The descending tracts are the pathways by which motor signals are sent from the brain to lower motor neurones. The lower motor neurones then directly innervate muscles to produce movement.
The motor tracts can be functionally divided into two major groups:
Pyramidal tracts – These tracts originate in the cerebral cortex, carrying motor fibres to the spinal cord and brain stem. They are responsible for the voluntary control of the musculature of the body and face.
Extrapyramidal tracts – These tracts originate in the brain stem, carrying motor fibres to the spinal cord. They are responsible for the involuntary and automatic control of all musculature, such as muscle tone, balance, posture and locomotion
There are no synapses within the descending pathways. At the termination of the descending tracts, the neurones synapse with a lower motor neurone. Thus, all the neurones within the descending motor system are classed as upper motor neurones. Their cell bodies are found in the cerebral cortex or the brain stem, with their axons remaining within the CNS.
Pyramidal Tracts
The pyramidal tracts derive their name from the medullary pyramids of the medulla oblongata, which they pass through.
These pathways are responsible for the voluntary control of the musculature of the body and face.
Functionally, these tracts can be subdivided into two:
Corticospinal tracts – supply the musculature of the body.
Corticobulbar tracts – supplies the musculature of the head and neck.
We shall now discuss both pathways in further detail.
Corticospinal Tracts
The corticospinal tracts begin in the cerebral cortex, from which they receive a range of inputs:
Primary motor cortex
Premotor cortex
Supplementary motor area
They also receive nerve fibres from the somatosensory area, which play a role in regulating the activity of the ascending tracts.
After originating from the cortex, the neurones converge and descend through the internal capsule (a white matter pathway, located between the thalamus and the basal ganglia). This is clinically important, as the internal capsule is particularly susceptible to compression from haemorrhagic bleeds, known as a ‘capsular stroke‘. Such an event could cause a lesion of the descending tracts.
After the internal capsule, the neurones pass through the crus cerebri of the midbrain, the pons and into the medulla.
In the most inferior (caudal) part of the medulla, the track divides into two:
The fibres within the lateral corticospinal tract decussate (cross over to the other side of the CNS). They then descend into the spinal cord, terminating in the ventral horn (at all segmental levels). From the ventral horn, the lower motor neurones go on to supply the muscles of the body.
The anterior corticospinal tract remains ipsilateral, descending into the spinal cord. They then decussate and terminate in the ventral horn of the cervical and upper thoracic segmental levels.
Te corticobulbar tracts arise from the lateral aspect of the primary motor cortex. They receive the same inputs as the corticospinal tracts. The fibres converge and pass through the internal capsule to the brainstem.
The neurones terminate on the motor nuclei of the cranial nerves. Here, they synapse with lower motor neurones, which carry the motor signals to the muscles of the face and neck.
Clinically, it is important to understand the organisation of the corticobulbar fibres. Many of these fibres innervate the motor neurones bilaterally. For example, fibres from the left primary motor cortex act as upper motor neurones for the right and left trochlear nerves. There are a few exceptions to this rule:
Upper motor neurones for the facial nerve (CN VII) have a contralateral innervation. This only affects the muscles in the lower quadrant of the face – below the eyes. (The reasons for this are beyond the scope of this article)
Upper motor neurons for the hypoglossal (CN XII) nerve only provide contralateral innervation.
Extrapyramidal Tracts
The extrapyramidal tracts originate in the brainstem, carrying motor fibres to the spinal cord. They are responsible for the involuntary and automatic control of all musculature, such as muscle tone, balance, posture and locomotion.
There are four tracts in total. The vestibulospinal and reticulospinal tracts do not decussate, providing ipsilateral innervation. The rubrospinal and tectospinal tracts do decussate and therefore provide contralateral innervation
Vestibulospinal Tracts
There are two vestibulospinal pathways; medial and lateral. They arise from the vestibular nuclei, which receive input from the organs of balance. The tracts convey this balance information to the spinal cord, where it remains ipsilateral.
Fibres in this pathway control balance and posture by innervating the ‘anti-gravity’ muscles (flexors of the arm, and extensors of the leg), via lower motor neurones.
Reticulospinal Tracts
The two reticulospinal tracts have differing functions:
The medial reticulospinal tract arises from the pons. It facilitates voluntary movements and increases muscle tone.
The lateral reticulospinal tract arises from the medulla. It inhibits voluntary movements and reduces muscle tone.
Rubrospinal Tracts
The rubrospinal tract originates from the red nucleus, a midbrain structure. As the fibres emerge, they decussate (cross over to the other side of the CNS), and descend into the spinal cord. Thus, they have a contralateral innervation.
Its exact function is unclear, but it is thought to play a role in the fine control of hand movements
Tectospinal Tracts
This pathway begins at the superior colliculus of the midbrain. The superior colliculus is a structure that receives input from the optic nerves. The neurones then quickly decussate, and enter the spinal cord. They terminate at the cervical levels of the spinal cord.
The tectospinal tract coordinates movements of the head in relation to visual stimuli.
Motor pathways carry signals from the brain to skeletal muscle and smooth muscle such as those contained in glands. The system consists of upper and lower motor neurons. The information provided below is primarily focused on the motor pathways that coordinate skeletal muscle movement, i.e. motor pathways related to voluntary control of skeletal muscles.
Motor Pathways
The connections between the motor cortex in the forebrain and motor neurons within the spinal cord are made up of two pyramidal tracts; the pyramidal system and the extrapyramidal system. These motor pathways are transmitted via the ventral horns within the spine. Upper motor neurons are located mainly within the neopallium of the cerebellum. They govern the excitation or inhibition of lower motor neurons.
Stimulation of the motor neurons is a result of activity within the cerebral cortex and/or thalamus. There is a balance between the excitatory and inhibitory inputs from these parts of the brain. The thalamus effectively acts as a relay station from the cerebrum and cerebellum before neurons lead into the motor pathways of the spine.
Pyramidal System (Corticospinal)
The pyramidal tract produces fine movements associated with skill, e.g. writing and playing a musical instrument in humans. This tract is composed of direct connections that contain no synapses within the brain stem. Nerve fibers of the pyramidal system originate in the cerebral cortex and then pass to the thalamus, and medulla oblongata. Therefore the neurons pass directly through the ventral aspect of the medulla oblongata in a pyramidal shape providing the reason for the name of this tract. Some fibers decussate in the medulla oblongata, whilst others remain ipsilateral until they leave the spinal cord where they cross the midline of the body. The result of this is that all fibers cross the midline at some point so that the left side of the brain controls the right side of the body and vice versa.
Motor tracts within the pyramidal system are fundamental in the control and coordination of muscle groups that require concentration and conscious thought to control. This is particularly true for movements of the hands and fingers and therefore these pyramidal tracts are most developed in primates, although may exist in other species such as the cat, where they aid in grooming. It is thought that the evolution of pyramidal tracts is closely associated with the development of conscious and fine movements. In most domestic species that lack the ability to undertake fine movements the pyramidal tracts are primarily involved in the control of the jaw, lips, and aspects of the face.
Extrapyramidal System
The extrapyramidal system represents part of the motor pathway system that has synapses within the brain stem which is in contrast to those of the pyramidal system. The extrapyramidal tract is distinguishable from the pyramidal system as tracts do not run within the pyramids of the medulla oblongata and instead run outside. This extrapyramidal pathway contains various multisynaptic pathways that relay within several nuclei in the brain. These nuclei are dispersed from the telencephalon to the medulla oblongata and may be visible grossly.
Other parts of the extrapyramidal tract take origin from the tectum and reticular formation. These synapses within the brain stem make it possible for the motor neuron signals to be influenced as they enter the ventral horn of the spinal cord. The cerebellum utilizes this influence to ensure that movements are smooth and coordinated.
There are a number of neurons involved in modifying the neuronal signals in the extrapyramidal tract. These include the neurons that relay within nuclei which include the red nucleus, the substantia nigra, the caudate nucleus, the subthalamic nuclei, and the olive in the medulla oblongata. The reticular formation is also involved in the extrapyramidal pathway. Neurons that relay in the red nucleus and reticular formation relay directly onto lower motor neurons whilst others relay to other nuclei. The main descending motor tracts from the red nucleus and the reticular formation are the rubrospinal tract, the reticulospinal tract, the vestibulospinal tract, and the tectospinal tract. The rubrospinal tract is important in carnivores and ungulates as it modulates pattern generators in the spinal cord.
The extrapyramidal tract is responsible for the control of larger muscles and also groups of muscles. This track constitutes a major part of the coordination system in which groups of muscles are used to maintain posture and smooth movements during locomotion. These types of movements do not require the same level of conscious input or concentration as those of the pyramidal tract. It is thought that the extrapyramidal system represents an earlier evolutionary development than the pyramidal system and therefore is more often a feature of animals less able to perform complex movements. It is the most important system in domestic species.
Organization of Motor Neuron Pathways
The motor system is the part of the central nervous system that is involved with the movement.
Key Points
The pyramidal tract, which includes both the corticospinal and corticobulbar tracts, serves as the motor pathway for upper motor neuronal signals coming from the cerebral cortex and from primitive brainstem motor nuclei.
Peripheral motor nerves carry the motor impulses from the spinal cord to the voluntary muscles.
The large majority (90%) of motor neurons cross (decussate) to the contralateral side of the brain at the level of the brainstem.
Key Terms
extrapyramidal system: A biological neural network that is part of the motor system that causes involuntary movements.
corticospinal tract: The nervous system tract that conducts impulses from the brain to the spinal cord. It contains mostly motor axons and is made up of two separate tracts in the spinal cord: the lateral corticospinal tract and the anterior corticospinal tract.
motor system: The part of the central nervous system that is involved with the movement. It consists of the pyramidal and extrapyramidal systems.
cerebral cortex: The gray, folded, outermost layer of the cerebrum that is responsible for higher brain processes such as sensation, voluntary muscle movement, thought, reasoning, and memory.
Decussation of the pyramids: A deep dissection, lateral view of a brainstem. The pyramidal tract is visible in red, and pyramidal decussation is labeled at the lower right.
The motor system is the part of the central nervous system that is involved with the movement. It consists of the pyramidal and extrapyramidal systems.
The motor pathway also called the pyramidal tract or the corticospinal tract serves as the motor pathway for upper motor neuronal signals coming from the cerebral cortex and from primitive brainstem motor nuclei. There are upper and lower motor neurons in the corticospinal tract.
The motor impulses originate in the giant pyramidal cells (Betz cells) of the motor area, i.e., the precentral gyrus of the cerebral cortex. These are the upper motor neurons of the corticospinal tract. The axons of these cells pass from the cerebral cortex to the midbrain and the medulla oblongata. Peripheral motor nerves carry the motor impulses from the anterior horn to the voluntary muscles.
