The peritoneum is the serous membrane that lines the abdominal cavity. It is composed of mesothelial cells that are supported by a thin layer of fibrous tissue and is embryologically derived from the mesoderm. The peritoneum serves to support the organs of the abdomen and acts as a conduit for the passage of nerves, blood vessels, and lymphatics. Although the peritoneum is thin, it is made of 2 layers with a potential space between them. The potential space between the 2 layers contains about 50 to 100 ml of serous fluid that prevents friction and allows the layers and organs to glide freely.[rx] The outer layer is the parietal peritoneum, which attaches to the abdominal and pelvic walls. The inner visceral layer wraps around the internal organs located inside the intraperitoneal space. The structures bound by the peritoneal cavity may be intraperitoneal or retroperitoneal.
Structure and Function
The boundaries of the peritoneal cavity include:
Anterior abdominal muscles
Vertebrae
Pelvic floor
Diaphragm
The peritoneum is comprised of 2 layers: the superficial parietal layer and the deep visceral layer. The peritoneal cavity contains the omentum, ligaments, and mesentery. Intraperitoneal organs include the stomach, spleen, liver, first and fourth parts of the duodenum, jejunum, ileum, transverse, and sigmoid colon. Retroperitoneal organs lie behind the posterior sheath of the peritoneum and include the aorta, esophagus, second and third parts of the duodenum, ascending and descending colon, pancreas, kidneys, ureters, and adrenal glands.
An important space in the peritoneal cavity is the epiploic foramen, also known as the foramen of Winslow. This foramen allows communication between the greater and lesser sacs. It is bordered by the hepatoduodenal ligament anteriorly, the inferior vena cava (IVC) posteriorly, the duodenum inferiorly, and the caudate lobe of the liver superiorly. The foramen provides access to a surgeon, should they need to clamp the hepatoduodenal ligament to stop a hemorrhage or gain anatomical access to the lesser sac. The foramen can also serve as a location for a lesser sac hernia.
The greater omentum loosely hangs from the greater curvature of the stomach and folds over the anterior of the intestine before curving back superiority to attach to the transverse colon. It acts as a protective or insulating layer. The mesentery helps attach the abdominal organs to the abdominal wall and contains many blood vessels, nerves, and lymphatics. Intraperitoneal organs are usually mobile while those in the retroperitoneum are usually fixed to the posterior abdominal wall. The dorsal mesentery also gives off the transverse and sigmoid mesocolons, which are important due to them containing the blood, nerve, and lymphatic supply for related structures.
The Peritoneum
The peritoneum, the serous membrane that forms the lining of the abdominal cavity, covers most of the intra-abdominal organs.
Key Points
The peritoneum supports the abdominal organs and serves as a conduit for their blood and lymph vessels and nerves.
There are two layers of the peritoneum: the outer layer, called the parietal peritoneum, is attached to the abdominal wall; the inner layer, the visceral peritoneum, is wrapped around the internal organs that are located inside the intraperitoneal cavity.
The mesentery is the double layer of the visceral peritoneum.
The potential space between these two layers, the peritoneal cavity, is filled with a small amount of slippery serous fluid that allows the two layers to slide freely over each other.
The structures in the abdomen are classified as intraperitoneal, retroperitoneal, or intraperitoneal, depending on whether they are covered with visceral peritoneum and are attached by mesenteries.
There are two main regions of the peritoneum connected by the epiploic foramen: the greater sac or general cavity of the abdomen, and the lesser sac or omental bursa.
Intraperitoneal organs and retroperitoneal organs weave in and out of these membranes and serve varying functions. Retroperitoneal structures tend to be more static than intraperitoneal ones.
Key Terms
greater omentum: A large fold of visceral peritoneum that hangs down from the stomach.
retroperitoneal: Located outside of the peritoneum.
serous membrane: A thin membrane that secretes serum that lines an internal body cavity, such as the peritoneum, the pericardium, and the pleura.
peritoneum: In mammals, the serous membrane that lines the cavity of the abdomen and is folded over the viscera.
intraperitoneal: Within the cavity of the peritoneum.
mesentery: The membrane that attaches the intestines to the wall of the abdomen and maintains their position in the abdominal cavity to supply them with blood vessels, nerves, and lymphatics.
EXAMPLES
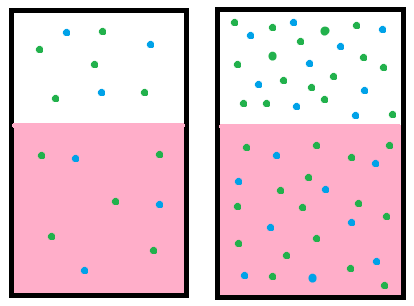
In one form of dialysis, called peritoneal dialysis, a glucose solution is sent through a tube into the peritoneal cavity. The fluid is left there for a prescribed amount of time to absorb waste products and then removed through the tube. This form of dialysis is effective because of the high number of arteries and veins in the peritoneal cavity which, through the mechanism of diffusion, remove waste products from the blood.
The peritoneum is the serous membrane that forms the lining of the abdominal cavity of the coelom. It covers most of the intra-abdominal, or coelomic, organs. It is composed of a layer of mesothelial tissue, supported by a thin layer of connective tissue.
The peritoneum provides support and protection for the abdominal organs and is the main conduit for the associated lymph vessels, nerves, and abdominal arteries and veins.
The abdominal cavity is the open space surrounded by the vertebrae, abdominal muscles, diaphragm, and pelvic floor. Remember not to confuse the abdominal cavity with the intraperitoneal space, which is located within the abdominal cavity and wrapped in peritoneum tissue. For example, a kidney is inside the abdominal cavity but is retroperitoneal—located outside the peritoneum.
The peritoneum and the kidney: A sagittal section through the posterior abdominal wall, showing the kidney residing outside the peritoneum.
Although they ultimately form one continuous sheet, there are two layers of peritoneum and potential space between those layers.
The outer layer, called the parietal peritoneum, is attached to the abdominal wall.
The inner layer, the visceral peritoneum, is wrapped around the internal organs that are located inside the intraperitoneal cavity.
The potential space between these two layers is the peritoneal cavity. It is filled with a small amount of slippery serous fluid that allows the two layers to slide freely over each other.
The term mesentery is often used to refer to a double layer of the visceral peritoneum. There are generally blood vessels, nerves, and other structures between these layers. The space between the two layers is technically outside of the peritoneal sac, and thus not in the peritoneal cavity.
The Regions of the Peritoneum
There are two main regions of the peritoneum, connected by the epiploic foramen (also known as the mental foramen or foramen of Winslow). The first is the greater sac or general cavity of the abdomen. The second is the lesser sac or omental bursa.
The lesser sac is divided into two omenta: the gastrohepatic and the gastrocolic. The gastrohepatic omentum is attached to the lesser curvature of the stomach and the liver. The gastrocolic omentum hangs from the greater curve of the stomach and loops down in front of the intestines before curving upwards to attach to the transverse colon. Like a curtain of tissue, it is draped in front of the intestines to insulate and protect them.
Substructures of the peritoneum: This is a midsagittal, cross-section drawing of the epiploic foramen, the greater sac or general cavity (red), and the lesser sac or omental bursa (blue).
Abdomen Structures
The structures in the abdomen are classified as intraperitoneal, retroperitoneal, or intraperitoneal depending on whether they are covered with visceral peritoneum and are attached by mesenteries, such as the mesentery and mesocolon.
Intraperitoneal Structures
Intraperitoneal organs include the stomach, the first five centimeters, and the fourth part of the duodenum, the jejunum, the ileum, the cecum, the appendix, the transverse colon, the sigmoid colon, and the upper third of the rectum.
Other organs located in the intraperitoneal space are the liver, spleen, and tail of the pancreas. In women, the uterus, fallopian tubes, ovaries, and gonadal blood vessels are located in the intraperitoneal.
Retroperitoneal Structures
Retroperitoneal structures include the rest of the duodenum, the ascending colon, the descending colon, the middle third of the rectum, and the remainder of the pancreas. Other organs located in the retroperitoneal space are the kidneys, adrenal glands, proximal ureters, and renal vessels. Organs located below the peritoneum in the subperitoneal space include the lower third of the rectum and the urinary bladder.
Intraperitoneal Structures
Structures that are intraperitoneal are generally mobile, while those that are retroperitoneal are relatively fixed in their location. Some structures, such as the kidneys, are primarily retroperitoneal, while others such as the majority of the duodenum, are secondarily retroperitoneal, meaning that structure developed intraperitoneally, but lost its mesentery and thus became retroperitoneal.
Peritoneum: The peritoneum is illustrated, indicated by blue.
Blood Supply and Lymphatics
The parietal peritoneum receives blood from the abdominal wall vasculature, including the iliac, lumbar, epigastric, and intercostal arteries. The visceral peritoneum receives supply from the superior and inferior mesenteric arteries. The two portions of the peritoneum also differ in their venous drainage: the parietal peritoneum drains into the inferior vena cava while the visceral peritoneum drains into the portal vein.[rx]
Nerves
A thorough understanding of the innervation of the peritoneum is important as it has clinical implications. The peritoneum has both somatic and autonomic innervations that help explain why various abdominal pathologies, such as peritonitis or appendicitis present the way they do. The parietal peritoneum receives its innervation from spinal nerves T10 through L1. This innervation is somatic and allows for the sensation of pain and temperature that can be localized. The visceral peritoneum receives autonomic innervation from the Vagus nerve and sympathetic innervation that result in the difficulty to localize abdominal sensations triggered by organ distension.[rx][rx]
Gastrointestinal Nervous System Control/The gastrointestinal (GI) tract is the body’s organ system responsible for digestion, absorption, and excretion of matter vital for energy expenditure and compatibility with life. It utilizes a multitude of organs to achieve this including the mouth, esophagus, stomach, small and large intestines, rectum, liver, biliary tract, pancreas, and glands that work together via complex mechanisms. It can do this using three distinct centers of control[rx]:
Myogenic control – The intrinsic rhythm of the GI musculature. This rhythm primarily occurs via slow waves, a natural property of GI smooth muscle, the rate of which gets set via pacemaker activity of the interstitial cells of Cajal (ICC).
Hormonal control – Utilizes various hormones including cholecystokinin, gastrin, and secretin, among multiple others for a myriad of functions.
Neural control – including the GI’s intrinsic enteric nervous system and the autonomic nervous system.[rx]
These processes all work together to achieve four major actions required for a proper functioning GI tract: motility, secretion, digestion, and absorption. This activity will primarily focus on neural control, specifically the physiologic function of the enteric nervous system and autonomic nervous system, and their associated pathology.
Enteric Nervous System
The enteric nervous system (ENS) is a subdivision of the autonomic nervous system (ANS) that directly controls the gastrointestinal system.
Key Points
The enteric nervous system (ENS), which is embedded in the lining of the gastrointestinal system, can operate independently of the brain and the spinal cord.
The ENS consists of two plexuses, the submucosal and the myenteric. The myenteric plexus increases the tone of the gut and the velocity and intensity of contractions. The submucosal plexus is involved with local conditions and controls local secretion, absorption, and muscle movements.
While described as a second brain, the enteric nervous system normally communicates with the central nervous system (CNS) through the parasympathetic (via the vagus nerve ) and sympathetic (via the prevertebral ganglia) nervous systems, but can still function when the vagus nerve is severed.
The ENS includes efferent neurons, afferent neurons, and interneurons, all of which make the ENS capable of carrying reflexes and acting as an integrating center in the absence of CNS input.
The ENS contains support cells, which are similar to the astroglia of the brain, and a diffusion barrier around the capillaries surrounding the ganglia, which is similar to the blood–brain barrier of cerebral blood vessels.
Key Terms
enteric nervous system: A subdivision of the peripheral nervous system that directly controls the gastrointestinal system.
EXAMPLES
The second brain of the enteric nervous system is the reason we get butterflies in our stomach or need to use the restroom more frequently when we are nervous and/or under stress.
The gastrointestinal (GI) system has its own nervous system, the enteric nervous system (ENS). Neurogastroenterology is the study of the enteric nervous system, a subdivision of the autonomic nervous system (ANS) that directly controls the gastrointestinal system. The ENS is capable of autonomous functions such as the coordination of reflexes.
Although it receives considerable innervation from the autonomic nervous system, it can and does operate independently of the brain and the spinal cord. The ENS consists of some 100 million neurons, one-thousandth of the number of neurons in the brain, and about one-tenth the number of neurons in the spinal cord. The enteric nervous system is embedded in the lining of the gastrointestinal system.
Ganglia of the ENS
The neurons of the ENS are collected into two types of ganglia:
The myenteric (Auerbach’s) plexus, located between the inner and outer layers of the muscularis externa
The submucosal (Meissner’s) plexus, located in the submucosa
The Myenteric Plexus
The myenteric plexus is mainly organized as a longitudinal chains of neurons. When stimulated, this plexus increases the tone of the gut as well as the velocity and intensity of its contractions. This plexus is concerned with motility throughout the whole gut. Inhibition of the myenteric system helps to relax the sphincters —the muscular rings that control the flow of digested food or food waste.
The Submucosal Plexus
The submucosal plexus is more involved with local conditions and controls local secretion and absorption, as well as local muscle movements. The mucosa and epithelial tissue associated with the submucosal plexus have sensory nerve endings that feed signals to both layers of the enteric plexus. These tissues also send information back to the sympathetic pre-vertebral ganglia, the spinal cord, and the brain stem.
Neural control of the gut: An illustration of neural control of the gut wall by the autonomic nervous system and the enteric nervous system.
Function and Structure of the ENS
The enteric nervous system has been described as a second brain. There are several reasons for this. For instance, the enteric nervous system can operate autonomously. It normally communicates with the central nervous system (CNS) through the parasympathetic (e.g., via the vagus nerve) and sympathetic (e.g., via the prevertebral ganglia) nervous systems. However, vertebrate studies show that when the vagus nerve is severed, the enteric nervous system continues to function.
Invertebrates, the enteric nervous system includes efferent neurons, afferent neurons, and interneurons, all of which make the enteric nervous system capable of carrying reflexes and acting as an integrating center in the absence of CNS input. For instance, the sensory neurons report mechanical and chemical conditions, while the motor neurons control peristalsis and the churning of intestinal contents through the intestinal muscles. Other neurons control the secretion of enzymes.
The enteric nervous system also makes use of more than 30 neurotransmitters, most of which are identical to the ones found in the CNS, such as acetylcholine, dopamine, and serotonin. More than 90% of the body’s serotonin is in the gut, as well as about 50% of the body’s dopamine, which is currently being studied to further our understanding of its utility in the brain.
The enteric nervous system has the capacity to alter its response depending on factors such as bulk and nutrient composition. In addition, the ENS contains support cells that are similar to the astroglia of the brain, as well as a diffusion barrier around the capillaries that surround the ganglia, which is similar to the blood-brain barrier of the cerebral blood vessels.
Regulation of ENS Function
The parasympathetic nervous system is able to stimulate the enteric nerves in order to increase enteric function. The parasympathetic enteric neurons function in defecation and provide a rich nerve supply to the sigmoid colon, the rectum, and the anus.
Conversely, stimulation of the enteric nerves by the sympathetic nervous system will inhibit enteric function and capabilities. Neurotransmitter secretion and direct inhibition of the enteric plexuses cause this stall in function. If the gut tract is irritated or distended, afferent nerves will send signals to the medulla of the brain for further processing.
Mechanism
As mentioned previously, mediation of the innervation of the GI system is via the enteric nervous system and the autonomic nervous system. Enteric nervous system- is the intrinsic nervous system of the GI tract, containing a mesh-like system of neurons. This system coordinates digestion, secretion, and motility to achieve adequate nutrient absorption. It does this through information stimulating the CNS such as sight and smell, and by local mechanical and chemical receptors found within the GI tract. Included in the enteric nervous system is the ICC. These cells positioned between the two muscular layers create the intrinsic pacemaker activity and are primarily responsible for slow-wave propagation found throughout the GI tract. Included in the enteric nervous system is the myenteric plexus, which exhibits control over the longitudinal and circular muscle layers. Additionally, it is estimated that 30% of the neurons in this plexus are sensory neurons.
The second aspect included in the neural control of the GI tract is the autonomic system. This system is comprised of the sympathetic and parasympathetic systems. In the case of the GI tract, the parasympathetic tract is typically excitatory. The parasympathetic system exerts its effects primarily via the vagus (innervates the esophagus, stomach, pancreas, upper large intestine) and pelvic nerves (innervates the lower large intestine, rectum, and anus.) The vagus nerve regulates tone and volume by activating the enteric motor neurons. They do this by synapsing on the myenteric motor neurons and either exhibiting inhibitory action via nitric oxide, or excitatory action via acetylcholine and neurokinins. The enteric motor neurons, including the myenteric plexus, then synapse on the ICC’s found within muscle bundles. These cells then communicate via gap junctions to the smooth muscles cells.
Sympathetic activity in the GI tract is fundamentally inhibitory. These fibers originate from spinal cord levels T-8 through L-2. These fibers then synapse on the pre-vertebral ganglia and continue onward to finally synapse on the myenteric and submucosal plexuses, which respond to manipulate smooth muscle cells, secretory cells, and endocrine cells.
Before a food bolus can reach the esophagus, it must be swallowed. It is that action of swallowing that then begins the sequence of peristalsis in the esophagus. Initially, swallowing induces a stimulus that begins the sequence of peristalsis within the esophagus. This stimulus activates the lower motor neurons in the nucleus ambiguous in the brainstem. When the peripheral end of these neurons is stimulated via the vagus nerve, different segments of the esophagus contract. Initially, the caudal end of the dorsal nucleus of the vagus (DMN) is activated via an inhibitory pathway. This inhibition is exerted on all the parts of the esophagus. However, the inhibition lingers for a longer time in the distal areas of the esophagus. Once the inhibition ceases, there is excitatory input leading to sequential activation of the neurons in the rostral zone of the DMN leading a contraction wave that is considered peristaltic. This action allows the area proximal to the food bolus to contract while the area distal remains relaxed, propelling the food down the esophagus. The nerves that allow for this peristaltic motion within the esophagus consist of the myenteric plexus and its association with the circular and longitudinal muscular layers. To continue from the esophagus to the stomach, the food bolus must propel through the lower esophageal sphincter. While this sphincter is typically contracted via the effects of acetylcholine on its intrinsic muscle activity, the neurological sequelae of swallowing inhibit this normally remains contracted sphincter, allowing it to relax before the peristaltic wave reaches down the esophagus.[rx]
The stomach has two main centers of control consisting of nervous control and hormonal control, including hormones such as gastrin and cholecystokinin, which relax the proximal stomach, and contracts the distal stomach. The pacemaker cells in the fundus of the stomach establish a basal electrical rhythm continuously that spread down to the pyloric sphincter, creating a rate of approximately three to eight contractions per minute. Relaxation of the stomach is pivotal for its acceptance of the incoming food bolus and is mediated predominately by inhibitory vagal fibers. These fibers are stimulated first by the action of swallowing, and second by stretch receptors that are activated when the bolus reaches the stomach. The stomach then acts as a sieve, mixing food particles with gastric fluids, and breaking those particles down into smaller parts. This occurs through three main mechanisms: First is the non-adrenergic, non-cholinergic (NANC) control. This mechanism utilizes substances such as nitric oxide, vasoactive intestinal peptides, and others. The second is sympathetic fiber activation utilizing norepinephrine. The third, is excitatory vagal stimulation. These three processes serve to give the stomach a unique mixing motion, dubbed segmentation. In this process, mechanoreceptors in the gastric wall activate, leading to a unique parasympathetic sequence. Once the bolus reaches the pylorus, long vago-vagal activity, as well as short reflexes through the enteric nervous system, activate the pyloric pump and contract the pyloric sphincter leading to both the mixing of particles and inhibition of the forward movement of the bolus through the pylorus respectively. The antral pump stimulated by mechanoreceptors as well as the enteric system then propels food back to the fundus, which creates a circuit. Throughout this process, the smallest particles, as well as some fluids are released into the duodenum, until finally, most of the bolus has made its way out of the stomach[rx].
The small intestine utilizes two different mechanisms regarding motility. First is the pacemaker activity which propagates slow waves. The second is the migrating motility complex (MMC). This process is dependent on the enteric nervous system and has three phases. The first is the quiet phase in which there is minimal propulsion, which lasts approximately 70 minutes. The second phase includes intermittent motor activity, in which there are one to five contractions with each slow wave. This entire phase lasts between 10 and 20 minutes. Last, there is the regular, propagating contractile activity phase in which there are regular contractions, and the bulk of the food gets moved through the small intestine in a peristaltic pattern, which lasts a total of five minutes. This peristaltic pattern is under the mediated of the “law of the intestine” in which distension of one area is sensed by mechanoreceptors, leading to contraction above the area of distension, and relaxation below the area. This phase is mediated predominately by the autonomic and enteric nervous systems, and repeat every 90 to 120 minutes[rx].
The large intestine is mainly involved in the storage and propulsion of feces, and take approximately 8-15 hours to accomplish this task. They accomplish this task in three ways: The first is the mixing movement, in which there is no net movement of its contents. The second mode of motility is through Haustral migration in which there are slow waves as well as long bursts of spike activity. Haustrations form from the concomitant constricted and relaxed portions of the intestines. The large intestines accomplish Haustral migration in a similar pattern as the stomach and proximal small intestine, through the process of segmentation, with the distinction of stronger contractions due to the ring-like contractions of the circular muscle as it encircles the large intestine in its entirety. The purpose of this movement type is to mix chyme and fecal material while providing slow forward movement. Lastly is the “mass movement,” which consists of frequent, powerful propulsions. Mediation of this process is via the enteric nervous system of the transverse and descending colon. This mechanism is similar to the peristaltic contractions seen previously.[rx]
Rectum and Anus: As stool reaches the distal large intestine, rectum, and anal sphincter, the myenteric plexus is stimulated to initiate peristalsis as well as relax the internal anal sphincter. This reflex, called the rectosphincteric reflex, also stimulates the external anal sphincter to contract, leading to the urge to defecate. At the same time, there is parasympathetic activation leading to relaxation of the internal anal sphincter to allow the passage of stool. The external sphincter, as well as the puborectalis muscle, is then voluntarily controlled to either avoid the leakage of contents via voluntary constriction or to allow defecation, via voluntary relaxation. The striated muscle of the puborectalis muscle, as well as the external anal sphincter, are both innervated by somatic fibers of the pudendal nerves.[rx] While hormonal control exerts significant influence on salivary and gastric secretions, there are numerous effects of nervous control as well.
The salivary glands are mainly under sympathetic control, specifically with cranial nerves VII and IX. These stimulate the secretion of serous, low viscous saliva. This saliva secreted relative to parasympathetic activation is copious in amount and contains large amounts of potassium and bicarbonate, and scant amounts of protein. These glands are under sympathetic control as well but to a lesser extent. Sympathetic fibers extend through the superior cervical ganglion and stimulate the secretion of highly viscous, thick saliva. The saliva produced is minimal in amount, is rich in protein, and low in potassium and bicarbonate.[rx]
Gastric secretions are various and originate from parietal cells, chief cells, as well as mucous neck cells. Parietal cells secrete primarily hydrochloric acid (HCl), and intrinsic factors. There are three mechanisms for the release of parietal cell contents, one of which is of neural influence. The first phase of gastric secretion is the cephalic phase. In this phase, a person sees, smells, or thinks about food, activating an area in the medulla oblongata. This then activates the Vagus nerve which secretes acetylcholine, which synapses at the muscarinic receptor allowing for the release of gastric contents. The gastric phase then begins as a bolus enters the stomach. Distension of the stomach activates stretch receptors in the wall of the stomach as well as chemoreceptors in the mucosa of the stomach, stimulating short reflexes which then stimulate the submucosal and myenteric plexuses, leading to parasympathetic activation and gastric secretion.[rx]
Intestinal secretions are similar to that gastric secretions. Intestinal distension activates mechanoreceptors, and intestinal contents activate chemoreceptors both leading to parasympathetic activation and intestinal secretions.
Gastrointestinal Reflex Pathways
The digestive system functions via a system of long reflexes, short reflexes, and extrinsic reflexes from gastrointestinal (GI) peptides that work together.
Key Points
Long reflexes to the digestive system involve a sensory neuron that sends external or internal digestive information to the brain. This type of reflex includes reactions to food, emotion, or danger.
Short reflexes to the digestive system provide shortcuts for the enteric nervous system (ENS) to act quickly and effectively and form a sort of digestive brain. It reacts to digestive movement and chemical changes.
