The venous system refers to the network of veins that work to deliver deoxygenated blood back to your heart. Veins are a type of blood vessel that returns deoxygenated blood from your organs back to your heart. These are different from your arteries, which deliver oxygenated blood from your heart to the rest of your body.
Deoxygenated blood that flows into your veins is collected within tiny blood vessels called capillaries. Capillaries are the smallest blood vessels in your body. Oxygen passes through the walls of your capillaries to your tissues. Carbon dioxide can also move into your capillaries from the tissue before entering your veins.
Venules
Venules are small blood vessels in the microcirculation that connect capillary beds to veins.
Key Points
Many venules unite to form a vein.
Venule walls have three layers: an inner endothelium composed of squamous endothelial cells that act as a membrane, a middle layer of muscle and elastic tissue, and an outer layer of fibrous connective tissue.
High-endothelial venules are specialized post-capillary venous swellings characterized by plump endothelial cells, in contrast with the thinner endothelial cells found in regular venues.
Key Terms
high endothelial venule: A specialized post-capillary venous swelling of the lymphatic system that allows lymphocytes (white blood cells) to easily exit the circulatory system.
venule: A small blood vessel in the microcirculation that allows deoxygenated blood to return from capillary beds to veins.
A venule is a small blood vessel in the microcirculation that allows deoxygenated blood to return from capillary beds to larger blood vessels called veins. Venules range from 8 to 100μm in diameter and are formed when capillaries come together. Many venules unite to form a vein.
Venule: Venules form when capillaries come together and converging venules from a vein.
Venule walls have three layers: an inner endothelium composed of squamous endothelial cells that act as a membrane, a middle layer of muscle and elastic tissue, and an outer layer of fibrous connective tissue. The middle layer is poorly developed so that venules have thinner walls than arterioles. Venules are extremely porous so that fluid and blood cells can move easily from the bloodstream through their walls.
In contrast to regular venules, high-endothelial venules (HEV) are specialized post-capillary venous swellings. They are characterized by plump endothelial cells as opposed to the usual thinner endothelial cells found in regular venues. HEVs enable lymphocytes (white blood cells) circulating in the blood to directly enter a lymph node by crossing through the HEV.
Veins
Veins are blood vessels that carry blood from tissues and organs back to the heart; they have thin walls and one-way valves.
Key Points
The difference between veins and arteries is the direction of blood flow (out of the heart through arteries, returning to the heart through veins).
Veins differ from arteries in structure and function. For example, arteries are more muscular than veins, veins are often closer to the skin, and veins contain valves to help keep blood flowing toward the heart, while arteries do not have valves and carry blood away from the heart.
Veins are also called capacitance vessels because they contain 60% of the body’s blood volume.
The return of blood to the heart is assisted by the action of the skeletal- muscle pump. As muscles move, they squeeze the veins running through them. Veins contain a series of one-way valves, and they are squeezed, blood is pushed through the valves, which then close to prevent backflow.
Key Terms
venous pooling: When blood accumulates in the lower extremities, resulting in low venous return to the heart which can result in fainting.
skeletal-muscle pump: Rhythmic contraction of limb muscles that occurs during normal locomotory activity (walking, running, swimming), which promotes venous return by the pumping action on veins within muscles.
portal vein: A short, wide vein that carries blood to the liver from the organs of the digestive system.
Veins are blood vessels that carry blood towards the heart. Most carry deoxygenated blood from the tissues back to the heart, but the pulmonary and umbilical veins both carry oxygenated blood to the heart. The difference between veins and arteries is the direction of blood flow (out of the heart through arteries, back to the heart through veins), not their oxygen content. Veins differ from arteries in structure and function. For example, arteries are more muscular than veins, veins are often closer to the skin, and veins contain valves to help keep blood flowing toward the heart, while arteries do not have valves and carry blood away from the heart. The precise location of veins is much more variable than that of arteries since veins often display anatomical variation from person to person.
Veins are also called capacitance vessels because they contain 60% of the body’s blood volume. In the systemic circulation, oxygenated blood is pumped by the left ventricle through the arteries to the muscles and organs of the body, where its nutrients and gases are exchanged at capillaries. The blood then enters venules, then veins filled with cellular waste and carbon dioxide. The deoxygenated blood is taken by veins to the right atrium of the heart, which transfers the blood to the right ventricle, where it is then pumped through the pulmonary arteries to the lungs. In pulmonary circulation the veins return oxygenated blood from the lungs to the left atrium, which empties into the left ventricle, completing the cycle of blood circulation.
Mechanisms to Return Blood
The return of blood to the heart is assisted by the action of the skeletal-muscle pump and by the thoracic pump action of breathing during respiration. As muscles move, they squeeze the veins that run through them. Veins contain a series of one-way valves. As the vein is squeezed, it pushes blood through the valves, which then close to prevent backflow. Standing or sitting for prolonged periods can cause low venous return from venous pooling. In venous pooling, the smooth muscles surrounding the veins become slack and the veins fill with the majority of the blood in the body, keeping blood away from the brain, which can cause unconsciousness.
Venous valve: Venous valves prevent backflow and ensure that blood flows in one direction.
Although most veins take the blood back to the heart, portal veins carry blood between capillary beds. For example, the hepatic portal vein takes blood from the capillary beds in the digestive tract and transports it to the capillary beds in the liver. The blood is then drained into the gastrointestinal tract and spleen, where it is taken up by the hepatic veins and blood is taken back into the heart. Since this is an important function in mammals, damage to the hepatic portal vein can be dangerous. Blood clotting in the hepatic portal vein can cause portal hypertension, which results in a decrease of blood fluid to the liver.
Vein Classification
Veins are classified in a number of ways, including superficial vs. deep, pulmonary vs. systemic, and large vs. small:
Superficial veins: Superficial veins are close to the surface of the body and have no corresponding arteries.
Deep veins: Deep veins are deeper in the body and have corresponding arteries.
Communicating veins: Communicating veins (or perforator veins) directly connect superficial veins to deep veins.
Pulmonary veins: The pulmonary veins deliver oxygenated blood from the lungs to the heart.
Systemic veins: Systemic veins drain the tissues of the body and deliver deoxygenated blood to the heart.
Which conditions affect the venous system?
Many conditions can affect your venous system. Some of the most common ones include:
Deep vein thrombosis (DVT). A blood clot forms in a deep vein, usually in your leg. This clot can potentially travel to your lungs, causing pulmonary embolism.
Superficial thrombophlebitis. An inflamed superficial vein, usually in your leg, develops a blood clot. While the clot can occasionally travel to a deep vein, causing DVT, thrombophlebitis is generally less serious than DVT.
Varicose veins. Superficial veins near the surface of the skin visibly swell. This happens when one-way valves break down or vein walls weaken, allowing blood to flow backward.
Chronic venous insufficiency. Blood collects in the superficial and deep veins of your legs due to the improper functioning of one-way valves. While similar to varicose veins, chronic venous insufficiency usually causes more symptoms, including coarse skin texture and ulcers in some cases.
What are the symptoms of a venous condition?
While the symptoms of a venous condition can vary widely, some common ones include:
inflammation or swelling
tenderness or pain
veins that feel warm to the touch
a burning or itching sensation
These symptoms are especially common in your legs. If you notice any of these and they don’t improve after a few days, make an appointment with your doctor.
They can perform venography. In this procedure, your doctor injects contrast die into your veins to produce an X-ray image of a particular area.
Tips for healthy veins
Follow these tips to keep your vein walls and valves strong and properly functioning:
Get regular exercise to keep blood moving through your veins.
Try to maintain a healthy weight, which reduces your risk of high blood pressure. High blood pressure can weaken your veins over time due to added pressure.
Avoid long periods of standing or sitting. Try to change positions regularly throughout the day.
When sitting down, avoid crossing your legs for long periods of time or regularly switch positions so one leg isn’t on top for a long period of time.
When flying, drink plenty of water and try to stand up and stretch as often as possible. Even while sitting, you can flex your ankles to encourage blood flow.
Artery /Arteries make up a major part of the circulatory system, with the veins and heart being the other main components. Arteries make up tubelike structures that are responsible for the transportation of fluid (i.e., blood for the circulatory system and lymph for the lymphatic system) to and from every organ in the body. Mainly, arteries manage the transportation of oxygen, nutrients, and hormones through our bodies. Arteries can dispense fresh oxygen to the body after it gets loaded onto the Fe 2+ found in the center of hemoglobin. The oxygen binds to hemoglobin and is carried by the arteries to areas that are lacking oxygen. Through a shift in affinity for the oxygen, it is then unloaded to specific areas through high surface areas knowns as capillaries.[rx] Far from being a changeless structure, arteries adapt through signals received from the central nervous system, as they also react to an outer stimulus like pressure, temperature, and substances. Vascular nerves are responsible for innervating the arteries allowing them to change to their stimuli. As catecholamines get released into the blood, the nerves send signals to the arteries to either constrict or dilate, leading to changes in pressure.[rx]
Arteries are composed of smooth muscle allowing constriction and dilation through the parasympathetic nervous system.[rx] Arteries differ from veins in the sense that they most often are carrying oxygenated blood away from the heart and into the rest of the body system. This is not always the case; however, as the pulmonary artery moves unoxygenated blood from the heart to the lungs to complete the gas exchange in the alveoli.[rx] Arteries play a crucial role in maintaining homeostasis in the body. As individuals age, health issues begin presenting themselves in the form of stiffening or thicking of the arteries; however, many different issues develop with age and poor diet. Additionally, arteries begin to clog with a thicking of plaque known as atherosclerosis.[rx] As problems arise in the structure of the arteries, it begins leading to more strain on the heart, which develops congestive heart failure and which is often fatal. The arteries are vital to maintaining a healthy cardiovascular system, thus a healthy lifestyle.
Artery Function
Arteries are high-pressure blood vessels that carry oxygenated blood away from the heart to all other tissues and organs.
Key Points
Arteries are blood vessels that carry blood away from the heart. This blood is normally oxygenated, with the exception of blood in the pulmonary artery.
Arteries typically have a thicker tunica media than veins, containing more smooth muscle cells and elastic tissue. This allows for modulation of vessel caliber and thus control of blood pressure.
The arterial system is the higher-pressure portion of the circulatory system, with pressure varying between the peak pressure during heart contraction ( systolic pressure ) and the minimum (diastolic) pressure between contractions when the heart expands and refills.
The increase in arterial pressure during systole, or ventricular contraction, results in the pulse pressure, an indicator of cardiac function.
Key Terms
systolic pressure: The peak arterial pressure during heart contraction.
diastolic pressure: The minimum arterial pressure between contractions, when the heart expands and refills.
artery: An efferent blood vessel from the heart, conveying blood away from the heart regardless of oxygenation status.
Arteries are blood vessels that carry blood away from the heart under pressure. This blood is usually oxygenated, with the exception of that in the pulmonary artery, which carries deoxygenated blood to the lungs.
Arterial system: Simplified diagram of the human arterial system in anterior view.
As with veins, arteries are comprised of three layers: the tunicae intima, media, and external. In arteries, the tunica media, which contains smooth muscle cells and elastic tissue, is thicker than that of veins so it can modulate vessel caliber and thus control and maintain blood pressure.
Arterial pressure varies between the peak pressure during heart contraction, called the systolic pressure, and the minimum or diastolic pressure between contractions, when the heart expands and refills. This pressure variation within the artery produces the observable pulse that reflects heart activity. The pressure in the arterial system decreases steadily, highest in the aorta and lowest in the venous system, as blood approaches the heart after delivery of oxygen to tissues in the systemic circulation.
Arteries of the systemic circulation can be subdivided into muscular or elastic types according to the relative compositions of elastic and muscle tissue in their tunica media. Larger arteries are typically elastic and smaller arteries are more likely to be muscular. These arteries deliver blood to the arterioles, which in turn deliver blood to the capillary networks associated with the body’s tissues.
Elastic Arteries
An elastic or conducting artery has a large number of collagen and elastin filaments in the tunica media.
Key Points
Elastic arteries include the largest arteries in the body, those closest to the heart. They give rise to medium-sized vessels known as muscular or distributing, arteries.
Elastic arteries differ from muscular arteries both in size and in the relative amount of elastic tissue contained within the tunica media.
Arterial elasticity gives rise to the Windkessel effect, which helps to maintain relatively constant pressure in the arteries despite the pulsating nature of blood flow.
Key Terms
elastic arteries: An artery with a large number of collagen and elastin filaments, giving it the ability to stretch in response to each pulse.
tunica media: The middle layer of a vein wall with bands of thin smooth muscle.
Elastic arteries contain larger numbers of collagen and elastin filaments in their tunica media than muscular arteries do, giving them the ability to stretch in response to each pulse.
Elastic arteries include the largest arteries in the body, those closest to the heart, and give rise to the smaller muscular arteries. The pulmonary arteries, the aorta, and its branches together comprise the body’s system of elastic arteries. In these large arteries, the amount of elastic tissue is considerable and the smooth muscle fiber cells are arranged in 5 to 7 layers in both circular and longitudinal directions.
Anatomy of the Arterial Wall: Arterial wall layers including the tunica intima and the tunica media. Inelastic arteries, the tunica media is rich with elastic and connective tissue.
The aorta: The aorta makes up most of the elastic arteries in the body.
Arterial elasticity gives rise to the Windkessel effect, which through passive contraction after expansion helps to maintain relatively constant pressure in the arteries despite the pulsating nature of the blood flow from the heart.
The Aorta
Due to its position as the first part of the systemic circulatory system closest to the heart and the resultant high pressures it will experience, the aorta is perhaps the most elastic artery, featuring an incredibly thick tunica media-rich in elastic filaments. The aorta is so thick that it requires its own capillary network to supply it with sufficient oxygen and nutrients to function, the vasa vasorum.
When the left ventricle contracts to force blood into the aorta, the aorta expands. This stretching generates the potential energy that will help maintain blood pressure during diastole when the aorta contracts passively. Additionally, the elastic recoil helps conserve the energy from the pumping heart and smooth the flow of blood around the body through the Windkessel effect.
Muscular Arteries
Distributing arteries are medium-sized arteries that draw blood from an elastic artery and branch into resistance vessels.
Key Points
In contrast to the mechanism, elastic arteries use to store energy generated by the heart‘s contraction, distributing arteries contain layers of smooth muscle.
Key Terms
muscular arteries: Medium-sized arteries that draw blood from an elastic artery and branch into resistance vessels, including small arteries and arterioles.
elastic lamina: A layer of elastic tissue that forms the outermost part of the tunica intima of blood vessels. It is readily visualized with light microscopy in sections of muscular arteries.
arteriole: One of the small branches of an artery, especially one that connects with capillaries.
Splenic Artery: Transverse section of the human spleen showing the distribution of the splenic artery and its branches
Muscular or distributing arteries are medium-sized arteries that draw blood from an elastic artery and branch into resistance vessels, including small arteries and arterioles. In contrast to the mechanism elastic arteries use to store and dissipate the energy generated by the heart’s contraction, muscular arteries contain layers of smooth muscle providing allowing for involuntary control of vessel caliber and thus control of blood flow. Muscular arteries can be identified by the well-defined elastic lamina that lies between the tunica intima and media.
The splenic artery (lienal artery), the blood vessel that supplies oxygenated blood to the spleen, is an example of a muscular artery. It branches from the celiac artery and follows a course superior to the pancreas. The splenic artery branches off to the stomach and pancreas before reaching the spleen and gives rise to arterioles that directly supply capillaries of these organs.
Anastomoses
A circulatory anastomosis is a connection or looped interaction between two blood vessels.
Key Points
Anastomoses occur normally in the body in the circulatory system, serving as backup routes for blood flow if one link is blocked or otherwise compromised.
Anastomoses between arteries and between veins result in a multitude of arteries and veins, respectively, serving the same volume of tissue.
Pathological anastomoses result from trauma or disease and are referred to as fistulae.
Key Terms
circulatory anastomosis: A connection between two blood vessels, such as between arteries (arterio-arterial anastomosis), between veins (veno-venous anastomosis), or between an artery and a vein (arterio-venous anastomosis).
fistula: An abnormal connection or passageway between organs or vessels that normally do not connect.
An anastomosis refers to any joint between two vessels. Circulatory anastomoses are named based on the vessels they join: two arteries (arterio-arterial anastomosis), two veins (veno-venous anastomosis), or between an artery and a vein (arterio-venous anastomosis).
Anastomoses: The blood vessels of the rectum and anus, showing the distribution and anastomosis on the posterior surface near the termination of the gut.
Anastomoses between arteries and anastomoses between veins result in a multitude of arteries and veins serving the same volume of tissue. Such anastomoses occur normally in the body in the circulatory system, serving as backup routes for blood to flow if one link is blocked or otherwise compromised, but may also occur pathologically.
Examples of Anastomoses
Arterio-arterial anastomoses include actual joins (e.g. palmar arch, plantar arch) and potential ones, which may only function if the normal vessel is damaged or blocked (e.g. coronary arteries and cortical branch of cerebral arteries). Important examples include:
The circle of Willis in the brain.
The arrangement of the brain’s arteries into the circle of Willis creates redundancies for cerebral circulation. If one part of the circle becomes blocked or narrowed or one of the arteries supplying the circle is blocked or narrowed, blood flow from the other blood vessels can often preserve the cerebral perfusion well enough to maintain function.
Joint anastomoses. Almost all joints receive anastomotic blood supply from more than one source. Examples include the knee and geniculate arteries, shoulder and circumflex humeral, and hip and circumflex iliac.
Coronary artery anastomoses. The coronary arteries are functionally ended arteries, so these meetings are referred to as anatomical anastomosis, which lacks function. As blockage of one coronary artery generally results in the death of the heart tissue due to lack of sufficient blood supply from the other branch, when two arteries or their branches join, the area of the myocardium receives a dual blood supply. If one coronary artery is obstructed by an atheroma, a degradation of the arterial walls, the second artery is still able to supply oxygenated blood to the myocardium. However, this can only occur if the atheroma progresses slowly, giving the anastomosis time to form.
The Circle of Willis: Schematic representation of the circle of Willis—arteries of the brain and brain stem. Blood flows up to the brain through the vertebral arteries and through the internal carotid arteries.
Pathological anastomoses result from trauma or disease and are usually referred to as fistulae. They can be very severe if they result in the bypassing of key tissues by the circulatory system.
Arterioles
An arteriole is a small-diameter blood vessel in the microcirculation system that branches out from an artery and leads to capillaries.
Key Points
Arterioles have muscular walls and are the primary site of vascular resistance, which reduces the pressure and velocity of flow for gas and nutrient exchange to occur within the capillaries.
Arterioles are innervated and can also respond to other circulating factors to regulate their caliber.
Key Terms
microcirculation: The flow of blood through the smallest vessels: arterioles, capillaries, and venules.
arteriole: One of the small branches of an artery, especially one that connects with capillaries.
An arteriole is a small-diameter blood vessel that forms part of the microcirculation that extends from an artery and leads to capillaries.
Capillary: Arterioles are part of the microcirculation system, along with capillaries, arteries, veins, venules, and tissue cells.
Microcirculation involves the flow of blood in the smallest blood vessels, including arterioles, capillaries, and venules.
Arterioles have muscular walls that usually consist of one or two layers of smooth muscle. They are the primary site of vascular resistance. This reduces the pressure and velocity of blood flow to enable gas and nutrient exchange to occur within the capillaries. Arterioles are innervated and also respond to various circulating hormones and other factors such as pH in order to regulate their caliber, thus modulating the amount of blood flow into the capillary network and tissues.
Capillaries
Capillaries, the smallest blood vessels in the body, are part of microcirculation.
Key Points
Capillaries measure 5-10 μm in diameter and are only one cell thick.
Capillaries connect arterioles and venules and enable the exchange of water, oxygen, carbon dioxide, and many other nutrients and waste substances between the blood and surrounding tissues.
There are three main types of capillaries: continuous, fenestrated, and sinusoidal.
Key Terms
capillary: Any of the small blood vessels that connect arteries to veins.
microcirculation: The flow of blood through the smallest vessels such as arterioles, capillaries, and venules.
Capillaries, which form part of the micro-circulation, are the smallest of the body’s blood vessels at between 5-10
μm in diameter with the endothelial vessel wall of only one cell thick. They are surrounded by a thin basal lamina of connective tissue.
Structure of a capillary: Capillaries are of small diameter with the vessel wall being a single cell thick. Capillaries are surrounded by a thin basal lamina of connective tissue.
Capillary Function
Capillaries form a network through body tissues that connect arterioles and venules and facilitates the exchange of water, oxygen, carbon dioxide, and many other nutrients and waste substances between the blood and surrounding tissues.
The thin wall of the capillary and close association with its resident tissue allow for gas and lipophilic molecules to pass through without the need for special transport mechanisms. This allows bidirectional diffusion depending on osmotic gradients.
Formation of New Capillaries
During embryological development, new capillaries are formed by vasculogenesis, the process of blood vessel formation occurring by de novo production of endothelial cells and their formation into vascular tubes. The term angiogenesis denotes the formation of new capillaries from pre-existing blood vessels.
The Capillary Bed
Capillaries do not function independently. The capillary bed is an interwoven network of capillaries that supplies an organ. The more metabolically active the cells, the more capillaries required to supply nutrients and carry away waste products.
A capillary bed can consist of two types of vessels: true capillaries, which branch mainly from arterioles and provide exchange between cells and the circulation, and vascular shunts, short vessels that directly connect arterioles and venules at opposite ends of the bed, allowing for bypass.
Types of Capillaries
There are three main types of capillaries:
Continuous: Endothelial cells provide an uninterrupted lining, only allowing small molecules like water and ions to diffuse through tight junctions. This leaves gaps of unjoined membrane called intercellular clefts.
Fenestrated: Fenestrated capillaries have pores in the endothelial cells (60-80 nanometers in diameter) that are spanned by a diaphragm of radially oriented fibrils. They allow small molecules and limited amounts of protein to diffuse.
Sinusoidal: Sinusoidal capillaries are a special type of fenestrated capillaries that have larger openings (30–40 μm in diameter) in the endothelium. These types of blood vessels allow red and white blood cells (7.5μm–25μm diameter) and various serum proteins to pass using a process aided by a discontinuous basal lamina. Sinusoid blood vessels are primarily located in the bone marrow, lymph nodes, and adrenal gland. Some sinusoids are special in that they do not have tight junctions between cells. These are called discontinuous sinusoidal capillaries, present in the liver and spleen where the greater movement of cells and materials is necessary.
Control of Flow
Capillary beds may control blood flow via autoregulation. This allows an organ to maintain constant flow despite a change in central blood pressure. This is achieved by the myogenic response and by tubuloglomerular feedback in the kidney. When blood pressure increases, the arterioles that lead to the capillary bed are stretched and subsequently constrict to counteract the increased tendency for high pressure to increase blood flow. In the lungs, special mechanisms have been adapted to meet the needs of the increased necessity of blood flow during exercise. When heart rate increases and more blood must flow through the lungs, capillaries are recruited and are distended to make room for increased blood flow while resistance decreases.
Arteries make up a major part of the circulatory system, with the veins and heart being the other main components. Arteries make up tubelike structures that are responsible for the transportation of fluid (i.e., blood for the circulatory system and lymph for the lymphatic system) to and from every organ in the body. Mainly, arteries manage the transportation of oxygen, nutrients, and hormones through our bodies. Arteries can dispense fresh oxygen to the body after it gets loaded onto the Fe 2+ found in the center of hemoglobin. The oxygen binds to hemoglobin and is carried by the arteries to areas that are lacking oxygen. Through a shift in affinity for the oxygen, it is then unloaded to specific areas through high surface areas knowns as capillaries.[rx] Far from being a changeless structure, arteries adapt through signals received from the central nervous system, as they also react to an outer stimulus like pressure, temperature, and substances. Vascular nerves are responsible for innervating the arteries allowing them to change to their stimuli. As catecholamines get released into the blood, the nerves send signals to the arteries to either constrict or dilate, leading to changes in pressure.[rx]
Arteries are composed of smooth muscle allowing constriction and dilation through the parasympathetic nervous system.[rx] Arteries differ from veins in the sense that they most often are carrying oxygenated blood away from the heart and into the rest of the body system. This is not always the case; however, as the pulmonary artery moves unoxygenated blood from the heart to the lungs to complete the gas exchange in the alveoli.[rx] Arteries play a crucial role in maintaining homeostasis in the body. As individuals age, health issues begin presenting themselves in the form of stiffening or thicking of the arteries; however, many different issues develop with age and poor diet. Additionally, arteries begin to clog with a thicking of plaque known as atherosclerosis.[rx] As problems arise in the structure of the arteries, it begins leading to more strain on the heart, which develops congestive heart failure and which is often fatal. The arteries are vital to maintaining a healthy cardiovascular system, thus a healthy lifestyle.
Artery Function
Arteries are high-pressure blood vessels that carry oxygenated blood away from the heart to all other tissues and organs.
Key Points
Arteries are blood vessels that carry blood away from the heart. This blood is normally oxygenated, with the exception of blood in the pulmonary artery.
Arteries typically have a thicker tunica media than veins, containing more smooth muscle cells and elastic tissue. This allows for modulation of vessel caliber and thus control of blood pressure.
The arterial system is the higher-pressure portion of the circulatory system, with pressure varying between the peak pressure during heart contraction ( systolic pressure ) and the minimum (diastolic) pressure between contractions when the heart expands and refills.
The increase in arterial pressure during systole, or ventricular contraction, results in the pulse pressure, an indicator of cardiac function.
Key Terms
systolic pressure: The peak arterial pressure during heart contraction.
diastolic pressure: The minimum arterial pressure between contractions, when the heart expands and refills.
artery: An efferent blood vessel from the heart, conveying blood away from the heart regardless of oxygenation status.
Arteries are blood vessels that carry blood away from the heart under pressure. This blood is usually oxygenated, with the exception of that in the pulmonary artery, which carries deoxygenated blood to the lungs.
Arterial system: Simplified diagram of the human arterial system in anterior view.
As with veins, arteries are comprised of three layers: the tunicae intima, media, and external. In arteries, the tunica media, which contains smooth muscle cells and elastic tissue, is thicker than that of veins so it can modulate vessel caliber and thus control and maintain blood pressure.
Arterial pressure varies between the peak pressure during heart contraction, called the systolic pressure, and the minimum or diastolic pressure between contractions, when the heart expands and refills. This pressure variation within the artery produces the observable pulse that reflects heart activity. The pressure in the arterial system decreases steadily, highest in the aorta and lowest in the venous system, as blood approaches the heart after delivery of oxygen to tissues in the systemic circulation.
Arteries of the systemic circulation can be subdivided into muscular or elastic types according to the relative compositions of elastic and muscle tissue in their tunica media. Larger arteries are typically elastic and smaller arteries are more likely to be muscular. These arteries deliver blood to the arterioles, which in turn deliver blood to the capillary networks associated with the body’s tissues.
Elastic Arteries
An elastic or conducting artery has a large number of collagen and elastin filaments in the tunica media.
Key Points
Elastic arteries include the largest arteries in the body, those closest to the heart. They give rise to medium-sized vessels known as muscular or distributing, arteries.
Elastic arteries differ from muscular arteries both in size and in the relative amount of elastic tissue contained within the tunica media.
Arterial elasticity gives rise to the Windkessel effect, which helps to maintain relatively constant pressure in the arteries despite the pulsating nature of blood flow.
Key Terms
elastic arteries: An artery with a large number of collagen and elastin filaments, giving it the ability to stretch in response to each pulse.
tunica media: The middle layer of a vein wall with bands of thin smooth muscle.
Elastic arteries contain larger numbers of collagen and elastin filaments in their tunica media than muscular arteries do, giving them the ability to stretch in response to each pulse.
Elastic arteries include the largest arteries in the body, those closest to the heart, and give rise to the smaller muscular arteries. The pulmonary arteries, the aorta, and its branches together comprise the body’s system of elastic arteries. In these large arteries, the amount of elastic tissue is considerable and the smooth muscle fiber cells are arranged in 5 to 7 layers in both circular and longitudinal directions.
Anatomy of the Arterial Wall: Arterial wall layers including the tunica intima and the tunica media. Inelastic arteries, the tunica media is rich with elastic and connective tissue.
The aorta: The aorta makes up most of the elastic arteries in the body.
Arterial elasticity gives rise to the Windkessel effect, which through passive contraction after expansion helps to maintain relatively constant pressure in the arteries despite the pulsating nature of the blood flow from the heart.
The Aorta
Due to its position as the first part of the systemic circulatory system closest to the heart and the resultant high pressures it will experience, the aorta is perhaps the most elastic artery, featuring an incredibly thick tunica media-rich in elastic filaments. The aorta is so thick that it requires its own capillary network to supply it with sufficient oxygen and nutrients to function, the vasa vasorum.
When the left ventricle contracts to force blood into the aorta, the aorta expands. This stretching generates the potential energy that will help maintain blood pressure during diastole when the aorta contracts passively. Additionally, the elastic recoil helps conserve the energy from the pumping heart and smooth the flow of blood around the body through the Windkessel effect.
Muscular Arteries
Distributing arteries are medium-sized arteries that draw blood from an elastic artery and branch into resistance vessels.
Key Points
In contrast to the mechanism, elastic arteries use to store energy generated by the heart‘s contraction, distributing arteries contain layers of smooth muscle.
Key Terms
muscular arteries: Medium-sized arteries that draw blood from an elastic artery and branch into resistance vessels, including small arteries and arterioles.
elastic lamina: A layer of elastic tissue that forms the outermost part of the tunica intima of blood vessels. It is readily visualized with light microscopy in sections of muscular arteries.
arteriole: One of the small branches of an artery, especially one that connects with capillaries.
Splenic Artery: Transverse section of the human spleen showing the distribution of the splenic artery and its branches
Muscular or distributing arteries are medium-sized arteries that draw blood from an elastic artery and branch into resistance vessels, including small arteries and arterioles. In contrast to the mechanism elastic arteries use to store and dissipate the energy generated by the heart’s contraction, muscular arteries contain layers of smooth muscle providing allowing for involuntary control of vessel caliber and thus control of blood flow. Muscular arteries can be identified by the well-defined elastic lamina that lies between the tunica intima and media.
The splenic artery (lienal artery), the blood vessel that supplies oxygenated blood to the spleen, is an example of a muscular artery. It branches from the celiac artery and follows a course superior to the pancreas. The splenic artery branches off to the stomach and pancreas before reaching the spleen and gives rise to arterioles that directly supply capillaries of these organs.
Anastomoses
A circulatory anastomosis is a connection or looped interaction between two blood vessels.
Key Points
Anastomoses occur normally in the body in the circulatory system, serving as backup routes for blood flow if one link is blocked or otherwise compromised.
Anastomoses between arteries and between veins result in a multitude of arteries and veins, respectively, serving the same volume of tissue.
Pathological anastomoses result from trauma or disease and are referred to as fistulae.
Key Terms
circulatory anastomosis: A connection between two blood vessels, such as between arteries (arterio-arterial anastomosis), between veins (veno-venous anastomosis), or between an artery and a vein (arterio-venous anastomosis).
fistula: An abnormal connection or passageway between organs or vessels that normally do not connect.
An anastomosis refers to any joint between two vessels. Circulatory anastomoses are named based on the vessels they join: two arteries (arterio-arterial anastomosis), two veins (veno-venous anastomosis), or between an artery and a vein (arterio-venous anastomosis).
Anastomoses: The blood vessels of the rectum and anus, showing the distribution and anastomosis on the posterior surface near the termination of the gut.
Anastomoses between arteries and anastomoses between veins result in a multitude of arteries and veins serving the same volume of tissue. Such anastomoses occur normally in the body in the circulatory system, serving as backup routes for blood to flow if one link is blocked or otherwise compromised, but may also occur pathologically.
Examples of Anastomoses
Arterio-arterial anastomoses include actual joins (e.g. palmar arch, plantar arch) and potential ones, which may only function if the normal vessel is damaged or blocked (e.g. coronary arteries and cortical branch of cerebral arteries). Important examples include:
The circle of Willis in the brain.
The arrangement of the brain’s arteries into the circle of Willis creates redundancies for cerebral circulation. If one part of the circle becomes blocked or narrowed or one of the arteries supplying the circle is blocked or narrowed, blood flow from the other blood vessels can often preserve the cerebral perfusion well enough to maintain function.
Joint anastomoses. Almost all joints receive anastomotic blood supply from more than one source. Examples include the knee and geniculate arteries, shoulder and circumflex humeral, and hip and circumflex iliac.
Coronary artery anastomoses. The coronary arteries are functionally ended arteries, so these meetings are referred to as anatomical anastomosis, which lacks function. As blockage of one coronary artery generally results in the death of the heart tissue due to lack of sufficient blood supply from the other branch, when two arteries or their branches join, the area of the myocardium receives a dual blood supply. If one coronary artery is obstructed by an atheroma, a degradation of the arterial walls, the second artery is still able to supply oxygenated blood to the myocardium. However, this can only occur if the atheroma progresses slowly, giving the anastomosis time to form.
The Circle of Willis: Schematic representation of the circle of Willis—arteries of the brain and brain stem. Blood flows up to the brain through the vertebral arteries and through the internal carotid arteries.
Pathological anastomoses result from trauma or disease and are usually referred to as fistulae. They can be very severe if they result in the bypassing of key tissues by the circulatory system.
Arterioles
An arteriole is a small-diameter blood vessel in the microcirculation system that branches out from an artery and leads to capillaries.
Key Points
Arterioles have muscular walls and are the primary site of vascular resistance, which reduces the pressure and velocity of flow for gas and nutrient exchange to occur within the capillaries.
Arterioles are innervated and can also respond to other circulating factors to regulate their caliber.
Key Terms
microcirculation: The flow of blood through the smallest vessels: arterioles, capillaries, and venules.
arteriole: One of the small branches of an artery, especially one that connects with capillaries.
An arteriole is a small-diameter blood vessel that forms part of the microcirculation that extends from an artery and leads to capillaries.
Capillary: Arterioles are part of the microcirculation system, along with capillaries, arteries, veins, venules, and tissue cells.
Microcirculation involves the flow of blood in the smallest blood vessels, including arterioles, capillaries, and venules.
Arterioles have muscular walls that usually consist of one or two layers of smooth muscle. They are the primary site of vascular resistance. This reduces the pressure and velocity of blood flow to enable gas and nutrient exchange to occur within the capillaries. Arterioles are innervated and also respond to various circulating hormones and other factors such as pH in order to regulate their caliber, thus modulating the amount of blood flow into the capillary network and tissues.
Capillaries
Capillaries, the smallest blood vessels in the body, are part of microcirculation.
Key Points
Capillaries measure 5-10 μm in diameter and are only one cell thick.
Capillaries connect arterioles and venules and enable the exchange of water, oxygen, carbon dioxide, and many other nutrients and waste substances between the blood and surrounding tissues.
There are three main types of capillaries: continuous, fenestrated, and sinusoidal.
Key Terms
capillary: Any of the small blood vessels that connect arteries to veins.
microcirculation: The flow of blood through the smallest vessels such as arterioles, capillaries, and venules.
Capillaries, which form part of the micro-circulation, are the smallest of the body’s blood vessels at between 5-10
μm in diameter with the endothelial vessel wall of only one cell thick. They are surrounded by a thin basal lamina of connective tissue.
Structure of a capillary: Capillaries are of small diameter with the vessel wall being a single cell thick. Capillaries are surrounded by a thin basal lamina of connective tissue.
Capillary Function
Capillaries form a network through body tissues that connect arterioles and venules and facilitates the exchange of water, oxygen, carbon dioxide, and many other nutrients and waste substances between the blood and surrounding tissues.
The thin wall of the capillary and close association with its resident tissue allow for gas and lipophilic molecules to pass through without the need for special transport mechanisms. This allows bidirectional diffusion depending on osmotic gradients.
Formation of New Capillaries
During embryological development, new capillaries are formed by vasculogenesis, the process of blood vessel formation occurring by de novo production of endothelial cells and their formation into vascular tubes. The term angiogenesis denotes the formation of new capillaries from pre-existing blood vessels.
The Capillary Bed
Capillaries do not function independently. The capillary bed is an interwoven network of capillaries that supplies an organ. The more metabolically active the cells, the more capillaries required to supply nutrients and carry away waste products.
A capillary bed can consist of two types of vessels: true capillaries, which branch mainly from arterioles and provide exchange between cells and the circulation, and vascular shunts, short vessels that directly connect arterioles and venules at opposite ends of the bed, allowing for bypass.
