The Glasgow Coma Scale was first published in 1974 at the University of Glasgow by neurosurgery professors Graham Teasdale and Bryan Jennett. The Glasgow Coma Scale (GCS) is used to objectively describe the extent of impaired consciousness in all types of acute medical and trauma patients. The scale assesses patients according to three aspects of responsiveness: eye-opening, motor, and verbal responses. Reporting each of these separately provides a clear, communicable picture of a patient’s state.[rx]
Function
Scoring and Parameters
The Glasgow Coma Scale divides into three parameters: best eye response (E), best verbal response (V) and best motor response (M). The levels of response in the components of the Glasgow Coma Scale are ‘scored’ from 1, for no response, up to normal values of 4 (Eye-opening response) 5 ( Verbal response) and 6 (Motor response) The total Coma Score thus has values between three and 15, three being the worst and 15 being the highest.
The score is the sum of the scores as well as the individual elements. For example, a score of 10 might be expressed as GCS10 = E3V4M3.
Application of the Glasgow Coma Scale in Pediatrics
The Glasgow Coma Scale can be used in children older than 5 years with no modification. Younger children and infants are not able to provide the necessary verbal responses for the practitioner to use the scale to assess their orientation or obey the commands to evaluate their motor response. Since a Pediatric Glasgow Coma Scale was initially described in Adelaide, there have been several modifications without any particular one becoming universally accepted.[rx] The versions below derive from those of James and the Pediatric Emergency Care Applied Research Network[rx][rx]
Children less than 2 years old (pre-verbal) / Children greater than 2 years old (verbal)
Best eye response
No eye opening / 1 No eye-opening
Eye-opening to pain / 2 Eye-opening to pain
Eye-opening to sound / 3 Eye-opening to sound
Eyes open spontaneously / 4 Eyes open spontaneously
Best verbal response
None / 1 None
Moans in response to pain / 2 Incomprehensible sounds
Cries in response to pain / 3 Incomprehensible words
Irritable/cries / 4 Confused
Coos and babbles / 5 Orientated – appropriate
Best motor response
No motor response / 1 No motor response.
Abnormal extension to pain / 2 Abnormal extension to pain
Abnormal flexion to pain / 3 Abnormal flexion to pain
Withdrawal to pain / 4 Withdrawal to pain
Withdraws to touch / 5 Localises to pain
Moves spontaneously and purposefully / 6 Obeys commands
Issues of Concern
The following factors may interfere with the Glasgow Coma Scale assessment
Pre-existing factors
Language barriers
Intellectual or neurological deficit
Hearing loss or speech impediment
Effects of current treatment
Physical (e.g., intubation): If a patient is intubated and unable to speak, they are evaluated only on the motor and eye-opening response and the suffix T is added to their score to indicate intubation.
Pharmacological (e.g., sedation) or paralysis: If possible, the clinician should obtain the score before sedating the patient.
Effects of other injuries or lesions
Orbital/cranial fracture
Spinal cord damage
Hypoxic-ischemic encephalopathy after cold exposure
There are instances when the Glasgow Coma Scale is unobtainable despite efforts to overcome the issues listed above. It is essential that the total score is not reported without testing and including all of the components because the score will be low and could cause confusion.
Glasgow Coma Scale Pupils Score
The Glasgow Coma Scale Pupils Score (GCS-P) was described by Paul Brennan, Gordon Murray, and Graham Teasdale in 2018 as a strategy to combine the two key indicators of the severity of traumatic brain injury into a single simple index.[rx][rx]
Calculation of the GCS-P is by subtracting the Pupil Reactivity Score (PRS) from the Glasgow Coma Scale (GCS) total score:
GCS-P = GCS – PRS
The Pupil Reactivity Score is calculated as follows.
Pupils unreactive to light – Pupil Reactivity Score
Both pupils – 2
One pupil – 1
Neither pupil – 0
The GCS-P score can range from 1 and 15 and extends the range over which early severity can be shown to relate to outcomes of either mortality or independent recovery.
Classification of Severity of TBI
The relationship between the GCS Score and outcome l is the basis for a common classification of acute traumatic brain injury:
Severe, GCS 3 to 8
Moderate, GCS 9 to 12
Mild, GCS 13 to 15
With the GCS-P score values between one and 8 denote a severe injury.
Sacroiliac Joint Fracture/Sacroiliitis are common terms used to describe the pain of the sacroiliac joint. It is usually caused by abnormal motion (i.e. hyper- or hypo-mobile) or malalignment of the sacroiliac joint. The joint can be hyper or hypo-mobile which can cause pain. Pain is usually localized over the buttock. Patients usually describe the pain as sharp, dull, achy, stabbing, or shooting pain directly over the affected joint.
Sacroiliac joint (SIJ) pain refers to the pain arising from the SIJ joint structures. SIJ dysfunction generally refers to an aberrant position or movement of SIJ structures that may or may not result in pain. This paper aims to clarify the difference between these clinical concepts and present currently available evidence regarding the diagnosis and treatment of SIJ disorders.
Sacroiliitis is inflammation within the sacroiliac joint. It is a feature of spondyloarthropathies, such as axial spondyloarthritis (including ankylosing spondylitis), psoriatic arthritis, reactive arthritis or arthritis related to inflammatory bowel diseases, including ulcerative colitis or Crohn’s disease. It is also the most common presentation of arthritis from brucellosis.
Anatomy of Sacroiliac Joint Fracture
Six variants of the sacroiliac joints have been observed: accessory joints, iliosacral complex, bipartite iliac bony plate, crescent-like iliac bony plate, semicircular defects at the sacral or iliac side and ossification centers.
Accessory sacroiliac joint – Accessory sacroiliac joint is found medial to the posterior superior iliac spine and lateral to the second sacral foramen amongst a rudimentary transverse tuberosity. On CT imaging, accessory joints have articular surfaces that resemble osseous projects from the ilium to the sacrum. An accessory joint can be present at birth; however, they more commonly result from the stress of weight-bearing. Accessory joints are more commonly present in the obese population and the older population, as well as a higher prevalence in women with 3 or more childbirths, compared to 2 or less.
Iliosacral complex– Iliosacral complex forms from a projection from the ilium articulating with a complementary sacral recess. These complexes can be unilateral or bilateral, and like accessory joints, these complexes exist at the posterior sacroiliac joint from the level of first to the second sacral foramen. This variant has been seen more in older patients greater than 60 years, as well as obese women more so than normal-weight women.
Bipartite iliac bony plate – Bipartite iliac bony plate is located at the posterior portion of the sacroiliac joint and appears as described, consisting of two parts and appears unilaterally.
Semicircular defects on the iliac/sacral side – The fourth variant is semicircular defects on either the sacral or iliac aspects of the articular surface of the sacroiliac joint. These can be unilateral or bilateral and again are present at the posterior portion of the sacroiliac joint from the level of the first to the second sacral foramen. This defect has been observed more in women than men and in patients older than 60 years.
Crescent-like iliac bony plate– The fifth variant is a crescent-like articular surface which may be present unilaterally or bilaterally. CT imaging demonstrates a crescent-like iliac plate with accompanying a bulged sacral surface. This defect is found usually at the posterior portion of the sacral iliac joint spanning the levels of the first and second sacral foramen. This defect was observed only in women and more commonly in patients greater than 60 years old.
Ossification centers of the sacral wings – The sixth anatomical variant observed is ossification centers presenting as triangular osseous bodies located within the joint space at the anterior portion of the sacroiliac joint. This defect is found at the level of the first sacral foramen, typically unilaterally.[rx][rx]
Causes of Sacroiliac Joint Fracture
High energy trauma (e.g. MVA, falls) – can lead to pelvic ring injuries with a spectrum of injury to the SI joint ligaments
Ligament strain and/or stress or occult fractures
Degenerative arthritis
Degenerative conditions of the spine (most common causes)
Spondylolisthesis: in the degenerative setting, this occurs as a result of a pathologic cascade including intervertebral disc degeneration, ensuing intersegmental instability, and facet joint arthropathy
Spinal stenosis
Adult isthmic spondylolisthesis is typically caused by an acquired defect in the par interarticularis
Pars defects (i.e. spondylolisis) in adults are most often secondary to repetitive microtrauma
Trauma (e.g. burst fractures with bony fragment retropulsion)
Clinicians should recognize spinal fractures can occur in younger, healthy patient populations secondary to high-energy injuries (e.g. MVA, fall from height) or secondary low energy injuries and spontaneous fractures in the elderly populations, including any patient with osteoporosis
Associated hemorrhage from the injury can result in a deteriorating clinical and neurologic exam
Benign or malignant tumors
Metastatic tumors (most common)
Primary tumors
Ependymoma
Schwannoma
Neurofibroma
Lymphoma
Lipomas
Paraganglioma
Ganglioneuroma
Osteoblastoma
Infection
Osteodiscitis
Osteomyelitis
Epidural abscess
Fungal infections (e.g. Tuberculosis)
Other infections: lyme disease, HIV/AIDS-defining ilnesses, Herpes zoster (HZ)
Spondyloarthropathies such as Ankylosing spondylitis, reactive arthritis, psoriatic arthritis, and inflammatory bowel disease (Crohn disease and Ulcerative colitis) should be considered with sacroiliac joint pain especially those with systemic manifestations
Moderate impact exercise (e.g. lifting, jogging)
Secondary conditions
secondary to previous spinal fusion procedures
secondary to scoliosis and/or leg length discrepancy
Any form of spondyloarthropathies – which includes ankylosing spondylitis, psoriatic arthritis, reactive arthritis or arthritis related to inflammatory bowel diseases, including ulcerative colitis or Crohn’s disease.
Pregnancy – can cause inflammation as a result of the widening and stretching of the sacroiliac joints to prepare for childbirth. Additionally, the added weight carried during childbearing can put an extra amount of stress on the SI joints, leading to abnormal wear.
Symptoms of Sacroiliac Joint Fracture
Sciatic-like pain – in the buttocks and/or backs of the thighs that feels hot, sharp, and stabbing and may include numbness and tingling. Sciatic-like pain from sacroiliac joint dysfunction rarely extends below the knee.
Stiffness – and reduced range-of-motion in the lower back, hips, pelvis, and groin, which may cause difficulty with movements such as walking up stairs or bending at the waist.
Worsened pain – when putting added pressure on the sacroiliac joint, such as climbing stairs, running or jogging, and lying or putting weight on one side.
Instability – in the pelvis and/or lower back, which may cause the pelvis to feel like it will buckle or give way when standing, walking, or moving from standing to sitting.
The following are signs and symptoms that may be associated with an SI joint (SIJ) problem
Mechanical SIJ dysfunction usually causes a dull unilateral low back pain.[rx]
The pain is often a mild to moderate ache around the dimple or posterior superior iliac spine (PSIS) region.[rx]
The pain may become worse and sharp while doing activities such as standing up from a seated position or lifting the knee towards the chest during stair climbing.
Pain is typically on one side or the other (unilateral PSIS pain), but the pain can occasionally be bilateral.
When the pain of SIJ dysfunction is severe (which is infrequent), there can be referred pain into the hip, groin, and occasionally down the leg, but rarely does the pain radiate below the knee.
Pain can be referred from the SIJ down into the buttock or back of the thigh, and rarely to the foot.
Low back pain and stiffness, often unilateral, that often increases with prolonged sitting or prolonged walking.
Pain may occur during sexual intercourse; however, this is not specific to just sacroiliac joint problems.
In most clinical evaluations, common laboratory findings in the aseptic setting include:
WBC count – usually normal (elevated in infection/septic presentation)
ESR – elevated
CRP – elevated
HLA-B27 – About 1-2% of patients with ankylosing spondylitis will be HLA-B27 positive
Rheumatoid Factor (RF) – Negative in the setting of true ankylosing spondylitis
Special provocative tests can be very helpful in reproducing the patient’s pain:
“Fortin finger sign”- reproduction of pain after applying a deep palpation with the four-hand fingers posteriorly at the patient’s SI joint(s).
FABER test– reproduction of pain after flexing the hip while also abducting and externally rotating the hip.
Sacral distraction test– reproduction of pain after applying pressure to the anterior superior iliac spine.
Iliac compression test– reproduction of pain after applying pressure downward on the superior aspect of the iliac crest.Apply compression to the joint with the patient lying on his or her side. The pressure is applied downward to the uppermost iliac crest.[rx]
Gaenslen test– reproduction of pain after having the patient flex the hip on the unaffected side and then dangle the affected leg off the examining table. The pressure is then directed downward on the leg to extend further the hip, which causes stress on the SI joint.
Sacral thrust test– reproduction of pain with the patient prone and then applying an anterior pressure through the sacrum.
Iliac Gapping Test – Distraction can be performed to the anterior sacroiliac ligaments by applying pressure to the anterior superior iliac spine.[rx]
Patrick test – To identify if the pain may come from the sacroiliac joint during flexion, abduction, and external rotation, the clinician externally rotates the hip while the patient lies supine. Then, downward pressure is applied to the medial knee stressing both the hip and sacroiliac joint.[rx][rx][rx]
Thigh Thrust – This test applies anteroposterior shear stress on the SI joint. The patient lies supine with one hip flexed to 90 degrees. The examiner stands on the same side as the flexed leg. The examiner provides either a quick thrust or steadily increasing pressure through the line of the femur. The pelvis is stabilized at the sacrum or at the opposite ASIS with the hand of the examiner.
Palpation tests – in which deep thumb pressure is applied directly over the entire SI joint on each side. A positive test is a tenderness over the affected SI joint, which should then be correlated with other provocative tests. When several types of motion palpation tests are included with clusters of provocative tests such as those described above, the highest level of accuracy was found.
Radiological Imaging
X-rays – The first test typically performed and one that is very accessible at most clinics and outpatient offices. Three views (AP, lateral, and oblique) views help assess the overall alignment of the spine as well as for the presence of any degenerative or spondylotic changes.
CT Scan – This imaging is the most sensitive test to examine the bony structures of the spine. It can also show calcified sacroiliac joint dysfunction or any insidious process that may result in bony loss or destruction. In patients that are unable to or are otherwise ineligible to undergo an MRI, CT myelography can be used as an alternative to visualize a herniated disc.
MRI – The preferred imaging modality and the most sensitive study to visualize a herniated disc, as it has the most significant ability to demonstrate soft-tissue structures and the nerve as it exits the foramen and sacroiliac joint dysfunction
Electrodiagnostic testing – (Electromyography and nerve conduction studies) can be an option in patients that demonstrate equivocal symptoms or imaging findings as well as to rule out the presence of a peripheral mononeuropathy. The sensitivity of detecting cervical radiculopathy with electrodiagnostic testing ranges from 50% to 71%.[rx]
The contralateral (crossed) straight leg raise test – As in the straight leg raise test, the patient is lying supine, and the examiner elevates the asymptomatic leg. The test is positive if the maneuver reproduces the patient’s typical pain and paresthesia. The test has a specificity greater than 90%.
Myelography – An X-ray of the spinal canal following the injection of contrast material into the surrounding cerebrospinal fluid spaces will reveal the displacement of the contrast material. It can show the presence of structures that can cause pressure on the spinal cord or nerves, such as herniated discs, tumors, or bone spurs.
Transcranial Magnetic Stimulation (TMS) – The presence and severity of myelopathy can be evaluated by means of transcranial magnetic stimulation (TMS), a neurophysiological method that measures the time required for a neural impulse to cross the pyramidal tracts, starting from the cerebral cortex and ending at the anterior horn cells of the cervical, thoracic, or lumbar spinal cord and sacroiliac joint dysfunction. This measurement is called the central conduction time (CCT).
Electromyography and nerve conduction studies (EMG/NCS) – measure the electrical impulses along with nerve roots, peripheral nerves, and muscle tissue. Tests can indicate if there is ongoing nerve damage, if the nerves are in a state of healing from a past injury, or if there is another site of nerve compression. EMG/NCS studies are typically used to pinpoint the sources of nerve dysfunction distal to the spine.
Evaluating clinicians must first rule out associated “red flag” symptoms including
Thoracic pain
Fever/unexplained weight loss
Night sweats
Bowel or bladder dysfunction
Malignancy (document/record any previous surgeries, chemo/radiation, recent scans and bloodwork, and history of metastatic disease)
Can be seen in association with pain at night, pain at rest, unexplained weight loss, or night sweats
Significant medical comorbidities
Neurologic deficit or serial exam deterioration
Gait ataxia
Saddle anesthesia
Age of onset (bimodal — Age < 20 years or Age > 55 years)
Treatment of Sacroiliac Joint Fracture
Prehospital Management
Prehospital management of a suspected SI joint fracture should adhere to the following principles:
Read the mechanism of injury.
Ask the alert patient about the presence of pain in the pelvic, back or groin regions and routinely immobilize the pelvis if there is any positive reply.
The examination is unreliable (especially if reduced GCS, or distracting injuries) and the SI joint should not be palpated, to avoid further internal hemorrhage.
If there is any suspicion of SI joint fracture, immobilize the pelvis using an external compression splint (commercial or modified eg, sheet).
Use a scoop stretcher to facilitate the patient’s movement on to a spinal board or vacuum mattress for transport. In the emergency department, this process should be reversed.
Fluid resuscitation to maintain a radial pulse only.
Do not remove a pelvic splint in the presence of a suspected unstable pelvic injury until it is radiologically confirmed that there is no fracture or the patient is in a theatre.
Non-Surgical Treatment
Treatment available can be broadly
Skeletal traction – Available evidence suggests that treatment depends on the part of the SI joint that is fractured. Traction may be useful for SI joint fracture because it counteracts the force of the muscle pulling the two separated parts together, and thus may decrease bleeding and pain.[rx] Traction should not be used in the and SI joint fracture or when there is any other trauma to the leg or pelvis.[rx][rx] It is typically only a temporary measure used before surgery. [rx]
Get medical help immediately – If you fall on an outstretched arm, get into a car accident or are hit while playing a sport and feel intense pain in your hip area, then get medical care immediately. You’ll innately know that something is seriously wrong because you won’t be able to lift your leg up. Other symptoms include immediate swelling and/or bruising near the fracture, grinding sounds with arm movements and potential numbness, and tingling in the leg.
Apply ice – After you get home from the hospital SI joint fracture (regardless if you had surgery or not), you should apply a bag of crushed ice (or something cold) to your injured in order to reduce the swelling and numb the pain. Ice therapy is effective for acute (recent) injuries that involve swelling because it reduces blood flow by constricting local blood vessels. Apply the crushed ice to your radial head fractures for 15 minutes three to five times daily until the soreness and inflammation eventually fades away
Massages – Various massage techniques are used to relax muscles and ease tension.
Heating and cooling – This includes the use of hot packs and plasters, a hot bath, going to the sauna, or using an infrared lamp. Heat can also help relax tense muscles. Cold packs, like cold wraps or gel packs, are also used to help with irritated nerves.
Ultrasound therapy – Here the lower back is treated with sound waves. The small vibrations that are produced generate heat to relax body tissue.
Lumbar Manipulation – There is limited evidence suggesting that manipulation may provide short-term benefits for lumbar pain. Complications from manipulation are rare and can include worsening radiculopathy, myelopathy, spinal cord injury, and vertebral artery injury. These complications occur ranging from 5 to 10 per 10 million manipulations.
Lumbar Corset or Collar for Immobilization – In patients with acute neck pain, a short course (approximately one week) of collar immobilization may be beneficial during the acute inflammatory period.
Supports or braces – When the SI joint is too loose (hypermobile), a pelvic brace can be wrapped around the waist and pulled snugly to stabilize the area. A pelvic brace is about the size of a wide belt and can be helpful when the joint is inflamed and painful.
Physical Therapy
Commonly prescribed after a short period of rest and immobilization. Modalities include a range of motion exercises, strengthening exercises, ice, heat, ultrasound, and electrical stimulation therapy. Despite their frequent use, no evidence demonstrates their efficacy over placebo. However, there is no proven harm, and with a possible benefit, their use is recommended in the absence of myelopathy.
Exercising in water – can be a great way to stay physically active when other forms of exercise are painful. Exercises that involve lots of twisting and bending may or may not benefit you. Your physical therapist will design an individualized exercise program to meet your specific needs.
Weight-training exercises – though very important, need to be done with proper form to avoid stress to the back.
Reduce pain and other symptoms – Your physical therapist will help you understand how to avoid or modify the activities that caused the injury, so healing can begin. Your physical therapist may use different types of treatments and technologies to control and reduce your pain and symptoms.
Improve posture –If your physical therapist finds that poor posture has contributed to your SI joint, the therapist will teach you how to improve your posture so that pressure is reduced in the injured area, and healing can begin and progress as rapidly as possible.
Improve motion – Your physical therapist will choose specific activities and treatments to help restore normal movement in any stiff joints/ sacroiliitis. These might begin with “passive” motions that the physical therapist performs for you to move your spine, and progress to “active” exercises and stretches that you do yourself. You can perform these motions at home and in your workplace to help hasten healing and pain relief.
Improve flexibility – Your physical therapist will determine if any of the involved muscles are tight, start helping you to stretch them, and teach you how to stretch them at home.
Improve strength – If your physical therapist finds any weak or injured muscles, your physical therapist will choose, and teach you, the correct exercises to steadily restore your strength and agility. For neck and back disc herniations, “core strengthening” is commonly used to restore the strength and coordination of muscles around your back, hips, abdomen, and pelvis.
Improve endurance – Restoring muscular endurance is important after an injury. Your physical therapist will develop a program of activities to help you regain the endurance you had before the injury, and improve it.
Learn a home program – Your physical therapist will teach you strengthening, stretching, and pain-reduction exercises to perform at home. These exercises will be specific for your needs; if you do them as prescribed by your physical therapist, you can speed your recovery.
Eat Nutritiously During Your Recovery
All bones and tissues in the body need certain nutrients in order to heal properly and in a timely manner. Eating a nutritious and balanced diet that includes lots of minerals and vitamins are proven to help heal broken bones of all types. Therefore focus on eating lots of fresh produce (fruits and veggies), whole grains, lean meats, and fish to give your body the building blocks needed to properly repair your. In addition, drink plenty of purified water, milk, and other dairy-based beverages to augment what you eat.
Broken bones need ample minerals (calcium, phosphorus, magnesium, boron) and protein to become strong and healthy again.
Excellent sources of minerals/protein include dairy products, tofu, beans, broccoli, nuts and seeds, sardines, and salmon.
Important vitamins that are needed for bone healing include vitamin C (needed to make collagen), vitamin D (crucial for mineral absorption), and vitamin K (binds calcium to bones and triggers collagen formation).
Conversely, don’t consume food or drink that is known to impair bone/tissue healing, such as alcoholic beverages, sodas, most fast food items, and foods made with lots of refined sugars and preservatives.
Non-steroidal anti-inflammatory drugs (NSAIDs) – These painkillers belong to the same group of drugs as acetylsalicylic acid (ASA, the drug in medicines like “Aspirin”). NSAIDs that may be an option for the treatment of sciatica include diclofenac, ibuprofen, and naproxen. Anti-inflammatory drugs are drugs that reduce inflammation. This includes substances produced by the body itself like cortisone. It also includes artificial substances like ASA – acetylsalicylic acid (or “aspirin”) or ibuprofen –, which relieve pain and reduce fever as well as reducing inflammation.
Acetaminophen (paracetamol) – Acetaminophen (paracetamol) is also a painkiller, but it is not an NSAID. It is well tolerated and can be used as an alternative to NSAIDs – especially for people who do not tolerate NSAID painkillers because of things like stomach problems or asthma. But higher doses of acetaminophen can cause liver and kidney damage. The package insert advises adults not to take more than 4 grams (4000 mg) per day. This is the amount in, for example, 8 tablets containing 500 milligrams each. It is not only important to take the right dose, but also to wait long enough between doses.
Opioids – Strong painkillers that may only be used under medical supervision. Opioids are available in many different strengths, and some are available in the form of a patch. Morphine, for example, is a very strong drug, while tramadol is a weaker opioid. These drugs may have a number of different side effects, some of which are serious.
Skeletal Muscle relaxant – If muscle spasms are prominent, the addition of a muscle relaxant may merit consideration for a short period. For example, cyclobenzaprine is an option at a dose of 5 mg taken orally three times daily. Antidepressants (amitriptyline) and anticonvulsants (gabapentin and pregabalin) have been used to treat neuropathic pain, and they can provide a moderate analgesic effect.
Steroids – Anti-inflammatory drugs that can be used to treat various diseases systemically. That means that they are taken as tablets or injected. The drug spreads throughout the entire body to soothe inflammation and relieve pain. Steroids may increase the risk of gastric ulcers, osteoporosis, infections, skin problems, glaucoma, and glucose metabolism disorders.
Muscle relaxants – Sedatives which also relax the muscles. Like other psychotropic medications, they can cause fatigue and drowsiness, and affect your ability to drive. Muscle relaxants can also affect liver functions and cause gastro-intestinal complications. Drugs from the benzodiazepine group, such as tetrazepam, can lead to dependency if they are taken for longer than two weeks.
Anticonvulsants – These medications are typically used to treat epilepsy, but some are approved for treating nerve pain (neuralgia). Their side effects include drowsiness and fatigue. This can affect your ability to drive.
Antidepressants – These drugs are usually used for treating depression. Some of them are also approved for the treatment of pain. Possible side effects include nausea, dry mouth, low blood pressure, irregular heartbeat, and fatigue.
Topical Medications – These prescription-strength creams, gels, ointments, patches, and sprays help relieve pain and inflammation through the skin.
Calcium & vitamin D3 – to improve bone health and healing fracture. As a general rule, men and women age 50 and older should consume 1,200 milligrams of calcium a day, and 600 international units of vitamin D a day.
Glucosamine & Diacerein, Chondroitin sulfate – can be used to tightening the loose tension, cartilage, ligament, and cartilage, ligament regenerate cartilage or inhabit the further degeneration of cartilage, ligament
Injections – Injection therapy uses mostly local anesthetics and/or anti-inflammatory medications like corticosteroids (for example cortisone). These drugs are injected into the area immediately surrounding the affected nerve root.
Surgical and other procedures
If other methods haven’t relieved your pain, you doctor might suggest:
Joint injections – Corticosteroids can be injected into the joint to reduce inflammation and pain. You can get only a few joint injections a year because the steroids can weaken your joint’s bones and tendons.
Radiofrequency denervation – Radiofrequency energy can damage or destroy the nerve tissue causing your pain.
Electrical stimulation – Implanting an electrical stimulator into the sacrum might help reduce pain caused by sacroiliitis.
Joint fusion – Although surgery is rarely used to treat sacroiliitis, fusing the two bones together with metal hardware can sometimes relieve sacroiliitis pain.
Prevention
A positive attitude, regular activity, and a prompt return to work are all very important elements of recovery. If regular job duties cannot be performed initially, modified (light or restricted) duty may be prescribed for a limited time.
Prevention is key to avoiding recurrence
Proper lifting techniques
Good posture during sitting, standing, moving, and sleeping
Spondylolisthesis and Pars Fractures/Lumbar degenerative spondylolisthesis/Pars Interarticularis Defect (otherwise referred to as spondylolysis) represents a common cause of axial back pain in adolescents, especially in the case of young athletes. The pars interarticularis (pars) lies between the superior and inferior articular process bilaterally at each vertebral level. Anatomically, one can describe the pars as the region between two, one superior and one inferior, zygapophyseal joints. The definition of pars interarticularis defect is a unilateral or bilateral overuse or fatigue stress fracture involving the pars interarticularis of the posterior vertebral arch. This injury occurs almost exclusively in the lower lumbar region, most often at L5 [rx].
Spondylolysis is a unilateral or bilateral defect in the region of the pars interarticularis, which may or may not be accompanied by vertebral displacement, and is most commonly the result of repetitive trauma to the growing immature skeleton of a genetically susceptible individual. [rx][rx][rx] The pars interarticularis is considered the isthmus or bone bridge between the inferior and superior articular surfaces of a single vertebra. [rx][rx][rx]
Types of Spondylolisthesis and Pars Fractures
Injury of the pars interarticularis is among the most common causes of low back pain, especially in adolescent athletes. Sometimes these lesions develop in an asymptomatic manner, and they are detected in adulthood when the injury becomes chronic and symptomatic.[rx]
The spectrum of pathologies in the pars interarticularis ranges from bone stress, pars fracture (spondylolysis) to isthmic spondylolisthesis, which represents an anterior vertebral slippage. Bone stress is considered the earliest sign of disease. Repetitive bone stress causes bone remodeling and may result in spondylolysis, a non-displaced fracture of the pars interarticularis.[rx] Also, radiographically visualized spondylolysis is associated with spondylolisthesis about 25% of cases.[rx][rx]
Spondylolisthesis, a related condition to spondylolysis, is defined by the forward displacement of the upper vertebra relative to the caudal vertebra. In 1976 Wiltse et al.[rx] classified spondylolisthesis into five types:
Type I or dysplastic – is attributed to congenital dysplasia of the superior articular process of the sacrum.
Type II or isthmic – is due to a lesion in the pars interarticularis; these subclassify as:
(a) Lytic, when a fatigue pars fracture is present
(b) Pars elongation due to multiple healed stress fractures
(c) Acute pars fracture
Type III or degenerative – originates from facet instability without a pars fracture.
Type IV or traumatic – the displacement is due to an acute posterior arch fracture other than pars.
Type V or pathological – is due to posterior vertebral arch bone disease.[rx]
Type VI or iatrogenic – it is a potential sequel to spinal surgery.
