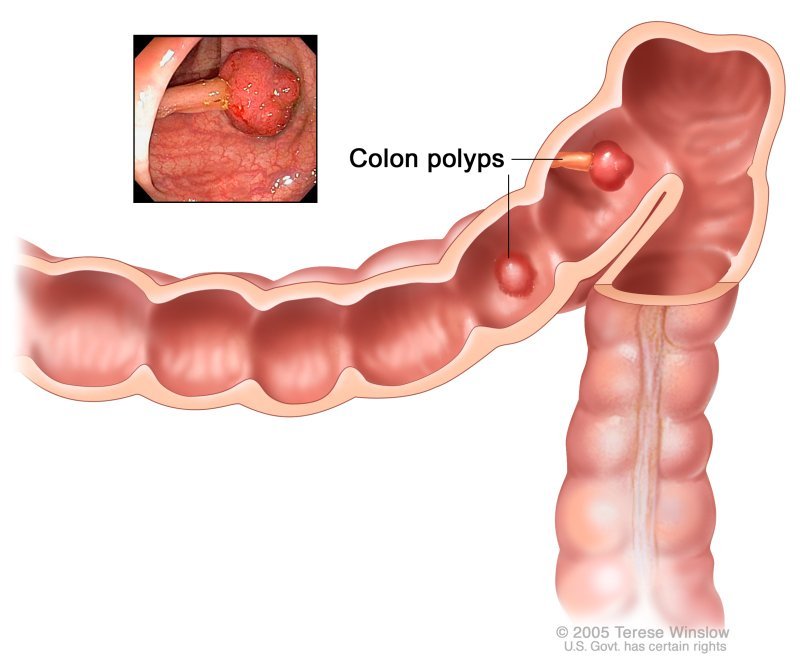
Polyps are abnormal tissue growths that most often look like small, flat bumps or tiny mushroomlike stalks. Most polyps are small and less than half an inch wide. Polyps in the colon are the most common, but it’s also possible to develop polyps in places that include: ear canal. cervix.
Polyp is an abnormal growth of tissue projecting from a mucous membrane. If it is attached to the surface by a narrow elongated stalk, it is said to be pedunculated; if it is attached without a stalk, it is said to be sessile. Polyps are commonly found in the colon, stomach, nose, ear, sinus(es), urinary bladder, and uterus. They may also occur elsewhere in the body where there are mucous membranes, including the cervix, vocal folds, and small intestine. Some polyps are tumors (neoplasms) and others are non-neoplastic, for example, hyperplastic or dysplastic. The neoplastic ones are usually benign, although some can be pre-malignant, or concurrent with a malignancy.
Types of Polyps
Inflammatory polyps (pseudopolyps) – There is a well-defined association between identifying pseudopolyps and the spectrum of inflammatory bowel disease. However, a variety of other infectious and non-infectious colitis, including amoebic, ischemic, and schistosomal colitis might be attributed. The larger lesions with greater than 1.5 cm diameter, classifying as giant pseudopolyps, might present as an extensive polyposis syndrome.[rx]
Familial juvenile polyposis – is inherited via an autosomal dominant pattern. Colon and rectum are most commonly involved. Malignant degeneration through the adenoma and carcinoma transformation is possible. Due to the high malignant yield, annual screening should merit consideration from the age of 10 to 12 years. Although it is an uncommon polyposis syndrome in adults, it has a remarkable significant percentage of polyposis syndrome in the pediatric population.[rx]
Hyperplastic polyps – The colon is most commonly affected by hyperplastic polyps. Although the hyperplastic polyps do not classify as premalignant lesions, due to the similarities with adenomatous polyps in colonoscopy, once diagnosed, they require removal. They may occur as a polyposis syndrome with multiple/ giant polyps harboring a significantly increased risk of malignancy.[rx]
Familial polyposis coli – Familial adenomatous polyposis (FAP) or familial polyposis coli is considered as one of the rare causes of colorectal adenocarcinomas. Specific mutation of APC and positive family history are evident in the majority of patients. There is already an extremely significant value of timely screening and surveillance in positive family and personal history of FAP, respectively. Among those affected with FAP, the risk of colorectal cancer goes way up to 100% by the age of 50.[rx]
Turcot syndrome – Familial colorectal adenocarcinomas, including FAP and HNPCC, may accompany a variety of central nervous system tumors known as Turcot syndrome. Moreover, Turcot syndrome categorizes according to the type of CNS tumor and number of colonic polyps in a couple of subgroups; type I, attributes to the glial tumors and a small number of colonic polyps, while a significant number of polyps and greater risk of medulloblastoma have been well-documented in type II.[rx]
Cowden syndrome and PTEN hamartoma – PTEN acts as a tumor suppressor gene. Cowden syndrome, as an autosomal dominant syndrome and related to PTEN hamartoma tumor syndrome (PHTS), has a broad range of clinical manifestations including trichilemmomas in the face, malignant pathologies in the breast, thyroid, and gastrointestinal polyps. Obtaining timely screening schedules to exclude malignancies in these patients is crucial. Traditionally, there was a remarkable 80% germline PTEN mutation in patients affected by Cowden syndrome; however, recently, the specificity of these criteria has been questioned.[rx]
Peutz-Jeghers syndrome – Peutz-Jeghers syndrome, or mucocutaneous pigmentation and polyposis syndrome, is classified as an autosomal dominant hamartomatous polyposis. Although evidence of the remarkable malignant potential is lacking, stepwise screening plans are generally the recommended approach to evaluate not only the GI tract but also other possible sites for malignancies, including breast, upper gastrointestinal tract, pancreas, cervix, ovaries, and testicles.[rx]
Cronkite-Canada syndrome – Cronkite-Canada syndrome is a rare non-inherited disorder in which patients develop gastrointestinal polyposis in correlation with alopecia, cutaneous pigmentation, and fingernail/toenail atrophy. Diarrhea is a prominent symptom, and malabsorption, vomiting, and protein-losing enteropathy may occur. Most patients die of this disease despite maximal medical therapy, and surgery is only for complications of polyposis such as obstruction. Cowden syndrome is an autosomal dominant disorder with hamartomas of all three of the embryonal cell layers. Facial trichilemmomas, breast cancer, thyroid disease, and gastrointestinal polyps are typical of the syndrome. Patients should have screening for cancers.[25]
Attenuated familial adenomatous polyposis (AFAP) – is a recognized variant of FAP. Patients present later in life with fewer polyps (usually 10–100) predominantly located in the right colon, when compared to classic FAP. Colorectal carcinoma develops in more than 50% of these patients but occurs later (average age, 55 years). Patients are also at risk for duodenal polyposis. However, in contrast to FAP, APC gene mutations are present in only about 30% of patients with AFAP. When present, these mutations express in an autosomal dominant pattern. Mutations in MYH, a gene involved in the repair of DNA, also result in the AFAP phenotype but are expressed in an autosomal recessive pattern.[rx]
Serrated polyps – including sessile serrated adenomas and traditional serrated adenomas, are a recently recognized, histologically distinct group of neoplastic polyps. Endoscopically they are flat lesions and frequently difficult to visualize. These lesions were long thought to be similar to hyperplastic polyps with minimal malignant potential. However, it has become clear that some of these polyps will develop into invasive cancers. Additionally, research has described a familial serrated polyposis syndrome.[rx]
Causes of Polyps
Men and people who smoke have a higher risk for bladder polyps. Women over 40 years of age and women who have had children are more likely to develop polyps in the uterus.
For cervical polyps, the risk increases in women over 20 years or age and women who are premenopausal.
People who habitually stress their vocal cords or have acid reflux have a higher risk for throat polyps. But there are no known risk factors for aural polyps.
Talk to your doctor about your individual risks for polyps if you are concerned about a specific type.
Risks for colon polyps
For colon polyps, the risk factors include:
eating a high-fat, low-fiber diet
being over 50 years of age
having a family history of colon polyps and cancer
using tobacco and alcohol
having an intestinal inflammation disorder like Crohn’s disease
being obese
not getting enough exercise
having type 2 diabetes that isn’t well-managed
African-Americans are also at a higher risk of developing colon polyps.
Risks for stomach polyps
The risk for stomach polyps increases with the following:
age — more common in middle to old age
bacterial stomach infections
familial adenomatous polyposis (FAP), a rare genetic syndrome
regular use of proton pump inhibitors like Nexium, Prilosec, and Protonix
Risks for nasal polyps
Nasal polyps are more likely to develop in people who experience the following conditions:
ongoing sinus infections
allergies
asthma
cystic fibrosis
sensitivity to aspirin
Symptoms of Polyps
Each type of polyp can cause unique symptoms based on location. Below are some common polyp types, their locations, and symptoms.
Type of polyps
Location
Symptoms
aural
ear canal
loss of hearing and blood drainage from the ear
cervical
cervix, where the uterus connects to the vagina
typically no symptoms, but can include bleeding during menstruation (heavier) or sex, or an unusual discharge
colorectal (colon)
large intestine, colon, and rectum
blood in stool, abdominal pain, constipation, diarrhea
nasal
nose or near sinuses
similar to the common cold such as headache, nose pain, loss of smell
hoarse and breathy voice that develops over a few days to several weeks
bladder
bladder lining
blood in urine, painful urination, frequent urination
Most colon polyps are noncancerous and do not often cause symptoms until they are in their later stages. But like gastric polyps, they can develop into cancer.
Diagnosis Of Polyps
Doctors can find colon polyps only by using certain tests or procedures, such as a colonoscopy or imaging study. Your doctor may first take a medical and family history and perform a physical exam to help decide which test or procedure is best for you.
For example, your doctor may ask if you have any symptoms. He or she may also ask if you have a family history of colon polyps or colorectal cancer. After taking a medical and family history, your doctor may perform a physical exam.
Tests and procedures
Flexible sigmoidoscopy – For a flexible sigmoidoscopy, a trained medical professional uses a sigmoidoscope—a flexible, narrow tube with a light and tiny camera on one end—to look inside your rectum and lower colon. Flexible sigmoidoscopy can show irritated or swollen tissue, ulcers, polyps, and cancer.
Colonoscopy – During a colonoscopy, a trained medical professional uses a long, flexible, narrow tube with a light and tiny camera on one end, called a colonoscope, to look inside your rectum and colon. Colonoscopy can show irritated and swollen tissue, ulcers, polyps, and cancer. The most sensitive test for colorectal polyps and cancer. If polyps are found, your doctor may remove them immediately or take tissue samples (biopsies) for analysis.
Virtual colonoscopy – Virtual colonoscopy uses x-rays and a computer to create images of your rectum and colon from outside the body. Virtual colonoscopy can show ulcers, polyps, and cancer. Doctors can’t remove polyps during virtual colonoscopy.
Lower gastrointestinal series – For a lower gastrointestinal (GI) series, a doctor uses x-rays and a chalky liquid called barium to view your large intestine. The barium will make your large intestine easier to see on an x-ray. A lower GI series is also called a barium enema.
Virtual colonoscopy – a minimally invasive test that uses a CT scan to view your colon. Virtual colonoscopy requires the same bowel preparation as a colonoscopy. If a polyp is found, you’ll need a colonoscopy to have it removed.
CT colonography – Also known as a virtual colonoscopy, this uses X-rays and a computer to take pictures of your colon from outside your body. Your doctor can’t take polyps out during this test. If they spot any, you’ll need to have a regular colonoscopy. You’re awake for this test, but you’ll still need to do a special diet to clear out your bowel beforehand.
Flexible sigmoidoscopy – in which a slender, lighted tube is inserted in your rectum to examine it and the last third of your colon (sigmoid) and rectum. If a polyp is found, you’ll need a colonoscopy to have it removed.
Stool-based tests – This type of test works by checking for the presence of blood in the stool or assessing your stool DNA. If your stool test is positive you will need a colonoscopy.
Fecal occult blood testing – (FOBT) may indicate bleeding from a colonic polyp. A positive FOBT due to bleeding from a polyp correlates to the polyp size and proximity to the rectum. Most small polyps will fail to result in a positive FOBT, although the test has a higher sensitivity for larger polyps and for carcinomas. For this reason, FOBT is a part of the screening algorithm for the early detection of colon cancer, despite its poor sensitivity for polyps.
Fecal immunochemical testing – (FIT or iFOBT) is a newer, more sensitive screening method than the traditional FOBT. It utilizes specific antibodies to the globin component of the hemoglobin. A recent study compared FIT against colonoscopy as a screening tool for both colorectal cancer and adenomas [rx].
Colonoscopic spectroscopy – using near-infrared autofluorescence (NIR AF) was recently proposed as an adjunct for in vivo diagnosis of colonic ‘pre-cancer and cancer during clinical colonoscopic screening. This method was found to have a sensitivity and specificity of approximately 80% and 90%, respectively, for the classification of benign, pre-cancer lesions and cancer in the colon [rx]. This method, although promising, is still experimental and is not routinely used in clinical practice.
Narrow-band imaging – (NBI) is another new endoscopic imaging technique that highlights surface structures and superficial mucosal capillaries during colonoscopy. Even though disagreement exists regarding its effectiveness in increasing the colonoscopic view’s sensitivity, it has recently been shown to have a high sensitivity and specificity for differentiating neoplastic and non-neoplastic polyps [rx, rx]. This modality has also not entered routine clinical practice.
Computed tomographic colonography – (also called ‘CT colonography’ or ‘virtual colonoscopy’) is another screening modality, which is suggested for patients who refuse colonoscopy. This modality uses computed tomography of an air-distended prepared colon. With an optimal colon preparation and an experienced radiologist reading the images, some reports indicate that the sensitivity of CT colonography for detecting polyps larger than 5 mm (which are believed to be clinically significant) exceeds 90% [rx, rx]
Magnetic resonance colonography – (MRC) is another diagnostic modality that is currently being evaluated. The rationale for using MRC is based on the relatively high radiation exposure during CT colonography [rx]. A recent small-scale study has demonstrated a low sensitivity (despite a high specificity) for detecting large (>10 mm) polyps using MRC [rx]. Therefore, the evidence does not support MRC as a standard diagnostic modality for detecting colorectal polyps and this modality is not routinely used in clinical practice.
Capsule endoscopy – is a diagnostic modality that was originally developed to diagnose and evaluate small bowel lesions. Since the capsule passes through the prepared colon after traversing the ileocecal valve and continues to transmit images, it can also detect colonic lesions. A large cohort with suspected colonic lesions underwent a capsule endoscopy with a dual camera capsule designed especially to evaluate the colon (PILLcam colon) and, immediately afterward, had a colonoscopy. The sensitivity and specificity of the capsule endoscopy were shown to be inferior to colonoscopy [rx].
Fecal DNA and antigen testing – is another futuristic modality expected to yield results within the next few decades [rx]. Several technical advances have recently been seen to increase its accuracy, including the use of a DNA preservative buffer with stool collection, DNA amplification methods, and automated assays of several DNA markers [rx]. The stool was analyzed with an automated multi-target stool DNA assay to measure β-actin, mutant KRAS, aberrantly methylated BMP3 and NDRG4, and fecal hemoglobin.
Stool DNA analysis – identified individuals with colorectal cancer with 98% sensitivity and 90% specificity. Its sensitivity in respect of advanced adenomas was 57% and for high-grade dysplasia, it was 83% [rx]. In the future, should this modality prove to have even a higher positive predictive value for detecting adenoma or carcinoma, it might obviate the need for any invasive screening tests.
Second Examination
If no polyps are found on the first examination it is recommended that a second examination should be done 10 years later.
If the only polyps that are found are hyperplastic polyps, and they are limited to the rectum and sigmoid colon and they are all less than one centimeter in size, a second examination is recommended in 10 years.
If one or two tubular adenomas are found and they are less than one centimeter in size, a second examination is recommended in five years through a longer interval may be reasonable as well.
If three to ten adenomas are found, it is recommended that a second examination be done in three years.
If more than ten adenomas are found, it is recommended that a second examination be done in three years or less.
If one or more tubular adenomas are found that are greater than one centimeter in size, a second examination is recommended in three years.
If one or more adenomas are found of any size and their histology is villous, a second examination is recommended in three years.
If one or more adenomas are found and any show high-grade dysplasia, a second examination is recommended in three years.
If serrated polyps are found, recommendations are less secure because much less information is available about the future risk of polyps and cancers. Concerns are greater (and the interval to the next examination should be shorter) if the polyps are proximal (in the ascending colon), are larger (more than one centimeter in size), and particularly if they show dysplasia.
Treatment For Colonic Polyps
Doctors treat colon polyps by removing them.
In most cases, doctors use special tools during a colonoscopy or flexible sigmoidoscopy to remove colon polyps. After doctors remove the polyp, they send it for testing to check for cancer. A pathologist will review the test results and send a report to your doctor. Doctors can remove almost all polyps without surgery.
If you have colon polyps, your doctor will ask you to get tested regularly in the future because you have a higher chance of developing more polyps.
Your doctor is likely to remove all polyps discovered during a bowel examination.
Eat less meat – Eat a healthy diet, with minimal red meat—especially processed or cured meats. Studies suggest that people with meat-rich diets tend to have higher rates of colon cancer.
antioxidants– Several associations have been explored for antioxidants including selenium, beta carotene, and vitamins A, C, and E. Most of the studies that have been done do not support a role for these agents in preventing polyps or in preventing colon cancer. A limited amount of support is available for the use of selenium to prevent polyps, but selenium is not recommended for use outside of experimental trials.
Supplemental dietary calcium – has been demonstrated in one study to prevent the formation of polyps. The benefit was seen with supplementation of 1200 mg of calcium per day. There is some concern about using calcium since higher dietary and supplemental levels are associated with an increase in vascular disease. The intake of calcium that was studied was higher than the recommended intake of calcium, 800 mg per day.
NSAIDs – The best support for a treatment to prevent polyps is with nonsteroidal anti-inflammatory drugs (NSAIDs), a class of drugs that includes aspirin, ibuprofen (Motrin, Advil), celecoxib (Celebrex), and many others. Aspirin has been shown in several studies to reduce the formation of polyps by 30% to 50%. The effect is likely to occur with higher doses of aspirin (more than the 81-325 mg that is recommended for cardiovascular disease prevention), and there is concern about aspirin’s side effect of gastrointestinal bleeding at these doses.
Celecoxib (Celebrex), a “COX-2 selective NSAID” – or Cox-2 inhibitor has been shown to reduce colon polyps 30% to 50% as well, but there is a lingering concern about the possible cardiovascular side effects that may be seen with most NSAIDs (though the data supporting this side effect is conflicting). It may be used in patients with genetic polyposis syndromes who choose not to have their colons removed. Celecoxib might be considered in patients with a low risk for cardiovascular disease who develop adenomatous polyps frequently.
Sulindac (Clinoril) – a “non-selective NSAID” has been shown to prevent polyps in patients with sporadic adenoma as well as genetic syndromes. As with celecoxib, there is concern about cardiovascular side effects and gastrointestinal ulceration and bleeding.
Aspirin – Taking a low dose of aspirin every day for a long period of time may help prevent polyps from developing into colorectal cancer in some people. However, taking aspirin daily may cause side effects such as bleeding in your stomach or intestines. Talk with your doctor before you start taking aspirin daily.
Some types of colon polyp are far likelier to become malignant than are others. But a doctor who specializes in analyzing tissue samples (pathologist) usually must examine polyp tissue under a microscope to determine whether it’s potentially cancerous.
Surgery
Removal with forceps or a wire loop (polypectomy) – If a polyp is larger than 0.4 inches (about 1 centimeter), a liquid may be injected under it to lift and isolate the polyp from surrounding tissue so that it can be removed.
Minimally invasive surgery – Polyps that are too large or that can’t be removed safely during screening are usually removed laparoscopically, which is performed by inserting an instrument called a laparoscope into the bowel.
Colon and rectum removal – If you have a rare inherited syndrome, such as FAP, you may need surgery to remove your colon and rectum (total proctocolectomy).
Laparoscopy – During a laparoscopy, the doctor will make a small incision into the abdomen or pelvis and insert an instrument called a laparoscope into the bowel. They use this technique to remove polyps that are too large or cannot be removed safely by colonoscopy.
Removing the colon and rectum – This procedure, known as a total proctocolectomy, is only necessary when a person has a severe condition or cancer. Doctors recommend this option for those with rare inherited conditions, such as familial adenomatous polyposis (FAP). FAP is an inherited condition that causes cancer of the colon and rectum, and polyp removal may prevent cancer from developing.
Colon cancer screening can detect polyps and early cancers in the large intestine. This type of screening can find problems that can be treated before cancer develops or spreads. Regular screenings may reduce the risk for death and complications caused by colorectal cancer.
Regular screening, beginning at age 50, is the key to preventing colorectal cancer and finding it early. The U.S. Preventive Services Task Force (USPSTF) recommends external icon that adults age 50 to 75 be screened for colorectal cancer. The Task Force recommends that adults age 76 to 85 ask their doctor if they should be screened.
The Task Force recommends several colorectal cancer screening strategies, including stool tests, flexible sigmoidoscopy, colonoscopy, and CT colonography (virtual colonoscopy).
Alternative Names
Screening for colon cancer; Colonoscopy – screening; Sigmoidoscopy – screening; Virtual colonoscopy – screening; Fecal immunochemical test; Stool DNA test; cDNA test; Colorectal cancer – screening; Rectal cancer – screening
Pathogenesis of Colon Cancer Screening
Most CRCs begin as protuberances tethered to the inner surface of the colon or rectum, clinically knows as “polyps.” These are mainly of two types: flat or raised, relative to the inner-epithelial lining.
Raised polyps show two distinctive growth patterns of mushroomed growth:
With a stalk (pedunculated polyps)
Without a stalk (sessile polyps)
About 10 percent of CRC patients carry one or more pathogenic “non-Lynch syndrome mutations,” including mutations in high-penetrance genes such as APC, bi-allelic MUTYH, BRCA1, BRCA2, PALB2, CDKN2A, and TP53.[rx]
Right-sided CRCs tend to be diagnosed in advanced stages compared to left-sided, as the cecum and right colon have a larger caliber, and stool is more liquid, causing symptoms of partial obstruction such as pain, swelling, and constipation. Blood in stools (hematochezia or melena) isn’t readily observed and comes much later as compared to the left side, making screening tools pivotal in management for early detection and therapy.[rx][rx]
Risk factors for CRC and Colon cancer screening
Risk factor assessment helps to categorize the patient as high, average, or low-risk. Aggressive multiple interval-based testing starts as early as the teenage years[rx] in patients with a positive family history or co-existing genetic cancer syndromes. A relaxed approach towards screening and further management can be seen in the majority of cases that are at average risk.[rx]
1.) Family history (especially first degree relatives)
Colorectal carcinoma
Pre-cancerous adenomas
2.) Genetic cancer syndromes
Familial adenomatous polyposis (FAP and its variants Gardner and Turcot syndrome)
Lynch syndrome
Hereditary non-polyposis colorectal cancer (HNPCC)
Peutz-Jeghers syndrome
Juvenile polyposis
3.) Medical history
Previously resected or diagnosed adenomatous colorectal polyps; or any of the above mentioned genetic-cancer syndromes
Poor diet (low fiber; high amounts of red and processed meat consumption)
5.) Race
Higher incidence and mortality among African-Americans, particularly men. CRC occurrence is higher in African-Americans less than 50 years of age, hence earlier screening, starting from age 45 years, is recommended by USPSTF.[rx]
Clinical Significance of Colon Cancer Screening
Screening Tools
The various modalities for early detection of CRCs are as follows:
Stool-based Tests
Fecal immuno-chemical test (FIT)
Guaiac fecal occult blood test (gFOBT), also known as HSgFOBT (high-sensitivity guaiac-based fecal occult blood test)
Stool DNA test (FIT-DNA): also known as MT-sDNA test (Multi-targeted-stool DNA test)
Visualization-based Tests
Sigmoidoscopy
Colonoscopy
Optical- standard
Virtual- Radiological: CTC and Capsule colonoscopy.
Barium enema
Blood-based Test
Methylated SEPT-9
Age to Initiate Screening
The U.S. Preventive Services Task Force (USPSTF) and many other expert councils recommend 50 years of age to initiate screening for average-risk patients. In African-Americans, it can be lowered to 45 years of age due to high early-onset incidence.[1] For those with high-risk attributes (positive family history or cancer syndromes), screening can be initiated from as early as the teenage years.[9] Screening for those with a positive family history is recommended to start 10 years before the age of diagnosis of the family member. USPSTF doesn’t recommend routine CRC screening in adults 86 years and older.
Contraindications for Screening
Contraindications might vary depending upon the screening method. Most stool-based tests can be carried out easily. However, other screening methods involve sedation, consumption of contrast, and further instrumentation of the colon. Bowel preparation is a vital pre-requisite, using either a laxative or non-laxative method. The type of bowel preparation should be determined based on the patient’s medical conditions. Colonoscopy should generally be avoided if there is a concern for bowel perforation. Care should be taken for the following conditions:
Active colonic inflammation (e.g., acute diarrhea, active inflammatory bowel disease)
Recent deep endoscopic biopsy/polypectomy/mucosectomy
Known or suspected colonic perforation
Symptomatic or high-grade bowel obstruction
The patient is unwilling to give consent
The patient is uncooperative or unable to achieve sedation
Risk of colonic perforation in patients undergoing colonoscopies such as those with toxic mega-colon and fulminant colitis[rx]
Other contraindications limited to colonoscopy include- inadequate bowel preparation, recent myocardial infarction, arrhythmias, or medically unstable patients.
Evidence of Effectiveness of Various Screening Tests:
1.) Guaiac FOBT (gFOBT) vs. Fecal Immune-chemical Test (FIT)
Evidence of Effectiveness
FIT is more sensitive than gFOBT for colon lesions.[rx]
High-sensitivity gFOBT has a sensitivity of 62% to 79% and a specificity of 87% to 96% for detecting colorectal cancer.[rx]
FIT has a sensitivity of 79% to 88% and a specificity of 91% to 93%.
Evidence suggests a decline in the mortality rate by 15% to 33% when gFOBT/FIT is performed every 1- 2 years in people aged 50 to 80 years.[rx]
FIT has high sensitivity (80%) for detecting CRC, while only 25% to 56% sensitivity for detecting advanced adenomas.[rx][rx]
2.) Stool DNA Test
Evidence of Effectiveness
Its sensitivity and specificity were 92% to 95% and 84% to 95%, respectively. Its sensitivity to detect advanced precancerous lesions such as advanced adenomas and sessile serrated polyps measuring less than 1 cm was 42% and its specificity to detect “all nonadvanced findings,” including non-neoplastic findings, was 87%.[rx]
It displays a higher sensitivity than FIT, (92% vs. 74%) with more false positives. However, it detected less than half of advanced adenomas (42%), limiting its preventive role, due to its low specificity (87% to 90%).[rx]
No evidence of mortality reduction currently exists.
3.) Sigmoidoscopy
Evidence of Effectiveness
Evidence suggests that regular screening with sigmoidoscopy alone after 50 years of age (55 to 64 years) significantly lowers mortality related to rectal or lower colonic cancer by 60% to 70%.[rx][rx]
There is a reduction of CRC incidence by 33 to 42 percent through various randomized controlled trials.[rx][rx]
4.) Colonoscopy
Evidence of Effectiveness
Reduction in CRC incidence and mortality was 31% and 46%, respectively, as established by six observational studies, which further suggested strong evidence of a reduction in incidence and mortality of both distal and proximal colorectal cancers. Sigmoidoscopy only helps in curtailing distal CRC-related mortality and incidence.[rx]
Colonoscopy is very effective in preventing left-sided CRC than right-sided CRCs, which could also contribute to a shift in the distribution of cancers in the colon.[rx]
The sensitivity of colonoscopy after bowel preparation to detect adenomas 6 mm or larger ranged from 75% to 93%, and specificity ranged from 89% to 91%.[rx]
For adenomatous polyps 6 mm or larger, a systematic review reported the sensitivity of colonoscopy for detection varied from 75 percent to 93 percent. The miss rate for polyps of any size was 22 percent, with rates increasing inversely with the size of the lesion. Adenomas smaller than 5 mm were missed in as many as 25% of patients.[rx][rx]
5.) Colon Capsule Endoscopy
Evidence of Effectiveness
Studies showed that in asymptomatic patients using high-quality optic colonoscopy as the standard, capsule endoscopy identified subjects with more than one adenoma of greater than or equal to 6 mm with a sensitivity of 88 percent and specificity 82 percent, and even higher rates in larger adenomas.[rx]
6.) Computed Tomography Colonography
Evidence of Effectiveness
Even though it’s a sophisticated modality when compared to colonoscopy, multiple studies demonstrate a fluctuating sensitivity for CRC lesions, between 67 and 94 percent, while colonoscopy is 92% sensitive. However, CT colonography (CTC) has a very high specificity at 96 to 98 percent.[rx]
Patients who underwent both colonoscopy and CTC saw a surge of 14 to 15 non-rectal neoplasms, missed by colonoscopy, which was located on mucosal folds.[rx][rx]
It can still miss some flattened and small polyps (less than 8 mm).[rx]
7.) Methylated SEPT-9
Evidence of effectiveness
It can detect advanced CRC; however, relevance in early-stage detection is yet to be established. The methylated SEPT-9 DNA assay has a sensitivity for CRC of 75 percent and specificity of 87 percent, with increasing detection rates in advanced cancers.[rx]
Due to poor sensitivity, its role as a primary screening tool is questionable. It also has a false positive rate of 4.7 percent.[rx][rx]
There is no evidence yet that this test can reduce CRC deaths. However, as a non-invasive testing option, it can have significantly increased compliance and participation among high-risk groups.[rx]
Screening Protocols and Algorithms (Image 1)
1.) Fecal Occult Blood Test
Since polyps and CRCs have a high propensity to bleed, FOBT can detect occult blood.[rx]
Sample collection: The patient is given a stool collection kit or asked to get one from the pharmacy (as per local protocols) and is asked to bring in stool samples (sometimes by mail) within 24 hours of collection, as sensitivity to test declines proportionally to delay.[rx][rx]
Sample processing: Don’t rehydrate samples, as it may falsely increase sensitivity, leading to an increased number of false positives.[rx]
Guaiac FOBT (gFOBT)
Consists of guaiac as the main reagent derived from a plant that exclusively grows in the Caribbean. It detects organic heme by oxidation. Therefore, the presence of dietary heme from red meat, peroxidase from some plants, and anti-oxidants like vitamin C or E can lead to false positives. Fasting is advised before the test.
Fecal Immune-Chemical Test (FIT)
Employs antibodies to specifically detect human heme-based globin. Dietary and medication restrictions prior to tests aren’t required. The test is very specific for detecting colonic/rectal bleeding.
Advantages
Bowel preparation isn’t a prerequisite.
Dietary or medication restrictions aren’t a prerequisite for FIT.
Samples can be collected at home, hence convenience and higher adherence.[rx]
Cost-effective compared to other CRC screening tests.
There is no risk of damage to the colon.
Disadvantages
The test does not detect some polyps and cancers.
False-positive test results are possible.
Dietary restrictions are needed before guaiac FOBT.
Additional procedures, such as colonoscopy, may be needed if results are positive.
2.) Stool DNA Test
Also known as the FIT-DNA test, it comes as an FDA-approved kit. It’s a multi-target test that detects occult blood along with nine DNA biomarkers of three genes associated with CRC and advanced adenoma.[rx][rx]
Sample collection: Like FOBTs, the patient is provided a stool collection kit and asked to collect a stool sample, which can be delivered via mail or can be delivered personally to a laboratory/office, ideally within 72 hours.
Advantages
No bowel preparation is required.
No dietary or medication restrictions as a pre-requisite.
Samples can be collected at home, hence convenience and high adherence.
No risk of damage to the colon.
Disadvantages
More expensive than gFOBT or FIT.
Test sensitivity for adenomas is low.
False-positive test results can be seen.
Additional procedures, such as colonoscopy is advised if results are positive.
3.) Sigmoidoscopy
Examination of the rectum and sigmoid colon using a sigmoidoscope, an instrument consisting of a flexible tube with a lens and light source for visualization and a tool for removing tissues (polyp/adenoma) or taking biopsy samples.
The sigmoidoscope is inserted through the anus up to the splenic flexure, after insufflating carbon dioxide for better visualization.
Advantages
Minimal discomfort and complications are rare.
Biopsy and polypectomy (removal of a polyp or adenoma) can be performed during the same procedure.
Less extensive cleansing of the colon is required than for colonoscopy, as it only probes the sigmoid colon.
Disadvantages
Pre-cancerous or CRC lesions in the right colon will be missed due to limited visualization.
Bowel preparation by either enema or laxatives is a prerequisite.
Medication and diet changes may be needed before the test.
Small risk of bleeding or perforation of the colon lining.
Additional procedures, such as colonoscopy, may be needed to detect synchronous lesions.
4.) Colonoscopy
A colonoscope is inserted through the anus and through the entire colon ending in the cecum.
Abnormal growths can be visualized and can be either removed (polypectomy) in whole, or a small sample can be taken for biopsy in a single procedure.
Since the procedure is more invasive than sigmoidoscopy, it requires rigorous bowel preparation and dietary modifications.[rx]
Advantages
One of the most sensitive and definitive methods (gold standard) currently available for the detection of both pre-cancerous adenomas and CRC.
It allows for the best visualization of the cecum and the entire colon, unlike sigmoidoscopy.
Biopsy and polypectomy can be done in a single procedure.
Disadvantages
Even though this test is highly sensitive, it still may not detect all small or sessile polyps and cancers.
Thorough cleansing of the colon is a prerequisite.
Diet and medication modifications are prerequisites.
Some form of sedation is almost always used. Hence, the patient must have someone to accompany them. Rest and avoiding any work is advised after the procedure.
Small risk of bleeding or perforation of the colon; this risk increases with age, with the presence of other health problems, and when polyps are removed.[rx]
5.) Colon Capsule Endoscopy
Approved by the US Food and Drug Administration (FDA) to be used only in patients who had an incomplete colonoscopy. The patient swallows a capsule containing tiny wireless cameras that take images as the capsule traverses the colon.
Advantages
Colon capsule endoscopy requires bowel preparation; however, it does not require sedation or dietary or medication adjustments.
Disadvantages
It doesn’t accommodate polypectomy or biopsy and is only meant for lesion visualization. This test appears to have a sensitivity and specificity, similar to colonoscopy. However, it is not indicated as a primary screening tool.
6.) Computed Tomography Colonography
The procedure isn’t invasive and doesn’t require sedation. However, bowel preparation and carbon dioxide insufflation are still needed for better visualization.
It may additionally require an intravenous catheter for glucagon administration for bowel relaxation. Images are then obtained during a single 32-second breath-hold.[rx]
Advantages
A minimally invasive procedure, hence little to no risk of damage to the colon.
No sedation is required.
Disadvantages
Thorough cleansing of the colon is a prerequisite.
It can miss small polyps.
Additional procedures, such as standard colonoscopy is advised should CTC come back positive for lesions.
It exposes an already at-risk patient to ionizing radiation and discomfort of contrast with possible allergy.
7.) Fecal Tagging
It’s a laxative-free CTC approach, done by oral administration of a contrast agent over several days before the procedure, making fecal material in the colon distinct from colon tissue by “tagging” it.
Radiographs of the colon are then obtained.
Sensitivity is somewhat lower than conventional CTC with laxative bowel preparation.[rx]
8.) Barium Enema
Either single or double-contrast is rarely used, and neither is recommended by any other expert group, due to its poor screening indices and because of the advent of better endoscopic and CTC procedures with better results.
Screening Frequencies and Ideal Intervals for Surveillance and Follow-up (Image 2)
1.) Guaiac FOBT (gFOBT) & Fecal Immune-chemical Test (FIT)
Frequency of testing: Experts recommend sigmoidoscopy every 5 years for people at average risk who have had negative test results.[rx]
2.) Stool DNA Test
Frequency of testing: The current recommendation is once every three years. If positive on any of the occasions, endoscopic studies such as colonoscopy and sigmoidoscopy are recommended.[rx]
3.) Sigmoidoscopy
Screening frequency: Sigmoidoscopy should be performed at five-year intervals from baseline intervention, with gFOBT/FIT every three years.[rx][rx]
3.) Colonoscopy
Screening frequency: Patients undergoing colonoscopy should have a 10-year interval between screening colonoscopies if the examination is negative and of adequate quality.[rx][rx]
4.) Computed Tomography Colonography
Screening frequency – Current USPSTF recommends CTCevery five years from baseline CTC or optical colonoscopy.
Disease conditions associate with Colon Cancer Screening
Inflammatory polyps (pseudopolyps) – There is a well-defined association between identifying pseudopolyps and the spectrum of inflammatory bowel disease. However, a variety of other infectious and non-infectious colitis, including amoebic, ischemic, and schistosomal colitis might be attributed. The larger lesions with greater than 1.5 cm diameter, classifying as giant pseudopolyps, might present as an extensive polyposis syndrome.[rx]
Familial juvenile polyposis – is inherited via an autosomal dominant pattern. Colon and rectum are most commonly involved. Malignant degeneration through the adenoma and carcinoma transformation is possible. Due to the high malignant yield, annual screening should merit consideration from the age of 10 to 12 years. Although it is an uncommon polyposis syndrome in adults, it has a remarkable significant percentage of polyposis syndrome in the pediatric population.[rx]
Hyperplastic polyps – The colon is most commonly affected by hyperplastic polyps. Although the hyperplastic polyps do not classify as premalignant lesions, due to the similarities with adenomatous polyps in colonoscopy, once diagnosed, they require removal. They may occur as a polyposis syndrome with multiple/ giant polyps harboring a significantly increased risk of malignancy.[rx]
Familial polyposis coli – Familial adenomatous polyposis (FAP) or familial polyposis coli is considered as one of the rare causes of colorectal adenocarcinomas. Specific mutation of APC and positive family history are evident in the majority of patients. There is already an extremely significant value of timely screening and surveillance in positive family and personal history of FAP, respectively. Among those affected with FAP, the risk of colorectal cancer goes way up to 100% by the age of 50.[rx]
Turcot syndrome – Familial colorectal adenocarcinomas, including FAP and HNPCC, may accompany with a variety of central nervous system tumors known as Turcot syndrome. Moreover, Turcot syndrome categorizes according to the type of CNS tumor and number of colonic polyps in a couple of subgroups; type I, attributes to the glial tumors and a small number of colonic polyps, while a significant number of polyps and greater risk of medulloblastoma have been well-documented in type II.[rx]
Cowden syndrome and PTEN hamartoma – PTEN acts as a tumor suppressor gene. Cowden syndrome, as an autosomal dominant syndrome and related to PTEN hamartoma tumor syndrome (PHTS), has a broad range of clinical manifestations including trichilemmomas in the face, malignant pathologies in the breast, thyroid, and gastrointestinal polyps. Obtaining timely screening schedules to exclude malignancies in these patients is crucial. Traditionally, there was a remarkable 80% germline PTEN mutation in patients affected by Cowden syndrome; however, recently, the specificity of these criteria has been questioned.[rx]
Peutz-Jeghers syndrome – Peutz-Jeghers syndrome, or mucocutaneous pigmentation and polyposis syndrome, is classified as an autosomal dominant hamartomatous polyposis. Although evidence of the remarkable malignant potential is lacking, stepwise screening plans are generally the recommended approach to evaluate not only the GI tract but also other possible sites for malignancies, including breast, upper gastrointestinal tract, pancreas, cervix, ovaries, and testicles.[rx]
Cronkite-Canada syndrome – Cronkite-Canada syndrome is a rare non-inherited disorder in which patients develop gastrointestinal polyposis in correlation with alopecia, cutaneous pigmentation, and fingernail/toenail atrophy. Diarrhea is a prominent symptom, and malabsorption, vomiting, and protein-losing enteropathy may occur. Most patients die of this disease despite maximal medical therapy, and surgery is only for complications of polyposis such as obstruction. Cowden syndrome is an autosomal dominant disorder with hamartomas of all three of the embryonal cell layers. Facial trichilemmomas, breast cancer, thyroid disease, and gastrointestinal polyps are typical of the syndrome. Patients should have screening for cancers.[25]
Attenuated familial adenomatous polyposis (AFAP) – is a recognized variant of FAP. Patients present later in life with fewer polyps (usually 10–100) predominantly located in the right colon, when compared to classic FAP. Colorectal carcinoma develops in more than 50% of these patients but occurs later (average age, 55 years). Patients are also at risk for duodenal polyposis. However, in contrast to FAP, APC gene mutations are present in only about 30% of patients with AFAP. When present, these mutations express in an autosomal dominant pattern. Mutations in MYH, a gene involved in the repair of DNA, also result in the AFAP phenotype but are expressed in an autosomal recessive pattern.[rx]
Serrated polyps – including sessile serrated adenomas and traditional serrated adenomas, are a recently recognized, histologically distinct group of neoplastic polyps. Endoscopically they are flat lesions and frequently difficult to visualize. These lesions were long thought to be similar to hyperplastic polyps with minimal malignant potential. However, it has become clear that some of these polyps will develop into invasive cancers. Additionally, research has described a familial serrated polyposis syndrome.[rx]
Colonic Polyps /Colon polyps also known as colorectal polyps are their macroscopic appearance as sessile (flat, arising directly from the mucosal layer) or pedunculated (extending from the mucosa through a fibrovascular stalk) growths on the lining of your colon and rectum. You can have more than one colon polyp. Colon polyps are protrusions occurring in the colon lumen most commonly sporadic or as part of other syndromes. Polyps are classified as diminutive if 5 mm in diameter or less, small if 6 to 9 mm, or large if they are 1 cm in diameter or more. Polyps can be depressed, flat, sessile or pedunculated. Few polyps arise from submucosa including lipomas, carcinoids, or lymphoid aggregates. Most commonly, however, they result from the mucosa, and they can be adenomatous, serrated, or non-neoplastic.
Types of colonic polyps
Polyps in the colon can vary in size and number. There are 5 types of colon polyps
Hyperplastic polyps – are harmless and don’t develop into cancer.
Adenomatous polyps – are the most common. Although most will never develop into cancer, they do have the potential to become colon cancer.
Malignant polyps – are polyps that are noted under microscopic examination to have cancer cells in them.