The intragastric reflex is stimulated by the senses. This reflex releases acid in the duodenum or in the stomach and suppresses the release of digestive proteins.
The gastrocolic reflex increases movement in the gastrointestinal tract and reacts to stretches in the stomach walls as well as in the colon. It is responsible for the urge to defecate, the movement of digested material in the small intestine, and it makes room for more food within the stomach.
The gastroileal reflex works with the gastrocolic reflex to stimulate the urge to defecate. It does so by opening the ileocecal valve and moving the digested contents from the ileum of the small intestine into the colon for compaction.
GI peptides act on a variety of tissues including the brain, the digestive accessory organs, and the GI tract.
Key Terms
gastrocolic reflex: One of the three extrinsic physiological reflexes that control the motility or peristalsis of the gastrointestinal tract; it involves an increase in the motility of the colon, creates the urge to defecate along with the gastroileal reflex, and helps make room for food in the stomach.
intragastric reflex: One of the three extrinsic reflexes of the gastrointestinal tract that is stimulated by the presence of acid levels in the duodenum or in the stomach. It releases acids and controls the release of stomach proteins such as gastrin.
gastroileal reflex: One of the three extrinsic reflexes of the gastrointestinal tract that works with the gastrocolic reflex to stimulate the urge to defecate. This reflex is stimulated by the opening of the ileocecal valve and moves the digested contents from the ileum of the small intestine into the colon for compaction.
EXAMPLES
The gastrocolic reflex can cause irritable bowel syndrome. This can lead to abdominal pain, diarrhea, or constipation.
Food in the Digestive System
The digestive system has a complex system of food movement and secretion regulation, which are vital for its proper function. Movement and secretion are regulated by long reflexes from the central nervous system (CNS), short reflexes from the enteric nervous system (ENS), and reflexes from the gastrointestinal system (GI) peptides that work in harmony with each other.
In addition, there are three overarching reflexes that control the movement, digestion, and defecation of food and food waste:
The enterogastric reflex
The gastrocolic reflex
The gastroileal reflex
Long and Short Reflexes
Long reflexes to the digestive system involve a sensory neuron that sends information to the brain. This sensory information can come from within the digestive system, or from outside the body in the form of emotional response, danger, or a reaction to food.
These alternative sensory responses from outside the digestive system are also known as feedforward reflexes. Emotional responses can also trigger GI responses, such as the butterflies in the stomach feeling when nervous.
Control of the digestive system is also maintained by the enteric nervous system (ENS), which can be thought of as a digestive brain that helps to regulate motility, secretion, and growth. The enteric nervous system can act as a fast, internal response to digestive stimuli. When this occurs, it is called a short reflex.
Three Main Types of Gastrointestinal Reflex
The Enterogastric Reflex
The intragastric reflex is stimulated by the presence of acid levels in the duodenum at a pH of 3–4 or in the stomach at a pH of 1.5. When this reflex is stimulated, the release of gastrin from G- cells in the antrum of the stomach is shut off. In turn, this inhibits gastric motility and the secretion of gastric acid (HCl). Enterogastric reflex activation causes decreased motility.
The Gastrocolic Reflex
Peristalsis: The gastrocolic reflex is one of a number of physiological reflexes that control the motility, or peristalsis, of the gastrointestinal tract.
The gastrocolic reflex is the physiological reflex that controls the motility, or peristalsis, of the gastrointestinal tract. It involves an increase in motility of the colon in response to stretch in the stomach and the byproducts of digestion in the small intestine. Thus, this reflex is responsible for the urge to defecate following a meal. The small intestine also shows a similar motility response. The gastrocolic reflex also helps make room for food in the stomach.
The Gastroileal Reflex
The gastroileal reflex is a third type of gastrointestinal reflex. It works with the gastrocolic reflex to stimulate the urge to defecate. This urge is stimulated by the opening of the ileocecal valve and the movement of the digested contents from the ileum of the small intestine into the colon for compaction.
GI Peptides that Contribute to Gastrointestinal Signals
GI peptides are signal molecules that are released into the blood by the GI cells themselves. They act on a variety of issues that include the brain, the digestive accessory organs, and the GI tract.
The effects range from excitatory or inhibitory effects on motility and secretion to feelings of satiety or hunger when acting on the brain. These hormones fall into three major categories:
The gastrin family
The secretin family
A third family that is composed of the hormones that do not fit into either of these two families
Cellular
The GI tract is organized in distinct cellular layers, each containing unique properties integral to the physiological activity of the system as a whole. The layers include:
Mucosa: Facing the lumen, the mucosa contains an epithelial cell layer, a lamina propria, and muscularis mucosae. These three components primarily provide protection from luminal matter and offer the first barrier of support.
Submucosa: Found beneath the mucosa, this layer contains the submucosal, or Meissner plexus. Submucosal ganglia and connecting fiber bundles form plexuses in the small and large intestines, but not the stomach and esophagus. This arrangement of nerves receives data from mechanoreceptors and chemoreceptors and manipulates secretion as well as blood flow.[rx]
Muscularis Externa: found beneath the submucosa, it includes the Myenteric plexus (Auerbach plexus) wedged between the proximal circular layer and the outer longitudinal muscular layer. The myenteric plexus forms a continuous network that extends from the upper esophagus to the internal anal sphincter, and primarily influences motor control through its effects on smooth muscle, thereby regulating GI motility. It accomplishes this by increasing intestinal length and decreasing intestinal radius. These nerves communicate with one another, primarily via gap junctions and are innervated by excitatory and inhibitory motor neurons[rx]. Smooth muscle cells in this layer run from the distal esophagus to the internal anal sphincter and coordinate contractions to produce the motor patterns of GI motility.[rx] The longitudinal muscle cells are innervated and undergo activation by excitatory motor neurons, and act to contract and shorten the intestinal length while increasing the intestinal radius.
Serosa: Facing the blood, this layer is formed by an epithelial layer and connective tissue, and primarily offers support, providing a barrier between blood and the GI tract.
Lastly, one specialized group of cells instrumental to GI function include Intramuscular interstitial cells of Cajal (ICC). These cells are interposed between nerve terminals and smooth muscle cells, coupling with the smooth muscle cells to produce the pacemaker activity of the GI tract.
Function
The GI tract consists mainly of the esophagus, stomach, small intestine, and large intestine, with each containing all of, or a combination of four functions mentioned previously.
After swallowing, a food bolus must travel from the pharynx to the stomach. The esophagus acts as a conduit between these two points and has a unique system of propelling food from its proximal to its distal end and through the lower esophageal sphincter.
Separated from the esophagus proximally by the LES, and the duodenum distally by the pyloric sphincter, the stomach uses a complex system of neural and hormonal signals to accomplish three main tasks: Acting as a reservoir, breaking food down into smaller particles and mixing them with gastric juices, and emptying gastric content at a controlled rate.
The principal function of the small intestine is the absorption of food. The small intestines display an unsynchronized pattern of contractions ideal for the movement of food back and forth to allow both the mixing with digestive enzymes as well as to allow time for absorption. However, there is an overall albeit slow push forward which takes approximately 90 to 120 minutes to allow the first part of a meal to reach the large intestines, whereas the final portions of a meal may not arrive for five hours.
The function of the large intestine is primarily to store fecal material, extract water and ions while secreting mucus, and move fecal material toward the rectum. In this process, there are no digestive enzymes secreted by the colon, and absorption of nutrients does not occur.
The primary purpose of the rectum and anus are to propagate feces forward and to allow for the act of defecation.
Salivary, gastric, intestinal, biliary, and pancreatic secretions are paramount for the digestion of food. These processes not only break food down, but they react with them chemically, altering the structures to allow for either excretion or absorption, the latter of which the body can then utilize for energy expenditure among a myriad of functions.
The small intestine is a crucial component of the digestive system that allows for the breakdown and absorption of important nutrients that permit the body to function at its peak performance. The small intestine accomplishes this via a complex network of blood vessels, nerves, and muscles that work together to achieve this task. It is a massive organ that has an average length of 3 to 5 meters. It divides into the duodenum, jejunum, and ileum.[rx][rx][rx]
The duodenum is the shortest section, on average measuring from 20 cm to 25 cm in length. Its proximal end is connected to the antrum of the stomach, separated by the pylorus, and the distal end blends into the beginning of the jejunum. The duodenum surrounds the pancreas, in the shape of a “C” and receives chyme from the stomach, pancreatic enzymes, and bile from the liver; this is the only part of the small intestines where Brunner’s glands are present on histology.
The jejunum is roughly 2.5 meters in length, contains plicae circulares (muscular flaps), and villi to absorb the products of digestion.
The ileum is the final portion of the small intestine, measuring around 3 meters, and ends at the cecum. It absorbs any final nutrients, with major absorptive products being vitamin B12 and bile acids.
Layers of the Small Intestine
Serosa: The serosa is the outside layer of the small intestine and consists of mesothelium and epithelium, which encircles the jejunum and ileum, and the anterior surface of the duodenum since the posterior side is retroperitoneal. The epithelial cells in the small intestine have a rapid renewal rate, with cells lasting for only 3 to 5 days.
Muscularis: The muscularis consists of two smooth muscle layers, a thin outer longitudinal layer that shortens and elongates the gut, and a thicker inner circular layer of smooth muscle, which causes constriction. Nerves lie between these two layers and allow these to muscle layers to work together to propagate food in a proximal to distal direction.
Submucosa: The submucosa consists of a layer of connective tissue that contains the blood vessels, nerves, and lymphatics.
Mucosa: The mucosa is the innermost layer and is designed for maximal absorption by being covered with villi protruding into the lumen that increases the surface area. The crypt layer of the small bowel that is the area of continual cell renewal and proliferation. Cells move from the crypts to the villi and change into either enterocytes, goblet cells, Paneth cells, or enteroendocrine cells.
Of importance is the mesentery, which is a double fold of the peritoneum that not only anchors the small intestines to the back of the abdominal wall, but also contains the blood vessels, nerves, and lymphatic vessels that supply the small intestine.[rx][rx]
Structure and Function
The principal function of the small intestine is to break down food, absorb nutrients needed for the body, and get rid of unnecessary components. It also plays a role in the immune system, acting as a barrier to a multitude of flora that inhabits the gut and making sure no harmful bacteria enter the body.
The duodenum is the initial portion of the small intestine and is where absorption actually begins. It is often described as being split into four parts: superior, descending, horizontal, and ascending. The superior portion is the only section that is peritoneal; the rest is retroperitoneal. Pancreatic enzymes enter the descending duodenum via the hepatopancreatic ampulla and break down chyme, a mix of stomach acid and food, from the stomach. Bicarbonate is also secreted into the duodenum to neutralize stomach acid before reaching the jejunum. Lastly, the liver introduces bile into the duodenum, which allows for the breakdown and absorption of lipids from food products. A significant landmark for the duodenum is the ligament of Trietz, a ligament made of skeletal muscle that tethers the duodenal-jejunal flexure to the posterior wall.
The primary function of the jejunum is to absorb sugars, amino acids, and fatty acids. Both the jejunum and ileum are peritoneal.
The ileum absorbs any remaining nutrients that did not get absorbed by the duodenum or jejunum, in particular vitamin B12, as well as bile acids that will go on to be recycled.
Blood Supply and Lymphatics
The arterial blood supply for the small intestine first comes from the celiac trunk and the superior mesenteric artery (SMA).
The superior pancreaticoduodenal artery is fed from the gastroduodenal artery, which branches from the proper hepatic artery, which is traceable back to the celiac trunk. It anastomoses with the inferior pancreaticoduodenal artery, which comes from the SMA, to supply blood to the duodenum.
The jejunum and ileum receive their blood supply from a rich network of arteries that travel through the mesentery and originate from the SMA. The multitude of arterial branches that split from the SMA is known as the arterial arcades, and they give rise to the vasa recta that deliver the blood to the jejunum and ileum.
The venous blood mimics that of the arterial supply, which coalesces into the superior mesenteric vein (SMV), which then joins with the splenic vein to form the portal vein.
Lymphatic drainage starts at the mucosa of the small intestine, into nodes next to the small intestine in the mesentery, to nodes near the arterial arcades, then to nodes near the SMA/SMV. Lymph then flows into the cisterna chyli and then up the thoracic ducts, and then empties into the venous system left internal jugular, and subclavian veins meet. The lymphatic drainage of the small intestine is a major transport system for absorbed lipids, the immune defense system, and the spread of cancer cells coming from the small intestine, explaining Virchow’s node enlargement from small intestine cancers.
Nerves
The nervous system of the small intestine is made up of the parasympathetic and sympathetic divisions of the autonomic nervous system. The parasympathetic fibers originate from the Vagus nerve and control secretions and motility. The sympathetic fibers come from three sets of splanchnic nerve ganglion cells located around the SMA. Motor impulses from these nerves control blood vessels, along with gut secretions and motility. Painful stimuli from the small intestine travel through the sympathetic fibers as well.
Muscles
Two layers of smooth muscle form the small intestine. The outermost layer is the thin, longitudinal muscle that contracts, relaxes, shortens, and lengthens the gut allowing food to move in one direction. The innermost layer is a thicker, circular muscle. This layer enables the gut to contract and break apart larger food particles. It also stops food from moving in the wrong direction by blocking the more proximal end. The two muscle layers work together to propagate food from the proximal end to the distal end.
Clinical Significance
With shortening or destruction of the small intestine, there can be a decrease in the absorption of essential vitamins, minerals, and other nutrients for the body that can cause a myriad of problems that can interfere with other systems of the body.[rx][rx][rx]
Duodenal ulcers can be a serious health risk. They most commonly occur on the posterior wall of the superior portion of the duodenum. Complete ulceration of an ulcer through the wall of the duodenum can result in peritonitis and damage to the surrounding organs. The most common risk factor in developing these ulcers is infection with Helicobacter pylori.
Wilke’s syndrome, also known as SMA syndrome, occurs due to compression of the duodenum between the superior mesenteric artery and the abdominal aorta. This condition creates an obstruction and often leads to nausea, vomiting, and abdominal pain. It most commonly presents in individuals who lack intra-abdominal fat, such as those suffering from anorexia nervosa or cancer.
The ileocecal valve is an important landmark for Meckel disease, an ileal diverticulum that, when present, is often located close to the valve. A common mnemonic device to remember the details of this pathology is by using the “Rules of 2’s” (Two years old, 2 feet from the ileocecal valve, 2% of the population). It classically presents in a young male patient with hematochezia and periumbilical pain. However, it can often be asymptomatic.
Crohn disease is a chronic inflammatory disease that most often affects the ileum but can be found throughout the GI tract (except for the rectum, which is generally spared).
The stomach is a hollow organ that is part of the gastrointestinal system, and it is responsible for functions including the formation of chyme, synthesis of proteins necessary for vitamin absorption, microbial defenses, and propagates the peristaltic reflex. Contrary to popular thought, the stomach does not contribute to the absorption of any nutrients. This organ can is in the peritoneal cavity, located in the left upper abdominal quadrant, or in the epigastric abdominal region that acts to relay ingested food between the nervous system and the endocrine system. Gastric acid secretion, peristaltic propulsion, and other physiologic functions of the stomach are finely controlled by the integration of the enteric nervous system, parasympathetic nervous system, and the secretion of various neurohormonal molecules (i.e., gastrin, HCl acid, intrinsic factor, bicarbonate, mucus, etc.)[rx][rx][rx]
The stomach is a muscular organ located on the left side of the upper abdomen. The stomach receives food from the esophagus. As food reaches the end of the esophagus, it enters the stomach through a muscular valve called the lower esophageal sphincter. The stomach secretes acids and enzymes that digest food.
As a component of the alimentary canal (i.e., the tubal passageway for ingested food to be digested, absorbed, then excreted as waste), the stomach’s physiological function is structured around creating an environment where the food ingested can be safely acted on by proteolytic enzymes and acidic solutions. There are pathologic consequences that can develop with the failure of the gastric mucosa to isolate the lumenal contents from the surrounding peritoneal cavity.
Cellular
As with most physiologic processes, the structure of an organ largely defines the function it contributes to the body. The gastric wall is specifically designed to aid in the formation of a transient acidic environment that allows for the digestion of food into a semisolid mixture called chyme. The stomach organ has four regions; fundus, cardia, body, and pylorus. The inner surface of the stomach is corrugated to increase the surface area of the gastric mucosa allowing for gastric expansion with food ingestion. The wall of the stomach consists of four different tissue layers; mucosal layer, submucosa, muscularis externa, and adventitia/serosa. The gastric mucosal layer further subdivides into three layers; the surface epithelium, a connective tissue layer called the lamina propria and the muscular mucosa. The gastric epithelial layer invaginates into the lamina propria forming the gastric pits and glands. These gastric glands are lined with four specialized cells; surface mucous cells (foveolar cells), parietal cells, chief cells, and neuroendocrine cells (G-cells or ECL-like cells) that all contribute independent functions.[rx][rx]
The surface mucus cells (foveolar cells) are mucus-producing cells that primarily line the gastric mucosa. The secreted mucus acts as a barrier to the corrosive nature of the gastric acid. The rest of the specialized cells are found deep within the gastric glands (i.e., gastric pits).
Parietal cells – are specialized secretory epithelial cells that secrete gastric acid (HCl formation) into the lumen of the stomach through the gastric pits, primarily in the fundus. In addition to secreting HCl, the parietal cells secrete a protein called intrinsic factor. Intrinsic factor is necessary for the absorption of vitamin B12 in the terminal ileum of the small intestines. Three regulating molecules control these cells: acetylcholine (enteric nervous innervation) via muscarinic receptors, histamines (neuroendocrine cells) to histamine receptors, and gastrin (neuroendocrine cells) to gastrin receptors. All receptors appear on the basal side of the parietal cells, and they control a protein channel called H+/K+ ATPase on the lumenal side of the parietal cell. This protein transports one proton into the gastric lumen while intaking one K+ ion. Chloride ions follow the proton gradient via K+/Cl- channel into the gastric lumen leading to the formation of HCl.[rx]
Chief cells – are specialized secretory cells found at the base of the gastric glands within the fundus of the stomach that secrete the zymogen called pepsinogen. Pepsinogen is the inactive form of a proteolytic enzyme called pepsin, which is needed to digest proteins into small units called polypeptides. The zymogen pepsinogen only becomes activated by the gastric acid produced by the parietal cells. This mechanism acts as a safety measure to ensure the proteins found outside of the gastric lumen are not digested inappropriately. Chief cells are stimulated by cholinergic activity from the parasympathetic and by the hormone Gastrin.[rx]
Neuroendocrine cells – (i.e., enterochromaffin-like cells, or G-cells) are also found in the gastric glands on the gastric mucosa that secretes various molecules that aid in the production of gastric acid.
The ECL-like cells produce and secrete Histamine when stimulated by a hormone called gastrin, which indirectly increases the HCl production by way of histamines’ direct actions on the parietal cells. ECL-like cells are primarily located in the fundus of the stomach.
G-cells are located in the pylorus region of the stomach, and they produce the neuroendocrine hormone called gastrin. Gastrin is capable of indirectly and directly increasing HCl production by two mechanisms. The first is by stimulation of the ECL-like cells to release Histamine, which then potentiates Parietal cells. The second is by direct stimulation of the Parietal cells themselves. Both mechanisms increase the H+/K+ ATPase activity.
D-cells are located in the pylorus of the stomach, and they secrete an inhibitory molecule called Somatostatin. D cells are activated when the stomach lumen reaches a certain level of acidity. Somatostatin then acts to suppress the release of gastrin, reducing the overall production of gastric acid.[rx]
Compared to other organs of the GI tract, the stomach is unique in that its muscular externa features an inner oblique layer in addition to a circular and longitudinal layer. Exterior to the submucosa is the submucosal Meissner’s plexus, which controls secretions and blood flow. In between the circular and longitudinal layers of the muscular externa is the myenteric Auerbach’s plexus, which controls GI motility.
The right and left gastric arteries left and right gastro-omental arteries and short gastric arteries are responsible for blood supply to the stomach. Celiac ganglia and the vagus nerve innervate the stomach. The vagus nerve serves as an essential link between the brain and the gut respective to appetite control, acid secretion, and gastric motility.
Function
In addition to the stomach’s secretory function, the stomach also has a muscular component, as do all structures within the alimentary canal. The muscularis externa is composed of smooth muscle cells that orient in three directions: an oblique layer (unique to only the stomach), a circular muscle layer, and the longitudinal layer. Together these three muscle layers are responsible for the gastric movements needed to break the food bolus into smaller components. A food bolus, which consists of partially digested food from the mouth and the esophagus, is processed by the stomach into chyme, which is a more readily absorbable substance by the small intestine. The stomach accomplishes this food processing through forceful back-and-forth churning motions by the inner oblique layer of the muscular externa. The circular and longitudinal layers facilitate gastric emptying of chyme through the pyloric sphincter, which allows only liquids and small enough food particles to pass through. Gastric emptying may be slowed by the presence of fats and acids in the duodenum, stress, exercise, and various hormones. Chyme that is not emptied will continue to churn in the stomach until it, too, can pass through the pyloric sphincter. Slow-wave contractions of the gastric smooth muscles are generated by myenteric interstitial cells of Cajal, which serve as GI pacemakers.[rx]
There are three movements associated with gastric motility.
Peristaltic wave:
Contraction of the longitudinal layer rhythmically – Peristalsis can only occur in a forward motion with receptive relaxation of the distal intestinal region.[rx][rx]
Segmentation (i.e., mixing component):
Rhythmic contraction of the circular muscle layer
The myenteric plexus control sets the segmentation motor pattern as the pacemaker. Rhythmic transient depolarizations within this nervous system create a “waxing and waning” pattern of electrical amplitudes contributing to the formation of a “churning” motion. This motion is capable of slowing the speed of chyme progression through the system, thus allowing for optimal nutrient absorption.[rx]
Ancillary movements:
Stomach Relaxation: As a food bolus is transferred from the esophagus into the stomach lumen via the relaxation of the lower esophageal sphincter (LES), relaxation of the stomach is needed to allow for the accumulation of ingested food. The stomach acts as a temporary container so that the digestion of its contents can take place in a uniform and controlled manner. The relaxation occurs through the parasympathetic activation of the vagus nerve, which inhibits the contraction of the gastric muscle layer.
All mechanical movements are the result of coordinated muscle contractions. The muscle layer is regulated primarily by the enteric nervous system (ENS), which is the intrinsic nervous system of the alimentary canal. The ENS can become activated by various inputs from the CNS like olfaction, sight, mechanical reception of the food bolus, or chemical mediators (PSNS/SNS). The mesh-work of neurons that makes up the ENS is found between the longitudinal and circular muscle layers. Commonly, it is referred to as the Auerbach’s plexus or myenteric plexus. The degree and rate of peristalsis are established by the myenteric interstitial cells of Cajal (ICC), as previously mentioned.[rx]
The stomach itself does not significantly contribute directly to the body’s absorption of nutrients, although it absorbs some substances such as alcohol and aspirin.[rx] Parietal cells secrete intrinsic factor, which is essential in the absorption of vitamin B12 distally in the digestive tract by enterocytes of the terminal ileum.
Brief Cellular Review
(refer to the “cellular” section for more information)
Hydrochloric acid (HCl), the main constituent of gastric acid, is secreted by parietal cells. The hydrogen (H) and chloride (Cl) components of HCl are secreted separately by hydrogen/potassium ATPase pumps and chloride channels in the stomach. Pepsinogen, a proenzyme for pepsin, is secreted by chief cells. Collectively, gastric acid creates an acidic environment that denatures proteins and activates the conversion of pepsinogen to pepsin.[rx] Pepsin breaks down proteins into smaller peptides, which may be further processed and later absorbed in the small intestine. The secretion of acid is under the regulation of both hormonal and neural components, including gastrin, histamine, prostaglandins, somatostatin, gastric inhibitory polypeptide, secretin, and the vagus nerve.[rx] Interventional inhibition of acid secretion to avoid various complications of excess acid is commonly done by administering proton pump inhibitors.
The acidic environment of the stomach is not only useful for protein denaturing but also for protection against potentially infectious agents. All material consumed by the body must pass through the stomach, making it an important defense against microbes. Many bacteria are killed or inhibited by the stomach’s acidity.
Additionally, secretory cells of the gastric glands include foveolar cells and enteroendocrine cells. Foveolar cells protect the stomach from the corrosive nature of its acidic environment by producing mucus and bicarbonate (HCO3). Enteroendocrine cells secrete various digestive hormones such as gastrin, somatostatin, and ghrelin. Gastrin release occurs in response to increased gastric distension, increased gastric pH, and the presence of amino acids in the stomach.[rx]
Blood Supply and Lymphatics
Arterial Blood Supply
The celiac trunk, which is the first major branch of the aorta after the aorta traverses the diaphragm. The celiac trunk immediately divides into three predominant arteries: the common hepatic artery, the splenic artery, and the left gastric artery.