For this activity, the focus will be on type II or isthmic spondylolisthesis.
Spondylolisthesis was classified by Meyerding et al. [rx] in five subtypes according to the magnitude of slippage on plain lateral lumbar radiograph measured in accordance to the inferior vertebra.
Grade I, less than 25% of displacement,
Grade II, between 25 and 50%,
Grade III, between 50 and 75%,
Grade IV, between 75 and 100% and
Grade V or spondyloptosis, when there is no contact between the vertebrae endplates. The commonly used Grade V, representing more than a 100% slip or spondyloptosis, is not part of the original grading system.
The majority of pars lesions or spondylolysis occur at L5 (85 to 95%), with L4 being the second most commonly affected vertebra (5 to 15%). The other lumbar levels are less often affected.[rx][rx][rx][rx][rx] The defect is unilateral in 22% of the cases.
Causes of Pars Interarticularis Defect
These sports include gymnastics and dance as the highest prevalence with an increased incidence also seen in football (particularly linemen), rugby, wrestling, martial arts, soccer, basketball, cheerleading, pitching, golf, tennis, volleyball servers, weightlifting, and butterfly and breaststroke swimming.[rx][rx][rx][rx]
Pars defects (spondylolysis) subdivide into five categories according to the Wiltse-Newman Classification[rx]
Dysplastic – congenital abnormalities/attenuated pars (approximately 20%)
Isthmic – lesions in the pars resulting from a stress fracture or acute fractures (approximately 50%)
Type II-A: pars fatigue fracture
Type II-B: pars elongation due to a healed fracture
Type II-C: pars acute fracture
Degenerative – degeneration of the intervertebral discs that results in segmental instability and alterations of the articular processes
A traumatic – acute fracture that results in fractures to various regions of the neural arch
Pathological – bone disease such as tumors and infections that result in lesions to the pars
There are many causes of spondylolisthesis including congenital, degenerative, traumatic, pathologic, iatrogenic, and isthmic. Isthmic spondylolisthesis, which will be the topic of this discussion, refers to a defect in the pars interarticularis that then results in anterior subluxation over time, most commonly at L5-S1 followed by L4-5. The resulting anterior subluxation can produce back pain, central canal stenosis, and lateral recess or foraminal stenosis.
Symptoms of Lumbar Spondylolysis and Spondylolisthesis
Numbness or tingling – People who have a herniated disk often have radiating numbness or tingling in the body part served by the affected nerves.
Weakness – Muscles served by the affected nerves tend to weaken. This can cause you to stumble, or affect your ability to lift or hold items.
A general stiffening of the back and a tightening of the hamstrings, with a resulting change in both posture and gait.
A leaning-forward or semi-kyphotic posture may be seen, due to compensatory changes.
A “waddle” may be seen in more advanced causes, due to compensatory pelvic rotation due to decreased lumbar spine rotation.
A result of the change in gait is often a noticeable atrophy in the gluteal muscles due to lack of use.
Generalized lower-back pain may also be seen, with intermittent shooting pain from the buttocks to the posterior thigh, and/or lower leg via the sciatic nerve.
Pain in the neck, back, low back, arms, or legs
Inability to bend or rotate the neck or back
Numbness or tingling in the neck, shoulders, arms, hands, hips, legs, or feet
Weakness in the arms or legs
Limping when walking
Increased pain when coughing, sneezing, reaching, or sitting
Inability to stand up straight; being “stuck” in a position, such as stooped forward or leaning to the side
Difficulty getting up from a chair
Inability to remain in 1 position for a long period of time, such as sitting or standing, due to pain
Pain that is worse in the morning
This is a sharp, often shooting pain that extends from the buttock down the back of one leg. It is caused by pressure on the spinal nerve.
Numbness or a tingling sensation in the leg and/or foot
Weakness in the leg and/or foot
Diagnosis of Pars Interarticularis Defect
Physical Exam
The major components of the physical exam for spondylolisthesis consists of observation, palpation, and maneuvers. The most common finding is pain with lumbar extension. Neurological examination is often normal in patients with spondylolisthesis, but lumbosacral radiculopathy is commonly seen in patients with degenerate spondylolisthesis.[rx]
Observation
The patient should be observed walking and standing. Most patients present with a normal gait. An abnormal gait is often the sign of a high-grade case. A patient with high-grade spondylolisthesis may present with a posterior pelvic tilt causing a loss in the normal contour of the buttocks. An antalgic gait, rounded back and decreased hip extension, can result from severe pain.[rx][rx]
Palpation
Detection of spondylolisthesis by palpation is most often done by palpating for the spinous process.[rx] Each level of the lumbar spine should be palpated. Spinous process palpation by itself is not a definitive method for the detection of spondylolisthesis.[rx]
Maneuvers
Spinal range of motion testing – Range of motion limitations may be seen.
Lumbar hyperextension – Extension often elicits pain. This can be assessed by having the patient hyperextend the lumbar spine, provide resistance against back extensions, or undergo repeated lumbar extensions.
Sport-specific motion – Patients can be asked to repeat aggravating movements that they experience during their activity. During the movement, ask the patient to point to any places with focal pain.
Straight leg raise – Maneuver used to assess for hamstring tightness. The straight leg raise has been found to be positive in only 10% of patients with spondylolisthesis.[rx]
Muscle strength exercises – Lower abdominal, gluteal, and lumbar extensors should be assessed for weakness. Weakness in these muscles can increase lordosis and contribute to sacroiliac instability.[rx] Abdominal flexor strength can be assessed with the abdominal flexor endurance test. The test involves the patient lying supine while holding a 45 degree flexed trunk and 90 degree flexed knees for 30 seconds. Gluteal strength can be assessed with a single leg squat. Lastly, a lumbar extension can be assessed with a single leg bridge.
Imaging
Scintigraphy – is an excellent screening tool for low back pain in children or adolescents. It has shown high sensitivity for the detection of acute injuries and bone stress reaction in the pars. However, some lesions may not display an increased contrast uptake.
Computed tomography scan (CT) – may be helpful in some cases due to its higher specificity. The tomographic finding of an acute injury include the margin reabsorption in the pars; pars sclerosis may indicate chronic stress, and marginal sclerosis with widening may indicate a chronic condition.
Magnetic resonance imaging (MRI) – offers advantages in terms of visualizing other types of pathology present in the lumbar spine and may potentially detect pars edema secondary to stress in their clinical course.[rx] The lack of ionizing radiation with MRI may also make it a particularly desirable modality for studying pars lesions, especially in the female adolescent population.[rx]
Electrodiagnostic testing – (Electromyography and nerve conduction studies) can be an option in patients that demonstrate equivocal symptoms or imaging findings as well as to rule out the presence of a peripheral mononeuropathy. The sensitivity of detecting cervical radiculopathy with electrodiagnostic testing ranges from 50% to 71%.[rx]
The straight leg raise test – With the patient lying supine, the examiner slowly elevates the patient’s led at an increasing angle, while keeping the leg straight at the knee joint. The test is positive if it reproduces the patient’s typical pain and paresthesia.[rx]
The contralateral (crossed) straight leg raise test – As in the straight leg raise test, the patient is lying supine, and the examiner elevates the asymptomatic leg. The test is positive if the maneuver reproduces the patient’s typical pain and paresthesia. The test has a specificity greater than 90%.
Myelography – An X-ray of the spinal canal following the injection of contrast material into the surrounding cerebrospinal fluid spaces will reveal the displacement of the contrast material. It can show the presence of structures that can cause pressure on the spinal cord or nerves, such as herniated discs, tumors, or bone spurs.
Treatment of Lumbar Spondylolysis and Spondylolisthesis
There is insufficient evidence to support the natural course or treated pars defect as the preferred management. Management generally reflects the following treatment algorithm. [rx][rx][rx]
Physical therapy plus activity restriction
Symptomatic spondylolysis (type II)
Symptomatic low-grade spondylolisthesis
Physical therapy program for 6 months and include
Hamstring stretching
Pelvic tilts
Core strengthening
TLSO bracing for 6 to 12 weeks
Acute pars stress reaction
Spondylolysis (type II) that has failed to improve with physical therapy
Low-grade spondylolisthesis that has failed to improve with physical therapy
Brace immobilization is superior to activity restriction alone for acute stress reaction
Non-Pharmacological Treatment
Conservative Treatments – Acute cervical or lumbar radiculopathies secondary to pars interarticularis injury a are typically managed with non-surgical treatments as the majority of patients (75 to 90%) will improve. Modalities that can be used include[rx][rx][rx]:
Rest the area by avoiding any activity that causes worsening symptoms in the arms or legs.
Stay active around the house, and go on short walks several times per day. The movement will decrease pain and stiffness and help you feel better.
Apply ice packs to the affected area for 15 to 20 minutes every 2 hours.
Sit in firm chairs. Soft couches and easy chairs may make your problems worse.
Deep tissue massage may be helpful
Acupuncture – In acupuncture, the therapist inserts fine needles into certain points on the body with the aim of relieving pain.
Reiki – Reiki is a Japanese treatment that aims to relieve pain by using specific hand placements.
Moxibustion – This method is used heat specific parts of the body (called “therapy points”) by using glowing sticks made of mugwort (“Moxa”) or heated needles that are put close to the therapy points.
Massages – Various massage techniques are used to relax muscles and ease tension.
Heating and cooling – This includes the use of hot packs and plasters, a hot bath, going to the sauna, or using an infrared lamp. Heat can also help relax tense muscles. Cold packs, like cold wraps or gel packs, are also used to help with irritated nerves.
Ultrasound therapy – Here the lower back is treated with sound waves. The small vibrations that are produced generate heat to relax body tissue.
Cervical Manipulation – There is limited evidence suggesting that cervical manipulation may provide short-term benefits for neck pain and pars interarticularis injury. Complications from manipulation are rare and can include worsening radiculopathy, myelopathy, spinal cord injury, and vertebral artery injury. These complications occur ranging from 5 to 10 per 10 million manipulations.
Lumbar Corset or Collar for Immobilization – In patients with acute neck pain, a short course (approximately one week) of collar immobilization may be beneficial during the acute inflammatory period.
Traction – May be beneficial in reducing the radicular symptoms associated with pars interarticularis injury. Theoretically, traction would widen the neuroforamen and relieve the stress placed on the affected nerve, which, in turn, would result in the improvement of symptoms. This therapy involves placing approximately 8 to 12 lbs of traction at an angle of approximately 24 degrees of neck flexion over a period of 15 to 20 minutes.
Physical Therapy
Commonly prescribed after a short period of rest and immobilization. Modalities include a range of motion exercises, strengthening exercises, ice, heat, ultrasound, and electrical stimulation therapy. Despite their frequent use, no evidence demonstrates their efficacy over placebo. However, there is no proven harm, and with a possible benefit, their use is recommended in the absence of myelopathy.
Exercising in water – can be a great way to stay physically active when other forms of exercise are painful. Exercises that involve lots of twisting and bending may or may not benefit you. Your physical therapist will design an individualized exercise program to meet your specific needs.
Weight-training exercises – though very important, need to be done with proper form to avoid stress to the back and neck.
Reduce pain and other symptoms – Your physical therapist will help you understand how to avoid or modify the activities that caused the injury, so healing can begin. Your physical therapist may use different types of treatments and technologies to control and reduce your pain and symptoms.
Improve posture –If your physical therapist finds that poor posture has contributed to your herniated disc, the therapist will teach you how to improve your posture so that pressure is reduced in the injured area, and healing can begin and progress as rapidly as possible.
Improve motion – Your physical therapist will choose specific activities and treatments to help restore normal movement in any stiff joints. These might begin with “passive” motions that the physical therapist performs for you to move your spine, and progress to “active” exercises and stretches that you do yourself. You can perform these motions at home and in your workplace to help hasten healing and pain relief.
Improve flexibility – Your physical therapist will determine if any of the involved muscles are tight, start helping you to stretch them, and teach you how to stretch them at home.
Improve strength – If your physical therapist finds any weak or injured muscles, your physical therapist will choose, and teach you, the correct exercises to steadily restore your strength and agility. For neck and back disc herniations, “core strengthening” is commonly used to restore the strength and coordination of muscles around your back, hips, abdomen, and pelvis.
Improve endurance – Restoring muscular endurance is important after an injury. Your physical therapist will develop a program of activities to help you regain the endurance you had before the injury, and improve it.
Learn a home program – Your physical therapist will teach you strengthening, stretching, and pain-reduction exercises to perform at home. These exercises will be specific for your needs; if you do them as prescribed by your physical therapist, you can speed your recovery.
Eat Nutritiously During Your Recovery
All bones and tissues in the body need certain nutrients in order to heal properly and in a timely manner. Eating a nutritious and balanced diet that includes lots of minerals and vitamins are proven to help heal broken bones of all types. Therefore focus on eating lots of fresh produce (fruits and veggies), whole grains, lean meats, and fish to give your body the building blocks needed to properly repair your. In addition, drink plenty of purified water, milk, and other dairy-based beverages to augment what you eat.
Broken bones need ample minerals (calcium, phosphorus, magnesium, boron) and protein to become strong and healthy again.
Excellent sources of minerals/protein include dairy products, tofu, beans, broccoli, nuts and seeds, sardines, and salmon.
Important vitamins that are needed for bone healing include vitamin C (needed to make collagen), vitamin D (crucial for mineral absorption), and vitamin K (binds calcium to bones and triggers collagen formation).
Conversely, don’t consume food or drink that is known to impair bone/tissue healing, such as alcoholic beverages, sodas, most fast food items, and foods made with lots of refined sugars and preservatives.
Medication
Pharmacotherapy – There is no evidence to demonstrate the efficacy of non-steroidal anti-inflammatories (NSAIDs) in the treatment of cervical radiculopathy. However, they are commonly used and can be beneficial for some patients. The use of COX-1 versus COX-2 inhibitors does not alter the analgesic effect, but there may be decreased gastrointestinal toxicity with the use of COX-2 inhibitors. Clinicians can consider steroidal anti-inflammatories (typically in the form of prednisone) in severe acute pain for a short period. A typical regimen is prednisone 60 to 80 mg/day for five days, which can then be slowly tapered off over the following 5 m to 14 days. Another regimen involves a prepackaged tapered dose of Methylprednisolone that tapers from 24 mg to 0 mg over 7 days.
Non-steroidal anti-inflammatory drugs (NSAIDs) – These painkillers belong to the same group of drugs as acetylsalicylic acid (ASA, the drug in medicines like “Aspirin”). NSAIDs that may be an option for the treatment of sciatica include diclofenac, ibuprofen, and naproxen. Anti-inflammatory drugs are drugs that reduce inflammation. This includes substances produced by the body itself like cortisone. It also includes artificial substances like ASA – acetylsalicylic acid (or “aspirin”) or ibuprofen –, which relieve pain and reduce fever as well as reducing inflammation.
Acetaminophen (paracetamol) – Acetaminophen (paracetamol) is also a painkiller, but it is not an NSAID. It is well tolerated and can be used as an alternative to NSAIDs – especially for people who do not tolerate NSAID painkillers because of things like stomach problems or asthma. But higher doses of acetaminophen can cause liver and kidney damage. The package insert advises adults not to take more than 4 grams (4000 mg) per day. This is the amount in, for example, 8 tablets containing 500 milligrams each. It is not only important to take the right dose, but also to wait long enough between doses.
Opioids – Strong painkillers that may only be used under medical supervision. Opioids are available in many different strengths, and some are available in the form of a patch. Morphine, for example, is a very strong drug, while tramadol is a weaker opioid. These drugs may have a number of different side effects, some of which are serious.
Skeletal Muscle relaxant – If muscle spasms are prominent, the addition of a muscle relaxant may merit consideration for a short period. For example, cyclobenzaprine is an option at a dose of 5 mg taken orally three times daily. Antidepressants (amitriptyline) and anticonvulsants (gabapentin and pregabalin) have been used to treat neuropathic pain, and they can provide a moderate analgesic effect.
Steroids – Anti-inflammatory drugs that can be used to treat various diseases systemically. That means that they are taken as tablets or injected. The drug spreads throughout the entire body to soothe inflammation and relieve pain. Steroids may increase the risk of gastric ulcers, osteoporosis, infections, skin problems, glaucoma, and glucose metabolism disorders.
Muscle relaxants – Sedatives which also relax the muscles. Like other psychotropic medications, they can cause fatigue and drowsiness, and affect your ability to drive. Muscle relaxants can also affect liver functions and cause gastro-intestinal complications. Drugs from the benzodiazepine group, such as tetrazepam, can lead to dependency if they are taken for longer than two weeks.
Anticonvulsants – These medications are typically used to treat epilepsy, but some are approved for treating nerve pain (neuralgia). Their side effects include drowsiness and fatigue. This can affect your ability to drive.
Antidepressants – These drugs are usually used for treating depression. Some of them are also approved for the treatment of pain. Possible side effects include nausea, dry mouth, low blood pressure, irregular heartbeat, and fatigue.
Topical Medications – These prescription-strength creams, gels, ointments, patches, and sprays help relieve pain and inflammation through the skin.
Calcium & vitamin D3 – to improve bone health and healing fracture. As a general rule, men and women age 50 and older should consume 1,200 milligrams of calcium a day, and 600 international units of vitamin D a day.
Glucosamine & Diacerein, Chondroitin sulfate – can be used to tightening the loose tension, cartilage, ligament, and cartilage, ligament regenerate cartilage or inhabit the further degeneration of cartilage, ligament
Injections near the spine – Injection therapy uses mostly local anesthetics and/or anti-inflammatory medications like corticosteroids (for example cortisone). These drugs are injected into the area immediately surrounding the affected nerve root. There are different ways of doing this:
In lumbar spinal nerve analgesia (LSPA) – the medication is injected directly at the point where the nerve root exits the spinal canal. This has a numbing effect on the nerve root.
In lumbar epidural analgesia – the medication is injected into what is known as the epidural space (“epidural injection”). The epidural space surrounds the spinal cord and the spinal fluid in the spinal canal. This is also where the nerve roots are located. During this treatment, the spine is monitored using computer tomography or X-rays to make sure that the injection is placed at exactly the right spot.
Interventional Treatments – Spinal steroid injections are a common alternative to surgery. Perineural injections (translaminar and transforaminal epidurals, selective nerve root blocks) are an option with pathological confirmation by MRI. These procedures should take place under radiologic guidance.[rx]
Surgical treatment
There are no clear radiological or medical guidelines or indications for surgical interventions in degenerative spondylolisthesis.[rx] A minimum of three months of conservative management should be completed prior to considering surgical intervention.[rx] Three indications for potential surgical treatment are as follows: persistent or recurrent back pain or neurologic pain with a persistent reduction of quality of life despite a reasonable trial of conservative (non-operative) management, new or worsening bladder or bowel symptoms, or a new or worsening neurological deficit.[rx][rx]:
Pars defect that has failed nonoperative management
Multiple pars defects
Low-grade spondylolisthesis (Myerding grade I & II) that fails conservative treatment, is progressive, has neurologic deficits, or likely to progress
What Is Spinal Cord Injury?/Spinal Cord Injury, The spinal cord is a tubular structure composed of nervous tissue that extends from the brainstem and continuing distally before tapering at the lower thoracic/upper lumbar region as the conus medullaris. The spinal cord is anchored distally by the filum terminal, a fibrous extension of the pia mater anchoring the spinal cord to the coccyx.[rx] Protecting the spinal cord is the surrounding cerebrospinal fluid (CSF), supportive soft tissue membranes and meninges, and the osseous vertebral column.[rx]
Traumatic spinal cord injury (TSCI) is sudden forceful damage to the spinal nerves resulting in temporary or permanent paralysis, bladder and bowel dysfunction, and autonomic imbalance among other consequences [rx,rx]. A person with spinal cord injury is at immediate risk of respiratory and cardiac failure which may lead to death in the acute phase [rx]. Those who survive the acute phase faces a lifelong risk of secondary complications such as pressure ulcers, urinary tract infections, deep venous thrombosis, contractures, chronic pain, and spasms [rx,rx].
Trauma to the spinal cord may result from a road traffic accident (RTA), fall, assault and recreational or occupational accident [rx,rx]. The World Health Organization informs that up to 90% of all spinal cord lesions are due to trauma and that the leading cause globally is RTA [rx].
Anatomy of Spinal Cord
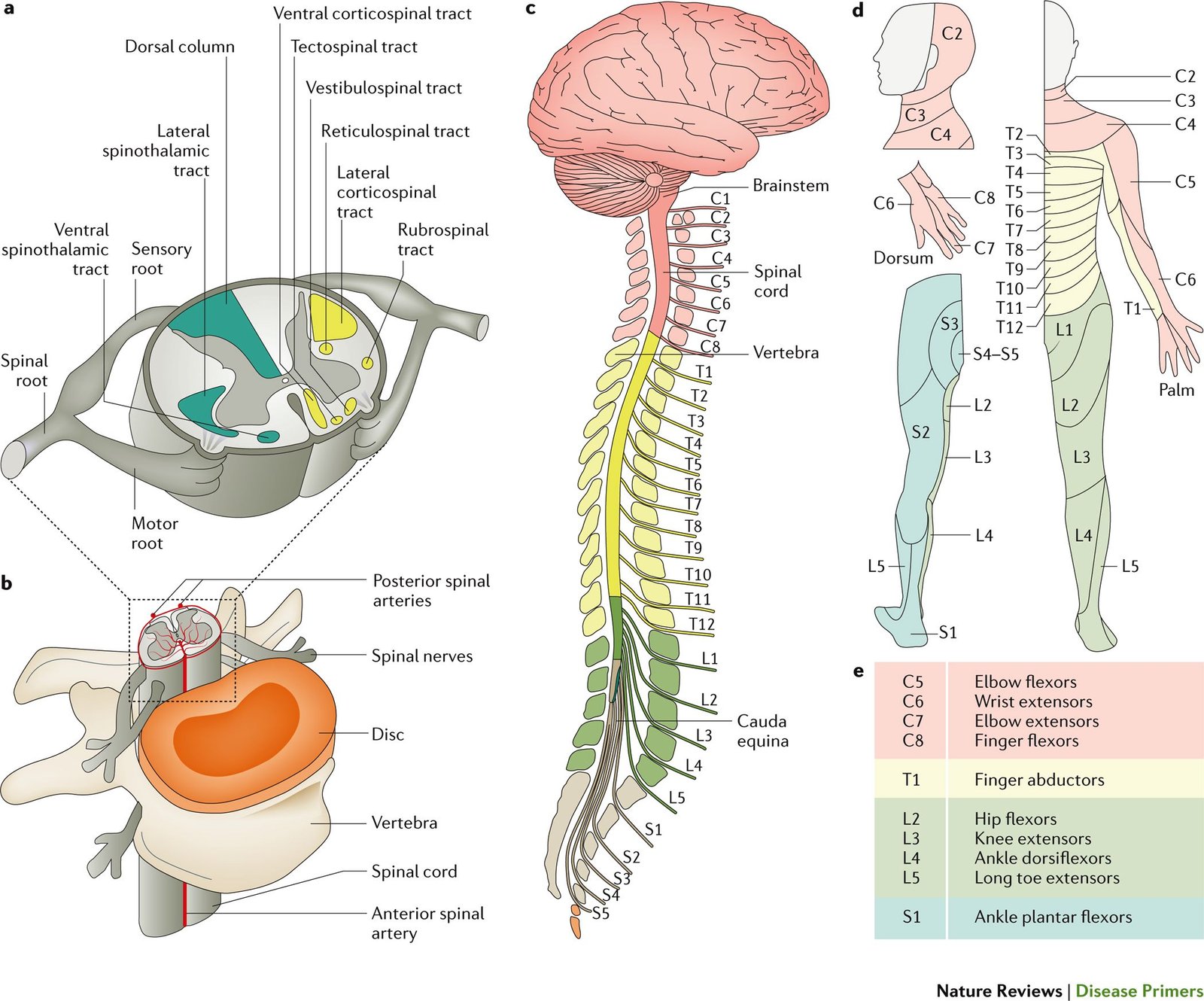
The major tracts and their most defining features are as follows
Ascending Tracts
Dorsal column – contains the gracile fasciculus and cuneate fasciculus, which together are the dorsal funiculus. The dorsal column is responsible for pressure and vibration sensation as well as two-point discrimination, movement sense, and conscious proprioception. The dorsal column decussates at the superior portion of the medulla oblongata and forms medial lemniscus.
Lateral spinothalamic – carries pain and temperature information. The lateral spinothalamic tract decussates at the anterior commissure two segments above the entry to the spinal cord.
Anterior spinothalamic – carries crude touch and pressure information. It decussates similar to the lateral spinothalamic tract.[rx]
Dorsal and ventral spinocerebellar – transmit unconscious proprioception sensory information to the cerebellum. The ventral spinocerebellar tract does not decussate, while the dorsal spinocerebellar tract decussates twice, making them both ipsilateral.[rx]
Descending Tracts
Lateral and anterior corticospinal – involved in conscious control of the skeletal muscle. The majority of lateral corticospinal tract fibers decussate at the inferior portion of the medulla oblongata while anterior corticospinal descends ipsilaterally in the spinal cord and decussates at the segmental level. Lateral corticospinal tract, also called pyramidal tract, innervates primarily contralateral muscles of the limbs, while anterior innervates proximal muscles of the trunk.
Vestibulospinal – carries information from the inner ear to control head positioning and is involved in modifying muscle tone to maintain posture and balance. The vestibulospinal tract does not decussate.
Rubrospinal – is involved in the movement of the flexor and extensor muscles. The rubrospinal tract originates from the red nuclei in the midbrain and decussates at the start of its pathway.
Reticulospinal – originates from the reticular formation housed in the brainstem and it facilitates, influences, and supplements the corticospinal tract.[rx] The reticulospinal tract does not decussate.
There is a laminar distribution of neurons in the gray matter, characterized by density and topography
Lamina I – is located at the tip of the dorsal horn and is composed of loosely packed neuropil along with neurons of low neuronal density. The most abundant neuron in lamina I is the Waldeyer cell: large, fusiform, and with a disk-shaped dendritic domain.[rx][rx]
Lamina II – is composed mostly of islet cells with rostrocaudal axes, which contain GABA and are thought to be inhibitory, and stalked cells with dorsoventral dendritic trees.[rx]
Lamina III – has cells of intermediate size, including antenna-like and radial neurons, many of which contain GABA or glycine and are also considered inhibitory.[rx][rx]
Lamina IV – contains antenna-like cells and transverse cells, with dendrites that mostly go to Laminas II and III, and whose axons are mainly thought to enter the spinothalamic tract. Lateral from lamina IV is the lateral spinal nucleus, which sends signals to lamina IV from the midbrain and brainstem.[rx][rx]
Lamina V and VI – are composed of medium-sized multipolar neurons, that can be fusiform or triangular. These neurons communicate with the reticular formation of the brainstem.
Lamina VII – is composed of homogenous medium-sized multipolar neurons, and contains, in individual segments, well-defined nuclei, including the intermediolateral nucleus (T1-L1), which has autonomic functions, and the dorsal nucleus of Clarke (T1-L2), which make up the dorsal spinocerebellar tract.
Lamina VIII – consists of neurons with dorsoventrally polarized dendritic trees.
Lamina IX – has the cell bodies of motor neurons, with dendrites extending dorsally into laminas as far as VI. Lamina IX – also has Renshaw cells, inhibitory interneurons, placed at the medial border of motor nuclei.
Lamina X – is the substantia grisea centralis or the gray matter that surrounds the central canal. In the distal portion, lamina X consists of bipolar cells with fan-shaped dendritic trees, and in the ventral portion, lamina X consists of bipolar cells with poorly ramified longitudinal dendrites.[rx]
Meninges and Spaces
Epidural space – fatty space between the bony framework of the spinal vertebral column and the thick dura mater surrounding the spinal cord. It contains adipose tissue and blood vessels.
Dura mater – Thick outermost covering (meninges) of the spinal cord, extending down to the level of the S2 vertebra
Arachnoid mater – The middle covering of the spinal cord
Subarachnoid space – Space between the arachnoid mater and the innermost covering of the spinal cord. It contains Cerebrospinal fluid.
Pia mater – The innermost covering of the spinal cord, intimately adhering to its surface, it stabilizes the spinal cord through lateral extensions of the pia called the denticulate ligaments, extending between the ventral and dorsal roots unto the dura mater.