Adenomas – Two-thirds of colon polyps are the precancerous type, called adenomas. It can take seven to 10 or more years for an adenoma to evolve into cancer—if it ever does. Overall, only 5% of adenomas progress to cancer, but your individual risk is hard to predict. Doctors remove all the adenomas they find
Sessile serrated polyps – Once thought harmless, this type of adenoma is now known to be risky. These are also removed.
Causes of Colonic Polyps
Hereditary disorders that cause colon polyps include:
Lynch syndrome – also called hereditary nonpolyposis colorectal cancer. People with Lynch syndrome tend to develop relatively few colon polyps, but those polyps can quickly become malignant. Lynch syndrome is the most common form of inherited colon cancer and is also associated with tumors in the breast, stomach, small intestine, urinary tract, and ovaries.
Familial adenomatous polyposis (FAP) – a rare disorder that causes hundreds or even thousands of polyps to develop in the lining of your colon beginning during your teenage years. If the polyps aren’t treated, your risk of developing colon cancer is nearly 100 percent, usually before age 40. Genetic testing can help determine your risk of FAP.
MYH-associated polyposis (MAP) – A problem with the MYH gene causes many polyps to grow or colon cancer to happen at a young age.
Peutz-Jeghers syndrome – The condition starts with freckles that show up all over the body. It also causes colon polyps that can become cancer.
Serrated polyposis syndrome – This causes a specific type of polyp, serrated adenomatous polyps, to grow in the upper part of the colon. They can turn into colon cancer.
Gardner’s syndrome – a variant of FAP that causes polyps to develop throughout your colon and small intestine. You may also develop noncancerous tumors in other parts of your body, including your skin, bones and abdomen.
MYH-associated polyposis (MAP) – a condition similar to FAP that is caused by mutations in the MYH gene. People with MAP often develop multiple adenomatous polyps and colon cancer at a young age. Genetic testing can help determine your risk of MAP.
Peutz-Jeghers syndrome – a condition that usually begins with freckles developing all over the body, including the lips, gums, and feet. Then noncancerous polyps develop throughout the intestines. These polyps may become malignant, so people with this condition have an increased risk of colon cancer.
Serrated polyposis syndrome – a condition that leads to multiple serrated adenomatous polyps in the upper part of the colon. These polyps may become malignant.
Symptoms of Colonic Polyps
Most people with colon polyps don’t have symptoms. You can’t tell that you have polyps because you feel well. When colon polyps do cause symptoms, you may
But some people with colon polyps experience:
Rectal bleeding – This can be a sign of colon polyps or cancer or other conditions, such as hemorrhoids or minor tears in your anus.
Change in stool color – Blood can show up as red streaks in your stool or make stool appear black. A change in color may also be caused by foods, medications, and supplements.
Change in bowel habits – Constipation or diarrhea that lasts longer than a week may indicate the presence of a large colon polyp. But a number of other conditions can also cause changes in bowel habits.
Pain – A large colon polyp can partially obstruct your bowel, leading to crampy abdominal pain.
Iron deficiency anemia – Bleeding from polyps can occur slowly over time, without visible blood in your stool. Chronic bleeding robs your body of the iron needed to produce the substance that allows red blood cells to carry oxygen to your body (hemoglobin). The result is iron-deficiency anemia, which can make you feel tired and short of breath.
Red blood mixed in with or on the surface of the stool
Black stools if the polyp is bleeding substantially and is located in the proximal colon (cecum and ascending colon)
Weakness, light-headedness, fainting, pale skin, and rapid heart rate due to iron deficiency anemia
The presence of invisible (occult) blood in stool that is tested when screening for colon cancer at visits to a doctor’s office (Because of the tendency of polyps to bleed slowly, intermittently, and in small amounts, occult blood testing of stool often is used to screen for colon cancer.)
Rarely diarrhea when large villous polyps secrete fluid into the intestine
Rarely constipation if the polyp is very large and obstructs the colon
Rarely intussusception, a condition in which a polyp drags the portion of the colon to which it is attached into the more distal colon (i.e., telescopes into the more distal colon) and leads to obstruction of the colon. This can cause all of the signs and symptoms of intestinal obstruction including abdominal pain and distention, nausea, and vomiting.
Have bleeding from your rectum. You might notice blood on your underwear or on toilet paper after you’ve had a bowel movement.
Have blood in your stool. Blood can make stool look black or can show up as red streaks in your stool.
Feel tired because you have anemia and not enough iron in your body. Bleeding from colon polyps can lead to anemia and a lack of iron.
Many other health problems can also cause these symptoms. However, if you have bleeding from your rectum or blood in your stool, contact your doctor right away.
Diagnosis of Colonic Polyps
Doctors can find colon polyps only by using certain tests or procedures, such as a colonoscopy or imaging study. Your doctor may first take a medical and family history and perform a physical exam to help decide which test or procedure is best for you.
For example, your doctor may ask if you have any symptoms. He or she may also ask if you have a family history of colon polyps or colorectal cancer. After taking a medical and family history, your doctor may perform a physical exam.
Tests and procedures
Flexible sigmoidoscopy – For flexible sigmoidoscopy, a trained medical professional uses a sigmoidoscope—a flexible, narrow tube with a light and tiny camera on one end—to look inside your rectum and lower colon. Flexible sigmoidoscopy can show irritated or swollen tissue, ulcers, polyps, and cancer.
Colonoscopy – During a colonoscopy, a trained medical professional uses a long, flexible, narrow tube with a light and tiny camera on one end, called a colonoscope, to look inside your rectum and colon. Colonoscopy can show irritated and swollen tissue, ulcers, polyps, and cancer. The most sensitive test for colorectal polyps and cancer. If polyps are found, your doctor may remove them immediately or take tissue samples (biopsies) for analysis.
Virtual colonoscopy – Virtual colonoscopy uses x-rays and a computer to create images of your rectum and colon from outside the body. Virtual colonoscopy can show ulcers, polyps, and cancer. Doctors can’t remove polyps during virtual colonoscopy.
Lower gastrointestinal series – For a lower gastrointestinal (GI) series, a doctor uses x-rays and a chalky liquid called barium to view your large intestine. The barium will make your large intestine easier to see on an x-ray. A lower GI series is also called a barium enema.
Virtual colonoscopy – a minimally invasive test that uses a CT scan to view your colon. Virtual colonoscopy requires the same bowel preparation as a colonoscopy. If a polyp is found, you’ll need a colonoscopy to have it removed.
CT colonography – Also known as a virtual colonoscopy, this uses X-rays and a computer to take pictures of your colon from outside your body. Your doctor can’t take polyps out during this test. If they spot any, you’ll need to have a regular colonoscopy. You’re awake for this test, but you’ll still need to do a special diet to clear out your bowel beforehand.
Flexible sigmoidoscopy – in which a slender, lighted tube is inserted in your rectum to examine it and the last third of your colon (sigmoid) and rectum. If a polyp is found, you’ll need a colonoscopy to have it removed.
Stool-based tests – This type of test works by checking for the presence of blood in the stool or assessing your stool DNA. If your stool test is positive you will need a colonoscopy.
Fecal occult blood testing – (FOBT) may indicate bleeding from a colonic polyp. A positive FOBT due to bleeding from a polyp correlates to the polyp size and proximity to the rectum. Most small polyps will fail to result in a positive FOBT, although the test has a higher sensitivity for larger polyps and for carcinomas. For this reason, FOBT is a part of the screening algorithm for the early detection of colon cancer, despite its poor sensitivity for polyps.
Fecal immunochemical testing – (FIT or iFOBT) is a newer, more sensitive screening method than the traditional FOBT. It utilizes specific antibodies to the globin component of the hemoglobin. A recent study compared FIT against colonoscopy as a screening tool for both colorectal cancer and adenomas [rx].
Colonoscopic spectroscopy – using near-infrared autofluorescence (NIR AF) was recently proposed as an adjunct for in vivo diagnosis of colonic ‘pre-cancer and cancer during clinical colonoscopic screening. This method was found to have a sensitivity and specificity of approximately 80% and 90%, respectively, for the classification of benign, pre-cancer lesions and cancer in the colon [rx]. This method, although promising, is still experimental and is not routinely used in clinical practice.
Narrow-band imaging – (NBI) is another new endoscopic imaging technique that highlights surface structures and superficial mucosal capillaries during colonoscopy. Even though disagreement exists regarding its effectiveness in increasing the colonoscopic view’s sensitivity, it has recently been shown to have a high sensitivity and specificity for differentiating neoplastic and non-neoplastic polyps [rx, rx]. This modality has also not entered routine clinical practice.
Computed tomographic colonography – (also called ‘CT colonography’ or ‘virtual colonoscopy’) is another screening modality, which is suggested for patients who refuse colonoscopy. This modality uses computed tomography of an air-distended prepared colon. With an optimal colon preparation and an experienced radiologist reading the images, some reports indicate that the sensitivity of CT colonography for detecting polyps larger than 5 mm (which are believed to be clinically significant) exceeds 90% [rx, rx]
Magnetic resonance colonography – (MRC) is another diagnostic modality that is currently being evaluated. The rationale for using MRC is based on the relatively high radiation exposure during CT colonography [rx]. A recent small-scale study has demonstrated a low sensitivity (despite a high specificity) for detecting large (>10 mm) polyps using MRC [rx]. Therefore, the evidence does not support MRC as a standard diagnostic modality for detecting colorectal polyps and this modality is not routinely used in clinical practice.
Capsule endoscopy – is a diagnostic modality that was originally developed to diagnose and evaluate small bowel lesions. Since the capsule passes through the prepared colon after traversing the ileocecal valve and continues to transmit images, it can also detect colonic lesions. A large cohort with suspected colonic lesions underwent a capsule endoscopy with a dual camera capsule designed especially to evaluate the colon (PILLcam colon) and, immediately afterward, had a colonoscopy. The sensitivity and specificity of the capsule endoscopy were shown to be inferior to colonoscopy [rx].
Fecal DNA and antigen testing – is another futuristic modality expected to yield results within the next few decades [rx]. Several technical advances have recently been seen to increase its accuracy, including the use of a DNA preservative buffer with stool collection, DNA amplification methods, and automated assays of several DNA markers [rx]. The stool was analyzed with an automated multi-target stool DNA assay to measure β-actin, mutant KRAS, aberrantly methylated BMP3 and NDRG4, and fecal hemoglobin.
Stool DNA analysis – identified individuals with colorectal cancer with 98% sensitivity and 90% specificity. Its sensitivity in respect of advanced adenomas was 57% and for high-grade dysplasia, it was 83% [30]. In the future, should this modality prove to have even a higher positive predictive value for detecting adenoma or carcinoma, it might obviate the need for any invasive screening tests.
Second examination
If no polyps are found on the first examination it is recommended that a second examination should be done 10 years later.
If the only polyps that are found are hyperplastic polyps, and they are limited to the rectum and sigmoid colon and they are all less than one centimeter in size, a second examination is recommended in 10 years.
If one or two tubular adenomas are found and they are less than one centimeter in size, a second examination is recommended in five years through a longer interval may be reasonable as well.
If three to ten adenomas are found, it is recommended that a second examination be done in three years.
If more than ten adenomas are found, it is recommended that a second examination be done in three years or less.
If one or more tubular adenomas are found that are greater than one centimeter in size, a second examination is recommended in three years.
If one or more adenomas are found of any size and their histology is villous, a second examination is recommended in three years.
If one or more adenomas are found and any show high-grade dysplasia, a second examination is recommended in three years.
If serrated polyps are found, recommendations are less secure because much less information is available about the future risk of polyps and cancers. Concerns are greater (and the interval to the next examination should be shorter) if the polyps are proximal (in the ascending colon), are larger (more than one centimeter in size), and particularly if they show dysplasia.
Treatment for Colonic Polyps
Doctors treat colon polyps by removing them.
In most cases, doctors use special tools during a colonoscopy or flexible sigmoidoscopy to remove colon polyps. After doctors remove the polyp, they send it for testing to check for cancer. A pathologist will review the test results and send a report to your doctor. Doctors can remove almost all polyps without surgery.
If you have colon polyps, your doctor will ask you to get tested regularly in the future because you have a higher chance of developing more polyps.
Your doctor is likely to remove all polyps discovered during a bowel examination.
Eat less meat – Eat a healthy diet, with minimal red meat—especially processed or cured meats. Studies suggest that people with meat-rich diets tend to have higher rates of colon cancer.
antioxidants– Several associations have been explored for antioxidants including selenium, beta carotene, and vitamins A, C, and E. Most of the studies that have been done do not support a role for these agents in preventing polyps or in preventing colon cancer. A limited amount of support is available for the use of selenium to prevent polyps, but selenium is not recommended for use outside of experimental trials.
Supplemental dietary calcium – has been demonstrated in one study to prevent the formation of polyps. The benefit was seen with supplementation of 1200 mg of calcium per day. There is some concern about using calcium since higher dietary and supplemental levels are associated with an increase in vascular disease. The intake of calcium that was studied was higher than the recommended intake of calcium, 800 mg per day.
NSAIDs – The best support for a treatment to prevent polyps is with nonsteroidal anti-inflammatory drugs (NSAIDs), a class of drugs that includes aspirin, ibuprofen (Motrin, Advil), celecoxib (Celebrex), and many others. Aspirin has been shown in several studies to reduce the formation of polyps by 30% to 50%. The effect is likely to occur with higher doses of aspirin (more than the 81-325 mg that is recommended for cardiovascular disease prevention), and there is concern about aspirin’s side effect of gastrointestinal bleeding at these doses.
Celecoxib (Celebrex), a “COX-2 selective NSAID” – or Cox-2 inhibitor has been shown to reduce colon polyps 30% to 50% as well, but there is a lingering concern about the possible cardiovascular side effects that may be seen with most NSAIDs (though the data supporting this side effect is conflicting). It may be used in patients with genetic polyposis syndromes who choose not to have their colons removed. Celecoxib might be considered in patients with a low risk for cardiovascular disease who develop adenomatous polyps frequently.
Sulindac (Clinoril) – a “non-selective NSAID” has been shown to prevent polyps in patients with sporadic adenoma as well as genetic syndromes. As with celecoxib, there is concern about cardiovascular side effects and gastrointestinal ulceration and bleeding.
Aspirin – Taking a low dose of aspirin every day for a long period of time may help prevent polyps from developing into colorectal cancer in some people. However, taking aspirin daily may cause side effects such as bleeding in your stomach or intestines. Talk with your doctor before you start taking aspirin daily.
Some types of colon polyp are far likelier to become malignant than are others. But a doctor who specializes in analyzing tissue samples (pathologist) usually must examine polyp tissue under a microscope to determine whether it’s potentially cancerous.
Surgery
Removal with forceps or a wire loop (polypectomy) – If a polyp is larger than 0.4 inches (about 1 centimeter), a liquid may be injected under it to lift and isolate the polyp from surrounding tissue so that it can be removed.
Minimally invasive surgery – Polyps that are too large or that can’t be removed safely during screening are usually removed laparoscopically, which is performed by inserting an instrument called a laparoscope into the bowel.
Colon and rectum removal – If you have a rare inherited syndrome, such as FAP, you may need surgery to remove your colon and rectum (total proctocolectomy).
Laparoscopy – During a laparoscopy, the doctor will make a small incision into the abdomen or pelvis and insert an instrument called a laparoscope into the bowel. They use this technique to remove polyps that are too large or cannot be removed safely by colonoscopy.
Removing the colon and rectum – This procedure, known as a total proctocolectomy, is only necessary when a person has a severe condition or cancer. Doctors recommend this option for those with rare inherited conditions, such as familial adenomatous polyposis (FAP). FAP is an inherited condition that causes cancer of the colon and rectum, and polyp removal may prevent cancer from developing.
Seek Care Right Away
Call your doctor right away if you have any of the following symptoms after he or she removes a colon polyp:
severe pain in your abdomen
fever
bloody bowel movements that do not get better
bleeding from your anus that does not stop
dizziness
weakness
How can I prevent colon polyps?
Researchers don’t know a sure way to prevent colon polyps. However, you can take steps to lower your chances of developing colon polyps.
Eating, diet, and nutrition
Eating, diet, and nutrition changes—such as eating less red meat and more fruits and vegetables—may lower your chances of developing colon polyps.
You can make the following healthy lifestyle choices to help lower your chances of developing colon polyps:
get regular physical activity
don’t smoke cigarettes, and if you do smoke, quit
avoid drinking alcohol
lose weight if you’re overweight
Being physically active and losing weight if you’re overweight may lower your chances of developing colon polyps.
How Can I Prevent Colon Polyps?
Healthy habits can lower your odds of having colon polyps. For example, you should:
Eat a diet with lots of fruits, vegetables, and fiber-rich foods like beans, lentils, peas, and high-fiber cereal.
Lose weight if you’re overweight.
Limit red meat, processed meats, and foods that are high in fat.
Talk to your doctor about whether calcium and vitamin D supplements are right for you. Some studies suggest they could lower your odds of colon cancer, but others don’t.
If you have a family history of colon polyps, ask your doctor if you should get genetic counseling and when you should start screening for polyps.
Talk to your doctor about taking aspirin regularly. There is some evidence that aspirin has a preventive effect against colon cancer.
Colorectal Polyps/Colon polyps also known as colorectal polyps are their macroscopic appearance as sessile (flat, arising directly from the mucosal layer) or pedunculated (extending from the mucosa through a fibrovascular stalk) growths on the lining of your colon and rectum. You can have more than one colon polyp. Colon polyps are protrusions occurring in the colon lumen most commonly sporadic or as part of other syndromes. Polyps are classified as diminutive if 5 mm in diameter or less, small if 6 to 9 mm, or large if they are 1 cm in diameter or more. Polyps can be depressed, flat, sessile or pedunculated. Few polyps arise from submucosa including lipomas, carcinoids, or lymphoid aggregates. Most commonly, however, they result from the mucosa, and they can be adenomatous, serrated, or non-neoplastic.
Types of colonic polyps
Polyps in the colon can vary in size and number. There are 5 types of colon polyps
Hyperplastic polyps – are harmless and don’t develop into cancer.
Adenomatous polyps – are the most common. Although most will never develop into cancer, they do have the potential to become colon cancer.
Malignant polyps – are polyps that are noted under microscopic examination to have cancer cells in them.
Adenomas – Two-thirds of colon polyps are the precancerous type, called adenomas. It can take seven to 10 or more years for an adenoma to evolve into cancer—if it ever does. Overall, only 5% of adenomas progress to cancer, but your individual risk is hard to predict. Doctors remove all the adenomas they find
Sessile serrated polyps – Once thought harmless, this type of adenoma is now known to be risky. These are also removed.
Causes of Colorectal Polyps
Hereditary disorders that cause colon polyps include:
Lynch syndrome – also called hereditary nonpolyposis colorectal cancer. People with Lynch syndrome tend to develop relatively few colon polyps, but those polyps can quickly become malignant. Lynch syndrome is the most common form of inherited colon cancer and is also associated with tumors in the breast, stomach, small intestine, urinary tract, and ovaries.
Familial adenomatous polyposis (FAP) – a rare disorder that causes hundreds or even thousands of polyps to develop in the lining of your colon beginning during your teenage years. If the polyps aren’t treated, your risk of developing colon cancer is nearly 100 percent, usually before age 40. Genetic testing can help determine your risk of FAP.
MYH-associated polyposis (MAP) – A problem with the MYH gene causes many polyps to grow or colon cancer to happen at a young age.
Peutz-Jeghers syndrome – The condition starts with freckles that show up all over the body. It also causes colon polyps that can become cancer.
Serrated polyposis syndrome – This causes a specific type of polyp, serrated adenomatous polyps, to grow in the upper part of the colon. They can turn into colon cancer.
Gardner’s syndrome – a variant of FAP that causes polyps to develop throughout your colon and small intestine. You may also develop noncancerous tumors in other parts of your body, including your skin, bones and abdomen.
MYH-associated polyposis (MAP) – a condition similar to FAP that is caused by mutations in the MYH gene. People with MAP often develop multiple adenomatous polyps and colon cancer at a young age. Genetic testing can help determine your risk of MAP.
Peutz-Jeghers syndrome – a condition that usually begins with freckles developing all over the body, including the lips, gums, and feet. Then noncancerous polyps develop throughout the intestines. These polyps may become malignant, so people with this condition have an increased risk of colon cancer.
Serrated polyposis syndrome – a condition that leads to multiple serrated adenomatous polyps in the upper part of the colon. These polyps may become malignant.
Symptoms of Colorectal Polyps
Most people with colon polyps don’t have symptoms. You can’t tell that you have polyps because you feel well. When colon polyps do cause symptoms, you may
But some people with colon polyps experience:
Rectal bleeding – This can be a sign of colon polyps or cancer or other conditions, such as hemorrhoids or minor tears in your anus.
Change in stool color – Blood can show up as red streaks in your stool or make stool appear black. A change in color may also be caused by foods, medications, and supplements.
Change in bowel habits – Constipation or diarrhea that lasts longer than a week may indicate the presence of a large colon polyp. But a number of other conditions can also cause changes in bowel habits.
Pain – A large colon polyp can partially obstruct your bowel, leading to crampy abdominal pain.
Iron deficiency anemia – Bleeding from polyps can occur slowly over time, without visible blood in your stool. Chronic bleeding robs your body of the iron needed to produce the substance that allows red blood cells to carry oxygen to your body (hemoglobin). The result is iron-deficiency anemia, which can make you feel tired and short of breath.
Red blood mixed in with or on the surface of the stool
Black stools if the polyp is bleeding substantially and is located in the proximal colon (cecum and ascending colon)
Weakness, light-headedness, fainting, pale skin, and rapid heart rate due to iron deficiency anemia
The presence of invisible (occult) blood in stool that is tested when screening for colon cancer at visits to a doctor’s office (Because of the tendency of polyps to bleed slowly, intermittently and in small amounts, occult blood testing of stool often is used to screen for colon cancer.)
Rarely diarrhea when large villous polyps secrete fluid into the intestine
Rarely constipation if the polyp is very large and obstructs the colon
Rarely intussusception, a condition in which a polyp drags the portion of the colon to which it is attached into the more distal colon (i.e., telescopes into the more distal colon) and leads to obstruction of the colon. This can cause all of the signs and symptoms of intestinal obstruction including abdominal pain and distention, nausea and vomiting.
Have bleeding from your rectum. You might notice blood on your underwear or on toilet paper after you’ve had a bowel movement.
Have blood in your stool. Blood can make stool look black or can show up as red streaks in your stool.
Feel tired because you have anemia and not enough iron in your body. Bleeding from colon polyps can lead to anemia and a lack of iron.
Many other health problems can also cause these symptoms. However, if you have bleeding from your rectum or blood in your stool, contact your doctor right away.
Diagnosis of Colorectal Polyps
Doctors can find colon polyps only by using certain tests or procedures, such as a colonoscopy or imaging study. Your doctor may first take a medical and family history and perform a physical exam to help decide which test or procedure is best for you.
For example, your doctor may ask if you have any symptoms. He or she may also ask if you have a family history of colon polyps or colorectal cancer. After taking a medical and family history, your doctor may perform a physical exam.
Tests and procedures
Flexible sigmoidoscopy – For a flexible sigmoidoscopy, a trained medical professional uses a sigmoidoscope—a flexible, narrow tube with a light and tiny camera on one end—to look inside your rectum and lower colon. Flexible sigmoidoscopy can show irritated or swollen tissue, ulcers, polyps, and cancer.
Colonoscopy – During a colonoscopy, a trained medical professional uses a long, flexible, narrow tube with a light and tiny camera on one end, called a colonoscope, to look inside your rectum and colon. Colonoscopy can show irritated and swollen tissue, ulcers, polyps, and cancer. The most sensitive test for colorectal polyps and cancer. If polyps are found, your doctor may remove them immediately or take tissue samples (biopsies) for analysis.
Virtual colonoscopy – Virtual colonoscopy uses x-rays and a computer to create images of your rectum and colon from outside the body. Virtual colonoscopy can show ulcers, polyps, and cancer. Doctors can’t remove polyps during virtual colonoscopy.
Lower gastrointestinal series – For a lower gastrointestinal (GI) series, a doctor uses x-rays and a chalky liquid called barium to view your large intestine. The barium will make your large intestine easier to see on an x-ray. A lower GI series is also called a barium enema.
Virtual colonoscopy – a minimally invasive test that uses a CT scan to view your colon. Virtual colonoscopy requires the same bowel preparation as a colonoscopy. If a polyp is found, you’ll need a colonoscopy to have it removed.
CT colonography – Also known as a virtual colonoscopy, this uses X-rays and a computer to take pictures of your colon from outside your body. Your doctor can’t take polyps out during this test. If they spot any, you’ll need to have a regular colonoscopy. You’re awake for this test, but you’ll still need to do a special diet to clear out your bowel beforehand.
Flexible sigmoidoscopy – in which a slender, lighted tube is inserted in your rectum to examine it and the last third of your colon (sigmoid) and rectum. If a polyp is found, you’ll need a colonoscopy to have it removed.
Stool-based tests – This type of test works by checking for the presence of blood in the stool or assessing your stool DNA. If your stool test is positive you will need a colonoscopy.
Fecal occult blood testing – (FOBT) may indicate bleeding from a colonic polyp. A positive FOBT due to bleeding from a polyp correlates to the polyp size and proximity to the rectum. Most small polyps will fail to result in a positive FOBT, although the test has a higher sensitivity for larger polyps and for carcinomas. For this reason, FOBT is a part of the screening algorithm for the early detection of colon cancer, despite its poor sensitivity for polyps.
Fecal immunochemical testing – (FIT or iFOBT) is a newer, more sensitive screening method than the traditional FOBT. It utilizes specific antibodies to the globin component of the hemoglobin. A recent study compared FIT against colonoscopy as a screening tool for both colorectal cancer and adenomas [rx].
Colonoscopic spectroscopy – using near-infrared autofluorescence (NIR AF) was recently proposed as an adjunct for in vivo diagnosis of colonic ‘pre-cancer and cancer during clinical colonoscopic screening. This method was found to have a sensitivity and specificity of approximately 80% and 90%, respectively, for the classification of benign, pre-cancer lesions and cancer in the colon [rx]. This method, although promising, is still experimental and is not routinely used in clinical practice.
Narrow-band imaging – (NBI) is another new endoscopic imaging technique that highlights surface structures and superficial mucosal capillaries during colonoscopy. Even though disagreement exists regarding its effectiveness in increasing the colonoscopic view’s sensitivity, it has recently been shown to have a high sensitivity and specificity for differentiating neoplastic and non-neoplastic polyps [rx, rx]. This modality has also not entered routine clinical practice.
Computed tomographic colonography – (also called ‘CT colonography’ or ‘virtual colonoscopy’) is another screening modality, which is suggested for patients who refuse colonoscopy. This modality uses computed tomography of an air-distended prepared colon. With an optimal colon preparation and an experienced radiologist reading the images, some reports indicate that the sensitivity of CT colonography for detecting polyps larger than 5 mm (which are believed to be clinically significant) exceeds 90% [rx, rx]
Magnetic resonance colonography – (MRC) is another diagnostic modality that is currently being evaluated. The rationale for using MRC is based on the relatively high radiation exposure during CT colonography [rx]. A recent small-scale study has demonstrated a low sensitivity (despite a high specificity) for detecting large (>10 mm) polyps using MRC [rx]. Therefore, the evidence does not support MRC as a standard diagnostic modality for detecting colorectal polyps and this modality is not routinely used in clinical practice.
Capsule endoscopy – is a diagnostic modality that was originally developed to diagnose and evaluate small bowel lesions. Since the capsule passes through the prepared colon after traversing the ileocecal valve and continues to transmit images, it can also detect colonic lesions. A large cohort with suspected colonic lesions underwent a capsule endoscopy with a dual camera capsule designed especially to evaluate the colon (PILLcam colon) and, immediately afterward, had a colonoscopy. The sensitivity and specificity of the capsule endoscopy were shown to be inferior to colonoscopy [rx].
Fecal DNA and antigen testing – is another futuristic modality expected to yield results within the next few decades [rx]. Several technical advances have recently been seen to increase its accuracy, including the use of a DNA preservative buffer with stool collection, DNA amplification methods, and automated assays of several DNA markers [rx]. The stool was analyzed with an automated multi-target stool DNA assay to measure β-actin, mutant KRAS, aberrantly methylated BMP3 and NDRG4, and fecal hemoglobin.
Stool DNA analysis – identified individuals with colorectal cancer with 98% sensitivity and 90% specificity. Its sensitivity in respect of advanced adenomas was 57% and for high-grade dysplasia, it was 83% [30]. In the future, should this modality prove to have even a higher positive predictive value for detecting adenoma or carcinoma, it might obviate the need for any invasive screening tests.
Second examination
If no polyps are found on the first examination it is recommended that a second examination should be done 10 years later.
If the only polyps that are found are hyperplastic polyps, and they are limited to the rectum and sigmoid colon and they are all less than one centimeter in size, a second examination is recommended in 10 years.
If one or two tubular adenomas are found and they are less than one centimeter in size, a second examination is recommended in five years through a longer interval may be reasonable as well.
If three to ten adenomas are found, it is recommended that a second examination be done in three years.
If more than ten adenomas are found, it is recommended that a second examination be done in three years or less.
If one or more tubular adenomas are found that are greater than one centimeter in size, a second examination is recommended in three years.
If one or more adenomas are found of any size and their histology is villous, a second examination is recommended in three years.
If one or more adenomas are found and any show high-grade dysplasia, a second examination is recommended in three years.
If serrated polyps are found, recommendations are less secure because much less information is available about the future risk of polyps and cancers. Concerns are greater (and the interval to the next examination should be shorter) if the polyps are proximal (in the ascending colon), are larger (more than one centimeter in size), and particularly if they show dysplasia.
Treatment for Colorectal Polyps
Doctors treat colon polyps by removing them.
In most cases, doctors use special tools during a colonoscopy or flexible sigmoidoscopy to remove colon polyps. After doctors remove the polyp, they send it for testing to check for cancer. A pathologist will review the test results and send a report to your doctor. Doctors can remove almost all polyps without surgery.
If you have colon polyps, your doctor will ask you to get tested regularly in the future because you have a higher chance of developing more polyps.
Your doctor is likely to remove all polyps discovered during a bowel examination.
Eat less meat – Eat a healthy diet, with minimal red meat—especially processed or cured meats. Studies suggest that people with meat-rich diets tend to have higher rates of colon cancer.
antioxidants– Several associations have been explored for antioxidants including selenium, beta carotene, and vitamins A, C, and E. Most of the studies that have been done do not support a role for these agents in preventing polyps or in preventing colon cancer. A limited amount of support is available for the use of selenium to prevent polyps, but selenium is not recommended for use outside of experimental trials.
Supplemental dietary calcium – has been demonstrated in one study to prevent the formation of polyps. The benefit was seen with supplementation of 1200 mg of calcium per day. There is some concern about using calcium since higher dietary and supplemental levels are associated with an increase in vascular disease. The intake of calcium that was studied was higher than the recommended intake of calcium, 800 mg per day.
NSAIDs – The best support for a treatment to prevent polyps is with nonsteroidal anti-inflammatory drugs (NSAIDs), a class of drugs that includes aspirin, ibuprofen (Motrin, Advil), celecoxib (Celebrex), and many others. Aspirin has been shown in several studies to reduce the formation of polyps by 30% to 50%. The effect is likely to occur with higher doses of aspirin (more than the 81-325 mg that is recommended for cardiovascular disease prevention), and there is concern about aspirin’s side effect of gastrointestinal bleeding at these doses.
Celecoxib (Celebrex), a “COX-2 selective NSAID” – or Cox-2 inhibitor has been shown to reduce colon polyps 30% to 50% as well, but there is a lingering concern about the possible cardiovascular side effects that may be seen with most NSAIDs (though the data supporting this side effect is conflicting). It may be used in patients with genetic polyposis syndromes who choose not to have their colons removed. Celecoxib might be considered in patients with a low risk for cardiovascular disease who develop adenomatous polyps frequently.
Sulindac (Clinoril) – a “non-selective NSAID” has been shown to prevent polyps in patients with sporadic adenoma as well as genetic syndromes. As with celecoxib, there is concern about cardiovascular side effects and gastrointestinal ulceration and bleeding.
Aspirin – Taking a low dose of aspirin every day for a long period of time may help prevent polyps from developing into colorectal cancer in some people. However, taking aspirin daily may cause side effects such as bleeding in your stomach or intestines. Talk with your doctor before you start taking aspirin daily.
Some types of colon polyp are far likelier to become malignant than are others. But a doctor who specializes in analyzing tissue samples (pathologist) usually must examine polyp tissue under a microscope to determine whether it’s potentially cancerous.
Surgery
Removal with forceps or a wire loop (polypectomy) – If a polyp is larger than 0.4 inches (about 1 centimeter), a liquid may be injected under it to lift and isolate the polyp from surrounding tissue so that it can be removed.
Minimally invasive surgery – Polyps that are too large or that can’t be removed safely during screening are usually removed laparoscopically, which is performed by inserting an instrument called a laparoscope into the bowel.
Colon and rectum removal – If you have a rare inherited syndrome, such as FAP, you may need surgery to remove your colon and rectum (total proctocolectomy).
Laparoscopy – During a laparoscopy, the doctor will make a small incision into the abdomen or pelvis and insert an instrument called a laparoscope into the bowel. They use this technique to remove polyps that are too large or cannot be removed safely by colonoscopy.
Removing the colon and rectum – This procedure, known as a total proctocolectomy, is only necessary when a person has a severe condition or cancer. Doctors recommend this option for those with rare inherited conditions, such as familial adenomatous polyposis (FAP). FAP is an inherited condition that causes cancer of the colon and rectum, and polyp removal may prevent cancer from developing.
Seek Care Right Away
Call your doctor right away if you have any of the following symptoms after he or she removes a colon polyp:
severe pain in your abdomen
fever
bloody bowel movements that do not get better
bleeding from your anus that does not stop
dizziness
weakness
How can I prevent colon polyps?
Researchers don’t know a sure way to prevent colon polyps. However, you can take steps to lower your chances of developing colon polyps.
Eating, diet, and nutrition
Eating, diet, and nutrition changes—such as eating less red meat and more fruits and vegetables—may lower your chances of developing colon polyps.
You can make the following healthy lifestyle choices to help lower your chances of developing colon polyps:
get regular physical activity
don’t smoke cigarettes, and if you do smoke, quit
avoid drinking alcohol
lose weight if you’re overweight
Being physically active and losing weight if you’re overweight may lower your chances of developing colon polyps.
How Can I Prevent Colon Polyps?
Healthy habits can lower your odds of having colon polyps. For example, you should:
Eat a diet with lots of fruits, vegetables, and fiber-rich foods like beans, lentils, peas, and high-fiber cereal.
Lose weight if you’re overweight.
Limit red meat, processed meats, and foods that are high in fat.
Talk to your doctor about whether calcium and vitamin D supplements are right for you. Some studies suggest they could lower your odds of colon cancer, but others don’t.
If you have a family history of colon polyps, ask your doctor if you should get genetic counseling and when you should start screening for polyps.
Talk to your doctor about taking aspirin regularly. There is some evidence that aspirin has a preventive effect against colon cancer.
Steatorrhea is a common complication as a result of a mechanical block in the biliary tract or by intrahepatic lesions. When bile salt entry into the duodenum is hindered, the emulsification of dietary fats is incomplete. Steatorrhea is more frequently seen in patients with cholestatic disease, e.g., primary biliary cirrhosis (PBC) and primary sclerosing cholangitis (PSC). The reduced absorption of fat results in nausea, indigestion, and steatorrhea, with accompanying calcium and fat-soluble vitamin malabsorption.
The definition of steatorrhea is an increase in fat excretion in the stools. Steatorrhea is one of the clinical features of fat malabsorption and noted in many conditions such as exocrine pancreatic insufficiency (EPI), celiac disease, and tropical sprue. An increase in the fat content of stools results in the production of pale, large volume, malodorous, loose stools. Screening for steatorrhea may be carried out by examining stool samples for the presence of fat by Sudan III staining. However, quantitative fecal fat estimation is required to confirm the diagnosis.
Among the macronutrients, digestion and absorption of fat involve a complex mechanism. Fat absorption requires bile acids, digestive enzymes, and a normally functioning small intestinal mucosa. Dietary lipids, mostly as triacylglycerols, are initially emulsified by bile acids and then hydrolyzed by the pancreatic lipases and colipases into free fatty acids and monoglycerides. In the proximal small bowel, these hydrolyzed lipids form micelles by the action of bile acids. The micelles are then absorbed across the intestinal villi and transported as chylomicrons via the intestinal lymphatics. Therefore, any defects in the availability or function of bile acids, pancreatic digestive enzymes or absorptive villi will lead to steatorrhea.[rx]
Causes of Steatorrhea
The causes of steatorrhea are numerous and subclassify under three broad categories: (1) conditions leading to EPI, (2) bile acid deficiency states, and (3) diseases affecting the small intestine. Most notable disorders in each category are given below[rx][rx]:
EPI – due to chronic pancreatitis, cystic fibrosis (CF), and conditions resulting in pancreatic duct obstruction or resection of the pancreas (e.g., pancreatic tumors)
Bile acid deficiency – either due to cholestasis (e.g. primary biliary cirrhosis, currently referred as primary biliary cholangitis (PBC), primary sclerosing cholangitis (PSC)) or inability to absorb bile acids in the distal ileum resulting in diminished bile acid pool (e.g. ileal resection or Crohn disease of the ileum) or deconjugation of bile acids (e.g., small intestinal bacterial overgrowth (SIBO))
Diseases affecting proximal small intestines – such as celiac disease, tropical sprue, giardiasis, Whipple disease, lymphoma, amyloidosis, SIBO, and HIV enteropathy. Other rare causes of steatorrhea include lipase inhibitors such as orlistat, Zollinger-Ellison syndrome (increased production of gastric acid inactivates the pH-sensitive pancreatic lipases), and graft-versus-host disease.[rx]
EPI – Chronic exposure to alcohol is the most common etiological factor for chronic pancreatitis. The other notable risk factors for chronic pancreatitis include predisposing genetic mutations (PRSS-1, SPINK-1, CFTR, CTRC), autoimmune pancreatitis, pancreatic duct obstruction, and chronic nicotine exposure.[rx] The exact pathophysiological pathways underlying chronic pancreatitis are unclear but may include mechanisms such as chronic ongoing parenchymal inflammation with acinar cell destruction, and ductal dysfunction, etc.[rx] The histopathological changes include pancreatic atrophy with fibrous scarring, which may be focal or diffuse.[rx]
CF – is a multisystem disease as a result of mutations in the gene which encodes the CF transmembrane conductance regulator (CFTR).[rx] In the pancreas, CFTR dysfunction results in thick viscous secretions along with defective bicarbonate flow resulting in EPI.
Cholestatic diseases – The mechanisms underlying the development of chronic cholestatic liver diseases, including PBC and PSC, are not entirely understood. Both these disorders are characterized by portal inflammation and progressive fibrosis and eventually resulting in end-stage liver disease. Here, the reduction in bile flow results in the accumulation of toxic bile products, which leads to biliary epithelial damage.[rx] This decrease in bile reaching the small bowel interferes with fat absorption and causes steatorrhea in these patients.
Celiac disease – It is a chronic autoimmune-mediated enteropathy related to exposure to dietary gluten in genetically susceptible individuals. The genes which encode for major histocompatibility complex (MHC) class II proteins HLA-DQ2 and HLA-DQ8 are prerequisites for this disease. Ingestion of gluten (specifically the gliadin peptides from wheat, rye, and barley) by susceptible individuals, along with some unknown trigger factors, leads to pathogenesis.[rx] Gliadin polypeptides are resistant to degradation in the gastrointestinal tract and can cross the small intestinal epithelial barrier. In the lamina propria, these peptides get deamidated by local extracellular tissue transglutaminase (TTG).[rx] This deamidation increases the affinity of gliadin binding to the antigen-binding groove of HLA DQ2 or HLA DQ8 on antigen-presenting cells. Upon presentation to CD4+ T lymphocytes, the gliadin peptides trigger an immune response causing local inflammation, which results in the destruction of villi. In addition to adaptive immune dysfunction, patients with celiac disease also have defects in innate intestinal immunity. The histopathological changes include increased intraepithelial lymphocytes, intestinal villous atrophy (blunting or flattening of the villi), and crypt hyperplasia (elongation of the crypts).[rx] These changes lead to malabsorption of fats and fat-soluble vitamins.
SIBO – Under physiological conditions, several defense mechanisms regulate the microbiota in the gastrointestinal tract and prevent small intestine bacterial overgrowth. The significant factors in SIBO prevention include immunoglobin A, gastric acidity, bile, and defensins.[rx] The aboral peristalsis with migratory motor complexes and an intact ileocaecal valve also play a vital role in preventing SIBO.[rx] Any disturbances in these mechanisms could result in bacterial overgrowth.[rx][rx] Deconjugation of bile acids causes fat malabsorption along with other factors such as ongoing inflammation, increased intestinal permeability.[rx][rx]
Associate Causes
Conditions affecting the pancreas. Exocrine pancreatic insufficiency[rx] can be caused by chronic pancreatitis, cystic fibrosis and pancreatic cancer (if it obstructs biliary outflow).[rx]
Conditions affecting bile salts. Obstruction of the bile ducts by gallstones (choledocholithiasis), primary sclerosing cholangitis, liver damage (intrahepatic cholestasis), hypolipidemic drugs, or changes following gallbladder removal (cholecystectomy).[rx]
Conditions producing intestinal malabsorption. These include celiac disease, bacterial overgrowth, tropical sprue, Giardiasis (a protozoan parasite infection), Zollinger-Ellison syndrome, short bowel syndrome, inflammatory bowel disease, and abetalipoproteinemia.[rx][rx]
Other causes: Drugs that can produce steatorrhea include orlistat, a slimming pill, or as an adverse effect of octreotide or lanreotide, used to treat acromegaly or other neuroendocrine tumors.[rx] It can be found in Graves’ disease/hyperthyroidism.[rx]
Alcoholic pancreatitis
Hereditary pancreatitis (mutations in genes such as PRSS-1, SPINK-1, CFTR, CTRC)
Pancreatic insufficiency due to inherited conditions such as CF, Shwachman-Diamond syndrome, Pearson marrow syndrome, and Johanson–Blizzard syndrome
Celiac disease
Tropical sprue
Chronic liver diseases such as PBC, PSC
Advanced pancreatic cancer
Distal ileal pathology (e.g., Crohn disease) or resection
Steatorrhea is only one of several common symptoms of malabsorption. Others include:
abdominal cramps
diarrhea
gas
indigestion
weight loss
foamy, frothy, or mucous-filled stool
foul-smelling stool
diarrhea or loose or runny stool that is bulkier than normal
light-colored stool, often a light brown, green, orange, or yellow
stool that floats
stool that appears to be covered in a thick, greasy film
stool that is difficult to flush away
abdominal pain, cramping, bloating, and gassiness
heartburn and indigestion
general exhaustion
minor muscle, bone, and joint ache
Malnutrition and dehydration may be caused by severe or chronic cases of steatorrhea. Further, serious symptoms can occur as well, especially when associated with underlying medical conditions.