The left gastric artery runs the lesser curvature of the stomach and eventually anastomoses with the common hepatic artery. The greater curvature of the stomach receives vascular supply from the anastomoses of the left and right gastroepiploic arteries. The left originates as a branch of the splenic artery, and the right originates from the common hepatic artery.[rx]
Venous Drainage
The stomach predominately drains via the portal system to the liver before entering the inferior vena cava. The anastomoses drain the lesser curvature of the left and right gastric vein to the portal vein. The greater curvature is drained by the anastomoses between the left and right veins to the superior mesenteric vein, which eventually drains into the portal vein as well.
Lymphatic Drainage
The lymphatic vessels travel with the vasculature of the stomach along the lesser and greater curvatures of the stomach. Lymph fluid drains sequentially through several lymph node systems depending on the stomach region. Half of the fundus drains to the pancreaticolienal group, while the remaining half and the cardia drain to the Superior gastric group of lymph nodes. The body of the stomach drains to the inferior gastric subpyloric group of nodes, while the pyloric region drains to the suprapyloric group of nodes. All groups drain eventually into the celiac lymph node. Once the lymph is at the celiac node, the lymph drains through the cisterna chyli to the Thoracic duct where it returns to the heart.
Pathophysiology
The stomach is susceptible to several primary pathologies that all manifest with similar symptomatology of epigastric pain, burning, gnawing discomfort, nausea/vomiting (+/- blood), satiety, and distention. Pathologies can subdivide into the following categories:
Anatomical Pathologies
Hypertrophic Pyloric Stenosis – HPS is a condition that results from hyperplasia of the muscular layers in the mucosal wall of the pylorus in the stomach. The thickening of the pylorus leads to structural obstruction of the gastric outlet clinically presented with projectile nonbilious, non-bloody vomitus in an infant. Commonly, this condition develops in caucasian, first-born males around four weeks of age.
Hypochloremic hypokalemic metabolic alkalosis develops from hydrochloric acid loss and the body’s attempt to compensate for the alkalosis by increasing the renal tubular reabsorption of H+ ions, by eliminating K+ ions. On physical exam, a palpable epigastric mass, the shape, and size of an olive (“palpable olive”) may be apparent. Definitive treatment is a surgical correction called a pyloromyotomy.[rx]
Ulcerative Pathologies
Peptic Ulcer Disease – Gastric ulcers occur when the mucosa and submucosa of the stomach lining break down and are commonly due to H. pylori or long-term NSAID use. Less common causes include stress, diet, infection, and rarely, tumors. Often, ulcers are present in either the stomach mucosa (pain worsens after eating) or the duodenal mucosa (pain improves after eating). Patients often describe the pain as a burning or gnawing-type of pain felt in the epigastric region that may or may not radiate to the back. For patients who are clinically suspicious for peptic ulcer disease, an EGD (esophagogastroduodenoscopy) evaluation is a standard of care along with H. pylori testing. If H. pylori-positive, patient treatment will be with a proton pump inhibitor, amoxicillin, and clarithromycin. For penicillin-allergic patients, metronidazole can be an alternative. For H. pylori-negative patients with gastric ulcerations, further history should be obtained regarding NSAID use or other symptoms that could elucidate a potential etiology.
The gold standard for testing is esophagogastroduodenoscopy (EGD). Management typically includes H2-receptor antagonists and proton pump inhibitors (PPIs).[rx]
Gastroesophageal Reflux Disease – Gastroesophageal reflux disease (GERD) is a common medical problem due to the reflux of gastric acid into the esophagus, causing symptoms or esophageal mucosal injury. Inappropriate relaxation of the lower esophageal sphincter is the common cause of reflux symptoms. The symptoms may include heartburn, regurgitation, dyspepsia, hoarseness, and chronic cough. Treatment will include weight loss and lifestyle changes to decrease the reflux or use of acid-reducing medications such as proton pump inhibitors.
Dyspepsia – Dyspepsia describes symptoms of indigestion, including nausea, vomiting, fullness, heartburn, belching, and abdominal pain. Functional dyspepsia refers to patients experiencing these symptoms in the absence of any clear cause.[rx] However, most cases of dyspepsia result from pathologies, a number of which involve the stomach.
Inflammatory Conditions
Inflammatory Bowel Disease – Crohn’s disease is a non-caseating chronic granulomatous condition that is a type of inflammatory bowel disease. Crohn’s disease is capable of affecting any portion of the alimentary canal, from the mouth to the anus, including the stomach. Crohn’s disease is characterized by transmural inflammation that is non-continuous (skip lesions). Histologically, non-caseating granulomas are the hallmark finding. Endoscopy may show “cobblestoning” of the mucosa, mucosal strictures (i.e., string sign), or other sequelae throughout the GI tract. The terminal ileum is the most commonly affected region, but cases with gastric involvement have been noted with an incidence of <4%. Acute inflammatory flares are treated with steroids, and maintenance medical immunomodulating therapies are available.[rx]
Gastritis – Gastritis refers to gastric mucosa inflammation. Acute cases of gastritis are due to an imbalance between the stomach’s acidic environment and its mucosal defense to the acid. This condition can arise with alcohol, chronic use of nonsteroidal anti-inflammatory drugs (NSAIDs), chemotherapy, decreased mucosal perfusion, or increased acid production. Chronic cases of gastritis involve atrophy of the gastric mucosa and intestinal metaplasia and primarily divide into two subtypes: autoimmune gastritis and bacterial gastritis. Autoimmune gastritis involves the autoimmune destruction of parietal cells, while bacterial gastritis refers to a gastric infection by Helicobacter pylori.
Helicobacter Gastritis – Helicobacter pylori (H. pylori) gram-negative bacteria is the primary pathogen responsible for peptic ulcers and gastric cancers (MALToma and adenocarcinoma) with a global prevalence of infection >50%. H. pylori-associated MALT lymphoma is incredibly unique in the fact that it is a type of cancer that can be treated effectively with antibiotics. H. pylori can colonize the stomach by neutralizing the acidic environment immediately surrounding the bacteria. The pathogen contains an enzyme called urease that is capable of converting urea to ammonia, which increases the pH, providing a protected environment until the pathogen can travel to and attach to the surface of the foveolar cells. Once anchored, the pathogen is protected by the mucus buffer. Patients will present with epigastric burning, gnawing discomfort, dyspepsia, nighttime awakening, and relief with antacids. A urea breath test can determine if urease-positive bacteria have colonized the patient. Endoscopy is also recommended to evaluate for ulceration and intestinal metaplasia.
Two widely accepted management regimens:
Triple Therapy: PPI + clarithromycin + amoxicillin (alt: metronidazole)
Quadruple Therapy: (history of previous macrolide exposure) PPI + bismuth subcitrate + metronidazole + tetracycline
Gastric Cancers:
90% of gastric cancers are determined to be adenocarcinomas with the remaining percentages divided between MALToma, carcinoid tumors, and stromal tumors.
Gastric Adenocarcinoma
Two types of adenocarcinoma are common:
Intestinal Type: The intestinal type results from metaplasia and atrophy due to chronic gastritis, and is associated with smoking, alcohol, nitrosamines, and type A blood. Intestinal type tumors are typically intrusive growths on the lesser curvature of the stomach and may ulcerate.
Diffuse: The diffuse type is less common but characteristically results in a diffuse thickening of the gastric wall leading to a phenomenon called “linitis plastic.”
Gastric cancers are associated with several extra-systemic clinical findings, including acanthosis nigricans, Leser-Treat sign, Virchow’s node, Sister Mary Joseph’s nodule, and Krukenberg tumors. Most gastric cancers are adenocarcinomas, and the most commonly metastasize to the liver.
Management is mostly dependent on staging but commonly may involve tumor resection followed by adjuvant chemotherapy/radiation regimens. Gastric cancers have a good prognosis if the tumor is found early. However, most lesions are asymptomatic until later stages of disease progression.
Other Pathologies:
Menetrier’s disease – Menetrier disease is hyperplasia of foveolar cells leading to overproduction of mucus, leading to excessive protein loss and minimal gastric acid production. The patient presents with non-specific abdominal pain and edema. On endoscopy evaluation, gastric rugae will appear hypertrophied.
GAVE (Gastric Antral Vascular Ectasia) – Angiodysplasia conditions leading to the fragility of gastric blood vessels that are susceptible to rupture and bleeding. Patients can present with chronic anemia, GI bleeds, or hematemesis. On endoscopy, the lining of the stomach appears similar to the striations on a watermelon (i.e., watermelon stomach).
Gastroparesis – Gastroparesis is a condition where the gastric intrinsic nervous system called the enteric nervous system becomes impaired as a result of various etiologies like uncontrolled diabetes mellitus. Failure of the enteric nervous system fails the peristaltic contractions leading to stagnation of chyme propagation within and through the stomach. This condition can be idiopathic or caused by connective tissue disease, neurologic dysfunction, diabetes, infection, cancer, or obstruction
Stomach Conditions
Gastroesophageal reflux – Stomach contents, including acid, can travel backward up the esophagus. There may be no symptoms or reflux may cause heartburn or coughing.
Gastroesophageal reflux disease (GERD) – When symptoms of reflux become bothersome or occur frequently, they’re called GERD. Infrequently, GERD can cause serious problems of the esophagus.
Dyspepsia – Another name for stomach upset or indigestion. Dyspepsia may be caused by almost any benign or serious condition that affects the stomach.
Gastric ulcer (stomach ulcer) – An erosion in the lining of the stomach, often causing pain and/or bleeding. Gastric ulcers are most often caused by NSAIDs or H. pylori infection.
Peptic ulcer disease – Doctors consider ulcers in either the stomach or the duodenum (the first part of the small intestine) peptic ulcer disease.
Gastritis – Inflammation of the stomach, often causing nausea and/or pain. Gastritis can be caused by alcohol, certain medications, H. pylori infection, or other factors.
Stomach cancer – Gastric cancer is an uncommon form of cancer in the U.S. Adenocarcinoma and lymphoma make up most of the cases of stomach cancer.
Zollinger-Ellison syndrome (ZES) – One or more tumors that secrete hormones that lead to increased acid production. Severe GERD and peptic ulcer disease result from this rare disorder.
Gastric varices – In people with severe liver disease, veins in the stomach may swell and bulge under increased pressure. Called varices, these veins are at high risk for bleeding, although less so than esophageal varices are.
Stomach bleeding – Gastritis, ulcers, or gastric cancers may bleed. Seeing blood or black material in vomit or stool is usually a medical emergency.
Gastroparesis (delayed gastric emptying) – Nerve damage from diabetes or other conditions may impair the stomach’s muscle contractions. Nausea and vomiting are the usual symptoms.
Stomach Tests
Upper endoscopy (esophagogastroduodenoscopy or EGD) – A flexible tube with a camera on its end (endoscope) is inserted through the mouth. The endoscope allows examination of the esophagus, stomach, and duodenum (the first part of the small intestine).
Computed tomography (CT scan) – A CT scanner uses X-rays and a computer to create images of the stomach and abdomen.
Magnetic resonance imaging – Using a magnetic field, a scanner creates high-resolution images of the stomach and abdomen.
pH testing – Using a tube through the nose into the esophagus, acid levels in the esophagus can be monitored. This can help diagnose or change treatment for GERD.
Barium swallow – After swallowing barium, X-ray films of the esophagus and stomach are taken. This can sometimes diagnose ulcers or other problems.
Upper GI series – X-rays are taken of the esophagus, stomach, and upper part of the small intestine.
Gastric emptying study – A test of how rapidly food passes through the stomach. The food is labeled with a chemical and viewed on a scanner.
Stomach biopsy – During an endoscopy, a doctor can take a small piece of stomach tissue for tests. This can diagnose H. pylori infection, cancer, or other problems.
H. pylori test – While most people with H. pylori infection don’t develop ulcers, simple blood or stool tests can be done to check for infection in people with ulcers or to verify that the infection is wiped out after treatment..
Stomach Treatments
Histamine (H2) blockers – Histamine increases stomach acid secretion; blocking histamine can reduce acid production and GERD symptoms.
Proton pump inhibitors – These medicines directly inhibit the acid pumps in the stomach. They must be taken daily to be effective.
Antacids – These medicines can help against the effects of acid but don’t kill bacteria or stop acid production.
Endoscopy – During an upper endoscopy, tools on the endoscope can sometimes stop stomach bleeding, if present.
Motility agents – Medicines can increase the contraction of the stomach, improving symptoms of gastroparesis.
Stomach surgery – Cases of severe stomach bleeding, ruptured ulcers, or cancer require surgery to be cured.
Antibiotics – H. pylori infection can be cured with antibiotics, which are taken with other medicines to heal the stomach.
The digestive system comprises the gastrointestinal tract and accessory organs. The gastrointestinal tract consists of the oral cavity, pharynx, esophagus, stomach, small intestine, and large intestine. The accessory organs are the teeth, tongue, and glandular organs such as salivary glands, liver, gallbladder, and pancreas.
The digestive system functions to provide mechanical processing, digestion, absorption of food, secretion of water, acids, enzymes, buffer, salt, and excretion of waste products.
Digestion is the process of mechanically and enzymatically breaking down food into substances for absorption into the bloodstream. The food contains three macronutrients that require digestion before they can be absorbed: fats, carbohydrates, and proteins. Through the process of digestion, these macronutrients are broken down into molecules that can traverse the intestinal epithelium and enter the bloodstream for use in the body. Digestion is a form of catabolism or breaking down of substances that involves two separate processes: mechanical digestion and chemical digestion. Mechanical digestion involves physically breaking down food substances into smaller particles to more efficiently undergo chemical digestion. The role of chemical digestion is to further degrade the molecular structure of the ingested compounds by digestive enzymes into a form that is absorbable into the bloodstream. Effective digestion involves both of these processes, and defects in either mechanical digestion or chemical digestion can lead to nutritional deficiencies and gastrointestinal pathologies.
Anatomy of the Digestive System
The human gastrointestinal tract refers to the stomach and intestine, and sometimes to all the structures from the mouth to the anus.
Key Points
The major organs of the digestive system are the stomach and intestine.
The upper gastrointestinal tract consists of the esophagus, stomach, and duodenum.
The lower gastrointestinal tract includes the small intestine and the large intestine.
Digestive juices are produced by the pancreas and the gallbladder.
The small intestine includes the duodenum, jejunum, and ileum.
The large intestine includes the cecum, colon, rectum, and anus.
Key Terms
upper gastrointestinal tract: This tract consists of the esophagus, stomach, and duodenum.
lower gastrointestinal tract: This tract includes most of the small intestine and all of the large intestine.
Upper and lower gastrointestinal tract: The major organs of the human gastrointestinal system.
The human gastrointestinal tract refers to the stomach and intestine, and sometimes to all the structures from the mouth to the anus.
Upper Gastrointestinal Tract
The upper gastrointestinal tract consists of the esophagus, stomach, and duodenum. The exact demarcation between upper and lower can vary. Upon gross dissection, the duodenum may appear to be a unified organ, but it is often divided into two parts based upon function, arterial supply, or embryology.
The upper gastrointestinal tract includes the:
Esophagus, the fibromuscular tube that food passes through—aided by peristaltic contractions—the pharynx to the stomach.
Stomach, which secretes protein-digesting enzymes called proteases and strong acids to aid in food digestion, before sending the partially digested food to the small intestines.
Duodenum, the first section of the small intestine that may be the principal site for iron absorption.
Lower Gastrointestinal Tract
The lower gastrointestinal tract includes most of the small intestine and all of the large intestine. According to some sources, it also includes the anus.
The small intestine has three parts:
Small intestine: This image shows the position of the small intestine in the gastrointestinal tract.
Duodenum: Here the digestive juices from the pancreas ( digestive enzymes ) and the gallbladder ( bile ) mix together. The digestive enzymes break down proteins and bile and emulsify fats into micelles. The duodenum contains Brunner’s glands that produce bicarbonate, and pancreatic juice that contains bicarbonate to neutralize hydrochloric acid in the stomach.
Jejunum: This is the midsection of the intestine, connecting the duodenum to the ileum. It contains the plicae circulares and villi to increase the surface area of that part of the GI tract.
Ileum: This has villi, where all soluble molecules are absorbed into the blood ( through the capillaries and lacteals).
The large intestine has four parts:
Cecum, the vermiform appendix that is attached to the cecum.
Colon, which includes the ascending colon, transverse colon, descending colon, and sigmoid flexure. The main function of the colon is to absorb water, but it also contains bacteria that produce beneficial vitamins like vitamin K.
Rectum.
Anus.
The ligament of Treitz is sometimes used to divide the upper and lower GI tracts.
Processes and Functions of the Digestive System
Digestion is necessary for absorbing nutrients from food and occurs through two processes: mechanical and chemical digestion.
Key Points
Two important functions of the digestive system are digestion and absorption.
The nutrients that come from food are derived from proteins, fats, carbohydrates, vitamins, and minerals. These complex macromolecules must be broken down and absorbed in the gastrointestinal (GI) tract.
Mechanical digestion starts in the mouth, with the physical processing of food by the teeth, and continues in the stomach.
Chemical digestion starts with the release of enzymes in saliva, and continues in the stomach and intestines.
During absorption, the nutrients that come from food pass through the wall of the small intestine and into the bloodstream.
Key Terms
mastication: The process of mechanical breakdown by the teeth; also known as chewing.
bolus: Moistened and mechanically manipulated food.
mechanical digestion: The breaking down of food into digestible chunks, normally using the teeth.
chemical digestion: A process that involves the action of enzymes to break down food into components that can be absorbed by the small intestine.
gastrointestinal tract: This tract consists of the stomach and intestine, and sometimes includes all the structures from the mouth to the anus. The digestive system is a broader term that includes other structures, including the accessory organs of digestion, such as the liver, gallbladder, and pancreas.
The Digestive System
The proper functioning of the gastrointestinal (GI) tract is imperative for our well-being and life-long health. A non-functioning or poorly-functioning GI tract can be the source of many chronic health problems that can interfere with your quality of life.
Here is a look at the importance of two main functions of the digestive system: digestion and absorption.
Digestion
The gastrointestinal tract is responsible for the breakdown and absorption of the various foods and liquids needed to sustain life. Many different organs have essential roles in the digestion of food, from the mechanical breakdown of food by the teeth to the creation of bile (an emulsifier) by the liver.
Bile production plays an important role in digestion: it is stored and concentrated in the gallbladder during fasting stages and discharged to the small intestine. Pancreatic juices are excreted into the digestive system to break down complex molecules such as proteins and fats.
Absorption
Absorption occurs in the small intestines, where nutrients directly enter the bloodstream.
Each component of the digestive system plays a special role in these complementary processes. The structure of each component highlights the function of that particular organ, providing seamless anatomy to keep our body fueled and healthy.
Components of the Digestive System
The digestive system is comprised of the alimentary canal, or the digestive tract, and other accessory organs that play a part in digestion—such as the liver, the gallbladder, and the pancreas. The alimentary canal and the GI tract are terms that are sometimes used interchangeably.
The alimentary canal is the long tube that runs from the mouth (where the food enters) to the anus (where indigestible waste leaves). The organs in the alimentary canal include the mouth (the site of mastication), the esophagus, the stomach, the small and large intestines, the rectum, and the anus. From mouth to anus, the average adult digestive tract is about thirty feet (30′) long.
Processes of Digestion
Food is the body’s source of fuel. The nutrients in food give the body’s cells the energy they need to operate. Before food can be used it has to be mechanically broken down into tiny pieces, then chemically broken down so nutrients can be absorbed.
In humans, proteins need to be broken down into amino acids, starches into sugars, and fats into fatty acids and glycerol. This mechanical and chemical breakdown encompasses the process of digestion.
To recap these twin processes
Mechanical digestion: Larger pieces of food get broken down into smaller pieces while being prepared for chemical digestion; this process starts in the mouth and continues into the stomach.
Chemical digestion: Several different enzymes break down macromolecules into smaller molecules that can be absorbed. The process starts in the mouth and continues into the intestines.
Moistening and Breakdown of Food
Digestion begins in the mouth. A brain reflex triggers the flow of saliva when we see or even think about food. Enzymes in saliva then begin the chemical breakdown of food; teeth aid in the mechanical breakdown of larger food particles.
Saliva moistens the food, while the teeth masticate the food and make it easier to swallow. To accomplish this moistening goal, the salivary glands produce an estimated three liters of saliva per day.
Amylase, the digestive enzyme found in saliva, starts to break down starch into simple sugars before the food even leaves the mouth. The nervous pathway involved in salivary excretion requires stimulation of receptors in the mouth, sensory impulses to the brain stem, and parasympathetic impulses to salivary glands. Once the food is moistened and rolled and ready to swallow, it is known as a bolus.
Swallowing and the Movement of Food
For swallowing to happen correctly a combination of 25 muscles must all work together at the same time. Swallowing occurs when the muscles in your tongue and mouth move the bolus into your pharynx.
The pharynx, which is the passageway for food and air, is about five inches (5″) long—a remarkably small space. A small flap of skin called the epiglottis closes over the pharynx to prevent food from entering the trachea, which would cause choking. Instead, food is pushed into the muscular tube called the esophagus. Waves of muscle movement called peristalsis, move the bolus down to the stomach.
While in the digestive tract, the food is really passing through the body rather than being in the body. The smooth muscles of the tubular digestive organs move the food efficiently along as it is broken down into easily absorbed ions and molecules.
Large-scale Breakdown in the Stomach
Once the bolus reaches the stomach, gastric juices mix with the partially digested food and continue the breakdown process. The bolus is converted into a slimy material called chyme.
Major digestive hormones: There are at least five major digestive hormones in the gut of mammals that help process food through chemical digestion in the gall bladder, duodenum, stomach, and pancreas. These hormones are cholecystokinin, gastric inhibitory polypeptide, motilin, secretin, and gastrin.
The stomach is a muscular bag that maneuvers food particles, mixing highly acidic gastric juice and powerful digestive enzymes with the chyme to prepare for nutrient absorption in the small intestine. Stimulatory hormones such as gastrin and motilin help the stomach pump gastric juice and move chyme. The complex network of hormones eventually prepares chyme for entry into the duodenum, the first segment of the small intestine.
Absorption in the Small Intestine
During absorption, the nutrients that come from food (such as proteins, fats, carbohydrates, vitamins, and minerals) pass through the wall of the small intestine and into the bloodstream. In this way, nutrients can be distributed throughout the rest of the body. The small intestine increases surface area for absorption through tiny interior projections, like small fingers, called villi.
Waste Compaction in the Large Intestine
In the large intestine, there is resorption of water and absorption of certain minerals as feces are formed. Feces are the waste parts of the food that the body passes out through the anus.
Organs of the Digestive System
The organs of the digestive system can be divided into upper and lower digestive tracts. The upper digestive tract consists of the esophagus, stomach, and small intestine; the lower tract includes all of the large intestine, the rectum, and anus.
Key Points
The gastrointestinal tract is made up of upper and lower tracts.
Food moves from the mouth to the stomach via the esophagus.
The small intestine has three parts: the duodenum, jejunum, and ileum.
The large intestine has four parts: the cecum, colon, rectum, and anus.
Key Terms
small intestine: A winding, digestive tube and the site of large-scale nutrient absorption comprised of the duodenum, jejunum, and ileum.
esophagus: An organ in vertebrates that is a muscular tube through which food passes from the pharynx to the stomach.
stomach: An organ in animals that stores and breaks down food in the process of digestion.
large intestine: The second to last part of the digestive system is comprised of the cecum and colon.
The human body uses a variety of mental and physiological cues to initiate the process of digestion. Throughout our gastrointestinal (GI) tract, each organ serves a specific purpose to bring our food from the plate to a digestible substance from which nutrients can be extracted.
The Digestive Tube
The organs of the gastrointestinal tract: This diagram shows the relationship between the various organs of the digestive system. It shows how the oral cavity connects to the esophagus and descends into the stomach and then the small intestine. It then connects to the large intestine, then the rectum, and, finally, the anus.
Our digestive system is like a long tube, with different segments doing different jobs. The major organs within our digestive system can be split into two major segments of this tube: the upper gastrointestinal tract, and the lower gastrointestinal tract.
The Upper Gastrointestinal Tract
The upper gastrointestinal, or GI, the tract is made up of three main parts:
The esophagus.
