functional impairment.
Surgery For Backache
When other therapies fail, surgery may be considered an option to relieve pain caused by serious musculoskeletal injuries or nerve compression. It may be months following surgery before the patient is fully healed, and he or she may suffer permanent loss of flexibility.
Vertebroplasty and kyphoplasty – are minimally invasive treatments to repair compression fractures of the vertebrae caused by osteoporosis. Vertebroplasty uses three-dimensional imaging to assist in guiding a fine needle through the skin into the vertebral body, the largest part of the vertebrae. A block of glue-like bone cement is then injected into the vertebral body space, which quickly hardens to stabilize and strengthen the bone and provide pain relief. In kyphoplasty, prior to injecting the bone cement, a special balloon is inserted and gently inflated to restore height to the vertebral structure and reduce spinal deformity.
Spinal laminectomy – (also known as spinal decompression) is performed when spinal stenosis causes a narrowing of the spinal canal that causes pain, numbness, or weakness. During the procedure, the lamina or bony walls of the vertebrae, along with any bone spurs, are removed. The aim of the procedure is to open up the spinal column to remove pressure on the nerves.
Discectomy or microdiscectomy – may be recommended to remove a disc, in cases where it has herniated and presses on a nerve root or the spinal cord, which may cause intense and enduring pain. Microdiscectomy is similar to a conventional discectomy; however, this procedure involves removing the herniated disc through a much smaller incision in the back and a more rapid recovery. Laminectomy and discectomy are frequently performed together and the combination is one of the more common ways to remove pressure on a nerve root from a herniated disc or bone spur.
Foraminotomy – is an operation that “cleans out” or enlarges the bony hole (foramen) where a nerve root exits the spinal canal. Bulging discs or joints thickened with age can cause narrowing of the space through which the spinal nerve exits and can press on the nerve, resulting in pain, numbness, and weakness in an arm or leg. Small pieces of bone over the nerve are removed through a small slit, allowing the surgeon to cut away the blockage and relieve pressure on the nerve.
Intradiscal electrothermal therapy (IDET) – is a treatment for discs that are cracked or bulging as a result of degenerative disc disease. The procedure involves inserting a catheter through a small incision at the site of the disc in the back. A special wire is passed through the catheter and an electrical current is applied to heat the disc, which helps strengthen the collagen fibers of the disc wall, reducing the bulging and the related irritation of the spinal nerve. IDET is of questionable benefit.
Nucleoplasty also called plasma disc decompression (PDD) – is a type of laser surgery that uses radiofrequency energy to treat people with low back pain associated with mildly herniated discs. Under x-ray guidance, a needle is inserted into the disc. A plasma laser device is then inserted into the needle and the tip is heated to 40-70 degrees Celsius, creating a field that vaporizes the tissue in the disc, reducing its size and relieving pressure on the nerves. Several channels may be made depending on how tissue needs to be removed to decompress the disc and nerve root.
Radiofrequency denervation – is a procedure using electrical impulses to interrupt nerve conduction (including the conduction of pain signals). Using x-ray guidance, a needle is inserted into a target area of nerves and a local anesthetic is introduced as a way of confirming the involvement of the nerves in the person’s back pain. Next, the region is heated, resulting in localized destruction of the target nerves. Pain relief associated with the technique is temporary and the evidence supporting this technique is limited.
Spinal fusion – is used to strengthen the spine and prevent painful movements in people with degenerative disc disease or spondylolisthesis (following laminectomy). The spinal disc between two or more vertebrae is removed and the adjacent vertebrae are “fused” by bone grafts and/or metal devices secured by screws. The fusion can be performed through the abdomen, a procedure known as an anterior lumbar interbody fusion, or through the back, called posterior fusion. Spinal fusion may result in some loss of flexibility in the spine and requires a long recovery period to allow the bone grafts to grow and fuse the vertebrae together. Spinal fusion has been associated with an acceleration of disc degeneration at adjacent levels of the spine.
Artificial disc replacement – is considered an alternative to spinal fusion for the treatment of people with severely damaged discs. The procedure involves removal of the disc and its replacement by a synthetic disc that helps restore height and movement between the vertebrae.
Other Rx of Backache
Chiropractic Care
Sixty percent of people with sciatica who didn’t get relief from other therapies and then tried spinal manipulation experienced the same degree of pain relief as patients who eventually had surgery, found a 2010 study in the Journal of Manipulative and Physiological Therapeutics. The 120 people in the study saw a chiropractor about 3 times a week for 4 weeks and then continued weekly visits, tapering off treatment as they felt better. In people who responded to chiropractic care, benefits lasted up to a year. “Spinal manipulation may create a response in the nervous system that relieves pain and restores normal mobility to the injured area,” says study researcher Gordon McMorland, DC, of National Spine Care in Calgary, Alberta. “It also reduces inflammation, creating an environment that promotes the body’s natural healing mechanisms.”
Acupuncture
You can get relief as soon as the first session, though it takes about 12 sessions to see improvement,” says Jingduan Yang, MD, assistant professor at the Jefferson Myrna Brind Center of Integrative Medicine at Thomas Jefferson University. A small study in the Journal of Traditional Chinese Medicine found that of 30 people with sciatica, 17 got complete relief and 10 saw symptoms improve with warming acupuncture, in which the needles are heated.
Yoga
A study in the journal Pain reported that people with chronic back pain who practiced Iyengar yoga for 16 weeks saw pain reduced by 64% and disability by 77%. Although yoga’s effects on sciatica are less clear, gentle forms may be beneficial. By strengthening muscles and improving flexibility, a yoga practice can help sciatica sufferers “move and function better so they don’t fall into a posture that aggravates sciatica,” says James W. Carson, Ph.D., a psychologist at the Comprehensive Pain Center at Oregon Health & Science University. For extra grip and stability, try these grip socks from Natural Fitness.
Massage
Don’t expect a chilled-out spa massage if you have sciatica. In this instance, trigger-point therapy is best, says Jeff Smoot, vice president of the American Massage Therapy Association. The sciatic nerve sits underneath a muscle called the piriformis, which is located beneath the glutes. “When the piriformis muscle gets tight, it pinches the sciatic nerve, causing tingling and numbness down into the leg,” says Smoot. He applies pressure to irritated and inflamed areas, or trigger points, in the piriformis muscle, as well as in muscles in the lower back and glutes. Typically, Smoot schedules treatments 7 to 10 days apart. If patients don’t see progress by the fourth visit, “they need to try another form of therapy,” he says.
Shiatsu,
Also known as finger pressure therapy, is a type of massage where pressure is applied along energy lines in the body. The shiatsu therapist applies pressure with his/her fingers, thumbs and elbows.
Topical Preparations
St. John’s wort oil, a liniment, is “one of my favorites for nerve pain,” says Tieraona Low Dog, MD, director of the fellowship at the Arizona Center for Integrative Medicine. Apply the anti-inflammatory oil two or three times a day where there’s pain. Another option: an OTC cayenne pepper plaster or cream; capsaicin, found in chiles, hinders the release of pain-causing compounds from nerves. For severe cases, Low Dog uses the prescription chile patch Qutenza, designed for shingles pain. “One application is effective for weeks,” says Low Dog.
Ice or Heat
Because the sciatic nerve is buried deep within the buttock and leg, ice or heat on the surface of the body won’t ease that inner inflammation. But the timehonored treatments can act as counterirritants—that is, “they give your body other input in the painful area, and that brings the pain down a notch,” says Ruppert. Apply an ice pack or a heating pad as needed for 15 minutes.
Devil’s Claw
The herbal medication devil’s claw is “quite a potent anti-inflammatory, working like ibuprofen and similar drugs to inhibit substances that drive inflammation,” says Low Dog. She generally starts patients on 1,500 to 2,000 mg twice a day. Look for a brand that has a standardized extract of roughly 50 mg of harpagoside, the active compound. Safety reviews show that the supplement is well tolerated by most people but should be avoided by patients with peptic ulcers or on blood-thinning medications.
Pain Relievers and Muscle Relaxants
Taking a nonsteroidal anti-inflammatory drug, either OTC (like ibuprofen) or Rx, can ease the distress. Because painful muscle spasms may also accompany a disk herniation, doctors sometimes prescribe muscle relaxants or pain-reducing tricyclic antidepressants. A caveat: “These won’t help with the pain caused by pressure on the sciatic nerve,” says A. Nick Shamie, MD, a spokesperson for the American Academy of Orthopaedic Surgeon.
Epidural Steroid Injections
People whose pain doesn’t lessen within about a month and who aren’t helped by other therapies may find their pain remedied by an x-ray-guided injection of steroid into the lower back near the sciatic nerve, says Raj Rao, MD, a spokesperson for the AAOS. “The hope is to reduce inflammation within that nerve branch,” explains Rao. Because of concerns about side effects, such as loss of bone density, the epidural shots are limited to three a year.
CBT (cognitive behavioral therapy)
CBT can help patients manage chronic back pain. The therapy is based on the principle that the way a person feels is, in part, dependent on the way they think about things.
People who can be taught to train themselves to react in a different way to pain may experience less perceived pain. CBT may use relaxation techniques as well as strategies to maintain a positive attitude. Studies have found that patients with CBT tend to become more active and do exercise, resulting in a lower risk of back pain recurrence.
Exercise and Physical Therapy
Moving is usually the last thing people dogged by sciatica want to do, but it’s important to be physically active. “Lying in bed makes it more likely that the pain will last longer,” says Ruppert. “Exercise increases blood flow to the disk and the nerve, helping to get rid of the chemicals causing the inflammation.” Take 15- to 20-minute walks. If that hurts too much, give swimming or water aerobics a try; there’s not as much pressure on the back when you’re in the water, says Ruppert. It may also be worth seeing a physical therapist, who can prescribe stretching exercises to restore flexibility to the back or moves that strengthen core muscles, helping to stabilize the spine and reduce the likelihood of a similar injury.
Here are six exercises for Lumbago /Backache
Pigeon pose
Pigeon Pose is a common yoga pose. It works to broadly open the hips. There are multiple versions of this stretch. The first is a starting version of the pigeon pose, known as the reclining pigeon pose. If you are just starting your treatment, you should try the reclining pose first. Once you can do the reclining version without pain, work with your physical therapist on the sitting and forward versions.
Reclining pose
While on the back, bring your right leg up to a right angle and grasp it with both hands behind the thigh, locking your fingers.
Take your left leg and place your ankle against the knee. Hold the position for a moment before changing legs. This helps stretch the tiny piriformis muscle, which sometimes becomes inflamed and presses against the sciatic nerve causing pain.
Repeat by switching sides and doing the same exercise with the other leg.
Sitting pose
Sit on the floor with your legs stretched out straight in front of you. Then bend your right leg, putting your right ankle on top of the left knee.
Lean forward and allow your upper body to lean toward your thigh. Hold for 15 to 30 seconds and then switch sides. This stretches the glutes and lower back.
Forward pose
Kneel on the floor on all fours.
Pick up your right leg and move it forward so that your lower leg is on the ground, horizontal to the body. Your right foot should be in front of your right knee while your right knee stays to the right.
Stretch the left leg out all the way behind you on the floor, with the top of the foot on the ground and toes pointing back.
Shift your body weight gradually from your arms to your legs so that your legs are supporting your weight. Sit up straight with your hands on either side of your legs.
Take a deep breath. While exhaling, lean your upper body forward over your lower leg. Support your weight with your arms as much as possible.
Knee to opposite shoulder
This simple stretch helps relieve sciatica pain by loosening your gluteal and piriformis muscles, which can become inflamed and press against the sciatic nerve.
Lie on your back with your legs extended outward and your feet flexed upward.
Clasp your hands around your knee and gently pull your right leg across your body toward your left shoulder. Hold it there for 30 seconds and then push your knee so your leg returns to its starting position.
Repeat for a total of 3 reps, and then switch legs. Remember to only pull your knee as far as it will comfortably go. You should feel a relieving stretch in your muscle, not pain.
Sitting spinal stretch
Sciatica pain is triggered when vertebrae in the spine compress. This stretch helps create space in the spine to relieve pressure from the sciatic nerve.
Sit on the ground with your legs extended straight out with your feet flexed upward.
Bend your right knee and place your foot flat on the floor on the outside of your opposite knee.
Place your left elbow on the outside of your right knee to help you gently turn your body toward the right. Hold for 30 seconds and repeat three times, then perform this stretch with your left leg bent and body turned to the left side.
Standing hamstring stretch
This stretch can help ease pain and tightness in the hamstring caused by sciatica.
Place your right foot on an elevated surface at or below your hip level. This could be a chair, ottoman, or step on a staircase. Flex your foot so your toes and leg are straight. If your knee tends to hyperextend, keep a slight bend in it.
Bend your body forward slightly toward your foot. The further you go, the deeper the stretch. Do not push so far that you feel pain.
Release the hip of your raised leg downward as opposed to it lifting up. If you need help easing your hip down, loop a yoga strap or long exercise band over your right thigh and under your left foot. Hold for at least 30 seconds, and then repeat on the other side.
Exercise with care
Kovacs emphasizes that you should not assume that you will be able to be as flexible as the exercises ideally call for. “Don’t think that because of what you see on YouTube or TV that you can get into these positions,” he said. “Most people who demonstrate the exercises have great flexibility and have been doing it for years. If you have any kind of pain, you should stop.”
Corina Martinez, a physical therapist at Duke Sports Medicine Center and a member of the American Medical Society for Sports Medicine, says that there is no one-size-fits-all exercise for people suffering from sciatic nerve pain. “Do you feel better when you bring your knees to the chest, or when they extend back a little more? If one feels better, that is the treatment you want to pursue.”
Martinez says that anyone experiencing even mild sciatic nerve pain symptoms for more than a month should see a doctor or physical therapist. They may find relief with an in-home exercise program tailored specifically to how their pain presents itself.
What complications are associated with
Chronic (ongoing and lasting) pain is a complication of untreated sciatica. If the “pinched nerve” is seriously injured, chronic muscle weakness, such as a “drop foot,” might occur.
What is the outlook for people with
Sciatic pain usually goes away with time and rest. Most people with sciatica (80 percent to 90 percent) will get better without surgery. About half of affected individuals recover from an episode within six weeks.
Can sciatica be prevented?
Some sources of sciatica are not preventable, such as degenerative disc disease, back strain due to pregnancy, and accidental falls.
Although it might not be possible to prevent all cases of sciatica, you can take steps to protect your back and reduce your risk.
Practice proper lifting techniques. Lift with your back straight, bringing yourself up with your hips and legs, and holding the object close to your chest. Use this technique for lifting everything, no matter how light.
Avoid/ stop cigarette smoking, which promotes disc degeneration.
Exercise regularly to strengthen the muscles of your back and abdomen, which work to
support your spine.
Use good posture when sitting, standing, and sleeping. Good posture helps to relieve the pressure on your lower back.
Avoid sitting for long periods.
Preventing of Backache
Steps to lower the risk of developing back pain consist mainly of addressing some of the risk factors.
Exercise – regular exercise helps build strength as well as keeping your body weight down. Experts say that low-impact aerobic activities are best; activities that do not strain or jerk the back. Before starting any exercise program, talk to a health care professional.
There are two main types of exercise that people can do to reduce the risk of back pain:
Core-strengthening exercises– exercises that work the abdominal and back muscles, helping to strengthen muscles that protect the back.
Flexibility – exercises aimed at improving flexibility in your core, including your spine, hips, and upper legs, may help too.
Smoking – a significantly higher percentage of smokers have back pain incidences compared to non-smokers of the same age, height and weight.
Bodyweight – the number of weight people carry, as well as where they carry it, affects the risk of developing back pain. The difference in back pain risk between obese and normal-weight individuals is considerable. People who carry their weight in the abdominal area versus the buttocks and hip area are also at greater risk.
Posture when standing – make sure you have a neutral pelvic position. Stand upright, head facing forward, back straight, and balance your weight evenly on both feet – keep your legs straight and your head in line with your spine. If you regularly use a computer, it is important to ensure that you have a chair with good back support and adopt a good posture and head position.
Posture when sitting – a good seat should have good back support, armrests and a swivel base (for working). When sitting try to keep your knees and hips level and keep your feet flat on the floor – if you can’t, use a footstool. You should ideally be able to sit upright with support in the small of your back. If you are using a keyboard, make sure your elbows are at right-angles and that your forearms are horizontal.
Lifting things – the secret for protecting your back when lifting things is to think “legs not back”. In other words, use your legs to do the lifting, more than your back.
Keep your back as straight as you can, keeping your feet apart with one leg slightly forward so you can maintain balance. Bend only at the knees, hold the weight close to your body, and straighten the legs while changing the position of your back as little as possible.
Bending your back initially is unavoidable, but when you bend your back try not to stoop or squat, and be sure to tighten your stomach muscles so that your pelvis is pulled in. Most important, do not straighten your legs before lifting; otherwise you will be using your back for most of the work.
Do not lift and twist at the same time. If something is particularly heavy, see if you can lift it with someone else. While you are lifting keep looking straight ahead, not up nor down, so that the back of your neck is like a continuous straight line from your spine.
Moving things – remember that it is better for your back to push things across the floor, using your leg strength, rather than pulling them.
Shoes – flat shoes place less of a strain on the back.
Driving – it is important to have proper support for your back. Make sure the wing mirrors are properly positioned so you do not need to twist. The pedals should be squarely in front of your feet. If you are on a long journey, have plenty of breaks – get out of the car and walk around.