Spinal cord
The length is about 45 cm in men and 43 cm in women[rx]
Anatomic course originates in the brainstem before coursing through the foramen magnum. The spinal cord continues distally through the cervical and thoracic regions of the spinal column before terminating as a tapered structure known as the conus medullaris
The spinal cord proper terminates at the L1-L2 vertebral level and is anchored distally via the filum terminale, representing an extension of the pia mater with fibrous attachments to the coccyx
The spinal cord comprises 5 segments, cervical, thoracic, lumbar, sacral and coccygeal
Long, cylindrical structure with varying levels of thickness/width depending on the corresponding vertebral levels
31 total nerve root segments
8 cervical
12 thoracic
5 lumbar
5 sacral
1 coccygeal
Cord width ranges – from 0.64-0.83 cm in the thoracic region to 1.27-1.33 cm in the cervical and lumbar regions
A 2016 systematic review of the literature demonstrated that, on average, the largest transverse diameter corresponded to the C5 neuronal segment (1.33 +/- 0.22 cm) and the smallest transverse diameter, on average, corresponded to the T8 segment (0.83 +/- 0.21 cm)[rx]
Enlarged regions of gray matter correspond to nerve root distribution to the upper and lower extremities
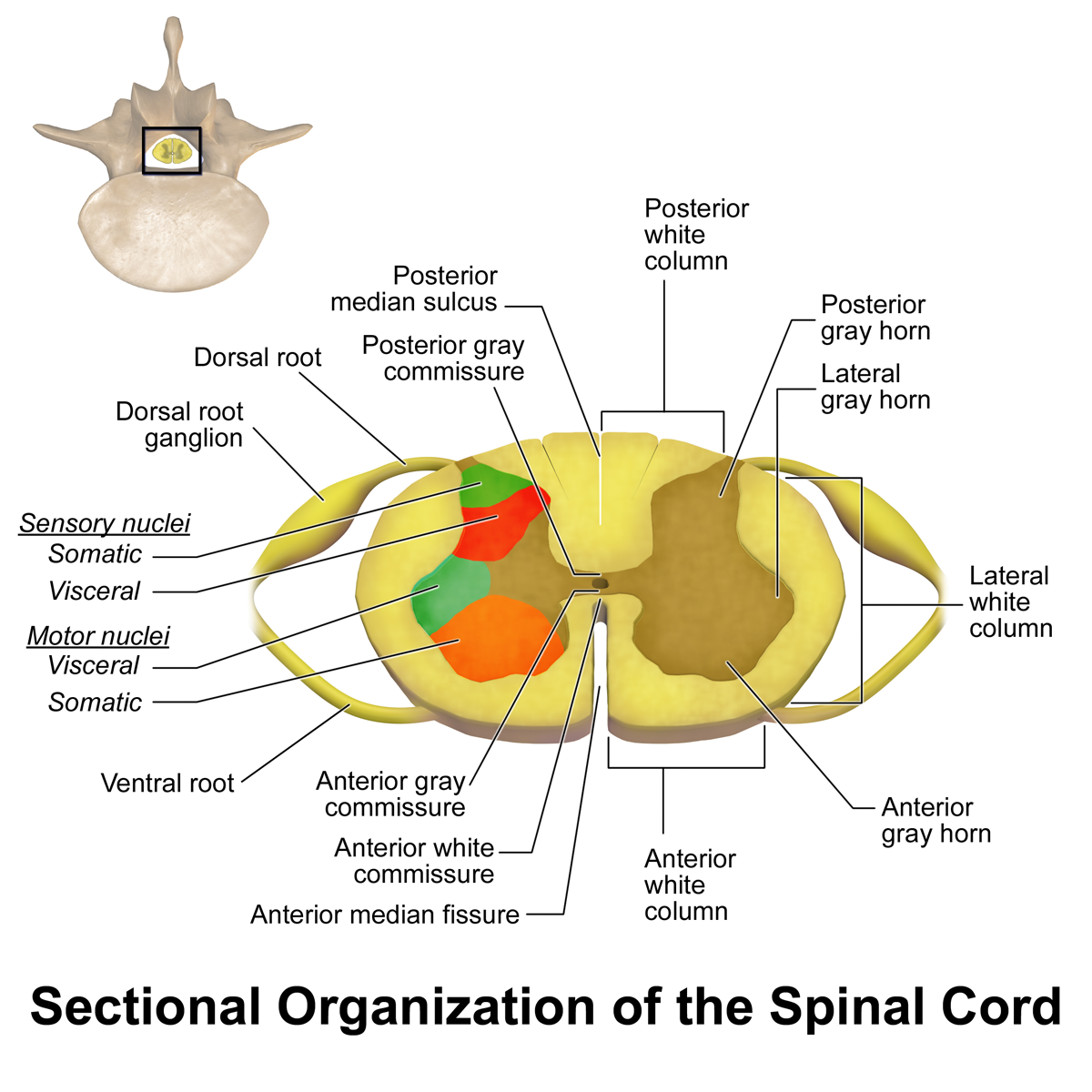
A cross-sectional –
Its view of the spinal cord shows its organization into the gray and white matter. The anterior aspect of the cord is identifiable with the presence of anterior median fissure. The gray matter is organized into an H- shaped body of cell bodies. The anterior horn comprises motor nuclei while the posterior horn comprises sensory nuclei.
The surrounding white matter is organized into anterior, posterior, and lateral columns (funiculi), from neuronal axons organized into tracts that convey neural messages back and forth the CNS (the ascending and descending tracts).
The anterolateral columns carry temperature and pain information, while the dorsal column communicates the sense of touch, proprioception, vibration. The cervical and thoracic spinal segments present an intermedio lateral gray horn which gives off preganglionic sympathetic fibers onto the sympathetic trunk on both sides of the spinal cord.
The spinal cord’s central canal
It is an extension of the 4th ventricle. It contains CSF, surrounding it is the gray commissure and the anterior white commissure. Decussation of the tracts of the white columns occurs at the anterior white commissure.
Types of Spinal Cord Injury
Incomplete Spinal Cord Injury
Tetraplegia
Cervical spine injury resulting in the impaired arm, trunk leg, pelvic organ function. These injuries, which are the result of damage to the cervical spinal cord, are typically the most severe, producing varying degrees of paralysis of all limbs. Sometimes known as quadriplegia, tetraplegia eliminates your ability to move below the site of the injury and may produce difficulties with bladder and bowel control, respiration, and other routine functions. The higher up on the cervical spinal cord the injury is, the more severe symptoms will likely be.
Paraplegia
This occurs when sensation and movement are removed from the lower half of the body, including the legs. These injuries are the product of damage to the thoracic spinal cord. As with cervical spinal cord injuries, injuries are typically more severe when they are closer to the top vertebra.
Thoracic/lumbar/sacral spinal injury leading to impaired trunk/leg/pelvic organ function
Preserved arm function.
Triplegia
Triplegia causes a loss of sensation and movement in one arm and both legs and is typically the product of an incomplete spinal cord injury.
Complete Injuries
By definition – complete SCI yields no sparing of the motor or sensory function below the injured level
The patient must have already recovered from the acute phase of spinal shock (usually 48 hours from presentation)
Spinal shock: by definition, the temporary (typically 48 hours) loss of all spinal cord function (including reflex activity) below the level of injury
Absent bulbocavernosus reflex
Flaccid paralysis
Bradycardia/hypotension
Spina bifida – Neural tube defect in which the neural tube does not completely close leaving a dorsal defect. Folate deficiency in early pregnancy is a risk factor.[rx] The severity of symptoms depends on the extent of the defect; myelomeningocele is the most severe variant with the spinal cord, meninges both exposed. Other variants include meningocele, which exposes only the meninges, and spina bifida occulta which is the mildest. Symptoms include loss of lower limb sensations, lower limb weakness, urinary incontinence, bowel incontinence
Spinal shock – is the temporary loss of spinal reflex activity with motor and sensory losses. This loss results from loss of sympathetic vascular tone resulting in paradoxical bradycardia with hypotension. During spinal shock, patients appear physiologically completely paralyzed but may show significant recovery after the initial phases of spinal shock have resolved.
Partial Complete spinal cord injuries (SCIs)
Central cord syndrome
This injury is an injury to the center of the cord, and damages nerves that carry signals from the brain to the spinal cord. Loss of fine motor skills, paralysis of the arms, and partial impairment—usually less pronounced—in the legs are common. Some survivors also suffer a loss of bowel or bladder control or lose the ability to sexually function.[rx]
Most common incomplete SCI
Pathophysiology: central gray matter injury
Mechanism(s): hyperextension (i.e., from a fall) in a patient with underlying cervical spinal canal stenosis
Clinical presentation:
Upper extremity loss of motor function (lower extremity motor function no affected/minimally affected)
Sensory sparing variable
Prognosis: Good
Anterior cord syndrome
This type of injury, to the front of the spinal cord, damages the motor and sensory pathways in the spinal cord. You may retain some sensation but struggle with movement.[rx]
Second most common incomplete SCI
Pathophysiology: injuries occur secondary to direct compression to the anterior spinal cord (e.g., hyperflexion injuries, anterior spinal artery occlusion, or disc prolapse)
Brown-Square syndrome – This variety of injury is the product of damage to one side of the spinal cord. The injury may be more pronounced on one side of the body; for instance, movement may be impossible on the right side but maybe fully retained on the left. The degree to which Brown-Sequard patients are injured greatly varies from patient to patient.[rx]
Pathophysiology: Injury to (only) the nerve roots of the cauda equina itself (i.e., spares the spinal cord itself)
Mechanism(s):
disc herniations
burst fractures (e.g., associated hematoma from trauma)
Clinical presentation:
bilateral buttock/lower extremity pain
bowel/bladder dysfunction (urinary retention)
saddle anesthesia
loss of lower extremity motor/sensory function
differentiated from conus medullaris syndrome in that findings are asymmetrical, as opposed to symmetrical (i.e. conus medullaris motor symptoms are symmetrical on presentation)
Prognosis: surgical decompression within the first 48 hours appears to yield improved overall outcomes (although the overall prognosis remains guarded)
Often confused with cauda equina syndrome, although this must be recognized as a separate clinical entity
Pathophysiology: injury to the spinal cord at L1-L2 level.
Mechanism(s):
Direct spinal trauma to the thoracolumbar junction[rx]
Clinical presentation:
Saddle anesthesia
bowel/bladder dysfunction (often presents with dysfunction more acutely compared to cauda equina which can evolve over a variable period time prior to the patient’s presentation)
classically presents with mild, symmetrical motor symptoms (often mixed upper and lower motor neuron syndromes)
can present with both spasticity and flaccid paresis
hyperreflexia and/or hyporeflexia
Prognosis: guarded.
Causes of Spinal Cord Injuries
Most spinal cord injuries are preventable, and knowing the causes of these injuries can help you avoid becoming a victim. And if you or someone you love already deal with the frustration and pain of a spinal cord injury, knowing the most common sources of these injuries can help you feel a bit less alone.
Auto Accidents – Nationwide, car accidents claim more than lives annually. Unsurprisingly, then, car accidents are the leading cause of spinal cord injuries, accounting for (29.3%) male injuries and (48.3%) female injuries. Find out what to do after a car accident.
Falls – Falls were the second-leading cause of SCI accounting for (22%) of male injuries and 1,262 (21.5%) of female injuries.
Gunshot Wounds – Gun-related injuries accounted for (16.9%) of male SCIs and (9.1%) of female injuries.
Diving Injuries – Propelling headfirst into the water is an inherently dangerous activity. (7%) men suffered spinal cord injuries due to diving accidents with (2.1%) female divers experiencing an SCI.
Motorcycle Accidents – The lack of external protection means that even minor motorcycle collisions can be deadly. In (6.9%) men suffered spinal cord injuries while on motorcycles, with a mere (2.5%) women experiencing such injuries.
Falling Objects – Those in industries where falling objects are common are especially vulnerable. Men (3.3%) and 37 women (.6%) experienced spinal cord injuries due to falling objects.
Medical and Surgical Complications – Choosing the right doctor, and carefully monitoring any unusual symptoms can help you avoid a medically induced SCI. (2.2%) men suffered spinal cord injuries due to medical complications.
Pedestrian Injuries – Ample research suggests that pedestrians are often distracted by phones and other devices, and many such pedestrians are in denial about the extent of their distraction. (1.5%) men suffered pedestrian-related spinal cord injuries, with women (2.2%) meeting a similar fate.
Bicycle Accidents – Helmets save lives. Over time, fatal bicycle accidents have generally declined, suggesting that helmet laws are working to keep cyclists safe. Nevertheless, men (1.7%) and women (.8%) suffered bicycling-related spinal cord injuries.
Traumatic – (ground-level falls in the elderly, high-energy motor vehicle accidents in any age group)
The incidence and prevalence of traumatic SCI in the United States is higher compared to rates reported in the literature for other countries worldwide[rx][rx]
The average age at clinical presentation continues to increase, corresponding to the aging of the general population[rx]
Heightened clinical suspicion should be given to vertebral compression fractures which can occur spontaneously (i.e., in the absence of trauma)
Spinal cord disorders – injuries (SCIs), or syndromes may include (but are not limited to)[rx][rx][rx]
Unclassified, which includes injuries that don’t fit neatly into a single category, or for which adequate data is not available.
Penetrating wounds, such as an object entering the brain or spinal cord.
All-terrain vehicle (ATV) accidents.
Accidents in other vehicles, such as jet skis and boats.
Snow skiing.
Football.
Winter sports such as snowboarding.
Horseback riding.
Surfing, including body surfing.
Other sports-related injuries.
Birth injuries, which typically affect the spinal cord in the neck area
Falls
Sports injuries
Diving accidents
Trampoline accidents
Violence (gunshot or stab wounds)
Infections that form an abscess on the spinal cord
Symptoms of Spinal Cord Injury
A spinal cord injury is not the sort of thing you have to wonder about having. If you’ve suffered a spinal cord injury, your life is in danger, and you’ll know you’re injured. You can’t use symptoms to diagnose the sort of spinal cord injury you have, and every patient’s prognosis is different. Some make a miraculous recovery within months; others need years of physical therapy and still make little to no progress.
The outcome depends on the nature of the injury, the quality of medical care you receive, the degree to which you work at your own recovery by adopting a healthy lifestyle, your psychological health, luck, and innumerable other factors.
A partial list of common spinal cord injury symptoms includes:
Varying degrees of paralysis, including tetraplegia/quadriplegia, and paraplegia
Difficulty breathing; the need to be on a respirator
Problems with bladder and bowel function
Frequent infections; the likelihood of this increases if you are on a feeding or breathing tube
Extreme pain or pressure in the neck, head or back
Pneumonia (more than half of cervical spinal cord injury survivors struggle with bouts of pneumonia)
Unusual lumps on the head or spine
Diagnosis of Spinal Cord Injury
Physical Exam
Patients with SCI will present with varying clinical pictures, depending on the level of the injury. The clinician should note the specific injury type and classification. Descriptive categories include:[rx],[rx]
Paraplegia
SCI causing dysfunction from the trunk/pelvic regions to the lower extremities
Patients have spared upper extremity function which preserves varying levels of independent mobility
Tetraplegia
SCI injuries at the level of the cervical spine, leading to dysfunction of the upper extremities, trunk/pelvic regions, and lower extremities
Patients are particularly susceptible to progressive losses in BMD as well as spontaneous VCFs without an apparent mechanism
Complete SCI
Patient is diagnosed with a complete SCI in the acute setting after the resolution of the spinal shock state (i.e., after the return of the patient’s bulbocavernosus reflex)
Patients have no spared motor or sensory function below the defined level of injury (i.e., American Spinal Injury Association [ASIA] A injuries)
Incomplete SCI
Injuries are subdivided into syndromes of clinical manifestation based on the anatomic area of injury to the spinal cord
All of these syndromes demonstrate some preserved motor or sensory function below the defined level of injury
Syndromes include the following:
Anterior cord
Posterior cord
Central cord
Cauda equina
Conus medullaris
Brown-Sequard
In addition to documenting a comprehensive motor and sensory exam, careful palpation and heightened clinical suspicion for spontaneous/occult fractures are critical. The most common location for spontaneous fractures is in the sub lesson regions, especially the lower extremity long bones.[rx] The clinician should note any focal or diffuse areas of swelling, including deformity and overall limb alignment.
ASIA Impairment Scale for classifying spinal cord injury[rx][rx]
Grade
Muscle function
Grade
Description
0
No muscle contraction
A
Complete injury. No motor or sensory function is preserved in the sacral segments S4 or S5.
1
Muscle flickers
B
Sensory incomplete. Sensory but not motor function is preserved below the level of injury, including the sacral segments.
2
Full range of motion, gravity eliminated
C
Motor incomplete. Motor function is preserved below the level of injury, and more than half of muscles tested below the level of injury have a muscle grade less than 3 (see muscle strength scores, left).
3
Full range of motion, against gravity
D
Motor incomplete. Motor function is preserved below the level of injury and at least half of the key muscles below the neurological level have a muscle grade of 3 or more.
4
Full range of motion against resistance
E
Normal. No motor or sensory deficits, but deficits existed in the past.
5
Normal strength
Function after complete cervical spinal cord injury[rx]
Level
Motor Function
Respiratory function
C1–C4
Full paralysis of the limbs
Cannot breathe without mechanical ventilation
C5
Paralysis of the wrists, hands, and triceps
Difficulty coughing, may need help clearing secretions
C6
Paralysis of the wrist flexors, triceps, and hands
C7–C8
Some hand muscle weakness, difficulty grasping and releasing
[/stextbox]
Electrophysiological testing
Evoked potentials (EPs) measure electrical signals going to the brain and can determine whether there is motor or somatosensory impairment. The signal gets detected by electroencephalography (EEG) or electromyography (EMG).
Evoked potentials can be used to assess for spinal cord damage in the setting of spinal cord injury and tumors, as well as to measure the functional impairment and predict disease progression in multiple sclerosis.[rx] Somatosensory evoked potentials (SEPs) and motor evoked potentials (MEPs) are frequently used intra-operatively for monitoring and can be used post-operatively as surrogate endpoints to check muscle strength and sensory status.[rx][rx]
Lumbar puncture
A lumbar puncture, or spinal tap, samples the cerebrospinal fluid from the subarachnoid space. The needle to obtain the sample should be inserted between lumbar spinal canal levels L3 and L4 to avoid contact with the spinal cord.[rx]
The cerebrospinal fluid is then sent to a laboratory to establish whether any insult can be determined. For instance, a lumbar puncture can confirm or exclude bacterial meningitis, which will produce a cloudy fluid suggestive of a high leukocyte count. It is also important to know when not to use a lumbar puncture. Contraindications to lumbar puncture include signs of cerebral herniation, focal neurological signs, uncorrected coagulopathies, or cardiorespiratory compromise.[17]
Deep tendon testing
Part of the neurological exam is a test of the deep tendon reflexes, which are involuntary motor responses to various stimuli that function via reflex arcs within the spinal cord. They can be used to test the function of the motor and sensory nerves at specific spinal cord levels. Reflex grading is on a scale of 0 (absent reflex) to 5+ (sustained clonus).[rx] Some commonly tested reflexes are as follows:
Biceps reflex: C5/C6
Brachioradialis reflex: C6
Triceps reflex: C7
Patellar reflex: L2/L3/L4
Achilles reflex: S1
Additionally, the Babinski reflex, or the extensor plantar reflex, can be seen in newborns but is an abnormal response after between six to twelve months of age, and indicative of an abnormality in the corticospinal system.[rx]
Plain radiograph
These have no real role in traumatic cord injury in patients with significant trauma as they have limited sensitivity for detecting spinal cord trauma and bony injuries associated with it.
CT
This is best for assessing the associated bony injuries which may need concomitant treatment consideration but does not assess the cord itself.
MRI
Apart from routine axial and sagittal T1 and T2 imaging additional sequences should be considered depending on the clinical concern. T2 sequences (e.g. gradient echo, SWI) are more sensitive to hemorrhage, while STIR sequences are more sensitive to associated ligamentous injury.
Spinal cord swelling
focal cord enlargement at the level of trauma without signal change 5 best seen on sagittal T1
Spinal cord edema
as per swelling but with additional increased T2 signal
Spinal cord contusion
thick high T2 signal rim around small central low T1 signal above or below the level of trauma.
blooming on T2 sequences
Intramedullary hemorrhage
thin high T2 signal rim around large central low T1 signal 5
blooming on T2* sequences
see aging blood on MRI for other timescales
Spinal cord transection
discontinuity of cord best seen on sagittal sequences
Clinical evaluation – Your doctor will make a detailed list of all of your symptoms and may conduct blood tests, ask you to move your limbs, follow movement in your eyes, and conduct other tests to narrow down your symptoms.
Imaging tests – Your doctor may order MRI imaging or other forms of radiological imaging to view your spinal column, spinal cord, and brain.
Treatment of Spinal Cord Injury
Spinal injury: First aid
If you suspect a back or neck (spinal) injury, do not move the affected person. Permanent paralysis and other serious complications can result. Assume a person has a spinal injury if:
There’s evidence of a head injury with an ongoing change in the person’s level of consciousness
The person complains of severe pain in his or her neck or back
An injury has exerted substantial force on the back or head
The person complains of weakness, numbness, or paralysis or lacks control of his or her limbs, bladder or bowels
The neck or body is twisted or positioned oddly
Keep the person still – Place heavy towels or rolled sheets on both sides of the neck or hold the head and neck to prevent movement.
Avoid moving the head or neck – Provide as much first aid as possible without moving the person’s head or neck. If the person shows no signs of circulation (breathing, coughing or movement), begin CPR, but do not tilt the head back to open the airway. Use your fingers to gently grasp the jaw and lift it forward. If the person has no pulse, begin chest compressions.
Keep the helmet on – If the person is wearing a helmet, don’t remove it. A football helmet facemask should be removed if you need to access the airway.
Don’t roll alone – If you must roll the person because he or she is vomiting, choking on blood or because you have to make sure the person is still breathing, you need at least one other person. With one of you at the head and another along the side of the injured person, work together to keep the person’s head, neck and back aligned while rolling the person onto one side.
Unlike many other injuries, the most important component of spinal cord injury treatment begins before you even get to the doctor. Remaining still, avoiding moving your spinal column, and prompt emergency care, can all increase the odds that you survive while minimizing the long-term effects of your injury.
From there, doctors will focus on stabilizing you, since the first hours after a spinal cord injury are critical to a patient’s survival. Assistance with breathing, a collar to keep your neck still, blood transfusions, and other procedures to address your immediate symptoms may be necessary.
Eat Nutritiously During Your Recovery
All bones and tissues in the body need certain nutrients in order to heal properly and in a timely manner. Eating a nutritious and balanced diet that includes lots of minerals and vitamins are proven to help heal broken bones of all types. Therefore focus on eating lots of fresh produce (fruits and veggies), whole grains, lean meats, and fish to give your body the building blocks needed to properly repair your. In addition, drink plenty of purified water, milk, and other dairy-based beverages to augment what you eat.
Broken bones need ample minerals (calcium, phosphorus, magnesium, boron) and protein to become strong and healthy again.
Excellent sources of minerals/protein include dairy products, tofu, beans, broccoli, nuts and seeds, sardines, and salmon.
Important vitamins that are needed for bone healing include vitamin C (needed to make collagen), vitamin D (crucial for mineral absorption), and vitamin K (binds calcium to bones and triggers collagen formation).
Conversely, don’t consume food or drink that is known to impair bone/tissue healing, such as alcoholic beverages, sodas, most fast food items, and foods made with lots of refined sugars and preservatives.
Physical Therapy
Although there will be some pain, it is important to maintain arm motion to prevent stiffness. Often, patients will begin doing exercises for elbow motion immediately after the injury. It is common to lose some leg strength. Once the bone begins to heal, your pain will decrease and your doctor may start gentle hip, knee exercises. These exercises will help prevent stiffness and weakness. More strenuous exercises will be started gradually once the fracture is completely healed.
Follow-Up Care
You will need to see your doctor regularly until your fracture heals. During these visits, he or they will take x-rays to make sure the bone is healing in a good position. After the bone has healed, you will be able to gradually return to your normal activities.
Opioids – Also known as narcotics, these medications are intense pain relievers that should only be used under a doctor’s careful supervision.
Topical Medications – These prescription-strength creams, gels, ointments, patches, and sprays help relieve pain and inflammation through the skin.
Calcium & vitamin D3 – to improve bone health and healing fracture. As a general rule, men and women age 50 and older should consume 1,200 milligrams of calcium a day, and 600 international units of vitamin D a day.
Glucosamine & Diacerein, Chondroitin sulfate – can be used to tightening the loose tension, cartilage, ligament, and cartilage, ligament regenerate cartilage or inhabit the further degeneration of cartilage, ligament
Antidepressants – A drug that blocks pain messages from your brain and boosts the effects of endorphins (your body’s natural painkillers).
Your doctor will work with you and your family to construct a detailed plan for your SCI rehabilitation. Every injury is different, but common treatments for a spinal cord injury may involve:
Care to address, but not treat, your immediate symptoms. For instance, a ventilator can help you breathe and a feeding tube can help you eat if you are unable to do so.
Palliative care to help you be more comfortable. If you struggle with insomnia or chronic pain, your doctor might prescribe medication to help.
Lifestyle changes, such as a healthier diet or giving up smoking.
Physical therapy to help retrain your brain and body; many spinal cord injury survivors are able to regain significant mobility with physical therapy.
Family and individual counseling to help you cope with the pain and stress of life with a spinal cord injury.
Surgery as needed to correct injury-related health problems.
Spinal cord injury research is always looking for breakthroughs in treatments, such as stem cell therapy for SCI. Stem cell therapies have long been marketed as a holy grail for a range of diseases, including spinal cord injuries. Recent data suggests that further research could point toward a cure for spinal cord injuries.
Vibration Therapy
Low magnitude mechanical signals (LMMS) as a therapeutic modality has demonstrated bone formation capabilities in both human and rodent models. However, beyond limited case reports there is little evidence available to advocate its definitive therapeutic potential. Similarly, low-intensity vibration treatment protocols have shown some promising results in a small case series of SCI-induced osteoporotic patients. [rx],[rx]
Calcium and Vitamin D
Without question, all patients should be taking calcium and vitamin D supplementation. Patients should be educated on the recommended daily intake for calcium and vitamin D. The National Osteoporosis Foundation (NOF) recommends 1200 to 1500 mg of calcium per day and 800 to 1000 IUs of daily vitamin D for adults over the age of 50. In the setting of SCI-induced osteoporosis, all patients should begin supplementation regardless of age at presentation. [rx]
Anti-Osteoporotic Pharmacotherapy Options
Pharmacotherapy agents work through either anti-resorptive or anabolic means. In general, bisphosphonates are the most commonly prescribed medication class for osteoporosis treatment. These drugs are divided into non-nitrogen and nitrogen-containing compounds. The latter are considered first-line therapy for osteoporosis.[rx]
However, a major concern with SCI-induced osteoporosis coupled with the bisphosphonate anti-resorptive mechanism on bone is the inability to actually demonstrate measurable increases in BMD levels.[rx]
In one study, alendronate was able to prevent further bone loss in 55 patients with chronic SCI-induced osteoporosis at the 2-year follow-up. However, this is a stark contrast to alendronate’s proven track record and documented capabilities to increase BMD values measured in an ambulatory (i.e., not SCI-induced), post-menopausal women with osteoporosis. [rx]
While alendronate, risedronate, and intravenous zoledronic acid have all demonstrated reduced fragility fracture rates in the general osteoporosis population, the clinical evidence has yet to be demonstrated in the SCI-induced osteoporosis population.[rx] Clinicians are encouraged to recognize the subtle differences in efficacy and evidence-based approaches for the pharmacologic management of these vulnerable patients.
Denosumab
Denosumab, a monoclonal antibody against receptor activator of nuclear factor-kappa-? ligand (RANKL), has recently been studied specifically in patients afflicted with SCI-induced osteoporosis. In 2016, one study demonstrated increases in lumbar and femoral BMD values as measured by DXA scans after 1 year of treatment compared to baseline BMD values. Denosumab was administered in a 60 mg every 6 months protocol during the study period. [rx]
Anabolic Agents and Emerging Pharmacotherapy Agents
Teriparatide is a recombinant form of PTH that stimulates osteoblasts to produce more bone. Teriparatide is now FDA approved for osteoporosis treatment in males and females, but more studies are needed in order to improve our understanding of its effects on BMD levels and clinical outcomes in SCI-induced osteoporotic patients. [rx],[rx]
Exercises for after a Spinal Cord Injury
Particularly in the early days after a spinal cord injury, you might be tempted to languish in bed. Moving around certainly seems counter-intuitive when you’ve suffered a catastrophic injury to your body. But the benefits of exercise don’t disappear just because you’ve been injured. Quite the contrary, in fact. Exercises after a spinal cord injury can expedite your SCI rehabilitation in addition to offering a myriad of health benefits.
Exercises
Yoga – ideal for spinal cord injury survivors because the gentle stretching encourages healthy breathing patterns, and can reduce the pain of spending all or most of your day in a wheelchair.
Water Aerobics – The water reduces pain and joint trauma, and can help support your weight even if you’ve lost a significant portion of your mobility or sensation.
Weightlifting – Lifting weights can help you regain significant muscle control. It will also enable you to maintain strength in regions unaffected by your spinal cord injury.
Seated Aerobics – You can still get an incredible aerobic workout from your wheelchair. Talk to your doctor about seated aerobic classes specifically targeted to spinal cord injury survivors
Rowing – Rowing is an ideal aerobic activity because it only requires movement in your upper body, but uses your lower body to stabilize your movements, making it an ideal choice for injury survivors with incomplete spinal cord injuries.
Walking – If your spinal cord injury is incomplete or you have only sustained nerve damage, you may still be able to walk. Maximize your muscle function by walking as frequently as is comfortable, maintaining a steady gait, and an upright posture.
Improving mental health by reducing depression and anxiety
Reducing the risk of cancer
Improving symptoms of chronic pain
Helping you avoid chronic illnesses such as diabetes and osteoporosis
Reducing your risk of falls
Improving your chances of living a longer life.
New technologies
Inventive medical devices can help people with spinal cord injury become more independent and more mobile. Some devices may also restore function. These include:
Modern wheelchair – Improved, lighter weight wheelchairs are making people with spinal cord injuries more mobile and more comfortable. For some, an electric wheelchair may be needed. Some wheelchairs can even climb stairs, travel over rough terrain, and elevate a seated passenger to eye level to reach high places without help.