The stomach.
The small intestine.
The Lower Gastrointestinal Tract
The lower GI tract contains the remainder of the system:
The large intestine.
The rectum.
The anus.
The exact dividing line between upper and lower tracts can vary, depending on which medical specialist is examining the GI tract.
Food Breakdown and Absorption: The Upper GI Tract
When we take a bite of food, the food material gets chewed up and processed in the mouth, where saliva begins the process of chemical and mechanical breakdown. The chewing process is also known as mastication.
When we mix up food with saliva, the resulting mushy wad is called a bolus. The bolus gets swallowed and begins its journey through the upper gastrointestinal tract.
The Esophagus
The upper GI tract begins with the esophagus, the long muscular tube that carries food to the stomach. The throat cavity in which our esophagus originates is known as the pharynx. As we swallow, the bolus moves down our esophagus, from the pharynx to the stomach, through waves of muscle movement known as peristalsis. Next, the bolus reaches the stomach itself.
The Stomach
The stomach is a muscular, hollow bag that is an important part of the upper GI tract. Many organisms have a variety of stomach types, with many segments or even multiple stomachs. As humans, we have only one stomach.
Here our bolus gets mixed with digestive acids, furthering the breakdown of the bolus, and turning the bolus material into a slimy mess called chyme. The chyme moves on into the small intestine, where nutrients are absorbed.
The Small Intestine
The small intestine is an impressive digestive tube, spanning an average of 20 feet in length. The twists and turns of the small intestine, along with tiny interior projections known as villi, help to increase the surface area for nutrient absorption.
This snaking tube is made up of three parts, in order from the stomach:
The duodenum.
The jejunum.
The ileum.
As the chyme makes its way through each segment of the small intestine, pancreatic juices from the pancreas start to break down proteins. Soapy bile from the liver, stored in the gallbladder, gets squirted into the small intestine to help emulsify—or break apart—fats.
Now thoroughly digested, with its nutrients absorbed along the path of the small intestine, what remains of our food gets passed into the lower GI tract.
Waste Compaction and Removal: The Lower Gastrointestinal Tract
The Large Intestine (Colon)
Following nutrient absorption, the food waste reaches the large intestine or colon. The large intestine is responsible for compacting waste material, removing water, and producing feces —our solid-waste product.
Accessory organs like the cecum and appendix, which are remnants of our evolutionary past, serve as special pockets at the beginning of the large intestine. The compacted and dried-out waste passes to the rectum, and out of the body through the anus. Healthy gut bacteria in the large intestine also help to metabolize our waste as it finishes its journey.
Ventilation controls its main function is to send signals to the muscles that control respiration to cause breathing to occur. The ventral respiratory group stimulates expiratory movements. The dorsal respiratory group stimulates inspiratory movements.
The control of ventilation refers to the physiological mechanisms involved in the control of breathing, which is the movement of air into and out of the lungs. Ventilation facilitates respiration. Respiration refers to the utilization of oxygen and balancing of carbon dioxide by the body as a whole, or by individual cells in cellular respiration.[rx]
The most important function of breathing is supplying of oxygen to the body and balancing the carbon dioxide levels. Under most conditions, the partial pressure of carbon dioxide (PCO2), or concentration of carbon dioxide, controls the respiratory rate.
Neural Mechanisms (Respiratory Center)
The medulla and the pons are involved in the regulation of the ventilatory pattern of respiration.
Key Points
The ventral respiratory group controls voluntarily forced exhalation and acts to increase the force of inspiration.
The dorsal respiratory group (nucleus tractus solitarius) controls mostly inspiratory movements and their timing.
Ventilatory rate (minute volume) is tightly controlled and determined primarily by blood levels of carbon dioxide as determined by metabolic rate.
Chemoreceptors can detect changes in blood pH that require changes in involuntary respiration to correct. The apneustic (stimulating) and pnuemotaxic (limiting) centers of the pons work together to control the rate of breathing.
The medulla sends signals to the muscles that initiate inspiration and expiration and controls nonrespiratory air movement reflexes, like coughing and sneezing.
Key Terms
respiratory control centers: The medulla sends signals to the muscles involved in breathing, and the pons control the rate of breathing.
chemoreceptors: These are receptors in the medulla and in the aortic and carotid bodies of the blood vessels that detect changes in blood pH and signal the medulla to correct those changes.
Involuntary respiration is any form of respiratory control that is not under direct, conscious control. Breathing is required to sustain life, so involuntary respiration allows it to happen when voluntary respiration is not possible, such as during sleep. Involuntary respiration also has metabolic functions that work even when a person is conscious.
The Respiratory Centers
Anatomy of the brainstem: The brainstem, which includes the pons and medulla.
Involuntary respiration is controlled by the respiratory centers of the upper brainstem (sometimes termed the lower brain, along with the cerebellum). This region of the brain controls many involuntary and metabolic functions besides the respiratory system, including certain aspects of cardiovascular function and involuntary muscle movements (in the cerebellum).
The respiratory centers contain chemoreceptors that detect pH levels in the blood and send signals to the respiratory centers of the brain to adjust the ventilation rate to change acidity by increasing or decreasing the removal of carbon dioxide (since carbon dioxide is linked to higher levels of hydrogen ions in the blood).
There are also peripheral chemoreceptors in other blood vessels that perform this function as well, which include the aortic and carotid bodies.
The Medulla
The medulla oblongata is the primary respiratory control center. Its main function is to send signals to the muscles that control respiration to cause breathing to occur. There are two regions in the medulla that control respiration:
The ventral respiratory group stimulates expiratory movements.
The dorsal respiratory group stimulates inspiratory movements.
The medulla also controls the reflexes for nonrespiratory air movements, such as coughing and sneezing reflexes, as well as other reflexes, like swallowing and vomiting.
The Pons
The pons is the other respiratory center and is located underneath the medulla. Its main function is to control the rate or speed of involuntary respiration. It has two main functional regions that perform this role:
The apneustic center sends signals for inspiration for long and deep breaths. It controls the intensity of breathing and is inhibited by the stretch receptors of the pulmonary muscles at a maximum depth of inspiration, or by signals from the pnuemotaxic center. It increases tidal volume.
The pnuemotaxic center sends signals to inhibit inspiration that allows it to finely control the respiratory rate. Its signals limit the activity of the phrenic nerve and inhibit the signals of the apneustic center. It decreases tidal volume.
The apneustic and pnuemotaxic centers work against each other together to control the respiratory rate.
Neural Mechanisms (Cortex)
The cerebral cortex of the brain controls voluntary respiration.
Key Points
The motor cortex within the cerebral cortex of the brain controls voluntary respiration (the ascending respiratory pathway).
Voluntary respiration may be overridden by aspects of involuntary respiration, such as chemoreceptor stimulus, and hypothalamus stress response.
The phrenic nerves, vagus nerves, and posterior thoracic nerves are the major nerves involved in respiration.
Voluntary respiration is needed to perform higher functions, such as voice control.
Key Terms
The Phrenic Nerves: A set of two nerves that brings nerve impulses from the spinal cord to the diaphragm.
primary motor cortex: The region in the brain that initiates all voluntary muscular movement, including those for respiration.
Voluntary respiration is any type of respiration that is under conscious control. Voluntary respiration is important for the higher functions that involve air supply, such as voice control or blowing out candles. Similar to how involuntary respiration’s lower functions are controlled by the lower brain, voluntary respiration’s higher functions are controlled by the upper brain, namely parts of the cerebral cortex.
The Motor Cortex
The primary motor cortex is the neural center for voluntary respiratory control. More broadly, the motor cortex is responsible for initiating any voluntary muscular movement.
The processes that drive its functions aren’t fully understood, but it works by sending signals to the spinal cord, which sends signals to the muscles it controls, such as the diaphragm and the accessory muscles for respiration. This neural pathway is called the ascending respiratory pathway.
Different parts of the cerebral cortex control different forms of voluntary respiration. Initiation of the voluntary contraction and relaxation of the internal and external intercostal muscles takes place in the superior portion of the primary motor cortex.
The center for diaphragm control is posterior to the location of thoracic control (within the superior portion of the primary motor cortex). The inferior portion of the primary motor cortex may be involved in controlled exhalation.
Activity has also been seen within the supplementary motor area and the premotor cortex during voluntary respiration. This is most likely due to the focus and mental preparation of the voluntary muscular movement that occurs when one decides to initiate that muscle movement.
Note that voluntary respiratory nerve signals in the ascending respiratory pathway can be overridden by chemoreceptor signals from involuntary respiration. Additionally, other structures may override voluntary respiratory signals, such as the activity of limbic center structures like the hypothalamus.
During periods of perceived danger or emotional stress, signals from the hypothalamus take over the respiratory signals and increase the respiratory rate to facilitate the fight or flight response.
Topography of the primary motor cortex: Topography of the primary motor cortex, on an outline drawing of the human brain. Each part of the primary motor cortex controls a different part of the body.
Nerves Used in Respiration
There are several nerves responsible for the muscular functions involved in respiration. There are three types of important respiratory nerves:
The phrenic nerves – The nerves that stimulate the activity of the diaphragm. They are composed of two nerves, the right and left phrenic nerve, which passes through the right and left side of the heart respectively. They are autonomic nerves.
The vagus nerve – Innervates the diaphragm as well as movements in the larynx and pharynx. It also provides parasympathetic stimulation for the heart and the digestive system. It is a major autonomic nerve.
The posterior thoracic nerves – These nerves stimulate the intercostal muscles located around the pleura. They are considered to be part of a larger group of intercostal nerves that stimulate regions across the thorax and abdomen. They are somatic nerves.
These three types of nerves continue the signal of the ascending respiratory pathway from the spinal cord to stimulate the muscles that perform the movements needed for respiration.
Damage to any of these three respiratory nerves can cause severe problems, such as diaphragm paralysis if the phrenic nerves are damaged. Less severe damage can cause irritation to the phrenic or vagus nerves, which can result in hiccups.
Chemoreceptor Regulation of Breathing
Chemoreceptors detect the levels of carbon dioxide in the blood by monitoring the concentrations of hydrogen ions in the blood.
Key Points
An increase in carbon dioxide concentration leads to a decrease in the pH of blood due to the production of H+ ions from carbonic acid.
In response to a decrease in blood pH, the respiratory center (in the medulla ) sends nervous impulses to the external intercostal muscles and the diaphragm, to increase the breathing rate and the volume of the lungs during inhalation.
Hyperventilation causes alakalosis, which causes a feedback response of decreased ventilation (to increase carbon dioxide), while hypoventilation causes acidosis, which causes a feedback response of increased ventilation (to remove carbon dioxide).
Any situation with hypoxia (too low oxygen levels) will cause a feedback response that increases ventilation to increase oxygen intake.
Vomiting causes alkalosis and diarrhea causes acidosis, which will cause an appropriate respiratory feedback response.
Key Terms
hypoxia: A system-wide deficiency in the levels of oxygen that reach the tissues.
central chemoreceptors: Located within the medulla, they are sensitive to the pH of their environment.
peripheral chemoreceptors: The aortic and carotid bodies, which act principally to detect variation of the oxygen concentration in the arterial blood, also monitor arterial carbon dioxide and pH.
Chemoreceptor regulation of breathing is a form of negative feedback. The goal of this system is to keep the pH of the bloodstream within normal neutral ranges, around 7.35.
Chemoreceptors
A chemoreceptor, also known as a chemosensor, is a sensory receptor that transduces a chemical signal into an action potential. The action potential is sent along nerve pathways to parts of the brain, which are the integrating centers for this type of feedback. There are many types of chemoreceptors in the body, but only a few of them are involved in respiration.
The respiratory chemoreceptors work by sensing the pH of their environment through the concentration of hydrogen ions. Because most carbon dioxide is converted to carbonic acid (and bicarbonate ) in the bloodstream, chemoreceptors are able to use blood pH as a way to measure the carbon dioxide levels of the bloodstream.
The main chemoreceptors involved in respiratory feedback are:
Central chemoreceptors: These are located on the ventrolateral surface of the medulla oblongata and detect changes in the pH of spinal fluid. They can be desensitized over time from chronic hypoxia (oxygen deficiency) and increased carbon dioxide.
Peripheral chemoreceptors: These include the aortic body, which detects changes in blood oxygen and carbon dioxide, but not pH, and the carotid body which detects all three. They do not desensitize and have less of an impact on the respiratory rate compared to the central chemoreceptors.
Chemoreceptor Negative Feedback
Negative feedback responses have three main components: the sensor, the integrating sensor, and the effector. For the respiratory rate, the chemoreceptors are the sensors for blood pH, the medulla and pons from the integrating center, and the respiratory muscles are the effector.
Consider a case in which a person is hyperventilating from an anxiety attack. Their increased ventilation rate will remove too much carbon dioxide from their body. Without that carbon dioxide, there will be less carbonic acid in the blood, so the concentration of hydrogen ions decreases and the pH of the blood rises, causing alkalosis.
In response, the chemoreceptors detect this change and send a signal to the medulla, which signals the respiratory muscles to decrease the ventilation rate so carbon dioxide levels and pH can return to normal levels.
There are several other examples in which chemoreceptor feedback applies. A person with severe diarrhea loses a lot of bicarbonate in the intestinal tract, which decreases bicarbonate levels in the plasma. As bicarbonate levels decrease while hydrogen ion concentrations stay the same, blood pH will decrease (as bicarbonate is a buffer) and become more acidic.
In cases of acidosis, feedback will increase ventilation to remove more carbon dioxide to reduce the hydrogen ion concentration. Conversely, vomiting removes hydrogen ions from the body (as the stomach contents are acidic), which will cause decreased ventilation to correct alkalosis.
Chemoreceptor feedback also adjusts for oxygen levels to prevent hypoxia, though only the peripheral chemoreceptors sense oxygen levels. In cases where oxygen intake is too low, feedback increases ventilation to increase oxygen intake.
A more detailed example would be that if a person breathes through a long tube (such as a snorkeling mask) and has increased amounts of dead space, feedback will increase ventilation.
Respiratory feedback: The chemoreceptors are the sensors for blood pH, the medulla and pons form the integrating center, and the respiratory muscles are the effector.
Proprioceptor Regulation of Breathing
The Hering–Breuer inflation reflex prevents overinflation of the lungs.
Key Points
Pulmonary stretch receptors present in the smooth muscle of the airways and the pleura respond to excessive stretching of the lung during large inspirations.
The Hering–Breuer inflation reflex is initiated by stimulation of
stretch receptors. The deflation reflex is initiated by stimulation
of the compression receptors (called proprioceptors) or deactivation of
stretch receptors when the lungs deflate.
Activation of the pulmonary stretch receptors (via the vagus nerve ) results in inhibition of the inspiratory stimlus in the medulla, and thus inhibition of inspiration and initiation of expiration.
An increase in pulmonary stretch receptor activity leads to an elevation of heart rate ( tachycardia ).
A cyclical, elevated heart rate from inspiration is called sinus arrhythmia and is a normal response in youth. Inhibition of inspiration is important to allow expiration to occur.
Key Terms
sinus arrhythmia: A normal cyclical heart rate change in which an increase in heart rate occurs during inspiration, but returns to normal during expiration.
pulmonary stretch receptors: A sensory receptor that sends an action potential when it detects pressure, tension, stretch, or distortion.
The lungs are a highly elastic organ capable of expanding to a much larger volume during inflation. While the volume of the lungs is proportional to the pressure of the pleural cavity as it expands and contracts during breathing, there is a risk of over-inflation of the lungs if inspiration becomes too deep for too long. Physiological mechanisms exist to prevent over-inflation of the lungs.
The Hering–Bauer Reflex
Cardiac and respiratory branches of the vagus nerve: The vagus nerve is the neural pathway for stretch receptor regulation of breathing.
The Hering–Breuer reflex (also called the inflation reflex) is triggered to prevent over-inflation of the lungs. There are many stretch receptors in the lungs, particularly within the pleura and the smooth muscles of the bronchi and bronchioles, that activate when the lungs have inflated to their ideal maximum point.
These stretch receptors are mechanoreceptors, which are a type of sensory receptor that specifically detects mechanical pressure, distortion, and stretch, and are found in many parts of the human body, especially the lungs, stomach, and skin. They do not detect fine-touch information like most sensory receptors in the human body, but they do create a feeling of tension or fullness when activated, especially in the lungs or stomach.
When the lungs are inflated to their maximum volume during inspiration, the pulmonary stretch receptors send an action potential signal to the medulla and pons in the brain through the vagus nerve.
The pneumatic center of the pons sends signals to inhibit the apneustic center of the pons, so it doesn’t activate the inspiratory area (the dorsal medulla), and the inspiratory signals that are sent to the diaphragm and accessory muscles stop. This is called the inflation reflex.
As inspiration stops, expiration begins and the lung begins to deflate. As the lungs deflate the stretch receptors are deactivated (and compression receptors called proprioceptors may be activated) so the inhibitory signals stop and inhalation can begin again—this is called the deflation reflex.
Early physiologists believed this reflex played a major role in establishing the rate and depth of breathing in humans. While this may be true for most animals, it is not the case for most adult humans at rest. However, the reflex may determine the breathing rate and depth in newborns and in adult humans when tidal volume is more than 1 L, such as when exercising.
Additionally, people with emphysema have an impaired Hering–Bauer reflex due to a loss of pulmonary stretch receptors from the destruction of lung tissue, so their lungs can over-inflate as well as collapse, which contributes to shortness of breath.
Sinus Arrhythmia
As the Hering–Bauer reflex uses the vagus nerve as its neural pathway, it also has a few cardiovascular system effects because the vagus nerve also innervates the heart.
During stretch receptor activation, the inhibitory signal that travels through the vagus nerve is also sent to the sinus-atrial node of the heart. Its stimulation causes a short-term increase in resting heart rate, which is called tachycardia.
The heart rate returns to normal during expiration when the stretch receptors are deactivated. When this process is cyclical it is called a sinus arrhythmia, which is a generally normal physiological phenomenon in which there is short-term tachycardia during inspiration.
Sinus arrhythmias do not occur in everyone and are more common in youth. The sensitivity of the sinus-atrial node to the inflation reflex is lost over time, so sinus arrhythmias are less common in older people.
Control of respiratory rhythm
Ventilatory pattern
Respiratory centre and its groups of neurons
Breathing is normally an unconscious, involuntary, automatic process. The pattern of motor stimuli during breathing can be divided into an inhalation stage and an exhalation stage. Inhalation shows a sudden, ramped increase in motor discharge to the respiratory muscles (and the pharyngeal constrictor muscles).[rx] Before the end of inhalation, there is a decline in, and end of motor discharge. Exhalation is usually silent, except at high respiratory rates.
The respiratory center in the medulla and pons of the brainstem controls the rate and depth of respiration, (the respiratory rhythm), through various inputs. These include signals from the peripheral chemoreceptors and central chemoreceptors; from the vagus nerve and glossopharyngeal nerve carrying input from the pulmonary stretch receptors, and other mechanoreceptors in the lungs.[rx][rx] as well as signals from the cerebral cortex and hypothalamus.
Medulla
ventral respiratory group (includes the pre-Bötzinger complex). The ventral respiratory group controls voluntarily forced exhalation and acts to increase the force of inhalation. Regulates rhythm of inhalation and exhalation.
dorsal respiratory group (solitary nucleus). The dorsal respiratory group controls mostly movements of inhalation and their timing.
Pons
pneumotaxic center.
Coordinates speed of inhalation and exhalation
Sends inhibitory impulses to the inspiratory area
Involved in fine-tuning of respiration rate.
apneustic center
Coordinates speed of inhalation and exhalation.
Sends stimulatory impulses to the inspiratory area – activates and prolongs inhalations
Overridden by pneumatic control from the apneustic area to end inhalation
Control of ventilatory pattern
Ventilation is normally unconscious and automatic but can be overridden by conscious alternative patterns.[rx] Thus the emotions can cause yawning, laughing, sighing (etc.), social communication causes speech, song, and whistling, while entirely voluntary overrides are used to blow out candles, and breath-holding (for instance, to swim underwater). Hyperventilation may be entirely voluntary or in response to emotional agitation or anxiety when it can cause the distressing hyperventilation syndrome. The voluntary control can also influence other functions such as the heart rate as in yoga practices and meditation.[rx]
The ventilatory pattern is also temporarily modified by complex reflexes such as sneezing, straining, burping, coughing and vomiting.
Determinants of ventilatory rate
Ventilatory rate (respiratory minute volume) is tightly controlled and determined primarily by blood levels of carbon dioxide as determined by metabolic rate. Blood levels of oxygen become important in hypoxia. These levels are sensed by central chemoreceptors on the surface of the medulla oblongata for increased pH (indirectly from the increase of carbon dioxide in cerebrospinal fluid), and the peripheral chemoreceptors in the arterial blood for oxygen and carbon dioxide. Afferent neurons from the peripheral chemoreceptors are via the glossopharyngeal nerve (CN IX) and the vagus nerve (CN X).
The concentration of CO2 rises in the blood when the metabolic use of O2, and the production of CO2 is increased during, for example, exercise. The CO2 in the blood is transported largely as bicarbonate (HCO3−) ions, by conversion first to carbonic acid (H2CO3), by the enzyme carbonic anhydrase, and then by disassociation of this acid to H+ and HCO3−. Build-up of CO2 therefore causes an equivalent build-up of the disassociated hydrogen ions, which, by definition, decreases the pH of the blood. The pH sensors on the brain stem immediately respond to this fall in pH, causing the respiratory center to increase the rate and depth of breathing. The consequence is that the partial pressure of CO2 (PCO2) does not change from rest going into exercise. During very short-term bouts of intense exercise the release of lactic acid into the blood by the exercising muscles causes a fall in the blood plasma pH, independently of the rise in the PCO2, and this will stimulate pulmonary ventilation sufficiently to keep the blood pH constant at the expense of a lowered PCO2.
Mechanical stimulation of the lungs can trigger certain reflexes as discovered in animal studies. In humans, these seem to be more important in neonates and ventilated patients, but of little relevance in health. The tone of respiratory muscle is believed to be modulated by muscle spindles via a reflex arc involving the spinal cord.
Drugs can greatly influence the rate of respiration. Opioids and anesthetics tend to depress ventilation, by decreasing the normal response to raised carbon dioxide levels in the arterial blood. Stimulants such as amphetamines can cause hyperventilation.
Pregnancy tends to increase ventilation (lowering plasma carbon dioxide tension below normal values). This is due to increased progesterone levels and results in enhanced gas exchange in the placenta.
Feedback control
Receptors play important roles in the regulation of respiration and include the central and peripheral chemoreceptors, and pulmonary stretch receptors, a type of mechanoreceptor.
Central chemoreceptors of the central nervous system, located on the ventrolateral medullary surface, are sensitive to the pH of their environment.[rx][rx]
Peripheral chemoreceptors act most importantly to detect variation of the PO2 in the arterial blood, in addition to detecting arterial PCO2 and pH.
Mechanoreceptors are located in the airways and parenchyma and are responsible for a variety of reflex responses. These include:
The Hering-Breuer reflex terminates inhalation to prevent overinflation of the lungs, and the reflex responses of coughing, airway constriction, and hyperventilation.
The upper airway receptors are responsible for reflex responses such as sneezing, coughing, closure of the glottis, and hiccups.
The spinal cord reflex responses include the activation of additional respiratory muscles as compensation, gasping response, hypoventilation, and an increase in breathing frequency and volume.
The nasopulmonary and mesothoracic reflexes regulate the mechanism of breathing through deepening the inhale. Triggered by the flow of the air, the pressure of the air in the nose, and the quality of the air, impulses from the nasal mucosa are transmitted by the trigeminal nerve to the respiratory center in the brainstem, and the generated response is transmitted to the bronchi, the intercostal muscles and the diaphragm.
Respiratory Adjustments/Acclimatization is the process of adjustment that the respiratory system makes due to chronic exposure to a high altitude. Over a period of time, the body adjusts to accommodate the lower partial pressure of oxygen.
The increase in muscular work and metabolic rate associated with exercise necessitates both elevated 02 uptakes by the gills (M02) and enhanced 02 delivery to the tissues. Both of these processes can be considered limiting factors in determining overall exercise performance. The present discussion primarily focuses on the various factors affecting the transfer of 02 across the gill during exercise.
Adjustments During Exercise
Aerobic and anaerobic exercise work to increase the mechanical efficiency of the heart.
Key Points
There is tremendous variation in an individual’s response to exercise.
The beneficial effects of physical activity include improved cognition from the increased flow of blood and oxygen to the brain and reduced stress response.