Your bed – you should have a mattress that keeps you spine straight, while at the same time supporting the weight of your shoulders and buttocks. Use a pillow, but not one that forces your neck into a steep angle.
Home Remedies for Lumbago /Backache
Ice and Heat
Ice works wonders on lower back pain. Wrap some ice cubes in a plastic bag to prepare an ice pack. Then cover it with a towel and apply it on the painful area for 20 minutes. Repeat the same process several times a day. Then after 48 hours, you can switch to heat method. Dip a towel in warm water. Flatten and fold it on to the affected area. Place heating pad on it with a plastic cover between towel and heating pad. Leave it for 20 minutes. Do it several times a day. It reduces swelling and relaxes the nerves that are responsible for sending pain signals to the brain.
Rest
Get sufficient rest. Don’t exhaust yourself physically and mentally. When sleeping, keep changing your positions. When you lie on back, put a pillow under your knees. Similarly, if you lie on your side, draw your knees near your chest and keep a pillow between your knees.
Right Posture
Your sitting and standing posture is very important to keep back pain at bay. One should not be in a bending position for a long time whether sitting or standing. Sitting on the edge of the chair and slouching should be avoided. The angle of the chair in the office should be 110 degrees.
Lemon Juice
Lemon juice is an effective home remedy for back pain. Drink lemon juice twice a day for better results.
Poppy Seeds
Prepare a mixture of poppy seeds and rock candy by grinding together 100 gm of each. Take this mixture twice a day with a glass of milk. You will get relief from back pain.
Massage with Olive Oil
Massage with olive oil to reduce stress by relaxing tensed muscles. It also helps release stiffness in joints and relieves upper back pain.
Stretching
Stretching is the easiest back pain treatment. If your job demands sitting or standing for long hours, just take a break of 5 minutes every hour and walk or simply stretch your body to avoid back pain.
Wheat
Wheat has pain minimizing component in it. Mix cuscus grass and coriander with overnight soaked wheat. Add 1 cup of milk and bring it to boil. Consume this mixture twice a day
Garlic
Eat 2-3 garlic cloves on an empty stomach every morning to get relief from back pain. You can also use garlic oil. Massage your back with this oil, cover it with warm blanket and lie on your back. Bathe using warm water after 20 minutes. This is a wonderful home remedy to treat back pain.
Ginger
The anti-inflammatory properties of ginger make it an ideal home remedy to get rid of back pain. Add ½ teaspoon of black peppercorns, ½ teaspoon of cloves and 1 teaspoon of ginger powder in a cup of boiling water to prepare herbal tea. Drink it 2-3 times a day.
Alternatively, grate some ginger to prepare a paste. Apply it on the affected area. Then massage with eucalyptus oil.
Put thin ginger slices in a pan of boiling water. Simmer it for 10-15 minutes. Strain and allow it to cool down at room temperature. Add honey to sweeten it. Drink it twice or thrice a day.
Milk
Since milk is a great source of calcium, it is extremely beneficial for strong bones and preventing back pain. People of every age group should consume milk. For quick relief, add a few drops of honey and a pinch of turmeric in the milk.
Epsom Salt
A natural healer, epsom salt reduces swelling in back. It contains magnesium and sulfate which help muscles function properly, thus, provide relief from pain. Add 2 cups of Epsom salt to a tub of warm water. Let it soak for 30 minute. Take bath with this water.
Rice
Rice is easily available in every household. It’s an effective home remedy for back pain. Put 1 cup uncooked rice in a thick sock and place it in the microwave for ½ – 1 minute. Now apply it onto the back.
Oats
Mash cooked whole oats with vinegar. Apply it on the back when hot. It soothes the aching back.
Potatoes
Mash the peeled and boiled potatoes. Let them cool and then apply on back. You will experience relief from back pain.
Coconut Oil
Take some coconut oil. Mix camphor in it and boil for 5-7 minutes. Allow it to cool. Store it in a bottle. Massage with this oil two times a day to cure back pain.
Capsaicin Cream
Capsaicin is an important ingredient of chilies. Apply capsaicin cream on the back. It will reduce the production of chemicals that transmit signals of pain to your brain.
Herbal Remedies for Lumbago /Backache
Willow Bark
White willow tree’s bark is considered an excellent herbal remedy for treating back pain. It has pain-relieving properties same as aspirin. So it will help reduce your back pain.
Basil Leaves
Basil leaves are very famous for their medicinal benefits. They aid in curing lower back pain. Boil 10-12 fresh basil leaves in a cup of water until it becomes half. Add a pinch of salt to it. Drink it once or twice a day depending on the severity of your pain.
Herbal Oils
Herbal oils like almond oil, eucalyptus oil, coconut oil or olive oil are very effective in alleviating back pain. Massage with warm oils on the painful area to relax the nerves causing pain.
Chamomile
Take some chamomile flowers. Steep them in a cup of boiling water for 15-20 minutes. Drink it 2-3 times a day. It will relax the tense muscles, thereby cure backache.
Note: – Pregnant ladies and those allergic to chamomile flowers should first consult doctor before taking this.
Ginger
Though more studies are needed, says Dr. Kiefer, ginger extract may help with joint and muscle pain because it contains phytochemicals, which help stop inflammation. Few side effects have been linked to ginger when taken in small doses.
Feverfew
Feverfew has been used for centuries to treat headaches, stomachaches, and toothaches. Nowadays it’s also used for migraines and rheumatoid arthritis. More studies are required to confirm whether feverfew is actually effective, but the herb may be worth trying since it hasn’t been associated with serious side effects. Mild side effects include canker sores and irritation of the tongue and lips. Pregnant women should avoid this remedy.
Turmeric
This spice has been used to relieve arthritis pain and heartburn, and to reduce inflammation. It’s unclear how turmeric works against pain or inflammation, but its activity may be due to a chemical called curcumin, which has anti-inflammatory properties. Turmeric is usually safe to use, but high doses or long-term use may cause indigestion. Also, people with gallbladder disease should avoid using turmeric.
Homeopathic Medicines for Lumbago /Backache
Rhus Tox
Rhus Tox tops the list of Homeopathic medicines for back pain. I have seen magnificent results in back pain from use of Rhus Tox. Rhus Tox is indicated for both upper and lower back pain, especially where the back pain is accompanied by intense stiffness. The back pain that arises from muscle strain also recovers wonderfully well with Rhus Tox. Persons suffering from back pain as a result of exertion or lifting heavy weights have found complete relief when prescribed Rhus Tox, making it one of the most reliable Homeopathic medicines for back pain. A prominent symptom to look out for while prescribing Rhus Tox is that the back pain gets worse with rest, while walking or hard pressure bring relief from pain.
Bryonia
In my clinical practice, Bryonia has shown marvellous results in lower back pain that worsens with the slightest of motion. Apart from motion, this pain also gets worse with standing or from turning in the bed, a key sign that Bryonia will work best. The pain may be accompanied by marked stiffness in such cases, for which Bryonia would rate among the best Homeopathic medicines for back pain. Lying down and taking rest brings relief from pain.
Aesculus
Aesculus is one of the most effective Homeopathic medicines for lower back pain that gets worse from stooping. In this case, the pain is most marked in the sacrum and hip region. The lower back feels as if it would break. Stiffness in the lower back is also intense. Aesculus is also one of the best Homeopathic medicines for back pain which gets worse when rising from a sitting position. Here it takes the person repeated efforts to rise from a chair or another sitting position.
Kali Carb
I would rank Kali Carb as one of the top grade Homeopathic medicines for back pain that arises after childbirth. The most prominent symptoms indicative of Kali Carb as the best suited Homeopathic medicines for back pain in such instances are stiffness and weakness in the lower back. The pain is very severe, with a feeling that the back might break. The back pain makes it difficult to walk. Women feel the need to lie down to get relief from the pain which may radiate to the upper back or down to the thigh and hips. Where these symptoms exist, Kali Carb comes highly recommended as one of the best Homeopathic medicines for back pain. Apart from post-partum backache, Kali Carb is also useful for backache in women before or during menses and after a miscarriage.
Cobaltum
Cobaltum ranks on top of the list of Homeopathic medicines for back pain that worsens from sitting. In such cases, the person feels better while walking or lying down. The back pain may radiate down the legs and feet in some cases, but the person will surely feel a weakness in the legs, a sure sign that Cobaltum will provide sustained relief.
Colocynth & Magnesium Phos
I have successfully treated several cases of back pain radiating down the legs and/or feet with two main Homeopathic medicines. These top rated Homeopathic medicines for back pain are Colocynth and Magnesium Phos. Among these, Colocynth is most effective Homeopathic medicine for back pain when the lower back pain radiates to the left leg and foot. Magnesium Phos brings relief when the lower back pain radiates down the right leg. The pain, in both the cases, can be of a shooting, cramping or tearing nature. However, both the medicines have proven their ability to bring lasting relief from pain and established themselves as the best Homeopathic medicines for back pain.
Cimicifuga & Kalmia
Two highly recommended Homeopathic medicines for back pain in the cervical region are Cimicifuga and Kalmia. I have seen remarkable results with use of Cimicifuga in cervical back pain accompanied by stiffness, contraction and sensitiveness in the neck. If pressure worsens the neck pain, Cimicifuga will offer effective treatment. However, in cases where the cervical pain radiates down the arm or hands, Kalmia has proved to be one of the most helpful Homeopathic medicines for back pain treatment. Persons feeling a weakness, numbness or tingling sensation in the arms and hands along with neck pain also recover fully well with use of Homeopathic medicine Kalmia.
Ruta & Hypericum
Ruta and Hypericum are highly suitable Homeopathic medicines for back pain resulting from injury. Ruta is prescribed for a back that is sore and bruised from injury. The pain is most marked over the sacrum and coccyx region. The injured person may feel a weakness in the lower back. Where such symptoms are noted, Ruta is the most prominent among Homeopathic medicines for back pain and has shown effective results. Homeopathic medicine Hypericum is recommended when pain from the tail bone radiates up the spine and down the limbs after injury. The pain is very sharp and intense. Motion, walking and stooping all make the pain worse. The spine is very tender and sensitive to touch in such cases where Hypericum has shown best results.
Symptoms, Causes of Piriformis Syndromeis a neuromuscular condition characterized by hip and buttock pain. This syndrome is often overlooked in clinical settings because its presentation may be similar to that of lumbar radiculopathy, primary sacral dysfunction, or innominate dysfunction. The ability to recognize piriformis syndrome requires an understanding of the structure and function of the piriformismuscle and its relationship to the sciatic nerve. The authors review the anatomic and clinical features of this condition, summarizing the osteopathic medical approach to diagnosis and management. A holistic approach to diagnosis requires a thorough neurologic history and physical assessment of the patient based on the pathologic characteristics of piriformis syndrome. The authors note that several nonpharmacologic therapies, including osteopathic manipulative treatment, can be used alone or in conjunction with pharmacotherapeutic options in the management of piriformis syndrome.[Rx]
Piriformis syndrome (PS) is a painful musculoskeletal condition, characterized by a combination of symptoms including buttock or hip pain due to compressed and/or irritated sciatic nerve by the piriformis muscle as it passes deeply through your buttock, resulting in pain. It is an uncommon neuromuscular disorder that is caused when the piriformis muscle compresses the sciatic nerve.[Rx]
Piriformis syndrome is an often misdiagnosed cause of sciatica, leg, or buttock pain, and disability. The sciatic nerve may be compressed within the buttock by the piriformismuscle, with pain increased by muscular contraction, palpation, or prolonged sitting. A thorough medical history and physical examination are essential to proper diagnosis. Diagnostic testing may be used to differentiate piriformis syndrome from other causes of sciatica, lower extremity weakness, and pain. This article reviews the pathophysiology and management of piriformis syndrome.
The piriformis is a flat, pyramid-shaped muscle that lies parallel to (in line with) the gluteus medius muscle’s back margin and underneath the gluteus maximus muscle in the hip area.
Pain in your buttocks and radiating sciatic pain is sometimes the result of piriformis syndrome, or tightening and irritation of the piriformis muscle.
Anatomy of Piriformis Syndrome
Sciatic nerve
Inferior to piriformis
Superior to superior gemellus
Muscles
External rotators of the thigh include (superior to inferior)
Piriformis
Superior gemellus
Obturator internus
Inferior gemellus
Obturator externus
Quadratus femoris
Causes of Piriformis Syndrome
Muscle spasm in the piriformis muscle, either because of irritation in the piriformis muscle itself, or irritation of a nearby structure such as the sacroiliac joint or hip
Repetitive, improper movements or physical activities, such as those commonly found in long-distance running, sitting for lengthy periods of time and/or sports
Sudden injury, trauma or accident causing irritation to the piriformis muscle or nearby areas, such as the hip or sacroiliac joint
Previous injuries near the back, pelvis, piriformis muscle or sciatic nerve
an injury, such as a fall, a blow to the area, or a car accident
overuse, such as from frequent running, excessive exercise, or over-stretching
a sedentary lifestyle, especially with long periods of sitting
changing from a sedentary lifestyle to more frequent exercise
buttock muscles wasting away
Tightening of the muscle, in response to injury or spasm
Swelling of the piriformis muscle, due to injury or spasm
Bleeding in the area of the piriformis muscle.
muscle tension and excess weight due to pregnancy
Causes of piriformis syndrome include the following: [2]
Trauma to the hip or buttock area
Piriformis muscle hypertrophy (often seen in athletes during periods of increased weightlifting requirements or pre-season conditioning)
Sitting for prolonged periods (taxi drivers, office workers, bicycle riders)
Anatomic anomalies
Bipartite piriformis muscle
Sciatic nerve course/branching variations with respect to the piriformis muscle
Early (proximal) divisions of the sciatic nerve into its tibial and common peroneal components can predispose patients to piriformis syndrome, with these branches passing through and below the piriformis muscle or above and below the muscle [4]
In >80% of the population, the sciatic nerve courses deep to and exits inferiorly to the piriformis muscle belly/tendon [3]
Symptoms of Piriformis Syndrome
Tenderness, pain, numbness or tingling in the buttocks or along the back of the leg that intensifies without activity
Pain in the buttock or hip area is the most common symptom.
Pain may radiate from the buttock area down into the lower leg along the path of the sciatic nerve. Some patients may complain of low back pain.
There may be numbness and tingling in the buttock area, which can sometimes radiate down to the lower leg.
Pain with bowel movements may be present.
Women can sometimes experience painful intercourse.
There may be tenderness in the buttock area when pressure is applied. Certain patients may have a palpable “sausage-shaped” mass in the buttock area from piriformis muscle contraction/spasm.
Difficulty participating in daily activities
Aching, soreness or tightness in the buttocks that can worsen with long periods of sitting, running or walking up or down stairs
A noticeably reduced range of motion through the hip joint
Discomfort when light pressure is applied over the p
Sciatic pain is sharp and searing, rather than dull, and is described as “pins and needles.” You may also experience numbness and weakness in this leg. This pain can be debilitating and make it difficult to stand and walk.
Common complaints associated with piriformis syndrome include
Pain that becomes more severe following prolonged periods of sitting
A dull and achy pain located in the gluteus region
Test Diagnosis of Piriformis Syndrome is a neuromuscular condition characterized by hip and buttock pain. This syndrome is often overlooked in clinical settings because its presentation may be similar to that of lumbar radiculopathy, primary sacral dysfunction, or innominate dysfunction. The ability to recognize piriformis syndrome requires an understanding of the structure and function of the piriformismuscle and its relationship to the sciatic nerve. The authors review the anatomic and clinical features of this condition, summarizing the osteopathic medical approach to diagnosis and management. A holistic approach to diagnosis requires a thorough neurologic history and physical assessment of the patient based on the pathologic characteristics of piriformis syndrome. The authors note that several nonpharmacologic therapies, including osteopathic manipulative treatment, can be used alone or in conjunction with pharmacotherapeutic options in the management of piriformis syndrome.[Rx]
Piriformis syndrome (PS) is a painful musculoskeletal condition, characterized by a combination of symptoms including buttock or hip pain due to compressed and/or irritated sciatic nerve by the piriformis muscle as it passes deeply through your buttock, resulting in pain. It is an uncommon neuromuscular disorder that is caused when the piriformis muscle compresses the sciatic nerve.[Rx]
Piriformis syndrome is an often misdiagnosed cause of sciatica, leg, or buttock pain, and disability. The sciatic nerve may be compressed within the buttock by the piriformismuscle, with pain increased by muscular contraction, palpation, or prolonged sitting. A thorough medical history and physical examination are essential to proper diagnosis. Diagnostic testing may be used to differentiate piriformis syndrome from other causes of sciatica, lower extremity weakness, and pain. This article reviews the pathophysiology and management of piriformis syndrome.
The piriformis is a flat, pyramid-shaped muscle that lies parallel to (in line with) the gluteus medius muscle’s back margin and underneath the gluteus maximus muscle in the hip area.
Pain in your buttocks and radiating sciatic pain is sometimes the result of piriformis syndrome, or tightening and irritation of the piriformis muscle.