Computer adaptations – For someone who has limited hand function, computers can be very powerful tools, but they’re difficult to operate. Computer adaptations range from simple to complex, such as key guards or voice recognition.
Electronic aids to daily living – Essentially any device that uses electricity can be controlled with an electronic aid to daily living. Devices can be turned on or off by a switch or voice-controlled and computer-based remotes.
Electrical stimulation devices – These sophisticated devices use electrical stimulation to produce actions. They’re often called functional electrical stimulation systems, and they use electrical stimulators to control arm and leg muscles to allow people with spinal cord injuries to stand, walk, reach and grip.
Robotic gait training – This emerging technology is used for retraining walking ability after a spinal cord injury.
Spinal Cord Injury Recovery
Your SCI rehabilitation journey can be long and often unpredictable. Some spinal cord injury sufferers spontaneously walk years after their injury. Others are never able to move again. While medical science can do a lot to predict what might happen to you, there are no guarantees when it comes to spinal cord injuries. What we do know is that a healthy lifestyle, sound psychological health, family support, and receiving treatment at a model system of care can all improve outcomes.
Physical Recovery
There is no single definition of physical recovery. Though many spinal cord injury survivors do regain some degree of function, some don’t. Thus, focusing solely on physical recovery can leave you feeling hopeless and overwhelmed.
Some common milestones for physical recovery include:
The reduction of swelling at the site of the injury.
Recovering from surgery.
Regaining some sensation below the site of the injury.
Regaining some movement below the site of the injury.
Learning to use assistive devices such as wheelchairs and prostheses.
Finding new ways to complete old tasks; for instance, you might change your approach to sex or making food.
Strengthening your body so you can work around your injuries. You might learn how to type with a part of your body other than your hands, for instance.
Psychological Recovery
Spinal cord injury guides, as well as doctors, lawyers, and loved ones, often focus on physical recovery. But this dogged fixation can actually undermine your psychological recovery. Poor psychological health can worsen your physical health, and believing that physical recovery is the only way to be happy can likewise undermine your psychological well-being. It is possible to be happy even in the face of a painful injury. Indeed, one study found that 86% of quadriplegics rated their lives as better than average.
This attitude can take some time to cultivate, but once you’ve mastered it, you may realize an important truth about life: happiness comes from within, and the way you think about things affects the way you perceive them. Spinal cord injuries are challenging, and there is no shame in seeking psychological help. Many survivors struggle with depression, anxiety, and other mental health issues, but with family support and lots of help, you can find new ways to live a life you love.
Complications
Cardiac and circulatory issues
Respiratory difficulties or loss of function
Numbness or loss of feeling below the injury site
Paralysis
Bladder and bowel function loss
Urinary tract infections (UTIs)
Thermoregulatory impairment (inability to regulate body temperature)
Bladder control – Your bladder will continue to store urine from your kidneys. However, your brain may not be able to control your bladder as well because the message carrier (the spinal cord) has been injured. The changes in bladder control increase your risk of urinary tract infections. The changes may also cause kidney infections and kidney or bladder stones. During rehabilitation, you’ll learn new techniques to help empty your bladder.
Bowel control – Although your stomach and intestines work much as they did before your injury, control of your bowel movements is often altered. A high-fiber diet may help regulate your bowels, and you’ll learn techniques to optimize your bowel function during rehabilitation.
Skin sensation – Below the neurological level of your injury, you may have lost part of or all skin sensations. Therefore, your skin can’t send a message to your brain when it’s injured by certain things such as prolonged pressure, heat, or cold.
Circulatory control – A spinal cord injury may cause circulatory problems ranging from low blood pressure when you rise (orthostatic hypotension) to swelling of your extremities. These circulation changes may also increase your risk of developing blood clots, such as deep vein thrombosis or a pulmonary embolus.
Respiratory system – Your injury may make it more difficult to breathe and cough if your abdominal and chest muscles are affected. These include the diaphragm and the muscles in your chest wall and abdomen.
Muscle tone – Some people with spinal cord injuries experience one of two types of muscle tone problems: uncontrolled tightening or motion in the muscles (spasticity) or soft and limp muscles lacking muscle tone (flaccidity).
Fitness and wellness – Weight loss and muscle atrophy are common soon after a spinal cord injury. Limited mobility may lead to a more sedentary lifestyle, placing you at risk of obesity, cardiovascular disease, and diabetes.
Sexual health – Sexuality, fertility, and sexual function may be affected by a spinal cord injury. Men may notice changes in erection and ejaculation; women may notice changes in lubrication. Physicians specializing in urology or fertility can offer options for sexual functioning and fertility.
Pain – Some people experience pain, such as muscle or joint pain, from overuse of particular muscle groups. Nerve pain can occur after a spinal cord injury, especially in someone with an incomplete injury.
Depression – Coping with all the changes a spinal cord injury brings and living with pain causes some people to experience depression.
Prevention
The leading causes of spinal cord injury are road traffic crashes, falls, and violence (including attempted suicide). A significant proportion of traumatic spinal cord injury is due to work or sports-related injuries. Effective interventions are available to prevent several of the main causes of spinal cord injury, including improvements in roads, vehicles and people’s behavior on the roads to avoid road traffic crashes, window guards to prevent falls, and policies to thwart the harmful use of alcohol and access to firearms to reduce violence.
Drive safely – Car crashes are one of the most common causes of spinal cord injuries. Wear a seat belt every time you drive or ride in a car. Make sure that your children wear a seat belt or use an age- and weight-appropriate child safety seat. To protect them from airbag injuries, children under age 12 should always ride in the back seat.
Check water depth before diving – To make sure you don’t dive into shallow water, don’t dive into a pool unless it’s 12 feet (about 3.7 meters) or deeper, don’t dive into an aboveground pool, and don’t dive into any water of which you don’t know the depth.
Prevent falls – Use a step stool with a grab bar to reach objects in high places. Add handrails along stairways. Put nonslip mats on tile floors and in the tub or shower. For young children, use safety gates to block stairs and consider installing window guards.
Take precautions when playing sports – Always wear recommended safety gear. Avoid leading with your head in sports. For example, don’t slide headfirst in baseball, and don’t tackle using the top of your helmet in football. Use a spotter for new moves in gymnastics.
Don’t drink and drive. Don’t drive while intoxicated or under the influence of drugs. Don’t ride with a driver who’s been drinking.
Improving care and overcoming barriers
Many of the consequences associated with spinal cord injury do not result from the condition itself, but from inadequate medical care and rehabilitation services, and from barriers in the physical, social and policy environments. Implementation of the UN Convention on the Rights of Persons with Disabilities (CRPD) requires action to address these gaps and barriers. Essential measures for improving the survival, health, and participation of people with spinal cord injury include the following.
Timely, appropriate pre-hospital management: quick recognition of suspected spinal cord injury, rapid evaluation, and initiation of injury management, including immobilization of the spine.
Acute care (including surgical intervention) appropriate to the type and severity of the injury, degree of instability, presence of neural compression, and in accordance with the wishes of the patient and their family.
Access to ongoing health care, health education, and products (e.g. catheters) to reduce the risk of secondary conditions and improve the quality of life.
Access to skilled rehabilitation and mental health services to maximize functioning, independence, overall wellbeing, and community integration. Management of bladder and bowel function is of primary importance.
Access to appropriate assistive devices that can enable people to perform everyday activities they would not otherwise be able to undertake, reducing functional limitations and dependency. Only 5-15% of people in low- and middle-income countries have access to the assistive devices they need.
Specialized knowledge and skills among providers of medical care and rehabilitation services.
Essential measures to secure the right to education and economic participation include legislation, policy, and programs that promote the following:
physically accessible homes, schools, workplaces, hospitals, and transportation;
inclusive education;
elimination of discrimination in employment and educational settings;
Vocational rehabilitation to optimize the chance of employment;
micro-finance and other forms of self-employment benefits to support alternative forms of economic self-sufficiency;
access to social support payments that do not act as a disincentive to return to work; and
correct understanding of spinal cord injury and positive attitudes towards people living with it.
WHO response
WHO works across the spectrum from primary prevention of traumatic and non-traumatic causes of spinal cord injury, improvements in trauma care, strengthening health and rehabilitation services, and support for the inclusion of people with spinal cord injuries. WHO:
works in a multisectoral manner, in partnership with national stakeholders from a variety of sectors (e.g. health, police, transport, education) to improve prevention of spinal cord injury including of road traffic injuries, falls, violence and neural tube defects;
guides and supports the Member States to increase awareness of disability issues, and promotes the inclusion of disability as a component in national health policies and programs;
facilitates data collection and dissemination of disability-related data and information;
develops normative tools, including guidelines and good practice examples to strengthen primary prevention (road traffic crashes, falls and violence), trauma care, health care, rehabilitation and support and assistance;
builds capacity among health policy-makers and service providers;
promotes scaling up of community-based rehabilitation; and
promotes strategies to ensure that people with disabilities are knowledgeable about their own health conditions, and that health-care personnel support and protect the rights and dignity of persons with disabilities.
Following strategies should be undertaken for better recovery
Close routine follow-up with the neurologist/internist.
Educate patients for clean intermittent catheterization (CIC) to avoid urinary tract infections and secondary complications.
Educate patients to avoid immobility, and regularly change position after 2-4 hours.
Close follow-up with a physical therapist for muscle and core strengthening exercises to avoid muscle atrophy.
Blood pressure monitoring at home.
Close follow-up with the psychiatrist to look for any signs of depression and suicidal ideation.
Spinal Cord Injury/The spinal cord is a tubular structure composed of nervous tissue that extends from the brainstem and continuing distally before tapering at the lower thoracic/upper lumbar region as the conus medullaris. The spinal cord is anchored distally by the filum terminal, a fibrous extension of the pia mater anchoring the spinal cord to the coccyx.[rx] Protecting the spinal cord is the surrounding cerebrospinal fluid (CSF), supportive soft tissue membranes and meninges, and the osseous vertebral column.[rx]
Traumatic spinal cord injury (TSCI) is sudden forceful damage to the spinal nerves resulting in temporary or permanent paralysis, bladder and bowel dysfunction, and autonomic imbalance among other consequences [rx,rx]. A person with spinal cord injury is at immediate risk of respiratory and cardiac failure which may lead to death in the acute phase [rx]. Those who survive the acute phase faces a lifelong risk of secondary complications such as pressure ulcers, urinary tract infections, deep venous thrombosis, contractures, chronic pain, and spasms [rx,rx].
Trauma to the spinal cord may result from a road traffic accident (RTA), fall, assault and recreational or occupational accident [rx,rx]. The World Health Organization informs that up to 90% of all spinal cord lesions are due to trauma and that the leading cause globally is RTA [rx].
Anatomy of Spinal Cord
The major tracts and their most defining features are as follows
Ascending Tracts
Dorsal column – contains the gracile fasciculus and cuneate fasciculus, which together are the dorsal funiculus. The dorsal column is responsible for pressure and vibration sensation as well as two-point discrimination, movement sense, and conscious proprioception. The dorsal column decussates at the superior portion of the medulla oblongata and forms medial lemniscus.
Lateral spinothalamic – carries pain and temperature information. The lateral spinothalamic tract decussates at the anterior commissure two segments above the entry to the spinal cord.
Anterior spinothalamic – carries crude touch and pressure information. It decussates similar to the lateral spinothalamic tract.[rx]
Dorsal and ventral spinocerebellar – transmit unconscious proprioception sensory information to the cerebellum. The ventral spinocerebellar tract does not decussate, while the dorsal spinocerebellar tract decussates twice, making them both ipsilateral.[rx]
Descending Tracts
Lateral and anterior corticospinal – involved in conscious control of the skeletal muscle. The majority of lateral corticospinal tract fibers decussate at the inferior portion of the medulla oblongata while anterior corticospinal descends ipsilaterally in the spinal cord and decussates at the segmental level. Lateral corticospinal tract, also called pyramidal tract, innervates primarily contralateral muscles of the limbs, while anterior innervates proximal muscles of the trunk.
Vestibulospinal – carries information from the inner ear to control head positioning and is involved in modifying muscle tone to maintain posture and balance. The vestibulospinal tract does not decussate.
Rubrospinal – is involved in the movement of the flexor and extensor muscles. The rubrospinal tract originates from the red nuclei in the midbrain and decussates at the start of its pathway.
Reticulospinal – originates from the reticular formation housed in the brainstem and it facilitates, influences, and supplements the corticospinal tract.[rx] The reticulospinal tract does not decussate.
There is a laminar distribution of neurons in the gray matter, characterized by density and topography
Lamina I – is located at the tip of the dorsal horn and is composed of loosely packed neuropil along with neurons of low neuronal density. The most abundant neuron in lamina I is the Waldeyer cell: large, fusiform, and with a disk-shaped dendritic domain.[rx][rx]
Lamina II – is composed mostly of islet cells with rostrocaudal axes, which contain GABA and are thought to be inhibitory, and stalked cells with dorsoventral dendritic trees.[rx]
Lamina III – has cells of intermediate size, including antenna-like and radial neurons, many of which contain GABA or glycine and are also considered inhibitory.[rx][rx]
Lamina IV – contains antenna-like cells and transverse cells, with dendrites that mostly go to Laminas II and III, and whose axons are mainly thought to enter the spinothalamic tract. Lateral from lamina IV is the lateral spinal nucleus, which sends signals to lamina IV from the midbrain and brainstem.[rx][rx]
Lamina V and VI – are composed of medium-sized multipolar neurons, that can be fusiform or triangular. These neurons communicate with the reticular formation of the brainstem.
Lamina VII – is composed of homogenous medium-sized multipolar neurons, and contains, in individual segments, well-defined nuclei, including the intermediolateral nucleus (T1-L1), which has autonomic functions, and the dorsal nucleus of Clarke (T1-L2), which make up the dorsal spinocerebellar tract.
Lamina VIII – consists of neurons with dorsoventrally polarized dendritic trees.
Lamina IX – has the cell bodies of motor neurons, with dendrites extending dorsally into laminas as far as VI. Lamina IX – also has Renshaw cells, inhibitory interneurons, placed at the medial border of motor nuclei.
Lamina X – is the substantia grisea centralis or the gray matter that surrounds the central canal. In the distal portion, lamina X consists of bipolar cells with fan-shaped dendritic trees, and in the ventral portion, lamina X consists of bipolar cells with poorly ramified longitudinal dendrites.[rx]
Meninges and Spaces
Epidural space – fatty space between the bony framework of the spinal vertebral column and the thick dura mater surrounding the spinal cord. It contains adipose tissue and blood vessels.
Dura mater – Thick outermost covering (meninges) of the spinal cord, extending down to the level of the S2 vertebra
Arachnoid mater – The middle covering of the spinal cord
Subarachnoid space – Space between the arachnoid mater and the innermost covering of the spinal cord. It contains Cerebrospinal fluid.
Pia mater – The innermost covering of the spinal cord, intimately adhering to its surface, it stabilizes the spinal cord through lateral extensions of the pia called the denticulate ligaments, extending between the ventral and dorsal roots unto the dura mater.
Spinal cord
The length is about 45 cm in men and 43 cm in women[rx]
Anatomic course originates in the brainstem before coursing through the foramen magnum. The spinal cord continues distally through the cervical and thoracic regions of the spinal column before terminating as a tapered structure known as the conus medullaris
The spinal cord proper terminates at the L1-L2 vertebral level and is anchored distally via the filum terminale, representing an extension of the pia mater with fibrous attachments to the coccyx
The spinal cord comprises 5 segments, cervical, thoracic, lumbar, sacral and coccygeal
Long, cylindrical structure with varying levels of thickness/width depending on the corresponding vertebral levels
31 total nerve root segments
8 cervical
12 thoracic
5 lumbar
5 sacral
1 coccygeal
Cord width ranges – from 0.64-0.83 cm in the thoracic region to 1.27-1.33 cm in the cervical and lumbar regions
A 2016 systematic review of the literature demonstrated that, on average, the largest transverse diameter corresponded to the C5 neuronal segment (1.33 +/- 0.22 cm) and the smallest transverse diameter, on average, corresponded to the T8 segment (0.83 +/- 0.21 cm)[rx]
Enlarged regions of gray matter correspond to nerve root distribution to the upper and lower extremities
A cross-sectional –
Its view of the spinal cord shows its organization into the gray and white matter. The anterior aspect of the cord is identifiable with the presence of anterior median fissure. The gray matter is organized into an H- shaped body of cell bodies. The anterior horn comprises motor nuclei while the posterior horn comprises sensory nuclei.
The surrounding white matter is organized into anterior, posterior, and lateral columns (funiculi), from neuronal axons organized into tracts that convey neural messages back and forth the CNS (the ascending and descending tracts).
The anterolateral columns carry temperature and pain information, while the dorsal column communicates the sense of touch, proprioception, vibration. The cervical and thoracic spinal segments present an intermedio lateral gray horn which gives off preganglionic sympathetic fibers onto the sympathetic trunk on both sides of the spinal cord.
The spinal cord’s central canal
It is an extension of the 4th ventricle. It contains CSF, surrounding it is the gray commissure and the anterior white commissure. Decussation of the tracts of the white columns occurs at the anterior white commissure.
Types of Spinal Cord Injury
Incomplete Spinal Cord Injury
Tetraplegia
Cervical spine injury resulting in the impaired arm, trunk leg, pelvic organ function. These injuries, which are the result of damage to the cervical spinal cord, are typically the most severe, producing varying degrees of paralysis of all limbs. Sometimes known as quadriplegia, tetraplegia eliminates your ability to move below the site of the injury and may produce difficulties with bladder and bowel control, respiration, and other routine functions. The higher up on the cervical spinal cord the injury is, the more severe symptoms will likely be.
Paraplegia
This occurs when sensation and movement are removed from the lower half of the body, including the legs. These injuries are the product of damage to the thoracic spinal cord. As with cervical spinal cord injuries, injuries are typically more severe when they are closer to the top vertebra.
Thoracic/lumbar/sacral spinal injury leading to impaired trunk/leg/pelvic organ function
Preserved arm function.
Triplegia
Triplegia causes a loss of sensation and movement in one arm and both legs and is typically the product of an incomplete spinal cord injury.
Complete Injuries
By definition – complete SCI yields no sparing of the motor or sensory function below the injured level
The patient must have already recovered from the acute phase of spinal shock (usually 48 hours from presentation)
Spinal shock: by definition, the temporary (typically 48 hours) loss of all spinal cord function (including reflex activity) below the level of injury
Absent bulbocavernosus reflex
Flaccid paralysis
Bradycardia/hypotension
Spina bifida – Neural tube defect in which the neural tube does not completely close leaving a dorsal defect. Folate deficiency in early pregnancy is a risk factor.[rx] The severity of symptoms depends on the extent of the defect; myelomeningocele is the most severe variant with the spinal cord, meninges both exposed. Other variants include meningocele, which exposes only the meninges, and spina bifida occulta which is the mildest. Symptoms include loss of lower limb sensations, lower limb weakness, urinary incontinence, bowel incontinence
Spinal shock – is the temporary loss of spinal reflex activity with motor and sensory losses. This loss results from loss of sympathetic vascular tone resulting in paradoxical bradycardia with hypotension. During spinal shock, patients appear physiologically completely paralyzed but may show significant recovery after the initial phases of spinal shock have resolved.
Partial Complete spinal cord injuries (SCIs)
Central cord syndrome
This injury is an injury to the center of the cord, and damages nerves that carry signals from the brain to the spinal cord. Loss of fine motor skills, paralysis of the arms, and partial impairment—usually less pronounced—in the legs are common. Some survivors also suffer a loss of bowel or bladder control or lose the ability to sexually function.[rx]
Most common incomplete SCI
Pathophysiology: central gray matter injury
Mechanism(s): hyperextension (i.e., from a fall) in a patient with underlying cervical spinal canal stenosis
Clinical presentation:
Upper extremity loss of motor function (lower extremity motor function no affected/minimally affected)
Sensory sparing variable
Prognosis: Good
Anterior cord syndrome
This type of injury, to the front of the spinal cord, damages the motor and sensory pathways in the spinal cord. You may retain some sensation but struggle with movement.[rx]
Second most common incomplete SCI
Pathophysiology: injuries occur secondary to direct compression to the anterior spinal cord (e.g., hyperflexion injuries, anterior spinal artery occlusion, or disc prolapse)
Brown-Square syndrome – This variety of injury is the product of damage to one side of the spinal cord. The injury may be more pronounced on one side of the body; for instance, movement may be impossible on the right side but maybe fully retained on the left. The degree to which Brown-Sequard patients are injured greatly varies from patient to patient.[rx]
Pathophysiology: Injury to (only) the nerve roots of the cauda equina itself (i.e., spares the spinal cord itself)
Mechanism(s):
disc herniations
burst fractures (e.g., associated hematoma from trauma)
Clinical presentation:
bilateral buttock/lower extremity pain
bowel/bladder dysfunction (urinary retention)
saddle anesthesia
loss of lower extremity motor/sensory function
differentiated from conus medullaris syndrome in that findings are asymmetrical, as opposed to symmetrical (i.e. conus medullaris motor symptoms are symmetrical on presentation)
Prognosis: surgical decompression within the first 48 hours appears to yield improved overall outcomes (although the overall prognosis remains guarded)
Often confused with cauda equina syndrome, although this must be recognized as a separate clinical entity
Pathophysiology: injury to the spinal cord at L1-L2 level.
Mechanism(s):
Direct spinal trauma to the thoracolumbar junction[rx]
Clinical presentation:
Saddle anesthesia
bowel/bladder dysfunction (often presents with dysfunction more acutely compared to cauda equina which can evolve over a variable period time prior to the patient’s presentation)
classically presents with mild, symmetrical motor symptoms (often mixed upper and lower motor neuron syndromes)
can present with both spasticity and flaccid paresis
hyperreflexia and/or hyporeflexia
Prognosis: guarded.
Causes of Spinal Cord Injuries
Most spinal cord injuries are preventable, and knowing the causes of these injuries can help you avoid becoming a victim. And if you or someone you love already deal with the frustration and pain of a spinal cord injury, knowing the most common sources of these injuries can help you feel a bit less alone.
Auto Accidents – Nationwide, car accidents claim more than lives annually. Unsurprisingly, then, car accidents are the leading cause of spinal cord injuries, accounting for (29.3%) male injuries and (48.3%) female injuries. Find out what to do after a car accident.
Falls – Falls were the second-leading cause of SCI accounting for (22%) of male injuries and 1,262 (21.5%) of female injuries.
Gunshot Wounds – Gun-related injuries accounted for (16.9%) of male SCIs and (9.1%) of female injuries.
Diving Injuries – Propelling headfirst into the water is an inherently dangerous activity. (7%) men suffered spinal cord injuries due to diving accidents with (2.1%) female divers experiencing an SCI.
Motorcycle Accidents – The lack of external protection means that even minor motorcycle collisions can be deadly. In (6.9%) men suffered spinal cord injuries while on motorcycles, with a mere (2.5%) women experiencing such injuries.
Falling Objects – Those in industries where falling objects are common are especially vulnerable. Men (3.3%) and 37 women (.6%) experienced spinal cord injuries due to falling objects.
Medical and Surgical Complications – Choosing the right doctor, and carefully monitoring any unusual symptoms can help you avoid a medically induced SCI. (2.2%) men suffered spinal cord injuries due to medical complications.
Pedestrian Injuries – Ample research suggests that pedestrians are often distracted by phones and other devices, and many such pedestrians are in denial about the extent of their distraction. (1.5%) men suffered pedestrian-related spinal cord injuries, with women (2.2%) meeting a similar fate.
Bicycle Accidents – Helmets save lives. Over time, fatal bicycle accidents have generally declined, suggesting that helmet laws are working to keep cyclists safe. Nevertheless, men (1.7%) and women (.8%) suffered bicycling-related spinal cord injuries.
Traumatic – (ground-level falls in the elderly, high-energy motor vehicle accidents in any age group)
The incidence and prevalence of traumatic SCI in the United States is higher compared to rates reported in the literature for other countries worldwide[rx][rx]
The average age at clinical presentation continues to increase, corresponding to the aging of the general population[rx]
Heightened clinical suspicion should be given to vertebral compression fractures which can occur spontaneously (i.e., in the absence of trauma)
Spinal cord disorders – injuries (SCIs), or syndromes may include (but are not limited to)[rx][rx][rx]
Unclassified, which includes injuries that don’t fit neatly into a single category, or for which adequate data is not available.
Penetrating wounds, such as an object entering the brain or spinal cord.
All-terrain vehicle (ATV) accidents.
Accidents in other vehicles, such as jet skis and boats.
Snow skiing.
Football.
Winter sports such as snowboarding.
Horseback riding.
Surfing, including body surfing.
Other sports-related injuries.
Birth injuries, which typically affect the spinal cord in the neck area
Falls
Sports injuries
Diving accidents
Trampoline accidents
Violence (gunshot or stab wounds)
Infections that form an abscess on the spinal cord
Symptoms of Spinal Cord Injury
A spinal cord injury is not the sort of thing you have to wonder about having. If you’ve suffered a spinal cord injury, your life is in danger, and you’ll know you’re injured. You can’t use symptoms to diagnose the sort of spinal cord injury you have, and every patient’s prognosis is different. Some make a miraculous recovery within months; others need years of physical therapy and still make little to no progress.
The outcome depends on the nature of the injury, the quality of medical care you receive, the degree to which you work at your own recovery by adopting a healthy lifestyle, your psychological health, luck, and innumerable other factors.
A partial list of common spinal cord injury symptoms includes:
Varying degrees of paralysis, including tetraplegia/quadriplegia, and paraplegia
Difficulty breathing; the need to be on a respirator
Problems with bladder and bowel function
Frequent infections; the likelihood of this increases if you are on a feeding or breathing tube
Extreme pain or pressure in the neck, head or back
Pneumonia (more than half of cervical spinal cord injury survivors struggle with bouts of pneumonia)
Unusual lumps on the head or spine
Diagnosis of Spinal Cord Injury
Physical Exam
Patients with SCI will present with varying clinical pictures, depending on the level of the injury. The clinician should note the specific injury type and classification. Descriptive categories include:[rx],[rx]
Paraplegia
SCI causing dysfunction from the trunk/pelvic regions to the lower extremities
Patients have spared upper extremity function which preserves varying levels of independent mobility
Tetraplegia
SCI injuries at the level of the cervical spine, leading to dysfunction of the upper extremities, trunk/pelvic regions, and lower extremities
Patients are particularly susceptible to progressive losses in BMD as well as spontaneous VCFs without an apparent mechanism
Complete SCI
Patient is diagnosed with a complete SCI in the acute setting after the resolution of the spinal shock state (i.e., after the return of the patient’s bulbocavernosus reflex)
Patients have no spared motor or sensory function below the defined level of injury (i.e., American Spinal Injury Association [ASIA] A injuries)
Incomplete SCI
Injuries are subdivided into syndromes of clinical manifestation based on the anatomic area of injury to the spinal cord
All of these syndromes demonstrate some preserved motor or sensory function below the defined level of injury
Syndromes include the following:
Anterior cord
Posterior cord
Central cord
Cauda equina
Conus medullaris
Brown-Sequard
In addition to documenting a comprehensive motor and sensory exam, careful palpation and heightened clinical suspicion for spontaneous/occult fractures are critical. The most common location for spontaneous fractures is in the sub lesson regions, especially the lower extremity long bones.[rx] The clinician should note any focal or diffuse areas of swelling, including deformity and overall limb alignment.
ASIA Impairment Scale for classifying spinal cord injury[rx][rx]
Grade
Muscle function
Grade
Description
0
No muscle contraction
A
Complete injury. No motor or sensory function is preserved in the sacral segments S4 or S5.
1
Muscle flickers
B
Sensory incomplete. Sensory but not motor function is preserved below the level of injury, including the sacral segments.
2
Full range of motion, gravity eliminated
C
Motor incomplete. Motor function is preserved below the level of injury, and more than half of muscles tested below the level of injury have a muscle grade less than 3 (see muscle strength scores, left).
3
Full range of motion, against gravity
D
Motor incomplete. Motor function is preserved below the level of injury and at least half of the key muscles below the neurological level have a muscle grade of 3 or more.
4
Full range of motion against resistance
E
Normal. No motor or sensory deficits, but deficits existed in the past.
5
Normal strength
Function after complete cervical spinal cord injury[rx]
Level
Motor Function
Respiratory function
C1–C4
Full paralysis of the limbs
Cannot breathe without mechanical ventilation
C5
Paralysis of the wrists, hands, and triceps
Difficulty coughing, may need help clearing secretions
C6
Paralysis of the wrist flexors, triceps, and hands
C7–C8
Some hand muscle weakness, difficulty grasping and releasing
[/stextbox]
Electrophysiological testing
Evoked potentials (EPs) measure electrical signals going to the brain and can determine whether there is motor or somatosensory impairment. The signal gets detected by electroencephalography (EEG) or electromyography (EMG).