Types of Capillaries
There are three main types of capillaries:
Continuous: Endothelial cells provide an uninterrupted lining, only allowing small molecules like water and ions to diffuse through tight junctions. This leaves gaps of unjoined membrane called intercellular clefts.
Fenestrated: Fenestrated capillaries have pores in the endothelial cells (60-80 nanometers in diameter) that are spanned by a diaphragm of radially oriented fibrils. They allow small molecules and limited amounts of protein to diffuse.
Sinusoidal: Sinusoidal capillaries are a special type of fenestrated capillaries that have larger openings (30–40 μm in diameter) in the endothelium. These types of blood vessels allow red and white blood cells (7.5μm–25μm diameter) and various serum proteins to pass using a process aided by a discontinuous basal lamina. Sinusoid blood vessels are primarily located in the bone marrow, lymph nodes, and adrenal gland. Some sinusoids are special in that they do not have tight junctions between cells. These are called discontinuous sinusoidal capillaries, present in the liver and spleen where the greater movement of cells and materials is necessary.
Control of Flow
Capillary beds may control blood flow via autoregulation. This allows an organ to maintain constant flow despite a change in central blood pressure. This is achieved by the myogenic response and by tubuloglomerular feedback in the kidney. When blood pressure increases, the arterioles that lead to the capillary bed are stretched and subsequently constrict to counteract the increased tendency for high pressure to increase blood flow. In the lungs, special mechanisms have been adapted to meet the needs of the increased necessity of blood flow during exercise. When heart rate increases and more blood must flow through the lungs, capillaries are recruited and are distended to make room for increased blood flow while resistance decreases.
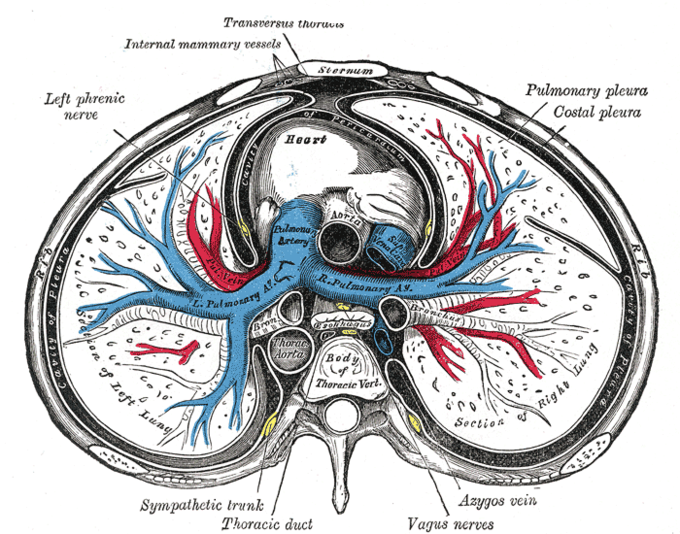
The heart is a muscular organ situated in the center of the chest behind the sternum. It consists of four chambers: the two upper chambers are called the right and left atria, and the two lower chambers are called the right and left ventricles. The right atrium and ventricle together are often called the right heart, and the left atrium and left ventricle together functionally form the left heart.[rx][rx][rx][rx]
The heart provides the body’s organs and tissues with a constant supply of blood – and with it vital oxygen and nutrients. You can think of the heart as a central pump that keeps the blood circulating around the body.
At rest, an adult heart beats about 60 to 80 times a minute. Each time the heart beats it pumps blood through the body. When we exert ourselves physically, our heart beats faster. This increases the speed at which blood flows through our body. The blood can then absorb more oxygen from the lungs per minute in order to supply the body’s cells with more oxygen.
Your heart is about the same size as your fist and weighs around 300 g (about 0.7 pounds). In people who do endurance sports, it can weigh up to 500 g (about 1.1 pounds). The heart is located more or less in the middle of the chest, slightly to the left, behind the breastbone (sternum). You can normally feel someone’s heart beat if you put your hand on their chest.
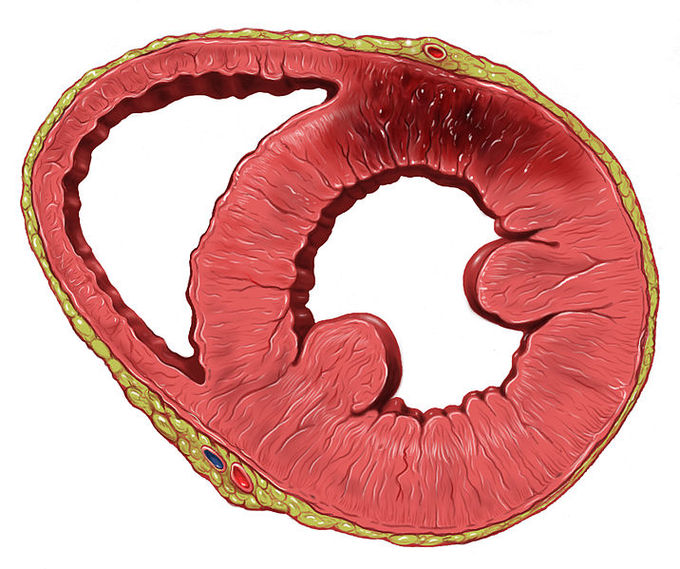
The heart is a hollow muscle. A wall through the middle (known as the septum) divides it into two halves. Each half has two chambers called the atrium and ventricle. The left ventricle pumps oxygen-rich blood out of the heart and into the body (systemic circulation) through an artery called the aorta. The first blood vessels that branch off from the aorta are the coronary arteries. They go straight to the muscle of the heart itself, and supply the heart with oxygen and nutrients.
The blood that has been “used” by the body – and is then low in oxygen – flows back to the heart. More specifically, it enters the right atrium and from there it flows into the right ventricle. The right ventricle pumps the low-oxygen blood into the pulmonary artery, which leads to the lungs (pulmonary circulation). In the lungs, the blood releases carbon dioxide and picks up oxygen. Then it flows back to the heart through the pulmonary veins – this time to the left side of the heart. From there, the blood is pumped back into the body.
There are 4 heart valves between the right atrium and right ventricle (Tricuspid valve), the left atrium and left ventricle (Mitral valve), and where the blood leaves the heart through the arteries (Pulmonary valve, Aortic valve). They ensure that the blood flows in the right direction and doesn’t flow back.
The flow of blood in the heart
Put simply, the valves of the heart function like one-way gates. Each valve is made up of a ring to which two or three flaps of tissue (called cusps or leaflets) are attached. The flaps are always somewhat curved – a bit like sails billowing in the wind. When the blood pushes against these flaps in the direction of the “wind,” they close the valve. When the blood pushes in the other direction, it is able to flow through the valve.
Electrical Events
Cardiac contraction is initiated in the excitable cells of the sinoatrial (SA) node by both spontaneous depolarization and sympathetic activity.
Key Points
The sinoatrial (SA) and atrioventricular (AV) nodes make up the intrinsic conduction system of the heart by setting the rate at which the heartbeats.
The SA node generates action potentials spontaneously.
The SA node fires at a normal rate of 60–100 beats per minute (bpm), and causes depolarization in atrial muscle tissue and subsequent atrial contraction.
The AV node slows the impulses from the SA node, firing at a normal rate of 40-60 bpm, and causes depolarization of the ventricular muscle tissue and ventricular contraction.
Sympathetic nervous stimulation increases the heart rate, while parasympathetic nervous stimulation decreases the heart rate.
Key Terms
pacemaker: A structure that sets the rate at which the heartbeats. Under normal conditions, the SA node serves this function for the heart.
atrioventricular (AV) node: The bundle of conducting tissue that receives impulses from the SA node and delays them before stimulating depolarization in the muscles of the ventricles.
The heart’s activity is dependent on the electrical impulses from the sinoatrial (SA) node and atrioventricular (AV) node, which form the intrinsic conduction system of the heart. The SA and AV nodes act as a pacemaker for the heart, determining the rate at which it beats, even without signals from the larger nervous system of the human body. The SA and AV nodes initiate the electrical impulses that cause contraction within the atria and ventricles of the heart.
Sinoatrial Node
The SA node is a bundle of nerve cells located on the outer layer of the right atria. These cells are specialized to undergo spontaneous depolarization and generation of action potentials without stimulation from the rest of the nervous system. The SA node nerve impulses travel through the atria and cause direct muscle cell depolarization and contraction of the atria. The SA node stimulates the right atria directly and stimulates the left atria through the Bachmann’s bundle. The SA node impulses also travel to the AV node, which stimulates ventricular contraction.
The SA node generates its own action potentials but may be influenced by the autonomic nervous system. Without autonomic nervous stimulation, the SA node will set the heart rate itself, acting as the primary pacemaker for the heart. The SA node fires to set a heart rate in a range of 60–100 beats per minute (bpm), a normal range that varies from person to person.
Atrioventricular Node
The AV node is a bundle of conducting tissue (not formally classified as nerve tissue) located at the junction between the atria and ventricles of the heart. The AV node receives action potentials from the SA node, and transmits them through the bundle of His, left and right bundle branches, and Purkinje fibers, which cause depolarization of ventricular muscle cells leading to ventricular contraction. The AV node slightly slows the neural impulse from the SA node, which causes a delay between depolarization of the atria and the ventricles.
The normal firing rate in the AV node is lower than that of the SA node because it slows the rate of neural impulses. Without autonomic nervous stimulation, it sets the rate of ventricular contraction at 40–60 bpm. Certain types of autonomic nervous stimulation alter the rate of firing in the AV node. Sympathetic nervous stimulation still increases heart rate, while parasympathetic nervous stimulation decreases heart rate by acting on the AV node.
The Cardiac Conduction System: The system of nerves that work together to set the heart rate and stimulate muscle cell depolarization within the heart.
Electrocardiogram and Correlation of ECG Waves with Systole
An electrocardiogram, or ECG, is a recording of the heart’s electrical activity as a graph over a period of time.
Key Points
An ECG is used to measure the rate and regularity of heartbeats as well as the size and position of the chambers, the presence of damage to the heart, and the effects of drugs or devices used to regulate the heart, such as a pacemaker.
The ECG device detects and amplifies the tiny electrical changes on the skin that are caused when the heart muscle depolarizes during each heartbeat, and then translates the electrical pulses of the heart into a graphic representation.
A typical ECG tracing of the cardiac cycle (heartbeat) consists of a P wave (atrial depolarization ), a QRS complex (ventricular depolarization), and a T wave (ventricular repolarization). An additional wave, the U wave ( Purkinje repolarization), is often visible, but not always.
The ST complex is usually elevated during a myocardial infarction.
Atrial fibrillation occurs when the P wave is missing and represents irregular, rapid, and inefficient atrial contraction, but is generally not fatal on its own.
Ventricular fibrillation occurs when all normal waves of an ECG are missing, represents rapid and irregular heartbeats, and will quickly cause sudden cardiac death.
Key Terms
fibrillation: A condition in which parts of the ECG do not appear normally, representing irregular, rapid, disorganized, and inefficient contractions of the atria or ventricles.
ST-segment: The line between the QRS complex and the T wave, representing the time when the ventricles are depolarized before repolarization begins.
An electrocardiogram (ECG or EKG) is a recording of the heart’s electrical activity as a graph over a period of time, as detected by electrodes attached to the outer surface of the skin and recorded by a device external to the body. The graph can show the heart’s rate and rhythm. It can also detect enlargement of the heart, decreased blood flow, or the presence of current or past heart attacks. ECGs are the primary clinical tool to measure the electrical and mechanical performance of the heart.
The ECG works by detecting and amplifying tiny electrical changes on the skin that occur during heart muscle depolarization. The output for the ECG forms a graph that shows several different waves, each corresponding to a different electrical and mechanical event within the heart. Changes in these waves are used to identify problems with the different phases of heart activity.
ECG: Illustration of a patient undergoing a 12-lead ECG.
The P Wave
Normal Systole ECG: The U wave is not visible in all ECGs.
The first wave on an ECG is the P wave, indicating atrial depolarization in which the atria contract (atrial systole ). The P wave is the first wave on the ECG because the action potential for the heart is generated in the sinoatrial (SA) node, located on the atria, which sends action potentials directly through Bachmann’s bundle to depolarize the atrial muscle cells.
Increased or decreased P waves can indicate problems with the potassium ion concentration in the body that will alter nerve activity. A missing P wave indicates atrial fibrillation, a cardiac arrhythmia in which the heart beats irregularly, preventing efficient ventricular diastole. This is generally not fatal on its own.
The QRS Complex
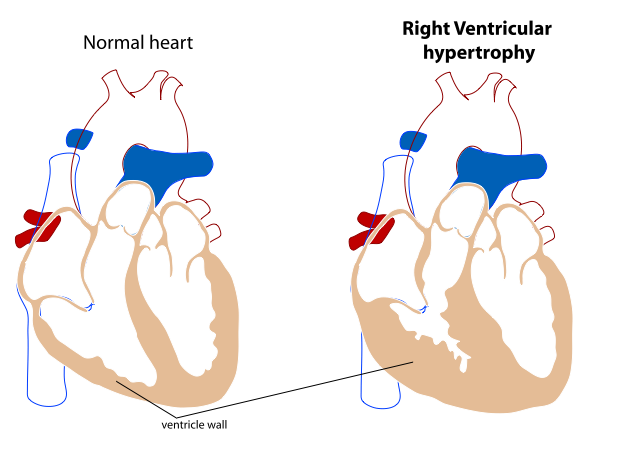
The QRS complex refers to the combination of the Q, R, and S waves, and indicates ventricular depolarization and contraction (ventricular systole). The Q and S waves are downward waves while the R wave, an upward wave, is the most prominent feature of an ECG. The QRS complex represents action potentials moving from the AV node, through the bundle of His and left and right branches and Purkinje fibers into the ventricular muscle tissue. Abnormalities in the QRS complex may indicate cardiac hypertrophy or myocardial infarctions.
The T Wave and ST Segment
Animation of a Normal ECG Wave: The red lines represent the movement of the electrical signal through the heart.
The T Wave indicates ventricular repolarization, in which the ventricles relax following depolarization and contraction. The ST segment refers to the gap (flat or slightly upcurved line) between the S wave and the T wave and represents the time between ventricular depolarization and repolarization. An elevated ST segment is the classic indicator for myocardial infarctions, though missing or downward-sloping ST segments may indicate myocardial ischemia.
Following the T wave is the U wave, which represents the repolarization of the Purkinje fibers. It is not always visible on an ECG because it is a very small wave in comparison to the others.
Ventricular Fibrillation
When ECG output shows no identifiable P waves, QRS complexes, or T waves, it indicates ventricular fibrillation, a severe arrhythmia. During ventricular fibrillation, the heart beats extremely fast and irregularly and can no longer pump blood, acting as a mass of quivering, disorganized muscle movements. Ventricular fibrillation will cause sudden cardiac death within minutes unless electrical resuscitation (with an AED) is performed immediately. It generally occurs with myocardial infractions and heart failure and is thought to be caused by action potentials that re-enter the AV nodes from the muscle tissue and induce rapid, irregular, weak contractions of the heart that fail to pump blood.
Heart Sounds
The two major heart sounds are “lub” (from the closure of AV valves) and “dub: (from the closure of aortic and pulmonary valves).
Key Points
The heart tone “lub,” or S1, is caused by the closure of the mitral and tricuspid atrioventricular (AV) valves at the beginning of ventricular systole.
The heart tone “dub,” or S2 ( a combination of A2 and P2), is caused by the closure of the aortic valve and pulmonary valve at the end of ventricular systole.
The splitting of the second heart tone, S2, into two distinct components, A2 and P2, can sometimes be heard in younger people during inspiration. During expiration, the interval between the two components shortens and the tones become merged.
Murmurs are a “whoosh” or “slosh” sound that indicates backflow through the valves.
S3 and S4 are “ta” sounds that indicate ventricles that are either too weak or too stiff to effectively pump blood.
Key Terms
dub: The second heart tone, or S2 (A2 and P2), caused by the closure of the aortic valve and pulmonary valve at the end of ventricular systole.
club: The first heart tone, or S1, caused by the closure of the atrioventricular valves (mitral and tricuspid) at the beginning of ventricular contraction or systole.
Heart murmurs A sound made by backflow of blood through either set of valve that cannot close or open properly.
The closing of the heart valves produces a sound. This sound may be described as either a “lub” or a “dub” sound. Heart sounds are a useful indicator for evaluating the health of the valves and the heart as a whole.
S1
The first heart sound, called S1, makes a “lub” sound caused by the closure of the mitral and tricuspid valves as ventricular systole begins. There is a very slight split between the closure of the mitral and tricuspid valves, but it is not long enough to create multiple sounds.
S2
The second heart sound, called S2, makes a “dub” sound caused by the closure of the semilunar (aortic and pulmonary) valves following ventricular systole. S2 is split because aortic valve closure occurs before pulmonary valve closure. During inspiration (breathing in) there is slightly increased blood return to the right side of the heart, which causes the pulmonary valve to stay open slightly longer than the aortic valve. Due to this, the naming convention is to divide the second sound into two-second sounds, A2 (aortic), and P2 (pulmonary). The time between A2 and P2 is variable depending on the respiratory rate, but the split is generally only prominent in children during inspiration. In adults and during expiration, the split is usually not long enough to suggest two sounds.
Abnormal Heart Sounds
Abnormal heart sounds may indicate problems with the health of the valves. Heart murmurs sound like a “whoosh” or “slosh” and indicate regurgitation or backflow of blood through the valves because they cannot close properly. Heart murmurs are common and generally not serious, but some may be more severe and/or caused by severe underlying problems within the heart. Murmurs may also be caused by valve stenosis (improper opening) and cardiac shunts, a severe condition in which a defect in the septum allows blood to flow between both sides of the heart.
Third and fourth heart sounds, S3 and S4, differ from S1 and S2 because they are caused by abnormal contraction and relaxation of the heart instead of the closure of valves and are more often indicative of more severe problems than are heart murmurs. S3 represents a flabby or weak ventricle that fills with more blood than it is able to pump, while S4 represents a stiff ventricle, such as those found in cardiac hypertrophy. S3 makes a “ta” sound after the “lub-dub” while S4 makes a “ta” sound before the “lub-dub.”
Opening and Closing of Heart Valves: The closing of the heart valves generates the “lub, dub” sounds that can be heard though a stethoscope.
Cardiac Cycle
The cardiac cycle describes the heart’s phases of contraction and relaxation that drive blood flow throughout the body.
Key Points
Every single beat of the heart involves three major stages: cardiac diastole, when chambers are relaxed and filling passively; atrial systole when the atria contract leading to ventricular filling; and ventricular systole when blood is ejected into both the pulmonary artery and aorta.
Pulse is a way of measuring heartbeat, based on the arterial distensions or pulses that occur as blood is pushed through the arteries.
Resting heart rate typically ranges from 60 to 100 bpm (beats per minute). Athletes often have significantly lower than average heart rates while the sedentary and obese typically have elevated heart rates.
Systolic blood pressure is the pressure during heart contraction, while diastolic blood pressure is the pressure during heart relaxation.
The normal range for blood pressure is between 90/60 mmHg and 120/80 mmHg.
Key Terms
cardiac cycle: The term used to describe the relaxation and contraction that occur as a heart works to pump blood through the body.
cardiac output: The volume of blood pumped by the heart each minute, calculated as heart rate (HR) X (times) stroke volume (SV).
pulse: Pressure waves generated by the heart in systole move the arterial walls, creating a palpable pressure wave felt by touch.
The cardiac cycle is the term used to describe the relaxation and contraction that occur as the heart works to pump blood through the body. Heart rate is a term used to describe the frequency of the cardiac cycle. It is considered one of the four vital signs and is a regulated variable. Usually, heart rate is calculated as the number of contractions (heartbeats) of the heart in one minute and expressed as “beats per minute” (bpm). When resting, the adult human heart beats at about 70 bpm (males) and 75 bpm (females), but this varies among individuals. The reference range is normally between 60 bpm (lower is termed bradycardia) and 100 bpm (higher is termed tachycardia). Resting heart rates can be significantly lower in athletes and significantly higher in the obese. The body can increase the heart rate in response to a wide variety of conditions in order to increase the cardiac output, the blood ejected by the heart, which improves oxygen supply to the tissues.
Pulse
Pressure waves generated by the heart in systole, or ventricular contraction, move the highly elastic arterial walls. Forward movement of blood occurs when the arterial wall boundaries are pliable and compliant. These properties allow the arterial wall to distend when pressure increases, resulting in a pulse that can be detected by touch. Exercise, environmental stress, or psychological stress can cause the heart rate to increase above the resting rate. The pulse is the most straightforward way of measuring the heart rate, but it can be a crude and inaccurate measurement when cardiac output is low. In these cases (as happens in some arrhythmias), there is little pressure change and no corresponding change in pulse, and the heart rate may be considerably higher than the measured pulse.
Cardiac Cycle
Every single heartbeat includes three major stages: atrial systole, ventricular systole, and complete cardiac diastole.
Atrial systole is the contraction of the atria that causes ventricular filling.
Ventricular systole is the contraction of the ventricles in which blood is ejected into the pulmonary artery or aorta, depending on side.
Complete cardiac diastole occurs after systole. The blood chambers of the heart relax and fill with blood once more, continuing the cycle.
Systolic and Diastolic Blood Pressure
Throughout the cardiac cycle, the arterial blood pressure increases during the phases of active ventricular contraction and decreases during ventricular filling and atrial systole. Thus, there are two types of measurable blood pressure: systolic during contraction and diastolic during relaxation. Systolic blood pressure is always higher than diastolic blood pressure, generally presented as a ratio in which systolic blood pressure is over diastolic blood pressure. For example, 115/75 mmHg would indicate a systolic blood pressure of 115 mmHg and diastolic blood pressure or 75 mmHg. The normal range for blood pressure is between 90/60 mmHg and 120/80 mmHg. Pressures higher than that range may indicate hypertension, while lower pressures may indicate hypotension. Blood pressure is a regulated variable that is directly related to blood volume, based on cardiac output during the cardiac cycle.
The Cardiac Cycle: Changes in contractility lead to pressure differences in the heart’s chambers that drive the movement of blood.
Contractile Myofilament
The structure of the smooth muscle actomyosin array is similar to striated muscle with several important differences:
there is no troponin complex in smooth muscle
contraction is regulated by Ca2+ calmodulin-dependent myosin light chain kinase (MLCK) mediated phosphorylation of the regulatory light chains of myosin, which enables actin-myosin interaction and cross-bridge cycling
in the absence of Ca2+ and calmodulin (CaM), caldesmon interacts with actomyosin inhibiting the activity of myosin ATPase
the activity of myosin light chain phosphatase (MLCP) directly causes the dephosphorylation of myosin LC20 leading to the relaxation
the actin: myosin ratio is higher in smooth muscle averaging 15:1 in vascular smooth muscle in comparison to 6:1 in skeletal or cardiac muscle. There are no intercalated disks or z-disks, however, dense bodies in smooth muscle are thought to be analogous to z-disks
Cardiac Output
Cardiac output (Q or CO) is the volume of blood pumped by the heart, in particular by the left or right ventricle, in one minute.
Key Points
Cardiac output, a measure of how much blood the heart pumps over the course of a minute, is calculated by multiplying heart rate by stroke volume.
The heart rate is increased by sympathetic nervous stimulation and decreased by parasympathetic nervous stimulation.
Stroke volume is end-diastolic volume (venous return) minus end-systolic volume, the amount of blood left over in the heart after systole.
The ejection fraction is stroke volume divided by end-diastolic volume.
Mean arterial blood pressure is cardiac output multiplied by total peripheral resistance. A twofold change in vascular size will cause a 16-fold change in resistance in the opposite direction.
Starling’s mechanism states that changes in venous return (preload) to the heart will change cardiac output, which will also change mean arterial blood pressure in the same direction. This means that blood volume and blood pressure are directly related to one another.
Key Terms
mean arterial blood pressure: A measure of blood pressure based on cardiac output and vascular resistance.
cardiac output: The volume of blood pumped by the heart, in particular by the left or right ventricle, in the time interval of one minute.
Cardiac output (CO) is a measure of the heart’s performance. While there are many clinical techniques to measure CO, it is best described as a physiological and mathematical relationship between different variables. When one of the variables changes, CO as a whole will change as a result. This can also be used to predict other regulated variables, such as blood pressure and blood volume. The mathematical description of CO is that CO=Heart Rate (HR)×Stroke Volume (SV)CO=Heart Rate (HR)×Stroke Volume (SV). Changes in HR, SV, or their components, will change CO.
Heart Rate
The heart rate is determined by spontaneous action potential generation in the sinoatrial (SA) node and conduction in the atrioventricular (AV) node. It refers to the number of heartbeats over the course of a minute. Sympathetic nervous system activation will stimulate the SA and AV nodes to increase the heart rate, which will increase cardiac output. Parasympathetic nervous system activation will conversely act on the SA and AV nodes to decrease the heart rate, which will decrease cardiac output. For the SA node, the rate of depolarization is altered, while the AV node’s rate of conduction is altered by autonomic nerve stimulation.
Stroke Volume
Stroke volume refers to the amount of blood ejected from the heart during a single beat. It is a measure of the contractility of the heart based on end-diastolic volume (EDV), mathematically described as SV=EDV−ESV (end systolic volumeSV=EDV−ESV (end-systolic volume. EDV is the volume of blood in the ventricles at the end of diastole, while ESV is the volume of blood left inside the ventricles at the end of systole, making SV the difference between EDV and ESV. Contractility of the heart refers to the variability in how much blood the heart ejects based on changes in stroke volume rather than changes in heart rate.
Additionally, another indicator known as the ejection fraction (EF) is used to evaluate stroke volume and contractility. It is described as EF=(SVEDV)×100%EF=(SVEDV)×100%and is a measure of the proportion of blood ejected during systole compared to the amount of blood that was present in the heart. A higher EF suggests more efficient heart activity.
Mean Arterial Pressure
Cardiac output is an indicator of mean arterial blood pressure (MAP), the average measure of blood pressure within the body. It is described as MAP=CO×TPR (total peripheral resistance)MAP=CO×TPR (total peripheral resistance). TPR is a measure of resistance in the blood vessels, which acts as the force by which blood must overcome to flow through the arteries determined by the diameter of the blood vessels. The exact relationship is such that a twofold increase in blood vessel diameter (doubling the diameter) would decrease resistance by 16-fold, and the opposite is true as well. When CO increases, MAP will increase, but if CO decreases, MAP will decrease.
Starling’s Law of the Heart
Frank Starling’s Law: This chart indicates stroke volume compared to ventricular preload, with labels for preload dependent zone, responsive patient SVV > 10%, and nonresponsive patient SVV < 10 %.
CO can also predict blood pressure based on blood volume. Starling’s law of the heart states that the SV of the heart increases in response to an increase in EDV when all other factors remain constant. Essentially, this means that higher venous blood return to the heart (also called the preload) will increase SV, which will in turn increase CO. This is because sarcomeres are stretched further when EDV increases, allowing the heart to eject more blood and keep the same ESV if no other factors change.
The main implication of this law is that increases in blood volume or blood return to the heart will increase cardiac output, which will lead to an increase in MAP. The opposite scenario is true as well. For example, a dehydrated person will have a low blood volume and lower venous return to the heart, which will decrease cardiac output and blood pressure. Those that stand up quickly after lying down may feel light-headed because their venous return to the heart is momentarily impaired by gravity, temporarily decreasing blood pressure and supply to the brain. The adjustment for blood pressure is a quick process, while blood volume is slowly altered. Blood volume itself is another regulated variable, regulated slowly through complex processes in the renal system that alter blood pressure based on the Starling mechanism.
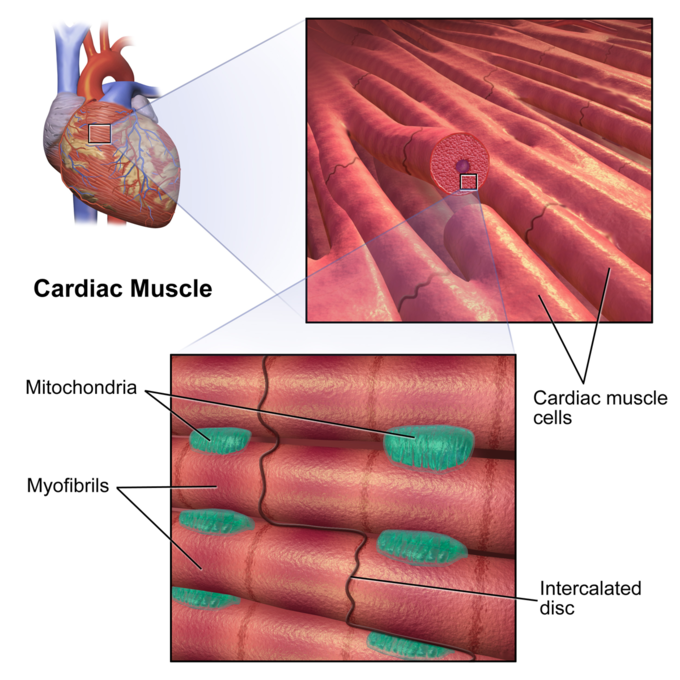
What is cardiac muscle?
Cardiac muscle tissue is one of the three types of muscle tissue in your body. The other two types are skeletal muscle tissue and smooth muscle tissue. Cardiac muscle tissue is only found in your heart, where it performs coordinated contractions that allow your heart to pump blood through your circulatory system.
Keep reading to learn more about the function and structure of cardiac muscle tissue, as well as conditions that affect this type of muscle tissue.
How does it function?
Cardiac muscle tissue works to keep your heart pumping through involuntary movements. This is one feature that differentiates it from skeletal muscle tissue, which you can control.
It does this through specialized cells called pacemaker cells. These control the contractions of your heart. Your nervous system sends signals to pacemaker cells that prompt them to either speed up or slow down your heart rate.
Your pacemaker cells are connected to other cardiac muscle cells, allowing them to pass along signals. This results in a wave of contractions of your cardiac muscle, which creates your heartbeat.
What does cardiac muscle tissue look like when it moves?
Use this interactive 3-D diagram to explore the movement of cardiac muscle tissue
What are heart muscles made of?
Intercalated discs
Intercalated discs are small connections that join cardiac muscle cells (cardiomyocytes) to each other.
Gap junctions
Gap junctions are part of the intercalated discs. When one cardiac muscle cell is stimulated to contract, a gap junction transfers the stimulation to the next cardiac cell. This allows the muscle to contract in a coordinated way.
Desmosomes
Like gap junctions, desmosomes are also found within intercalated discs. They help hold the cardiac muscle fibers together during a contraction.
Nucleus
The nucleus is the “control center” of a cell. It contains all of the cell’s genetic material. While skeletal muscle cells can have multiple nuclei, cardiac muscle cells typically only have one nucleus.
What is cardiomyopathy?
Cardiomyopathy is one of the main conditions that can affect your cardiac muscle tissue. It’s a disease that makes it harder for your heart to pump blood.
There are several different types of cardiomyopathy:
Hypertrophic cardiomyopathy. The cardiac muscles enlarge and thicken for no apparent reason. It’s usually found in the lower chambers of the heart, called the ventricles.
Dilated cardiomyopathy. The ventricles become larger and weaker. This makes it hard for them to pump, which makes the rest of your heart work harder to pump blood.
Restrictive cardiomyopathy. The ventricles become stiff, which prevents them from filling to their full volume.
Arrhythmogenic right ventricular dysplasia. The cardiac muscle tissue of your right ventricle is replaced with fatty or fiber-rich tissue. This can lead to arrhythmia, which refers to an abnormal heart rate or rhythm.
Not all cases of cardiomyopathy produce symptoms. However, it can sometimes cause:
trouble breathing, especially when exercising
fatigue
swollen ankles, feet, legs, abdomen, or neck veins
It’s usually hard to pinpoint the cause of cardiomyopathy. But several things can increase your risk of developing it, including:
a family history of cardiomyopathy or heart failure
high blood pressure
obesity
heavy alcohol consumption
use of certain recreational drugs
past heart attacks or heart infections
How does exercise impact cardiac muscle tissue?
As with many other muscles in your body, exercise can strengthen your cardiac muscle. Exercise can also help reduce your risk of developing cardiomyopathy and make your heart work more efficiently.
The American Heart Association recommends at least 150 minutes of moderate exercise per week. To reach this goal, try to get about 30 minutes of exercise five days a week.
As for the type of exercise, cardio workouts are named for their cardiac muscle benefits. Regular cardio exercise can help lower your blood pressure, reduce your heart rate, and make your heart pump more effectively. Common types of cardio exercises include walking, running, biking, and swimming.
If you already have a heart condition, make sure to talk to your doctor before starting any kind of exercise program. You might need to take some precautions to avoid putting too much stress on your heart.
The bottom line
Cardiac muscle tissue is one of the three types of muscle in your body. It’s only found in your heart, where it’s involved in coordinated contractions that keep your heart beating. To keep your cardiac muscle working efficiently and to reduce your risk of cardiac conditions — including cardiomyopathy — try to get in some sort of exercise more days of the week than not.
How Your Heart Works
Your heart
The human heart is one of the hardest-working organs in the body.
On average, it beats around 75 times a minute. As the heartbeats, it provides pressure so blood can flow to deliver oxygen and important nutrients to tissue all over your body through an extensive network of arteries, and it has return blood flow through a network of veins.
In fact, the heart steadily pumps an average of 2,000 gallons of blood through the body each day.
Your heart is located underneath your sternum and ribcage, and between your two lungs.
The heart’s chambers
The heart’s four chambers function as a double-sided pump, with an upper and continuous lower chamber on each side of the heart.
The heart’s four chambers are:
Right atrium. This chamber receives venous oxygen-depleted blood that has already circulated around through the body, not including the lungs, and pumps it into the right ventricle.
Right ventricle. The right ventricle pumps blood from the right atrium to the pulmonary artery. The pulmonary artery sends the deoxygenated blood to the lungs, where it picks up oxygen in exchange for carbon dioxide.
Left atrium. This chamber receives oxygenated blood from the pulmonary veins of the lungs and pumps it to the left ventricle.
Left ventricle. With the thickest muscle mass of all the chambers, the left ventricle is the hardest pumping part of the heart, as it pumps blood that flows to the heart and the rest of the body other than the lungs.
The heart’s two atria are both located on the top of the heart. They are responsible for receiving blood from your veins.
The heart’s two ventricles are located at the bottom of the heart. They are responsible for pumping blood into your arteries.
Your atria and ventricles contract to make your heartbeat and to pump the blood through each chamber. Your heart chambers fill up with blood before each beat, and the contraction pushes the blood out into the next chamber. The contractions are triggered by electrical pulses that start from the sinus node, also called the sinoatrial node (SA node), located in the tissue of your right atrium.
The pulses then travel through your heart to the atrioventricular node, also called the AV node, located near the center of the heart between the atria and the ventricles. These electrical impulses keep your blood flowing in proper rhythm.
The heart’s valves
The heart has four valves, one each at the downstream end of each chamber, so that, under normal conditions, blood can’t flow backward, and the chambers can fill with blood and pump blood forward properly. These valves can sometimes be repaired or replaced if they become damaged.
The heart’s valves are:
Tricuspid (right AV) valve. This valve opens to allow blood to flow from the right atrium to the right ventricle.
Pulmonary valve. This valve opens to allow blood to flow from the left ventricle into the pulmonary artery to the lungs so that the heart and rest of the body can receive more oxygen.
Mitral (left AV) valve. This valve opens to let blood flow from the left atrium to the left ventricle.
Aortic valve. This valve opens to let blood leave the left ventricle so that the blood can flow to the heart and the rest of the body, save the lungs.
Blood flow through the heart
When working properly, deoxygenated blood coming back from organs, other than the lungs, enters the heart through two major veins known as the vena cavae, and the heart returns its venous blood back to itself through the coronary sinus.
From these venous structures, the blood enters the right atrium and passes through the tricuspid valve into the right ventricle. The blood then flows through the pulmonary valve into the pulmonary artery trunk, and next travels through the right and left pulmonary arteries to the lungs, where the blood receives oxygen during air exchange.
On its way back from the lungs, the oxygenated blood travels through the right and left pulmonary veins into the left atrium of the heart. The blood then flows through the mitral valve into the left ventricle, the heart’s powerhouse chamber.