Anatomy of Piriformis Syndrome
Sciatic nerve
Inferior to piriformis
Superior to superior gemellus
Muscles
External rotators of the thigh include (superior to inferior)
Piriformis
Superior gemellus
Obturator internus
Inferior gemellus
Obturator externus
Quadratus femoris
Causes of Piriformis Syndrome
Muscle spasm in the piriformis muscle, either because of irritation in the piriformis muscle itself, or irritation of a nearby structure such as the sacroiliac joint or hip
Repetitive, improper movements or physical activities, such as those commonly found in long-distance running, sitting for lengthy periods of time and/or sports
Sudden injury, trauma or accident causing irritation to the piriformis muscle or nearby areas, such as the hip or sacroiliac joint
Previous injuries near the back, pelvis, piriformis muscle or sciatic nerve
an injury, such as a fall, a blow to the area, or a car accident
overuse, such as from frequent running, excessive exercise, or over-stretching
a sedentary lifestyle, especially with long periods of sitting
changing from a sedentary lifestyle to more frequent exercise
buttock muscles wasting away
Tightening of the muscle, in response to injury or spasm
Swelling of the piriformis muscle, due to injury or spasm
Bleeding in the area of the piriformis muscle.
muscle tension and excess weight due to pregnancy
Causes of piriformis syndrome include the following: [2]
Trauma to the hip or buttock area
Piriformis muscle hypertrophy (often seen in athletes during periods of increased weightlifting requirements or pre-season conditioning)
Sitting for prolonged periods (taxi drivers, office workers, bicycle riders)
Anatomic anomalies
Bipartite piriformis muscle
Sciatic nerve course/branching variations with respect to the piriformis muscle
Early (proximal) divisions of the sciatic nerve into its tibial and common peroneal components can predispose patients to piriformis syndrome, with these branches passing through and below the piriformis muscle or above and below the muscle [4]
In >80% of the population, the sciatic nerve courses deep to and exits inferiorly to the piriformis muscle belly/tendon [3]
Symptoms of Piriformis Syndrome
Tenderness, pain, numbness or tingling in the buttocks or along the back of the leg that intensifies without activity
Pain in the buttock or hip area is the most common symptom.
Pain may radiate from the buttock area down into the lower leg along the path of the sciatic nerve. Some patients may complain of low back pain.
There may be numbness and tingling in the buttock area, which can sometimes radiate down to the lower leg.
Pain with bowel movements may be present.
Women can sometimes experience painful intercourse.
There may be tenderness in the buttock area when pressure is applied. Certain patients may have a palpable “sausage-shaped” mass in the buttock area from piriformis muscle contraction/spasm.
Difficulty participating in daily activities
Aching, soreness or tightness in the buttocks that can worsen with long periods of sitting, running or walking up or down stairs
A noticeably reduced range of motion through the hip joint
Discomfort when light pressure is applied over the p
Sciatic pain is sharp and searing, rather than dull, and is described as “pins and needles.” You may also experience numbness and weakness in this leg. This pain can be debilitating and make it difficult to stand and walk.
Common complaints associated with piriformis syndrome include
Pain that becomes more severe following prolonged periods of sitting
A dull and achy pain located in the gluteus region
FAIR Test – The flexion, adduction, and internal rotation test flex the hip to stretch the piriformis and compress the sciatic nerve. It measures delays in sciatic nerve signals due to its compression under the piriformis.
Piriformis syndrome tests
There are also a few specific tests for piriformis syndrome that have been highlighted in scientific studies.
Pain will shoot down the back of your leg when your leg is raised straight (typically by a partner) while you lie on your back. This is indicative of irritation of the sciatic nerve, though it is not specific to piriformis syndrome.
The straight-leg raise test can cause sciatica-like pain if you have piriformis syndrome, but might also indicate the presence of low back problems
Knees against resistance test
This test can be performed while sitting.
Attempt to push your knees out against resistance (provided by a partner or rope). If this causes pain, piriformis syndrome is likely.
Pain might also occur if you attempt to abduct your hips from a sitting position against resistance provided by a partner or a rope.
Piriformis stretch test
Finally, two maneuvers which put a stretch on the piriformis muscle can also be used to test for piriformis pain.
Having a partner rotate your hip and leg inwards while you lie on your back with your knees straight can produce pain, as can lying on your unaffected side and rotating the painful side across your body with your knee bent.
One test which can produce piriformis-specific pain is a supine internal leg rotation, assisted by either by a partner or a rope, as illustrated here.
Stretching the piriformis in this position can elicit pain (red area) if you have piriformis syndrome
Though these piriformis-specific tests can help confirm the presence of piriformis syndrome, they are not accurate enough to rule it out.
But here’s the kicker
Hopayian et al.’s review study found no one technique to be reliable or accurate enough to endorse; rather, they cited the more general symptom of aggravation or modulation of piriformis pain when you stretch or tension the piriformis muscle.
You might also be able to feel a thickening in the piriformis muscle itself, deep within your glutes, but this is also not enough by itself to definitively diagnose piriformis syndrome.
Treatment Exercise of piriformis syndromeis a neuromuscular condition characterized by hip and buttock pain. This syndrome is often overlooked in clinical settings because its presentation may be similar to that of lumbar radiculopathy, primary sacral dysfunction, or innominate dysfunction. The ability to recognize piriformis syndrome requires an understanding of the structure and function of the piriformismuscle and its relationship to the sciatic nerve. The authors review the anatomic and clinical features of this condition, summarizing the osteopathic medical approach to diagnosis and management. A holistic approach to diagnosis requires a thorough neurologic history and physical assessment of the patient based on the pathologic characteristics of piriformis syndrome. The authors note that several nonpharmacologic therapies, including osteopathic manipulative treatment, can be used alone or in conjunction with pharmacotherapeutic options in the management of piriformis syndrome.[Rx]
Treatment of Piriformis Syndrome
Clinical treatment options include
Botox injections that can reduce muscle spasms and relieve pain.
Prescription pain medications or muscle relaxants. A person should discuss the risks and benefits of pain medication with their doctor, as these drugs can be addictive.
Corticosteroid or anesthetic injections.
Alternative treatments, such as acupuncture, chiropractic manipulation, and trigger point therapy.
Physical therapy to regain use of the piriformis, and to prevent wasting related to disuse and dysfunction in surrounding muscles.
Physiotherapy
Stretching exercises and massage,
Avoidance of contributory activities as noted before
The best piriformis stretch (that actually works!)
This is exactly what is accomplished in the stretches recommended by Douglas Keskula and Michael Tamburello in a 1992 article on treatments for piriformis syndrome.
Supine piriformis stretch with a crossover (moving left knee towards right shoulder) ,
Supine piriformis stretch without a crossover (moving heel towards right shoulder)
Supine piriformis stretch assisted by opposite leg (moving right knee towards right
You should be gentle with the stretches, not overly aggressive—this may put too much stress on the already-irritated piriformis.
Piriformis exercises
Strengthening exercises are also recommended in several different scientific papers.
As the piriformis works as an abductor and rotator of the hip, strengthening both the piriformis itself and the other hip muscles that surround it is a primary goal of treatment.
RunnersConnect Insider Bonus
Download our full Piriformis Prevention Routine inside your Insider Members area.
It’s a PDF with images and descriptions of the 10 most effective prevention and rehab exercises for runners with Piriformis issues.
Click here to access
Not a RunnersConnect Insider member? It’s FREE to join. Click here to get your guide and get started free
A 2010 case report by Jason Tonley and a group of fellow physical therapists describes in detail a strengthening protocol used to successfully treat piriformis syndrome in a 30-year-old recreational athlete who displayed many of the classic signs of poor hip muscle coordination: inward knee rotation during single-leg squats and poor hip abduction and external rotation strength.
To address this, the authors prescribed a 14-week, three-step program for hip muscle rehabilitation.
The first phase consisted only of glute bridges and clamshell leg lifts, both using a theraband for resistance.
After four weeks, the patient progressed to weight-bearing exercises: standing mini-squats (with a theraband), “monster walk” side steps (also with a band), a “sit-to-stand” exercise, and single-leg mini-squats.
Following four weeks of the second phase, the patient progressed to lunges, deep squats, and even plyometric-style hops and landings (with the intent to prepare him to return to basketball and tennis, his principle sports).
In all phases of rehab, the patient progressed over time to three sets of fifteen repeats of each exercise.
These are the piriformis stretches I have been looking for! Great detail!CLICK TO TWEET
A similar program designed for runners is illustrated below. Start gradually, but build up over time to three sets of 15 repeats of each exercise.
Phase I: Four weeks
a. Clamshell exercise, adding resistance with theraband
b. Glute bridge with theraband (hold, for up to two minutes)
c. Side leg lift
Phase II: Four weeks
Do all Phase I exercises, and add the following:
a. Standing mini-squats with a theraband
b. “Monster walk” side steps (continuously moving in one direction, then moving back the other), also with a band
c. Single-leg “sit-to-stand” from chair
d. Single-leg mini-squats off a step
Phase III: 6 weeks.
Do all phase I and II exercises, and add the following:
a. Front and diagonal lunges
While the rehab program in Conley et al. was immensely successful with their patient, a case report obviously isn’t as useful as a randomized clinical trial.
It’s unclear how useful this program would be for other athletes with piriformis syndrome, but given the lack of high-quality studies, and the dearth of research on treatments specifically for athletes, Conley et al.’s program is still a pretty good place to start.
Consider this:
Combining these strength exercises with the stretches described above should address both muscle weakness and tightness.
These stretches and exercises were just what I needed for my piriformis syndrome!
Other research on piriformis syndrome has focused on treatments for more stubborn cases.
Is this you?
Some isolated studies describe injections into the piriformis muscle, either of a local anesthetic like lidocaine or of a corticosteroid. Studies indicate that pain relief from injections is highly variable, with some patients experiencing long-lasting relief, and others getting none at all.
You won’t believe this:
Some newer trials have even investigated BOTOX injections (the muscle-paralyzing drug better-known for its use in cosmetic surgery) for treating recalcitrant piriformis syndrome.
Given how little is known about injectable treatments for piriformis syndrome, especially considering that none of the studies on this topic involved athletes, it’s hard to draw any concrete recommendations—these options are something you should discuss with your doctor.
Looking for a last resort?
Surgical release of the piriformis muscle has also been described in multiple papers as a last-resort treatment for piriformis syndrome. As with injectable treatments, studies on surgical patients invariably focus on sedentary people, often with additional existing back or spine problems, so it’s nearly impossible to extract any information useful to a runner. Again, talk to a trusted doctor if you are considering surgery.
RunnersConnect Insider Bonus
Download our full Piriformis Prevention Routine inside your Insider Members area.
It’s a PDF with images and descriptions of the 10 most effective prevention and rehab exercises for runners with
Not a RunnersConnect Insider member? It’s FREE to join. Click here to get started
Other Piriformis Syndrome Treatment Options
Though there’s not much in the literature about treating piriformis syndrome in runners, it occurs commonly enough for several “folk treatments” and workarounds to have emerged. Among these are:
Having a massage or stretching out the piriformis muscle and reduce tightness. One way many runners do so is by rolling their glute muscles on a tennis ball or a lacrosse ball (perfectly shaped to put controlled pressure on the glute area).
Deep tissue massage techniques are also popular, and they may well accomplish the same goal as the “myofascial release” massage techniques that are described in some case studies by physical therapists.
Another popular method to address piriformis syndrome is to simply avoid doing things that irritate the piriformis muscle: prolonged sitting, in particular, can be very irritating, so modifying your routine so you don’t need to sit as often or for as long can be helpful.
Standing desks are becoming more popular, and taking a short break every hour or so allows you to get your piriformis stretches in, too. If nothing else, experimenting with different sitting surfaces (harder, softer, flatter, or more contoured) might also reduce irritation.
If you are still able to do some running, avoiding workouts or conditions which irritate your piriformis will also help—common culprits include high speeds, uphills and downhills, and tight turns.
Of course, it goes without saying that none of this is supported by scientific research, so you’ll have to experiment with what works for you and what does not.
Summary of treatment for piriformis syndrome
Conservative treatments
These are methods that are fairly simple, inexpensive, and can be done on your own at home.
Before jumping right into treatment, it is important to emphasize that these treatments have been developed specifically with piriformis syndrome in mind, not buttock or sciatic pain in general.
Remember
If you’re not sure whether you have piriformis syndrome, you should see a doctor to get a proper diagnosis. Other injuries which cause similar symptoms will require different treatments.
Stretching routine incorporating the following exercises.
Begin by stretching very gently, building up over time to three sets of 5-10 individual stretches, each held for five seconds. Over time, you can build up to 60 seconds for each stretch.
Supine piriformis stretch with a crossover
Supine piriformis stretch without a crossover
Supine piriformis stretch assisted by opposite leg
Hip strengthening exercises
Based on Conley et al.’s paper, with a few minor modifications to make the exercises more relevant for runners. Start gradually, but build up over time to three sets of 15 repeats of each exercise.
Phase I: four weeks
Clamshell exercise, adding resistance with theraband
Glute bridge with theraband (hold for up to two minutes)
Side leg lift
Phase II: four weeks
Do all phase I exercises, and add the following:
Standing mini-squats with a theraband
“Monster walk” side steps, also with a band
Single-leg “sit-to-stand” from the chair
Single-leg mini-squats off a step
Phase III: 6 weeks.
Do all phase I and II exercises, and add the following:
Front and diagonal lunges
Gentle daily rolling
Use a foam roller (making sure you do not make these 4 mistakes), tennis ball, or lacrosse ball to loosen up the piriformis muscle and glutes.
This article breaks piriformis syndrome into helpful phases, a must read!
Piriformis syndrome treatment for those who have tried everything else
These are treatments with more cost and less certainty about outcomes but may prove useful when you are fed up of your pain.
Working with a physical therapist to develop a specialized rehab program
Because the literature is so sparse on appropriate exercises for treating piriformis syndrome in runners, it might make sense to see a PT if your case is particularly troublesome or long-lasting.
That way, you can address any aspects of your own individual muscular tightness or weakness that might contribute to your injury
Active Release Technique or Graston Technique
These soft tissue mobilization exercises don’t have any support in the scientific literature but have been praised anecdotally by some, though not all, runners with piriformis syndrome.
Injections of a local anesthetic, corticosteroid, or BOTOX
If you have a recalcitrant case of piriformis syndrome that has not responded to many months of conservative rehab, you can talk to your doctor about an injectable treatment.
If all else fails, surgery is a final alternative. This is also something you should consult with a trusted doctor about.
Additional exercise
You may do all of these exercises right away.
Gluteal stretch – Lie on your back with both knees bent. Rest the ankle on your injured side over the knee of your other leg. Grasp the thigh of the leg on the uninjured side and pull toward your chest. You will feel a stretch along the buttocks on the injured side and possibly along the outside of your hip. Hold the stretch for 15 to 30 seconds. Repeat 3 times.
Standing hamstring stretch – Put the heel of the leg on your injured side on a stool about 15 inches high. Keep your leg straight. Lean forward, bending at the hips, until you feel a mild stretch in the back of your thigh. Make sure you don’t roll your shoulders or bend at the waist when doing this or you will stretch your lower back instead of your leg. Hold the stretch for 15 to 30 seconds. Repeat 3 times.
Resisted hip abduction – Stand sideways near a door with your injured side further from the door. Tie elastic tubing around the ankle on your injured side. Knot the other end of the tubing and close the knot in the door near the floor. Pull the tubing out to the side, keeping your leg straight. Return to the starting position. Do 2 sets of 15. For more resistance, move farther away from the door.
The plank – Lie on your stomach resting on our forearms. With your legs straight, lift your hips off the floor until they are in line with your shoulders. Support yourself on your forearms and toes. Hold this position for 15 seconds. (If this is too difficult, you can modify it by placing your knees on the floor.) Repeat 3 times. Work up to increase your hold time to 30 to 60 seconds.
Side plank – Lie on your side with your legs, hips, and shoulders in a straight line. Prop yourself up onto your forearm with your elbow directly under your shoulder. Lift your hips off the floor and balance on your forearm and the outside of your foot. Try to hold this position for 15 seconds and then slowly lower your hip to the ground. Switch sides and repeat. Work up to holding for 1 minute. This exercise can be made easier by starting with your knees and hips flexed toward your chest.
Prone hip extension with bent leg – Lie on your stomach with a pillow under your hips. Bend the knee on your injured side. Draw your belly button in towards your spine and tighten your abdominal muscles. Lift your bent leg off the floor about 6 inches (15 centimeters). Keep your other leg straight. Hold for 5 seconds. Then lower your leg and relax. Do 2 sets of 15.
Clam exercise – Lie on your uninjured side with your hips and knees bent and feet together. Slowly raise your top leg toward the ceiling while keeping your heels touching each other. Hold for 2 seconds and lower slowly. Do 2 sets of 15 repetitions.
Causes, Symptoms of Lumbar Disc Herniation /Spinal disc herniation also is known as a slipped disc, is a medical condition affecting the spine in which a tear in the outer, fibrous ring of an intervertebral disc allows the soft, central portion to bulge out beyond the damaged outer rings. Disc herniation is usually due to age-related degeneration of the outer ring, known as the annulus fibrosis, although trauma, lifting injuries, or straining have been implicated as well. Tears are almost always postero-lateral (on the back of the sides) owing to the presence of the posterior longitudinal ligament in the spinal canal. This tear in the disc ring may result in the release of chemicals causing inflammation, which may directly cause severe pain even in the absence of nerve root compression.
