Adult Forearm Fractures/The forearm is the part of the arm between the wrist and the elbow. It is made up of two bones: the radius and the ulna. Forearm fractures are common in childhood, accounting for more than 40% of all childhood fractures. About three out of four forearm fractures in children occur at the wrist end of the radius.
Forearm fractures often occur when children are playing on the playground or participating in sports. If a child takes a tumble and falls onto an outstretched arm, there is a chance it may result in a forearm fracture. A child’s bones heal more quickly than an adult’s, so it is important to treat a fracture promptly—before healing begins—to avoid future problems.
Adult Forearm Fractures – Types, Classifications
Colles’, Smith’s, Isolated Radial Shaft Fractures, Both Bone Fractures – The Colles’ fracture is the most common fracture of the distal radius in adults. It gets its name from Irish Surgeon, Dr. Abraham Colles, who first described this injury pattern in 1814. The mechanism of injury is classically a FOOSH. It is a metaphyseal fracture that occurs around 1.5 inches proximal to the carpal articulation. Characteristically it presents with dorsal angulation and displacement of the distal fragment of the radius. On X-Ray, the wrist will present with what is known as the “dinner-fork” deformity. Smith’s fracture is essentially the opposite of the Colles’ fracture. It is often referred to as a “reverse Colles’,” and occurs with a fall onto or a direct blow or force to the dorsum of the hand.
Chauffeur’s/Radial Styloid Fracture – The Chauffeur’s fracture is an intra-articular fracture of the radius that includes the radial styloid. The fracture fragment can be variable in size. The injury is often the result of a FOOSH injury with a blow to the back of the wrist causing dorsiflexion and abduction causing the scaphoid to compress against the radial styloid. Patients may have small avulsions of the radial styloid that are not clinically significant, but these injuries are often associated with disruption of the radioscaphocapitate and other collateral ligaments; this can lead to lunate dislocation and scapholunate disruption. These fractures were historically suffered by drivers who would need to start their cars using a hand crank. Occasionally these cranks would backfire and forcefully strike drivers on the back of the wrist.
Die-Punch Fracture – A die punch fracture is an intra-articular fracture involving the lunate facet of the radius. The lunate facet is one of the three articular surfaces of the distal radius. It lies between the ulnar articulation and the scaphoid facet. It connects the distal radius to the lunate bone in the wrist. A die-punch fracture occurs with axial loading of the lunate, which causes an impaction fracture to the lunate facet of the radius. This fracture often occurs in isolation but can have associated injuries.
Galeazzi Fracture-Dislocation – The Galeazzi fracture-dislocation is a fracture of the distal third of the radius with an associated distal radioulnar joint (DRUJ) dislocation. These fractures are typically the result of FOOSH injuries. It is an uncommon injury pattern, and the DRUJ component is easi to miss for clinicians. They are labeled based on the direction of ulnar displacement. For example, if the DRUJ disruption causes volar deviation of the ulna, this is classified as a “Volar Galeazzi.”
Barton’s Fracture – A Barton’s fracture is an intra-articular rim fracture of the distal radius. It can be classified as either dorsal or volar. Dorsal rim fractures are more common and result from forced dorsiflexion and pronation. Volar rim fractures often occur with a fall onto a supinated hand/wrist. These forces disrupt the radiocarpal ligaments and subsequent avulsion fracture of the radial rim. In dorsal fractures, the avulsed fragment migrates dorsally. The opposite is true with volar fractures. These fractures are unstable and often present with a dislocation of the carpal bones. [rx][rx]
Greenstick and Buckle/Torus Fractures – Both Torus and greenstick fractures are incomplete fractures. Pediatric bones are poorly mineralized relative to adults and can bend without frankly breaking. These fractures can occur in any long bone but frequently occur in the metaphysis of the distal radius. Torus fractures occur with axial loading whereas Greenstick fractures result from bending forces. Torus fractures are characterized by buckling of the bony cortex and periosteum without any true fracture lines. There is generally minimal deformity with Torus fractures, and the periosteum and cortex are intact. Greenstick fractures will show bony bending. There will be a fracture of the convex surface with an intact concave surface. These fractures are extremely common in children, and unfortunately frequently missed.
Salter-Harris Type Fractures – A Salter-Harris fracture is a pediatric fracture that involves the epiphyseal plate. These fractures can occur in any bone that has a growth plate but frequently occur in the distal radius. The Salter-Harris scheme was first developed by Doctors William Harris and Robert Salter in 1963 and remains the most common classification system for epiphyseal fractures. Salter-Harris fractures are graded I through IX, with I through V being the most frequently used in clinical practice. Type I is a fracture that runs transversely through the growth plate. Type II runs through the growth plate and the metaphysis. Type III involves the growth plate and epiphysis. Type IV is a fracture of metaphysis, epiphysis, and growth plate. Type V is a complete direct compression fracture of the growth plate. Each of these has a different prognosis and management. [rx][rx][rx]
Torus fracture – This is also called a buckle fracture. The topmost layer of bone on one side of the bone is compressed, causing the other side to bend away from the growth plate. This is a stable fracture, meaning that the broken pieces of bone are still in position and have not separated apart (displaced).
Metaphyseal fracture – The fracture is across the upper or lower portion of the shaft of the bone and does not affect the growth plate.
Growth plate fracture – Also called a physical fracture, this fracture occurs at or across the growth plate. In most cases, this type of fracture occurs in the growth plate of the radius near the wrist. Because the growth plate helps determine the future length and shape of the mature bone, this type of fracture requires prompt attention.
Galeazzi Fractures most commonly result from a fall onto an outstretched hand with an extended wrist and hyperpronated forearm. The energy from the radius fracture gets transmitted towards the radioulnar joint leading to dislocation of the DRUJ. These fractures occur with a bimodal distribution, diaphyseal forearm fractures in young males are commonly due to high-energy trauma (e.g., sports injuries, falls from height, motor vehicle collisions) and fractures in aging females are due to low-energy traumas such as falls from ground level.[rx][rx][rx]
Classification System of Galeazzi Fractures
Two classification systems have been proposed when categorizing Galeazzi fractures.
The first classifications were based on the position of the distal radius:
Type I: Dorsal displacement
Type II: Volar displacement
The second classification system is based on Rettig ME and Raskin KB who categorized Galeazzi fractures based on fracture stability. They found stability to be dependent on the distance of the radial fracture from the distal radial articular surface:
Type I:
Fracture occurring distally from the 7.5 cm demarcation (i.e., closer to the wrist)
Associated with significant DRUJ instability in more than 50% of cases
Type II:
Fracture occurring proximally from the 7.5 cm demarcation (i.e., further from the wrist)
Associated with significant DRUJ instability in only around 5% of cases
Causes of Galeazzi Fractures
Sudden forceful fall down
Road traffic accident
Falls – Falling onto an outstretched hand is one of the most common causes of a broken distal radius.
Sports injuries – Many distal radius fractures occur during contact sports or sports in which you might fall onto an outstretched hand — such as in-line skating or snowboarding.
Motor vehicle crashes – Motor vehicle crashes can cause wrist bones to break, sometimes into many pieces, and often require surgical repair.
Have osteoporosis – a disease that weakens your bones
Eave low muscle mass or poor muscle strength – or lack agility and have poor balance (these conditions make you more likely to fall)
Walk or do other activities in the snow or on the ice – or do activities that require a lot of forwarding momenta, such as in-line skating and skiing
Wave an inadequate intake of calcium or vitamin D
Football or soccer, especially on artificial turf
Rugby
Horseback riding
Hockey
Skiing
Snowboarding
In-line skating
Jumping on a trampoline
Symptoms Of Galeazzi Fractures
Common symptoms of a distal radius fractures include:
Severe pain that might worsen when gripping or squeezing or moving your hand or wrist
Deformity of the wrist, causing it to look crooked and bent.
Your wrist is in great pain.
Your wrist, arm, or hand is numb.
Your fingers are pale.
Diagnosis of Galeazzi Fractures
Imaging
If a forearm fracture and dislocation are suspected, radiographs are warranted. An anteroposterior and lateral view will usually identify the injury. An additional oblique view may help better classify the injury. Additional radiographs of the distal wrist and proximal elbow should be obtained with any suspicion of coexistent injury.
If a distal to mid-shaft radial fracture is seen on the radiograph, a close examination of the DRUJ is merited. Signs of DRUJ disruption include:
Widening of the DRUJ on the PA view
Ulnar styloid fracture
Displacement of the ulna dorsally on the lateral view
Radial shortening greater than 5 mm (would need to compare with unaffected limb)
Usually, advanced imaging is not needed for an initial assessment. For pre-operative planning, a CT scan may be used to evaluate for non-union, and magnetic resonance imaging (MRI) can help evaluate for TFCC tears and interosseous membrane disruption.
Treatment / Management of Galeazzi Fractures
All suspected or confirmed Galeazzi fractures will require orthopedist consultation. While awaiting consult, patients should be placed in a sugar-tong splint. In most cases, conservative management is indicated in children while surgical intervention is warranted in adults. Prior reports suggested treatment with closed reduction and immobilization alone, in adults, yielded poor outcomes in greater than 90% of patients.[rx][rx]
Initial Management
Initial management for a presumed fracture includes rest, ice, immobilization, and elevation. In most cases, closed reduction of the radius followed by a reduction of the ulna in the DRUJ should be attempted in the acute setting.
Pediatrics
Children tend to have overall better long-term outcomes compared to adults. The approach is usually conservative with closed reduction and splinting. Above-elbow casting in supination is the preferred immobilization. Irreducible and unstable injuries, as well as variants of the Galeazzi fracture, may require surgical intervention with open reduction and internal fixation (ORIF).
Non-Surgical
Treatment available can be broadly
Get medical help immediately – If you fall on an outstretched arm, get into a car accident or are hit while playing a sport and feel intense pain in your shoulder area, then get medical care immediately. Distal radius fractures cause significant pain in the front part of your shoulder, closer to the base of your neck. You’ll innately know that something is seriously wrong because you won’t be able to lift your arm up. Other symptoms include immediate swelling and/or bruising near the fracture, grinding sounds with arm movements and potential numbness and tingling in the arm/hand.
Apply ice to your fractured clavicle – After you get home from the hospital distal radius fractures (regardless if you had surgery or not), you should apply a bag of crushed ice (or something cold) to your injured in order to reduce the swelling and numb the pain. Ice therapy is effective for acute (recent) injuries that involve swelling because it reduces blood flow by constricting local blood vessels. Apply the crushed ice to your clavicle for 15 minutes three to five times daily until the soreness and inflammation eventually fades away
Lightly exercise after the pain fades – After a couple of weeks when the swelling has subsided and the pain has faded away, remove your arm sling for short periods and carefully move your arm and shoulder in all different directions. Don’t aggravate the distal radius fractures so that it hurts, but gently reintroduce movements to the involved joints and muscles. Start cautiously, maybe starting with light calisthenics and then progress to holding light weights (five-pound weights to start). Your distal radius fractures need to move a little bit during the later phases of the injury to stimulate complete recovery.
Practice stretching and strengthening exercises – of the fingers, elbow, and shoulder if your doctor recommends them.
A splint – which you might use for a few days to a week while the swelling goes down; if a splint is used initially, a cast is usually put on about a week later.
A cast – which you might need for six to eight weeks or longer, depending on how bad the break is (you might need a second cast if the first one gets too loose after the swelling goes away.)
Get a supportive arm sling – Due to their anatomical position, distal radius fractures can’t be cast like a broken limb can. Instead, a supportive arm sling or “figure-eight” splint is typically used for support and comfort, either immediately after the injury if it’s just a hairline fracture or following surgery, if it’s a complicated fracture. A figure-eight splint wraps around both shoulders and the base of your neck in order to support the injured shoulder and keep it positioned up and back. Sometimes a larger swath of material is wrapped around the sling to keep it closer to your body. You’ll need to wear the sling constantly until there is no pain with arm movements, which takes between two to four weeks for children or four to eight weeks for adults.
Get a referral to physical therapy – Once you’ve recovered and able to remove your arm sling splint for good, you’ll likely notice that the muscles surrounding your shoulder and upper chest look smaller and feel weaker. That’s because muscle tissue atrophies without movement. If this occurs, then you’ll need to get a referral for some physical rehabilitation. Rehab can start once you are cleared by your orthopedist, are pain-free, and can perform all the basic arm and shoulder movements. A physiotherapist or athletic trainer can show you specific rehabilitation exercises and stretches to restore your muscle strength, joint movements, and flexibility
Rigid fixation – osteosynthesis with locking plate, hook plate fixation, fixation with a distal radius locking plate, coracoclavicular screws, Knowles pin fixation.
Flexible fixation – simple k wire fixation, tension band wiring, suture anchors, vicryl tape, dacron arterial graft for coracoclavicular ligament reconstruction.
A splint – which you might use for a few days to a week while the swelling goes down; if a splint is used initially, a cast is usually put on about a week later.
A cast – which you might need for six to eight weeks or longer, depending on how bad the break is (you might need a second cast if the first one gets too loose after the swelling goes away.)
Rest Your Hand
Once you’re discharged from the hospital in an arm sling, your top priority is to rest your shoulder and not further inflame the injury. Of course, the arm sling not only provides support, but it also restricts movement, which is why you should keep it on even during sleep. Avoiding the temptation to move your shoulder and arm will help the bone mend quicker and the pain fades away sooner.
Depending on what you do for a living and if the injury is to your dominant side, you may need to take a couple of weeks off work to recuperate.
Healing takes between four to six weeks in younger people and up to 12 weeks in the elderly, but it depends on the severity of the fractured clavicle.
Athletes in good health are typically able to resume their sporting activities within two months of breaking they’re ulnar styloid depending on the severity of the break and the specific sport.
Sleeping on your back (with the sling on) is necessary to keep the pressure off your shoulder and prevent stressing the clavicle injury.
Eat Nutritiously During Your Recovery
All bones and tissues in the body need certain nutrients in order to heal properly and in a timely manner. Eating a nutritious and balanced diet that includes lots of minerals and vitamins is proven to help heal broken bones of all types, including ulnar styloid. Therefore, focus on eating lots of fresh produce (fruits and veggies), whole grains, lean meats, and fish to give your body the building blocks needed to properly repair your clavicle. In addition, drink plenty of purified water, milk, and other dairy-based beverages to augment what you eat.
Broken bones need ample minerals (calcium, phosphorus, magnesium, boron) and protein to become strong and healthy again.
Excellent sources of minerals/protein include dairy products, tofu, beans, broccoli, nuts and seeds, sardines and salmon.
Important vitamins that are needed for bone healing include vitamin C (needed to make collagen), vitamin D (crucial for mineral absorption), and vitamin K (binds calcium to bones and triggers collagen formation).
Conversely, don’t consume food or drink that is known to impair bone/tissue healing, such as alcoholic beverages, sodas, most fast food items and foods made with lots of refined sugars and preservatives.
Physical Therapy
Although there will be some pain, it is important to maintain arm motion to prevent stiffness. Often, patients will begin doing exercises for elbow motion immediately after the injury. After a proximal ulna fracture, it is common to lose some shoulder and arm strength. Once the bone begins to heal, your pain will decrease and your doctor may start gentle shoulder exercises. These exercises will help prevent stiffness and weakness. More strenuous exercises will be started gradually once the fracture is completely healed.
Follow-Up Care
You will need to see your doctor regularly until your fracture heals. During these visits, he or will take x-rays to make sure the bone is healing in a good position. After the bone has healed, you will be able to gradually return to your normal activities.
Breathing Exercise
To elevate breathing problem or remove the lung congestion if needed.
Opioids – Also known as narcotics, these medications are intense pain relievers that should only be used under a doctor’s careful supervision.
Topical Medications – These prescription-strength creams, gels, ointments, patches, and sprays help relieve pain and inflammation through the skin.
NSAIDs – Prescription-strength drugs that reduce both pain and inflammation. Pain medicines and anti-inflammatory drugs help to relieve pain and stiffness, allowing for increased mobility and exercise. There are many common over-the-counter medicines called non-steroidal anti-inflammatory drugs (NSAIDs). They include and Ketorolac, Aceclofenac, naproxen
Glucosamine & Diacerein, Chondroitin sulfate – can be used to tightening the loose tension, cartilage, ligament, and cartilage, ligament regenerate cartilage or inhabit the further degeneration of cartilage, ligament
Corticosteroid- to healing the nerve inflammation and clotted blood in the joints.
Wrist Distal Radius Fracture/A distal radius fracture, commonly known as a wrist fracture, is defined by the involvement of the metaphysis of the distal radius. The fracture may or may not involve the radiocarpal joint, distal radioulnar joint, and/or the distal ulna.[rx] This injury is commonly associated with high-energy mechanisms in younger patients and lower energy mechanisms or falls in older patients.[rx] The fracture results in acute wrist pain and swelling, and if left untreated, it can result in significant morbidity. Treatment can involve both non-operative and operative management and ultimately depends on multiple factors.[rx]
Causes of Wrist Distal Radius Fracture
High-energy injuries may result in significantly displaced or highly comminuted unstable fractures to the distal radius.
Common mechanisms in younger individuals
Falls from height
Motor vehicle accident
Injuries sustained during athletic participation
Simple falls from standing height
Sudden forceful fall down
Road traffic accident
Falls – Falling onto an outstretched hand is one of the most common causes of a broken distal radius.
Sports injuries – Many distal radius fractures occur during contact sports or sports in which you might fall onto an outstretched hand — such as in-line skating or snowboarding.
Motor vehicle crashes – Motor vehicle crashes can cause wrist bones to break, sometimes into many pieces, and often require surgical repair.
Have osteoporosis – a disease that weakens your bones
Eave low muscle mass or poor muscle strength – or lack agility and have poor balance (these conditions make you more likely to fall)
Walk or do other activities in the snow or on the ice – or do activities that require a lot of forwarding momenta, such as in-line skating and skiing
Fracture-dislocation or subluxation of the wrist. The dorsal or volar rim of the distal radius gets displaced with the hand and carpus
Volar involvement is more common
Chauffeur’s fracture
Avulsion fracture of the radial styloid
Die-punch fracture
A depressed fracture of the lunate fossa of the articular surface of the distal radius
Diagnosis of Wrist Distal Radius Fracture
History and Physical
Patients will typically present with variable wrist deformity and displacement of the hand relative to the wrist. The wrist usually swells, with ecchymosis, tenderness, and painful range of motion. The mechanism of injury should be investigated to assist in assessing the energy and level of destruction. It is essential to establish the patient’s functional status before the injury as well as occupational demands as these may aid in determining treatment direction. Document co-existing medical conditions that may affect healing such as osteoporosis, diabetes, and/or tobacco use.
The physical examination should include careful attention to the following
Condition of the surrounding skin and soft tissue
Quality of vascular perfusion and pulses
The integrity of nerve function
Sensory 2-point discrimination
Motor function of intrinsic, thenar, and hypothenar muscles of the hand
Careful attention to median nerve function as acute carpal tunnel syndrome can occur up to 20% of the time[rx]
The integrity of the median nerve requires assessment and documentation
Associated injuries include
Ipsilateral elbow
Ipsilateral shoulder
Distal radial ulnar joint
Radial styloid fracture
Triangular fibrocartilage complex
Scapholunate ligament
Lunotriquetral ligament
Magnetic Resonance Imaging – Diffuse decrease in lunate bone marrow signal on T1-weighted images is a hallmark of the disease. Signal changes on T2-weighted images or short-TI inversion recovery (STIR, which nullifies signal from fat) images vary with progression and extent of osteonecrosis. MRI also assesses the integrity of the articular cartilage.[rx][rx]
Radiography – Normal early in the disease. Findings, when present, depend on the morphological stage and include diffuse lunate sclerosis, cystic changes, articular surface collapse, carpal collapse, mid-carpal and/or radio-carpal secondary arthrosis. Coronal fractures may occur in lunates with a type I morphology.[rx][rx]
Computed Tomography –Is useful for surgical planning. It is also more sensitive than radiography for detecting subtle subchondral fractures, coronal lunate fractures, fragmentation, carpal instability, and the degree of trabecular disruption. Patients are frequently re-staged after CT imaging.[rx]
Nuclear Scintigraphy – Findings are non-specific. It previously found use as an adjunct for diagnosing early-stage disease. It has fallen out of favor since introducing MRI.[rx]
Differential Diagnosis
Radiographs confirm the diagnosis; however, the following must merit consideration:
Associated and contributory injuries should always be in the differential
Pathologic fracture
Associated injuries to the carpus
Treatment of Wrist Distal Radius Fracture
Nonoperative management
Fractures that are non-displaced and within the distal third of the bone can be managed non-operatively with immobilization in a cast.[rx] There is active debate as to whether a long or short arm cast is optimal and whether a thumb spica should be included to immobilize the thumb, but there is no evidence currently to suggest one option is better than the other.
The cast usually needs to remain on for six weeks with repeat radiographs taken at this time to assess for the union. Time to union varies depending on the location of the fracture. The distal-third would be expected to heal within 6-8 weeks, middle-third within 8-12 weeks and proximal third within 12-24 weeks. The relative increase in time to healing while moving from distal to proximal is secondary to the tenuous blood supply and retrograde arterial flow.
Opioids – Also known as narcotics, these medications are intense pain relievers that should only be used under a doctor’s careful supervision.
Topical Medications – These prescription-strength creams, gels, ointments, patches, and sprays help relieve pain and inflammation through the skin.
NSAIDs – Prescription-strength drugs that reduce both pain and inflammation. Pain medicines and anti-inflammatory drugs help to relieve pain and stiffness, allowing for increased mobility and exercise. There are many common over-the-counter medicines called non-steroidal anti-inflammatory drugs (NSAIDs). They include and Ketorolac, Aceclofenac, naproxen
Glucosamine & Diacerein, Chondroitin sulfate – can be used to tightening the loose tension, cartilage, ligament, and cartilage, ligament regenerate cartilage or inhabit the further degeneration of cartilage, ligament
Corticosteroid- to healing the nerve inflammation and clotted blood in the joints.