Anaerobic respiration happens during exercise if the body does not get enough oxygen to meet its metabolic demands.
Extremely intense, long-term cardiovascular exercise can be deleterious and has been associated with asthma and sudden cardiac death.
Sudden cardiac death from exercise has a genetic component that is worsened by cardiac hypertrophy.
Key Terms
anaerobic exercise: This occurs during exercise when the body’s oxygen intake doesn’t meet oxygen demands to produce enough ATP.
asthma: A long-term respiratory condition, marked by airway obstruction from bronchospasm. It is often in response to an allergen, cold air, exercise, or emotional stress.
During exercise, the human body needs a greater amount of oxygen to meet the increased metabolic demands of the muscle tissues. Various short-term respiratory changes must occur in order for those metabolic demands to be reached. Eventually, exercise can induce long-term cardiovascular and respiratory changes, which can be both healthy and unhealthy.
Short-Term Changes
During exercise, carbon dioxide levels (the metabolic waste) rise in arterial blood. Carbon dioxide induces vasodilation in the arteries while the heart rate increases, which leads to better blood flow and tissue perfusion, and better oxygen delivery to the tissues.
In particular, the blood flow to the brain and heart is increased, while increased blood flow to the muscles makes exercise easier. Additionally, the respiratory rate increases as a result of higher carbon dioxide levels (through chemoreceptor regulation), which allows the body to release more carbon dioxide while increasing oxygen intake.
If exercise is too intense for oxygen demands to be satisfied in the short term, anaerobic respiration will be used to make up for the ATP deficit in the muscles. This can cause a buildup of lactic acid in the muscles, which is the byproduct of lactic acid fermentation (the most common anaerobic respiration process in the human body).
This is one reason why muscles may become sore during exercise, though the lactic acid is eventually removed through conversion to glucose in the liver.
Beneficial Long-Term Changes
In the long run, exercise results in increased levels of arterial oxygen levels at rest, due to chemoreceptor desensitization to carbon dioxide levels and a lack of oxygen supply relative to oxygen demands during exercise. Over time, the elevated respiratory rate past what is needed to restore normal blood pH levels following exercise causes a long-term increase in arterial oxygen levels.
Increased oxygen levels in the body are especially important to the long-term health of the brain and heart, two organs that are vital to sustain life and that require large amounts of oxygen to function well. Brain plasticity and cognition also improves as a result.
Exercise also has beneficial effects for reducing stress responses in the body due to increased endorphin production in the brain from exercise. In long-term exercise of appropriate intensity, the volume and strength of the heart are improved, which makes additional exercise easier.
Adverse Long-Term Changes
When exercise is performed at too intense levels for too long or without adequate rest, it can cause long-term, adverse health effects. Muscle tissue repair is impaired in those that exercise too frequently. Exercise-induced asthma is another common complication from too much exercise.
Normally asthma is caused by an allergic response within the lungs, but exercise can induce a similar response from too much intake of dry and cold air during the increased respiratory rate from exercise. It is most common in those that do more cardiac-oriented exercise.
The air in the lungs is meant to be moistened and humidified before entering the lungs, but if it is not adequately treated in the upper airways, it can induce bronchospasm in the bronchioles, which causes the wheezing and coughing that occurs during an asthma attack. Asthma treatments (such as medicines from an inhaler) can help prevent exercise-induced asthma, though it is only a particular risk in those who already have allergic asthma, or who simply exercise at too much intensity for what their body is capable of handling.
Sudden cardiac death is notable for occurring in otherwise healthy and young athletes who train too much for long-distance running. While many factors that can lead to sudden cardiac death in athletes are genetic (such as inherited problems with heart rhythm or coronary artery blood supply), many of these deaths are caused by cardiac hypertrophy, in which the heart becomes too thick from damage and scarring from too-intense exercise over long periods of time.
Initially, hypertrophy improves blood flow due to increases in the strength of the heart, but it eventually leads to heart failure as the tissues become too thick to pump normally.
Athletes with genetic susceptibilities are more likely to experience sudden cardiac death as a response to their hypertrophied heart, which can contribute to the development of a severe arrhythmia (such as ventricular fibrillation). Exercising at appropriate intensities significantly reduces the risk of sudden cardiac death, though those with genetic susceptibilities should take more caution.
Adjustments at High Altitude
The human body can adapt to high altitudes through immediate and long-term acclimatization processes.
Key Points
At high altitudes, in the short term, the lack of oxygen is sensed by the peripheral chemoreceptors, which causes an increase in ventilation. An increase in heart rate and a decrease in stroke volume also occurs.
During acclimatization over a few days to weeks, the body produces more red blood cells to counteract the lower oxygen saturation in blood in high altitudes.
Full adaptation to high altitude is achieved when the increase of red blood cells reaches a plateau and stops.
Increased red blood cell levels remain for about two weeks after acclimatization, which makes it a popular training regimen for athletes.
Key Terms
acclimatization: Long-term adjustment to high altitude, which is primarily due to increased red blood cell production and capillary tissue perfusion.
hematocrit: This is the number of red blood cells in a given volume of blood.
The human body can adapt to high altitudes through immediate and long-term acclimatization. At high altitudes, there is lower air pressure compared to a lower altitude or sea-level altitude.
Due to Boyle’s law, at higher altitudes, the partial pressure of oxygen in the air is lower, and less oxygen is breathed in with every breath. The partial pressure gradients for gas exchange are also decreased, along with the percentage of oxygen saturation in hemoglobin.
Humans can survive at high altitudes with impaired short-term functions that eventually adjust in the long term. Some altitudes are too high for acclimatization to work and can cause death if people stay there for too long.
Short-Term Adjustments
At high altitudes, in the short term, the lack of oxygen is sensed by the peripheral chemoreceptors, which causes an increase in breathing rate ( hyperventilation ). However, hyperventilation also causes the adverse effect of alkalosis due to increasing the rate by which carbon dioxide is removed from the body, which inhibits the respiratory center from enhancing the respiratory rate to meet the oxygen demands.
Additionally, the peripheral chemoreceptors cause sympathetic nervous system stimulation, which causes the heart rate to increase while stroke volume decreases, and digestion is impaired. Shortness of breath is common, and urination increases.
Along with alkalosis, these effects make up the symptoms of altitude sickness, which become worse during exercise at high altitudes (which involves more anaerobic respiration than at lower altitudes), but falls off during acclimatization.
Acclimatization
Acclimatization to high altitude requires days or even weeks. Gradually, the body compensates for the respiratory alkalosis by kidney excretion of bicarbonate, which allows adequate respiration to provide oxygen without risking alkalosis. It takes about four days at any given altitude and can be enhanced by drugs such as acetazolamide (which decreases fluid retention).
Staying hydrated during acclimatization is important to minimize altitude sickness symptoms and to counteract increased urination. The heart rate and ventilation rate at rest both remain elevated despite the acclimatization, while the heart rate at maximum activity level will be reduced.
The main difference brought about by acclimatization that explains why it makes high altitudes more comfortable for the body is increased levels of circulating red blood cells, which improve the carrying capacity of oxygen by hemoglobin in the body. This is an adaptive response due to erythropoietin secretions in the kidneys (from lack of oxygen in the tissues ) that act on the liver to increase erythrocyte (red blood cell) production.
Blood volume decreases, which also increases the hematocrit, which is the concentration of hemoglobin in the blood. This increase in red blood cells remains for a few weeks after one returns to a lower altitude, so those who acclimatize to high altitude will experience improved athletic performance at lower altitudes. Capillary density and tissue perfusion also increase.
These physiological changes make high-altitude athletic training popular for athletes, such as Olympic athletes. Full hematological adaptation to high altitude is achieved when the increase of red blood cells reaches a plateau and stops.
The length of full hematological adaptation can be approximated by multiplying the altitude in kilometers by 11.4 days. For example, to adapt to 4,000 meters (13,000 ft.) of altitude would require 45.6 days.
The upper altitude limit of this linear relationship has not been fully established, in part because extremely high altitudes have such little oxygen content that they would be fatal regardless of acclimatization.
Breathing control its main function is to send signals to the muscles that control respiration to cause breathing to occur. The ventral respiratory group stimulates expiratory movements. The dorsal respiratory group stimulates inspiratory movements.
The control of ventilation refers to the physiological mechanisms involved in the control of breathing, which is the movement of air into and out of the lungs. Ventilation facilitates respiration. Respiration refers to the utilization of oxygen and balancing of carbon dioxide by the body as a whole, or by individual cells in cellular respiration.[rx]
The most important function of breathing is supplying of oxygen to the body and balancing the carbon dioxide levels. Under most conditions, the partial pressure of carbon dioxide (PCO2), or concentration of carbon dioxide, controls the respiratory rate.
Neural Mechanisms (Respiratory Center)
The medulla and the pons are involved in the regulation of the ventilatory pattern of respiration.
Key Points
The ventral respiratory group controls voluntarily forced exhalation and acts to increase the force of inspiration.
The dorsal respiratory group (nucleus tractus solitarius) controls mostly inspiratory movements and their timing.
Ventilatory rate (minute volume) is tightly controlled and determined primarily by blood levels of carbon dioxide as determined by metabolic rate.
Chemoreceptors can detect changes in blood pH that require changes in involuntary respiration to correct. The apneustic (stimulating) and pnuemotaxic (limiting) centers of the pons work together to control the rate of breathing.
The medulla sends signals to the muscles that initiate inspiration and expiration and controls nonrespiratory air movement reflexes, like coughing and sneezing.
Key Terms
respiratory control centers: The medulla sends signals to the muscles involved in breathing, and the pons control the rate of breathing.
chemoreceptors: These are receptors in the medulla and in the aortic and carotid bodies of the blood vessels that detect changes in blood pH and signal the medulla to correct those changes.
Involuntary respiration is any form of respiratory control that is not under direct, conscious control. Breathing is required to sustain life, so involuntary respiration allows it to happen when voluntary respiration is not possible, such as during sleep. Involuntary respiration also has metabolic functions that work even when a person is conscious.
The Respiratory Centers
Anatomy of the brainstem: The brainstem, which includes the pons and medulla.
Involuntary respiration is controlled by the respiratory centers of the upper brainstem (sometimes termed the lower brain, along with the cerebellum). This region of the brain controls many involuntary and metabolic functions besides the respiratory system, including certain aspects of cardiovascular function and involuntary muscle movements (in the cerebellum).
The respiratory centers contain chemoreceptors that detect pH levels in the blood and send signals to the respiratory centers of the brain to adjust the ventilation rate to change acidity by increasing or decreasing the removal of carbon dioxide (since carbon dioxide is linked to higher levels of hydrogen ions in the blood).
There are also peripheral chemoreceptors in other blood vessels that perform this function as well, which include the aortic and carotid bodies.
The Medulla
The medulla oblongata is the primary respiratory control center. Its main function is to send signals to the muscles that control respiration to cause breathing to occur. There are two regions in the medulla that control respiration:
The ventral respiratory group stimulates expiratory movements.
The dorsal respiratory group stimulates inspiratory movements.
The medulla also controls the reflexes for nonrespiratory air movements, such as coughing and sneezing reflexes, as well as other reflexes, like swallowing and vomiting.
The Pons
The pons is the other respiratory center and is located underneath the medulla. Its main function is to control the rate or speed of involuntary respiration. It has two main functional regions that perform this role:
The apneustic center sends signals for inspiration for long and deep breaths. It controls the intensity of breathing and is inhibited by the stretch receptors of the pulmonary muscles at a maximum depth of inspiration, or by signals from the pnuemotaxic center. It increases tidal volume.
The pnuemotaxic center sends signals to inhibit inspiration that allows it to finely control the respiratory rate. Its signals limit the activity of the phrenic nerve and inhibit the signals of the apneustic center. It decreases tidal volume.
The apneustic and pnuemotaxic centers work against each other together to control the respiratory rate.
Neural Mechanisms (Cortex)
The cerebral cortex of the brain controls voluntary respiration.
Key Points
The motor cortex within the cerebral cortex of the brain controls voluntary respiration (the ascending respiratory pathway).
Voluntary respiration may be overridden by aspects of involuntary respiration, such as chemoreceptor stimulus, and hypothalamus stress response.
The phrenic nerves, vagus nerves, and posterior thoracic nerves are the major nerves involved in respiration.
Voluntary respiration is needed to perform higher functions, such as voice control.
Key Terms
The Phrenic Nerves: A set of two nerves that brings nerve impulses from the spinal cord to the diaphragm.
primary motor cortex: The region in the brain that initiates all voluntary muscular movement, including those for respiration.
Voluntary respiration is any type of respiration that is under conscious control. Voluntary respiration is important for the higher functions that involve air supply, such as voice control or blowing out candles. Similar to how involuntary respiration’s lower functions are controlled by the lower brain, voluntary respiration’s higher functions are controlled by the upper brain, namely parts of the cerebral cortex.
The Motor Cortex
The primary motor cortex is the neural center for voluntary respiratory control. More broadly, the motor cortex is responsible for initiating any voluntary muscular movement.
The processes that drive its functions aren’t fully understood, but it works by sending signals to the spinal cord, which sends signals to the muscles it controls, such as the diaphragm and the accessory muscles for respiration. This neural pathway is called the ascending respiratory pathway.
Different parts of the cerebral cortex control different forms of voluntary respiration. Initiation of the voluntary contraction and relaxation of the internal and external intercostal muscles takes place in the superior portion of the primary motor cortex.
The center for diaphragm control is posterior to the location of thoracic control (within the superior portion of the primary motor cortex). The inferior portion of the primary motor cortex may be involved in controlled exhalation.
Activity has also been seen within the supplementary motor area and the premotor cortex during voluntary respiration. This is most likely due to the focus and mental preparation of the voluntary muscular movement that occurs when one decides to initiate that muscle movement.
Note that voluntary respiratory nerve signals in the ascending respiratory pathway can be overridden by chemoreceptor signals from involuntary respiration. Additionally, other structures may override voluntary respiratory signals, such as the activity of limbic center structures like the hypothalamus.
During periods of perceived danger or emotional stress, signals from the hypothalamus take over the respiratory signals and increase the respiratory rate to facilitate the fight or flight response.
Topography of the primary motor cortex: Topography of the primary motor cortex, on an outline drawing of the human brain. Each part of the primary motor cortex controls a different part of the body.
Nerves Used in Respiration
There are several nerves responsible for the muscular functions involved in respiration. There are three types of important respiratory nerves:
The phrenic nerves – The nerves that stimulate the activity of the diaphragm. They are composed of two nerves, the right and left phrenic nerve, which passes through the right and left side of the heart respectively. They are autonomic nerves.
The vagus nerve – Innervates the diaphragm as well as movements in the larynx and pharynx. It also provides parasympathetic stimulation for the heart and the digestive system. It is a major autonomic nerve.
The posterior thoracic nerves – These nerves stimulate the intercostal muscles located around the pleura. They are considered to be part of a larger group of intercostal nerves that stimulate regions across the thorax and abdomen. They are somatic nerves.
These three types of nerves continue the signal of the ascending respiratory pathway from the spinal cord to stimulate the muscles that perform the movements needed for respiration.
Damage to any of these three respiratory nerves can cause severe problems, such as diaphragm paralysis if the phrenic nerves are damaged. Less severe damage can cause irritation to the phrenic or vagus nerves, which can result in hiccups.
Chemoreceptor Regulation of Breathing
Chemoreceptors detect the levels of carbon dioxide in the blood by monitoring the concentrations of hydrogen ions in the blood.
Key Points
An increase in carbon dioxide concentration leads to a decrease in the pH of blood due to the production of H+ ions from carbonic acid.
In response to a decrease in blood pH, the respiratory center (in the medulla ) sends nervous impulses to the external intercostal muscles and the diaphragm, to increase the breathing rate and the volume of the lungs during inhalation.
Hyperventilation causes alakalosis, which causes a feedback response of decreased ventilation (to increase carbon dioxide), while hypoventilation causes acidosis, which causes a feedback response of increased ventilation (to remove carbon dioxide).
Any situation with hypoxia (too low oxygen levels) will cause a feedback response that increases ventilation to increase oxygen intake.
Vomiting causes alkalosis and diarrhea causes acidosis, which will cause an appropriate respiratory feedback response.
Key Terms
hypoxia: A system-wide deficiency in the levels of oxygen that reach the tissues.
central chemoreceptors: Located within the medulla, they are sensitive to the pH of their environment.
peripheral chemoreceptors: The aortic and carotid bodies, which act principally to detect variation of the oxygen concentration in the arterial blood, also monitor arterial carbon dioxide and pH.
Chemoreceptor regulation of breathing is a form of negative feedback. The goal of this system is to keep the pH of the bloodstream within normal neutral ranges, around 7.35.
Chemoreceptors
A chemoreceptor, also known as a chemosensor, is a sensory receptor that transduces a chemical signal into an action potential. The action potential is sent along nerve pathways to parts of the brain, which are the integrating centers for this type of feedback. There are many types of chemoreceptors in the body, but only a few of them are involved in respiration.
The respiratory chemoreceptors work by sensing the pH of their environment through the concentration of hydrogen ions. Because most carbon dioxide is converted to carbonic acid (and bicarbonate ) in the bloodstream, chemoreceptors are able to use blood pH as a way to measure the carbon dioxide levels of the bloodstream.
The main chemoreceptors involved in respiratory feedback are:
Central chemoreceptors: These are located on the ventrolateral surface of the medulla oblongata and detect changes in the pH of spinal fluid. They can be desensitized over time from chronic hypoxia (oxygen deficiency) and increased carbon dioxide.
Peripheral chemoreceptors: These include the aortic body, which detects changes in blood oxygen and carbon dioxide, but not pH, and the carotid body which detects all three. They do not desensitize and have less of an impact on the respiratory rate compared to the central chemoreceptors.
Chemoreceptor Negative Feedback
Negative feedback responses have three main components: the sensor, the integrating sensor, and the effector. For the respiratory rate, the chemoreceptors are the sensors for blood pH, the medulla and pons from the integrating center, and the respiratory muscles are the effector.
Consider a case in which a person is hyperventilating from an anxiety attack. Their increased ventilation rate will remove too much carbon dioxide from their body. Without that carbon dioxide, there will be less carbonic acid in the blood, so the concentration of hydrogen ions decreases and the pH of the blood rises, causing alkalosis.
In response, the chemoreceptors detect this change and send a signal to the medulla, which signals the respiratory muscles to decrease the ventilation rate so carbon dioxide levels and pH can return to normal levels.
There are several other examples in which chemoreceptor feedback applies. A person with severe diarrhea loses a lot of bicarbonate in the intestinal tract, which decreases bicarbonate levels in the plasma. As bicarbonate levels decrease while hydrogen ion concentrations stay the same, blood pH will decrease (as bicarbonate is a buffer) and become more acidic.
In cases of acidosis, feedback will increase ventilation to remove more carbon dioxide to reduce the hydrogen ion concentration. Conversely, vomiting removes hydrogen ions from the body (as the stomach contents are acidic), which will cause decreased ventilation to correct alkalosis.
Chemoreceptor feedback also adjusts for oxygen levels to prevent hypoxia, though only the peripheral chemoreceptors sense oxygen levels. In cases where oxygen intake is too low, feedback increases ventilation to increase oxygen intake.
A more detailed example would be that if a person breathes through a long tube (such as a snorkeling mask) and has increased amounts of dead space, feedback will increase ventilation.
Respiratory feedback: The chemoreceptors are the sensors for blood pH, the medulla and pons form the integrating center, and the respiratory muscles are the effector.
Proprioceptor Regulation of Breathing
The Hering–Breuer inflation reflex prevents overinflation of the lungs.
Key Points
Pulmonary stretch receptors present in the smooth muscle of the airways and the pleura respond to excessive stretching of the lung during large inspirations.
The Hering–Breuer inflation reflex is initiated by stimulation of
stretch receptors. The deflation reflex is initiated by stimulation
of the compression receptors (called proprioceptors) or deactivation of
stretch receptors when the lungs deflate.
Activation of the pulmonary stretch receptors (via the vagus nerve ) results in inhibition of the inspiratory stimlus in the medulla, and thus inhibition of inspiration and initiation of expiration.
An increase in pulmonary stretch receptor activity leads to an elevation of heart rate ( tachycardia ).
A cyclical, elevated heart rate from inspiration is called sinus arrhythmia and is a normal response in youth. Inhibition of inspiration is important to allow expiration to occur.
Key Terms
sinus arrhythmia: A normal cyclical heart rate change in which an increase in heart rate occurs during inspiration, but returns to normal during expiration.
pulmonary stretch receptors: A sensory receptor that sends an action potential when it detects pressure, tension, stretch, or distortion.
The lungs are a highly elastic organ capable of expanding to a much larger volume during inflation. While the volume of the lungs is proportional to the pressure of the pleural cavity as it expands and contracts during breathing, there is a risk of over-inflation of the lungs if inspiration becomes too deep for too long. Physiological mechanisms exist to prevent over-inflation of the lungs.
The Hering–Bauer Reflex
Cardiac and respiratory branches of the vagus nerve: The vagus nerve is the neural pathway for stretch receptor regulation of breathing.
The Hering–Breuer reflex (also called the inflation reflex) is triggered to prevent over-inflation of the lungs. There are many stretch receptors in the lungs, particularly within the pleura and the smooth muscles of the bronchi and bronchioles, that activate when the lungs have inflated to their ideal maximum point.
These stretch receptors are mechanoreceptors, which are a type of sensory receptor that specifically detects mechanical pressure, distortion, and stretch, and are found in many parts of the human body, especially the lungs, stomach, and skin. They do not detect fine-touch information like most sensory receptors in the human body, but they do create a feeling of tension or fullness when activated, especially in the lungs or stomach.
When the lungs are inflated to their maximum volume during inspiration, the pulmonary stretch receptors send an action potential signal to the medulla and pons in the brain through the vagus nerve.
The pneumatic center of the pons sends signals to inhibit the apneustic center of the pons, so it doesn’t activate the inspiratory area (the dorsal medulla), and the inspiratory signals that are sent to the diaphragm and accessory muscles stop. This is called the inflation reflex.
As inspiration stops, expiration begins and the lung begins to deflate. As the lungs deflate the stretch receptors are deactivated (and compression receptors called proprioceptors may be activated) so the inhibitory signals stop and inhalation can begin again—this is called the deflation reflex.
Early physiologists believed this reflex played a major role in establishing the rate and depth of breathing in humans. While this may be true for most animals, it is not the case for most adult humans at rest. However, the reflex may determine the breathing rate and depth in newborns and in adult humans when tidal volume is more than 1 L, such as when exercising.
Additionally, people with emphysema have an impaired Hering–Bauer reflex due to a loss of pulmonary stretch receptors from the destruction of lung tissue, so their lungs can over-inflate as well as collapse, which contributes to shortness of breath.
Sinus Arrhythmia
As the Hering–Bauer reflex uses the vagus nerve as its neural pathway, it also has a few cardiovascular system effects because the vagus nerve also innervates the heart.
During stretch receptor activation, the inhibitory signal that travels through the vagus nerve is also sent to the sinus-atrial node of the heart. Its stimulation causes a short-term increase in resting heart rate, which is called tachycardia.
The heart rate returns to normal during expiration when the stretch receptors are deactivated. When this process is cyclical it is called a sinus arrhythmia, which is a generally normal physiological phenomenon in which there is short-term tachycardia during inspiration.
Sinus arrhythmias do not occur in everyone and are more common in youth. The sensitivity of the sinus-atrial node to the inflation reflex is lost over time, so sinus arrhythmias are less common in older people.
Control of respiratory rhythm
Ventilatory pattern
Respiratory centre and its groups of neurons
Breathing is normally an unconscious, involuntary, automatic process. The pattern of motor stimuli during breathing can be divided into an inhalation stage and an exhalation stage. Inhalation shows a sudden, ramped increase in motor discharge to the respiratory muscles (and the pharyngeal constrictor muscles).[rx] Before the end of inhalation, there is a decline in, and end of motor discharge. Exhalation is usually silent, except at high respiratory rates.
The respiratory center in the medulla and pons of the brainstem controls the rate and depth of respiration, (the respiratory rhythm), through various inputs. These include signals from the peripheral chemoreceptors and central chemoreceptors; from the vagus nerve and glossopharyngeal nerve carrying input from the pulmonary stretch receptors, and other mechanoreceptors in the lungs.[rx][rx] as well as signals from the cerebral cortex and hypothalamus.
Medulla
ventral respiratory group (includes the pre-Bötzinger complex). The ventral respiratory group controls voluntarily forced exhalation and acts to increase the force of inhalation. Regulates rhythm of inhalation and exhalation.
dorsal respiratory group (solitary nucleus). The dorsal respiratory group controls mostly movements of inhalation and their timing.
