Cervical spondylosis is a generalized disease process affecting all levels of the cervical spine. Cervical spondylosis encompasses a sequence of degenerative changes in the intervertebral discs, osteophytosis of the vertebral bodies, hypertrophy of the facets and laminal arches, and ligamentous and segmental instability. The natural history of cervical spondylosis is associated with the aging process. Senescent and pathologic processes are thus morphologically indistinguishable. Clinical manifestations of cervical spondylosis may arise when morphologic sequelae are superimposed on a developmentally narrow spinal canal. The two clinical syndromes of spondylotic radiculopathy and myelopathy are distinct, yet they may overlap.[rx]
Cervical spondylosis is a term that encompasses a wide range of progressive degenerative changes that affect all the components of the cervical spine (i.e., intervertebral discs, facet joints, joints of Luschka, ligaments Flava, and laminae). It is a natural process of aging and presents in the majority of people after the fifth decade of life.[rx]
Causes of Cervical Spondylosis
A clinical syndrome caused by compression on the spinal cord that is characterized by
clumsiness in hands
gait imbalance
degenerative cervical spondylosis (CSM)
compression usually caused by anterior degenerative changes (osteophytes, disc osteophyte complex)
degenerative spondylolisthesis and hypertrophy of ligamentum flavum may contribute
the most common cause of cervical myelopathy
Congenital stenosis
Symptoms usually begin when congenital narrowing combined with spondylotic degenerative changes in older patients
OPLL
tumor
epidural abscess
trauma
cervical kyphosis
Neurologic injury
mechanism of injury can be
direct cord compression
ischemic injury secondary to compression of the anterior spinal artery
tandem stenosis occurs in the lumbar and cervical spine in ~20% of patients
tends to be slowly progressive and rarely improves with nonoperative modalities
progression characterized by steplike deterioration with periods of stable symptoms
early recognition and treatment prior to spinal cord damage is critical for good clinical outcomes
Risk Factors for Cervical Spondylosis
The lists below are the factors that you will have a higher risk of getting neck pain and cervical spondylosis:
Genetics – if your family has a history of neck pain
Smoking – clearly linked to increased neck pain
Occupation – jobs with lots of neck motion and overhead work
Mental health issues – depression/anxiety
Injuries/trauma – car wreck or on-the-job injury
“Red flag” features and the conditions they may suggest
Malignancy, infection, or inflammation
Fever, night sweats
Unexpected weight loss
History of inflammatory arthritis, malignancy, infection, tuberculosis, HIV infection, drug dependency, or immunosuppression
Excruciating pain
Intractable night pain
Cervical lymphadenopathy
Exquisite tenderness over a vertebral body
Myelopathy
Gait disturbance or clumsy hands, or both
Objective neurological deficit—upper motor neuron signs in the legs and lower motor neuron signs in the arms
Sudden onset in a young patient suggests disc prolapse
Other
History of severe osteoporosis
History of neck surgery
Drop attacks, especially when moving the neck, suggest vascular disease
Intractable or increasing pain
Symptoms of Cervical spondylosis
The pain can be from minor to major and it becomes worse when looking up or down for a long period of time, such example is reading a book or driving. To improve the pain, most people tend to takes rest or even lay down. The pain usually becomes worse in the morning and at the end of the day.
Symptoms of cervical spondylosis include
Neck stiffness and pain
Numbness and weakness in the upper limbs
Difficulty in walking, losing balance, or weakness in limbs
Difficulty in turning the head fully or bending the neck, which may hinder drive
Muscle spasms in neck and shoulders
Headaches
Grinding and popping feeling in the neck when rotating the head
Loss of bladder and bowel control.