The blood travels out the left ventricle through the aortic valve, and into the aorta, extending upward from the heart. From there, the blood moves through a maze of arteries to get to every cell in the body other than the lungs.
The heart’s crown
The structure of the heart’s blood supply is called the coronary circulatory system. The word “coronary” comes from the Latin word meaning “of a crown.” The arteries that fuel the heart’s muscle encircle the heart like a crown.
Coronary heart disease, also called coronary artery disease, typically develops when calcium-containing cholesterol and fat plaques collect in and hurt the arteries that feed the heart muscle. If a portion of one of these plaques ruptures, it can suddenly block one of the vessels and cause the heart muscle to begin to die (myocardial infarction) because it’s starved for oxygen and nutrients. This can also occur if a blood clot forms in one of the arteries of the heart, which can happen right after a plaque rupture.
Fun Facts About the Heart You Didn’t Know
How the heart works
The heart is part of your body’s circulatory system. It’s made up of the atria, ventricles, valves, and various arteries and veins. The main function of your heart is to keep blood that’s full of oxygen circulating throughout your body. Because your heart is crucial to your survival, it’s important to keep it healthy with a well-balanced diet and exercise, and avoid things that can damage it, like smoking.
While you’re probably familiar with a few heart-healthy tips, there are some fun facts about the heart that you may not know.
24 fun facts about the heart
The average heart is the size of a fist in an adult.
Your heart will beat about 115,000 times each day.
Your heart pumps about 2,000 gallons of blood every day.
An electrical system controls the rhythm of your heart. It’s called the cardiac conduction system.
The heart can continue beating even when it’s disconnected from the body.
The first open-heart surgery occurred in 1893. It was performed by Daniel Hale Williams, who was one of the few black cardiologists in the United States at the time.
The first implantable pacemaker was used in 1958. Arne Larsson, who received the pacemaker, lived longer than the surgeon who implanted it. Larsson died at 86 of a disease that was unrelated to his heart.
The youngest person to receive heart surgery was only a minute old. She had a heart defect that many babies don’t survive. Her surgery was successful, but she’ll eventually need a heart transplant.
The earliest known case of heart disease was identified in the remains of a 3,500-year-old Egyptian mummy.
The fairy fly, which is a kind of wasp, has the smallest heart of any living creature.
The American pygmy shrew is the smallest mammal, but it has the fastest heartbeat at 1,200 beats per minute.
Whales have the largest heart of any mammal.
The giraffe has a lopsided heart, with their left ventricle being thicker than the right. This is because the left side has to get blood up the giraffe’s long neck to reach their brain.
Most heart attacks happen on a Monday.
Christmas day is the most common day of the year for heart attacks to happen.
The human heart weighs less than 1 pound. However, a man’s heart, on average, is 2 ounces heavier than a woman’s heart.
A woman’s heart beats slightly faster than a man’s heart.
The beating sound of your heart is caused by the valves of the heart opening and closing.
It’s possible to have a broken heart. It’s called broken heart syndrome and can have similar symptoms as a heart attack. The difference is that a heart attack is from heart disease and broken heart syndrome is caused by a rush of stress hormones from an emotional or physical stress event.
Death from a broken heart, or broken heart syndrome, is possible but extremely rare.
The iconic heart shape as a symbol of love is traditionally thought to come from the silphium plant, which was used as an ancient form of birth control.
If you were to stretch out your blood vessel system, it would extend over 60,000 miles.
Heart cells stop dividing, which means heart cancer is extremely rare.
Laughing is good for your heart. It reduces stress and gives a boost to your immune system.
The takeaway
Your heart affects every part of your body. That also means that diet, lifestyle, and your emotional well-being can affect your heart. Emotional and physical health are both important for maintaining a healthy heart.
28 Healthy Heart Tips
Stop smoking—no ifs, ands, or butts
There are many steps you can take to help protect your health and blood vessels. Avoiding tobacco is one of the best.
In fact, smoking is one of the top controllable risk factors for heart disease. If you smoke or use other tobacco products, the American Heart Association (AHA), National Heart, Lung, and Blood InstituteTrusted Source (NHLBI), and Centers for Disease Control and PreventionTrusted Source (CDC) all encourage you to quit. It can make a huge difference to not just your heart, but your overall health, too.
Focus on the middle
That is, focus on your middle. Research in the Journal of the American College of Cardiology has linked excess belly fat to higher blood pressure and unhealthy blood lipid levels. If you’re carrying extra fat around your middle, it’s time to slim down. Eating fewer calories and exercising more can make a big difference.
Play between the sheets
Or you can play on top of the sheets! That’s right, having sex can be good for your heart. Sexual activity may add more than just pleasure to your life. It may also help lower your blood pressure and risk of heart disease. Research published in the American Journal of CardiologyTrusted Source shows that a lower frequency of sexual activity is associated with higher rates of cardiovascular disease.
Knit a scarf
Put your hands to work to help your mind unwind. Engaging in activities such as knitting, sewing, and crocheting can help relieve stress and do your ticker some good. Other relaxing hobbies, such as woodworking, cooking, or completing jigsaw puzzles, may also help take the edge off stressful days.
Power up your salsa with beans
When paired with low-fat chips or fresh veggies, salsa offers a delicious and antioxidant-rich snack. Consider mixing in a can of black beans for an added boost of heart-healthy fiber. According to the Mayo Clinic, a diet rich in soluble fiber can help lower your level of low-density lipoprotein, or “bad cholesterol.” Other rich sources of soluble fiber include oats, barley, apples, pears, and avocados.
Let the music move you
Whether you prefer a rumba beat or two-step tune, dancing makes for a great heart-healthy workout. Like other forms of aerobic exercise, it raises your heart rate and gets your lungs pumping. It also burns up to 200 calories or more per hour, reports the Mayo Clinic.
Go fish
Eating a diet rich in omega-3 fatty acids can also help ward off heart disease. Many fish, such as salmon, tuna, sardines, and herring, are rich sources of omega-3 fatty acids. Try to eat fish at least twice a week, suggests the AHA. If you’re concerned about mercury or other contaminants in fish, you may be happy to learn that its heart-healthy benefits tend to outweigh the risks for most people.
Laugh out loud
Don’t just LOL in emails or Facebook posts. Laugh out loud in your daily life. Whether you like watching funny movies or cracking jokes with your friends, laughter may be good for your heart. According to the AHA, research suggests laughing can lower stress hormones, decrease inflammation in your arteries, and raise your levels of high-density lipoprotein (HLD), also known as “good cholesterol.”
Stretch it out
Yoga can help you improve your balance, flexibility, and strength. It can help you relax and relieve stress. As if that’s not enough, yoga also has the potential to improve heart health. According to research published in the Journal of Evidence-Based Complementary & Alternative MedicineTrusted Source, yoga demonstrates the potential to reduce your risk of cardiovascular disease.
Raise a glass
Moderate consumption of alcohol can help raise your levels of HDL or good cholesterol. It can also help prevent blood clot formation and artery damage. According to the Mayo Clinic, red wine, in particular, may offer benefits for your heart. That doesn’t mean you should guzzle it at every meal. The key is to only drink alcohol in moderation.
Sidestep salt
If the entire U.S. population reduced its average salt intake to just half a teaspoon a day, it would significantly cut the number of people who develop coronary heart disease every year, report researchers in the New England Journal of Medicine. The authors suggest that salt is one of the leading drivers of rising healthcare costs in the United States. Processed and restaurant-prepared foods tend to be especially high in salt. So think twice before filling up on your favorite fast-food fix. Consider using a salt substitute, such as Dash, if you have high blood pressure or heart failure.
Move it, move it, move it
No matter how much you weigh, sitting for long periods of time could shorten your lifespan, warn researchers in the Archives of Internal Medicine and the American Heart AssociationTrusted Source. Couch potato and desk jockey lifestyles seem to have an unhealthy effect on blood fats and blood sugar. If you work at a desk, remember to take regular breaks to move around. Go for a stroll on your lunch break, and enjoy regular exercise in your leisure time.
Know your numbers
Keeping your blood pressure, blood sugar, cholesterol, and triglycerides in check is important for good heart health. Learn the optimal levels for your sex and age group. Take steps to reach and maintain those levels. And remember to schedule regular check-ups with your doctor. If you want to make your doctor happy, keep good records of your vitals or lab numbers, and bring them to your appointments.
Eat chocolate
Dark chocolate not only tastes delicious, it also contains heart-healthy flavonoids. These compounds help reduce inflammation and lower your risk of heart disease, suggest scientists in the journal Nutrients. Eaten in moderation, dark chocolate — not oversweetened milk chocolate — can actually be good for you. The next time you want to indulge your sweet tooth, sink it into a square or two of dark chocolate. No guilt required.
Kick your housework up a notch
Vacuuming or mopping the floors may not be as invigorating as a Body Slam or Zumba class. But these activities and other household chores do get you moving. They can give your heart a little workout while burning calories too. Put your favorite music on and add some pep to your step while you complete your weekly chores.
Go nuts
Almonds, walnuts, pecans, and other tree nuts deliver a powerful punch of heart-healthy fats, protein, and fiber. Including them in your diet can help lower your risk of cardiovascular disease. Remember to keep the serving size small, suggests the AHA. While nuts are full of healthy stuff, they’re also high in calories.
Be a kid
Fitness doesn’t have to be boring. Let your inner child take the lead by enjoying an evening of roller skating, bowling, or laser tag. You can have fun while burning calories and giving your heart a workout.
Consider pet therapy
Our pets offer more than good company and unconditional love. They also provide numerous health benefits. Studies reported by the National Institutes of Health (NIH) suggest that owning a pet may help improve your heart and lung function. It may also help lower your chances of dying from heart disease.
Start and stop
Start and stop, then start and stop again. During interval training, you alternate bursts of intense physical activity with bouts of lighter activity. The Mayo Clinic reports that doing so can boost the number of calories you burn while working out.
Cut the fat
Slicing your saturated fat intake to no more than 7 percent of your daily calories can cut your risk of heart disease, advises the USDA. If you don’t normally read nutrition labels, considering starting today. Take stock of what you’re eating and avoid foods that are high in saturated fat.
Take the scenic route home
Put down your cell phone, forget about the driver who cut you off, and enjoy your ride. Eliminating stress while driving can help lower your blood pressure and stress levels. That’s something your cardiovascular system will appreciate.
Make time for breakfast
The first meal of the day is an important one. Eating a nutritious breakfast every day can help you maintain a healthy diet and weight. To build a heart-healthy meal, reach for:
whole grains, such as oatmeal, whole-grain cereals, or whole-wheat toast
lean protein sources, such as turkey bacon or a small serving of nuts or peanut butter
low-fat dairy products, such as low-fat milk, yogurt, or cheese
fruits and vegetables
Take the stairs
Exercise is essential for good heart health, so why not sneak it in at every opportunity? Take the stairs instead of the elevator. Park on the far side of the parking lot. Walk to a colleague’s desk to talk, instead of emailing them. Play with your dog or kids at the park, instead of just watching them. Every little bit adds up to better fitness.
Brew up a heart-healthy potion
No magic is needed to brew up a cup of green or black tea. Drinking one to three cups of tea per day may help lower your risk of heart problems, reports the AHA. For example, it’s linked to lower rates of angina and heart attacks.
Brush your teeth regularly
Good oral hygiene does more than keep your teeth white and glistening. According to the Cleveland Clinic, some research suggests that the bacteria that cause gum disease can also raise your risk of heart disease. While the research findings have been mixed, there’s no downside to taking good care of your teeth and gums.
Walk it off
The next time you feel overwhelmed, exasperated, or angry, take a stroll. Even a five-minute walk can help clear your head and lower your stress levels, which is good for your health. Taking a half-hour walk every day is even better for your physical and mental health.
Pump some iron
Aerobic fitness is key to keeping your heart healthy, but it’s not the only type of exercise you should do. It’s also important to include regular strength training sessions in your schedule. The more muscle mass you build, the more calories you burn. That can help you maintain a heart-healthy weight and fitness level.
Find your happy place
A sunny outlook may be good for your heart, as well as your mood. According to the Harvard T. H. Chan School of Public Health, chronic stress, anxiety, and anger can raise your risk of heart disease and stroke. Maintaining a positive outlook on life may help you stay healthier for longer.
Cardiomyopathy
What is cardiomyopathy?
Cardiomyopathy is a progressive disease of the myocardium or heart muscle. In most cases, the heart muscle weakens and is unable to pump blood to the rest of the body as well as it should. There are many different types of cardiomyopathy caused by a range of factors, from coronary heart disease to certain drugs. These can all lead to an irregular heartbeat, heart failure, a heart valve problem, or other complications.
Medical treatment and follow-up care are important. They can help prevent heart failure or other complications.
What are the types of cardiomyopathy?
Cardiomyopathy generally has four types.
Dilated cardiomyopathy
The most common form, dilated cardiomyopathy (DCM), occurs when your heart muscle is too weak to pump blood efficiently. The muscles stretch and become thinner. This allows the chambers of your heart to expand.
This is also known as an enlarged heart. You can inherit it, or it can be due to coronary artery disease.
Hypertrophic cardiomyopathy
Hypertrophic cardiomyopathy is believed to be genetic. It occurs when your heart walls thicken and prevent blood from flowing through your heart. It’s a fairly common type of cardiomyopathy. It can also be caused by long-term high blood pressure or aging. Diabetes or thyroid disease can also cause hypertrophic cardiomyopathy. There are other instances that the cause is unknown.
Arrhythmogenic right ventricular dysplasia (ARVD)
Arrhythmogenic right ventricular dysplasia (ARVD) is a very rare form of cardiomyopathy, but it’s the leading cause of sudden death in young athletes. In this type of genetic cardiomyopathy, fat and extra fibrous tissue replace the muscle of the right ventricle. This causes abnormal heart rhythms.
Restrictive cardiomyopathy
Restrictive cardiomyopathy is the least common form. It occurs when the ventricles stiffen and can’t relax enough to fill up with blood. Scarring of the heart, which frequently occurs after a heart transplant, may be a cause. It can also occur as a result of heart disease.
Other types
Most of the following types of cardiomyopathy belong to one of the previous four classifications, but each has unique causes or complications.
Peripartum cardiomyopathy occurs during or after pregnancy. This rare type occurs when the heart weakens within five months of delivery or within the final month of pregnancy. When it occurs after delivery, it’s sometimes called postpartum cardiomyopathy. This is a form of dilated cardiomyopathy, and it’s a life-threatening condition. There’s no cause.
Alcoholic cardiomyopathy is due to drinking too much alcohol over a long period of time, which can weaken your heart so it can no longer pump blood efficiently. Your heart then becomes enlarged. This is a form of dilated cardiomyopathy.
Ischemic cardiomyopathy occurs when your heart can no longer pump blood to the rest of your body due to coronary artery disease. Blood vessels to the heart muscle narrow and become blocked. This deprives the heart muscle of oxygen. Ischemic cardiomyopathy is a common cause of heart failure. Alternatively, nonischemic cardiomyopathy is any form that isn’t related to coronary artery disease.
Noncompaction cardiomyopathy also called spongiform cardiomyopathy, is a rare disease present at birth. It results from abnormal development of the heart muscle in the womb. Diagnosis may occur at any stage of life.
Who is at risk for cardiomyopathy?
Cardiomyopathy can affect people of all ages. Major risk factors include the following:
a family history of cardiomyopathy, sudden cardiac arrest, or heart failure
coronary heart disease
diabetes
severe obesity
sarcoidosis
hemochromatosis
amyloidosis
heart attack
long-term high blood pressure
alcoholism
According to research, HIV, HIV treatments, and dietary and lifestyle factors can also increase your risk of cardiomyopathy. HIV can increase your risk of heart failure and dilated cardiomyopathy, in particular. If you have HIV, talk to your doctor about regular tests to check the health of your heart. You should also follow a heart-healthy diet and exercise program.
What are the symptoms of cardiomyopathy?
The symptoms of all types of cardiomyopathy tend to be similar. In all cases, the heart can’t adequately pump blood to the tissues and organs of the body. It can result in symptoms such as:
general weakness and fatigue
shortness of breath, particularly during exertion or exercise
lightheadedness and dizziness
chest pain
heart palpitations
fainting attacks
high blood pressure
edema, or swelling, of your feet, ankles, and legs
What is the treatment for cardiomyopathy?
Treatment varies depending on how damaged your heart is due to cardiomyopathy and the resulting symptoms.
Some people may not require treatment until symptoms appear. Others who are beginning to struggle with breathlessness or chest pain may need to make some lifestyle adjustments or take medications.
You can’t reverse or cure cardiomyopathy, but you can control it with some of the following options:
heart-healthy lifestyle changes
medications, including those used to treat high blood pressure, prevent water retention, keep the heart beating with a normal rhythm, prevent blood clots, and reduce inflammation
surgically implanted devices, like pacemakers and defibrillators
surgery
heart transplant, which is considered a last resort
The goal of treatment is to help your heart be as efficient as possible and to prevent further damage and loss of function.
What is the long-term outlook?
Cardiomyopathy can be life-threatening and can shorten your life expectancy if severe damage occurs early on. The disease is also progressive, which means it tends to get worse over time. Treatments can prolong your life. They can do this by slowing the decline of your heart’s condition or by providing technologies to help your heart do its job.
Those with cardiomyopathy should make several lifestyle adjustments to improve heart health. These may include:
maintaining a healthy weight
eating a modified diet
limiting caffeine intake
getting enough sleep
managing stress
quitting smoking
limiting alcohol intake
getting support from their family, friends, and doctor
One of the biggest challenges is sticking with a regular exercise program. Exercise can be very tiring for someone with a damaged heart. However, exercise is extremely important for maintaining a healthy weight and prolonging heart function. It’s important to check with your doctor and engage in a regular exercise program that’s not too taxing but that gets you moving every day.
The type of exercise that’s best for you will depend on the type of cardiomyopathy you have. Your doctor will help you determine an appropriate exercise routine, and they’ll tell you the warning signs to watch out for while exercising.
Warning Signs of a Heart Attack
Did you know that you can have a heart attack without feeling any chest pain? Heart failure and heart disease don’t show the same signs for everyone, especially women.
The heart is a muscle that contracts to pump blood throughout the body. A heart attack (often called a myocardial infarction) occurs when the heart muscle doesn’t get enough blood. Blood carries oxygen and nutrients to the heart muscle. When there isn’t enough blood flowing to your heart muscle, the affected part can get damaged or die. This is dangerous and sometimes deadly.
Heart attacks happen suddenly, but they normally result from long-standing heart disease. Typically, a waxy plaque builds up on the walls inside your blood vessels that feed the heart muscle. Sometimes a chunk of the plaque, called a blood clot, breaks off and prevents blood from passing through the vessel to your heart muscle, resulting in a heart attack.
Less commonly, something like stress, physical exertion, or cold weather causes the blood vessel to contract or spasm, which decreases the amount of blood that can get to your heart muscle.
There are many risk factors that contribute to having a heart attack, including:
age
heredity
high blood pressure
high cholesterol
obesity
poor diet
excessive alcohol consumption (on a regular basis: more than one drink per day for women and more than two drinks per day for men)
stress
physical inactivity
A heart attack is a medical emergency. It’s really important to listen to what your body is telling you if you think you might be having one. It’s better to seek emergency medical treatment and be wrong than to not get help when you’re having a heart attack.
Chest pain, pressure, and discomfort
Most people with heart attacks experience some sort of chest pain or discomfort. But it’s important to understand that chest pains don’t occur in every heart attack.
Chest pain is a common sign of a heart attack. People have described this sensation as feeling like an elephant is standing on their chest.
Some people don’t describe chest pain as pain at all. Instead, they may say they felt chest tightness or squeezing. Sometimes this discomfort can seem bad for a few minutes and then go away. Sometimes the discomfort comes back hours or even a day later. These could all be signs your heart muscle isn’t getting enough oxygen.
If you experience chest pains or tightness, you or someone around you should call 911 immediately.
Not just chest pain
Pain and tightness can also radiate in other areas of the body. Most people associate a heart attack with pain working its way down the left arm. That can happen, but pain can also appear in other locations, including:
upper abdomen
shoulder
back
neck/throat
teeth or jaw
According to the American Heart Association, women tend to report heart attacks that cause pain specifically in the lower abdomen and lower portion of the chest.
The pain may not be concentrated in the chest at all. It could feel like pressure in the chest and pain in other parts of the body. Upper back pain is another symptom women more commonly cite than men.
Sweating day and night
Sweating more than usual — especially if you aren’t exercising or being active — could be an early warning sign of heart problems. Pumping blood through clogged arteries takes more effort from your heart, so your body sweats more to try to keep your body temperature down during the extra exertion. If you experience cold sweats or clammy skin, then you should consult your doctor.
Night sweats are also a common symptom for women experiencing heart troubles. Women may mistake this symptom for an effect of menopause. However, if you wake up and your sheets are soaked or you cannot sleep due to your sweating, this could be a sign of a heart attack, especially in women.
Fatigue
Fatigue can be a less commonly recognized heart attack sign in women. According to the American Heart Association, some women may even think their heart attack symptoms are flu-like symptoms.
A heart attack can cause exhaustion due to the extra stress on your heart to try to pump while an area of blood flow is blocked. If you often feel tired or exhausted for no reason, it could be a sign that something is wrong.
Fatigue and shortness of breath are more common in women than men and may begin months before a heart attack. That’s why it’s important to see a doctor as early as possible when you experience early signs of fatigue.
Shortness of breath
Your breathing and your heart pumping blood effectively are very closely related. Your heart pumps blood so it can circulate to your tissues as well as get oxygen from your lungs. If your heart can’t pump blood well (as is the case with a heart attack), you can feel short of breath.
Shortness of breath can sometimes be an accompanying symptom of unusual fatigue in women. For example, some women report they would get unusually short of breath and tired from the activity they were performing. Going to the mailbox could leave them exhausted and unable to catch their breath. This can be a common sign of heart attack in women.
Lightheadedness
Lightheadedness and dizziness can occur with a heart attack and are often symptoms women describe. Some women report they feel like they might pass out if they try to stand up or overexert themselves. This sensation is certainly not a normal feeling and shouldn’t be ignored if you experience it.
Heart palpitations
Heart palpitations can range from feeling like your heart is skipping a beat to having changes in heart rhythm that can feel like your heart is pounding or throbbing. Your heart and body rely on a consistent, steady beat to best move blood throughout your body. If the beat gets out of rhythm, this could be a sign you’re having a heart attack.
Heart palpitations due to a heart attack can create a sense of unease or anxiety, especially in women. Some people may describe heart palpitations as a sensation their heart is pounding in their neck, not just their chest.
Changes in your heart’s rhythm shouldn’t be ignored, because once the heart is consistently out of rhythm, it requires medical intervention to get back into rhythm. If your palpitations are accompanied by dizziness, chest pressure, chest pain, or fainting, they could be confirmation that a heart attack is occurring.
Indigestion, nausea, and vomiting
Often people begin experiencing mild indigestion and other gastrointestinal problems before a heart attack. Because heart attacks usually occur in older people who typically have more indigestion problems, these symptoms can get dismissed as heartburn or another food-related complication.
If you normally have an iron stomach, indigestion or heartburn could be a signal that something else is going on.
What you should do during a heart attack
If you think you are having a heart attack, you or someone nearby should call emergency services immediately. It’s unsafe to drive yourself to the hospital during a heart attack, so call an ambulance. While you may feel awake and alert enough to drive, the chest pain could get so severe that you may have trouble breathing or difficulty thinking clearly.
After you call emergency services
When you call emergency services, the dispatcher may ask you about the medicines you take and your allergies. If you don’t currently take a blood thinner and you aren’t allergic to aspirin, the dispatcher may advise you to chew an aspirin while you’re waiting on medical attention. If you have nitroglycerin tablets, you may also wish to use these as directed by your doctor to reduce chest pain.
If you have a list of medications you currently take or any information about your medical history, you may wish to take this information with you. It can speed your medical care.
At the hospital
When you arrive at the hospital, you can expect the emergency medical personnel to take an electrocardiogram (EKG). This is a pain-free way to measure your heart’s electrical activity.
If you’re having a heart attack, an EKG is performed to look for unusual electrical patterns in your heart. The EKG can help your doctor determine if the heart muscle is damaged and what part of your heart was damaged. A doctor will also likely order a blood draw. If you’re having a heart attack, your body usually releases certain proteins and enzymes as a result of the stress to your heart.
If you’re having a heart attack, your doctor will discuss treatment options with you. Your risk of severe heart damage is lowered if you start treatment within several hours of developing symptoms.
How to prevent future heart problems
According to the Centers for Disease Control and PreventionTrusted Source, an estimated 200,000 deaths from heart disease and stroke are preventable. Even if you have risk factors for heart disease or have already had a heart attack, there are things you can do to reduce your risk of having a heart attack in the future.
People who have already had a heart attack should make sure to take all medications prescribed to them by their doctor. If your doctor placed cardiac stents to keep your heart vessels open or you had to have bypass surgery for your heart, taking the medications your doctor prescribed to you is vital to preventing a future heart attack.
Sometimes if you require surgery for another condition, your doctor may recommend stopping some medications you take for your heart. An example might be an antiplatelet (anticlot) medication like clopidogrel (Plavix), prasugrel (Effient), or ticagrelor (Brilinta). Always check with the doctor you see for your heart before you stop taking any of your medications. It’s unsafe to abruptly stop many medications, and stopping abruptly could increase your risk of a heart attack.
The heart is a muscular organ situated in the center of the chest behind the sternum. It consists of four chambers: the two upper chambers are called the right and left atria, and the two lower chambers are called the right and left ventricles. The right atrium and ventricle together are often called the right heart, and the left atrium and left ventricle together functionally form the left heart.[rx][rx][rx][rx]
Anatomy of the Heart
The heart is an organ responsible for pumping blood through the blood vessels using rhythmic contractions of cardiac muscle.
Key Points
The heart is a four-chambered muscular organ containing an involuntary conduction system that initiates rhythmic contractions to pump blood throughout the body.
The heart has its own blood supply and is controlled by self-regulating nerve bundles called nodes.
The SA and AV nodes send impulses through the Purkinje fibers that cause muscle contractions to the heart.
The heart is composed of three layers: the epicardium (outer layer) which prevents excess expansion or movement of the heart, the myocardium (middle layer) which initiates contractions driving the cardiac cycle, and the endocardium (inner layer) that lines the cavities and valves.
The heart contains two upper chambers called atria and two lower chambers called ventricles. The left and right sides of the heart are separated by the septum.
Valves prevent the backflow of blood and separate the atria from the ventricle and the ventricle from the pulmonary artery or aorta.
Key Terms
heart: A fist-sized muscular organ in the chest that pumps blood through the body using involuntary contractions of cardiac muscle.
ventricle: One of two lower chambers of the heart that receives blood from the atria and pumps it out into pulmonary or systemic circulation, depending on side.
myocardium: The middle of the three layers forming the wall of the heart, containing cardiac muscle tissue. Innervated by the Purkinje fibers.
The human heart is the pump for the circulatory system, and along with the circulatory system is considered to be an organ of the cardiovascular system. It consists of four chambers and pumps blood through both systemic and pulmonary circulation to enable gas exchange and tissue oxygenation. The heart is located in the thoracic cavity between the lungs and protected by the rib cage.
Structure of the Heart
The heart consists of four chambers separated into two sides. Each side contains an atrium that receives blood into the heart and flows it into a ventricle, which pumps the blood out of the heart. The atria and ventricle on each side of the heart are linked together by valves that prevent the backflow of blood. The wall that separates the left and right sides of the heart is called the septum.
The left heart deals with systemic circulation, while the right heart deals with pulmonary circulation. The left side of the heart receives oxygenated blood from the pulmonary vein and pumps it into the aorta, while the right side of the heart receives deoxygenated blood from the vena cava and pumps it into the pulmonary vein. The pulmonary vein and aorta also have valves connecting them to their respective ventricle.
The heart has its own self-sustaining conduction system that sends nervous impulses to cardiac tissue. The sinoatrial (SA) and atrioventricular (AV) nodes are bundles of nerve fibers that form this conduction system. They are located in the left atrial wall of the heart and send nerve impulses to a large, highly specialized set of nerves called the Purkinje fibers, which in turn send those nerve impulses to the cardiac muscle tissue. These nodes can send impulses to the heart without central nervous system stimulation but may be influenced by nervous stimulation to alter heart rate. The heart also has its own blood supply, the cardiac arteries that provide tissue oxygenation to the heart as the blood within the heart are not used for oxygenation by the heart.
Cardiac Histology
The heart is enclosed in a double-walled protective membrane called the pericardium, which is a mesothelium tissue of the thoracic cavity. The double membrane of the pericardium contains pericardial fluid which nourishes the heart and prevents shock. This composite sac protects the heart, anchors it to surrounding structures, and prevents the heart from overfilling with blood.
The wall of the heart is composed of three layers of different tissues. The outer layer is called the epicardium, or visceral pericardium since it is also the inner wall of the pericardium. The middle layer of the heart, the myocardium, and contains specialized cardiac muscle tissue responsible for contraction. Cardiac muscle tissue is distinct from skeletal or smooth muscle because it pumps involuntarily based on conduction from the AV and SA nodes. The inner layer is called the endocardium and is in contact with the blood that the heart pumps. It also merges with the inner lining of blood vessels and covers heart valves. Cardiac tissue is permanent tissue that does not heal or regenerate when damaged. As a result, is prone to scarring and enlargement due to mechanical stress and injury.
The Mammalian Heart: The position of valves ensures proper directional flow of blood through the cardiac interior. Note the difference in the thickness of the muscled walls of the atrium and the left and right ventricle.
Pericardium
The pericardium is a thick, membranous, fluid-filled sac which encloses, protects, and nourishes the heart.
Key Points
The pericardium is a mesothelium tissue of the thoracic cavity which surrounds the heart. The outer layer, the fibrous pericardium, is comprised of dense connective tissue that protects the heart, anchors it to the surrounding walls, and prevents it from overfilling.
The inner layer of the pericardium, the serous pericardium, is further divided into two layers, an outer parietal layer and an inner visceral layer with the pericardial cavity in between the two layers.
The serous pericardium functions to lubricate the heart with pericardial fluid, which is stored in the space between the parietal and visceral layers.
Pericarditis is inflammation of the pericardium, often due to infection, which can constrict and put harmful pressure on the heart.
Key Terms
fibrous pericardium: Composed of dense connective tissue which protects the heart, anchors it to the surrounding walls, and prevents the heart from overfilling with blood.
serous pericardium: Located deeper than the fibrous pericardium, this structure contains two layers that lubricate the heart to prevent friction from occurring during heart activity.
pericardium: A serous membrane that surrounds and protects the heart.
The pericardium is the thick, membranous, fluid-filled sac that surrounds the heart and the roots of the vessels that enter and leave this vital organ, functioning as a protective membrane. The pericardium is one of the mesothelium tissues of the thoracic cavity, along with the pleura which cover the lungs. The pericardium is composed of two layers, an outer fibrous pericardium and an inner serous pericardium.
Membranes of the Thoracic Cavity: A transverse section of the thorax, showing the contents of the middle and the posterior mediastinum. The pleural and pericardial cavities are exaggerated since normally there is no space between parietal and visceral pleura and between pericardium and heart.
Fibrous Pericardium
The fibrous pericardium is the outer layer of the pericardium. It is composed of dense connective tissue which anchors the heart to the mediastinum of the chest wall. It prevents the heart from overfilling with blood and protects it from nearby infections by completely separating it from the rest of the thoracic cavity. It is continuous with the outer fibrous layer of the neighboring great blood vessels.
Serous Pericardium
The serous pericardium, the inner layer of the pericardium, is composed of two different layers. The outer layer, the parietal layer, is completely adhered to the fibrous pericardium. The inner layer is known as the visceral layer, which covers and protects the great vessels and heart. The space between the parietal and visceral layers is called the pericardial cavity.
The visceral layer is referred to as the epicardium in the areas where it is in direct contact with the heart. The space between these two serous layers, the parietal and the visceral, is the pericardial cavity, which contains pericardial fluid. The serous pericardium, with its two membranes and the fluid-filled pericardial cavity, provides protection to the heart and a lubricated sliding surface within which the heart can move in response to its own contractions and to the movement of adjacent structures such as the diaphragm and the lungs.
Function of the Pericardium
The pericardium is important because it protects the heart from trauma, shock, stress, and even infections from the nearby lungs. It supports the heart and anchors it to the mediastinum so it doesn’t move within the body. The pericardium lubricates the heart and prevents it from becoming too large if blood volume is overloaded (though it will not prevent chronic heart enlargement).
Despite these functions, pericardium is still vulnerable to problems of its own. Pericarditis is the term for inflammation in the pericardium, typically due to infection. Pericarditis is often a severe disease because it can constrict and apply pressure on the heart and work against its normal function. Pericarditis comes in many types depending on which tissue layer is infected.
Layers of the Heart Walls
The heart wall is comprised of three layers: the outer epicardium, the middle myocardium, and the inner endocardium.
Key Points
The epicardium is a thin layer of connective tissue and fat serving as an additional layer of protection for the heart. It is considered a continuation of the serous pericardium.
The myocardium is the muscle tissue of the heart, composed of cardiac muscle cells called cardiomyocytes that receive nervous stimulation from the sinoatrial (SA) and atrioventricular (AV nodes via the Purkinje fibers.
Cardiomyocytes are shorter than skeletal myocytes and contain fewer nuclei. The cardiac muscle is striated.
The endocardium is composed of endothelial cells that provide a smooth, non-adherent surface for blood collection and pumping and may help regulate contractility.
An infection or inflammation of the endocardium is called infective endocarditis.
Key Terms
Purkinje fibers: A bundle of nerve fibers located under the endocardium, which supply nervous impulses to the myocardium’s cardiac muscle tissues.
endocardium: A thin serous membrane that lines the interior of the heart and valves.
cardiomyocyte: A cardiac muscle cell (or myocyte) in the heart, which makes up the cardiac muscle tissue.
The heart wall is comprised of three layers, the epicardium (outer), myocardium (middle), and endocardium (inner). These tissue layers are highly specialized and perform different functions. During ventricular contraction, the wave of depolarization from the SA and AV nodes moves from within the endocardial wall through the myocardial layer to the epicardial surface of the heart.
Epicardium
The Heart Wall: The wall of the heart is composed of three layers, the thin outer epicardium, the thick middle myocardium, and the very thin inner endocardium. The dark area on the heart wall is scarring from a previous myocardial infarction (heart attack).
The outer layer of the heart wall is the epicardium. The epicardium refers to both the outer layer of the heart and the inner layer of the serous visceral pericardium, which is attached to the outer wall of the heart. The epicardium is a thin layer of elastic connective tissue and fat that serves as an additional layer of protection from trauma or friction for the heart under the pericardium. This layer contains the coronary blood vessels, which oxygenate the tissues of the heart with a blood supply from the coronary arteries.
Myocardium
The middle layer of the heart wall is the myocardium—the muscle tissue of the heart and the thickest layer of the heart wall. It is composed of cardiac muscle cells or cardiomyocytes. Cardiomyocytes are specialized muscle cells that contract like other muscle cells but differ in shape. Compared to skeletal muscle cells, cardiac muscle cells are shorter and have fewer nuclei. Cardiac muscle tissue is also striated (forming protein bands) and contains tubules and gap junctions, unlike skeletal muscle tissue. Due to their continuous rhythmic contraction, cardiomyocytes require a dedicated blood supply to deliver oxygen and nutrients and remove waste products such as carbon dioxide from the cardiac muscle tissue. This blood supply is provided by the coronary arteries.
Endocardium
The inner layer of the heart wall is the endocardium, composed of endothelial cells that provide a smooth, elastic, non-adherent surface for blood collection and pumping. The endocardium may regulate metabolic waste removal from heart tissues and act as a barrier between the blood and the heart muscle, thus controlling the composition of the extracellular fluid in which the cardiomyocytes bathe. This in turn can affect the contractility of the heart.
This issue also covers the valves of the heart and is histologically continuous with the vascular endothelium of the major blood vessels entering and leaving the heart. The Purkinje fibers are located just beneath the endocardium and send nervous impulses from the SA and AV nodes outside of the heart into the myocardial tissues.
The endocardium can become infected, a serious inflammatory condition called infective endocarditis. This and other potential problems with the endocardium may damage the valves and impair the normal flow of blood through the heart.