Lumbar Disc Herniation /Spinal disc herniation also is a common condition that frequently affects the spine in young and middle-aged patients.1,5,11 The lumbar intervertebral disc is a complex structure composed of collagen, proteoglycans, and sparse fibro chondrocyte cells that serve to dissipate forces exerted on the spine. As part of the normal aging process, the disc fibro chondrocytes can undergo senescence, and proteoglycan production diminishes. This leads to a loss of hydration and disc collapse, which increases strain on the fibers of the annulus fibrosus surrounding the disc. Tears and fissures in the annulus can result, facilitating a herniation of disc material, should sufficient forces be placed on the disc. Alternatively, a large biomechanical force placed on a healthy, normal disc may lead to extrusion of disc material in the setting of catastrophic failure of the annular fibers.5
Anatomy of Spinal Disc Herniation
Herniated = from “a hernia,” a part of the body that bulges out through an abnormal opening Disc = the disk-shaped cushions between the bones of the spine
The vertebral column (also called the spinal column orbackbone) is made up of 33 bones known as vertebra (plural, vertebrae). Each vertebra is separated from the adjacent vertebrae by intervertebral discs, a spongy but strong connective tissue. The intervertebral discs, along with ligaments and facet joints, connect the individual vertebrae to help maintain the spine’s normal alignment and curvature while also permitting movement.
The image at left shows the entire spinal column from beside and from the front. The bones of the spinal column are orange in color, and the intervertebral discs are white.
In the center of the spinal colum,n there is an open channel called the spinal canal. The spinal cord and spinal nerves are located in the spinal canal, where they are surrounded by spinal fluid and protected by the strong spinal column. On each side of the spine, small openings between adjacent vertebrae called foramina (singular, foramen) allow nerve roots to enter and exit the spinal canal.
The spine is divided into the following distinct regions:
Cervicalspine – consists of seven vertebrae in the neck. These vertebrae are small and allow for the mobile nature of the neck.
Thoracic spine – consists of 12 vertebrae in the upper and mid-back. These are larger and stronger than the cervical vertebrae. Each thoracic vertebra is attached to a rib on either side. This provides significant stiffness and strength to the thoracic portion of the spine.
Lumbar spine – usually consists of five vertebrae in the lower back, but may vary between four and six. These vertebrae are the largest because they withstand the greatest amount of force in the spine. The lumbar spine is also more mobile than the thoracic spine. Because of these factors, the lumbar spine is the most frequently affected by degenerative conditions, spinal stenosis, and herniated discs.
Sacrococcygeal – the very lowest portion of the spine. The sacrococcygeal region consists of one single bone, made of fused vertebrae in the sacrum (five vertebrae) and coccyx (four vertebrae). It attaches to the pelvis on either side. In a small number of people, there may be a disc between the first and second sacral vertebrae. Alternatively, the fifth vertebra in the lumbar (lower) spine may occasionally be fused to the sacrum, leaving only 4 lumbar vertebrae.
A herniated disc occurs when the fibrous outer portion of the disc ruptures or tears, and the jelly-like core squeezes out. When the herniated disc compresses a nearby nerve, as in the image below, the result can be a pinched nerve. A pinched nerve may cause pain, numbness, tingling or weakness in the arms or legs. The substance that makes up the disc’s jelly-like core can also inflame and irritate the nerve, causing additional pain.
Prolapse of intervertebral disc closeup 3d image. (c) alexmit/Big Stock
A bulging disc occurs when the outer wall of the disc weakens but doesn’t rupture, and “bulges” outward. A herniated disc may actually begin as a bulging disc whose outer wall is then ruptured by a great amount of pressure.
Disc herniation can occur in the cervical, thoracic, or lumbar spine. The location of the pain depends on the location of the herniated disc. If the herniation occurs in the neck, for example, it can cause pain that radiates into the shoulder and arm; if it occurs in the lower back, the pain produced can radiate down into the hip and leg. Depending on the location, it can damage the spinal cord.
Symptoms of Spinal Disc Herniation
A cervical herniated disc may put pressure on a cervical spinal nerve and can cause symptoms like pain, pins and needles, numbness or weakness in the neck, shoulders, or arms. A large disc herniation in the cervical spine may compress the spinal cord within the spinal canal and cause numbness, stiffness, and weakness in the legs and possibly some difficulty with bowel and bladder control.
A thoracic herniated disc may cause pain in the mid back around the level of the disc herniation. If the disc herniation compresses a thoracic spinal nerve as it travels through the foramen, then pain or numbness may travel around the rib cage from the back to the front of the chest or upper abdomen. A large disc herniation in the thoracic spine may compress the spinal cord within the spinal canal and cause numbness, stiffness and weakness in the legs and possibly some difficulty with bowel and bladder control.
A lumbar herniated disc may cause the following symptoms:
Intermittent or continuous back pain (this may be made worse by movement, coughing, sneezing, or standing for long periods of time)
Sciatica — pain that starts near the back or buttock and travels down the leg to the calf or into the foot.
Muscle weakness in the legs
Numbness in the leg or foot
Decreased reflexes at the knee or ankle
Changes in bladder or bowel function
Difficulty walking
Incoordination
The symptoms of disc disease may resemble other conditions or medical problems. Always consult a doctor for a diagnosis.
Causes and Risk Factors
Herniated discs can often be the result of degenerative disc disease. As people age, the intervertebral discs lose their water content and ability to cushion the vertebrae. As a result, the discs are not as flexible. Furthermore, the fibrous outer portion of the disc is more likely to rupture or tear.
Acute disc herniations can occur in young, healthy people as a result of an injury or tear to the outer layer of the disc (called the annulus fibrosis) that allows the central, jelly-like portion of the disc (called the nucleus pulposis) to herniate into the spinal canal or foramen.
Tests and Diagnosis of Spinal Disc Herniation
Physical examination
The straight leg raise may be positive, as this finding has low specificity; however, it has high sensitivity. Thus the finding of a negative SLR sign is important in helping to “rule out” the possibility of a lower lumbar disc herniation. A variation is to lift the leg while the patient is sitting.[32] However, this reduces the sensitivity of the test.[33]
Imaging
Projection radiography (X-ray imaging) – Although traditional plain X-rays are limited in their ability to image soft tissues such as discs, muscles, and nerves, they are still used to confirm or exclude other possibilities such as tumors, infections, fractures, etc. In spite of these limitations, X-ray can still play a relatively inexpensive role in confirming the suspicion of the presence of a herniated disc. If a suspicion is thus strengthened, other methods may be used to provide final confirmation.
Computed tomography scan (CT or CAT scan) – A diagnostic image created after a computer reads x-rays. It can show the shape and size of the spinal canal, its contents, and the structures around it, including soft tissues. However, visual confirmation of a disc herniation can be difficult with a CT.
Magnetic resonance imaging (MRI) without contrast – A diagnostic test that produces three-dimensional images of body structures using powerful magnets and computer technology. It can show the spinal cord, nerve roots, and surrounding areas, as well as enlargement, degeneration, and tumors. It shows soft tissues better than CAT scans. An MRI performed with a high magnetic field strength usually provides the most conclusive evidence for the diagnosis of a disc herniation. T2-weighted images allow for clear visualization of protruded disc material in the spinal canal.
Myelogram An x-ray of the spinal canal following injection of a contrast material into the surrounding cerebrospinal fluid spaces. By revealing displacement of the contrast material, it can show the presence of structures that can cause pressure on the spinal cord or nerves, such as herniated discs, tumors, or bone spurs. Because myelography involves the injection of foreign substances, MRI scans are now preferred for most patients. Myelograms still provide excellent outlines of space-occupying lesions, especially when combined with CT scanning (CT myelography).
Electromyogram and nerve conduction studies (EMG/NCS) – These tests measure the electrical impulse along nerve roots, peripheral nerves, and muscle tissue. This will indicate whether there is ongoing nerve damage, if the nerves are in a state of healing from a past injury, or whether there is another site of nerve compression. EMG/NCS studies are typically used to pinpoint the sources of nerve dysfunction distal to the spine.
Computerized tomography (CT) scan – a series of X-rays, assembled by a computer into 3-dimensional images of the body’s structures
Myelography – a procedure that involves injecting a liquid dye into the spinal column followed by a series of X-rays and a computerized tomography (CT) scan. This procedure may provide useful images that reveal the indentations of the spinal fluid sac caused by bulging or herniated discs, or bone spurs that might be pressing on the spinal cord or nerves.
Electromyography (EMG) – tests the electrical activity of a nerve root to help determine the cause of pain.
The presence and severity of myelopathy can be evaluated by means of transcranial magnetic stimulation (TMS), a neurophysiological method that allows the measurement of the time required for a neural impulse to cross the pyramidal tracts, starting from the cerebral cortex and ending at the anterior horn cells of the cervical, thoracic or lumbar spinal cord. This measurement is called Central Conduction Time (CCT). TMS can aid physicians to:
determine whether myelopathy exists
identify the level of the spinal cord where myelopathy is located. This is especially useful in cases where more that two lesions may be responsible for the clinical symptoms and signs, such as in patients with two or more cervical disc hernias[34]
follow-up the progression of myelopathy in time, for example before and after cervical spine surgery
TMS can also help in the differential diagnosis of different causes of pyramidal tract damage.[35]
Since a herniated disc may cause similar symptoms to other degenerative spinal conditions, a surgeon may order a variety of diagnostic procedures to rule out other possible conditions.
Treatment of Spinal Disc Herniation, Exercise, Home Remedies. Lumbar disc herniation is a common condition that frequently affects the spine in young and middle-aged patients.1,5,11 The lumbar intervertebral disc is a complex structure composed of collagen, proteoglycans, and sparse fibrochondrocytic cells that serve to dissipate forces exerted on the spine. As part of the normal aging process, the disc fibrochondrocytes can undergo senescence, and proteoglycan production diminishes. This leads to a loss of hydration and disc collapse, which increases strain on the fibers of the annulus fibrosus surrounding the disc. Tears and fissures in the annulus can result, facilitating a herniation of disc material, should sufficient forces be placed on the disc. Alternatively, a large biomechanical force placed on a healthy, normal disc may lead to extrusion of disc material in the setting of catastrophic failure of the annular fibers.5
Treatment of Spinal Disc Herniation
Before discussing surgery as an option, the surgeon may initiate the following nonoperative treatments. Specific treatment for lumbar disk disease will be determined by your health care provider based on
Your age, overall health, and medical history
The extent of the condition
Type of condition
Your tolerance for specific medications, procedures, or therapies
Expectations for the course of the condition
Your opinion or preference
Typically, conservative therapy is the first line of treatment to manage lumbar disk disease. This may include a combination of the following:
Bed rest
Patient education on proper body mechanics (to help decrease the chance of worsening pain or damage to the disk)
Physical therapy, which may include ultrasound, massage, conditioning, and exercise
Weight control
Use of a lumbosacral back support
Medications Treatment of Spinal Disc Herniation
Analgesics – Prescription-strength drugs that relieve pain but not inflammation.
Antidepressants: A Drugs that block pain messages from your brain and boost the effects of endorphins (your body’s natural painkillers).
Corticosteroids: Also known as oral steroids, these medications reduce inflammation.
Muscle Relaxants: These medications provide relief from spinal muscle spasms.
Neuropathic Agents: Drugs(pregabalin & gabapentin) that address neuropathic—or nerve-related—pain. This includes burning, numbness, and tingling.
Opioids – Also known as narcotics, these medications are intense pain relievers that should only be used under a doctor’s careful supervision.
Topical Medications – These prescription-strength creams, gels, ointments, patches, and sprays help relieve pain and inflammation through the skin.
NSAIDs – Prescription-strength drugs that reduce both pain and inflammation. Pain medicines and anti-inflammatory drugs help to relieve pain and stiffness, allowing for increased mobility and exercise. There are many common over-the-counter medicines called non-steroidal anti-inflammatory drugs (NSAIDs). They include aspirin, ibuprofen (Motrin, Advil), and naproxen (Naprosyn, Aleve).
Glucosamine & diaceraine can be used to tightening the loose tension and regenerate cartilage or inhabit the further degeneration of cartilage.
Corticosteroid to healing the nerve inflammation and clotted blood in the joints.
The dietary supplement to remove the general weakness & improved the health.
There is little evidence to suggest that drug treatments are effective in treating a herniated disc.
NSAIDs and cytokine inhibitors don’t seem to improve symptoms of sciatica caused by disc herniation.
We found no evidence examining the effectiveness of analgesics, antidepressants, or muscle relaxants in people with a herniated disc.
We found no evidence of sufficient quality to judge the effectiveness of epidural injections of corticosteroids.
With regard to non-drug treatments, spinal manipulation seems to be more effective at relieving local or radiating pain in people with acute back pain and sciatica with disc protrusion compared with sham manipulation, although concerns exist regarding possible further herniation from spinal manipulation in people who are surgical candidates.
Neither bed rest nor traction seems effective in treating people with sciatica caused by disc herniation.
We found insufficient evidence of advice to stay active, acupuncture, massage, exercise, heat, or ice to judge their efficacy in treating people with a herniated disc.
About 10% of people have sufficient pain after 6 weeks for surgery to become a consideration.
Both standard discectomy and microdiscectomy seem to increase self-reported improvement to a similar extent.
We found insufficient evidence judging the effectiveness of automated percutaneous discectomy, laser discectomy, or percutaneous disc decompression.
Surgical Treatment of Spinal Disc Herniation
When these conservative measures fail, surgery for removal of a herniated disk may be recommended. Surgery is done under general anesthesia. An incision is placed in the lower back over the area where the disk is herniated. Some bone from the back of the spine may be removed to gain access to the area where the disk is located. Typically, the herniated part of the disk and any extra loose pieces of disk are removed from the disk space.
Surgical treatment for a herniated disc will be based on the following
The history, severity, and duration of pain
Whether or not the patient has received previous treatments for disc disorders and how effective the treatments were
Whether or not there is any evidence of neurologic damage such as sensory loss, weakness, impaired coordination, or bowel or bladder problems
Surgery for patients with disc disorders of the spine is usually recommended for those patients who do not find relief with non-operative treatment over a period of 6-12 weeks. Surgery is also recommended in patients who have a neurologic deficit (numbness, weakness or reduced function due to pressure on the spinal cord or nerves). Early intervention in those cases is best in order to maximize the likelihood of neurologic recovery.
Your surgeon may perform the following surgical procedures:
Microdiscectomy: A procedure that uses a microscope and microsurgical tools to remove the portion of the disc that is pressing against the nerve, relieving the pressure caused by a herniated disc. Microdiscectomy is frequently performed for herniated discs in the cervical, thoracic, and lumbosacral spine. This procedure is performed under general anesthesia through a small skin incision over the spine. The muscles of the spine are gently elevated or spread apart to expose a small segment of the spine. A small amount of the back part of the spine, called the lamina and facet joint, is trimmed under high magnification of the microscope to provide safe access to the spinal canal. Using microsurgical techniques, our neurosurgeons identify and remove the herniated piece of the disc while protecting the compressed nerve. Most patients may go home either on the day of surgery or the next morning.
Anterior (from the front) or lateral (from the side) surgical approaches may be required for large or calcified thoracic disc herniations that cause spinal cord compression.
Anterior Cervical Discectomy and Fusion (ACDF): a procedure that involves the removal of the herniated disc in the cervical spine through the front of the neck. A fusion surgery may be required to make the spine stable after the discectomy.
After surgery, restrictions may be placed on the patient’s activities for several weeks while healing is taking place to prevent another disk herniation from occurring. Your surgeon will discuss any restrictions with you.
Others Treatment of Spinal Disc Herniation
Chiropractic Care
Sixty percent of people with sciatica who didn’t get relief from other therapies and then tried spinal manipulation experienced the same degree of pain relief as patients who eventually had surgery, found a 2010 study in the Journal of Manipulative and Physiological Therapeutics. The 120 people in the study saw a chiropractor about 3 times a week for 4 weeks and then continued weekly visits, tapering off treatment as they felt better. In people who responded to chiropractic care, benefits lasted up to a year. “Spinal manipulation may create a response in the nervous system that relieves pain and restores normal mobility to the injured area,” says study researcher Gordon McMorland, DC, of National Spine Care in Calgary, Alberta. “It also reduces inflammation, creating an environment that promotes the body’s natural healing mechanisms.”
Acupuncture
“You can get relief as soon as the first session, though it takes about 12 sessions to see improvement,” says Jingduan Yang, MD, assistant professor at the Jefferson Myrna Brind Center of Integrative Medicine at Thomas Jefferson University. A small study in the Journal of Traditional Chinese Medicine found that of 30 people with sciatica, 17 got complete relief and 10 saw symptoms improve with warming acupuncture, in which the needles are heated.
Yoga
A study in the journal Pain reported that people with chronic back pain who practiced Iyengar yoga for 16 weeks saw pain reduced by 64% and disability by 77%. Although yoga’s effects on sciatica are less clear, gentle forms may be beneficial. By strengthening muscles and improving flexibility, a yoga practice can help sciatica sufferers “move and function better so they don’t fall into a posture that aggravates sciatica,” says James W. Carson, Ph.D., a psychologist at the Comprehensive Pain Center at Oregon Health & Science University. For extra grip and stability, try these grip socks from Natural Fitness.