Cortical upper motor neurons originate from Brodmann areas 1, 2, 3, 4, and 6, then descend into the posterior limb of the internal capsule, through the crus cerebri, down through the pons, and to the medullary pyramids, where about 90% of the axons cross to the contralateral side at the decussation of the pyramids. They then descend as the lateral corticospinal tract.
These axons synapse with lower motor neurons in the ventral horns of all levels of the spinal cord. The remaining 10% of axons descend on the ipsilateral side as the ventral corticospinal tract. These axons also synapse with lower motor neurons in the ventral horns. Most of them will cross to the contralateral side of the cord (via the anterior white commissure) just before synapsing.
Brodmann areas of the brain: This drawing shows the regions of the human cerebral cortex as delineated by Korvinian Brodmann on the basis of cytoarchitecture.
The midbrain nuclei include four motor tracts that send upper motor neuronal axons down the spinal cord to lower motor neurons. These are the rubrospinal tract, the vestibulospinal tract, the tectospinal tract, and the reticulospinal tract.
The function of lower motor neurons can be divided into two different groups: the lateral corticospinal tract and the anterior cortical spinal tract. The lateral tract contains upper motor neuronal axons that synapse on the dorsal lateral lower motor neurons, which are involved in distal limb control.
The anterior corticospinal tract descends ipsilaterally in the anterior column, where the axons emerge and either synapse on ventromedial lower motor neurons in the ventral horn ipsilaterally or descussate at the anterior white commissure where they synapse on ventromedial lower motor neurons contralaterally.
The ventromedial lower motor neurons control the large, postural muscles of the axial skeleton. These lower motor neurons, unlike those of the dorsal lateral, are located in the ventral horn throughout the spinal cord.
Spinal cord tracts: This diagram of spinal cord tracts shows the motor and efferent pathways in red and the sensory and afferent pathways in blue. Included in the diagram are the following motor pathways: corticospinal tracts (pyramidal tract), and extrapyramidal tracts (tectospinal tract not delineated).
The Role of the Basal Ganglia in Movement
The basal ganglia are responsible for voluntary motor control, procedural learning, and eye movement, as well as cognitive and emotional functions.
Key Points
The basal ganglia are studied extensively in the context of two disorders of the basal ganglia: Parksinson’s disease and Huntington’s disease.
Hemiballismus, a movement disorder arising from neuronal damage in the subthalamic nucleus, presents with violent movements of the arms and legs.
Eye movement, a function of the basal ganglia, is influenced by the superior colliculus, a region of the brain that directs eye movement to specific points in space in response to stimuli.
Basal ganglia are also thought to play a role in motivation.
In the basal ganglia,
the majority of the neurons uses gamma-aminobutyric acid (GABA) as the neurotransmitter
and have inhibitory effects on their
targets.
Key Terms
hemiballismus: A rare movement disorder with involuntary flinging motions of the extremities.
voluntary motor control: The act of directing motion with intent.
forebrain: The anterior part of the brain, including the cerebrum, thalamus, and hypothalamus.
nucleus accumbens: A region in the basal forebrain rostral to the preoptic area of the hypothalamus. This region and the olfactory tubercle collectively form the ventral striatum.
Location of the Basal Ganglia
The basal ganglia (or basal nuclei) are a group of nuclei of varied origin in the brains of vertebrates that act as a cohesive functional unit. They are situated at the base of the forebrain and are strongly connected with the cerebral cortex, thalamus, and other brain areas.
The basal ganglia are associated with a variety of functions, including voluntary motor control, procedural learning relating to routine behaviors or habits such as bruxism and eye movements, as well as cognitive and emotional functions.
Basal ganglia: Locations of the basal ganglia.
Action Selection
Currently, popular theories hold that the basal ganglia play a primary role in action selection. Action selection is the decision of which of several possible behaviors to execute at a given time.
Experimental studies show that the basal ganglia exert an inhibitory influence on a number of motor systems, and that a release of this inhibition permits a motor system to become active. The behavior switching that takes place within the basal ganglia is influenced by signals from many parts of the brain, including the prefrontal cortex, which plays a key role in executive functions.
Movement
The greatest source of insight into the functions of the basal ganglia has come from the study of two neurological disorders, Parkinson’s disease and Huntington’s disease. For both of these disorders, the nature of the neural damage is well-understood and can be correlated with the resulting symptoms.
Parkinson’s disease involves the major loss of dopaminergic cells in the substantia nigra. Huntington’s disease involves the massive loss of medium spiny neurons in the striatum.
The symptoms of the two diseases are virtually opposite: Parkinson’s disease is characterized by a gradual loss of the ability to initiate movement, whereas Huntington’s disease is characterized by an inability to prevent parts of the body from moving unintentionally.
It is noteworthy that, although both diseases have cognitive symptoms, especially in their advanced stages, the most salient symptoms relate to the ability to initiate and control movement. Thus, both are classified primarily as movement disorders.
A different movement disorder, called hemiballismus, may result from damage restricted to the subthalamic nucleus. Hemiballismus is characterized by violent and uncontrollable flinging movements of the arms and legs.
Function in Eye Movement
One of the most intensively studied functions of the basal ganglia is their role in controlling eye movements. Eye movement is influenced by an extensive network of brain regions that converge on a midbrain area called the superior colliculus (SC).
The SC is a layered structure whose layers form two-dimensional retinotopic maps of visual space. A bump of neural activity in the deep layers of the SC drives eye movement toward the corresponding point in space.
Motivation
Although the role of the basal ganglia in motor control is clear, there are also many indications that it is involved in the control of behavior in a more fundamental way, at the level of motivation. In Parkinson’s disease, the ability to execute the components of movement is not greatly affected, but motivational factors such as hunger fail to cause movements to be initiated or switched at the proper times.
The immobility of patients with Parkinson’s disease has sometimes been described as a paralysis of the will. These patients have occasionally been observed to show a phenomenon called kinesia paradoxical, in which a person who is an otherwise immobile response to an emergency in a coordinated and energetic way, then lapses back into immobility once the emergency has passed.
The role in the motivation of the limbic part of the basal ganglia—the nucleus accumbens (NA), ventral pallidum, and ventral tegmental area (VTA)—is particularly well established. Thousands of experimental studies combine to demonstrate that the dopaminergic projection from the VTA to the NA plays a central role in the brain’s reward system.
Numerous things that people find rewarding, including addictive drugs, good-tasting food, and sex, have been shown to elicit activation of the VTA dopamine system. Damage to the NA or VTA can produce a state of profound torpor.
Neurotransmitters
In most regions of the brain, the predominant classes of neurons use glutamate as the neurotransmitter and have excitatory effects on their targets. In the basal ganglia, however, the great majority of neurons uses gamma-aminobutyric acid (GABA) as the neurotransmitter and have inhibitory effects on their targets.
The inputs from the cortex and thalamus to the striatum and subthalamic nucleus are glutamatergic, but the outputs from the striatum, pallidum, and substantia nigra pars reticulata all use GABA. Thus, following the initial excitation of the striatum, the internal dynamics of the basal ganglia are dominated by inhibition and disinhibition.
Other neurotransmitters have important modulatory effects. Dopamine is used by the projection from the substantia nigra pars compacta to the dorsal striatum and also in the analogous projection from the ventral tegmental area to the ventral striatum (nucleus accumbens).
Acetylcholine also plays an important role, as it is used both by several external inputs to the striatum and by a group of striatal interneurons. Although cholinergic cells make up only a small fraction of the total population, the striatum has one of the highest acetylcholine concentrations of any brain structure.
Main circuits of the basal ganglia: This diagram shows the main circuits of the basal ganglia. Two coronal slices have been superimposed to include the involved basal ganglia structures. The + and – signs at the point of the arrows indicate whether the pathway is excitatory or inhibitory, respectively, in effect. Green arrows refer to excitatory glutamatergic pathways, red arrows refer to inhibitory GABAergic pathways and turquoise arrows refer to dopaminergic pathways that are excitatory on the direct pathway and inhibitory on the indirect pathway.
Modulation of Movement by the Cerebellum
The cerebellum is important for motor control—specifically coordination, precision, and timing—as well as some forms of motor learning.
Key Points
The cerebellum is a parallel grooved structure at the bottom of the brain containing a highly regular cellular arrangement of Purkinje cells, granule cells, and other cell types.
The cerebellum adjusts to changes in sensorimotor relationships, possibly functioning as in the Marr-Albus theory: Strong inputs from a single climbing fiber serve as a teaching signal to change the strength of impulses from the corresponding group of parallel fibers.
Four principles of cerebellum function have been identified. They include: feedforward processing, divergence and convergence, modularity, and plasticity.
Key Terms
Purkinje cells: A class of GABAergic neurons located in the cerebellum.
mossy fibers: One of the major inputs to the cerebellum from sources such as the cerebral cortex.
granule cells: These cells receive excitatory input from mossy fibers that originate from pontine nuclei.
The cerebellum is a region of the brain that plays an important role in motor control. It may also be involved in some cognitive functions such as attention and language, and in regulating fear and pleasure responses, but its movement-related functions are the most solidly established. The cerebellum does not initiate movement, but it contributes to coordination, precision, and accurate timing.
It receives input from sensory systems of the spinal cord and from other parts of the brain, including the cerebral cortex, and integrates these inputs to fine-tune motor activity. Because of this fine-tuning function, damage to the cerebellum does not cause paralysis, but instead produces disorders in fine movement, equilibrium, posture, and motor learning.
The cerebellum differs from most other parts of the brain, especially the cerebral cortex, in regards to the ability of signals to move unidirectionally from input to output. This feedforward mode of operation means that the cerebellum cannot generate self-sustaining patterns of neural activity, in contrast to the cerebral cortex. However, the cerebellum can receive information from the cerebral cortex and processes this information to send motor impulses to the skeletal muscle.
Cerebellum: View of the cerebellum from above and behind.
Anatomy of the Cerebellum
Cerebellum cells: View of the cerebellum from above and behind.
In terms of anatomy, the cerebellum has the appearance of a separate structure attached to the bottom of the brain, tucked underneath the cerebral hemispheres. The surface of the cerebellum is covered with finely spaced parallel grooves, in striking contrast to the broad irregular convolutions of the cerebral cortex. These parallel grooves conceal the fact that the cerebellum is actually a continuous thin layer of tissue (the cerebellar cortex), tightly folded in the style of an accordion.