Pons
pneumotaxic center.
Coordinates speed of inhalation and exhalation
Sends inhibitory impulses to the inspiratory area
Involved in fine-tuning of respiration rate.
apneustic center
Coordinates speed of inhalation and exhalation.
Sends stimulatory impulses to the inspiratory area – activates and prolongs inhalations
Overridden by pneumatic control from the apneustic area to end inhalation
Control of ventilatory pattern
Ventilation is normally unconscious and automatic but can be overridden by conscious alternative patterns.[rx] Thus the emotions can cause yawning, laughing, sighing (etc.), social communication causes speech, song, and whistling, while entirely voluntary overrides are used to blow out candles, and breath-holding (for instance, to swim underwater). Hyperventilation may be entirely voluntary or in response to emotional agitation or anxiety when it can cause the distressing hyperventilation syndrome. The voluntary control can also influence other functions such as the heart rate as in yoga practices and meditation.[rx]
The ventilatory pattern is also temporarily modified by complex reflexes such as sneezing, straining, burping, coughing and vomiting.
Determinants of ventilatory rate
Ventilatory rate (respiratory minute volume) is tightly controlled and determined primarily by blood levels of carbon dioxide as determined by metabolic rate. Blood levels of oxygen become important in hypoxia. These levels are sensed by central chemoreceptors on the surface of the medulla oblongata for increased pH (indirectly from the increase of carbon dioxide in cerebrospinal fluid), and the peripheral chemoreceptors in the arterial blood for oxygen and carbon dioxide. Afferent neurons from the peripheral chemoreceptors are via the glossopharyngeal nerve (CN IX) and the vagus nerve (CN X).
The concentration of CO2 rises in the blood when the metabolic use of O2, and the production of CO2 is increased during, for example, exercise. The CO2 in the blood is transported largely as bicarbonate (HCO3−) ions, by conversion first to carbonic acid (H2CO3), by the enzyme carbonic anhydrase, and then by disassociation of this acid to H+ and HCO3−. Build-up of CO2 therefore causes an equivalent build-up of the disassociated hydrogen ions, which, by definition, decreases the pH of the blood. The pH sensors on the brain stem immediately respond to this fall in pH, causing the respiratory center to increase the rate and depth of breathing. The consequence is that the partial pressure of CO2 (PCO2) does not change from rest going into exercise. During very short-term bouts of intense exercise the release of lactic acid into the blood by the exercising muscles causes a fall in the blood plasma pH, independently of the rise in the PCO2, and this will stimulate pulmonary ventilation sufficiently to keep the blood pH constant at the expense of a lowered PCO2.
Mechanical stimulation of the lungs can trigger certain reflexes as discovered in animal studies. In humans, these seem to be more important in neonates and ventilated patients, but of little relevance in health. The tone of respiratory muscle is believed to be modulated by muscle spindles via a reflex arc involving the spinal cord.
Drugs can greatly influence the rate of respiration. Opioids and anesthetics tend to depress ventilation, by decreasing the normal response to raised carbon dioxide levels in the arterial blood. Stimulants such as amphetamines can cause hyperventilation.
Pregnancy tends to increase ventilation (lowering plasma carbon dioxide tension below normal values). This is due to increased progesterone levels and results in enhanced gas exchange in the placenta.
Feedback control
Receptors play important roles in the regulation of respiration and include the central and peripheral chemoreceptors, and pulmonary stretch receptors, a type of mechanoreceptor.
Central chemoreceptors of the central nervous system, located on the ventrolateral medullary surface, are sensitive to the pH of their environment.[rx][rx]
Peripheral chemoreceptors act most importantly to detect variation of the PO2 in the arterial blood, in addition to detecting arterial PCO2 and pH.
Mechanoreceptors are located in the airways and parenchyma and are responsible for a variety of reflex responses. These include:
The Hering-Breuer reflex terminates inhalation to prevent overinflation of the lungs, and the reflex responses of coughing, airway constriction, and hyperventilation.
The upper airway receptors are responsible for reflex responses such as sneezing, coughing, closure of the glottis, and hiccups.
The spinal cord reflex responses include the activation of additional respiratory muscles as compensation, gasping response, hypoventilation, and an increase in breathing frequency and volume.
The nasopulmonary and mesothoracic reflexes regulate the mechanism of breathing through deepening the inhale. Triggered by the flow of the air, the pressure of the air in the nose, and the quality of the air, impulses from the nasal mucosa are transmitted by the trigeminal nerve to the respiratory center in the brainstem, and the generated response is transmitted to the bronchi, the intercostal muscles and the diaphragm.
Respiratory control its main function is to send signals to the muscles that control respiration to cause breathing to occur. The ventral respiratory group stimulates expiratory movements. The dorsal respiratory group stimulates inspiratory movements.
The control of ventilation refers to the physiological mechanisms involved in the control of breathing, which is the movement of air into and out of the lungs. Ventilation facilitates respiration. Respiration refers to the utilization of oxygen and balancing of carbon dioxide by the body as a whole, or by individual cells in cellular respiration.[rx]
The most important function of breathing is supplying of oxygen to the body and balancing the carbon dioxide levels. Under most conditions, the partial pressure of carbon dioxide (PCO2), or concentration of carbon dioxide, controls the respiratory rate.
Neural Mechanisms (Respiratory Center)
The medulla and the pons are involved in the regulation of the ventilatory pattern of respiration.
Key Points
The ventral respiratory group controls voluntarily forced exhalation and acts to increase the force of inspiration.
The dorsal respiratory group (nucleus tractus solitarius) controls mostly inspiratory movements and their timing.
Ventilatory rate (minute volume) is tightly controlled and determined primarily by blood levels of carbon dioxide as determined by metabolic rate.
Chemoreceptors can detect changes in blood pH that require changes in involuntary respiration to correct. The apneustic (stimulating) and pnuemotaxic (limiting) centers of the pons work together to control the rate of breathing.
The medulla sends signals to the muscles that initiate inspiration and expiration and controls nonrespiratory air movement reflexes, like coughing and sneezing.
Key Terms
respiratory control centers: The medulla sends signals to the muscles involved in breathing, and the pons control the rate of breathing.
chemoreceptors: These are receptors in the medulla and in the aortic and carotid bodies of the blood vessels that detect changes in blood pH and signal the medulla to correct those changes.
Involuntary respiration is any form of respiratory control that is not under direct, conscious control. Breathing is required to sustain life, so involuntary respiration allows it to happen when voluntary respiration is not possible, such as during sleep. Involuntary respiration also has metabolic functions that work even when a person is conscious.
The Respiratory Centers
Anatomy of the brainstem: The brainstem, which includes the pons and medulla.
Involuntary respiration is controlled by the respiratory centers of the upper brainstem (sometimes termed the lower brain, along with the cerebellum). This region of the brain controls many involuntary and metabolic functions besides the respiratory system, including certain aspects of cardiovascular function and involuntary muscle movements (in the cerebellum).
The respiratory centers contain chemoreceptors that detect pH levels in the blood and send signals to the respiratory centers of the brain to adjust the ventilation rate to change acidity by increasing or decreasing the removal of carbon dioxide (since carbon dioxide is linked to higher levels of hydrogen ions in the blood).
There are also peripheral chemoreceptors in other blood vessels that perform this function as well, which include the aortic and carotid bodies.
The Medulla
The medulla oblongata is the primary respiratory control center. Its main function is to send signals to the muscles that control respiration to cause breathing to occur. There are two regions in the medulla that control respiration:
The ventral respiratory group stimulates expiratory movements.
The dorsal respiratory group stimulates inspiratory movements.
The medulla also controls the reflexes for nonrespiratory air movements, such as coughing and sneezing reflexes, as well as other reflexes, like swallowing and vomiting.
The Pons
The pons is the other respiratory center and is located underneath the medulla. Its main function is to control the rate or speed of involuntary respiration. It has two main functional regions that perform this role:
The apneustic center sends signals for inspiration for long and deep breaths. It controls the intensity of breathing and is inhibited by the stretch receptors of the pulmonary muscles at a maximum depth of inspiration, or by signals from the pnuemotaxic center. It increases tidal volume.
The pnuemotaxic center sends signals to inhibit inspiration that allows it to finely control the respiratory rate. Its signals limit the activity of the phrenic nerve and inhibit the signals of the apneustic center. It decreases tidal volume.
The apneustic and pnuemotaxic centers work against each other together to control the respiratory rate.
Neural Mechanisms (Cortex)
The cerebral cortex of the brain controls voluntary respiration.
Key Points
The motor cortex within the cerebral cortex of the brain controls voluntary respiration (the ascending respiratory pathway).
Voluntary respiration may be overridden by aspects of involuntary respiration, such as chemoreceptor stimulus, and hypothalamus stress response.
The phrenic nerves, vagus nerves, and posterior thoracic nerves are the major nerves involved in respiration.
Voluntary respiration is needed to perform higher functions, such as voice control.
Key Terms
The Phrenic Nerves: A set of two nerves that brings nerve impulses from the spinal cord to the diaphragm.
primary motor cortex: The region in the brain that initiates all voluntary muscular movement, including those for respiration.
Voluntary respiration is any type of respiration that is under conscious control. Voluntary respiration is important for the higher functions that involve air supply, such as voice control or blowing out candles. Similar to how involuntary respiration’s lower functions are controlled by the lower brain, voluntary respiration’s higher functions are controlled by the upper brain, namely parts of the cerebral cortex.
The Motor Cortex
The primary motor cortex is the neural center for voluntary respiratory control. More broadly, the motor cortex is responsible for initiating any voluntary muscular movement.
The processes that drive its functions aren’t fully understood, but it works by sending signals to the spinal cord, which sends signals to the muscles it controls, such as the diaphragm and the accessory muscles for respiration. This neural pathway is called the ascending respiratory pathway.
Different parts of the cerebral cortex control different forms of voluntary respiration. Initiation of the voluntary contraction and relaxation of the internal and external intercostal muscles takes place in the superior portion of the primary motor cortex.
The center for diaphragm control is posterior to the location of thoracic control (within the superior portion of the primary motor cortex). The inferior portion of the primary motor cortex may be involved in controlled exhalation.
Activity has also been seen within the supplementary motor area and the premotor cortex during voluntary respiration. This is most likely due to the focus and mental preparation of the voluntary muscular movement that occurs when one decides to initiate that muscle movement.
Note that voluntary respiratory nerve signals in the ascending respiratory pathway can be overridden by chemoreceptor signals from involuntary respiration. Additionally, other structures may override voluntary respiratory signals, such as the activity of limbic center structures like the hypothalamus.
During periods of perceived danger or emotional stress, signals from the hypothalamus take over the respiratory signals and increase the respiratory rate to facilitate the fight or flight response.
Topography of the primary motor cortex: Topography of the primary motor cortex, on an outline drawing of the human brain. Each part of the primary motor cortex controls a different part of the body.
Nerves Used in Respiration
There are several nerves responsible for the muscular functions involved in respiration. There are three types of important respiratory nerves:
The phrenic nerves – The nerves that stimulate the activity of the diaphragm. They are composed of two nerves, the right and left phrenic nerve, which passes through the right and left side of the heart respectively. They are autonomic nerves.
The vagus nerve – Innervates the diaphragm as well as movements in the larynx and pharynx. It also provides parasympathetic stimulation for the heart and the digestive system. It is a major autonomic nerve.
The posterior thoracic nerves – These nerves stimulate the intercostal muscles located around the pleura. They are considered to be part of a larger group of intercostal nerves that stimulate regions across the thorax and abdomen. They are somatic nerves.
These three types of nerves continue the signal of the ascending respiratory pathway from the spinal cord to stimulate the muscles that perform the movements needed for respiration.
Damage to any of these three respiratory nerves can cause severe problems, such as diaphragm paralysis if the phrenic nerves are damaged. Less severe damage can cause irritation to the phrenic or vagus nerves, which can result in hiccups.
Chemoreceptor Regulation of Breathing
Chemoreceptors detect the levels of carbon dioxide in the blood by monitoring the concentrations of hydrogen ions in the blood.
Key Points
An increase in carbon dioxide concentration leads to a decrease in the pH of blood due to the production of H+ ions from carbonic acid.
In response to a decrease in blood pH, the respiratory center (in the medulla ) sends nervous impulses to the external intercostal muscles and the diaphragm, to increase the breathing rate and the volume of the lungs during inhalation.
Hyperventilation causes alakalosis, which causes a feedback response of decreased ventilation (to increase carbon dioxide), while hypoventilation causes acidosis, which causes a feedback response of increased ventilation (to remove carbon dioxide).
Any situation with hypoxia (too low oxygen levels) will cause a feedback response that increases ventilation to increase oxygen intake.
Vomiting causes alkalosis and diarrhea causes acidosis, which will cause an appropriate respiratory feedback response.
Key Terms
hypoxia: A system-wide deficiency in the levels of oxygen that reach the tissues.
central chemoreceptors: Located within the medulla, they are sensitive to the pH of their environment.
peripheral chemoreceptors: The aortic and carotid bodies, which act principally to detect variation of the oxygen concentration in the arterial blood, also monitor arterial carbon dioxide and pH.
Chemoreceptor regulation of breathing is a form of negative feedback. The goal of this system is to keep the pH of the bloodstream within normal neutral ranges, around 7.35.
Chemoreceptors
A chemoreceptor, also known as a chemosensor, is a sensory receptor that transduces a chemical signal into an action potential. The action potential is sent along nerve pathways to parts of the brain, which are the integrating centers for this type of feedback. There are many types of chemoreceptors in the body, but only a few of them are involved in respiration.
The respiratory chemoreceptors work by sensing the pH of their environment through the concentration of hydrogen ions. Because most carbon dioxide is converted to carbonic acid (and bicarbonate ) in the bloodstream, chemoreceptors are able to use blood pH as a way to measure the carbon dioxide levels of the bloodstream.
The main chemoreceptors involved in respiratory feedback are:
Central chemoreceptors: These are located on the ventrolateral surface of the medulla oblongata and detect changes in the pH of spinal fluid. They can be desensitized over time from chronic hypoxia (oxygen deficiency) and increased carbon dioxide.
Peripheral chemoreceptors: These include the aortic body, which detects changes in blood oxygen and carbon dioxide, but not pH, and the carotid body which detects all three. They do not desensitize and have less of an impact on the respiratory rate compared to the central chemoreceptors.
Chemoreceptor Negative Feedback
Negative feedback responses have three main components: the sensor, the integrating sensor, and the effector. For the respiratory rate, the chemoreceptors are the sensors for blood pH, the medulla and pons from the integrating center, and the respiratory muscles are the effector.
Consider a case in which a person is hyperventilating from an anxiety attack. Their increased ventilation rate will remove too much carbon dioxide from their body. Without that carbon dioxide, there will be less carbonic acid in the blood, so the concentration of hydrogen ions decreases and the pH of the blood rises, causing alkalosis.
In response, the chemoreceptors detect this change and send a signal to the medulla, which signals the respiratory muscles to decrease the ventilation rate so carbon dioxide levels and pH can return to normal levels.
There are several other examples in which chemoreceptor feedback applies. A person with severe diarrhea loses a lot of bicarbonate in the intestinal tract, which decreases bicarbonate levels in the plasma. As bicarbonate levels decrease while hydrogen ion concentrations stay the same, blood pH will decrease (as bicarbonate is a buffer) and become more acidic.
In cases of acidosis, feedback will increase ventilation to remove more carbon dioxide to reduce the hydrogen ion concentration. Conversely, vomiting removes hydrogen ions from the body (as the stomach contents are acidic), which will cause decreased ventilation to correct alkalosis.
Chemoreceptor feedback also adjusts for oxygen levels to prevent hypoxia, though only the peripheral chemoreceptors sense oxygen levels. In cases where oxygen intake is too low, feedback increases ventilation to increase oxygen intake.
A more detailed example would be that if a person breathes through a long tube (such as a snorkeling mask) and has increased amounts of dead space, feedback will increase ventilation.
Respiratory feedback: The chemoreceptors are the sensors for blood pH, the medulla and pons form the integrating center, and the respiratory muscles are the effector.
Proprioceptor Regulation of Breathing
The Hering–Breuer inflation reflex prevents overinflation of the lungs.
Key Points
Pulmonary stretch receptors present in the smooth muscle of the airways and the pleura respond to excessive stretching of the lung during large inspirations.
The Hering–Breuer inflation reflex is initiated by stimulation of
stretch receptors. The deflation reflex is initiated by stimulation
of the compression receptors (called proprioceptors) or deactivation of
stretch receptors when the lungs deflate.
Activation of the pulmonary stretch receptors (via the vagus nerve ) results in inhibition of the inspiratory stimlus in the medulla, and thus inhibition of inspiration and initiation of expiration.
An increase in pulmonary stretch receptor activity leads to an elevation of heart rate ( tachycardia ).
A cyclical, elevated heart rate from inspiration is called sinus arrhythmia and is a normal response in youth. Inhibition of inspiration is important to allow expiration to occur.
Key Terms
sinus arrhythmia: A normal cyclical heart rate change in which an increase in heart rate occurs during inspiration, but returns to normal during expiration.
pulmonary stretch receptors: A sensory receptor that sends an action potential when it detects pressure, tension, stretch, or distortion.
The lungs are a highly elastic organ capable of expanding to a much larger volume during inflation. While the volume of the lungs is proportional to the pressure of the pleural cavity as it expands and contracts during breathing, there is a risk of over-inflation of the lungs if inspiration becomes too deep for too long. Physiological mechanisms exist to prevent over-inflation of the lungs.
The Hering–Bauer Reflex
Cardiac and respiratory branches of the vagus nerve: The vagus nerve is the neural pathway for stretch receptor regulation of breathing.
The Hering–Breuer reflex (also called the inflation reflex) is triggered to prevent over-inflation of the lungs. There are many stretch receptors in the lungs, particularly within the pleura and the smooth muscles of the bronchi and bronchioles, that activate when the lungs have inflated to their ideal maximum point.
These stretch receptors are mechanoreceptors, which are a type of sensory receptor that specifically detects mechanical pressure, distortion, and stretch, and are found in many parts of the human body, especially the lungs, stomach, and skin. They do not detect fine-touch information like most sensory receptors in the human body, but they do create a feeling of tension or fullness when activated, especially in the lungs or stomach.
When the lungs are inflated to their maximum volume during inspiration, the pulmonary stretch receptors send an action potential signal to the medulla and pons in the brain through the vagus nerve.
The pneumatic center of the pons sends signals to inhibit the apneustic center of the pons, so it doesn’t activate the inspiratory area (the dorsal medulla), and the inspiratory signals that are sent to the diaphragm and accessory muscles stop. This is called the inflation reflex.
As inspiration stops, expiration begins and the lung begins to deflate. As the lungs deflate the stretch receptors are deactivated (and compression receptors called proprioceptors may be activated) so the inhibitory signals stop and inhalation can begin again—this is called the deflation reflex.
Early physiologists believed this reflex played a major role in establishing the rate and depth of breathing in humans. While this may be true for most animals, it is not the case for most adult humans at rest. However, the reflex may determine the breathing rate and depth in newborns and in adult humans when tidal volume is more than 1 L, such as when exercising.
Additionally, people with emphysema have an impaired Hering–Bauer reflex due to a loss of pulmonary stretch receptors from the destruction of lung tissue, so their lungs can over-inflate as well as collapse, which contributes to shortness of breath.
Sinus Arrhythmia
As the Hering–Bauer reflex uses the vagus nerve as its neural pathway, it also has a few cardiovascular system effects because the vagus nerve also innervates the heart.
During stretch receptor activation, the inhibitory signal that travels through the vagus nerve is also sent to the sinus-atrial node of the heart. Its stimulation causes a short-term increase in resting heart rate, which is called tachycardia.
The heart rate returns to normal during expiration when the stretch receptors are deactivated. When this process is cyclical it is called a sinus arrhythmia, which is a generally normal physiological phenomenon in which there is short-term tachycardia during inspiration.
Sinus arrhythmias do not occur in everyone and are more common in youth. The sensitivity of the sinus-atrial node to the inflation reflex is lost over time, so sinus arrhythmias are less common in older people.
Control of respiratory rhythm
Ventilatory pattern
Respiratory centre and its groups of neurons
Breathing is normally an unconscious, involuntary, automatic process. The pattern of motor stimuli during breathing can be divided into an inhalation stage and an exhalation stage. Inhalation shows a sudden, ramped increase in motor discharge to the respiratory muscles (and the pharyngeal constrictor muscles).[rx] Before the end of inhalation, there is a decline in, and end of motor discharge. Exhalation is usually silent, except at high respiratory rates.
The respiratory center in the medulla and pons of the brainstem controls the rate and depth of respiration, (the respiratory rhythm), through various inputs. These include signals from the peripheral chemoreceptors and central chemoreceptors; from the vagus nerve and glossopharyngeal nerve carrying input from the pulmonary stretch receptors, and other mechanoreceptors in the lungs.[rx][rx] as well as signals from the cerebral cortex and hypothalamus.
Medulla
ventral respiratory group (includes the pre-Bötzinger complex). The ventral respiratory group controls voluntary forced exhalation and acts to increase the force of inhalation. Regulates rhythm of inhalation and exhalation.
dorsal respiratory group (solitary nucleus). The dorsal respiratory group controls mostly movements of inhalation and their timing.
Pons
pneumotaxic center.
Coordinates speed of inhalation and exhalation
Sends inhibitory impulses to the inspiratory area
Involved in fine-tuning of respiration rate.
apneustic center
Coordinates speed of inhalation and exhalation.
Sends stimulatory impulses to the inspiratory area – activates and prolongs inhalations
Overridden by pneumatic control from the apneustic area to end inhalation
Control of ventilatory pattern
Ventilation is normally unconscious and automatic but can be overridden by conscious alternative patterns.[rx] Thus the emotions can cause yawning, laughing, sighing (etc.), social communication causes speech, song, and whistling, while entirely voluntary overrides are used to blow out candles, and breath-holding (for instance, to swim underwater). Hyperventilation may be entirely voluntary or in response to emotional agitation or anxiety when it can cause the distressing hyperventilation syndrome. The voluntary control can also influence other functions such as the heart rate as in yoga practices and meditation.[rx]
The ventilatory pattern is also temporarily modified by complex reflexes such as sneezing, straining, burping, coughing and vomiting.
Determinants of ventilatory rate
Ventilatory rate (respiratory minute volume) is tightly controlled and determined primarily by blood levels of carbon dioxide as determined by metabolic rate. Blood levels of oxygen become important in hypoxia. These levels are sensed by central chemoreceptors on the surface of the medulla oblongata for increased pH (indirectly from the increase of carbon dioxide in cerebrospinal fluid), and the peripheral chemoreceptors in the arterial blood for oxygen and carbon dioxide. Afferent neurons from the peripheral chemoreceptors are via the glossopharyngeal nerve (CN IX) and the vagus nerve (CN X).
The concentration of CO2 rises in the blood when the metabolic use of O2, and the production of CO2 is increased during, for example, exercise. The CO2 in the blood is transported largely as bicarbonate (HCO3−) ions, by conversion first to carbonic acid (H2CO3), by the enzyme carbonic anhydrase, and then by disassociation of this acid to H+ and HCO3−. Build-up of CO2 therefore causes an equivalent build-up of the disassociated hydrogen ions, which, by definition, decreases the pH of the blood. The pH sensors on the brain stem immediately respond to this fall in pH, causing the respiratory center to increase the rate and depth of breathing. The consequence is that the partial pressure of CO2 (PCO2) does not change from rest going into exercise. During very short-term bouts of intense exercise the release of lactic acid into the blood by the exercising muscles causes a fall in the blood plasma pH, independently of the rise in the PCO2, and this will stimulate pulmonary ventilation sufficiently to keep the blood pH constant at the expense of a lowered PCO2.
Mechanical stimulation of the lungs can trigger certain reflexes as discovered in animal studies. In humans, these seem to be more important in neonates and ventilated patients, but of little relevance in health. The tone of respiratory muscle is believed to be modulated by muscle spindles via a reflex arc involving the spinal cord.
Drugs can greatly influence the rate of respiration. Opioids and anesthetics tend to depress ventilation, by decreasing the normal response to raised carbon dioxide levels in the arterial blood. Stimulants such as amphetamines can cause hyperventilation.
Pregnancy tends to increase ventilation (lowering plasma carbon dioxide tension below normal values). This is due to increased progesterone levels and results in enhanced gas exchange in the placenta.