Massage
Don’t expect a chilled-out spa massage if you have sciatica. In this instance, trigger-point therapy is best, says Jeff Smoot, vice president of the American Massage Therapy Association. The sciatic nerve sits underneath a muscle called the piriformis, which is located beneath the glutes. “When the piriformis muscle gets tight, it pinches the sciatic nerve, causing tingling and numbness down into the leg,” says Smoot. He applies pressure to irritated and inflamed areas, or trigger points, in the piriformis muscle, as well as in muscles in the lower back and glutes. Typically, Smoot schedules treatments 7 to 10 days apart. If patients don’t see progress by the fourth visit, “they need to try another form of therapy,” he says.
Topical Preparations
St. John’s wort oil, a liniment, is “one of my favorites for nerve pain,” says Tieraona Low Dog, MD, director of the fellowship at the Arizona Center for Integrative Medicine. Apply the anti-inflammatory oil two or three times a day where there’s pain. Another option: an OTC cayenne pepper plaster or cream; capsaicin, found in chiles, hinders the release of pain-causing compounds from nerves. For severe cases, Low Dog uses the prescription chile patch Qutenza, designed for shingles pain. “One application is effective for weeks,” says Low Dog.
Ice or Heat
Because the sciatic nerve is buried deep within the buttock and leg, ice or heat on the surface of the body won’t ease that inner inflammation. But the time-honored treatments can act as counterirritants—that is, “they give your body other input in the painful area, and that brings the pain down a notch,” says Ruppert. Apply an ice pack or a heating pad as needed for 15 minutes.
Devil’s Claw
The herbal medication devil’s claw is “quite a potent anti-inflammatory, working like ibuprofen and similar drugs to inhibit substances that drive inflammation,” says Low Dog. She generally starts patients on 1,500 to 2,000 mg twice a day. Look for a brand that has a standardized extract of roughly 50 mg of harpagoside, the active compound. Safety reviews show that the supplement is well tolerated by most people but should be avoided by patients with peptic ulcers or on blood-thinning medications.
Epidural Steroid Injections
People whose pain doesn’t lessen within about a month and who aren’t helped by other therapies may find their pain remedied by an x-ray-guided injection of steroid into the lower back near the sciatic nerve, says Raj Rao, MD, a spokesperson for the AAOS. “The hope is to reduce inflammation within that nerve branch,” explains Rao. Because of concerns about side effects, such as loss of bone density, the epidural shots are limited to three a year.
Physiotherapy in Herniated Disc
In stage 1&2 of herniated disc physiotherapy must be applied to cure herniated his.I n the case of stage 3&4, physiotherapy can’t be applied due to avoiding another case of foot drop.
In accordance with NIH journal
Physiotherapy for a lumbar disc bulge
Physiotherapy treatment for a lumbar disc bulge is vital to ensure an optimal outcome and may comprise:
soft tissue massage
electrotherapy (e.g. ultrasound)
lumbar taping
the use of a back brace
mobilization
traction
the use of a lumbar roll for sitting
dry needling
exercises to push the disc back ‘in’ and to improve strength, core stability and flexibility
education
activity modification advice
biomechanical correction
ergonomic advice
clinical Pilates
hydrotherapy
a functional restoration program
a gradual return to activity program
Physical therapy often plays a major role in herniated disc recovery. Its methods not only offer immediate pain relief, but they also teach you how to condition your body to prevent further injury.
There are a variety of physical therapy techniques. Passive treatments relax your body and include deep tissue massage, hot and cold therapy, electrical stimulation (eg, TENS), and hydrotherapy.
Your physical therapy program will usually begin with passive treatments. But once your body heals, you will start active treatments that strengthen your body and prevent further pain. Your physical therapist will work with you to develop a plan that best suits you.
Passive Physical Treatments for Herniated Discs
Deep Tissue Massage
There are more than 100 types of massage, but a deep tissue massage is an ideal option if you have a herniated disc because it uses a great deal of pressure to relieve deep muscle tension and spasms, which develop to prevent muscle motion at the affected area.
Hot and Cold Therapy
Both hot and cold therapies offer their own set of benefits, and your physical therapist may alternate between them to get the best results. Your physical therapist may use heat to increase blood flow to the target area. Blood helps heal the area by delivering extra oxygen and nutrients. Blood also removes waste byproducts from muscle spasms. Conversely, cold therapy (also called cryotherapy) slows circulation. This reduces inflammation, muscle spasms, and pain. Your physical therapist may place an ice pack on the target area, give you an ice massage, or even use a spray known as fluoromethane to cool inflamed tissues.
Hydrotherapy
As the name suggests, hydrotherapy involves water. As a passive treatment, hydrotherapy may involve simply sitting in a whirlpool bath or warm shower. Hydrotherapy gently relieves pain and relaxes muscles.
A TENS machine uses an electrical current to stimulate your muscles. It sounds intense, but it really isn’t painful. Electrodes taped to your skin send a tiny electrical current to key points on the nerve pathway. TENS reduces muscle spasms and is generally believed to trigger the release of endorphins, which are your body’s natural painkillers.
Traction
The goal of traction is to reduce the effects of gravity on the spine. By gently pulling apart the bones, the intent is to reduce the disc herniation. The analogy is much like a flat tire “disappearing” when you put a jack under the car and take pressure off the tire. It can be performed in the cervical or lumbar spine.
Active Treatments You May Try in Physical Therapy
Active treatments help address flexibility, posture, strength, core stability, and joint movement. An exercise program may also be prescribed to achieve optimal results. This will not only curb recurrent pain but will also benefit your overall health. Your physical therapist will work with you to develop a program based on your specific diagnosis and health history.
Core stability
Many people don’t realize how important a strong core is to their spinal health. Your core (abdominal) muscles help your back muscles support your spine. When your core muscles are weak, it puts extra pressure on your back muscles. Your physical therapist may teach you to core stabilizing exercises to strengthen your back.
Flexibility
Learning proper stretching and flexibility techniques will prepare you for aerobic and strength exercises. Flexibility helps your body move easier by warding off stiffness.
Hydrotherapy
In contrast to simply sitting in a hot tub or bath like its passive counterpart, active hydrotherapy may involve water aerobics to help condition your body without unnecessary stress.
Muscle strengthening
Strong muscles are a great support system for your spine and better handle pain.
Your physical therapist will teach you ways to condition and strengthen your back to help prevent future pain. You may learn self-care principles so you understand how to best treat your symptoms. The ultimate goal is for you to develop the knowledge to maintain a pain-free lifestyle.
It’s essential that you learn how to exercise and condition your back after the formal physical therapy ends. If you don’t implement the lessons you learned during physical therapy, you won’t enjoy its long-term results. By taking care of your back on your own, you may prevent further herniated disc pain
8 Best Exercises For Slipped Disc In Lower Back
Our spinal cord is supported by a number of muscles. Relevant exercises help relieve the pain and reduce the symptoms. Muscle exercises of those muscles associated with the affected area are necessary. Patients must know the region that has a slipped disc and then opt for exercises related to that muscle. The list of best exercises for the slipped disc are mentioned as follows:
Abdominal Isometrics – It can be performed either on floor, mat or bed. This exercise involves moving your lower back towards the surface at which you are performing this exercise. Leg movement must be reduced in this exercise and stomach muscles must be made active. This reduces pain in lower back because of the attachment of abdominal muscles to the lower side of the vertebral column. Ten repetitions are effective.
Crunches – Lie on a flat surface with knees bent. Cross your arm under your head, raise your head and chest in such a manner that your rib cage curl interiorly towards your backbone. Perform this exercise slowly and gradually. In the beginning, perform fewer crunches and repeat it daily and increase the number of turns as you gain strength.
Lower back extension – Lie in an upside down position, raise your upper body with the help of elbow and hold up yourself in an elevated position for a short span of time and then slowly lower down. Please make sure that during this exercise you do not raise your pelvis girdle (hip region).
Bilateral knee to the chest – Lay down on a flat surface and draw your knee towards your abdominal region, repeat it 5 times and then switch leg. You can also increase the number of turns each time you repeat it.
Iso-hip flexion – Lay down over a flat surface and draw your knees towards your chest region in a 90-degree position with your stomach. Place your hands over your knees and then exert your hand pressure to lower your knee. Then utilize the knee pressure to resist the downward movement of your legs, in all both movements should just exert pressure and allow no movements. This position should be maintained for a few seconds and then lowered slowly and gradually.
Air bike – Sit on a chair with your chest and shoulders supported. Align your knees and feet together and then bring them towards your body and perform a pedaling motion in the air then repeat the same motion while moving your knees farther away from the body. Follow ten repetitions each time and increase its number as you gain strengths
Hamstring stretch: Lie on a flat surface with your knees bent, place your hands under your knees and then slightly pull your leg towards your chest, repeat it with another leg. This exercise must involve a stretch over lower thigh muscle
Lumbar roll: Lie on a flat surface with your knee bent and your feet lying on the floor then move your legs together towards the right side and then towards your left side. Repeating these movements 5 times on each side.
The above mentioned best exercises for the slipped disc can be followed but if pain increases or muscle pain is persisting then quit these exercises right away. These exercises not only help in reducing the pain but they also activate efficient muscle movement. Along with these exercise tips, proper body postures must be also maintained to prevent further disc damages.
Home Remady for Herniated Disc/Slip Disc
Consciousness
In case of PLID home remedies are not special treatment just only home practice & creating public awareness. All should be done in PLID stage 1&2
Walking
Walking every day keeps muscle disorders away. Walking can also help to prevent herniated disc. Walk on a flat road for 20 minutes as many times as you can in a day. Take longer steps as it will help you to keep away the pain of herniated disc. Do not give strain to yourself as it might increase the pain.
Rest
www.rxharun.com
Rest is essential for patients suffering from a herniated disc. Take short rest periods from time to time. When you are sleeping make sure you don’t stay in the same position for a long time. Do not sleep on your stomach. Also, take care of the mattress you are sleeping on. Don’t let it be too soft and spongy. Buy a mattress that has a good surface area and is soft in nature.
Physiotherapy And Yoga( only home practice)
Physiotherapy is a very cheap and good way of getting rid of a herniated disc from itself. Therapists will teach your proper exercises and stretches which will improve the disc shape to a great extent.
You will notice good differences while performing daily chores after just 4-5 sessions of therapy.
Physiotherapy also promotes faster healing of the disorder.
Turmeric
Turmeric contains curcumin which is a very good anti-oxidant and anti-inflammatory agent. This is why it stops the gel-like fluid inside the discs from coming out and bulge. It also shows antihistamine properties which help to reduce pain because of slowed blood circulation to the area of pain.
Dimethyl Sulfoxide (DMSO)
Dimethyl sulfoxide is a derivative from sulfur which has antioxidant properties as well as the organic sulfur present in it helps in the growth of new cells and detoxification of the body. The growth of new cells helps to replace the old cells of the discs and prevent the fluid from leaking outside.
Massage With Essential Oils
Massage with essential oils on the full body, especially on the spine and lower back regions, will help in good blood circulation and promote the growth of new cells. It will help relieve pain and promote better absorption of oxygen and nutrients. Essential oils will also regenerate the cells of the disc and hence stop the disc from getting slipped.
Acupressure And Acupuncture
In both techniques, the pressure is used for relieving the pain from the swelled area. In acupressure fingers, tips and elbow are used and acupuncture needles are used. But this should be done with the help of an experienced practitioner and not alone.
This is not recommended for patients having high blood pressure and for women who are pregnant.
TENS
TENS stands for Transcutaneous Electrical Nerve Stimulation and this is one of the best remedies for the herniated disc at home. This treatment uses low voltage electric current which is applied to the affected area and helps the body to release endorphin which decreases the pain.
Cayenne Pepper
It is a very effective ingredient for the treatment of herniated disc. You can drink its tea or make a paste of the pepper using water and apply on the affected area.
Diet
Diet is necessary to keep away all types of bad conditions that might affect you. Drink a lot of water and eat a balanced diet. Take excess of fibers and proteins. During this condition, you should avoid dairy products and red meat. Also, avoid fat-free foods.
Epsom Salt
Epsom salt is one of the widely used natural painkiller and anti-inflammatory agent.
You can use this by adding 3-4 cups of salt in a hot water bath. Stay inside the bath for 15 minutes. It will help you achieve maximum relaxation.
Do not use this remedy if you are diabetic or pregnant. If you are on any type of medication consult your doctor before bathing in Epsom salt.
Horsetail
Horsetail is a herb which has high quantities of minerals in it. It nourishes our tissues and has the ability to heal broken bones and torn ligaments.
All you need to do is add some horsetail leaves to half a liter of water. Boil on low heat till the water quantity reduces to half its quantity. Cool the solution and filter it off. You can drink 5 ml of the solution thrice a day. It will heal herniated disc very fast.
California Poppy
California poppy is anti-inflammatory and analgesic in nature. This is what makes it a good treatment for the herniated disc.
You can tear the leaves of California poppy into small pieces and make a paste out of it using water. Use little hot water so that when you apply the paste to the affected area it is still warm.
White Willow Bark
White willow bark is used for reducing the discomfort of herniated discs. The chemical structure of this drugs shows a marked similarity to aspirin hence acts as an analgesic but doesn’t irritate your gut. It is also astringent and anti-inflammatory in nature.
This herb might react with drugs hence do consult your doctor if you are on any kind of medication.
Comfrey Leaves
Comfrey leaves have the power to heal bones and connective tissues of the body. All you need to do is take some fresh leaves and add it to cold water. Let it remain undisturbed for around 12 hours. After 12 hours heat the above solution and filter it. Add the filtrate to bath water and take a bath in it 2 times a day. Do not consume it orally because it contains hepatic-toxin alkaloids.
Boswellia
Boswellia is a naturally occurring painkiller which is a very effective remedy for a herniated disc.
All you can do is make a decoction of Boswellia and consume it 2 times a day to reduce pain and discomfort associated with herniated discs.
Boswellia is an organic painkiller that effectively treats the problem of a herniated disc. It is also an herbal cure for osteoarthritis.
Omega-3 Fatty Acids
Omega-3 Fatty acids are helpful in decreasing the inflammation and pain experienced due to herniated disc disorder. This acid forms collagen which is used by the broken discs for repairing itself.
Eat foods that are high in this kind of fats like fish, almonds, sprouts, and walnuts.
Colchicine
Colchicine is an active amino-alkaloid found in the plant of Kurchi or autumn crocus. This powder is obtained by crushing the seeds of the plant. It has anti-inflammatory properties which are effective against the slipped disc.
Make a paste with kurchi powder and honey and consume it once a day.
You can also make tea out of the powder or mix the powder in milk and have it once or twice a day.
Burdock
Burdock contains a lot of anti-oxidants which is helpful to detoxify the body and remove all kinds of harmful substances and decrease the pain and inflammation in your body. It also treats arthritis.
Burdock can be consumed as a decoction once or twice a day.
Passionflower
Passionflower is helpful for slipped discs because the essential oils present is antispasmodic in nature. It reduces pain and inflammation.
You can massage with passionflower essential oil or take capsules made from it, however, do consult your doctor before taking capsules.
Additional Tips
If you are overweight, try to lose some pounds.
Exercise every day.
Lift things in a proper way, as guided by a therapist. Do not lift heavy weights.
Stop smoking and drinking.
Always make sure you are in the right posture whatever activity you may be doing.
Wear flat and soft shoes. Avoid heels.
Walk and move around cautiously.
Slipped discs can be really painful but with the right treatment and precautions, you can become as fit as you were before. So start taking home remedies and consult a doctor whenever you feel any kind of severe pain.