Symptoms associated with severe or chronic steatorrhea include:
Patients with steatorrhea present with bulky, pale, foul-smelling oily stools. These fatty stools tend to float in the toilet bowl and often challenging to flush as well. In the early stages, steatorrhea may be asymptomatic and go unnoticed. Patients also have other nonspecific manifestations of fat malabsorption such as chronic diarrhea, abdominal discomfort, bloating sensation, and weight loss. Children may present with growth failure and delayed puberty. In severe cases, loss of subcutaneous fat and muscle wasting may be evident. Manifestations of fat-soluble vitamin (A, D, E, and K) deficiencies can accompany fat malabsorption. Celiac patients can present with a variety of extraintestinal signs such as anemia, oral ulcers, and dermatitis herpetiformis rash. Abdominal pain is a predominant symptom in patients with chronic pancreatitis but also reported in other conditions such as SIBO, inflammatory bowel disease, and celiac disease. CF patients have sinopulmonary manifestations. Jaundice, fatigue, and pruritis are suggestive of cholestatic liver diseases such as PBC or PSC. Signs for end-stage liver disease such as splenomegaly, ascites can be noted in PBC or PSC.
Lab Test
The diagnosis of steatorrhea is based on clinical findings, laboratory tests, and radiological images. Endoscopy with small intestinal biopsy, liver biopsy, and other specialized investigations may be needed to detect the exact etiology of steatorrhea.
Quantitative estimation of fecal fat (exceeding 7 g per 24 hours) is an essential first step for the diagnosis of steatorrhea. The standard method of fecal fat quantification is by calculating the coefficient of fat absorption (CFA).[rx] With a standard quantity of fat ingestion, CFA is the percentage of dietary fat that is absorbed.[rx] Patients should follow a strict diet for five days containing 100 g of fats daily.[rx] Stools are collected in the last 72-hour for fecal fat estimation. CFA over 92% is considered normal.[rx] Even though accurate, this method is cumbersome and unpleasant for most patients. For evaluation of EPI, fecal elastase may be utilized instead of the 72-hour fecal fat testing. A value of more than 200 mcg/g of stool is considered normal; 100 to 200 mcg/g as indeterminate, and less than 100 mcg/g is abnormal and indicative of EPI. Here the advantage is the requirement of a single stool sample. However, in the early stages of EPI, this test has a lower sensitivity. Also, a formed stool is necessary for testing. Otherwise, the fecal elastase could be falsely low due to dilution.
For evaluation of chronic pancreatitis (1) A plain abdominal radiograph may show pancreatic calcification, (2) Abdominal CT or MRI scans may reveal calcifications of chronic pancreatitis and ductal dilatation, (3) Magnetic resonance cholangiopancreatography (MRCP) or endoscopic retrograde cholangiopancreatography (ERCP) can offer a more detailed evaluation of pancreatic parenchymal and ductal changes in chronic pancreatitis.[rx][rx] Similarly, MRCP, ERCP, and endoscopic ultrasound (EUS) are indispensable in the evaluation of pancreatic tumors.
For evaluation of celiac disease: (1) Estimation of serum tissue transglutaminase IgA antibodies (TTG-IgA) with total serum IgA is the recommended screening test.[rx] IgA endomysial antibodies (EMA-IgA) has the highest specificity and is an option if TTG-IgA is weakly positive.[rx] In patients with IgA deficiency, both TTG-IgA and EMA-IgA may be falsely low. In this population, TTG-IgG and deamidated gliadin peptide IgG (DGP-IgG) are the recommendations for screening.[rx] Patients with positive serological tests should be followed up with duodenal biopsies for confirmation.[rx]
In patients suspected to have the chronic liver disease: (1) serum liver tests may reflect a cholestatic pattern, (2) elevation of alkaline phosphatase and gamma-glutamyl transferase are frequent findings in both PBC and PSC (3) AST, ALT, and bilirubin may be normal or elevated (4) Anti-mitochondrial antibodies are noted in 90 to 95% of patients with PBC.[rx] Liver biopsy is not routinely needed for the diagnosis of PBC. If done, a liver biopsy may show the destruction of interlobular bile ducts and cirrhotic changes in the later stages.
In PSC, magnetic resonance cholangiography (MRC) is the preferred modality and may show a multifocal narrowing of both intrahepatic and extrahepatic biliary ductal strictures. These strictures may be seen alternating with dilation, which is referred to as the “beaded” appearance.[rx] ERCP or percutaneous transhepatic cholangiography is also helpful to delineate the biliary anatomy in PSC but not routinely utilized for the diagnosis due to their invasiveness.[rx] In PSC, a liver biopsy is not a routine test, and when done, may demonstrate periductular fibrosis (onion skin fibrosis).[rx] Even though specific, this finding is infrequent.[rx] In PSC, a liver biopsy may be helpful in a few particular circumstances, such as for the evaluation of small duct PSC and also to exclude coexistent autoimmune hepatitis, which is referred to as overlap syndrome.[rx] About 80% of patients with PSC have IBD. Due to this strong association, if previously undiagnosed, a workup for IBD is recommended at the time of diagnosis of PSC.
Endoscopy with direct aspiration and culture of the small intestinal contents was traditionally the gold standard test for SIBO.[rx] However, due to its invasive nature and lack of consensus on the definition regarding SIBO, this method is less preferred.[rx] Breath tests utilizing either glucose or lactulose are commonly used in clinical practice.[rx]
Treatment of Steatorrhea
Treatment of steatorrhea depends on the underlying conditions which cause steatorrhea.
In patients with EPI, pancreatic enzyme replacement therapy (PERT) is the cornerstone of treatment.[rx]
Along with PERT, patients with EPI should receive normal to a high-fat diet and fat-soluble vitamin supplementation.[rx] Fat restriction may improve the symptoms associated with steatorrhea but will worsen the nutritional status and is no longer a recommendation.
In patients with SIBO, an empiric trial of antibiotics is recommended. In many institutions, rifaximin is preferable to other antibiotics such as ciprofloxacin, metronidazole, norfloxacin, doxycycline, and amoxicillin-clavulanic acid.[rx][rx]
In patients with celiac disease, diet-centered recommendations include a strict life-long gluten-free diet, education about the disease, management of nutritional deficiencies, access to an advocacy group, and consultation with a skilled dietitian.[rx]
Ursodeoxycholic acid is the first-line treatment of choice for PBC.[rx] About 40% of patients may not respond to ursodeoxycholic acid and may eventually need a liver transplant.[30]
Even though ursodeoxycholic acid is often used in PSC, medical therapy is not effective in curtailing the disease progression. ERCP with stent dilatation is useful for symptomatic improvement in biliary ductal strictures in large intrahepatic or extrahepatic ducts.[rx] Liver transplantation is the definitive treatment for PSC and, post-transplant recurrence is not uncommon.
Home remedies for treating and preventing steatorrhea include
staying hydrated
reducing dietary fiber intake
reducing dietary fat intake
quitting or reducing smoking
stopping or reducing alcohol use
reducing or limiting potassium oxalate intake
increasing dietary intake of fat-soluble vitamins by taking nutritional supplements, such as vitamins A, D, E, and K. A range of multivitamin supplements are available for purchase online.
increasing dietary intake of vitamin B-12, folic acid, iron, magnesium, and calcium
taking over-the-counter antidiarrheal medications, including loperamide (Imodium) and bismuth subsalicylate (Kaopectate, Pepto-Bismol). A range of antidiarrheal medications is available for purchase over the counter or online.
taking an over-the-counter antacid, anti-bloating, and gas medications
Severe or chronic cases of steatorrhea will normally need medical intervention. People with steatorrhea because of an underlying medical condition will also usually need medical treatment.
Medications used to treat and prevent steatorrhea include:
intravenous fluids (IV) to restore electrolytes and stop dehydration
anti-diarrheal medications
pancreatic enzyme replacement therapy (PERT)
Proton-pump inhibitors or PPIs
MHC oils
Complications
Weight loss in adults and other consequences of malnutrition such as increased susceptibility to infections, and increased morbidity and mortality from various disease states. Additionally, in children, malnutrition results in growth failure and poor neurological development
Deficiencies of fat-soluble vitamins (A, D, E, and K)
Poor bone health resulting in osteopenia, osteoporosis, and fractures (CF, celiac disease)
Iron deficiency anemia, zinc deficiency (celiac disease)
Dermatitis herpetiformis, non-Hodgkin lymphoma, adenocarcinoma of the upper gastrointestinal tract (celiac disease)
Megaloblastic anemia due to B12 deficiency (in terminal ileum disease and SIBO)
How do you get rid of chronic diarrhea?/Chronic diarrhea is defined as the passage of loose or liquid stools, watery stools three or more times a day for at least 4 weeks, and urgent need to evacuate or feelings of abdominal discomfort, or increased frequency of these, lasting more than 4 weeks.[rx,rx] Stool consistency is determined by the relationship between fecal water and the water-holding capacity of insoluble fecal solids. As stools consist predominantly of water (60–85%), consistency is difficult to quantify, and for this reason, stool weight is used as a reasonable indirect estimation of consistency. Diarrhea, therefore, can be defined by the weight or volume of stools measured over 24–72h (on average, 2–3 days). The normal weight of stool output over a 24-h period in children and adults is less that 200g; thus, stool weight >200g/24h is an objective definition of diarrhoea. However, it is important to note that up to 20% of patients with liquid diarrhoea, and thus a lower stool weight, are excluded from this definition.
Diarrhea that lasts for more than 2-4 weeks is considered persistent or chronic. In an otherwise healthy person, chronic diarrhea can be a nuisance at best or become a serious health issue. For someone who has a weakened immune system, chronic diarrhea may represent a life-threatening illness.
Types of Chronic Diarrhea
Chronic diarrhea is extremely broad. Categorizing the type of diarrhea will help to narrow down the underlying cause.[rx]
Watery Diarrhea
Osmotic diarrhea
Osmotic laxative use (magnesium, phosphate, or sulfate ingestion)
The most commonly recognized definition of diarrhea is based on World Health Organization parameters and
define diarrhea by the passage of 3 or looser than normal stools in the preceding 24-hour period. An episode
of diarrhea is defined as lasting 1 day or more and usually ends after at least 2 days without diarrhea.
Acute diarrhea
Episode of self-limiting diarrhea with acute onset, typically lasting 5 to 7 days. In most cases, it is due to an
intestinal infection and may be combined to fever and vomiting, meeting the definition of acute gastroenteritis.
Acute diarrhea may be also related to extra-intestinal infections (i.e. urinary infection, viral respiratory
infections), food-poisoning, iatrogenic intestinal damage (i.e. chemotherapy, radiotherapy) or other intestinal
and extra-intestinal diseases such as acute appendicitis.
Prolonged diarrhea
Acute onset diarrhea lasting from 7 to 14 days not covering the definition of persistent diarrhea. It is usually
due to persistent infections or to post-infectious intestinal damage (i.e. carbohydrate malabsorption, small
intestine bacterial overgrowth) that may prolong the duration of diarrhea behind the expected time.
Some experts refer to this as acute-protracted diarrhea.
Persistent diarrhea
Diarrhea lasting 14 days or more, usually associated with weight loss, ultimately leading to severe nutritional
impairment and that may require clinical nutrition.
The classical definition of persistent diarrhea was intended to exclude some causes of chronic diarrhea such
as celiac disease or inflammatory bowel diseases.
Chronic diarrhea
In many contexts chronic diarrhea is a synonymous of persistent diarrhea. The World Health Organization
uses this definition rather than persistent diarrhea.
However, chronic diarrhea usually does not have an acute onset and is the manifestation of structural and
inflammatory bowel disorders.
Some experts refer to chronic diarrhea in case of episodes lasting more than 4 weeks.
Post-infectious diarrhea
Acute onset diarrhea lasting 7 to 14 days and following an episode of acute gastroenteritis. This definition is
covered by prolonged diarrhea.
Intractable diarrhea
Non-infectious diarrhea lasting more than 14 days, intractable despite extensive hospital therapy.
Typical of young infants, usually below 3 months (but not only). Typically needs intravenous fluids or clinical
nutrition and is related to high mortality.
Congenital diarrhea
Congenital diarrhea is an inherited enteropathy with a typical onset early in life. For many of these conditions,
severe chronic diarrhea represents the main clinical manifestation, while in others, diarrhea is only a
component of a more complex multi-organ or systemic disease.
[stextbox id=’custom’]
Classification of chronic diarrhoea.
Chronic watery diarrhoea
1. Osmotic
Osmotic laxatives (Mg+2, PO−, SO4−2)
Carbohydrate malabsorption
Excessive consumption of poorly absorbed carbohydrates
Common diseases and disorders that cause chronic diarrhea include
Infections of the digestive tract – Infections from harmful viruses, bacteria, or parasites sometimes lead to chronic diarrhea. Children may become infected through contaminated water, beverages, or food; or through person-to-person contact. After infection, some children have problems digesting carbohydrates such as lactose or proteins in foods such as milk, milk products, or soy. These problems can cause prolonged diarrhea—often for up to 6 weeks—after an infection. Also, some bacterial and parasitic infections that cause diarrhea do not go away quickly without treatment.
Celiac disease – Celiac disease is a digestive disorder that damages the small intestine. The disease is triggered by eating foods containing gluten. Gluten is a protein found naturally in wheat, barley, and rye. Gluten is common in foods such as bread, pasta, cookies, and cakes. Celiac disease can cause chronic diarrhea in children of any age.
Functional GI disorders – In functional GI disorders, symptoms are caused by changes in how the digestive tract works. Children with a functional GI disorder have frequent symptoms, yet the digestive tract does not become damaged. Functional GI disorders are not diseases; they are groups of symptoms that occur together. Two functional GI disorders that cause chronic diarrhea in children are toddler’s diarrhea and irritable bowel syndrome (IBS).
Toddler’s diarrhea – also called functional diarrhea, or chronic nonspecific diarrhea of childhood—is a common cause of chronic diarrhea in toddlers (ages 1 to 3), and preschool-age children (ages 3 to 5). Children with toddler’s diarrhea pass four or more watery or loose stools a day and do not have any other symptoms. They typically are growing well, gaining weight, and are healthy. Toddler’s diarrhea develops between the ages of 6 months and 3 years, and it usually goes away on its own by the time children begin grade school. Researchers think that drinking too many sugar-sweetened beverages, especially those high in high-fructose corn syrup and sorbitol, may cause a toddler’s diarrhea.
IBS – The most common symptoms of IBS are abdominal pain, discomfort, or cramping; with diarrhea, constipation, or both. The pain or discomfort of IBS typically gets better with the passage of stool or gas. IBS does not cause symptoms such as weight loss, vomiting, or blood in the stool. IBS is a common cause of chronic diarrhea in grade school-age children and adolescents. Doctors rarely diagnose IBS in younger children because younger children are not able to report symptoms of IBS such as abdominal pain or discomfort.
Food allergies and intolerances – Food allergies, lactose intolerance, fructose intolerance, and sucrose intolerance are common causes of chronic diarrhea.
Food allergies – Milk, milk products, and soy allergies are the most common food allergies that affect the digestive tract in children. Food allergies usually appear in the first year of life. Many children outgrow allergies to milk, milk products, and soy by age 3. Allergies to other foods such as cereal grains, eggs, and seafood may also affect the digestive tract in children.
Lactose intolerance – Lactose intolerance is a common condition that may cause diarrhea after eating foods or drinking beverages that contain milk or milk products. Low levels of lactase—the enzyme that helps digest lactose—or lactase deficiency, and malabsorption of lactose cause lactose intolerance. The most common type of lactase deficiency in children develops over time, beginning after about age 2, when a child’s body begins to produce less lactase. Children who have lactase deficiency may not experience symptoms of lactose intolerance until they become older teenagers or adults. Infants—newborns to age 1—rarely have lactose intolerance at birth. However, premature infants may experience lactose intolerance for a short time after birth. People sometimes mistake milk allergy, which can cause diarrhea in infants, for lactose intolerance.
Fructose intolerance – Fructose intolerance is a condition that may cause diarrhea after eating foods or drinking beverages that contain fructose, a sugar found in fruits, fruit juices, and honey. Fructose is added to many foods and soft drinks as a sweetener called high-fructose corn syrup. Fructose malabsorption causes fructose intolerance. The amount of fructose that a child’s body can absorb varies. A child’s ability to absorb fructose increases with age. Some children may be able to tolerate more fructose as they get older.
Sucrose intolerance – Sucrose intolerance is a condition that may cause diarrhea after eating foods or drinking beverages that contain sucrose, also known as table sugar or white sugar. Sucrose malabsorption causes sucrose intolerance. Children who are sucrose intolerant lack the enzyme that helps digest sucrose. Most children with sucrose intolerance are better able to tolerate sucrose as they get older.
Inflammatory bowel disease (IBD) – The two main types of IBD are Crohn’s disease and ulcerative colitis. These disorders can affect children at any age. However, they commonly begin in the grade school years or in adolescence.
Small intestinal bacterial overgrowth (SIBO) – SIBO is an increase in the number of bacteria or a change in the type of bacteria in your small intestine. SIBO is often related to diseases that damage the digestive system such as Crohn’s disease.
Irritable Bowel Syndrome (IBS) – This is defined as chronically abnormal bowel habits (diarrhea and/or constipation) associated with abdominal pain in the absence of any pathology. Females are more likely to be diagnosed with IBS than males. Symptoms of IBS are usually worsened by stress. The symptoms are generally described as crampy lower abdominal pain with associated diarrhea, constipation, or alternating diarrhea and constipation. Symptoms are often alleviated by defecation, although this is not necessary for diagnosis. For patients with diarrhea, usually describe their bowel movements as being small or moderate amounts of loose stool. Usually, bowel movements are associated with urgency.[rx]
Medications – Certain medications are known to induce diarrhea in patients. Currently, there are greater than 700 drugs that are associated with diarrhea. Medical practitioners must look to the addition of new medications which may be associated with diarrhea. When the offending agent is discontinued, diarrhea may stop within as little as a day but may take longer if there is an injury to the intestinal mucosa. Patients who are receiving chemotherapy can have diffuse or segmental colitis. [rx] Olmesartan producing a sprue-like enteropathy was first described in 2012. In this disease state, the intestinal mucosa will mimic the findings of celiac sprue, but the patients are not actually insensitive to gluten.[rx]
Crohn Disease – Crohn’s disease is an inflammatory bowel disease that is an autoimmune disease.[rx] Typical symptoms include diarrhea (often associated with blood and/or mucus), abdominal pain, and signs of bowel obstructions. Perirectal fistulas may be present on the exam which may help to clue the physician into the diagnosis. Although this disease can present anywhere in the gastrointestinal tract, it most commonly affects the terminal ileum.[rx]
Ulcerative Colitis – Ulcerative colitis is the other major component of inflammatory bowel disease. This disease has an unknown etiology. Patients often present with abdominal pain, diarrhea, and hematochezia. Other signs that may aid diagnosis are weight loss and pallor secondary to anemia.[rx]
Microscopic Colitis – This is a common cause of chronic watery diarrhea. There are two subtypes of microscopic colitis: collagenous and lymphocytic colitis. It is diagnosed based on an endoscopic biopsy.[rx]
Celiac Disease – This disease process occurs in individuals who develop an immune-mediated reaction triggered by the ingestion of gluten. Celiac disease occurs in only about 1% of the population, but the incidence is rising. Symptoms include abdominal cramping, diarrhea, and weight loss. Diagnosis requires a biopsy of the intestine showing villous atrophy. Most patients will produce the antibody against tissue transglutaminase.[rx]
Chronic Pancreatitis – Pancreatic enzymes are essential for the proper digestion of fats, proteins, and carbohydrates. Patients with chronic pancreatitis will develop recurrent bouts of acute pancreatitis and chronic abdominal pain. Chronic pancreatitis will eventually lead to scarring and fibrosis of the pancreas, which will decrease the number of pancreatic enzymes, and malabsorption. This will lead to steatorrhea and weight loss.[rx]
Lactose Intolerance – The ability to digest lactose comes from an enzyme present in the intestine called lactase. This allows the lactose to be broken down into simple sugar and be absorbed. When this enzyme is absent, the lactose is not able to be absorbed by the intestine. This will increase the osmolality within the lumen of the intestine producing watery diarrhea shortly after the ingestion of lactose-containing foods.[rx]
Malabsorption Syndromes – This term is very nonspecific and encompasses any disorder where the intestine has a decreased ability to absorb nutrients while not requiring intravenous supplementation for health and/or growth.[rx]
Post-cholecystectomy Diarrhea – Diarrhea after a cholecystectomy occurs in up to 12% of patients. Over time, symptoms generally resolve on their own without intervention.[rx] Since the gallbladder is removed, the bile produced by the liver directly enters the colon instead of being stored. The increased amount of bile acids in the colon produces diarrhea.[rx]
Chronic Infections – Certain long-lasting infections of the gastrointestinal tract can be linked to chronic diarrhea. A few of these infections include C. difficile, Vibrio cholera, Salmonella, Shigella, Entamoeba histolytica, E. Coli, Giardia, Cryptosporidium, Whipple Disease, and Cyclospora.[rx] A clinician should always have a suspicion of an infectious cause of diarrhea. Risk factors include travel and immunosuppression.
Symptoms of Chronic Diarrhea
The main symptom of chronic diarrhea is passing loose, watery stools three or more times a day for at least 4 weeks.
Depending on the cause, children with chronic diarrhea may also have one or more of the following symptoms:
bloody stools
chills
fever
loss of control of bowel movements
nausea or vomiting
pain or cramping in the abdomen
Chronic diarrhea may cause malabsorption and may lead to dehydration.
Chronic diarrhoea: signs, symptoms and analytical findings suggestive of an organic cause.
Blood in stools
Fever
Recent weight loss (>5kg) (in absence of concomitant depression)
Recent onset of symptoms, or change in the characteristics of previous symptoms
Onset at an advanced age (≥50 years)
Family history of colorectal cancer or polyps
Nocturnal diarrhoea
Diarrhoea persists after fasting
High-volume stool output or steatorrhoea
Weight of stool output over 24h >400g/day
Abnormalities on physical examination (pallor, hepatosplenomegaly, adenopathies, abdominal mass, etc.)
Anaemia, macrocytosis, hypoprothrombinaemia, hypoalbuminaemia or other laboratory findings (e.g. elevated ESR or C-reactive protein)
The infection often starts suddenly with projectile vomiting or severe diarrhea. It is considered to be diarrhea if you have more than three very loose or liquid bowel movements within 24 hours. People who have diarrhea often have a stomach aches, cramps, and bloating too. Diarrhea and nausea are sometimes also accompanied by fever, headache, and joint pain. Dizziness and feeling faint could be signs that your body has lost too much liquid and salts (electrolytes). If that happens, immediate medical attention is needed. Other reasons to seek medical help for diarrhea include:
No improvement after 48 hours
High fever
Blood in your poo (it has red blood in it or is black)
The mucous coating on the poo
Severe pain
Diagnosis of Chronic Diarrhea
When you see the doctor you will first be asked
whether your symptoms started suddenly or gradually,
what your poo looks like (consistency and appearance),
how long and how frequently you have had diarrhea,
whether you also have symptoms such as stomach ache, vomiting or fever, and
what you had to eat before getting diarrhea.
It is also important for them to know
whether you have been traveling recently,
what medications you were or are taking,
whether you have any diagnosed allergies or intolerances, and
whether you have a chronic disease, such as diabetes.
If you have bloody or persistent diarrhea, a sample of your stool (poo) or blood may be needed to find out what kind of infection you have. The same applies if there is mucus in diarrhea.
Your doctor will ask about your medical history, symptoms, and any medicines you take. Your doctor will also perform a physical exam and may order an upper gastrointestinal (GI) endoscopy with biopsies or other tests.
History and physical exam vary widely from patient to patient depending on the severity and etiology of the disease. The physical exam is often normal in patients with chronic diarrhea; however, signs of unintentional weight loss points towards a more severe disease. Although history and physical exam will rarely lead to a specific cause of chronic diarrhea, it is an integral part of any patient encounter. It is important to have the patient describe their diarrhea. Specific descriptions such as hematochezia, mucus in the stool, or steatorrhea help narrow the differential diagnosis greatly. Some specific physical exam signs may clue the examiner towards a diagnosis.
For all patients complaining of chronic diarrhea, a thorough history and physical exam are necessary. The following laboratory testing should also take place for every patient with chronic diarrhea:
Complete blood count with differential to examine for infection and anemia
Erythrocyte sedimentation rate and C-reactive protein to look for infections
Thyroid function tests to screen for hyperthyroidism
Complete metabolic profile to search for electrolyte abnormalities, renal function
Total protein and albumin to look for signs of protein malnutrition
Stool occult blood to look for a gastrointestinal bleed
If the patient has any alarming symptoms, a referral for an endoscopy is necessary. Alarm symptoms include
Symptom onset after age 50
Rectal bleeding/melena
Nocturnal pain or diarrhea
Progressive abdominal pain
Unexplained weight loss, fever, or other systemic symptoms
Laboratory abnormalities such as iron deficiency anemia, elevated ESR/CRP, elevated fecal calprotectin, or fecal occult blood
First degree relative with inflammatory bowel disease or colorectal cancer
If patients do not have alarming symptoms, stool laboratory assessment is a recommendation. If the patient has recent antibiotic use, checking the stool for C. difficile toxin is warranted; C. difficile toxin should be reviewed on all patients with chronic diarrhea, regardless of antibiotic use, if their diarrhea classically fits the description of C. difficile: watery diarrhea occurring 3 or more times per day.
When categorizing the stool, it is essential to check for the following labs:
Stool electrolytes
Fecal leukocytes (fecal lactoferrin or fecal calprotectin are a substitute in place of fecal leukocytes)
Fecal chymotrypsin and elastase
Occult blood
Stool fat (48 to 72 hour timed collection is ideal)
While chronic diarrhea has a very broad differential diagnosis, categorizing the stool can help narrow down the list. Fecal leukocytes/calprotectin/lactoferrin are markers of inflammation. The presence of these markers will point towards inflammatory diarrhea, such as Crohn’s disease, or ulcerative colitis.
Fecal chymotrypsin and elastase are pancreatic enzymes that can present in the stool in the setting of pancreatic insufficiency. These two tests do not definitively diagnose pancreatic insufficiency. If these are positive on stool testing, the physician should check blood tests for pancreatic enzymes, and potentially refer to a gastroenterologist for further studies.
For patients with watery diarrhea, stool electrolytes will further categorize their diarrhea into either osmotic diarrhea or secretory diarrhea based on the calculation of the stool osmotic gap. The calculation is as follows:
290 mOsm/kg – 2(Na[feces]+K[feces])
If the result of the above formula is less than 50 mOsm/kg, then the diarrhea is secretory. If the result is greater than 75 mOsm/kg, then the diarrhea is osmotic.[rx]
Lab Test
Upper GI endoscopy – Upper GI endoscopy is a procedure in which a doctor uses an endoscope—a flexible tube with a camera—to see the lining of your upper GI tract, including your esophagus, stomach, and duodenum. During upper GI endoscopy, a doctor obtains biopsies by passing an instrument through the endoscope to take small pieces of tissue from your stomach lining. A pathologist will examine the tissue with a microscope. Doctors may use upper GI endoscopy to diagnose gastritis or gastropathy, determine the cause, and manage complications.
Blood tests – Doctors may use blood tests to check for other causes of gastritis or signs of complications. For a blood test, a health care professional will take a blood sample from you and send the sample to a lab.
Stool tests – Doctors may use stool tests to check for H. pylori infection and for blood in your stool, a sign of bleeding in your stomach.
Timed stool collection – Neither patients nor laboratory technicians relish in the timed stool test (48–72 hrs of stool collection; normal stool weight is 200g/24 hrs with less than 7g fat), yet this is the standard for assessing steatorrhea. A fresh stool sample is necessary to differentiate secretory from osmotic diarrhea. Stool weight greater than 1000g/24 hrs leads to a different diagnostic approach (a search for a possible neuroendocrine cause) than a value of 300g/24 hrs. Approximately 25% of patients referred specifically for a diarrhea evaluation actually have normal stool weight (Sellin J, unpublished observations). The 48 hr stool collection test can also be used to measure fecal bile acids.[rx]
Blood tests for neuroendocrine tumors – hormone-secreting tumors are rare causes of secretory diarrhea, typically detected by measuring serum levels of chromogranin, gastrin, vasoactive intestinal polypeptide, or calcitonin, as well as urine level of 5-hydroxy indole acetic acid. However, due to the rarity of these tumors and low pretest probability, many positive results from these tests (especially borderline results) turn out to be false positives.[rx] These tests should therefore almost never be considered early in the course of an evaluation.
Urea breath test – Doctors may use a urea breath test to check for H. pylori infection. For the test, you will swallow a capsule, liquid, or pudding that contains urea that is “labeled” with a special carbon atom. If H. pylori is present, the bacteria will convert the urea into carbon dioxide. After a few minutes, you will breathe into a container, exhaling carbon dioxide. A health care professional will test your exhaled breath. If the test detects the labeled carbon atoms, the health care professional will confirm an H. pylori infection in your digestive tract.
Upper GI series – Doctors may use an upper GI series to check for signs of gastritis or gastropathy. An upper GI series is a procedure in which a doctor uses x-rays and a chalky liquid called barium to view your upper GI tract.
MR enterography – is recommended for evaluation of small bowel abnormalities depending on availability (Grade of evidence level 1, Strength of recommendation strong).
Video capsule endoscopy (VCE) – is recommended for assessing small bowel abnormalities depending on local availability (Grade of evidence level 1, Strength of recommendation strong).
Small bowel barium follow-through or barium enteroclysis – for the evaluation of small bowel abnormalities due to its poor sensitivity and specificity (Grade of evidence level 5, Strength of recommendation strong).
Fecal elastase testing – when fat malabsorption is suspected. We do not recommend PABA testing (Grade of evidence level 1, Strength of recommendation strong).
MRI (rather than CT) – is recommended for assessing structural anomalies of the pancreas in suspected chronic chronic diarrhea (Grade of evidence level 2, Strength of recommendation strong).
Treatment for Chronic Diarrhea
How doctors treat chronic diarrhea depends on the cause. Doctors may be able to reduce or stop chronic diarrhea by treating the cause.
A bland ‘BRAT’ diet including bananas, toast, oatmeal, white rice, applesauce, and soup/broth is well tolerated and may improve symptoms. [rx] Anti-diarrheal therapy with anti-secretory or anti-motility agents may be started to reduce the frequency of stools.
Non Pharmacological
Food allergies – If your child has a food allergy, his or her doctor will recommend avoiding foods that trigger the allergy. Keeping a diary of what your child eats and drinks and his or her bowel habits will help your child’s doctor find out what foods trigger the allergy.
Lactose intolerance – If your is lactose intolerant, his or her doctor will recommend reducing or avoiding foods and beverages that contain milk or milk products. Most with lactose intolerance can tolerate some amount of lactose in what they eat or drink. The amount of change needed in what a child eats or drinks depends on how much lactose a child can consume without symptoms. Your child’s doctor may recommend dietary supplements that contain lactase, the enzyme that helps digest lactose. Your child’s doctor may also recommend calcium supplements.
Fructose intolerance – If is fructose intolerant, will recommend reducing or avoiding foods and beverages that contain fructose.
Sucrose intolerance – If is sucrose intolerant, his or her doctor will recommend reducing or avoiding foods and beverages that contain sucrose.
Medication
Drugs used in Treatment of Chronic Watery Diarrhea
Drug class
Agent
Dose
Opiates (μ-opiate receptor-selective)
Diphenoxylate
2.5–5 mg, 4 times/day
Loperamide
2–4 mg, 4 times/day
Codeine
15–60 mg, 4 times/day
Opium tincture
2–20 drops, 4 times/day
Morphine
2–20 mg, 4 times/day
Eluxadoline
100 mg twice daily (μ-opioid agonist and δ-opioid antagonist) for IBS-D
Adrenergic α2 receptor agonist
Clonidine
0.1–0.3 mg 3 times/day; Weekly patch
Somatostatin analog
Octreotide
50–250 μg 3 times/day (subcutaneously)
Bile acid-binding resin
Cholestyramine
4 g daily or up to 4 times/day
Colestipol
4 g daily or up to 4 times/day
Colesevelam
1875 mg up to twice daily
Fiber supplements
Calcium polycarbophil
5–10 g daily
Psyllium
10–20 g daily
Soluble fiber
Pectin
2 capsules before meals
Calcium
1000 mg twice or 3 times daily
Serotonin 5-HT3 receptor antagonists
Alosetron
0.5–1.0 mg twice daily
Ondansetron
2–8 mg twice daily
Azithromycin – in a single dosage 0r ciprofloxacillin in a double dosage for 7 days . In a randomized trial, Azithromycin was found to be clinically and bacteriological successful in 82% and 94% of patients treated respectively.[rx] Cefixime and ceftibuten can be used as first-line to treat in due to widespread resistance to commonly used antibiotics.[rx] The alternative regimen includes pivmecillinam, an extended-spectrum penicillin is effective in decreasing diarrhea duration and eradication of chronic diarrhea organisms in the stool.[rx][rx]
Loperamide – is a safe mu-receptor agonist used to decrease gut peristalsis. Loperamide is a safe mu-receptor agonist used to decrease gut peristalsis and decrease the gut motility. Loperamide is not suitable for children under the age of twelve years, and racecadotril is prescription-only for children.
Nitazoxanide – is a broad-spectrum antimicrobial agent with activity against protozoa, nematodes, cestodes, trematodes, and bacteria, with a favorable safety profile [rx, rx]. It is effective in childhood cryptosporidiosis [rx] but not consistently in undernourished children or in HIV-infected patients [rx]. Anecdotal cases of children successfully treated with nitazoxanide because of PD (<30 days) have been reported [rx]. This strategy seems to be effective in select situations, saving time-consuming tests to identify the cause of diarrhea [rx].
Cholestyramine – Other medications used for chronic diarrhea include bile acid-binding resins such as cholestyramine. Clonidine is an alpha2-adrenergic agonist that also slows the intestinal tract, and is an option for diarrhea secondary to opioid withdrawal as well as diarrhea secondary to loss of noradrenergic innervation in patients with diabetes. The use of this medication has limitations due to the antihypertensive effect. However, this medication may be useful for patients with hypertension and chronic diarrhea.
Ceftriaxone – Intra venous or parenteral antibiotics are indicated in children with suspected and proven chronic diarrhoea who have a severe infection with signs of bacteremia including lethargy, temperature >39° C (102.2°F), underlying immune deficiency including AIDS and those unable to take oral medications.[rx] Ceftriaxone is recommended as a single dose or for five days.
Anticholinergic medications – can be used to treat diarrhea as well. Tricyclic antidepressants which are used to treat depression or pain can also treat diarrhea.[rx]
Immunoglobulin – available for intravenous use, may be administered orally (300 mg/kg of body weight) in a single dose. The rationale of passive immunotherapy is based on the demonstration of neutralizing antibodies against all viruses in a medical preparation of immunoglobulins [rx].
Cholestyramine – Other medications used for chronic diarrhea include bile acid-binding resins such as cholestyramine. Clonidine is an alpha2-adrenergic agonist that also slows the intestinal tract, and is an option for diarrhea secondary to opioid withdrawal as well as diarrhea secondary to loss of noradrenergic innervation in patients with diabetes. The use of this medication has limitations due to the antihypertensive effect. However, this medication may be useful for patients with hypertension and chronic diarrhea.
Yeast tablets – Sometimes certain types of yeast tablets (Perenterol) are recommended. These tablets are thought to help the body get rid of germs faster and to support natural gut flora. Charcoal tablets dissolved in water can also be taken to relieve diarrhea symptoms. But there’s a lack of good-quality research in this area so no conclusions can be drawn about the benefits and harms of these treatment options. People who are very ill or have a very weak immune system shouldn’t take yeast tablets.
Zinc supplementation – is reported to reduce both the stool volume and stool frequency by 30 percent and is a consideration in severe cases.[rx] Although diets such as BRAT (banana, rice, apple, and toast) or bland diet have been proposed to improve the condition and are somewhat better tolerated; no reliable data or prospective studies are available to confirm this, and the assumptions are mostly based on limited studies or personal experiences.
Foods to avoid
Fried and greasy foods are usually not well-tolerated in people who have diarrhea. You should also consider limiting high-fiber foods like bran as well as fruits and vegetables that can increase bloating. Foods to avoid include:
alcohol
artificial sweeteners (found in chewing gum, diet soft drinks and sugar substitutes)
beans
berries
broccoli
cabbage
cauliflower
chickpeas
coffee
corn
ice cream
green leafy vegetables
milk
peas
peppers
prunes
tea
Foods to eat
While it might sound counterintuitive to eat if you have diarrhea, eating certain foods can help alleviate your diarrhea symptoms and ensure your health doesn’t worsen from not eating. Stick to low-fiber “BRAT” foods that will help firm up your stool. These include:
bananas
rice (white)
applesauce
toast
Other foods that are usually well-tolerated when experiencing diarrhea include:
oatmeal
boiled or baked potatoes (with skins peeled)
baked chicken with skin removed
chicken soup (which also aids in rehydration)
Probiotics
Probiotics are sources of “good” bacteria that work in your intestinal tract to create a healthy gut environment. They’re essentially live microorganisms that exist in certain foods, including:
aged soft cheeses
beet kvass
cottage cheese
dark chocolate
green olives
kefir
kimchi
kombucha
sauerkraut
miso
natto
pickles
sourdough bread
tempeh
yogurt
Probiotics also come in powder or pill form.
The good bacteria that live in your intestinal tract are necessary for the normal functioning of your gastrointestinal system. They play an important role in protecting your intestines against infection. When your system is changed by antibiotics or overwhelmed by unhealthy bacteria or viruses, you can get diarrhea. Probiotics can help with diarrhea by restoring the balance of bacteria in your gut.
Saccharomyces boulardii is a yeast probiotic. While it’s not a bacterium, it acts like one. S. boulardii may improve antibiotic-associated diarrhea. It also seems to provide relief for traveler’s diarrhea. It may help your intestines fight off unwanted pathogens and ensure they’re absorbing nutrients properly. Because it is yeast, it should be used with caution in people with inadequate immune systems.
Prevention
Viruses and bacteria can spread through contact with poo, vomit, and contaminated objects, water, or food.
This means that it is very important to frequently wash your hands thoroughly with soap if you have acute diarrhea, in order to protect others from infection. Washing your hands also protects you from infection if someone you know is infected. A hand disinfectant can help too. If you have a second bathroom at home, whoever is ill can be the only one to use it.
Clothes should be washed at temperatures above 60 degrees Celsius (about 140 degrees Fahrenheit) if possible. It is important to pay attention to hygiene in the kitchen and while preparing food. Anyone with acute diarrhea shouldn’t prepare food for others.
When traveling to tropical or subtropical climates, you may need to avoid uncooked, unpeeled fruit and vegetables and not drink tap water. Don’t eat undercooked meat or fish.
keeping a food diary and seeing how cutting particular foods from the diet affect the diarrhea
discussing the side effects of any current medications with a doctor
requesting a change in medications if necessary
taking probiotic supplements regularly
drinking only clean or filtered water
washing the hands both before and after food preparation
cleaning and thoroughly cooking meat before eating it
washing fresh produce before eating it
cleaning kitchen surfaces regularly
washing the hands regularly, especially after using the bathroom or coming into contact with a person who is ill
Complications
Complications of shigella infection include intestinal and systemic complications listed below. [rx]
Intestinal Complications
Colon perforation – Very rare and primarily occurs in infants and malnourished patients. It is associated with S. flexneri and S. dysenteriae 1. [rx]
Intestinal obstruction – usually seen in severe disease and S. dysenteriae 1.[rx]
Toxic megacolon – Usually occurs in S. dysenteriae 1 infection.[rx]
Proctitis or rectal prolapse – Invasion of shigella organisms into colonic mucosa can lead to rectal prolapse and proctitis in infants and young children.[rx]
Bacteremia – Common in young children under the age of 5.[rx][rx][rx]
Hemolytic-uremic syndrome – Although uncommon, HUS is the most frequent acute kidney injury in young children and infants.[rx]
Moderate to severe hypovolemia
Hyponatremia – Usually associated with S. dysenteriae 1 infection.[rx]
Leukemoid reaction – Common in children between ages 2-10 years old.[rx]
Neurologic symptoms – Generalized seizures are the most common neurologic complication. This is usually associated with a higher mortality rate.[rx][rx]
Reactive arthritis or Reiter syndrome – Uncommon sterile inflammatory arthritis. It is usually caused by S. flexneri infection. Arthritis can occur alone or in conjunction with conjunctivitis and urethritis.[rx]
Vulvovaginitis – with or without diarrhea-Seen in young girls associated with painless vaginal discharge.[rx]
Keratitis – Rare but should be considered in a young child with keratitis and a history of recent diarrheal illness. [rx]
Acute myocarditis – Seen in children with S. Sonnei infection.[rx]
Weight loss – in adults and other consequences of malnutrition such as increased susceptibility to infections, and increased morbidity and mortality from various disease states. Additionally, in children, malnutrition results in growth failure and poor neurological development
Deficiencies of fat-soluble vitamins (A, D, E, and K)
Poor bone health resulting in osteopenia, osteoporosis, and fractures (CF, celiac disease)
Iron deficiency anemia, zinc deficiency (celiac disease)
Dermatitis herpetiformis, non-Hodgkin lymphoma, adenocarcinoma of the upper gastrointestinal tract (celiac disease)
Megaloblastic anemia due to B12 deficiency (in terminal ileum disease and SIBO)
Chronic diarrhea is defined as the passage of loose or liquid stools, watery stools three or more times a day for at least 4 weeks and urgent need to evacuate or feelings of abdominal discomfort, or increased frequency of these, lasting more than 4 weeks.[rx,rx] Stool consistency is determined by the relationship between faecal water and the water-holding capacity of insoluble faecal solids. As stools consist predominantly of water (60–85%), consistency is difficult to quantify, and for this reason stool weight is used as a reasonable indirect estimation of consistency. Diarrhoea, therefore, can be defined by the weight or volume of stools measured over 24–72h (on average, 2–3 days). The normal weight of stool output over a 24-h period in children and adults is less that 200g; thus, stool weight >200g/24h is an objective definition of diarrhoea. However, it is important to note that up to 20% of patients with liquid diarrhoea, and thus a lower stool weight, are excluded from this definition.