Axial neck pain (oftentimes absent)
Occipital headache common
Extremity paresthesias
Diffuse non-dermatomal numbness and tingling
Weakness and clumsiness
Weakness and decreased manual dexterity (dropping object, difficulty manipulating fine objects)
Gait instability patient feels “unstable” on feet
Weakness walking up and downstairs
Gait changes are the most important clinical predictor
Urinary retention rare and only appear late in disease progression, not very useful in diagnosis due to the high prevalence of urinary conditions in this patient population
Cervical pain aggravated by movement
Referred pain (occiput, between the shoulder blades, upper limbs)
Retro-orbital or temporal pain (from C1 to C2)
Cervical stiffness—reversible or irreversible
Vague numbness, tingling, or weakness in upper limbs
Dizziness or vertigo
Poor balance
Rarely, syncope triggers a migraine pseudo-angina
Poorly localized tenderness
Limited range of movement (forward flexion, backward extension, lateral flexion, and rotation to both sides)
Minor neurological changes like inverted supinator jerks (unless complicated by myelopathy or radiculopathy)
Diagnosis of Cervical Spondylosis
Classically, symptomatic cervical spondylosis presents as one or more of the following three primary clinical syndromes
Axial neck pain
Commonly complain of stiffness and pain in the cervical spine that is most severe in the upright position and relieved with bed rest when removing the load from the neck
Neck motion, especially in hyperextension and side-bending, typically increases the pain
In upper and lower cervical spine disease, patients may report radiating pain into the back of the ear or occiput versus radiating pain into the superior trapezius or periscapular musculature, respectively
Occasionally, patients can present with atypical symptoms of cervical angina such as jaw pain or chest pain.
Cervical radiculopathy
Radicular symptoms usually follow a myotomal distribution depending on the nerve root(s) involved and can present as unilateral or bilateral neck pain, arm pain, scapular pain, paresthesia, and arm or hand weakness
Pain is exacerbated by head tilt toward the affected side or by hyperextension and side-bending toward the affected side.
Cervical myelopathy
Typically has an insidious onset with or without neck pain (frequently absent)
Can initially present with hand weakness and clumsiness, resulting in the inability to complete tasks requiring fine motor coordination (e.g., buttoning a shirt, tying shoelaces, picking up small objects)
Frequent reports of gait instability and unexplained falls
Urinary symptoms (i.e., incontinence) are rare and typically appear late in disease progression
Physical exam of Cervical spondylosis
Other non-specific neck pain lesions—acute neck strain, postural neck ache, or whiplash
Fibromyalgia – and psychogenic neck pain
Mechanical lesions – disc prolapse or diffuse idiopathic skeletal hyperostosis
Inflammatory disease – rheumatoid arthritis, ankylosing spondylitis, or polymyalgia rheumatica
Metabolic diseases – Paget’s disease, osteoporosis, gout, or pseudo-gout
Infections – osteomyelitis or tuberculosis
Malignancy – primary tumors, secondary deposits, or myeloma
lower extremity weakness is more concerning finding
finger escape sign when the patient holds fingers extended and adducted, the small finger spontaneously abducts due to the weakness of intrinsic muscle grip and release test normally a patient can make a fist and release 20 times in 10 seconds. myelopathic patients may struggle to do this
Upper motor neuron signs
Hoffman’s sign (quick flexion of both the thumb and index finger when the middle fingernail is snapped)
Inverted radial reflex (flexion of the fingers in response to the brachioradialis reflex)
Pathological clonus
Babinski sign
Sensory dysfunction
Glove-like sensory loss in hands
Proprioceptive dysfunction
Proprioception dysfunction
due to dorsal column involvement
occurs in advanced disease
associated with a poor prognosis
Decreased pain sensation
pinprick testing should be done to look for a global decrease in sensation or dermatomal changes
due to the involvement of lateral spinothalamic tract
vibratory changes are usually only found in the severe case of long-standing myelopathy
Assessment tools
Lhermitte sign
Romberg test
9-Hole peg test
Grip and release test (observe a decreasing number of cycles)
Timed gait, 30-m walking test
Tandem gait
Upper motor neuron signs (spasticity)
Hyperreflexia – may be absent when there is concomitant peripheral nerve disease (cervical or lumbar nerve root compression, spinal stenosis, diabetes)
Hoffmann’s sign – snapping patients distal phalanx of the middle finger leads to spontaneous flexion of other fingers
Sustained clonus
> three beats defined as sustained clonus
sustained clonus has poor sensitivity (~13%) but high specificity (~100%) for cervical myelopathy
Babinski test
considered positive with the extension of the great toe