Spondylolysis refers to a posterior defect of the vertebral body occurring at the pars interarticularis. Typically, this defect results from trauma or chronic repetitive loading and hyperextension. If this instability leads to translation of the vertebral body, this is spondylolisthesis.[rx][rx] This process requires either a fracture or deformation of the posterior spinal elements resulting in elongation of the pars interarticularis. This condition can potentially occur in all age groups, with the underlying cause varying based on the age. If the slip progresses to the point of neurologic compromise, then surgical intervention may be necessary to decompress and stabilize affected segments.[rx] Absent any motor deficits, a nonoperative course of analgesia, activity modification, and injections should be the initial therapeutic approach for several months.[rx]
Types of Spondylolysis
Pars defects (spondylolysis) subdivide into five categories according to the Wiltse-Newman Classification[rx]:
Dysplastic – congenital abnormalities/attenuated pars (approximately 20%)
Isthmic – lesions in the pars resulting from a stress fracture or acute fractures (approximately 50%)
Type II-A – pars fatigue fracture
Type II-B – pars elongation due to a healed fracture
Type II-C – pars acute fracture
Degenerative – degeneration of the intervertebral discs that results in segmental instability and alterations of the articular processes
Traumatic – an acute fracture that results in fractures to various regions of the neural arch
Pathological – bone disease such as tumors and infections that result in lesions to the pars
Causes of Spondylolysis
A clinical syndrome caused by compression on the spinal cord that is characterized by
clumsiness in hands
gait imbalance
degenerative cervical spondylosis (CSM)
compression usually caused by anterior degenerative changes (osteophytes, disc-osteophyte complex)
degenerative spondylolisthesis and hypertrophy of ligamentum flavum may contribute
a most common cause of cervical myelopathy
Congenital stenosis
Symptoms usually begin when congenital narrowing combined with spondylotic degenerative changes in older patients
OPLL
tumor
epidural abscess
trauma
cervical kyphosis
Neurologic injury
mechanism of injury can be
direct cord compression
ischemic injury secondary to compression of the anterior spinal artery
tandem stenosis occurs in the lumbar and cervical spine in ~20% of patients
tends to be slowly progressive and rarely improves with nonoperative modalities
progression characterized by steplike deterioration with periods of stable symptoms
early recognition and treatment prior to spinal cord damage is critical for good clinical outcomes
Risk factors
Sports involving repetitive or forceful hyperextension of the spine, especially when combined with rotation are the main mechanism of injury for spondylolysis. The stress fracture of the pars interarticularis occurs on the side opposite of activity. For instance, for a right-handed player, the fracture occurs on the left side of the vertebrae.[rx]
Spondylolysis has a higher occurrence in the following activities:[rx]
Baseball
Military service
Tennis
Diving
Cheerleading
Gymnastics
Gridiron Football
Association Football
Wrestling
Weightlifting
Roller Derby
Cricket
Pole Vault
Rugby
Volleyball
Gym
Ultimate Frisbee (especially during impact from laying out)
Ballet
Muay Thai
Although this condition can be caused by repetitive trauma to the lumbar spine in strenuous sports, other risk factors can also predispose individuals to spondylosis. Males are more commonly affected by spondylolysis than females.[rx] In one study looking at youth athletes, it was found that the mean age of individuals with spondylolisthesis was 20 years of age.[rx] Spondylolysis also runs in families suggesting a hereditary component such as a predisposition to weaker vertebrae.[rx]
Risk Factors
The lists below are the factors that you will have a higher risk of getting neck pain and cervical spondylosis:
Genetics – if your family has a history of neck pain
Smoking – clearly linked to increased neck pain
Occupation – jobs with lots of neck motion and overhead work
Mental health issues – depression/anxiety
Injuries/trauma – car wreck or on-the-job injury
Malignancy, infection, or inflammation
Fever, night sweats
Unexpected weight loss
History of inflammatory arthritis, malignancy, infection, tuberculosis, HIV infection, drug dependency, or immunosuppression
Excruciating pain
Intractable night pain
Cervical lymphadenopathy
Exquisite tenderness over a vertebral body
Myelopathy
Gait disturbance or clumsy hands, or both
Objective neurological deficit—upper motor neuron signs in the legs and lower motor neuron signs in the arms
Sudden onset in a young patient suggests disc prolapse
Other
History of severe osteoporosis
History of neck surgery
Drop attacks, especially when moving the neck, suggest vascular disease
weakness and decreased manual dexterity (dropping object, difficulty manipulating fine objects)
Gait instability patient feels “unstable” on feet
weakness walking up and downstairs
gait changes are the most important clinical predictor
urinary retention rare and only appear late in disease progression, not very useful in diagnosis due to the high prevalence of urinary conditions in this patient population
Cervical pain aggravated by movement
Referred pain (occiput, between the shoulder blades, upper limbs)
Retro-orbital or temporal pain (from C1 to C2)
Cervical stiffness—reversible or irreversible
Vague numbness, tingling, or weakness in upper limbs
Dizziness or vertigo
Poor balance
Rarely, syncope triggers a migraine, pseudo-angina
Poorly localized tenderness
Limited range of movement (forward flexion, backward extension, lateral flexion, and rotation to both sides)
Minor neurological changes like inverted supinator jerks (unless complicated by myelopathy or radiculopathy)
Diagnosis of Spondylolysis
Other non-specific neck pain lesions—acute neck strain, postural neck ache, or whiplash
Fibromyalgia – and psychogenic neck pain
Mechanical lesions—disc prolapse or diffuse idiopathic skeletal hyperostosis
Inflammatory disease—rheumatoid arthritis, ankylosing spondylitis, or polymyalgia rheumatica
Metabolic diseases—Paget’s disease, osteoporosis, gout, or pseudo-gout
Infections—osteomyelitis or tuberculosis
Malignancy—primary tumors, secondary deposits, or myeloma
lower extremity weakness is more concerning finding
finger escape sign when the patient holds fingers extended and adducted, the small finger spontaneously abducts due to the weakness of intrinsic muscle grip and release test normally a patient can make a fist and release 20 times in 10 seconds. myelopathic patients may struggle to do this
Upper motor neuron signs
Hoffman’s sign (quick flexion of both the thumb and index finger when the middle fingernail is snapped)
Inverted radial reflex (flexion of the fingers in response to the brachioradialis reflex)
Pathological clonus
Babinski sign
Sensory dysfunction
Glove-like sensory loss in hands
Proprioceptive dysfunction
Proprioception dysfunction
due to dorsal column involvement
occurs in advanced disease
associated with a poor prognosis
Decreased pain sensation
pinprick testing should be done to look for the global decrease in sensation or dermatomal changes
due to the involvement of lateral spinothalamic tract
vibratory changes are usually only found in a severe case of long-standing myelopathy
Assessment tools
Lhermitte sign
Romberg test
9-Hole peg test
Grip and release test (observe a decreasing number of cycles)
Timed gait, 30-m walking test
Tandem gait
Upper motor neuron signs (spasticity)
Hyperreflexia – may be absent when there is concomitant peripheral nerve disease (cervical or lumbar nerve root compression, spinal stenosis, diabetes)
Hoffmann’s sign – snapping patients distal phalanx of the middle finger leads to spontaneous flexion of other fingers
Sustained clonus > three beats defined as sustained clonus, sustained clonus has poor sensitivity (~13%) but high specificity (~100%) for cervical myelopathy
Babinski test – considered positive with the extension of the great to toe-to-heel walk patient has difficulty performing
Romberg test – patient stands with arms held forward and eyes closed loss of balance consistent with posterior column dysfunction
provocative tests – Lhermitte Sign >test is positive when extreme cervical flexion leads to electric shock-like sensations that radiate down the spine and into the extremities
Motor dysfunction
Upper extremities
0
Unable to move hands
1
Unable to eat with a spoon but able to move hands
2
Unable to button shirt but able to eat with a spoon
3
Able to button shirt with great difficulty
4
Able to button shirt with slight difficulty
Lower extremities
0
Complete loss of motor & sensory function
1
Sensory preservation without the ability to move legs
2
Able to move legs but unable to walk
3
Able to walk on the flat floor with a walking aid (cane or crutch)
4
Able to walk up- &/or downstairs w/aid of a handrail
5
Moderate-to-significant lack of stability but able to walk up &/or downstairs without a handrail
6
Mild lack of stability but able to walk unaided with smooth reciprocation
recommended views cervical AP, lateral, oblique, flexion, and extension views
general findings degenerative changes of uncovertebral and facet joints
osteophyte formation
disc space narrowing
decreased sagittal diameter
cord compression occurs with canal diameter is < 13mm
lateral radiograph important to look for the diameter of the spinal canal
a Pavlov ratio of less than 0.8 suggests a congenitally narrow spinal canal predisposing to stenosis and cord compression
Sagittal alignment
C2 to C7 alignment determined by tangential lines on the posterior edge of the C2 and C7 body on lateral radiographs in a neutral position
local kyphosis angle the angle between the lines drawn at the posterior margin of most cranial and caudal vertebral bodies forming the maximum local kyphosis
oblique radiograph important to look for foraminal stenosis which often caused by uncovertebral joint arthrosis
flexion and extension views important to look for angular or translational instability look for compensatory subluxation above or below the spondylotic/stiff segment
sensitivity/specificity changes often do not correlate with symptoms 70% of patients by 70 yrs of age will have degenerative changes seen on plain x -rays.
Manual Test
Spinal range of motion testing – Range of motion limitations may be seen.
Lumbar hyperextension – Extension often elicits pain. This can be assessed by having the patient hyperextend the lumbar spine, provide resistance against back extensions, or undergo repeated lumbar extensions.
The neurological examination – would specifically show increased lumbar lordosis, tight hamstrings, reduced trunk range of motion (particularly with extension), tenderness to palpation overlying the pars fracture site, a positive stork test (single leg hyperextension and rotation of the spine which reproduces the patient pain and is diagnostic of spondylolysis until proven otherwise), with the characteristic absence of any radiculopathy. Again, radicular symptoms can occur, but they are uncommon.[rx][rx][rx]
The Stork test or one-legged hyperextension maneuver – is thought to be the only pathognomonic finding during examination. It involves asking the patient to stand on one leg and to extend the low back. When properly done, the leg is straight and the trunk tilted as a result of the lumbosacral extension. Concurrent ipsilateral knee flexion may produce trunk tilt without low back extension and subsequently, produce lower test sensitivity. Pain indicates possible spondylolysis on the ipsilateral side.[rx][rx][rx]
Passive Lumbar Extension test (PLE) – The patient is in the prone position; both lower extremities are then elevated simultaneously to a height of about 30 cm from the table while maintaining the knees extended and gently pulling the legs. The result of is test is considered as positive if the patient, during the elevation of both lower legs, complains of symptoms in his or her lumbar region, including “low back pain,” “very heavy feeling on the low back,” and “feeling as if the low back was coming off” and if such pain disappears when the lower legs are repositioned in the starting position. The sensitivity and specificity of the PLE are good (0.84 and 0.90, respectively).[rx]
Prone Instability Test (PIT) – The patient lies in the prone position with the trunk on the examining table and both legs over the edge, with the feet resting on the floor. The examiner performs passive lumbar intervertebral motion testing posteroanterior (PA) mobilization. The patient is asked to report any provocation of pain. The patient then lifts the legs off the floor (hand-holding to the table may be used to maintain position), and the passive intervertebral motion testing is reapplied to any segments that were identified as painful. A positive test result occurs when pain is provoked during the first part of the test but disappears when the test is repeated with the legs off the floor. The interexaminer reliability of the PIT is good (0.87).[rx]
Active Straight Leg Raise Test (ASLR) – This test investigates the ability of the pelvic girdle to transfer loads from the lumbopelvic region to the legs. The patient lies in the supine position with his or her legs straight and relaxed in physiological lateral rotation, and feet 20 cm apart. The patient is instructed to raise a straight leg about 20 cm off the table. The patient is asked to report any weakness, pain, or other unpleasant feelings during the test and any difference in feeling between the 2 sides. The examiner observes the speed of raising, the appearance of a tremor in the leg, the amount of rotation of the trunk, and the verbal and nonverbal emotional expressions of the patient. Impairment is scored on a 4-point scale: 0 (the patient feels no restriction), 1 (the patient reports decreased ability to raise the leg, but the examiner does not observe any sign of impairment), 2 (the patient reports decreased ability to raise the leg, and the examiner observes signs of impairment), and 3 (inability to raise the leg).
The ASLR – results are clinically reliable in patients with LBP and pelvic girdle dysfunction.[rx,rx] The sensitivity and specificity of the ASLR are good (0.87 and 0.94, respectively) for posterior pelvic pain in pregnancy.[rx]
Bridging maneuvers – also seem to be reliable and valid methods to investigate stabilization endurance in patients with LBP.[rx]
Prone Bridge Test – the patient lies in the prone position propped on his or her elbows. The elbows are spaced shoulder-width apart, and the feet are placed with a narrow base, but not touching. The patient raises his or her pelvis off the table so that only the forearms and the toes are in contact with the table. Shoulders, hips, and ankles are maintained in a straight line. This position is sustained until fatigue or pain prevents the maintenance of the test position.
The Supine Bridge Test – is performed in the supine position, with the lower limbs flexed and the soles of the feet on the table with a narrow base, but without touching. The thighs should not be in contact. The hands are positioned by the ears. The patient raises his or her pelvis from the table so that the shoulders, hips, and knees are maintained in a straight line. This position is held until fatigue or pain prevents the continued holding of the test position.
Bilateral extensor digitorum brevis test – wasting is a reliable clinical bedside marker while assessing for underlying lumbar canal stenosis.[rx]
The five repetitive sit-to-stand test (5R-STS) – wherein a patient with the ability to perform the test in around 10 seconds does not rate as having a significant functional impairment.[rx]
Aberrant Movement Pattern During Active Trunk Flexion – is an observational test starting from the standing position. Selected authors[rx-rx] have suggested that aberrant spinal motion during physiological movements that produce catching and disruption of a normal smooth arc of motion is suggestive of spinal instability. The patient is asked to bend forward as much as possible while the examiner identifies any abnormality in the movement pattern (painful arc during bending, painful arc on return, Gowers sign, instability catch, or reversal of lumbopelvic rhythm). The test result is considered positive if any of these patterns are present.
Muscle strength exercises – Lower abdominal, gluteal, and lumbar extensors should be assessed for weakness. Weakness in these muscles can increase lordosis and contribute to sacroiliac instability.[rx] Abdominal flexor strength can be assessed with the abdominal flexor endurance test. The test involves the patient lying supine while holding a 45 degree flexed trunk and 90 degree flexed knees for 30 seconds. Gluteal strength can be assessed with a single leg squat. Lastly, a lumbar extension can be assessed with a single leg bridge.
Imaging
X-ray – Following the history and examination, the best screening tool is an AP and lateral weight-bearing X-ray of the lumbar spine.[rx]Lumbosacral spondylolisthesis can be best assessed mainly on the lateral view, but occasional coronal deformity should not be missed. In cases where clinical examination indicates an abnormal sagittal balance of the spinal column, a whole spine lateral standing X-ray is indicated. In the majority of cases, an isthmic defect will be detected on radiographs but in doubtful cases. An MRI scan is recommended. Oblique X-rays of the lumbosacral junction, Computerised Tomography (CT) scan, SPECT scans may also identify the defect but involve ionic radiation.
MRI scans – are more sensitive in identifying pars lesions. MRI can also identify stress reactions that occur even before a fracture line develops.[rx] In dysplastic cases, dome-shaped or significantly inclined sacrum can present as well as trapezoid-shaped L5 and dysplastic facets of S1. Neoplasms and infections are an extremely rare primary cause of spondylolisthesis but should merit consideration as a differential diagnosis in patients with constitutional symptoms. To assess dynamic instability, flexion and extension views should be obtained. Either 4 mm of translation or 10 degrees of angulation of motion compared to the adjacent motion segment are diagnostic for spondylolisthesis.
T-2 weighted sequence test – is best to assess spinal canal stenosis, foraminal stenosis, and nerve root impingement, as well as the morphology of lumbar and sacral vertebrae which presence correlated with history and examination findings, will dictate the surgical management). The most commonly affected nerve root is L5.
Scintigraphy – is an excellent screening tool for low back pain in children or adolescents. It has shown high sensitivity for the detection of acute injuries and bone stress reaction in the pars. However, some lesions may not display an increased contrast uptake. Computed tomography scan (CT) – may be helpful in some cases due to its higher specificity. The tomographic finding of an acute injury include the margin reabsorption in the pars; pars sclerosis may indicate chronic stress, and marginal sclerosis with widening may indicate a chronic condition. The identification of patients with a normal CT scan and abnormalities on bone scintigraphy or Single-photon emission computed tomography (SPECT) is important as these patients are presumed to be in a very early stage of the disease and have a higher chance of healing with timely conservative treatment.
Normal SPECT ( Single Photon Emission Computed Tomography) – is considered the best diagnostic adjunct when plain radiographs are negative. Several of the abnormalities identified on SPECT proved to represent spinal pathology other than spondylolysis, including infection and osteoid osteoma. Although these modalities may present with increased sensitivity in detecting pars lesions compared with plain film, they are not necessarily highly specific for this disorder. Repetitive stress causes local bone remodeling and abnormal uptake of scintigraphic tracer. SPECT has 10 to 20 times more contrast than planar bone scintigraphy; it is more sensitive than radiography and planar bone scans and improves anatomic localization of skeletal lesions without exposing the patient to additional radiation.[rx]
Magnetic resonance imaging (MRI) – offers advantages in terms of visualizing other types of pathology present in the lumbar spine and may potentially detect pars edema secondary to stress in their clinical course.[rx] The lack of ionizing radiation with MRI may also make it a particularly desirable modality for studying pars lesions, especially in the female adolescent population.[rx] However, it is worth noting that MRI, like CT, does not assess whether a bony lesion is metabolically active and is less sensitive and specific than scintigraphy or SPECT.
Single Photon Emission Computed Tomography (SPECT) – scan is a test to analyze blood flow to an area of the body. A small amount of radioactive tracer is injected into a vein. As the tracer circulates in the blood, it is absorbed by the tissues and then gives off energy. The energy is seen by the CT scanner and can detect stress fractures, spondylolysis, infection, and tumors by the differences in how the radioactive substance is absorbed by normal healthy tissue vs. diseased tissue.
Treatment of Spondylolysis
Treatment typically begins with conservative therapy, including nonsteroidal anti-inflammatory drugs (NSAIDs), heat, light exercise, traction, bracing, and/or bed rest.
The majority of the cases can be treated non-operatively by:
Thoracolumbosacral / lumbosacral brace – [rx] In acute cases in the adolescent sportsperson bracing to prevent extension is shown to be superior to just activity modification. Activity modification (avoidance of hyperextension)[rx]
Core muscles strengthening – focusing on the deep abdominal muscles and the multifidus muscle[rx]
Low-intensity pulsed ultrasound (LIPUS) – in addition to conservative treatment appears to be very promising for achieving a higher rate of bony union. LIPUS requires more supporting studies but may prove to become a standard of care in the future.[rx]
Physical therapy – should be done for 6 months and include hamstring stretching, pelvic tilts, abdominal strengthening, and close follow up of low-grade dysplastic lysis as there is a higher chance of progression. In cases of adult degenerative spondylolisthesis with canal stenosis, an epidural steroid injection can provide short term relief.[rx]
Bracing – Some patients may need to wear a back brace for a period of time to limit movement in the spine and provide an opportunity for a recent pars fracture to heal. Relative 6 to 12 weeks of spinal bracing (Corset versus TLSO), thus, limiting spinal mobilization and stress on the pars interarticularis. However, a recent meta-analysis found that 83% of patients treated non-operatively improved clinically regardless of any spinal bracing.