Chambers of the Heart
The heart has four chambers. The two atria receive blood into the heart and the two ventricles pump blood into circulation.
Key Points
The right and left atria are the top chambers of the heart and receive blood into the heart. The right atrium receives deoxygenated blood from systemic circulation and the left atrium receives oxygenated blood from the pulmonary circulation.
The atria do not have inlet valves but are separated from the ventricles by valves. The atria facilitate circulation by allowing uninterrupted blood flow into the heart during ventricular systole.
The atria have several mechanisms in place to ensure that venous blood flow isn’t impaired, such as the lack of valves and the presence of light and brief contractions during atrial systole.
The right ventricle pumps deoxygenated blood into pulmonary circulation. The left ventricle pumps oxygenated blood into systemic circulation. The left ventricle is thicker because systemic circulation involves a much larger blood volume than pulmonary circulation.
Systole describes contraction when blood is pumped from the heart into circulation by the ventricles. It can also describe atrial systole, in which blood moves from the atria to the ventricles during ventricular diastole.
Diastole describes relaxation when blood moves into the heart while the ventricles prepare to eject that same blood during systole.
Key Terms
diastole: The relaxation and dilation of the heart chambers between contractions, during which they fill with blood.
systole: The rhythmic contraction of the heart by which blood is ejected from one chamber to the next, or out of the heart and into the arteries.
The heart is the complex pump of the circulatory system, pumping blood throughout the body for the purposes of tissue oxygenation and gas exchange. The heart has four chambers through which blood flows: two sets of each type of chamber (atria and ventricles), one per side, each with distinct functions. The left side of the heart deals with systemic circulation while the right side of the heart deals with pulmonary circulation.
The Atria
The atria are chambers in which blood enters the heart. They are located on the anterior end of the heart, with one atrium on each side. The right atrium receives deoxygenated blood from systemic circulation through the superior vena cava and inferior venae cavae. The left atrium receives oxygenated blood from pulmonary circulation through the left and right pulmonary veins.
Blood passively flows into the atria without passing through valves. The atria relax and dilate (expand) while they fill with blood in a process called atrial diastole. The atria and ventricles are separated by the mitral and tricuspid valves. The atria undergo atrial systole, a brief contraction of the atria that ejects blood from the atria through the valves and into the ventricles. The chordae tendinae are elastic tendons that attach to the valve from the ventricles and relax during atrial systole and ventricular diastole, but contract and close off the valve during ventricular systole.
One of the defining characteristics of the atria is that they do not impede venous flow into the heart. Atria has four essential characteristics that cause them to promote continuous venous flow:
There are no atrial inlet valves to interrupt blood flow during atrial systole. The venous blood entering the heart has a very low pressure compared to arterial blood, and valves would require venous blood pressure to build up over a long period of time to enter the atria.
The atrial systole contractions are incomplete and do not block flow from the veins through the atria into the ventricles. During atrial systole, blood not only empties from the atria to the ventricles, but continues to flow uninterrupted from the veins right through the atria into the ventricles.
The atrial contractions are slight, preventing significant back pressure that would impede venous flow.
The relaxation of the atria is coordinated to begin before the start of ventricular contraction, which also helps prevent the heart from beating too slowly.
Ventricles
The ventricles are located on the posterior end of the heart beneath their corresponding atrium. The right ventricle receives deoxygenated blood from the right atria and pumps it through the pulmonary vein and into the pulmonary circulation, which goes into the lungs for gas exchange. The left ventricle receives oxygenated blood from the left atria and pumps it through the aorta into the systemic circulation to supply the tissues of the body with oxygen.
The walls of the ventricles are thicker and stronger than those of the atria. The physiologic load on the ventricles, which pumps blood throughout the body and lungs, is much greater than the pressure generated by the atria to fill the ventricles. Further, the left ventricle has thicker walls than the right because it pumps blood throughout the body, while the right ventricle pumps only to the lungs, which is a much smaller volume of blood.
During ventricular diastole, the ventricles relax and fill with blood. During ventricular systole, the ventricles contract, pumping blood through the semi-lunar valves into the systemic circulation.
Structure of the heart: Structure diagram of a coronal section of the human heart from an anterior view. The two larger chambers are the ventricles.
Great Vessels of the Heart
Great vessels are the major vessels that directly carry blood into or out of the heart.
Key Points
Five great vessels enter and leave the heart: the superior and inferior vena cava, the pulmonary artery, the pulmonary vein, and the aorta.
The superior vena cava and inferior vena cava are veins that return deoxygenated blood from circulation in the body and empty it into the right atrium.
The pulmonary artery carries deoxygenated blood from the right ventricle into the lungs for oxygenation.
The pulmonary veins carry oxygenated blood from the lungs into the left atrium where it is returned to the systemic circulation.
The aorta is the largest artery in the body. It carries oxygenated blood from the left ventricle of the heart into the systemic circulation.
The aorta has many subdivisions that branch off into smaller arteries. These subdivisions are the ascending and descending aorta, the aortic arch, and the thoracic and abdominal aorta.
Key Terms
pulmonary arteries: The arteries that take deoxygenated blood away from the right side of the heart and into the capillaries of the lungs for the purpose of gas exchange.
aorta: The great artery which carries the blood from the heart into the systemic circulation.
venae cavae: The two large vessels, the superior and inferior vena cava, that bring deoxygenated blood from systemic circulation to the heart.
The human circulatory system is a double system, meaning there are two separate systems of blood flow: pulmonary circulation and systemic circulation. The adult human heart consists of two separate pumps, the right side (right atrium and ventricle,) which pumps deoxygenated blood into the pulmonary circulation, and the left side (left atrium and ventricle), which pumps oxygenated blood into the systemic circulation. Great vessels are the major vessels that carry blood into the heart and away from the heart to and from the pulmonary or systemic circuit. The great vessels collect and distribute blood across the body from numerous smaller vessels.
The Venae Cavae
The Systemic Circuit: The venae cavae and the aorta from the systemic circuit, which circulates blood to the head, extremities, and abdomen.
The superior and inferior vena cava are collectively called the venae cavae. The venae cavae, along with the aorta, are the great vessels involved in the systemic circulation. These veins return deoxygenated blood from the body into the heart, emptying it into the right atrium. The venae cavae are not separated from the right atrium by valves.
Superior Vena Cava
The superior vena cava is a large, short vein that carries deoxygenated blood from the upper half of the body to the right atrium. The right and left subclavian veins, jugular veins, and thyroid veins feed into the superior vena cava. The subclavian veins are significant because the thoracic lymphatic duct drains lymph fluid into the subclavian veins, making the superior vena cava a site of lymph fluid recirculation into the plasma. The superior vena cava begins above the heart.
Inferior Vena Cava
The inferior vena cava is the largest vein in the body and carries deoxygenated blood from the lower half of the body into the heart. The left and right common iliac veins converge to form the inferior vena cava at its lowest point. The inferior vena cava begins posterior to the abdominal cavity and travels to the heart next to the abdominal aorta. Along the way up the body from the iliac veins, the renal and suprarenal veins ( kidney and adrenal glands), lumbar veins (from the back), and hepatic veins (from the liver) all drain into the inferior vena cava.
The Aorta
The aorta is the largest of the arteries in systemic circulation. Blood is pumped from the left ventricle through the aortic valve into the aorta. The aorta is a highly elastic artery and is able to dilate and constrict in response to blood pressure and volume. When the left ventricle contracts to force blood through the aortic valve into the aorta, the aorta expands. This expansion provides potential energy to help maintain blood pressure during diastole, when the aorta passively contracts. Blood pressure is highest in the aorta and diminishes through circulation, reaching its lowest points at the end of venous circulation. The difference in pressure between the aorta and right atrium accounts for blood flow in the circulation, as blood flows from areas of high pressure to areas of low pressure.
Components of the Aorta
The aortic arch contains peripheral baroreceptors (pressure sensors) and chemoreceptors (chemical sensors) that relay information concerning blood pressure, blood pH, and carbon dioxide levels to the medulla oblongata of the brain. This information is processed by the brain and the autonomic nervous system mediates the homeostatic responses that involve feedback in the lungs and kidneys. The aorta extends around the heart and travels downward, diverging into the iliac arteries. The five components of the aorta are:
The ascending aorta lies between the heart and the arch of the aorta. It breaks off into the aortic sinuses, some of which form the coronary arteries.
The arch of the aorta is the peak of the aorta, which breaks off into the left carotid artery, brachiocephalic trunk, and the left subclavian artery.
The descending aorta is the section from the arch of the aorta to the point where it divides into the common iliac arteries. It is subdivided into the thoracic and abdominal aorta.
The thoracic aorta is the part of the descending aorta above the diaphragm. It branches off into the bronchial, mediastinal, esophageal, and phrenic arteries.
The abdominal aorta is the part of the descending aorta below the diaphragm, which divides into the iliac arteries and branches into the renal and suprarenal arteries. This part of the aorta is vulnerable to bursting and hemorrhage (aneurysm) from persistently high blood pressure.
The Pulmonary Arteries
The pulmonary arteries carry deoxygenated blood from the right ventricle into the alveolar capillaries of the lungs to unload carbon dioxide and take up oxygen. These are the only arteries that carry deoxygenated blood, and are considered arteries because they carry blood away from the heart. The short, wide vessel branches into the left and right pulmonary arteries that deliver deoxygenated blood to the respective lungs. Blood first passes through the pulmonary valve as it is ejected into the pulmonary arteries.
Pulmonary circuit: Diagram of pulmonary circulation. Oxygen-rich blood is shown in red; oxygen-depleted blood in blue.
The Pulmonary Veins
The pulmonary veins carry oxygenated blood from the lungs to the left atrium of the heart. Despite carrying oxygenated blood, this great vessel is still considered a vein because it carries blood towards the heart. Four pulmonary veins enter the left atrium. The right pulmonary veins pass behind the right atrium and superior vena cava while the left pass in front of the descending thoracic aorta. The pulmonary arteries and veins are both considered part of pulmonary circulation.
Myocardial Thickness and Function
The myocardium (cardiac muscle) is the thickest section of the heart wall and contains cardiomyocytes, the contractile cells of the heart.
Key Points
Coordinated contraction of cardiomyocytes causes the heart to contract and expel blood into circulation.
The myocardium is thickest in the left ventricle, as the left ventricle must create a lot of pressure to pump blood into the aorta and throughout the systemic circulation.
Cardiac muscle has a high density of mitochondria and a large blood supply, which keep it functioning continuously.
Sarcomeres are the basic unit of muscle tissue, composed primarily of actin and myosin myofibrils.
The heart’s thickness may change over time and adapt to compensate for diseases, which often results in heart failure.
Key Terms
Cardiac hypertrophy: An adaptive disease in which the walls of the heart become too thick to pump blood effectively. It is generally a complication of hypertension.
sarcomere: The basic contractile unit of contractile muscle, which contains myofibril filaments made out of myosin and actin, the two proteins that slide past one another to cause a muscle contraction.
cardiomyocyte: A cardiac muscle cell (myocyte) in the heart.
The myocardium, or cardiac muscle, is the thickest section of the heart wall and contains cardiomyocytes, the contractile cells of the heart. As a type of muscle tissue, the myocardium is unique among all other muscle tissues in the human body. The thickness of the myocardium determines the strength of the heart’s ability to pump blood.
Myocardial Histology
The structure of cardiac muscle shares some characteristics with skeletal muscle but has many distinctive features of its own. Cardiomyocytes are shorter than skeletal myocytes and have fewer nuclei. Each muscle fiber connects to the plasma membrane (sarcolemma) with distinctive tubules ( T-tubule ). At these T-tubules, the sarcolemma is studded with a large number of calcium channels which allow calcium ion exchange at a rate much faster than that of the neuromuscular junction in skeletal muscle. The flux of calcium ions into the muscle cells causes stimulates an action potential, which causes the cells to contract.
Cardiac muscle, like skeletal muscle, is comprised of sarcomeres, the basic, contractile units of muscle. Sarcomeres are composed of long, fibrous proteins that slide past each other when the muscles contract and relax. Two of the important proteins found in sarcomeres are myosin, which forms the thick filament, and actin, which forms the thin filament. Myosin has a long, fibrous tail and a globular head that binds to actin. The myosin head also binds to ATP, the source of energy for cellular metabolism, and is required for the cardiomyocytes to sustain themselves and function normally. Together, myosin and actin form myofibril filaments, the elongated, contractile threads found in muscle tissue. Cardiac muscle and skeletal muscle both contain the protein myoglobin, which stores oxygen.
Cardiac muscle is adapted to be highly resistant to fatigue. Cardiomyocytes have a large number of mitochondria, enabling continuous aerobic respiration. Cardiac muscle also has a large blood supply relative to its size, which provides a continuous stream of nutrients and oxygen while providing ample removal of metabolic waste.
Cardiac Muscle: The tissue structure of cardiac muscle contains sarcomeres that are made of myofibrils with intercalated disks, that contain cardiomyocytes, and have many mitochondrial.
Myocardial Thickness
The myocardium has variable levels of thickness within the heart. Chambers of the heart with a thicker myocardium are able to pump blood with more pressure and force compared to chambers of the heart with a thinner myocardium. The myocardium is thinnest within the atria, as these chambers primarily fill through passive blood flow. The right ventricle myocardium is thicker than the atrial myocardium, as this muscle must pump all blood returning to the heart into the lungs for oxygenation. The myocardium is thickest in the left ventricle, as this chamber must create substantial pressure to pump blood into the aorta and throughout the systemic circulation.
The thickness of the myocardium may change in some individuals as a compensatory adaptation to disease, either thickening and becoming stiff or becoming thinner and flabby. Cardiac hypertrophy is a common result of hypertension (high blood pressure) in which the cells of the myocardium enlarge as an adaptive response to pumping against the higher pressure. Eventually, hypertrophy may become so severe that heart failure occurs when the heart becomes so stiff that it can no longer pump blood. A flabby heart is typically the result of myocardial infections, in which the heart muscle becomes so weak that it cannot efficiently pump blood, which also leads to heart failure.
Right Ventricular Hypertrophy: If the heart adapts to become too thick, it will not be able to pump blood as efficiently, and heart failure may occur.
Fibrous Skeleton of the Heart
The cardiac skeleton, also known as the heart’s fibrous skeleton, consists of dense connective tissue in the heart that separates the atria from the ventricles.
Key Points
The cardiac skeleton consists of four bands of dense connective tissue, called fibrous rings, that surround the base of the pulmonary trunk, aorta, and mitral and tricuspid valves.
The heart‘s fibrous skeleton stops the flow of electrical currents between the chambers of the heart so that it only flows through the atrioventricular (AV) bundle. This causes a delay in depolarization so that the ventricles contract after they fill with blood.
The AV bundle is a bundle of electrically connected cardiomyocytes that transmit impulses from the AV node to the apex of the heart. It is located in the center of the cardiac skeleton.
The cardiac skeleton consists mainly of the protein collagen, a glycoprotein found in all connective tissues.
Key Terms
collagen: A glycoprotein that forms elongated fibers, usually found in the extracellular matrix of connective tissue.
fibrous rings: Four dense bands of tough elastic tissue that encircle the bases of the valves of the heart.
The cardiac skeleton, or fibrous skeleton of the heart, is the structure of dense connective tissue that separates the atria from the ventricles. The fibrous skeleton provides critical support for the heart and separates the flow of electrical impulses through the heart.
Fibrous Ring Structure
Fibrous Rings of the Heart: Transverse section of the heart showing the fibrous rings surrounding the valves.
The primary structure of the cardiac skeleton consists of four dense bands of tough elastic tissue called fibrous rings that encircle the bases of the heart valves. The fibrous skeleton is composed primarily of collagen, a protein found in every type of connective tissue in the human body. There are four fibrous rings:
The aortic ring encircles the aortic valve. It provides support for the aortic valve so that it is open, yet does not have backflow.
The pulmonary ring encircles the pulmonary valve. Similar to the aortic ring, it provides structural support for the pulmonary valve.
The left fibrous ring encircles the bicuspid valve. This ring is the thickest and strongest of all the fibrous rings due to the thickness of the left ventricle, which requires more structural support than the other chambers of the heart. It also surrounds the coronary arteries and AV node.
The right fibrous ring encircles the tricuspid valve. It also surrounds the coronary arteries and AV node.
The fibrous skeleton provides a great amount of structural and functional support for the valves of the heart by enabling them to stay open and provides a point of attachment for the valves to the wall of the heart.
Electrical Functions
The fibrous skeleton of the heart acts as an insulator for the flow of electrical current across the heart. It stops the flow of electricity between the different chambers of the heart so that electrical impulses do not flow directly between the atria and ventricles. The sinoatrial (SA) node lies on the top of the heart, while the AV node is located at the center of the fibrous skeleton, the only path by which electricity can flow through the heart.
This electrical separation is essential for cardiac function because electrical impulses flow from the top of the heart to the bottom of the heart. The separation allows the AV node and AV bundle to delay the wave of depolarization so that the atria can contract and assist in the ventricular filling before the ventricles themselves depolarize and contract. Without the fibrous skeleton of the heart, the heart’s ability to pump blood would be considerably less efficient since the ventricles would contract before filled to capacity. The fibrous skeleton of the heart also protects against cardiac arrhythmias.
Blood Supply and Lymphatics
The heart is supplied by two coronary arteries: the left main coronary artery and the right coronary artery. The left main coronary artery carries 80% of the flow to the heart muscle. It is a short artery that divides into two branches, (1) the left anterior descending artery that supplies anterior two-thirds of the inter-ventricular septum and adjoining part of the left ventricular anterior wall, and (2) the circumflex coronary artery that supplies blood to the lateral and posterior portions of the left ventricle.
The right coronary artery and its branches supply the right ventricle, right atrium, and left ventricle’s inferior wall.
Coronary arteries and veins course over the surface of the heart. Most coronary veins coalesce into the coronary sinus that runs in the left posterior atrioventricular groove and opens into the right atrium. Other small veins, called thebesian veins, open directly into all four chambers of the heart.
Small lymphatic vessels form a dense network beneath the epicardium and endocardium of the ventricles and open into a lymphatic duct in the atrioventricular groove. However, the detailed lymphatic anatomy of the human heart has not been worked out.
Nerves
The sinus node and the AV node are both supplied by sympathetic nerve fibers from the sympathetic ganglia and parasympathetic fibers through the vagus nerve and parasympathetic ganglia behind the heart.
Transfusion is a routine medical procedure in which donated blood is provided to you through a narrow tube placed within a vein in your arm. This potentially life-saving procedure can help replace blood lost due to surgery or injury.
A transfusion is defined as an infusion of whole blood or any one of its components. Transfusions like any other medical intervention have benefits and risks. Hemolytic transfusion reactions are one of the possible complications from transfusions. Hemolysis is described as rupture of red blood cells and leakage of their contents. The site of hemolysis can be intravascular (in circulation) or extravascular (in the reticuloendothelial system). Hemolytic transfusion reactions can be immune or non-immune mediated.[rx][rx][rx]
Blood transfusion is the process of transferring blood products into one’s circulation intravenously.[rx] Transfusions are used for various medical conditions to replace lost components of the blood. Early transfusions used whole blood, but modern medical practice commonly uses only components of the blood, such as red blood cells, white blood cells, plasma, clotting factors, and platelets.
Types of blood transfusions
According to the American Red Cross, there are four common types of blood transfusions:
Red blood cell transfusions: A person may receive a red blood cell transfusion if they have experienced blood loss, if they have anemia (such as iron deficiency anemia), or if they have a blood disorder.
Platelet transfusions: A platelet transfusion can help those who have lower platelet counts, such as from chemotherapy or a platelet disorder.
Plasma transfusions: Plasma contains proteins important for health. A person may receive a plasma transfusion if they have experienced severe burns, infections, or liver failure.
Whole blood transfusion: A person may receive a whole blood transfusion if they have experienced a severe traumatic hemorrhage and require red blood cells, white blood cells, and platelets.
Before a blood transfusion, a healthcare professional will remove the white blood cells from the blood. This is because they can carry viruses.
That said, they may transfuse white blood cells called granulocytes to help a person recover from an infection that has not responded to antibiotics. Healthcare professionals can collect granulocytes using a process called apheresis.
Pathophysiology
The pathophysiology varies based on the transfusion reaction.[rx][rx][rx]
Acute Transfusion Reactions
Mild allergic: Attributed to hypersensitivity to a foreign protein in the donor product.
Anaphylactic: Similar to a mild allergic reaction, however resulting in a more severe reaction. Sometimes this can occur in a patient with IgA deficiency who makes alloantibodies against IgA and then receives blood products containing IgA.
Febrile non-hemolytic: Generally thought to be caused by cytokines released from blood donor leukocytes (white blood cells).
Septic: Caused by bacteria or bacterial byproducts (such as endotoxin) which may contaminate blood.
Acute hemolytic transfusion reactions: Can result in intravascular or extravascular hemolysis, depending on the specific etiology (cause). Immune-mediated reactions are often a result of recipient antibodies present to blood donor antigens. Non-immune reactions are possible, and occur when red blood cells are damaged before transfusion (e.g., by heat or incorrect osmotic conditions).
Transfusion-associated circulatory overload (TACO):Occurs when the volume of the transfused component causes hypervolemia (volume overload).
Transfusion-related acute lung injury: Acute lung injury is due to antibodies in the donor product (human leukocyte antigen or human neutrophil antigen) reacting with antigens in the recipient. The recipient’s immune system responds and causes the release of mediators that lead to pulmonary edema. Possibly contributing to this are clinical conditions that predispose the patient including infection, recent surgery, or inflammation.
Delayed Transfusion Reactions
Delayed hemolytic transfusion reaction: Typically caused by an anamnestic response to a foreign antigen that the patient was previously exposed to (generally by prior transfusion or pregnancy).
Transfusion-associated graft-versus-host disease: Results from engraftment of donor lymphocytes (commonly found in cellular blood products) into an immunocompromised recipient’s bone marrow. The donor lymphocytes recognize the patient as foreign and react against the recipient’s body. The patient’s immune system is unable to clear the foreign lymphocytes. This is rare but often fatal.
Transfusions of Whole Blood
Whole blood refers to human blood transfusion from a standard blood donation.
Key Points
Whole blood can be separated into its components: red blood cells, plasma, and platelets.
Blood can be transfused in either its relatively unprocessed form as whole blood or through the administration of its processed and separated cellular or plasma components.
Plateletpheresis is a more efficient way to extract platelets than whole blood extraction because plateletpheresis produces platelets that are more highly concentrated.
The blood is separated into distinct plasma and cellular layers by centrifugation, sedimentation, or simply through gravity over a longer period of time.
Whole blood transfusion has similar risks to a transfusion of red blood cells and must be cross-matched based on blood type to avoid hemolytic transfusion reactions and other complications.
Key Terms
buffy coat: The fraction of an anticoagulated blood sample that contains most of the white blood cells and platelets following density gradient centrifugation of the blood.
centrifuge: A device in which a mixture of denser and lighter materials (normally dispersed in a liquid) is separated by rotation around a central axis at high speed.
plasma: The straw-colored/pale-yellow liquid component of blood that normally holds the blood cells of whole blood in suspension.
Blood transfusions are a key therapeutic component to treating those with excessive blood loss from severe injury or surgery. Whole blood refers to blood drawn directly from the body from which none of the components, such as plasma or platelets, have been removed. The blood is typically combined with an anticoagulant during the collection process but is otherwise unprocessed. Whole blood may also be altered and processed for use in blood transfusion.
Blood Processing
Centrifuged Blood: Whole blood is a term used in transfusion medicine for human blood from a standard blood donation.
Historically, blood was transfused as whole blood without further processing. Most blood banks now split the whole blood into two or more components, typically red blood cells and a plasma component such as fresh frozen plasma, which is extracted frozen plasma from the blood splitting process.
Platelets for transfusion can also be prepared from the buffy coat of whole blood, which has therapeutic benefits for those with platelet disorders or impaired clotting ability. Some blood banks have replaced this with platelets collected by plateletpheresis, a process in which platelets are extracted during initial blood collection. Plateletpheresis is more efficient because whole blood platelets typically aren’t concentrated enough to have a useful effect, while plateletpheresis platelets are highly packed and concentrated. It also minimizes the chance of platelet transplant rejection because a single donor will be able to contribute enough platelets via plateletpheresis.
The collected blood is generally separated into components by one of three laboratory methods:
Centrifuge quickly separates whole blood into plasma, buffy coats, and red cells by using centrifugal force to drop the cellular components to the bottom of a container.
Sedimentation, in which whole blood sits overnight, causing the red blood cells and plasma to settle and slowly separate by the force of normal gravity.
Practical Considerations
Whole blood transfusion has similar risks to those of transfusion of red blood cells. It must be cross-matched on the basis of blood type to avoid hemolytic transfusion reactions. Most of the indications for use are identical to those for red blood cells. Whole blood is not used because the extra plasma can contribute to transfusion-associated circulatory overload (TACO), a potential complication that can dangerously increase blood pressure, causing pulmonary edema and acute respiratory distress.
Whole blood is sometimes “recreated” from stored red blood cells and fresh frozen plasma for neonatal transfusions. This provides a final product with a very specific hematocrit (percentage of red cells) with type O red cells and types AB plasma to minimize the chance of complications.
Whole blood is typically stored under the same conditions as red blood cells and can be kept up to 35 days if collected with CPDA-1 storage solution or 21 days with other common storage solutions such as CPD. If the blood will be used to make platelets, it is kept at room temperature until the process is complete. This must be done quickly to minimize the warm storage of RBCs in the unit.
Blood Transfusions: Blood transfusions are common during surgeries.
Plasma and Blood Volume Expanders
A volume expander is a type of intravenous therapy that provides a fluid replacement for the circulatory system.
Key Points
During blood loss, the amount of oxygen that can be delivered to the tissues is reduced due to lost red blood cells and decreased blood volume, which also causes a decrease in blood pressure.
Although they cannot replace lost red blood cells, blood volume expanders can help improve oxygen delivery in instances of blood loss by increasing blood volume and blood pressure so that blood can flow to the tissues.
Survival is possible with low red blood cell and hemoglobin levels as long as blood volume and blood pressure are maintained so blood continues to reach tissues.
Hypovolemic shock occurs when tissue oxygenation drops due to a decrease in blood volume.
Crystalloid volume expanders are aqueous solutions of mineral salts or other water-soluble molecules. Although they decrease the osmotic pressure by diluting the red blood cells, they increase both vascular and interstitial volume.
Colloid volume expanders contain larger insoluble molecules, such as gelatin or hydroxyethyl starch, and theoretically increase the intravascular volume but not interstitial and intracellular volumes.
Key Terms
crystalloid: Aqueous solutions of mineral salts or other water-soluble molecules, such as saline solution.
hypovolemic shock: Shock due to decreased blood volume, such as through severe bleeding or vomiting. It activates dangerous compensatory mechanisms that maintain blood flow to the brain while causing other organs to fail.
When blood is lost, the greatest immediate need is to stop further blood loss, then lost volume must be replaced. Blood volume is directly proportional to the blood pressure in the body, and when both decrease the flow of blood to important tissues may be inhibited. The remaining red blood cells can still oxygenate body tissue. A volume expander is a type of intravenous therapy that provides blood volume for the circulatory system. It may be used for fluid replacement.
Blood Volume and Oxygen Transport
Normal human blood has a significant excess oxygen transport capability because not all of the hemoglobin molecules are loaded with oxygen under normal conditions. As long as pulmonary function is sufficient for gas exchange and there is enough blood volume to have sufficient blood pressure, very low hemoglobin levels will be enough to sustain the patient. Those with low hemoglobin content will not be able to tolerate situations where a greater amount of oxygen is required (exercise, for example) until their hemoglobin levels are restored.
The body has compensatory feedback mechanisms to deal with lower hemoglobin levels. For instance, the heart pumps more blood with each beat, which increases blood pressure. Blood pressure is detected by the renal system, which increases blood volume and blood pressure by excreting less water during blood filtration. As a result of partial pressure gradient changes, more oxygen is released to the tissues. These adaptations are so effective that if only half of the red blood cells remain, oxygen delivery will still be around 75% of normal. A patient at rest only uses 25% of the oxygen available in their blood. In extreme cases, patients have survived with a hemoglobin level of about 1/7 the normal (i.e. 2 g/dl), although levels this low are very dangerous.
When blood loss is significant, the red blood cell level ultimately drops to a level that is too low for adequate tissue oxygenation. This is marked by hypoxia and hypovolemic shock, a condition in which tissue oxygenation drops from a lack of blood volume and harmful compensatory mechanisms activate, causing more damage. In these situations, the only alternatives are blood transfusion, packed red blood cells, or oxygen therapy.
Types of Volume Expanders
Saline solution: A bag of saline. Saline can be used to increase blood volume when a blood transfusion is not possible.
There are two main types of volume expanders: crystalloids and colloids. Crystalloids are aqueous solutions of mineral salts or other water-soluble molecules. Colloids contain larger insoluble molecules, such as gelatin; blood itself is a colloid. There are also a few other volume expanders that may be used in certain situations:
Colloids: These solutions preserve a high-colloid osmotic pressure (protein-exerted pressure) in the blood, while this parameter is decreased by crystalloids due to hemodilution. The higher osmotic pressure from colloids draws fluids inward, preventing it from leaking out into the tissues as easily, which increases intravascular blood volume.
Crystalloids: The most commonly used crystalloid fluid is normal saline, a solution of sodium chloride at 0.9% concentration, which is close to the concentration in the blood (isotonic). Saline solution is administered intravenously (IV drips) and increases both intravascular and interstitial volume. They decrease osmotic pressure by diluting the blood.
Dextrose Water: This solution contains dextrose, a form of glucose. It is given to patients who have dangerously low blood sugar levels (important for cellular metabolism) as well as low blood volume.
Another common volume expander includes hydroxyethyl starch (HES/HAES, common trade names: Hespan, Voluven) which is considered a colloid. An intravenous solution of hydroxyethyl starch is used to prevent shock following severe blood loss caused by trauma, surgery, or another problem. It increases the blood volume, allowing red blood cells to continue to deliver oxygen to the body. When tissue blood perfusion is maintained, shock is averted as the dangerous compensatory mechanisms of shock aren’t activated.
Blood Groups and Blood Types
Red blood cells have surface-expressed proteins that define the self/not-self nature of the cells.
Key Points
Surface-expressed proteins called antigens on red blood cells determine an individual’s blood type. There are two types of antigen groups: the ABO system antigens and a Rhesus D antigen.
Exposure to a blood group antigen that is not recognized as self will cause the immune system to make specific antibodies to the new blood group antigen, often leading to the destruction of the cells.
Knowing an individual’s antigen type is important to ensure compatibility if a transfusion is needed.
Blood type is inherited. O type is the most common despite being a recessive gene because it is more highly expressed in the gene pool, while type A and type B are dominant (and type AB is codominant) but are less common because they are less expressed in the gene pool.
Individuals may also be positive or negative for the rhesus D antigen in addition to their blood type. Rhesus D complications are common during fetal development if the parents differ in rhesus antigen expression.
Key Terms
antibodies: Also known as an immunoglobulin (Ig), a large Y-shaped protein produced by B-cells that is used by the immune system to identify and neutralize foreign objects such as bacteria and viruses.
antigen: A substance that induces an immune response, usually foreign.
Red blood cells have surface-expressed proteins that act as antigens, which are molecules that can illicit an immune system response. Red blood cells belong to different groups on the basis of the type of antigen that they express. Blood type determines compatibility for receiving blood transfusions from other people.
The ABO Blood Group System
If an individual is exposed to a blood group antigen (A or B) that is not recognized as self, the individual can become sensitized to that antigen. This will cause the immune system to make specific antibodies to a particular blood group antigen and form an immunological memory against that antigen. These antibodies can bind to antigens on the surface of transfused red blood cells (or other foreign tissue cells), often leading to destruction of the cells by recruitment of other components of the immune system.
Knowledge of an individual’s blood type is important to identify appropriate blood for transfusion or tissue for organ transplantation. There are four blood types that differ based on the antigen expressed by the red blood cell and by the type of associated antibody found in the plasma. The type of antigen determines which blood types that blood type may safely be donated to, while the type of antibody determines which types of antigen (and types of blood) will be rejected by the body.
Blood type classification: Blood type (or blood group) is determined, in part, by the ABO blood group antigens present on red blood cells.
Blood group A individuals have the A antigen on the surface of their RBCs, and blood serum containing IgM antibodies against the B antigen. Therefore, a group A individual can only receive blood from individuals of groups A or O types and can donate blood to individuals of groups A or AB.
Blood group B individuals have the B antigen on the surface of their RBCs, and blood serum containing IgM antibodies against the A antigen. Therefore, a group B individual can only receive blood from individuals of groups B or O and can donate blood to individuals of groups B or AB.
Blood Group AB individuals have both A and B antigens on the surface of their RBCs, and their blood serum does not contain any antibodies against either A or B antigen. Therefore, an individual with type AB blood can receive blood from any group, but can only donate blood to another group AB individual. AB blood is also known as the “universal receiver.”
Blood group O individuals do not have either A or B antigens on the surface of their RBCs, but their blood serum contains IgM antibodies against both A and B antigens. Therefore, a group O individual can only receive blood from a group O individual, but they can donate blood to individuals of any ABO blood group (i.e. A, B, O, or AB). O blood is also known as “universal donor.”
Blood types are inherited and represent genetic contributions from both parents. The gene that codes for blood type contain three alleles: IA and IB which give type A and B blood and are dominant, and I, which is recessive, and codes type O. Children will have blood types similar to their parents based on inheritance. The I allele is far more commonly expressed in the gene pool than IA and IB, which is why type O blood is the most common type despite being a recessive phenotype. Type AB is the rarest because it is the combination of less commonly expressed alleles, and is the result of codominance between IA and IB alleles.
Rhesus Factor
Many people also have the rhesus D (Rh) antigen expressed by their red blood cells. Those that have Rh antigens are positive for Rh, while those that don’t have it are Rh-negative (ie. type O+ is type O with rhesus, type A- is type A without rhesus). Rh-positive individuals do not have the antibodies for the Rh factor but can make them if exposed to Rh. Besides being a consideration for blood transfusion, parents who differ based on Rh status must be cautious to ensure that maternal antibodies do not destroy their child’s red blood cells during fetal development, which can cause hemolytic anemia.
Typing and Cross-Matching for Transfusions
Blood banks test donor blood to ensure recipient compatibility, reducing the risk of hemolytic reaction, renal failure, and death.
Key Points
Transfusion medicine is important to treat those with blood loss.
Given enough time, cross-matching is performed to ensure that donated blood will not cause a transfusion reaction.
Cross-matching involves mixing a sample of the recipient’s serum with a sample of the donor’s red blood cells and checking if the mixture agglutinates due to antibody reactivity.
If a transfusion with non-matched blood occurs, the patient risks red blood cell destruction, renal failure, shock, and death.
Key Terms
hemolysis: The destruction of red blood cells from pathological causes, such as infection or immune system mediated damage.
agglutinate: The act of red blood cells clumping together due to antibody reactivity.
Transfusion medicine is extremely effective at treating those with severe blood loss. Transfusions are often a required component of major surgeries. Due to the different antigen blood types, blood must be cross-matched during processing to avoid potential complications.
The Cross-Matching Process
Much of the routine work of a blood bank involves testing blood from both donors and recipients to ensure that every recipient is given blood that is compatible and is as safe as possible. Several laboratory tests allow cross-matching of compatible blood between donor and recipient. Patients should ideally receive their own blood or type-specific blood products to minimize the chance of a transfusion reaction. Risks can be further reduced by cross-matching blood, but this process isn’t always performed if time is short and the need for transfusion has not been anticipated.
Agglutinated RBC: Red blood cells can agglutinate if the serum contains antibodies against the expressed proteins. In this image, the blood serum contains anti-A3 antibodies, which attack and agglutinate type A blood.
Cross-matching involves mixing a sample of the recipient’s serum with a sample of the donor’s red blood cells and checking if the mixture agglutinates, or forms clumps. These clumps are the result of antibodies binding the red blood cells together. If agglutination is not obvious by direct vision, blood bank technicians check for agglutination with a microscope. If agglutination occurs, that particular donor’s blood cannot be transfused to that particular recipient. In a blood bank, it is vital that all blood specimens are correctly identified, so labeling has been standardized using a barcode system known as ISBT 128. The blood group may be included on identification by military personnel in case they need an emergency blood transfusion.