Within this thin layer are several types of neurons with a highly regular arrangement, the most important being Purkinje cells and granule cells. This complex neural network gives rise to a massive signal-processing capability, but almost all of its output is directed to a set of small, deep cerebellar nuclei lying in the interior of the cerebellum.
Function
Marr-Albus Theory
In addition to its direct role in motor control, the cerebellum is also necessary for several types of motor learning, the most notable one being learning to adjust to changes in sensorimotor relationships.
Several theoretical models have been developed to explain sensorimotor calibration in terms of synaptic plasticity within the cerebellum. Most of them derive from early models formulated by David Marr and James Albus, which were motivated by the observation that each cerebellar Purkinje cell receives two dramatically different types of input.
It receives input from thousands of parallel fibers, each individually very weak. However, each cerebellar Purkinje cell also gets input from one single climbing fiber, which is so strong that a single climbing fiber action potential will reliably cause a target Purkinje cell to fire a burst of action potentials.
The basic concept of the Marr-Albus theory is that the climbing fiber serves as a teaching signal, which induces a long-lasting change in the strength of synchronously activated parallel fiber inputs. Observations of long-term depression in parallel fiber inputs have provided support for theories of this type, but their validity remains controversial.
Insights from Cerebellar Dysfunction
The strongest clues to the function of the cerebellum have come from examining the consequences of damage to it. Animals and humans with cerebellar dysfunction show, above all, problems with motor control. They continue to be able to generate motor activity, but it loses precision, producing erratic, uncoordinated, or incorrectly timed movements.
A standard test of cerebellar function is to reach with the tip of the finger for a target at arm’s length. A healthy person will move the fingertip in a rapid straight trajectory, whereas a person with cerebellar damage will reach slowly and erratically, with many mid-course corrections.
Deficits in non-motor functions are more difficult to detect. Thus, the general conclusion reached decades ago is that the basic function of the cerebellum is not to initiate movements, or to decide which movements to execute, but rather to calibrate the detailed form of a movement.
The comparative simplicity and regularity of the cerebellar anatomy led to an early hope that it might imply a similar simplicity of computational function. Although a full understanding of cerebellar function remains elusive, at least four principles are identified as important: 1) feedforward processing, 2) divergence and convergence, 3) modularity, and 4) plasticity.
Feedforward processing – Refers to the unidirectional movement of signals through the system from input to output, with the very little recurrent internal transmission. This means that the cerebellum, in contrast to the cerebral cortex, cannot generate self-sustaining patterns of neural activity. Signals enter the circuit, are processed by each stage in sequential order, and then leave.
Divergence and convergence: The 1000 or so Purkinje cells belonging to a microzone may receive input from as many as 100 million parallel fibers, and focus their own output down to a group of less than 50 deep nuclear cells. Thus, the cerebellar network receives a modest number of inputs, processes them very extensively through its rigorously structured internal network, and sends out the results via a very limited number of output cells.
Modularity: The cerebellar system is functionally divided into independent modules. All modules have a similar internal structure, but with different inputs and outputs. The output of one module does not appear to significantly influence the activity of other modules
Plasticity: The synapses between parallel fibers and Purkinje cells, and the synapses between mossy fibers and deep nuclear cells, are both susceptible to modification of their strength. The influence of each parallel fiber on nuclear cells is adjustable. This arrangement gives tremendous flexibility for fine-tuning the relationship between the cerebellar inputs and outputs.
Functions of the Cerebellum in Integrating Movements
The cerebellum uses feedforward processing and modularity to process information.
Key Points
The function of the cerebellum can be described by the principles of feedforward processing and modularity.
Feedforward processing means signals move in one direction through the cerebellum, from input to output.
Modularity describes the modular nature of the cerebellar system, where modules with similar structures function relatively independently. Modules consist of clusters of neurons with common inputs but distinct outputs.
Key Terms
Purkinje: Purkinje cells are a class of GABAergic neurons located in the cerebellar cortex. They are some of the largest neurons in the human brain, with an intricately elaborate dendritic arbor characterized by a large number of dendritic spines.
feedforward processing: A property of some neural circuits where signals move unidirectionally through the system from input to output, with very little recurrent internal transmission.
microzone: A group of Purkinje cells that all have the same somatotopic receptive field. Microzones contain on the order of 1,000 Purkinje cells each, arranged in a long, narrow strip, and oriented perpendicular to the cortical folds.
Cerebellar Function
Feedforward Processing
The cerebellum differs from most other parts of the brain in that the signal processing is almost entirely feedforward—that is, signals move unidirectionally through the system from input to output, with very little recurrent internal transmission.
The small amount of recurrence that does exist consists of mutual inhibition; there are no mutually excitatory circuits. This feedforward mode of operation means that the cerebellum, in contrast to the cerebral cortex, cannot generate self-sustaining patterns of neural activity.
Signals enter the circuit, are processed by each stage in sequential order, and then leave. As Eccles, Ito, and Szentágothai wrote. This elimination in the design of all possibility of reverberatory chains of neuronal excitation is undoubtedly a great advantage in the performance of the cerebellum as a computer because what the rest of the nervous system requires from the cerebellum is presumably not some output expressing the operation of complex reverberatory circuits in the cerebellum, but the rather quick and clear response to the input of any particular set of information.”
Divergence and Convergence
Cells of the Cerebellum: Transverse section of a cerebellar folium, showing its principal cell types and connections.
In the human cerebellum, information from 200 million mossy fiber inputs is expanded to 40 billion granule cells, whose parallel fiber outputs then converge onto 15 million Purkinje cells. Because of the way that they are lined up longitudinally, the 1,000 or so Purkinje cells belonging to a microzone may receive input from as many as 100 million parallel fibers and focus their own output down to a group of less than 50 deep nuclear cells.
Thus, the cerebellar network receives a modest number of inputs, processes them very extensively through its rigorously structured internal network, and sends out the results via a very limited number of output cells.
Modularity
The cerebellar system is functionally divided into more or less independent modules, that probably number in the hundreds to thousands. All modules have a similar internal structure, but different inputs and outputs.
A module (a multizonal microcompartment in the terminology of Apps and Garwicz) consists of a small cluster of neurons in the inferior olivary nucleus, a set of long narrow strips of Purkinje cells in the cerebellar cortex (microzones), and a small cluster of neurons in one of the deep cerebellar nuclei.
Different modules share input from mossy fibers and parallel fibers, but in other respects they appear to function independently. The output of one module does not appear to significantly influence the activity of other modules.
Plasticity
The synapses between parallel fibers and Purkinje cells, and the synapses between mossy fibers and deep nuclear cells, are both susceptible to modification of their strength. In a single cerebellar module, input from as many as a billion parallel fibers converge onto a group of less than 50 deep nuclear cells, and the influence of each parallel fiber on those nuclear cells is adjustable. This arrangement gives tremendous flexibility for fine-tuning the relationships between the cerebellar inputs and outputs.
Zones and microzones in the cerebellum: This schematic illustration of the structure of zones and microzones in the cerebellum shows three levels of magnification. These zones and microzones help explain the modular nature of the cerebellar function. On the left is a simplified illustration of what the cerebellar cortex would look like if all the folds were straightened out—the vertical dimension is the rostrocaudal axis of the cerebellum, the horizontal dimension is the mediolateral axis. A zone is a longitudinally oriented strip of the cortex, and a microzone is a thin, longitudinally oriented portion of a zone. As the illustration on the right shows, Purkinje cell dendritic trees are flattened in a way that aligns with the microzone length, and parallel fibers cross the microzones at right angles.
Gross motor (physical) skills are those which require whole-body movement and which involve the large (core stabilizing) muscles of the body to perform everyday functions, such as standing, walking, running, and sitting upright. It also includes eye-hand coordination skills such as ball skills (throwing, catching, kicking).
Why are gross motor skills important?
Gross motor skills are important to enable children to perform everyday functions, such as walking, running, skipping, as well as playground skills (e.g. climbing) and sporting skills (e.g. catching, throwing, and hitting a ball with a bat). These are crucial for everyday self-care skills like dressing (where you need to be able to stand on one leg to put your leg into a pant leg without falling over).
Gross motor abilities also have an influence on other everyday functions. For example, a child’s ability to maintain tabletop posture (upper body support) will affect their ability to participate in fine motor skills (e.g. writing, drawing, and cutting) and sitting upright to attend to class instruction, which then impacts their academic learning. Gross motor skills impact your endurance to cope with a full day of school (sitting upright at a desk, moving between classrooms, carrying your heavy school bag).
What are the building blocks necessary to develop gross motor skills?
Muscular strength: The ability to exert force against resistance.
Muscular endurance: The ability of a muscle or group of muscles to exert force repeatedly against resistance.
Motor (muscle) planning: The ability to move the body with appropriate sequencing and timing to perform bodily movements with refined control.
Motor learning: A change in motor (muscle) behavior resulting from practice or past experience.
Postural control: The ability to stabilize the trunk and neck to enable coordination of other limbs.
Sensory processing: Accurate registration, interpretation, and response to sensory stimulation in the environment and one’s own body.
Body awareness: Knowing body parts and understanding the body’s movement in space in relation to other limbs and objects.
Balance: The ability to maintain position whether that is static, dynamic (moving), or rotational.
Coordination: Ability to integrate multiple movements into efficient movement.
Crossing Mid-line: The ability to cross the imaginary line running from the child’s nose to the pelvis that divides the body into left and right sides.
Proprioception: This is information that the brain receives from our muscles and joints to make us aware of body position and body movement.
Muscle Tone: The resting muscle tension of a muscle which is the continuous and passive partial contraction of the muscles.
How can you tell if my child has problems with gross motor skills?
If a child has difficulties with gross motor skills they might:
Be late in reaching developmental milestones (i.e. sit, crawl, walk, run and hop).
Move stiffly and lacks fluid body movement or alternatively looks awkward and appears clumsy.
Avoid physical activity.
Participate in physical activity for only short periods (have low endurance).
Cannot maintain an upright posture when sitting on a mat or at a tabletop.
Be unable to perform the same skills as their peers (e.g. catch, kick, hop and jump).
Appear less skillful than their peers in sports.
Be unable to follow multiple-step instructions to complete a physical task (e.g. obstacle course).
Be unable to plan and correctly sequence events or steps in a process (e.g. step forward before throwing).
Fail to perform movements safely (e.g. climbing).
Need to put in more effort than their peers to complete a task.
Tire frequently with physical activity.
Lose previously mastered skills if they do not keep practicing them.
Be unable to ‘generalize’ or transfer a skill (use the same skill in a different setting/way) (e.g. can easily change between throwing a big/heavy ball to a light/small ball).