Activity modifications – including cessation of activities, especially those involving a hyperextension of the spine. Athletic activities may be gradually resumed as the pain subsides.
Physical therapy – emphasizing spinal stabilization through stretching of the hip flexors, hamstrings, quadriceps, gastrocnemius-soleus complex, and strengthening of the abdominal and back muscles utilizing a pain-free range of motion with the application of the progressive resistance training protocol such as William’s flexion exercises is generally advised.
Adjunctive treatments – including ice/heat therapy, massage, osteopathic or chiropractic manipulation, and cognitive-behavioral therapy (CBT) are generally well-tolerated, are of benefits, and should be considered.
Manual Manipulation – Chiropractic manipulation provided by chiropractors, or manual manipulation provided by osteopathic physicians, physiatrists or other appropriately trained health professionals, can help reduce pain by mobilizing painful joint dysfunction.
Holistic therapy – Some patients find that acupuncture, acupressure, yoga, nutrition/diet changes, and biofeedback are helpful in managing pain as well as improving your overall health.
Medications
Analgesics – such as acetaminophen (Tylenol), can relieve pain but don’t have the anti-inflammatory effects of NSAIDs. Long-term use of analgesics and NSAIDs may cause stomach ulcers as well as kidney and liver problems.
Steroids – can be used to reduce the swelling and inflammation of the nerves. They are taken orally (as a Medrol dose pack) in a tapering dosage over a 5-day period. They have the advantage of providing pain relief within a 24-hour period.
Anti-inflammatory medications (NSAIDs)– in combination with paracetamol (Tylenol) can be tried initially. There are many common over-the-counter medicines called non-steroidal anti-inflammatory drugs (NSAIDs). They include aspirin, ibuprofen (Motrin, Advil), and naproxen (Naprosyn, Aleve).
Antidepressants– such as tricyclics and serotonin and norepinephrine reuptake inhibitors have been commonly prescribed for chronic low back pain, but their benefit for nonspecific low back pain is unproven, according to a review of studies assessing their benefit.
Muscle Relaxants – If the muscles around the slipped disc experience painful spasms, a muscle relaxant such as Valium may be useful. The drawback to drugs like these is that they do not limit their power to the affected nerve. Instead, they have a generally relaxing effect and will interfere with daily activities. Such as cyclobenzaprine (Flexeril), which might be prescribed to relieve the discomfort associated with muscle spasms. However, these medicines might cause confusion in older people. Depending on the level of pain, prescription pain medicines might be used in the initial period of treatment.
Corticosteroid – to healing the nerve inflammation and clotted blood in the joints. If inflammation is severe, a doctor may also prescribe a steroid. Steroids, such as cortisone, reduce swelling quickly. A cortisone shot directly in the affected area will have an immediate effect on the displaced disc. If a severe radicular component is present, a short course of oral steroids such as prednisone or methylprednisolone can be considered.[rx] Epidural steroid injections, either interlaminar or transforaminal, performed under fluoroscopic guidance can help with severe radicular (leg) pain but lacks conclusive benefit in relieving back pain in lumbar spondylolysis.[rx]
Counter-irritants – such as creams or sprays applied topically stimulate the nerves in the skin to provide feelings of warmth or cold in order to dull the sensation of pain. Topical analgesics reduce inflammation and stimulate blood flow.
Nerve Relaxant — Pregabalin or gabapentin and anti-inflammatory drugs help to relieve pain and stiffness, allowing for increased mobility and exercise.
Epidural Injections – For patients with severe pain, especially leg pain, epidural steroid injections may be a reasonable treatment option. The injections are effective in helping to curb pain and increase a patient’s function in up to 50% of cases. If an epidural steroid injection does work to relieve the patient’s pain, it can be done up to three times per year. The length of time that the lumbar epidural injection can be effective is variable, as the pain relief can last one week or a year.
Epidural steroid injections – An injection of a corticosteroid and a numbing agent is delivered into the epidural space of the spinal canal or nerve root canals to reduce the swelling of the nerves.
Facet injections – An injection of a corticosteroid and a numbing agent is delivered directly into the painful facet joint.
Facet rhizotomy – If facet joint injections relieve your pain, an ablation procedure may be performed to “burn” the small nerves around the facet joint to deaden the pain signals
Surgery
Non-operative management of acute cases among sportspersons was successful in 95% of patients, and only 5% required surgical intervention. Among that treated non-operatively, 82% returned to their previous level of play.[rx] Operative treatment is reserved for those with intractable pain or neurological symptoms, including claudication or radiculopathy.[rx]
Surgical intervention has shown >80% success in appropriately selected patients, with a low incidence of complications. Surgical techniques include the following:
Pedicle screw hook fixation – In the pediatric population with pars fracture or non-union, surgical repair of the pars may be an option with lag screw or tension band wire technique or pedicle screw hook fixation.[rx][rx]
Uninstrumented fusion in situ – A randomized control trial by Moller [rx] showed that there was no advantage in adding instrumentation. Pain, functional disability, and fusion rates were similar in both groups.
Decompression – Though there was some skepticism in just performing decompression of the nerve roots without fusion, i.e Gills procedure, results show 70 % good results with regards to patient satisfaction. Only grade I and II patients met the inclusion criteria for the study.[rx]
Instrumented posterolateral fusion – with decompression is the standard procedure.[rx]
Anterior-posterior transforaminal – and direct lateral lumbosacral interbody fusion, reduction, and fusion.[rx] The anterior, posterior, transforaminal, and direct lateral indicates the path through which the interbody device or cage is inserted. Posterior lumbar interbody fusion (PLIF) involves the insertion of the cage between the vertebral bodies medial to facets. Transforaminal lumbar interbody fusion (TLIF) requires facetectomy and a more lateralized and transforaminal approach to the disc space. Anterior Lumbar Interbody Fusion (ALIF) – is via a trans or retroperitoneal approach and offers better access to disc space and endplate. They can also be associated with retrograde ejaculation and sexual dysfunction. Direct lateral or the transposons approach can only access the disc spaces above the L5 vertebrae. The iliac crest is in the path of reaching the L5/S1 disc on the direct lateral approach.[rx]
Reduction with spondylolectomy – (vertebrectomy) of L5 and fusion of L4 on S1.[rx] In severe slips removing the L5 vertebrae allows reduction and better spinal alignment
Sacral dome resection and fusion.[rx] – Operative options should be considered only if non-operative options fail or symptoms are significant. The reduction of the slip is controversial as in approximately 20% of cases, it causes L5 nerve root injury. Nevertheless, some evidence suggests better functional and cosmetic outcomes for patients who underwent reduction and instrumented fusion.[rx]
Foraminal decompression – may also be necessary. Interbody fusion with the maintenance of intervertebral space improves the foraminal height, helps restore lumbar lordosis, and avoids fusion to L4 in high-grade slips. Each case requires an individual approach, and factors like the degree of spondylolisthesis, predominant neurological symptoms, and patients’ comorbidities should be taken into consideration.[rx] Minimally invasive surgical techniques are gaining in popularity.[rx]
Anterior Lumbar Interbody Fusion (ALIF) – Anterior Lumbar Interbody Fusion is an innovative technique utilized to remove a degenerative disc in your lumbar spine. Using a minimally invasive approach this procedure is done from the front of the spine and creates a solid bridge between at least two vertebrae. The goal of this surgical technique is to alleviate pain, numbness, or tingling caused by a degenerative lumbar disc. You may be a candidate for lumbar fusion once we performed a detailed evaluation confirming that this is the source of your symptoms.
Lateral Interbody Fusion (XLIF, DLIF) – A Direct Lumbar Interbody Fusion (DLIF) or eXtreme Lateral Interbody Fusion (XLIF) is a lumbar fusion procedure from the side or a lateral approach. Typically, this approach is best for patients with spinal abnormalities from the mid to upper lumbar spine as well as the lower thoracic spine. Using a minimally invasive approach, the surgeon will separate the tissue fibers to approach the side of the spine. Once direct visualization is achieved, your surgeon will remove the disc material and place an appropriately sized cage or interbody device with bone graft material into the disc space. By placing an interbody device, realigns the spine and recreates disc space, thereby decompressing nerves. Further stabilization can be achieved through a plate and/or posterior instrumented fusion.
Lumbar Fusion – A fusion is a surgical technique that involves eliminating the motion in between vertebrae by “welding” the bones together. By fusing the bones together, they heal into a single, solid unit. A fusion procedure may be recommended to eliminate painful motion, restore your alignment or posture, or provide stability to your spine. In certain cases, your surgeon may perform a laminectomy in addition to the fusion procedure if you have leg symptoms, such as pain or numbness. Our goal is to identify that your degenerative disc is the cause of your ongoing symptoms. Fusion surgery is one way to treat your symptoms.
Posterior Instrumented Fusion (PIF) – A posterior instrumented fusion involves the placement of screws and rods. This can be done for interbody fusion or for deformity surgery such as scoliosis or kyphosis. With this procedure, innovative technology can be utilized which allows your surgeon to visualize the placement of hardware during the procedure. This provides for increased precision and accuracy of screw placement and less soft tissue cutting.
Posterior Lumbar Interbody Fusion (PLIF) – A Posterior Lumbar Interbody Fusion (PLIF) is a lumbar fusion procedure from the back or posterior approach. During this procedure, your surgeon will make a midline incision in order to expose the posterior spine elements, such as the spinous process, lamina, and facet joints. Bone is removed to create a window to open the spinal canal. This creates access to remove disc material in order to prepare the space for implants to fuse the bones together. Screws and rods are used to stabilize this fusion process.
Transforaminal Lumbar Interbody Fusion (TLIF) – Transforaminal Lumbar Interbody Fusion (TLIF) is a lumbar fusion procedure from the back or posterior approach. During this procedure, your surgeon will make a midline incision in order to expose the posterior spine elements, such as the spinous process, lamina, and facet joints. Once the posterior elements have been exposed, a window is created by removing the facet joint or facetectomy. Then the thecal sac and nerve root are retracted in order to expose the targeted disc space laterally. An incision is made into the annulus of the affected disc. Most of the disc material is removed to provide a bony fusion surface. Once the area is prepped, bone graft material is placed along with an interbody cage or interbody device. Posterior instrumentation is placed in addition to further stabilization and fusion of the spine.
Physical rehabilitation methods
Physiotherapy is the most common method used to apply a non-operative treatment of symptoms associated with DS. Therapeutic protocols may include the use of modalities for pain relief, bracing, exercise, ultrasound, electrical stimulation, and activity modification [rx, rx, rx, rx]. Unfortunately, some of the evidence for the effectiveness of physical rehabilitation methods are coming from case reports [rx, rx] and cannot be generalized to the rest of the population. Physiotherapy treatment is recommended to reduce pain [rx], to restore range of motion and function, and to strengthen and stabilize the spine [rx, rx] and restore mobility of the neural tissue [rx]. However, no study has yet shown their usefulness in patients with DS. Further, we review studies that mostly investigated treatment options for other types of spondylolisthesis, spinal segmental instability, and spinal stenosis in an attempt to understand their rationale and to apply it to the treatment of DS.
Bracing
We did not find any studies that specifically evaluated brace treatment for symptoms associated with DS. Patients treated with the corset showed a statistically significant improvement in walking distance and decrement of pain score in daily activities in comparison with patients who did not wear the corset. Because most patients with symptomatic DS suffer from neurogenic claudication, the use of bracing needs to be examined for the treatment of patients with DS. The other rationale to use bracing in patients with DS is to decrease segmental spinal instability, although it is not the main pain generator in DS. Bell et al. [rx] showed that adolescents with grade I and II isthmic spondylolysis who received brace treatment for 25 months were pain-free and none had demonstrated a significant increase in slip percent. In addition, patients with lateral recess stenosis with impingement of the nerve root can potentially benefit from a brace that prevents rotation.
Flexion/extension strengthening exercises
Those doing flexion and those doing extension back strengthening exercises. All patients received instructions on posture, lifting techniques, and the use of heat for the relief of symptoms. After 3 months, only 27% of patients who were instructed in flexion exercises had moderate or severe pain and only 32% were unable to work or had limited their work. Of the patients who were instructed in extension exercises, 67% had moderate or severe pain and 61% were unable to work or had limited their work.[rx]
Specific muscular and biomechanical impairments have been identified in people with spinal stenosis, including paraspinal muscle denervation [rx] and trunk extensor muscle function [rx]. Such findings suggest that non-surgical physical interventions possibly should include exercises specifically directed toward the spinal extensor muscle group, but taking into account the results of Sinaki et al. [rx] study it should be done with great caution and without an actual extension at the spine (e.g., isometric exercise). There have been no reports in the literature of exercise regimens that have targeted the spinal extensor muscle group in those with spinal stenosis [rx].
Stabilization exercises
O’Sullivan et al. [rx] found that individuals with chronic LBP and a radiological diagnosis of spondylolysis or spondylolisthesis who underwent a 10-week specific exercise treatment program involving the specific training of the deep abdominal muscles, with co-activation of the lumbar multifidus proximal to the pars defects showed a statistically significant reduction in pain intensity and functional disability levels, which was maintained at 30-month follow-up. The control group that received treatment as directed by their treating practitioner showed no significant change in these parameters after intervention or at follow-up. Lindgren et al. [rx] found that exercise therapy in patients with chronic low back pain and segmental instability symptoms can improve strength and electromyographic parameters of paraspinal muscles, but not change the radiographic signs of instability.
Combined treatment
As we mentioned before, symptoms associated with spinal stenosis are the main complaint of patients with DS. Simotas et al. [rx] report on a case series of 49 patients treated non-operatively for spinal stenosis. In addition to pharmacologic intervention that may have included oral analgesics and ESI, the intervention consisted of therapeutic exercise (postural instruction, lumbopelvic mobilization exercises, and a flexion-based exercise program). After 3 years, nine of 49 patients (18%) had surgical intervention. Five patients (10%) reported their condition to be worse, and the remaining 35 patients (71%) either reported no deterioration in their condition or reported improvement (slight or sustained). The authors conclude that aggressive nonoperative treatment for spinal stenosis remains a reasonable option.
Spinal manipulation
Spinal manipulation is an alternative treatment often pursued by patients. No randomized clinical trials of patients with spondylolisthesis or spinal stenosis have been done. We found only one study [rx] that evaluated the effectiveness of spinal manipulative therapy for LBP by comparing two groups of patients: a small group (25) of patients with lumbar spondylolisthesis and a larger group (260) of patients without spondylolisthesis. This study showed that the results of manipulative treatment are not significantly different in patients with or without lumbar spondylolisthesis. Patients may have some short-term pain relief from chiropractic manipulation, but no long term benefit has been proven.
Complications
The most common reported neurological complication after lumbosacral spondylolisthesis surgery is L5 nerve root dysfunction. It is most frequently associated with high-grade slips and attempts of slip reduction as well as of foraminal stenosis decompression. L5 nerve root dysfunction is usually transient and resolves within a few months in the postoperative period. In their cadaveric study, Petraco et al. found out that 71% of total nerve strain occurs during the second half of the reduction.[rx]
Pseudoarthrosis
Dural tear
Neurologic deficits
Pseudoarthrosis
Progression of slippage
Hardware failure
Chronic pain
Lower extremity radicular pain
Muscle wasting
Disability
Spinal deformity
Pulmonary embolism
Adjacent segment disease (2 to 3%)
Surgical site infection (0.1 to 2%)
Positioning neuropathy: Lateral femoral cutaneous nerve – from a prone position with iliac bolster, ulnar nerve or brachial plexopathy with inappropriate arm position)[rx]
Complication rate increases with age, increased intraoperative blood loss, longer operative time, the number of levels fused.
Anti Virus, You’ve come to the right place if you want to finally narrow down the best antivirus for your computer and mobile devices. We’ve tested and reviewed the latest antivirus packages – both free and premium – from the biggest names in cybersecurity, so you can be confident that our recommendations can be trusted.
Creators of malware and viruses are always coming up with new ways to gain access to your PC and other internet-enabled devices (with your mobile phone and tablet included). Luckily online software security companies are constantly updating their security software packages. We’re already starting to see their 2019 packages come to market, with user experience tweaks
Total Protection blocked all the malware samples we used to test antivirus software, which included malicious websites, rootkits, Trojans, viruses and phishing schemes. It gives you in-browser reports about the threats it blocks, which we found more convenient than trying to find this information from the dashboard. These reports include the type of threat blocked and the risk of continuing to the site or downloading the infected content. It also lists the IP addresses connected with the threat, which allows tech-savvy users to avoid websites connected to those addresses.
When viruses tried to download to our computers, McAfee interrupted and tagged them. Even when we tried to resume the download, McAfee again stopped the download and displayed its warning messages. When we persisted, McAfee quickly caught the threats as the downloads completed and move them to the quarantine folder.
Overall this antimalware program wasn’t difficult to set up. It required the same steps and processes as most antivirus software. Links and tabs are clearly labeled, and the most important features, like real-time scanning and automatic updates, are active once the program is installed. We did find it hard to locate the quarantine folder but finally found it after clicking on the Settings icon. Also, while McAfee automatically updates itself, you do have to restart your computer for updates to go into effect.