An intrascaphoid angle greater than 35 degrees (humpback deformity)
A radiolunate angle of more than 15 degrees
Transcaphoid perilunate dislocation
Proximal pole fractures
Comminuted fractures
Non displaced waist fractures in individuals that need to return quickly to work/sport
Nonunion or avascular necrosis
Surgical fixation involves the insertion of a single or multiple screws and can be done percutaneously or via an open procedure. The latter is preferable for non-unions and those fractures that exhibit gross displacement with the former for acute, minimally displaced fractures.
Technique
The positioning of the screw is crucial and should be in the middle third of the central axis of the scaphoid; this provides the most stability, reduces time to union, and improves alignment.
Access to the scaphoid can be via a dorsal or volar approach. The decision is made based on surgeon preference and the location of the fracture. The volar approach uses the interval between flexor carpi radialis and the radial artery and is the optimal approach for waist and distal pole fractures. It has the benefits of allowing exposure of the entire scaphoid and radioscapholunate ligament and is least damaging to the vascular supply. The dorsal approach is preferred for proximal pole fractures but places the vascular supply at greater risk of injury.
Nonunion
Treatment of scaphoid non-union is approachable in a variety of ways.[rx] Early on in its course, open reduction and internal fixation with bone grafting can is an option. Bone graft can be sourced from the distal radius or the iliac crest.
Complications
Median Nerve Neuropathy (Carpal Tunnel Syndrome)[rx]
Most frequent neurologic complication
One percent to 12% of low-energy fractures and up to 30% of high-energy fractures
Treat with acute carpal tunnel release in progressive paresthesias, weakness in thumb opposition if symptoms do not respond to closed reduction, and if they last greater than 24 to 48 hours
Avascular Necrosis of the Lunate/Kienbock’s Disease, also known as avascular necrosis of the lunate, is a condition in which the lunate bone, one of eight small bones in the wrist, loses its blood supply, leading to the death of the bone. The lunate is a central bone in the wrist that is important for proper movement and support of the joint. It works closely with the two forearm bones (radius and ulna) to help the wrist move.
Kienbock disease refers to avascular necrosis of the lunate carpal bone, known as keratomalacia. It was first recognized and described by Austrian radiologist Robert Kienböck in 1910.[rx]
Staging of Kienbock’s Disease
Staging of Kienböck disease is essential for treatment planning and divides into morphological and functional staging.
Morphologic Staging follows the Lichtman Classification, which is based on radiographic and MR imaging findings and has low interobserver variability.[rx][rx][rx]
Stage 1: Normal radiograph, lunate signal intensity changes on MRI.
Stage 2: Lunate sclerosis on radiography with or without fracture lines. The lunate shape is normal.
Stage 3: Collapse of the lunate articular surface.
3A: with preserved carpal alignment and height.
3B: with scaphoid flexion and loss of carpal height.
3C: with an associated coronal fracture
Stage 4: Stage 3B + radio-carpal or mid-carpal arthrosis.
Functional Staging – relies on contrast-enhanced MRI to assess osseous perfusion and the extent of necrosis. It is helpful to guide revascularization techniques during surgery for morphologic stages 2 and 3A. The pre- and post-contrast images are acquired using a T2 fat-suppressed sequence.[rx][rx]
Stage 1: Intense homogeneous contrast enhancement reflects bone marrow ischemia and edema and a viable lunate (corresponds to morphologic stage 1).
Stage 2: Patchy, inhomogeneous enhancement reflects partial necrosis. The remaining viable portion is usually distal.
No consensus is present regarding the primary causative factor of Kienböck disease. It is multifactorial, related to the following variables:
Ulnar negative variance (or ulna minus) – This refers to a disproportionately shortened ulna when compared to the radius. As deduced from the previous section, a shortened ulna results in excessive mechanical stress and repetitive microtrauma exerted on the lunate by the relatively long radius. In some studies, up to 78% of Kienböck cases correlate with this finding.[rx]
Vascular supply to the lunate bone – The lunate receives its blood supply from a variable number of dorsal and volar penetrating arteries that branch off of the dorsal and palmar radiocarpal and intercarpal arches. Intraosseous collaterals are sparse. The lower the number of penetrating arteries (especially volar branches from the radiocarpal palmar arch), the greater the likelihood of developing the disease.[rx][rx]
Lunate morphology – The risk of developing Kienböck disease increases as lunate size decreases, forcing the lunate to carry a larger axial load. The lunate can either have a square/rectangular shape (type II or type III), or a more triangular shape whereby the medial articular facet is absent (type I). The latter has a weaker trabecular pattern and is a risk factor for disease development and progression.[rx]
Radial inclination angle – the radial inclination angle is a measurement of the angle formed between the horizontal and a line drawn from the ulnar tip of the radial articular surface to the tip of the radial styloid. The risk of developing Kienböck disease increases as the radial inclination angle decreases.[rx]
Skeletal variations – The ulna can be shorter than the radius, which may cause issues. Or, the shape of the lunate bone may be irregular.
Trauma – A single incident or multiple incidents may cause this disease.
Other medical conditions – Kienbock’s disease can be found more commonly in people who have medical conditions that affect blood supply, and it is also associated with diseases like lupus, sickle cell anemia and cerebral palsy.
Symptoms of Kienbock’s Disease/Avascular Necrosis of the Lunate
Diagnosis of Kienbock’s Disease/Avascular Necrosis of the Lunate
Kienböck disease is a clinical and imaging diagnosis. Both radiography/computed tomography and magnetic resonance imaging (MRI) is highly specific. However, MRI is the most sensitive and detects radiographically occult cases.
Magnetic Resonance Imaging – Diffuse decrease in lunate bone marrow signal on T1-weighted images is a hallmark of the disease. Signal changes on T2-weighted images or short-TI inversion recovery (STIR, which nullifies signal from fat) images vary with progression and extent of osteonecrosis. MRI also assesses the integrity of the articular cartilage.[rx][rx]
Radiography – Normal early in the disease. Findings, when present, depend on the morphological stage and include diffuse lunate sclerosis, cystic changes, articular surface collapse, carpal collapse, mid-carpal, and/or radio-carpal secondary arthrosis. Coronal fractures may occur in lunates with a type I morphology.[rx][rx]
Computed Tomography – This is useful for surgical planning. It is also more sensitive than radiography for detecting subtle subchondral fractures, coronal lunate fractures, fragmentation, carpal instability, and the degree of trabecular disruption. Patients are frequently re-staged after CT imaging.[rx]
Nuclear Scintigraphy – Findings are non-specific. It previously found use as an adjunct for diagnosing early-stage disease. It has fallen out of favor since introducing MRI.[rx]
Ulnar impaction syndrome – More common with ulnar positive variance and results from repetitive microtrauma to the lunate from a relatively long ulna. Similar to Kienböck disease, ulnar impaction syndrome results in decreased T1-weighted signal coupled with increased T2 signal if hyperemia exists, or decreased T2 signal if the disease has already progressed to lunate sclerosis. The signal changes in Kienböck disease, however, are more diffuse or more severe on the radial side of the lunate. Additionally, ulnar impaction syndrome affects the ulnar head and triquetrum, which are intact in Kienböck patients.[rx][rx].
Lunate intraosseous ganglion – Intraosseous ganglia are true cysts which have low T1 signal and high T2 signal on MRI. Sharp, smooth margins on both MRI and radiography allow distinction from Kienböck disease.[rx]
Bone contusion – It May be difficult to distinguish early-stage Kienböck disease on MRI. A history of recent trauma and concomitant injuries to the wrist/hand, in this case, would aid in making the diagnosis.[rx]
Arthritis – Bone marrow signal changes in inflammatory or degenerative arthritides may mimic those seen in Kienböck disease. Distinguishing features include demographics, clinical presentation, and absence of ulna minus in arthritis.[rx]
Osteoid osteoma – Osteoid osteoma of the carpal bones is rare, and only a few case reports exist in the literature. Clinical presentation and the finding of a lucent nidus within a sclerotic rim on CT differentiate it from Kienböck disease.[rx]
Enostosis/bone island – Has low signal intensity on all sequences, however, it shows preserved bone morphology and the area of “sclerosis” is stellate and interdigitated with the normal trabeculae.[rx]
Treatment of Kienbock’s Disease/Avascular Necrosis of the Lunate
The goal of treating Kienböck disease is pain relief, wrist motion preservation, and preservation of grip strength.[rx]
Treatment of Kienböck disease depends on the stage of the disease and its causative factors. Stage I is always treated with splinting or cast immobilization. Stage II can also be treated with immobilization if necrosis is incomplete. Stages II with complete necrosis, III, and IV require “joint-leveling” surgery possibly coupled with vascular bone grafting or transfer of branches from adjacent arteries. Later stages with lunate collapse and secondary wrist degenerative arthrosis may also require proximal row corpectomy or intercarpal arthrodesis. Radial shortening osteotomy is the most common procedure performed to unload the lunate in cases with coexistent ulnar negative variance. Treatment may improve symptoms and functionality without affecting imaging findings in the advanced stages.[rx][rx][rx] Treatment usually depends on how early the disease is diagnosed. A physical therapist can advise on less painful ways to use the wrist.
Non-surgical options
Resting the wrist – During the early stages, it might be possible to splint and cast the wrist for several months. Resting the wrist increases the chance of restoring blood flow to the lunate bone.
Anti-inflammatory drugs – Ibuprofen, aspirin, and other painkillers may help manage swelling and pain during the early stages.
Cortisone injections – These may help with symptoms. If over-the-counter (OTC) anti-inflammatory medications start to become less effective, the doctor may recommend surgery.
A physical therapist can teach the patient how to use the wrist in a way that is less painful and slows down the progression of the disease.
Surgical procedures
Several different surgical procedures are available for patients with Kienböck’s disease.
The options depend on several factors, including the stage of the disease, the person’s activity level, and their personal goals.
Revascularization – Revascularization involves restoring or increasing the blood supply to the lunate bone. The surgeon removes a portion of bone with all its attached blood vessels from another bone and inserts it into the lunate bone. This is possible during stages 1 and 2, before the bone deteriorates too far. An external fixator may be used to hold the bones stay in place while they heal. An external fixator is a metal device that is attached to the outside of the wrists, with pins that insert into the bone.
Joint leveling – Joint leveling is an option when the two bones of the forearm, the radius, and the ulna, have different lengths. Bone grafts may be applied to lengthen the bone, or a section of bone is removed to shorten it. Joint leveling may stop the disease from progressing by reducing the forces that compress the lunate bone.
Proximal row corpectomy – Proximal row corpectomy (PRC) involves the removal of the lunate bone and the two bones on either side of it. It is an option if the bone is broken into pieces or severely collapsed. If the lunate is severely collapsed or broken into pieces, it can be removed. In this procedure, the two bones on either side of the lunate are also removed. This procedure, called a proximal row corpectomy, will relieve pain while maintaining partial wrist motion.
Joint leveling – If the two bones of the lower arm are not the same length, a joint leveling procedure may be recommended. Bones can be made longer using bone grafts or shortened by removing a section of the bone. This leveling procedure reduces the forces that compress the lunate and often stop the progression of the disease.
Fusion – Fusion can be partial or complete. Partial fusion involves fusing some of the wrist bones together, effectively making one solid bone. This can reduce symptoms of pain and maintain some wrist motion. If the patient has severe arthritis of the wrist, the doctor may recommend fusing all the bones to reduce pain and improve wrist function. Wrist motion will be lost, but the patient will still be able to rotate their forearm.
Implant arthroplasty – The lunate bone is replaced with a prosthetic replica made of a special, durable, pyrolytic carbon material while preserving the normal anatomy of the other bones. This is a relatively new procedure, so the long-term results are not yet known. Some patients may undergo several different procedures during their lifetime.
Metaphyseal core decompression – In this procedure, the surgeon “scrapes off” part of the radius and ulna without actually removing any osseous tissue.[rx]
Capitate-shortening osteotomy – A central bony wedge of the capitate is removed, followed by fusing the two remaining capitate bone segments.[rx]
Total wrist joint replacement – (arthroplasty)[rx]
Prognosis of Avascular Necrosis of the Lunate
Kienbock disease is invariably progressive, and joint destruction occurs within 3-5 years of onset.[rx]
Prognosis depends on:
Functional Staging – The greater the extent of viable bone, the better the prognosis.[rx]
Negative ulnar variance – The greater the negative variance, the more severe the disease and the more likely it is to progress.[rx]
Age at diagnosis – Patients diagnosed at an older age are more likely to have advanced-stage disease and are more likely to progress.[rx]
It is significant to note that the severity of symptoms does not always correlate with the morphologic stage.
Ulna/The ulna is a long bone found in the forearm that stretches from the elbow to the smallest finger, and when in anatomical position, is found on the medial side of the forearm. It runs parallel to the radius, the other long bone in the forearm, and is the bigger and longest (by about an inch) of the two.
Anatomy and Bone Landmarks of Ulna
Proximal ulna
The ulna is a long bone that helps stabilize the antebrachial region from the medial side of the forearm. Its proximal end consists of the following processes (2) and notches (2):
Olecranon: A hook-shaped process, located on the posterior aspect of the proximal ulnar end,
Trochlear notch: A C-shaped notch, located anterior to the olecranon. It articulates with the trochlea of the humerus at the elbow joint.
Coronoid process
Radial notch: The articular facet of the radioulnar joint which can be found on the lateral aspect of its head.
You’re almost ready to test what you’ve learned about the radius and ulna! Discover why exactly anatomy quiz questions are the secret to your success. Cadaveric radius, ulna and humerus with labeled landmarks of the elbow joint
Ulnar shaft
The shaft of the ulna is tapered distally and thicker around the neck and proximal portion. Its lateral side is sharp and gives rise to the interosseous membrane between the two bones of the forearm, hence the name – interosseous border.
From a posterior aspect, the ulna is rounded and smooth and can be palpated subcutaneously for the entire length of the antebrachial region. Just below the coronoid process at the highest point of the shaft, the ulnar tuberosity forms the muscular attachment of the brachialis muscle.
On the lateral side and inferior to the radial notch, the supinator fossa is a concavity that is limited by the supinator crest and holds the originating fibers of the supinator muscle. Just below this muscle attachment, a second, smaller one can be found for the flexor pollicis longus.
Anteriorly, midway down the ulnar bony shaft, there exists a nutrient foramen, which governs bone growth from the time of the seventh intrauterine week up until the eleventh year of life. This is covered by the flexor digitorum profundus muscle which spans the majority of the ulnar shaft.
Posteriorly, on the distal side of the olecranon, the anconeus muscle finds its distal attachment or insertion. The origin for the flexor carpi ulnaris muscles and ulnar head of the supinator muscle are also located on the proximal posterior surface.
Three consecutive muscle attachments can be seen in descending order just below the attachment of the interosseous membrane as it travels down the shaft and they are:
The abductor pollicis longus muscle,
The extensor pollicis longus muscle and
The extensor indicis muscle.
Distal ulna
The distal head of the ulna is comprised of the articular circumference which articulates with the wrist bones and posteriorly, a bony projection known as the styloid process. Just above it on the medial aspect of the bone, the attachment of the pronator quadratus which runs between the radius and the ulna is positioned.
Muscles Attachment of Ulna
The radius and ulna serve as insertion sites for several muscles originating more proximally in the arm[rx][rx]:
Biceps brachii – inserts on the radial tuberosity, a bony prominence on the medial aspect of the proximal end of the radius; allows for flexion and supination of the forearm.
Brachialis – inserts on the coronoid process of the ulna and the ulnar tuberosity; allows for flexion of the forearm.
Triceps and anconeus – insert on the olecranon process of the ulna allowing for the extension of the forearm.
Within the forearm, muscles are classically grouped into anterior and posterior compartments[rx][rx]:
Anterior Compartment:
Flexor carpi radialis, palmaris longus, and the humeral heads of the pronator teres and flexor carpi ulnaris – originate from the common flexor origin. The ulnar head of the pronator teres originates from the coronoid process. The ulnar head of the flexor carpi ulnaris arises from the olecranon. The pronator teres inserts to the lateral surface of the radius and is responsible for pronation and flexion of the forearm. Each of the other muscles inserts in the wrist or hand and is responsible for more distal movements.
Flexor digitorum superficialis – arises from the anterior border of the radius, the medial epicondyle of the humerus, and the coronoid process and inserts on the middle phalanges of the medial four digits.
Flexor digitorum profundus – arises from the ulna and interosseous membrane and inserts on the distal phalanges.
Flexor pollicis longus – originates from the radius and the interosseous membrane and inserts on the distal phalanx of the thumb.
Pronator quadratus – originates from the distal end of the ulna and inserts on the distal end of the radius. Responsible for forearm pronation.
Posterior Compartment
Brachioradialis, extensor carpi radialis longus, extensor carpi radialis brevis, extensor digitorum, extensor digiti minimi, and extensor carpi ulnaris – originate from the distal lateral edge of the humerus. The brachioradialis inserts just proximal to the styloid process of the radius and is responsible for flexion of the forearm, especially in pronation. The remainder of the muscles originating from this area insert distally and are responsible for movements within the wrist and hand.
Supinator – originates from the lateral epicondyle, radial collateral and annular ligaments, supinator fossa and the crest of the ulna with insertion on the lateral side of the radius. It is responsible for forearm supination.
Abductor pollicis longus and extensor pollicis longus – originates from the posterior surface of the ulna and interosseous membrane with attachments in the hand.
Extensor indicis – originates from the posterior surface of the distal third of the ulna and the interosseous membrane with attachment in the hand.
Extensor pollicis brevis – originates from the posterior surface of the distal third of the radius and the interosseous membrane with attachment in the hand.
The following muscles insert into the ulna
Triceps brachii – posterior section of the superior surface of the olecranonAnconeus – olecranonBrachialis – the volar surface of the coronoid process
The following muscles originate from the ulna[rx][rx]:
Pronator teres – the medial surface of the coronoid process
Flexor carpi ulnaris – olecranon process
Flexor digitorum superficialis – coronoid process
Flexor digitorum profundus – anteromedial surface
Pronator quadratus – distal anterior shaft
Extensor carpi ulnaris – posterior border
Supinator – proximal ulna
Abductor pollicis longus – posterior surface
Extensor pollicis longus – dorsal shaft
Extensor indicis – posterior distal shaft
Nerves of Ulna
The nerves of the brachial plexus provide motor and sensory innervation to the antebrachium.
The wrist joint receives innervation from the three major nerves of the forearm.[rx]
Median nerve: Via the anterior interosseous branch
Radial nerve: Via the posterior interosseous branch
Ulnar nerve: Directly through its deep motor branches
The radial nerve provides sensory innervation for the posterior forearm and motor innervation to the brachioradialis, extensor carpi radialis brevis, extensor carpi radialis longus, supinator, extensor carpi ulnaris, abductor pollicis longus, abductor pollicis brevis, extensor pollicis longus, extensor pollicis brevis, extensor indicis, extensor digitorum, and extensor digiti minimi muscles.
The medial and lateral antebrachial cutaneous nerves provide sensory innervation to the anteromedial and anterolateral forearm respectfully.
The musculocutaneous nerve is the source of motor innervation to the biceps brachii.
The median nerve provides motor innervation to the pronator teres, flexor carpi radialis, palmaris longus, flexor digitorum superficialis, flexor pollicis longus, pronator quadratus, and the lateral half of the flexor digitorum profundus muscles.
The ulnar nerve supplies motor innervation to the flexor carpi ulnaris and flexor digitorum profundus muscles.[rx]
Functions of Ulna
Joints
The ulna forms part of the wrist joint and elbow joints. Specifically, the ulna joins (articulates) with:
trochlea of the humerus, at the right side elbow as a hinge joint with the semilunar trochlear notch of the ulna.
the radius, near the elbow as a pivot joint, allows the radius to cross over the ulna in pronation.
the distal radius, where it fits into the ulnar notch.
the radius along its length via the interosseous membrane that forms a syndesmosis joint
Musculotendinous Attachment of Ulna
Anteriorly
Proximal
brachialis: ulnar tuberosity
pronator teres (ulnar head): coronoid process
flexor digitorum superficialis (humeroulnar head): coronoid process
abductor pollicis longus: posterior surface of ulna
extensor pollicis longus: middle third of the posterior surface of ulna
extensor indicis: posterior surface of ulna
Ligamentous
Proximal
medial collateral ligaments of the elbow
anterior band: inferior medial epicondyle to the sublime tubercle
posterior band: medial epicondyle to the medial olecranon
middle band (Transverse or Cooper’s ligament): medial olecranon to the medial coronoid process
anterior and posterior capsular ligaments of the elbow.
Medial
anterior and posterior attachments of the annular ligament
quadrate ligament
oblique cord
interosseous membrane
Distal
triangular fibrocartilage
ulnar collateral ligament of the wrist
Bones of the left forearm. Anterior aspect.
The radius and ulna of the left forearm, posterior surface.
Muscle
Direction
Attachment
Triceps brachii muscle
Insertion
posterior part of the superior surface of Olecranon process (via common tendon)
Anconeus muscle
Insertion
olecranon process (lateral aspect)
Brachialis muscle
Insertion
the anterior surface of the coronoid process of the ulna
Pronator teres muscle
Origin
the medial surface on the middle portion of the coronoid process (also shares an origin with medial epicondyle of the humerus)
Flexor carpi ulnaris muscle
Origin
olecranon process and posterior surface of the ulna (also shares an origin with medial epicondyle of the humerus)
Flexor digitorum superficialis muscle
Origin
coronoid process (also shares an origin with medial epicondyle of the humerus and shaft of the radius)
Flexor digitorum profundus muscle
Origin
the anteromedial surface of the ulna (also shares an origin with the interosseous membrane)
Pronator quadratus muscle
Origin
distal portion of the anterior ulnar shaft
Extensor carpi ulnaris muscle
Origin
the posterior border of ulna (also shares an origin with lateral epicondyle of the humerus)
Supinator muscle
Origin
proximal ulna (also shares an origin with lateral epicondyle of the humerus)
Abductor pollicis longus muscle
Origin
the posterior surface of the ulna (also shares an origin with the posterior surface of the radius bone)
Extensor pollicis longus muscle
Origin
dorsal shaft of the ulna (also shares an origin with the dorsal shaft of the radius and the interosseous membrane)
Extensor indicis muscle
Origin
the posterior surface of the distal ulna (also shares an origin with the interosseous membrane)
Clinical Significance of Ulna
Regardless of the site of the fracture, management should begin with a history and physical followed by plain films of the affected site, and if possible the joint above and below, orthogonal radiographic views of each site are mandatory to appropriately manage each fracture within the guidelines of the standard of care management. Common fractures include[rx]:
Dorsally displaced distal radius fractures (commonly referred to as “Colle fractures”) – One of the most common forearm fractures. It involves a complete transverse fracture of the distal 2 cm of the radius. The distal fragment is displaced posteriorly resulting in the classic “dinner fork” deformity. The etiology is usually a fall on an outstretched hand with concomitant hyperextension. The fracture site can often be comminuted, and avulsion of the ulnar styloid process is also a feature.