Diarrhea that lasts for more than 2-4 weeks is considered persistent or chronic. In an otherwise healthy person, chronic diarrhea can be a nuisance at best or become a serious health issue. For someone who has a weakened immune system, chronic diarrhea may represent a life-threatening illness.
Types of Chronic Diarrhea
Chronic diarrhea is extremely broad. Categorizing the type of diarrhea will help to narrow down the underlying cause.[rx]
Watery Diarrhea
Osmotic diarrhea
Osmotic laxative use (magnesium, phosphate, or sulfate ingestion)
The most commonly recognized definition of diarrhea is based on World Health Organization parameters and
define diarrhea by the passage of 3 or looser than normal stools in the preceding 24-hour period. An episode
of diarrhea is defined as lasting 1 day or more and usually ends after at least 2 days without diarrhea.
Acute diarrhea
Episode of self-limiting diarrhea with acute onset, typically lasting 5 to 7 days. In most cases, it is due to an
intestinal infection and may be combined to fever and vomiting, meeting the definition of acute gastroenteritis.
Acute diarrhea may be also related to extra-intestinal infections (i.e. urinary infection, viral respiratory
infections), food-poisoning, iatrogenic intestinal damage (i.e. chemotherapy, radiotherapy) or other intestinal
and extra-intestinal diseases such as acute appendicitis.
Prolonged diarrhea
Acute onset diarrhea lasting from 7 to 14 days not covering the definition of persistent diarrhea. It is usually
due to persistent infections or to post-infectious intestinal damage (i.e. carbohydrate malabsorption, small
intestine bacterial overgrowth) that may prolong the duration of diarrhea behind the expected time.
Some experts refer to this as acute-protracted diarrhea.
Persistent diarrhea
Diarrhea lasting 14 days or more, usually associated with weight loss, ultimately leading to severe nutritional
impairment and that may require clinical nutrition.
The classical definition of persistent diarrhea was intended to exclude some causes of chronic diarrhea such
as celiac disease or inflammatory bowel diseases.
Chronic diarrhea
In many contexts chronic diarrhea is a synonymous of persistent diarrhea. The World Health Organization
uses this definition rather than persistent diarrhea.
However, chronic diarrhea usually does not have an acute onset and is the manifestation of structural and
inflammatory bowel disorders.
Some experts refer to chronic diarrhea in case of episodes lasting more than 4 weeks.
Post-infectious diarrhea
Acute onset diarrhea lasting 7 to 14 days and following an episode of acute gastroenteritis. This definition is
covered by prolonged diarrhea.
Intractable diarrhea
Non-infectious diarrhea lasting more than 14 days, intractable despite extensive hospital therapy.
Typical of young infants, usually below 3 months (but not only). Typically needs intravenous fluids or clinical
nutrition and is related to high mortality.
Congenital diarrhea
Congenital diarrhea is an inherited enteropathy with a typical onset early in life. For many of these conditions,
severe chronic diarrhea represents the main clinical manifestation, while in others, diarrhea is only a
component of a more complex multi-organ or systemic disease.
[stextbox id=’custom’]
Classification of chronic diarrhoea.
Chronic watery diarrhoea
1. Osmotic
Osmotic laxatives (Mg+2, PO−, SO4−2)
Carbohydrate malabsorption
Excessive consumption of poorly absorbed carbohydrates
Common diseases and disorders that cause chronic diarrhea include
Infections of the digestive tract – Infections from harmful viruses, bacteria, or parasites sometimes lead to chronic diarrhea. Children may become infected through contaminated water, beverages, or food; or through person-to-person contact. After infection, some children have problems digesting carbohydrates such as lactose or proteins in foods such as milk, milk products, or soy. These problems can cause prolonged diarrhea—often for up to 6 weeks—after an infection. Also, some bacterial and parasitic infections that cause diarrhea do not go away quickly without treatment.
Celiac disease – Celiac disease is a digestive disorder that damages the small intestine. The disease is triggered by eating foods containing gluten. Gluten is a protein found naturally in wheat, barley, and rye. Gluten is common in foods such as bread, pasta, cookies, and cakes. Celiac disease can cause chronic diarrhea in children of any age.
Functional GI disorders – In functional GI disorders, symptoms are caused by changes in how the digestive tract works. Children with a functional GI disorder have frequent symptoms, yet the digestive tract does not become damaged. Functional GI disorders are not diseases; they are groups of symptoms that occur together. Two functional GI disorders that cause chronic diarrhea in children are toddler’s diarrhea and irritable bowel syndrome (IBS).
Toddler’s diarrhea – also called functional diarrhea, or chronic nonspecific diarrhea of childhood—is a common cause of chronic diarrhea in toddlers (ages 1 to 3), and preschool-age children (ages 3 to 5). Children with toddler’s diarrhea pass four or more watery or loose stools a day and do not have any other symptoms. They typically are growing well, gaining weight, and are healthy. Toddler’s diarrhea develops between the ages of 6 months and 3 years, and it usually goes away on its own by the time children begin grade school. Researchers think that drinking too many sugar-sweetened beverages, especially those high in high-fructose corn syrup and sorbitol, may cause a toddler’s diarrhea.
IBS – The most common symptoms of IBS are abdominal pain, discomfort, or cramping; with diarrhea, constipation, or both. The pain or discomfort of IBS typically gets better with the passage of stool or gas. IBS does not cause symptoms such as weight loss, vomiting, or blood in the stool. IBS is a common cause of chronic diarrhea in grade school-age children and adolescents. Doctors rarely diagnose IBS in younger children because younger children are not able to report symptoms of IBS such as abdominal pain or discomfort.
Food allergies and intolerances – Food allergies, lactose intolerance, fructose intolerance, and sucrose intolerance are common causes of chronic diarrhea.
Food allergies – Milk, milk products, and soy allergies are the most common food allergies that affect the digestive tract in children. Food allergies usually appear in the first year of life. Many children outgrow allergies to milk, milk products, and soy by age 3. Allergies to other foods such as cereal grains, eggs, and seafood may also affect the digestive tract in children.
Lactose intolerance – Lactose intolerance is a common condition that may cause diarrhea after eating foods or drinking beverages that contain milk or milk products. Low levels of lactase—the enzyme that helps digest lactose—or lactase deficiency, and malabsorption of lactose cause lactose intolerance. The most common type of lactase deficiency in children develops over time, beginning after about age 2, when a child’s body begins to produce less lactase. Children who have lactase deficiency may not experience symptoms of lactose intolerance until they become older teenagers or adults. Infants—newborns to age 1—rarely have lactose intolerance at birth. However, premature infants may experience lactose intolerance for a short time after birth. People sometimes mistake milk allergy, which can cause diarrhea in infants, for lactose intolerance.
Fructose intolerance – Fructose intolerance is a condition that may cause diarrhea after eating foods or drinking beverages that contain fructose, a sugar found in fruits, fruit juices, and honey. Fructose is added to many foods and soft drinks as a sweetener called high-fructose corn syrup. Fructose malabsorption causes fructose intolerance. The amount of fructose that a child’s body can absorb varies. A child’s ability to absorb fructose increases with age. Some children may be able to tolerate more fructose as they get older.
Sucrose intolerance – Sucrose intolerance is a condition that may cause diarrhea after eating foods or drinking beverages that contain sucrose, also known as table sugar or white sugar. Sucrose malabsorption causes sucrose intolerance. Children who are sucrose intolerant lack the enzyme that helps digest sucrose. Most children with sucrose intolerance are better able to tolerate sucrose as they get older.
Inflammatory bowel disease (IBD) – The two main types of IBD are Crohn’s disease and ulcerative colitis. These disorders can affect children at any age. However, they commonly begin in the grade school years or in adolescence.
Small intestinal bacterial overgrowth (SIBO) – SIBO is an increase in the number of bacteria or a change in the type of bacteria in your small intestine. SIBO is often related to diseases that damage the digestive system such as Crohn’s disease.
Irritable Bowel Syndrome (IBS) – This is defined as chronically abnormal bowel habits (diarrhea and/or constipation) associated with abdominal pain in the absence of any pathology. Females are more likely to be diagnosed with IBS than males. Symptoms of IBS are usually worsened by stress. The symptoms are generally described as crampy lower abdominal pain with associated diarrhea, constipation, or alternating diarrhea and constipation. Symptoms are often alleviated by defecation, although this is not necessary for diagnosis. For patients with diarrhea, usually describe their bowel movements as being small or moderate amounts of loose stool. Usually, bowel movements are associated with urgency.[rx]
Medications – Certain medications are known to induce diarrhea in patients. Currently, there are greater than 700 drugs that are associated with diarrhea. Medical practitioners must look to the addition of new medications which may be associated with diarrhea. When the offending agent is discontinued, diarrhea may stop within as little as a day but may take longer if there is an injury to the intestinal mucosa. Patients who are receiving chemotherapy can have diffuse or segmental colitis. [rx] Olmesartan producing a sprue-like enteropathy was first described in 2012. In this disease state, the intestinal mucosa will mimic the findings of celiac sprue, but the patients are not actually insensitive to gluten.[rx]
Crohn Disease – Crohn’s disease is an inflammatory bowel disease that is an autoimmune disease.[rx] Typical symptoms include diarrhea (often associated with blood and/or mucus), abdominal pain, and signs of bowel obstructions. Perirectal fistulas may be present on the exam which may help to clue the physician into the diagnosis. Although this disease can present anywhere in the gastrointestinal tract, it most commonly affects the terminal ileum.[rx]
Ulcerative Colitis – Ulcerative colitis is the other major component of inflammatory bowel disease. This disease has an unknown etiology. Patients often present with abdominal pain, diarrhea, and hematochezia. Other signs that may aid diagnosis are weight loss and pallor secondary to anemia.[rx]
Microscopic Colitis – This is a common cause of chronic watery diarrhea. There are two subtypes of microscopic colitis: collagenous and lymphocytic colitis. It is diagnosed based on an endoscopic biopsy.[rx]
Celiac Disease – This disease process occurs in individuals who develop an immune-mediated reaction triggered by the ingestion of gluten. Celiac disease occurs in only about 1% of the population, but the incidence is rising. Symptoms include abdominal cramping, diarrhea, and weight loss. Diagnosis requires a biopsy of the intestine showing villous atrophy. Most patients will produce the antibody against tissue transglutaminase.[rx]
Chronic Pancreatitis – Pancreatic enzymes are essential for the proper digestion of fats, proteins, and carbohydrates. Patients with chronic pancreatitis will develop recurrent bouts of acute pancreatitis and chronic abdominal pain. Chronic pancreatitis will eventually lead to scarring and fibrosis of the pancreas, which will decrease the number of pancreatic enzymes, and malabsorption. This will lead to steatorrhea and weight loss.[rx]
Lactose Intolerance – The ability to digest lactose comes from an enzyme present in the intestine called lactase. This allows the lactose to be broken down into simple sugar and be absorbed. When this enzyme is absent, the lactose is not able to be absorbed by the intestine. This will increase the osmolality within the lumen of the intestine producing watery diarrhea shortly after the ingestion of lactose-containing foods.[rx]
Malabsorption Syndromes – This term is very nonspecific and encompasses any disorder where the intestine has a decreased ability to absorb nutrients while not requiring intravenous supplementation for health and/or growth.[rx]
Post-cholecystectomy Diarrhea – Diarrhea after a cholecystectomy occurs in up to 12% of patients. Over time, symptoms generally resolve on their own without intervention.[rx] Since the gallbladder is removed, the bile produced by the liver directly enters the colon instead of being stored. The increased amount of bile acids in the colon produces diarrhea.[rx]
Chronic Infections – Certain long-lasting infections of the gastrointestinal tract can be linked to chronic diarrhea. A few of these infections include C. difficile, Vibrio cholera, Salmonella, Shigella, Entamoeba histolytica, E. Coli, Giardia, Cryptosporidium, Whipple Disease, and Cyclospora.[rx] A clinician should always have a suspicion of an infectious cause of diarrhea. Risk factors include travel and immunosuppression.
Symptoms of Chronic Diarrhea
The main symptom of chronic diarrhea is passing loose, watery stools three or more times a day for at least 4 weeks.
Depending on the cause, children with chronic diarrhea may also have one or more of the following symptoms:
bloody stools
chills
fever
loss of control of bowel movements
nausea or vomiting
pain or cramping in the abdomen
Chronic diarrhea may cause malabsorption and may lead to dehydration.
Chronic diarrhoea: signs, symptoms and analytical findings suggestive of an organic cause.
Blood in stools
Fever
Recent weight loss (>5kg) (in absence of concomitant depression)
Recent onset of symptoms, or change in the characteristics of previous symptoms
Onset at an advanced age (≥50 years)
Family history of colorectal cancer or polyps
Nocturnal diarrhoea
Diarrhoea persists after fasting
High-volume stool output or steatorrhoea
Weight of stool output over 24h >400g/day
Abnormalities on physical examination (pallor, hepatosplenomegaly, adenopathies, abdominal mass, etc.)
Anaemia, macrocytosis, hypoprothrombinaemia, hypoalbuminaemia or other laboratory findings (e.g. elevated ESR or C-reactive protein)
The infection often starts suddenly with projectile vomiting or severe diarrhea. It is considered to be diarrhea if you have more than three very loose or liquid bowel movements within 24 hours. People who have diarrhea often have a stomach aches, cramps, and bloating too. Diarrhea and nausea are sometimes also accompanied by fever, headache, and joint pain. Dizziness and feeling faint could be signs that your body has lost too much liquid and salts (electrolytes). If that happens, immediate medical attention is needed. Other reasons to seek medical help for diarrhea include:
No improvement after 48 hours
High fever
Blood in your poo (it has red blood in it or is black)
The mucous coating on the poo
Severe pain
Diagnosis of Chronic Diarrhea
When you see the doctor you will first be asked
whether your symptoms started suddenly or gradually,
what your poo looks like (consistency and appearance),
how long and how frequently you have had diarrhea,
whether you also have symptoms such as stomach ache, vomiting or fever, and
what you had to eat before getting diarrhea.
It is also important for them to know
whether you have been traveling recently,
what medications you were or are taking,
whether you have any diagnosed allergies or intolerances, and
whether you have a chronic disease, such as diabetes.
If you have bloody or persistent diarrhea, a sample of your stool (poo) or blood may be needed to find out what kind of infection you have. The same applies if there is mucus in diarrhea.
Your doctor will ask about your medical history, symptoms, and any medicines you take. Your doctor will also perform a physical exam and may order an upper gastrointestinal (GI) endoscopy with biopsies or other tests.
History and physical exam vary widely from patient to patient depending on the severity and etiology of the disease. The physical exam is often normal in patients with chronic diarrhea; however, signs of unintentional weight loss points towards a more severe disease. Although history and physical exam will rarely lead to a specific cause of chronic diarrhea, it is an integral part of any patient encounter. It is important to have the patient describe their diarrhea. Specific descriptions such as hematochezia, mucus in the stool, or steatorrhea help narrow the differential diagnosis greatly. Some specific physical exam signs may clue the examiner towards a diagnosis.
For all patients complaining of chronic diarrhea, a thorough history and physical exam are necessary. The following laboratory testing should also take place for every patient with chronic diarrhea:
Complete blood count with differential to examine for infection and anemia
Erythrocyte sedimentation rate and C-reactive protein to look for infections
Thyroid function tests to screen for hyperthyroidism
Complete metabolic profile to search for electrolyte abnormalities, renal function
Total protein and albumin to look for signs of protein malnutrition
Stool occult blood to look for a gastrointestinal bleed
If the patient has any alarming symptoms, a referral for an endoscopy is necessary. Alarm symptoms include
Symptom onset after age 50
Rectal bleeding/melena
Nocturnal pain or diarrhea
Progressive abdominal pain
Unexplained weight loss, fever, or other systemic symptoms
Laboratory abnormalities such as iron deficiency anemia, elevated ESR/CRP, elevated fecal calprotectin, or fecal occult blood
First degree relative with inflammatory bowel disease or colorectal cancer
If patients do not have alarming symptoms, stool laboratory assessment is a recommendation. If the patient has recent antibiotic use, checking the stool for C. difficile toxin is warranted; C. difficile toxin should be reviewed on all patients with chronic diarrhea, regardless of antibiotic use, if their diarrhea classically fits the description of C. difficile: watery diarrhea occurring 3 or more times per day.
When categorizing the stool, it is essential to check for the following labs:
Stool electrolytes
Fecal leukocytes (fecal lactoferrin or fecal calprotectin are a substitute in place of fecal leukocytes)
Fecal chymotrypsin and elastase
Occult blood
Stool fat (48 to 72 hour timed collection is ideal)
While chronic diarrhea has a very broad differential diagnosis, categorizing the stool can help narrow down the list. Fecal leukocytes/calprotectin/lactoferrin are markers of inflammation. The presence of these markers will point towards inflammatory diarrhea, such as Crohn’s disease, or ulcerative colitis.
Fecal chymotrypsin and elastase are pancreatic enzymes that can present in the stool in the setting of pancreatic insufficiency. These two tests do not definitively diagnose pancreatic insufficiency. If these are positive on stool testing, the physician should check blood tests for pancreatic enzymes, and potentially refer to a gastroenterologist for further studies.
For patients with watery diarrhea, stool electrolytes will further categorize their diarrhea into either osmotic diarrhea or secretory diarrhea based on the calculation of the stool osmotic gap. The calculation is as follows:
290 mOsm/kg – 2(Na[feces]+K[feces])
If the result of the above formula is less than 50 mOsm/kg, then the diarrhea is secretory. If the result is greater than 75 mOsm/kg, then the diarrhea is osmotic.[rx]
Lab Test
Upper GI endoscopy – Upper GI endoscopy is a procedure in which a doctor uses an endoscope—a flexible tube with a camera—to see the lining of your upper GI tract, including your esophagus, stomach, and duodenum. During upper GI endoscopy, a doctor obtains biopsies by passing an instrument through the endoscope to take small pieces of tissue from your stomach lining. A pathologist will examine the tissue with a microscope. Doctors may use upper GI endoscopy to diagnose gastritis or gastropathy, determine the cause, and manage complications.
Blood tests – Doctors may use blood tests to check for other causes of gastritis or signs of complications. For a blood test, a health care professional will take a blood sample from you and send the sample to a lab.
Stool tests – Doctors may use stool tests to check for H. pylori infection and for blood in your stool, a sign of bleeding in your stomach.
Timed stool collection – Neither patients nor laboratory technicians relish in the timed stool test (48–72 hrs of stool collection; normal stool weight is 200g/24 hrs with less than 7g fat), yet this is the standard for assessing steatorrhea. A fresh stool sample is necessary to differentiate secretory from osmotic diarrhea. Stool weight greater than 1000g/24 hrs leads to a different diagnostic approach (a search for a possible neuroendocrine cause) than a value of 300g/24 hrs. Approximately 25% of patients referred specifically for a diarrhea evaluation actually have normal stool weight (Sellin J, unpublished observations). The 48 hr stool collection test can also be used to measure fecal bile acids.[rx]
Blood tests for neuroendocrine tumors – hormone-secreting tumors are rare causes of secretory diarrhea, typically detected by measuring serum levels of chromogranin, gastrin, vasoactive intestinal polypeptide, or calcitonin, as well as urine level of 5-hydroxy indole acetic acid. However, due to the rarity of these tumors and low pretest probability, many positive results from these tests (especially borderline results) turn out to be false positives.[rx] These tests should therefore almost never be considered early in the course of an evaluation.
Urea breath test – Doctors may use a urea breath test to check for H. pylori infection. For the test, you will swallow a capsule, liquid, or pudding that contains urea that is “labeled” with a special carbon atom. If H. pylori is present, the bacteria will convert the urea into carbon dioxide. After a few minutes, you will breathe into a container, exhaling carbon dioxide. A health care professional will test your exhaled breath. If the test detects the labeled carbon atoms, the health care professional will confirm an H. pylori infection in your digestive tract.
Upper GI series – Doctors may use an upper GI series to check for signs of gastritis or gastropathy. An upper GI series is a procedure in which a doctor uses x-rays and a chalky liquid called barium to view your upper GI tract.
MR enterography – is recommended for evaluation of small bowel abnormalities depending on availability (Grade of evidence level 1, Strength of recommendation strong).
Video capsule endoscopy (VCE) – is recommended for assessing small bowel abnormalities depending on local availability (Grade of evidence level 1, Strength of recommendation strong).
Small bowel barium follow-through or barium enteroclysis – for the evaluation of small bowel abnormalities due to its poor sensitivity and specificity (Grade of evidence level 5, Strength of recommendation strong).
Fecal elastase testing – when fat malabsorption is suspected. We do not recommend PABA testing (Grade of evidence level 1, Strength of recommendation strong).
MRI (rather than CT) – is recommended for assessing structural anomalies of the pancreas in suspected chronic chronic diarrhea (Grade of evidence level 2, Strength of recommendation strong).
Treatment for Chronic Diarrhea
How doctors treat chronic diarrhea depends on the cause. Doctors may be able to reduce or stop chronic diarrhea by treating the cause.
A bland ‘BRAT’ diet including bananas, toast, oatmeal, white rice, applesauce, and soup/broth is well tolerated and may improve symptoms. [rx] Anti-diarrheal therapy with anti-secretory or anti-motility agents may be started to reduce the frequency of stools.
Non Pharmacological
Food allergies – If your child has a food allergy, his or her doctor will recommend avoiding foods that trigger the allergy. Keeping a diary of what your child eats and drinks and his or her bowel habits will help your child’s doctor find out what foods trigger the allergy.
Lactose intolerance – If your is lactose intolerant, his or her doctor will recommend reducing or avoiding foods and beverages that contain milk or milk products. Most with lactose intolerance can tolerate some amount of lactose in what they eat or drink. The amount of change needed in what a child eats or drinks depends on how much lactose a child can consume without symptoms. Your child’s doctor may recommend dietary supplements that contain lactase, the enzyme that helps digest lactose. Your child’s doctor may also recommend calcium supplements.
Fructose intolerance – If is fructose intolerant, will recommend reducing or avoiding foods and beverages that contain fructose.
Sucrose intolerance – If is sucrose intolerant, his or her doctor will recommend reducing or avoiding foods and beverages that contain sucrose.
Medication
Drugs used in Treatment of Chronic Watery Diarrhea
Drug class
Agent
Dose
Opiates (μ-opiate receptor-selective)
Diphenoxylate
2.5–5 mg, 4 times/day
Loperamide
2–4 mg, 4 times/day
Codeine
15–60 mg, 4 times/day
Opium tincture
2–20 drops, 4 times/day
Morphine
2–20 mg, 4 times/day
Eluxadoline
100 mg twice daily (μ-opioid agonist and δ-opioid antagonist) for IBS-D
Adrenergic α2 receptor agonist
Clonidine
0.1–0.3 mg 3 times/day; Weekly patch
Somatostatin analog
Octreotide
50–250 μg 3 times/day (subcutaneously)
Bile acid-binding resin
Cholestyramine
4 g daily or up to 4 times/day
Colestipol
4 g daily or up to 4 times/day
Colesevelam
1875 mg up to twice daily
Fiber supplements
Calcium polycarbophil
5–10 g daily
Psyllium
10–20 g daily
Soluble fiber
Pectin
2 capsules before meals
Calcium
1000 mg twice or 3 times daily
Serotonin 5-HT3 receptor antagonists
Alosetron
0.5–1.0 mg twice daily
Ondansetron
2–8 mg twice daily
Azithromycin – in a single dosage 0r ciprofloxacillin in a double dosage for 7 days . In a randomized trial, Azithromycin was found to be clinically and bacteriological successful in 82% and 94% of patients treated respectively.[rx] Cefixime and ceftibuten can be used as first-line to treat in due to widespread resistance to commonly used antibiotics.[rx] The alternative regimen includes pivmecillinam, an extended-spectrum penicillin is effective in decreasing diarrhea duration and eradication of chronic diarrhea organisms in the stool.[rx][rx]
Loperamide – is a safe mu-receptor agonist used to decrease gut peristalsis. Loperamide is a safe mu-receptor agonist used to decrease gut peristalsis and decrease the gut motility. Loperamide is not suitable for children under the age of twelve years, and racecadotril is prescription-only for children.
Nitazoxanide – is a broad-spectrum antimicrobial agent with activity against protozoa, nematodes, cestodes, trematodes, and bacteria, with a favorable safety profile [rx, rx]. It is effective in childhood cryptosporidiosis [rx] but not consistently in undernourished children or in HIV-infected patients [rx]. Anecdotal cases of children successfully treated with nitazoxanide because of PD (<30 days) have been reported [rx]. This strategy seems to be effective in select situations, saving time-consuming tests to identify the cause of diarrhea [rx].
Cholestyramine – Other medications used for chronic diarrhea include bile acid-binding resins such as cholestyramine. Clonidine is an alpha2-adrenergic agonist that also slows the intestinal tract, and is an option for diarrhea secondary to opioid withdrawal as well as diarrhea secondary to loss of noradrenergic innervation in patients with diabetes. The use of this medication has limitations due to the antihypertensive effect. However, this medication may be useful for patients with hypertension and chronic diarrhea.
Ceftriaxone – Intra venous or parenteral antibiotics are indicated in children with suspected and proven chronic diarrhoea who have a severe infection with signs of bacteremia including lethargy, temperature >39° C (102.2°F), underlying immune deficiency including AIDS and those unable to take oral medications.[rx] Ceftriaxone is recommended as a single dose or for five days.
Anticholinergic medications – can be used to treat diarrhea as well. Tricyclic antidepressants which are used to treat depression or pain can also treat diarrhea.[rx]
Immunoglobulin – available for intravenous use, may be administered orally (300 mg/kg of body weight) in a single dose. The rationale of passive immunotherapy is based on the demonstration of neutralizing antibodies against all viruses in a medical preparation of immunoglobulins [rx].
Cholestyramine – Other medications used for chronic diarrhea include bile acid-binding resins such as cholestyramine. Clonidine is an alpha2-adrenergic agonist that also slows the intestinal tract, and is an option for diarrhea secondary to opioid withdrawal as well as diarrhea secondary to loss of noradrenergic innervation in patients with diabetes. The use of this medication has limitations due to the antihypertensive effect. However, this medication may be useful for patients with hypertension and chronic diarrhea.
Yeast tablets – Sometimes certain types of yeast tablets (Perenterol) are recommended. These tablets are thought to help the body get rid of germs faster and to support natural gut flora. Charcoal tablets dissolved in water can also be taken to relieve diarrhea symptoms. But there’s a lack of good-quality research in this area so no conclusions can be drawn about the benefits and harms of these treatment options. People who are very ill or have a very weak immune system shouldn’t take yeast tablets.
Zinc supplementation – is reported to reduce both the stool volume and stool frequency by 30 percent and is a consideration in severe cases.[rx] Although diets such as BRAT (banana, rice, apple, and toast) or bland diet have been proposed to improve the condition and are somewhat better tolerated; no reliable data or prospective studies are available to confirm this, and the assumptions are mostly based on limited studies or personal experiences.
Foods to avoid
Fried and greasy foods are usually not well-tolerated in people who have diarrhea. You should also consider limiting high-fiber foods like bran as well as fruits and vegetables that can increase bloating. Foods to avoid include:
alcohol
artificial sweeteners (found in chewing gum, diet soft drinks and sugar substitutes)
beans
berries
broccoli
cabbage
cauliflower
chickpeas
coffee
corn
ice cream
green leafy vegetables
milk
peas
peppers
prunes
tea
Foods to eat
While it might sound counterintuitive to eat if you have diarrhea, eating certain foods can help alleviate your diarrhea symptoms and ensure your health doesn’t worsen from not eating. Stick to low-fiber “BRAT” foods that will help firm up your stool. These include:
bananas
rice (white)
applesauce
toast
Other foods that are usually well-tolerated when experiencing diarrhea include:
oatmeal
boiled or baked potatoes (with skins peeled)
baked chicken with skin removed
chicken soup (which also aids in rehydration)
Probiotics
Probiotics are sources of “good” bacteria that work in your intestinal tract to create a healthy gut environment. They’re essentially live microorganisms that exist in certain foods, including:
aged soft cheeses
beet kvass
cottage cheese
dark chocolate
green olives
kefir
kimchi
kombucha
sauerkraut
miso
natto
pickles
sourdough bread
tempeh
yogurt
Probiotics also come in powder or pill form.
The good bacteria that live in your intestinal tract are necessary for the normal functioning of your gastrointestinal system. They play an important role in protecting your intestines against infection. When your system is changed by antibiotics or overwhelmed by unhealthy bacteria or viruses, you can get diarrhea. Probiotics can help with diarrhea by restoring the balance of bacteria in your gut.
Saccharomyces boulardii is a yeast probiotic. While it’s not a bacterium, it acts like one. S. boulardii may improve antibiotic-associated diarrhea. It also seems to provide relief for traveler’s diarrhea. It may help your intestines fight off unwanted pathogens and ensure they’re absorbing nutrients properly. Because it is yeast, it should be used with caution in people with inadequate immune systems.
Prevention
Viruses and bacteria can spread through contact with poo, vomit, and contaminated objects, water, or food.
This means that it is very important to frequently wash your hands thoroughly with soap if you have acute diarrhea, in order to protect others from infection. Washing your hands also protects you from infection if someone you know is infected. A hand disinfectant can help too. If you have a second bathroom at home, whoever is ill can be the only one to use it.
Clothes should be washed at temperatures above 60 degrees Celsius (about 140 degrees Fahrenheit) if possible. It is important to pay attention to hygiene in the kitchen and while preparing food. Anyone with acute diarrhea shouldn’t prepare food for others.
When traveling to tropical or subtropical climates, you may need to avoid uncooked, unpeeled fruit and vegetables and not drink tap water. Don’t eat undercooked meat or fish.
keeping a food diary and seeing how cutting particular foods from the diet affect the diarrhea
discussing the side effects of any current medications with a doctor
requesting a change in medications if necessary
taking probiotic supplements regularly
drinking only clean or filtered water
washing the hands both before and after food preparation
cleaning and thoroughly cooking meat before eating it
washing fresh produce before eating it
cleaning kitchen surfaces regularly
washing the hands regularly, especially after using the bathroom or coming into contact with a person who is ill
Complications
Complications of shigella infection include intestinal and systemic complications listed below. [rx]
Intestinal Complications
Colon perforation – Very rare and primarily occurs in infants and malnourished patients. It is associated with S. flexneri and S. dysenteriae 1. [rx]
Intestinal obstruction – usually seen in severe disease and S. dysenteriae 1.[rx]
Toxic megacolon – Usually occurs in S. dysenteriae 1 infection.[rx]
Proctitis or rectal prolapse – Invasion of shigella organisms into colonic mucosa can lead to rectal prolapse and proctitis in infants and young children.[rx]
Bacteremia – Common in young children under the age of 5.[rx][rx][rx]
Hemolytic-uremic syndrome – Although uncommon, HUS is the most frequent acute kidney injury in young children and infants.[rx]
Moderate to severe hypovolemia
Hyponatremia – Usually associated with S. dysenteriae 1 infection.[rx]
Leukemoid reaction – Common in children between ages 2-10 years old.[rx]
Neurologic symptoms – Generalized seizures are the most common neurologic complication. This is usually associated with a higher mortality rate.[rx][rx]
Reactive arthritis or Reiter syndrome – Uncommon sterile inflammatory arthritis. It is usually caused by S. flexneri infection. Arthritis can occur alone or in conjunction with conjunctivitis and urethritis.[rx]
Vulvovaginitis – with or without diarrhea-Seen in young girls associated with painless vaginal discharge.[rx]
Keratitis – Rare but should be considered in a young child with keratitis and a history of recent diarrheal illness. [rx]
Acute myocarditis – Seen in children with S. Sonnei infection.[rx]
Weight loss – in adults and other consequences of malnutrition such as increased susceptibility to infections, and increased morbidity and mortality from various disease states. Additionally, in children, malnutrition results in growth failure and poor neurological development
Deficiencies of fat-soluble vitamins (A, D, E, and K)
Poor bone health resulting in osteopenia, osteoporosis, and fractures (CF, celiac disease)
Iron deficiency anemia, zinc deficiency (celiac disease)
Dermatitis herpetiformis, non-Hodgkin lymphoma, adenocarcinoma of the upper gastrointestinal tract (celiac disease)
Megaloblastic anemia due to B12 deficiency (in terminal ileum disease and SIBO)
Celiac Disease/Coeliac disease is also known as celiac sprue is a unique autoimmune, genetic element (human leukocyte antigen (HLA)-DQ2 and HLA-DQ8), based gluten-sensitive immune-mediated enteropathic with the auto-antigen involved (tissue transglutaminase (tTG)), and the environmental trigger (gluten) are all well-defined condition where the immune system mistakes healthy cells for harmful ones and produces antibodies which result in the small intestine becoming inflamed and less able to absorb nutrients, maldigestion, and malabsorption of most nutrients and vitamins. It can cause a range of symptoms including diarrhea.
Celiac disease (CD) is an autoimmune condition characterized by a specific serological and histological profile triggered by gluten ingestion in genetically predisposed individuals [rx]. Gluten is the general term for alcohol-soluble proteins present in various cereals, including wheat, rye, barley, spelled, and Kamut [rx].
Celiac disease is a chronic digestive and immune disorder that damages the small intestine. The disease is triggered by eating foods containing gluten. Gluten is a protein found naturally in wheat, barley, and rye, and is common in foods such as bread, pasta, cookies, and cakes. Many products contain gluten, such as prepackaged foods, lip balms and lipsticks, toothpaste, vitamin and nutrient supplements, and, rarely, medicines.
Types of Celiac Disease
Recently a consensus paper redefined the types of celiac disease.
Classic celiac disease – refers to the presence of symptoms of malabsorption such as diarrhea, failure to thrive, and weight loss and may occur in adults and children.
Non-classic celiac disease – refers to celiac disease without prominent gastrointestinal symptoms or malabsorption; however, individuals with atypical celiac disease can also have gastrointestinal symptoms such as reflux, abdominal pain, bloating, vomiting, constipation, and dyspepsia. Approximately 70% of individuals are diagnosed based on extraintestinal manifestations associated with celiac disease. This group includes monosymptomatic and subclinical forms.
Marsh classification of histologic findings in celiac disease
Marsh 0
Normal mucosal architecture without significant intraepithelial lymphocytic infiltration.
Marsh I
Lymphocytic enteritis: Normal mucosal architecture with a marked infiltration of villous epithelium by lymphocytes; arbitrarily defined marked as more than 30 lymphocytes per 100 enterocytes
Marsh II
Lymphocytic enteritis with crypt hyperplasia: intraepithelial lymphocytosis and elongation and branching of crypts in which there is an increased proliferation of epithelial cells
Marsh III
Intraepithelial lymphocytosis, crypt hyperplasia, and villous atrophy. There are 3 distinct stages of villous atrophy
Marsh IIIA
Partial villous atrophy, the villi are blunt and shortened. Arbitrarily, samples are classified as partial villous atrophy if the villus-crypt ratio was less than 1:1
Marsh IIIB
Subtotal villous atrophy, villi are clearly atrophic but still recognizable
Marsh IIIC
Total villous atrophy, villi are rudimentary or absent, and the mucosa resembles colonic mucosa.
Causes of Celiac Disease
The symptoms of celiac disease are due to the damage of enterocytes in the small intestine. In the full-blown clinical picture, the typical features of the small intestine are chronic inflammation and villi atrophy. [rx][rx][rx]
An individual has to have HLA-dominant DQ2 or DQ8 genes. The disease is a result of the immune system reacting adversely to gluten, and one of the important proteins involved is an antibody to tissue transglutaminase. There are however other pathways proposed that contribute to the disease. The glycoprotein gliadin (present in gluten) has a direct toxic effect on enterocytes by the up-regulating production of IL-15.
Celiac disease is also called celiac sprue, nontropical sprue, and gluten-sensitive enteropathy.
Celiac disease can only occur in people who have certain genes. You are more likely to develop the celiac disease if someone in your family has the disease.
Celiac disease affects children and adults in all parts of the world. In the United States, celiac disease is more common among white Americans than among other racial or ethnic groups. A celiac disease diagnosis is more common in females than in males.
Celiac disease is also more common in people who have certain chromosomal disorders, such as Down syndrome, Turner syndrome, and Williams syndrome.
Experts have found that some people have both celiac disease and other disorders related to the immune system. These disorders include
type 1 diabetes
thyroid diseases, such as Hashimoto’s disease, Graves’ disease, Addison’s disease, and primary hyperparathyroidism
selective immunoglobulin A (IgA) deficiency, a condition in which your body makes little or no IgA, an antibody that fights infections
rheumatic diseases, such as Sjögren’s syndrome NIH external link
liver diseases, such as autoimmune hepatitis, primary sclerosing cholangitis, and primary biliary cholangitis
Research suggests that celiac disease only occurs in people who have certain genes and eat food that contains gluten. Experts are studying other factors that may play a role in causing the disease.
Genes
The celiac disease almost always occurs in people who have one of two groups of normal gene variants, called DQ2 and DQ8. People who do not have these gene variants are very unlikely to develop celiac disease. About 30 percent of people have DQ2 or DQ8. However, only about 3 percent of people with DQ2 or DQ8 develop celiac disease.4
Researchers are studying other genes that may increase the chance of developing celiac disease in people who have DQ2 or DQ8.
Gluten
Consuming gluten triggers the abnormal immune system response that causes celiac disease. However, not all people who have the gene variants DQ2 or DQ8 and eat gluten develop the disease. Research suggests that among children with a genetic predisposition for celiac disease, those who eat more gluten in early childhood may have a greater risk for celiac disease.
Other factors
Researchers are studying other factors that may increase a person’s chances of developing celiac disease. For example, research suggests that a higher number of infections in early life and certain digestive tract infections may increase the risk. Experts also think changes in the microbiome—the bacteria in the digestive tract that help with digestion—could play a role in the development of celiac disease.
Symptoms of Celiac Disease
Symptoms of celiac disease vary widely, and a person may have multiple symptoms that come and go. If you have celiac disease, you may have digestive problems or other symptoms. Digestive symptoms are more common in children than in adults. Digestive symptoms of celiac disease may include
The main symptoms are stomach pain, gas, and bloating, diarrhea, weight loss, anemia, edema, bone or joint pain.
Anemia due to defective absorption of vitamin B12, folate, or iron
Coagulopathy due to impaired absorption of vitamin K
Osteoporosis
Neurological symptoms like muscle weakness, paresthesias, seizures, and ataxia
bloating
chronic diarrhea
constipation
gas
lactose intolerance due to damage to the small intestine
loose, greasy, bulky, and bad-smelling stools
nausea or vomiting
pain in the abdomen
frequent bouts of diarrhea or loose stools
nausea, feeling sick, and vomiting
stomach pain and cramping
lots of gas and bloating
feeling tired all the time, ongoing fatigue
anemia (you would be told if you’re anemic following a blood test)
weight loss (although not in all cases)
regular mouth ulcers
constipation or hard stools
For children with celiac disease, being unable to absorb nutrients at a time when they are so important to normal growth and development can lead to
damage to the permanent teeth’s enamel
delayed puberty
failure to thrive, meaning that an infant or a child weighs less or is gaining less weight than expected for his or her age
mood changes or feeling annoyed or impatient
slowed growth and short height
weight loss
Anemia due to defective absorption of vitamin B12, folate or iron
Coagulopathy due to impaired absorption of vitamin K
Osteoporosis
Neurological symptoms like muscle weakness, paresthesias, seizures and ataxia
Some people with celiac disease have symptoms that affect other parts of the body. These symptoms may include
dermatitis herpetiformis
fatigue, or feeling tired
joint or bone pain
mental health problems, such as depression or anxiety
nervous system symptoms, such as headaches, balance problems, seizures, or peripheral neuropathy
reproductive problems in women and girls—which may include infertility, delayed start of menstrual periods, missed menstrual periods, or repeated miscarriages and male infertility
symptoms involving the mouth, such as canker sores; a dry mouth; or a red, smooth, shiny tongue
Anemia due to defective absorption of vitamin B12, folate or iron
Coagulopathy due to impaired absorption of vitamin K
Osteoporosis
Neurological symptoms like muscle weakness, paresthesias, seizures and ataxia
Most people with celiac disease have one or more symptoms before they are diagnosed and begin treatment. Symptoms typically improve and may go away after a person begins eating a gluten-free diet. Symptoms may return if a person consumes small amounts of gluten.
Depending on how old you are when a doctor diagnoses your celiac disease, some symptoms, such as short height and tooth defects, may not improve. People with celiac disease who have no symptoms can still develop complications over time if they do not get treatment.