What other problems can occur when a child has gross motor difficulties?
If a child has gross motor difficulties, they might also have difficulties with:
Drawing and pencil skills lacking in a skillful outcome.
Writing and drawing for long periods of time.
Activities of Daily Living (dressing independently, holding and using cutlery).
Maintaining posture while sitting on the floor or at a table.
Low energy levels.
Seem tired or lethargic and take longer to respond to stimuli around them.
Sensory processing (responding appropriately to the environment).
Chewing and swallowing food.
Dribbling inappropriately.
Demonstrate poor articulation of sounds.
Difficulties with manipulation of small toys and utensils.
What can be done to improve gross motor skills?
Improve attention to task and alertness levels in readiness to respond quickly when they lose their balance and to respond to changes in the environment around them.
Increase Core strength: Strengthen the ‘core’ (namely the large central muscles) of the body to provide greater body (especially trunk) stability.
Simplify specific physical skills into one or two-step components to teach at a time. Then gradually add together components until the skill is able to be performed in its entirety (e.g. skipping – start with a step, then a hop).
Gradually increase duration and intensity of activity to increase endurance.
Improve sensory processing to ensure appropriate attention and arousal to attempt the tasks, as well as ensuring the body is receiving and interpreting the correct messages from the muscles in terms of their position, their relationship to each other, the speed at which they move, and how much force they are using.
A multi-sensory approach (using as many of the 7 senses) to learn new skills will ensure a child has the best chance of learning appropriate strategies to respond to a physical demand or challenge.
Cognitive planning strategies can be used to talk the child through tasks (e.g. ‘Always point to where you are aiming’).
Task analysis to assist with chunking of information and backward chaining (i.e. learning small parts of a task at a time).
Develop the underlying skills necessary to support whole body (gross motor) skills, such as providing activities to support:
What activities can help improve gross motor skills?
Hop Scotch for hopping, or other games that encourage direct task/skill practice.
Simon Says for body awareness and movement planning (praxis).
Wheelbarrow walking races for upper body strength and postural or trunk control.
Unstable surfaces: Walking/climbing over unstable surfaces (e.g. large pillows) as it requires a lot of effort and increases overall body strength.
Catching and balancing: Standing with one foot on a ball while catching another ball (encourages balance while practicing catching and throwing).
Large balls: Begin catching with a large ball/balloon and only after the skill is mastered, move to a smaller sized ball.
Obstacle courses: to combine lots of gross motor skills together into one practice.
Playground climbing and swinging.
Swimming
Why should I seek therapy if I notice difficulties with gross motor skills in my child?
Therapeutic intervention to help a child with gross motor difficulties is important to:
Increase your child’s confidence in gross motor activities (e.g. playing on the playground, running, jumping).
Enhance their self-esteem (so they aren’t ostracized or picked last for sports teams due to their physical ability skill challenges).
Increase sporting ability and confidence to engage in sports. Participating in sport enables a child to enrich their lives with positive people and develop strong friendships.
Help your child develop the strength and endurance to manage the physical needs of a full school day.
Provide your child with a strong base of support so that they are better able to use their arms and hands for fine motor skills (such as manipulating small objects, such as pencils, scissors, keys, buttons and zips).
If left untreated what can difficulties with gross motor skills lead to?
When children have difficulties with gross motor skills, they might also have difficulties with:
Managing a full school day due to poor strength and endurance.
Poor self-esteem when they realise their skills do not match their peers.
Bullying when others become more aware of a child’s difficulties.
Poor fine motor skills (e.g. writing, drawing and cutting) due to poor core stability, meaning they do not have a strong base to support the use of their arms and hands.
What type of therapy is recommended for gross motor skill difficulties?
If your child has difficulties with gross motor skills, it is recommended they consult an Occupational Therapist.
It may also be appropriate to consult a Physiotherapy for gross motor skills. It is important to acknowledge however that in many (but not all) paediatric cases, there is a large overlap in the skills addressed by Physiotherapy and Occupational Therapy.
A motor skill is a learned ability to cause a predetermined movement outcome with maximum certainty. Motor learning is the relatively permanent change in the ability to perform a skill as a result of practice or experience. Performance is an act of executing a motor skill. The goal of motor skill is to optimize the ability to perform the skill at the rate of success, precision, and to reduce the energy consumption required for performance. Continuous practice of a specific motor skill will result in greatly improved performance.
Motor activity is represented by several behaviors (e.g., ambulation, grooming, rearing, sniffing) that involve coordinated involvement of sensory, motor, and associative processes. Motor activity testing often is performed in a novel environment using an automated detection system. Rodents may exhibit a substantial diurnal cyclicity in their level of spontaneous motor activity that must be considered when designing test batteries and interpreting data. Motor activity changes may result from CNS and/or PNS damage.
Types of motor skills
Gross motor skills require the use of large muscle groups to perform tasks like walking, balancing, and crawling. The skill required is not extensive and therefore are usually associated with continuous tasks. Much of the development of these skills occurs during early childhood. The performance level of gross motor skills remains unchanged after periods of non-use.[rx] Gross motor skills can be further divided into two subgroups: oculomotor skills, such as running, jumping, sliding, and swimming; and object-control skills such as throwing, catching, and kicking. Motor skills are movements and actions of the muscles. Typically, they are categorized into eighteen groups:
Fine motor skills – requires the use of smaller muscle groups to perform smaller movements with the wrists, hands, fingers, and feet, and toes. These tasks are precise in nature, like playing the piano, writing carefully, and blinking. Generally, there is a retention loss of fine motor skills over a period of non-use. Discrete tasks usually require more fine motor skills than gross motor skills.[rx] Fine motor skills can become impaired. Some reasons for impairment could be an injury, illness, stroke, congenital deformities, cerebral palsy, and developmental disabilities. Problems with the brain, spinal cord, peripheral nerves, muscles, or joints can also have an effect on fine motor skills, and decrease control.[rx]
Development
Motor skills develop in different parts of a body along three principles:
Cephalocaudal – development from head to foot. The head develops earlier than the hand. Similarly, hand coordination develops before the coordination of the legs and feet. For example, an infant is able to follow something with their eyes before they can touch or grab it.[rx]
Proximodistal – the movement of limbs that are closer to the body develop before the parts that are further away, such as a baby learns to control the upper arm before the hands or fingers. Fine movements of the fingers are the last to develop in the body.[rx]
Gross to specific – a pattern in which larger muscle movements develop before finer movements. For example, a child only being able to pick up large objects, to then picking up an object that is small between the thumb and fingers. The earlier movements involve larger groups of muscles, but as the child grows finer movements become possible and specific things can be achieved.[rx]
In children, a critical period for the acquisition of motor skills is preschool years (ages 3–5), as fundamental neuroanatomic structure shows significant development, elaboration, and myelination over the course of this period.[rx] Many factors contribute to the rate at which children develop their motor skills. Unless afflicted with a severe disability, children are expected to develop a wide range of basic movement abilities and motor skills.[rx] Motor development progresses in seven stages throughout an individual’s life: reflexive, rudimentary, fundamental, sports skill, growth and refinement, peak performance, and regression. Development is age-related but is not age-dependent. In regard to age, it is seen that typical developments are expected to attain gross motor skills used for postural control and vertical mobility by 5 years of age.[rx]
There are six aspects of development:
Qualitative – changes in movement-process results in changes in movement-outcome.
Sequential – certain motor patterns precede others.
Cumulative – current movements are built on previous ones.
Directional – cephalocaudal or proximodistal
Multifactorial – numerous-factors impact
Individual – dependent on each person
In the childhood stages of development, gender differences can greatly influence motor skills. In the article “An Investigation of Age and Gender Differences in Preschool Children’s Specific Motor Skills”, girls scored significantly higher than boys on visual motor and graphomotor tasks. The results from this study suggest that girls attain manual dexterity earlier than boys.[rx] Variability of results in the tests can be attributed towards the multiplicity of different assessment tools used.[rx] Furthermore, gender differences in motor skills are seen to be affected by environmental factors. In essence, “parents and teachers often encourage girls to engage in [quiet] activities requiring fine motor skills, while they promote boys’ participation in dynamic movement actions”.[rx] In the journal article “Gender Differences in Motor Skill Proficiency From Childhood to Adolescence” by Lisa Barrett, the evidence for gender-based motor skills is apparent. In general, boys are more skillful in object control and object manipulation skills. These tasks include throwing, kicking, and catching skills. These skills were tested and concluded that boys perform better with these tasks. There was no evidence for the difference in locomotor skill between the genders, but both are improved in the intervention of physical activity. Overall, the predominance of development was on balance skills (gross motor) in boys and manual skills (fine motor) in girls.[rx]
Components of development
Growth – increase in the size of the body or its parts as the individual progresses toward maturity (quantitative structural changes)
Maturation – refers to qualitative changes that enable one to progress to higher levels of functioning; it is primarily innate
Experience or learning – refers to factors within the environment that may alter or modify the appearance of various developmental characteristics through the process of learning
Adaptation – refers to the complex interplay or interaction between forces within the individual (nature) and the environment (nurture)
Influences on development
Stress and arousal – stress and anxiety is the result of an imbalance between demand and the capacity of the individual. In this context, arousal defines the amount of interest in the skill. The optimal performance level is moderate stress or arousal.[rx] An example of an insufficient arousal state is an overqualified worker performing repetitive jobs. An example of an excessive stress level is an anxious pianist at a recital. The “Practice-Specificity-Based Model of Arousal” (Movahedi, 2007) holds that, for best and peak performances to occur, motor task performers need only to create an arousal level similar to the one they have experienced throughout training sessions. For peak performance, performers do not need to have high or low arousal levels. It is important that they create the same level of arousal throughout training sessions and competition. In other words, high levels of arousal can be beneficial if athletes experience such heightened levels of arousal during some consecutive training sessions. Similarly, low levels of arousal can be beneficial if athletes experience such low levels of arousal during some consecutive training sessions.[rx]
Fatigue – the deterioration of performance when a stressful task is continued for a long time, similar to the muscular fatigue experienced when exercising rapidly or over a long period. Fatigue is caused by over-arousal. Fatigue impacts an individual in many ways: perceptual changes in which visual acuity or awareness drops, slowing of performance (reaction times or movement speed), irregularity of timing, and disorganization of performance.