Potential Transfusion Complications
If a patient receives blood during a transfusion that is not compatible with his or her blood type, severe problems can occur. Acute hemolytic transfusion reactions occur if donated blood cells are attacked by matching host antibodies. This can cause shock-like symptoms, such as fever, hypotension, and disseminated intravascular coagulation from immune system-mediated endothelial damage. Transfusion reactions are also associated with acute renal failure. Lung injury is common as well, due to pulmonary edema from fluid overload if plasma volume becomes too high or neutrophil activation during a transfusion reaction. If the donated blood is contaminated with bacteria, it may induce septic shock in the patient.
Transfusion adverse events
Negative reactions to receiving a blood transfusion are very rare. They are known as ‘transfusion adverse events’.
Most transfusion adverse events are mild – such as itching, fever, hives or rash – and can be treated easily. The most common adverse reaction to a blood transfusion is a mild fever, which occur in less than one in 1,000 transfusions. Most transfusion adverse events occur within 24 hours of a transfusion.
Severe reactions are very rare, but can be life-threatening. They need immediate treatment. A severe reaction may involve:
breathing difficulties – which may be caused by severe allergic reaction (anaphylaxis), bacterial infection, red cell breakdown or transfusion-related acute lung injury (TRALI)
high fever and shaking
low blood pressure
dark urine
aches and pains.
If you experience any symptoms of a negative reaction to transfusion, let your health care team know immediately.
Complications
There are multiple complications of blood transfusions, including infections, hemolytic reactions, allergic reactions, transfusion-related lung injury (TRALI), transfusion-associated circulatory overload, and electrolyte imbalance.[rx][rx][rx]
According to the American Association of Blood Banks (AABB), febrile reactions are the most common, followed by transfusion-associated circulatory overload, allergic reaction, TRALI, hepatitis C viral infection, hepatitis B viral infection, human immunodeficiency virus (HIV) infection, and fatal hemolysis which is extremely rare, only occurring almost 1 in 2 million transfused units of RBC.
For comparison, the lifetime odds of dying from a lightning strike are about 1 in 161,000.
List of approximate risk per unit transfusion of RBC (adapted from AABB clinical guidelines published JAMA November 15, 2016).[rx]
Adverse Event and Approximate Risk Per Unit Transfusion of RBC
Human immunodeficiency virus infection: 1:1,467,000
Fatal hemolysis: 1:1,972,000
Febrile reactions are the most common transfusion adverse event. Transfusing with leukocyte-reduced blood products, which most blood products in the United States are, may help reduce febrile reactions. If this occurs, the transfusion should be halted, and the patient evaluated, as a hemolytic reaction can initially appear similar and consider performing a hemolytic or infectious workup. The treatment is with acetaminophen and, if needed, diphenhydramine for symptomatic control. After treatment and exclusion of other causes, the transfusion can be resumed at a slower rate.
Transfusion-associated circulatory overload is characterized by respiratory distress secondary to cardiogenic pulmonary edema. This reaction is most common in patients who are already in a fluid overloaded state, such as congestive heart failure or acute renal failure. Diagnosis is based on symptom onset within 6 to 12 hours of receiving a transfusion, clinical evidence of fluid overload, pulmonary edema, elevated brain natriuretic peptide, and response to diuretics.
Preventive efforts, as well as treatment, include limiting the number of transfusions to the lowest amount necessary, transfusing over the slowest possible time and administering diuretics before or between transfusions.
Allergic reaction, often manifested as urticaria and pruritis, occurs in less than 1% of transfusions. More severe symptoms, such as bronchospasm, wheezing, and anaphylaxis are rare. Allergic reactions may be seen in patients who are IgA deficient as exposure to IgA in donor products can cause a severe anaphylactoid reaction. This can be avoided by washing the plasma from the cells prior to transfusion. Mild symptoms, such as pruritis and urticaria can be treated with antihistamines. More severe symptoms can be treated with bronchodilators, steroids, and epinephrine.
Transfusion-related lung injury (TRALI) is uncommon, occurring in about 1:12,000 transfusion. Patients will develop symptoms within 2 to 4 hours after receiving a transfusion. Patients will develop acute hypoxemic respiratory distress, similar to acute respiratory distress syndrome (ARDS). Patients will have pulmonary edema without evidence of left heart failure, normal CVP. Diagnosis is made based on a history of recent transfusion, chest x-ray with diffuse patchy infiltrates, and the exclusion of other etiologies. While there is a 10% mortality, the remaining 90% will resolve within 96 hours with supportive care only.
Infections are a potential complication. The risk of infections has been decreased due to the screening of potential donors so that hepatitis C and human immunodeficiency virus risk are less than 1 in a million. Bacterial infection can also occur, but does so rarely, about once in every 250,000 units of red cells transfused.
Fatal hemolysis is extremely rare, occurring only in 1 out of nearly 2 million transfusions. It is the result of ABO incompatibility, and the recipient’s antibodies recognize and induce hemolysis in donor’s transfused cells. Patients will develop an acute onset of fevers and chills, low back pain, flushing, dyspnea as well as becoming tachycardic and going into shock. Treatment is to stop the transfusion, leave the IV in place, intravenous fluids with normal saline, keeping urine output greater than 100 mL/hour, diuretics may also be needed and cardiorespiratory support as appropriate. A hemolytic workup should also be performed which includes sending the donor blood and tubing as well as post-transfusion labs (see below for list) from the recipient to the blood bank.
Retype and crossmatch
Direct and indirect Coombs tests
Complete blood count (CBC), creatinine, PT, and PTT (draw from the other arm)
Electrolyte abnormalities can also occur, although these are rare, and more likely associated with large volume transfusion.
Hypocalcemia can result as citrate, an anticoagulant in blood products binds with calcium.
Hyperkalemia can occur from the release of potassium from cells during storage. Higher risk in neonates and patients with renal insufficiency.
Hypokalemia can result as a result of alkalinization of the blood as citrate is converted to bicarbonate by the liver in patients with normal hepatic function.
Anatomy of Hemostasis/Hemostasis is the natural process that stops blood loss when an injury occurs.It involves three steps: (1) vascular spasm ( vasoconstriction ); (2) platelet plug formation; and (3) coagulation. Vasoconstriction is a reflex in which blood vessels narrow to increase blood pressure.
Hemostasis or hemostasis is a process to prevent and stop bleeding, meaning to keep blood within a damaged blood vessel (the opposite of hemostasis is hemorrhage). It is the first stage of wound healing. This involves coagulation, blood changing from a liquid to a gel. Intact blood vessels are central to moderating blood’s tendency to form clots. The endothelial cells of intact vessels prevent blood clotting with a heparin-like molecule and thrombomodulin and prevent platelet aggregation with nitric oxide and prostacyclin. When an endothelial injury occurs, the endothelial cells stop the secretion of coagulation and aggregation inhibitors and instead secrete the von Willebrand factor, which initiates the maintenance of hemostasis after injury. Hemostasis has three major steps: 1) vasoconstriction, 2) temporary blockage of a break by a platelet plug, and 3) blood coagulation or formation of a fibrin clot. These processes seal the hole until tissues are repaired.
Overview of Hemostasis
Hemostasis is the natural process that stops blood loss when an injury occurs.
Pharmaceutical agents currently used to treat hemostatic disorders
Drug
Trade name
Targeted molecule/system
Clinical use
acetylsalicylic acid
Aspirin
cyclo-oxygenase, TXA2 synthesis
block platelet aggregation, arterial thrombosis
clopidogrel
Plavix
ADP receptor P2Y12
block platelet activation, arterial thrombosis
prasugrel
Effient
ADP receptor P2Y12
block platelet activation, arterial thrombosis
abciximab
ReoPro
integrin αIIbβ3
block platelet aggregation, arterial thrombosis
eptifibatide
Integrilin
integrin αIIbβ3
block platelet aggregation, arterial thrombosis
tirofiban
Aggrastat
integrin αIIbβ3
block platelet aggregation, arterial thrombosis
dipyridamole
Persantine
adenosine reuptake
block platelet activation, arterial thrombosis
unfractionated heparin
Heparin
thrombin, factor Xa
blocks coagulation, venous thrombosis
low molecular weight heparin
several names, e.g. Lovenox
factor Xa
blocks coagulation, venous thrombosis
fondaparinux
Arixtra
factor Xa
blocks coagulation, venous thrombosis
rivaroxaban
Xarelto
factor Xa
blocks coagulation, venous thrombosis
argatroban
Argatroban
thrombin
prevent thrombosis during percutaneous coronary intervention (PCI)
dabigatran
Pradaxa
thrombin
prevent thrombosis during/after joint surgery
bivalirudin
Angiomax
thrombin
prevent thrombosis during PCI
lepirudin
Refludan
thrombin
prevent thrombosis in patients with heparin- induced thrombocytopenia
desirudin
Iprivask
thrombin
venous thrombosis during/after joint surgery
coumarin derivatives
several names, e.g. Coumadin
vitamin K antagonist
venous thrombosis, long-term prophylaxis
factor VIII
multiple names
replace factor VIII
hemophilia A
factor IX
multiple names
replace factor IX
hemophilia B
desmopressin
several names, e.g. DDAVP
von Willebrand factor
von Willebrand disease
tranexamic acid
Lysteda
fibrinolysis
von Willebrand disease
von Willebrand factor
Humate-P
von Willebrand factor
von Willebrand disease
Key Points
Hemostasis is the natural process that stops blood loss when an injury occurs.It involves three steps: (1) vascular spasm ( vasoconstriction ); (2) platelet plug formation; and (3) coagulation.
Vasoconstriction is a reflex in which blood vessels narrow to increase blood pressure.
Next, platelet plug formation involves the activation, aggregation, and adherence of platelets into a plug that serves as a barrier against blood flow.
Coagulation involves a complex cascade in which a fibrin mesh is cleaved from fibrinogen.
Fibrin acts as a “molecular glue” during clot formation, holding the platelet plug together.
Key Terms
hemostasis: The process of slowing and stopping the flow of blood to initiate wound healing.
coagulation: The process by which blood forms gelatinous clots.
heparin: A fibrinolytic molecule expressed on endothelial cells or produced as a blood thinner medicine. It prevents the activation of platelets and clotting factors.
Hemostasis is the natural process in which blood flow slows and clot forms to prevent blood loss during an injury, with hemo- meaning blood, and stasis meaning stopping. During hemostasis, blood changes from a fluid liquid to a gelatinous state.
Mechanism
Vaso Constriction. Within about 30 minutes of damage/trauma to the blood vessels, an avascular spasm ensues, which leads to vasoconstriction. At the site of the disrupted endothelial lining, the extracellular matrix (ECM)/ collagen becomes exposed to the blood components.[rx]
Platelet Adhesion. This ECM releases cytokines and inflammatory markers that lead to adhesion of the platelets and their aggregation at that site which leads to the formation of a platelet plug and sealing of the defect. Platelet adhesion is a complex process mediated by interactions between various receptors and proteins including tyrosine kinase receptors, glycoprotein receptors, other G-protein receptors as well as the von Willebrand Factor (vWF). The von Willebrand Factor functions via binding to the Gp 1b-9 within the platelets.[rx]
Platelet Activation. The platelets that have adhered undergo very specific changes. They release their cytoplasmic granules that include ADP, thromboxane A2, serotonin, and multiple other activation factors. They also undergo a transformation of their shape into a pseudopodal shape which in turn leads to release reactions of various chemokines. P2Y1 receptors help in the conformational changes in platelets.[rx]
Platelet Aggregation. With the mechanisms mentioned above, various platelets are activated, adhered to each other, and the damaged endothelial surface leading to the formation of a primary platelet plug.
Extrinsic Pathway. The tissue factor binds to factor VII and activates it. The activated factor VII (factor VIIa) further activates factor X and factor IX via proteolysis. Activated factor IX (factor IXa) binds with its cofactor–activated factor VIII (factor VIIa), which leads to the activation of factor X (factor Xa). Factor Xa binds to activated factor V (factor Va) and calcium and generates a prothrombinase complex that cleaves the prothrombin into thrombin.[rx]
Intrinsic Pathway. With thrombin production, there occurs conversion of factor XI to activated factor XI (factor XIa). Factor XIa with activated factor VII and tissue factor converts factor IX to activated factor IX (factor IXa). The activated factor IX combines with activated factor VIII (factor VIIIa) and activates factor X. Activated factor X (factor Xa) binds with activated factor V (factor Va) and converts prothrombin to thrombin. Thrombin acts as a cofactor and catalysis and enhances the bioactivity of many of the aforementioned proteolytic pathways.[rx]
Fibrin Clot Formation. The final steps in the coagulation cascade involve the conversion of fibrinogen to fibrin monomers which polymerizes and forms fibrin polymer mesh and result in a cross-linked fibrin clot. This reaction is catalyzed by activated factor XIII (factor XIIIa) that stimulates the lysine and the glutamic acid side chains causing cross-linking of the fibrin molecules and formation of a stabilized clot.
Clot Resolution (Tertiary Hemostasis). Activated platelets contract their internal actin and myosin fibrils in their cytoskeleton, which leads to shrinkage of the clot volume. Plasminogen then activates to plasmin, which promotes lysis of the fibrin clot; this restores the flow of blood in the damaged/obstructed blood vessels.[rx]
Steps of Hemostasis
Hemostasis includes three steps that occur in a rapid sequence: (1) vascular spasm, or vasoconstriction, a brief and intense contraction of blood vessels; (2) formation of a platelet plug; and (3) blood clotting or coagulation, which reinforces the platelet plug with fibrin mesh that acts as a glue to hold the clot together. Once blood flow has ceased, tissue repair can begin.
Angiogenesis Generates New Blood Vessels: Blood vessel with an erythrocyte (red blood cell) within its lumen, endothelial cells forming its tunica intima or inner layer, and pericytes forming its tunica adventitia (outer layer).
Vasoconstriction
Intact blood vessels are central to moderating blood’s clotting tendency. The endothelial cells of intact vessels prevent clotting by expressing a fibrinolytic heparin molecule and thrombomodulin, which prevents platelet aggregation and stops the coagulation cascade with nitric oxide and prostacyclin. When the endothelial injury occurs, the endothelial cells stop the secretion of coagulation and aggregation inhibitors and instead secrete von Willebrand factor, which causes platelet adherence during the initial formation of a clot. The vasoconstriction that occurs during hemostasis is a brief reflexive contraction that causes a decrease in blood flow to the area.
Platelet Plug Formation
Platelets create the “platelet plug” that forms almost directly after a blood vessel has been ruptured. Within twenty seconds of an injury in which the blood vessel’s epithelial wall is disrupted, coagulation is initiated. It takes approximately sixty seconds until the first fibrin strands begin to intersperse among the wound. After several minutes, the platelet plug is completely formed by fibrin.
Contrary to popular belief, clotting of a skin injury is not caused by exposure to air, but by platelets adhering to and being activated by collagen in the blood vessels’ endothelium. The activated platelets then release the contents of their granules, which contain a variety of substances that stimulate further platelet activation and enhance the hemostatic process.
When the lining of a blood vessel breaks and endothelial cells are damaged, revealing subendothelial collagen proteins from the extracellular matrix, thromboxane causes platelets to swell, grow filaments, and start clumping together, or aggregating. Von Willebrand’s factor causes them to adhere to each other and the walls of the vessel. This continues as more platelets congregate and undergo these same transformations. This process results in a platelet plug that seals the injured area. If the injury is small, the platelet plug may be able to form within several seconds.
Coagulation Cascade
If the platelet plug is not enough to stop the bleeding, the third stage of hemostasis begins the formation of a blood clot. Platelets contain secretory granules. When they stick to the proteins in the vessel walls, they degranulate, thus releasing their products, which include ADP (adenosine diphosphate), serotonin, and thromboxane A2 (which activates other platelets).
First, blood changes from a liquid to a gel. At least 12 substances called clotting factors or tissue factors take part in a cascade of chemical reactions that eventually create a mesh of fibrin within the blood. Each of the clotting factors has a very specific function. Prothrombin, thrombin, and fibrinogen are the main factors involved in the outcome of the coagulation cascade. Prothrombin and fibrinogen are proteins that are produced and deposited in the blood by the liver.
When blood vessels are damaged, vessels and nearby platelets are stimulated to release a substance called prothrombin activator, which in turn activates the conversion of prothrombin, a plasma protein, into an enzyme called thrombin. This reaction requires calcium ions. Thrombin facilitates the conversion of a soluble plasma protein called fibrinogen into long, insoluble fibers or threads of the protein, fibrin. Fibrin threads wind around the platelet plug at the damaged area of the blood vessel, forming an interlocking network of fibers and a framework for the clot. This net of fibers traps and helps hold platelets, blood cells, and other molecules tight to the site of injury, functioning as the initial clot. This temporary fibrin clot can form in less than a minute and slows blood flow before platelets attach.
Next, platelets in the clot begin to shrink, tightening the clot and drawing together the vessel walls to initiate the process of wound healing. Usually, the whole process of clot formation and tightening takes less than a half hour.
Vascular Spasm
Vasoconstriction is the narrowing of the blood vessels, which reduces blood loss during injury.
Key Points
Vasoconstriction is the narrowing of the blood vessels, which increases blood pressure but can decrease blood flow and loss.
Vasoconstriction is mediated by the contraction of the smooth muscles lining a blood vessel.
Vasoconstriction is caused by thromboxane A2 from activated platelets and injured epithelial cells, nervous system reflexes from pain, and direct injury to vascular smooth muscle.
Vasopressins are drugs that may induce vasoconstriction and increase blood pressure.
Vasoconstriction only lasts for a few minutes during hemostasis. During inflammation that follows the injury, it is replaced by vasodilation as the healing process begins.
Key Terms
endothelial cells: The endothelium comprises the thin layer of endothelial cells
that lines the interior surface of blood and lymphatic vessels, forming an interface between circulating blood or lymph in the lumen and the rest of the vessel wall.
vascular: Of, pertaining to, or containing vessels that conduct or circulate fluids such as blood, lymph, or sap through the body of an animal or plant.
inflammation: A process that occurs during injury and generally follows hemostasis in which vasoconstriction ends and vasodilation begins.
Vasoconstriction is the narrowing of the blood vessels resulting from the contraction of the smooth muscle wall of the vessels, particularly in the large arteries and small arterioles. The process is the opposite of vasodilation, the dilation, and the expansion of blood vessels. During hemostasis, a brief spasm of vasoconstriction occurs, which slows blood flow into the injured area while the clot forms.
Vasoconstriction during hemostasis: Blood vessel experiencing vasoconstriction as its smooth muscle contracts while the blood clot forms.
Mechanisms of Vasoconstriction
The vasoconstriction response is triggered by factors such as a direct injury to vascular smooth muscle, signaling molecules released by injured endothelial cells and activated platelets (such as thromboxane A2), and nervous system reflexes initiated by local pain receptors. The spasm response becomes more effective as the amount of damage is increased. Vascular spasm is much more effective at slowing the flow of blood in smaller blood vessels. Vasoconstriction also causes an increase in blood pressure for affected blood vessels.
Smooth muscle in the vessel wall goes through intense contractions that constrict the vessel. If the vessels are small, spasms compress the inner walls together and may be able to stop the bleeding completely. If the vessels are medium to large-sized, the spasms slow down the immediate outflow of blood, lessening the damage but still preparing the vessel for the later steps of hemostasis. The spasm response becomes stronger and lasts longer in more severe injuries. Vasoconstriction may be induced by drugs called vasopressins, which increase blood pressure and can help treat certain conditions.
Injury and Inflammation
During injury, vasoconstriction is brief, lasting only a few minutes while the platelet plug and coagulation cascade occur. This is because as tissues are damaged during an injury, inflammation occurs as a result of inflammatory mediator release from immune system cells (such as mast cells or NK cells) that receive cell stress cytokines from damaged endothelial cells or vasoactive amines (serotonin) that are secreted by activated platelets. During inflammation, vasodilation occur, along with increased vascular permeability and leukocyte chemotaxis, ending the spasm of vasoconstriction and hemostasis as wound healing begins.
Platelet Plug Formation
At the site of vessel injury, platelets stick together to create a plug, which is the beginning of blood clot formation.
Key Points
Platelets adhere to the damaged endothelium to form a platelet plug, temporarily sealing the break in the vessel wall.
Activated platelets release factors to stimulate further platelet activation, perpetuating plug formation in a positive feedback loop, while other factors stimulate the coagulation cascade and maintain vasoconstriction.
Platelets adhere to the collagen fibers in the vessel wall
by becoming adhesive and filamentous
due to the stimulus of von Willebrand factor.
During platelet aggregation, platelets bind to von Willebrand factor and fibrinogen to stick together and seal the break in the endothelium.
Key Terms
von Willebrand Factor: The factor responsible for causing platelet adherence and aggregation. It is increased by positive feedback during platelet activation.
collagen: A glycoprotein that forms elongated fibers, usually found in the extracellular matrix of connective tissue such as the matrix beneath the vascular endothelium.
The second critical step in hemostasis, which follows vasoconstriction, is platelet plug formation. The three steps to platelet plug formation are platelet adherence, activation, and aggregation.
Platelet Adherence
Platelets: A blood slide of platelets aggregating or clumping together. The platelets are small, bright purple fragments.
Normally, the endothelial cells express molecules that inhibit platelet adherence and activation while platelets circulate through the blood vessels. These molecules include nitric oxide, prostacyclin (PGI2), and endothelial ADP-use.
During an injury, subendothelial collagen from the extracellular matrix beneath the endothelial cells is exposed to the epithelium as the normal epithelial cells are damaged and removed, which releases von Willebrand Factor (VWF). VWF causes the platelets to change form with adhesive filaments (extensions) that adhere to the subendothelial collagen on the endothelial wall.
Platelet Activation
After platelet adherence occurs, the subendothelial collagen binds to receptors on the platelet, which activates it. During platelet activation, the platelet releases a number of important cytokines and chemical mediators via degranulation. The released chemicals include ADP, VWF, thromboxane A2, platelet-derived growth factor (PDGF), vascular endothelial growth factor (VEGF), serotonin, and coagulation factors. The extra ADP and VWF is especially important because it causes nearby platelets to adhere and activate, as well as release more ADP, VWF, and other chemicals. Platelet plug formation is considered a positive feedback process because ADP and VWF levels are successively increased as more and more platelets activate to form the plug.
ADP: The chemical structure of ADP, a molecule that causes platelet activation and is involved in the positive feedback component of platelet activation.
The other factors released during platelet activation perform other important functions. Thromboxane is an arachidonic acid derivative (similar to prostaglandins) that activates other platelets and maintains vasoconstriction. Serotonin is a short-lived inflammatory mediator with a vasoconstrictive effect that contributes to vascular changes associated with inflammation during an injury. PDGF and VEGF are involved in angiogenesis, the growth of new blood vessels, and cell cycle proliferation (division) following injury. The coagulation factors include factors V and VIII, which are involved in the coagulation cascade that converts fibrinogen into fibrin mesh after platelet plug formation.
Platelet Aggregation
The final step of platelet plug formation is an aggregation of the platelets into a barrier-like plug. Receptors on the platelet bind to VWF and fibrinogen molecules, which hold the platelets together. Platelets may also bind to subendothelial VWF to anchor them to the damaged endothelium. The completed plug will cover the damaged components of the endothelium and will stop blood from flowing out of it, but if the wound is large enough, blood will not coagulate until the fibrin mesh from the coagulation cascade is produced, which strengthens the platelet plug. If the wound is minor, the platelet plug may be enough to stop the bleeding without the coagulation cascade.
Coagulation
Coagulation is the process by which a blood clot forms to reduce blood loss after damage to a blood vessel.
Key Points
The coagulation cascade is a series of reactions, which is classically divided into three pathways: the contact (also known as the intrinsic) pathway, the tissue factor (also known as the extrinsic pathway), and the common pathway.
The intrinsic pathway occurs when negatively charged molecule contact causes a cascade of factors that produce factor X. The extrinsic pathway occurs when tissue damage causes the release of tissue factor, creating a smaller cascade that produces factor X. The common pathway merges both pathways as factor X is used to create thrombin from prothrombin.
Secondary hemostasis involves factors of the coagulation cascade, which collectively strengthen the platelet plug.
Coagulation can be harmful if blood clots embolize and obstruct other blood vessels. Clots can also occur if blood pools from prolonged immobility.
A number of anticoagulants exist to inhibit various parts of the coagulation cascade, inactivate thrombin, or degrade fibrin directly.
Key Terms
fibrin: An elastic, insoluble, whitish protein produced by the action of thrombin on fibrinogen and forming an interlacing fibrous network in the coagulation of blood.
endothelium: A thin layer of flat epithelial cells that lines the heart, serous cavities, lymph vessels, and blood vessels.
thrombin: The end product of the coagulation cascade, which cleaves fibrin from fibrinogen.
Coagulation is the process by which a blood clot forms to reduce blood loss after damage to a blood vessel. Several components of the coagulation cascade, including both cellular (e.g. platelets) and protein (e.g. fibrin) components, are involved in blood vessel repair. The role of the cellular and protein components can be categorized as primary hemostasis (the platelet plug) and secondary hemostasis (the coagulation cascade). The coagulation cascade is classically divided into three pathways: the contact (also known as the intrinsic) pathway, the tissue factor (also known as the extrinsic pathway), and the common pathway. Both the contact pathway and the tissue factor feed into and activate the common pathway.
Coagulation Pathway
Secondary Hemostasis
Hemostasis can either be primary or secondary. Primary hemostasis refers to platelet plug formation, which forms the primary clot. Secondary hemostasis refers to the coagulation cascade, which produces a fibrin mesh to strengthen the platelet plug. Secondary hemostasis occurs simultaneously with primary hemostasis, but generally finishes after it. The coagulation factors circulate as inactive enzyme precursors, which, upon activation, take part in the series of reactions that make up the coagulation cascade. The coagulation factors are generally serine proteases (enzymes).
Coagulation Cascade
Intrinsic Pathway
The intrinsic pathway (contact activation pathway) occurs during exposure to negatively charged molecules, such as molecules on bacteria and various types of lipids. It begins with formation of the primary complex on collagen by high-molecular-weight kininogen (HMWK), prekallikrein, and factor XII (Hageman factor). This initiates a cascade in which factor XII is activated, which then activates factor XI, which activated factor IX, which along with factor VIII activates factor X in the common pathway.
Extrinsic Pathway
The main role of the extrinsic (tissue factor) pathway is to generate a “thrombin burst,” a process by which large amounts of thrombin, the final component that cleaves fibrinogen into fibrin, is released instantly. The extrinsic pathway occurs during tissue damage when damaged cells release tissue factor III. Tissue factor III acts on tissue factor VII in circulation and feeds into the final step of the common pathway, in which factor X causes thrombin to be created from prothrombin.
Common Pathway
In the final common pathway, prothrombin is converted to thrombin. When factor X is activated by either the intrinsic or extrinsic pathways, it activates prothrombin (also called factor II) and converts it into thrombin using factor V. Thrombin then cleaves fibrinogen into fibrin, which forms the mesh that binds to and strengthens the platelet plug, finishing coagulation and thus hemostasis. It also activates more factor V, which later acts as an anticoagulant with inhibitor protein C, and factor XIII, which covalently bonds to fibrin to strengthen its attachment to the platelets.
Coagulation Problems
While the coagulation cascade is critical for hemostasis and wound healing, it can also cause problems. An embolism is any thrombosis (blood clot) that breaks off without being dissolved and travels through the bloodstream to another site. If it obstructs an artery that supplies blood to a tissue or organ, it can cause ischemia and infarcation to those tissues, leading to a pulmonary embolism, stroke, or heart attack).
Coagulation can occur even without injury, as blood pooling from prolonged immobility can cause clotting factors to accumulate and activate a coagulation cascade independently. Additionally, endothelial damage caused by immune system factors like inflammation or hypersensitivity may also cause unnecessary thrombosis and embolism. For example, during severe bacterial infections (septic shock), inflammation-induced tissue damage and the negatively charged molecules of bacteria activate both pathways of the coagulation cascade and cause disseminated intravascular coagulation (DIC), in which many clots form and break off, leading to massive organ failure.
Anticoagulants
Many anticoagulants prevent unnecessary coagulation, and those that genetically lack the ability to produce these molecules will be more susceptible to coagulation. These mechanisms include:
Protein C: a vitamin K-dependent serine protease enzyme that degrades Factor V and factor VIII.
Antithrombin: a serine protease inhibitor that degrades thrombin, Factor IXa, Factor Xa, Factor XIa, and Factor XIIa.
Tissue factor pathway inhibitor (TFPI): limits the action of tissue factor (TF) and the factors it produces.
Plasmin: generated by proteolytic cleavage of plasminogen, a potent fibrinolytic that degrades fibrin and destroys clots.
Prostacyclin (PGI2): released by the endothelium and inhibits platelet activation.
Thrombomodulin: released by the endothelium and converts thrombin into an inactive form.
Role of Vitamin K
Vitamin K is an essential factor of the coagulation cascade.
Key Points
Vitamin K is involved in the synthesis of many factors of the coagulation cascade.
Vitamin K is antagonized (inhibited) by the anticoagulant drug warfarin.
Calcium and phospholipids are needed to activate tenase, which converts prothrombin to thrombin.
Both calcium and vitamin K are needed to synthesize Protein C, an anticoagulant that prevents excessive coagulation after the coagulation cascade occurs.
Deficiency of any of these clotting cofactors will cause an impaired ability for blood to coagulate, which can contribute to excessive bleeding and hemorrhage.
Key Terms
warfarin: An anticoagulant medication that is used for the prophylaxis of thrombosis and embolism in many disorders.
tenase: An enzyme activated by a calcium and phospholipid complex that converts prothrombin to thrombin in the common pathway.
Coagulation is a complex cascade that requires many different cofactors and molecules to occur. Vitamin K, calcium, and phospholipids are necessary cofactors for proper coagulation, and people deficient in these substances will be more susceptible to uncontrolled bleeding.
Blood Coagulation Pathways: Blood coagulation pathways in vivo showing the central role played by thrombin.
Vitamin K
Vitamin K is a fat-soluble vitamin necessary for the synthesis of coagulation factors involved in the coagulation cascade. Factors II, VII, IX, and X are all important for the intrinsic and common pathways of coagulation. Vitamin K also synthesizes Protein C, Protein S, and Protein Z, anticoagulant proteins that degrade specific coagulation factors, preventing excessive thrombosis following the initial coagulation cascade.
Vitamin K can be inhibited by the anticoagulant drug warfarin, which acts as an antagonist for vitamin K. Warfarin is used in medicine for those at high risk of thromboembolism to prevent coagulation cascade by reducing vitamin K dependent synthesis of coagulation factors. Warfarin’s effects can be overcome by ingesting more vitamin K to reactivate the coagulation factor synthesis pathway.
Vitamin K deficiency is associated with impaired coagulation function and excessive bleeding and hemorrhage (internal bleeding, often severe). This can be caused by poor diet, malabsorption in the intestines, or liver failure. Those with vitamin K deficiency produce alternative proteins that improperly bind with phospholipids, which also contributes to the lack of coagulant function.
Calcium and Phospholipids
Calcium and phospholipids (a platelet membrane constituent) are required cofactors for prothrombin activation enzyme complexes to function. This enzyme is called tenase, and converts prothrombin to thrombin. Calcium mediates the binding of the tenase enzyme complexes (via the terminal gamma-carboxy residues on FXa and FIXa) to the phospholipid surfaces expressed by platelets, which in turn activates prothrombin to produce thrombin, which then produces fibrin from fibrinogen. Calcium acts as a catalyst for this reaction, speeding up the rate of the reaction to occur within the time frame of the factors involved in the coagulation cascade. Calcium is also required to synthesize the anticoagulant Protein C (along with vitamin K).
Calcium deficiencies inhibit proper blood coagulation. This can be caused by a nutritional deficiency or acute problems in which calcium is allocated elsewhere in the blood. Phospholipid deficiency is also associated with thrombocytopenia (platelet deficiency) because the phospholipids involved with clotting come from platelets. Thrombocytopenia causes more severe issues with blood clotting as the platelet plug will not be able to form or activate the coagulation cascade.
Clot Retraction and Repair
Clot retraction is the shrinking of a blood clot facilitated by thrombolytic agents.
Key Points
Clot retraction is dependent on the release of multiple coagulation factors, specifically Factor XIIIa at the end of the coagulation cascade.
The formation of blood clots can cause a number of serious diseases. By breaking down the clot, the disease process can be arrested or the complications reduced.
Clot retraction is the “shrinking” of a blood clot over a number of days. The edges of the blood vessel wall at the point of injury are slowly brought together to repair the damage.
Clot retraction occurs due to the contraction, knotting, and twisting of the fibrin mesh.
The steps of wound healing that follow clot retraction include inflammation, tissue proliferation, collagen and granulation tissue deposition, angiogenesis, wound contraction, and epithelialization.
Key Terms
Clot retraction: The shrinking of a blood clot over the day following initial clot formation.
angiogenesis: Growth of new blood vessels during wound healing.
thrombus: Ablood clot formed from platelets and other elements that forms in a blood vessel in a living organism. It may cause thrombosis or obstruction of the vessel at its point of formation or travel to other areas of the body
The blood clots produced in hemostasis are merely the first step in repair and healing that occur after injury. Following a clot, inflammation draws leukocytes to the injury site to eliminate any pathogens that may have entered the body during the initial injury. Then, over the course of the next 24 hours, the clot retracts as tissue healing begins.
Clot Retraction
As the healing process occurs following blood clot formation, the clot must be destroyed in order to prevent thromboembolic events, in which clots break off from the endothelium and cause ischemic damage elsewhere in the body. By reducing the size of and breaking down the clot, the disease process can be arrested or the complications reduced.
Clot retraction refers to a regression in the size of the blood clot over a number of days. During this process, the edges of the endothelium at the point of injury are slowly brought together again to repair the damage. Clot retraction is dependent on the release of multiple coagulation factors released at the end of the coagulation cascade, most notably factor XIIIa cross-links. These factors cause the fibrin mesh to contract by forming twists and knots that condense the size of the clot. Clot retraction generally occurs within 24 hours of initial clot formation and decreases the size of the clot by 90%. Following clot retraction, a separate process called fibrinolysis occurs which degrades the fibrin of the clot while macrophages consume the expended platelets, thus preventing possible thromboembolism.
Wound Healing
While the clot retracts, the wound begins to heal. The first step of wound healing is epithelial cell migration, which forms a scab before the clot retracts. This occurs due to the stimulus of platelet-derived growth factor (PDGF). After clot retraction, true repair begins as tissue proliferation starts and collagen from the extracellular matrix is deposited in the wound while granulation tissue forms. Then new blood vessels grow into the healing tissue in a process called angiogenesis, which is stimulated by vascular endothelial growth factor (VEGF). The wound itself contracts, reducing in size. After these steps occur, new epithelial cells grow to cover the wound. If the wound was severe or unevenly shaped, or if healing takes too long, scarring may occur from collagen deposition. Most scarring on the skin is benign, but scarring inside the tissues of organs such as the heart or the lungs can cause health problems.
Fibrinolysis
Fibrinolysis is a process of breaking down clots in order to prevent them from growing and becoming problematic.
Key Points
Fibrinolysis is the breakdown of a fibrin clot.
Plasmin is the enzyme that breaks down fibrin. It is activated from inactive plasminogen by tissue plasminogen activator (tPA) and urokinase.
Tissue plasminogen activator (tPA) and urokinase are inhibited by plasminogen activator inhibitor-1 and plasminogen activator inhibitor-2 (PAI-1 and PAI-2).
Many drugs have fibrinolytic properties that can be used to treat uncontrolled clotting and embolism, including streptokinase, synthetic t-PA, aspirin, heparin, warfarin, and citrates.
Patients suspected to be having a blood clot-induced stroke should be screened for hemorrhage and aneurysm first since fibrinolytic treatment would help with a stroke but make bleeding conditions much more dangerous.
Key Terms
fibrin: An elastic, insoluble, whitish protein produced by the action of thrombin on fibrinogen and forming an interlacing fibrous network in the coagulation of blood.
protease: An enzyme that cuts or cleaves proteins.
Plasmin: A protease that breaks down plasmin. It is cleaved from inactive plasminogen.
Fibrinolysis is a process that removes clots following hemostasis and clot retraction, preventing uncontrolled thrombosis and embolism. There are two types of fibrinolysis: primary fibrinolysis and secondary fibrinolysis. Primary fibrinolysis is a normal body process, whereas secondary fibrinolysis is the breakdown of clots due to a medication, medical disorder, or other cause.