Individuals with disorders associated with celiac disease (e.g., Down syndrome, Turner syndrome, Williams syndrome, selective IgA deficiency, insulin-dependent diabetes mellitus, Sjögren syndrome, thyroiditis)
Absence of history of self-limited enteritis and/or tropical sprue
According to NCBI.NLM.NIH symptoms are
The following extraintestinal symptoms are secondary to malabsorption [rx,rx]
Peripheral neuropathy (vitamin B12 and B1 deficiency)
Anemia (iron, vitamin B12 and folate deficiency)
Growth failure in children
Bone pain (osteoporosis and osteopenia, vitamin D and calcium deficiency)
Muscle cramps (magnesium and calcium deficiency)
Night blindness (vitamin A deficiency)
Weight loss (impaired absorption of most nutrients)
Edema (protein and albumin loss)
Weakness (hypokalemia and electrolyte depletion)
Bleeding and hematoma (vitamin K deficiency)
The following extraintestinal symptoms/manifestations are probably not secondary to malabsorption (atypical CD) [rx]
Neurological disorders such as depression, epilepsy, migraine, ataxia
Dermatitis herpetiformis
Elevated liver enzymes, liver failure
Infertility
Stomatitis
IgA nephritis
Myocarditis
Idiopathic pulmonary hemosiderosis
Arthritis
The following diseases/conditions are associated with celiac disease [rx–rx]
Autoimmune diseases such as type 1 diabetes, Sjögren syndrome, thyroid diseases (Hashimoto’s thyroiditis and Graves’s disease), autoimmune hepatitis and primary biliary cirrhosis
Selective IgA deficiency
Turner’s syndrome
Down’s syndrome
Dermatitis herpetiformis
Dermatitis herpetiformis is an itchy, blistering skin rash that usually appears on the elbows, knees, buttocks, back, or scalp. Among people with untreated celiac disease, about 2 to 3 percent of children and 10 to 20 percent of adults have dermatitis herpetiformis.3 Some people with celiac disease may have the rash and no other symptoms. After a person starts a gluten-free diet, the rash may take some time to heal and may return if a person consumes small amounts of gluten.
Children
Children with celiac disease are more likely than adults to have digestive problems, including:
Nausea and vomiting
Chronic diarrhea
Swollen belly
Constipation
Gas
Pale, foul-smelling stools
The inability to absorb nutrients might result in:
Failure to thrive for infants
Damage to tooth enamel
Weight loss
Anemia
Irritability
Short stature
Delayed puberty
Neurological symptoms, including attention-deficit/hyperactivity disorder (ADHD), learning disabilities, headaches, lack of muscle coordination and seizures
Diagnosis of Celiac Disease
Doctors use information from your medical and family history, a physical exam, a dental exam, and medical test results to look for signs that you might have celiac disease and should be tested. Doctors typically diagnose celiac disease with blood tests and biopsies of the small intestine.
Medical and family history
Your doctor will ask about your symptoms.
Celiac disease isn’t diagnosed based on symptoms alone because some of the symptoms are like the symptoms of other digestive disorders, such as irritable bowel syndrome (IBS) or lactose intolerance. Some people with celiac disease have symptoms that affect parts of the body outside the digestive tract.
The doctor will review your medical history, including your history of conditions that are more common in people who have celiac disease. Your doctor will also ask about your family’s medical history and whether anyone in your family has been diagnosed with celiac disease.
Physical exam
During a physical exam, a doctor may
check for signs of weight loss or growth problems
examine your skin for rashes, such as dermatitis herpetiformis
listen to sounds in the abdomen using a stethoscope
tap on the abdomen to check for pain or swelling
In some cases, a dentist may notice signs of celiac disease during an exam. Celiac disease may cause problems with the teeth and mouth, such as defects in tooth enamel or canker sores.
Doctors most often use blood tests and biopsies of the small intestine to diagnose or rule out celiac disease. Doctors don’t recommend starting a gluten-free diet before diagnostic testing because a gluten-free diet can affect test results.
In some cases, doctors may order additional tests, such as skin biopsies and genetic tests, to help diagnose or rule out celiac disease.
Lab Test
Blood tests – A health care professional will take a blood sample from you and send the sample to a lab. Blood tests can show levels of certain antibodies that are often higher than normal in people who have untreated celiac disease. Blood tests may also show signs of health problems that could be related to celiac disease, such as anemia.
Biopsies of the small intestine – A doctor obtains biopsies of the small intestine during an upper GI endoscopy. For an upper GI endoscopy, a doctor uses an endoscope—a flexible tube with a camera—to see the lining of your upper GI tract, including the first part of your small intestine. The doctor passes an instrument through the endoscope to take small pieces of tissue from your small intestine. A pathologist will examine the tissue under a microscope to look for signs of celiac disease.
Skin biopsies – A doctor may order skin biopsies if you have a rash that could be dermatitis herpetiformis. For skin biopsies, a doctor removes small pieces of skin tissue on and next to the rash. A pathologist will examine the tissue under a microscope to look for signs of dermatitis herpetiformis.
Genetic testing – In some cases, a health care professional may take a blood sample or use a swab to collect cells from the inside of your cheek. The sample will be tested for groups of gene variants called DQ2 and DQ8. If you do not have these gene variants, you are very unlikely to have celiac disease. Having DQ2 or DQ8 alone does not mean you have celiac disease. Most people with these gene variants do not develop celiac disease. If you do have DQ2 or DQ8, your doctor may recommend additional tests to check for or rule out celiac disease.
HLA tests – Based on studies for which sensitivity could be calculated, the ACG estimated the negative predictive value of the HLA-DQ2/HLA-DQ8 combination test at more than 99 percent in diagnosing celiacdisease.
Screening is testing – for diseases when you have no symptoms. Doctors in the United States do not routinely screen people for celiac disease. However, blood relatives of people with celiac disease and those with type 1 diabetes should talk with their doctor about their chances of getting the disease to see if they should be tested.
Endoscopy – This test uses a long tube with a tiny camera that’s put into your mouth and passed down your throat (upper endoscopy). The camera enables your doctor to view your small intestine and take a small tissue sample (biopsy) to analyze for damage to the villi.
Capsule endoscopy – This test uses a tiny wireless camera to take pictures of your entire small intestine. The camera sits inside a vitamin-sized capsule, which you swallow. As the capsule travels through your digestive tract, the camera takes thousands of pictures that are transmitted to a recorder.
Serological tests
Anti-tissue transglutaminase antibodies – the best strategy for serological diagnosis is the blood detection of IgA anti-tissue transglutaminase antibodies (tTGA) by enzyme-linked immunosorbent assay (ELISA). These antibodies show a sensitivity up to 97%, a specificity around 96%, and an accuracy of 98%, whereas IgA anti-endomysial (IgA EMA) antibodies are employed as a confirmatory test in tTGA positive cases due to their higher specificity (about 100% vs 91% of tTGA). In concomitance of IgA deficiency and celiac disease, found in around 2%-10% of the patients, it is recommended to detect celiac disease testing tTG-IgG. “False-negative” occurs, as previously reported, in the case of IgA deficiency. The IgA EMA represents the most specific test (approximately 100%), with a sensitivity around 94% and a diagnostic accuracy of 97%[rx]. However, EMA is routinely detected by indirect subjective immunofluorescence[rx]. These antibodies can also result falsely negative in case of IgA deficiency and in children aged > 2 years.
anti-gliadin antibodies – The antigliadin (AGA) antibodies (IgG and IgA) are today no longer recommended because of their low sensitivity and specificity and inferior accuracy, except in younger children[rx].
Deamidated gliadin peptides – Actually detection of antigliadin antibodies has been replaced by the more recently developed immunoassays employing antibodies to deamidated gliadin peptides, IgA and IgG. To increase the diagnostic accuracy, in the last years the clinicians tend to prescribe serial testing.
Blood tests check other parts of your immune system.
Intestinal fatty acid-binding protein tests show if there’s damage to the intestine.
A complete blood count looks for anemia (low red blood cells).
C-reactive protein tests show if there’s inflammation.
Metabolic panels test liver and kidney function.
Vitamin D, B12, and folate tests look for vitamin deficiencies.
Iron and ferritin tests look for iron deficiency.
Swallowing a small camera can show problems in your digestive tract.
Imaging tests show signs in the intestine, like wall thickening or changes to blood vessels.
Genetic testing looks for human leukocyte antigens to rule out celiac disease.
Electrolytes may reveal hypocalcemia, hypokalemia, metabolic acidosis
Anemia due to deficiency of folate, iron or Vit B12
Prothrombin time may be prolonged
Stool are greasy and have a rancid odor
In individuals on a gluten-containing diet:
Elevated serum tissue transglutaminase (tTG) IgA
Elevated serum anti-deamidated gliadin-related peptide (a-DGP) IgA and IgG
Elevated serum endomysial antibody (EMA) IgA; highest specificity (~99%) but sensitivity subject to observer variability
Treatment for Celiac Disease
Gluten-free diet
Doctors treat celiac disease by helping people to follow a gluten-free diet. Gluten is a protein found naturally in certain grains, including wheat, barley, and rye. Gluten is also added to many other foods and products. In people who have celiac disease, consuming gluten triggers an abnormal immune system reaction that damages the small intestine.
Symptoms greatly improve for most people with celiac disease who stick to a gluten-free diet. For most people, following a gluten-free diet will heal damage in the small intestine and prevent more damage. Many people see symptoms improve within days to weeks of starting the diet.
Your doctor will explain the gluten-free diet and may refer you to a registered dietitian who specializes in treating people who have celiac disease. The dietitian will teach you how to avoid gluten while following a healthy diet and recommend substitutes for foods that contain gluten. He or she will help you
check food and product labels for gluten
design everyday meal plans
make healthy choices about foods and drinks
Avoiding medicines and other products that may contain gluten
In addition to prescribing a gluten-free diet, your doctor will want you to avoid all hidden sources of gluten. If you have celiac disease, ask a pharmacist about ingredients in
herbal and nutritional supplements
prescription and over-the-counter medicines
vitamin and mineral supplements
Medicines are rare sources of gluten. Even if gluten is present in a medicine, it is likely to be in such small quantities that it would not cause any symptoms.
Other products can be hidden sources of gluten. You may take in small amounts of gluten if you consume these products, use them around your mouth, or transfer them from your hands to your mouth by accident. Products that may contain gluten include
children’s modeling dough, such as Play-Doh
cosmetics
lipstick, lip gloss, and lip balm
skin and hair products
toothpaste and mouthwash
communion wafers
Reading product labels can sometimes help you avoid gluten. Some companies label their products as being gluten-free. In the United States, products labeled gluten-free must have less than 20 parts per million of gluten, which should not be a problem for the vast majority of people. If a label doesn’t tell you what is in a product, ask the company that makes the product for an ingredients list. You cannot assume that the product is gluten-free.
Gluten-degrading enzymes
Enzyme supplement therapy with bacterial prolyl-endopeptidases expressed by various microorganisms has been proposed to accelerate gluten digestion in the gastrointestinal tract and thus to destroy T cell epitopes[rx]. Prolyl-endopeptidases are proline-specific enzymes capable to cleave gluten peptides. Actually, there are introduced into clinical trials two drug candidates, ALV003 and AN-PEP (Aspergillus niger prolyl-endoprotease). Recent data on results of two phases 1 clinical trials have revealed that pre-treating gluten with ALV003 eliminates the peripheral blood T cell response in celiac disease patients, suggesting the potential therapeutic utility of gluten-specific enzymes to treat celiac disease[rx]. Currently is undergoing clinical phase IIa testing showing significantly reduce gluten-related T-cell responses compared with placebo but without a significant reduction of symptoms typically induced by the gluten[rx].
AN-PEP is an enzyme that degrades gluten peptides efficiently in a pH compatible with that found in the stomach. Therefore this enzyme might be suitable for oral supplementation but further studies are necessary[rx].
Modified grains
Can be developed either through selective breeding of early wheat species or using small interfering RNA (siRNA) technology to mutate or silence immunostimulatory sequence[tx].
Blocking gluten entry across the intestinal epithelium
Zonulin inhibitor larazotide (AT-1001) corrects intestinal barrier defects. It has been explored in an animal model[rx]. AT-1001 is currently the best-studied pharmacologic agent to treat patients with celiac disease, actually undergone in phase II clinical trials[rx]. It has been shown that patients treated with AT-1001 had an improved symptom score, a less pronounced autoantibody response and pro-inflammatory production, and lower urinary nitrate excretion when compared with the placebo controls[rx].
Rho/Rho-kinase inhibition
It has been clarified that the increase in intestinal permeability is dependent on Rho kinase (ROCK) activity[rx]. In addition to regulating tight junction structure and function, ROCK is known to regulate axon growth[rx,rx]. The drug could be used to establish whether ROCK inhibition can reverse the gluten-dependent increase in intestinal permeability in these patients[rx].
Immunotherapy
The first observation of the occurrence of celiac disease following allogeneic bone marrow transplantation performed in a patient with acute leukemia, made evident the involvement of T-lymphocyte in the pathogenesis of this condition[rx]. Since then, a lot of acknowledgments have been acquired such that many efforts are being made to develop immunologic therapeutic tools. Cytokine therapies based either on amplification of regulatory cytokines or on blockage of inflammatory cytokines expression are largely diffused for management of severe autoimmune disorders. Also for celiac disease resistant to dietary approach and especially for refractory celiac disease, the use of immunomodulators is developing. IL-15 blocking antibodies have shown the capability to induce intra-epithelial lymphocytes apoptosis in the intestinal epithelium of human IL-15 transgenic mouse models[rx].
Continues RX
Treatment with a gluten-free diet should be started only after the diagnosis has been established by intestinal biopsy.
A dietitian experienced in treating celiac disease should be involved.
Symptoms may improve rapidly while serologic tests may take up to 12 months to normalize on the gluten-free diet.
For some individuals, even a small amount of gluten (i.e., 100 mg) can damage the small intestine. Note that a slice of bread contains approximately 2.5 grams of gluten.
It can be difficult to adhere to the gluten-free diet, as gluten is found in many foods and other ingested products. Some hidden sources of gluten:
Non-starchy foods such as soy sauce and beer
Non-food items such as some medications and cosmetics (e.g., lipstick)
Nutritional deficiencies and metabolic bone disease should be treated in the usual manner.
Therapies Under Investigation
Several novel therapeutic approaches that potentially could be used as alternatives for or additives to a gluten-free diet are being investigated (reviewed in Castillo et al [2015] and Rashtak & Murray [2012]):
Larazotide, a tight junction regulatory peptide that is considered to prevent the passage of gliadin peptides into the mucosa. This drug is in clinical trials.
Peptides that block the binding groove of DQ2 and DQ8 to prevent activation of gluten-sensitive T cells. The viability of this approach is currently uncertain.
Transglutaminase (tTG) inhibitors
Cytokine blockers, particularly for refractory celiac disease. Of particular interest is an anti-IL15 antibody.
Drugs that selectively inhibit leukocyte adhesion and migration of lymphocytes into inflamed tissues
Detoxifying gluten, using oral proteases. Latiglutenase, a glutenous, is currently in clinical trials.
Gluten-sequestering polymers. An oral polymeric resin, P(HEMA-co-SS), binds to gluten and is under study.
Gluten tolerization. A peptide-based vaccine could desensitize or induce tolerance in individuals with celiac disease. A prototype vaccine, Nexvax2, involving a set of gluten peptides recognized by HLA-DQ2, is in clinical trials.
Rho/Rho-kinase inhibition to theoretically reverse the gluten-dependent increase in intestinal permeability [Sollid & Khosla 2011]
Antibodies to proteins involved in autoimmune pathologies, including anti-IFN-γ, anti-CD3, anti-CD20 therapy, and anti-IL-15. [Sollid & Khosla 2011]
Another approach: interfering with the homing of gluten-specific T cells to the gut mucosa by using CCR9 antagonists. A Phase II clinical trial is listed in Sollid & Khosla [2011].
Follow-up
Your doctor may recommend regular follow-up visits to make sure symptoms and health problems related to celiac disease are improving on a gluten-free diet. Follow-up may include blood tests to check levels of certain antibodies, which are higher in untreated celiac disease but typically return to normal after treatment. In some cases, doctors may recommend additional biopsies to find out if the small intestine has healed.
What if a gluten-free diet isn’t working?
If you continue to have celiac disease symptoms while you are following a gluten-free diet, talk with your doctor or a registered dietitian, who can help you find the cause. In about 20 percent of people with celiac disease, symptoms continue or come back even while they are following a gluten-free diet.7 Symptoms may be caused by consuming small amounts of gluten, other health problems, or refractory celiac disease.
Consuming small amounts of gluten
If your symptoms continue or come back after you start a gluten-free diet, you may still be eating or drinking a small amount of gluten. Keep a food journal and talk with your doctor and a registered dietitian about your diet and products you use that might contain gluten. Finding and avoiding all sources of gluten may help your symptoms improve. Hidden sources of gluten include additives made with wheat, such as
modified food starch
malt flavoring
preservatives
stabilizer
Other health problems
Your doctor may order tests to confirm the diagnosis of celiac disease and check for other health problems. Health problems that cause symptoms similar to those of celiac disease and may occur along with celiac disease include irritable bowel syndrome, lactose intolerance, microscopic colitis, problems with the pancreas, or small intestinal bacterial overgrowth.
Refractory celiac disease
Refractory celiac disease is a rare condition in which symptoms and damage to the small intestine continue or come back, even while a person is following a strict gluten-free diet. Refractory celiac disease may lead to complications, such as malnutrition or a type of cancer called enteropathy-associated T-cell lymphoma.
Therapies Under Investigation
Other tests include looking at the impact of malabsorption (due to celiac disease). The following can be monitored: full blood count, iron stores, folate, ferritin, levels of vitamin D and other fat-soluble vitamins, and bone mineral density.
Several novel therapeutic approaches that potentially could be used as alternatives for or additives to a gluten-free diet are being investigated (reviewed in Castillo et al [2015] and Rashtak & Murray [2012]):
Larazotide, a tight junction regulatory peptide that is considered to prevent the passage of gliadin peptides into the mucosa. This drug is in clinical trials.
Peptides that block the binding groove of DQ2 and DQ8 prevent activation of gluten-sensitive T cells. The viability of this approach is currently uncertain.
Transglutaminase (tTG) inhibitors
Cytokine blockers, particularly for refractory celiac disease. Of particular interest is an anti-IL15 antibody.
Drugs that selectively inhibit leukocyte adhesion and migration of lymphocytes into inflamed tissues
Detoxifying gluten, using oral proteases. Latiglutenase, a glutenous, is currently in clinical trials.
Gluten-sequestering polymers. An oral polymeric resin, P(HEMA-co-SS), binds to gluten and is under study.
Gluten tolerization. A peptide-based vaccine could desensitize or induce tolerance in individuals with celiac disease. A prototype vaccine, Nexvax2, involving a set of gluten peptides recognized by HLA-DQ2, is in clinical trials.
Rho/Rho-kinase inhibition to theoretically reverse the gluten-dependent increase in intestinal permeability [Sollid & Khosla 2011]
Antibodies to proteins involved in autoimmune pathologies, including anti-IFN-γ, anti-CD3, anti-CD20 therapy, and anti-IL-15. [Sollid & Khosla 2011]
Another approach: interfering with the homing of gluten-specific T cells to the gut mucosa by using CCR9 antagonists. A Phase II clinical trial is listed in Sollid & Khosla [2011].
accelerated osteoporosis NIH external link or bone softening, known as osteomalacia
anemia
malnutrition, a condition in which you don’t get enough vitamins, minerals, and other nutrients you need to be healthy
nervous system problems
problems related to the reproductive system
Rare complications can include
adenocarcinoma, a type of cancer of the small intestine
liver damage, which may lead to cirrhosis or liver failure
non-Hodgkin lymphoma
In rare cases, you may continue to have trouble absorbing nutrients even though you have been following a strict gluten-free diet. If you have this condition, called refractory celiac disease, your small intestine is severely damaged and can’t heal. You may need to receive intravenous (IV) nutrients and specialized treatment.
If you have coeliac disease, it’s crucial you do not eat any gluten. If you have untreated or undiagnosed coeliac disease and you’re still eating gluten, several complications can occur.
It’s a common misconception that eating a little gluten will not harm you. Eating even tiny amounts can trigger symptoms of coeliac disease and increase your risk of developing the complications outlined below.
Malabsorption
Malabsorption (where your body does not fully absorb nutrients) can lead to a deficiency of certain vitamins and minerals. This can cause conditions such as:
iron deficiency anaemia
vitamin B12 and folate deficiency anaemia
osteoporosis – a condition where your bones become brittle and weak
Malnutrition
As coeliac disease causes your digestive system to work less effectively, severe cases can sometimes lead to a critical lack of nutrients in your body. This is known as malnutrition, and can result in your body being unable to function normally or recover from wounds and infections.
If you have severe malnutrition, you may become fatigued, dizzy and confused. Your muscles may begin to waste away and you may find it difficult to keep warm. In children, malnutrition can cause stunted growth and delayed development.
Treatment for malnutrition usually involves increasing the number of calories in your diet and taking supplements.
Lactose intolerance
If you have coeliac disease, you’re more likely to also develop lactose intolerance, where your body lacks the enzyme to digest the milk sugar (lactose) found in dairy products. Lactose intolerance causes symptoms such as bloating, diarrhoea and abdominal discomfort.
Unlike gluten in coeliac disease, lactose does not damage your body. But you may get some gut-related symptoms when you eat foods containing lactose because you can’t digest it properly.
Lactose intolerance can be effectively treated by not eating and drinking dairy products that contain lactose. You may also need to take calcium supplements – dairy products are an important source of calcium, so you’ll need to compensate for not eating them.
Cancer
Cancer is a very rare but serious complication of coeliac disease.
Someone with coeliac disease has a slightly increased risk of developing certain cancers. Recent research shows that this increased risk is less than previously thought.
Cancers associated with coeliac disease are small bowel cancer, small bowel lymphoma and Hodgkin lymphoma. However, most people with coeliac disease will not develop any of these.
If you’ve been following a gluten-free diet for 3 to 5 years, your risk of developing these types of cancer is the same as that of the general population.
Coeliac disease in pregnancy
Poorly controlled coeliac disease in pregnancy can increase the risk of developing pregnancy-related complications, such as giving birth to a baby with a low birthweight.
How will I need to change my diet if I have celiac disease?
If you have celiac disease, you will need to remove foods and drinks that contain gluten from your diet. Following a gluten-free diet can relieve celiac disease symptoms and heal damage to the small intestine. People with celiac disease need to follow a gluten-free diet for life to prevent symptoms and intestinal damage from coming back. Your doctor or a registered dietitian can guide you on what to eat and drink to maintain a balanced diet.
If you or your child has been diagnosed with celiac disease, you may find support groups helpful as you learn about and adjust to a gluten-free lifestyle. Your doctor or a registered dietitian may be able to recommend support groups and other reliable sources of information.
What foods and drinks contain gluten?
Gluten occurs naturally in certain grains, including
wheat and types of wheat, such as durum, emmer, semolina, and spelled
barley, which may be found in malt, malt extract, malt vinegar, and brewer’s yeast
rye
triticale, a cross between wheat and rye
Gluten is found in foods that contain ingredients made from these grains, including baked goods, baking mixes, bread, cereals, and pasta. Drinks such as beer, lagers, ale, flavored liquors, and malt beverages may also contain gluten.
Many foods such as colorings, flavorings, starches, and thickeners—are made from grains that contain gluten. These ingredients are added to many processed foods, including foods that are boxed, canned, frozen, packaged, or prepared. Therefore, gluten may be found in a variety of foods, including candy, condiments, hot dogs and sausages, ice cream, salad dressing, and soups.
Cross-contact
Cross-contact occurs when foods or products that contain gluten come into contact with gluten-free foods. Cross-contact can spread gluten to gluten-free foods, making the gluten-free foods unsafe for people with celiac disease to consume. Cross-contact can occur at any time, including when foods are grown, processed, stored, prepared, or served.
How can I identify and avoid foods and drinks that contain gluten?
A registered dietitian can help you learn to identify and avoid foods and drinks that contain gluten when you shop, prepare foods at home, or eat out.
For example, when you shop and eat at home
carefully read food labels to check for grains that contain gluten—such as wheat, barley, and rye—and ingredients or additives made from those grains.
check for gluten-free food labeling.
don’t eat foods if you aren’t sure whether they contain gluten. If possible, contact the company that makes the food or visit the company’s website for more information.
store and prepare your gluten-free foods separately from other family members’ foods that contain gluten to prevent cross-contact.
When you eat out at restaurants or social gatherings
before you go out to eat, search online for restaurants that offer a gluten-free menu.
review restaurant menus online or call ahead to make sure a restaurant can accommodate you safely.
at the restaurant, let the server know that you have celiac disease. Ask about food ingredients, how food is prepared, and whether a gluten-free menu is available. Ask to talk with the chef if you would like more details about the menu.
when attending social gatherings, let the host know you have celiac disease and find out if gluten-free foods will be available. If not, or if you are unsure, bring gluten-free foods that are safe for you to eat.
What should I eat if I have celiac disease?
If you have celiac disease, you will need to follow a gluten-free diet. Your doctor and a registered dietitian can help you plan a healthy, balanced diet to make sure that you get the nutrients you need.
Gluten-free foods
Many foods, such as meat, fish, fruits, vegetables, rice, and potatoes, without additives or some seasonings, are naturally gluten-free. Flour made from gluten-free foods, such as potatoes, rice, corn, soy, nuts, cassava, amaranth, quinoa, buckwheat, or beans are safe to eat.
You can also buy packaged gluten-free foods, such as gluten-free types of baked goods, bread, and pasta. These foods are available from many grocery stores, restaurants, and at specialty food companies. Packaged gluten-free foods tend to cost more than the same foods that have gluten, and restaurants may charge more for gluten-free types of foods.
Talk with your doctor or a registered dietitian about whether you should include oats in your diet and how much. Research suggests that most people with celiac disease can safely eat moderate amounts of oats. If you do eat oats, make sure they are gluten-free. Cross-contact between oats and grains that contain gluten is common and can make oats unsafe for people with celiac disease.
Gluten-free labeling
The U.S. Food and Drug Administration (FDA) requires that foods labeled gluten-free meet specific standards. One requirement is that foods with the terms gluten-free, no gluten, free of gluten, or without gluten on the label must contain less than 20 parts per million of gluten. This amount of gluten is too small to cause problems in most people with celiac disease.
The FDA rule does not apply to foods regulated by the U.S. Department of Agriculture, including meat, poultry, and some egg products. The rule also does not apply to most alcoholic beverages, which are regulated by the U.S. Department of the Treasury.
Should I start a gluten-free diet before I talk with my doctor?
No. If you think you might have celiac disease, you should talk with your doctor about testing to diagnose celiac disease before you begin a gluten-free diet. If you avoid gluten before you have tested, the test results may not be accurate.
Also, if you start avoiding gluten without advice from a doctor or a registered dietitian, your diet may not provide enough of the nutrients you need, such as fiber, iron, and calcium. Some packaged gluten-free foods may be higher in fat and sugar than the same foods that contain gluten. If you are diagnosed with celiac disease, your doctor and dietitian can help you plan a healthy gluten-free diet.
If you don’t have celiac disease or another health problem related to gluten, your doctor may not recommend a gluten-free diet. In recent years, more people without celiac disease have begun avoiding gluten, believing that a gluten-free diet is healthier or could help them lose weight. However, researchers have found no evidence that a gluten-free diet promotes better health or weight loss for the general population.
Screening of persons at risk for celiac disease
Asymptomatic/atypical manifestations
first-degree relatives 10 – 20%
Down syndrome 5 – 12%
Ullrich–Turner syndrome 2 – 5%
Williams–Beuren syndrome 9%
selective IgA deficiency 2 – 8%
autoimmune thyroiditis 3 – 7%
autoimmune hepatitis (children) 12 – 13%
type 1 diabetes 2 – 12%
juvenile chronic arthritis 1.5 – 2.5%
Oligosymptomatic manifestations
failure to thrive
weight loss
short stature / growth retardation
delayed puberty (amenorrhea)
iron-deficiency anemia
anorexia
dyspeptic symptoms (nausea/vomiting)
chronic, recurrent abdominal pain (bloating)
chronic constipation
chronic fatigue/diminished performance
recurrent aphthous sores
chronic/intermittent diarrhea
difficulty concentrating
depressed mood
chronic headache
elevated transaminases
tooth-enamel defects
osteoporosis/osteopenia
Complications of classic celiac disease
acute global/selective malabsorption (anemia and other consequences)
Prolyl endopeptidases – Prolyl endopeptidases (PEPs) are endoproteolytic enzymes expressed in micro-organisms and plants. These enzymes cleave proline-rich gluten to smaller peptides that are ready for digestion by intestinal brush-border enzymes (aminopeptidases and carboxypeptidases). Limited efficiency was found, since PEP required 3 h preincubation with gluten containing foods to achieve full detoxification of peptides and to prevent intestinal transport of active gluten fragments[rx]. This is unlikely to be achieved by co-administration of PEP and gluten-containing diet.
A two-stages cross-over phase II clinical trial was performed using asymptomatic CD patients eating, a slice of bread daily and a slice of bread pre-treated with PEP daily[rx]. After 2 wk of PEP-treated gluten challenge, the majority of patients did not develop malabsorption, measured by fecal fat excretion and D-xylose malabsorption tests. The tests likely lacked the necessary sensitivity to assess minor malabsorption resulting from active CD, since no histological confirmation was performed to determine deterioration in the Marsh grading[rx]. When PEPs were consumed as jam spread on a slice of gluten-containing bread by CD patients, villous blunting was seen in small bowel biopsy histological evaluation in most patients[rx]. Further studies are needed to determine the appropriate dose of enzyme and time of administration relative to the quantity of ingested gluten.
ALV003 – ALV003, a mixture of two glutenases, an endoprotease from germinating barley and PEP, was pretreated with wheat flour and tested in CD patients[rx]. Symptoms typically associated with gluten ingestion were not significantly reduced by ALV003 pre-treatment, but ALV003 abolished immune responses induced by gluten in CD patients. A randomized controlled phase IIa clinical trial has been performed where CD patients received either ALV003 or placebo daily for 6 wk at the time of 2 g gluten contained bread. This proof-of-concept study demonstrated that ALV003 can attenuate gluten-induced small intestinal mucosal injury in CD patients[rx]. After six weeks period, biopsies proved lower small intestinal mucosal injury in patients treated with ALV003 than placebo-treated patients despite of persistent intestinal inflammation in many patients on a strict GFD. Placebo-treated patients were found to have suffered more adverse events, most commonly including abdominal distention, flatulence, eructation, abdominal pain and diarrhea[rx].
Lactobacilli – Lactobacilli added to sourdough for fermentation are able to lyse the proline-/glutamine-rich gluten peptides and thus decrease immunotoxicity[rx–rx]. A mixture of fermented wheat flour with oat, millet and buckwheat allows sourdough bread to retain its baking characteristics. A pilot study in patients with CD suggested that this bread was well tolerated[rx]. However, these patients were challenged for only 2 d, which is clearly not sufficient to draw any firm conclusions. Hence, another 60-d diet of fully hydrolyzed wheat flour with sourdough lactobacilli and fungal proteases (8 ppm residual gluten; n = 5) was further studied. The pretreated flour was rendered non-toxic by serological, morphometrical, and immunohistochemical analysis[rx]. A larger group of subjects in the trial and palatability of digested flour baked products needs to be taken into consideration.
VSL3 – VSL3 is a probiotic containing lyophilised bacteria, including bifidobacteria (Bifidobacterium longum, Bifidobacterium infantis and Bifidobacterium breve), lactobacilli (Lactobacillus acidophilus, Lactobacillus casei, Lactobacillus delbrueckii subsp., Lactobacillus bulgaricus and Lactobacillus plantarum) and Streptococcus salivarius subsp., Thermophiles. It is used to hydrolyse gliadin peptides in pre-treated flour and tested for efficacy in rat intestinal cell line and celiac jejunal biopsies[rx]. VSL3 pre-digested gliadins did not show an increase of the infiltration of CD3+ intraepithelial lymphocytes and caused a less pronounced effect on intestinal mucosa permeability (determined by lower F-actin rearrangement and zonulin release). Hence, VSL#3 may have importance during food processing to produce pre-digested gluten-free products.
Prevention of toxic gliadin peptide absorption
Larazotide – Larazotide (AT-1001, Alba Therapeutics, Baltimore, MA), is a synthetic hexapeptide derived from Zonula Occludens toxin of Vibrio cholera[rx]. It is used to inhibit the opening of tight junctions of the small intestine epithelial cells. Clinical trial phase I in CD patients suggested that Larazotide therapy is well tolerated by patients and reduces intestinal barrier dysfunction, proinflammatory cytokine production, and gastrointestinal symptoms in CD individuals after gluten exposure[rx]. Encouraging results were obtained from a 6-wk phase IIb trial in terms of symptoms and antibody titers[rx], showing larazotide acetate a promising drug candidate. This drug inhibits the paracellular route of gliadin absorption through tight junctions, which is not the only mechanism of gliadin absorption. Indeed, gliadin may gain access to the mucosa through transcellular pathways in addition to paracellular route[rx,rx]. Hence, this strategy might be best exploited in combination with other treatments.
Synthetic polymer poly (hydroxyethylmethacrylate-co-styrene sulfonate) – Poly (hydroxyethylmethacrylate-co-styrene sulfonate) [P (HEMA-co-SS)] forms supra-molecular particles upon gliadin complexation in gastric and intestinal conditions[rx,rx], and deteriorates gliadin’s effect on epithelial cells[rx]. This complexation decreases the effect of gastrointestinal (GI) digestive enzymes on gliadin absorption, and thus the formation of immunogenic peptides is reduced. Gluten-sensitive HLA-HCD4/DQ8 mice co-administered with P (HEMA-co-SS) showed attenuated gliadin-induced changes in permeability and inflammation[217]. Low side effect, cost and possibility to be taken, occasionally with gluten-containing food, makes it an attractive option. Further investigation of the mechanisms of action and its interaction with human tissues is required before its efficacy is investigated in human trials[rx].
Anti-gliadin egg yolk antibody – Oral antibody passive immunotherapy may be of value due to the advantages of reduced cost, ease of administration, and potential to treat localized conditions in the gastrointestinal tract[rx]. Among antibodies, chicken egg yolk immunoglobulin (IgY), is ideal for passive immunotherapy, as it may be readily obtained in large quantities from egg yolk, presenting a more cost-effective, convenient, and hygienic alternative to mammalian antibodies. Oral immunotherapeutic IgY is a promising alternative to neutralize gliadin in the GI tract and prevention it from absorption[rx]. Mannitol contained antibody preparation is highly resistant against GI enzymes and proved to effectively neutralized gliadin under simulated GI conditions in the presence of food. In vivo study; BALB/c mice fed with IgY formulation and gliadin ratio of 1:5 (w/w), demonstrated that gliadin absorption in the gastrointestinal tract was minimal at < 1%[rx]. Further investigations in CD patients is requires to prove its efficacy and determine dosing regimen of antibody relative to the amount of gliadin ingestion.
Blockage of selective deamidation of specific glutamine residues by tissue transglutaminase 2 inhibitor
Transglutaminases (a family of eight enzymes) have diverse functions in human and are involved in several biological and pathological processes[rx]. tTG2 is an enzyme that has a pro-inflammatory effect and increases the immunostimulatory epitopes present in the lamina propria of the small intestine. Blockage of tTG2 may be a promising approach to inhibit the inflammatory process upon gluten ingestion. There are two essential classes of tTG2 inhibitors; irreversible and reversible inhibitors[rx]. Irreversible inhibitors form a stable covalent bond with this enzyme, and thus prevent deamidation of gliadin peptides[rx,rx]. Reversible inhibitors are more desirable to minimize possible side effects. These include aldehyde-bearing tTG modulators[rx], cinnamoyl triazole derivatives[rx], and the highly specific modified peptide targeting the active cysteine site of tTG2[rx]. Since a few gluten T-cell epitopes can be recognized without being deamidated by tTG2[rx,rx], this approach will not inhibit the innate response[rx], or the immune response induced by non-deamidated peptides[rx]. To be able to use tTG2 inhibitors clinically, it is critical to design highly specific inhibitors, since all human tTG share high sequence homology.
Vaccine application to restore immune tolerance towards gluten
Autoimmune enteropathy in CD has been proposed to be due to impairment of immunoregulatory mechanisms that controls oral tolerance. Systematic peptide mapping of T-cell was performed to determine gliadin reactive epitopes recognized by approximately 90% of CD patients. A clinical trial phase I study has been initiated as Nexvax2 (Nexpep Pty, Ltd., Australia) peptide vaccine-containing mixture of immunotoxic α- and ω-gliadins and B-hordein[rx].
Engineered Lactococcus lactis secreting a DQ8-re-stricted gliadin peptide administered orally[rx], or recombinant α-gliadin in HLA-DQ8 administered intranasally in transgenic mouse model[rx], have been studied to modulate immune response to gluten. However, it is difficult to appreciate how the vaccine or the intranasal peptide administration can modulate the Tr1 response. More work is needed to assess the effect of these therapies on the spectrum of gluten peptides presented to the gut.
Dermal inoculation of human hookworm (Necator americanus) has also been used to modulate the immune response to gluten[rx]. A phase II trial with CD patients suggested that hookworm infection on its own may not obviate the necessity for a restricted diet in CD, but appears to be safe and might impact on immune pathology[rx]. Here in, hookworm infection is expected to reduce gluten sensitivity and immune reactivity.
Modulation of immune response to dietary gliadin
HLA-DQ blocker: HLA-DQ blocker is used to block the binding sites of HLA-DQ2 or DQ8 for it to be unrecognized by T cells as well to block the presentation of the antigen. This is not a new concept that was developed without much success to treat type 1 diabetes mellitus and rheumatoid arthritis, due to difficulties in effective drug delivery[rx,rx]. By amino-acid substitution of gliadin T-cell stimulatory sequence, the epitope can be converted to an agonist or antagonist, abolishing the inflammatory cascade[rx]. IFN-γ production by peripheral blood lymphocytes was prevented when either an alanine or lysine amino acid was substituted through the immunodominant α-gliadin peptide, corresponding to the peptide’s anchor to the HLA-DQ cleft[rx]. To develop this as a new therapeutic agent, more studies need to be performed, looking at the mass T-cell action of the gut towards these modified peptides.
Interleukin blocker – Modulation of cytokine production has been evaluated for the treatment of several autoimmune diseases, although their side effects may be severe. Modulation of proinflammatory IL-15 and anti-inflammatory IL-10 cytokines has been suggested to influence the immune balance between tolerance and autoimmunity[rx,rx–rx]. Blocking IL-15 may promote maintenance of epithelial integrity, limit epithelial destruction, leading to decreased passage of dietary gliadin.
NKG2D antagonists – MICA molecules, strongly expressed on active CD epithelial cell surface upon gliadin challenge[rx], interact with the NKG2D-activating receptor on human natural killer cells and CD8 T cells, leading to villous atrophy due to an IEL-mediated damage to enterocytes[rx,rx]. Thus, NKG2D antagonists[rx] and anti-NKG2D antibodies[rx], have been proposed as therapeutics in CD.
Restoration of intestinal architecture by R-spondin-1
R-spondin-1 is an intestinal mitogen, shown to stimulate crypt cell growth, accelerate mucosal regeneration and restore intestinal architecture in mouse models of colitis[rx]. This agent has yet to be tested in human to be considered as a therapeutic agent in CD.
Lifestyle and home remedies
If you’ve been diagnosed with celiac disease, you’ll need to avoid all foods that contain gluten. Ask your doctor for a referral to a dietitian, who can help you plan a healthy gluten-free diet.
Read labels
Avoid packaged foods unless they’re labeled as gluten-free or have no gluten-containing ingredients, including emulsifiers and stabilizers that can contain gluten. In addition to cereals, pastas and baked goods, other packaged foods that can contain gluten include:
Beers, lagers, ales and malt vinegars
Candies
Gravies
Imitation meats or seafood
Processed luncheon meats
Rice mixes
Salad dressings and sauces, including soy sauce
Seasoned snack foods, such as tortilla and potato chips
Seitan
Self-basting poultry
Soups
Pure oats aren’t harmful for most people with celiac disease, but oats can be contaminated by wheat during growing and processing. Ask your doctor if you can try eating small amounts of pure oat products.
Allowed foods
Many basic foods are allowed in a gluten-free diet, including:
Eggs
Fresh meats, fish and poultry that aren’t breaded, batter-coated or marinated
Fruits
Lentils
Most dairy products, unless they make your symptoms worse
Nuts
Potatoes
Vegetables
Wine and distilled liquors, ciders and spirits
Grains and starches allowed in a gluten-free diet include:
Malnutrition – This occurs if your small intestine can’t absorb enough nutrients. Malnutrition can lead to anemia and weight loss. In children, malnutrition can cause slow growth and short stature.
Bone weakening – Malabsorption of calcium and vitamin D can lead to a softening of the bone (osteomalacia or rickets) in children and a loss of bone density (osteopenia or osteoporosis) in adults.
Infertility and miscarriage – Malabsorption of calcium and vitamin D can contribute to reproductive issues.
Lactose intolerance – Damage to your small intestine might cause you abdominal pain and diarrhea after eating or drinking dairy products that contain lactose. Once your intestine has healed, you might be able to tolerate dairy products again.
Cancer – People with celiac disease who don’t maintain a gluten-free diet have a greater risk of developing several forms of cancer, including intestinal lymphoma and small bowel cancer.
Nervous system problems – Some people with celiac disease can develop problems such as seizures or a disease of the nerves to the hands and feet (peripheral neuropathy).
Coeliac disease also known as celiac sprue is a unique autoimmune, genetic element (human leukocyte antigen (HLA)-DQ2 and HLA-DQ8), based gluten-sensitive immune-mediated enteropathic with the auto-antigen involved (tissue transglutaminase (tTG)), and the environmental trigger (gluten) are all well-defined condition where the immune system mistakes healthy cells for harmful ones and produces antibodies which result in the small intestine becoming inflamed and less able to absorb nutrients, maldigestion, and malabsorption of most nutrients and vitamins. It can cause a range of symptoms including diarrhea.
Celiac disease (CD) is an autoimmune condition characterized by a specific serological and histological profile triggered by gluten ingestion in genetically predisposed individuals [rx]. Gluten is the general term for alcohol-soluble proteins present in various cereals, including wheat, rye, barley, spelled, and Kamut [rx].
Celiac disease is a chronic digestive and immune disorder that damages the small intestine. The disease is triggered by eating foods containing gluten. Gluten is a protein found naturally in wheat, barley, and rye, and is common in foods such as bread, pasta, cookies, and cakes. Many products contain gluten, such as prepackaged foods, lip balms and lipsticks, toothpaste, vitamin and nutrient supplements, and, rarely, medicines.
Types of Celiac Disease
Recently a consensus paper redefined the types of celiac disease.
Classic celiac disease – refers to the presence of symptoms of malabsorption such as diarrhea, failure to thrive, and weight loss and may occur in adults and children.