Vigilance – the effect of the loss of vigilance is the same as fatigue, but is instead caused by a lack of arousal. Some tasks include actions that require little work and high attention.[rx]
Gender – gender plays an important role in the development of the child. Girls are more likely to be seen performing fine stationary visual motor skills, whereas boys predominantly exercise object-manipulation skills. While researching motor development in preschool-aged children, girls were more likely to be seen performing skills such as skipping, hopping, or skills with the use of hands only. Boys were seen to perform gross skills such as kicking or throwing a ball or swinging a bat. There are gender-specific differences in qualitative throwing performance, but not necessarily in quantitative throwing performance. Male and female athletes demonstrated similar movement patterns in humerus and forearm actions but differed in trunk, stepping, and backswing actions.
Stages of motor learning
Motor learning is a change, resulting from practice. It often involves improving the accuracy of movements both simple and complex as one’s environment changes. Motor learning is a relatively permanent skill as the capability to respond appropriately is acquired and retained.[rx]
The stages of motor learning are the cognitive phase, the associative phase, and the autonomous phase.
Cognitive phase – When a learner is new to a specific task, the primary thought process starts with, “What needs to be done?” Considerable cognitive activity is required so that the learner can determine appropriate strategies to adequately reflect the desired goal. Good strategies are retained and inefficient strategies are discarded. The performance is greatly improved in a short amount of time.
Associative phase – The learner has determined the most effective way to do the task and starts to make subtle adjustments in performance. Improvements are more gradual and movements become more consistent. This phase can last for a long time. The skills in this phase are fluent, efficient, and aesthetically pleasing.
Autonomous phase – This phase may take several months to years to reach. The phase is dubbed “autonomous” because the performer can now “automatically” complete the task without having to pay any attention to performing it. Examples include walking and talking or sight-reading while doing simple arithmetic.[rx]
Peripheral Motor Endings
A neuromuscular junction exists between the axon terminal and the motor endplate of a muscle fiber where neurotransmitters are released.
Key Points
A neuromuscular junction is a junction between the axon terminal of a motor neuron and the plasma membrane of the motor endplate of a muscle fiber.
With the arrival of an action potential to the axon terminal, voltage-dependent calcium channels open, and calcium infuses into the cell. The influx of calcium ions causes the docking of acetylcholine-containing vesicles at the plasma membrane of the neuron and exocytosis into the synaptic cleft.
Acetylcholine is a neurotransmitter contained in the vesicles of the pre-synaptic neuron. It is released into the synaptic cleft and activates nicotinic acetylcholine receptors on the motor endplate, and causes local motor endplate depolarization, also known as the endplate potential (EPP).
The endplate potential propagates across the surface of the muscle fiber, causing the fiber to contract and continuing the process of excitation-contraction coupling.
Key Terms
axon: A nerve fiber that is a long, slender projection of a nerve cell that conducts nerve impulses away from the body of the cell to a synapse.
voltage-dependent calcium channels: A group of voltage-gated ion channels found in excitable cells (e.g., muscle, glial cells, neurons, etc. ) with permeability to the ion Ca2+.
presynaptic neuron: The neuron that releases neurotransmitters into the synaptic cleft.
nicotinic acetylcholine receptor: These are cholinergic receptors that form ligand-gated ion channels in the plasma membranes of certain neurons and on the postsynaptic side of the neuromuscular junction.
synaptic cleft: A small space between neurons.
excitation-contraction coupling: This process is fundamental to muscle physiology, whereby the electrical stimulus is usually an action potential and the mechanical response is a contraction.
A neuromuscular junction is the synapse or junction of the axon terminal of a motor neuron with the motor end plate, as shown in Figures 1 and 2. The highly excitable region of muscle fiber plasma membrane is responsible for initiation of action potentials across the muscle’s surface, ultimately causing the muscle to contract.
Invertebrates, the signal passes through the neuromuscular junction via the neurotransmitter acetylcholine.
Figure 1. Detailed view of a neuromuscular junction: Detailed view of a neuromuscular junction: 1) Presynaptic terminal; 2) Sarcolemma; 3) Synaptic vesicle; 4) Nicotinic acetylcholine receptor; 5) Mitochondrion.
Figure 2. Neuromuscular junction: Electron micrograph showing a cross section through the neuromuscular junction. T is the axon terminal and M is the muscle fiber. The arrow shows junctional folds with basal lamina. Postsynaptic densities are visible on the tips between the folds. Scale is 0.3 µm.
Upon the arrival of an action potential at the presynaptic neuron terminal, voltage-dependent calcium channels open and Ca2+ ions flow from the extracellular fluid into the presynaptic neuron’s cytosol. This influx of Ca2+ causes neurotransmitter-containing vesicles to dock and fuse to the presynaptic neuron’s cell membrane, which results in the emptying of the vesicle’s contents (acetylcholine) into the synaptic cleft; this process is known as exocytosis.
Acetylcholine diffuses into the synaptic cleft and binds to the nicotinic acetylcholine receptors located on the motor endplate.
These receptors open to allow sodium ions to flow in and potassium ions to flow out of the muscle’s cytosol, producing a local depolarization of the motor endplate, known as an end-plate potential (EPP). This depolarization spreads across the surface of the muscle fiber and continues the excitation-contraction coupling to contract the muscle.
The action potential spreads through the muscle fiber’s network of T-tubules, depolarizing the inner portion of the muscle fiber. The depolarization activates L-type, voltage-dependent calcium channels (dihydropyridine receptors) in the T-tubule membrane, which are in close proximity to calcium-release channels (ryanodine receptors) in the adjacent sarcoplasmic reticulum.
As intracellular calcium levels rise, the motor proteins responsible for the contractile response are able to interact, as shown in Figure 3, to form cross-bridges and undergo shortening.
CLINICAL EXAMPLE of Motor Activity
Myasthenia gravis is an autoimmune disorder in which circulating antibodies block the nicotinic acetylcholine receptors on the motor endplate of the neuromuscular junction. This blockage of acetylcholine receptors causes muscle weakness, often first exhibiting drooping eyelids and expanding to include overall muscle weakness and fatigue.
The effects of myasthenia gravis illustrate the importance of effective and functioning neuromuscular junctions for communication between neurons and muscles to allow contraction and relaxation of muscle fibers.
Figure 3. Muscle contraction and actin-myosin interactions: Skeletal muscle contracts following activation by an action potential. The binding of acetylcholine at the motor endplate leads to intracellular calcium release and interactions between myofibrils to elicit contraction.
Overview of Motor Integration
A motor unit is comprised of a single alpha-motor neuron and all the muscle fibers it innervates.
Key Points
Motor units contain muscle fibers of all the same type; these may be many muscle fibers (as in the case of quadriceps) or a few muscle fibers (as in the case of the muscles that control eye movement).
Groups of motor units often work together to coordinate the contractions of a single muscle; all of the motor units that subserve a single muscle are considered a motor unit pool.
Motor units are generally recruited in order of smallest to largest (from fewest fibers to most fibers) as contraction increases. This is known as Henneman’s Size Principle.
The smaller the motor unit, the more precise the action of the muscle.
Key Terms
Henneman’s size principle: According to this principle, motor unit recruitment is always in the same order from smallest to largest motor unit. Additionally, the motor unit action potential is an all-or-none phenomenon—once the recruitment threshold (the stimulus intensity at which a motor unit begins to fire) is reached, it fires fully.
alpha motor neuron: Alpha motor neurons (α-MNs) are large, lower motor neurons of the brainstem and spinal cord. They innervate the extrafusal muscle fibers of skeletal muscle and are directly responsible for initiating their contraction. Alpha motor neurons are distinct from gamma motor neurons, which innervate the intrafusal muscle fibers of muscle spindles.
motor unit: A neuron with its associated muscle fibers.
Rectus femoris: The rectus femoris muscle is one of the four quadriceps muscles of the human body. These muscles may have as many as a thousand fibers in each motor unit.
A motor unit consists of a single alpha motor neuron and all of the corresponding muscle fibers it innervates; all of these fibers will be of the same type (either fast twitch or slow-twitch).
When a motor unit is activated, all of its fibers contract. Groups of motor units often work together to coordinate the contractions of a single muscle. All of the motor units that subserve a single muscle are considered a motor unit pool.
The number of muscle fibers within each unit can vary. Thigh muscles, for example, can have a thousand fibers in each unit, eye muscles might have ten. In general, the number of muscle fibers innervated by a motor unit is a function of a muscle’s need for refined motion.
The smaller the motor unit, the more precise the action of the muscle. Muscles requiring more refined motion are innervated by motor units that synapse with fewer muscle fibers.
Motor unit recruitment is the progressive activation of a muscle by the successive recruitment of motor units to accomplish increasing gradations of contractile strength. The activation of more motor neurons will result in more muscle fibers being activated, and therefore a stronger muscle contraction.
Motor unit recruitment is a measure of how many motor neurons are activated in a particular muscle. It is therefore a measure of how many muscle fibers of that muscle are activated. The higher the recruitment, the stronger the muscle contraction will be.
Motor units are generally recruited in order of smallest to largest (from fewest fibers to most fibers) as contraction increases. This is known as Henneman’s Size Principle.
The orbicularis oris (eye) muscle: These small motor units may contain only 10 fibers per motor unit. The more precise the action of the muscle, the fewer fibers innervated.
Motor Unit Categories
Motor units are generally categorized based upon the similarities between several factors such as:
Physiological
Contraction speed in isometric contractions:
Rate of rise of force.
Time to peak of a twitch contraction (response to a single nerve impulse).
Biochemical
Histochemical (the oldest form of biochemical fiber typing):
Glycolytic enzyme activity.
Oxidative enzyme activity.
Sensitivity of myosin ATPase to acid and alkali.
Immunohistochemical (a more recent form of fiber typing):
Myosin heavy chain (MHC).
Myosin light chain—alkali (MLC1).
Myosin light chain—regulatory (MLC2).
FUNCTIONAL EXAMPLE
The quadriceps muscles contain many thousands of muscle fibers in general, both slow and fast-twitch, to produce sufficient force for body movements such as standing, walking, running, and jumping.
The eye muscles, on the other hand, contain few muscle fibers, enabling them to be more exact in movement so that vision is not jumpy, but consequently, they produce very little force.
Clothing fastenings – buttons that are supposed to go into buttonholes or loops, zippers, snaps, ties, collar stays or button-down collars, and shoelaces
Using tableware – a knife, fork, or spoon, both for personal use and the utensils used with serving dishes
Opening and closing food containers – screw tops, carton spouts, plastic leftover containers, and boxes
Twisting doorknobs – also locks, slide chains, and keys
Personal care – shaving, brushing teeth, doing hair, applying makeup (especially eyeliner), putting on post-back earrings, inserting contact lenses, bathing, showering, and using the toilet
Handwriting – holding a pen or pencil, printing vs. cursive writing, size of individual letters, consistent size of letters, and writing in straight lines
Needlework – threading a needle, making the correct size and consistent stitches, casting on/off knitting, maintaining proper thread/yarn tension
Video gaming – thumbing the joystick, pressing keys in rapid succession, and watching the screen and operating the controller at the same time
Operating other electronic equipment – using a keyboard, a telephone or alarm system touchpad
Musical instruments – coordinating both hands to play the instrument, putting fingers in the right places on strings, over holes, or on keys
Children show fine motor coordination and the skills that go with them as they grow older and develop.