Reverse Colles fracture (Smith fracture) – A complete transverse fracture of the distal 2 cm of the radius with anterior displacement of the distal fragment. Usually secondary to a fall on a flexed hand.
Monteggia fracture – A fracture within the proximal third of the ulna with concomitant dislocation of the radial head.[rx]
Galeazzi’s fracture – A fracture of the distal third of the radius with accompanying dislocation of the distal radioulnar joint.
Barton’s fracture – An intraarticular fracture of the distal radius with concomitant dislocation of the radiocarpal joint.[rx]
Essex-Lopresti fracture-dislocation – Fracture of the radial head with dislocation of the distal radioulnar joint and rupture of the interosseous membrane.[rx]
Chauffeur fracture – An intraarticular fracture of the radial styloid process.[rx]
“Both Bone” forearm fractures – descriptive term to describe many different types of patterns involving fractures of the radius and ulnar shaft long bone
Incomplete fracture patterns of the forearm
Isolated ulnar shaft fracture -(greenstick fracture of the ulna)
Isolated “buckle” or “torus” fracture pattern of the radius
Seen in pediatric patients as a manifestation of a pathologic force compromising one cortex of the bone (resulting in compression on one side depending on the direction of the force).
Monteggia fractures most commonly result from a direct blow to the forearm with the elbow extended and forearm in hyperpronation. The energy from the ulnar fracture gets transmitted along the interosseous membrane leading to rupture of the proximal quadrate and annular ligaments, disrupting the radiocapitellar joint. In conjunction with the bimodal distribution, diaphyseal forearm fractures in young males are commonly due to high-energy trauma, for example, falls from height, sports injuries, motor vehicle accidents, and fractures in elderly females are due to low-energy trauma such as a ground-level fall.[rx][rx][rx]
Classification System of Monteggia Fractures
In 1967, Dr. Jose Luis Babo classified Monteggia fractures into four types. These types depend on the direction of the radial head dislocation.[rx]
Type I
The proximal ulna is fractured and radial head dislocation directed anteriorly.
Most common type in children accounting for 70% of cases, 15% of cases in adults.
Mechanism of Injury: (1) direct blow to posterior elbow, (2) hyper-pronated force on an outstretched arm, (3) contracted biceps resists forearm extension causing dislocation and followed by impact leading to ulna fracture.
Type II
Both the ulnar shaft fracture and radial head dislocation are directed posteriorly
Mechanism of Injury: Axial load directed up the forearm with a slightly flexed elbow.
Most common type in adults accounting for approximately 80% of cases.
Associated with an instability of the ulnohumeral joint and high rates of radial head fracture and posterior interosseous nerve injury.
Type III
Ulnar fracture with a radial head dislocation directed laterally.
Mechanism of Injury: Varus force on an extended elbow leads to a greenstick fracture of the ulna.
More frequently seen in children.
Type IV
Fractures of the ulnar and radial shafts with an anterior radial head dislocation
Rarest type and poorly understood mechanism.
Causes of Monteggia Fractures
Mechanisms include:
Fall on an outstretched hand with the forearm in excessive pronation (hyper-pronation injury). The ulna fractures in the proximal one-third of the shaft due to extreme dislocation. Depending on the impact and forces applied in each direction, degree of energy absorption determines pattern, the involvement of the radial head, and whether or not open soft tissue occurs.
Direct blow on the back of the upper forearm would be a very uncommon cause. In this context, isolated ulnar shaft fractures are most commonly seen in defense against blunt trauma (e.g. nightstick injury). Such an isolated ulnar shaft fracture is not a Monteggia fracture. It is called a ‘nightstick fracture’.
Diagnosis of Monteggia Fractures
Exam:
– r/o tear of the annular ligament
– associated nerve injury:
– paralysis of deep branch of the radial nerve is most common;
– the posterior interosseous nerve may be wrapped around the neck of radius, preventing reduction;
– note: that patients whose operative treatment is delayed may be found to have a progressive PIN palsy from
constant pressure exerted by the dislocated radial head;
– spontaneous recovery is usual & exploration is not indicated;
– Radiographs:
– dislocation of radial head may be missed, even though frx of the ulna is obvious (need AP, lateral and oblique X-rays of the elbow)
– a line is drawn thru radial shaft and radial head should align w/ capitalism in any position if the radial head is in normal position
– this is esp true on the lateral projection;
– the apex of angular deformity of ulna usually indicates the direction of radial head dislocation;
– Reduction:
– immobilize forearm in neutral rotation w/ slight supination, w/ cast carefully molded over the lateral side of the ulna at the level of fracture;
– keep elbow flexed ( > 90 deg), to relax biceps so that full supination can be avoided w/o losing reduction;
– Non-Operative Treatment:
– realize that even w/ successful closed reduction of the ulna (and accompanying reduction of the radial head) that subsequently
there may be slow and progressive shortening and angulation;
– hence, these patients will require close follow up;
Treatment of Monteggia Fractures
Nonoperative
closed reduction
indications
more common and successful in children
must ensure stabilty and anatomic alignment of ulna fracture
technique
cast in supination for Bado I and III
Operative
ORIF of ulna shaft fracture
indications
acute fractures which are open or unstable (long oblique)
comminuted fractures
most Monteggia fractures in adults are treated surgically
ORIF of ulna shaft fracture, open reduction of radial head
indications
failure to reduce radial head with ORIF of ulnar shaft only
ensure ulnar reduction is correct
complex injury pattern
IM Nailing of ulna
indications
transverse or short oblique fracture
Delayed Dx:
– when dx is delayed < 3 months, ORIF is indicated;
– when > 3 months has elapsed, consider non-op treatment because bony ankylosis of the elbow may occur following surgery;
– bony ankylosis may be more disabling than the joint instability
– in a child, a dislocated radial head should never be resected, since it will cause cubitus valgus, prominence of the distal end of ulna,
and radial deviation of the head
Pearls and Pitfalls of Technique
Missing pediatric – Monteggia leads to poor results. All “isolated ulna fractures” must be scrutinized for radio capitellar subluxation. Careful weekly radiographic follow-up, for the first 3 weeks after reduction is important to ensure the maintenance of reduction throughout treatment.
Radiographic reading – Radiocapitellar line: The radial neck line should bisect the capitellar ossific nucleus.
Ulnar bow sign: subtle bowing in the direction of the radial head dislocation. The posterior ulnar border should be straight.
Most pediatric Monteggia fractures can be treated via closed means. Comminution, long oblique and very proximal ulna fractures have a higher risk of needing operative fixation.
Residual radiocapitellar instability is almost always a result of residual ulnar deformity.
Adult fractures often involve collateral ligament injury and radial head and coronoid fractures.
The surgeon should be prepared to perform appropriate repairs and replacements.
Osteoporosis must be taken into account when treating adult fractures.The threshold should be low for use of locking plate technology and for replacement instead of repair of the radial head.
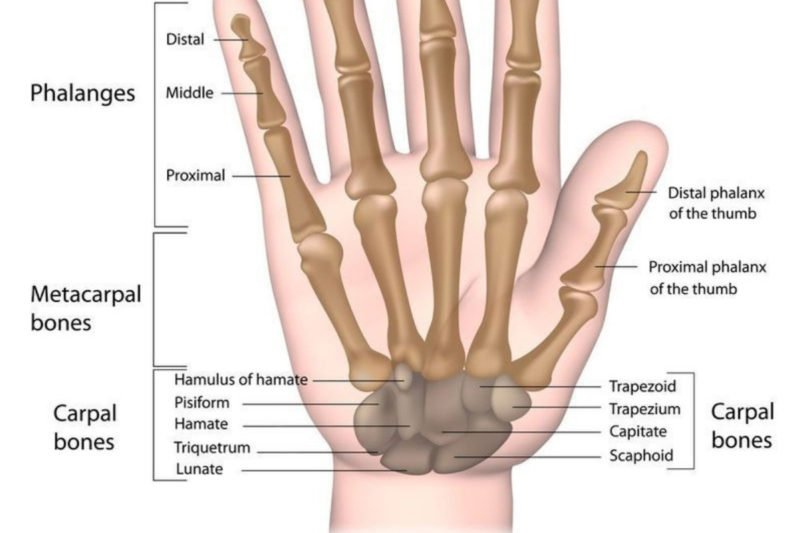
Hamate fractures are rare and underreported. These injuries are usually misdiagnosed or confused with simple wrist sprains. Delayed diagnosis is not uncommon. The hamate is a triangular-shaped bone that forms part of the distal carpal row, articulating with the capitate (radially), triquetrum (proximally), and fifth and fourth metacarpals (distally).
Considering its unique anatomy (Figure 1), hamate fractures usually get subdivided into two broad groups: hook fractures and body fractures.[rx][rx]
Classification of hamate fractures:
Type 1: Hook of the hamate fracture
Type 2: Body of the hamate fracture
2a: Coronal (may be dorsal oblique or splitting fracture)
2b: Transverse fracture
Associated hook fracture injuries:
Ulnar artery injury
Ulnar nerve injury
Associated body fracture Injuries:
Fourth and fifth metacarpal fracture-dislocation
Greater arc perilunate fracture-dislocation
Differential Diagnosis
Ulnar flexor carpi tendinitis and triangular fibrocartilage complex injuries are a common misdiagnosis.[rx] A hamate fracture accompanies a small percentage (1 to 2%) of distal radius fracture.[rx]
Other differential diagnoses include:
Bipartite hamate
Scaphoid fracture
Capitate fracture
Triquetrum fracture
Pisiform fracture
Ligamentous injuries (without fracture)
Carpal bone dislocations
Treatment / Management
Surgical indications: displaced fractures, nonunion, ulnar nerve compression, median nerve compression, ulnar artery compression, tendon rupture and metacarpal subluxation.
Hook fractures:
Acute, nondisplaced: Immobilization, ulnar gutter cast for six weeks. There is still debate whether patients may profit from initial surgical treatment in this type of fractures. Sport players will usually benefit from early surgical management, returning to sports activities in three months.
Acute, displaced: Excision of a bony fragment is the gold standard procedure. Open reduction and internal fixation (screws or Kirschner wires) is another proven treatment. Both alternatives showed similar clinical results.[23]
Chronic pain, nonunion: These signs require fracture pinning with bone grafting.
Residual instability of fourth and/or fifth metacarpals
Nonunion – This is the most likely complication arising from missed scaphoid fractures. The risk is higher in those that are very displaced or have associated carpal fractures. These will generally require operative intervention with screw fixation. There are three stages:
1 – Radioscaphoid arthritis
2 – Scaphocapitate arthritis
3 – Lunocapitate arthritis
Scaphoid nonunion advanced collapse (SNAC) is the end-stage and is managed with wrist fusion or proximal row corpectomy.
Avascular necrosis – The incidence of this is approximately 30-40%. This is most likely to affect the proximal pole
Scapholunate dissociation
Delayed union – typically 90-95% if operatively managed fracture unites, but if there is doubt, CT scan may be needed to confirm union.
Stiff Elbow (Elbow Contracture)/Elbow stiffness is a relatively common condition and represents a significant disability. There are multiple causes of loss of elbow range of motion. Therefore, a proper clinical history is important for therapeutic surgical or non-surgical planning.[rx]
Elbow Joints Injuries are the most common cause of elbow pain. Some people may not recall having had a specific injury, especially if symptoms began gradually or during everyday activities. To better understand elbow injuries, you may want to review the structure and function of the elbow.
Your elbow joint is made up of bone, cartilage, ligaments, and fluid. Muscles and tendons help the elbow joint move. When any of these structures is hurt or diseased, you have elbow problems. Many things can make your elbow hurt. A common cause is a tendinitis, an inflammation or injury to the tendons that attach muscle to bone. Tendinitis of the elbow is a sports injury, often from playing tennis or golf. You may also get tendinitis from the overuse of the elbow. Other causes of elbow pain include sprains and strains, fractures (broken bones), dislocations, bursitis, and arthritis. Treatment depends on the cause.
Types of Elbow Joints Fractures
Sudden (acute) injury
An acute injury may be caused by a direct blow, penetrating injury, or fall or by twisting, jerking, jamming, or bending an elbow abnormally. Pain may be sudden and severe. Bruising and swelling may develop soon after the injury. Acute injuries include:
Bruises from a tear or rupture of small blood vessels under the skin.
Injuries to ligaments, the ropy fibers that connect bones to bones around joints.
Injuries to tendons that connect muscles to bones.
Injuries to joints (sprains) that stretch or tear the ligaments.
Pulled muscles (strains) caused by overstretching muscles.
Muscle tears or ruptures, such as your biceps or triceps in your upper arm.
Broken bones (fractures) of the upper arm bone (humerus) or the forearm bones (ulna or radius) at the elbow joint.
Dislocations of the elbow joint (out of its normal position).
Overuse injuries
Overuse injuries occur when too much stress is placed on a joint or other tissue, often by overdoing an activity or through repetition of an activity. Overuse injuries include:
Bursitis. Swelling behind the elbow may be olecranon bursitis (Popeye elbow).
Tendinosis, which is a series of microtears in the connective tissue in or around the tendon.
Soreness or pain felt on the outside (lateral) part of the elbow may be tennis elbow (lateral epicondylitis). This is the most common type of tendinopathy that affects the elbow and most often is caused by overuse of the forearm muscles. This overuse may occur during sports, such as tennis, swimming, golf, and sports involving throwing; jobs, such as carpentry or plumbing; or daily activities, such as lifting objects or gardening.
Soreness or pain in the inner (medial) part of the elbow may be golfer’s elbow. In children who participate in sports that involve throwing, the same elbow pain may be described as Little Leaguer’s elbow.
Pinched nerves, such as ulnar nerve compression, which is the pinching of the ulnar nerve near the elbow joint. This usually occurs with repeated motions.
Supracondylar Fractures
This type of fracture involves the distal humerus just above the elbow. It is the most common type of elbow fracture and accounts for approximately 60% of all elbow fractures. It is considered an injury of the immature skeleton and occurs in young children between 5 to 10 years of age. Based on the mechanism of injury and the displacement of the distal fragment, professionals classify these as either extension or flexion type fractures.[rx][rx][rx] Beware that a nondisplaced fracture may be subtle and may only be recognized by one of the following:
Posterior fat pad sign
Anterior sail sign
Disruption of the anterior humeral line
Radiographically, these fractures are classified into three types:
Type I – minimal or no displacement
Type II – displaced fracture, posterior cortex intact
Type III – totally displaced fracture, anterior and posterior cortices disrupted
In a flexion type fracture that happens in less than 5% of cases, the elbow is displaced anteriorly. The typical mechanism is when a direct anterior force is applied against a flexed elbow, which causes anterior displacement of the distal fragment. With the displacement of the fragment, the periosteum tears posteriorly. Since the mechanism is a direct force, flexion type fractures are often open.[rx][rx][rx][rx]
Type I fracture – non-displaced or minimally displaced
Type II fractures – incomplete fracture; anterior cortex is intact
Type III fracture – completely displaced; distal fragment migrates proximally and anteriorly
One of the most serious complications is neurovascular injury following the fracture, as the brachial artery and median nerve are located close to the site of the fracture and can be easily compromised.
Gartland Classification
Supracondylar fractures can be classified depending on the degree of displacement:
Gartland Type 1 Fracture – Minimally displaced or occult fracture. The fracture is difficult to see on x-rays. The anterior humeral line still intersects the anterior half of the capitellum. The only visible sign on an x-ray will be a positive fat pad sign.
Gartland Type 2 Fracture – Fracture that is displaced more posteriorly, but the posterior cortex remains intact.
Gartland Type 3 Fracture – Completely displaced fracture with cortical disruption. Posteromedial displacement is more common happening in 75% of cases compared to posterolateral displacement which occurs in 25% of cases.
Lateral Condyle Fractures
These types of fractures are the second most common type of elbow fracture in children and account for 15% to 20% of all elbow fractures. This fracture involves the lateral condyle of the distal humerus, which is the outer bony prominence of the elbow.
The peak age for the occurrence of lateral condyle fractures is four to ten years old. Most commonly, these are Salter-Harris type IV ( a fracture that transects the metaphysis, physis, and epiphysis) involving the lateral condyle.
Two types of classifications are used to describe lateral condyle fractures
Milch classification
Milch 1 – Less common type. Fracture line traverses laterally to the trochlear groove. Elbow is stable.
Milch II – More common type. Fracture passes through the trochlear groove. Elbow is unstable.
Displacement Classification
Type 1 – Displacement of less than 2 mm
Type 2 – more than 2 mm but less than 4 mm displacement. The fragment is close to the humerus
Type 3 – Wide displacement, the articular surface is disrupted.
Medial Epicondyle Fractures
These fractures are the third most common type of elbow fracture in children. It is an extra-articular fracture. It involves a fracture of the medial epicondyle apophysis, which is located on the posteromedial aspect of the elbow. It commonly occurs in early adolescence, between the ages of nine to 14 years of age.
It is more common in boys and occurs during athletic activities such as football, baseball, or gymnastics. The common mechanisms of injury are a posterior elbow dislocation and repeated valgus stress. An example is throwing a baseball repeatedly. One term for this is “little league elbow.”
A common presentation is medial elbow pain, tenderness over the medial epicondyle, and valgus instability.
Radial Head and Neck Fractures
These fractures comprise about 1% to 5% of all pediatric elbow fractures. Most commonly these are Salter-Harris type II fractures that transect the physis and extend into the metaphysis for a short distance. This usually occurs between the ages of nine to ten years.
Olecranon Fractures
Olecranon fractures are uncommon in children. These are mostly associated with radial head and neck fractures.
Causes of Stiff Elbow (Elbow Contracture)
In general, elbow trauma can subdivide into the following categories:
Traumatic injuries
Soft tissue injuries range from mild, superficial soft tissue injuries (e.g., simple contusions, strains, or sprains) to traumatic arthrotomies following gunshot wounds or penetrating lacerations
The osseoligamentous spectrum of injury encompasses fractures, fracture-dislocations, ligamentous injuries, and simple versus complex dislocation patterns
“Simple” referring to no associated fracture accompanying the dislocation
“Complex” refers to an associated fracture accompanying the dislocation
Terrible triad elbow injuries
Elbow dislocation – Typically posterolateral direction with associated LCL complex injury. Elbow dislocation is the two most common dislocated joint after the shoulder – most are posterior dislocations
A radial head/neck fracture
Coronoid fracture
Attritional injuries – Encompasses subacute or chronic presentations following various repetitive motion mechanisms
Often seen in athletes involved in any upper extremity sport-related activity requiring repetitive motions (e.g., overhead throwers/baseball pitchers, tennis)
Manual laborers with analogous occupational repetitive demands
Traumatic injuries
Traumatic injuries range from simple contusions to more complex osseoligamentous fracture-dislocation patterns. The latter is often seen following a fall on an outstretched hand while the forearm is supinated and the elbow is either partially flexed or fully extended
Attritional injuries
Another form of elbow injuries consists of the subacute-to-chronic variety that occurs secondary to repetitive motions, eventually leading to various tendinosis conditions. These can include but are not limited to, lateral epicondylitis (tennis elbow), and chronic partial UCL injuries or strains.[rx][rx]
Pediatric considerations
Elbow trauma in children most commonly occurs via sport or following falls. Moreover, careful attention during the assessment is necessary, given the characteristic sequence of ossification center appearance and fusion, which can make the radiographic assessment rather challenging. Commonly encountered pediatric elbow fractures include (but are not limited to)[rx]
Supracondylar fractures
Most common in children peak ages 5 to 10 years, rarely occurs at greater than 15 years
Extension type (98%) – fall on an outstretched hand with fully extended or hyperextended armType 1: minimal or no displacement type 2: slightly displaced fracture, posterior cortex intact type 3: totally displaced fracture, the posterior cortex is broken.
Flexion type – blow directly to a flexed elbowType 1: minimal or no displacement type 2: slightly displaced fracture, anterior cortex intact type 3: totally displaced fracture, the anterior cortex is broken
Lateral condyle fractures
Medial epicondyle fractures
Radial head and neck fractures – Usually indirect mechanism (such as fall on an outstretched hand), and the radial head being driven into capitellum
Olecranon fractures
Another common elbow injury in children
Subluxated radial head (nursemaid’s elbow)
Accounts for 20% of all upper extremity injuries in children
Peak age 1 to 4 years; occurs more frequently in females than males
Mechanism of injury: sudden longitudinal pull on the forearm with forearm pronated
Signs and Symptoms of Stiff Elbow (Elbow Contracture)
Symptoms include:
The child stops using the arm, which is held in extension (or slightly bent) and palm down.[rx]
Minimal swelling.
All movements are permitted except supination.
Pain on the outer part of the elbow (lateral epicondyle)
Point tenderness over the lateral epicondyle—a prominent part of the bone on the outside of the elbow
Pain from gripping and movements of the wrist, especially wrist extension (e.g. turning a screwdriver) and lifting movements[rx]
Sudden intense pain at the back of the elbow will be felt at the time of injury.
The patient will in most cases be unable to straighten the elbow.