Feedback control
Receptors play important roles in the regulation of respiration and include the central and peripheral chemoreceptors, and pulmonary stretch receptors, a type of mechanoreceptor.
Central chemoreceptors of the central nervous system, located on the ventrolateral medullary surface, are sensitive to the pH of their environment.[rx][rx]
Peripheral chemoreceptors act most importantly to detect variation of the PO2 in the arterial blood, in addition to detecting arterial PCO2 and pH.
Mechanoreceptors are located in the airways and parenchyma and are responsible for a variety of reflex responses. These include:
The Hering-Breuer reflex terminates inhalation to prevent overinflation of the lungs, and the reflex responses of coughing, airway constriction, and hyperventilation.
The upper airway receptors are responsible for reflex responses such as sneezing, coughing, closure of the glottis, and hiccups.
The spinal cord reflex responses include the activation of additional respiratory muscles as compensation, gasping response, hypoventilation, and an increase in breathing frequency and volume.
The nasopulmonary and mesothoracic reflexes regulate the mechanism of breathing through deepening the inhale. Triggered by the flow of the air, the pressure of the air in the nose, and the quality of the air, impulses from the nasal mucosa are transmitted by the trigeminal nerve to the respiratory center in the brainstem, and the generated response is transmitted to the bronchi, the intercostal muscles and the diaphragm.
Exchanging Oxygen and Carbon Dioxide/Gas exchange is the process by which oxygen and carbon dioxide move between the bloodstream and the lungs. This is the primary function of the respiratory system and is essential for ensuring a constant supply of oxygen to tissues, as well as removing carbon dioxide to prevent its accumulation.
In the original sense of the Latin word, “respiration” means repeated inhaling and exhaling of air with the associated movements of the thorax. Respiratory movements produce an airflow for the transport of O2 into the lungs, and of CO2, the end product of oxidative metabolism, out of the lungs. But respiration in today’s meaning includes all the processes involved in the transport of O2 and CO2 between the environment and body tissues, performed by pulmonary ventilation, pulmonary O2 and CO2 exchange, blood circulation, and O2 and CO2 exchange in tissues. Gas exchange in tissues is intimately related to the consumption of O2 and production of CO2 by oxidative tissue metabolism whose main purpose is the provision of energy for life processes
External Respiration
Respiration is the transport of oxygen to the cells within tissues and the transport of carbon dioxide in the opposite direction.
Key Points
External respiration describes the exchange of gasses between the external environment and the bloodstream.
The components of external respiration include alveolar surface area, ventilation and perfusion matching, and partial pressure gradients.
Partial pressure gradients allow gasses to flow from areas of high pressure to areas of lower pressure.
Ventilation and perfusion in the alveoli must be balanced to maintain efficient gas exchange.
Key Terms
passive diffusion: The net movement of material from an area of high concentration to an area of lower concentration without any energy input.
perfusion: The blood supply to the alveolar capillaries that must be balanced with ventilation.
Equilibrium: The rate of change of the gasses in the alveoli and capillary become equal to eachother at the end of gas exchange.
External Respiration
External respiration is the formal term for gas exchange. It describes both the bulk flow of air into and out of the lungs and the transfer of oxygen and carbon dioxide into the bloodstream through diffusion. While the bulk flow of air from the external environment happens due to pressure changes in the lungs, the mechanisms of alveolar gas exchange are more complicated. The primary three components of external respiration are the surface area of the alveolar membrane, the partial pressure gradients of the gasses, and the matching of perfusion and ventilation.
Surface Area
The alveoli have a very high surface area to volume ratio that allows for efficient gas exchange. The alveoli are covered with a high density of capillaries that provide many sites for gas exchange.
The walls of the alveolar membrane are thin and covered with a fluid, extra-cellular matrix that provides a surface for gas molecules in the air of the lungs to diffuse into, from which they can then diffuse into the capillaries.
Partial Pressure Gradients
Partial pressure gradients (differences in partial pressure) allow the loading of oxygen into the bloodstream and the unloading of carbon dioxide out of the bloodstream. These two processes occur at the same time.
Gas exchange in the alveolus: External respiration is a result of partial pressure gradients, alveolar surface area, and ventilation and perfusion matching.
Oxygen has a partial pressure gradient of about 60 mmHg (100 mmHg in alveolar air and 40 mmHg in deoxygenated blood ) and diffuses rapidly from the alveolar air into the capillary.
Equilibrium between the alveolar air and capillaries is reached quickly, within the first third of the length of the capillary within a third of a second. The partial pressure of oxygen in the oxygenated blood of the capillary after oxygen loading is about 100 mmHg.
The process is similar in carbon dioxide. The partial pressure gradient for carbon dioxide is much smaller compared to oxygen, being only 5 mmHg (45 mmHg in deoxygenated blood and 40 mmHg in alveolar air).
Based on Henry’s law, the greater solubility of carbon dioxide in blood compared to oxygen means that diffusion will still occur very rapidly despite the lower partial pressure gradient. Equilibrium between the alveolar air and the capillaries for carbon dioxide is reached within the first half of the length of the capillaries within half a second. The partial pressure of carbon dioxide in the blood leaving the capillaries is 40 mmHg.
Ventilation and Perfusion Matching
The exchange of gas and blood supply to the lungs must be balanced in order to facilitate efficient external respiration. While a severe ventilation-perfusion mismatch indicates severe lung disease, minor imbalances can be corrected by maintaining air flow that is proportional to capillary blood flow, which maintains the balance of ventilation and perfusion.
Perfusion in the capillaries adjusts to changes in PAO2. Constriction in the airways (such as from the bronchospasms in an asthma attack) lead to decreased PAO2 because the flow of air into the lungs is slowed.
In response, the arteries being supplied by the constricted airway undergo vasoconstriction, reducing the flow of blood into those alveoli so that the perfusion doesn’t become much greater relative to the decreased ventilation (a type of ventilation-perfusion mismatch called a shunt).
Alternatively, breathing in higher concentrations of oxygen from an oxygen tank will cause vasodilation and increased blood perfusion in the capillaries.
Ventilation adjusts from changes in PACO2. When airflow becomes higher relative to perfusion, PACO2 decreases, so the bronchioles will constrict in order to maintain to the balance between airflow (ventilation) and perfusion. When airflow is reduced, PACO2 increases, so the bronchioles will dilate in order to maintain the balance.
Internal Respiration
Cellular respiration is the metabolic process by which an organism obtains energy through the reaction of oxygen with glucose.
Key Points
Cellular respiration is the metabolic process by which an organism obtains energy by reacting oxygen with glucose to give water, carbon dioxide, and adenosine triphosphate (energy).
The 3 steps of cellular respiration are glycolysis, the Krebs cycle, and oxidative phosphorylation.
Carbon dioxide is a waste product of cellular respiration that comes from the carbon in glucose and the oxygen used in cellular respiration.
Internal respiration involves gas exchange between the bloodstream and tissues, and cellular respiration.
Gas exchange in tissues is a result of tissue surface area, gas partial pressure gradients, and the blood perfusion of those tissues.
Key Terms
Cellular respiration: The cellular process of producing adenosine triphosphate (ATP), water, and carbon dioxide from glucose and oxygen.
Oxidative Phosphorylation: The final step of cellular phosphorylation in which oxygen is used to a create an electron transport chain that produces a large amount of ATP from nicotinamide adenine dinucleotide (NADH).
Internal respiration refers to two distinct processes. The first is the exchange of gasses between the bloodstream and the tissues. The second is the process of cellular respiration, from which cells utilize oxygen to perform basic metabolic functions.
Gas Exchange with Tissues
Gas exchange occurs in the alveoli so that oxygen is loaded into the bloodstream and carbon dioxide is unloaded from the bloodstream. Afterward, oxygen is brought to the left side of the heart via the pulmonary vein, which pumps it into the systemic circulation.
Red blood cells carry the oxygen into the capillaries of the tissues of the body. Oxygen diffuses into the cells of the tissues, while carbon dioxide diffuses out of the cells of the tissues and into the bloodstream.
The factors that influence tissue gas exchange are similar to the factors of alveolar gas exchange, and include partial pressure gradients between the blood and the tissues, the blood perfusion of those tissues, and the surface areas of those tissues. Each of those factors generally increase gas exchange as those factors are increased (i.e., more oxygen diffusion in tissues with more blood perfusion).
Regarding the partial pressure gradients in systemic capillaries, they have a PaO2 of 100mmHg and a PaCO2 of 40mmHG within the capillary and a PaO2 of 40 mmHg and PaCO2 of 45 mmHg inside issue cells, which allows gas exchange to occur.
Cellular Respiration
Cellular respiration is the metabolic process by which an organism obtains energy through the reaction of oxygen with glucose to produce water, carbon dioxide and ATP, which is the functional source of energy for the cell. The oxygen supply for cellular respiration comes from the external respiration of the respiratory system.
Overview of cellular respiration: A diagram of cellular respiration including glycolysis, the Krebs cycle (also called the citric acid cycle), and the electron transport chain.
Cellular respiration includes three major steps, and occurs mainly in the cytoplasm of the cell and within the mitochondria of the cell. The net formula for cellular respiration is:
Glycolysis: The breakdown of glucose into pyruvate, ATP, H2O, and heat.
Krebs Cycle: Produces NADH from pyruvate.
Oxidative Phosphorylation: Produces ATP from NADH, oxygen, and H+. The oxygen plays the role of electron receptor in an electron transport chain to produce ATP.
The carbon dioxide waste is the result of the carbon from glucose (C6H12O6) being broken down to produce the pyruvate and NADH intermediates needed to produce ATP at the end of respiration. The energy stored in ATP can then be used to drive processes that require energy, including biosynthesis, locomotion, or transportation of molecules across cell membranes.
Cellular respiration can occur anaerobically without oxygen, such as through lactic acid fermentation. Human cells may use lactic acid fermentation in muscle tissue during strenuous exercise when there isn’t enough oxygen to power the tissues. This process is very inefficient compared to aerobic respiration, as without oxidative phosphorylation, the cell cannot produce nearly as much ATP (2 ATP compared to 38 during cellular respiration).
Oxygen Transport
Hemoglobin is the primary transporter of oxygen with an oxygen binding capacity between 1.36 and 1.37 ml O2 per gram Hgb.
Key Points
About 98.5% of the oxygen in a sample of arterial blood in a healthy human breathing air at sea-level pressure is bound to the hemoglobin in blood.
Each molecule of hemoglobin is made up of four heme groups.
The oxygen dissociation curve shows the amount of oxygen saturated in hemoglobin for a given partial pressure of oxygen.
The curve shifts right when oxygen’s affinity for binding to hemoglobin is decreased, and shifts left when its affinity for binding is increased.
A rightward shift occurs during exercise, decreasing blood pH and increasing temperature, or during anemia (with a downward shift as well).
A leftward shift occurs during increased blood pH, decreased temperature, or carbon monoxide exposure.
Key Terms
hemoglobin: A protein found in red blood cells that provides a binding site for oxygen to transport it to the tissues of the body.
dissociation curve: The oxygen–hemoglobin dissociation curve plots the proportion of hemoglobin saturated with oxygen on the vertical axis against the partial pressure of oxygen on the horizontal axis.
Hemoglobin
About 98.5% of the oxygen in a sample of arterial blood in a healthy human breathing air at sea-level pressure is bound to the hemoglobin in blood (Hgb). Hemoglobin is a protein found in red blood cells (also called erythrocytes).
There are roughly 270 million hemoglobin molecules in a single red blood cell, and each contains 4 heme groups. The function of Hgb is to provide a binding site for oxygen to carry oxygen throughout the bloodstream to the systemic tissues for cellular respiration.
Hemoglobin: Hemoglobin is the iron-containing, oxygen-transport metalloprotein in the red blood cells of all vertebrates.
About 1.5% of oxygen is physically dissolved in the other blood liquids and not connected to Hgb. It has an oxygen binding capacity between 1.36 and 1.37 ml O2 per gram Hgb.
Oxyhemoglobin Dissociation Curve
The percentage of oxygen that is saturated in the hemoglobin of blood is generally represented by a curve that shows the relationship between PaO2 and O2 saturation. The saturation of O2 in hemoglobin is an indicator of how much O2 is able to reach the tissues of the body.
Higher PaO2 means higher saturation of oxygen in the blood. Under normal conditions the PaO2 in systemic blood is equal to 50%, about 26.6 mmHg,; this is called the P50.
The curve starts to plateau at PaO2 higher than 60 mmHg, meaning that increases in PaO2 after that point won’t significantly increase saturation. This also means that the approximate carrying capacity for oxygen in hemoglobin has been reached and excess oxygen won’t go into hemoglobin.
The carrying capacity can be increased if more hemoglobin is added to the system, such as through greater red blood cell generation in high altitudes, or from blood transfusions. The lower areas of the curve show saturation when oxygen is unloaded into the tissues.
The oxyhemoglobin dissociation curve: The oxygen–hemoglobin dissociation curve plots the percent hemoglobin saturation (y-axis) against the partial pressure of oxygen in the blood (PO2). The blue curve is a standard curve, while the red and green curves are right and leftward shifts respectively.
The oxyhemoglobin dissociation curve can shift in response to a variety of factors. A change in the P50 of the curve is a sign that the dissociation curve as a whole has shifted. Shifts indicate a change in affinity for oxygen’s binding to hemoglobin, which changes the ability of oxygen to bind to hemoglobin and stay bound to it (i.e., not be released from it).
Rightward shifts indicate a decreased affinity for the binding of hemoglobin so that less oxygen binds to hemoglobin, and more oxygen is unloaded from it into the tissues. The curve shifts right during decreased blood pH (called the Bohr effect), increased temperature, and during exercise among other things.
Anemia (a disorder marked by a decreased red blood cell count and less hemoglobin) also causes a rightward shift but also changes the shape of the curve so that it moves downward as well as a result of the reduced levels of hemoglobin.
Leftward shifts indicate an increased affinity for the binding of hemoglobin so that more oxygen binds to hemoglobin, but less oxygen is unloaded from it into the tissues. Causes of leftward shifts include increased blood pH, decreased temperature, and carbon monoxide exposure. Carbon monoxide binds to hemoglobin in place of oxygen, so that less oxygen reaches the tissues; this can be fatal if severe enough.
Carbon Dioxide Transport
CO2 is carried in blood in three different ways: dissolved in plasma, bound to hemoglobin, or as a bicarbonate ion.
Key Points
Carbon dioxide is transported through the bloodstream either dissolved in the blood, bound the hemoglobin, or converted to bicarbonate ions.
The Haldane effect is the decreased binding of carbon dioxide in hemoglobin due to increased oxygen levels and increased binding of carbon dioxide to hemoglobin from decreased oxygen levels.
CO2 + H2O → H2CO3 → H+ + HCO3− is the bicarbonate formation reaction in the plasma.
Increased carbon dioxide means increased blood acidity, while decreased carbon dioxide means increased blood acidity.
The bicarbonate reaction is reversible, which allows bicarbonate to turn back into dissolved carbon dioxide to diffuse from the alveolus.
Key Terms
red blood cell: A type of cell in the blood of vertebrates that contains hemoglobin and transports oxygen from the lungs to the tissues; an erythrocyte.
Bicarbonate: A negatively charged ion that accumulates in plasma when carbon dioxide dissolves in water and reacts with it. It also acts as a buffer for blood pH.
carbonic anhydrase: An enzyme that catalyzes the bicarbonate reaction in either direction.
Carbon Dioxide Transport
Carbon dioxide is the product of cellular respiration and is transported from the cells of tissues in the body to the alveoli of the lungs through the bloodstream. Carbon dioxide is carried in the blood in three different ways.
Dissolved in the Plasma
About 5% of carbon dioxide is transported in the plasma of the blood as dissolved CO2 molecules that aren’t bound to anything else. Carbon dioxide has a much higher solubility than oxygen, which explains why a relatively greater amount of carbon dioxide is dissolved in the plasma compared to oxygen.
Bound to Hemoglobin
Structure of human hemoglobin: Hemoglobin is a tetramer of alpha (red) and beta (blue) subunits with iron containing heme groups (green).
While oxygen binds to the iron content in the heme of hemoglobin, carbon dioxide can bind to the amino acid chains on hemoglobin. When carbon dioxide clings to hemoglobin it forms carbanimohemoglobin.
About 10% of carbon dioxide in the human body is transported this way. Carbanimohemoglobin gives red blood cells a bluish color, which is one of the reasons why the veins that carry deoxygenated blood appear to be blue.
A property of hemoglobin called the Haldane effect states that deoxygenated blood has an increased capacity to carry carbon dioxide, while oxygenated blood has a decreased capacity to carry carbon dioxide.
This property means that hemoglobin will primarily carry oxygen in systemic circulation until it unloads that oxygen and is able to carry a relatively higher amount of carbon dioxide. This is due to deoxygenated blood’s increased capacity to carry carbon dioxide, and from the carbon dioxide loaded from the tissues during tissue gas exchange.
Bicarbonate Ions
The majority (85%) of carbon dioxide travels in the bloodstream as bicarbonate ions. The reaction that describes the formation of bicarbonate ions in the blood is:
CO2 + H2O → H2CO3 → H+ + HCO3–
This means that carbon dioxide reacts with water to form carbonic acid, which dissociates in solution to form hydrogen ions and bicarbonate ions.
The main implication of this process is that the pH of blood becomes a way of determining the amount of carbon dioxide in the blood. This is because if carbon dioxide increases in the body, it will manifest as increased concentrations of bicarbonate and increased concentrations of hydrogen ions that reduce blood pH and make the blood more acidic.
Conversely, if carbon dioxide levels are reduced, there will be less bicarbonate and fewer hydrogen ions dissolved in the blood, so pH will increase and blood will become more basic. Bicarbonate ions act as a buffer for the pH of blood so that blood pH will be neutral as long as bicarbonate and hydrogen ions are balanced.
This connection explains how ventilation rate and blood chemistry are related, as hyperventilation will cause alkalosis, and hypoventilation will cause acidosis, due to the changes in carbon dioxide levels that they cause.
Bicarbonate is also carried in the fluids of tissues besides the blood vessels, especially in the duodenum and intestine, so problems in those organs can cause a respiratory system response.
Transport to the Alveoli
After carbon dioxide travels through the bloodstream to the capillaries covering the alveoli of the lungs through any of the 3 methods listed above, it must return to dissolved carbon dioxide form in order to diffuse across the capillary into the alveolus. Dissolved carbon dioxide is already able to diffuse into the alveolus, while hemoglobin-bound carbon dioxide is unloaded into the plasma.
For carbon dioxide stored in bicarbonate, it undergoes a reaction reversal. Bicarbonate ions dissolved in the plasma enter the red blood cells by diffusing across a chloride ion gradient (replacing chloride inside the cell), and combining with hydrogen to form carbonic acid.
Next, the action of carbonic anhydrase breaks carbonic acid down into carbon dioxide in water, which leaves the cell by diffusion. The dissolved carbon dioxide is then able to diffuse into the alveolus.
Gas exchange is the process by which oxygen and carbon dioxide move between the bloodstream and the lungs. This is the primary function of the respiratory system and is essential for ensuring a constant supply of oxygen to tissues, as well as removing carbon dioxide to prevent its accumulation.
In the original sense of the Latin word, “respiration” means repeated inhaling and exhaling of air with the associated movements of the thorax. Respiratory movements produce an airflow for the transport of O2 into the lungs, and of CO2, the end product of oxidative metabolism, out of the lungs. But respiration in today’s meaning includes all the processes involved in the transport of O2 and CO2 between the environment and body tissues, performed by pulmonary ventilation, pulmonary O2 and CO2 exchange, blood circulation, and O2 and CO2 exchange in tissues. Gas exchange in tissues is intimately related to the consumption of O2 and production of CO2 by oxidative tissue metabolism whose main purpose is the provision of energy for life processes
External Respiration
Respiration is the transport of oxygen to the cells within tissues and the transport of carbon dioxide in the opposite direction.
Key Points
External respiration describes the exchange of gasses between the external environment and the bloodstream.
The components of external respiration include alveolar surface area, ventilation and perfusion matching, and partial pressure gradients.
Partial pressure gradients allow gasses to flow from areas of high pressure to areas of lower pressure.
Ventilation and perfusion in the alveoli must be balanced to maintain efficient gas exchange.
Key Terms
passive diffusion: The net movement of material from an area of high concentration to an area of lower concentration without any energy input.
perfusion: The blood supply to the alveolar capillaries that must be balanced with ventilation.
Equilibrium: The rate of change of the gasses in the alveoli and capillary become equal to eachother at the end of gas exchange.
External Respiration
External respiration is the formal term for gas exchange. It describes both the bulk flow of air into and out of the lungs and the transfer of oxygen and carbon dioxide into the bloodstream through diffusion. While the bulk flow of air from the external environment happens due to pressure changes in the lungs, the mechanisms of alveolar gas exchange are more complicated. The primary three components of external respiration are the surface area of the alveolar membrane, the partial pressure gradients of the gasses, and the matching of perfusion and ventilation.
Surface Area
The alveoli have a very high surface area to volume ratio that allows for efficient gas exchange. The alveoli are covered with a high density of capillaries that provide many sites for gas exchange.
The walls of the alveolar membrane are thin and covered with a fluid, extra-cellular matrix that provides a surface for gas molecules in the air of the lungs to diffuse into, from which they can then diffuse into the capillaries.
Partial Pressure Gradients
Partial pressure gradients (differences in partial pressure) allow the loading of oxygen into the bloodstream and the unloading of carbon dioxide out of the bloodstream. These two processes occur at the same time.
Gas exchange in the alveolus: External respiration is a result of partial pressure gradients, alveolar surface area, and ventilation and perfusion matching.
Oxygen has a partial pressure gradient of about 60 mmHg (100 mmHg in alveolar air and 40 mmHg in deoxygenated blood ) and diffuses rapidly from the alveolar air into the capillary.
Equilibrium between the alveolar air and capillaries is reached quickly, within the first third of the length of the capillary within a third of a second. The partial pressure of oxygen in the oxygenated blood of the capillary after oxygen loading is about 100 mmHg.
The process is similar in carbon dioxide. The partial pressure gradient for carbon dioxide is much smaller compared to oxygen, being only 5 mmHg (45 mmHg in deoxygenated blood and 40 mmHg in alveolar air).
Based on Henry’s law, the greater solubility of carbon dioxide in blood compared to oxygen means that diffusion will still occur very rapidly despite the lower partial pressure gradient. Equilibrium between the alveolar air and the capillaries for carbon dioxide is reached within the first half of the length of the capillaries within half a second. The partial pressure of carbon dioxide in the blood leaving the capillaries is 40 mmHg.
Ventilation and Perfusion Matching
The exchange of gas and blood supply to the lungs must be balanced in order to facilitate efficient external respiration. While a severe ventilation-perfusion mismatch indicates severe lung disease, minor imbalances can be corrected by maintaining air flow that is proportional to capillary blood flow, which maintains the balance of ventilation and perfusion.
Perfusion in the capillaries adjusts to changes in PAO2. Constriction in the airways (such as from the bronchospasms in an asthma attack) lead to decreased PAO2 because the flow of air into the lungs is slowed.
In response, the arteries being supplied by the constricted airway undergo vasoconstriction, reducing the flow of blood into those alveoli so that the perfusion doesn’t become much greater relative to the decreased ventilation (a type of ventilation-perfusion mismatch called a shunt).
Alternatively, breathing in higher concentrations of oxygen from an oxygen tank will cause vasodilation and increased blood perfusion in the capillaries.
Ventilation adjusts from changes in PACO2. When airflow becomes higher relative to perfusion, PACO2 decreases, so the bronchioles will constrict in order to maintain to the balance between airflow (ventilation) and perfusion. When airflow is reduced, PACO2 increases, so the bronchioles will dilate in order to maintain the balance.
Internal Respiration
Cellular respiration is the metabolic process by which an organism obtains energy through the reaction of oxygen with glucose.
Key Points
Cellular respiration is the metabolic process by which an organism obtains energy by reacting oxygen with glucose to give water, carbon dioxide, and adenosine triphosphate (energy).
The 3 steps of cellular respiration are glycolysis, the Krebs cycle, and oxidative phosphorylation.
Carbon dioxide is a waste product of cellular respiration that comes from the carbon in glucose and the oxygen used in cellular respiration.
Internal respiration involves gas exchange between the bloodstream and tissues, and cellular respiration.
Gas exchange in tissues is a result of tissue surface area, gas partial pressure gradients, and the blood perfusion of those tissues.
Key Terms
Cellular respiration: The cellular process of producing adenosine triphosphate (ATP), water, and carbon dioxide from glucose and oxygen.