Non-classic celiac disease – refers to celiac disease without prominent gastrointestinal symptoms or malabsorption; however, individuals with atypical celiac disease can also have gastrointestinal symptoms such as reflux, abdominal pain, bloating, vomiting, constipation, and dyspepsia. Approximately 70% of individuals are diagnosed based on extraintestinal manifestations associated with celiac disease. This group includes monosymptomatic and subclinical forms.
Marsh classification of histologic findings in celiac disease
Marsh 0
Normal mucosal architecture without significant intraepithelial lymphocytic infiltration.
Marsh I
Lymphocytic enteritis: Normal mucosal architecture with a marked infiltration of villous epithelium by lymphocytes; arbitrarily defined marked as more than 30 lymphocytes per 100 enterocytes
Marsh II
Lymphocytic enteritis with crypt hyperplasia: intraepithelial lymphocytosis and elongation and branching of crypts in which there is an increased proliferation of epithelial cells
Marsh III
Intraepithelial lymphocytosis, crypt hyperplasia, and villous atrophy. There are 3 distinct stages of villous atrophy
Marsh IIIA
Partial villous atrophy, the villi are blunt and shortened. Arbitrarily, samples are classified as partial villous atrophy if the villus-crypt ratio was less than 1:1
Marsh IIIB
Subtotal villous atrophy, villi are clearly atrophic but still recognizable
Marsh IIIC
Total villous atrophy, villi are rudimentary or absent, and the mucosa resembles colonic mucosa.
Causes of Coeliac disease
The symptoms of celiac disease are due to the damage of enterocytes in the small intestine. In the full-blown clinical picture, the typical features of the small intestine are chronic inflammation and villi atrophy. [rx][rx][rx]
An individual has to have HLA-dominant DQ2 or DQ8 genes. The disease is a result of the immune system reacting adversely to gluten, and one of the important proteins involved is an antibody to tissue transglutaminase. There are however other pathways proposed that contribute to the disease. The glycoprotein gliadin (present in gluten) has a direct toxic effect on enterocytes by the up-regulating production of IL-15.
Celiac disease is also called celiac sprue, nontropical sprue, and gluten-sensitive enteropathy.
Celiac disease can only occur in people who have certain genes. You are more likely to develop the celiac disease if someone in your family has the disease.
Celiac disease affects children and adults in all parts of the world. In the United States, celiac disease is more common among white Americans than among other racial or ethnic groups. A celiac disease diagnosis is more common in females than in males.
Celiac disease is also more common in people who have certain chromosomal disorders, such as Down syndrome, Turner syndrome, and Williams syndrome.
Experts have found that some people have both celiac disease and other disorders related to the immune system. These disorders include
type 1 diabetes
thyroid diseases, such as Hashimoto’s disease, Graves’ disease, Addison’s disease, and primary hyperparathyroidism
selective immunoglobulin A (IgA) deficiency, a condition in which your body makes little or no IgA, an antibody that fights infections
rheumatic diseases, such as Sjögren’s syndrome NIH external link
liver diseases, such as autoimmune hepatitis, primary sclerosing cholangitis, and primary biliary cholangitis
Research suggests that celiac disease only occurs in people who have certain genes and eat food that contains gluten. Experts are studying other factors that may play a role in causing the disease.
Genes
The celiac disease almost always occurs in people who have one of two groups of normal gene variants, called DQ2 and DQ8. People who do not have these gene variants are very unlikely to develop celiac disease. About 30 percent of people have DQ2 or DQ8. However, only about 3 percent of people with DQ2 or DQ8 develop celiac disease.4
Researchers are studying other genes that may increase the chance of developing celiac disease in people who have DQ2 or DQ8.
Gluten
Consuming gluten triggers the abnormal immune system response that causes celiac disease. However, not all people who have the gene variants DQ2 or DQ8 and eat gluten develop the disease. Research suggests that among children with a genetic predisposition for celiac disease, those who eat more gluten in early childhood may have a greater risk for celiac disease.
Other factors
Researchers are studying other factors that may increase a person’s chances of developing celiac disease. For example, research suggests that a higher number of infections in early life and certain digestive tract infections may increase the risk. Experts also think changes in the microbiome—the bacteria in the digestive tract that help with digestion—could play a role in the development of celiac disease.
Symptoms of Celiac Disease
Symptoms of celiac disease vary widely, and a person may have multiple symptoms that come and go. If you have celiac disease, you may have digestive problems or other symptoms. Digestive symptoms are more common in children than in adults. Digestive symptoms of celiac disease may include
The main symptoms are stomach pain, gas, and bloating, diarrhea, weight loss, anemia, edema, bone or joint pain.
Anemia due to defective absorption of vitamin B12, folate, or iron
Coagulopathy due to impaired absorption of vitamin K
Osteoporosis
Neurological symptoms like muscle weakness, paresthesias, seizures, and ataxia
bloating
chronic diarrhea
constipation
gas
lactose intolerance due to damage to the small intestine
loose, greasy, bulky, and bad-smelling stools
nausea or vomiting
pain in the abdomen
frequent bouts of diarrhea or loose stools
nausea, feeling sick, and vomiting
stomach pain and cramping
lots of gas and bloating
feeling tired all the time, ongoing fatigue
anemia (you would be told if you’re anemic following a blood test)
weight loss (although not in all cases)
regular mouth ulcers
constipation or hard stools
For children with celiac disease, being unable to absorb nutrients at a time when they are so important to normal growth and development can lead to
damage to the permanent teeth’s enamel
delayed puberty
failure to thrive, meaning that an infant or a child weighs less or is gaining less weight than expected for his or her age
mood changes or feeling annoyed or impatient
slowed growth and short height
weight loss
Anemia due to defective absorption of vitamin B12, folate or iron
Coagulopathy due to impaired absorption of vitamin K
Osteoporosis
Neurological symptoms like muscle weakness, paresthesias, seizures and ataxia
Some people with celiac disease have symptoms that affect other parts of the body. These symptoms may include
dermatitis herpetiformis
fatigue, or feeling tired
joint or bone pain
mental health problems, such as depression or anxiety
nervous system symptoms, such as headaches, balance problems, seizures, or peripheral neuropathy
reproductive problems in women and girls—which may include infertility, delayed start of menstrual periods, missed menstrual periods, or repeated miscarriages and male infertility
symptoms involving the mouth, such as canker sores; a dry mouth; or a red, smooth, shiny tongue
Anemia due to defective absorption of vitamin B12, folate or iron
Coagulopathy due to impaired absorption of vitamin K
Osteoporosis
Neurological symptoms like muscle weakness, paresthesias, seizures and ataxia
Most people with celiac disease have one or more symptoms before they are diagnosed and begin treatment. Symptoms typically improve and may go away after a person begins eating a gluten-free diet. Symptoms may return if a person consumes small amounts of gluten.
Depending on how old you are when a doctor diagnoses your celiac disease, some symptoms, such as short height and tooth defects, may not improve. People with celiac disease who have no symptoms can still develop complications over time if they do not get treatment.
Individuals with disorders associated with celiac disease (e.g., Down syndrome, Turner syndrome, Williams syndrome, selective IgA deficiency, insulin-dependent diabetes mellitus, Sjögren syndrome, thyroiditis)
Absence of history of self-limited enteritis and/or tropical sprue
According to NCBI.NLM.NIH symptoms are
The following extraintestinal symptoms are secondary to malabsorption [rx,rx]
Peripheral neuropathy (vitamin B12 and B1 deficiency)
Anemia (iron, vitamin B12 and folate deficiency)
Growth failure in children
Bone pain (osteoporosis and osteopenia, vitamin D and calcium deficiency)
Muscle cramps (magnesium and calcium deficiency)
Night blindness (vitamin A deficiency)
Weight loss (impaired absorption of most nutrients)
Edema (protein and albumin loss)
Weakness (hypokalemia and electrolyte depletion)
Bleeding and hematoma (vitamin K deficiency)
The following extraintestinal symptoms/manifestations are probably not secondary to malabsorption (atypical CD) [rx]
Neurological disorders such as depression, epilepsy, migraine, ataxia
Dermatitis herpetiformis
Elevated liver enzymes, liver failure
Infertility
Stomatitis
IgA nephritis
Myocarditis
Idiopathic pulmonary hemosiderosis
Arthritis
The following diseases/conditions are associated with celiac disease [rx–rx]
Autoimmune diseases such as type 1 diabetes, Sjögren syndrome, thyroid diseases (Hashimoto’s thyroiditis and Graves’s disease), autoimmune hepatitis and primary biliary cirrhosis
Selective IgA deficiency
Turner’s syndrome
Down’s syndrome
Dermatitis herpetiformis
Dermatitis herpetiformis is an itchy, blistering skin rash that usually appears on the elbows, knees, buttocks, back, or scalp. Among people with untreated celiac disease, about 2 to 3 percent of children and 10 to 20 percent of adults have dermatitis herpetiformis.3 Some people with celiac disease may have the rash and no other symptoms. After a person starts a gluten-free diet, the rash may take some time to heal and may return if a person consumes small amounts of gluten.
Children
Children with celiac disease are more likely than adults to have digestive problems, including:
Nausea and vomiting
Chronic diarrhea
Swollen belly
Constipation
Gas
Pale, foul-smelling stools
The inability to absorb nutrients might result in:
Failure to thrive for infants
Damage to tooth enamel
Weight loss
Anemia
Irritability
Short stature
Delayed puberty
Neurological symptoms, including attention-deficit/hyperactivity disorder (ADHD), learning disabilities, headaches, lack of muscle coordination and seizures
Diagnosis of Celiac Disease
Doctors use information from your medical and family history, a physical exam, a dental exam, and medical test results to look for signs that you might have celiac disease and should be tested. Doctors typically diagnose celiac disease with blood tests and biopsies of the small intestine.
Medical and family history
Your doctor will ask about your symptoms.
Celiac disease isn’t diagnosed based on symptoms alone because some of the symptoms are like the symptoms of other digestive disorders, such as irritable bowel syndrome (IBS) or lactose intolerance. Some people with celiac disease have symptoms that affect parts of the body outside the digestive tract.
The doctor will review your medical history, including your history of conditions that are more common in people who have celiac disease. Your doctor will also ask about your family’s medical history and whether anyone in your family has been diagnosed with celiac disease.
Physical exam
During a physical exam, a doctor may
check for signs of weight loss or growth problems
examine your skin for rashes, such as dermatitis herpetiformis
listen to sounds in the abdomen using a stethoscope
tap on the abdomen to check for pain or swelling
In some cases, a dentist may notice signs of celiac disease during an exam. Celiac disease may cause problems with the teeth and mouth, such as defects in tooth enamel or canker sores.
Doctors most often use blood tests and biopsies of the small intestine to diagnose or rule out celiac disease. Doctors don’t recommend starting a gluten-free diet before diagnostic testing because a gluten-free diet can affect test results.
In some cases, doctors may order additional tests, such as skin biopsies and genetic tests, to help diagnose or rule out celiac disease.
Lab Test
Blood tests – A health care professional will take a blood sample from you and send the sample to a lab. Blood tests can show levels of certain antibodies that are often higher than normal in people who have untreated celiac disease. Blood tests may also show signs of health problems that could be related to celiac disease, such as anemia.
Biopsies of the small intestine – A doctor obtains biopsies of the small intestine during an upper GI endoscopy. For an upper GI endoscopy, a doctor uses an endoscope—a flexible tube with a camera—to see the lining of your upper GI tract, including the first part of your small intestine. The doctor passes an instrument through the endoscope to take small pieces of tissue from your small intestine. A pathologist will examine the tissue under a microscope to look for signs of celiac disease.
Skin biopsies – A doctor may order skin biopsies if you have a rash that could be dermatitis herpetiformis. For skin biopsies, a doctor removes small pieces of skin tissue on and next to the rash. A pathologist will examine the tissue under a microscope to look for signs of dermatitis herpetiformis.
Genetic testing – In some cases, a health care professional may take a blood sample or use a swab to collect cells from the inside of your cheek. The sample will be tested for groups of gene variants called DQ2 and DQ8. If you do not have these gene variants, you are very unlikely to have celiac disease. Having DQ2 or DQ8 alone does not mean you have celiac disease. Most people with these gene variants do not develop celiac disease. If you do have DQ2 or DQ8, your doctor may recommend additional tests to check for or rule out celiac disease.
HLA tests – Based on studies for which sensitivity could be calculated, the ACG estimated the negative predictive value of the HLA-DQ2/HLA-DQ8 combination test at more than 99 percent in diagnosing celiacdisease.
Screening is testing – for diseases when you have no symptoms. Doctors in the United States do not routinely screen people for celiac disease. However, blood relatives of people with celiac disease and those with type 1 diabetes should talk with their doctor about their chances of getting the disease to see if they should be tested.
Endoscopy – This test uses a long tube with a tiny camera that’s put into your mouth and passed down your throat (upper endoscopy). The camera enables your doctor to view your small intestine and take a small tissue sample (biopsy) to analyze for damage to the villi.
Capsule endoscopy – This test uses a tiny wireless camera to take pictures of your entire small intestine. The camera sits inside a vitamin-sized capsule, which you swallow. As the capsule travels through your digestive tract, the camera takes thousands of pictures that are transmitted to a recorder.
Serological tests
Anti-tissue transglutaminase antibodies – the best strategy for serological diagnosis is the blood detection of IgA anti-tissue transglutaminase antibodies (tTGA) by enzyme-linked immunosorbent assay (ELISA). These antibodies show a sensitivity up to 97%, a specificity around 96%, and an accuracy of 98%, whereas IgA anti-endomysial (IgA EMA) antibodies are employed as a confirmatory test in tTGA positive cases due to their higher specificity (about 100% vs 91% of tTGA). In concomitance of IgA deficiency and celiac disease, found in around 2%-10% of the patients, it is recommended to detect celiac disease testing tTG-IgG. “False-negative” occurs, as previously reported, in the case of IgA deficiency. The IgA EMA represents the most specific test (approximately 100%), with a sensitivity around 94% and a diagnostic accuracy of 97%[rx]. However, EMA is routinely detected by indirect subjective immunofluorescence[rx]. These antibodies can also result falsely negative in case of IgA deficiency and in children aged > 2 years.
Anti-gliadin antibodies – The antigliadin (AGA) antibodies (IgG and IgA) are today no longer recommended because of their low sensitivity and specificity and inferior accuracy, except in younger children[rx].
Deamidated gliadin peptides – Actually detection of antigliadin antibodies has been replaced by the more recently developed immunoassays employing antibodies to deamidated gliadin peptides, IgA and IgG. To increase the diagnostic accuracy, in the last years the clinicians tend to prescribe serial testing.
Blood tests check other parts of your immune system.
Intestinal fatty acid binding protein tests show if there’s damage to the intestine.
A complete blood count looks for anemia (low red blood cells).
C-reactive protein tests show if there’s inflammation.
Metabolic panels test liver and kidney function.
Vitamin D, B12, and folate tests look for vitamin deficiencies.
Iron and ferritin tests look for iron deficiency.
Swallowing a small camera can show problems in your digestive tract.
Imaging tests show signs in the intestine, like wall thickening or changes to blood vessels.
Genetic testing looks for human leukocyte antigens to rule out celiac disease.
Electrolytes may reveal hypocalcemia, hypokalemia, metabolic acidosis
Anemia due to deficiency of folate, iron or Vit B12
Prothrombin time may be prolonged
Stool are greasy and have a rancid odor
In individuals on a gluten-containing diet:
Elevated serum tissue transglutaminase (tTG) IgA
Elevated serum anti-deamidated gliadin-related peptide (a-DGP) IgA and IgG
Elevated serum endomysial antibody (EMA) IgA; highest specificity (~99%) but sensitivity subject to observer variability
Treatment for Celiac Disease
Gluten-free diet
Doctors treat celiac disease by helping people to follow a gluten-free diet. Gluten is a protein found naturally in certain grains, including wheat, barley, and rye. Gluten is also added to many other foods and products. In people who have celiac disease, consuming gluten triggers an abnormal immune system reaction that damages the small intestine.
Symptoms greatly improve for most people with celiac disease who stick to a gluten-free diet. For most people, following a gluten-free diet will heal damage in the small intestine and prevent more damage. Many people see symptoms improve within days to weeks of starting the diet.
Your doctor will explain the gluten-free diet and may refer you to a registered dietitian who specializes in treating people who have celiac disease. The dietitian will teach you how to avoid gluten while following a healthy diet and recommend substitutes for foods that contain gluten. He or she will help you
check food and product labels for gluten
design everyday meal plans
make healthy choices about foods and drinks
Avoiding medicines and other products that may contain gluten
In addition to prescribing a gluten-free diet, your doctor will want you to avoid all hidden sources of gluten. If you have celiac disease, ask a pharmacist about ingredients in
herbal and nutritional supplements
prescription and over-the-counter medicines
vitamin and mineral supplements
Medicines are rare sources of gluten. Even if gluten is present in a medicine, it is likely to be in such small quantities that it would not cause any symptoms.
Other products can be hidden sources of gluten. You may take in small amounts of gluten if you consume these products, use them around your mouth, or transfer them from your hands to your mouth by accident. Products that may contain gluten include
children’s modeling dough, such as Play-Doh
cosmetics
lipstick, lip gloss, and lip balm
skin and hair products
toothpaste and mouthwash
communion wafers
Reading product labels can sometimes help you avoid gluten. Some companies label their products as being gluten-free. In the United States, products labeled gluten-free must have less than 20 parts per million of gluten, which should not be a problem for the vast majority of people. If a label doesn’t tell you what is in a product, ask the company that makes the product for an ingredients list. You cannot assume that the product is gluten-free.
Gluten-degrading enzymes
Enzyme supplement therapy with bacterial prolyl-endopeptidases expressed by various microorganisms has been proposed to accelerate gluten digestion in the gastrointestinal tract and thus to destroy T cell epitopes[rx]. Prolyl-endopeptidases are proline-specific enzymes capable to cleave gluten peptides. Actually, there are introduced into clinical trials two drug candidates, ALV003 and AN-PEP (Aspergillus niger prolyl-endoprotease). Recent data on results of two phases 1 clinical trials have revealed that pre-treating gluten with ALV003 eliminates the peripheral blood T cell response in celiac disease patients, suggesting the potential therapeutic utility of gluten-specific enzymes to treat celiac disease[rx]. Currently is undergoing clinical phase IIa testing showing significantly reduce gluten-related T-cell responses compared with placebo but without a significant reduction of symptoms typically induced by the gluten[rx].
AN-PEP is an enzyme that degrades gluten peptides efficiently in a pH compatible with that found in the stomach. Therefore this enzyme might be suitable for oral supplementation but further studies are necessary[rx].
Modified grains
Can be developed either through selective breeding of early wheat species or using small interfering RNA (siRNA) technology to mutate or silence immunostimulatory sequence[tx].
Blocking gluten entry across the intestinal epithelium
Zonulin inhibitor larazotide (AT-1001) corrects intestinal barrier defects. It has been explored in an animal model[rx]. AT-1001 is currently the best-studied pharmacologic agent to treat patients with celiac disease, actually undergone in phase II clinical trials[rx]. It has been shown that patients treated with AT-1001 had an improved symptom score, a less pronounced autoantibody response and pro-inflammatory production, and lower urinary nitrate excretion when compared with the placebo controls[rx].
Rho/Rho-kinase inhibition
It has been clarified that the increase in intestinal permeability is dependent on Rho kinase (ROCK) activity[rx]. In addition to regulating tight junction structure and function, ROCK is known to regulate axon growth[rx,rx]. The drug could be used to establish whether ROCK inhibition can reverse the gluten-dependent increase in intestinal permeability in these patients[rx].
Immunotherapy
The first observation of the occurrence of celiac disease following allogeneic bone marrow transplantation performed in a patient with acute leukemia, made evident the involvement of T-lymphocyte in the pathogenesis of this condition[rx]. Since then, a lot of acknowledgments have been acquired such that many efforts are being made to develop immunologic therapeutic tools. Cytokine therapies based either on amplification of regulatory cytokines or on blockage of inflammatory cytokines expression are largely diffused for management of severe autoimmune disorders. Also for celiac disease resistant to dietary approach and especially for refractory celiac disease, the use of immunomodulators is developing. IL-15 blocking antibodies have shown the capability to induce intra-epithelial lymphocytes apoptosis in the intestinal epithelium of human IL-15 transgenic mouse models[rx].
Continues RX
Treatment with a gluten-free diet should be started only after the diagnosis has been established by intestinal biopsy.
A dietitian experienced in treating celiac disease should be involved.
Symptoms may improve rapidly while serologic tests may take up to 12 months to normalize on the gluten-free diet.
For some individuals, even a small amount of gluten (i.e., 100 mg) can damage the small intestine. Note that a slice of bread contains approximately 2.5 grams of gluten.
It can be difficult to adhere to the gluten-free diet, as gluten is found in many foods and other ingested products. Some hidden sources of gluten:
Non-starchy foods such as soy sauce and beer
Non-food items such as some medications and cosmetics (e.g., lipstick)
Nutritional deficiencies and metabolic bone disease should be treated in the usual manner.
Therapies Under Investigation
Several novel therapeutic approaches that potentially could be used as alternatives for or additives to a gluten-free diet are being investigated (reviewed in Castillo et al [2015] and Rashtak & Murray [2012]):
Larazotide, a tight junction regulatory peptide that is considered to prevent the passage of gliadin peptides into the mucosa. This drug is in clinical trials.
Peptides that block the binding groove of DQ2 and DQ8 to prevent activation of gluten-sensitive T cells. The viability of this approach is currently uncertain.
Transglutaminase (tTG) inhibitors
Cytokine blockers, particularly for refractory celiac disease. Of particular interest is an anti-IL15 antibody.
Drugs that selectively inhibit leukocyte adhesion and migration of lymphocytes into inflamed tissues
Detoxifying gluten, using oral proteases. Latiglutenase, a glutenous, is currently in clinical trials.
Gluten-sequestering polymers. An oral polymeric resin, P(HEMA-co-SS), binds to gluten and is under study.
Gluten tolerization. A peptide-based vaccine could desensitize or induce tolerance in individuals with celiac disease. A prototype vaccine, Nexvax2, involving a set of gluten peptides recognized by HLA-DQ2, is in clinical trials.
Rho/Rho-kinase inhibition to theoretically reverse the gluten-dependent increase in intestinal permeability [Sollid & Khosla 2011]
Antibodies to proteins involved in autoimmune pathologies, including anti-IFN-γ, anti-CD3, anti-CD20 therapy, and anti-IL-15. [Sollid & Khosla 2011]
Another approach: interfering with the homing of gluten-specific T cells to the gut mucosa by using CCR9 antagonists. A Phase II clinical trial is listed in Sollid & Khosla [2011].
Follow-up
Your doctor may recommend regular follow-up visits to make sure symptoms and health problems related to celiac disease are improving on a gluten-free diet. Follow-up may include blood tests to check levels of certain antibodies, which are higher in untreated celiac disease but typically return to normal after treatment. In some cases, doctors may recommend additional biopsies to find out if the small intestine has healed.
What if a gluten-free diet isn’t working?
If you continue to have celiac disease symptoms while you are following a gluten-free diet, talk with your doctor or a registered dietitian, who can help you find the cause. In about 20 percent of people with celiac disease, symptoms continue or come back even while they are following a gluten-free diet.7 Symptoms may be caused by consuming small amounts of gluten, other health problems, or refractory celiac disease.
Consuming small amounts of gluten
If your symptoms continue or come back after you start a gluten-free diet, you may still be eating or drinking a small amount of gluten. Keep a food journal and talk with your doctor and a registered dietitian about your diet and products you use that might contain gluten. Finding and avoiding all sources of gluten may help your symptoms improve. Hidden sources of gluten include additives made with wheat, such as
modified food starch
malt flavoring
preservatives
stabilizer
Other health problems
Your doctor may order tests to confirm the diagnosis of celiac disease and check for other health problems. Health problems that cause symptoms similar to those of celiac disease and may occur along with celiac disease include irritable bowel syndrome, lactose intolerance, microscopic colitis, problems with the pancreas, or small intestinal bacterial overgrowth.
Refractory celiac disease
Refractory celiac disease is a rare condition in which symptoms and damage to the small intestine continue or come back, even while a person is following a strict gluten-free diet. Refractory celiac disease may lead to complications, such as malnutrition or a type of cancer called enteropathy-associated T-cell lymphoma.
Therapies Under Investigation
Other tests include looking at the impact of malabsorption (due to celiac disease). The following can be monitored: full blood count, iron stores, folate, ferritin, levels of vitamin D and other fat-soluble vitamins, and bone mineral density.
Several novel therapeutic approaches that potentially could be used as alternatives for or additives to a gluten-free diet are being investigated (reviewed in Castillo et al [2015] and Rashtak & Murray [2012]):
Larazotide, a tight junction regulatory peptide that is considered to prevent the passage of gliadin peptides into the mucosa. This drug is in clinical trials.
Peptides that block the binding groove of DQ2 and DQ8 prevent activation of gluten-sensitive T cells. The viability of this approach is currently uncertain.
Transglutaminase (tTG) inhibitors
Cytokine blockers, particularly for refractory celiac disease. Of particular interest is an anti-IL15 antibody.
Drugs that selectively inhibit leukocyte adhesion and migration of lymphocytes into inflamed tissues
Detoxifying gluten, using oral proteases. Latiglutenase, a glutenous, is currently in clinical trials.
Gluten-sequestering polymers. An oral polymeric resin, P(HEMA-co-SS), binds to gluten and is under study.
Gluten tolerization. A peptide-based vaccine could desensitize or induce tolerance in individuals with celiac disease. A prototype vaccine, Nexvax2, involving a set of gluten peptides recognized by HLA-DQ2, is in clinical trials.
Rho/Rho-kinase inhibition to theoretically reverse the gluten-dependent increase in intestinal permeability [Sollid & Khosla 2011]
Antibodies to proteins involved in autoimmune pathologies, including anti-IFN-γ, anti-CD3, anti-CD20 therapy, and anti-IL-15. [Sollid & Khosla 2011]
Another approach: interfering with the homing of gluten-specific T cells to the gut mucosa by using CCR9 antagonists. A Phase II clinical trial is listed in Sollid & Khosla [2011].
accelerated osteoporosis NIH external link or bone softening, known as osteomalacia
anemia
malnutrition, a condition in which you don’t get enough vitamins, minerals, and other nutrients you need to be healthy
nervous system problems
problems related to the reproductive system
Rare complications can include
adenocarcinoma, a type of cancer of the small intestine
liver damage, which may lead to cirrhosis or liver failure
non-Hodgkin lymphoma
In rare cases, you may continue to have trouble absorbing nutrients even though you have been following a strict gluten-free diet. If you have this condition, called refractory celiac disease, your small intestine is severely damaged and can’t heal. You may need to receive intravenous (IV) nutrients and specialized treatment.
If you have coeliac disease, it’s crucial you do not eat any gluten. If you have untreated or undiagnosed coeliac disease and you’re still eating gluten, several complications can occur.
It’s a common misconception that eating a little gluten will not harm you. Eating even tiny amounts can trigger symptoms of coeliac disease and increase your risk of developing the complications outlined below.
Malabsorption
Malabsorption (where your body does not fully absorb nutrients) can lead to a deficiency of certain vitamins and minerals. This can cause conditions such as:
iron deficiency anaemia
vitamin B12 and folate deficiency anaemia
osteoporosis – a condition where your bones become brittle and weak
Malnutrition
As coeliac disease causes your digestive system to work less effectively, severe cases can sometimes lead to a critical lack of nutrients in your body. This is known as malnutrition, and can result in your body being unable to function normally or recover from wounds and infections.
If you have severe malnutrition, you may become fatigued, dizzy and confused. Your muscles may begin to waste away and you may find it difficult to keep warm. In children, malnutrition can cause stunted growth and delayed development.
Treatment for malnutrition usually involves increasing the number of calories in your diet and taking supplements.
Lactose intolerance
If you have coeliac disease, you’re more likely to also develop lactose intolerance, where your body lacks the enzyme to digest the milk sugar (lactose) found in dairy products. Lactose intolerance causes symptoms such as bloating, diarrhoea and abdominal discomfort.
Unlike gluten in coeliac disease, lactose does not damage your body. But you may get some gut-related symptoms when you eat foods containing lactose because you can’t digest it properly.
Lactose intolerance can be effectively treated by not eating and drinking dairy products that contain lactose. You may also need to take calcium supplements – dairy products are an important source of calcium, so you’ll need to compensate for not eating them.
Cancer
Cancer is a very rare but serious complication of coeliac disease.
Someone with coeliac disease has a slightly increased risk of developing certain cancers. Recent research shows that this increased risk is less than previously thought.
Cancers associated with coeliac disease are small bowel cancer, small bowel lymphoma and Hodgkin lymphoma. However, most people with coeliac disease will not develop any of these.
If you’ve been following a gluten-free diet for 3 to 5 years, your risk of developing these types of cancer is the same as that of the general population.
Coeliac disease in pregnancy
Poorly controlled coeliac disease in pregnancy can increase the risk of developing pregnancy-related complications, such as giving birth to a baby with a low birthweight.
How will I need to change my diet if I have celiac disease?
If you have celiac disease, you will need to remove foods and drinks that contain gluten from your diet. Following a gluten-free diet can relieve celiac disease symptoms and heal damage to the small intestine. People with celiac disease need to follow a gluten-free diet for life to prevent symptoms and intestinal damage from coming back. Your doctor or a registered dietitian can guide you on what to eat and drink to maintain a balanced diet.
If you or your child has been diagnosed with celiac disease, you may find support groups helpful as you learn about and adjust to a gluten-free lifestyle. Your doctor or a registered dietitian may be able to recommend support groups and other reliable sources of information.
What foods and drinks contain gluten?
Gluten occurs naturally in certain grains, including
wheat and types of wheat, such as durum, emmer, semolina, and spelled
barley, which may be found in malt, malt extract, malt vinegar, and brewer’s yeast
rye
triticale, a cross between wheat and rye
Gluten is found in foods that contain ingredients made from these grains, including baked goods, baking mixes, bread, cereals, and pasta. Drinks such as beer, lagers, ale, flavored liquors, and malt beverages may also contain gluten.
Many foods such as colorings, flavorings, starches, and thickeners—are made from grains that contain gluten. These ingredients are added to many processed foods, including foods that are boxed, canned, frozen, packaged, or prepared. Therefore, gluten may be found in a variety of foods, including candy, condiments, hot dogs and sausages, ice cream, salad dressing, and soups.
Cross-contact
Cross-contact occurs when foods or products that contain gluten come into contact with gluten-free foods. Cross-contact can spread gluten to gluten-free foods, making the gluten-free foods unsafe for people with celiac disease to consume. Cross-contact can occur at any time, including when foods are grown, processed, stored, prepared, or served.
How can I identify and avoid foods and drinks that contain gluten?
A registered dietitian can help you learn to identify and avoid foods and drinks that contain gluten when you shop, prepare foods at home, or eat out.
For example, when you shop and eat at home
carefully read food labels to check for grains that contain gluten—such as wheat, barley, and rye—and ingredients or additives made from those grains.
check for gluten-free food labeling.
don’t eat foods if you aren’t sure whether they contain gluten. If possible, contact the company that makes the food or visit the company’s website for more information.
store and prepare your gluten-free foods separately from other family members’ foods that contain gluten to prevent cross-contact.
When you eat out at restaurants or social gatherings
before you go out to eat, search online for restaurants that offer a gluten-free menu.
review restaurant menus online or call ahead to make sure a restaurant can accommodate you safely.
at the restaurant, let the server know that you have celiac disease. Ask about food ingredients, how food is prepared, and whether a gluten-free menu is available. Ask to talk with the chef if you would like more details about the menu.
when attending social gatherings, let the host know you have celiac disease and find out if gluten-free foods will be available. If not, or if you are unsure, bring gluten-free foods that are safe for you to eat.
What should I eat if I have celiac disease?
If you have celiac disease, you will need to follow a gluten-free diet. Your doctor and a registered dietitian can help you plan a healthy, balanced diet to make sure that you get the nutrients you need.
Gluten-free foods
Many foods, such as meat, fish, fruits, vegetables, rice, and potatoes, without additives or some seasonings, are naturally gluten-free. Flour made from gluten-free foods, such as potatoes, rice, corn, soy, nuts, cassava, amaranth, quinoa, buckwheat, or beans are safe to eat.
You can also buy packaged gluten-free foods, such as gluten-free types of baked goods, bread, and pasta. These foods are available from many grocery stores, restaurants, and at specialty food companies. Packaged gluten-free foods tend to cost more than the same foods that have gluten, and restaurants may charge more for gluten-free types of foods.
Talk with your doctor or a registered dietitian about whether you should include oats in your diet and how much. Research suggests that most people with celiac disease can safely eat moderate amounts of oats. If you do eat oats, make sure they are gluten-free. Cross-contact between oats and grains that contain gluten is common and can make oats unsafe for people with celiac disease.
Gluten-free labeling
The U.S. Food and Drug Administration (FDA) requires that foods labeled gluten-free meet specific standards. One requirement is that foods with the terms gluten-free, no gluten, free of gluten, or without gluten on the label must contain less than 20 parts per million of gluten. This amount of gluten is too small to cause problems in most people with celiac disease.
The FDA rule does not apply to foods regulated by the U.S. Department of Agriculture, including meat, poultry, and some egg products. The rule also does not apply to most alcoholic beverages, which are regulated by the U.S. Department of the Treasury.
Should I start a gluten-free diet before I talk with my doctor?
No. If you think you might have celiac disease, you should talk with your doctor about testing to diagnose celiac disease before you begin a gluten-free diet. If you avoid gluten before you have tested, the test results may not be accurate.
Also, if you start avoiding gluten without advice from a doctor or a registered dietitian, your diet may not provide enough of the nutrients you need, such as fiber, iron, and calcium. Some packaged gluten-free foods may be higher in fat and sugar than the same foods that contain gluten. If you are diagnosed with celiac disease, your doctor and dietitian can help you plan a healthy gluten-free diet.
If you don’t have celiac disease or another health problem related to gluten, your doctor may not recommend a gluten-free diet. In recent years, more people without celiac disease have begun avoiding gluten, believing that a gluten-free diet is healthier or could help them lose weight. However, researchers have found no evidence that a gluten-free diet promotes better health or weight loss for the general population.
Screening of persons at risk for celiac disease
Asymptomatic/atypical manifestations
first-degree relatives 10 – 20%
Down syndrome 5 – 12%
Ullrich–Turner syndrome 2 – 5%
Williams–Beuren syndrome 9%
selective IgA deficiency 2 – 8%
autoimmune thyroiditis 3 – 7%
autoimmune hepatitis (children) 12 – 13%
type 1 diabetes 2 – 12%
juvenile chronic arthritis 1.5 – 2.5%
Oligosymptomatic manifestations
failure to thrive
weight loss
short stature / growth retardation
delayed puberty (amenorrhea)
iron-deficiency anemia
anorexia
dyspeptic symptoms (nausea/vomiting)
chronic, recurrent abdominal pain (bloating)
chronic constipation
chronic fatigue/diminished performance
recurrent aphthous sores
chronic/intermittent diarrhea
difficulty concentrating
depressed mood
chronic headache
elevated transaminases
tooth-enamel defects
osteoporosis/osteopenia
Complications of classic celiac disease
acute global/selective malabsorption (anemia and other consequences)
Prolyl endopeptidases – Prolyl endopeptidases (PEPs) are endoproteolytic enzymes expressed in micro-organisms and plants. These enzymes cleave proline-rich gluten to smaller peptides that are ready for digestion by intestinal brush-border enzymes (aminopeptidases and carboxypeptidases). Limited efficiency was found, since PEP required 3 h preincubation with gluten containing foods to achieve full detoxification of peptides and to prevent intestinal transport of active gluten fragments[rx]. This is unlikely to be achieved by co-administration of PEP and gluten-containing diet.
A two-stages cross-over phase II clinical trial was performed using asymptomatic CD patients eating, a slice of bread daily and a slice of bread pre-treated with PEP daily[rx]. After 2 wk of PEP treated gluten challenge, majority of patients did not develop malabsorption, measured by faecal fat excretion and D-xylose malabsorption tests. The tests likely lacked the necessary sensitivity to assess minor malabsorption resulting from active CD, since no histological confirmation was performed to determine deterioration in the Marsh grading[rx]. When PEPs were consumed as jam spread on a slice of gluten-containing bread by CD patients, villous blunting was seen in small bowel biopsy histological evaluation in most patients[rx]. Further studies are needed to determine the appropriate dose of enzyme and time of administration relative to the quantity of ingested gluten.
ALV003 – ALV003, a mixture of two glutenases, an endoprotease from germinating barley and PEP, was pretreated with wheat flour and tested in CD patients[rx]. Symptoms typically associated with gluten ingestion were not significantly reduced by ALV003 pre-treatment, but ALV003 abolished immune responses induced by gluten in CD patients. A randomized controlled phase IIa clinical trial has been performed where CD patients received either ALV003 or placebo daily for 6 wk at the time of 2 g gluten contained bread. This proof-of-concept study demonstrated that ALV003 can attenuate gluten-induced small intestinal mucosal injury in CD patients[rx]. After six weeks period, biopsies proved lower small intestinal mucosal injury in patients treated with ALV003 than placebo-treated patients despite of persistent intestinal inflammation in many patients on a strict GFD. Placebo-treated patients were found to have suffered more adverse events, most commonly including abdominal distention, flatulence, eructation, abdominal pain and diarrhea[rx].
Lactobacilli – Lactobacilli added to sourdough for fermentation are able to lyse the proline-/glutamine-rich gluten peptides and thus decrease immunotoxicity[rx–rx]. A mixture of fermented wheat flour with oat, millet and buckwheat allows sourdough bread to retain its baking characteristics. A pilot study in patients with CD suggested that this bread was well tolerated[rx]. However, these patients were challenged for only 2 d, which is clearly not sufficient to draw any firm conclusions. Hence, another 60-d diet of fully hydrolyzed wheat flour with sourdough lactobacilli and fungal proteases (8 ppm residual gluten; n = 5) was further studied. The pretreated flour was rendered non-toxic by serological, morphometrical, and immunohistochemical analysis[rx]. A larger group of subjects in the trial and palatability of digested flour baked products needs to be taken into consideration.
VSL3 – VSL3 is a probiotic containing lyophilised bacteria, including bifidobacteria (Bifidobacterium longum, Bifidobacterium infantis and Bifidobacterium breve), lactobacilli (Lactobacillus acidophilus, Lactobacillus casei, Lactobacillus delbrueckii subsp., Lactobacillus bulgaricus and Lactobacillus plantarum) and Streptococcus salivarius subsp., Thermophiles. It is used to hydrolyse gliadin peptides in pre-treated flour and tested for efficacy in rat intestinal cell line and celiac jejunal biopsies[rx]. VSL3 pre-digested gliadins did not show an increase of the infiltration of CD3+ intraepithelial lymphocytes and caused a less pronounced effect on intestinal mucosa permeability (determined by lower F-actin rearrangement and zonulin release). Hence, VSL#3 may have importance during food processing to produce pre-digested gluten-free products.
Prevention of toxic gliadin peptide absorption
Larazotide – Larazotide (AT-1001, Alba Therapeutics, Baltimore, MA), is a synthetic hexapeptide derived from Zonula Occludens toxin of Vibrio cholera[rx]. It is used to inhibit the opening of tight junctions of the small intestine epithelial cells. Clinical trial phase I in CD patients suggested that Larazotide therapy is well tolerated by patients and reduces intestinal barrier dysfunction, proinflammatory cytokine production, and gastrointestinal symptoms in CD individuals after gluten exposure[rx]. Encouraging results were obtained from a 6-wk phase IIb trial in terms of symptoms and antibody titers[rx], showing larazotide acetate a promising drug candidate. This drug inhibits the paracellular route of gliadin absorption through tight junctions, which is not the only mechanism of gliadin absorption. Indeed, gliadin may gain access to the mucosa through transcellular pathways in addition to paracellular route[rx,rx]. Hence, this strategy might be best exploited in combination with other treatments.
Synthetic polymer poly (hydroxyethylmethacrylate-co-styrene sulfonate) – Poly (hydroxyethylmethacrylate-co-styrene sulfonate) [P (HEMA-co-SS)] forms supra-molecular particles upon gliadin complexation in gastric and intestinal conditions[rx,rx], and deteriorates gliadin’s effect on epithelial cells[rx]. This complexation decreases the effect of gastrointestinal (GI) digestive enzymes on gliadin absorption, and thus the formation of immunogenic peptides is reduced. Gluten-sensitive HLA-HCD4/DQ8 mice co-administered with P (HEMA-co-SS) showed attenuated gliadin-induced changes in permeability and inflammation[217]. Low side effect, cost and possibility to be taken, occasionally with gluten-containing food, makes it an attractive option. Further investigation of the mechanisms of action and its interaction with human tissues is required before its efficacy is investigated in human trials[rx].
Anti-gliadin egg yolk antibody – Oral antibody passive immunotherapy may be of value due to the advantages of reduced cost, ease of administration, and potential to treat localized conditions in the gastrointestinal tract[rx]. Among antibodies, chicken egg yolk immunoglobulin (IgY), is ideal for passive immunotherapy, as it may be readily obtained in large quantities from egg yolk, presenting a more cost-effective, convenient, and hygienic alternative to mammalian antibodies. Oral immunotherapeutic IgY is a promising alternative to neutralize gliadin in the GI tract and prevention it from absorption[rx]. Mannitol contained antibody preparation is highly resistant against GI enzymes and proved to effectively neutralized gliadin under simulated GI conditions in the presence of food. In vivo study; BALB/c mice fed with IgY formulation and gliadin ratio of 1:5 (w/w), demonstrated that gliadin absorption in the gastrointestinal tract was minimal at < 1%[rx]. Further investigations in CD patients is requires to prove its efficacy and determine dosing regimen of antibody relative to the amount of gliadin ingestion.