Rapid swelling and bruising may start to appear. Trying to move the elbow will be painful and the back of the elbow will be very tender to touch.
Caused by longitudinal traction with the wrist in pronation, although in a series only 51% of people were reported to have this mechanism, with 22% reporting falls, and patients less than 6 months of age noted to have the injury after rolling over in bed.
Symptoms include pain and tenderness on the inside of the elbow. Bruising and swelling may be present for more severe injuries.
Impact injuries causing damage to the medial ligament usually involves a lateral force (towards the outside) being applied to the forearm, placing the medial (inner) joint under stress.
The patient presents with swelling over the lateral elbow with a limited range of motion, particularly forearm rotation and elbow extension ± elbow effusion and bruising. Pain is increased with passive rotation.
The most reliable clinical sign is point tenderness over the radial head.
Needs careful assessment for nerve and vascular involvement, especially with brachial artery, median and ulnar nerves.
It is important to detect crepitation or a mechanical blockage of motion from displaced fracture fragments. This often requires aspiration of a haemarthrosis with the installation of local anesthetic for pain relief.
If there is significant wrist pain and/or central forearm pain, there may be acute longitudinal radioulnar dissociation with disruption of the distal radioulnar joint.
Overuse injuries of the MCL may also occur. Repetitive motions that place a lot of stress on the inner elbow can cause damage to the ligament. For example, throwers (track and field and ball sports such as baseball) are prone to this injury. Especially if the technique is poor!
Diagnosis of Stiff Elbow (Elbow Contracture)
Physical Examination
The examiner should perform and document relevant findings, including:
Skin integrity
Critical when assessing for the presence of an open fracture and/or traumatic arthrotomy
Presence of swelling or effusion
Comprehensive neurovascular examination
How the patient carries their arm may give clues to the diagnosis.
Bony injuries
Supracondylar fracture
Flexion type
Patient supports injured forearm with other arm and elbow in 90º flexion
Loss of olecranon prominence
Extension type
Patient hold arm at side in S-type configuration
Soft tissue injuries
Elbow dislocations:
Posterior: abnormal prominence of olecranon
Anterior: loss of olecranon prominence
Radial head subluxation
Elbow slightly flexed and forearm pronated resists moving the arm at the elbow
Sensory and motor testing of the Median and Ulnar nerves
Median
Test for sensory function
Two-point discrimination over the tip of the index finger.
Test for motor function
“OK” sign with thumb and index finger and abduction of the thumb (recurrent branch)
Ulnar
Test for sensory function
Two-point discrimination of the little finger
Test for motor function
Abduct index finger against resistance
Compartment Syndrome
Acute compartment syndrome can usually develop over a few hours after a serious injury. Some symptoms of acute compartment syndrome are:
A new persistent deep pain
Pain that seems greater than expected for the severity of the injury
Numbness and tingling in the limb
Swelling, tightness and bruising
Radiological Test
Radiographic studies that are necessary for all patients presenting with varying degrees of elbow trauma include:
Anteroposterior (AP) elbow
Lateral elbow
Oblique views (optional, depending on fracture/injury)
Traction view (optional, can facilitate the assessment of comminuted fracture patterns)
Ipsilateral shoulder to wrist orthogonal views
Especially in the setting of high energy trauma or when exam and evaluation are limited
Fat pad sign
Seen with intra-articular injuries
Normally, anterior fat pad is a narrow radiolucent strip anterior to humerus
The posterior fat pad is normally not visible
Anterior fat pad sign indicates joint effusion/ injury when raised and becomes more perpendicular to the anterior humeral cortex (sail sign)
Posterior fat pad sign indicates effusion/injury
In adults, posterior fat pad sign without other obvious fracture implies radial head fracture
In children, it implies supracondylar fracture
Pediatric Considerations
Fractures in children often occur through unossified cartilage, making radiographic interpretation confusing
A line of mensuration drawn down the anterior surface of the humerus should always bisect the capitellum in lateral view.
If any bony relationship appears questionable on radiographs, obtain a comparison view of uninvolved elbow.
Suspect nonaccidental trauma if history does not tip injury.
Ossification centers: 1 appear: (CRITOE)
Capitellum 3 to 6 months
Radial head 3 to 5 years
Medial (Internal) epicondyle 5 to 7 years
Trochlea 9 to 10 years
Olecranon 9 to 10 years
Lateral Epicondyle
It is essential to do bilateral radiographic imaging in pediatric cases.
A nurse elbow can reduce spontaneously when the patient supinates the arm.
Advanced imaging sequences
Computerized tomography (CT) scans are often a consideration in the setting of comminuted fracture patterns for pre-operative surgical planning. Magnetic resonance imaging (MRI) can be an option in the setting of soft tissue and ligamentous injury evaluation, or when suspecting stress or occult fractures.[rx][rx][rx]
Alert
Based on the complex anatomy of the elbow, a few things require attention:
Neurovascular injuries to numerous structures that pass about the elbow, including anterior interosseous nerve, ulnar and radial nerves, brachial artery
Volkmann ischemic contracture is compartment syndrome of the forearm
Differential Diagnosis
It is important to remember all possible diagnoses including (but not limited to):
Fracture
Dislocation
Sprain
Strain
Ligamentous insufficiencies (e.g., UCL)
Bursitis
Tendinopathic conditions (acute or chronic)
Pediatric differential considerations include
Child abuse
Distal humeral physeal injuries
Nursemaids elbow
Fracture(s)
Avulsions
Monteggia fracture-dislocations
Physeal injuries/reactions
Treatment of Stiff Elbow (Elbow Contracture)
Doctors sometimes recommend very different treatments for both tennis elbow and golfer’s elbow. According to the studies done so far, the following treatments can help:
Rest, ice
Physical therapy when appropriate – Eccentric exercises for lateral epicondylitis
Braces/bandages – These are worn around the elbow or on the forearm to take the strain off the muscles.
Injections – Injections into the elbow with various substances, such as Botox, hyaluronic acid or autologous blood (the body’s own blood).
Extracorporeal shockwave therapy (ESWT) – A device generates shock or pressure waves that are transferred to the tissue through the skin. This is supposed to improve the circulation of blood in the tissue and speed up the healing process.
Laser therapy – The tissue is treated with concentrated beams of light. This is supposed to stimulate the circulation of blood and the body’s cell metabolism.
Stretching and strengthening exercises: Special exercises that stretch and strengthen the muscles of the arm and wrist.
Manual therapy – This includes active and passive exercises, as well as massages.
Ultrasound therapy – The arm is exposed to high-frequency sound waves. This warms the tissue, which improves the circulation of blood.
Transcutaneous electrical nerve stimulation (TENS) – TENS devices transfer electrical impulses to the nervous system through the skin. These are supposed to keep the pain signals from reaching the brain.
Acupuncture – The acupuncture needles are inserted into certain points on the surface of the arm. Here, too, the aim is to minimize the perception of pain.
Cold – The elbow is regularly cooled with ice packs.
Massages –A massage technique called “transverse friction massage” is often used to treat tennis elbow and golfer’s elbow. It is applied to the tendons and the muscles, using the tips of one or two fingers.
Emergency department treatment and procedures
Uncomplicated posterolateral dislocation usually treated with closed reduction. If there is evidence of entrapped medial epicondylar fragment, open reduction may be needed.[rx][rx]
Orthopedic consultation is the standard for all but nondisplaced, stable fractures, which as a rule, can be splinted 24 to 48 hours orthopedic follow-up
Fractures generally requiring orthopedic consultation:
Fractures involving articular surfaces such as capitellum or trochlea
Supracondylar fractures:
ED physician can handle type 1 with 24 to 48 hours orthopedic follow-up
The elbow may be flexed and splinted with a posterior splint
Types 2 and 3 require an immediate orthopedic consult
Reduce these in ED when the fracture is associated with vascular compromise
Anterior dislocation:
Reduce immediately if vascular structures compromised
Then flexed to 90º and place the posterior splint
Posterior dislocation:
Reduce immediately if vascular structures compromised
Then flexed 90º and place posterior splint.
Radial head fracture:
Minimally displaced fractures may need aspiration to remove hemarthrosis: instill bupivacaine and immobilize.
Other types should have an orthopedic consult.
Radial head subluxation
In one continuous motion, supinate and flex elbow while placing slight pressure on the radial head.
Hyper pronation technique is possibly more effective – while grasping the patient’s elbow, the wrist is hyper-pronated until feeling a palpable click.
A palpable click will often accompany the reduction
If the exam suggests fracture, but radiograph is negative, splint and have the patient follow up in 24 to 48 hours for re-evaluation
Medication
Conscious sedation is often necessary to achieve reductions
Painkillers – especially non-steroidal anti-inflammatory drugs (NSAIDs).
Injections – Steroid injections.
Ibuprofen – 600 to 800 mg (pediatric: 5 to 10 mg/kg) PO TID
Naprosyn – 250 to 500 mg (pediatric: 10 to 20 mg/kg) PO BID
Tylenol with codeine – 1 or 2 tabs (pediatric 0.5 to 1 mg/kg codeine) PO: do not exceed acetaminophen 4g/24 hours
Morphine sulfate – 0.1 mg/kg IV
Hydromorphone 5 mg/acetaminophen 300mg
Hydrocodone/acetaminophen – 1 to 2 tabs PO
Attritional injuries management modalities
Most of these injections contain one of the following active ingredients. These include but are not limited to[rx][rx][rx]:
Corticosteroid injection – when applicable
Platelet-rich plasma (PRP) considerations – 2016 study noted efficacy in managing UCL insufficiency
Steroids: reduce inflammation. Studies show that steroid injections can temporarily relieve pain. But there is also evidence that they can disrupt the healing process: People who were first given several steroid injections had more pain after a few months than people who didn’t receive any steroid injections. Frequent steroid injections carry the risk of tissue dying (atrophy), for instance, leaving a visible mark on the elbow.
Hyaluronic acid – A substance made by the body, found in tissue and joints. It is typically used to treat osteoarthritis. One study suggests that hyaluronic acid might be effective in the treatment of tennis elbow. But further research is needed to assess its pros and cons.
Botox – inhibits the sending of signals between the nerve cells. This has a paralyzing effect on the muscles. According to studies done on this so far, Botox can relieve the pain just a little at most. Also, Botox injections can have side effects like partial paralysis in the fingers that can last several weeks.
Autologous blood injections – Blood is taken from a vein in the arm and then injected into the elbow. This blood may be treated in different ways before it is injected. One common form of treatment with autologous blood is called platelet-rich plasma (PRP) therapy. It involves separating the blood into its various elements in a centrifuge. Then a concentrated solution of blood platelets is injected into the elbow. There is no evidence that treatment using autologous blood is effective.
Disposition
Admission Criteria
Vascular injuries, open fracture
Fractures requiring operative reduction or internal fixation.
Admit all patients with extensive swelling or ecchymosis for overnight observation and elevation to monitor for and decrease the risk for compartment syndrome.
Discharge Criteria
Stable fractures or reduced dislocations with none of the above features.
Splint and arrange orthopedic follow-up in 24 to 48 hours
Uncomplicated soft tissue injuries.
It is crucial to recall that prolonged elbow immobilization can cause stiffness to the patient, so the main goal is to get the elbow’s range of movement back as soon as possible.
Surgery
Different surgical approaches are used. Most of them involve detaching parts of the forearm muscles or separating and destroying the nerves that carry the pain signals.
Complications of Stiff Elbow (Elbow Contracture)
Complications of lateral epicondylitis can include recurrence of the injury when normal activity is resumed, rupture of the tendons with repeated steroid injections, and failure to improve conservative treatment.
Neuropraxia – This occurs because of nerve injury. It resolves in three to four months. Nerve injury occurs in 11% of supracondylar fractures. Most commonly injured is the interosseous nerve, followed by the radial, median, and ulnar nerves.[rx][rx]
The anterior interosseous nerve (arising from the median nerve) and may be involved either due to traction or contusion.
The radial nerve may be involved with posteromedial displacement
Median nerve involvement may occur with posterolateral displacement
Ulnar nerve involvement may occur with a flexion type supracondylar fracture. The ulnar nerve is most commonly involved due to posterior displacement of the proximal fragment.
Beware that motor testing can only identify anterior interosseous nerve injury. This testing can be done by flexing at the index finger distal interphalangeal and thumb interphalangeal joints and making the “okay” sign. Inability to do so represents a lack of sensory component in the anterior interosseous nerve.
Vascular injury – Brachial artery injury should always be suspected, particularly if the radial pulse is absent. However, vascular injury may occur even if the hand is pink and well perfused. This may be due to partial transection of a vessel.
Compartment syndrome – this may occur after a supracondylar fracture. Evaluate for the early or impending signs by determining if a radial pulse is absent. This injury results from prolonged ischemia of the forearm. It should be suspected if the following are present:
Inability to open the hand in children
Pain on passive extension of the fingers
Tenderness over the forearm
Absence of a radial pulse
A careful neurovascular examination is therefore important to promptly recognize this serious complication.
Malunion– Fracture malunion can lead to cubitus valgus or cubitus varus deformity (common in supracondylar fracture). A common complication is a loss of the carrying angle, which results in a cubitus varus, or “Gunstock,” deformity.
Nonunion – Lateral condylar fractures are more prone to nonunion. These, therefore, require revision surgery.
Postoperative complications can include the following:
Failing to address concomitant pathology
patients report inferior outcomes and lack of improvement if the primary cause of symptoms is not addressed; patients should be educated regarding the risks and benefits of surgery — the former include but are not limited to infection, blood loss, neurovascular injury, continued pain, stiffness, or continued or worsening overall dysfunction
radial nerve entrapment can be missed or not addressed clinically in up to 5% of patients being managed for lateral epicondylitis
Iatrogenic LUCL injury
occurs iatrogenically with increased risk if the surgical dissection extends beyond the radial head equator
postoperative iatrogenic posterolateral rotatory instability (PLRI) can develop if the extension or LUCL compromise is significant
Iatrogenic neurovascular injury
radial nerve injury
Heterotopic ossification
decrease risk with via copious saline irrigation following decortication and debridement
Elbow Joints Arthritis/The most common type of fracture in the pediatric population is elbow fractures. Most commonly, individuals fall on their outstretched hand. Prompt assessment and management of elbow fractures are critical, as these fractures carry the risk of neurovascular compromise.
Elbow Joints Injuries are the most common cause of elbow pain. Some people may not recall having had a specific injury, especially if symptoms began gradually or during everyday activities. To better understand elbow injuries, you may want to review the structure and function of the elbow.
Your elbow joint is made up of bone, cartilage, ligaments, and fluid. Muscles and tendons help the elbow joint move. When any of these structures is hurt or diseased, you have elbow problems. Many things can make your elbow hurt. A common cause is a tendinitis, an inflammation or injury to the tendons that attach muscle to bone. Tendinitis of the elbow is a sports injury, often from playing tennis or golf. You may also get tendinitis from the overuse of the elbow. Other causes of elbow pain include sprains and strains, fractures (broken bones), dislocations, bursitis, and arthritis. Treatment depends on the cause.
Types of Elbow Joints Fractures
Sudden (acute) injury
An acute injury may be caused by a direct blow, penetrating injury, or fall or by twisting, jerking, jamming, or bending an elbow abnormally. Pain may be sudden and severe. Bruising and swelling may develop soon after the injury. Acute injuries include:
Bruises from a tear or rupture of small blood vessels under the skin.
Injuries to ligaments, the ropy fibers that connect bones to bones around joints.
Injuries to tendons that connect muscles to bones.
Injuries to joints (sprains) that stretch or tear the ligaments.
Pulled muscles (strains) caused by overstretching muscles.
Muscle tears or ruptures, such as your biceps or triceps in your upper arm.
Broken bones (fractures) of the upper arm bone (humerus) or the forearm bones (ulna or radius) at the elbow joint.
Dislocations of the elbow joint (out of its normal position).
Overuse injuries
Overuse injuries occur when too much stress is placed on a joint or other tissue, often by overdoing an activity or through repetition of an activity. Overuse injuries include:
Bursitis. Swelling behind the elbow may be olecranon bursitis (Popeye elbow).
Tendinosis, which is a series of microtears in the connective tissue in or around the tendon.
Soreness or pain felt on the outside (lateral) part of the elbow may be tennis elbow (lateral epicondylitis). This is the most common type of tendinopathy that affects the elbow and most often is caused by overuse of the forearm muscles. This overuse may occur during sports, such as tennis, swimming, golf, and sports involving throwing; jobs, such as carpentry or plumbing; or daily activities, such as lifting objects or gardening.
Soreness or pain in the inner (medial) part of the elbow may be golfer’s elbow. In children who participate in sports that involve throwing, the same elbow pain may be described as Little Leaguer’s elbow.
Pinched nerves, such as ulnar nerve compression, which is the pinching of the ulnar nerve near the elbow joint. This usually occurs with repeated motions.
Supracondylar Fractures
This type of fracture involves the distal humerus just above the elbow. It is the most common type of elbow fracture and accounts for approximately 60% of all elbow fractures. It is considered an injury of the immature skeleton and occurs in young children between 5 to 10 years of age. Based on the mechanism of injury and the displacement of the distal fragment, professionals classify these as either extension or flexion type fractures.[rx][rx][rx] Beware that a nondisplaced fracture may be subtle and may only be recognized by one of the following:
Posterior fat pad sign
Anterior sail sign
Disruption of the anterior humeral line
Radiographically, these fractures are classified into three types:
Type I – minimal or no displacement
Type II – displaced fracture, posterior cortex intact
Type III – totally displaced fracture, anterior and posterior cortices disrupted
In a flexion type fracture that happens in less than 5% of cases, the elbow is displaced anteriorly. The typical mechanism is when a direct anterior force is applied against a flexed elbow, which causes anterior displacement of the distal fragment. With the displacement of the fragment, the periosteum tears posteriorly. Since the mechanism is a direct force, flexion type fractures are often open.[rx][rx][rx][rx]
Type I fracture – non-displaced or minimally displaced
Type II fractures – incomplete fracture; anterior cortex is intact
Type III fracture – completely displaced; distal fragment migrates proximally and anteriorly
One of the most serious complications is neurovascular injury following the fracture, as the brachial artery and median nerve are located close to the site of the fracture and can be easily compromised.
Gartland Classification
Supracondylar fractures can be classified depending on the degree of displacement:
Gartland Type 1 Fracture – Minimally displaced or occult fracture. The fracture is difficult to see on x-rays. The anterior humeral line still intersects the anterior half of the capitellum. The only visible sign on an x-ray will be a positive fat pad sign.
Gartland Type 2 Fracture – Fracture that is displaced more posteriorly, but the posterior cortex remains intact.
Gartland Type 3 Fracture – Completely displaced fracture with cortical disruption. Posteromedial displacement is more common happening in 75% of cases compared to posterolateral displacement which occurs in 25% of cases.
Lateral Condyle Fractures
These types of fractures are the second most common type of elbow fracture in children and account for 15% to 20% of all elbow fractures. This fracture involves the lateral condyle of the distal humerus, which is the outer bony prominence of the elbow.
The peak age for the occurrence of lateral condyle fractures is four to ten years old. Most commonly, these are Salter-Harris type IV ( a fracture that transects the metaphysis, physis, and epiphysis) involving the lateral condyle.
Two types of classifications are used to describe lateral condyle fractures
Milch classification
Milch 1 – Less common type. Fracture line traverses laterally to the trochlear groove. Elbow is stable.
Milch II – More common type. Fracture passes through the trochlear groove. Elbow is unstable.
Displacement Classification
Type 1 – Displacement of less than 2 mm
Type 2 – more than 2 mm but less than 4 mm displacement. The fragment is close to the humerus
Type 3 – Wide displacement, the articular surface is disrupted.
Medial Epicondyle Fractures
These fractures are the third most common type of elbow fracture in children. It is an extra-articular fracture. It involves a fracture of the medial epicondyle apophysis, which is located on the posteromedial aspect of the elbow. It commonly occurs in early adolescence, between the ages of nine to 14 years of age.
It is more common in boys and occurs during athletic activities such as football, baseball, or gymnastics. The common mechanisms of injury are a posterior elbow dislocation and repeated valgus stress. An example is throwing a baseball repeatedly. One term for this is “little league elbow.”
A common presentation is medial elbow pain, tenderness over the medial epicondyle, and valgus instability.
Radial Head and Neck Fractures
These fractures comprise about 1% to 5% of all pediatric elbow fractures. Most commonly these are Salter-Harris type II fractures that transect the physis and extend into the metaphysis for a short distance. This usually occurs between the ages of nine to ten years.
Olecranon Fractures
Olecranon fractures are uncommon in children. These are mostly associated with radial head and neck fractures.
Causes of Elbow Joints Arthritis
In general, elbow trauma can subdivide into the following categories:
Traumatic injuries
Soft tissue injuries range from mild, superficial soft tissue injuries (e.g., simple contusions, strains, or sprains) to traumatic arthrotomies following gunshot wounds or penetrating lacerations
The osseoligamentous spectrum of injury encompasses fractures, fracture-dislocations, ligamentous injuries, and simple versus complex dislocation patterns
“Simple” referring to no associated fracture accompanying the dislocation
“Complex” refers to an associated fracture accompanying the dislocation
Terrible triad elbow injuries
Elbow dislocation – Typically posterolateral direction with associated LCL complex injury. Elbow dislocation is the two most common dislocated joint after the shoulder – most are posterior dislocations
A radial head/neck fracture
Coronoid fracture
Attritional injuries – Encompasses subacute or chronic presentations following various repetitive motion mechanisms
Often seen in athletes involved in any upper extremity sport-related activity requiring repetitive motions (e.g., overhead throwers/baseball pitchers, tennis)
Manual laborers with analogous occupational repetitive demands
Traumatic injuries
Traumatic injuries range from simple contusions to more complex osseoligamentous fracture-dislocation patterns. The latter is often seen following a fall on an outstretched hand while the forearm is supinated and the elbow is either partially flexed or fully extended
Attritional injuries
Another form of elbow injuries consists of the subacute-to-chronic variety that occurs secondary to repetitive motions, eventually leading to various tendinosis conditions. These can include but are not limited to, lateral epicondylitis (tennis elbow), and chronic partial UCL injuries or strains.[rx][rx]
Pediatric considerations
Elbow trauma in children most commonly occurs via sport or following falls. Moreover, careful attention during the assessment is necessary, given the characteristic sequence of ossification center appearance and fusion, which can make the radiographic assessment rather challenging. Commonly encountered pediatric elbow fractures include (but are not limited to)[rx]
Supracondylar fractures
Most common in children peak ages 5 to 10 years, rarely occurs at greater than 15 years
Extension type (98%) – fall on an outstretched hand with fully extended or hyperextended armType 1: minimal or no displacement type 2: slightly displaced fracture, posterior cortex intact type 3: totally displaced fracture, the posterior cortex is broken.