Mechanisms of Primary Fibrinolysis
Primary fibrinolysis normally occurs following clot retraction, in which the clot has already condensed considerably in size. The main enzyme in primary fibrinolysis is plasmin, a proteolytic enzyme that degrades fibrin mesh. Plasmin cleaves fibrin at various places, leading to the production of circulating fragments that are cleared by other proteases or by the kidneys and liver.
Plasmin is produced in an inactive form, plasminogen, in the liver. Plasminogen cannot cleave fibrin and circulates in the bloodstream. Instead, it is incorporated into the clot when it is formed and then activated into plasmin later. Plasminogen is activated to plasmin by tissue plasminogen activator (t-PA) and urokinase, an enzyme found in the urine.
Fibrinolysis: Blue arrows denote stimulation and red arrows inhibition.
T-PA is released into the blood very slowly by the damaged endothelium of the blood vessels. T-PA and urokinase are themselves inhibited by plasminogen activator inhibitor-1 and plasminogen activator inhibitor-2 (PAI-1 and PAI-2). In contrast, plasmin further stimulates plasmin generation by producing more active forms of both tissue plasminogen activator (tPA) and urokinase. Following fibrin degradation by plasmin, old activated platelets from the platelet plug are phagocytized and destroyed by macrophages.
Alpha 2-antiplasmin and alpha 2-macroglobulin inactivate plasmin. Plasmin activity is also reduced by thrombin -activatable fibrinolysis inhibitor (TAFI), which modifies fibrin to make it more resistant to the tPA-mediated plasminogen. Plasmin operates on a negative feedback process because it is reduced when the fibrin clot is fully degraded.
Mechanisms of Secondary Fibrinolysis
Secondary fibrinolysis generally refers to the treatment of pathological thromboembolism. If blood clots embolize to different parts of the body, they can cause tissue death by blocking off blood flow to those tissues. This is a common cause of heart attacks, pulmonary embolism, and strokes. Several medications exist to help treat and prevent these conditions.
Fibrinolytic drugs include synthesized tissue plasminogen activator and streptokinase, a bacterial enzyme that has degraded fibrin directly. Clots may also be prevented or kept from worsening through the use of blood thinners ( anticoagulants ). Aspirin has anticoagulant properties because it inhibits cyclo-oxygenase-dependent pathways of platelet activation, which can prevent clotting from worsening. Heparin is a fast-acting anticoagulant produced by the body and used as a drug that inhibits the activity of thrombin. Warfarin inhibits vitamin K cofactor activation during the coagulation cascade, and citrates chelate calcium to prevent prothrombin activation into thrombin.
All of these treatments have been shown to have tremendous therapeutic benefits in treating those with thromboembolic diseases; however, they can make the injury much more difficult to treat by disrupting the clotting process. For example, patients thought to be suffering from a stroke (obstructed artery in the brain ) must be screened through imaging before given aspirin or a fibrinolytic drug, because if they have an aneurysm or hemorrhage (burst blood vessel or bleeding in the brain), administering fibrinolytic treatment would make their condition worse and possibly fatal by inhibiting the clotting that could save their lives.
Function
Hemodynamic Stability. Under normal circumstances, there exists a fine balance between the procoagulant and anticoagulant pathway. This mechanism ensures control of hemorrhage as needed and cessation of pro-coagulant pathway activation beyond the injury site/or without any bleeding. When this equilibrium becomes compromised under any condition, this may lead to thrombotic/bleeding complications.[rx] The hemostatic system also helps in wound healing.
Cardiovascular System. PGA1 and PGA2 cause peripheral arteriolar dilation. Prostacyclin produces vasodilation, and thromboxane A2 causes vasoconstriction. Prostacyclin inhibits platelet aggregation and produces vasodilation whereas thromboxane A2 and endoperoxides promote platelet aggregation and cause vasoconstriction. The balance between the prostacyclin and thromboxane A2 determines the degree of platelet plug formation. Thus, prostaglandins greatly influence temporary hemostasis.
Related Testing
Indications. The assessment of platelet function as well as its dysfunction has become vital in the current era in multiple clinical scenarios; several examples are:
For patients with clotting or bleeding disorders
For patients after cardiac stenting or stroke to monitor the activity of the antiplatelet agents
For perioperative evaluation.
Platelet Specific. Various tests have undergone development for platelet testing; they include[rx][rx]:
Bleeding time (BT)
Light transmission platelet aggregation
Impedance platelet aggregation
Global thrombosis test
PFA-100/200
VerifyNow system
Thromboelastography (TEG)
Flow cytometric analysis of platelet function
Coagulation Cascade Specific. There has been the development of various tests that evaluate specific events in the coagulation cascade.
They help in the determination of where the deficiency exists in the intrinsic, extrinsic, or the final common pathways as well as identification of qualitative or quantitative defects of the specific clotting factors.
Prothrombin time, developed in 1935, assesses the extrinsic and common coagulation cascade function.
Activated partial thromboplastin time assesses the intrinsic and the common pathways of coagulation.
Thrombin time evaluates the formation of fibrin in the final common pathway of coagulation.
The reptilase time and the various fibrinogen assays assess the fibrin formation step.
Mixing studies, factor activity assays, and factor inhibitor assays are special tests for further evaluation of the presence of inhibitors or antibodies as well as deficiency of factors.
Pathophysiology
General Principle. Virchow’s triad of hypercoagulability, vascular stasis, and vascular trauma, described in 1856, remains a true predictor of thrombosis.
Hypercoagulability
Stasis
Trauma
Etiologies. The physiology of coagulation undergoes alteration due to various factors, including:
Genetics
Medications
Procoagulant
Anticoagulation defects of the coagulation cascade
Quantitative defects of the integral components of the coagulation
Qualitative defects of the integral components of coagulation.
Clinical Presentations. With the altering of hemostatic physiology, various clinical outcomes including:
Pulmonary embolism
Deep vein thrombosis
Stroke
Myocardial infarction
Coagulopathies. Few of the disorders of coagulation include:
Anti-thrombin 3 deficiency,
Protein C deficiency,
Hyperhomocysteinemia,
Anti-phospholipid antibody syndrome
Risk Factors. Some acquired factors influencing the coagulation include[rx]:
Thrombocytes/ Platelets are the smallest blood cells, colorless cell fragments in our blood that form clots and stop or prevent bleeding. Typically around 2μm in diameter and anucleated, with an average lifespan of 7 to 10 days in humans. The platelet is a circulating anuclear fragment of a bone marrow megakaryocyte, 3 to 4 μm in diameter, with limited synthetic capability. The mean normal platelet count is between 250,000 and 260,000 cells/mm3, although there is a wide range of accepted normal values in most laboratories that extend as low as 150,000 to as high as 400,000/mm3.[rx][rx] Platelets are made in our bone marrow, the sponge-like tissue inside our bones. Bone marrow contains stem cells that develop into red blood cells, white blood cells, and platelets.
Platelets are small blood cells with several physiological purposes; the best studied is thrombosis activation. Through their clotting activity and activation of the coagulation cascade, they are crucial to maintaining adequate blood volume in those with vascular injury. The initiation of this activity begins with tissue injury and results in the release and binding of several glycoproteins, growth factors, and clotting factors. The complexity of these processes allows for many pharmacologic targets, which provides several options when it comes to antithrombotic therapy.[rx][rx][rx]
Platelet Count (PLT)
Just as it sounds, this is the actual number of platelets you have (per microliter of blood).
Low range: Less than 150,000 platelets per microliter
Normal range: 150,000 to 450,000 platelets per microliter1
Elevated range: 500,000 to 1,000,000 platelets per microliter
If your platelet count falls below 50,000, you may experience prolonged bleeding times.
Structure of Platelets
Platelets form by the fragmentation of megakaryocytes within the bone marrow. Megakaryocytes duplicate in the marrow without dividing, resulting in the production of giant cells. Within these giant cells, organelles organize into discrete domains, which will eventually become individual platelets, separated by a network of invaginating plasma membranes. These megakaryocytes are positioned next to the sinusoidal walls, such that shearing forces from circulating blood fragment the megakaryocyte cytoplasm into individual platelets and sweep these new platelets into the bloodstream.[rx]
Platelets circulate in the blood in discoid form but undergo significant structural changes following activation, mediated by actin and myosin within the cytoplasm. The platelets transform from discoid forms into compact spheres with dendritic extensions, which allow platelet adhesion. A variety of membrane-bound glycoprotein receptors facilitates the adhesion and aggregation of platelets.[rx]
As described above, platelets are anuclear but do contain RNA, ribosomes, mitochondria, and various granules, which are important in enacting platelet function.[rx] There are three distinct types of platelet granule
α-granules: the most abundant and largest secretory granules. They contain most of the platelet factors involved in hemostasis, including p-selectin, von Willebrand Factor, and fibrinogen[rx]
Dense granules: the smallest granules, which are visible on electron microscopy as dense bodies. They contain ADP and serotonin, as well as high levels of calcium
Lysosomes: contain hydrolytic enzymes including acid phosphatase and arylsulfatase[rx]
An ‘open canalicular system’ formed of deep surface membrane invaginations facilitates the secretion of granules.[rx] This system also has a key role in the transport of membrane receptors, allowing them to cluster, stabilize platelet adhesion sites, and amplify signals.[rx]
Structurally a platelet is divided into three zones
Peripheral zone – this zone is primarily involved in the adhesion and aggregation function
Glycocalyx – This is the thick carbohydrate-rich structure found on the exterior surface of platelets and serves as the site of the first contact during the hemostatic response by platelets, and it is made up of major and minor glycoproteins. GP-Ib-IX-V complex involved in adhesion at the site of vascular injury. GPIIb-IIIa is involved in aggregation by attachment through fibrinogen to other platelets.
Unit membrane – It is made of a lipid bilayer and open canalicular system, which serves a vital role in the acceleration of coagulation through the anionic phospholipid, phosphatidylserine, provided by the surface of activated platelets when clotting is initiated which converts prothrombin to thrombin.
The submembrane area – It plays a vital role in transmitting signals from the surface to organelles in the cytoplasm regulating signal processes of platelet activation.
Sol-gel zone – This is the matrix that is made of microtubules and microfilament, which plays a vital role in platelet structure and its support. This zone is responsible for various shape changes on activation during hemostasis and during ex vivo storage. Organelles are embedded within this matrix.
Organelle zone
Alpha-granules which stores fibrinogen fibronectin FV vWF, PDGF cytokines, chemokines, TG-beta-1, and VEGF
Dense- granules stores calcium ATP, ADP, serotonin, and pyrophosphate
Mitochondria- Are the powerhouse of platelets
Glycogen
Lysosome and peroxisome
When a platelet is activated, secretions from the α and dense granules are involved in further platelet activation and aggregation. Secretions also have immune-mediated effects.[rx]
Platelets Overviews
Platelets, also called thrombocytes, are membrane-bound cell fragments that are essential for clot formation during wound healing.
Key Points
Platelets, also called thrombocytes, are derived from megakaryocytes, which are derived from stem cells in the bone marrow.
Platelets circulate in the blood and are involved in hemostasis, leading to the formation of blood clots and blood coagulation.
Platelets lack a nucleus but do contain some organelles, such as mitochondria and endoplasmic reticulum fragments.
If the number of platelets in the blood is too low, excessive bleeding can occur. However, if the number of platelets is too high, blood clots can form ( thrombosis ), which may obstruct blood vessels.
Platelets are a natural source of growth factors involved in wound healing, coagulants, and inflammatory mediators.
Key Terms
extracellular matrix: All the connective tissues and fibers that are not part of a cell, but rather provide support.
platelet: A small, colorless, disc-shaped particle found in the blood of mammals. It plays an important role in the formation of blood clots.
Platelets, also called thrombocytes, are membrane-bound cell fragments derived from the fragmentation of larger precursor cells called megakaryocytes, which are derived from stem cells in the bone marrow. Platelets are important for the blood clotting process, making them essential for wound healing.
Platelet Structure and Distribution
Platelets are irregularly shaped, have no nucleus, and typically measure only 2–3 micrometers in diameter. Platelets are not true cells but are instead classified as cell fragments produced by megakaryocytes. Because they lack a nucleus, they do not contain nuclear DNA. However, they do contain mitochondria and mitochondrial DNA, as well as endoplasmic reticulum fragments and granules from the megakaryocyte parent cells. Platelets also contain adhesive proteins that allow them to adhere to fibrin mesh and the vascular endothelium, as well as to a microtubule and microfilament skeleton that extends into filaments during platelet activation. Less than 1% of whole blood consists of platelets. They are about 1/10th to 1/20th as abundant as white blood cells.
Platelet: Image from a light microscope (40×) from a peripheral blood smear surrounded by red blood cells. One platelet can be seen in the upper left side of the image (purple) and is significantly smaller in size than the red blood cells (stained pink) and the two large neutrophils (stained purple).
Functions of Platelets
Platelets circulate in blood plasma and are primarily involved in hemostasis (stopping the flow of blood during injury), by causing the formation of blood clots, also known as coagulation. The adhesive surface proteins of platelets allow them to accumulate on the fibrin mesh at an injury site to form a platelet plug that clots the blood. The complex process of wound repair can only begin once the clot has stopped bleeding.
Platelets secrete many factors involved in coagulation and wound healing. During coagulation, they release factors that increase local platelet aggregation (thromboxane A), mediate inflammation (serotonin), and promote blood coagulation through increasing thrombin and fibrin (thromboplastin). They also release wound healing-associated growth factors including platelet-derived growth factor (PDGF), which directs cell movement; TGF beta, which stimulates the deposition of extracellular matrix tissue into a wound during healing; and vascular endothelial growth factor (VEGF), which stimulates angiogenesis, or the regrowth of blood vessels. These growth factors play a significant role in the repair and regeneration of connective tissues. Local application of these platelet-produced healing-associated factors in increased concentrations has been used as an adjunct to wound healing for several decades.
or
Platelets have a crucial role in thrombus formation and hemostasis. Platelets circulate in the blood in a quiescent discoid form but may become activated by contact with damaged blood vessel walls. Following blood vessel damage, substances in the exposed subendothelial extracellular matrix such as collagen and von Willebrand factor may bind to platelet surface receptors.[rx] Platelets will adhere to sites of injury, and receptor binding will lead to platelet activation.
As described above, platelets undergo a structural transformation at this point and begin to secrete granule contents to promote platelet aggregation and platelet plug formation. Activated platelets release factors such as ADP, thromboxane A2, and thrombin, which can promote activation of other nearby platelets in a positive feedback mechanism.[rx] Activation also leads to the surface expression of glycoprotein IIb-IIIa. This protein binds to fibrinogen, allowing cross-linking of platelets and mediating platelet aggregation.[rx] A final change during activation is the expression of phosphatidylserine, which generates a negative charge on platelet surfaces. This negative charge allows clotting factor complexes to assemble on the surface, as part of the secondary hemostasis response.[rx]
The above processes ultimately lead to the production of a thrombus: a structure formed of aggregated, activated platelets, combined with a mesh of cross-linked fibrin and entrapped erythrocytes and leukocytes. This thrombus restores the structural integrity of the damaged vessel wall and prevents blood loss while the vessel heals.
There is additional growing evidence of the role of platelets in inflammatory and immune responses. Leukocytes are recruited to thrombi via interactions with platelet P-selectin, and platelet α-granules contain a range of pro-inflammatory cytokines. Antiplatelet medications have been found to affect immunity and may even reduce mortality related to infection and sepsis.[rx]
Platelets: A blood slide of platelets aggregating, or, clumping together. The platelets are the small, bright purple fragments.
If the number of platelets is too low, excessive bleeding can occur and wound healing will be impaired. However, if the number of platelets is too high, blood clots can form (thrombosis), which may obstruct blood vessels and result in ischemic tissue damage caused by a stroke, myocardial infarction, pulmonary embolism, or the blockage of blood vessels to other parts of the body. Thrombosis also occurs when blood is allowed to pool, which causes clotting factors and platelets to form a blood clot even in the absence of an injury.
Platelet Formation
Platelets are membrane-bound cell fragments derived from megakaryocytes, which are produced during thrombopoiesis.
Key Points
Megakaryocytes are produced from stem cells in the bone marrow by a process called thrombopoiesis.
Megaryocytes create platelets by releasing protoplatelets that break up into numerous smaller, functional platelets.
Thrombopoiesis is stimulated and regulated by the hormone thrombopoietin.
Platelets have an average life span of five to ten days.
Old platelets are destroyed by phagocytosis. The spleen holds a reservoir of additional platelets.
Abnormal numbers of platelets result from problems in thrombopoiesis. This is associated with various disorders and potential pathological complications.
Key Terms
megakaryocyte: A large cell found in bone marrow that is responsible for the production of platelets.
Thrombopoietin: A hormone produced by the liver or kidneys that stimulates megakaryocyte differentiation and platelet release.
bone marrow: The fatty vascular tissue that fills the cavities of bones; the place where new blood cells are produced.
Platelets are small, clear, irregularly-shaped cell fragments produced by larger precursor cells called megakaryocytes. Platelets are also called thrombocytes because they are involved in the blood clotting process, which is necessary for wound healing. Platelets are continuously produced as a component product of hematopoiesis (blood cell formation).
Thrombopoiesis
Platelets are produced during hematopoiesis in a sub-process called thrombopoiesis, or the production of thrombocytes. Thrombopoiesis occurs from common myeloid progenitor cells in the bone marrow, which differentiate into promegakaryocytes and then into megakaryocytes. Megakaryocytes stay in the bone marrow and are thought to produce protoplatelets within their cytoplasm, which are released in cytoplasmic extensions upon cytokine stimulus. The protoplatelets then break up into hundreds of platelets that circulate throughout the bloodstream, while the remaining nucleus of the ruptured megakaryocyte is consumed by macrophages.
Megakaryocyte and platelet production is regulated by thrombopoietin, a hormone produced by the liver and kidneys. Thrombopoietin stimulates the differentiation of myeloid progenitor cells into megakaryocytes and causes the release of platelets. Thrombopoietin is regulated by a negative feedback mechanism based on platelet levels in the body so that high levels of platelets result in lower levels of thrombopoietin, while low levels of platelets result in higher levels of
thrombopoietin.
Each megakaryocyte produces between 5,000 and 10,000 platelets before its cellular components are fully depleted. Altogether, around 10^11 platelets are produced each day in a healthy adult. The average lifespan of a platelet is just 5 to 10 days. Old platelets are destroyed by macrophage phagocytosis in the spleen and by Kupffer cells in the liver. Up to 40% of platelets are stored in the spleen as a reserve, released when needed by sympathetically-induced splenic muscle contractions during severe injury.
Hematopoiesis: Myeloid progenitor cells differentiate into promegakaryocytes, and megakaryocytes, which release platelets.
Implications of Platelet Formation
Balanced thrombopoiesis is important because it directly influences the amount of platelets in the body and their associated complications. If the number of platelets is too low, excessive bleeding can occur, even from minor or superficial injuries. If the number of platelets is too high, blood clots can form (thrombosis) and travel through the bloodstream, which may obstruct blood vessels and result in ischemic events. These include stroke, myocardial infarction, pulmonary embolism, or infarction of other tissues.
An abnormality or disease of the platelets is called a thrombocytopathy, which could be either a low number of platelets (thrombocytopenia), a decrease in function of platelets (thrombasthenia), or an increase in the number of platelets (thrombocytosis). In any case, issues with the number of circulating platelets is often due to issues in thrombopoietin feedback regulation, but may also be associated with genetic characteristics and certain medications and diseases. For example, thrombocytopenia often occurs in leukemia patients. Cancerous myeloid cells crowd out healthy ones in the bone marrow, causing impaired thrombopoiesis.
Disorders of Platelets
The three broad categories of platelet disorders are “not enough”; “dysfunctional”; and “too many”.[rx]:vii
Thrombocytopenia
Immune thrombocytopenias (ITP) – formerly known as immune thrombocytopenic purpura and idiopathic thrombocytopenic purpura
Myeloproliferative neoplasms – platelets are both elevated and activated
Essential thrombocytosis
Polycythemia vera
Associated with other myeloid neoplasms
Congenital
What Causes Low Platelets?
A low platelet count occurs when:
A person’s bone marrow is damaged and unable to make enough of its own platelets. This can be caused by certain cancers, such as Leukemia – and it can also be caused by cancer treatments.
Platelets have been lost due to severe bleeding, such as following a traumatic injury or during surgery.
Platelets have been destroyed by autoimmune diseases, certain medicines, infections, or other conditions.
The patient’s spleen, which filters the bloodstream, removes too many platelets.
Symptoms of low platelets include bruising easily and unusual bleeding, such as excessive bleeding from a small cut or blood in urine or stool.
Bone marrow problems
Your bone marrow is the spongy tissue inside the bone. It’s where all the components of blood, including platelets, are produced. If your bone marrow isn’t producing enough platelets, you’ll have a low platelet count. The causes of low platelet production include:
aplastic anemia
vitamin B-12 deficiency
folate deficiency
iron deficiency
viral infections, including HIV, Epstein-Barr, and chickenpox
exposure to chemotherapy, radiation, or toxic chemicals
consuming too much alcohol
cirrhosis
leukemia
myelodysplasia
Platelet destruction
Each platelet lives about 10 days in a healthy body. A low platelet count can also be a result of the body destroying too many platelets. This can be due to the side effects of certain medications, include diuretics and anti-seizure medications. It can also be a symptom of:
If the body has too many platelets in circulation, you may develop a condition called thrombocytosis.
The following factors may contribute to high platelet count:3
Primary bone marrow disorder – Essential thrombocytosis is a condition in which the megakaryocytes in the bone marrow produce too many platelets, increasing the risk of blood clots.
Chronic inflammation in the body – Inflammatory conditions such as rheumatoid arthritis (RA) and inflammatory bowel disease (IBD) may result in elevated platelet counts as high levels of inflammation may cause the bone marrow to produce more white blood cells and platelets to combat cellular damage.
Infection – Bone marrow cells increase the production of white blood cells and platelets to help fight infection, causing an elevation in platelet count.
Iron deficiency anemia – Reactive or secondary thrombocytosis may result when the body is undergoing a breakdown of red blood cells and the bone marrow cells go into overproduction to meet needs.
Spleen removal – Up to one-third of platelets are stored in the spleen at any time, and so removal of this organ will cause an increase in platelet concentration in the bloodstream. This is generally a temporary condition, however.
Cancer – High platelet counts can also be seen in cancer, especially with gastrointestinal cancer, as well as lymphoma, lung, ovarian, and breast cancer. This is thought to be due to the inflammation associated with the malignancy stimulating the production of platelets in the bone marrow.
In addition, a temporary increase in the platelet count can happen after major surgery or trauma.
What are the symptoms of a low platelet count?
Whether or not you experience symptoms depends on your platelet count.
Mild cases, such as when a low platelet count is caused by pregnancy, usually don’t cause any symptoms. More severe cases may cause uncontrollable bleeding, which requires immediate medical attention.
If you have a low platelet count, you may experience:
red, purple, or brown bruises, which are called purpura
a rash with small red or purple dots called petechiae
nosebleeds
bleeding gums
bleeding from wounds that lasts for a prolonged period or doesn’t stop on its own
heavy menstrual bleeding
bleeding from the rectum
blood in your stool
blood in your urine
In more serious cases, you may bleed internally. Symptoms of internal bleeding include:
blood in the urine
blood in the stool
bloody or very dark vomit
Talk to your doctor immediately if you experience any signs of internal bleeding.
Rarely, this condition may lead to bleeding in your brain. If you have a low platelet count and experience headaches or any neurological problems, tell your doctor right away.
We believe in health equity—the equal opportunity for everyone to live their healthiest life. Join us in transforming health outcomes through the power of storytelling.
How is a low platelet count diagnosed?
If your doctor suspects a low platelet count, they’ll first perform a physical examination. During the exam, your doctor will check your body for any unusual bruising or evidence of petechiae, which is a sign of capillary bleeding that often accompanies a low platelet count.
Your doctor may also feel your abdomen to check for an enlarged spleen, which can cause a low platelet count. You may also be asked if you have any family history of bleeding disorders since these types of disorders can run in families.
Blood tests
To diagnose this condition, your doctor needs to do a complete blood count test. This test looks at the number of blood cells in your blood. It’ll tell your doctor if your platelet count is lower than it should be. A typical platelet count will range between 150,000 and 450,000 platelets per mL blood.
Your doctor may also wish to have your blood tested for platelet antibodies. These are proteins that destroy platelets. Platelet antibodies can be produced as a side effect to certain drugs, such as heparin, or for unknown reasons.
Your doctor may also order blood-clotting tests, which include partial thromboplastin time and prothrombin time. These tests simply require a sample of your blood. Certain chemicals will be added to the sample to determine how long it takes your blood to clot.
Ultrasound
If your doctor suspects that your spleen is enlarged, they may order an ultrasound. This test will use sound waves to make a picture of your spleen. It can help your doctor determine if your spleen is the proper size.
Bone marrow aspiration and biopsy
If your doctor suspects that there’s a problem in your bone marrow, they may order a bone marrow aspiration. During an aspiration, your doctor will use a needle to remove a small amount of bone marrow from one of your bones.
A bone marrow biopsy may also be ordered. Your doctor will use a needle to take a sample of your core bone marrow, usually from the hipbone. It may be performed at the same time as a bone marrow aspiration.
What is the treatment for a low platelet count?
The treatment for a low platelet count depends on the cause and severity of your condition. If your condition is mild, your doctor may wish to hold off on treatment and simply monitor you.
Your doctor may recommend that you take measures to prevent your condition from worsening. This could include:
avoiding contact sports
avoiding activities with a high risk of bleeding or bruising
limiting alcohol consumption
stopping or switching medications that affect platelets, including aspirin and ibuprofen
If your low platelet count is more severe, you may need medical treatment. This may include:
blood or platelet transfusions
changing medications that are causing a low platelet count
Platelets, or thrombocytes, are the smallest blood cells, colorless cell fragments in our blood that form clots and stop or prevent bleeding. Typically around 2μm in diameter and anucleated, with an average lifespan of 7 to 10 days in humans. The platelet is a circulating anuclear fragment of a bone marrow megakaryocyte, 3 to 4 μm in diameter, with limited synthetic capability. The mean normal platelet count is between 250,000 and 260,000 cells/mm3, although there is a wide range of accepted normal values in most laboratories that extend as low as 150,000 to as high as 400,000/mm3.[rx][rx] Platelets are made in our bone marrow, the sponge-like tissue inside our bones. Bone marrow contains stem cells that develop into red blood cells, white blood cells, and platelets.
Platelets are small blood cells with several physiological purposes; the best studied is thrombosis activation. Through their clotting activity and activation of the coagulation cascade, they are crucial to maintaining adequate blood volume in those with vascular injury. The initiation of this activity begins with tissue injury and results in the release and binding of several glycoproteins, growth factors, and clotting factors. The complexity of these processes allows for many pharmacologic targets, which provides several options when it comes to antithrombotic therapy.[rx][rx][rx]
Platelet Count (PLT)
Just as it sounds, this is the actual number of platelets you have (per microliter of blood).
Low range: Less than 150,000 platelets per microliter
Normal range: 150,000 to 450,000 platelets per microliter1
Elevated range: 500,000 to 1,000,000 platelets per microliter
If your platelet count falls below 50,000, you may experience prolonged bleeding times.
Structure of Platelets
Platelets form by the fragmentation of megakaryocytes within the bone marrow. Megakaryocytes duplicate in the marrow without dividing, resulting in the production of giant cells. Within these giant cells, organelles organize into discrete domains, which will eventually become individual platelets, separated by a network of invaginating plasma membranes. These megakaryocytes are positioned next to the sinusoidal walls, such that shearing forces from circulating blood fragment the megakaryocyte cytoplasm into individual platelets and sweep these new platelets into the bloodstream.[rx]
Platelets circulate in the blood in discoid form but undergo significant structural changes following activation, mediated by actin and myosin within the cytoplasm. The platelets transform from discoid forms into compact spheres with dendritic extensions, which allow platelet adhesion. A variety of membrane-bound glycoprotein receptors facilitates the adhesion and aggregation of platelets.[rx]
As described above, platelets are anuclear but do contain RNA, ribosomes, mitochondria, and various granules, which are important in enacting platelet function.[rx] There are three distinct types of platelet granule
α-granules: the most abundant and largest secretory granules. They contain most of the platelet factors involved in hemostasis, including p-selectin, von Willebrand Factor, and fibrinogen[rx]
Dense granules: the smallest granules, which are visible on electron microscopy as dense bodies. They contain ADP and serotonin, as well as high levels of calcium
Lysosomes: contain hydrolytic enzymes including acid phosphatase and arylsulfatase[rx]
An ‘open canalicular system’ formed of deep surface membrane invaginations facilitates the secretion of granules.[rx] This system also has a key role in the transport of membrane receptors, allowing them to cluster, stabilize platelet adhesion sites, and amplify signals.[rx]
Structurally a platelet is divided into three zones
Peripheral zone – this zone is primarily involved in the adhesion and aggregation function
Glycocalyx – This is the thick carbohydrate-rich structure found on the exterior surface of platelets and serves as the site of the first contact during the hemostatic response by platelets, and it is made up of major and minor glycoproteins. GP-Ib-IX-V complex involved in adhesion at the site of vascular injury. GPIIb-IIIa is involved in aggregation by attachment through fibrinogen to other platelets.
Unit membrane – It is made of a lipid bilayer and open canalicular system, which serves a vital role in the acceleration of coagulation through the anionic phospholipid, phosphatidylserine, provided by the surface of activated platelets when clotting is initiated which converts prothrombin to thrombin.
The submembrane area – It plays a vital role in transmitting signals from the surface to organelles in the cytoplasm regulating signal processes of platelet activation.
Sol-gel zone – This is the matrix that is made of microtubules and microfilament, which plays a vital role in platelet structure and its support. This zone is responsible for various shape changes on activation during hemostasis and during ex vivo storage. Organelles are embedded within this matrix.
Organelle zone
Alpha-granules which stores fibrinogen fibronectin FV vWF, PDGF cytokines, chemokines, TG-beta-1, and VEGF
Dense- granules stores calcium ATP, ADP, serotonin, and pyrophosphate
Mitochondria- Are the powerhouse of platelets
Glycogen
Lysosome and peroxisome
When a platelet is activated, secretions from the α and dense granules are involved in further platelet activation and aggregation. Secretions also have immune-mediated effects.[rx]
Platelets Overviews
Platelets, also called thrombocytes, are membrane-bound cell fragments that are essential for clot formation during wound healing.
Key Points
Platelets, also called thrombocytes, are derived from megakaryocytes, which are derived from stem cells in the bone marrow.
Platelets circulate in the blood and are involved in hemostasis, leading to the formation of blood clots and blood coagulation.
Platelets lack a nucleus but do contain some organelles, such as mitochondria and endoplasmic reticulum fragments.
If the number of platelets in the blood is too low, excessive bleeding can occur. However, if the number of platelets is too high, blood clots can form ( thrombosis ), which may obstruct blood vessels.
Platelets are a natural source of growth factors involved in wound healing, coagulants, and inflammatory mediators.
Key Terms
extracellular matrix: All the connective tissues and fibers that are not part of a cell, but rather provide support.
platelet: A small, colorless, disc-shaped particle found in the blood of mammals. It plays an important role in the formation of blood clots.
Platelets, also called thrombocytes, are membrane-bound cell fragments derived from the fragmentation of larger precursor cells called megakaryocytes, which are derived from stem cells in the bone marrow. Platelets are important for the blood clotting process, making them essential for wound healing.
Platelet Structure and Distribution
Platelets are irregularly shaped, have no nucleus, and typically measure only 2–3 micrometers in diameter. Platelets are not true cells but are instead classified as cell fragments produced by megakaryocytes. Because they lack a nucleus, they do not contain nuclear DNA. However, they do contain mitochondria and mitochondrial DNA, as well as endoplasmic reticulum fragments and granules from the megakaryocyte parent cells. Platelets also contain adhesive proteins that allow them to adhere to fibrin mesh and the vascular endothelium, as well as to a microtubule and microfilament skeleton that extends into filaments during platelet activation. Less than 1% of whole blood consists of platelets. They are about 1/10th to 1/20th as abundant as white blood cells.
Platelet: Image from a light microscope (40×) from a peripheral blood smear surrounded by red blood cells. One platelet can be seen in the upper left side of the image (purple) and is significantly smaller in size than the red blood cells (stained pink) and the two large neutrophils (stained purple).
Functions of Platelets
Platelets circulate in blood plasma and are primarily involved in hemostasis (stopping the flow of blood during injury), by causing the formation of blood clots, also known as coagulation. The adhesive surface proteins of platelets allow them to accumulate on the fibrin mesh at an injury site to form a platelet plug that clots the blood. The complex process of wound repair can only begin once the clot has stopped bleeding.
Platelets secrete many factors involved in coagulation and wound healing. During coagulation, they release factors that increase local platelet aggregation (thromboxane A), mediate inflammation (serotonin), and promote blood coagulation through increasing thrombin and fibrin (thromboplastin). They also release wound healing-associated growth factors including platelet-derived growth factor (PDGF), which directs cell movement; TGF beta, which stimulates the deposition of extracellular matrix tissue into a wound during healing; and vascular endothelial growth factor (VEGF), which stimulates angiogenesis, or the regrowth of blood vessels. These growth factors play a significant role in the repair and regeneration of connective tissues. Local application of these platelet-produced healing-associated factors in increased concentrations has been used as an adjunct to wound healing for several decades.
or
Platelets have a crucial role in thrombus formation and hemostasis. Platelets circulate in the blood in a quiescent discoid form but may become activated by contact with damaged blood vessel walls. Following blood vessel damage, substances in the exposed subendothelial extracellular matrix such as collagen and von Willebrand factor may bind to platelet surface receptors.[rx] Platelets will adhere to sites of injury, and receptor binding will lead to platelet activation.
As described above, platelets undergo a structural transformation at this point and begin to secrete granule contents to promote platelet aggregation and platelet plug formation. Activated platelets release factors such as ADP, thromboxane A2, and thrombin, which can promote activation of other nearby platelets in a positive feedback mechanism.[rx] Activation also leads to the surface expression of glycoprotein IIb-IIIa. This protein binds to fibrinogen, allowing cross-linking of platelets and mediating platelet aggregation.[rx] A final change during activation is the expression of phosphatidylserine, which generates a negative charge on platelet surfaces. This negative charge allows clotting factor complexes to assemble on the surface, as part of the secondary hemostasis response.[rx]
The above processes ultimately lead to the production of a thrombus: a structure formed of aggregated, activated platelets, combined with a mesh of cross-linked fibrin and entrapped erythrocytes and leukocytes. This thrombus restores the structural integrity of the damaged vessel wall and prevents blood loss while the vessel heals.
There is additional growing evidence of the role of platelets in inflammatory and immune responses. Leukocytes are recruited to thrombi via interactions with platelet P-selectin, and platelet α-granules contain a range of pro-inflammatory cytokines. Antiplatelet medications have been found to affect immunity and may even reduce mortality related to infection and sepsis.[rx]
Platelets: A blood slide of platelets aggregating, or, clumping together. The platelets are the small, bright purple fragments.
If the number of platelets is too low, excessive bleeding can occur and wound healing will be impaired. However, if the number of platelets is too high, blood clots can form (thrombosis), which may obstruct blood vessels and result in ischemic tissue damage caused by a stroke, myocardial infarction, pulmonary embolism, or the blockage of blood vessels to other parts of the body. Thrombosis also occurs when blood is allowed to pool, which causes clotting factors and platelets to form a blood clot even in the absence of an injury.
Platelet Formation
Platelets are membrane-bound cell fragments derived from megakaryocytes, which are produced during thrombopoiesis.
Key Points
Megakaryocytes are produced from stem cells in the bone marrow by a process called thrombopoiesis.
Megaryocytes create platelets by releasing protoplatelets that break up into numerous smaller, functional platelets.
Thrombopoiesis is stimulated and regulated by the hormone thrombopoietin.
Platelets have an average life span of five to ten days.
Old platelets are destroyed by phagocytosis. The spleen holds a reservoir of additional platelets.
Abnormal numbers of platelets result from problems in thrombopoiesis. This is associated with various disorders and potential pathological complications.
Key Terms
megakaryocyte: A large cell found in bone marrow that is responsible for the production of platelets.