Evoked potentials can be used to assess for spinal cord damage in the setting of spinal cord injury and tumors, as well as to measure the functional impairment and predict disease progression in multiple sclerosis.[rx] Somatosensory evoked potentials (SEPs) and motor evoked potentials (MEPs) are frequently used intra-operatively for monitoring and can be used post-operatively as surrogate endpoints to check muscle strength and sensory status.[rx][rx]
Lumbar puncture
A lumbar puncture, or spinal tap, samples the cerebrospinal fluid from the subarachnoid space. The needle to obtain the sample should be inserted between lumbar spinal canal levels L3 and L4 to avoid contact with the spinal cord.[rx]
The cerebrospinal fluid is then sent to a laboratory to establish whether any insult can be determined. For instance, a lumbar puncture can confirm or exclude bacterial meningitis, which will produce a cloudy fluid suggestive of a high leukocyte count. It is also important to know when not to use a lumbar puncture. Contraindications to lumbar puncture include signs of cerebral herniation, focal neurological signs, uncorrected coagulopathies, or cardiorespiratory compromise.[17]
Deep tendon testing
Part of the neurological exam is a test of the deep tendon reflexes, which are involuntary motor responses to various stimuli that function via reflex arcs within the spinal cord. They can be used to test the function of the motor and sensory nerves at specific spinal cord levels. Reflex grading is on a scale of 0 (absent reflex) to 5+ (sustained clonus).[rx] Some commonly tested reflexes are as follows:
Biceps reflex: C5/C6
Brachioradialis reflex: C6
Triceps reflex: C7
Patellar reflex: L2/L3/L4
Achilles reflex: S1
Additionally, the Babinski reflex, or the extensor plantar reflex, can be seen in newborns but is an abnormal response after between six to twelve months of age, and indicative of an abnormality in the corticospinal system.[rx]
Plain radiograph
These have no real role in traumatic cord injury in patients with significant trauma as they have limited sensitivity for detecting spinal cord trauma and bony injuries associated with it.
CT
This is best for assessing the associated bony injuries which may need concomitant treatment consideration but does not assess the cord itself.
MRI
Apart from routine axial and sagittal T1 and T2 imaging additional sequences should be considered depending on the clinical concern. T2 sequences (e.g. gradient echo, SWI) are more sensitive to hemorrhage, while STIR sequences are more sensitive to associated ligamentous injury.
Spinal cord swelling
focal cord enlargement at the level of trauma without signal change 5 best seen on sagittal T1
Spinal cord edema
as per swelling but with additional increased T2 signal
Spinal cord contusion
thick high T2 signal rim around small central low T1 signal above or below the level of trauma.
blooming on T2 sequences
Intramedullary hemorrhage
thin high T2 signal rim around large central low T1 signal 5
blooming on T2* sequences
see aging blood on MRI for other timescales
Spinal cord transection
discontinuity of cord best seen on sagittal sequences
Clinical evaluation – Your doctor will make a detailed list of all of your symptoms and may conduct blood tests, ask you to move your limbs, follow movement in your eyes, and conduct other tests to narrow down your symptoms.
Imaging tests – Your doctor may order MRI imaging or other forms of radiological imaging to view your spinal column, spinal cord, and brain.
Treatment of Spinal Cord Injury
Spinal injury: First aid
If you suspect a back or neck (spinal) injury, do not move the affected person. Permanent paralysis and other serious complications can result. Assume a person has a spinal injury if:
There’s evidence of a head injury with an ongoing change in the person’s level of consciousness
The person complains of severe pain in his or her neck or back
An injury has exerted substantial force on the back or head
The person complains of weakness, numbness, or paralysis or lacks control of his or her limbs, bladder or bowels
The neck or body is twisted or positioned oddly
Keep the person still – Place heavy towels or rolled sheets on both sides of the neck or hold the head and neck to prevent movement.
Avoid moving the head or neck – Provide as much first aid as possible without moving the person’s head or neck. If the person shows no signs of circulation (breathing, coughing or movement), begin CPR, but do not tilt the head back to open the airway. Use your fingers to gently grasp the jaw and lift it forward. If the person has no pulse, begin chest compressions.
Keep the helmet on – If the person is wearing a helmet, don’t remove it. A football helmet facemask should be removed if you need to access the airway.
Don’t roll alone – If you must roll the person because he or she is vomiting, choking on blood or because you have to make sure the person is still breathing, you need at least one other person. With one of you at the head and another along the side of the injured person, work together to keep the person’s head, neck and back aligned while rolling the person onto one side.
Unlike many other injuries, the most important component of spinal cord injury treatment begins before you even get to the doctor. Remaining still, avoiding moving your spinal column, and prompt emergency care, can all increase the odds that you survive while minimizing the long-term effects of your injury.
From there, doctors will focus on stabilizing you, since the first hours after a spinal cord injury are critical to a patient’s survival. Assistance with breathing, a collar to keep your neck still, blood transfusions, and other procedures to address your immediate symptoms may be necessary.
Eat Nutritiously During Your Recovery
All bones and tissues in the body need certain nutrients in order to heal properly and in a timely manner. Eating a nutritious and balanced diet that includes lots of minerals and vitamins are proven to help heal broken bones of all types. Therefore focus on eating lots of fresh produce (fruits and veggies), whole grains, lean meats, and fish to give your body the building blocks needed to properly repair your. In addition, drink plenty of purified water, milk, and other dairy-based beverages to augment what you eat.
Broken bones need ample minerals (calcium, phosphorus, magnesium, boron) and protein to become strong and healthy again.
Excellent sources of minerals/protein include dairy products, tofu, beans, broccoli, nuts and seeds, sardines, and salmon.
Important vitamins that are needed for bone healing include vitamin C (needed to make collagen), vitamin D (crucial for mineral absorption), and vitamin K (binds calcium to bones and triggers collagen formation).
Conversely, don’t consume food or drink that is known to impair bone/tissue healing, such as alcoholic beverages, sodas, most fast food items, and foods made with lots of refined sugars and preservatives.
Physical Therapy
Although there will be some pain, it is important to maintain arm motion to prevent stiffness. Often, patients will begin doing exercises for elbow motion immediately after the injury. It is common to lose some leg strength. Once the bone begins to heal, your pain will decrease and your doctor may start gentle hip, knee exercises. These exercises will help prevent stiffness and weakness. More strenuous exercises will be started gradually once the fracture is completely healed.
Follow-Up Care
You will need to see your doctor regularly until your fracture heals. During these visits, he or they will take x-rays to make sure the bone is healing in a good position. After the bone has healed, you will be able to gradually return to your normal activities.
Opioids – Also known as narcotics, these medications are intense pain relievers that should only be used under a doctor’s careful supervision.
Topical Medications – These prescription-strength creams, gels, ointments, patches, and sprays help relieve pain and inflammation through the skin.
Calcium & vitamin D3 – to improve bone health and healing fracture. As a general rule, men and women age 50 and older should consume 1,200 milligrams of calcium a day, and 600 international units of vitamin D a day.
Glucosamine & Diacerein, Chondroitin sulfate – can be used to tightening the loose tension, cartilage, ligament, and cartilage, ligament regenerate cartilage or inhabit the further degeneration of cartilage, ligament
Antidepressants – A drug that blocks pain messages from your brain and boosts the effects of endorphins (your body’s natural painkillers).
Your doctor will work with you and your family to construct a detailed plan for your SCI rehabilitation. Every injury is different, but common treatments for a spinal cord injury may involve:
Care to address, but not treat, your immediate symptoms. For instance, a ventilator can help you breathe and a feeding tube can help you eat if you are unable to do so.
Palliative care to help you be more comfortable. If you struggle with insomnia or chronic pain, your doctor might prescribe medication to help.
Lifestyle changes, such as a healthier diet or giving up smoking.
Physical therapy to help retrain your brain and body; many spinal cord injury survivors are able to regain significant mobility with physical therapy.
Family and individual counseling to help you cope with the pain and stress of life with a spinal cord injury.
Surgery as needed to correct injury-related health problems.
Spinal cord injury research is always looking for breakthroughs in treatments, such as stem cell therapy for SCI. Stem cell therapies have long been marketed as a holy grail for a range of diseases, including spinal cord injuries. Recent data suggests that further research could point toward a cure for spinal cord injuries.
Vibration Therapy
Low magnitude mechanical signals (LMMS) as a therapeutic modality has demonstrated bone formation capabilities in both human and rodent models. However, beyond limited case reports there is little evidence available to advocate its definitive therapeutic potential. Similarly, low-intensity vibration treatment protocols have shown some promising results in a small case series of SCI-induced osteoporotic patients. [rx],[rx]
Calcium and Vitamin D
Without question, all patients should be taking calcium and vitamin D supplementation. Patients should be educated on the recommended daily intake for calcium and vitamin D. The National Osteoporosis Foundation (NOF) recommends 1200 to 1500 mg of calcium per day and 800 to 1000 IUs of daily vitamin D for adults over the age of 50. In the setting of SCI-induced osteoporosis, all patients should begin supplementation regardless of age at presentation. [rx]
Anti-Osteoporotic Pharmacotherapy Options
Pharmacotherapy agents work through either anti-resorptive or anabolic means. In general, bisphosphonates are the most commonly prescribed medication class for osteoporosis treatment. These drugs are divided into non-nitrogen and nitrogen-containing compounds. The latter are considered first-line therapy for osteoporosis.[rx]
However, a major concern with SCI-induced osteoporosis coupled with the bisphosphonate anti-resorptive mechanism on bone is the inability to actually demonstrate measurable increases in BMD levels.[rx]
In one study, alendronate was able to prevent further bone loss in 55 patients with chronic SCI-induced osteoporosis at the 2-year follow-up. However, this is a stark contrast to alendronate’s proven track record and documented capabilities to increase BMD values measured in an ambulatory (i.e., not SCI-induced), post-menopausal women with osteoporosis. [rx]
While alendronate, risedronate, and intravenous zoledronic acid have all demonstrated reduced fragility fracture rates in the general osteoporosis population, the clinical evidence has yet to be demonstrated in the SCI-induced osteoporosis population.[rx] Clinicians are encouraged to recognize the subtle differences in efficacy and evidence-based approaches for the pharmacologic management of these vulnerable patients.
Denosumab
Denosumab, a monoclonal antibody against receptor activator of nuclear factor-kappa-? ligand (RANKL), has recently been studied specifically in patients afflicted with SCI-induced osteoporosis. In 2016, one study demonstrated increases in lumbar and femoral BMD values as measured by DXA scans after 1 year of treatment compared to baseline BMD values. Denosumab was administered in a 60 mg every 6 months protocol during the study period. [rx]
Anabolic Agents and Emerging Pharmacotherapy Agents
Teriparatide is a recombinant form of PTH that stimulates osteoblasts to produce more bone. Teriparatide is now FDA approved for osteoporosis treatment in males and females, but more studies are needed in order to improve our understanding of its effects on BMD levels and clinical outcomes in SCI-induced osteoporotic patients. [rx],[rx]
Exercises for after a Spinal Cord Injury
Particularly in the early days after a spinal cord injury, you might be tempted to languish in bed. Moving around certainly seems counter-intuitive when you’ve suffered a catastrophic injury to your body. But the benefits of exercise don’t disappear just because you’ve been injured. Quite the contrary, in fact. Exercises after a spinal cord injury can expedite your SCI rehabilitation in addition to offering a myriad of health benefits.
Exercises
Yoga – ideal for spinal cord injury survivors because the gentle stretching encourages healthy breathing patterns, and can reduce the pain of spending all or most of your day in a wheelchair.
Water Aerobics – The water reduces pain and joint trauma, and can help support your weight even if you’ve lost a significant portion of your mobility or sensation.
Weightlifting – Lifting weights can help you regain significant muscle control. It will also enable you to maintain strength in regions unaffected by your spinal cord injury.
Seated Aerobics – You can still get an incredible aerobic workout from your wheelchair. Talk to your doctor about seated aerobic classes specifically targeted to spinal cord injury survivors
Rowing – Rowing is an ideal aerobic activity because it only requires movement in your upper body, but uses your lower body to stabilize your movements, making it an ideal choice for injury survivors with incomplete spinal cord injuries.
Walking – If your spinal cord injury is incomplete or you have only sustained nerve damage, you may still be able to walk. Maximize your muscle function by walking as frequently as is comfortable, maintaining a steady gait, and an upright posture.
Improving mental health by reducing depression and anxiety
Reducing the risk of cancer
Improving symptoms of chronic pain
Helping you avoid chronic illnesses such as diabetes and osteoporosis
Reducing your risk of falls
Improving your chances of living a longer life.
New technologies
Inventive medical devices can help people with spinal cord injury become more independent and more mobile. Some devices may also restore function. These include:
Modern wheelchair – Improved, lighter weight wheelchairs are making people with spinal cord injuries more mobile and more comfortable. For some, an electric wheelchair may be needed. Some wheelchairs can even climb stairs, travel over rough terrain, and elevate a seated passenger to eye level to reach high places without help.
Computer adaptations – For someone who has limited hand function, computers can be very powerful tools, but they’re difficult to operate. Computer adaptations range from simple to complex, such as key guards or voice recognition.
Electronic aids to daily living – Essentially any device that uses electricity can be controlled with an electronic aid to daily living. Devices can be turned on or off by a switch or voice-controlled and computer-based remotes.
Electrical stimulation devices – These sophisticated devices use electrical stimulation to produce actions. They’re often called functional electrical stimulation systems, and they use electrical stimulators to control arm and leg muscles to allow people with spinal cord injuries to stand, walk, reach and grip.
Robotic gait training – This emerging technology is used for retraining walking ability after a spinal cord injury.
Spinal Cord Injury Recovery
Your SCI rehabilitation journey can be long and often unpredictable. Some spinal cord injury sufferers spontaneously walk years after their injury. Others are never able to move again. While medical science can do a lot to predict what might happen to you, there are no guarantees when it comes to spinal cord injuries. What we do know is that a healthy lifestyle, sound psychological health, family support, and receiving treatment at a model system of care can all improve outcomes.
Physical Recovery
There is no single definition of physical recovery. Though many spinal cord injury survivors do regain some degree of function, some don’t. Thus, focusing solely on physical recovery can leave you feeling hopeless and overwhelmed.
Some common milestones for physical recovery include:
The reduction of swelling at the site of the injury.
Recovering from surgery.
Regaining some sensation below the site of the injury.
Regaining some movement below the site of the injury.
Learning to use assistive devices such as wheelchairs and prostheses.
Finding new ways to complete old tasks; for instance, you might change your approach to sex or making food.
Strengthening your body so you can work around your injuries. You might learn how to type with a part of your body other than your hands, for instance.
Psychological Recovery
Spinal cord injury guides, as well as doctors, lawyers, and loved ones, often focus on physical recovery. But this dogged fixation can actually undermine your psychological recovery. Poor psychological health can worsen your physical health, and believing that physical recovery is the only way to be happy can likewise undermine your psychological well-being. It is possible to be happy even in the face of a painful injury. Indeed, one study found that 86% of quadriplegics rated their lives as better than average.
This attitude can take some time to cultivate, but once you’ve mastered it, you may realize an important truth about life: happiness comes from within, and the way you think about things affects the way you perceive them. Spinal cord injuries are challenging, and there is no shame in seeking psychological help. Many survivors struggle with depression, anxiety, and other mental health issues, but with family support and lots of help, you can find new ways to live a life you love.
Complications
Cardiac and circulatory issues
Respiratory difficulties or loss of function
Numbness or loss of feeling below the injury site
Paralysis
Bladder and bowel function loss
Urinary tract infections (UTIs)
Thermoregulatory impairment (inability to regulate body temperature)
Bladder control – Your bladder will continue to store urine from your kidneys. However, your brain may not be able to control your bladder as well because the message carrier (the spinal cord) has been injured. The changes in bladder control increase your risk of urinary tract infections. The changes may also cause kidney infections and kidney or bladder stones. During rehabilitation, you’ll learn new techniques to help empty your bladder.
Bowel control – Although your stomach and intestines work much as they did before your injury, control of your bowel movements is often altered. A high-fiber diet may help regulate your bowels, and you’ll learn techniques to optimize your bowel function during rehabilitation.
Skin sensation – Below the neurological level of your injury, you may have lost part of or all skin sensations. Therefore, your skin can’t send a message to your brain when it’s injured by certain things such as prolonged pressure, heat, or cold.
Circulatory control – A spinal cord injury may cause circulatory problems ranging from low blood pressure when you rise (orthostatic hypotension) to swelling of your extremities. These circulation changes may also increase your risk of developing blood clots, such as deep vein thrombosis or a pulmonary embolus.
Respiratory system – Your injury may make it more difficult to breathe and cough if your abdominal and chest muscles are affected. These include the diaphragm and the muscles in your chest wall and abdomen.
Muscle tone – Some people with spinal cord injuries experience one of two types of muscle tone problems: uncontrolled tightening or motion in the muscles (spasticity) or soft and limp muscles lacking muscle tone (flaccidity).
Fitness and wellness – Weight loss and muscle atrophy are common soon after a spinal cord injury. Limited mobility may lead to a more sedentary lifestyle, placing you at risk of obesity, cardiovascular disease, and diabetes.
Sexual health – Sexuality, fertility, and sexual function may be affected by a spinal cord injury. Men may notice changes in erection and ejaculation; women may notice changes in lubrication. Physicians specializing in urology or fertility can offer options for sexual functioning and fertility.
Pain – Some people experience pain, such as muscle or joint pain, from overuse of particular muscle groups. Nerve pain can occur after a spinal cord injury, especially in someone with an incomplete injury.
Depression – Coping with all the changes a spinal cord injury brings and living with pain causes some people to experience depression.
Prevention
The leading causes of spinal cord injury are road traffic crashes, falls, and violence (including attempted suicide). A significant proportion of traumatic spinal cord injury is due to work or sports-related injuries. Effective interventions are available to prevent several of the main causes of spinal cord injury, including improvements in roads, vehicles and people’s behavior on the roads to avoid road traffic crashes, window guards to prevent falls, and policies to thwart the harmful use of alcohol and access to firearms to reduce violence.
Drive safely – Car crashes are one of the most common causes of spinal cord injuries. Wear a seat belt every time you drive or ride in a car. Make sure that your children wear a seat belt or use an age- and weight-appropriate child safety seat. To protect them from airbag injuries, children under age 12 should always ride in the back seat.
Check water depth before diving – To make sure you don’t dive into shallow water, don’t dive into a pool unless it’s 12 feet (about 3.7 meters) or deeper, don’t dive into an aboveground pool, and don’t dive into any water of which you don’t know the depth.
Prevent falls – Use a step stool with a grab bar to reach objects in high places. Add handrails along stairways. Put nonslip mats on tile floors and in the tub or shower. For young children, use safety gates to block stairs and consider installing window guards.
Take precautions when playing sports – Always wear recommended safety gear. Avoid leading with your head in sports. For example, don’t slide headfirst in baseball, and don’t tackle using the top of your helmet in football. Use a spotter for new moves in gymnastics.
Don’t drink and drive. Don’t drive while intoxicated or under the influence of drugs. Don’t ride with a driver who’s been drinking.
Improving care and overcoming barriers
Many of the consequences associated with spinal cord injury do not result from the condition itself, but from inadequate medical care and rehabilitation services, and from barriers in the physical, social and policy environments. Implementation of the UN Convention on the Rights of Persons with Disabilities (CRPD) requires action to address these gaps and barriers. Essential measures for improving the survival, health, and participation of people with spinal cord injury include the following.
Timely, appropriate pre-hospital management: quick recognition of suspected spinal cord injury, rapid evaluation, and initiation of injury management, including immobilization of the spine.
Acute care (including surgical intervention) appropriate to the type and severity of the injury, degree of instability, presence of neural compression, and in accordance with the wishes of the patient and their family.
Access to ongoing health care, health education, and products (e.g. catheters) to reduce the risk of secondary conditions and improve the quality of life.
Access to skilled rehabilitation and mental health services to maximize functioning, independence, overall wellbeing, and community integration. Management of bladder and bowel function is of primary importance.
Access to appropriate assistive devices that can enable people to perform everyday activities they would not otherwise be able to undertake, reducing functional limitations and dependency. Only 5-15% of people in low- and middle-income countries have access to the assistive devices they need.
Specialized knowledge and skills among providers of medical care and rehabilitation services.
Essential measures to secure the right to education and economic participation include legislation, policy, and programs that promote the following:
physically accessible homes, schools, workplaces, hospitals, and transportation;
inclusive education;
elimination of discrimination in employment and educational settings;
Vocational rehabilitation to optimize the chance of employment;
micro-finance and other forms of self-employment benefits to support alternative forms of economic self-sufficiency;
access to social support payments that do not act as a disincentive to return to work; and
correct understanding of spinal cord injury and positive attitudes towards people living with it.
WHO response
WHO works across the spectrum from primary prevention of traumatic and non-traumatic causes of spinal cord injury, improvements in trauma care, strengthening health and rehabilitation services, and support for the inclusion of people with spinal cord injuries. WHO:
works in a multisectoral manner, in partnership with national stakeholders from a variety of sectors (e.g. health, police, transport, education) to improve prevention of spinal cord injury including of road traffic injuries, falls, violence and neural tube defects;
guides and supports the Member States to increase awareness of disability issues, and promotes the inclusion of disability as a component in national health policies and programs;
facilitates data collection and dissemination of disability-related data and information;
develops normative tools, including guidelines and good practice examples to strengthen primary prevention (road traffic crashes, falls and violence), trauma care, health care, rehabilitation and support and assistance;
builds capacity among health policy-makers and service providers;
promotes scaling up of community-based rehabilitation; and
promotes strategies to ensure that people with disabilities are knowledgeable about their own health conditions, and that health-care personnel support and protect the rights and dignity of persons with disabilities.
Following strategies should be undertaken for better recovery
Close routine follow-up with the neurologist/internist.
Educate patients for clean intermittent catheterization (CIC) to avoid urinary tract infections and secondary complications.
Educate patients to avoid immobility, and regularly change position after 2-4 hours.
Close follow-up with a physical therapist for muscle and core strengthening exercises to avoid muscle atrophy.
Blood pressure monitoring at home.
Close follow-up with the psychiatrist to look for any signs of depression and suicidal ideation.
Knee arthroplasty is a reconstruction of the knee joint. It is more commonly referred to as a total knee replacement and is a very reliable procedure with predictable results. Total knee arthroplasty (TKA) is an excellent treatment option for individuals with symptomatic osteoarthritis in at least 2 of the 3 compartments of the knee and who have failed conservative treatment.[rx][rx] Additionally, partial knee arthroplasty (PKA) is an excellent treatment option for individuals with symptomatic osteoarthritis localized to 1 compartment of the knee and who have failed conservative treatment.[rx] The primary goal of either surgery is durable pain relief with the improvement of functional status.
Anatomy and Physiology of Knee Arthroplasty
The knee is a synovial hinge joint with minimal rotational motion. It is comprised of the distal femur, proximal tibia, and the patella. There are 3 separate articulations and compartments: medial femorotibial, lateral femorotibial, and patellofemoral. The stability of the knee joint is provided by the congruity of the joint as well as by the collateral ligaments. The capsule surrounds the entire joint and extends proximally into the suprapatellar pouch. Articular cartilage covers the femoral condyles, tibial plateaus, trochlear groove, and patellar facets. Menisci are interposed in the medial and lateral compartments between the femur and tibia which act to protect the articular cartilage and support the knee.
The mechanical axis of the femur, defined by a line drawn from the center of the femoral head to the center of the knee, is 3 degrees valgus to the vertical axis. The anatomic axis of the femur, defined by a line bisecting the femoral shaft, is 6 degrees valgus to the mechanical axis of the femur and 9 degrees valgus to the vertical axis.[rx] The proximal tibia is oriented to 3 degrees of varus. The varus position of the proximal tibia, along with the offset of the hip center of rotation, results in the weight-bearing surface of the tibia is parallel to the ground. The sagittal alignment of the proximal tibia is sloped posteriorly approximately 5 to 7 degrees. The asymmetry of the natural bony anatomy maintains the alignment of the joint and ligamentous tension.
Indications of Knee Arthroplasty
TKA is a well-described treatment option for patients suffering from knee pain secondary to osteoarthritis who have failed conservative treatment measures. It is a reliable procedure that provides pain relief and improves the patient’s functional status.[rx] Furthermore, the need for correction of a significant or progressive deformity at the knee with evidence of osteoarthritis can also be an indication for a TKA. A patient with persistent knee pain without radiographic evidence of knee osteoarthritis should have further workup to exclude other possible sources of their pain.
Presence of active infection elsewhere in the body
Extensor mechanism dysfunction
Medically unstable patient
Relative
Neuropathic joint
Poor overlying skin condition
Morbid obesity
Noncompliance due to major psychiatric disorder, alcohol, or drug abuse
Insufficient bone stock for reconstruction
Poor patient motivation or unrealistic expectation
Severe peripheral vascular disease
Equipment of Knee Arthroplasty
A TKA system will consist of instrumentation that helps the surgeon prepare the ends of the femur, tibia, and patella to receive an implant. The instrumentation will be specific to the brand and type of implant being used with each company and model having specific intricacies.
In general, the instrumentation will consist of:
Intramedullary femoral guide to help establish the distal femoral alignment
The distal femoral cutting guide
Femoral sizing guide
The 4-in-1 femoral cutting guide
The extramedullary or intramedullary tibial guide
The proximal tibial cutting guide
Patella sizing guide
Femoral component trial
Tibial baseplate trial
Patellar button trial
Trial plastic bearing
The final implants will come in individual sterile packages and will consist of:
Femoral component, typically made of cobalt-chrome
Tibial component, typically made of cobalt-chrome or titanium
Tibial polyethylene bearing, made of an ultra high molecular weight (UHMW) polyethylene
Patellar button, made of UHMW polyethylene
Personnel
Anesthesia team
Operating room nurse
Surgical technician
Surgical assistant
Preparation
Full medical and drug history before surgery
Appropriate pre-surgical workup, clearance, and optimization
Pre-operative radiographs of the affected knee
Pre-operative templating of the affected knee to estimate the component size
Primary TKA system of choice
Have various final implant sizes ready and available in the hospital
Have increasing prosthesis constraint options ready and available in the hospital
Have revision total knee replacement system of choice ready and available if needed
+/- antibiotic cement, surgeon preference
The Technique of Knee Arthroplasty
The goal of TKA is the same regardless of surgeon, implant, or technique. The variability in the procedure lies in the technique. Some of the variations in operative technique for TKA are listed below.
General anesthesia versus regional anesthesia
Tourniquet versus tourniquet-less surgery
Standard versus patient-specific instrumentation
Standard versus patient-specific implants
Traditional versus robotic-assisted TKA
Traditional versus navigation-assisted TKA
Traditional versus sensor-assisted TKA
Measured resection versus gap balancing
Cruciate-retaining implant versus cruciate stabilized the implant
Accidental Knee Dislocation/Knee Injury is a potentially devastating injury and is often a surgical emergency. This injury requires prompt identification, evaluation with appropriate imaging, and consultation with surgery for definitive treatment. Vascular injury and compartment syndrome are dreaded complications that the clinician should not miss in the workup of a knee dislocation. Note that this is in distinct contrast to patellar dislocations, which generally do not require immediate surgical or vascular intervention.[rx][rx]
A knee dislocation is a knee injury in which there is a complete disruption of the joint between the tibia and the femur. Symptoms include knee pain and instability of the knee. Complications may include injury to an artery around the knee, most commonly the artery behind the knee, or compartment syndrome.[rx][rx][rx]
Types /Classification of Knee Dislocation
They may be divided into five types: anterior, posterior, lateral, medial, and rotatory. This classification is based on the movement of the tibia with respect to the femur. Anterior dislocations are the most common, followed by posterior dislocations. They may also be classified based on what ligaments are damaged.[rx]
Kennedy classification based on the direction of displacement of the tibia
Anterior (30-50%)
most common
due to hyperextension injury
usually involves tear of PCL
an arterial injury is generally an intimal tear due to traction
the highest rate of peroneal nerve injury
Posterior (30-40%)
2nd most common
due to axial load to the flexed knee (dashboard injury)
The highest rate of vascular injury (25%) based on Kennedy classification
has highest incidence of a complete tear of the popliteal artery
Lateral (13%)
due to a varus or valgus force
usually involves tears of both ACL and PCL
Medial (3%)
varus or valgus force
usually disrupted PLC and PCL
Rotational (4%)
posterolateral is most common rotational dislocation
usually irreducible
buttonholing of femoral condyle through the capsule
Anatomic Classification System
TYPE
DESCRIPTION
KDI
Dislocation with single cruciate + single collateral ligament
KDII
Both cruciate ligaments torn, collateral ligaments intact
KDIIIM
ACL + PCL + MCL
L
ACL + PCL + LCL/PLC
KDIV
Both cruciate ligaments + both collateral ligaments torn
KDV
Fracture-dislocation
The letters C and N can be added to denote arterial and neurologic injury, respectively.
Schenck Classification
based on a pattern of multi ligamentous injury of knee dislocation (KD)
The Schenck and Wascher classifications of knee dislocations.
Group
Sub-Group
Definition
KD-I
Single cruciate only
KD-II
Bicruciate disruption only (rare)
KD-III
Bicruciate and posteromedial or posterolateral disruption (common)
KD-IV
Bicruciate and posteromedial and posterolateral disruption
KD-V
Dislocation with associated fracture
KD-V1
Single cruciate only
KD-V2
Bicruciate disruption only
KD-V3M
Bicruciate and posteromedial disruption
KD-V3L
Bicruciate and posterolateral disruption
KD-V4
Bicruciate and posteromedial and posterolateral disruption
C
Indicates associated arterial injury when suffixed to main group
N
Indicates associated neural injury when suffixed to main group
Causes of Accidental Knee Dislocation
Car accidents – If you bang your knee against a hard surface like your dashboard, the force of the blow may be strong enough to dislocate your knee.