Flexion type – blow directly to a flexed elbowType 1: minimal or no displacement type 2: slightly displaced fracture, anterior cortex intact type 3: totally displaced fracture, the anterior cortex is broken
Lateral condyle fractures
Medial epicondyle fractures
Radial head and neck fractures – Usually indirect mechanism (such as fall on an outstretched hand), and the radial head being driven into capitellum
Olecranon fractures
Another common elbow injury in children
Subluxated radial head (nursemaid’s elbow)
Accounts for 20% of all upper extremity injuries in children
Peak age 1 to 4 years; occurs more frequently in females than males
Mechanism of injury: sudden longitudinal pull on the forearm with forearm pronated
Signs and Symptoms of Elbow Joints Arthritis
Symptoms include:
The child stops using the arm, which is held in extension (or slightly bent) and palm down.[rx]
Minimal swelling.
All movements are permitted except supination.
Pain on the outer part of the elbow (lateral epicondyle)
Point tenderness over the lateral epicondyle—a prominent part of the bone on the outside of the elbow
Pain from gripping and movements of the wrist, especially wrist extension (e.g. turning a screwdriver) and lifting movements[rx]
Sudden intense pain at the back of the elbow will be felt at the time of injury.
The patient will in most cases be unable to straighten the elbow.
Rapid swelling and bruising may start to appear. Trying to move the elbow will be painful and the back of the elbow will be very tender to touch.
Caused by longitudinal traction with the wrist in pronation, although in a series only 51% of people were reported to have this mechanism, with 22% reporting falls, and patients less than 6 months of age noted to have the injury after rolling over in bed.
Symptoms include pain and tenderness on the inside of the elbow. Bruising and swelling may be present for more severe injuries.
Impact injuries causing damage to the medial ligament usually involves a lateral force (towards the outside) being applied to the forearm, placing the medial (inner) joint under stress.
The patient presents with swelling over the lateral elbow with a limited range of motion, particularly forearm rotation and elbow extension ± elbow effusion and bruising. Pain is increased with passive rotation.
The most reliable clinical sign is point tenderness over the radial head.
Needs careful assessment for nerve and vascular involvement, especially with brachial artery, median and ulnar nerves.
It is important to detect crepitation or a mechanical blockage of motion from displaced fracture fragments. This often requires aspiration of a haemarthrosis with the installation of local anesthetic for pain relief.
If there is significant wrist pain and/or central forearm pain, there may be acute longitudinal radioulnar dissociation with disruption of the distal radioulnar joint.
Overuse injuries of the MCL may also occur. Repetitive motions that place a lot of stress on the inner elbow can cause damage to the ligament. For example, throwers (track and field and ball sports such as baseball) are prone to this injury. Especially if the technique is poor!
Diagnosis of Elbow Joints Arthritis
Physical Examination
The examiner should perform and document relevant findings, including:
Skin integrity
Critical when assessing for the presence of an open fracture and/or traumatic arthrotomy
Presence of swelling or effusion
Comprehensive neurovascular examination
How the patient carries their arm may give clues to the diagnosis.
Bony injuries
Supracondylar fracture
Flexion type
Patient supports injured forearm with other arm and elbow in 90º flexion
Loss of olecranon prominence
Extension type
Patient hold arm at side in S-type configuration
Soft tissue injuries
Elbow dislocations:
Posterior: abnormal prominence of olecranon
Anterior: loss of olecranon prominence
Radial head subluxation
Elbow slightly flexed and forearm pronated resists moving the arm at the elbow
Sensory and motor testing of the Median and Ulnar nerves
Median
Test for sensory function
Two-point discrimination over the tip of the index finger.
Test for motor function
“OK” sign with thumb and index finger and abduction of the thumb (recurrent branch)
Ulnar
Test for sensory function
Two-point discrimination of the little finger
Test for motor function
Abduct index finger against resistance
Compartment Syndrome
Acute compartment syndrome can usually develop over a few hours after a serious injury. Some symptoms of acute compartment syndrome are:
A new persistent deep pain
Pain that seems greater than expected for the severity of the injury
Numbness and tingling in the limb
Swelling, tightness and bruising
Radiological Test
Radiographic studies that are necessary for all patients presenting with varying degrees of elbow trauma include:
Anteroposterior (AP) elbow
Lateral elbow
Oblique views (optional, depending on fracture/injury)
Traction view (optional, can facilitate the assessment of comminuted fracture patterns)
Ipsilateral shoulder to wrist orthogonal views
Especially in the setting of high energy trauma or when exam and evaluation are limited
Fat pad sign
Seen with intra-articular injuries
Normally, anterior fat pad is a narrow radiolucent strip anterior to humerus
The posterior fat pad is normally not visible
Anterior fat pad sign indicates joint effusion/ injury when raised and becomes more perpendicular to the anterior humeral cortex (sail sign)
Posterior fat pad sign indicates effusion/injury
In adults, posterior fat pad sign without other obvious fracture implies radial head fracture
In children, it implies supracondylar fracture
Pediatric Considerations
Fractures in children often occur through unossified cartilage, making radiographic interpretation confusing
A line of mensuration drawn down the anterior surface of the humerus should always bisect the capitellum in lateral view.
If any bony relationship appears questionable on radiographs, obtain a comparison view of uninvolved elbow.
Suspect nonaccidental trauma if history does not tip injury.
Ossification centers: 1 appear: (CRITOE)
Capitellum 3 to 6 months
Radial head 3 to 5 years
Medial (Internal) epicondyle 5 to 7 years
Trochlea 9 to 10 years
Olecranon 9 to 10 years
Lateral Epicondyle
It is essential to do bilateral radiographic imaging in pediatric cases.
A nurse elbow can reduce spontaneously when the patient supinates the arm.
Advanced imaging sequences
Computerized tomography (CT) scans are often a consideration in the setting of comminuted fracture patterns for pre-operative surgical planning. Magnetic resonance imaging (MRI) can be an option in the setting of soft tissue and ligamentous injury evaluation, or when suspecting stress or occult fractures.[rx][rx][rx]
Alert
Based on the complex anatomy of the elbow, a few things require attention:
Neurovascular injuries to numerous structures that pass about the elbow, including anterior interosseous nerve, ulnar and radial nerves, brachial artery
Volkmann ischemic contracture is compartment syndrome of the forearm
Differential Diagnosis
It is important to remember all possible diagnoses including (but not limited to):
Fracture
Dislocation
Sprain
Strain
Ligamentous insufficiencies (e.g., UCL)
Bursitis
Tendinopathic conditions (acute or chronic)
Pediatric differential considerations include
Child abuse
Distal humeral physeal injuries
Nursemaids elbow
Fracture(s)
Avulsions
Monteggia fracture-dislocations
Physeal injuries/reactions
Treatment of Elbow Joints Arthritis
Doctors sometimes recommend very different treatments for both tennis elbow and golfer’s elbow. According to the studies done so far, the following treatments can help:
Rest, ice
Physical therapy when appropriate – Eccentric exercises for lateral epicondylitis
Braces/bandages – These are worn around the elbow or on the forearm to take the strain off the muscles.
Injections – Injections into the elbow with various substances, such as Botox, hyaluronic acid or autologous blood (the body’s own blood).
Extracorporeal shockwave therapy (ESWT) – A device generates shock or pressure waves that are transferred to the tissue through the skin. This is supposed to improve the circulation of blood in the tissue and speed up the healing process.
Laser therapy – The tissue is treated with concentrated beams of light. This is supposed to stimulate the circulation of blood and the body’s cell metabolism.
Stretching and strengthening exercises: Special exercises that stretch and strengthen the muscles of the arm and wrist.
Manual therapy – This includes active and passive exercises, as well as massages.
Ultrasound therapy – The arm is exposed to high-frequency sound waves. This warms the tissue, which improves the circulation of blood.
Transcutaneous electrical nerve stimulation (TENS) – TENS devices transfer electrical impulses to the nervous system through the skin. These are supposed to keep the pain signals from reaching the brain.
Acupuncture – The acupuncture needles are inserted into certain points on the surface of the arm. Here, too, the aim is to minimize the perception of pain.
Cold – The elbow is regularly cooled with ice packs.
Massages –A massage technique called “transverse friction massage” is often used to treat tennis elbow and golfer’s elbow. It is applied to the tendons and the muscles, using the tips of one or two fingers.
Emergency department treatment and procedures
Uncomplicated posterolateral dislocation usually treated with closed reduction. If there is evidence of entrapped medial epicondylar fragment, open reduction may be needed.[rx][rx]
Orthopedic consultation is the standard for all but nondisplaced, stable fractures, which as a rule, can be splinted 24 to 48 hours orthopedic follow-up
Fractures generally requiring orthopedic consultation:
Fractures involving articular surfaces such as capitellum or trochlea
Supracondylar fractures:
ED physician can handle type 1 with 24 to 48 hours orthopedic follow-up
The elbow may be flexed and splinted with a posterior splint
Types 2 and 3 require an immediate orthopedic consult
Reduce these in ED when the fracture is associated with vascular compromise
Anterior dislocation:
Reduce immediately if vascular structures compromised
Then flexed to 90º and place the posterior splint
Posterior dislocation:
Reduce immediately if vascular structures compromised
Then flexed 90º and place posterior splint.
Radial head fracture:
Minimally displaced fractures may need aspiration to remove hemarthrosis: instill bupivacaine and immobilize.
Other types should have an orthopedic consult.
Radial head subluxation
In one continuous motion, supinate and flex elbow while placing slight pressure on the radial head.
Hyper pronation technique is possibly more effective – while grasping the patient’s elbow, the wrist is hyper-pronated until feeling a palpable click.
A palpable click will often accompany the reduction
If the exam suggests fracture, but radiograph is negative, splint and have the patient follow up in 24 to 48 hours for re-evaluation
Medication
Conscious sedation is often necessary to achieve reductions
Painkillers – especially non-steroidal anti-inflammatory drugs (NSAIDs).
Injections – Steroid injections.
Ibuprofen – 600 to 800 mg (pediatric: 5 to 10 mg/kg) PO TID
Naprosyn – 250 to 500 mg (pediatric: 10 to 20 mg/kg) PO BID
Tylenol with codeine – 1 or 2 tabs (pediatric 0.5 to 1 mg/kg codeine) PO: do not exceed acetaminophen 4g/24 hours
Morphine sulfate – 0.1 mg/kg IV
Hydromorphone 5 mg/acetaminophen 300mg
Hydrocodone/acetaminophen – 1 to 2 tabs PO
Attritional injuries management modalities
Most of these injections contain one of the following active ingredients. These include but are not limited to[rx][rx][rx]:
Corticosteroid injection – when applicable
Platelet-rich plasma (PRP) considerations – 2016 study noted efficacy in managing UCL insufficiency
Steroids: reduce inflammation. Studies show that steroid injections can temporarily relieve pain. But there is also evidence that they can disrupt the healing process: People who were first given several steroid injections had more pain after a few months than people who didn’t receive any steroid injections. Frequent steroid injections carry the risk of tissue dying (atrophy), for instance, leaving a visible mark on the elbow.
Hyaluronic acid – A substance made by the body, found in tissue and joints. It is typically used to treat osteoarthritis. One study suggests that hyaluronic acid might be effective in the treatment of tennis elbow. But further research is needed to assess its pros and cons.
Botox – inhibits the sending of signals between the nerve cells. This has a paralyzing effect on the muscles. According to studies done on this so far, Botox can relieve the pain just a little at most. Also, Botox injections can have side effects like partial paralysis in the fingers that can last several weeks.
Autologous blood injections – Blood is taken from a vein in the arm and then injected into the elbow. This blood may be treated in different ways before it is injected. One common form of treatment with autologous blood is called platelet-rich plasma (PRP) therapy. It involves separating the blood into its various elements in a centrifuge. Then a concentrated solution of blood platelets is injected into the elbow. There is no evidence that treatment using autologous blood is effective.
Disposition
Admission Criteria
Vascular injuries, open fracture
Fractures requiring operative reduction or internal fixation.
Admit all patients with extensive swelling or ecchymosis for overnight observation and elevation to monitor for and decrease the risk for compartment syndrome.
Discharge Criteria
Stable fractures or reduced dislocations with none of the above features.
Splint and arrange orthopedic follow-up in 24 to 48 hours
Uncomplicated soft tissue injuries.
It is crucial to recall that prolonged elbow immobilization can cause stiffness to the patient, so the main goal is to get the elbow’s range of movement back as soon as possible.
Surgery
Different surgical approaches are used. Most of them involve detaching parts of the forearm muscles or separating and destroying the nerves that carry the pain signals.
Complications of Elbow Joints Arthritis
Complications of lateral epicondylitis can include recurrence of the injury when normal activity is resumed, rupture of the tendons with repeated steroid injections, and failure to improve conservative treatment.
Neuropraxia – This occurs because of nerve injury. It resolves in three to four months. Nerve injury occurs in 11% of supracondylar fractures. Most commonly injured is the interosseous nerve, followed by the radial, median, and ulnar nerves.[rx][rx]
The anterior interosseous nerve (arising from the median nerve) and may be involved either due to traction or contusion.
The radial nerve may be involved with posteromedial displacement
Median nerve involvement may occur with posterolateral displacement
Ulnar nerve involvement may occur with a flexion type supracondylar fracture. The ulnar nerve is most commonly involved due to posterior displacement of the proximal fragment.
Beware that motor testing can only identify anterior interosseous nerve injury. This testing can be done by flexing at the index finger distal interphalangeal and thumb interphalangeal joints and making the “okay” sign. Inability to do so represents a lack of sensory component in the anterior interosseous nerve.
Vascular injury – Brachial artery injury should always be suspected, particularly if the radial pulse is absent. However, vascular injury may occur even if the hand is pink and well perfused. This may be due to partial transection of a vessel.
Compartment syndrome – this may occur after a supracondylar fracture. Evaluate for the early or impending signs by determining if a radial pulse is absent. This injury results from prolonged ischemia of the forearm. It should be suspected if the following are present:
Inability to open the hand in children
Pain on passive extension of the fingers
Tenderness over the forearm
Absence of a radial pulse
A careful neurovascular examination is therefore important to promptly recognize this serious complication.
Malunion– Fracture malunion can lead to cubitus valgus or cubitus varus deformity (common in supracondylar fracture). A common complication is a loss of the carrying angle, which results in a cubitus varus, or “Gunstock,” deformity.
Nonunion – Lateral condylar fractures are more prone to nonunion. These, therefore, require revision surgery.
Postoperative complications can include the following:
Failing to address concomitant pathology
patients report inferior outcomes and lack of improvement if the primary cause of symptoms is not addressed; patients should be educated regarding the risks and benefits of surgery — the former include but are not limited to infection, blood loss, neurovascular injury, continued pain, stiffness, or continued or worsening overall dysfunction
radial nerve entrapment can be missed or not addressed clinically in up to 5% of patients being managed for lateral epicondylitis
Iatrogenic LUCL injury
occurs iatrogenically with increased risk if the surgical dissection extends beyond the radial head equator
postoperative iatrogenic posterolateral rotatory instability (PLRI) can develop if the extension or LUCL compromise is significant
Iatrogenic neurovascular injury
radial nerve injury
Heterotopic ossification
decrease risk with via copious saline irrigation following decortication and debridement
Elbow Joints Fractures/The most common type of fracture in the pediatric population is elbow fractures. Most commonly, individuals fall on their outstretched hand. Prompt assessment and management of elbow fractures are critical, as these fractures carry the risk of neurovascular compromise.
Elbow Joints Injuries are the most common cause of elbow pain. Some people may not recall having had a specific injury, especially if symptoms began gradually or during everyday activities. To better understand elbow injuries, you may want to review the structure and function of the elbow. See a picture of the elbow.
Your elbow joint is made up of bone, cartilage, ligaments, and fluid. Muscles and tendons help the elbow joint move. When any of these structures is hurt or diseased, you have elbow problems. Many things can make your elbow hurt. A common cause is a tendinitis, an inflammation or injury to the tendons that attach muscle to bone. Tendinitis of the elbow is a sports injury, often from playing tennis or golf. You may also get tendinitis from the overuse of the elbow. Other causes of elbow pain include sprains and strains, fractures (broken bones), dislocations, bursitis, and arthritis. Treatment depends on the cause.
Types of Elbow Joints Fractures
Sudden (acute) injury
An acute injury may be caused by a direct blow, penetrating injury, or fall or by twisting, jerking, jamming, or bending an elbow abnormally. Pain may be sudden and severe. Bruising and swelling may develop soon after the injury. Acute injuries include:
Bruises from a tear or rupture of small blood vessels under the skin.
Injuries to ligaments, the ropy fibers that connect bones to bones around joints.
Injuries to tendons that connect muscles to bones.
Injuries to joints (sprains) that stretch or tear the ligaments.
Pulled muscles (strains) caused by overstretching muscles.
Muscle tears or ruptures, such as your biceps or triceps in your upper arm.
Broken bones (fractures) of the upper arm bone (humerus) or the forearm bones (ulna or radius) at the elbow joint.
Dislocations of the elbow joint (out of its normal position).
Overuse injuries
Overuse injuries occur when too much stress is placed on a joint or other tissue, often by overdoing an activity or through repetition of an activity. Overuse injuries include:
Bursitis. Swelling behind the elbow may be olecranon bursitis (Popeye elbow).
Tendinosis, which is a series of microtears in the connective tissue in or around the tendon.
Soreness or pain felt on the outside (lateral) part of the elbow may be tennis elbow (lateral epicondylitis). This is the most common type of tendinopathy that affects the elbow and most often is caused by overuse of the forearm muscles. This overuse may occur during sports, such as tennis, swimming, golf, and sports involving throwing; jobs, such as carpentry or plumbing; or daily activities, such as lifting objects or gardening.
Soreness or pain in the inner (medial) part of the elbow may be golfer’s elbow. In children who participate in sports that involve throwing, the same elbow pain may be described as Little Leaguer’s elbow.
Pinched nerves, such as ulnar nerve compression, which is the pinching of the ulnar nerve near the elbow joint. This usually occurs with repeated motions.
Supracondylar Fractures
This type of fracture involves the distal humerus just above the elbow. It is the most common type of elbow fracture and accounts for approximately 60% of all elbow fractures. It is considered an injury of the immature skeleton and occurs in young children between 5 to 10 years of age. Based on the mechanism of injury and the displacement of the distal fragment, professionals classify these as either extension or flexion type fractures.[rx][rx][rx] Beware that a nondisplaced fracture may be subtle and may only be recognized by one of the following:
Posterior fat pad sign
Anterior sail sign
Disruption of the anterior humeral line
Radiographically, these fractures are classified into three types:
Type I – minimal or no displacement
Type II – displaced fracture, posterior cortex intact
Type III – totally displaced fracture, anterior and posterior cortices disrupted
In a flexion type fracture that happens in less than 5% of cases, the elbow is displaced anteriorly. The typical mechanism is when a direct anterior force is applied against a flexed elbow, which causes anterior displacement of the distal fragment. With the displacement of the fragment, the periosteum tears posteriorly. Since the mechanism is a direct force, flexion type fractures are often open.[rx][rx][rx][rx]
Type I fracture – non-displaced or minimally displaced
Type II fractures – incomplete fracture; anterior cortex is intact
Type III fracture – completely displaced; distal fragment migrates proximally and anteriorly
One of the most serious complications is neurovascular injury following the fracture, as the brachial artery and median nerve are located close to the site of the fracture and can be easily compromised.
Gartland Classification
Supracondylar fractures can be classified depending on the degree of displacement:
Gartland Type 1 Fracture – Minimally displaced or occult fracture. The fracture is difficult to see on x-rays. The anterior humeral line still intersects the anterior half of the capitellum. The only visible sign on an x-ray will be a positive fat pad sign.
Gartland Type 2 Fracture – Fracture that is displaced more posteriorly, but the posterior cortex remains intact.
Gartland Type 3 Fracture – Completely displaced fracture with cortical disruption. Posteromedial displacement is more common happening in 75% of cases compared to posterolateral displacement which occurs in 25% of cases.
Lateral Condyle Fractures
These types of fractures are the second most common type of elbow fracture in children and account for 15% to 20% of all elbow fractures. This fracture involves the lateral condyle of the distal humerus, which is the outer bony prominence of the elbow.
The peak age for the occurrence of lateral condyle fractures is four to ten years old. Most commonly, these are Salter-Harris type IV ( a fracture that transects the metaphysis, physis, and epiphysis) involving the lateral condyle.
Two types of classifications are used to describe lateral condyle fractures
Milch classification
Milch 1 – Less common type. Fracture line traverses laterally to the trochlear groove. Elbow is stable.
Milch II – More common type. Fracture passes through the trochlear groove. Elbow is unstable.
Displacement Classification
Type 1 – Displacement of less than 2 mm
Type 2 – more than 2 mm but less than 4 mm displacement. The fragment is close to the humerus
Type 3 – Wide displacement, the articular surface is disrupted.
Medial Epicondyle Fractures
These fractures are the third most common type of elbow fracture in children. It is an extra-articular fracture. It involves a fracture of the medial epicondyle apophysis, which is located on the posteromedial aspect of the elbow. It commonly occurs in early adolescence, between the ages of nine to 14 years of age.