Thrombopoietin: A hormone produced by the liver or kidneys that stimulates megakaryocyte differentiation and platelet release.
bone marrow: The fatty vascular tissue that fills the cavities of bones; the place where new blood cells are produced.
Platelets are small, clear, irregularly-shaped cell fragments produced by larger precursor cells called megakaryocytes. Platelets are also called thrombocytes because they are involved in the blood clotting process, which is necessary for wound healing. Platelets are continuously produced as a component product of hematopoiesis (blood cell formation).
Thrombopoiesis
Platelets are produced during hematopoiesis in a sub-process called thrombopoiesis, or the production of thrombocytes. Thrombopoiesis occurs from common myeloid progenitor cells in the bone marrow, which differentiate into promegakaryocytes and then into megakaryocytes. Megakaryocytes stay in the bone marrow and are thought to produce protoplatelets within their cytoplasm, which are released in cytoplasmic extensions upon cytokine stimulus. The protoplatelets then break up into hundreds of platelets that circulate throughout the bloodstream, while the remaining nucleus of the ruptured megakaryocyte is consumed by macrophages.
Megakaryocyte and platelet production is regulated by thrombopoietin, a hormone produced by the liver and kidneys. Thrombopoietin stimulates the differentiation of myeloid progenitor cells into megakaryocytes and causes the release of platelets. Thrombopoietin is regulated by a negative feedback mechanism based on platelet levels in the body so that high levels of platelets result in lower levels of thrombopoietin, while low levels of platelets result in higher levels of
thrombopoietin.
Each megakaryocyte produces between 5,000 and 10,000 platelets before its cellular components are fully depleted. Altogether, around 10^11 platelets are produced each day in a healthy adult. The average lifespan of a platelet is just 5 to 10 days. Old platelets are destroyed by macrophage phagocytosis in the spleen and by Kupffer cells in the liver. Up to 40% of platelets are stored in the spleen as a reserve, released when needed by sympathetically-induced splenic muscle contractions during severe injury.
Hematopoiesis: Myeloid progenitor cells differentiate into promegakaryocytes, and megakaryocytes, which release platelets.
Implications of Platelet Formation
Balanced thrombopoiesis is important because it directly influences the amount of platelets in the body and their associated complications. If the number of platelets is too low, excessive bleeding can occur, even from minor or superficial injuries. If the number of platelets is too high, blood clots can form (thrombosis) and travel through the bloodstream, which may obstruct blood vessels and result in ischemic events. These include stroke, myocardial infarction, pulmonary embolism, or infarction of other tissues.
An abnormality or disease of the platelets is called a thrombocytopathy, which could be either a low number of platelets (thrombocytopenia), a decrease in function of platelets (thrombasthenia), or an increase in the number of platelets (thrombocytosis). In any case, issues with the number of circulating platelets is often due to issues in thrombopoietin feedback regulation, but may also be associated with genetic characteristics and certain medications and diseases. For example, thrombocytopenia often occurs in leukemia patients. Cancerous myeloid cells crowd out healthy ones in the bone marrow, causing impaired thrombopoiesis.
Disorders of Platelets
The three broad categories of platelet disorders are “not enough”; “dysfunctional”; and “too many”.[rx]:vii
Thrombocytopenia
Immune thrombocytopenias (ITP) – formerly known as immune thrombocytopenic purpura and idiopathic thrombocytopenic purpura
Myeloproliferative neoplasms – platelets are both elevated and activated
Essential thrombocytosis
Polycythemia vera
Associated with other myeloid neoplasms
Congenital
What Causes Low Platelets?
A low platelet count occurs when:
A person’s bone marrow is damaged and unable to make enough of its own platelets. This can be caused by certain cancers, such as Leukemia – and it can also be caused by cancer treatments.
Platelets have been lost due to severe bleeding, such as following a traumatic injury or during surgery.
Platelets have been destroyed by autoimmune diseases, certain medicines, infections, or other conditions.
The patient’s spleen, which filters the bloodstream, removes too many platelets.
Symptoms of low platelets include bruising easily and unusual bleeding, such as excessive bleeding from a small cut or blood in urine or stool.
Bone marrow problems
Your bone marrow is the spongy tissue inside the bone. It’s where all the components of blood, including platelets, are produced. If your bone marrow isn’t producing enough platelets, you’ll have a low platelet count. The causes of low platelet production include:
aplastic anemia
vitamin B-12 deficiency
folate deficiency
iron deficiency
viral infections, including HIV, Epstein-Barr, and chickenpox
exposure to chemotherapy, radiation, or toxic chemicals
consuming too much alcohol
cirrhosis
leukemia
myelodysplasia
Platelet destruction
Each platelet lives about 10 days in a healthy body. A low platelet count can also be a result of the body destroying too many platelets. This can be due to the side effects of certain medications, include diuretics and anti-seizure medications. It can also be a symptom of:
If the body has too many platelets in circulation, you may develop a condition called thrombocytosis.
The following factors may contribute to high platelet count:3
Primary bone marrow disorder – Essential thrombocytosis is a condition in which the megakaryocytes in the bone marrow produce too many platelets, increasing the risk of blood clots.
Chronic inflammation in the body – Inflammatory conditions such as rheumatoid arthritis (RA) and inflammatory bowel disease (IBD) may result in elevated platelet counts as high levels of inflammation may cause the bone marrow to produce more white blood cells and platelets to combat cellular damage.
Infection – Bone marrow cells increase the production of white blood cells and platelets to help fight infection, causing an elevation in platelet count.
Iron deficiency anemia – Reactive or secondary thrombocytosis may result when the body is undergoing a breakdown of red blood cells and the bone marrow cells go into overproduction to meet needs.
Spleen removal – Up to one-third of platelets are stored in the spleen at any time, and so removal of this organ will cause an increase in platelet concentration in the bloodstream. This is generally a temporary condition, however.
Cancer – High platelet counts can also be seen in cancer, especially with gastrointestinal cancer, as well as lymphoma, lung, ovarian, and breast cancer. This is thought to be due to the inflammation associated with the malignancy stimulating the production of platelets in the bone marrow.
In addition, a temporary increase in the platelet count can happen after major surgery or trauma.
What are the symptoms of a low platelet count?
Whether or not you experience symptoms depends on your platelet count.
Mild cases, such as when a low platelet count is caused by pregnancy, usually don’t cause any symptoms. More severe cases may cause uncontrollable bleeding, which requires immediate medical attention.
If you have a low platelet count, you may experience:
red, purple, or brown bruises, which are called purpura
a rash with small red or purple dots called petechiae
nosebleeds
bleeding gums
bleeding from wounds that lasts for a prolonged period or doesn’t stop on its own
heavy menstrual bleeding
bleeding from the rectum
blood in your stool
blood in your urine
In more serious cases, you may bleed internally. Symptoms of internal bleeding include:
blood in the urine
blood in the stool
bloody or very dark vomit
Talk to your doctor immediately if you experience any signs of internal bleeding.
Rarely, this condition may lead to bleeding in your brain. If you have a low platelet count and experience headaches or any neurological problems, tell your doctor right away.
We believe in health equity—the equal opportunity for everyone to live their healthiest life. Join us in transforming health outcomes through the power of storytelling.
How is a low platelet count diagnosed?
If your doctor suspects a low platelet count, they’ll first perform a physical examination. During the exam, your doctor will check your body for any unusual bruising or evidence of petechiae, which is a sign of capillary bleeding that often accompanies a low platelet count.
Your doctor may also feel your abdomen to check for an enlarged spleen, which can cause a low platelet count. You may also be asked if you have any family history of bleeding disorders since these types of disorders can run in families.
Blood tests
To diagnose this condition, your doctor needs to do a complete blood count test. This test looks at the number of blood cells in your blood. It’ll tell your doctor if your platelet count is lower than it should be. A typical platelet count will range between 150,000 and 450,000 platelets per mL blood.
Your doctor may also wish to have your blood tested for platelet antibodies. These are proteins that destroy platelets. Platelet antibodies can be produced as a side effect to certain drugs, such as heparin, or for unknown reasons.
Your doctor may also order blood-clotting tests, which include partial thromboplastin time and prothrombin time. These tests simply require a sample of your blood. Certain chemicals will be added to the sample to determine how long it takes your blood to clot.
Ultrasound
If your doctor suspects that your spleen is enlarged, they may order an ultrasound. This test will use sound waves to make a picture of your spleen. It can help your doctor determine if your spleen is the proper size.
Bone marrow aspiration and biopsy
If your doctor suspects that there’s a problem in your bone marrow, they may order a bone marrow aspiration. During an aspiration, your doctor will use a needle to remove a small amount of bone marrow from one of your bones.
A bone marrow biopsy may also be ordered. Your doctor will use a needle to take a sample of your core bone marrow, usually from the hipbone. It may be performed at the same time as a bone marrow aspiration.
What is the treatment for a low platelet count?
The treatment for a low platelet count depends on the cause and severity of your condition. If your condition is mild, your doctor may wish to hold off on treatment and simply monitor you.
Your doctor may recommend that you take measures to prevent your condition from worsening. This could include:
avoiding contact sports
avoiding activities with a high risk of bleeding or bruising
limiting alcohol consumption
stopping or switching medications that affect platelets, including aspirin and ibuprofen
If your low platelet count is more severe, you may need medical treatment. This may include:
blood or platelet transfusions
changing medications that are causing a low platelet count
What Is White Blood Cells /White blood cells, or leukocytes (Greek; leucko=white and cyte = cell), are part of the immune system participating in both the innate and humoral immune responses. They circulate in the blood and mount inflammatory and cellular responses to injury or pathogens. White blood cells are part of the body’s immune system. They help the body fight infection and other diseases. Types of white blood cells are granulocytes (neutrophils, eosinophils, and basophils), monocytes, and lymphocytes (T cells and B cells). Checking the number of white blood cells in the blood is usually part of a complete blood cell (CBC) test. It may be used to look for conditions such as infection, inflammation, allergies, and leukemia. Also called leukocyte and WBC.
White blood cells (WBC) are a heterogeneous group of nucleated cells that can be found in circulation for at least a period of their life. Their normal concentration in the blood varies between 4000 and 10,000 per microliter. They play a most important role in phagocytosis and immunity and therefore in defense against infection.
These normal ranges can vary by lab. Another common measurement for the volume of blood is cubic millimeter or mm3. A microliter and cubic millimeter equal the same amount. The types of cells that make up WBCs usually fall within a normal percentage of your overall WBC count.
The normal percentages of the types of WBCs in your overall count are usually in these ranges, according to the Leukemia & Lymphoma Society (LLS):
Type of WBC
Normal percentage of overall WBC count
neutrophil
55 to 73 percent
lymphocyte
20 to 40 percent
eosinophil
1 to 4 percent
monocyte
2 to 8 percent
basophil
0.5 to 1 percent
Higher or lower numbers of WBCs than normal can be a sign of an underlying condition.
Over All Types And Functions
Neutrophils
Neutrophils are the commonest type of white blood cell found in a blood smear. They make up 60-70% of the total amount of white blood cells.
Neutrophils (also known as enterocytes or heterophils) are the most abundant type of granulocytes and makeup 40% to 70% of all white blood cells in humans.[rx] They form an essential part of the innate immune system, with their functions varying in different animals.[rx]
They are formed from stem cells in the bone marrow and differentiated into subpopulations of neutrophil-killers and neutrophil-cagers. They are short-lived and highly motile, or mobile, as they can enter parts of tissue where other cells/molecules cannot. Neutrophils may be subdivided into segmented neutrophils and banded neutrophils (or bands). They form part of the polymorphonuclear cells family (PMNs) together with basophils and eosinophils.[rx][rx][rx]
Neutrophils have 3 types of granules
azure granules (lysosomes),
secretory granules in salmon pink cytoplasm, anti-microbial enzymes.
have glycoproteins and gelatinase.
Function
Neutrophils are born in the bone marrow. They circulate in the blood for 6-10 hours and then enter the tissues. They are motile, and phagocytic and will destroy damaged tissue and bacteria. They self-destruct after one burst of activity. They are important in inflammatory reactions.
These cells are 12 – 17 µm in diameter – larger than neutrophils, and about 3 times the size of a red blood cell. You can see that eosinophils only have two lobes to their nucleus.
Neutrophils undergo a process called chemotaxis via amoeboid movement, which allows them to migrate toward sites of infection or inflammation. Cell surface receptors allow neutrophils to detect chemical gradients of molecules such as interleukin-8 (IL-8), interferon-gamma (IFN-γ), C3a, C5a, and Leukotriene B4, which these cells use to direct the path of their migration.
These cells have large acidophilic specific granules – this stain bright red, or reddish-purple. These granules contain proteins that are ‘destructive’ and toxic. Anti-microbial function highly motile, neutrophils quickly congregate at a focus of infection, attracted by cytokines expressed by activated endothelium, mast cells, and macrophages. Neutrophils express[rx] and release cytokines, which in turn amplify inflammatory reactions by several other cell types.
Neutrophils are phagocytes, capable of ingesting microorganisms or particles. For targets to be recognized, they must be coated in opsonins—a process known as antibody opsonization. They can internalize and kill many microbes, each phagocytic event resulting in the formation of a phagosome into which reactive oxygen species and hydrolytic enzymes are secreted. The consumption of oxygen during the generation of reactive oxygen species has been termed the “respiratory burst”, although unrelated to respiration or energy production.
Eosinophils
Eosinophils are fairly rarely found in blood smears – making up 1-6% of the total white blood cells. Eosinophils, sometimes called eosinophils or, less commonly, acidophils, are a variety of white blood cells and one of the immune system components responsible for combating multicellular parasites and certain infections in vertebrates.[rx] Along with mast cells and basophils, they also control mechanisms associated with allergy and asthma. They are granulocytes that develop during hematopoiesis in the bone marrow before migrating into blood, after which they are terminally differentiated and do not multiply.[rx] They form about 2 to 3% of WBCs.
Function
These cells are born in the bone marrow, and migrate from the peripheral blood system after a few hours, into loose connective tissue in the respiratory and gastrointestinal tracts. They phagocytose antigen-antibody complexes. They also produce histaminase, and aryl sulphatase B, two enzymes that inactivate two inflammatory agents released by mast cells. A high eosinophil blood count may indicate an allergic reaction.
Eosinophils are also important in killing parasitic worms. They are 14-16 µm in diameter, contain lots of deep blue staining granules (basic) and a bilobed nucleus. The granules contain heparin, histamine, and serotonin. prostaglandins and leukotrienes.
Following activation, eosinophils effector functions include production of the following:
Cationic granule proteins and their release by degranulation[rx][rx][rx]
Reactive oxygen species such as hypobromite, superoxide, and peroxide (hypobromous acid, which is preferentially produced by eosinophil peroxidase)[rx]
Lipid mediators like the eicosanoids from the leukotriene (e.g., LTC4, LTD4, LTE4) and prostaglandin (e.g., PGE2) families[rx]
Enzymes, such as elastase
Growth factors such as TGF beta, VEGF, and PDGF[rx][rx]
Cytokines such as IL-1, IL-2, IL-4, IL-5, IL-6, IL-8, IL-13, and TNF alpha[rx][rx]
There are also eosinophils that play a role in fighting viral infections, which is evident from the abundance of RNases they contain within their granules, and in fibrin removal during inflammation. Eosinophils, along with basophils and mast cells, are important mediators of allergic responses and asthma pathogenesis and are associated with disease severity. They also fight helminth (worm) colonization and may be slightly elevated in the presence of certain parasites. Eosinophils are also involved in many other biological processes, including postpubertal mammary gland development, oestrus cycling, allograft rejection, and neoplasia.[rx] They have also been implicated in antigen presentation to T cells.[rx]
Eosinophils are responsible for tissue damage and inflammation in many diseases, including asthma.[rx][rx] High levels of interleukin-5 has been observed to up-regulate the expression of adhesion molecules, which then facilitate the adhesion of eosinophils to endothelial cells, thereby causing inflammation and tissue damage.[rx]
An accumulation of eosinophils in the nasal mucosa is considered a major diagnostic criterion for allergic rhinitis (nasal allergies).
Basophils
Basophils are the rarest type of white blood cell, making up only 1% of the white blood cells found in a blood smear. Basophils are a type of white blood cell. Basophils are the least common type of granulocyte, representing about 0.5% to 1% of circulating white blood cells.[rx] However, they are the largest type of granulocyte. They are responsible for inflammatory reactions during an immune response, as well as in the formation of acute and chronic allergic diseases, including anaphylaxis, asthma, atopic dermatitis, and hay fever.[rx] They also produce compounds that coordinate immune responses, including histamine and serotonin that induce inflammation, heparin that prevents blood clotting,[rx] although there are less than that found in mast cell granules.[rx] Mast cells were once thought to be basophils that migrated from the blood into their resident tissues (connective tissue), but they are now known to be different types of cells.[rx]
Function
These cells are involved in immune responses to parasites. They have IgE receptors and the granules are released when the cells bind IgE. These cells also accumulate at sites of infection, and the release of prostaglandins, serotonin, and histamine help to increase blood flow to the area of damage, as part of the inflammatory response. The degranulation-release of histamine also plays a role in allergic reactions such as hay fever.
Basophils appear in many specific kinds of inflammatory reactions, particularly those that cause allergic symptoms. Basophils contain anticoagulant heparin, which prevents blood from clotting too quickly. They also contain the vasodilator histamine, which promotes blood flow to tissues. They can be found in unusually high numbers at sites of ectoparasite infection, e.g., ticks. Like eosinophils, basophils play a role in both parasitic infections and allergies.[rx] They are found in tissues where allergic reactions are occurring and probably contribute to the severity of these reactions.
Basophils have protein receptors on their cell surface that bind IgE, an immunoglobulin involved in macroparasite defense and allergy. It is the bound IgE antibody that confers a selective response of these cells to environmental substances, for example, pollen proteins or helminth antigens. Recent studies in mice suggest that basophils may also regulate the behavior of T cells and mediate the magnitude of the secondary immune response.[rx]
Agranulocytes
This is a photo of a lymphocyte in a blood smear. Most of the lymphocytes are small; a bit bigger than red blood cells, at about 6-9µm in diameter,
The rest (around 10%) are larger, about 10-14µm in diameter. These larger cells have more cytoplasm, more free ribosomes, and mitochondria. Lymphocytes can look like monocytes, except that lymphocytes do not have a kidney-bean-shaped nucleus, and lymphocytes are usually smaller. Larger lymphocytes are commonly activated lymphocytes.
They have a small spherical nucleus and has abundant dark staining condensed chromatin. Not much cytoplasm can be seen, and it is basophilic (pale blue/purple staining).
Lymphocyte
These are the second most common white blood cell (20-50%), and are easy to find in blood smears. Although the cells look similar there are two main types, B-cells and T-cells. B-cells develop in the bone marrow. T cells are born in the bone marrow but are matured in the Thymus. There will be more on this in the section on the immune system.
Lymphocytes are cells that help to regulate the body’s immune system.
The main types of lymphocytes are:
B lymphocytes (B cells)
T lymphocytes (T cells)
B lymphocytes
B lymphocytes are able to release antibodies which are Y-shaped proteins that bind to infected microbes or cells of the body that have become infected.
Antibodies can either neutralize the target microbe or can mark it out for attack by T lymphocytes.
T lymphocytes
There are a number of different T lymphocytes:
Helper T cells release a protein called cytokines which help to further direct the response of other white blood cells.
Cytotoxic T cells (also known as natural killer T cells) are able to release molecules that kill viruses and other antigens.
Memory T cells will be present after the body has fought off infection and help the body to deal more easily with any future infection of the same type.
Regulatory T cells (also known as suppressor T cells) help to regulate other T cells to prevent them from targeting the body’s own cells.
Lymphocytes are much more common in the lymphatic system than in blood. Lymphocytes are distinguished by having a deeply staining nucleus that may be eccentric in location, and a relatively small amount of cytoplasm. Lymphocytes include:
B cells make antibodies that can bind to pathogens, block pathogen invasion, activate the complement system, and enhance pathogen destruction.
T cells:
CD4+ helper T cells: T cells displaying co-receptor CD4 are known as CD4+ T cells. These cells have T-cell receptors and CD4 molecules that, in combination, bind antigenic peptides presented on major histocompatibility complex (MHC) class II molecules on antigen-presenting cells. Helper T cells make cytokines and perform other functions that help coordinate the immune response. In HIV infection, these T cells are the main index to identify the individual’s immune system integrity.
CD8+ cytotoxic T cells: T cells displaying co-receptor CD8 are known as CD8+ T cells. These cells bind antigens presented on the MHC I complex of virus-infected or tumor cells and kill them. Nearly all nucleated cells display MHC I.
γδ T cells possess an alternative T cell receptor (different from the αβ TCR found on conventional CD4+ and CD8+ T cells). Found in tissue more commonly than in blood, γδ T cells share characteristics of helper T cells, cytotoxic T cells, and natural killer cells.
Natural killer cells are able to kill cells of the body that do not display MHC class I molecules or display stress markers such as MHC class I polypeptide-related sequence A (MIC-A). Decreased expression of MHC class I and up-regulation of MIC-A can happen when cells are infected by a virus or become cancerous.
T lymphocytes and Type 1 Diabetes
In type 1 diabetes, the killer T cells target and kill the body’s own insulin-producing cells. Even if new insulin-producing islet cells are transplanted, the T cells will still try these cells off.
As a result, people who have had islet cell transplants need to take strong anti-immune drugs to preserve the transplanted cells. Researchers have therefore been investigating ways to regulate the immune response in type 1 diabetes.
Bone marrow transplants have had some success in modulating the immune system, however, bone marrow transplants introduce a risk of complications developing.
Function
The B-cells develop into plasma cells which make antibodies, The T-cells attack viruses, cancer cells, and transplants.
This is a photo of monocyte in a blood smear. These are the largest type of white blood cells and can be up to 20µm in diameter. They have a large eccentrically placed nucleus, which is kidney bean-shaped. They have abundant cytoplasm and some fine pink/purple granules in the cytoplasm.
Monocyte
Monocytes are the third most common type of white blood cell; about 2-10% of leukocytes are monocytes.
Monocytes can develop into two types of cell:
Dendritic cells – are antigen-presenting cells that are able to mark out cells that are antigens (foreign bodies) that need to be destroyed by lymphocytes.
Macrophages – are phagocyte cells that are larger and live longer than neutrophils. Macrophages are also able to act as antigen-presenting cells.
Function
Monocytes in the circulation are precursors of tissue macrophages that are actively phagocytic. Monocytes circulate in the blood for 1-3 days and then migrate into body tissues, where they transform into macrophages. They will phagocytose dead cells and bacteria. Some monocytes can also transform into osteoclasts.
Monocytes and their macrophage and dendritic-cell progeny serve three main functions in the immune system. These are phagocytosis, antigen presentation, and cytokine production. Phagocytosis is the process of uptake of microbes and particles followed by digestion and destruction of this material. Monocytes can perform phagocytosis using intermediary (opsonizing) proteins such as antibodies or complement that coat the pathogen, as well as by binding to the microbe directly via pattern-recognition receptors that recognize pathogens. Monocytes are also capable of killing infected host cells via antibody-dependent cell-mediated cytotoxicity. Vacuolization may be present in a cell that has recently phagocytized foreign matter.
Many factors produced by other cells can regulate the chemotaxis and other functions of monocytes. These factors include most particularly chemokines such as monocyte chemotactic protein-1 (CCL2) and monocyte chemotactic protein-3 (CCL7); certain arachidonic acid metabolites such as Leukotriene B4 and members of the 5-Hydroxyicosatetraenoic acid and 5-oxo-eicosatetraenoic acid family of OXE1 receptor agonists (e.g., 5-HETE and 5-oxo-ETE); and N-Formylmethionine leucyl-phenylalanine and other N-formylated oligopeptides which are made by bacteria and activate the formyl peptide receptor 1.[rx]
Microbial fragments that remain after such digestion can serve as antigens. The fragments can be incorporated into MHC molecules and then trafficked to the cell surface of monocytes (and macrophages and dendritic cells). This process is called antigen presentation and it leads to activation of T lymphocytes, which then mount a specific immune response against the antigen.
Other microbial products can directly activate monocytes and this leads to the production of pro-inflammatory and, with some delay, of anti-inflammatory cytokines. Typical cytokines produced by monocytes are TNF, IL-1, and IL-12. Monocytic cells may contribute to the severity and disease progression in Covid-19 patients.[rx]
White blood cells, or leukocytes (Greek; leucko=white and cyte = cell), are part of the immune system participating in both the innate and humoral immune responses. They circulate in the blood and mount inflammatory and cellular responses to injury or pathogens. White blood cells are part of the body’s immune system. They help the body fight infection and other diseases. Types of white blood cells are granulocytes (neutrophils, eosinophils, and basophils), monocytes, and lymphocytes (T cells and B cells). Checking the number of white blood cells in the blood is usually part of a complete blood cell (CBC) test. It may be used to look for conditions such as infection, inflammation, allergies, and leukemia. Also called leukocyte and WBC.
White blood cells (WBC) are a heterogeneous group of nucleated cells that can be found in circulation for at least a period of their life. Their normal concentration in the blood varies between 4000 and 10,000 per microliter. They play a most important role in phagocytosis and immunity and therefore in defense against infection.
These normal ranges can vary by lab. Another common measurement for the volume of blood is cubic millimeter or mm3. A microliter and cubic millimeter equal the same amount. The types of cells that make up WBCs usually fall within a normal percentage of your overall WBC count.
The normal percentages of the types of WBCs in your overall count are usually in these ranges, according to the Leukemia & Lymphoma Society (LLS):
Type of WBC
Normal percentage of overall WBC count
neutrophil
55 to 73 percent
lymphocyte
20 to 40 percent
eosinophil
1 to 4 percent
monocyte
2 to 8 percent
basophil
0.5 to 1 percent
Higher or lower numbers of WBCs than normal can be a sign of an underlying condition.
Types of WBCs
The different types of white blood cells (leukocytes) include neutrophils, basophils, eosinophils, lymphocytes, monocytes, and macrophages.
White blood cells are much less common than red blood cells. There are five types of white blood cell (leucocyte). These are divided into two main classes
Granulocytes (includes Neutrophils, Eosinophils and Basophils)
Agranulocytes (includes Lymphocytes and Monocytes).
Key Points
The two main types of leukocytes are granulocytes and mononuclear leukocytes (agranulocytes).
Leukocytes arise from hemopoietic stem cells in the bone marrow.
Leukocytes are involved in pathogen recognition, phagocytosis (ingestion of particles), pathogen destruction, inflammation mediation, and antigen presentation.
Granulocytes include neutrophils, basophils, eosinophils, and mast cells. Their granules contain enzymes that damage or digest pathogens and release inflammatory mediators into the bloodstream.
Mononuclear leukocytes include lymphocytes, monocytes, macrophages, and dendritic cells. This group is involved in both innate and adaptive immune system functions.
Key Terms
endocytosed: Engulfed during the process by which the plasma membrane of a cell folds inwards to ingest the material.
antigen: A substance, usually foreign, that induces an immune response.
pathogen: Any organism or substance, especially a microorganism, capable of causing disease. Examples include bacteria, viruses, protozoa, or fungi. Microorganisms are not considered pathogenic until the population has grown large enough to cause disease.
White blood cells (WBCs), or leukocytes, are immune system cells that defend the body against infectious disease and foreign materials. There are several different types of WBCs. They share commonalities but are distinct in form and function. WBCs are produced in the bone marrow by hemopoietic stem cells, which differentiate into either lymphoid or myeloid progenitor cells. A major distinguishing feature is the presence of granules; white blood cells are often characterized as granulocytes or agranulocytes.
Structure
Leukocytes can be classified as granulocytes and agranulocytes based on the presence and absence of microscopic granules in their cytoplasm when stained with Giemsa or Leishman stains.
Granulocytes
Neutrophils, basophils, and eosinophils are all granulocytes. These cells also all have azurophilic granules (lysosomes) and specific granules that contain substances unique to each cell’s function. Histologically, granulocytes can be distinguished from one another by the morphology of their nucleus, their size, and how their granules stain.[1]
Neutrophils are 12 to 15 µm in diameter, have multi-lobed nuclei typically consisting of 3 to 5 segments joined by thin strands, or isthmuses. Thus, they are also called polymorphonuclear neutrophils. Neutrophils contain specific granules in the cytoplasm that cannot be resolved by light microscopy and therefore give the cytoplasm a pale pink color. Neutrophils, when activated, migrate into the tissues via diapedesis. These cells have life spans of a few days, and when activated in connective tissue, undergo apoptosis and are then removed by macrophages.
Eosinophils have a bi-lobed nucleus with large cytoplasmic specific granules that are eosinophilic, staining red to pink.
Basophils are 12 to15 µm in diameter, have bi-lobed or S-shaped nuclei, and contain cytoplasmic specific granules (0.5 µm) in diameter that stain blue to purple. The basophilia of the granules is due to the presence of heparin and sulfated glycosaminoglycans. These cells have similar functions as mast cells.
Agranulocytes
Agranulocytes consist of lymphocytes and monocytes, and while they lack specific granules, they do contain azurophilic granules.
Monocytes are precursor cells for the mononuclear phagocytic system, which include cells such as macrophages, osteoclasts, microglial cells in connective tissue and organs. These cells constitute 4 to 8% of white blood cells, are 12 to 15 µm in diameter, have large nuclei that are indented or C- shaped, which can be eccentric. There is abundant cytoplasm, and the lysosomal granules at the resolution of the light microscope give the cytoplasm bluish-gray color.
Lymphocytes constitute approximately 25% white blood cells, are of varying sizes, and have spherical nuclei. The small lymphocytes are similar in size to red blood cells, have spherical heterochromatic nuclei, and scant cytoplasm. Larger lymphocytes, such as activated lymphocytes, have indented nuclei and are 9 to 18 µm in diameter with more cytoplasm containing azurophilic granules. Lymphocytes subdivide into several groups using the cluster of differentiation (CD) markers. The major groups are B lymphocytes and T lymphocytes.
Granulocytes
Granulocytes, also known as polymorphonuclear (PMN) leukocytes, are characterized by stained granules within their cytoplasm under a microscope. These granules are membrane-bound enzymes that act primarily in the digestion of endocytosed particles. They may also cause granule-dependent cell-mediated apoptosis through the release of perforins, granzymes, and proteases. The nucleus contains multiple lobes (polymorphonuclear) as opposed to a single rounded lobe. Granulocytes contain toll-like receptors that allow them to recognize pathogen-associated molecular patterns (PAMPS). All categories except neutrophils contain IgE receptors that implicate them in allergic responses. There are four types of granulocytes:
Granulocytes: From left to right, a neutrophil, an eosinophil, and a basophil.
Neutrophils defend against bacterial or fungal infection and other very small inflammatory processes. They are usually the first responders to microbial infection. Their activity and death in large numbers from degranulation forms purulent necrosis (pus).
Eosinophils primarily deal with parasitic infections. They are also the predominant inflammatory cells in allergic reactions.
Basophils are chiefly responsible for short-term inflammatory response (particularly from allergy or irritation) by releasing the chemical histamine, which causes the vasodilation that occurs with inflammation.
Mast cells function similarly to basophils in that they often mediate inflammation, but are more common and arise from a different hemopoietic lineage.
Mononuclear Leukocytes
Mononuclear (MN) leukocytes are characterized by a single round nucleus within the cytoplasm. Some MN leukocytes contain granules while others do not, but the members of this group are sometimes considered agranulocytes by naming convention. MN leukocytes contain lysosomes, small vesicles containing digestive enzymes that break down foreign matter that is endocytosed by the cell during phagocytosis. The cells include:
Lymphocytes, which come in three types. B-lymphocytes produce antibodies in the humoral immune response. T-lymphocytes participate in the cell-mediated immune response. NK cells are cytotoxic cells that participate in the innate immune response by killing virally infected and tumor cells and mediating fever and long-lasting inflammation. B and T lymphocytes contain MHC antigen receptors and their activity is antigen-specific. Other leukocytes will attack any pathogen but cannot distinguish between different types of pathogens.
Monocytes are large leukocytes that differentiate into macrophages and dendritic cells under varying conditions, while performing similar functions in phagocytosis and antigen presentation (the process by which molecular components are presented to lymphocytes to stimulate an adaptive immune response). Monocytes and their progeny contain toll-like receptors and granules.
Macrophages are monocytes that have migrated out of the blood stream and into the internal body tissues. They destroy necrotic cell debris and foreign material including viruses and bacteria, and can present antigens to naive lymphocytes. They typically arrive at the site of inflammation one to three days after the initial neutrophil response to clean up dead neutrophils, cellular debris, and remaining pathogens.
Dendritic cells are monocytes that have migrated to cells that are in contact with the external environment, such as the skin, intestines, or respiratory epithelium. Their name comes branched projections called dendrites, which increase their surface area. They phagocytize pathogens and present antigens to naive lymphocytes.
A Macrophage: A macrophage phagocytizes two smaller particles, possibly pathogens
WBC Function
Each type of white blood cell (WBC) has a specific function in defending the body against infections.
Key Points
Leukocyte functions often occur in the bloodstream and may represent either the innate or adaptive immune systems.
Innate immune system functions are non-specific and include phagocytosis, inflammation, and degranulation.
Adaptive immune system functions are antigen-specific and involve antigen presentation as well as cell-mediated and humoral-mediated activities.
Compared to innate immune system functions, adaptive immune system functions take more time to initiate but work much faster. They have a memory component to prevent reinfection by the same pathogen.
Key Terms
macrophage: A white blood cell that phagocytizes necrotic cell debris and foreign material, including viruses, bacteria, and tattoo ink. It presents foreign antigens on MHC II molecules to lymphocytes. Part of the innate immune system.
Inflammation: An innate immune system function in response to a pathogen or injury. Chemical mediators cause the blood vessels to dilate and become more permeable, which draws neutrophils to the area.
cytotoxic: Any mechanism that can cause the death of a cell (typically without phagocytosis), such as degranulation or cell-mediated apoptosis.
Leukocytes ( white blood cells) provide a number of functions that are primarily related to defending the body from pathogens (foreign invaders). Much leukocyte activity takes place within the bloodstream but is not restricted to this area. Many leukocytes are able to perform their functions in tissues or organs during normal transport and in response to injury. Leukocyte functions may be classified as either innate or adaptive based on several characteristics.
Innate Immune System Functions
The innate immune system refers to the body’s ability to prevent pathogen entry and destroy pathogens that do enter the body. Its functions are rapid responses that inhibit a pathogen as soon as it is detected in the body. Innate immune system functions involving leukocytes include:
Phagocytosis of pathogens. This process is performed primarily by neutrophils, macrophages, and dendritic cells, but most other leukocytes can do it as well. It involves the binding of an Fc receptor to a tail on a pathogen. The pathogen is engulfed by the leukocyte and destroyed with enzymes and free radicals.
Inflammation. This process is performed primarily by mast cells, eosinophils, basophils, and NK cells. When a pathogen is detected or vascular endothelial cells release stress cytokines from injury such as a cut, leukocytes release a variety of inflammatory cytokines such as histamine or TNF-alpha. These cause vasodilation, increase vascular permeability, and promote neutrophil movement to the inflammation site.
Degranulation. This process is performed by granulocytes like neutrophils. When pathogens are encountered, granule-dependent apoptosis (a mechanism of cytotoxicity) may be induced in the pathogen by releasing perforins, granzymes, and proteases from their granules.
Neutrophils Phagocytizing Bacteria: Here, neutrophils are depicted phagocytizing and completely engulfing bacteria.
Adaptive Immune System Functions
The adaptive immune system is specific to each pathogen on the basis of antigens, molecular components of pathogens used by leukocytes to recognize that specific pathogen. Compared to the innate immune system, adaptive immune functions work much faster and have a memory component that prevents reinfection by the same pathogen. However, more time typically passes before the adaptive immune system is functional. Adaptive immune functions of leukocytes include:
Antigen presentation. This process is primarily performed by macrophages and dendritic cells. Following phagocytosis, protein components (antigens) of the pathogen are expressed on leukocyte MHC molecules and presented to naive T cells (and B cells) in the lymph nodes. The T cells will then start the adaptive immune response by rapidly proliferating and differentiating.
Cell-mediated activities. This process is performed by T cells. Pathogens that bear the T cell’s antigen are destroyed through cytotoxic-induced apoptosis and protease activity.