Sports injuries – This is less common than car accidents, but it’s possible to dislocate your knee if you collide with great force with another player or with the ground when your knee is bent, or if you over-extend your knee (bend it back farther than it’s supposed to go).
Hard falls – It may happen to skiers or runners who lose control and fall on a bent or overextended knee. You may even dislocate your knee if you fall after stepping into a hole in the ground by mistake.
Result of major trauma – and about half occur as a result of minor trauma.[rx] Major trauma may include mechanisms like falls from a significant height, motor vehicle collisions, or a pedestrian being hit by a motor vehicle.
Genetic Disorder – often have other injuries.[rx] Minor trauma may include tripping while walking or while playing sports. Risk factors include obesity.[rx] The condition may also occur in a number of genetic disorders such as Ellis–van Creveld syndrome, Larsen syndrome, and Ehlers–Danlos syndrome.[rx]
Sudden forceful fall down
Road traffic accident
Falls – Falling onto an outstretched hand is one of the most common causes of the broken or dislocation knee.
Sports injuries – Many cervical spine fractures occur during contact sports or sports in which you might fall onto an outstretched hand — such as in-line skating or snowboarding.
Motor vehicle crashes – Motor vehicle crashes can cause the knee dislocation to break, sometimes into many pieces, and often require surgical repair.
Have osteoporosis – a disease that weakens your bones
Eave low muscle mass or poor muscle strength – or lack agility and have poor balance (these conditions make you more likely to fall)
Walk or do other activities in the snow or on the ice – or do activities that require a lot of forwarding momenta, such as in-line skating and skiing.
Previous fractures record.
Wave an inadequate intake of calcium or vitamin D.
Football or soccer, especially on artificial turf
Athletic injury with a sports injury.
The ligamentum patellae. Attached above to the lower border of the patella and below to the tuberosity of the tibia. A continuation of the central portion of the common tendon of the quadriceps femoris muscle. The oblique popliteal ligament. A tendinous expansion derived from the semimembranosus muscle. It strengthens the posterior aspect of the capsule.
Symptoms of Accidental Knee Dislocation
CT angiogram 3D reconstruction, the posterior view showing a normal artery on the left, and occlusion to right popliteal artery as a result of a knee dislocation
Symptoms include knee pain. The joint may also be obviously out of place. A joint effusion is not always present.[rx]
Hearing a “popping” sound at the time of injury
Severe pain in the area of the knee
A visible deformity at the knee joint
Instability of the knee joint, or feeling like your knee joint is “giving way”
Limitations in the range of movement of your knee
Inability to continue with activities, whether they involve day-to-day tasks or sports
Feeling the kneecap shift or slide out of the groove
Feeling the knee buckle or give way
Hearing a popping sound when the patella dislocates
Swelling
A change in the knee’s appearance — the knee may appear misshapen or deformed
Apprehension or fear when running or changing direction.
Ankle-Brachial Index (ABI) – Normal ABI (as well as pulses, Capillary Refill) may not exclude popliteal artery disruption
Hard signs of vascular injury
Distal pulse loss or ischemia (e.g. pallor, coolness)
Active bleeding
Expanding hematoma
Palpable thrill or bruit over the popliteal artery
Neurologic Exam (especially peroneal nerve)
First web space and dorsal foot sensation
Ankle dorsiflexion
Multidirectional instability
Multidirectional instability may be only finding if knee spontaneously reduced prior to presentation
Three of four ligaments are likely injured (ACL Tear, PCL Tear, LCL tear, MCL tear)
Skin changes
Dimple Sign – Anteromedial skinfold at medial joint line. Seen in posterolateral dislocation (not reducible without surgery)
Skin necrosis – Entrapped skin at femoral condyle
Overlying Laceration – Suggests open Knee Dislocation (accompanies 20-30% of Knee Dislocations)
Others exam may include
Checking the pulse in several places on your leg and knee – This is called checking posterior tibial and dorsal pedal pulses, which are located in the region of the knee and foot. Lower pulses in your injured leg could indicate an injury to a blood vessel in your leg.
Checking the blood pressure in your leg – Called the ankle-brachial index (ABI), this test compares the blood pressure measured in your arm to the blood pressure measured in your ankle. A low ABI measurement can indicate poor blood flow to your lower extremities.
Checking your sense of touch or sensation – Your doctor will assess the feeling in the injured leg versus the unaffected leg.
Checking nerve conduction – Tests like electromyography (EMG) or nerve conduction velocity (NCV) will measure the function of the nerves in your leg and knee.
Checking your skin color and temperature – If your leg is cold or changing colors, there may be blood vessel problems.
X-rays – These tests create clear pictures of bone. Your doctor may order x-rays to look for skeletal abnormalities in the knee, such as a shallow groove in the femur.
Magnetic resonance imaging (MRI) scans – These scans create better pictures of the soft structures surrounding the knee, like ligaments. An MRI is seldom necessary because the doctor can usually diagnose a dislocated patella through an examination and x-rays. However, if your doctor needs additional, more detailed images, he or she may order an MRI.
Treatment of Accidental Knee Dislocation
Nonoperative
Immobilization – Your doctor may recommend that your child wear a brace for 3 to 4 weeks. This stabilizes the knee while it heals.
Weightbearing – Because putting weight on the knee may cause pain and slow the healing process, your doctor may recommend using crutches for the first week or two after the injury.
Physical therapy – Once the knee has started to heal, your child’s doctor will recommend physical therapy to help your child regain normal motion. Specific exercises will strengthen the thigh muscles holding the knee joint in place. Your child’s commitment to the exercise program is important for a successful recovery. Typically, children return to activity 3 to 6 weeks after the injury.
Emergent closed reduction followed by vascular assessment/consult – indications to considered an orthopedic emergency, vascular consult indicated if pulses are absent or diminished following reduction if arterial injury confirmed by arterial duplex ultrasound or CT angiography
Immobilization as definitive management – successful closed reduction without vascular compromise, most cases require some form of surgical stabilization following reduction, outcomes of worse outcomes are seen with nonoperative management/prolonged immobilization will lead to loss of ROM with persistent instability.
Rest Your Leg – Once you’re discharged from the hospital in a legislating, your top priority is to rest your and not further inflame the injury. Of course, the arm sling not only provides support, but it also restricts movement, which is why you should keep it on even during sleep. Avoiding the temptation to move your will help the bone mend quicker and the pain fades away sooner.
Depending on what you do for a living and if the injury is to your dominant side, you may need to take a couple of weeks off work to recuperate.
Healing takes between four to six weeks in younger people and up to 12 weeks in the elderly, but it depends on the severity of the radial head fractures.
Athletes in good health are typically able to resume their sporting activities within two months of breaking they’re ulnar styloid depending on the severity of the break and the specific sport.
Sleeping on your back (with the sling on) is necessary to keep the pressure off your shoulder and prevent stressing the hip injury.
Eat Nutritiously During Your Recovery
All bones and tissues in the body need certain nutrients in order to heal properly and in a timely manner. Eating a nutritious and balanced diet that includes lots of minerals and vitamins are proven to help heal broken bones of all types. Therefore focus on eating lots of fresh produce (fruits and veggies), whole grains, lean meats, and fish to give your body the building blocks needed to properly repair your. In addition, drink plenty of purified water, milk, and other dairy-based beverages to augment what you eat.
Broken bones need ample minerals (calcium, phosphorus, magnesium, boron) and protein to become strong and healthy again.
Excellent sources of minerals/protein include dairy products, tofu, beans, broccoli, nuts and seeds, sardines, and salmon.
Important vitamins that are needed for bone healing include vitamin C (needed to make collagen), vitamin D (crucial for mineral absorption), and vitamin K (binds calcium to bones and triggers collagen formation).
Conversely, don’t consume food or drink that is known to impair bone/tissue healing, such as alcoholic beverages, sodas, most fast food items and foods made with lots of refined sugars and preservatives.
Physical Therapy
Although there will be some pain, it is important to maintain arm motion to prevent stiffness. Often, patients will begin doing exercises for elbow motion immediately after the injury. It is common to lose some leg strength. Once the bone begins to heal, your pain will decrease and your doctor may start gentle hip, knee exercises. These exercises will help prevent stiffness and weakness. More strenuous exercises will be started gradually once the fracture is completely healed.
Follow-Up Care
You will need to see your doctor regularly until your fracture heals. During these visits, he or they will take x-rays to make sure the bone is healing in a good position. After the bone has healed, you will be able to gradually return to your normal activities.
Opioids – Also known as narcotics, these medications are intense pain relievers that should only be used under a doctor’s careful supervision.
Topical Medications – These prescription-strength creams, gels, ointments, patches, and sprays help relieve pain and inflammation through the skin.
Calcium & vitamin D3 – to improve bone health and healing fracture. As a general rule, men and women age 50 and older should consume 1,200 milligrams of calcium a day, and 600 international units of vitamin D a day.
Glucosamine & Diacerein, Chondroitin sulfate – can be used to tightening the loose tension, cartilage, ligament, and cartilage, ligament regenerate cartilage or inhabit the further degeneration of cartilage, ligament
Antidepressants – A drug that blocks pain messages from your brain and boosts the effects of endorphins (your body’s natural painkillers).
Surgical Treatment
Open reduction
irreducible knee
posterolateral dislocation
open fracture-dislocation
obesity (may be difficult to obtain closed)
vascular injury
External fixation
vascular repair (takes precedence)
open fracture-dislocation
compartment syndrome
obese (if difficult to maintain reduction)
polytrauma patient
Delayed ligamentous reconstruction/repair
instability will require some kind of ligamentous repair or fixation
patients can be placed in a knee immobilizer until treated operatively
improved outcomes with early treatment (within 3 weeks)
Arthroscopy +/- open debridement
Arthroscopic or open debridement with removal of any loose bodies may be necessary for displaced osteochondral fractures or loose bodies.
MPFL re-attachment or reconstruction (proximal realignment)
Proximal realignment constitutes the reconstruction of the MPFL. In brief, to repair the ligament, a longitudinal incision is made at the border of the VMO, just anterior to the medial epicondyle. The ligament is usually re-attached to the femur using bone anchors. If the patient has had recurrent dislocations, then reconstruction may be necessary by harvesting gracilis or semitendinosus which are then attached to the patella and femur.
Isolated repair/reconstruction of the MPFL is not a recommendation in those with bony abnormalities including TT-TG distance greater than 20mm, convex trochlear dysplasia, severe patella alta, advanced cartilage degeneration or severe femoral anteversion.[rx]
Lateral release (distal realignment)
A lateral release cuts the retinaculum on the lateral aspect of the knee joint. The aim is to improve the alignment of the patella by reducing the lateral pull.
Osteotomy (distal realignment)
Where there is abnormal anatomy contributing to poor patella tracking and a high TT-TG distance, the alignment correction can be through an osteotomy. The most common procedure of this type is known as the Fulkerson-type osteotomy and involves an osteotomy as well as removing the small portion of bone to which the tendon attaches and repositioning it in a more anteromedial position on the tibia.
Trochleoplasty
Trochleoplasty is indicated in recurrent dislocators with a convex or flat trochlea. The trochlear groove is deepened to create a groove for the patella to glide through; this may take place alongside an MPFL reconstruction. Studies suggest it is not advisable in those with open growth plates or severely degenerative joints. This procedure is uncommon except in refractory cases.
Complications of Traumatic Knee Dislocation
Vascular compromise
incidence of – 5-15% in all dislocations. 40-50% in anterior or posterior dislocations
risk factors – KD IV injuries have the highest rate of vascular injuries
treatment-emergent vascular repair and prophylactic fasciotomies
Stiffness (arthrofibrosis)
incidence – most common complication (38%)
risk factors – more common with delayed mobilization
avoid stiffness with early reconstruction and motion
arthroscopic lysis of adhesion
manipulation under anesthesia
Laxity and instability
incidence – 37% of some instability, however, redislocation is uncommon
treatment – arthroscopic lysis of adhesion, manipulation under anesthesia
Peroneal nerve injury
incidence- 25% occurrence of a peroneal nerve injury, 50% recover partially
posterolateral dislocations
Treatment
A to prevent equinus contracture
neurolysis or exploration at the time of reconstruction
nerve repair or reconstruction or tendon transfers if chronic nerve palsy persists
a dynamic tendon transfer involves transferring the posterior tibial tendon (PTT) to the foot
Traumatic Knee Dislocation/Knee Injury is a potentially devastating injury and is often a surgical emergency. This injury requires prompt identification, evaluation with appropriate imaging, and consultation with surgery for definitive treatment. Vascular injury and compartment syndrome are dreaded complications that the clinician should not miss in the workup of a knee dislocation. Note that this is in distinct contrast to patellar dislocations, which generally do not require immediate surgical or vascular intervention.[rx][rx]
A knee dislocation is a knee injury in which there is a complete disruption of the joint between the tibia and the femur. Symptoms include knee pain and instability of the knee. Complications may include injury to an artery around the knee, most commonly the artery behind the knee, or compartment syndrome.[rx][rx][rx]
Types /Classification of Knee Dislocation
They may be divided into five types: anterior, posterior, lateral, medial, and rotatory. This classification is based on the movement of the tibia with respect to the femur. Anterior dislocations are the most common, followed by posterior dislocations. They may also be classified based on what ligaments are damaged.[rx]
Kennedy classification based on the direction of displacement of the tibia
Anterior (30-50%)
most common
due to hyperextension injury
usually involves tear of PCL
an arterial injury is generally an intimal tear due to traction
the highest rate of peroneal nerve injury
Posterior (30-40%)
2nd most common
due to axial load to the flexed knee (dashboard injury)
The highest rate of vascular injury (25%) based on Kennedy classification
has highest incidence of a complete tear of the popliteal artery
Lateral (13%)
due to a varus or valgus force
usually involves tears of both ACL and PCL
Medial (3%)
varus or valgus force
usually disrupted PLC and PCL
Rotational (4%)
posterolateral is most common rotational dislocation
usually irreducible
buttonholing of femoral condyle through the capsule
Anatomic Classification System
TYPE
DESCRIPTION
KDI
Dislocation with single cruciate + single collateral ligament
KDII
Both cruciate ligaments torn, collateral ligaments intact
KDIIIM
ACL + PCL + MCL
L
ACL + PCL + LCL/PLC
KDIV
Both cruciate ligaments + both collateral ligaments torn
KDV
Fracture-dislocation
The letters C and N can be added to denote arterial and neurologic injury, respectively.
Schenck Classification
based on a pattern of multi ligamentous injury of knee dislocation (KD)
The Schenck and Wascher classifications of knee dislocations.
Group
Sub-Group
Definition
KD-I
Single cruciate only
KD-II
Bicruciate disruption only (rare)
KD-III
Bicruciate and posteromedial or posterolateral disruption (common)
KD-IV
Bicruciate and posteromedial and posterolateral disruption
KD-V
Dislocation with associated fracture
KD-V1
Single cruciate only
KD-V2
Bicruciate disruption only
KD-V3M
Bicruciate and posteromedial disruption
KD-V3L
Bicruciate and posterolateral disruption
KD-V4
Bicruciate and posteromedial and posterolateral disruption
C
Indicates associated arterial injury when suffixed to main group
N
Indicates associated neural injury when suffixed to main group
Causes of Traumatic Knee Dislocation
Car accidents – If you bang your knee against a hard surface like your dashboard, the force of the blow may be strong enough to dislocate your knee.
Sports injuries – This is less common than car accidents, but it’s possible to dislocate your knee if you collide with great force with another player or with the ground when your knee is bent, or if you over-extend your knee (bend it back farther than it’s supposed to go).
Hard falls – It may happen to skiers or runners who lose control and fall on a bent or overextended knee. You may even dislocate your knee if you fall after stepping into a hole in the ground by mistake.
Result of major trauma – and about half occur as a result of minor trauma.[rx] Major trauma may include mechanisms like falls from a significant height, motor vehicle collisions, or a pedestrian being hit by a motor vehicle.
Genetic Disorder – often have other injuries.[rx] Minor trauma may include tripping while walking or while playing sports. Risk factors include obesity.[rx] The condition may also occur in a number of genetic disorders such as Ellis–van Creveld syndrome, Larsen syndrome, and Ehlers–Danlos syndrome.[rx]
Sudden forceful fall down
Road traffic accident
Falls – Falling onto an outstretched hand is one of the most common causes of the broken or dislocation knee.
Sports injuries – Many cervical spine fractures occur during contact sports or sports in which you might fall onto an outstretched hand — such as in-line skating or snowboarding.
Motor vehicle crashes – Motor vehicle crashes can cause the knee dislocation to break, sometimes into many pieces, and often require surgical repair.
Have osteoporosis – a disease that weakens your bones
Eave low muscle mass or poor muscle strength – or lack agility and have poor balance (these conditions make you more likely to fall)
Walk or do other activities in the snow or on the ice – or do activities that require a lot of forwarding momenta, such as in-line skating and skiing.
Previous fractures record.
Wave an inadequate intake of calcium or vitamin D.
Football or soccer, especially on artificial turf
Athletic injury with a sports injury.
The ligamentum patellae. Attached above to the lower border of the patella and below to the tuberosity of the tibia. A continuation of the central portion of the common tendon of the quadriceps femoris muscle. The oblique popliteal ligament. A tendinous expansion derived from the semimembranosus muscle. It strengthens the posterior aspect of the capsule.
Symptoms of Child Knee Dislocation
CT angiogram 3D reconstruction, the posterior view showing a normal artery on the left, and occlusion to right popliteal artery as a result of a knee dislocation
Symptoms include knee pain. The joint may also be obviously out of place. A joint effusion is not always present.[rx]
Hearing a “popping” sound at the time of injury
Severe pain in the area of the knee
A visible deformity at the knee joint
Instability of the knee joint, or feeling like your knee joint is “giving way”
Limitations in the range of movement of your knee
Inability to continue with activities, whether they involve day-to-day tasks or sports
Feeling the kneecap shift or slide out of the groove
Feeling the knee buckle or give way
Hearing a popping sound when the patella dislocates
Swelling
A change in the knee’s appearance — the knee may appear misshapen or deformed
Apprehension or fear when running or changing direction.
Ankle-Brachial Index (ABI) – Normal ABI (as well as pulses, Capillary Refill) may not exclude popliteal artery disruption
Hard signs of vascular injury
Distal pulse loss or ischemia (e.g. pallor, coolness)
Active bleeding
Expanding hematoma
Palpable thrill or bruit over the popliteal artery
Neurologic Exam (especially peroneal nerve)
First web space and dorsal foot sensation
Ankle dorsiflexion
Multidirectional instability
Multidirectional instability may be only finding if knee spontaneously reduced prior to presentation
Three of four ligaments are likely injured (ACL Tear, PCL Tear, LCL tear, MCL tear)
Skin changes
Dimple Sign – Anteromedial skinfold at medial joint line. Seen in posterolateral dislocation (not reducible without surgery)
Skin necrosis – Entrapped skin at femoral condyle
Overlying Laceration – Suggests open Knee Dislocation (accompanies 20-30% of Knee Dislocations)
Others exam may include
Checking the pulse in several places on your leg and knee – This is called checking posterior tibial and dorsal pedal pulses, which are located in the region of the knee and foot. Lower pulses in your injured leg could indicate an injury to a blood vessel in your leg.
Checking the blood pressure in your leg – Called the ankle-brachial index (ABI), this test compares the blood pressure measured in your arm to the blood pressure measured in your ankle. A low ABI measurement can indicate poor blood flow to your lower extremities.
Checking your sense of touch or sensation – Your doctor will assess the feeling in the injured leg versus the unaffected leg.
Checking nerve conduction – Tests like electromyography (EMG) or nerve conduction velocity (NCV) will measure the function of the nerves in your leg and knee.
Checking your skin color and temperature – If your leg is cold or changing colors, there may be blood vessel problems.
X-rays – These tests create clear pictures of bone. Your doctor may order x-rays to look for skeletal abnormalities in the knee, such as a shallow groove in the femur.
Magnetic resonance imaging (MRI) scans – These scans create better pictures of the soft structures surrounding the knee, like ligaments. An MRI is seldom necessary because the doctor can usually diagnose a dislocated patella through an examination and x-rays. However, if your doctor needs additional, more detailed images, he or she may order an MRI.
Treatment of Traumatic Knee Dislocation
Nonoperative
Immobilization – Your doctor may recommend that your child wear a brace for 3 to 4 weeks. This stabilizes the knee while it heals.
Weightbearing – Because putting weight on the knee may cause pain and slow the healing process, your doctor may recommend using crutches for the first week or two after the injury.
Physical therapy – Once the knee has started to heal, your child’s doctor will recommend physical therapy to help your child regain normal motion. Specific exercises will strengthen the thigh muscles holding the knee joint in place. Your child’s commitment to the exercise program is important for a successful recovery. Typically, children return to activity 3 to 6 weeks after the injury.
Emergent closed reduction followed by vascular assessment/consult – indications to considered an orthopedic emergency, vascular consult indicated if pulses are absent or diminished following reduction if arterial injury confirmed by arterial duplex ultrasound or CT angiography
Immobilization as definitive management – successful closed reduction without vascular compromise, most cases require some form of surgical stabilization following reduction, outcomes of worse outcomes are seen with nonoperative management/prolonged immobilization will lead to loss of ROM with persistent instability.
Rest Your Leg – Once you’re discharged from the hospital in a legislating, your top priority is to rest your and not further inflame the injury. Of course, the arm sling not only provides support, but it also restricts movement, which is why you should keep it on even during sleep. Avoiding the temptation to move your will help the bone mend quicker and the pain fades away sooner.
Depending on what you do for a living and if the injury is to your dominant side, you may need to take a couple of weeks off work to recuperate.
Healing takes between four to six weeks in younger people and up to 12 weeks in the elderly, but it depends on the severity of the radial head fractures.
Athletes in good health are typically able to resume their sporting activities within two months of breaking they’re ulnar styloid depending on the severity of the break and the specific sport.
Sleeping on your back (with the sling on) is necessary to keep the pressure off your shoulder and prevent stressing the hip injury.
Eat Nutritiously During Your Recovery
All bones and tissues in the body need certain nutrients in order to heal properly and in a timely manner. Eating a nutritious and balanced diet that includes lots of minerals and vitamins are proven to help heal broken bones of all types. Therefore focus on eating lots of fresh produce (fruits and veggies), whole grains, lean meats, and fish to give your body the building blocks needed to properly repair your. In addition, drink plenty of purified water, milk, and other dairy-based beverages to augment what you eat.
Broken bones need ample minerals (calcium, phosphorus, magnesium, boron) and protein to become strong and healthy again.
Excellent sources of minerals/protein include dairy products, tofu, beans, broccoli, nuts and seeds, sardines, and salmon.
Important vitamins that are needed for bone healing include vitamin C (needed to make collagen), vitamin D (crucial for mineral absorption), and vitamin K (binds calcium to bones and triggers collagen formation).
Conversely, don’t consume food or drink that is known to impair bone/tissue healing, such as alcoholic beverages, sodas, most fast food items and foods made with lots of refined sugars and preservatives.
Physical Therapy
Although there will be some pain, it is important to maintain arm motion to prevent stiffness. Often, patients will begin doing exercises for elbow motion immediately after the injury. It is common to lose some leg strength. Once the bone begins to heal, your pain will decrease and your doctor may start gentle hip, knee exercises. These exercises will help prevent stiffness and weakness. More strenuous exercises will be started gradually once the fracture is completely healed.
Follow-Up Care
You will need to see your doctor regularly until your fracture heals. During these visits, he or they will take x-rays to make sure the bone is healing in a good position. After the bone has healed, you will be able to gradually return to your normal activities.
Opioids – Also known as narcotics, these medications are intense pain relievers that should only be used under a doctor’s careful supervision.
Topical Medications – These prescription-strength creams, gels, ointments, patches, and sprays help relieve pain and inflammation through the skin.
Calcium & vitamin D3 – to improve bone health and healing fracture. As a general rule, men and women age 50 and older should consume 1,200 milligrams of calcium a day, and 600 international units of vitamin D a day.
Glucosamine & Diacerein, Chondroitin sulfate – can be used to tightening the loose tension, cartilage, ligament, and cartilage, ligament regenerate cartilage or inhabit the further degeneration of cartilage, ligament
Antidepressants – A drug that blocks pain messages from your brain and boosts the effects of endorphins (your body’s natural painkillers).
Surgical Treatment
Open reduction
irreducible knee
posterolateral dislocation
open fracture-dislocation
obesity (may be difficult to obtain closed)
vascular injury
External fixation
vascular repair (takes precedence)
open fracture-dislocation
compartment syndrome
obese (if difficult to maintain reduction)
polytrauma patient
Delayed ligamentous reconstruction/repair
instability will require some kind of ligamentous repair or fixation
patients can be placed in a knee immobilizer until treated operatively
improved outcomes with early treatment (within 3 weeks)
Arthroscopy +/- open debridement
Arthroscopic or open debridement with removal of any loose bodies may be necessary for displaced osteochondral fractures or loose bodies.
MPFL re-attachment or reconstruction (proximal realignment)
Proximal realignment constitutes the reconstruction of the MPFL. In brief, to repair the ligament, a longitudinal incision is made at the border of the VMO, just anterior to the medial epicondyle. The ligament is usually re-attached to the femur using bone anchors. If the patient has had recurrent dislocations, then reconstruction may be necessary by harvesting gracilis or semitendinosus which are then attached to the patella and femur.
Isolated repair/reconstruction of the MPFL is not a recommendation in those with bony abnormalities including TT-TG distance greater than 20mm, convex trochlear dysplasia, severe patella alta, advanced cartilage degeneration or severe femoral anteversion.[rx]
Lateral release (distal realignment)
A lateral release cuts the retinaculum on the lateral aspect of the knee joint. The aim is to improve the alignment of the patella by reducing the lateral pull.
Osteotomy (distal realignment)
Where there is abnormal anatomy contributing to poor patella tracking and a high TT-TG distance, the alignment correction can be through an osteotomy. The most common procedure of this type is known as the Fulkerson-type osteotomy and involves an osteotomy as well as removing the small portion of bone to which the tendon attaches and repositioning it in a more anteromedial position on the tibia.
Trochleoplasty
Trochleoplasty is indicated in recurrent dislocators with a convex or flat trochlea. The trochlear groove is deepened to create a groove for the patella to glide through; this may take place alongside an MPFL reconstruction. Studies suggest it is not advisable in those with open growth plates or severely degenerative joints. This procedure is uncommon except in refractory cases.
Complications of Traumatic Knee Dislocation
Vascular compromise
incidence of – 5-15% in all dislocations. 40-50% in anterior or posterior dislocations
risk factors – KD IV injuries have the highest rate of vascular injuries
treatment-emergent vascular repair and prophylactic fasciotomies
Stiffness (arthrofibrosis)
incidence – most common complication (38%)
risk factors – more common with delayed mobilization
avoid stiffness with early reconstruction and motion
arthroscopic lysis of adhesion
manipulation under anesthesia
Laxity and instability
incidence – 37% of some instability, however, redislocation is uncommon
treatment – arthroscopic lysis of adhesion, manipulation under anesthesia
Peroneal nerve injury
incidence- 25% occurrence of a peroneal nerve injury, 50% recover partially
posterolateral dislocations
Treatment
A to prevent equinus contracture
neurolysis or exploration at the time of reconstruction
nerve repair or reconstruction or tendon transfers if chronic nerve palsy persists
a dynamic tendon transfer involves transferring the posterior tibial tendon (PTT) to the foot
Knee Medial Dislocation/Knee Dislocation is a potentially devastating injury and is often a surgical emergency. This injury requires prompt identification, evaluation with appropriate imaging, and consultation with surgery for definitive treatment. Vascular injury and compartment syndrome are dreaded complications that the clinician should not miss in the workup of a knee dislocation. Note that this is in distinct contrast to patellar dislocations, which generally do not require immediate surgical or vascular intervention.[rx][rx]
A knee dislocation is a knee injury in which there is a complete disruption of the joint between the tibia and the femur. Symptoms include knee pain and instability of the knee. Complications may include injury to an artery around the knee, most commonly the artery behind the knee, or compartment syndrome.[rx][rx][rx]
Types /Classification of Knee Dislocation
They may be divided into five types: anterior, posterior, lateral, medial, and rotatory. This classification is based on the movement of the tibia with respect to the femur. Anterior dislocations are the most common, followed by posterior dislocations. They may also be classified based on what ligaments are damaged.[rx]
Kennedy classification based on the direction of displacement of the tibia
Anterior (30-50%)
most common
due to hyperextension injury
usually involves tear of PCL
an arterial injury is generally an intimal tear due to traction
the highest rate of peroneal nerve injury
Posterior (30-40%)
2nd most common
due to axial load to the flexed knee (dashboard injury)
The highest rate of vascular injury (25%) based on Kennedy classification
has highest incidence of a complete tear of the popliteal artery
Lateral (13%)
due to a varus or valgus force
usually involves tears of both ACL and PCL
Medial (3%)
varus or valgus force
usually disrupted PLC and PCL
Rotational (4%)
posterolateral is most common rotational dislocation
usually irreducible
buttonholing of femoral condyle through the capsule
Anatomic Classification System
TYPE
DESCRIPTION
KDI
Dislocation with single cruciate + single collateral ligament
KDII
Both cruciate ligaments torn, collateral ligaments intact
KDIIIM
ACL + PCL + MCL
L
ACL + PCL + LCL/PLC
KDIV
Both cruciate ligaments + both collateral ligaments torn
KDV
Fracture-dislocation
The letters C and N can be added to denote arterial and neurologic injury, respectively.