Kids develop gross motor skills at different rates. But when young kids have trouble with those skills, it can make gross motor activities like running, jumping, and throwing difficult. If your child’s gross motor skills need a little extra help, try these fun activities.
Trampolines – Using a trampoline is a great activity to improve balance. It can also be part of a sensory diet. Indoor trampoline parks are a fun place to socialize with other kids. But if you’re not confident your child will follow directions or if your child isn’t old enough for a trampoline park, you can also get a mini-trampoline for supervised use at home. Keep in mind that it’s important to follow safety rules, like having a jump bar.
Hopscotch – Hopping and jumping require strong gross motor skills, balance, and coordination. Hopscotch is a simple way to practice those skills. (As a bonus, it can help practice number skills, too!) If you don’t have a sidewalk to draw on or a playground nearby, you can set up hallway hopscotch using painter’s tape.
Martial arts classes – Mаrtіаl аrtѕ trаіnіng is a good way to help kids develop strength in their arms and legs. Actions like kicking, punching, and grappling work to develop those core muscle groups. It can help kids with balance and knowing where their body is in space — motor skills that can be a problem for kids with sensory issues. Martial arts can have additional benefits for kids with ADHD, too.
Playground play – Playing on the playground can have many benefits for kids. Swinging on a swing set can help kids develop balance. It also helps them learn how to coordinate shifting their weight and moving their legs back and forth. You may also want to encourage your child to use “unstable” playground equipment like rope ladders and wobble bridges. While they can be scary before kids get used to them, they help work trunk muscles.
Balloon and bubble play – Balloons and bubbles are a unique way to build gross motor skills because you can’t predict where they’re going to go. Kids can chase bubbles and try to pop as many as possible. While chasing them, they have to run, jump, zigzag, and move in ways that require sudden shifts in balance and weight. The same goes for throwing and trying to catch or kick balloons. For more structured play, you can set up a game of balloon volleyball.
Tricycles, scooters, and pedal cars – Some kids who struggle with gross motor skills may learn to ride a trike or bike later than their peers. But there are alternatives they can use to get places and practice balance. Some tricycles come with handles so you can push while your child practices pedaling. Or you could invest in a sturdy scooter or a pedal car. They’re all stepping stones to riding a bike. Once your child gets the hang of it, you can even set up an obstacle course or draw a track with chalk. (Just don’t forget the helmet!)
Dancing – Whether it’s a dance class or an indoor dance party, dancing is good gross motor practice. It helps kids develop balance, coordination, and motor sequencing skills. It also helps build your child’s awareness of rhythm. For little kids, try using songs with lyrics that add movement, like “I’m a Little Teapot” or “The Hokey Pokey.”
Obstacle courses – Obstacle courses get kids moving and give them a goal to accomplish. For an indoor course, use furniture, pillows, and blankets to create areas to crawl on, under, and through. Outdoors, you can use things like hula-hoops to jump in and out of, jumping jacks, belly crawling, bear walking, and other creative movements that challenge your child to balance, crawl, jump, and run.
The motor activity involves movement quality and quantity that both influence and are influenced by states of arousal. Imbedded in activity levels are the qualitative aspects of movement that include muscle tone, posture, coordination, symmetry, strength, purposefulness, and planning, or praxis.
Motor activity is represented by several behaviors (e.g., ambulation, grooming, rearing, sniffing) that involve coordinated involvement of sensory, motor, and associative processes. Motor activity testing often is performed in a novel environment using an automated detection system. Rodents may exhibit a substantial diurnal cyclicity in their level of spontaneous motor activity that must be considered when designing test batteries and interpreting data. Motor activity changes may result from CNS and/or PNS damage.
Types of motor skills
Gross motor skills require the use of large muscle groups to perform tasks like walking, balancing, and crawling. The skill required is not extensive and therefore are usually associated with continuous tasks. Much of the development of these skills occurs during early childhood. The performance level of gross motor skills remains unchanged after periods of non-use.[rx] Gross motor skills can be further divided into two subgroups: oculomotor skills, such as running, jumping, sliding, and swimming; and object-control skills such as throwing, catching, and kicking. Motor skills are movements and actions of the muscles. Typically, they are categorized into eighteen groups:
Fine motor skills – requires the use of smaller muscle groups to perform smaller movements with the wrists, hands, fingers, and feet, and toes. These tasks are precise in nature, like playing the piano, writing carefully, and blinking. Generally, there is a retention loss of fine motor skills over a period of non-use. Discrete tasks usually require more fine motor skills than gross motor skills.[rx] Fine motor skills can become impaired. Some reasons for impairment could be an injury, illness, stroke, congenital deformities, cerebral palsy, and developmental disabilities. Problems with the brain, spinal cord, peripheral nerves, muscles, or joints can also have an effect on fine motor skills, and decrease control.[rx]
Development
Motor skills develop in different parts of a body along three principles:
Cephalocaudal – development from head to foot. The head develops earlier than the hand. Similarly, hand coordination develops before the coordination of the legs and feet. For example, an infant is able to follow something with their eyes before they can touch or grab it.[rx]
Proximodistal – the movement of limbs that are closer to the body develop before the parts that are further away, such as a baby learns to control the upper arm before the hands or fingers. Fine movements of the fingers are the last to develop in the body.[rx]
Gross to specific – a pattern in which larger muscle movements develop before finer movements. For example, a child only being able to pick up large objects, to then picking up an object that is small between the thumb and fingers. The earlier movements involve larger groups of muscles, but as the child grows finer movements become possible and specific things can be achieved.[rx]
In children, a critical period for the acquisition of motor skills is preschool years (ages 3–5), as fundamental neuroanatomic structure shows significant development, elaboration, and myelination over the course of this period.[rx] Many factors contribute to the rate at which children develop their motor skills. Unless afflicted with a severe disability, children are expected to develop a wide range of basic movement abilities and motor skills.[rx] Motor development progresses in seven stages throughout an individual’s life: reflexive, rudimentary, fundamental, sports skill, growth and refinement, peak performance, and regression. Development is age-related but is not age-dependent. In regard to age, it is seen that typical developments are expected to attain gross motor skills used for postural control and vertical mobility by 5 years of age.[rx]
There are six aspects of development:
Qualitative – changes in movement-process results in changes in movement-outcome.
Sequential – certain motor patterns precede others.
Cumulative – current movements are built on previous ones.
Directional – cephalocaudal or proximodistal
Multifactorial – numerous-factors impact
Individual – dependent on each person
In the childhood stages of development, gender differences can greatly influence motor skills. In the article “An Investigation of Age and Gender Differences in Preschool Children’s Specific Motor Skills”, girls scored significantly higher than boys on visual motor and graphomotor tasks. The results from this study suggest that girls attain manual dexterity earlier than boys.[rx] Variability of results in the tests can be attributed towards the multiplicity of different assessment tools used.[rx] Furthermore, gender differences in motor skills are seen to be affected by environmental factors. In essence, “parents and teachers often encourage girls to engage in [quiet] activities requiring fine motor skills, while they promote boys’ participation in dynamic movement actions”.[rx] In the journal article “Gender Differences in Motor Skill Proficiency From Childhood to Adolescence” by Lisa Barrett, the evidence for gender-based motor skills is apparent. In general, boys are more skillful in object control and object manipulation skills. These tasks include throwing, kicking, and catching skills. These skills were tested and concluded that boys perform better with these tasks. There was no evidence for the difference in locomotor skill between the genders, but both are improved in the intervention of physical activity. Overall, the predominance of development was on balance skills (gross motor) in boys and manual skills (fine motor) in girls.[rx]
Components of development
Growth – increase in the size of the body or its parts as the individual progresses toward maturity (quantitative structural changes)
Maturation – refers to qualitative changes that enable one to progress to higher levels of functioning; it is primarily innate
Experience or learning – refers to factors within the environment that may alter or modify the appearance of various developmental characteristics through the process of learning
Adaptation – refers to the complex interplay or interaction between forces within the individual (nature) and the environment (nurture)
Influences on development
Stress and arousal – stress and anxiety is the result of an imbalance between demand and the capacity of the individual. In this context, arousal defines the amount of interest in the skill. The optimal performance level is moderate stress or arousal.[rx] An example of an insufficient arousal state is an overqualified worker performing repetitive jobs. An example of an excessive stress level is an anxious pianist at a recital. The “Practice-Specificity-Based Model of Arousal” (Movahedi, 2007) holds that, for best and peak performances to occur, motor task performers need only to create an arousal level similar to the one they have experienced throughout training sessions. For peak performance, performers do not need to have high or low arousal levels. It is important that they create the same level of arousal throughout training sessions and competition. In other words, high levels of arousal can be beneficial if athletes experience such heightened levels of arousal during some consecutive training sessions. Similarly, low levels of arousal can be beneficial if athletes experience such low levels of arousal during some consecutive training sessions.[rx]
Fatigue – the deterioration of performance when a stressful task is continued for a long time, similar to the muscular fatigue experienced when exercising rapidly or over a long period. Fatigue is caused by over-arousal. Fatigue impacts an individual in many ways: perceptual changes in which visual acuity or awareness drops, slowing of performance (reaction times or movement speed), irregularity of timing, and disorganization of performance.
Vigilance – the effect of the loss of vigilance is the same as fatigue, but is instead caused by a lack of arousal. Some tasks include actions that require little work and high attention.[rx]
Gender – gender plays an important role in the development of the child. Girls are more likely to be seen performing fine stationary visual motor skills, whereas boys predominantly exercise object-manipulation skills. While researching motor development in preschool-aged children, girls were more likely to be seen performing skills such as skipping, hopping, or skills with the use of hands only. Boys were seen to perform gross skills such as kicking or throwing a ball or swinging a bat. There are gender-specific differences in qualitative throwing performance, but not necessarily in quantitative throwing performance. Male and female athletes demonstrated similar movement patterns in humerus and forearm actions but differed in trunk, stepping, and backswing actions.
Stages of motor learning
Motor learning is a change, resulting from practice. It often involves improving the accuracy of movements both simple and complex as one’s environment changes. Motor learning is a relatively permanent skill as the capability to respond appropriately is acquired and retained.[rx]
The stages of motor learning are the cognitive phase, the associative phase, and the autonomous phase.