Gait and balance
toe-to-heel walk patient has difficulty performing
Romberg test patient stands with arms held forward and eyes closed loss of balance consistent with posterior column dysfunction
provocative tests: Lhermitte Sign >test is positive when extreme cervical flexion leads to electric shock-like sensations that radiate down the spine and into the extremities
Motor dysfunction
Upper extremities
0
Unable to move hands
1
Unable to eat with a spoon but able to move hands
2
Unable to button shirt but able to eat with a spoon
3
Able to button shirt with great difficulty
4
Able to button shirt with slight difficulty
Lower extremities
0
Complete loss of motor & sensory function
1
Sensory preservation without the ability to move legs
2
Able to move legs but unable to walk
3
Able to walk on a flat floor with a walking aid (cane or crutch)
4
Able to walk up- &/or downstairs w/aid of a handrail
5
Moderate-to-significant lack of stability but able to walk up &/or downstairs without a handrail
6
Mild lack of stability but able to walk unaided with smooth reciprocation
recommended views cervical AP, lateral, oblique, flexion, and extension views
general findings degenerative changes of uncovertebral and facet joints
osteophyte formation
disc space narrowing
decreased sagittal diameter
cord compression occurs with canal diameter is < 13mm
lateral radiograph important to look for the diameter of the spinal canal
a Pavlov ratio of less than 0.8 suggests a congenitally narrow spinal canal predisposing to stenosis and cord compression
Sagittal alignment
C2 to C7 alignment determined by tangential lines on the posterior edge of the C2 and C7 body on lateral radiographs in neutral position
Local kyphosis angle the angle between the lines drawn at the posterior margin of most cranial and caudal vertebral bodies forming the maximum local kyphosis
Oblique radiograph important to look for foraminal stenosis which often caused by uncovertebral joint arthrosis
Flexion and extension views important to look for angular or translational instability look for compensatory subluxation above or below the spondylotic/stiff segment
Sensitivity/specificity changes often do not correlate with symptoms 70% of patients by 70 yrs of age will have degenerative changes seen on plain x -rays
X-ray
Plain radiographs are an appropriate initial imaging study for neck and upper extremity pain in the absence of “red flag” symptoms. However, degenerative changes seen on imaging often poorly correlate with the presence of neck pain.[rx]
Common radiographic findings include osteophyte formation, disc space narrowing, endplate sclerosis, degenerative changes of uncovertebral and facet joints, and calcified/ossified soft tissues. AP, lateral, and oblique views of the spine are adequate to evaluate for foraminal stenosis, sagittal alignment, and size of the spinal canal.
The Torg-Pavlov ratio is obtainable by comparing the sagittal diameter of the spinal canal to the sagittal diameter of the vertebral body. The normal value is 1.0, with a ratio of <0.8 indicating cervical stenosis. Flexion and extension views also merit consideration if there is a concern for ligamentous instability.
MRI
MRI is a study of choice to evaluate the degree of the spinal cord and nerve root compression effacement of CSF indicates functional stenosis
Signal changes on T1-weighted images correlate with a poorer prognosis following surgical decompression spinal cord signal changes
Seen as bright signal on T2 images (myelomalacia) compression ratio of < 0.4 carries poor prognosis CR = smallest AP diameter of cord / largest transverse diameter of the cord
Sensitivity/specificity has a high rate of false-positive (28% greater than 40 will have findings of HNP or foraminal stenosis)
CT without contrast can provide complementary information with an MRI and is more useful to evaluate OPLL and osteophytes
CT myelography more invasive than an MRI but gives excellent information regarding degrees of spinal cord compression
Useful in patients that cannot have an MRI (pacemaker), or have artifact (local hardware)
Contrast is given via C1-C2 puncture and allowed to diffuse caudally, or given via a lumbar puncture and allowed to diffuse proximally by putting the patient in Trendelenburg position.
Computed tomography (CT)
CT provides a good definition of bony structures and is more sensitive than plain radiographs in assessing intervertebral foraminal stenosis in the setting of uncovertebral or facet hypertrophy. However, it is less sensitive than MRI for the evaluation of soft tissues and nerve root compression.
CT myelogram
CT is most useful when combined with the injection of intrathecal contrast (myelography) to better evaluate the location and amount of neural compression. It is more invasive than an MRI but can be a consideration in patients who have a contraindication to MRI (e.g., pacemaker) or have an artifact from the hardware.