Oxidative Phosphorylation: The final step of cellular phosphorylation in which oxygen is used to a create an electron transport chain that produces a large amount of ATP from nicotinamide adenine dinucleotide (NADH).
Internal respiration refers to two distinct processes. The first is the exchange of gasses between the bloodstream and the tissues. The second is the process of cellular respiration, from which cells utilize oxygen to perform basic metabolic functions.
Gas Exchange with Tissues
Gas exchange occurs in the alveoli so that oxygen is loaded into the bloodstream and carbon dioxide is unloaded from the bloodstream. Afterward, oxygen is brought to the left side of the heart via the pulmonary vein, which pumps it into the systemic circulation.
Red blood cells carry the oxygen into the capillaries of the tissues of the body. Oxygen diffuses into the cells of the tissues, while carbon dioxide diffuses out of the cells of the tissues and into the bloodstream.
The factors that influence tissue gas exchange are similar to the factors of alveolar gas exchange, and include partial pressure gradients between the blood and the tissues, the blood perfusion of those tissues, and the surface areas of those tissues. Each of those factors generally increase gas exchange as those factors are increased (i.e., more oxygen diffusion in tissues with more blood perfusion).
Regarding the partial pressure gradients in systemic capillaries, they have a PaO2 of 100mmHg and a PaCO2 of 40mmHG within the capillary and a PaO2 of 40 mmHg and PaCO2 of 45 mmHg inside issue cells, which allows gas exchange to occur.
Cellular Respiration
Cellular respiration is the metabolic process by which an organism obtains energy through the reaction of oxygen with glucose to produce water, carbon dioxide and ATP, which is the functional source of energy for the cell. The oxygen supply for cellular respiration comes from the external respiration of the respiratory system.
Overview of cellular respiration: A diagram of cellular respiration including glycolysis, the Krebs cycle (also called the citric acid cycle), and the electron transport chain.
Cellular respiration includes three major steps, and occurs mainly in the cytoplasm of the cell and within the mitochondria of the cell. The net formula for cellular respiration is:
Glycolysis: The breakdown of glucose into pyruvate, ATP, H2O, and heat.
Krebs Cycle: Produces NADH from pyruvate.
Oxidative Phosphorylation: Produces ATP from NADH, oxygen, and H+. The oxygen plays the role of electron receptor in an electron transport chain to produce ATP.
The carbon dioxide waste is the result of the carbon from glucose (C6H12O6) being broken down to produce the pyruvate and NADH intermediates needed to produce ATP at the end of respiration. The energy stored in ATP can then be used to drive processes that require energy, including biosynthesis, locomotion, or transportation of molecules across cell membranes.
Cellular respiration can occur anaerobically without oxygen, such as through lactic acid fermentation. Human cells may use lactic acid fermentation in muscle tissue during strenuous exercise when there isn’t enough oxygen to power the tissues. This process is very inefficient compared to aerobic respiration, as without oxidative phosphorylation, the cell cannot produce nearly as much ATP (2 ATP compared to 38 during cellular respiration).
Oxygen Transport
Hemoglobin is the primary transporter of oxygen with an oxygen binding capacity between 1.36 and 1.37 ml O2 per gram Hgb.
Key Points
About 98.5% of the oxygen in a sample of arterial blood in a healthy human breathing air at sea-level pressure is bound to the hemoglobin in blood.
Each molecule of hemoglobin is made up of four heme groups.
The oxygen dissociation curve shows the amount of oxygen saturated in hemoglobin for a given partial pressure of oxygen.
The curve shifts right when oxygen’s affinity for binding to hemoglobin is decreased, and shifts left when its affinity for binding is increased.
A rightward shift occurs during exercise, decreasing blood pH and increasing temperature, or during anemia (with a downward shift as well).
A leftward shift occurs during increased blood pH, decreased temperature, or carbon monoxide exposure.
Key Terms
hemoglobin: A protein found in red blood cells that provides a binding site for oxygen to transport it to the tissues of the body.
dissociation curve: The oxygen–hemoglobin dissociation curve plots the proportion of hemoglobin saturated with oxygen on the vertical axis against the partial pressure of oxygen on the horizontal axis.
Hemoglobin
About 98.5% of the oxygen in a sample of arterial blood in a healthy human breathing air at sea-level pressure is bound to the hemoglobin in blood (Hgb). Hemoglobin is a protein found in red blood cells (also called erythrocytes).
There are roughly 270 million hemoglobin molecules in a single red blood cell, and each contains 4 heme groups. The function of Hgb is to provide a binding site for oxygen to carry oxygen throughout the bloodstream to the systemic tissues for cellular respiration.
Hemoglobin: Hemoglobin is the iron-containing, oxygen-transport metalloprotein in the red blood cells of all vertebrates.
About 1.5% of oxygen is physically dissolved in the other blood liquids and not connected to Hgb. It has an oxygen binding capacity between 1.36 and 1.37 ml O2 per gram Hgb.
Oxyhemoglobin Dissociation Curve
The percentage of oxygen that is saturated in the hemoglobin of blood is generally represented by a curve that shows the relationship between PaO2 and O2 saturation. The saturation of O2 in hemoglobin is an indicator of how much O2 is able to reach the tissues of the body.
Higher PaO2 means higher saturation of oxygen in the blood. Under normal conditions the PaO2 in systemic blood is equal to 50%, about 26.6 mmHg,; this is called the P50.
The curve starts to plateau at PaO2 higher than 60 mmHg, meaning that increases in PaO2 after that point won’t significantly increase saturation. This also means that the approximate carrying capacity for oxygen in hemoglobin has been reached and excess oxygen won’t go into hemoglobin.
The carrying capacity can be increased if more hemoglobin is added to the system, such as through greater red blood cell generation in high altitudes, or from blood transfusions. The lower areas of the curve show saturation when oxygen is unloaded into the tissues.
The oxyhemoglobin dissociation curve: The oxygen–hemoglobin dissociation curve plots the percent hemoglobin saturation (y-axis) against the partial pressure of oxygen in the blood (PO2). The blue curve is a standard curve, while the red and green curves are right and leftward shifts respectively.
The oxyhemoglobin dissociation curve can shift in response to a variety of factors. A change in the P50 of the curve is a sign that the dissociation curve as a whole has shifted. Shifts indicate a change in affinity for oxygen’s binding to hemoglobin, which changes the ability of oxygen to bind to hemoglobin and stay bound to it (i.e., not be released from it).
Rightward shifts indicate a decreased affinity for the binding of hemoglobin so that less oxygen binds to hemoglobin, and more oxygen is unloaded from it into the tissues. The curve shifts right during decreased blood pH (called the Bohr effect), increased temperature, and during exercise among other things.
Anemia (a disorder marked by a decreased red blood cell count and less hemoglobin) also causes a rightward shift but also changes the shape of the curve so that it moves downward as well as a result of the reduced levels of hemoglobin.
Leftward shifts indicate an increased affinity for the binding of hemoglobin so that more oxygen binds to hemoglobin, but less oxygen is unloaded from it into the tissues. Causes of leftward shifts include increased blood pH, decreased temperature, and carbon monoxide exposure. Carbon monoxide binds to hemoglobin in place of oxygen, so that less oxygen reaches the tissues; this can be fatal if severe enough.
Carbon Dioxide Transport
CO2 is carried in blood in three different ways: dissolved in plasma, bound to hemoglobin, or as a bicarbonate ion.
Key Points
Carbon dioxide is transported through the bloodstream either dissolved in the blood, bound the hemoglobin, or converted to bicarbonate ions.
The Haldane effect is the decreased binding of carbon dioxide in hemoglobin due to increased oxygen levels and increased binding of carbon dioxide to hemoglobin from decreased oxygen levels.
CO2 + H2O → H2CO3 → H+ + HCO3− is the bicarbonate formation reaction in the plasma.
Increased carbon dioxide means increased blood acidity, while decreased carbon dioxide means increased blood acidity.
The bicarbonate reaction is reversible, which allows bicarbonate to turn back into dissolved carbon dioxide to diffuse from the alveolus.
Key Terms
red blood cell: A type of cell in the blood of vertebrates that contains hemoglobin and transports oxygen from the lungs to the tissues; an erythrocyte.
Bicarbonate: A negatively charged ion that accumulates in plasma when carbon dioxide dissolves in water and reacts with it. It also acts as a buffer for blood pH.
carbonic anhydrase: An enzyme that catalyzes the bicarbonate reaction in either direction.
Carbon Dioxide Transport
Carbon dioxide is the product of cellular respiration and is transported from the cells of tissues in the body to the alveoli of the lungs through the bloodstream. Carbon dioxide is carried in the blood in three different ways.
Dissolved in the Plasma
About 5% of carbon dioxide is transported in the plasma of the blood as dissolved CO2 molecules that aren’t bound to anything else. Carbon dioxide has a much higher solubility than oxygen, which explains why a relatively greater amount of carbon dioxide is dissolved in the plasma compared to oxygen.
Bound to Hemoglobin
Structure of human hemoglobin: Hemoglobin is a tetramer of alpha (red) and beta (blue) subunits with iron containing heme groups (green).
While oxygen binds to the iron content in the heme of hemoglobin, carbon dioxide can bind to the amino acid chains on hemoglobin. When carbon dioxide clings to hemoglobin it forms carbanimohemoglobin.
About 10% of carbon dioxide in the human body is transported this way. Carbanimohemoglobin gives red blood cells a bluish color, which is one of the reasons why the veins that carry deoxygenated blood appear to be blue.
A property of hemoglobin called the Haldane effect states that deoxygenated blood has an increased capacity to carry carbon dioxide, while oxygenated blood has a decreased capacity to carry carbon dioxide.
This property means that hemoglobin will primarily carry oxygen in systemic circulation until it unloads that oxygen and is able to carry a relatively higher amount of carbon dioxide. This is due to deoxygenated blood’s increased capacity to carry carbon dioxide, and from the carbon dioxide loaded from the tissues during tissue gas exchange.
Bicarbonate Ions
The majority (85%) of carbon dioxide travels in the bloodstream as bicarbonate ions. The reaction that describes the formation of bicarbonate ions in the blood is:
CO2 + H2O → H2CO3 → H+ + HCO3–
This means that carbon dioxide reacts with water to form carbonic acid, which dissociates in solution to form hydrogen ions and bicarbonate ions.
The main implication of this process is that the pH of blood becomes a way of determining the amount of carbon dioxide in the blood. This is because if carbon dioxide increases in the body, it will manifest as increased concentrations of bicarbonate and increased concentrations of hydrogen ions that reduce blood pH and make the blood more acidic.
Conversely, if carbon dioxide levels are reduced, there will be less bicarbonate and fewer hydrogen ions dissolved in the blood, so pH will increase and blood will become more basic. Bicarbonate ions act as a buffer for the pH of blood so that blood pH will be neutral as long as bicarbonate and hydrogen ions are balanced.
This connection explains how ventilation rate and blood chemistry are related, as hyperventilation will cause alkalosis, and hypoventilation will cause acidosis, due to the changes in carbon dioxide levels that they cause.
Bicarbonate is also carried in the fluids of tissues besides the blood vessels, especially in the duodenum and intestine, so problems in those organs can cause a respiratory system response.
Transport to the Alveoli
After carbon dioxide travels through the bloodstream to the capillaries covering the alveoli of the lungs through any of the 3 methods listed above, it must return to dissolved carbon dioxide form in order to diffuse across the capillary into the alveolus. Dissolved carbon dioxide is already able to diffuse into the alveolus, while hemoglobin-bound carbon dioxide is unloaded into the plasma.
For carbon dioxide stored in bicarbonate, it undergoes a reaction reversal. Bicarbonate ions dissolved in the plasma enter the red blood cells by diffusing across a chloride ion gradient (replacing chloride inside the cell), and combining with hydrogen to form carbonic acid.
Next, the action of carbonic anhydrase breaks carbonic acid down into carbon dioxide in water, which leaves the cell by diffusion. The dissolved carbon dioxide is then able to diffuse into the alveolus.
The gas laws are a group of physical laws modeling the behavior of gases developed from experimental observations from the 17th century onwards. While many of these laws apply to ‘ideal’ gases in closed systems at standard temperature and pressure (STP), their principles can still be useful in understanding and altering a significant number of physicochemical processes of the body as well as the mechanism of action of drugs (e.g., inhaled anesthetics).[rx]
This argument, which combines physics, medicine, physiology, and biology, starts from the assumption that pressure, volume, and temperature are interconnected variables. Indeed, each gas law holds one constant and observes the variation in the other two.
Types of Gas Laws
Boyle’s Law
Boyle’s law or Boyle–Mariotte law or Mariotte’s law (especially in France) takes the name of Robert Boyle (1627–1691) and is based on the research of Richard Towneley (1629-1707) and Henry Power (1623–1668). It states that at a constant temperature, the pressure is inversely proportional to volume:
P alpha 1/V or P·V = k, where k is a constant and is dependent on the temperature.
NB: alpha means ‘is proportional to.’
For the same gas under different conditions at the same temperature, it can also be expressed as:
P1·V1 = P2·V2
Charles’ Law
Charles’s law, discovered by Jacques Charles (1746-1823) in 1787 and refined by Joseph Louis Gay-Lussac (1778-1850) in 1808, states that at constant pressure, the volume is directly proportional to absolute temperature, for a fixed mass of a gas:
V alpha T, which can also be stated as V/T = k, where k is a constant, and similarly, V1/T1 = V2/T2
Gay-Lussac’s Law
Gay-Lussac’s Law or Third Gas Law states that for a constant volume, the pressure is directly proportional to absolute temperature:
P alpha T; also stated as P/T = K, where K is a constant, and similarly, P1/T1 = P2/T2
Those three laws can be mathematically combined and expressed as:
P1V1/T1 = P2V2/T2
In addition to the three fundamental laws, other gas laws must be considered.
Avogadro’s Law
Equal volumes of gases at the same temperature and pressure contain the same number of molecules (6.023·10^23, Avogadro’s number). In other words, the volume occupied by an ideal gas is proportional to the number of moles of gas and the molar volume of an ideal gas (the space occupied by 1 mole of the “ideal” gas) is 22.4 liters at standard temperature and pressure.
Ideal Gas Law
The ideal gas law is a combination of Boyle’s law, Charles’s law, Gay-Lussac’s law, and Avogadro’s law:
P·V = n·R·T
n is the number of moles of the gas (mol), R is the ideal gas constant (8.314 J/(K·mol), or 0.820 (L·atm)/(K·mol)), T is the absolute temperature (K), P is pressure, and V is volume.
Dalton’s Law and Henry’s Law
Dalton’s law of partial pressures states that, for a mixture of non-reacting gases, the sum of the partial pressure of each gas is equal to the total pressure exerted by the mixture, at constant temperature and volume:
Henry’s law states that for a constant temperature, the amount of dissolved gas in a liquid is directly proportional to the partial pressure of that gas (in contact with its surface). This relationship is no longer linear once a gas mixture is used, due to stabilization and destabilization effects on solubility[rx], and deviations are found with increasingly high pressures or concentrations[rx]:
P = K·M, where P is the partial pressure of the gas, K is Henry’s constant of proportionality, and M is the molar concentration of the gas.
Graham’s Law
The rate of diffusion (or effusion) of a gas is inversely proportional to the square root of the mass of its particles. When a gas had particularly large particles (or is particularly dense), it will mix more slowly with other gases, and oozes more slowly from its containers.
Dalton’s Law of Partial Pressure
Dalton’s law of partial pressures states that the pressure of a mixture of gases is the sum of the pressures of the individual components.
Key Points
This empirical law was observed by John Dalton in 1801 and is related to the ideal gas laws.
Atmospheric air is a mixture of nitrogen, water, oxygen, carbon dioxide, and other minor gasses. The relative concentrations of a gasses don’t change even as the pressure and volume of the total gasses change.
Gasses flow from areas of high to low pressure, so the partial pressures of inhaled and alveolar air determine why oxygen goes into the alveoli, and why carbon dioxide leaves the alveoli.
Dalton’s law is only completely accurate for ideal gasses.
Key Terms
Dalton’s law: The total pressure of a mixture of gases is the sum of the partial pressures of each gas in the mixture; it is only true for ideal gases.
Dalton’s law states that the total pressure exerted by the mixture of inert (non-reactive) gases is equal to the sum of the partial pressures of individual gases in a volume of air. This empirical law was observed by John Dalton in 1801 and is related to the ideal gas laws.
Dalton’s Law in Respiration
The air in the atmosphere is a mixture of many different gases, that vary in concentration. Dalton’s law states that at any given time, the percentage of each of these gasses in the air we breathe makes its contribution to total atmospheric pressure, and this contribution will depend on how much of each gas is in the air we breathe.
Dalton’s law also implies that the relative concentration of gasses (their partial pressures) does not change as the pressure and volume of the gas mixture changes so that air inhaled into the lungs will have the same relative concentration of gasses as atmospheric air. In the lungs, the relative concentration of gasses determines the rate at which each gas will diffuse across the alveolar membranes.
Mathematically, the pressure of a mixture of gases can be defined as the sum of the partial pressures of each of the gasses in the air.
For the purposes of gas exchange, O2 and CO2 are mainly considered due to their metabolic importance in gas exchange. Because gasses flow from areas of high pressure to areas of low pressure, atmospheric air has higher partial pressure of oxygen than alveolar air (PO2= 159mm Hg compared to PAO2= 100mm Hg).
Similarly, atmospheric air has a much lower partial pressure for carbon dioxide compared to alveolar air (PCO2= .3mm Hg compared to PACO2= 40mm Hg). These pressure differences explain why oxygen flows into the alveoli and why carbon dioxide flows out of the alveoli through passive diffusion (just as a similar process explains alveolar and arterial gas exchange).
While inhaled air is similar to atmospheric air due to Dalton’s law, exhaled air will have relative concentrations that are in between atmospheric and alveolar air due to the passive diffusion of gasses during gas exchange.
Dalton’s law is only truly applicable in every situation to ideal gasses. Therefore most gasses will not follow it exactly, especially in conditions of extremely high pressure, or in situations where intermolecular forces act to keep the gasses together.
Henry’s Law
Henry’s law states that the amount of a gas that dissolves in a liquid is directly proportional to the partial pressure of that gas.
Key Points
At a constant temperature, the amount of a given gas that dissolves in a given type and volume of liquid is directly proportional to the partial pressure of that gas in equilibrium with that liquid.
Gasses with a higher solubility will have more dissolved molecules than gasses with a lower solubility if they have the same partial pressure.
Henry’s law explains how gasses dissolve across the alveoli–capillary barrier.
Henry’s law predicts how gasses behave during gas exchange based on
the partial pressure gradients and solubility of oxygen and carbon
dioxide.
Key Terms
Henry’s law: At a constant temperature, the amount of a given gas that dissolves in a given type and volume of liquid is directly proportional to the partial pressure of that gas in equilibrium with that liquid.
partial pressure gradient: The difference between the partial pressures (and thus concentration) of gasses between gaseous and dissolved forms.
EXAMPLES
An everyday example of Henry’s law is given by carbonated soft drinks. Before the bottle or can is opened, the gas above the drink is almost pure carbon dioxide at a pressure slightly higher than atmospheric pressure. The drink itself contains dissolved carbon dioxide. When the bottle or can is opened, some of this gas escapes, giving the characteristic hiss (or pop in the case of a sparkling wine bottle). Because the pressure above the liquid is now lower, some of the dissolved carbon dioxides comes out of the solution as bubbles. If a glass of the drink is left in the open, the concentration of carbon dioxide in the solution will come into equilibrium with the carbon dioxide in the air, and the drink will go flat.
Henry’s law states that at a constant temperature, the amount of a gas that dissolves in a liquid is directly proportional to the partial pressure of that gas in equilibrium with that liquid. It was formulated by William Henry in 1803.
Henry’s law: Henry’s law states that when a gas is in contact with the surface of a liquid, the amount of the gas which will go into solution is proportional to the partial pressure of that gas.
The practical description for the law is that the solubility (i.e., equilibrium) of a gas in a liquid is directly proportional to the partial pressure of that gas. In addition, the partial pressure is able to predict the tendency to dissolve simply because the gasses with higher partial pressures have more molecules and will bounce into the solution they can dissolve into more often than gasses with lower partial pressures.
Henry’s law also applies to the solubility of other substances that aren’t gaseous, such as the equilibrium of organic pollutants in water being based on the relative concentration of that pollutant in the media its suspended in.
Henry’s law can be put into mathematical terms (at constant temperature):
p=kHcp=kHc
Where p is the partial pressure of the solute in the gas above the solution, c is the concentration of the solute, the solubility of the substance is k, and Henry’s law constant (H), which depends on the solute, the solvent, and the
temperature.
The solubility captures the tendency of a substance to go towards equilibrium in a solution, which explains why gasses that have the same partial pressure may have different tendencies to dissolve.
Henry’s Law in Respiration
The main application of Henry’s law in respiratory physiology is to predict how gasses will dissolve in the alveoli and bloodstream during gas exchange. The amount of oxygen that dissolves into the bloodstream is directly proportional to the partial pressure of oxygen in alveolar air.
The partial pressure of oxygen is greater in alveolar air than in deoxygenated blood, so oxygen has a high tendency to dissolve into deoxygenated blood. Conversely, the opposite is true for carbon dioxide, which has a greater partial pressure in deoxygenated blood than in the alveolar air, so it will diffuse out of the solution and back into gaseous form.
Recall that the difference in partial pressures between the bloodstream and alveoli (the partial pressure gradient) are much smaller for carbon dioxide compared to oxygen. Carbon dioxide has much higher solubility in the plasma of blood than oxygen (roughly 22 times greater), so more carbon dioxide molecules are able to diffuse across the small pressure gradient of the capillary and alveoli.
Oxygen has a larger partial pressure gradient to diffuse into the bloodstream, so its lower solubility in the blood doesn’t hinder it during gas exchange. Therefore, based on the properties of Henry’s law, both the partial pressure and solubility of oxygen and carbon dioxide determine how they will behave during gas exchange.
Flow-Volume loop showing successful FVC maneuver. Positive values represent expiration, negative values represent inspiration. At the start of the test both flow and volume are equal to zero (representing the volume in the spirometer rather than the lung). The trace moves clockwise for expiration followed by inspiration. After the starting point the curve rapidly mounts to a peak (the peak expiratory flow). (Note the FEV1 value is arbitrary in this graph and just shown for illustrative purposes; these values must be calculated as part of the procedure).
Total lung capacity: the volume in the lungs at maximal inflation, the sum of VC and RV.
TV
Tidal volume: that volume of air moved into or out of the lungs during quiet breathing (TV indicates a subdivision of the lung; when tidal volume is precisely measured, as in gas exchange calculation, the symbol TV or VT is used.)
RV
Residual volume: the volume of air remaining in the lungs after a maximal exhalation
ERV
Expiratory reserve volume: the maximal volume of air that can be exhaled from the end-expiratory position
IRV
Inspiratory reserve volume: the maximal volume that can be inhaled from the end-inspiratory level
IC
Inspiratory capacity: the sum of IRV and TV
IVC
Inspiratory vital capacity: the maximum volume of air inhaled from the point of maximum expiration
VC
Vital capacity: the volume of air breathed out after the deepest inhalation.
VT
Tidal volume: that volume of air moved into or out of the lungs during quiet breathing (VT indicates a subdivision of the lung; when tidal volume is precisely measured, as in gas exchange calculation, the symbol TV or VT is used.)
FRC
Functional residual capacity: the volume in the lungs at the end-expiratory position
The actual volume of the lung including the volume of the conducting airway.
FVC
Forced vital capacity: the determination of the vital capacity from a maximally forced expiratory effort
FEVt
Forced expiratory volume (time): a generic term indicating the volume of air exhaled under forced conditions in the first t seconds
FEV1
The volume that has been exhaled at the end of the first second of forced expiration
FIFA
Forced expiratory flow related to some portion of the FVC curve; modifiers refer to the amount of FVC already exhaled
FEFmax
The maximum instantaneous flow achieved during an FVC maneuver
FIF
Forced inspiratory flow: (Specific measurement of the forced inspiratory curve is denoted by nomenclature analogous to that for the forced expiratory curve. For example, maximum inspiratory flow is denoted FIFmax. Unless otherwise specified, volume qualifiers indicate the volume inspired from RV at the point of measurement.)
PEF
Peak expiratory flow: The highest forced expiratory flow measured with a peak flow meter
MVV
Maximal voluntary ventilation: volume of air expired in a specified period during repetitive maximal effort