Humoral activities. This process is performed by B cells, which secrete antigen-specific antibodies. The antibodies bind to pathogens to opsonize (mark) them for phagocytes to engulf, neutralize, or start a complement cascade in which proteins form a membrane attack complex to lyse the pathogen.
Memory cell activity. Following antigen presentation, memory B and T cells are created. These rapidly produce new T cells or antibodies if the same pathogen is detected in the future. This prevents that pathogen from reinfecting the organism.
WBC Formation
Hematopoiesis refers to the formation of blood cell components. It is necessary for vertebrate function.
Key Points
Hematopoietic stem cells are self-renewing and reside in the medulla of the bone ( bone marrow ).
All blood cells are divided into two main lineages, produced through lymphoid progenitor cells or myeloid progenitor cells depending on lineage type.
Lymphoid progenitor cells differentiate into B and T cells and NK cells.
Myeloid progenitor cells differentiate into myelocytes (granulocytes and monocytes) or non-leukocytes such as erythrocytes and megakaryocytes (which produce platelets).
Before birth, most blood cell formation occurs in the liver or spleen, which tend to enlarge when used for hematopoiesis. In adults, most blood production occurs in the bone marrow.
Key Terms
myelocyte: A large cell found in the bone marrow that becomes a granulocyte or monocyte when mature.
differentiation: The gradual changes that occur when a cell or tissue type changes into a different type. Cells generally become more specialized the more they differentiate and are considered to be terminally differentiated when they cannot differentiate (and often cannot divide) any further.
megakaryocyte: A large cell found in bone marrow, responsible for the production of platelets.
Hematopoiesis refers to the formation of blood cellular components, including both white and red blood cells. All cellular blood components are derived from hematopoietic stem cells located within the bone marrow. In a healthy adult, approximately 1011–1012 new blood cells are produced daily to maintain equilibrium levels in the peripheral circulation.
Leukocyte Haematopoiesis
Hematopoietic stem cells (HSCs) reside in the bone marrow and have the unique ability to give rise to all mature blood cell types through differentiation into other progenitor cells. HSCs are self-renewing. When they proliferate, at least some daughter cells remain HSCs, so the pool of stem cells does not become depleted over time. The daughters are the myeloid and lymphoid progenitor cells, which cannot self renew but differentiate into various myeloid leukocytes and lymphocytes respectively. This is one of the body’s vital processes.
Leukocyte Lineages
Two different leukocyte lineages and two non-leukocyte lineages arise from the progeny of HSCs. Following this split in differentiation, the subtypes undergo eventual differentiation into terminally-differentiated leukocytes, which typically do not divide independently.
The lymphocyte lineage derives from common lymphoid progenitor cells, which in turn become lymphoblasts before differentiating into T cells, B cells, and NK cells.
Myelocytes are an offshoot of common myeloid progenitor cells, which also differentiate into the erythropoietic and magakaryotic progenitors. This diverse group differentiates into granulocytes and monocytes. Monocytes further differentiate into macrophages or dendritic cells upon reaching certain tissues.
Megakaryocytes (the cells that produce platelets) and erythrocytes (red blood cells) are not formally considered to be leukocytes, but arise from the common myeloid progenitor cells that produce the other cellular components of blood.
Hematopoiesis in Humans: This diagram shows hematopoiesis as it occurs in humans.
Sites of Hematopoiesis in Pre- and Postnatal Periods
In developing embryos, blood formation occurs in aggregates of blood cells in the yolk sac called blood islands. However, most of the blood supply comes from the mother through the placenta. As development progresses, blood formation occurs primarily in the spleen, liver, and lymph nodes.
When bone marrow develops, it eventually assumes the task of forming most of the blood cells for the entire organism. However, maturation, activation, and some proliferation of lymphoid cells occur in lymphoid organs (spleen, thymus, and lymph nodes). In children, hematopoiesis occurs in the marrow of the long bones such as the femur and tibia. In adults, it occurs mainly in the pelvis, cranium, vertebrae, and sternum.
In some cases, the liver, thymus, and spleen may resume their hematopoietic function if necessary. This is called extramedullary hematopoiesis. It may cause these organs to hypertrophy and increase in size substantially. During fetal development, the liver functions as the main haematopoetic organ since bones and marrow develop later. Therefore, the liver is enlarged during development relative to its mature proportions.
Disorders
The two commonly used categories of white blood cell disorders divide them quantitatively into those causing excessive numbers (proliferative disorders) and those causing insufficient numbers (leukopenias).[rx] Leukocytosis is usually healthy (e.g., fighting an infection), but it also may be dysfunctionally proliferative. WBC proliferative disorders can be classed as myeloproliferative and lymphoproliferative. Some are autoimmune, but many are neoplastic.
Another way to categorize disorders of white blood cells is qualitative. There are various disorders in which the number of white blood cells is normal but the cells do not function normally.[rx]
Neoplasia of WBCs can be benign but is often malignant. Of the various tumors of the blood and lymph, cancers of WBCs can be broadly classified as leukemias and lymphomas, although those categories overlap and are often grouped as a pair.
Leucopenias
A range of disorders can cause decreases in white blood cells. This type of white blood cell decreased is usually the neutrophil. In this case the decrease may be called neutropenia or granulocytopenia. Less commonly, a decrease in lymphocytes (called lymphocytopenia or lymphopenia) may be seen.[rx]
Neutropenia
Neutropenia can be acquired or intrinsic.[rx] A decrease in levels of neutrophils on lab tests is due to either decreased production of neutrophils or increased removal from the blood.[rx] The following list of causes is not complete.
Medications – chemotherapy, sulfates or other antibiotics, phenothiazines, benzodiazepines, antithyroid, anticonvulsants, quinine, quinidine, indomethacin, procainamide, thiazides
Symptoms of neutropenia are associated with the underlying cause of the decrease in neutrophils. For example, the most common cause of acquired neutropenia is drug-induced, so an individual may have symptoms of medication overdose or toxicity. Treatment is also aimed at the underlying cause of neutropenia.[rx] One severe consequence of neutropenia is that it can increase the risk of infection.[rx]
Lymphocytopenia
Defined as total lymphocyte count below 1.0×109/L, the cells most commonly affected are CD4+ T cells. Like neutropenia, lymphocytopenia may be acquired or intrinsic and there are many causes.[rx] This is not a complete list.
Inherited immune deficiency – severe combined immunodeficiency, common variable immune deficiency, ataxia-telangiectasia, Wiskott–Aldrich syndrome, immunodeficiency with short-limbed dwarfism, immunodeficiency with thymoma, purine nucleoside phosphorylase deficiency, genetic polymorphism
Blood cell dysfunction – aplastic anemia
Infectious diseases – viral (AIDS, SARS, West Nile encephalitis, hepatitis, herpes, measles, others), bacterial (TB, typhoid, pneumonia, rickettsiosis, ehrlichiosis, sepsis), parasitic (acute phase of malaria)
Nutritional/Dietary – alcohol use disorder, zinc deficiency
Like neutropenia, symptoms and treatment of lymphocytopenia are directed at the underlying cause of the change in cell counts.
Proliferative disorders
An increase in the number of white blood cells in circulation is called leukocytosis.[rx] This increase is most commonly caused by inflammation.[rx] There are four major causes: increase of production in bone marrow, increased release from storage in bone marrow, decreased attachment to veins and arteries, decreased uptake by tissues.[rx] Leukocytosis may affect one or more cell lines and can be neutrophilic, eosinophilic, basophilic, monocytosis, or lymphocytosis.
Neutrophilia
Neutrophilia is an increase in the absolute neutrophil count in the peripheral circulation. Normal blood values vary by age.[rx] Neutrophilia can be caused by a direct problem with blood cells (primary disease). It can also occur as a consequence of an underlying disease (secondary). Most cases of neutrophilia are secondary to inflammation.[rx]
Chronic inflammation – especially juvenile rheumatoid arthritis, rheumatoid arthritis, Still’s disease, Crohn’s disease, ulcerative colitis, granulomatous infections (for example, tuberculosis), and chronic hepatitis
Cigarette smoking – occurs in 25–50% of chronic smokers and can last up to 5 years after quitting
Stress – exercise, surgery, general stress
Medication-induced – corticosteroids (for example, prednisone, β-agonists, lithium)
Cancer – either by growth factors secreted by the tumor or invasion of bone marrow by the cancer
Increased destruction of cells in peripheral circulation can stimulate bone marrow. This can occur in hemolytic anemia and idiopathic thrombocytopenic purpura
Eosinophilia
A normal eosinophil count is considered to be less than 0.65×109/L.[rx] Eosinophil counts are higher in newborns and vary with age, time (lower in the morning and higher at night), exercise, environment, and exposure to allergens.[rx] Eosinophilia is never a normal lab finding. Efforts should always be made to discover the underlying cause, though the cause may not always be found.[rx]
Red blood cells (RBC), are the functional component of blood responsible for the transportation of gases and nutrients throughout the human body. Their unique shape and composition allow for these specialized cells to carry out their essential functions. The role of the erythrocyte is critical in investigating many disease processes in a variety of body systems. Their structure, function, physiology, preparation, microscopy, and clinical importance are the subject of this review article.
Red blood cells (RBCs), also referred to as red cells red blood corpuscles (in humans or other animals not having nucleus in red blood cells), haematids, erythroid cells, or erythrocytes are the most common type of blood cell and the vertebrate’s principal means of delivering oxygen (O2) to the body tissues—via blood flow through the circulatory system.[rx] RBCs take up oxygen in the lungs, or in fish the gills, and release it into tissues while squeezing through the body’s capillaries.
RBC Anatomy
Red blood cells lack nuclei and have a biconcave shape.
Key Points
The biconcave shape allows RBCs to bend and flow smoothly through the body’s capillaries. It also facilitates oxygen transport.
Red blood cells are considered cells, but they lack a nucleus, DNA, and organelles like the endoplasmic reticulum or mitochondria.
Red blood cells cannot divide or replicate like other bodily cells. They cannot independently synthesize proteins.
The blood’s red color is due to the spectral properties of the hemic iron ions in hemoglobin.
Each human red blood cell contains approximately 270 million hemoglobin biomolecules, each carrying four heme groups to which oxygen binds.
Key Terms
iron: A metallic chemical element with atomic number 26 and symbol Fe. Iron-containing enzymes and proteins, often containing heme prosthetic groups, participate in many biological oxidations and in transport.
hemoglobin: The iron-containing substance in RBCs that transports oxygen from the lungs to the rest of the body. It consists of a protein (globulin) and haem (a porphyrin ring with an atom of iron at its center).
Human erythrocytes or red blood cells (RBCs) are the primary cellular component of blood. They are involved in oxygen transport through the body and have features that distinguish them from every other type of human cell. Adult humans have roughly 20-30 trillion RBCs at any given time, comprising approximately one-quarter of the total number of human cells.
External Structure
RBCs are disc-shaped with a flatter, concave center. This biconcave shape allows the cells to flow smoothly through the narrowest blood vessels. Gas exchange with tissues occurs in capillaries, tiny blood vessels that are only as wide as one cell. Many RBCs are wider than capillaries, but their shape provides the needed flexibility to squeeze through.
A typical human RBC has a disk diameter of 6–8 micrometers and a thickness of 2 micrometers, much smaller than most other human cells. These cells have an average volume of about 90 femtoliters (fL) with a surface area of about 136 square micrometers. They can swell up to a sphere shape containing 150 fL without bursting their cell membrane. When the shape does change, it inhibits their ability to carry oxygen or participate in gas exchange. This occurs in people with spherocytic (sphere-shaped) anemia or sickle-cell anemia.
Internal Structure
Although RBCs are considered cells, they lack a nucleus, nuclear DNA, and most organelles, including the endoplasmic reticulum and mitochondria. RBCs therefore cannot divide or replicate like other labile cells of the body. They also lack the components to express genes and synthesize proteins. While most cells have chemotaxis ways to travel through the body, RBCs are carried through the body by blood flow and pressure alone.
Hemoglobin molecules are the most important component of RBCs. Hemoglobin is a specialized protein that contains a binding site for the transport of oxygen and other molecules. The RBCs’ distinctive red color is due to the spectral properties of the binding of hemic iron ions in hemoglobin. Each human red blood cell contains approximately 270 million of these hemoglobin biomolecules, each carrying four heme groups (individual proteins). Hemoglobin comprises about a third of the total RBC volume. This protein is responsible for the transport of more than 98% of the oxygen, while the rest travels as dissolved molecules through the plasma.
RBC Physiology
The primary functions of red blood cells (RBCs) include carrying oxygen to all parts of the body, binding to hemoglobin, and removing carbon dioxide.
Key Points
Red blood cells contain hemoglobin, which contains four iron-binding heme groups.
Oxygen binds the heme groups of hemoglobin. Each hemoglobin molecule can bind four oxygen molecules.
The binding affinity of hemoglobin for oxygen is cooperative. It is increased by the oxygen saturation of the molecule. The binding of an initial oxygen molecule influences the shape of the other binding sites. This makes binding more favorable for additional oxygen molecules.
Each hemoglobin molecule contains four iron-binding heme groups which are the site of oxygen binding. Oxygen-bound hemoglobin is called oxyhemoglobin.
Red blood cells alter blood pH by catalyzing the reversible carbon dioxide to carbonic acid reaction through the enzyme carbonic anhydrase.
pH is also controlled by carbon dioxide binding to hemoglobin instead of being converted to carbonic acid.
Key Terms
carbonic anhydrase: The enzyme found in RBCs that catalyzes the reaction between carbonic acid and carbon dioxide and water.
cooperative binding: In binding in which multiple molecules can potentially bind to multiple binding sites when a first molecule is bound to a binding site, the same molecule is favored for the rest of the binding sites through increased binding affinity.
Red blood cells (RBCs) perform a number of human respiratory and cardiovascular system functions. Most of these functions are attributed to hemoglobin content. The main RBC functions are facilitating gas exchange and regulating blood pH.
Gas Exchange
Heme: This is a diagram of the molecular structure of heme.
RBCs facilitate gas exchange through a protein called hemoglobin. The word hemoglobin comes from “hemo” meaning blood and “globin” meaning protein. Hemoglobin is a quaternary structure protein consisting of many smaller tertiary structure proteins composed of amino acid polypeptide chains. Each hemoglobin molecule contains four iron-binding heme groups, which are the site of oxygen (O2) binding. Oxygen-bound hemoglobin is called oxyhemoglobin.
The binding of oxygen is a cooperative process. Hemoglobin bound oxygen causes a gradual increase in oxygen-binding affinity until all binding sites on the hemoglobin molecule are filled. As a result, the oxygen-binding curve of hemoglobin (also called the oxygen saturation or dissociation curve) is sigmoidal, or S-shaped, as opposed to the normal hyperbolic curve associated with noncooperative binding. This curve shows the saturation of oxygen bound to hemoglobin compared to the partial pressure of oxygen (concentration) in blood.
Oxygen saturation curve: Due to cooperative binding, the oxygen saturation curve is S-shaped.
pH Control
RBCs control blood pH by changing the form of carbon dioxide within the blood. Carbon dioxide is associated with blood acidity. That’s because most carbon dioxide travels through the blood as a bicarbonate ion, which is the dissociated form of carbonic acid in the solution. The respiratory system regulates blood pH by changing the rate at which carbon dioxide is exhaled from the body, which involves the RBC’s molecular activity. RBCs alter blood pH in a few different ways.
Quaternary structure: hemoglobin: Hemoglobin is a globular protein composed of four polypeptide subunits (two alpha chains, in blue, and two beta-pleated sheets, in red). The heme groups are the green structures nestled among the alpha and beta.
RBCs secrete the enzyme carbonic anhydrase, which catalyzes the conversion of carbon dioxide and water to carbonic acid. This dissociates in solution into bicarbonate and hydrogen ions, the driving force of pH in the blood. This reaction is reversible by the same enzyme. Carbonic anhydrase also removes water from carbonic acid to turn it back into carbon dioxide and water. This process is essential so carbon dioxide can exist as a gas during a gas exchange in the alveolar capillaries. As carbon dioxide is converted from its dissolved acid form and exhaled through the lungs, blood pH becomes less acidic. This reaction can occur without the presence of RBCs or carbonic anhydrase but at a much slower rate. With the catalyst activity of carbonic anhydrase, this reaction is one of the fastest in the human body.
Hemoglobin can also bind to carbon dioxide, which creates carbamino-hemoglobin. When carbon dioxide binds to hemoglobin, it doesn’t exist in the form of carbonic acid, which makes the blood less acidic and increases blood pH. However, because of allosteric effects on the hemoglobin molecule, the binding of carbon dioxide decreases the amount of oxygen bound for a given partial pressure of oxygen. This decrease in hemoglobin’s affinity for oxygen by the binding of carbon dioxide is known as the Bohr effect, which results in a rightward shift to the O2-saturation curve. Conversely, when the carbon dioxide levels in the blood decrease (i.e., in the lung capillaries), carbon dioxide and hydrogen ions are released from hemoglobin, increasing the oxygen affinity of the protein. A reduction in the total binding capacity of hemoglobin to oxygen (i.e. shifting the curve down, not just to the right) due to reduced pH is called the Haldane effect.
Red blood cell count
A red blood cell (RBC) count is a blood test that tells you how many red blood cells you have.
Red blood cells contain a substance called hemoglobin, which transports oxygen around the body. The amount of oxygen that’s delivered to your body’s tissues depends on the number of red blood cells you have and how well they work. An RBC count is usually carried out as part of a full blood cell (FBC) count. Women usually have a lower RBC count than men, and the level of red blood cells tends to decrease with age.
A normal RBC count would be
men – 4.7 to 6.1 million cells per microlitre (cells/mcL)
women – 4.2 to 5.4 million cells/mcL
The results of an RBC count can be used to help diagnose blood-related conditions, such as iron deficiency anemia (where there are fewer red blood cells than normal).
RBC Life Cycle
Human erythrocytes are produced through a process called erythropoiesis. They take about seven days to mature.
Key Points
After about 100-120 days, RBCs are removed from circulation through a process called eryptosis.
Erythropoiesis is the process by which human erythrocytes are produced. It is triggered by erythropoietin, a kidney hormone produced during hypoxia.
Erythropoiesis takes place in the bone marrow, where hemopoietic stem cells differentiate and eventually shed their nuclei to become reticulocytes. Iron, vitamin B12, and folic acid are required for hemoglobin synthesis and normal RBC maturation.
Reticulocytes mature into normal, functional RBCs after 24 hours in the bloodstream.
Following eryptosis, the liver breaks down old hemoglobin into biliverdin and iron. The iron is taken back to the bone marrow for reuse by transferrins, while biliverdin is broken down into bilirubin and excreted through the digestive system bile.
Key Terms
erythropoietin: A hormone produced by the kidneys in response to hypoxia, which stimulates erythropoiesis.
bilirubin: A bile pigment that arises when biliverdin is separated from the iron of old hemoglobin molecules in the liver. Bilirubin becomes part of bile salts in the digestive system and is excreted, while the iron content is reused.
Human erythrocytes are produced through a process called erythropoiesis, developing from committed stem cells to mature erythrocytes in about seven days. When matured, these cells circulate in the blood for about 100 to 120 days, performing their normal function of molecule transport. At the end of their lifespan, they degrade and are removed from circulation.
Scanning electron micrograph of blood cells: Shown on the left, the erythrocyte, or red blood cell, has a round, donut-like shape.
Erythropoiesis
Erythropoiesis is the process in which new erythrocytes are produced, which takes about seven days. Erythrocytes are continuously produced in the red bone marrow of large bones at a rate of about 2 million cells per second in a healthy adult. Erythrocytes differentiate from erythropoietic bone marrow cells, a type of hemopoietic stem cell found in the bone marrow. Unlike mature RBCs, bone marrow cells contain a nucleus. In the embryo, the liver is the main site of red blood cell production and bears similar types of stem cells at this stage of development.
Erythropoiesis can be stimulated by the hormone erythropoietin, which is synthesized by the kidney in response to hypoxia (systemic oxygen deficiency). In the last stages of development, immature RBCs absorb iron, Vitamin B12, and folic acid. These dietary nutrients are necessary for the proper synthesis of hemoglobin (iron) and normal RBC development (B12 and folic acid). Deficiency of any of these nutrients may cause anemia, a condition in which there aren’t enough fully functional RBCs carrying oxygen in the bloodstream. Just before and after leaving the bone marrow, the developing cells are known as reticulocytes. These immature RBCs have shed their nuclei following initial differentiation. After 24 hours in the bloodstream, reticulocytes mature into functional RBCs.
Eryptosis
Eryptosis, a form of apoptosis (programmed cell death), is the aging and death of mature RBCs. As an RBC age, it undergoes changes in its plasma membrane that make it susceptible to selective recognition by macrophages and subsequent phagocytosis in the reticuloendothelial system (spleen, liver, and bone marrow). This process removes old and defective cells and continually purges the blood. Eryptosis normally occurs at the same rate as erythropoiesis, keeping the total circulating red blood cell count in a state of equilibrium. Many diseases that involve damage to RBCs (hemolytic anemias, sepsis, malaria, pernicious or nutritional anemias) or normal cellular processes that cause cellular damage (oxidative stress) may increase the rate of eryptosis. Conversely, erythropoietin and nitric oxide (a vasodilator) will inhibit eryptosis.
Following eryptosis, the hemoglobin content within the RBC is broken down and recirculated throughout the body. The heme components of hemoglobin are broken down into iron ions and a green bile pigment called biliverdin. The biliverdin is reduced to the yellow bile pigment bilirubin, which is released into the plasma and recirculated to the liver, then bound to albumin and stored in the gallbladder. The bilirubin is excreted through the digestive system in the form of bile, while some of the iron is released into the plasma to be recirculated back into the bone marrow by a carrier protein called transferrin. This iron is then reused for erythropoiesis, but additional dietary iron is needed to support healthy RBC life cycles.
Red blood cells (RBCs), also called erythrocytes, are cells that circulate in the blood and carry oxygen throughout the body. The RBC count totals the number of red blood cells that are present in your sample of blood. It is one test among several that is included in a complete blood count (CBC) and is often used in the general evaluation of a person’s health.
Blood is made up of a few different types of cells suspended in fluid called plasma. In addition to RBCs, there are white blood cells (WBCs) and platelets. These cells are produced in the bone marrow and are released into the bloodstream as they mature. RBCs typically make up about 40% of the blood volume. RBCs contain hemoglobin, a protein that binds to oxygen and enables RBCs to carry oxygen from the lungs to the tissues and organs of the body. RBCs also help transport a small portion of carbon dioxide, a waste product of cell metabolism, from those tissues and organs back to the lungs, where it is expelled.
The typical lifespan of an RBC is 120 days. Thus the bone marrow must continually produce new RBCs to replace those that age and degrade or are lost through bleeding. A number of conditions can affect RBC production and some conditions may result in significant bleeding. Other disorders may affect the lifespan of RBCs in circulation, especially if the RBCs are deformed due to an inherited or acquired defect or abnormality. These conditions may lead to a rise or drop in the RBC count. Changes in the RBC count usually mirror changes in other RBC tests, including the hematocrit and hemoglobin level.
If RBCs are lost or destroyed faster than they can be replaced if bone marrow production is disrupted, or if the RBCs produced do not function normally, or do not contain enough hemoglobin, then you may develop anemia, which affects the amount of oxygen reaching tissues.
If too many RBCs are produced and released, then you can develop polycythemia. This can cause thicker blood, decreased blood flow, and related problems, such as headache, dizziness, problems with vision, and even excessive clotting or heart attack.
How is the test used?
A red blood cell (RBC) count is typically ordered as part of a complete blood count (CBC) and may be used as part of a health checkup to screen for a variety of conditions. This test may also be used to help diagnose and/or monitor a number of diseases that affect the production or lifespan of red blood cells.
When is it ordered?
An RBC count is ordered as a part of the complete blood count (CBC), often as part of a routine physical or as part of a pre-surgical workup. A CBC may be ordered when you have signs and symptoms suggesting a disease that might affect red blood cell production. Some common signs and symptoms associated with anemia that generally lead to a healthcare practitioner ordering a CBC are:
Weakness or fatigue
Lack of energy
Paleness
Some signs and symptoms that may appear with a high RBC count include
Disturbed vision
Headache, dizziness
Flushing
Enlarged spleen
A CBC may also be performed on a regular basis to monitor people who have been diagnosed with conditions such as
Bone marrow disorders
Kidney disease
Bleeding problems
Chronic anemia
Polycythemia
Cancer, like chemotherapy or radiation therapy, often decreases bone marrow production of all the blood cells
What does the test result mean?
Since an RBC count is performed as part of a complete blood count (CBC), results from other components are taken into consideration. A rise or drop in the RBC count must be interpreted in conjunction with other tests, such as hemoglobin, hematocrit, reticulocyte count, and/or red blood cell indices.
The following table summarizes what results may mean.
Test
Reference Range
Examples of Causes of Low Result
Examples of Causes of High Result
Red Blood Cell Count (RBC)
Conventional Units
Men: 4.5-5.9 x 106/microliter
Women: 4.1-5.1 x 106 microliter
SI Units
Men: 4.5-5.9 x 1012/L
Women: 4.1-5.1 x 1012/L
Known as anemia
Acute or chronic bleeding
RBC destruction (e.g., hemolytic anemia, etc.)
Nutritional deficiency (e.g., iron deficiency, vitamin B12 or folate deficiency)
Bone marrow disorders or damage
Chronic inflammatory disease
Chronic kidney disease
Known as polycythemia
Dehydration
Lung (pulmonary) disease
Kidney or another tumor that produces excess erythropoietin
Smoking
Living at high altitude
Genetic causes (altered oxygen sensing, abnormality in hemoglobin oxygen release)
Polycythemia vera—a rare disease
from Henry’s Clinical Diagnosis and Management by Laboratory Methods. 22nd ed.
McPherson R, Pincus M, eds. Philadelphia, PA: Elsevier Saunders; 2011.
Note: Conventional Units are typically used for reporting results in U.S. labs;
SI Units are used to report lab results outside of the U.S.
Some causes of a low RBC count (anemia) include
Trauma that leads to loss of blood
Conditions that cause red blood cells to be destroyed, such as hemolytic anemia caused by autoimmunity or defects in the red cell itself; the defects could be a hemoglobinopathy (e.g., sickle cell anemia), thalassemia, an abnormality in the RBC membrane (e.g., hereditary spherocytosis), or enzyme defect (e.g., G6PD deficiency).
Sudden (acute) or chronic bleeding from the digestive tract (e.g., ulcers, polyps, colon cancer) or other sites, such as the bladder or uterus (in women, heavy menstrual bleeding, for example)
Nutritional deficiency such as iron deficiency or vitamin B12 or folate deficiency
Bone marrow damage (e.g., toxin, radiation or chemotherapy, infection, drugs)
Bone marrow disorders such as leukemia, multiple myeloma, myelodysplastic syndrome, or lymphoma or other cancers that spread to the bone marrow
Chronic inflammatory disease or condition
Kidney failure—severe and chronic kidney diseases lead to decreased production of erythropoietin, a hormone produced by the kidneys that promote RBC production by the bone marrow.
Some causes of a high RBC count (polycythemia) include
Dehydration – as the volume of fluid in the blood drops, the count of RBCs per volume of fluid artificially rises.
Lung (pulmonary) disease – if someone is unable to breathe in and absorb sufficient oxygen, the body tries to compensate by producing more red blood cells.
Congenital heart disease – with this condition, the heart is not able to pump blood efficiently, resulting in a decreased amount of oxygen getting to tissues. The body tries to compensate by producing more red blood cells.
Kidney tumor that produces excess erythropoietin
Smoking
Genetic causes (altered oxygen sensing, abnormality in hemoglobin oxygen release)
Polycythemia vera—a rare disease in which the body produces too many RBCs
My RBC count is slightly out of range. What does this mean?
Your RBC count is interpreted by your healthcare practitioner within the context of other tests that you have had done as well as other factors, such as your medical history. A single result that is slightly high or low may or may not have medical significance. There are several reasons why a test result may differ on different days and why it may fall outside a designated reference range.
Biological variability (different results in the same person at different times): If you have the same test done on several different occasions, there’s a good chance that one result will fall outside a reference range even though you are in good health. For biological reasons, your values can vary from day today.
Individual variability (differences in results between different people): References ranges are usually established by collecting results from a large population and determining from the data an expected average result and expected differences from that average (standard deviation). There are individuals who are healthy but whose tests results, which are normal for them, do not always fall within the expected range of the overall population.
A test value that falls outside of the established reference range supplied by the laboratory may mean nothing significant. Generally, this is the case when the test value is only slightly higher or lower than the reference range and this is why a healthcare practitioner may repeat a test on you and why they may look at results from prior times when you had the same test performed.
However, a result outside the range may indicate a problem and warrant further investigation. Your healthcare provider will consider your medical history, physical exam, and other relevant factors to determine whether a result that falls outside of the reference range means something significant for you.
If my RBC Count is out of range, what other tests might be done?
An RBC count can be used to detect a problem with red blood cell production and/or lifespan, but it cannot determine the underlying cause. In addition to the full CBC, some other tests may be performed at the same time or as a follow-up to help establish a diagnosis. Examples include:
Blood smear—a laboratory professional examines the blood under the microscope to confirm results of a CBC and/or to look abnormal blood cells
Reticulocyte count—determines the number of young (immature) red blood cells
Iron studies—iron is important in the production of red blood cells
Vitamin B12 and folate levels—these vitamins are also important for red blood cell production
In more severe conditions, a bone marrow aspiration and biopsy—usually done by a pathologist to help detect abnormalities in the bone marrow and determine the cause of low or high blood cell counts or abnormal blood cells
How treatable are abnormal red blood cell counts?
First, a healthcare practitioner must determine the cause of someone’s abnormal RBC count so the appropriate treatment can be prescribed. For some anemias, treatment may include a dietary supplement or a change in diet to include nutritional foods. In some instances, it may only require a change in the person’s current medication. For more severe cases, treatment may involve transfusion with blood from a donor. For some, prescribing a drug to stimulate red cell production in the bone marrow may be required, especially for people who have received chemotherapy or radiation treatments.
How to Increase Your Red Blood Cell Count
Anemia and red blood cell count
Are you feeling weak or fatigued? You may be experiencing symptoms of anemia. Anemia occurs when your red blood cell (RBC) count is low. If your RBC count is low, your body has to work harder to deliver oxygen throughout your body.
RBCs are the most common cells in human blood. The body produces millions each day. RBCs are produced in the bone marrow and circulate around the body for 120 days. Then, they go to the liver, which destroys them and recycles their cellular components.
Anemia can put you at risk for a number of complications, so it’s important to get your RBC levels back on track as soon as possible.
Keep reading to learn how to increase your RBCs at home, how your doctor can help, and more.
5 nutrients that increase red blood cell counts
Eating foods rich in these five nutrients can help you improve your red blood cell levels.
Iron
Eating an iron-rich diet can increase your body’s production of RBCs. Iron-rich foods include:
red meat, such as beef
organ meat, such as kidney and liver
dark, leafy, green vegetables, such as spinach and kale
dried fruits, such as prunes and raisins
beans
legumes
egg yolks
Folic acid
Adding certain B vitamins to your diet can also be beneficial. Foods high in vitamin B-9 (folic acid) include:
enriched bread
enriched cereals
dark, leafy, green vegetables, such as spinach and kale
beans
lentils
peas
nuts
Vitamin B-12
Foods high in vitamin B-12 include:
red meat, such as beef
fish
dairy products, such as milk and cheese
eggs
Copper
Copper intake doesn’t directly result in RBC production, but it can help your RBCs access the iron they need to replicate. Foods high in copper include:
poultry
shellfish
liver
beans
cherries
nuts
Vitamin A
Vitamin A (retinol) also supports RBC production in this manner. Foods rich in vitamin A include:
dark, leafy green vegetables, such as spinach and kale
sweet potatoes
squash
carrots
red peppers
fruits, such as watermelon, grapefruit, and cantaloupe
8 supplements that increase red blood cell counts
If you aren’t getting enough key nutrients through your diet, you may want to talk to your doctor about taking supplements. Certain supplements can help increase your RBC production or support related processes in your body.
Some supplements can interact with medications that you may be taking, so be sure to get your doctor’s approval before adding them to your regimen.
Never take more than the recommended dosage found on the product’s label.
Supplements your doctor may suggest include
Iron – Iron deficiency commonly causes low RBC production. Women need about 18 milligrams (mg) per day, whereas men only need 8 mg per day.
Vitamin C – This vitamin may help your body better absorb iron. The average adult needs about 500 mg per day.
Copper – There may also be a link between low RBC production and copper deficiency. Women need 18 mg per day, and men need 8 mg per day. However, your daily copper requirement depends on a variety of factors, including sex, age, and body weight. Be sure to consult your doctor or a dietitian to understand how much you need.
Vitamin A (retinol) – Women need 700 micrograms (mcg) per day. For men, the recommendation increases to 900 mcg.
Vitamin B-12 – Most people who are 14 years and older need 2.4 mcg of this vitamin per day. If you’re pregnant, the recommended dosage raises to 2.6 mcg. If you’re breastfeeding, it jumps to 2.8 mcg.
Vitamin B-9 (folic acid) – The average person needs between 100 and 250 mcg per day. If you regularly menstruate, it’s recommended that you take 400 mcg. Women who are pregnant need 600 mcg per day.
Vitamin B-6 – Women need about 1.5 mg of this nutrient each day, and men need about 1.7 mg.
Vitamin E – The average adult needs about 15 mg per day.
How to Increase the Absorption of Iron From Foods
Iron is an essential mineral your body needs to function properly.
Thus, it’s vitally important to consume adequate amounts of it in your daily diet. Interestingly, the foods you eat influence not only how much iron you consume, but also how well it is absorbed into your body [rx].
Once it’s absorbed by your body, it’s used as a building block for hemoglobin, a protein found in red blood cells that helps shuttle oxygen around your body. Iron is also a component of myoglobin, an oxygen storage protein found in your muscles. This oxygen is used when you use your muscles.
The recommended intake range is 7–18 mg per day for the general population and up to 27 grams for pregnant women [rx].
Which Foods Contain It?
You may have heard that you can get iron from red meat, but there are many other foods that naturally contain iron.
In foods, iron is present in two forms: heme and non-heme.
Sources of Heme Iron
Heme iron is found in animal foods that contain hemoglobin, such as meat, fish and poultry.
Heme iron is the best form of iron, as up to 40% of it is readily absorbed by your body [rx].
Good food sources of heme iron include:
Beef
Pork
Chicken
Veal
Fish such as halibut, haddock, perch, salmon or tuna
Shellfish such as clams, oysters and mussels
Red meats and organ meats like liver are particularly good sources.
Sources of Non-Heme Iron
Non-heme iron primarily comes from plant sources and is present in grains, vegetables and fortified foods.
This is the form added to foods enriched or fortified with iron, as well as many supplements.
It’s estimated that 85–90% of total iron intake comes from the non-heme form, while 10–15% comes from the heme form [rx].
In terms of its bioavailability, non-heme iron is absorbed much less efficiently than heme iron.
Good sources of non-heme iron include:
Fortified cereals, rice, wheat and oats
Dark green leafy vegetables like spinach and kale
Dried fruits like raisins and apricots
Beans like lentils and soybeans
Heme iron is found in animal foods, while non-heme iron comes from plant sources. The heme form is better absorbed by your body than the non-heme form
Certain Populations May Be at Risk of Deficiency
Iron deficiency is the most common cause of anemia, which affects a billion people worldwide [rx].
A person who is iron deficient may have various symptoms, including fatigue, dizziness, headaches, sensitivity to cold, and shortness of breath when doing simple tasks.
Moreover, iron deficiency can result in poorer attention span and mental function. In fact, being deficient during early childhood has been linked to lower IQs [rx]
Children, adolescents, and women of reproductive age, particularly during pregnancy, are most at risk of iron deficiency. This is because their intake doesn’t meet their body’s high demand for it [rx]
Additionally, it’s commonly thought that vegetarians and vegans are more prone to iron deficiency. But, interestingly, studies have shown that vegetarian and vegan diets contain just as much iron, if not more, than diets containing meat
However, although vegetarians may consume as much iron as non-vegetarians, a review found that they are still at greater risk of deficiency [rx]
This is because they consume mainly non-heme iron, which is not absorbed as well as the heme form in animal products.
It’s generally recommended that vegetarians multiply their recommended iron intake by 1.8 times to compensate for the reduced absorption [rx].