Cognitive phase – When a learner is new to a specific task, the primary thought process starts with, “What needs to be done?” Considerable cognitive activity is required so that the learner can determine appropriate strategies to adequately reflect the desired goal. Good strategies are retained and inefficient strategies are discarded. The performance is greatly improved in a short amount of time.
Associative phase – The learner has determined the most effective way to do the task and starts to make subtle adjustments in performance. Improvements are more gradual and movements become more consistent. This phase can last for a long time. The skills in this phase are fluent, efficient, and aesthetically pleasing.
Autonomous phase – This phase may take several months to years to reach. The phase is dubbed “autonomous” because the performer can now “automatically” complete the task without having to pay any attention to performing it. Examples include walking and talking or sight-reading while doing simple arithmetic.[rx]
Peripheral Motor Endings
A neuromuscular junction exists between the axon terminal and the motor endplate of a muscle fiber where neurotransmitters are released.
Key Points
A neuromuscular junction is a junction between the axon terminal of a motor neuron and the plasma membrane of the motor endplate of a muscle fiber.
With the arrival of an action potential to the axon terminal, voltage-dependent calcium channels open, and calcium infuses into the cell. The influx of calcium ions causes the docking of acetylcholine-containing vesicles at the plasma membrane of the neuron and exocytosis into the synaptic cleft.
Acetylcholine is a neurotransmitter contained in the vesicles of the pre-synaptic neuron. It is released into the synaptic cleft and activates nicotinic acetylcholine receptors on the motor endplate, and causes local motor endplate depolarization, also known as the endplate potential (EPP).
The endplate potential propagates across the surface of the muscle fiber, causing the fiber to contract and continuing the process of excitation-contraction coupling.
Key Terms
axon: A nerve fiber that is a long, slender projection of a nerve cell that conducts nerve impulses away from the body of the cell to a synapse.
voltage-dependent calcium channels: A group of voltage-gated ion channels found in excitable cells (e.g., muscle, glial cells, neurons, etc. ) with permeability to the ion Ca2+.
presynaptic neuron: The neuron that releases neurotransmitters into the synaptic cleft.
nicotinic acetylcholine receptor: These are cholinergic receptors that form ligand-gated ion channels in the plasma membranes of certain neurons and on the postsynaptic side of the neuromuscular junction.
synaptic cleft: A small space between neurons.
excitation-contraction coupling: This process is fundamental to muscle physiology, whereby the electrical stimulus is usually an action potential and the mechanical response is a contraction.
A neuromuscular junction is the synapse or junction of the axon terminal of a motor neuron with the motor end plate, as shown in Figures 1 and 2. The highly excitable region of muscle fiber plasma membrane is responsible for initiation of action potentials across the muscle’s surface, ultimately causing the muscle to contract.
Invertebrates, the signal passes through the neuromuscular junction via the neurotransmitter acetylcholine.
Figure 1. Detailed view of a neuromuscular junction: Detailed view of a neuromuscular junction: 1) Presynaptic terminal; 2) Sarcolemma; 3) Synaptic vesicle; 4) Nicotinic acetylcholine receptor; 5) Mitochondrion.
Figure 2. Neuromuscular junction: Electron micrograph showing a cross section through the neuromuscular junction. T is the axon terminal and M is the muscle fiber. The arrow shows junctional folds with basal lamina. Postsynaptic densities are visible on the tips between the folds. Scale is 0.3 µm.
Upon the arrival of an action potential at the presynaptic neuron terminal, voltage-dependent calcium channels open and Ca2+ ions flow from the extracellular fluid into the presynaptic neuron’s cytosol. This influx of Ca2+ causes neurotransmitter-containing vesicles to dock and fuse to the presynaptic neuron’s cell membrane, which results in the emptying of the vesicle’s contents (acetylcholine) into the synaptic cleft; this process is known as exocytosis.
Acetylcholine diffuses into the synaptic cleft and binds to the nicotinic acetylcholine receptors located on the motor endplate.
These receptors open to allow sodium ions to flow in and potassium ions to flow out of the muscle’s cytosol, producing a local depolarization of the motor endplate, known as an end-plate potential (EPP). This depolarization spreads across the surface of the muscle fiber and continues the excitation-contraction coupling to contract the muscle.
The action potential spreads through the muscle fiber’s network of T-tubules, depolarizing the inner portion of the muscle fiber. The depolarization activates L-type, voltage-dependent calcium channels (dihydropyridine receptors) in the T-tubule membrane, which are in close proximity to calcium-release channels (ryanodine receptors) in the adjacent sarcoplasmic reticulum.
As intracellular calcium levels rise, the motor proteins responsible for the contractile response are able to interact, as shown in Figure 3, to form cross-bridges and undergo shortening.
CLINICAL EXAMPLE of Motor Activity
Myasthenia gravis is an autoimmune disorder in which circulating antibodies block the nicotinic acetylcholine receptors on the motor endplate of the neuromuscular junction. This blockage of acetylcholine receptors causes muscle weakness, often first exhibiting drooping eyelids and expanding to include overall muscle weakness and fatigue.
The effects of myasthenia gravis illustrate the importance of effective and functioning neuromuscular junctions for communication between neurons and muscles to allow contraction and relaxation of muscle fibers.
Figure 3. Muscle contraction and actin-myosin interactions: Skeletal muscle contracts following activation by an action potential. The binding of acetylcholine at the motor endplate leads to intracellular calcium release and interactions between myofibrils to elicit contraction.
Overview of Motor Integration
A motor unit is comprised of a single alpha-motor neuron and all the muscle fibers it innervates.
Key Points
Motor units contain muscle fibers of all the same type; these may be many muscle fibers (as in the case of quadriceps) or a few muscle fibers (as in the case of the muscles that control eye movement).
Groups of motor units often work together to coordinate the contractions of a single muscle; all of the motor units that subserve a single muscle are considered a motor unit pool.
Motor units are generally recruited in order of smallest to largest (from fewest fibers to most fibers) as contraction increases. This is known as Henneman’s Size Principle.
The smaller the motor unit, the more precise the action of the muscle.
Key Terms
Henneman’s size principle: According to this principle, motor unit recruitment is always in the same order from smallest to largest motor unit. Additionally, the motor unit action potential is an all-or-none phenomenon—once the recruitment threshold (the stimulus intensity at which a motor unit begins to fire) is reached, it fires fully.
alpha motor neuron: Alpha motor neurons (α-MNs) are large, lower motor neurons of the brainstem and spinal cord. They innervate the extrafusal muscle fibers of skeletal muscle and are directly responsible for initiating their contraction. Alpha motor neurons are distinct from gamma motor neurons, which innervate the intrafusal muscle fibers of muscle spindles.
motor unit: A neuron with its associated muscle fibers.
Rectus femoris: The rectus femoris muscle is one of the four quadriceps muscles of the human body. These muscles may have as many as a thousand fibers in each motor unit.
A motor unit consists of a single alpha motor neuron and all of the corresponding muscle fibers it innervates; all of these fibers will be of the same type (either fast twitch or slow-twitch).
When a motor unit is activated, all of its fibers contract. Groups of motor units often work together to coordinate the contractions of a single muscle. All of the motor units that subserve a single muscle are considered a motor unit pool.
The number of muscle fibers within each unit can vary. Thigh muscles, for example, can have a thousand fibers in each unit, eye muscles might have ten. In general, the number of muscle fibers innervated by a motor unit is a function of a muscle’s need for refined motion.
The smaller the motor unit, the more precise the action of the muscle. Muscles requiring more refined motion are innervated by motor units that synapse with fewer muscle fibers.
Motor unit recruitment is the progressive activation of a muscle by the successive recruitment of motor units to accomplish increasing gradations of contractile strength. The activation of more motor neurons will result in more muscle fibers being activated, and therefore a stronger muscle contraction.
Motor unit recruitment is a measure of how many motor neurons are activated in a particular muscle. It is therefore a measure of how many muscle fibers of that muscle are activated. The higher the recruitment, the stronger the muscle contraction will be.
Motor units are generally recruited in order of smallest to largest (from fewest fibers to most fibers) as contraction increases. This is known as Henneman’s Size Principle.
The orbicularis oris (eye) muscle: These small motor units may contain only 10 fibers per motor unit. The more precise the action of the muscle, the fewer fibers innervated.
Motor Unit Categories
Motor units are generally categorized based upon the similarities between several factors such as:
Physiological
Contraction speed in isometric contractions:
Rate of rise of force.
Time to peak of a twitch contraction (response to a single nerve impulse).
Biochemical
Histochemical (the oldest form of biochemical fiber typing):
Glycolytic enzyme activity.
Oxidative enzyme activity.
Sensitivity of myosin ATPase to acid and alkali.
Immunohistochemical (a more recent form of fiber typing):
Myosin heavy chain (MHC).
Myosin light chain—alkali (MLC1).
Myosin light chain—regulatory (MLC2).
FUNCTIONAL EXAMPLE
The quadriceps muscles contain many thousands of muscle fibers in general, both slow and fast-twitch, to produce sufficient force for body movements such as standing, walking, running, and jumping.
The eye muscles, on the other hand, contain few muscle fibers, enabling them to be more exact in movement so that vision is not jumpy, but consequently, they produce very little force.
Clothing fastenings – buttons that are supposed to go into buttonholes or loops, zippers, snaps, ties, collar stays or button-down collars, and shoelaces
Using tableware – a knife, fork, or spoon, both for personal use and the utensils used with serving dishes
Opening and closing food containers – screw tops, carton spouts, plastic leftover containers, and boxes
Twisting doorknobs – also locks, slide chains, and keys
Personal care – shaving, brushing teeth, doing hair, applying makeup (especially eyeliner), putting on post-back earrings, inserting contact lenses, bathing, showering, and using the toilet
Handwriting – holding a pen or pencil, printing vs. cursive writing, size of individual letters, consistent size of letters, and writing in straight lines
Needlework – threading a needle, making the correct size and consistent stitches, casting on/off knitting, maintaining proper thread/yarn tension
Video gaming – thumbing the joystick, pressing keys in rapid succession, and watching the screen and operating the controller at the same time
Operating other electronic equipment – using a keyboard, a telephone or alarm system touchpad
Musical instruments – coordinating both hands to play the instrument, putting fingers in the right places on strings, over holes, or on keys
Children show fine motor coordination and the skills that go with them as they grow older and develop.
Kids develop gross motor skills at different rates. But when young kids have trouble with those skills, it can make gross motor activities like running, jumping, and throwing difficult. If your child’s gross motor skills need a little extra help, try these fun activities.