We had slowdown issues while McAfee scanned our computer for threats. Several times while trying to use the cursor to attach files to email, open programs or navigate software, there was a significant lag, and we often made errant clicks because the computer hadn’t caught up with the cursor. While playing games online there was a noticeable lag that created a lot of distraction and in some games directly affected the outcome because we couldn’t keep control of the cursor. For this reason, we feel it’s better to let McAfee scan your computer when you don’t need to use it. However, if you do
Operating system: Windows only | Maximum devices covered: 1 | Standout features: Ransomware protection and remediation, privacy tools, VPN, Safepay
Accurate
Password manager
Cheap subscription
Can be resource-hungry
In a world packed with free security software, Bitdefender Antivirus Plus 2019’s annual fee may look expensive, but there’s plenty of bang for your buck. Plus, it has reintroduced its mega 60% discount on its top packages – including Antivirus Plus – too. See below for pricing.
Take a look at any rankings of big independent antivirus and Bitdefender’s premium security products always rise to the top.
It tends to be reliable and accurate in its virus detecting, featuring web filtering to blocks access to malicious sites, a secure browser that keeps your online banking ans shopping transactions safe, and there’s a password manager which auto-completes credit card details in web forms. It also scores high for its excellent anti-phishing module, which alerts you to malicious links in your search engine results and blocks access to dangerous sites.
New for the 2019 version of Antivirus Plus are multi-layer ransomware protection that heuristically learns the behaviour of such threats to keep you safe as well as the ability to scan all your linked devices via the Bitdefender Central mobile app.
There are one or two issues – it grabs more resources than average, and might conflict with some programs – but Bitdefender Antivirus Plus 2019 is still a likable package which offers excellent detection rates, great performance, and more than enough bonus features to justify the price.
Bitdefender Internet Security 2019 builds on AVP 2019 and triples the number of devices covered plus offers anti-spam, firewall, parental advisor and file encryption features.
For a little bit more you can purchase the Total Security 2019 edition. It adds all of the above and covers up to five PCs, Macs, Android, and iOS devices.
Operating system: Windows only | Maximum devices covered: 1 | Standout features: Advanced privacy security, financial security, global civilian intelligence network
Blocks even brand new malware
Low impact on system resources
Browser extension extras can be unreliable
Norton AntiVirus Basic is a top quality malware hunter which can automatically protect your PC all on its own – that’s a given. But one of the main reasons we’ve boosted it to number two in our best antivirus rankings is because it’s also one of the very best value paid-for security software options on the market.
Norton offers plenty of tweaks, options and settings for those who need them, as well as features like a handy URL blocker that keeps you away from malicious websites. If that misses something, an excellent file reputation service heuristically recognises suspect downloads immediately. And if malware still finds a way through, intelligent behaviour monitoring uses its up to date virus definitions to quarantine threats at the first sign of trouble.
If you’re a more hands-on type, you can easily run scans on demand. Maybe set up and save custom scans to check just the areas you need. Even schedule them to run at a particular time, but only if your system is idle, and it’s not running on battery power.
There can be problems with some of the browser extensions. The bundled Norton Identity Safe is a capable password manager when it’s running properly, but we’ve found the Chrome version sometimes stops working for no apparent reason. We’ve seen plenty of reviewers reporting similar problems, so there does seem to be a real issue here.
Still, you don’t have to use Identity Safe at all, and Norton AntiVirus Basic’s main functions deliver on all fronts: it’s easy to use, has the configuration options experts need, comes highly rated by the testing labs, and is carefully designed to have the least possible impact on your system performance.
Operating system: Windows and Mac | Maximum devices covered: 1 | Stand out features: Always-on security, identity protection, real-time anti-phishing, firewall monitor
Extremely light on system resources
Lightning fast
No testing data from the top labs
Just about every antivirus tool claims to be ‘lightweight’, but Webroot SecureAnywhere AntiVirus is the only one to really deliver on this front. Installation takes seconds, the program files barely grab 2MB of your hard drive, RAM footprint is tiny, and there are no bulky signature updates to tie up your bandwidth.
There’s no compromise on features, though. Along with the core protection, there’s smart behaviour monitoring, accurate real-time antiphishing, a firewall and network connection monitor, enhanced anti-ransomware, and other interesting extras.
It’s not easy to compare Webroot’s accuracy with the competition, as the big testing labs rarely evaluate the company’s products. But when they are reviewed, they generally score well, and our own tests show solid and reliable protection.
There’s a lot to like about SecureAnywhere AntiVirus, and Webroot’s 70-day 100% money-back guarantee suggests it’s confident in the product, too. If you’re tired of overly complicated and bloated engines, Webroot must be on your shortlist.
Expert-level antivirus for the more experienced user
Operating system: Windows only | Maximum devices covered: 5 | Stand out features: Ransomware Shield, UEFI Scanner, Exploit Blocker, cloud-powered scanning
Highly configurable
Device access control
Relatively expensive
Not for beginners
If you judge antivirus software on the length of its feature list, ESET NOD32 Antivirus 2018 Edition might be a disappointment. There’s no firewall, password manager, file shredder, vulnerability scanner or any of the bundled extras you’ll often find elsewhere.
This doesn’t mean the package is short on power, it’s just more focused on the fundamentals. ESET NOD32 Antivirus 2018 Edition comes with real-time malware protection, some of the best heuristic detection around, an anti-ransomware layer, exploit protection, URL filtering to block malicious websites, and modules to prevent attacks using PowerShell and malicious scripts.
A Device Control module limits the risk of infection from other devices by controlling access to USB sticks, external hard drives, optical storage media, even devices connecting by Bluetooth and FireWire. It’s an unusual extra but could make a difference if others are regularly plugging devices into your PC.
ESET NOD32 Antivirus 2018 Edition isn’t aimed at beginners. The interface is clumsy sometimes, some features are very advanced, and even the Help isn’t always exactly helpful.
Experienced users will appreciate ESET’s power and configurability, though. Above-average protection does a good job of keeping you safe, and a lightweight design ensures the package won’t slow you down.
One of the new features in the 2018 Edition is the UEFI Scanner which protects you from threats that attack your PC before Windows has even started.
ESET Internet Security builds on NOD 32 and triples the number of devices covered plus offers firewall, botnet protection, webcam protection, antispam and more.
Alternatively, you can purchase the ESET Smart Security Premium edition for not much more. It adds all of the above as well as password management and secure data.
Operating system: Windows, Mac, Android, iOS | Maximum devices covered: 3 | Standout features: Browsing and banking protection, Family Rules, ransomware protection
F-Secure Antivirus SAFE is a great collection of antivirus tools, and while it’s a bit more expensive than some of the other programmes on this best of list, the amount of features you get makes the cost worthwhile.
With F-Secure Antivirus SAFE, you get the brilliant antivirus software from F-Secure, along with banking protection for safe online shopping, family safety tools and a device finder that lets you track your lost Android or iOS device, and if needs be remotely lock or delete it as well.
The package typically receives maximum marks for protection from AV-Test, and generally scores highly with AV-Comparatives, too. They also say it can generate significantly more false positives than most of the competition, but how that affects you will vary depending on how you use your computer.
The interface is a major plus. It’s extremely easy to use, lightweight, and for the most part you can just leave the app alone to look after your PC. The program has minimal effect on your system performance, and if you do need to intervene then you can generally solve any issues in a couple of clicks.
In 2018, F-Secure Anti-Virus SAFE remains an appealing package: fast, lightweight, and able to run alongside many other security tools without conflict.
Trustworthy security for beginners and experts alike
Operating system: Windows only | Maximum devices covered: 5 | Stand out features: Automatic scans, drive-by cryptomining infection prevention, simplified security management
One of the best performing security packages
Supremely easy to use
Kaspersky’s full suites are better value
Kaspersky Anti-Virus 2018 is a stripped-back security package which focuses on the core security essentials: web filtering blocks dangerous URLs, an accurate engine detects and removes threats, smart monitoring technologies track and reverse malicious actions, and that’s about it.
Fortunately, what you do get works well. Very, very well. We’ve consistently found Kaspersky to be amongst the best at blocking malware, and removing it from an infected system, plus it’s regularly top-rated at sites like AV-Comparatives.
The program is easy to use, too. A well-designed interface has just the right number of buttons and options – not too basic, but not complicated or intimidating, either – and there are plenty of on-screen instructions to explain how everything works. Even a beginner will be at home right away.
If you just need accurate, reliable and consistent malware protection, Kaspersky Anti-Virus 2018 will serve you well.
Operating system: Windows only | Maximum devices covered: 1 | Stand out features: Ransomware protection, advanced AI learning, email scam safeguarding, Pay Guard
Affordable pricing
Might slow you down
Higher than average false positives
Trend Micro Antivirus+ Security is a capable package that’s simple to use with above average antispam and an effective ‘Folder Shield’ module to block ransomware.
How good is it? The top testing labs all rate it highly for protection, although there’s some disagreement on the details. In particular, AV-Comparatives says it gives a high number of false positives, which could be a real nuisance. But AV-Test reports high levels of accuracy and no issues with false positives at all.
If there’s a problem here, it’s likely to be performance impact. PassMark’s March 2017 Performance report assessed 15 security products on various performance-related benchmarks, and Trend Micro came bottom of the list.
Our experiences with the product are a little more favourable: protection levels appear similar to Bitdefender, false positives are only marginally higher, and it doesn’t slow down our system noticeably more than anything else.
We’d recommending running the trial for its full 30 days before you buy, then, to see if you notice any problems. But if you’re unaffected, its high levels of detection and excellent bonus features make Trend Micro a good choice.
Real-time malware detection, speedy cloud-based scanning, URL filtering to block malicious websites: Panda Antivirus Pro has all the goodies you’d expect from the best antivirus software.
That’s just the start. A simple two-way firewall helps to keep your system secure. An application control system can define exactly what runs on your PC, stopping even some brand new and undiscovered malware. A virtual keyboard helps you enter confidential data without it being intercepted by keyloggers. There’s even a tool to build a bootable USB rescue disc, ready to remove even the most stubborn threats.
Some of these bonus features are relatively basic. The Panda firewall does its job and can make you more secure, for instance, but it doesn’t compete with the standalone firewall competition. Experienced network users will probably want more.
The simplicity does at least keep everything very easy to use. Options are organized in a straightforward Windows 10-like interface, with all the main modules just a click or two away. Even the firewall doesn’t need to know anything more than your current network location: Home, Work or Public Place.
There’s not a lot of Panda test results from the independent labs around right now, but the figures we’ve seen show the company delivers above-average protection, and overall Panda Antivirus Pro does a good job of keeping malware at bay.

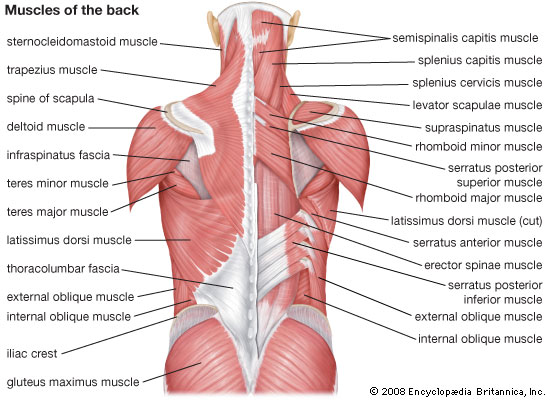
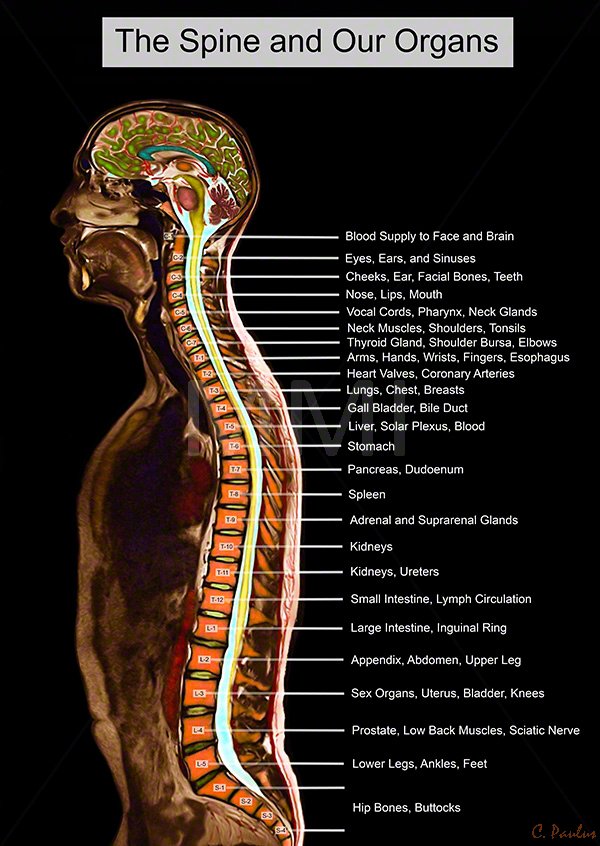









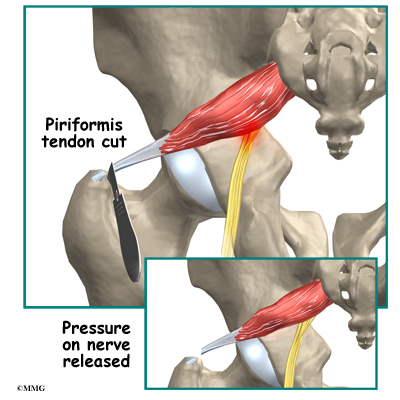

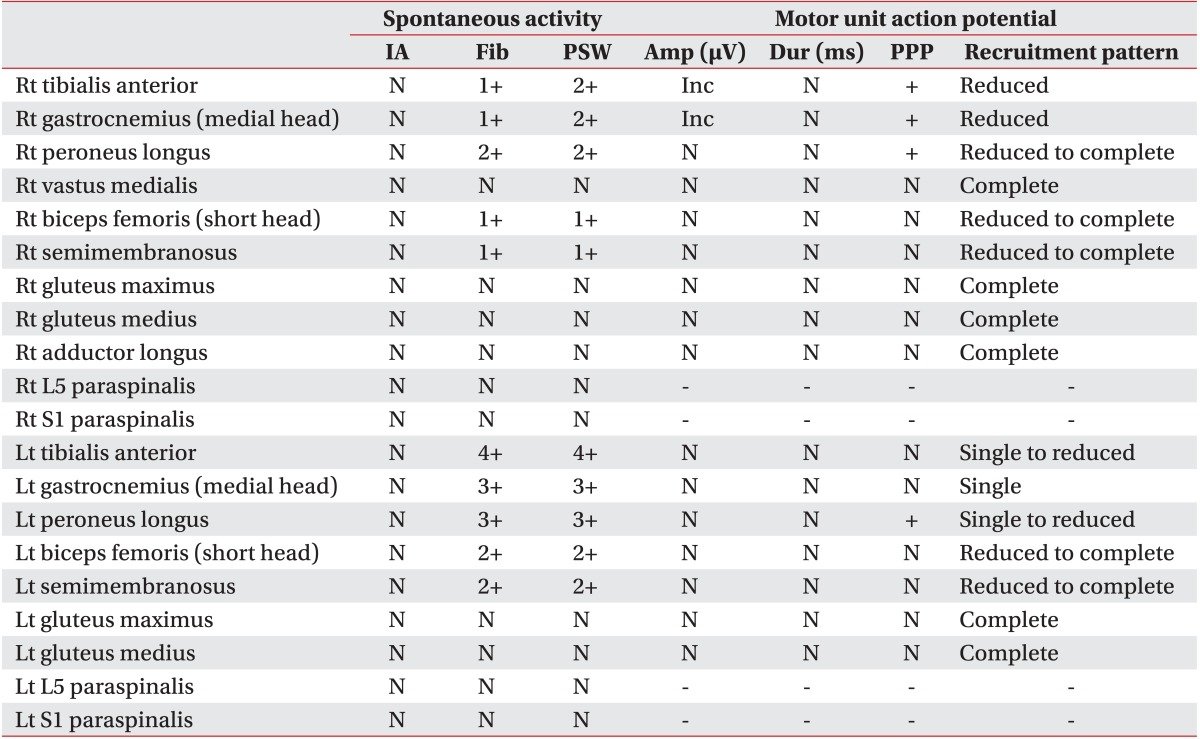




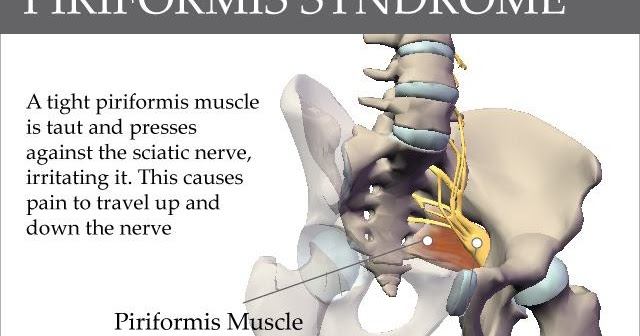

 ,
,

























{kind=link}