Schenck Classification
based on a pattern of multi ligamentous injury of knee dislocation (KD)
The Schenck and Wascher classifications of knee dislocations.
Group
Sub-Group
Definition
KD-I
Single cruciate only
KD-II
Bicruciate disruption only (rare)
KD-III
Bicruciate and posteromedial or posterolateral disruption (common)
KD-IV
Bicruciate and posteromedial and posterolateral disruption
KD-V
Dislocation with associated fracture
KD-V1
Single cruciate only
KD-V2
Bicruciate disruption only
KD-V3M
Bicruciate and posteromedial disruption
KD-V3L
Bicruciate and posterolateral disruption
KD-V4
Bicruciate and posteromedial and posterolateral disruption
C
Indicates associated arterial injury when suffixed to main group
N
Indicates associated neural injury when suffixed to main group
Causes of Knee Dislocation
Car accidents – If you bang your knee against a hard surface like your dashboard, the force of the blow may be strong enough to dislocate your knee.
Sports injuries – This is less common than car accidents, but it’s possible to dislocate your knee if you collide with great force with another player or with the ground when your knee is bent, or if you over-extend your knee (bend it back farther than it’s supposed to go).
Hard falls – It may happen to skiers or runners who lose control and fall on a bent or overextended knee. You may even dislocate your knee if you fall after stepping into a hole in the ground by mistake.
Result of major trauma – and about half occur as a result of minor trauma.[rx] Major trauma may include mechanisms like falls from a significant height, motor vehicle collisions, or a pedestrian being hit by a motor vehicle.
Genetic Disorder – often have other injuries.[rx] Minor trauma may include tripping while walking or while playing sports. Risk factors include obesity.[rx] The condition may also occur in a number of genetic disorders such as Ellis–van Creveld syndrome, Larsen syndrome, and Ehlers–Danlos syndrome.[rx]
Sudden forceful fall down
Road traffic accident
Falls – Falling onto an outstretched hand is one of the most common causes of the broken or dislocation knee.
Sports injuries – Many cervical spine fractures occur during contact sports or sports in which you might fall onto an outstretched hand — such as in-line skating or snowboarding.
Motor vehicle crashes – Motor vehicle crashes can cause the knee dislocation to break, sometimes into many pieces, and often require surgical repair.
Have osteoporosis – a disease that weakens your bones
Eave low muscle mass or poor muscle strength – or lack agility and have poor balance (these conditions make you more likely to fall)
Walk or do other activities in the snow or on the ice – or do activities that require a lot of forwarding momenta, such as in-line skating and skiing.
Previous fractures record.
Wave an inadequate intake of calcium or vitamin D.
Football or soccer, especially on artificial turf
Athletic injury with a sports injury.
The ligamentum patellae. Attached above to the lower border of the patella and below to the tuberosity of the tibia. A continuation of the central portion of the common tendon of the quadriceps femoris muscle. The oblique popliteal ligament. A tendinous expansion derived from the semimembranosus muscle. It strengthens the posterior aspect of the capsule.
Symptoms of Knee Medial Dislocation
CT angiogram 3D reconstruction, the posterior view showing a normal artery on the left, and occlusion to right popliteal artery as a result of a knee dislocation
Symptoms include knee pain. The joint may also be obviously out of place. A joint effusion is not always present.[rx]
Hearing a “popping” sound at the time of injury
Severe pain in the area of the knee
A visible deformity at the knee joint
Instability of the knee joint, or feeling like your knee joint is “giving way”
Limitations in the range of movement of your knee
Inability to continue with activities, whether they involve day-to-day tasks or sports
Feeling the kneecap shift or slide out of the groove
Feeling the knee buckle or give way
Hearing a popping sound when the patella dislocates
Swelling
A change in the knee’s appearance — the knee may appear misshapen or deformed
Apprehension or fear when running or changing direction.
Ankle-Brachial Index (ABI) – Normal ABI (as well as pulses, Capillary Refill) may not exclude popliteal artery disruption
Hard signs of vascular injury
Distal pulse loss or ischemia (e.g. pallor, coolness)
Active bleeding
Expanding hematoma
Palpable thrill or bruit over the popliteal artery
Neurologic Exam (especially peroneal nerve)
First web space and dorsal foot sensation
Ankle dorsiflexion
Multidirectional instability
Multidirectional instability may be only finding if knee spontaneously reduced prior to presentation
Three of four ligaments are likely injured (ACL Tear, PCL Tear, LCL tear, MCL tear)
Skin changes
Dimple Sign – Anteromedial skinfold at medial joint line. Seen in posterolateral dislocation (not reducible without surgery)
Skin necrosis – Entrapped skin at femoral condyle
Overlying Laceration – Suggests open Knee Dislocation (accompanies 20-30% of Knee Dislocations)
Others exam may include
Checking the pulse in several places on your leg and knee – This is called checking posterior tibial and dorsal pedal pulses, which are located in the region of the knee and foot. Lower pulses in your injured leg could indicate an injury to a blood vessel in your leg.
Checking the blood pressure in your leg – Called the ankle-brachial index (ABI), this test compares the blood pressure measured in your arm to the blood pressure measured in your ankle. A low ABI measurement can indicate poor blood flow to your lower extremities.
Checking your sense of touch or sensation – Your doctor will assess the feeling in the injured leg versus the unaffected leg.
Checking nerve conduction – Tests like electromyography (EMG) or nerve conduction velocity (NCV) will measure the function of the nerves in your leg and knee.
Checking your skin color and temperature – If your leg is cold or changing colors, there may be blood vessel problems.
X-rays – These tests create clear pictures of bone. Your doctor may order x-rays to look for skeletal abnormalities in the knee, such as a shallow groove in the femur.
Magnetic resonance imaging (MRI) scans – These scans create better pictures of the soft structures surrounding the knee, like ligaments. An MRI is seldom necessary because the doctor can usually diagnose a dislocated patella through an examination and x-rays. However, if your doctor needs additional, more detailed images, he or she may order an MRI.
Treatment of Knee Medial Dislocation
Nonoperative
Immobilization – Your doctor may recommend that your child wear a brace for 3 to 4 weeks. This stabilizes the knee while it heals.
Weightbearing – Because putting weight on the knee may cause pain and slow the healing process, your doctor may recommend using crutches for the first week or two after the injury.
Physical therapy – Once the knee has started to heal, your child’s doctor will recommend physical therapy to help your child regain normal motion. Specific exercises will strengthen the thigh muscles holding the knee joint in place. Your child’s commitment to the exercise program is important for a successful recovery. Typically, children return to activity 3 to 6 weeks after the injury.
Emergent closed reduction followed by vascular assessment/consult – indications to considered an orthopedic emergency, vascular consult indicated if pulses are absent or diminished following reduction if arterial injury confirmed by arterial duplex ultrasound or CT angiography
Immobilization as definitive management – successful closed reduction without vascular compromise, most cases require some form of surgical stabilization following reduction, outcomes of worse outcomes are seen with nonoperative management/prolonged immobilization will lead to loss of ROM with persistent instability.
Rest Your Leg – Once you’re discharged from the hospital in a legislating, your top priority is to rest your and not further inflame the injury. Of course, the arm sling not only provides support, but it also restricts movement, which is why you should keep it on even during sleep. Avoiding the temptation to move your will help the bone mend quicker and the pain fades away sooner.
Depending on what you do for a living and if the injury is to your dominant side, you may need to take a couple of weeks off work to recuperate.
Healing takes between four to six weeks in younger people and up to 12 weeks in the elderly, but it depends on the severity of the radial head fractures.
Athletes in good health are typically able to resume their sporting activities within two months of breaking they’re ulnar styloid depending on the severity of the break and the specific sport.
Sleeping on your back (with the sling on) is necessary to keep the pressure off your shoulder and prevent stressing the hip injury.
Eat Nutritiously During Your Recovery
All bones and tissues in the body need certain nutrients in order to heal properly and in a timely manner. Eating a nutritious and balanced diet that includes lots of minerals and vitamins are proven to help heal broken bones of all types. Therefore focus on eating lots of fresh produce (fruits and veggies), whole grains, lean meats, and fish to give your body the building blocks needed to properly repair your. In addition, drink plenty of purified water, milk, and other dairy-based beverages to augment what you eat.
Broken bones need ample minerals (calcium, phosphorus, magnesium, boron) and protein to become strong and healthy again.
Excellent sources of minerals/protein include dairy products, tofu, beans, broccoli, nuts and seeds, sardines, and salmon.
Important vitamins that are needed for bone healing include vitamin C (needed to make collagen), vitamin D (crucial for mineral absorption), and vitamin K (binds calcium to bones and triggers collagen formation).
Conversely, don’t consume food or drink that is known to impair bone/tissue healing, such as alcoholic beverages, sodas, most fast food items and foods made with lots of refined sugars and preservatives.
Physical Therapy
Although there will be some pain, it is important to maintain arm motion to prevent stiffness. Often, patients will begin doing exercises for elbow motion immediately after the injury. It is common to lose some leg strength. Once the bone begins to heal, your pain will decrease and your doctor may start gentle hip, knee exercises. These exercises will help prevent stiffness and weakness. More strenuous exercises will be started gradually once the fracture is completely healed.
Follow-Up Care
You will need to see your doctor regularly until your fracture heals. During these visits, he or they will take x-rays to make sure the bone is healing in a good position. After the bone has healed, you will be able to gradually return to your normal activities.
Opioids – Also known as narcotics, these medications are intense pain relievers that should only be used under a doctor’s careful supervision.
Topical Medications – These prescription-strength creams, gels, ointments, patches, and sprays help relieve pain and inflammation through the skin.
Calcium & vitamin D3 – to improve bone health and healing fracture. As a general rule, men and women age 50 and older should consume 1,200 milligrams of calcium a day, and 600 international units of vitamin D a day.
Glucosamine & Diacerein, Chondroitin sulfate – can be used to tightening the loose tension, cartilage, ligament, and cartilage, ligament regenerate cartilage or inhabit the further degeneration of cartilage, ligament
Antidepressants – A drug that blocks pain messages from your brain and boosts the effects of endorphins (your body’s natural painkillers).
Surgical Treatment
Open reduction
irreducible knee
posterolateral dislocation
open fracture-dislocation
obesity (may be difficult to obtain closed)
vascular injury
External fixation
vascular repair (takes precedence)
open fracture-dislocation
compartment syndrome
obese (if difficult to maintain reduction)
polytrauma patient
Delayed ligamentous reconstruction/repair
instability will require some kind of ligamentous repair or fixation
patients can be placed in a knee immobilizer until treated operatively
improved outcomes with early treatment (within 3 weeks)
Arthroscopy +/- open debridement
Arthroscopic or open debridement with removal of any loose bodies may be necessary for displaced osteochondral fractures or loose bodies.
MPFL re-attachment or reconstruction (proximal realignment)
Proximal realignment constitutes the reconstruction of the MPFL. In brief, to repair the ligament, a longitudinal incision is made at the border of the VMO, just anterior to the medial epicondyle. The ligament is usually re-attached to the femur using bone anchors. If the patient has had recurrent dislocations, then reconstruction may be necessary by harvesting gracilis or semitendinosus which are then attached to the patella and femur.
Isolated repair/reconstruction of the MPFL is not a recommendation in those with bony abnormalities including TT-TG distance greater than 20mm, convex trochlear dysplasia, severe patella alta, advanced cartilage degeneration or severe femoral anteversion.[rx]
Lateral release (distal realignment)
A lateral release cuts the retinaculum on the lateral aspect of the knee joint. The aim is to improve the alignment of the patella by reducing the lateral pull.
Osteotomy (distal realignment)
Where there is abnormal anatomy contributing to poor patella tracking and a high TT-TG distance, the alignment correction can be through an osteotomy. The most common procedure of this type is known as the Fulkerson-type osteotomy and involves an osteotomy as well as removing the small portion of bone to which the tendon attaches and repositioning it in a more anteromedial position on the tibia.
Trochleoplasty
Trochleoplasty is indicated in recurrent dislocators with a convex or flat trochlea. The trochlear groove is deepened to create a groove for the patella to glide through; this may take place alongside an MPFL reconstruction. Studies suggest it is not advisable in those with open growth plates or severely degenerative joints. This procedure is uncommon except in refractory cases.
Complications of Knee Lateral Dislocation
Vascular compromise
incidence of – 5-15% in all dislocations. 40-50% in anterior or posterior dislocations
risk factors – KD IV injuries have the highest rate of vascular injuries
treatment-emergent vascular repair and prophylactic fasciotomies
Stiffness (arthrofibrosis)
incidence – most common complication (38%)
risk factors – more common with delayed mobilization
avoid stiffness with early reconstruction and motion
arthroscopic lysis of adhesion
manipulation under anesthesia
Laxity and instability
incidence – 37% of some instability, however, redislocation is uncommon
treatment – arthroscopic lysis of adhesion, manipulation under anesthesia
Peroneal nerve injury
incidence- 25% occurrence of a peroneal nerve injury, 50% recover partially
posterolateral dislocations
Treatment
A to prevent equinus contracture
neurolysis or exploration at the time of reconstruction
nerve repair or reconstruction or tendon transfers if chronic nerve palsy persists
a dynamic tendon transfer involves transferring the posterior tibial tendon (PTT) to the foot
Knee Posterior Dislocation/Knee Dislocation is a potentially devastating injury and is often a surgical emergency. This injury requires prompt identification, evaluation with appropriate imaging, and consultation with surgery for definitive treatment. Vascular injury and compartment syndrome are dreaded complications that the clinician should not miss in the workup of a knee dislocation. Note that this is in distinct contrast to patellar dislocations, which generally do not require immediate surgical or vascular intervention.[rx][rx]
A knee dislocation is a knee injury in which there is a complete disruption of the joint between the tibia and the femur. Symptoms include knee pain and instability of the knee. Complications may include injury to an artery around the knee, most commonly the artery behind the knee, or compartment syndrome.[rx][rx][rx]
Types /Classification of Knee Dislocation
They may be divided into five types: anterior, posterior, lateral, medial, and rotatory. This classification is based on the movement of the tibia with respect to the femur. Anterior dislocations are the most common, followed by posterior dislocations. They may also be classified based on what ligaments are damaged.[rx]
Kennedy classification based on the direction of displacement of the tibia
Anterior (30-50%)
most common
due to hyperextension injury
usually involves tear of PCL
an arterial injury is generally an intimal tear due to traction
the highest rate of peroneal nerve injury
Posterior (30-40%)
2nd most common
due to axial load to the flexed knee (dashboard injury)
The highest rate of vascular injury (25%) based on Kennedy classification
has highest incidence of a complete tear of the popliteal artery
Lateral (13%)
due to a varus or valgus force
usually involves tears of both ACL and PCL
Medial (3%)
varus or valgus force
usually disrupted PLC and PCL
Rotational (4%)
posterolateral is most common rotational dislocation
usually irreducible
buttonholing of femoral condyle through the capsule
Anatomic Classification System
TYPE
DESCRIPTION
KDI
Dislocation with single cruciate + single collateral ligament
KDII
Both cruciate ligaments torn, collateral ligaments intact
KDIIIM
ACL + PCL + MCL
L
ACL + PCL + LCL/PLC
KDIV
Both cruciate ligaments + both collateral ligaments torn
KDV
Fracture-dislocation
The letters C and N can be added to denote arterial and neurologic injury, respectively.
Schenck Classification
based on a pattern of multi ligamentous injury of knee dislocation (KD)
The Schenck and Wascher classifications of knee dislocations.
Group
Sub-Group
Definition
KD-I
Single cruciate only
KD-II
Bicruciate disruption only (rare)
KD-III
Bicruciate and posteromedial or posterolateral disruption (common)
KD-IV
Bicruciate and posteromedial and posterolateral disruption
KD-V
Dislocation with associated fracture
KD-V1
Single cruciate only
KD-V2
Bicruciate disruption only
KD-V3M
Bicruciate and posteromedial disruption
KD-V3L
Bicruciate and posterolateral disruption
KD-V4
Bicruciate and posteromedial and posterolateral disruption
C
Indicates associated arterial injury when suffixed to main group
N
Indicates associated neural injury when suffixed to main group
Causes of Knee Dislocation
Car accidents – If you bang your knee against a hard surface like your dashboard, the force of the blow may be strong enough to dislocate your knee.
Sports injuries – This is less common than car accidents, but it’s possible to dislocate your knee if you collide with great force with another player or with the ground when your knee is bent, or if you over-extend your knee (bend it back farther than it’s supposed to go).
Hard falls – It may happen to skiers or runners who lose control and fall on a bent or overextended knee. You may even dislocate your knee if you fall after stepping into a hole in the ground by mistake.
Result of major trauma – and about half occur as a result of minor trauma.[rx] Major trauma may include mechanisms like falls from a significant height, motor vehicle collisions, or a pedestrian being hit by a motor vehicle.
Genetic Disorder – often have other injuries.[rx] Minor trauma may include tripping while walking or while playing sports. Risk factors include obesity.[rx] The condition may also occur in a number of genetic disorders such as Ellis–van Creveld syndrome, Larsen syndrome, and Ehlers–Danlos syndrome.[rx]
Sudden forceful fall down
Road traffic accident
Falls – Falling onto an outstretched hand is one of the most common causes of the broken or dislocation knee.
Sports injuries – Many cervical spine fractures occur during contact sports or sports in which you might fall onto an outstretched hand — such as in-line skating or snowboarding.
Motor vehicle crashes – Motor vehicle crashes can cause the knee dislocation to break, sometimes into many pieces, and often require surgical repair.
Have osteoporosis – a disease that weakens your bones
Eave low muscle mass or poor muscle strength – or lack agility and have poor balance (these conditions make you more likely to fall)
Walk or do other activities in the snow or on the ice – or do activities that require a lot of forwarding momenta, such as in-line skating and skiing.
Previous fractures record.
Wave an inadequate intake of calcium or vitamin D.
Football or soccer, especially on artificial turf
Athletic injury with a sports injury.
The ligamentum patellae. Attached above to the lower border of the patella and below to the tuberosity of the tibia. A continuation of the central portion of the common tendon of the quadriceps femoris muscle. The oblique popliteal ligament. A tendinous expansion derived from the semimembranosus muscle. It strengthens the posterior aspect of the capsule.
Symptoms of Knee Posterior Dislocation
CT angiogram 3D reconstruction, the posterior view showing a normal artery on the left, and occlusion to right popliteal artery as a result of a knee dislocation
Symptoms include knee pain. The joint may also be obviously out of place. A joint effusion is not always present.[rx]
Hearing a “popping” sound at the time of injury
Severe pain in the area of the knee
A visible deformity at the knee joint
Instability of the knee joint, or feeling like your knee joint is “giving way”
Limitations in the range of movement of your knee
Inability to continue with activities, whether they involve day-to-day tasks or sports
Feeling the kneecap shift or slide out of the groove
Feeling the knee buckle or give way
Hearing a popping sound when the patella dislocates
Swelling
A change in the knee’s appearance — the knee may appear misshapen or deformed
Apprehension or fear when running or changing direction.
Ankle-Brachial Index (ABI) – Normal ABI (as well as pulses, Capillary Refill) may not exclude popliteal artery disruption
Hard signs of vascular injury
Distal pulse loss or ischemia (e.g. pallor, coolness)
Active bleeding
Expanding hematoma
Palpable thrill or bruit over the popliteal artery
Neurologic Exam (especially peroneal nerve)
First web space and dorsal foot sensation
Ankle dorsiflexion
Multidirectional instability
Multidirectional instability may be only finding if knee spontaneously reduced prior to presentation
Three of four ligaments are likely injured (ACL Tear, PCL Tear, LCL tear, MCL tear)
Skin changes
Dimple Sign – Anteromedial skinfold at medial joint line. Seen in posterolateral dislocation (not reducible without surgery)
Skin necrosis – Entrapped skin at femoral condyle
Overlying Laceration – Suggests open Knee Dislocation (accompanies 20-30% of Knee Dislocations)
Others exam may include
Checking the pulse in several places on your leg and knee – This is called checking posterior tibial and dorsal pedal pulses, which are located in the region of the knee and foot. Lower pulses in your injured leg could indicate an injury to a blood vessel in your leg.
Checking the blood pressure in your leg – Called the ankle-brachial index (ABI), this test compares the blood pressure measured in your arm to the blood pressure measured in your ankle. A low ABI measurement can indicate poor blood flow to your lower extremities.
Checking your sense of touch or sensation – Your doctor will assess the feeling in the injured leg versus the unaffected leg.
Checking nerve conduction – Tests like electromyography (EMG) or nerve conduction velocity (NCV) will measure the function of the nerves in your leg and knee.
Checking your skin color and temperature – If your leg is cold or changing colors, there may be blood vessel problems.
X-rays – These tests create clear pictures of bone. Your doctor may order x-rays to look for skeletal abnormalities in the knee, such as a shallow groove in the femur.
Magnetic resonance imaging (MRI) scans – These scans create better pictures of the soft structures surrounding the knee, like ligaments. An MRI is seldom necessary because the doctor can usually diagnose a dislocated patella through an examination and x-rays. However, if your doctor needs additional, more detailed images, he or she may order an MRI.
Treatment of Knee Posterior Dislocation
Nonoperative
Immobilization – Your doctor may recommend that your child wear a brace for 3 to 4 weeks. This stabilizes the knee while it heals.
Weightbearing – Because putting weight on the knee may cause pain and slow the healing process, your doctor may recommend using crutches for the first week or two after the injury.
Physical therapy – Once the knee has started to heal, your child’s doctor will recommend physical therapy to help your child regain normal motion. Specific exercises will strengthen the thigh muscles holding the knee joint in place. Your child’s commitment to the exercise program is important for a successful recovery. Typically, children return to activity 3 to 6 weeks after the injury.
Emergent closed reduction followed by vascular assessment/consult – indications to considered an orthopedic emergency, vascular consult indicated if pulses are absent or diminished following reduction if arterial injury confirmed by arterial duplex ultrasound or CT angiography
Immobilization as definitive management – successful closed reduction without vascular compromise, most cases require some form of surgical stabilization following reduction, outcomes of worse outcomes are seen with nonoperative management/prolonged immobilization will lead to loss of ROM with persistent instability.
Rest Your Leg – Once you’re discharged from the hospital in a legislating, your top priority is to rest your and not further inflame the injury. Of course, the arm sling not only provides support, but it also restricts movement, which is why you should keep it on even during sleep. Avoiding the temptation to move your will help the bone mend quicker and the pain fades away sooner.
Depending on what you do for a living and if the injury is to your dominant side, you may need to take a couple of weeks off work to recuperate.
Healing takes between four to six weeks in younger people and up to 12 weeks in the elderly, but it depends on the severity of the radial head fractures.
Athletes in good health are typically able to resume their sporting activities within two months of breaking they’re ulnar styloid depending on the severity of the break and the specific sport.
Sleeping on your back (with the sling on) is necessary to keep the pressure off your shoulder and prevent stressing the hip injury.
Eat Nutritiously During Your Recovery
All bones and tissues in the body need certain nutrients in order to heal properly and in a timely manner. Eating a nutritious and balanced diet that includes lots of minerals and vitamins are proven to help heal broken bones of all types. Therefore focus on eating lots of fresh produce (fruits and veggies), whole grains, lean meats, and fish to give your body the building blocks needed to properly repair your. In addition, drink plenty of purified water, milk, and other dairy-based beverages to augment what you eat.
Broken bones need ample minerals (calcium, phosphorus, magnesium, boron) and protein to become strong and healthy again.
Excellent sources of minerals/protein include dairy products, tofu, beans, broccoli, nuts and seeds, sardines, and salmon.
Important vitamins that are needed for bone healing include vitamin C (needed to make collagen), vitamin D (crucial for mineral absorption), and vitamin K (binds calcium to bones and triggers collagen formation).
Conversely, don’t consume food or drink that is known to impair bone/tissue healing, such as alcoholic beverages, sodas, most fast food items and foods made with lots of refined sugars and preservatives.
Physical Therapy
Although there will be some pain, it is important to maintain arm motion to prevent stiffness. Often, patients will begin doing exercises for elbow motion immediately after the injury. It is common to lose some leg strength. Once the bone begins to heal, your pain will decrease and your doctor may start gentle hip, knee exercises. These exercises will help prevent stiffness and weakness. More strenuous exercises will be started gradually once the fracture is completely healed.
Follow-Up Care
You will need to see your doctor regularly until your fracture heals. During these visits, he or they will take x-rays to make sure the bone is healing in a good position. After the bone has healed, you will be able to gradually return to your normal activities.
Opioids – Also known as narcotics, these medications are intense pain relievers that should only be used under a doctor’s careful supervision.
Topical Medications – These prescription-strength creams, gels, ointments, patches, and sprays help relieve pain and inflammation through the skin.
Calcium & vitamin D3 – to improve bone health and healing fracture. As a general rule, men and women age 50 and older should consume 1,200 milligrams of calcium a day, and 600 international units of vitamin D a day.
Glucosamine & Diacerein, Chondroitin sulfate – can be used to tightening the loose tension, cartilage, ligament, and cartilage, ligament regenerate cartilage or inhabit the further degeneration of cartilage, ligament
Antidepressants – A drug that blocks pain messages from your brain and boosts the effects of endorphins (your body’s natural painkillers).
Surgical Treatment
Open reduction
irreducible knee
posterolateral dislocation
open fracture-dislocation
obesity (may be difficult to obtain closed)
vascular injury
External fixation
vascular repair (takes precedence)
open fracture-dislocation
compartment syndrome
obese (if difficult to maintain reduction)
polytrauma patient
Delayed ligamentous reconstruction/repair
instability will require some kind of ligamentous repair or fixation
patients can be placed in a knee immobilizer until treated operatively
improved outcomes with early treatment (within 3 weeks)
Arthroscopy +/- open debridement
Arthroscopic or open debridement with removal of any loose bodies may be necessary for displaced osteochondral fractures or loose bodies.
MPFL re-attachment or reconstruction (proximal realignment)
Proximal realignment constitutes the reconstruction of the MPFL. In brief, to repair the ligament, a longitudinal incision is made at the border of the VMO, just anterior to the medial epicondyle. The ligament is usually re-attached to the femur using bone anchors. If the patient has had recurrent dislocations, then reconstruction may be necessary by harvesting gracilis or semitendinosus which are then attached to the patella and femur.
Isolated repair/reconstruction of the MPFL is not a recommendation in those with bony abnormalities including TT-TG distance greater than 20mm, convex trochlear dysplasia, severe patella alta, advanced cartilage degeneration or severe femoral anteversion.[rx]
Lateral release (distal realignment)
A lateral release cuts the retinaculum on the lateral aspect of the knee joint. The aim is to improve the alignment of the patella by reducing the lateral pull.
Osteotomy (distal realignment)
Where there is abnormal anatomy contributing to poor patella tracking and a high TT-TG distance, the alignment correction can be through an osteotomy. The most common procedure of this type is known as the Fulkerson-type osteotomy and involves an osteotomy as well as removing the small portion of bone to which the tendon attaches and repositioning it in a more anteromedial position on the tibia.
Trochleoplasty
Trochleoplasty is indicated in recurrent dislocators with a convex or flat trochlea. The trochlear groove is deepened to create a groove for the patella to glide through; this may take place alongside an MPFL reconstruction. Studies suggest it is not advisable in those with open growth plates or severely degenerative joints. This procedure is uncommon except in refractory cases.
Complications of Knee Posterior Dislocation
Vascular compromise
incidence of – 5-15% in all dislocations. 40-50% in anterior or posterior dislocations
risk factors – KD IV injuries have the highest rate of vascular injuries
treatment-emergent vascular repair and prophylactic fasciotomies
Stiffness (arthrofibrosis)
incidence – most common complication (38%)
risk factors – more common with delayed mobilization
avoid stiffness with early reconstruction and motion
arthroscopic lysis of adhesion
manipulation under anesthesia
Laxity and instability
incidence – 37% of some instability, however, redislocation is uncommon
treatment – arthroscopic lysis of adhesion, manipulation under anesthesia
Peroneal nerve injury
incidence- 25% occurrence of a peroneal nerve injury, 50% recover partially
posterolateral dislocations
Treatment
A to prevent equinus contracture
neurolysis or exploration at the time of reconstruction
nerve repair or reconstruction or tendon transfers if chronic nerve palsy persists
a dynamic tendon transfer involves transferring the posterior tibial tendon (PTT) to the foot
Knee Anterior Dislocation/Knee Dislocation is a potentially devastating injury and is often a surgical emergency. This injury requires prompt identification, evaluation with appropriate imaging, and consultation with surgery for definitive treatment. Vascular injury and compartment syndrome are dreaded complications that the clinician should not miss in the workup of a knee dislocation. Note that this is in distinct contrast to patellar dislocations, which generally do not require immediate surgical or vascular intervention.[rx][rx]
A knee dislocation is a knee injury in which there is a complete disruption of the joint between the tibia and the femur. Symptoms include knee pain and instability of the knee. Complications may include injury to an artery around the knee, most commonly the artery behind the knee, or compartment syndrome.[rx][rx][rx]
Types /Classification of Knee Dislocation
They may be divided into five types: anterior, posterior, lateral, medial, and rotatory. This classification is based on the movement of the tibia with respect to the femur. Anterior dislocations are the most common, followed by posterior dislocations. They may also be classified based on what ligaments are damaged.[rx]
Kennedy classification based on the direction of displacement of the tibia
Anterior (30-50%)
most common
due to hyperextension injury
usually involves tear of PCL
an arterial injury is generally an intimal tear due to traction
the highest rate of peroneal nerve injury
Posterior (30-40%)
2nd most common
due to axial load to the flexed knee (dashboard injury)
The highest rate of vascular injury (25%) based on Kennedy classification
has highest incidence of a complete tear of the popliteal artery
Lateral (13%)
due to a varus or valgus force
usually involves tears of both ACL and PCL
Medial (3%)
varus or valgus force
usually disrupted PLC and PCL
Rotational (4%)
posterolateral is most common rotational dislocation
usually irreducible
buttonholing of femoral condyle through the capsule
Anatomic Classification System
TYPE
DESCRIPTION
KDI
Dislocation with single cruciate + single collateral ligament
KDII
Both cruciate ligaments torn, collateral ligaments intact
KDIIIM
ACL + PCL + MCL
L
ACL + PCL + LCL/PLC
KDIV
Both cruciate ligaments + both collateral ligaments torn
KDV
Fracture-dislocation
The letters C and N can be added to denote arterial and neurologic injury, respectively.