Blockage of selective deamidation of specific glutamine residues by tissue transglutaminase 2 inhibitor
Transglutaminases (a family of eight enzymes) have diverse functions in human and are involved in several biological and pathological processes[rx]. tTG2 is an enzyme that has a pro-inflammatory effect and increases the immunostimulatory epitopes present in the lamina propria of the small intestine. Blockage of tTG2 may be a promising approach to inhibit the inflammatory process upon gluten ingestion. There are two essential classes of tTG2 inhibitors; irreversible and reversible inhibitors[rx]. Irreversible inhibitors form a stable covalent bond with this enzyme, and thus prevent deamidation of gliadin peptides[rx,rx]. Reversible inhibitors are more desirable to minimize possible side effects. These include aldehyde-bearing tTG modulators[rx], cinnamoyl triazole derivatives[rx], and the highly specific modified peptide targeting the active cysteine site of tTG2[rx]. Since a few gluten T-cell epitopes can be recognized without being deamidated by tTG2[rx,rx], this approach will not inhibit the innate response[rx], or the immune response induced by non-deamidated peptides[rx]. To be able to use tTG2 inhibitors clinically, it is critical to design highly specific inhibitors, since all human tTG share high sequence homology.
Vaccine application to restore immune tolerance towards gluten
Autoimmune enteropathy in CD has been proposed to be due to impairment of immunoregulatory mechanisms that controls oral tolerance. Systematic peptide mapping of T-cell was performed to determine gliadin reactive epitopes recognized by approximately 90% of CD patients. A clinical trial phase I study has been initiated as Nexvax2 (Nexpep Pty, Ltd., Australia) peptide vaccine-containing mixture of immunotoxic α- and ω-gliadins and B-hordein[rx].
Engineered Lactococcus lactis secreting a DQ8-re-stricted gliadin peptide administered orally[rx], or recombinant α-gliadin in HLA-DQ8 administered intranasally in transgenic mouse model[rx], have been studied to modulate immune response to gluten. However, it is difficult to appreciate how the vaccine or the intranasal peptide administration can modulate the Tr1 response. More work is needed to assess the effect of these therapies on the spectrum of gluten peptides presented to the gut.
Dermal inoculation of human hookworm (Necator americanus) has also been used to modulate the immune response to gluten[rx]. A phase II trial with CD patients suggested that hookworm infection on its own may not obviate the necessity for a restricted diet in CD, but appears to be safe and might impact on immune pathology[rx]. Here in, hookworm infection is expected to reduce gluten sensitivity and immune reactivity.
Modulation of immune response to dietary gliadin
HLA-DQ blocker: HLA-DQ blocker is used to block the binding sites of HLA-DQ2 or DQ8 for it to be unrecognized by T cells as well to block the presentation of the antigen. This is not a new concept that was developed without much success to treat type 1 diabetes mellitus and rheumatoid arthritis, due to difficulties in effective drug delivery[rx,rx]. By amino-acid substitution of gliadin T-cell stimulatory sequence, the epitope can be converted to an agonist or antagonist, abolishing the inflammatory cascade[rx]. IFN-γ production by peripheral blood lymphocytes was prevented when either an alanine or lysine amino acid was substituted through the immunodominant α-gliadin peptide, corresponding to the peptide’s anchor to the HLA-DQ cleft[rx]. To develop this as a new therapeutic agent, more studies need to be performed, looking at the mass T-cell action of the gut towards these modified peptides.
Interleukin blocker – Modulation of cytokine production has been evaluated for the treatment of several autoimmune diseases, although their side effects may be severe. Modulation of proinflammatory IL-15 and anti-inflammatory IL-10 cytokines has been suggested to influence the immune balance between tolerance and autoimmunity[rx,rx–rx]. Blocking IL-15 may promote maintenance of epithelial integrity, limit epithelial destruction, leading to decreased passage of dietary gliadin.
NKG2D antagonists – MICA molecules, strongly expressed on active CD epithelial cell surface upon gliadin challenge[rx], interact with the NKG2D-activating receptor on human natural killer cells and CD8 T cells, leading to villous atrophy due to an IEL-mediated damage to enterocytes[rx,rx]. Thus, NKG2D antagonists[rx] and anti-NKG2D antibodies[rx], have been proposed as therapeutics in CD.
Restoration of intestinal architecture by R-spondin-1
R-spondin-1 is an intestinal mitogen, shown to stimulate crypt cell growth, accelerate mucosal regeneration and restore intestinal architecture in mouse models of colitis[rx]. This agent has yet to be tested in human to be considered as a therapeutic agent in CD.
Lifestyle and home remedies
If you’ve been diagnosed with celiac disease, you’ll need to avoid all foods that contain gluten. Ask your doctor for a referral to a dietitian, who can help you plan a healthy gluten-free diet.
Read labels
Avoid packaged foods unless they’re labeled as gluten-free or have no gluten-containing ingredients, including emulsifiers and stabilizers that can contain gluten. In addition to cereals, pastas and baked goods, other packaged foods that can contain gluten include:
Beers, lagers, ales and malt vinegars
Candies
Gravies
Imitation meats or seafood
Processed luncheon meats
Rice mixes
Salad dressings and sauces, including soy sauce
Seasoned snack foods, such as tortilla and potato chips
Seitan
Self-basting poultry
Soups
Pure oats aren’t harmful for most people with celiac disease, but oats can be contaminated by wheat during growing and processing. Ask your doctor if you can try eating small amounts of pure oat products.
Allowed foods
Many basic foods are allowed in a gluten-free diet, including:
Eggs
Fresh meats, fish and poultry that aren’t breaded, batter-coated or marinated
Fruits
Lentils
Most dairy products, unless they make your symptoms worse
Nuts
Potatoes
Vegetables
Wine and distilled liquors, ciders and spirits
Grains and starches allowed in a gluten-free diet include:
Malnutrition – This occurs if your small intestine can’t absorb enough nutrients. Malnutrition can lead to anemia and weight loss. In children, malnutrition can cause slow growth and short stature.
Bone weakening – Malabsorption of calcium and vitamin D can lead to a softening of the bone (osteomalacia or rickets) in children and a loss of bone density (osteopenia or osteoporosis) in adults.
Infertility and miscarriage – Malabsorption of calcium and vitamin D can contribute to reproductive issues.
Lactose intolerance – Damage to your small intestine might cause you abdominal pain and diarrhea after eating or drinking dairy products that contain lactose. Once your intestine has healed, you might be able to tolerate dairy products again.
Cancer – People with celiac disease who don’t maintain a gluten-free diet have a greater risk of developing several forms of cancer, including intestinal lymphoma and small bowel cancer.
Nervous system problems – Some people with celiac disease can develop problems such as seizures or a disease of the nerves to the hands and feet (peripheral neuropathy).
Chronic Diverticular Disease/Diverticulosis is a clinical condition of inflammation due to micro-perforation and herniations of the colonic mucosa and submucosa through the muscle layers, in which multiple sac-like protrusions, abscesses, fistulas, peritonitis, and colonic stenosis, small pouches, or sacs, form and push outward through weak spots in the wall of your colon(diverticula) that develop along the gastrointestinal tract. Though diverticula may form at weak points in the walls of either the small or large intestines, the majority occur in the large intestine (most commonly the sigmoid colon).
These pouches are most common in the lower part of your colon, called the sigmoid colon. One pouch is called a diverticulum. Multiple pouches are called diverticula. Most people with diverticulosis do not have symptoms or problems.
When diverticulosis does cause symptoms or problems, doctors call this diverticular disease. For some people, diverticulosis causes symptoms such as changes in bowel movement patterns or pain in the abdomen. Diverticulosis may also cause problems such as diverticular bleeding and diverticulitis.
Types of Diverticulitis
There are two types of diverticulitis:
Uncomplicated diverticulitis – Diverticula and the surrounding intestinal lining are inflamed but there are no signs of pus building up (abscesses) or the inflammation spreading.
Complicated diverticulitis – Abscesses have formed. Sometimes the inflammation has even already spread or the wall of the intestine has torn (intestinal perforation). The intestine may also become blocked or the inner lining of the tummy may become inflamed (peritonitis).
or
Acute diverticulitis – Surgery usually isn’t necessary for people who have acute diverticulitis. But there are exceptions: If abscesses (collections of pus) have formed, and treatment with antibiotics isn’t successful, surgery is unavoidable. The aim is then to prevent serious complications such as the wall of the intestine tearing (perforation) or the inner lining of the tummy becoming inflamed (peritonitis), which can lead to blood poisoning (septicemia).
Chronic diverticular disease – People who have recurrent diverticulitis or chronic symptoms generally don’t develop serious complications. Although such complications are possible, they tend to be rare if the inflammation is “uncomplicated” – in other words, as long as no abscesses have formed.
Causes of Diverticulitis
Experts are not sure what causes diverticulosis and diverticulitis. Researchers are studying several factors that may play a role in causing these conditions.
No one knows for certain why diverticulosis develops – however, a few theories have been suggested. Some experts believe that abnormal intermittent high pressure in the colon due to muscle spasm or straining with stool may cause diverticula to form at weak spots in the colon wall. Historically, low-fiber diets were felt to play a role in the development of diverticulosis.
Fiber – For more than 50 years, experts thought that following a low-fiber diet led to diverticulosis. However, recent research has found that a low-fiber diet may not play a role. This study also found that a high-fiber diet with more frequent bowel movements may be linked with a greater chance of having diverticulosis.4 Talk with your doctor about how much fiber you should include in your diet.
Genes – Some studies suggest that genes may make some people more likely to develop diverticulosis and diverticulitis. Experts are still studying the role genes play in causing these conditions.
Other factors – Studies have found links between diverticular disease—diverticulosis that causes symptoms or problems such as diverticular bleeding or diverticulitis—and the following factors:
Certain medicines – including nonsteroidal anti-inflammatory drugs (NSAIDs), such as aspirin and steroids
Intestinal motility – Another theory suggests the degeneration of glial neurons in the myenteric plexus and the interstitial cells of Cajal lead to slowed intestinal movement and consequently fecal content exerts increased pressure on the colon wall resulting in the formation of diverticula.[rx]
Lack of exercise
Obesity
Smoking
constipation
A diet that is low in dietary fiber (although this claim is controversial)
Connective tissue disorders (such as Marfan syndrome and Ehlers Danlos Syndrome) that may cause weakness in the colon wall
Diverticulitis may begin when bacteria or stool get caught in a pouch in your colon. A decrease in healthy bacteria and an increase in disease-causing bacteria in your colon may also lead to diverticulitis.
Symptoms of Diverticulitis
Most people with diverticulosis do not have symptoms. If your diverticulosis causes symptoms, they may include
bloating
constipation or diarrhea
cramping or pain in your lower abdomen
abdominal pain and bloating
constipation and diarrhea
flatulence
blood in the feces is usually minor, but bleeding can sometimes be heavy if a diverticulum gets inflamed or is near a blood vessel
anemia from repeated bleeding may occur.
Other conditions, such as irritable bowel syndrome and peptic ulcers, cause similar symptoms, so these symptoms may not mean you have diverticulosis. If you have these symptoms, see your doctor.
If you have diverticulosis and develop diverticular bleeding or diverticulitis, these conditions also cause symptoms.
In most cases, when you have diverticular bleeding, you will suddenly have a large amount of red or maroon-colored blood in your stool.
When you have diverticulitis, the inflamed pouches most often cause pain in the lower-left side of your abdomen. The pain is usually severe and comes on suddenly, though it can also be mild and get worse over several days. The intensity of the pain can change over time.
Diverticulitis may also cause
Diverticular bleeding may also cause dizziness or light-headedness, or weakness. See your doctor right away if you have any of these symptoms.
If you have symptoms such as bloating, constipation or diarrhea, or pain in your lower abdomen, see your doctor.
Constipation or diarrhea
Fevers and chills
Nausea or vomiting
Get constant, more severe tummy pain
Have a high temperature
Have diarrhea or constipation
Get mucus or blood in your poo, or bleeding from your bottom
Intermittent abdominal pain in the left lower quadrant with constipation, diarrhea or occasional large rectal bleeds (the pain may be triggered by eating and relieved by the passage of stool or flatus)
Tenderness in the left lower quadrant on abdominal examination.
In a minority of people and in people of Asian origin, pain and tenderness may be localized in the right lower quadrant
Symptoms may overlap with conditions such as irritable bowel syndrome, colitis, and malignancy.
Diagnosis of Diverticulitis
If your doctor suspects you may have diverticulosis or diverticulitis, your doctor may use your medical history, a physical exam, and tests to diagnose these conditions. Doctors may also diagnose diverticulosis if they notice pouches in the colon wall while performing tests, such as routine x-rays or colonoscopy, for other reasons.
Medical history
Your doctor will ask about your medical history, including your
bowel movement patterns
diet
health
medicines
symptoms
Physical exam
Your doctor will perform a physical exam, which may include a digital rectal exam. During a digital rectal exam, your doctor will have you bend over a table or lie on your side while holding your knees close to your chest. After putting on a glove, the doctor will slide a lubricated finger into your anus to check for pain, bleeding, hemorrhoids, or other problems.
Lab Test
Your doctor may use the following tests to help diagnose diverticulosis and diverticulitis:
Blood test – A health care professional may take a blood sample from you and send the sample to a lab to test for inflammation or anemia.
Stool sample – Your stool sample is checked for the presence of abnormal bacteria or parasites as possible causes of your infection, abdominal pain, blood in stool, diarrhea, or your other symptoms.
Stool tests – to check for the presence of blood in the feces or the presence of infections, which may mimic the symptoms of diverticulosis and diverticulitis.
Digital rectal exam – In this physical exam, your healthcare provider gently inserts a gloved, lubricated finger into your rectum to feel for any problems in your anus or rectum.
Barium enema (also called lower gastrointestinal tract radiography) – In this test, a liquid containing barium is injected into your anus. The liquid coats the inside of your colon, which helps make any problems in your colon more visible on X-rays.
Esophageal manometry – This technique measures the timing and strength of the contractions of your esophagus.
Sigmoidoscopy – In this exam, a thin flexible tube with a light on the end is inserted into your rectum and moved into your sigmoid colon. The tube is connected to a video camera. The camera allows a visual inspection of your sigmoid colon (where most diverticula form) and rectum.
Angiography – If you have rapid, heavy rectal bleeding, this procedure helps find where the bleeding is coming from. During this test, the arteries that supply the colon are injected with a harmless dye that allows the source of the bleeding to be seen.
Imaging Test
CT scan –A CT scan can show infected or inflamed diverticula and also reveal the severity of diverticulitis. A computerized tomography (CT) scan uses a combination of x-rays and computer technology to create images of your gastrointestinal (GI) tract.
An x-ray – technician performs the procedure in an outpatient center or a hospital. A radiologist reads and reports on the images. You don’t need anesthesia for this procedure.
CT scan – a health care professional may give you a solution to drink and an injection of a special dye called contrast medium. Contrast medium makes the structures inside your body easier to see during the procedure. You’ll lie on a table that slides into a tunnel-shaped device that takes the x-rays. A CT scan of your colon is the most common test doctors use to diagnose diverticulosis and diverticulitis.
Lower GI series
A lower GI series, also called a barium enema, is a procedure in which a doctor uses x-rays and a chalky liquid called barium to view your large intestine. The barium will make your large intestine more visible on an x-ray.
An x-ray technician and a radiologist perform a lower GI series at a hospital or an outpatient center. A health care professional will give you written bowel prep instructions to follow at home before the procedure. You don’t need anesthesia for this procedure.
For the procedure, you’ll be asked to lie on a table while the radiologist inserts a flexible tube into your anus and fills your large intestine with barium. You will need to hold still in various positions while the radiologist and technician take x-ray images and possibly an x-ray video, called fluoroscopy. If pouches are present in your colon, they will appear on the x-ray.
Colonoscopy
Colonoscopy is a procedure in which a doctor uses a long, flexible, narrow tube with a light and tiny camera on one end, called a colonoscope or endoscope, to look inside your rectum and colon.
A trained specialist performs a colonoscopy in a hospital or an outpatient center. A health care professional will give you written bowel prep instructions to follow at home before the procedure. You will receive sedatives, anesthesia, or pain medicine during the procedure.
During a colonoscopy, you’ll be asked to lie on a table while the doctor inserts a colonoscope into your anus and slowly guides it through your rectum and into your colon. Doctors may use a colonoscopy to confirm a diagnosis of diverticulosis or diverticulitis and rule out other conditions, such as cancer.
Treatment of Diverticulitis
Non-Pharmacological
The goal of treating diverticulosis is to prevent the pouches from causing symptoms or problems. Your doctor may recommend the following treatments.
High-fiber diet – Although a high-fiber diet may not prevent diverticulosis, it may help prevent symptoms or problems in people who already have diverticulosis. A doctor may suggest that you increase fiber in your diet slowly to reduce your chances of having gas and pain in your abdomen. Learn more about foods that are high in fiber.
Fiber supplements – Your doctor may suggest you take a fiber product such as methylcellulose (Citrucel) or psyllium (Metamucil) one to three times a day. These products are available as powders, pills, or wafers and provide 0.5 to 3.5 grams of fiber per dose. You should take fiber products with at least 8 ounces of water.
Diet – Some doctors advise people to try to carry on eating normally – or to eat a low-fiber diet for a while. Others recommend mainly eating soups or other non-solid foods, as well as drinking enough fluids, in the first few days. It’s not clear whether it really is better to avoid solid foods for a while. There aren’t any good studies in this area.
Nuts and Seeds – In the past, doctors thought you had to avoid certain foods if you had diverticulosis. These included nuts, seeds like sunflower and sesame, and even little seeds in fruits and vegetables such as cucumbers and strawberries. But recent research shows these foods don’t harm people with diverticulosis.
Draining – About 15 out of 100 people who have complicated diverticulitis have a pus-filled abscess. If necessary, the pus can be drained out of the body through a thin tube.
Drink plenty of water – Eating more fiber absorbs more water, so you’ll need to increase the amount of water you drink to keep stool soft and on the move. Many healthcare providers suggest drinking half your body’s weight in ounces. For example, if you weigh 160 pounds, you should drink 80 ounces of water each day.
Exercise daily – Physical movement helps food pass through your intestinal system. Exercise for 30 minutes on most days if you can.
Medicines
NSAIDs and Paracetamol – can be used to relieve pain. Some painkillers, including aspirin and ibuprofen, should not be taken regularly as they can cause stomach upsets. Ask a pharmacist about this.
Antispasmodics – Your doctor may prescribe antispasmodics such as mebeverine, and hyoscine hydrobromide, ondansetron, granisetron if you have persistent abdominal spasms.
Mesalazine – Some studies suggest that mesalazine (Asacol) taken every day or in cycles may help reduce symptoms that may occur with diverticulosis, such as pain in your abdomen or bloating. Studies suggest that the antibiotic rifaximin (Xifaxan) may also help with diverticulosis symptoms. The maintenance dose of Mesalazine 1.6g daily was administered to patients with the addition of probiotic VSL3 in patients with more severe disease to maintain remission
Antibiotics – The standard of outpatient care includes bowel rest, increase fluid intake, and oral antibiotic therapy (single or multiple drug regimen) that covers gram-negative rods and anaerobic bacteria. The most common regimen used in the United States consists of quinolones (ciprofloxacin) or sulfa drugs (trimethoprim/sulfamethoxazole) in combination with metronidazole (or clindamycin, if the patient is intolerant to metronidazole) or single-agent amoxicillin-clavulanate for 7 to 10 days.[rx][rx][rx] Inpatient management of diverticulitis requires intravenous antibiotics, intravenous fluids, and pain management. Again, antibiotics should cover gram-negative rods and anaerobes and be given for three to 5 days before switching to oral antibiotics for a ten to 14-day course. Bowel rest is preferred in patients requiring inpatient admission. Typically, defervescence and improvement in leukocytosis should be observed for two to four days of hospitalization, if not an alternative diagnosis or complications should be suspected. Prompt surgical evaluation should be considered.
Role of vitamin D – The role of vitamin D has recently been explored in diverticular disease. In a retrospective cohort study conducted by Maguire et al.,[rx] prediagnostic levels of vitamin D (25-OH) were measured and compared between 9,116 patients with uncomplicated diverticulosis and 922 patients who developed diverticulitis requiring hospitalization. The study found a statistically significant higher mean prediagnostic serum vitamin D (25-OH) level in patients with uncomplicated diverticulosis in comparison to patients who required hospitalization for diverticulitis.[rx]
Citrucel or Metamucil – They might suggest a fiber product like Citrucel or Metamucil. They come in pill, powder, or wafer forms. You’ll take it with lots of water.
Probiotics – Some studies show that probiotics may help with diverticulosis symptoms and may help prevent diverticulitis. However, researchers are still studying this subject. Probiotics are live bacteria like those that occur normally in your stomach and intestines. You can find probiotics in dietary supplements—in capsule, tablet, and powder form—and in some foods, such as yogurt. For safety reasons, talk with your doctor before using probiotics or any complementary or alternative medicines or medical practices.
Antibiotic Regimens for Acute Diverticulitis
Type of Treatment
(References)
Single Agent
Multiple Agents
Duration
Outpatient treatment of mild uncomplicated diverticulitis (rx, rx, rx)
Moxifloxacin 400 mg PO every 24 h
Amoxicillin-clavulanic acid 875 mg/125 mg PO every 12 h or 1000/62.5 mg tab 2 PO every 12 h
Trimethoprim-sulfamethoxazole 1 DS 160/800 mg PO every 12 h
Ciprofloxacin 750 mg PO every 12 h†
Levofloxacin 750 mg PO every 24 hEach in combination with metronidazole 500 mg PO every 6 h†
4–7 days if source controlled/abscess drained
Inpatient treatment of mild to moderately complicated diverticulitis (rx, rx)
Ertepenem 1g IV every 24 h
Moxifloxacin 400 mg IV every 24 h
Ticarcillin-clavulanic acid 200–300 mg/kg/d divided doses every 4–6 h
Cefazolin 1–2 g IV every 8 h
Cefuroxime 1.5 g IV every 8 h
Ceftriaxone 1–2 g IV every12–24 h
Cefotaxime 1–2 g IV every 6–8 h
Ciprofloxacin IV 400 mg every 12 h
Levofloxacin IV 750 mg every 24 hEach in combination with metronidazole 500 mg IV every 8–12 h or 1500 mg IV every 24 h
4–7 days if source controlled/abscess drained
Inpatient treatment of severe complicated diverticulitis, peritonitis (rx, rx)
Imipenem-cilastatin 500 mg every 6 h or 1g IV every 8 h
Meropenem 1 g IV every 8 h
Doripenem 500 mg IV every 8 h
Piperacillin-tazobactam 3.375g IV every 6 h
Cefepime 2g IV every 8 h
Ceftazidime 2g IV every 8 h
Ciprofloxacin 400 mg IV every 12 h
Levofloxacin 750 mg IV every 24 hEach in combination with metronidazole 500 mg IV every 8–12 h or 1500 mg IV every 24 h
4–7 days if source controlled/abscess drained
Surgery
Emergency surgery is required to treat peritonitis, the most serious potential complication of diverticulitis. Peritonitis requires surgical repair as well as intravenous antibiotics.
Surgery also may be required during the hospital stay to treat a particularly severe episode of diverticulitis. These include continuous bleeding, perforation of an abscess, attachment of two organs by a fistula, or colon obstruction caused by scarring from previous episodes of diverticulitis.
Surgical procedures to do this include
Cricopharyngeal myotomy – This involves making small cuts in the upper sphincter of the esophagus to widen it, so food can pass more easily through your esophagus.
Diverticulopexy with cricopharyngeal myotomy – This involves removing a larger diverticulum by turning it upside down and attaching it to the wall of the esophagus.
Diverticulectomy and cricopharyngeal myotomy – This involves removing the diverticulum while performing a cricopharyngeal myotomy. It’s a combination that’s often used to treat Zenker’s diverticula.
Endoscopic diverticulectomy – This is a minimally invasive procedure that divides the tissue between the diverticulum and esophagus, allowing food to drain from the diverticulum.
Colon resection – If your bleeding does not stop, a surgeon may perform abdominal surgery with a colon resection. In a colon resection, the surgeon removes the affected part of your colon and joins the remaining ends of your colon together. You will receive general anesthesia for this procedure.
In some cases, during a colon resection, it may not be safe for the surgeon to rejoin the ends of your colon right away. In this case, the surgeon performs a temporary colostomy. Several months later, in a second surgery, the surgeon rejoins the ends of your colon and closes the opening in your abdomen.
When is surgery for diverticulitis considered?
Surgery for diverticulitis is considered if you have:
Abscesses – An abscess is a container or “walled-off” infection in the abdomen. If the fluid in an abscess (a collection of bacteria and white blood cells) is not successfully drained with a needle or catheter, surgery is needed. In surgery, the abscess is cleaned up and the affected part of the colon is removed.
Perforation/peritonitis – A tear (perforation) in your colon allows pus or stool to leak into your abdominal cavity, resulting in peritonitis. This is a life-threatening infection that requires emergency surgery to clean the cavity and remove the damaged part of the colon.
Blockages or strictures – Previous infections in your colon can cause scars to form, which can result in a partial or complete blockage or strictures (narrowing of sections of the colon). A complete blockage requires surgery (partial blockage does not).
Fistulas – A fistula is an abnormal passageway or tunnel that forms and connects with another organ. An abscess that erodes into the surrounding tissue creates these passageways. A fistula in the colon can connect to the skin, bladder, vagina, uterus, or another part of the colon. Most fistulas don’t close on their own so surgery is needed.
Continued rectal bleeding (also called diverticular bleeding) – Diverticular bleeding occurs when a small blood vessel near the diverticula bursts. Mild bleeding usually stops on its own, but about 20% of cases require treatment. Surgery may be needed if other attempts to stop the bleeding fail, such as clipping, drug infusion, or cauterizing the bleeding artery. If bleeding is heavy and rapid, emergency surgery is needed.
Severe diverticulitis – that has not responded to other treatment methods. Multiple attacks despite following a high-fiber diet. You and your surgeon may decide surgery to remove the diseased part of the colon is the best method to prevent future attacks.
Complications
Over time, an esophageal diverticulum can lead to some health complications.
Aspiration pneumonia – If an esophageal diverticulum causes regurgitation, it can lead to aspiration pneumonia. This is a lung infection caused by inhaling things, such as food and saliva, that usually travel down your esophagus.
Obstruction – An obstruction near the diverticulum can make it hard, if not impossible, to swallow. This can also cause the pouch to rupture and bleed.
Squamous cell carcinoma – In very rare cases, ongoing irritation of the pouch can lead to squamous cell carcinoma.
Sacs can get infected, and even burst – This is diverticulitis. It’s treated with rest, fluids, and antibiotics.
The infection can spread and an abscess can form. A specialist will need to drain the pus.
A perforation (a hole along the stomach wall) can occur – It’s rare, but life-threatening and requires immediate surgery.
You can get a diverticular hemorrhage – This is rare. It happens when your arteries wear through the intestinal wall. It causes massive bleeding and requires hospitalization and blood transfusions.
Best High-Fiber Foods
You may not think much about fiber — until you find yourself dealing with an, er, irregular situation.
Indeed, dietary fiber is a magic ingredient that keeps you regular. But thwarting constipation is not its only job. “Fiber does lots of cool stuff in the body. Here’s why you need it — and where to get it.
Benefits of a high-fiber diet
Fiber is an unsung hero. Among its claims to fame, a high-fiber diet can:
Soften stool and prevent constipation.
Lower cholesterol, reducing the risk of heart disease.
Reduce the risk of diseases such as colorectal cancer.
Keep blood sugar levels from spiking.
Make you feel full longer, which can help you lose weight.
There are two types of fiber, both of which are good for you
Soluble fiber – pulls in water. It slows digestion and lowers cholesterol. Soluble fiber is found in foods such as beans, seeds, peas, barley, oat bran, and some fruits and vegetables.
Insoluble fiber – is your classic roughage. It helps stool speed through the intestines. You’ll find it in foods such as whole grains, wheat bran, and the peels and seeds of fruits and veggies.
Aim for 25 to 35 grams of fiber a day, Taylor says — and a mix of soluble and insoluble fiber is ideal.
What foods are high in fiber?
Fiber comes from plants, so don’t bother looking for it in your chicken dinner. But the plant kingdom has a lot to offer, and the best sources of dietary fiber might surprise you. Here are Taylor’s top 11.
1. Whole-wheat pasta
Carbs get a bad rap, but whole grains are a great source of fiber and are also rich in healthy phytonutrients, Taylor says. Skip the white pasta (which has been stripped of all the good stuff), and go for whole-wheat instead.
“Barley is a delicious grain that’s often overlooked,” Taylor says. Try tossing it in soups or mix up a grain bowl with your favorite meat and veggies.
“Legumes are star players. They’re some of the best sources of protein and fiber, they help keep you full, and they have amazing nutrient composition. Chickpeas are a fiber-full favorite from the legume list. Add them to soups or salads, snack on chickpea hummus, or roast them whole for a crunchy, shelf-stable snack.
Nutrition information: ½ cup cooked = 6g fiber, 140 calories, 23g carbs, 7g protein.
4. Edamame
Edamame, or immature soybeans, has a mild flavor and pleasing texture. They’re also one of the few plant sources that contain all the amino acids your body needs, so they’re a great choice for vegans and vegetarians. You can find them in the frozen food section, still in the pod, or already shelled. Add edamame to salads and stir-fries, Taylor suggests. (Edamame is often a big hit for kids to snack on, too.)
Nutrition information: ½ cup boiled and shelled = 4g fiber, 100 calories, 7g carbs, 9g protein.
5. Lentils and split peas
These two legumes have similar nutrition profiles and are used in similar ways. “Lentils and split peas are nutritional powerhouses. They cook quickly and are great in soups. Try swapping lentils for some of the meat in your chili to boost the plant-powered goodness, she recommends.
Nutrition information:
Lentils, ½ cup cooked = 8g fiber, 120 calories, 20g carbs, 9g protein.
Split peas, ½ cup boiled = 8g fiber, 120 calories, 20g carbs, 8g protein.
6. Berries
“All berries are good for you, but blackberries and raspberries have the most fiber. They’re also delicious. Fresh berries can be expensive, but frozen is often more economical. If you don’t love the mushy texture of thawed berries, blend them into a smoothie or stir them into your oatmeal, she suggests. “You can also cook them down and put them on waffles in place of syrup.”
Artichoke hearts are packed with fiber. Add them to salads or pile them on pizza. If dealing with these spiky veggies is too daunting, try the canned kind. (But if you’re eating canned, keep an eye on sodium levels so you don’t go overboard.)
Nutrition information: ½ cup cooked = 7g fiber, 45 calories, 9g carbs, 2g protein, 1g sugar.
9. Brussels sprouts
If you’ve been avoiding Brussels sprouts since you were a kid, they’re worth a second look. “Brussels sprouts are awesome. They’re delicious roasted or sautéed. (Plus, they’re cute.)
A spoonful of chia seeds can go a long way. They’re incredibly rich in fiber, contain omega-3 fatty acids, and have a nice protein punch, too. “You can throw them in oatmeal, yogurt, pudding, cereal, salads, and smoothies.
Many people love the jelly-like texture. If you aren’t one of them, try mixing them into a smoothie or yogurt right before you eat it, so they don’t have as much time to absorb water and plump up.
Haas avocados are a great source of healthy fats. And unlike most fiber-rich foods, you can use them as a condiment. “You can spread avocado on sandwiches instead of mayonnaise, or put it on your toast if you’re a true millennial.” Guacamole (with whole-grain crackers or paired with raw veggies) is another delicious way to get your daily fiber.
Nutrition information: ½ avocado = 5 g fiber, 120 calories, 6g carbs, 1g protein.
Eating more fiber? Read this first!
Before you jump on the fiber bandwagon, a word of caution: “Add fiber to your diet slowly,” Taylor says. If you aren’t used to a lot of fiber, eating too much can cause bloating and cramping. Increase high-fiber foods gradually over a few weeks to avoid that inflated feeling.
Another important tip
When adding fiber to your diet, be sure to drink enough water. Fiber pulls in water. That’s a good thing, but if you aren’t drinking enough, it can make constipation worse. To keep things moving, drink at least 2 liters of fluids each day.
If you increase your fiber slowly and steadily and drink lots of fluid, your body will adjust,” Taylor says. And you’ll be glad it did.
How much fiber should I eat?
The National Institute of Diabetes and Digestive and Kidney Disease recommends eating 14 grams per 1,000 calories consumed per day. For example, if you follow a 2,000 calorie diet every day, you should try to eat 28 grams of fiber each day. Every person, regardless of whether they have diverticula, should try to consume this much fiber every day. Fiber is the part of plant foods that can’t be digested.
Uncomplicated Diverticulitis/Diverticulosis is a clinical condition of inflammation due to micro-perforation and herniations of the colonic mucosa and submucosa through the muscle layers, in which multiple sac-like protrusions, abscesses, fistulas, peritonitis, and colonic stenosis, small pouches, or sacs, form and push outward through weak spots in the wall of your colon(diverticula) that develop along the gastrointestinal tract. Though diverticula may form at weak points in the walls of either the small or large intestines, the majority occur in the large intestine (most commonly the sigmoid colon).
These pouches are most common in the lower part of your colon, called the sigmoid colon. One pouch is called a diverticulum. Multiple pouches are called diverticula. Most people with diverticulosis do not have symptoms or problems.
When diverticulosis does cause symptoms or problems, doctors call this diverticular disease. For some people, diverticulosis causes symptoms such as changes in bowel movement patterns or pain in the abdomen. Diverticulosis may also cause problems such as diverticular bleeding and diverticulitis.
Types of Diverticulitis
There are two types of diverticulitis:
Uncomplicated diverticulitis – Diverticula and the surrounding intestinal lining are inflamed but there are no signs of pus building up (abscesses) or the inflammation spreading.
Complicated diverticulitis – Abscesses have formed. Sometimes the inflammation has even already spread or the wall of the intestine has torn (intestinal perforation). The intestine may also become blocked or the inner lining of the tummy may become inflamed (peritonitis).
or
Acute diverticulitis – Surgery usually isn’t necessary for people who have acute diverticulitis. But there are exceptions: If abscesses (collections of pus) have formed, and treatment with antibiotics isn’t successful, surgery is unavoidable. The aim is then to prevent serious complications such as the wall of the intestine tearing (perforation) or the inner lining of the tummy becoming inflamed (peritonitis), which can lead to blood poisoning (septicemia).
Chronic diverticular disease – People who have recurrent diverticulitis or chronic symptoms generally don’t develop serious complications. Although such complications are possible, they tend to be rare if the inflammation is “uncomplicated” – in other words, as long as no abscesses have formed.
Causes of Diverticulitis
Experts are not sure what causes diverticulosis and diverticulitis. Researchers are studying several factors that may play a role in causing these conditions.
No one knows for certain why diverticulosis develops – however, a few theories have been suggested. Some experts believe that abnormal intermittent high pressure in the colon due to muscle spasm or straining with stool may cause diverticula to form at weak spots in the colon wall. Historically, low-fiber diets were felt to play a role in the development of diverticulosis.
Fiber – For more than 50 years, experts thought that following a low-fiber diet led to diverticulosis. However, recent research has found that a low-fiber diet may not play a role. This study also found that a high-fiber diet with more frequent bowel movements may be linked with a greater chance of having diverticulosis.4 Talk with your doctor about how much fiber you should include in your diet.
Genes – Some studies suggest that genes may make some people more likely to develop diverticulosis and diverticulitis. Experts are still studying the role genes play in causing these conditions.
Other factors – Studies have found links between diverticular disease—diverticulosis that causes symptoms or problems such as diverticular bleeding or diverticulitis—and the following factors:
Certain medicines – including nonsteroidal anti-inflammatory drugs (NSAIDs), such as aspirin and steroids
Intestinal motility – Another theory suggests the degeneration of glial neurons in the myenteric plexus and the interstitial cells of Cajal lead to slowed intestinal movement and consequently fecal content exerts increased pressure on the colon wall resulting in the formation of diverticula.[rx]
Lack of exercise
Obesity
Smoking
constipation
A diet that is low in dietary fiber (although this claim is controversial)
Connective tissue disorders (such as Marfan syndrome and Ehlers Danlos Syndrome) that may cause weakness in the colon wall
Diverticulitis may begin when bacteria or stool get caught in a pouch in your colon. A decrease in healthy bacteria and an increase in disease-causing bacteria in your colon may also lead to diverticulitis.
Symptoms of Diverticulitis
Most people with diverticulosis do not have symptoms. If your diverticulosis causes symptoms, they may include
bloating
constipation or diarrhea
cramping or pain in your lower abdomen
abdominal pain and bloating
constipation and diarrhea
flatulence
blood in the feces is usually minor, but bleeding can sometimes be heavy if a diverticulum gets inflamed or is near a blood vessel
anemia from repeated bleeding may occur.
Other conditions, such as irritable bowel syndrome and peptic ulcers, cause similar symptoms, so these symptoms may not mean you have diverticulosis. If you have these symptoms, see your doctor.
If you have diverticulosis and develop diverticular bleeding or diverticulitis, these conditions also cause symptoms.
In most cases, when you have diverticular bleeding, you will suddenly have a large amount of red or maroon-colored blood in your stool.
When you have diverticulitis, the inflamed pouches most often cause pain in the lower-left side of your abdomen. The pain is usually severe and comes on suddenly, though it can also be mild and get worse over several days. The intensity of the pain can change over time.
Diverticulitis may also cause
Diverticular bleeding may also cause dizziness or light-headedness, or weakness. See your doctor right away if you have any of these symptoms.
If you have symptoms such as bloating, constipation or diarrhea, or pain in your lower abdomen, see your doctor.
Constipation or diarrhea
Fevers and chills
Nausea or vomiting
Get constant, more severe tummy pain
Have a high temperature
Have diarrhea or constipation
Get mucus or blood in your poo, or bleeding from your bottom
Intermittent abdominal pain in the left lower quadrant with constipation, diarrhea or occasional large rectal bleeds (the pain may be triggered by eating and relieved by the passage of stool or flatus)
Tenderness in the left lower quadrant on abdominal examination.
In a minority of people and in people of Asian origin, pain and tenderness may be localized in the right lower quadrant
Symptoms may overlap with conditions such as irritable bowel syndrome, colitis, and malignancy.
Diagnosis of Diverticulitis
If your doctor suspects you may have diverticulosis or diverticulitis, your doctor may use your medical history, a physical exam, and tests to diagnose these conditions. Doctors may also diagnose diverticulosis if they notice pouches in the colon wall while performing tests, such as routine x-rays or colonoscopy, for other reasons.
Medical history
Your doctor will ask about your medical history, including your
bowel movement patterns
diet
health
medicines
symptoms
Physical exam
Your doctor will perform a physical exam, which may include a digital rectal exam. During a digital rectal exam, your doctor will have you bend over a table or lie on your side while holding your knees close to your chest. After putting on a glove, the doctor will slide a lubricated finger into your anus to check for pain, bleeding, hemorrhoids, or other problems.
Lab Test
Your doctor may use the following tests to help diagnose diverticulosis and diverticulitis:
Blood test – A health care professional may take a blood sample from you and send the sample to a lab to test for inflammation or anemia.
Stool sample – Your stool sample is checked for the presence of abnormal bacteria or parasites as possible causes of your infection, abdominal pain, blood in stool, diarrhea, or your other symptoms.
Stool tests – to check for the presence of blood in the feces or the presence of infections, which may mimic the symptoms of diverticulosis and diverticulitis.
Digital rectal exam – In this physical exam, your healthcare provider gently inserts a gloved, lubricated finger into your rectum to feel for any problems in your anus or rectum.
Barium enema (also called lower gastrointestinal tract radiography) – In this test, a liquid containing barium is injected into your anus. The liquid coats the inside of your colon, which helps make any problems in your colon more visible on X-rays.
Esophageal manometry – This technique measures the timing and strength of the contractions of your esophagus.
Sigmoidoscopy – In this exam, a thin flexible tube with a light on the end is inserted into your rectum and moved into your sigmoid colon. The tube is connected to a video camera. The camera allows a visual inspection of your sigmoid colon (where most diverticula form) and rectum.
Angiography – If you have rapid, heavy rectal bleeding, this procedure helps find where the bleeding is coming from. During this test, the arteries that supply the colon are injected with a harmless dye that allows the source of the bleeding to be seen.
Imaging Test
CT scan –A CT scan can show infected or inflamed diverticula and also reveal the severity of diverticulitis. A computerized tomography (CT) scan uses a combination of x-rays and computer technology to create images of your gastrointestinal (GI) tract.
An x-ray – technician performs the procedure in an outpatient center or a hospital. A radiologist reads and reports on the images. You don’t need anesthesia for this procedure.
CT scan – a health care professional may give you a solution to drink and an injection of a special dye called contrast medium. Contrast medium makes the structures inside your body easier to see during the procedure. You’ll lie on a table that slides into a tunnel-shaped device that takes the x-rays. A CT scan of your colon is the most common test doctors use to diagnose diverticulosis and diverticulitis.
Lower GI series
A lower GI series, also called a barium enema, is a procedure in which a doctor uses x-rays and a chalky liquid called barium to view your large intestine. The barium will make your large intestine more visible on an x-ray.
An x-ray technician and a radiologist perform a lower GI series at a hospital or an outpatient center. A health care professional will give you written bowel prep instructions to follow at home before the procedure. You don’t need anesthesia for this procedure.
For the procedure, you’ll be asked to lie on a table while the radiologist inserts a flexible tube into your anus and fills your large intestine with barium. You will need to hold still in various positions while the radiologist and technician take x-ray images and possibly an x-ray video, called fluoroscopy. If pouches are present in your colon, they will appear on the x-ray.
Colonoscopy
Colonoscopy is a procedure in which a doctor uses a long, flexible, narrow tube with a light and tiny camera on one end, called a colonoscope or endoscope, to look inside your rectum and colon.
A trained specialist performs a colonoscopy in a hospital or an outpatient center. A health care professional will give you written bowel prep instructions to follow at home before the procedure. You will receive sedatives, anesthesia, or pain medicine during the procedure.
During a colonoscopy, you’ll be asked to lie on a table while the doctor inserts a colonoscope into your anus and slowly guides it through your rectum and into your colon. Doctors may use a colonoscopy to confirm a diagnosis of diverticulosis or diverticulitis and rule out other conditions, such as cancer.
Treatment of Diverticulitis
Non-Pharmacological
The goal of treating diverticulosis is to prevent the pouches from causing symptoms or problems. Your doctor may recommend the following treatments.