Discogram
Provocative discography is rarely necessary for cervical spondylosis. It is useful for the evaluation of patients who are experiencing cervical discogenic pain or have multiple herniations in which surgery is a strong possibility. However, the diagnostic procedure remains controversial as it may accelerate the degeneration of normal discs.[rx]
Electromyogram (EMG)
EMG can be useful in supplementing neuroimaging findings in the diagnosis of cervical radiculopathy. It is especially valuable in differentiating nerve root compression from other possible concomitant neurologic conditions, including peripheral neuropathies, entrapment neuropathies, brachial plexopathies, myopathies, and motor neuron diseases.
Nerve conduction studies high false-negative rate may be useful to distinguish peripheral from the central process (ALS)
Normal aging mild symptoms of myelopathy often confused with a “normal aging” process
Stroke
Movement disorders
Vitamin B12 deficiency
Amyotrophic lateral sclerosis (ALS)
Multiple sclerosis
Treatment of Cervical spondylosis
Nonoperative
Observation, NSAIDs, therapy, and lifestyle modifications
indications of mild disease with no functional impairment
the function is a more important determinant for surgery than physical exam finding
patients who are poor candidates for surgery
modalities medications (NSAIDS, gabapentin)
immobilization (hard collar in slight flexion)
physical therapy for neck strengthening, balance, and gait training
traction and chiropractic modalities are not likely to benefit and do have some risks
be sure to watch patients carefully for progression
outcomes improved nonoperative outcomes associated with patients with larger transverse area of the spinal cord (>70mm2)
some studies have shown improvement with immobilization in patients with very mild symptoms
Operative
surgical decompression, restoration of lordosis, stabilization
indications significant functional impairment AND 1-2 level disease lordotic, neutral or kyphotic alignment
techniques appropriate procedure depends on cervical alignment number of stenotic levels
medical conditions (e.g., goiter)
location of compression
anterior cervical diskectomy/corpectomy and fusion
posterior laminectomy and fusion
posterior laminoplasty
combined anterior and posterior procedure
cervical disk arthroplasty
outcomes prospective studies show improvement in overall pain, function, and neurologic symptoms with operative treatment early recognition and treatment prior to spinal cord damage is critical for good clinical outcomes
Goals
optimal surgical treatment depends on the individual. Things to consider include
number of stenotic levels
sagittal alignment of the spine
the degree of existing motion and desire to maintain
medical comorbidities (eg, dysphasia)
simplified treatment algorithm
Anterior Decompression and Fusion (ACDF) alone
Indications
the mainstay of treatment in most patients with single or two level disease
fixed cervical kyphosis of > 10 degrees anterior procedure can correct kyphosis
compression arising from 2 or fewer disc segments
pathology is anterior (OPLL, soft discs, disc osteophyte complexes)
Approach
uses Smith-Robinson anterior approach
Decompression of corpectomy and strut graft may be required for multilevel spondylosis two level corpectomies tend to be biomechanically vulnerable (preferable to combine single-level corpectomy with adjacent level diskectomy)
7% to 20% rates of graft dislodgement with cervical corpectomy with associated severe complications, including death, reported.