It is more common in boys and occurs during athletic activities such as football, baseball, or gymnastics. The common mechanisms of injury are a posterior elbow dislocation and repeated valgus stress. An example is throwing a baseball repeatedly. One term for this is “little league elbow.”
A common presentation is medial elbow pain, tenderness over the medial epicondyle, and valgus instability.
Radial Head and Neck Fractures
These fractures comprise about 1% to 5% of all pediatric elbow fractures. Most commonly these are Salter-Harris type II fractures that transect the physis and extend into the metaphysis for a short distance. This usually occurs between the ages of nine to ten years.
Olecranon Fractures
Olecranon fractures are uncommon in children. These are mostly associated with radial head and neck fractures.
Causes of Elbow Joints Fractures
In general, elbow trauma can subdivide into the following categories:
Traumatic injuries
Soft tissue injuries range from mild, superficial soft tissue injuries (e.g., simple contusions, strains, or sprains) to traumatic arthrotomies following gunshot wounds or penetrating lacerations
The osseoligamentous spectrum of injury encompasses fractures, fracture-dislocations, ligamentous injuries, and simple versus complex dislocation patterns
“Simple” referring to no associated fracture accompanying the dislocation
“Complex” refers to an associated fracture accompanying the dislocation
Terrible triad elbow injuries
Elbow dislocation – Typically posterolateral direction with associated LCL complex injury. Elbow dislocation is the two most common dislocated joint after the shoulder – most are posterior dislocations
A radial head/neck fracture
Coronoid fracture
Attritional injuries – Encompasses subacute or chronic presentations following various repetitive motion mechanisms
Often seen in athletes involved in any upper extremity sport-related activity requiring repetitive motions (e.g., overhead throwers/baseball pitchers, tennis)
Manual laborers with analogous occupational repetitive demands
Traumatic injuries
Traumatic injuries range from simple contusions to more complex osseoligamentous fracture-dislocation patterns. The latter is often seen following a fall on an outstretched hand while the forearm is supinated and the elbow is either partially flexed or fully extended
Attritional injuries
Another form of elbow injuries consists of the subacute-to-chronic variety that occurs secondary to repetitive motions, eventually leading to various tendinosis conditions. These can include but are not limited to, lateral epicondylitis (tennis elbow), and chronic partial UCL injuries or strains.[rx][rx]
Pediatric considerations
Elbow trauma in children most commonly occurs via sport or following falls. Moreover, careful attention during the assessment is necessary, given the characteristic sequence of ossification center appearance and fusion, which can make the radiographic assessment rather challenging. Commonly encountered pediatric elbow fractures include (but are not limited to)[rx]
Supracondylar fractures
Most common in children peak ages 5 to 10 years, rarely occurs at greater than 15 years
Extension type (98%) – fall on an outstretched hand with fully extended or hyperextended armType 1: minimal or no displacement type 2: slightly displaced fracture, posterior cortex intact type 3: totally displaced fracture, the posterior cortex is broken.
Flexion type – blow directly to a flexed elbowType 1: minimal or no displacement type 2: slightly displaced fracture, anterior cortex intact type 3: totally displaced fracture, the anterior cortex is broken
Lateral condyle fractures
Medial epicondyle fractures
Radial head and neck fractures – Usually indirect mechanism (such as fall on an outstretched hand), and the radial head being driven into capitellum
Olecranon fractures
Another common elbow injury in children
Subluxated radial head (nursemaid’s elbow)
Accounts for 20% of all upper extremity injuries in children
Peak age 1 to 4 years; occurs more frequently in females than males
Mechanism of injury: sudden longitudinal pull on the forearm with forearm pronated
Signs and Symptoms of Elbow Joints Fractures
Symptoms include:
The child stops using the arm, which is held in extension (or slightly bent) and palm down.[rx]
Minimal swelling.
All movements are permitted except supination.
Pain on the outer part of the elbow (lateral epicondyle)
Point tenderness over the lateral epicondyle—a prominent part of the bone on the outside of the elbow
Pain from gripping and movements of the wrist, especially wrist extension (e.g. turning a screwdriver) and lifting movements[rx]
Sudden intense pain at the back of the elbow will be felt at the time of injury.
The patient will in most cases be unable to straighten the elbow.
Rapid swelling and bruising may start to appear. Trying to move the elbow will be painful and the back of the elbow will be very tender to touch.
Caused by longitudinal traction with the wrist in pronation, although in a series only 51% of people were reported to have this mechanism, with 22% reporting falls, and patients less than 6 months of age noted to have the injury after rolling over in bed.
Symptoms include pain and tenderness on the inside of the elbow. Bruising and swelling may be present for more severe injuries.
Impact injuries causing damage to the medial ligament usually involves a lateral force (towards the outside) being applied to the forearm, placing the medial (inner) joint under stress.
The patient presents with swelling over the lateral elbow with a limited range of motion, particularly forearm rotation and elbow extension ± elbow effusion and bruising. Pain is increased with passive rotation.
The most reliable clinical sign is point tenderness over the radial head.
Needs careful assessment for nerve and vascular involvement, especially with brachial artery, median and ulnar nerves.
It is important to detect crepitation or a mechanical blockage of motion from displaced fracture fragments. This often requires aspiration of a haemarthrosis with the installation of local anesthetic for pain relief.
If there is significant wrist pain and/or central forearm pain, there may be acute longitudinal radioulnar dissociation with disruption of the distal radioulnar joint.
Overuse injuries of the MCL may also occur. Repetitive motions that place a lot of stress on the inner elbow can cause damage to the ligament. For example, throwers (track and field and ball sports such as baseball) are prone to this injury. Especially if the technique is poor!
Diagnosis of Elbow Joints Fractures
Physical Examination
The examiner should perform and document relevant findings, including:
Skin integrity
Critical when assessing for the presence of an open fracture and/or traumatic arthrotomy
Presence of swelling or effusion
Comprehensive neurovascular examination
How the patient carries their arm may give clues to the diagnosis.
Bony injuries
Supracondylar fracture
Flexion type
Patient supports injured forearm with other arm and elbow in 90º flexion
Loss of olecranon prominence
Extension type
Patient hold arm at side in S-type configuration
Soft tissue injuries
Elbow dislocations:
Posterior: abnormal prominence of olecranon
Anterior: loss of olecranon prominence
Radial head subluxation
Elbow slightly flexed and forearm pronated resists moving the arm at the elbow
Sensory and motor testing of the Median and Ulnar nerves
Median
Test for sensory function
Two-point discrimination over the tip of the index finger.
Test for motor function
“OK” sign with thumb and index finger and abduction of the thumb (recurrent branch)
Ulnar
Test for sensory function
Two-point discrimination of the little finger
Test for motor function
Abduct index finger against resistance
Compartment Syndrome
Acute compartment syndrome can usually develop over a few hours after a serious injury. Some symptoms of acute compartment syndrome are:
A new persistent deep pain
Pain that seems greater than expected for the severity of the injury
Numbness and tingling in the limb
Swelling, tightness and bruising
Radiological Test
Radiographic studies that are necessary for all patients presenting with varying degrees of elbow trauma include:
Anteroposterior (AP) elbow
Lateral elbow
Oblique views (optional, depending on fracture/injury)
Traction view (optional, can facilitate the assessment of comminuted fracture patterns)
Ipsilateral shoulder to wrist orthogonal views
Especially in the setting of high energy trauma or when exam and evaluation are limited
Fat pad sign
Seen with intra-articular injuries
Normally, anterior fat pad is a narrow radiolucent strip anterior to humerus
The posterior fat pad is normally not visible
Anterior fat pad sign indicates joint effusion/ injury when raised and becomes more perpendicular to the anterior humeral cortex (sail sign)
Posterior fat pad sign indicates effusion/injury
In adults, posterior fat pad sign without other obvious fracture implies radial head fracture
In children, it implies supracondylar fracture
Pediatric Considerations
Fractures in children often occur through unossified cartilage, making radiographic interpretation confusing
A line of mensuration drawn down the anterior surface of the humerus should always bisect the capitellum in lateral view.
If any bony relationship appears questionable on radiographs, obtain a comparison view of uninvolved elbow.
Suspect nonaccidental trauma if history does not tip injury.
Ossification centers: 1 appear: (CRITOE)
Capitellum 3 to 6 months
Radial head 3 to 5 years
Medial (Internal) epicondyle 5 to 7 years
Trochlea 9 to 10 years
Olecranon 9 to 10 years
Lateral Epicondyle
It is essential to do bilateral radiographic imaging in pediatric cases.
A nurse elbow can reduce spontaneously when the patient supinates the arm.
Advanced imaging sequences
Computerized tomography (CT) scans are often a consideration in the setting of comminuted fracture patterns for pre-operative surgical planning. Magnetic resonance imaging (MRI) can be an option in the setting of soft tissue and ligamentous injury evaluation, or when suspecting stress or occult fractures.[rx][rx][rx]
Alert
Based on the complex anatomy of the elbow, a few things require attention:
Neurovascular injuries to numerous structures that pass about the elbow, including anterior interosseous nerve, ulnar and radial nerves, brachial artery
Volkmann ischemic contracture is compartment syndrome of the forearm
Differential Diagnosis
It is important to remember all possible diagnoses including (but not limited to):
Fracture
Dislocation
Sprain
Strain
Ligamentous insufficiencies (e.g., UCL)
Bursitis
Tendinopathic conditions (acute or chronic)
Pediatric differential considerations include
Child abuse
Distal humeral physeal injuries
Nursemaids elbow
Fracture(s)
Avulsions
Monteggia fracture-dislocations
Physeal injuries/reactions
Treatment of Elbow Joints Fractures
Doctors sometimes recommend very different treatments for both tennis elbow and golfer’s elbow. According to the studies done so far, the following treatments can help:
Rest, ice
Physical therapy when appropriate – Eccentric exercises for lateral epicondylitis
Braces/bandages – These are worn around the elbow or on the forearm to take the strain off the muscles.
Injections – Injections into the elbow with various substances, such as Botox, hyaluronic acid or autologous blood (the body’s own blood).
Extracorporeal shockwave therapy (ESWT) – A device generates shock or pressure waves that are transferred to the tissue through the skin. This is supposed to improve the circulation of blood in the tissue and speed up the healing process.
Laser therapy – The tissue is treated with concentrated beams of light. This is supposed to stimulate the circulation of blood and the body’s cell metabolism.
Stretching and strengthening exercises: Special exercises that stretch and strengthen the muscles of the arm and wrist.
Manual therapy – This includes active and passive exercises, as well as massages.
Ultrasound therapy – The arm is exposed to high-frequency sound waves. This warms the tissue, which improves the circulation of blood.
Transcutaneous electrical nerve stimulation (TENS) – TENS devices transfer electrical impulses to the nervous system through the skin. These are supposed to keep the pain signals from reaching the brain.
Acupuncture – The acupuncture needles are inserted into certain points on the surface of the arm. Here, too, the aim is to minimize the perception of pain.
Cold – The elbow is regularly cooled with ice packs.
Massages –A massage technique called “transverse friction massage” is often used to treat tennis elbow and golfer’s elbow. It is applied to the tendons and the muscles, using the tips of one or two fingers.
Emergency department treatment and procedures
Uncomplicated posterolateral dislocation usually treated with closed reduction. If there is evidence of entrapped medial epicondylar fragment, open reduction may be needed.[rx][rx]
Orthopedic consultation is the standard for all but nondisplaced, stable fractures, which as a rule, can be splinted 24 to 48 hours orthopedic follow-up
Fractures generally requiring orthopedic consultation:
Fractures involving articular surfaces such as capitellum or trochlea
Supracondylar fractures:
ED physician can handle type 1 with 24 to 48 hours orthopedic follow-up
The elbow may be flexed and splinted with a posterior splint
Types 2 and 3 require an immediate orthopedic consult
Reduce these in ED when the fracture is associated with vascular compromise
Anterior dislocation:
Reduce immediately if vascular structures compromised
Then flexed to 90º and place the posterior splint
Posterior dislocation:
Reduce immediately if vascular structures compromised
Then flexed 90º and place posterior splint.
Radial head fracture:
Minimally displaced fractures may need aspiration to remove hemarthrosis: instill bupivacaine and immobilize.
Other types should have an orthopedic consult.
Radial head subluxation
In one continuous motion, supinate and flex elbow while placing slight pressure on the radial head.
Hyper pronation technique is possibly more effective – while grasping the patient’s elbow, the wrist is hyper-pronated until feeling a palpable click.
A palpable click will often accompany the reduction
If the exam suggests fracture, but radiograph is negative, splint and have the patient follow up in 24 to 48 hours for re-evaluation
Medication
Conscious sedation is often necessary to achieve reductions
Painkillers – especially non-steroidal anti-inflammatory drugs (NSAIDs).
Injections – Steroid injections.
Ibuprofen – 600 to 800 mg (pediatric: 5 to 10 mg/kg) PO TID
Naprosyn – 250 to 500 mg (pediatric: 10 to 20 mg/kg) PO BID
Tylenol with codeine – 1 or 2 tabs (pediatric 0.5 to 1 mg/kg codeine) PO: do not exceed acetaminophen 4g/24 hours
Morphine sulfate – 0.1 mg/kg IV
Hydromorphone 5 mg/acetaminophen 300mg
Hydrocodone/acetaminophen – 1 to 2 tabs PO
Attritional injuries management modalities
Most of these injections contain one of the following active ingredients. These include but are not limited to[rx][rx][rx]:
Corticosteroid injection – when applicable
Platelet-rich plasma (PRP) considerations – 2016 study noted efficacy in managing UCL insufficiency
Steroids: reduce inflammation. Studies show that steroid injections can temporarily relieve pain. But there is also evidence that they can disrupt the healing process: People who were first given several steroid injections had more pain after a few months than people who didn’t receive any steroid injections. Frequent steroid injections carry the risk of tissue dying (atrophy), for instance, leaving a visible mark on the elbow.
Hyaluronic acid – A substance made by the body, found in tissue and joints. It is typically used to treat osteoarthritis. One study suggests that hyaluronic acid might be effective in the treatment of tennis elbow. But further research is needed to assess its pros and cons.
Botox – inhibits the sending of signals between the nerve cells. This has a paralyzing effect on the muscles. According to studies done on this so far, Botox can relieve the pain just a little at most. Also, Botox injections can have side effects like partial paralysis in the fingers that can last several weeks.
Autologous blood injections – Blood is taken from a vein in the arm and then injected into the elbow. This blood may be treated in different ways before it is injected. One common form of treatment with autologous blood is called platelet-rich plasma (PRP) therapy. It involves separating the blood into its various elements in a centrifuge. Then a concentrated solution of blood platelets is injected into the elbow. There is no evidence that treatment using autologous blood is effective.
Disposition
Admission Criteria
Vascular injuries, open fracture
Fractures requiring operative reduction or internal fixation.
Admit all patients with extensive swelling or ecchymosis for overnight observation and elevation to monitor for and decrease the risk for compartment syndrome.
Discharge Criteria
Stable fractures or reduced dislocations with none of the above features.
Splint and arrange orthopedic follow-up in 24 to 48 hours
Uncomplicated soft tissue injuries.
It is crucial to recall that prolonged elbow immobilization can cause stiffness to the patient, so the main goal is to get the elbow’s range of movement back as soon as possible.
Surgery
Different surgical approaches are used. Most of them involve detaching parts of the forearm muscles or separating and destroying the nerves that carry the pain signals.
Complications of Elbow Joints Fractures
Complications of lateral epicondylitis can include recurrence of the injury when normal activity is resumed, rupture of the tendons with repeated steroid injections, and failure to improve conservative treatment.
Neuropraxia – This occurs because of nerve injury. It resolves in three to four months. Nerve injury occurs in 11% of supracondylar fractures. Most commonly injured is the interosseous nerve, followed by the radial, median, and ulnar nerves.[rx][rx]
The anterior interosseous nerve (arising from the median nerve) and may be involved either due to traction or contusion.
The radial nerve may be involved with posteromedial displacement
Median nerve involvement may occur with posterolateral displacement
Ulnar nerve involvement may occur with a flexion type supracondylar fracture. The ulnar nerve is most commonly involved due to posterior displacement of the proximal fragment.
Beware that motor testing can only identify anterior interosseous nerve injury. This testing can be done by flexing at the index finger distal interphalangeal and thumb interphalangeal joints and making the “okay” sign. Inability to do so represents a lack of sensory component in the anterior interosseous nerve.
Vascular injury – Brachial artery injury should always be suspected, particularly if the radial pulse is absent. However, vascular injury may occur even if the hand is pink and well perfused. This may be due to partial transection of a vessel.
Compartment syndrome – this may occur after a supracondylar fracture. Evaluate for the early or impending signs by determining if a radial pulse is absent. This injury results from prolonged ischemia of the forearm. It should be suspected if the following are present:
Inability to open the hand in children
Pain on passive extension of the fingers
Tenderness over the forearm
Absence of a radial pulse
A careful neurovascular examination is therefore important to promptly recognize this serious complication.
Malunion– Fracture malunion can lead to cubitus valgus or cubitus varus deformity (common in supracondylar fracture). A common complication is a loss of the carrying angle, which results in a cubitus varus, or “Gunstock,” deformity.
Nonunion – Lateral condylar fractures are more prone to nonunion. These, therefore, require revision surgery.
Postoperative complications can include the following:
Failing to address concomitant pathology
patients report inferior outcomes and lack of improvement if the primary cause of symptoms is not addressed; patients should be educated regarding the risks and benefits of surgery — the former include but are not limited to infection, blood loss, neurovascular injury, continued pain, stiffness, or continued or worsening overall dysfunction
radial nerve entrapment can be missed or not addressed clinically in up to 5% of patients being managed for lateral epicondylitis
Iatrogenic LUCL injury
occurs iatrogenically with increased risk if the surgical dissection extends beyond the radial head equator
postoperative iatrogenic posterolateral rotatory instability (PLRI) can develop if the extension or LUCL compromise is significant
Iatrogenic neurovascular injury
radial nerve injury
Heterotopic ossification
decrease risk with via copious saline irrigation following decortication and debridement
Elbow Joints Injuries are the most common cause of elbow pain. Some people may not recall having had a specific injury, especially if symptoms began gradually or during everyday activities. To better understand elbow injuries, you may want to review the structure and function of the elbow. See a picture of the elbow.
Dislocations may be isolated, involve damage to static supportive structures of the elbow, and may even cause fractures about the elbow. Because of this, it is important to recognize elbow dislocations and know the appropriate management to avoid any complications.
Your elbow joint is made up of bone, cartilage, ligaments, and fluid. Muscles and tendons help the elbow joint move. When any of these structures is hurt or diseased, you have elbow problems. Many things can make your elbow hurt. A common cause is a tendinitis, an inflammation or injury to the tendons that attach muscle to bone. Tendinitis of the elbow is a sports injury, often from playing tennis or golf. You may also get tendinitis from the overuse of the elbow. Other causes of elbow pain include sprains and strains, fractures (broken bones), dislocations, bursitis, and arthritis. Treatment depends on the cause.
Types of Elbow Joints Injuries
Sudden (acute) injury
An acute injury may be caused by a direct blow, penetrating injury, or fall or by twisting, jerking, jamming, or bending an elbow abnormally. Pain may be sudden and severe. Bruising and swelling may develop soon after the injury. Acute injuries include:
Bruises from a tear or rupture of small blood vessels under the skin.
Injuries to ligaments, the ropy fibers that connect bones to bones around joints.
Injuries to tendons that connect muscles to bones.
Injuries to joints (sprains) that stretch or tear the ligaments.
Pulled muscles (strains) caused by overstretching muscles.
Muscle tears or ruptures, such as your biceps or triceps in your upper arm.
Broken bones (fractures) of the upper arm bone (humerus) or the forearm bones (ulna or radius) at the elbow joint.
Dislocations of the elbow joint (out of its normal position).
Overuse injuries
Overuse injuries occur when too much stress is placed on a joint or other tissue, often by overdoing an activity or through repetition of an activity. Overuse injuries include:
Bursitis. Swelling behind the elbow may be olecranon bursitis (Popeye elbow).
Tendinosis, which is a series of microtears in the connective tissue in or around the tendon.
Soreness or pain felt on the outside (lateral) part of the elbow may be tennis elbow (lateral epicondylitis). This is the most common type of tendinopathy that affects the elbow and most often is caused by overuse of the forearm muscles. This overuse may occur during sports, such as tennis, swimming, golf, and sports involving throwing; jobs, such as carpentry or plumbing; or daily activities, such as lifting objects or gardening.
Soreness or pain in the inner (medial) part of the elbow may be golfer’s elbow. In children who participate in sports that involve throwing, the same elbow pain may be described as Little Leaguer’s elbow.
Pinched nerves, such as ulnar nerve compression, which is the pinching of the ulnar nerve near the elbow joint. This usually occurs with repeated motions.
Supracondylar Fractures
This type of fracture involves the distal humerus just above the elbow. It is the most common type of elbow fracture and accounts for approximately 60% of all elbow fractures. It is considered an injury of the immature skeleton and occurs in young children between 5 to 10 years of age. Based on the mechanism of injury and the displacement of the distal fragment, professionals classify these as either extension or flexion type fractures.[rx][rx][rx] Beware that a nondisplaced fracture may be subtle and may only be recognized by one of the following:
Posterior fat pad sign
Anterior sail sign
Disruption of the anterior humeral line
Radiographically, these fractures are classified into three types:
Type I – minimal or no displacement
Type II – displaced fracture, posterior cortex intact
Type III – totally displaced fracture, anterior and posterior cortices disrupted
In a flexion type fracture that happens in less than 5% of cases, the elbow is displaced anteriorly. The typical mechanism is when a direct anterior force is applied against a flexed elbow, which causes anterior displacement of the distal fragment. With the displacement of the fragment, the periosteum tears posteriorly. Since the mechanism is a direct force, flexion type fractures are often open.[rx][rx][rx][rx]
Type I fracture – non-displaced or minimally displaced
Type II fractures – incomplete fracture; anterior cortex is intact
Type III fracture – completely displaced; distal fragment migrates proximally and anteriorly
One of the most serious complications is neurovascular injury following the fracture, as the brachial artery and median nerve are located close to the site of the fracture and can be easily compromised.