Schenck Classification
based on a pattern of multi ligamentous injury of knee dislocation (KD)
The Schenck and Wascher classifications of knee dislocations.
Group
Sub-Group
Definition
KD-I
Single cruciate only
KD-II
Bicruciate disruption only (rare)
KD-III
Bicruciate and posteromedial or posterolateral disruption (common)
KD-IV
Bicruciate and posteromedial and posterolateral disruption
KD-V
Dislocation with associated fracture
KD-V1
Single cruciate only
KD-V2
Bicruciate disruption only
KD-V3M
Bicruciate and posteromedial disruption
KD-V3L
Bicruciate and posterolateral disruption
KD-V4
Bicruciate and posteromedial and posterolateral disruption
C
Indicates associated arterial injury when suffixed to main group
N
Indicates associated neural injury when suffixed to main group
Causes of Knee Dislocation
Car accidents – If you bang your knee against a hard surface like your dashboard, the force of the blow may be strong enough to dislocate your knee.
Sports injuries – This is less common than car accidents, but it’s possible to dislocate your knee if you collide with great force with another player or with the ground when your knee is bent, or if you over-extend your knee (bend it back farther than it’s supposed to go).
Hard falls – It may happen to skiers or runners who lose control and fall on a bent or overextended knee. You may even dislocate your knee if you fall after stepping into a hole in the ground by mistake.
Result of major trauma – and about half occur as a result of minor trauma.[rx] Major trauma may include mechanisms like falls from a significant height, motor vehicle collisions, or a pedestrian being hit by a motor vehicle.
Genetic Disorder – often have other injuries.[rx] Minor trauma may include tripping while walking or while playing sports. Risk factors include obesity.[rx] The condition may also occur in a number of genetic disorders such as Ellis–van Creveld syndrome, Larsen syndrome, and Ehlers–Danlos syndrome.[rx]
Sudden forceful fall down
Road traffic accident
Falls – Falling onto an outstretched hand is one of the most common causes of the broken or dislocation knee.
Sports injuries – Many cervical spine fractures occur during contact sports or sports in which you might fall onto an outstretched hand — such as in-line skating or snowboarding.
Motor vehicle crashes – Motor vehicle crashes can cause the knee dislocation to break, sometimes into many pieces, and often require surgical repair.
Have osteoporosis – a disease that weakens your bones
Eave low muscle mass or poor muscle strength – or lack agility and have poor balance (these conditions make you more likely to fall)
Walk or do other activities in the snow or on the ice – or do activities that require a lot of forwarding momenta, such as in-line skating and skiing.
Previous fractures record.
Wave an inadequate intake of calcium or vitamin D.
Football or soccer, especially on artificial turf
Athletic injury with a sports injury.
The ligamentum patellae. Attached above to the lower border of the patella and below to the tuberosity of the tibia. A continuation of the central portion of the common tendon of the quadriceps femoris muscle. The oblique popliteal ligament. A tendinous expansion derived from the semimembranosus muscle. It strengthens the posterior aspect of the capsule.
Symptoms of Knee Dislocation
CT angiogram 3D reconstruction, posterior view showing a normal artery on the left, and occlusion to right popliteal artery as a result of a knee dislocation
Symptoms include knee pain. The joint may also be obviously out of place. A joint effusion is not always present.[rx]
Hearing a “popping” sound at the time of injury
Severe pain in the area of the knee
A visible deformity at the knee joint
Instability of the knee joint, or feeling like your knee joint is “giving way”
Limitations in the range of movement of your knee
Inability to continue with activities, whether they involve day-to-day tasks or sports
Feeling the kneecap shift or slide out of the groove
Feeling the knee buckle or give way
Hearing a popping sound when the patella dislocates
Swelling
A change in the knee’s appearance — the knee may appear misshapen or deformed
Apprehension or fear when running or changing direction.
Ankle-Brachial Index (ABI) – Normal ABI (as well as pulses, Capillary Refill) may not exclude popliteal artery disruption
Hard signs of vascular injury
Distal pulse loss or ischemia (e.g. pallor, coolness)
Active bleeding
Expanding hematoma
Palpable thrill or bruit over the popliteal artery
Neurologic Exam (especially peroneal nerve)
First web space and dorsal foot sensation
Ankle dorsiflexion
Multidirectional instability
Multidirectional instability may be only finding if knee spontaneously reduced prior to presentation
Three of four ligaments are likely injured (ACL Tear, PCL Tear, LCL tear, MCL tear)
Skin changes
Dimple Sign – Anteromedial skinfold at medial joint line. Seen in posterolateral dislocation (not reducible without surgery)
Skin necrosis – Entrapped skin at femoral condyle
Overlying Laceration – Suggests open Knee Dislocation (accompanies 20-30% of Knee Dislocations)
Others exam may include
Checking the pulse in several places on your leg and knee – This is called checking posterior tibial and dorsal pedal pulses, which are located in the region of the knee and foot. Lower pulses in your injured leg could indicate an injury to a blood vessel in your leg.
Checking the blood pressure in your leg – Called the ankle-brachial index (ABI), this test compares the blood pressure measured in your arm to the blood pressure measured in your ankle. A low ABI measurement can indicate poor blood flow to your lower extremities.
Checking your sense of touch or sensation – Your doctor will assess the feeling in the injured leg versus the unaffected leg.
Checking nerve conduction – Tests like electromyography (EMG) or nerve conduction velocity (NCV) will measure the function of the nerves in your leg and knee.
Checking your skin color and temperature – If your leg is cold or changing colors, there may be blood vessel problems.
X-rays – These tests create clear pictures of bone. Your doctor may order x-rays to look for skeletal abnormalities in the knee, such as a shallow groove in the femur.
Magnetic resonance imaging (MRI) scans – These scans create better pictures of the soft structures surrounding the knee, like ligaments. An MRI is seldom necessary because the doctor can usually diagnose a dislocated patella through an examination and x-rays. However, if your doctor needs additional, more detailed images, he or she may order an MRI.
Treatment of Knee Dislocation
Nonoperative
Immobilization – Your doctor may recommend that your child wear a brace for 3 to 4 weeks. This stabilizes the knee while it heals.
Weightbearing – Because putting weight on the knee may cause pain and slow the healing process, your doctor may recommend using crutches for the first week or two after the injury.
Physical therapy – Once the knee has started to heal, your child’s doctor will recommend physical therapy to help your child regain normal motion. Specific exercises will strengthen the thigh muscles holding the knee joint in place. Your child’s commitment to the exercise program is important for a successful recovery. Typically, children return to activity 3 to 6 weeks after the injury.
Emergent closed reduction followed by vascular assessment/consult – indications to considered an orthopedic emergency, vascular consult indicated if pulses are absent or diminished following reduction if arterial injury confirmed by arterial duplex ultrasound or CT angiography
Immobilization as definitive management – successful closed reduction without vascular compromise, most cases require some form of surgical stabilization following reduction, outcomes of worse outcomes are seen with nonoperative management/prolonged immobilization will lead to loss of ROM with persistent instability.
Rest Your Leg – Once you’re discharged from the hospital in a legislating, your top priority is to rest your and not further inflame the injury. Of course, the arm sling not only provides support, but it also restricts movement, which is why you should keep it on even during sleep. Avoiding the temptation to move your will help the bone mend quicker and the pain fades away sooner.
Depending on what you do for a living and if the injury is to your dominant side, you may need to take a couple of weeks off work to recuperate.
Healing takes between four to six weeks in younger people and up to 12 weeks in the elderly, but it depends on the severity of the radial head fractures.
Athletes in good health are typically able to resume their sporting activities within two months of breaking they’re ulnar styloid depending on the severity of the break and the specific sport.
Sleeping on your back (with the sling on) is necessary to keep the pressure off your shoulder and prevent stressing the hip injury.
Eat Nutritiously During Your Recovery
All bones and tissues in the body need certain nutrients in order to heal properly and in a timely manner. Eating a nutritious and balanced diet that includes lots of minerals and vitamins are proven to help heal broken bones of all types. Therefore focus on eating lots of fresh produce (fruits and veggies), whole grains, lean meats, and fish to give your body the building blocks needed to properly repair your. In addition, drink plenty of purified water, milk, and other dairy-based beverages to augment what you eat.
Broken bones need ample minerals (calcium, phosphorus, magnesium, boron) and protein to become strong and healthy again.
Excellent sources of minerals/protein include dairy products, tofu, beans, broccoli, nuts and seeds, sardines, and salmon.
Important vitamins that are needed for bone healing include vitamin C (needed to make collagen), vitamin D (crucial for mineral absorption), and vitamin K (binds calcium to bones and triggers collagen formation).
Conversely, don’t consume food or drink that is known to impair bone/tissue healing, such as alcoholic beverages, sodas, most fast food items and foods made with lots of refined sugars and preservatives.
Physical Therapy
Although there will be some pain, it is important to maintain arm motion to prevent stiffness. Often, patients will begin doing exercises for elbow motion immediately after the injury. It is common to lose some leg strength. Once the bone begins to heal, your pain will decrease and your doctor may start gentle hip, knee exercises. These exercises will help prevent stiffness and weakness. More strenuous exercises will be started gradually once the fracture is completely healed.
Follow-Up Care
You will need to see your doctor regularly until your fracture heals. During these visits, he or they will take x-rays to make sure the bone is healing in a good position. After the bone has healed, you will be able to gradually return to your normal activities.
Opioids – Also known as narcotics, these medications are intense pain relievers that should only be used under a doctor’s careful supervision.
Topical Medications – These prescription-strength creams, gels, ointments, patches, and sprays help relieve pain and inflammation through the skin.
Calcium & vitamin D3 – to improve bone health and healing fracture. As a general rule, men and women age 50 and older should consume 1,200 milligrams of calcium a day, and 600 international units of vitamin D a day.
Glucosamine & Diacerein, Chondroitin sulfate – can be used to tightening the loose tension, cartilage, ligament, and cartilage, ligament regenerate cartilage or inhabit the further degeneration of cartilage, ligament
Antidepressants – A drug that blocks pain messages from your brain and boosts the effects of endorphins (your body’s natural painkillers).
Surgical Treatment
Open reduction
irreducible knee
posterolateral dislocation
open fracture-dislocation
obesity (may be difficult to obtain closed)
vascular injury
External fixation
vascular repair (takes precedence)
open fracture-dislocation
compartment syndrome
obese (if difficult to maintain reduction)
polytrauma patient
Delayed ligamentous reconstruction/repair
instability will require some kind of ligamentous repair or fixation
patients can be placed in a knee immobilizer until treated operatively
improved outcomes with early treatment (within 3 weeks)
Arthroscopy +/- open debridement
Arthroscopic or open debridement with removal of any loose bodies may be necessary for displaced osteochondral fractures or loose bodies.
MPFL re-attachment or reconstruction (proximal realignment)
Proximal realignment constitutes the reconstruction of the MPFL. In brief, to repair the ligament, a longitudinal incision is made at the border of the VMO, just anterior to the medial epicondyle. The ligament is usually re-attached to the femur using bone anchors. If the patient has had recurrent dislocations, then reconstruction may be necessary by harvesting gracilis or semitendinosus which are then attached to the patella and femur.
Isolated repair/reconstruction of the MPFL is not a recommendation in those with bony abnormalities including TT-TG distance greater than 20mm, convex trochlear dysplasia, severe patella alta, advanced cartilage degeneration or severe femoral anteversion.[rx]
Lateral release (distal realignment)
A lateral release cuts the retinaculum on the lateral aspect of the knee joint. The aim is to improve the alignment of the patella by reducing the lateral pull.
Osteotomy (distal realignment)
Where there is abnormal anatomy contributing to poor patella tracking and a high TT-TG distance, the alignment correction can be through an osteotomy. The most common procedure of this type is known as the Fulkerson-type osteotomy and involves an osteotomy as well as removing the small portion of bone to which the tendon attaches and repositioning it in a more anteromedial position on the tibia.
Trochleoplasty
Trochleoplasty is indicated in recurrent dislocators with a convex or flat trochlea. The trochlear groove is deepened to create a groove for the patella to glide through; this may take place alongside an MPFL reconstruction. Studies suggest it is not advisable in those with open growth plates or severely degenerative joints. This procedure is uncommon except in refractory cases.
Complications of Knee Anterior Dislocation
Vascular compromise
incidence of – 5-15% in all dislocations. 40-50% in anterior or posterior dislocations
risk factors – KD IV injuries have the highest rate of vascular injuries
treatment-emergent vascular repair and prophylactic fasciotomies
Stiffness (arthrofibrosis)
incidence – most common complication (38%)
risk factors – more common with delayed mobilization
avoid stiffness with early reconstruction and motion
arthroscopic lysis of adhesion
manipulation under anesthesia
Laxity and instability
incidence – 37% of some instability, however, redislocation is uncommon
treatment – arthroscopic lysis of adhesion, manipulation under anesthesia
Peroneal nerve injury
incidence- 25% occurrence of a peroneal nerve injury, 50% recover partially
posterolateral dislocations
Treatment
A to prevent equinus contracture
neurolysis or exploration at the time of reconstruction
nerve repair or reconstruction or tendon transfers if chronic nerve palsy persists
a dynamic tendon transfer involves transferring the posterior tibial tendon (PTT) to the foot
Types /Classification of Knee Dislocation/Knee Dislocation is a potentially devastating injury and is often a surgical emergency. This injury requires prompt identification, evaluation with appropriate imaging, and consultation with surgery for definitive treatment. Vascular injury and compartment syndrome are dreaded complications that the clinician should not miss in the workup of a knee dislocation. Note that this is in distinct contrast to patellar dislocations, which generally do not require immediate surgical or vascular intervention.[rx][rx]
A knee dislocation is a knee injury in which there is a complete disruption of the joint between the tibia and the femur. Symptoms include knee pain and instability of the knee. Complications may include injury to an artery around the knee, most commonly the artery behind the knee, or compartment syndrome.[rx][rx][rx]
Types /Classification of Knee Dislocation
They may be divided into five types: anterior, posterior, lateral, medial, and rotatory. This classification is based on the movement of the tibia with respect to the femur. Anterior dislocations are the most common, followed by posterior dislocations. They may also be classified based on what ligaments are damaged.[rx]
Kennedy classification based on the direction of displacement of the tibia
Anterior (30-50%)
most common
due to hyperextension injury
usually involves tear of PCL
an arterial injury is generally an intimal tear due to traction
the highest rate of peroneal nerve injury
Posterior (30-40%)
2nd most common
due to axial load to the flexed knee (dashboard injury)
The highest rate of vascular injury (25%) based on Kennedy classification
has highest incidence of a complete tear of the popliteal artery
Lateral (13%)
due to a varus or valgus force
usually involves tears of both ACL and PCL
Medial (3%)
varus or valgus force
usually disrupted PLC and PCL
Rotational (4%)
posterolateral is most common rotational dislocation
usually irreducible
buttonholing of femoral condyle through the capsule
Anatomic Classification System
TYPE
DESCRIPTION
KDI
Dislocation with single cruciate + single collateral ligament
KDII
Both cruciate ligaments torn, collateral ligaments intact
KDIIIM
ACL + PCL + MCL
L
ACL + PCL + LCL/PLC
KDIV
Both cruciate ligaments + both collateral ligaments torn
KDV
Fracture-dislocation
The letters C and N can be added to denote arterial and neurologic injury, respectively.
Schenck Classification
based on a pattern of multi ligamentous injury of knee dislocation (KD)
The Schenck and Wascher classifications of knee dislocations.
Group
Sub-Group
Definition
KD-I
Single cruciate only
KD-II
Bicruciate disruption only (rare)
KD-III
Bicruciate and posteromedial or posterolateral disruption (common)
KD-IV
Bicruciate and posteromedial and posterolateral disruption
KD-V
Dislocation with associated fracture
KD-V1
Single cruciate only
KD-V2
Bicruciate disruption only
KD-V3M
Bicruciate and posteromedial disruption
KD-V3L
Bicruciate and posterolateral disruption
KD-V4
Bicruciate and posteromedial and posterolateral disruption
C
Indicates associated arterial injury when suffixed to main group
N
Indicates associated neural injury when suffixed to main group
Causes of Knee Dislocation
Car accidents – If you bang your knee against a hard surface like your dashboard, the force of the blow may be strong enough to dislocate your knee.
Sports injuries – This is less common than car accidents, but it’s possible to dislocate your knee if you collide with great force with another player or with the ground when your knee is bent, or if you over-extend your knee (bend it back farther than it’s supposed to go).
Hard falls – It may happen to skiers or runners who lose control and fall on a bent or overextended knee. You may even dislocate your knee if you fall after stepping into a hole in the ground by mistake.
Result of major trauma – and about half occur as a result of minor trauma.[rx] Major trauma may include mechanisms like falls from a significant height, motor vehicle collisions, or a pedestrian being hit by a motor vehicle.
Major trauma – often have other injuries.[rx] Minor trauma may include tripping while walking or while playing sports. Risk factors include obesity.[rx] The condition may also occur in a number of genetic disorders such as Ellis–van Creveld syndrome, Larsen syndrome, and Ehlers–Danlos syndrome.[rx]
Sudden forceful fall down
Road traffic accident
Falls – Falling onto an outstretched hand is one of the most common causes of the broken or dislocation knee.
Sports injuries – Many cervical spine fractures occur during contact sports or sports in which you might fall onto an outstretched hand — such as in-line skating or snowboarding.
Motor vehicle crashes – Motor vehicle crashes can cause the knee dislocation to break, sometimes into many pieces, and often require surgical repair.
Have osteoporosis – a disease that weakens your bones
Eave low muscle mass or poor muscle strength – or lack agility and have poor balance (these conditions make you more likely to fall)
Walk or do other activities in the snow or on the ice – or do activities that require a lot of forwarding momenta, such as in-line skating and skiing.
Previous fractures record.
Wave an inadequate intake of calcium or vitamin D.
Football or soccer, especially on artificial turf
Athletic injury with a sports injury.
The ligamentum patellae. Attached above to the lower border of the patella and below to the tuberosity of the tibia. A continuation of the central portion of the common tendon of the quadriceps femoris muscle. The oblique popliteal ligament. A tendinous expansion derived from the semimembranosus muscle. It strengthens the posterior aspect of the capsule.
Symptoms of Knee Dislocation
CT angiogram 3D reconstruction, posterior view showing a normal artery on the left, and occlusion to right popliteal artery as a result of a knee dislocation
Symptoms include knee pain. The joint may also be obviously out of place. A joint effusion is not always present.[rx]
Hearing a “popping” sound at the time of injury
Severe pain in the area of the knee
A visible deformity at the knee joint
Instability of the knee joint, or feeling like your knee joint is “giving way”
Limitations in the range of movement of your knee
Inability to continue with activities, whether they involve day-to-day tasks or sports
Feeling the kneecap shift or slide out of the groove
Feeling the knee buckle or give way
Hearing a popping sound when the patella dislocates
Swelling
A change in the knee’s appearance — the knee may appear misshapen or deformed
Apprehension or fear when running or changing direction.
Ankle-Brachial Index (ABI) – Normal ABI (as well as pulses, Capillary Refill) may not exclude popliteal artery disruption
Hard signs of vascular injury
Distal pulse loss or ischemia (e.g. pallor, coolness)
Active bleeding
Expanding hematoma
Palpable thrill or bruit over the popliteal artery
Neurologic Exam (especially peroneal nerve)
First web space and dorsal foot sensation
Ankle dorsiflexion
Multidirectional instability
Multidirectional instability may be only finding if knee spontaneously reduced prior to presentation
Three of four ligaments are likely injured (ACL Tear, PCL Tear, LCL tear, MCL tear)
Skin changes
Dimple Sign – Anteromedial skinfold at medial joint line. Seen in posterolateral dislocation (not reducible without surgery)
Skin necrosis – Entrapped skin at femoral condyle
Overlying Laceration – Suggests open Knee Dislocation (accompanies 20-30% of Knee Dislocations)
Others exam may include
Checking the pulse in several places on your leg and knee – This is called checking posterior tibial and dorsal pedal pulses, which are located in the region of the knee and foot. Lower pulses in your injured leg could indicate an injury to a blood vessel in your leg.
Checking the blood pressure in your leg – Called the ankle-brachial index (ABI), this test compares the blood pressure measured in your arm to the blood pressure measured in your ankle. A low ABI measurement can indicate poor blood flow to your lower extremities.
Checking your sense of touch or sensation – Your doctor will assess the feeling in the injured leg versus the unaffected leg.
Checking nerve conduction – Tests like electromyography (EMG) or nerve conduction velocity (NCV) will measure the function of the nerves in your leg and knee.
Checking your skin color and temperature – If your leg is cold or changing colors, there may be blood vessel problems.
X-rays – These tests create clear pictures of bone. Your doctor may order x-rays to look for skeletal abnormalities in the knee, such as a shallow groove in the femur.
Magnetic resonance imaging (MRI) scans – These scans create better pictures of the soft structures surrounding the knee, like ligaments. An MRI is seldom necessary because the doctor can usually diagnose a dislocated patella through an examination and x-rays. However, if your doctor needs additional, more detailed images, he or she may order an MRI.
Treatment of Knee Dislocation
Nonoperative
Immobilization – Your doctor may recommend that your child wear a brace for 3 to 4 weeks. This stabilizes the knee while it heals.
Weightbearing – Because putting weight on the knee may cause pain and slow the healing process, your doctor may recommend using crutches for the first week or two after the injury.
Physical therapy – Once the knee has started to heal, your child’s doctor will recommend physical therapy to help your child regain normal motion. Specific exercises will strengthen the thigh muscles holding the knee joint in place. Your child’s commitment to the exercise program is important for a successful recovery. Typically, children return to activity 3 to 6 weeks after the injury.
Emergent closed reduction followed by vascular assessment/consult – indications to considered an orthopedic emergency, vascular consult indicated if pulses are absent or diminished following reduction if arterial injury confirmed by arterial duplex ultrasound or CT angiography
Immobilization as definitive management – successful closed reduction without vascular compromise, most cases require some form of surgical stabilization following reduction, outcomes of worse outcomes are seen with nonoperative management/prolonged immobilization will lead to loss of ROM with persistent instability.
Rest Your Leg – Once you’re discharged from the hospital in a legislating, your top priority is to rest your and not further inflame the injury. Of course, the arm sling not only provides support, but it also restricts movement, which is why you should keep it on even during sleep. Avoiding the temptation to move your will help the bone mend quicker and the pain fades away sooner.
Depending on what you do for a living and if the injury is to your dominant side, you may need to take a couple of weeks off work to recuperate.
Healing takes between four to six weeks in younger people and up to 12 weeks in the elderly, but it depends on the severity of the radial head fractures.
Athletes in good health are typically able to resume their sporting activities within two months of breaking they’re ulnar styloid depending on the severity of the break and the specific sport.
Sleeping on your back (with the sling on) is necessary to keep the pressure off your shoulder and prevent stressing the hip injury.
Eat Nutritiously During Your Recovery
All bones and tissues in the body need certain nutrients in order to heal properly and in a timely manner. Eating a nutritious and balanced diet that includes lots of minerals and vitamins are proven to help heal broken bones of all types. Therefore focus on eating lots of fresh produce (fruits and veggies), whole grains, lean meats, and fish to give your body the building blocks needed to properly repair your. In addition, drink plenty of purified water, milk, and other dairy-based beverages to augment what you eat.
Broken bones need ample minerals (calcium, phosphorus, magnesium, boron) and protein to become strong and healthy again.
Excellent sources of minerals/protein include dairy products, tofu, beans, broccoli, nuts and seeds, sardines, and salmon.
Important vitamins that are needed for bone healing include vitamin C (needed to make collagen), vitamin D (crucial for mineral absorption), and vitamin K (binds calcium to bones and triggers collagen formation).
Conversely, don’t consume food or drink that is known to impair bone/tissue healing, such as alcoholic beverages, sodas, most fast food items and foods made with lots of refined sugars and preservatives.
Physical Therapy
Although there will be some pain, it is important to maintain arm motion to prevent stiffness. Often, patients will begin doing exercises for elbow motion immediately after the injury. It is common to lose some leg strength. Once the bone begins to heal, your pain will decrease and your doctor may start gentle hip, knee exercises. These exercises will help prevent stiffness and weakness. More strenuous exercises will be started gradually once the fracture is completely healed.
Follow-Up Care
You will need to see your doctor regularly until your fracture heals. During these visits, he or they will take x-rays to make sure the bone is healing in a good position. After the bone has healed, you will be able to gradually return to your normal activities.
Opioids – Also known as narcotics, these medications are intense pain relievers that should only be used under a doctor’s careful supervision.
Topical Medications – These prescription-strength creams, gels, ointments, patches, and sprays help relieve pain and inflammation through the skin.
Calcium & vitamin D3 – to improve bone health and healing fracture. As a general rule, men and women age 50 and older should consume 1,200 milligrams of calcium a day, and 600 international units of vitamin D a day.
Glucosamine & Diacerein, Chondroitin sulfate – can be used to tightening the loose tension, cartilage, ligament, and cartilage, ligament regenerate cartilage or inhabit the further degeneration of cartilage, ligament
Antidepressants – A drug that blocks pain messages from your brain and boosts the effects of endorphins (your body’s natural painkillers).
Surgical Treatment
Open reduction
irreducible knee
posterolateral dislocation
open fracture-dislocation
obesity (may be difficult to obtain closed)
vascular injury
External fixation
vascular repair (takes precedence)
open fracture-dislocation
compartment syndrome
obese (if difficult to maintain reduction)
polytrauma patient
Delayed ligamentous reconstruction/repair
instability will require some kind of ligamentous repair or fixation
patients can be placed in a knee immobilizer until treated operatively
improved outcomes with early treatment (within 3 weeks)
Arthroscopy +/- open debridement
Arthroscopic or open debridement with removal of any loose bodies may be necessary for displaced osteochondral fractures or loose bodies.
MPFL re-attachment or reconstruction (proximal realignment)
Proximal realignment constitutes the reconstruction of the MPFL. In brief, to repair the ligament, a longitudinal incision is made at the border of the VMO, just anterior to the medial epicondyle. The ligament is usually re-attached to the femur using bone anchors. If the patient has had recurrent dislocations, then reconstruction may be necessary by harvesting gracilis or semitendinosus which are then attached to the patella and femur.
Isolated repair/reconstruction of the MPFL is not a recommendation in those with bony abnormalities including TT-TG distance greater than 20mm, convex trochlear dysplasia, severe patella alta, advanced cartilage degeneration or severe femoral anteversion.[rx]
Lateral release (distal realignment)
A lateral release cuts the retinaculum on the lateral aspect of the knee joint. The aim is to improve the alignment of the patella by reducing the lateral pull.
Osteotomy (distal realignment)
Where there is abnormal anatomy contributing to poor patella tracking and a high TT-TG distance, the alignment correction can be through an osteotomy. The most common procedure of this type is known as the Fulkerson-type osteotomy and involves an osteotomy as well as removing the small portion of bone to which the tendon attaches and repositioning it in a more anteromedial position on the tibia.
Trochleoplasty
Trochleoplasty is indicated in recurrent dislocators with a convex or flat trochlea. The trochlear groove is deepened to create a groove for the patella to glide through; this may take place alongside an MPFL reconstruction. Studies suggest it is not advisable in those with open growth plates or severely degenerative joints. This procedure is uncommon except in refractory cases.
Complications of Knee Dislocation
Vascular compromise
incidence of – 5-15% in all dislocations. 40-50% in anterior or posterior dislocations
risk factors – KD IV injuries have the highest rate of vascular injuries
treatment-emergent vascular repair and prophylactic fasciotomies
Stiffness (arthrofibrosis)
incidence – most common complication (38%)
risk factors – more common with delayed mobilization
avoid stiffness with early reconstruction and motion
arthroscopic lysis of adhesion
manipulation under anesthesia
Laxity and instability
incidence – 37% of some instability, however, redislocation is uncommon
treatment – arthroscopic lysis of adhesion, manipulation under anesthesia
Peroneal nerve injury
incidence- 25% occurrence of a peroneal nerve injury, 50% recover partially
posterolateral dislocations
Treatment
A to prevent equinus contracture
neurolysis or exploration at the time of reconstruction
nerve repair or reconstruction or tendon transfers if chronic nerve palsy persists
a dynamic tendon transfer involves transferring the posterior tibial tendon (PTT) to the foot