fixation anterior plating functions to increase fusion rates and preserve the position of the interbody cage or strut graft
pros & cons advantages compared to posterior approach lower infection rate blood loss less postoperative pain disadvantages avoid in patients with poor swallowing function
Laminectomy with posterior fusion
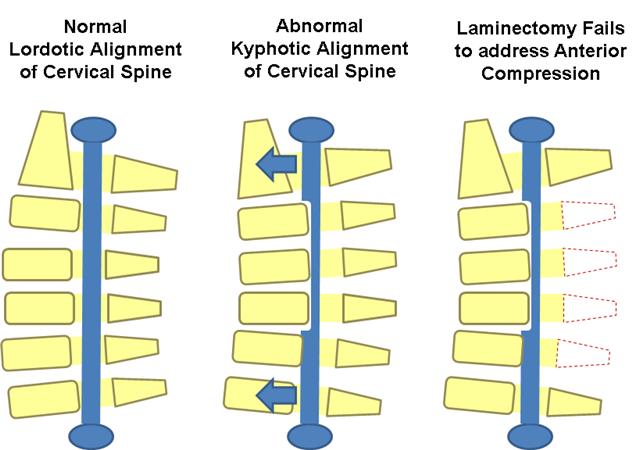
multilevel compression with kyphosis of < 10 degrees,> 13 degrees of fixed kyphosis is a contraindication for a posterior procedure
in the flexible kyphotic spine, posterior decompression and fusion may be indicated if kyphotic deformity can be corrected prior to instrumentation
Contraindications
fixed kyphosis of > 10 degrees is a contraindication to posterior decompression
will not adequately decompress spinal cord as it is “bowstringing” anterior
Pros & cons
fusion may improve neck pain associated with degenerative facets
not effective in patients with > 10 degrees fixed kyphosis
Laminoplasty
gaining in popularity
useful when maintaining motion is desired
avoids complications of fusion so may be indicated in patients at high risk of pseudoarthrosis
Contraindications
cervical kyphosis > 13 degrees is a contraindication to posterior decompression will not adequately decompress spinal cord as it is “bowstringing” anterior
severe axial neck pain is a relative contraindication and these patients should be fused
Technique
the volume of the canal is expanded by hinged-door laminoplasty followed by fusion usually performed from C3 to C7
open door technique hinges created unilaterally at the junction of lateral mass and lamina and opening on opposite side opening held open by bone, suture anchors, or special plates
French door technique hinge created bilaterally and the opening created midline
Pros & cons advantages
lower complication rate than multilevel anterior decompression especially in patients with OPLL a motion-preserving technique pseudoarthrosis not a concern in patients with poor healing potential (diabetes, chronic steroid users) can be combined with a subsequent anterior procedure
allows for decompression of multilevel stenotic myelopathy without compromising stability and motion (avoids postlaminectomy kyphosis)
Disadvantages
higher average blood loss than anterior procedures
postoperative neck pain
still associated with loss of motion outcomes equivalent to multilevel anterior decompression and fusion
Combined anterior and posterior surgery multilevel stenosis in the rigid kyphotic spine
multi-level anterior cervical corpectomies
postlaminectomy kyphosis
Laminectomy alone
indications rarely indicated due to risk of post laminectomy kyphosis
pros & cons progressive kyphosis 11 to 47% incidence if laminectomy performed alone without fusion
Surgical Infection
higher rate of surgical infection with posterior approach than anterior approach
Pseudoarthrosis incidence 12% for single level fusions, 30% for multilevel fusions treatment
treat with either posterior wiring or plating or repeat anterior decompression and plating if patient has symptoms of radiculopathy
Postoperative C5 palsy
reported to occur in ~ 4.6% of patients after surgery for cervical compression myelopathy
no significant differences between patients undergoing anterior decompression and fusion and posterior laminoplasty
occurs immediately postop to weeks following surgery
Mechanism
mechanism is controversial
in laminectomy patients, it is thought to be caused by tethering of nerve root with dorsal migration of spinal cord following removal of posterior elements
Prognosis
patients with postoperative C5 palsy generally have a good prognosis for functional recovery, but recovery takes time
Recurrent laryngeal nerve injury approach in the past it has been postulated that the RLN is more vulnerable to injury on the right due to a more aberrant pathway recent studies have shown there is not an increased injury rate with a right sided approach
treatment if you have a postoperative RLN palsy, watch over time
if not improved over 6 weeks, then ENT consult to scope patient and inject Teflon
if you are performing revision anterior cervical surgery, and there is any suspicion of an RLN from the first operation, obtain ENT consult to establish prior injury
if a patient has prior RLN nerve injury, perform revision surgery on the same as the prior injury/approach to prevent a bilateral RLN injury
Hardware failure and migration 7-20% with two-level anterior corpectomies two-level corpectomies should be stabilized from behind
Postlaminectomy kyphosis treat with anterior/posterior procedure
In a 2019 cohort study by El-Yahochouchi et al., the overall incidence of immediate and delayed adverse events following an epidural steroid injection was 2.4% and 4.9%, respectively.[rx] Complications include:

{kind=link}
{kind=link}
{kind=link}
About the author