High-fiber diet – Although a high-fiber diet may not prevent diverticulosis, it may help prevent symptoms or problems in people who already have diverticulosis. A doctor may suggest that you increase fiber in your diet slowly to reduce your chances of having gas and pain in your abdomen. Learn more about foods that are high in fiber.
Fiber supplements – Your doctor may suggest you take a fiber product such as methylcellulose (Citrucel) or psyllium (Metamucil) one to three times a day. These products are available as powders, pills, or wafers and provide 0.5 to 3.5 grams of fiber per dose. You should take fiber products with at least 8 ounces of water.
Diet – Some doctors advise people to try to carry on eating normally – or to eat a low-fiber diet for a while. Others recommend mainly eating soups or other non-solid foods, as well as drinking enough fluids, in the first few days. It’s not clear whether it really is better to avoid solid foods for a while. There aren’t any good studies in this area.
Nuts and Seeds – In the past, doctors thought you had to avoid certain foods if you had diverticulosis. These included nuts, seeds like sunflower and sesame, and even little seeds in fruits and vegetables such as cucumbers and strawberries. But recent research shows these foods don’t harm people with diverticulosis.
Draining – About 15 out of 100 people who have complicated diverticulitis have a pus-filled abscess. If necessary, the pus can be drained out of the body through a thin tube.
Drink plenty of water – Eating more fiber absorbs more water, so you’ll need to increase the amount of water you drink to keep stool soft and on the move. Many healthcare providers suggest drinking half your body’s weight in ounces. For example, if you weigh 160 pounds, you should drink 80 ounces of water each day.
Exercise daily – Physical movement helps food pass through your intestinal system. Exercise for 30 minutes on most days if you can.
Medicines
NSAIDs and Paracetamol – can be used to relieve pain. Some painkillers, including aspirin and ibuprofen, should not be taken regularly as they can cause stomach upsets. Ask a pharmacist about this.
Antispasmodics – Your doctor may prescribe antispasmodics such as mebeverine, and hyoscine hydrobromide, ondansetron, granisetron if you have persistent abdominal spasms.
Mesalazine – Some studies suggest that mesalazine (Asacol) taken every day or in cycles may help reduce symptoms that may occur with diverticulosis, such as pain in your abdomen or bloating. Studies suggest that the antibiotic rifaximin (Xifaxan) may also help with diverticulosis symptoms. The maintenance dose of Mesalazine 1.6g daily was administered to patients with the addition of probiotic VSL3 in patients with more severe disease to maintain remission
Antibiotics – The standard of outpatient care includes bowel rest, increase fluid intake, and oral antibiotic therapy (single or multiple drug regimen) that covers gram-negative rods and anaerobic bacteria. The most common regimen used in the United States consists of quinolones (ciprofloxacin) or sulfa drugs (trimethoprim/sulfamethoxazole) in combination with metronidazole (or clindamycin, if the patient is intolerant to metronidazole) or single-agent amoxicillin-clavulanate for 7 to 10 days.[rx][rx][rx] Inpatient management of diverticulitis requires intravenous antibiotics, intravenous fluids, and pain management. Again, antibiotics should cover gram-negative rods and anaerobes and be given for three to 5 days before switching to oral antibiotics for a ten to 14-day course. Bowel rest is preferred in patients requiring inpatient admission. Typically, defervescence and improvement in leukocytosis should be observed for two to four days of hospitalization, if not an alternative diagnosis or complications should be suspected. Prompt surgical evaluation should be considered.
Role of vitamin D – The role of vitamin D has recently been explored in diverticular disease. In a retrospective cohort study conducted by Maguire et al.,[rx] prediagnostic levels of vitamin D (25-OH) were measured and compared between 9,116 patients with uncomplicated diverticulosis and 922 patients who developed diverticulitis requiring hospitalization. The study found a statistically significant higher mean prediagnostic serum vitamin D (25-OH) level in patients with uncomplicated diverticulosis in comparison to patients who required hospitalization for diverticulitis.[rx]
Citrucel or Metamucil – They might suggest a fiber product like Citrucel or Metamucil. They come in pill, powder, or wafer forms. You’ll take it with lots of water.
Probiotics – Some studies show that probiotics may help with diverticulosis symptoms and may help prevent diverticulitis. However, researchers are still studying this subject. Probiotics are live bacteria like those that occur normally in your stomach and intestines. You can find probiotics in dietary supplements—in capsule, tablet, and powder form—and in some foods, such as yogurt. For safety reasons, talk with your doctor before using probiotics or any complementary or alternative medicines or medical practices.
Antibiotic Regimens for Acute Diverticulitis
Type of Treatment
(References)
Single Agent
Multiple Agents
Duration
Outpatient treatment of mild uncomplicated diverticulitis (rx, rx, rx)
Moxifloxacin 400 mg PO every 24 h
Amoxicillin-clavulanic acid 875 mg/125 mg PO every 12 h or 1000/62.5 mg tab 2 PO every 12 h
Trimethoprim-sulfamethoxazole 1 DS 160/800 mg PO every 12 h
Ciprofloxacin 750 mg PO every 12 h†
Levofloxacin 750 mg PO every 24 hEach in combination with metronidazole 500 mg PO every 6 h†
4–7 days if source controlled/abscess drained
Inpatient treatment of mild to moderately complicated diverticulitis (rx, rx)
Ertepenem 1g IV every 24 h
Moxifloxacin 400 mg IV every 24 h
Ticarcillin-clavulanic acid 200–300 mg/kg/d divided doses every 4–6 h
Cefazolin 1–2 g IV every 8 h
Cefuroxime 1.5 g IV every 8 h
Ceftriaxone 1–2 g IV every12–24 h
Cefotaxime 1–2 g IV every 6–8 h
Ciprofloxacin IV 400 mg every 12 h
Levofloxacin IV 750 mg every 24 hEach in combination with metronidazole 500 mg IV every 8–12 h or 1500 mg IV every 24 h
4–7 days if source controlled/abscess drained
Inpatient treatment of severe complicated diverticulitis, peritonitis (rx, rx)
Imipenem-cilastatin 500 mg every 6 h or 1g IV every 8 h
Meropenem 1 g IV every 8 h
Doripenem 500 mg IV every 8 h
Piperacillin-tazobactam 3.375g IV every 6 h
Cefepime 2g IV every 8 h
Ceftazidime 2g IV every 8 h
Ciprofloxacin 400 mg IV every 12 h
Levofloxacin 750 mg IV every 24 hEach in combination with metronidazole 500 mg IV every 8–12 h or 1500 mg IV every 24 h
4–7 days if source controlled/abscess drained
Surgery
Emergency surgery is required to treat peritonitis, the most serious potential complication of diverticulitis. Peritonitis requires surgical repair as well as intravenous antibiotics.
Surgery also may be required during the hospital stay to treat a particularly severe episode of diverticulitis. These include continuous bleeding, perforation of an abscess, attachment of two organs by a fistula, or colon obstruction caused by scarring from previous episodes of diverticulitis.
Surgical procedures to do this include
Cricopharyngeal myotomy – This involves making small cuts in the upper sphincter of the esophagus to widen it, so food can pass more easily through your esophagus.
Diverticulopexy with cricopharyngeal myotomy – This involves removing a larger diverticulum by turning it upside down and attaching it to the wall of the esophagus.
Diverticulectomy and cricopharyngeal myotomy – This involves removing the diverticulum while performing a cricopharyngeal myotomy. It’s a combination that’s often used to treat Zenker’s diverticula.
Endoscopic diverticulectomy – This is a minimally invasive procedure that divides the tissue between the diverticulum and esophagus, allowing food to drain from the diverticulum.
Colon resection – If your bleeding does not stop, a surgeon may perform abdominal surgery with a colon resection. In a colon resection, the surgeon removes the affected part of your colon and joins the remaining ends of your colon together. You will receive general anesthesia for this procedure.
In some cases, during a colon resection, it may not be safe for the surgeon to rejoin the ends of your colon right away. In this case, the surgeon performs a temporary colostomy. Several months later, in a second surgery, the surgeon rejoins the ends of your colon and closes the opening in your abdomen.
When is surgery for diverticulitis considered?
Surgery for diverticulitis is considered if you have:
Abscesses – An abscess is a container or “walled-off” infection in the abdomen. If the fluid in an abscess (a collection of bacteria and white blood cells) is not successfully drained with a needle or catheter, surgery is needed. In surgery, the abscess is cleaned up and the affected part of the colon is removed.
Perforation/peritonitis – A tear (perforation) in your colon allows pus or stool to leak into your abdominal cavity, resulting in peritonitis. This is a life-threatening infection that requires emergency surgery to clean the cavity and remove the damaged part of the colon.
Blockages or strictures – Previous infections in your colon can cause scars to form, which can result in a partial or complete blockage or strictures (narrowing of sections of the colon). A complete blockage requires surgery (partial blockage does not).
Fistulas – A fistula is an abnormal passageway or tunnel that forms and connects with another organ. An abscess that erodes into the surrounding tissue creates these passageways. A fistula in the colon can connect to the skin, bladder, vagina, uterus, or another part of the colon. Most fistulas don’t close on their own so surgery is needed.
Continued rectal bleeding (also called diverticular bleeding) – Diverticular bleeding occurs when a small blood vessel near the diverticula bursts. Mild bleeding usually stops on its own, but about 20% of cases require treatment. Surgery may be needed if other attempts to stop the bleeding fail, such as clipping, drug infusion, or cauterizing the bleeding artery. If bleeding is heavy and rapid, emergency surgery is needed.
Severe diverticulitis – that has not responded to other treatment methods. Multiple attacks despite following a high-fiber diet. You and your surgeon may decide surgery to remove the diseased part of the colon is the best method to prevent future attacks.
Complications
Over time, an esophageal diverticulum can lead to some health complications.
Aspiration pneumonia – If an esophageal diverticulum causes regurgitation, it can lead to aspiration pneumonia. This is a lung infection caused by inhaling things, such as food and saliva, that usually travel down your esophagus.
Obstruction – An obstruction near the diverticulum can make it hard, if not impossible, to swallow. This can also cause the pouch to rupture and bleed.
Squamous cell carcinoma – In very rare cases, ongoing irritation of the pouch can lead to squamous cell carcinoma.
Sacs can get infected, and even burst – This is diverticulitis. It’s treated with rest, fluids, and antibiotics.
The infection can spread and an abscess can form. A specialist will need to drain the pus.
A perforation (a hole along the stomach wall) can occur – It’s rare, but life-threatening and requires immediate surgery.
You can get a diverticular hemorrhage – This is rare. It happens when your arteries wear through the intestinal wall. It causes massive bleeding and requires hospitalization and blood transfusions.
Best High-Fiber Foods
You may not think much about fiber — until you find yourself dealing with an, er, irregular situation.
Indeed, dietary fiber is a magic ingredient that keeps you regular. But thwarting constipation is not its only job. “Fiber does lots of cool stuff in the body. Here’s why you need it — and where to get it.
Benefits of a high-fiber diet
Fiber is an unsung hero. Among its claims to fame, a high-fiber diet can:
Soften stool and prevent constipation.
Lower cholesterol, reducing the risk of heart disease.
Reduce the risk of diseases such as colorectal cancer.
Keep blood sugar levels from spiking.
Make you feel full longer, which can help you lose weight.
There are two types of fiber, both of which are good for you
Soluble fiber – pulls in water. It slows digestion and lowers cholesterol. Soluble fiber is found in foods such as beans, seeds, peas, barley, oat bran, and some fruits and vegetables.
Insoluble fiber – is your classic roughage. It helps stool speed through the intestines. You’ll find it in foods such as whole grains, wheat bran, and the peels and seeds of fruits and veggies.
Aim for 25 to 35 grams of fiber a day, Taylor says — and a mix of soluble and insoluble fiber is ideal.
What foods are high in fiber?
Fiber comes from plants, so don’t bother looking for it in your chicken dinner. But the plant kingdom has a lot to offer, and the best sources of dietary fiber might surprise you. Here are Taylor’s top 11.
1. Whole-wheat pasta
Carbs get a bad rap, but whole grains are a great source of fiber and are also rich in healthy phytonutrients, Taylor says. Skip the white pasta (which has been stripped of all the good stuff), and go for whole-wheat instead.
“Barley is a delicious grain that’s often overlooked,” Taylor says. Try tossing it in soups or mix up a grain bowl with your favorite meat and veggies.
“Legumes are star players. They’re some of the best sources of protein and fiber, they help keep you full, and they have amazing nutrient composition. Chickpeas are a fiber-full favorite from the legume list. Add them to soups or salads, snack on chickpea hummus, or roast them whole for a crunchy, shelf-stable snack.
Nutrition information: ½ cup cooked = 6g fiber, 140 calories, 23g carbs, 7g protein.
4. Edamame
Edamame, or immature soybeans, has a mild flavor and pleasing texture. They’re also one of the few plant sources that contain all the amino acids your body needs, so they’re a great choice for vegans and vegetarians. You can find them in the frozen food section, still in the pod, or already shelled. Add edamame to salads and stir-fries, Taylor suggests. (Edamame is often a big hit for kids to snack on, too.)
Nutrition information: ½ cup boiled and shelled = 4g fiber, 100 calories, 7g carbs, 9g protein.
5. Lentils and split peas
These two legumes have similar nutrition profiles and are used in similar ways. “Lentils and split peas are nutritional powerhouses. They cook quickly and are great in soups. Try swapping lentils for some of the meat in your chili to boost the plant-powered goodness, she recommends.
Nutrition information:
Lentils, ½ cup cooked = 8g fiber, 120 calories, 20g carbs, 9g protein.
Split peas, ½ cup boiled = 8g fiber, 120 calories, 20g carbs, 8g protein.
6. Berries
“All berries are good for you, but blackberries and raspberries have the most fiber. They’re also delicious. Fresh berries can be expensive, but frozen is often more economical. If you don’t love the mushy texture of thawed berries, blend them into a smoothie or stir them into your oatmeal, she suggests. “You can also cook them down and put them on waffles in place of syrup.”
Artichoke hearts are packed with fiber. Add them to salads or pile them on pizza. If dealing with these spiky veggies is too daunting, try the canned kind. (But if you’re eating canned, keep an eye on sodium levels so you don’t go overboard.)
Nutrition information: ½ cup cooked = 7g fiber, 45 calories, 9g carbs, 2g protein, 1g sugar.
9. Brussels sprouts
If you’ve been avoiding Brussels sprouts since you were a kid, they’re worth a second look. “Brussels sprouts are awesome. They’re delicious roasted or sautéed. (Plus, they’re cute.)
A spoonful of chia seeds can go a long way. They’re incredibly rich in fiber, contain omega-3 fatty acids, and have a nice protein punch, too. “You can throw them in oatmeal, yogurt, pudding, cereal, salads, and smoothies.
Many people love the jelly-like texture. If you aren’t one of them, try mixing them into a smoothie or yogurt right before you eat it, so they don’t have as much time to absorb water and plump up.
Haas avocados are a great source of healthy fats. And unlike most fiber-rich foods, you can use them as a condiment. “You can spread avocado on sandwiches instead of mayonnaise, or put it on your toast if you’re a true millennial.” Guacamole (with whole-grain crackers or paired with raw veggies) is another delicious way to get your daily fiber.
Nutrition information: ½ avocado = 5 g fiber, 120 calories, 6g carbs, 1g protein.
Eating more fiber? Read this first!
Before you jump on the fiber bandwagon, a word of caution: “Add fiber to your diet slowly,” Taylor says. If you aren’t used to a lot of fiber, eating too much can cause bloating and cramping. Increase high-fiber foods gradually over a few weeks to avoid that inflated feeling.
Another important tip
When adding fiber to your diet, be sure to drink enough water. Fiber pulls in water. That’s a good thing, but if you aren’t drinking enough, it can make constipation worse. To keep things moving, drink at least 2 liters of fluids each day.
If you increase your fiber slowly and steadily and drink lots of fluid, your body will adjust,” Taylor says. And you’ll be glad it did.
How much fiber should I eat?
The National Institute of Diabetes and Digestive and Kidney Disease recommends eating 14 grams per 1,000 calories consumed per day. For example, if you follow a 2,000 calorie diet every day, you should try to eat 28 grams of fiber each day. Every person, regardless of whether they have diverticula, should try to consume this much fiber every day. Fiber is the part of plant foods that can’t be digested.
Diverticulitis/Diverticulosis is a clinical condition of inflammation due to micro-perforation and herniations of the colonic mucosa and submucosa through the muscle layers, in which multiple sac-like protrusions, abscesses, fistulas, peritonitis, and colonic stenosis, small pouches, or sacs, form and push outward through weak spots in the wall of your colon(diverticula) that develop along the gastrointestinal tract. Though diverticula may form at weak points in the walls of either the small or large intestines, the majority occur in the large intestine (most commonly the sigmoid colon).
These pouches are most common in the lower part of your colon, called the sigmoid colon. One pouch is called a diverticulum. Multiple pouches are called diverticula. Most people with diverticulosis do not have symptoms or problems.
When diverticulosis does cause symptoms or problems, doctors call this diverticular disease. For some people, diverticulosis causes symptoms such as changes in bowel movement patterns or pain in the abdomen. Diverticulosis may also cause problems such as diverticular bleeding and diverticulitis.
Types of Diverticulitis
There are two types of diverticulitis:
Uncomplicated diverticulitis – Diverticula and the surrounding intestinal lining are inflamed but there are no signs of pus building up (abscesses) or the inflammation spreading.
Complicated diverticulitis – Abscesses have formed. Sometimes the inflammation has even already spread or the wall of the intestine has torn (intestinal perforation). The intestine may also become blocked or the inner lining of the tummy may become inflamed (peritonitis).
or
Acute diverticulitis – Surgery usually isn’t necessary for people who have acute diverticulitis. But there are exceptions: If abscesses (collections of pus) have formed, and treatment with antibiotics isn’t successful, surgery is unavoidable. The aim is then to prevent serious complications such as the wall of the intestine tearing (perforation) or the inner lining of the tummy becoming inflamed (peritonitis), which can lead to blood poisoning (septicemia).
Chronic diverticular disease – People who have recurrent diverticulitis or chronic symptoms generally don’t develop serious complications. Although such complications are possible, they tend to be rare if the inflammation is “uncomplicated” – in other words, as long as no abscesses have formed.
Causes of Diverticulitis
Experts are not sure what causes diverticulosis and diverticulitis. Researchers are studying several factors that may play a role in causing these conditions.
No one knows for certain why diverticulosis develops – however, a few theories have been suggested. Some experts believe that abnormal intermittent high pressure in the colon due to muscle spasm or straining with stool may cause diverticula to form at weak spots in the colon wall. Historically, low-fiber diets were felt to play a role in the development of diverticulosis.
Fiber – For more than 50 years, experts thought that following a low-fiber diet led to diverticulosis. However, recent research has found that a low-fiber diet may not play a role. This study also found that a high-fiber diet with more frequent bowel movements may be linked with a greater chance of having diverticulosis.4 Talk with your doctor about how much fiber you should include in your diet.
Genes – Some studies suggest that genes may make some people more likely to develop diverticulosis and diverticulitis. Experts are still studying the role genes play in causing these conditions.
Other factors – Studies have found links between diverticular disease—diverticulosis that causes symptoms or problems such as diverticular bleeding or diverticulitis—and the following factors:
Certain medicines – including nonsteroidal anti-inflammatory drugs (NSAIDs), such as aspirin and steroids
Intestinal motility – Another theory suggests the degeneration of glial neurons in the myenteric plexus and the interstitial cells of Cajal lead to slowed intestinal movement and consequently fecal content exerts increased pressure on the colon wall resulting in the formation of diverticula.[rx]
Lack of exercise
Obesity
Smoking
constipation
A diet that is low in dietary fiber (although this claim is controversial)
Connective tissue disorders (such as Marfan syndrome and Ehlers Danlos Syndrome) that may cause weakness in the colon wall
Diverticulitis may begin when bacteria or stool get caught in a pouch in your colon. A decrease in healthy bacteria and an increase in disease-causing bacteria in your colon may also lead to diverticulitis.
Symptoms of Diverticulitis
Most people with diverticulosis do not have symptoms. If your diverticulosis causes symptoms, they may include
bloating
constipation or diarrhea
cramping or pain in your lower abdomen
abdominal pain and bloating
constipation and diarrhea
flatulence
blood in the feces is usually minor, but bleeding can sometimes be heavy if a diverticulum gets inflamed or is near a blood vessel
anemia from repeated bleeding may occur.
Other conditions, such as irritable bowel syndrome and peptic ulcers, cause similar symptoms, so these symptoms may not mean you have diverticulosis. If you have these symptoms, see your doctor.
If you have diverticulosis and develop diverticular bleeding or diverticulitis, these conditions also cause symptoms.
In most cases, when you have diverticular bleeding, you will suddenly have a large amount of red or maroon-colored blood in your stool.
When you have diverticulitis, the inflamed pouches most often cause pain in the lower-left side of your abdomen. The pain is usually severe and comes on suddenly, though it can also be mild and get worse over several days. The intensity of the pain can change over time.
Diverticulitis may also cause
Diverticular bleeding may also cause dizziness or light-headedness, or weakness. See your doctor right away if you have any of these symptoms.
If you have symptoms such as bloating, constipation or diarrhea, or pain in your lower abdomen, see your doctor.
Constipation or diarrhea
Fevers and chills
Nausea or vomiting
Get constant, more severe tummy pain
Have a high temperature
Have diarrhea or constipation
Get mucus or blood in your poo, or bleeding from your bottom
Intermittent abdominal pain in the left lower quadrant with constipation, diarrhea or occasional large rectal bleeds (the pain may be triggered by eating and relieved by the passage of stool or flatus)
Tenderness in the left lower quadrant on abdominal examination.
In a minority of people and in people of Asian origin, pain and tenderness may be localized in the right lower quadrant
Symptoms may overlap with conditions such as irritable bowel syndrome, colitis, and malignancy.
Diagnosis of Diverticulitis
If your doctor suspects you may have diverticulosis or diverticulitis, your doctor may use your medical history, a physical exam, and tests to diagnose these conditions. Doctors may also diagnose diverticulosis if they notice pouches in the colon wall while performing tests, such as routine x-rays or colonoscopy, for other reasons.
Medical history
Your doctor will ask about your medical history, including your
bowel movement patterns
diet
health
medicines
symptoms
Physical exam
Your doctor will perform a physical exam, which may include a digital rectal exam. During a digital rectal exam, your doctor will have you bend over a table or lie on your side while holding your knees close to your chest. After putting on a glove, the doctor will slide a lubricated finger into your anus to check for pain, bleeding, hemorrhoids, or other problems.
Lab Test
Your doctor may use the following tests to help diagnose diverticulosis and diverticulitis:
Blood test – A health care professional may take a blood sample from you and send the sample to a lab to test for inflammation or anemia.
Stool sample – Your stool sample is checked for the presence of abnormal bacteria or parasites as possible causes of your infection, abdominal pain, blood in stool, diarrhea, or your other symptoms.
Stool tests – to check for the presence of blood in the feces or the presence of infections, which may mimic the symptoms of diverticulosis and diverticulitis.
Digital rectal exam – In this physical exam, your healthcare provider gently inserts a gloved, lubricated finger into your rectum to feel for any problems in your anus or rectum.
Barium enema (also called lower gastrointestinal tract radiography) – In this test, a liquid containing barium is injected into your anus. The liquid coats the inside of your colon, which helps make any problems in your colon more visible on X-rays.
Esophageal manometry – This technique measures the timing and strength of the contractions of your esophagus.
Sigmoidoscopy – In this exam, a thin flexible tube with a light on the end is inserted into your rectum and moved into your sigmoid colon. The tube is connected to a video camera. The camera allows a visual inspection of your sigmoid colon (where most diverticula form) and rectum.
Angiography – If you have rapid, heavy rectal bleeding, this procedure helps find where the bleeding is coming from. During this test, the arteries that supply the colon are injected with a harmless dye that allows the source of the bleeding to be seen.
Imaging Test
CT scan –A CT scan can show infected or inflamed diverticula and also reveal the severity of diverticulitis. A computerized tomography (CT) scan uses a combination of x-rays and computer technology to create images of your gastrointestinal (GI) tract.
An x-ray – technician performs the procedure in an outpatient center or a hospital. A radiologist reads and reports on the images. You don’t need anesthesia for this procedure.
CT scan – a health care professional may give you a solution to drink and an injection of a special dye called contrast medium. Contrast medium makes the structures inside your body easier to see during the procedure. You’ll lie on a table that slides into a tunnel-shaped device that takes the x-rays. A CT scan of your colon is the most common test doctors use to diagnose diverticulosis and diverticulitis.
Lower GI series
A lower GI series, also called a barium enema, is a procedure in which a doctor uses x-rays and a chalky liquid called barium to view your large intestine. The barium will make your large intestine more visible on an x-ray.
An x-ray technician and a radiologist perform a lower GI series at a hospital or an outpatient center. A health care professional will give you written bowel prep instructions to follow at home before the procedure. You don’t need anesthesia for this procedure.
For the procedure, you’ll be asked to lie on a table while the radiologist inserts a flexible tube into your anus and fills your large intestine with barium. You will need to hold still in various positions while the radiologist and technician take x-ray images and possibly an x-ray video, called fluoroscopy. If pouches are present in your colon, they will appear on the x-ray.
Colonoscopy
Colonoscopy is a procedure in which a doctor uses a long, flexible, narrow tube with a light and tiny camera on one end, called a colonoscope or endoscope, to look inside your rectum and colon.
A trained specialist performs a colonoscopy in a hospital or an outpatient center. A health care professional will give you written bowel prep instructions to follow at home before the procedure. You will receive sedatives, anesthesia, or pain medicine during the procedure.
During a colonoscopy, you’ll be asked to lie on a table while the doctor inserts a colonoscope into your anus and slowly guides it through your rectum and into your colon. Doctors may use a colonoscopy to confirm a diagnosis of diverticulosis or diverticulitis and rule out other conditions, such as cancer.
Treatment of Diverticulitis
Non-Pharmacological
The goal of treating diverticulosis is to prevent the pouches from causing symptoms or problems. Your doctor may recommend the following treatments.
High-fiber diet – Although a high-fiber diet may not prevent diverticulosis, it may help prevent symptoms or problems in people who already have diverticulosis. A doctor may suggest that you increase fiber in your diet slowly to reduce your chances of having gas and pain in your abdomen. Learn more about foods that are high in fiber.
Fiber supplements – Your doctor may suggest you take a fiber product such as methylcellulose (Citrucel) or psyllium (Metamucil) one to three times a day. These products are available as powders, pills, or wafers and provide 0.5 to 3.5 grams of fiber per dose. You should take fiber products with at least 8 ounces of water.
Diet – Some doctors advise people to try to carry on eating normally – or to eat a low-fiber diet for a while. Others recommend mainly eating soups or other non-solid foods, as well as drinking enough fluids, in the first few days. It’s not clear whether it really is better to avoid solid foods for a while. There aren’t any good studies in this area.
Nuts and Seeds – In the past, doctors thought you had to avoid certain foods if you had diverticulosis. These included nuts, seeds like sunflower and sesame, and even little seeds in fruits and vegetables such as cucumbers and strawberries. But recent research shows these foods don’t harm people with diverticulosis.
Draining – About 15 out of 100 people who have complicated diverticulitis have a pus-filled abscess. If necessary, the pus can be drained out of the body through a thin tube.
Drink plenty of water – Eating more fiber absorbs more water, so you’ll need to increase the amount of water you drink to keep stool soft and on the move. Many healthcare providers suggest drinking half your body’s weight in ounces. For example, if you weigh 160 pounds, you should drink 80 ounces of water each day.
Exercise daily – Physical movement helps food pass through your intestinal system. Exercise for 30 minutes on most days if you can.
Medicines
NSAIDs and Paracetamol – can be used to relieve pain. Some painkillers, including aspirin and ibuprofen, should not be taken regularly as they can cause stomach upsets. Ask a pharmacist about this.
Antispasmodics – Your doctor may prescribe antispasmodics such as mebeverine, and hyoscine hydrobromide, ondansetron, granisetron if you have persistent abdominal spasms.
Mesalazine – Some studies suggest that mesalazine (Asacol) taken every day or in cycles may help reduce symptoms that may occur with diverticulosis, such as pain in your abdomen or bloating. Studies suggest that the antibiotic rifaximin (Xifaxan) may also help with diverticulosis symptoms. The maintenance dose of Mesalazine 1.6g daily was administered to patients with the addition of probiotic VSL3 in patients with more severe disease to maintain remission
Antibiotics – The standard of outpatient care includes bowel rest, increase fluid intake, and oral antibiotic therapy (single or multiple drug regimen) that covers gram-negative rods and anaerobic bacteria. The most common regimen used in the United States consists of quinolones (ciprofloxacin) or sulfa drugs (trimethoprim/sulfamethoxazole) in combination with metronidazole (or clindamycin, if the patient is intolerant to metronidazole) or single-agent amoxicillin-clavulanate for 7 to 10 days.[rx][rx][rx] Inpatient management of diverticulitis requires intravenous antibiotics, intravenous fluids, and pain management. Again, antibiotics should cover gram-negative rods and anaerobes and be given for three to 5 days before switching to oral antibiotics for a ten to 14-day course. Bowel rest is preferred in patients requiring inpatient admission. Typically, defervescence and improvement in leukocytosis should be observed for two to four days of hospitalization, if not an alternative diagnosis or complications should be suspected. Prompt surgical evaluation should be considered.
Role of vitamin D – The role of vitamin D has recently been explored in diverticular disease. In a retrospective cohort study conducted by Maguire et al.,[rx] prediagnostic levels of vitamin D (25-OH) were measured and compared between 9,116 patients with uncomplicated diverticulosis and 922 patients who developed diverticulitis requiring hospitalization. The study found a statistically significant higher mean prediagnostic serum vitamin D (25-OH) level in patients with uncomplicated diverticulosis in comparison to patients who required hospitalization for diverticulitis.[rx]
Citrucel or Metamucil – They might suggest a fiber product like Citrucel or Metamucil. They come in pill, powder, or wafer forms. You’ll take it with lots of water.
Probiotics – Some studies show that probiotics may help with diverticulosis symptoms and may help prevent diverticulitis. However, researchers are still studying this subject. Probiotics are live bacteria like those that occur normally in your stomach and intestines. You can find probiotics in dietary supplements—in capsule, tablet, and powder form—and in some foods, such as yogurt. For safety reasons, talk with your doctor before using probiotics or any complementary or alternative medicines or medical practices.
Antibiotic Regimens for Acute Diverticulitis
Type of Treatment
(References)
Single Agent
Multiple Agents
Duration
Outpatient treatment of mild uncomplicated diverticulitis (rx, rx, rx)
Moxifloxacin 400 mg PO every 24 h
Amoxicillin-clavulanic acid 875 mg/125 mg PO every 12 h or 1000/62.5 mg tab 2 PO every 12 h
Trimethoprim-sulfamethoxazole 1 DS 160/800 mg PO every 12 h
Ciprofloxacin 750 mg PO every 12 h†
Levofloxacin 750 mg PO every 24 hEach in combination with metronidazole 500 mg PO every 6 h†
4–7 days if source controlled/abscess drained
Inpatient treatment of mild to moderately complicated diverticulitis (rx, rx)
Ertepenem 1g IV every 24 h
Moxifloxacin 400 mg IV every 24 h
Ticarcillin-clavulanic acid 200–300 mg/kg/d divided doses every 4–6 h
Cefazolin 1–2 g IV every 8 h
Cefuroxime 1.5 g IV every 8 h
Ceftriaxone 1–2 g IV every12–24 h
Cefotaxime 1–2 g IV every 6–8 h
Ciprofloxacin IV 400 mg every 12 h
Levofloxacin IV 750 mg every 24 hEach in combination with metronidazole 500 mg IV every 8–12 h or 1500 mg IV every 24 h
4–7 days if source controlled/abscess drained
Inpatient treatment of severe complicated diverticulitis, peritonitis (rx, rx)
Imipenem-cilastatin 500 mg every 6 h or 1g IV every 8 h
Meropenem 1 g IV every 8 h
Doripenem 500 mg IV every 8 h
Piperacillin-tazobactam 3.375g IV every 6 h
Cefepime 2g IV every 8 h
Ceftazidime 2g IV every 8 h
Ciprofloxacin 400 mg IV every 12 h
Levofloxacin 750 mg IV every 24 hEach in combination with metronidazole 500 mg IV every 8–12 h or 1500 mg IV every 24 h
4–7 days if source controlled/abscess drained
Surgery
Emergency surgery is required to treat peritonitis, the most serious potential complication of diverticulitis. Peritonitis requires surgical repair as well as intravenous antibiotics.
Surgery also may be required during the hospital stay to treat a particularly severe episode of diverticulitis. These include continuous bleeding, perforation of an abscess, attachment of two organs by a fistula, or colon obstruction caused by scarring from previous episodes of diverticulitis.
Surgical procedures to do this include
Cricopharyngeal myotomy – This involves making small cuts in the upper sphincter of the esophagus to widen it, so food can pass more easily through your esophagus.
Diverticulopexy with cricopharyngeal myotomy – This involves removing a larger diverticulum by turning it upside down and attaching it to the wall of the esophagus.
Diverticulectomy and cricopharyngeal myotomy – This involves removing the diverticulum while performing a cricopharyngeal myotomy. It’s a combination that’s often used to treat Zenker’s diverticula.
Endoscopic diverticulectomy – This is a minimally invasive procedure that divides the tissue between the diverticulum and esophagus, allowing food to drain from the diverticulum.
Colon resection – If your bleeding does not stop, a surgeon may perform abdominal surgery with a colon resection. In a colon resection, the surgeon removes the affected part of your colon and joins the remaining ends of your colon together. You will receive general anesthesia for this procedure.
In some cases, during a colon resection, it may not be safe for the surgeon to rejoin the ends of your colon right away. In this case, the surgeon performs a temporary colostomy. Several months later, in a second surgery, the surgeon rejoins the ends of your colon and closes the opening in your abdomen.
When is surgery for diverticulitis considered?
Surgery for diverticulitis is considered if you have:
Abscesses – An abscess is a container or “walled-off” infection in the abdomen. If the fluid in an abscess (a collection of bacteria and white blood cells) is not successfully drained with a needle or catheter, surgery is needed. In surgery, the abscess is cleaned up and the affected part of the colon is removed.
Perforation/peritonitis – A tear (perforation) in your colon allows pus or stool to leak into your abdominal cavity, resulting in peritonitis. This is a life-threatening infection that requires emergency surgery to clean the cavity and remove the damaged part of the colon.
Blockages or strictures – Previous infections in your colon can cause scars to form, which can result in a partial or complete blockage or strictures (narrowing of sections of the colon). A complete blockage requires surgery (partial blockage does not).
Fistulas – A fistula is an abnormal passageway or tunnel that forms and connects with another organ. An abscess that erodes into the surrounding tissue creates these passageways. A fistula in the colon can connect to the skin, bladder, vagina, uterus, or another part of the colon. Most fistulas don’t close on their own so surgery is needed.
Continued rectal bleeding (also called diverticular bleeding) – Diverticular bleeding occurs when a small blood vessel near the diverticula bursts. Mild bleeding usually stops on its own, but about 20% of cases require treatment. Surgery may be needed if other attempts to stop the bleeding fail, such as clipping, drug infusion, or cauterizing the bleeding artery. If bleeding is heavy and rapid, emergency surgery is needed.
Severe diverticulitis – that has not responded to other treatment methods. Multiple attacks despite following a high-fiber diet. You and your surgeon may decide surgery to remove the diseased part of the colon is the best method to prevent future attacks.
Complications
Over time, an esophageal diverticulum can lead to some health complications.
Aspiration pneumonia – If an esophageal diverticulum causes regurgitation, it can lead to aspiration pneumonia. This is a lung infection caused by inhaling things, such as food and saliva, that usually travel down your esophagus.
Obstruction – An obstruction near the diverticulum can make it hard, if not impossible, to swallow. This can also cause the pouch to rupture and bleed.
Squamous cell carcinoma – In very rare cases, ongoing irritation of the pouch can lead to squamous cell carcinoma.
Sacs can get infected, and even burst – This is diverticulitis. It’s treated with rest, fluids, and antibiotics.
The infection can spread and an abscess can form. A specialist will need to drain the pus.
A perforation (a hole along the stomach wall) can occur – It’s rare, but life-threatening and requires immediate surgery.
You can get a diverticular hemorrhage – This is rare. It happens when your arteries wear through the intestinal wall. It causes massive bleeding and requires hospitalization and blood transfusions.
Best High-Fiber Foods
You may not think much about fiber — until you find yourself dealing with an, er, irregular situation.
Indeed, dietary fiber is a magic ingredient that keeps you regular. But thwarting constipation is not its only job. “Fiber does lots of cool stuff in the body. Here’s why you need it — and where to get it.
Benefits of a high-fiber diet
Fiber is an unsung hero. Among its claims to fame, a high-fiber diet can:
Soften stool and prevent constipation.
Lower cholesterol, reducing the risk of heart disease.
Reduce the risk of diseases such as colorectal cancer.
Keep blood sugar levels from spiking.
Make you feel full longer, which can help you lose weight.
There are two types of fiber, both of which are good for you
Soluble fiber – pulls in water. It slows digestion and lowers cholesterol. Soluble fiber is found in foods such as beans, seeds, peas, barley, oat bran, and some fruits and vegetables.
Insoluble fiber – is your classic roughage. It helps stool speed through the intestines. You’ll find it in foods such as whole grains, wheat bran, and the peels and seeds of fruits and veggies.
Aim for 25 to 35 grams of fiber a day, Taylor says — and a mix of soluble and insoluble fiber is ideal.
What foods are high in fiber?
Fiber comes from plants, so don’t bother looking for it in your chicken dinner. But the plant kingdom has a lot to offer, and the best sources of dietary fiber might surprise you. Here are Taylor’s top 11.
1. Whole-wheat pasta
Carbs get a bad rap, but whole grains are a great source of fiber and are also rich in healthy phytonutrients, Taylor says. Skip the white pasta (which has been stripped of all the good stuff), and go for whole-wheat instead.
“Barley is a delicious grain that’s often overlooked,” Taylor says. Try tossing it in soups or mix up a grain bowl with your favorite meat and veggies.
“Legumes are star players. They’re some of the best sources of protein and fiber, they help keep you full, and they have amazing nutrient composition. Chickpeas are a fiber-full favorite from the legume list. Add them to soups or salads, snack on chickpea hummus, or roast them whole for a crunchy, shelf-stable snack.
Nutrition information: ½ cup cooked = 6g fiber, 140 calories, 23g carbs, 7g protein.
4. Edamame
Edamame, or immature soybeans, has a mild flavor and pleasing texture. They’re also one of the few plant sources that contain all the amino acids your body needs, so they’re a great choice for vegans and vegetarians. You can find them in the frozen food section, still in the pod, or already shelled. Add edamame to salads and stir-fries, Taylor suggests. (Edamame is often a big hit for kids to snack on, too.)
Nutrition information: ½ cup boiled and shelled = 4g fiber, 100 calories, 7g carbs, 9g protein.
5. Lentils and split peas
These two legumes have similar nutrition profiles and are used in similar ways. “Lentils and split peas are nutritional powerhouses. They cook quickly and are great in soups. Try swapping lentils for some of the meat in your chili to boost the plant-powered goodness, she recommends.
Nutrition information:
Lentils, ½ cup cooked = 8g fiber, 120 calories, 20g carbs, 9g protein.
Split peas, ½ cup boiled = 8g fiber, 120 calories, 20g carbs, 8g protein.
6. Berries
“All berries are good for you, but blackberries and raspberries have the most fiber. They’re also delicious. Fresh berries can be expensive, but frozen is often more economical. If you don’t love the mushy texture of thawed berries, blend them into a smoothie or stir them into your oatmeal, she suggests. “You can also cook them down and put them on waffles in place of syrup.”
Artichoke hearts are packed with fiber. Add them to salads or pile them on pizza. If dealing with these spiky veggies is too daunting, try the canned kind. (But if you’re eating canned, keep an eye on sodium levels so you don’t go overboard.)
Nutrition information: ½ cup cooked = 7g fiber, 45 calories, 9g carbs, 2g protein, 1g sugar.
9. Brussels sprouts
If you’ve been avoiding Brussels sprouts since you were a kid, they’re worth a second look. “Brussels sprouts are awesome. They’re delicious roasted or sautéed. (Plus, they’re cute.)
A spoonful of chia seeds can go a long way. They’re incredibly rich in fiber, contain omega-3 fatty acids, and have a nice protein punch, too. “You can throw them in oatmeal, yogurt, pudding, cereal, salads, and smoothies.
Many people love the jelly-like texture. If you aren’t one of them, try mixing them into a smoothie or yogurt right before you eat it, so they don’t have as much time to absorb water and plump up.
Haas avocados are a great source of healthy fats. And unlike most fiber-rich foods, you can use them as a condiment. “You can spread avocado on sandwiches instead of mayonnaise, or put it on your toast if you’re a true millennial.” Guacamole (with whole-grain crackers or paired with raw veggies) is another delicious way to get your daily fiber.
Nutrition information: ½ avocado = 5 g fiber, 120 calories, 6g carbs, 1g protein.
Eating more fiber? Read this first!
Before you jump on the fiber bandwagon, a word of caution: “Add fiber to your diet slowly,” Taylor says. If you aren’t used to a lot of fiber, eating too much can cause bloating and cramping. Increase high-fiber foods gradually over a few weeks to avoid that inflated feeling.
Another important tip
When adding fiber to your diet, be sure to drink enough water. Fiber pulls in water. That’s a good thing, but if you aren’t drinking enough, it can make constipation worse. To keep things moving, drink at least 2 liters of fluids each day.
If you increase your fiber slowly and steadily and drink lots of fluid, your body will adjust,” Taylor says. And you’ll be glad it did.
How much fiber should I eat?
The National Institute of Diabetes and Digestive and Kidney Disease recommends eating 14 grams per 1,000 calories consumed per day. For example, if you follow a 2,000 calorie diet every day, you should try to eat 28 grams of fiber each day. Every person, regardless of whether they have diverticula, should try to consume this much fiber every day. Fiber is the part of plant foods that can’t be digested.