Gartland Classification
Supracondylar fractures can be classified depending on the degree of displacement:
Gartland Type 1 Fracture – Minimally displaced or occult fracture. The fracture is difficult to see on x-rays. The anterior humeral line still intersects the anterior half of the capitellum. The only visible sign on an x-ray will be a positive fat pad sign.
Gartland Type 2 Fracture – Fracture that is displaced more posteriorly, but the posterior cortex remains intact.
Gartland Type 3 Fracture – Completely displaced fracture with cortical disruption. Posteromedial displacement is more common happening in 75% of cases compared to posterolateral displacement which occurs in 25% of cases.
Lateral Condyle Fractures
These types of fractures are the second most common type of elbow fracture in children and account for 15% to 20% of all elbow fractures. This fracture involves the lateral condyle of the distal humerus, which is the outer bony prominence of the elbow.
The peak age for the occurrence of lateral condyle fractures is four to ten years old. Most commonly, these are Salter-Harris type IV ( a fracture that transects the metaphysis, physis, and epiphysis) involving the lateral condyle.
Two types of classifications are used to describe lateral condyle fractures
Milch classification
Milch 1 – Less common type. Fracture line traverses laterally to the trochlear groove. Elbow is stable.
Milch II – More common type. Fracture passes through the trochlear groove. Elbow is unstable.
Displacement Classification
Type 1 – Displacement of less than 2 mm
Type 2 – more than 2 mm but less than 4 mm displacement. The fragment is close to the humerus
Type 3 – Wide displacement, the articular surface is disrupted.
Medial Epicondyle Fractures
These fractures are the third most common type of elbow fracture in children. It is an extra-articular fracture. It involves a fracture of the medial epicondyle apophysis, which is located on the posteromedial aspect of the elbow. It commonly occurs in early adolescence, between the ages of nine to 14 years of age.
It is more common in boys and occurs during athletic activities such as football, baseball, or gymnastics. The common mechanisms of injury are a posterior elbow dislocation and repeated valgus stress. An example is throwing a baseball repeatedly. One term for this is “little league elbow.”
A common presentation is medial elbow pain, tenderness over the medial epicondyle, and valgus instability.
Radial Head and Neck Fractures
These fractures comprise about 1% to 5% of all pediatric elbow fractures. Most commonly these are Salter-Harris type II fractures that transect the physis and extend into the metaphysis for a short distance. This usually occurs between the ages of nine to ten years.
Olecranon Fractures
Olecranon fractures are uncommon in children. These are mostly associated with radial head and neck fractures.
Causes of Elbow Joints Injuries
In general, elbow trauma can subdivide into the following categories:
Traumatic injuries
Soft tissue injuries range from mild, superficial soft tissue injuries (e.g., simple contusions, strains, or sprains) to traumatic arthrotomies following gunshot wounds or penetrating lacerations
The osseoligamentous spectrum of injury encompasses fractures, fracture-dislocations, ligamentous injuries, and simple versus complex dislocation patterns
“Simple” referring to no associated fracture accompanying the dislocation
“Complex” refers to an associated fracture accompanying the dislocation
Terrible triad elbow injuries
Elbow dislocation – Typically posterolateral direction with associated LCL complex injury. Elbow dislocation is the two most common dislocated joint after the shoulder – most are posterior dislocations
A radial head/neck fracture
Coronoid fracture
Attritional injuries – Encompasses subacute or chronic presentations following various repetitive motion mechanisms
Often seen in athletes involved in any upper extremity sport-related activity requiring repetitive motions (e.g., overhead throwers/baseball pitchers, tennis)
Manual laborers with analogous occupational repetitive demands
Traumatic injuries
Traumatic injuries range from simple contusions to more complex osseoligamentous fracture-dislocation patterns. The latter is often seen following a fall on an outstretched hand while the forearm is supinated and the elbow is either partially flexed or fully extended
Attritional injuries
Another form of elbow injuries consists of the subacute-to-chronic variety that occurs secondary to repetitive motions, eventually leading to various tendinosis conditions. These can include but are not limited to, lateral epicondylitis (tennis elbow), and chronic partial UCL injuries or strains.[rx][rx]
Pediatric considerations
Elbow trauma in children most commonly occurs via sport or following falls. Moreover, careful attention during the assessment is necessary, given the characteristic sequence of ossification center appearance and fusion, which can make the radiographic assessment rather challenging. Commonly encountered pediatric elbow fractures include (but are not limited to)[rx]
Supracondylar fractures
Most common in children peak ages 5 to 10 years, rarely occurs at greater than 15 years
Extension type (98%) – fall on an outstretched hand with fully extended or hyperextended armType 1: minimal or no displacement type 2: slightly displaced fracture, posterior cortex intact type 3: totally displaced fracture, the posterior cortex is broken.
Flexion type – blow directly to a flexed elbowType 1: minimal or no displacement type 2: slightly displaced fracture, anterior cortex intact type 3: totally displaced fracture, the anterior cortex is broken
Lateral condyle fractures
Medial epicondyle fractures
Radial head and neck fractures – Usually indirect mechanism (such as fall on an outstretched hand), and the radial head being driven into capitellum
Olecranon fractures
Another common elbow injury in children
Subluxated radial head (nursemaid’s elbow)
Accounts for 20% of all upper extremity injuries in children
Peak age 1 to 4 years; occurs more frequently in females than males
Mechanism of injury: sudden longitudinal pull on the forearm with forearm pronated
Signs and Symptoms of Elbow Joints Injuries
Symptoms include:
The child stops using the arm, which is held in extension (or slightly bent) and palm down.[rx]
Minimal swelling.
All movements are permitted except supination.
Pain on the outer part of the elbow (lateral epicondyle)
Point tenderness over the lateral epicondyle—a prominent part of the bone on the outside of the elbow
Pain from gripping and movements of the wrist, especially wrist extension (e.g. turning a screwdriver) and lifting movements[rx]
Sudden intense pain at the back of the elbow will be felt at the time of injury.
The patient will in most cases be unable to straighten the elbow.
Rapid swelling and bruising may start to appear. Trying to move the elbow will be painful and the back of the elbow will be very tender to touch.
Caused by longitudinal traction with the wrist in pronation, although in a series only 51% of people were reported to have this mechanism, with 22% reporting falls, and patients less than 6 months of age noted to have the injury after rolling over in bed.
Symptoms include pain and tenderness on the inside of the elbow. Bruising and swelling may be present for more severe injuries.
Impact injuries causing damage to the medial ligament usually involves a lateral force (towards the outside) being applied to the forearm, placing the medial (inner) joint under stress.
The patient presents with swelling over the lateral elbow with a limited range of motion, particularly forearm rotation and elbow extension ± elbow effusion and bruising. Pain is increased with passive rotation.
The most reliable clinical sign is point tenderness over the radial head.
Needs careful assessment for nerve and vascular involvement, especially with brachial artery, median and ulnar nerves.
It is important to detect crepitation or a mechanical blockage of motion from displaced fracture fragments. This often requires aspiration of a haemarthrosis with the installation of local anesthetic for pain relief.
If there is significant wrist pain and/or central forearm pain, there may be acute longitudinal radioulnar dissociation with disruption of the distal radioulnar joint.
Overuse injuries of the MCL may also occur. Repetitive motions that place a lot of stress on the inner elbow can cause damage to the ligament. For example, throwers (track and field and ball sports such as baseball) are prone to this injury. Especially if the technique is poor!
Diagnosis of Elbow Joints Injuries
Physical Examination
The examiner should perform and document relevant findings, including:
Skin integrity
Critical when assessing for the presence of an open fracture and/or traumatic arthrotomy
Presence of swelling or effusion
Comprehensive neurovascular examination
How the patient carries their arm may give clues to the diagnosis.
Bony injuries
Supracondylar fracture
Flexion type
Patient supports injured forearm with other arm and elbow in 90º flexion
Loss of olecranon prominence
Extension type
Patient hold arm at side in S-type configuration
Soft tissue injuries
Elbow dislocations:
Posterior: abnormal prominence of olecranon
Anterior: loss of olecranon prominence
Radial head subluxation
Elbow slightly flexed and forearm pronated resists moving the arm at the elbow
Sensory and motor testing of the Median and Ulnar nerves
Median
Test for sensory function
Two-point discrimination over the tip of the index finger.
Test for motor function
“OK” sign with thumb and index finger and abduction of the thumb (recurrent branch)
Ulnar
Test for sensory function
Two-point discrimination of the little finger
Test for motor function
Abduct index finger against resistance
Compartment Syndrome
Acute compartment syndrome can usually develop over a few hours after a serious injury. Some symptoms of acute compartment syndrome are:
A new persistent deep pain
Pain that seems greater than expected for the severity of the injury
Numbness and tingling in the limb
Swelling, tightness and bruising
Radiological Test
Radiographic studies that are necessary for all patients presenting with varying degrees of elbow trauma include:
Anteroposterior (AP) elbow
Lateral elbow
Oblique views (optional, depending on fracture/injury)
Traction view (optional, can facilitate the assessment of comminuted fracture patterns)
Ipsilateral shoulder to wrist orthogonal views
Especially in the setting of high energy trauma or when exam and evaluation are limited
Fat pad sign
Seen with intra-articular injuries
Normally, anterior fat pad is a narrow radiolucent strip anterior to humerus
The posterior fat pad is normally not visible
Anterior fat pad sign indicates joint effusion/ injury when raised and becomes more perpendicular to the anterior humeral cortex (sail sign)
Posterior fat pad sign indicates effusion/injury
In adults, posterior fat pad sign without other obvious fracture implies radial head fracture
In children, it implies supracondylar fracture
Pediatric Considerations
Fractures in children often occur through unossified cartilage, making radiographic interpretation confusing
A line of mensuration drawn down the anterior surface of the humerus should always bisect the capitellum in lateral view.
If any bony relationship appears questionable on radiographs, obtain a comparison view of uninvolved elbow.
Suspect nonaccidental trauma if history does not tip injury.
Ossification centers: 1 appear: (CRITOE)
Capitellum 3 to 6 months
Radial head 3 to 5 years
Medial (Internal) epicondyle 5 to 7 years
Trochlea 9 to 10 years
Olecranon 9 to 10 years
Lateral Epicondyle
It is essential to do bilateral radiographic imaging in pediatric cases.
A nurse elbow can reduce spontaneously when the patient supinates the arm.
Advanced imaging sequences
Computerized tomography (CT) scans are often a consideration in the setting of comminuted fracture patterns for pre-operative surgical planning. Magnetic resonance imaging (MRI) can be an option in the setting of soft tissue and ligamentous injury evaluation, or when suspecting stress or occult fractures.[rx][rx][rx]
Alert
Based on the complex anatomy of the elbow, a few things require attention:
Neurovascular injuries to numerous structures that pass about the elbow, including anterior interosseous nerve, ulnar and radial nerves, brachial artery
Volkmann ischemic contracture is compartment syndrome of the forearm
Differential Diagnosis
It is important to remember all possible diagnoses including (but not limited to):
Fracture
Dislocation
Sprain
Strain
Ligamentous insufficiencies (e.g., UCL)
Bursitis
Tendinopathic conditions (acute or chronic)
Pediatric differential considerations include
Child abuse
Distal humeral physeal injuries
Nursemaids elbow
Fracture(s)
Avulsions
Monteggia fracture-dislocations
Physeal injuries/reactions
Treatment of Elbow Joints Injuries
Doctors sometimes recommend very different treatments for both tennis elbow and golfer’s elbow. According to the studies done so far, the following treatments can help:
Rest, ice
Physical therapy when appropriate – Eccentric exercises for lateral epicondylitis
Braces/bandages – These are worn around the elbow or on the forearm to take the strain off the muscles.
Injections – Injections into the elbow with various substances, such as Botox, hyaluronic acid or autologous blood (the body’s own blood).
Extracorporeal shockwave therapy (ESWT) – A device generates shock or pressure waves that are transferred to the tissue through the skin. This is supposed to improve the circulation of blood in the tissue and speed up the healing process.
Laser therapy – The tissue is treated with concentrated beams of light. This is supposed to stimulate the circulation of blood and the body’s cell metabolism.
Stretching and strengthening exercises: Special exercises that stretch and strengthen the muscles of the arm and wrist.
Manual therapy – This includes active and passive exercises, as well as massages.
Ultrasound therapy – The arm is exposed to high-frequency sound waves. This warms the tissue, which improves the circulation of blood.
Transcutaneous electrical nerve stimulation (TENS) – TENS devices transfer electrical impulses to the nervous system through the skin. These are supposed to keep the pain signals from reaching the brain.
Acupuncture – The acupuncture needles are inserted into certain points on the surface of the arm. Here, too, the aim is to minimize the perception of pain.
Cold – The elbow is regularly cooled with ice packs.
Massages –A massage technique called “transverse friction massage” is often used to treat tennis elbow and golfer’s elbow. It is applied to the tendons and the muscles, using the tips of one or two fingers.
Emergency department treatment and procedures
Uncomplicated posterolateral dislocation usually treated with closed reduction. If there is evidence of entrapped medial epicondylar fragment, open reduction may be needed.[rx][rx]
Orthopedic consultation is the standard for all but nondisplaced, stable fractures, which as a rule, can be splinted 24 to 48 hours orthopedic follow-up
Fractures generally requiring orthopedic consultation:
Fractures involving articular surfaces such as capitellum or trochlea
Supracondylar fractures:
ED physician can handle type 1 with 24 to 48 hours orthopedic follow-up
The elbow may be flexed and splinted with a posterior splint
Types 2 and 3 require an immediate orthopedic consult
Reduce these in ED when the fracture is associated with vascular compromise
Anterior dislocation:
Reduce immediately if vascular structures compromised
Then flexed to 90º and place the posterior splint
Posterior dislocation:
Reduce immediately if vascular structures compromised
Then flexed 90º and place posterior splint.
Radial head fracture:
Minimally displaced fractures may need aspiration to remove hemarthrosis: instill bupivacaine and immobilize.
Other types should have an orthopedic consult.
Radial head subluxation
In one continuous motion, supinate and flex elbow while placing slight pressure on the radial head.
Hyper pronation technique is possibly more effective – while grasping the patient’s elbow, the wrist is hyper-pronated until feeling a palpable click.
A palpable click will often accompany the reduction
If the exam suggests fracture, but radiograph is negative, splint and have the patient follow up in 24 to 48 hours for re-evaluation
Medication
Conscious sedation is often necessary to achieve reductions
Painkillers – especially non-steroidal anti-inflammatory drugs (NSAIDs).
Injections – Steroid injections.
Ibuprofen – 600 to 800 mg (pediatric: 5 to 10 mg/kg) PO TID
Naprosyn – 250 to 500 mg (pediatric: 10 to 20 mg/kg) PO BID
Tylenol with codeine – 1 or 2 tabs (pediatric 0.5 to 1 mg/kg codeine) PO: do not exceed acetaminophen 4g/24 hours
Morphine sulfate – 0.1 mg/kg IV
Hydromorphone 5 mg/acetaminophen 300mg
Hydrocodone/acetaminophen – 1 to 2 tabs PO
Attritional injuries management modalities
Most of these injections contain one of the following active ingredients. These include but are not limited to[rx][rx][rx]:
Corticosteroid injection – when applicable
Platelet-rich plasma (PRP) considerations – 2016 study noted efficacy in managing UCL insufficiency
Steroids: reduce inflammation. Studies show that steroid injections can temporarily relieve pain. But there is also evidence that they can disrupt the healing process: People who were first given several steroid injections had more pain after a few months than people who didn’t receive any steroid injections. Frequent steroid injections carry the risk of tissue dying (atrophy), for instance, leaving a visible mark on the elbow.
Hyaluronic acid – A substance made by the body, found in tissue and joints. It is typically used to treat osteoarthritis. One study suggests that hyaluronic acid might be effective in the treatment of tennis elbow. But further research is needed to assess its pros and cons.
Botox – inhibits the sending of signals between the nerve cells. This has a paralyzing effect on the muscles. According to studies done on this so far, Botox can relieve the pain just a little at most. Also, Botox injections can have side effects like partial paralysis in the fingers that can last several weeks.
Autologous blood injections – Blood is taken from a vein in the arm and then injected into the elbow. This blood may be treated in different ways before it is injected. One common form of treatment with autologous blood is called platelet-rich plasma (PRP) therapy. It involves separating the blood into its various elements in a centrifuge. Then a concentrated solution of blood platelets is injected into the elbow. There is no evidence that treatment using autologous blood is effective.
Disposition
Admission Criteria
Vascular injuries, open fracture
Fractures requiring operative reduction or internal fixation.
Admit all patients with extensive swelling or ecchymosis for overnight observation and elevation to monitor for and decrease the risk for compartment syndrome.
Discharge Criteria
Stable fractures or reduced dislocations with none of the above features.
Splint and arrange orthopedic follow-up in 24 to 48 hours
Uncomplicated soft tissue injuries.
It is crucial to recall that prolonged elbow immobilization can cause stiffness to the patient, so the main goal is to get the elbow’s range of movement back as soon as possible.
Surgery
Different surgical approaches are used. Most of them involve detaching parts of the forearm muscles or separating and destroying the nerves that carry the pain signals.
Complications of Elbow Joints Injuries
Complications of lateral epicondylitis can include recurrence of the injury when normal activity is resumed, rupture of the tendons with repeated steroid injections, and failure to improve conservative treatment.
Neuropraxia – This occurs because of nerve injury. It resolves in three to four months. Nerve injury occurs in 11% of supracondylar fractures. Most commonly injured is the interosseous nerve, followed by the radial, median, and ulnar nerves.[rx][rx]
The anterior interosseous nerve (arising from the median nerve) and may be involved either due to traction or contusion.
The radial nerve may be involved with posteromedial displacement
Median nerve involvement may occur with posterolateral displacement
Ulnar nerve involvement may occur with a flexion type supracondylar fracture. The ulnar nerve is most commonly involved due to posterior displacement of the proximal fragment.
Beware that motor testing can only identify anterior interosseous nerve injury. This testing can be done by flexing at the index finger distal interphalangeal and thumb interphalangeal joints and making the “okay” sign. Inability to do so represents a lack of sensory component in the anterior interosseous nerve.
Vascular injury – Brachial artery injury should always be suspected, particularly if the radial pulse is absent. However, vascular injury may occur even if the hand is pink and well perfused. This may be due to partial transection of a vessel.
Compartment syndrome – this may occur after a supracondylar fracture. Evaluate for the early or impending signs by determining if a radial pulse is absent. This injury results from prolonged ischemia of the forearm. It should be suspected if the following are present:
Inability to open the hand in children
Pain on passive extension of the fingers
Tenderness over the forearm
Absence of a radial pulse
A careful neurovascular examination is therefore important to promptly recognize this serious complication.
Malunion– Fracture malunion can lead to cubitus valgus or cubitus varus deformity (common in supracondylar fracture). A common complication is a loss of the carrying angle, which results in a cubitus varus, or “Gunstock,” deformity.
Nonunion – Lateral condylar fractures are more prone to nonunion. These, therefore, require revision surgery.
Postoperative complications can include the following:
Failing to address concomitant pathology
patients report inferior outcomes and lack of improvement if the primary cause of symptoms is not addressed; patients should be educated regarding the risks and benefits of surgery — the former include but are not limited to infection, blood loss, neurovascular injury, continued pain, stiffness, or continued or worsening overall dysfunction
radial nerve entrapment can be missed or not addressed clinically in up to 5% of patients being managed for lateral epicondylitis
Iatrogenic LUCL injury
occurs iatrogenically with increased risk if the surgical dissection extends beyond the radial head equator
postoperative iatrogenic posterolateral rotatory instability (PLRI) can develop if the extension or LUCL compromise is significant
Iatrogenic neurovascular injury
radial nerve injury
Heterotopic ossification
decrease risk with via copious saline irrigation following decortication and debridement
Elbow Injuries are the most common cause of elbow pain. Some people may not recall having had a specific injury, especially if symptoms began gradually or during everyday activities. To better understand elbow injuries, you may want to review the structure and function of the elbow. See a picture of the elbow.
Dislocations may be isolated, involve damage to static supportive structures of the elbow, and may even cause fractures about the elbow. Because of this, it is important to recognize elbow dislocations and know the appropriate management to avoid any complications.
Your elbow joint is made up of bone, cartilage, ligaments, and fluid. Muscles and tendons help the elbow joint move. When any of these structures is hurt or diseased, you have elbow problems. Many things can make your elbow hurt. A common cause is a tendinitis, an inflammation or injury to the tendons that attach muscle to bone. Tendinitis of the elbow is a sports injury, often from playing tennis or golf. You may also get tendinitis from the overuse of the elbow. Other causes of elbow pain include sprains and strains, fractures (broken bones), dislocations, bursitis, and arthritis. Treatment depends on the cause.
Types of Elbow Injuries
Sudden (acute) injury
An acute injury may be caused by a direct blow, penetrating injury, or fall or by twisting, jerking, jamming, or bending an elbow abnormally. Pain may be sudden and severe. Bruising and swelling may develop soon after the injury. Acute injuries include:
Bruises from a tear or rupture of small blood vessels under the skin.
Injuries to ligaments, the ropy fibers that connect bones to bones around joints.
Injuries to tendons that connect muscles to bones.
Injuries to joints (sprains) that stretch or tear the ligaments.
Pulled muscles (strains) caused by overstretching muscles.
Muscle tears or ruptures, such as your biceps or triceps in your upper arm.
Broken bones (fractures) of the upper arm bone (humerus) or the forearm bones (ulna or radius) at the elbow joint.
Dislocations of the elbow joint (out of its normal position).
Overuse injuries
Overuse injuries occur when too much stress is placed on a joint or other tissue, often by overdoing an activity or through repetition of an activity. Overuse injuries include:
Bursitis. Swelling behind the elbow may be olecranon bursitis (Popeye elbow).
Tendinosis, which is a series of microtears in the connective tissue in or around the tendon.
Soreness or pain felt on the outside (lateral) part of the elbow may be tennis elbow (lateral epicondylitis). This is the most common type of tendinopathy that affects the elbow and most often is caused by overuse of the forearm muscles. This overuse may occur during sports, such as tennis, swimming, golf, and sports involving throwing; jobs, such as carpentry or plumbing; or daily activities, such as lifting objects or gardening.
Soreness or pain in the inner (medial) part of the elbow may be golfer’s elbow. In children who participate in sports that involve throwing, the same elbow pain may be described as Little Leaguer’s elbow.
Pinched nerves, such as ulnar nerve compression, which is the pinching of the ulnar nerve near the elbow joint. This usually occurs with repeated motions.
Supracondylar Fractures
This type of fracture involves the distal humerus just above the elbow. It is the most common type of elbow fracture and accounts for approximately 60% of all elbow fractures. It is considered an injury of the immature skeleton and occurs in young children between 5 to 10 years of age. Based on the mechanism of injury and the displacement of the distal fragment, professionals classify these as either extension or flexion type fractures.[rx][rx][rx] Beware that a nondisplaced fracture may be subtle and may only be recognized by one of the following:
Posterior fat pad sign
Anterior sail sign
Disruption of the anterior humeral line
Radiographically, these fractures are classified into three types:
Type I – minimal or no displacement
Type II – displaced fracture, posterior cortex intact
Type III – totally displaced fracture, anterior and posterior cortices disrupted
In a flexion type fracture that happens in less than 5% of cases, the elbow is displaced anteriorly. The typical mechanism is when a direct anterior force is applied against a flexed elbow, which causes anterior displacement of the distal fragment. With the displacement of the fragment, the periosteum tears posteriorly. Since the mechanism is a direct force, flexion type fractures are often open.[rx][rx][rx][rx]
Type I fracture – non-displaced or minimally displaced
Type II fractures – incomplete fracture; anterior cortex is intact
Type III fracture – completely displaced; distal fragment migrates proximally and anteriorly
One of the most serious complications is neurovascular injury following the fracture, as the brachial artery and median nerve are located close to the site of the fracture and can be easily compromised.
Gartland Classification
Supracondylar fractures can be classified depending on the degree of displacement:
Gartland Type 1 Fracture – Minimally displaced or occult fracture. The fracture is difficult to see on x-rays. The anterior humeral line still intersects the anterior half of the capitellum. The only visible sign on an x-ray will be a positive fat pad sign.
Gartland Type 2 Fracture – Fracture that is displaced more posteriorly, but the posterior cortex remains intact.
Gartland Type 3 Fracture – Completely displaced fracture with cortical disruption. Posteromedial displacement is more common happening in 75% of cases compared to posterolateral displacement which occurs in 25% of cases.
Lateral Condyle Fractures
These types of fractures are the second most common type of elbow fracture in children and account for 15% to 20% of all elbow fractures. This fracture involves the lateral condyle of the distal humerus, which is the outer bony prominence of the elbow.
The peak age for the occurrence of lateral condyle fractures is four to ten years old. Most commonly, these are Salter-Harris type IV ( a fracture that transects the metaphysis, physis, and epiphysis) involving the lateral condyle.
Two types of classifications are used to describe lateral condyle fractures
Milch classification
Milch 1 – Less common type. Fracture line traverses laterally to the trochlear groove. Elbow is stable.
Milch II – More common type. Fracture passes through the trochlear groove. Elbow is unstable.
Displacement Classification
Type 1 – Displacement of less than 2 mm
Type 2 – more than 2 mm but less than 4 mm displacement. The fragment is close to the humerus
Type 3 – Wide displacement, the articular surface is disrupted.
Medial Epicondyle Fractures
These fractures are the third most common type of elbow fracture in children. It is an extra-articular fracture. It involves a fracture of the medial epicondyle apophysis, which is located on the posteromedial aspect of the elbow. It commonly occurs in early adolescence, between the ages of nine to 14 years of age.
It is more common in boys and occurs during athletic activities such as football, baseball, or gymnastics. The common mechanisms of injury are a posterior elbow dislocation and repeated valgus stress. An example is throwing a baseball repeatedly. One term for this is “little league elbow.”
A common presentation is medial elbow pain, tenderness over the medial epicondyle, and valgus instability.
Radial Head and Neck Fractures
These fractures comprise about 1% to 5% of all pediatric elbow fractures. Most commonly these are Salter-Harris type II fractures that transect the physis and extend into the metaphysis for a short distance. This usually occurs between the ages of nine to ten years.
Olecranon Fractures
Olecranon fractures are uncommon in children. These are mostly associated with radial head and neck fractures.
Causes of Elbow Injuries
In general, elbow trauma can subdivide into the following categories:
Traumatic injuries
Soft tissue injuries range from mild, superficial soft tissue injuries (e.g., simple contusions, strains, or sprains) to traumatic arthrotomies following gunshot wounds or penetrating lacerations
The osseoligamentous spectrum of injury encompasses fractures, fracture-dislocations, ligamentous injuries, and simple versus complex dislocation patterns
“Simple” referring to no associated fracture accompanying the dislocation
“Complex” refers to an associated fracture accompanying the dislocation
Terrible triad elbow injuries
Elbow dislocation – Typically posterolateral direction with associated LCL complex injury. Elbow dislocation is the two most common dislocated joint after the shoulder – most are posterior dislocations
A radial head/neck fracture
Coronoid fracture
Attritional injuries – Encompasses subacute or chronic presentations following various repetitive motion mechanisms
Often seen in athletes involved in any upper extremity sport-related activity requiring repetitive motions (e.g., overhead throwers/baseball pitchers, tennis)
Manual laborers with analogous occupational repetitive demands
Traumatic injuries
Traumatic injuries range from simple contusions to more complex osseoligamentous fracture-dislocation patterns. The latter is often seen following a fall on an outstretched hand while the forearm is supinated and the elbow is either partially flexed or fully extended
Attritional injuries
Another form of elbow injuries consists of the subacute-to-chronic variety that occurs secondary to repetitive motions, eventually leading to various tendinosis conditions. These can include but are not limited to, lateral epicondylitis (tennis elbow), and chronic partial UCL injuries or strains.[rx][rx]
Pediatric considerations
Elbow trauma in children most commonly occurs via sport or following falls. Moreover, careful attention during the assessment is necessary, given the characteristic sequence of ossification center appearance and fusion, which can make the radiographic assessment rather challenging. Commonly encountered pediatric elbow fractures include (but are not limited to)[rx]
Supracondylar fractures
Most common in children peak ages 5 to 10 years, rarely occurs at greater than 15 years
Extension type (98%) – fall on an outstretched hand with fully extended or hyperextended armType 1: minimal or no displacement type 2: slightly displaced fracture, posterior cortex intact type 3: totally displaced fracture, the posterior cortex is broken.
Flexion type – blow directly to a flexed elbowType 1: minimal or no displacement type 2: slightly displaced fracture, anterior cortex intact type 3: totally displaced fracture, the anterior cortex is broken
Lateral condyle fractures
Medial epicondyle fractures
Radial head and neck fractures – Usually indirect mechanism (such as fall on an outstretched hand), and the radial head being driven into capitellum
Olecranon fractures
Another common elbow injury in children
Subluxated radial head (nursemaid’s elbow)
Accounts for 20% of all upper extremity injuries in children
Peak age 1 to 4 years; occurs more frequently in females than males
Mechanism of injury: sudden longitudinal pull on the forearm with forearm pronated
Signs and Symptoms of Elbow Injuries
Symptoms include:
The child stops using the arm, which is held in extension (or slightly bent) and palm down.[rx]
Minimal swelling.
All movements are permitted except supination.
Pain on the outer part of the elbow (lateral epicondyle)
Point tenderness over the lateral epicondyle—a prominent part of the bone on the outside of the elbow
Pain from gripping and movements of the wrist, especially wrist extension (e.g. turning a screwdriver) and lifting movements[rx]
Sudden intense pain at the back of the elbow will be felt at the time of injury.
The patient will in most cases be unable to straighten the elbow.
Rapid swelling and bruising may start to appear. Trying to move the elbow will be painful and the back of the elbow will be very tender to touch.
Caused by longitudinal traction with the wrist in pronation, although in a series only 51% of people were reported to have this mechanism, with 22% reporting falls, and patients less than 6 months of age noted to have the injury after rolling over in bed.
Symptoms include pain and tenderness on the inside of the elbow. Bruising and swelling may be present for more severe injuries.
Impact injuries causing damage to the medial ligament usually involves a lateral force (towards the outside) being applied to the forearm, placing the medial (inner) joint under stress.
The patient presents with swelling over the lateral elbow with a limited range of motion, particularly forearm rotation and elbow extension ± elbow effusion and bruising. Pain is increased with passive rotation.
The most reliable clinical sign is point tenderness over the radial head.
Needs careful assessment for nerve and vascular involvement, especially with brachial artery, median and ulnar nerves.
It is important to detect crepitation or a mechanical blockage of motion from displaced fracture fragments. This often requires aspiration of a haemarthrosis with the installation of local anesthetic for pain relief.
If there is significant wrist pain and/or central forearm pain, there may be acute longitudinal radioulnar dissociation with disruption of the distal radioulnar joint.
Overuse injuries of the MCL may also occur. Repetitive motions that place a lot of stress on the inner elbow can cause damage to the ligament. For example, throwers (track and field and ball sports such as baseball) are prone to this injury. Especially if the technique is poor!
Diagnosis of Elbow Injuries
Physical Examination
The examiner should perform and document relevant findings, including:
Skin integrity
Critical when assessing for the presence of an open fracture and/or traumatic arthrotomy
Presence of swelling or effusion
Comprehensive neurovascular examination
How the patient carries their arm may give clues to the diagnosis.
Bony injuries
Supracondylar fracture
Flexion type
Patient supports injured forearm with other arm and elbow in 90º flexion
Loss of olecranon prominence
Extension type
Patient hold arm at side in S-type configuration
Soft tissue injuries
Elbow dislocations:
Posterior: abnormal prominence of olecranon
Anterior: loss of olecranon prominence
Radial head subluxation
Elbow slightly flexed and forearm pronated resists moving the arm at the elbow
Sensory and motor testing of the Median and Ulnar nerves
Median
Test for sensory function
Two-point discrimination over the tip of the index finger.
Test for motor function
“OK” sign with thumb and index finger and abduction of the thumb (recurrent branch)
Ulnar
Test for sensory function
Two-point discrimination of the little finger
Test for motor function
Abduct index finger against resistance
Compartment Syndrome
Acute compartment syndrome can usually develop over a few hours after a serious injury. Some symptoms of acute compartment syndrome are:
A new persistent deep pain
Pain that seems greater than expected for the severity of the injury
Numbness and tingling in the limb
Swelling, tightness and bruising
Radiological Test
Radiographic studies that are necessary for all patients presenting with varying degrees of elbow trauma include:
Anteroposterior (AP) elbow
Lateral elbow
Oblique views (optional, depending on fracture/injury)
Traction view (optional, can facilitate the assessment of comminuted fracture patterns)
Ipsilateral shoulder to wrist orthogonal views
Especially in the setting of high energy trauma or when exam and evaluation are limited
Fat pad sign
Seen with intra-articular injuries
Normally, anterior fat pad is a narrow radiolucent strip anterior to humerus
The posterior fat pad is normally not visible
Anterior fat pad sign indicates joint effusion/ injury when raised and becomes more perpendicular to the anterior humeral cortex (sail sign)
Posterior fat pad sign indicates effusion/injury
In adults, posterior fat pad sign without other obvious fracture implies radial head fracture
In children, it implies supracondylar fracture
Pediatric Considerations
Fractures in children often occur through unossified cartilage, making radiographic interpretation confusing
A line of mensuration drawn down the anterior surface of the humerus should always bisect the capitellum in lateral view.
If any bony relationship appears questionable on radiographs, obtain a comparison view of uninvolved elbow.
Suspect nonaccidental trauma if history does not tip injury.
Ossification centers: 1 appear: (CRITOE)
Capitellum 3 to 6 months
Radial head 3 to 5 years
Medial (Internal) epicondyle 5 to 7 years
Trochlea 9 to 10 years
Olecranon 9 to 10 years
Lateral Epicondyle
It is essential to do bilateral radiographic imaging in pediatric cases.
A nurse elbow can reduce spontaneously when the patient supinates the arm.
Advanced imaging sequences
Computerized tomography (CT) scans are often a consideration in the setting of comminuted fracture patterns for pre-operative surgical planning. Magnetic resonance imaging (MRI) can be an option in the setting of soft tissue and ligamentous injury evaluation, or when suspecting stress or occult fractures.[rx][rx][rx]
Alert
Based on the complex anatomy of the elbow, a few things require attention:
Neurovascular injuries to numerous structures that pass about the elbow, including anterior interosseous nerve, ulnar and radial nerves, brachial artery
Volkmann ischemic contracture is compartment syndrome of the forearm
Differential Diagnosis
It is important to remember all possible diagnoses including (but not limited to):
Fracture
Dislocation
Sprain
Strain
Ligamentous insufficiencies (e.g., UCL)
Bursitis
Tendinopathic conditions (acute or chronic)
Pediatric differential considerations include
Child abuse
Distal humeral physeal injuries
Nursemaids elbow
Fracture(s)
Avulsions
Monteggia fracture-dislocations
Physeal injuries/reactions
Treatment of Elbow Injuries
Doctors sometimes recommend very different treatments for both tennis elbow and golfer’s elbow. According to the studies done so far, the following treatments can help:
Rest, ice
Physical therapy when appropriate – Eccentric exercises for lateral epicondylitis
Braces/bandages – These are worn around the elbow or on the forearm to take the strain off the muscles.
Injections – Injections into the elbow with various substances, such as Botox, hyaluronic acid or autologous blood (the body’s own blood).
Extracorporeal shockwave therapy (ESWT) – A device generates shock or pressure waves that are transferred to the tissue through the skin. This is supposed to improve the circulation of blood in the tissue and speed up the healing process.
Laser therapy – The tissue is treated with concentrated beams of light. This is supposed to stimulate the circulation of blood and the body’s cell metabolism.
Stretching and strengthening exercises: Special exercises that stretch and strengthen the muscles of the arm and wrist.
Manual therapy – This includes active and passive exercises, as well as massages.
Ultrasound therapy – The arm is exposed to high-frequency sound waves. This warms the tissue, which improves the circulation of blood.
Transcutaneous electrical nerve stimulation (TENS) – TENS devices transfer electrical impulses to the nervous system through the skin. These are supposed to keep the pain signals from reaching the brain.
Acupuncture – The acupuncture needles are inserted into certain points on the surface of the arm. Here, too, the aim is to minimize the perception of pain.
Cold – The elbow is regularly cooled with ice packs.
Massages –A massage technique called “transverse friction massage” is often used to treat tennis elbow and golfer’s elbow. It is applied to the tendons and the muscles, using the tips of one or two fingers.
Emergency department treatment and procedures
Uncomplicated posterolateral dislocation usually treated with closed reduction. If there is evidence of entrapped medial epicondylar fragment, open reduction may be needed.[rx][rx]
Orthopedic consultation is the standard for all but nondisplaced, stable fractures, which as a rule, can be splinted 24 to 48 hours orthopedic follow-up
Fractures generally requiring orthopedic consultation:
Fractures involving articular surfaces such as capitellum or trochlea
Supracondylar fractures:
ED physician can handle type 1 with 24 to 48 hours orthopedic follow-up
The elbow may be flexed and splinted with a posterior splint
Types 2 and 3 require an immediate orthopedic consult
Reduce these in ED when the fracture is associated with vascular compromise
Anterior dislocation:
Reduce immediately if vascular structures compromised
Then flexed to 90º and place the posterior splint
Posterior dislocation:
Reduce immediately if vascular structures compromised
Then flexed 90º and place posterior splint.
Radial head fracture:
Minimally displaced fractures may need aspiration to remove hemarthrosis: instill bupivacaine and immobilize.
Other types should have an orthopedic consult.
Radial head subluxation
In one continuous motion, supinate and flex elbow while placing slight pressure on the radial head.
Hyper pronation technique is possibly more effective – while grasping the patient’s elbow, the wrist is hyper-pronated until feeling a palpable click.
A palpable click will often accompany the reduction
If the exam suggests fracture, but radiograph is negative, splint and have the patient follow up in 24 to 48 hours for re-evaluation
Medication
Conscious sedation is often necessary to achieve reductions
Painkillers – especially non-steroidal anti-inflammatory drugs (NSAIDs).
Injections – Steroid injections.
Ibuprofen – 600 to 800 mg (pediatric: 5 to 10 mg/kg) PO TID
Naprosyn – 250 to 500 mg (pediatric: 10 to 20 mg/kg) PO BID
Tylenol with codeine – 1 or 2 tabs (pediatric 0.5 to 1 mg/kg codeine) PO: do not exceed acetaminophen 4g/24 hours
Morphine sulfate – 0.1 mg/kg IV
Hydromorphone 5 mg/acetaminophen 300mg
Hydrocodone/acetaminophen – 1 to 2 tabs PO
Attritional injuries management modalities
Most of these injections contain one of the following active ingredients. These include but are not limited to[rx][rx][rx]:
Corticosteroid injection – when applicable
Platelet-rich plasma (PRP) considerations – 2016 study noted efficacy in managing UCL insufficiency
Steroids: reduce inflammation. Studies show that steroid injections can temporarily relieve pain. But there is also evidence that they can disrupt the healing process: People who were first given several steroid injections had more pain after a few months than people who didn’t receive any steroid injections. Frequent steroid injections carry the risk of tissue dying (atrophy), for instance, leaving a visible mark on the elbow.
Hyaluronic acid – A substance made by the body, found in tissue and joints. It is typically used to treat osteoarthritis. One study suggests that hyaluronic acid might be effective in the treatment of tennis elbow. But further research is needed to assess its pros and cons.
Botox – inhibits the sending of signals between the nerve cells. This has a paralyzing effect on the muscles. According to studies done on this so far, Botox can relieve the pain just a little at most. Also, Botox injections can have side effects like partial paralysis in the fingers that can last several weeks.
Autologous blood injections – Blood is taken from a vein in the arm and then injected into the elbow. This blood may be treated in different ways before it is injected. One common form of treatment with autologous blood is called platelet-rich plasma (PRP) therapy. It involves separating the blood into its various elements in a centrifuge. Then a concentrated solution of blood platelets is injected into the elbow. There is no evidence that treatment using autologous blood is effective.
Disposition
Admission Criteria
Vascular injuries, open fracture
Fractures requiring operative reduction or internal fixation.
Admit all patients with extensive swelling or ecchymosis for overnight observation and elevation to monitor for and decrease the risk for compartment syndrome.
Discharge Criteria
Stable fractures or reduced dislocations with none of the above features.
Splint and arrange orthopedic follow-up in 24 to 48 hours
Uncomplicated soft tissue injuries.
It is crucial to recall that prolonged elbow immobilization can cause stiffness to the patient, so the main goal is to get the elbow’s range of movement back as soon as possible.
Surgery
Different surgical approaches are used. Most of them involve detaching parts of the forearm muscles or separating and destroying the nerves that carry the pain signals.
Complications of Elbow Injuries
Complications of lateral epicondylitis can include recurrence of the injury when normal activity is resumed, rupture of the tendons with repeated steroid injections, and failure to improve conservative treatment.
Neuropraxia – This occurs because of nerve injury. It resolves in three to four months. Nerve injury occurs in 11% of supracondylar fractures. Most commonly injured is the interosseous nerve, followed by the radial, median, and ulnar nerves.[rx][rx]
The anterior interosseous nerve (arising from the median nerve) and may be involved either due to traction or contusion.
The radial nerve may be involved with posteromedial displacement
Median nerve involvement may occur with posterolateral displacement
Ulnar nerve involvement may occur with a flexion type supracondylar fracture. The ulnar nerve is most commonly involved due to posterior displacement of the proximal fragment.
Beware that motor testing can only identify anterior interosseous nerve injury. This testing can be done by flexing at the index finger distal interphalangeal and thumb interphalangeal joints and making the “okay” sign. Inability to do so represents a lack of sensory component in the anterior interosseous nerve.
Vascular injury – Brachial artery injury should always be suspected, particularly if the radial pulse is absent. However, vascular injury may occur even if the hand is pink and well perfused. This may be due to partial transection of a vessel.
Compartment syndrome – this may occur after a supracondylar fracture. Evaluate for the early or impending signs by determining if a radial pulse is absent. This injury results from prolonged ischemia of the forearm. It should be suspected if the following are present:
Inability to open the hand in children
Pain on passive extension of the fingers
Tenderness over the forearm
Absence of a radial pulse
A careful neurovascular examination is therefore important to promptly recognize this serious complication.
Malunion– Fracture malunion can lead to cubitus valgus or cubitus varus deformity (common in supracondylar fracture). A common complication is a loss of the carrying angle, which results in a cubitus varus, or “Gunstock,” deformity.
Nonunion – Lateral condylar fractures are more prone to nonunion. These, therefore, require revision surgery.
Postoperative complications can include the following:
Failing to address concomitant pathology
patients report inferior outcomes and lack of improvement if the primary cause of symptoms is not addressed; patients should be educated regarding the risks and benefits of surgery — the former include but are not limited to infection, blood loss, neurovascular injury, continued pain, stiffness, or continued or worsening overall dysfunction
radial nerve entrapment can be missed or not addressed clinically in up to 5% of patients being managed for lateral epicondylitis
Iatrogenic LUCL injury
occurs iatrogenically with increased risk if the surgical dissection extends beyond the radial head equator
postoperative iatrogenic posterolateral rotatory instability (PLRI) can develop if the extension or LUCL compromise is significant
Iatrogenic neurovascular injury
radial nerve injury
Heterotopic ossification
decrease risk with via copious saline irrigation following decortication and debridement