Trampolines – Using a trampoline is a great activity to improve balance. It can also be part of a sensory diet. Indoor trampoline parks are a fun place to socialize with other kids. But if you’re not confident your child will follow directions or if your child isn’t old enough for a trampoline park, you can also get a mini-trampoline for supervised use at home. Keep in mind that it’s important to follow safety rules, like having a jump bar.
Hopscotch – Hopping and jumping require strong gross motor skills, balance, and coordination. Hopscotch is a simple way to practice those skills. (As a bonus, it can help practice number skills, too!) If you don’t have a sidewalk to draw on or a playground nearby, you can set up hallway hopscotch using painter’s tape.
Martial arts classes – Mаrtіаl аrtѕ trаіnіng is a good way to help kids develop strength in their arms and legs. Actions like kicking, punching, and grappling work to develop those core muscle groups. It can help kids with balance and knowing where their body is in space — motor skills that can be a problem for kids with sensory issues. Martial arts can have additional benefits for kids with ADHD, too.
Playground play – Playing on the playground can have many benefits for kids. Swinging on a swing set can help kids develop balance. It also helps them learn how to coordinate shifting their weight and moving their legs back and forth. You may also want to encourage your child to use “unstable” playground equipment like rope ladders and wobble bridges. While they can be scary before kids get used to them, they help work trunk muscles.
Balloon and bubble play – Balloons and bubbles are a unique way to build gross motor skills because you can’t predict where they’re going to go. Kids can chase bubbles and try to pop as many as possible. While chasing them, they have to run, jump, zigzag, and move in ways that require sudden shifts in balance and weight. The same goes for throwing and trying to catch or kick balloons. For more structured play, you can set up a game of balloon volleyball.
Tricycles, scooters, and pedal cars – Some kids who struggle with gross motor skills may learn to ride a trike or bike later than their peers. But there are alternatives they can use to get places and practice balance. Some tricycles come with handles so you can push while your child practices pedaling. Or you could invest in a sturdy scooter or a pedal car. They’re all stepping stones to riding a bike. Once your child gets the hang of it, you can even set up an obstacle course or draw a track with chalk. (Just don’t forget the helmet!)
Dancing – Whether it’s a dance class or an indoor dance party, dancing is good gross motor practice. It helps kids develop balance, coordination, and motor sequencing skills. It also helps build your child’s awareness of rhythm. For little kids, try using songs with lyrics that add movement, like “I’m a Little Teapot” or “The Hokey Pokey.”
Obstacle courses – Obstacle courses get kids moving and give them a goal to accomplish. For an indoor course, use furniture, pillows, and blankets to create areas to crawl on, under, and through. Outdoors, you can use things like hula-hoops to jump in and out of, jumping jacks, belly crawling, bear walking, and other creative movements that challenge your child to balance, crawl, jump, and run.
Distribution of Spinal Nerves means the branch is where the start to the end of the nerve and connect to distal parts of the body, muscle with each roughly corresponding to a segment of the vertebral column eight cervical spinal nerve pairs (C1–C8), 12 thoracic pairs (T1–T12), five lumbar pairs (L1–L5), five sacral pairs (S1–S5), and one coccygeal pair. Each pair connects the spinal cord with a specific region of the body. Near the spinal cord each spinal nerve branches into two roots. A total of 31 pairs of spinal nerves control motor, sensory, and other functions. These nerves are located at the cervical, thoracic, lumbar, sacral, and coccygeal levels.
In total, there are 31 pairs of spinal nerves, grouped regionally by spinal region. More specifically, there are eight cervical nerve pairs (C1-C8), twelve thoracic nerve pairs (T1-T12), five lumbar nerve pairs (L1-L5), and a single coccygeal nerve pair.
Cervical Plexus
The cervical plexus is the plexus of the ventral rami of the first four cervical spinal nerves.
Key Points
The cervical plexus describes the plexus of the ventral rami of the first four cervical spinal nerves that arise from the cervical spinal column in the neck.
The cervical spinal nerves that form the cervical plexus are located laterally (farther from the median line) to the transverse processes of the prevertebral skeletal muscles of the neck from the medial side, and vertebral (closer to the vertebral column) to these muscles from the lateral side.
The cervical plexus forms an anastomosis, a connection, with the accessory nerve, the hypoglossal nerve, and the sympathetic trunk.
The cervical plexus is located in the neck, internal to the sternocleidomastoid, an anterior neck muscle.
Key Terms
sympathetic trunk: Also called the sympathetic chain or gangliated cord, these are a paired bundle of nerve fibers that run from the base of the skull to the coccyx.
plexus: A network or interwoven mass, especially of nerves, blood vessels, or lymphatic vessels.
platysma: A superficial muscle that overlaps the sternocleidomastoid.
cervical plexus: A plexus of the ventral rami of the first four cervical spinal nerves that are located from the C1 to C4 cervical segment in the neck. They are located laterally to the transverse processes of the prevertebral muscles from the medial side and vertebral (scalenus, levator scapulae, splenius cervicis muscles) from the lateral side.
Structure and Distribution
The cervical plexus is a plexus of the ventral rami of the first four cervical spinal nerves located from the C1 to C4 cervical segment in the neck. They are located laterally to the transverse processes between prevertebral muscles from the medial side and anterolateral to them. scalenus and m. levator scapulae.
There is anastomosis with the accessory nerve, hypoglossal nerve, and sympathetic trunk. It is located deep in the neck, near the sternocleidomastoid muscle.
Nerves formed from the cervical plexus innervate the back of the head, as well as some neck muscles. The branches of the cervical plexus emerge from the posterior triangle at the nerve point, a point that lies midway on the posterior border of the sternocleidomastoid.
Branches and Their Functions
The cervical plexus has two types of branches: cutaneous and muscular.
Cutaneous branches include
The lesser occipital nerve, or small occipital nerve, is a cutaneous spinal nerve that arises between the second and third cervical vertebrae, along with the greater occipital nerve. It innervates the scalp in the lateral area of the head posterior to the ear.
The great auricular nerve originates from the cervical plexus and is composed of branches from spinal nerves C2 and C3. It provides sensory innervation for the skin over the parotid gland and mastoid process, and both surfaces of the outer ear.
The transverse cervical nerve (superficial cervical or cutaneous cervical) arises from the second and third cervical nerves, turns around the posterior border of the sternocleidomastoideus about its middle, then passes obliquely forward beneath the external jugular vein to the anterior border of the muscle, where it perforates the deep cervical fascia and divides beneath the platysma into ascending and descending branches that are distributed to the anterolateral parts of the neck.
The supraclavicular nerves (descending branches) arise from the third and fourth cervical nerves. They emerge beneath the posterior border of the sternocleidomastoideus and descend in the posterior triangle of the neck beneath the platysma and deep cervical fascia.
Muscular branches include
Ansa cervicalis (loop formed from C1–C3), geniohyoid (C1 only), thyrohyoid (C1 only), sternothyroid, sternohyoid, omohyoid: The ansa cervicalis is a loop of nerves that are part of the cervical plexus.
The phrenic nerve (C3–C5, but primarily C4) is a nerve that originates in the neck and passes down between the lung and heart to reach the diaphragm.
Segmental branches (C1–C4) innervate the anterior and middle scalenes.
There are two additional branches that are formed by the posterior roots of the spinal nerves
Preauricular nerve (from the posterior roots of C2–C3).
Postauricular nerve (from the posterior roots of C3–C4).
Cervical plexus: Diagram of the cervical plexus.
Brachial Plexus
The brachial plexus is formed by the four lower cervical spinal nerves and the first thoracic spinal nerve.
Key Points
The nerve bundles of the brachial plexus pass through the cervical-axillary canal to serve the axilla (armpit), brachium (arm), antebrachium (forearm), and hand.
The brachial plexus provides cutaneous (skin) and muscular innervations for the upper limbs, excluding the trapezius muscle and an area of skin near the axilla that are innervated by the spinal accessory nerve and the intercostobrachial nerve, respectively.
The brachial plexus is divided into roots, trunks, divisions, cords, and branches.
Key Terms
spinal accessory nerve: A nerve that controls specific muscles of the shoulder and neck.
axilla: The armpit, or the cavity beneath the junction of the arm and shoulder.
brachium: The upper arm.
Formation and Distribution
Right brachial plexus: The right brachial plexus with its short branches, viewed from the front.
The brachial plexus is a network of nerve fibers that run from the spine that is formed by the ventral rami of the lower four cervical and first thoracic nerve roots (C5–C8, T1).
The brachial plexus proceeds through the neck, the axilla (armpit region), and into the arm. It is a collection of nerves passing through the cervical-axillary canal to reach the axilla and innervate the brachium, the antebrachium, and the hand.
The brachial plexus is responsible for cutaneous and muscular innervation of the entire upper limb, with two exceptions: the trapezius muscle is innervated by the spinal accessory nerve (CN XI) and an area of skin near the axilla is innervated by the intercostobrachial nerve. Lesions on the brachial plexus can lead to severe functional impairment.
Branches and Divisions
The brachial plexus is divided into roots, trunks, divisions, cords, and branches. There are five terminal branches and numerous other preterminal or collateral branches that leave the plexus at various points along its length. Its structure includes:
Five roots: The five anterior rami of the spinal nerves, after they have given off their segmental supply to the muscles of the neck.
These roots merge to form three trunks: The superior or upper (C5–C6), the middle (C7), and the inferior or lower (C8, T1).
Each trunk then splits in two, to form six divisions: The anterior divisions of the upper, middle, and lower trunks and the posterior divisions of the upper, middle, and lower trunks.
These six divisions will regroup to become the three cords. The cords are named by their position with respect to the axillary artery:
The posterior cord is formed from the three posterior divisions of the trunks (C5–C8,T1).
The lateral cord is the anterior division from the upper and middle trunks (C5–C7).
The medial cord is simply a continuation of the anterior division of the lower trunk (C8, T1).
Most branches branch from the cords, but a few branch directly from earlier structures. The five on the left are considered terminal branches.
Brachial plexus: Diagram of the brachial plexus and its branches.
Lumbar Plexus
The lumbar plexus is formed by the subcostal nerve and divisions of the first four lumbar nerves that arise from the middle to the lower back.
Key Points
The lumbar plexus passes through the psoas major muscle and innervates the skin and muscles of the abdominal wall, thigh, and external genitalia.
The largest nerve that forms part of the lumbar plexus is the femoral nerve, which innervates the anterior thigh muscles and some of the skin distal to the inguinal ligament.
The ilioinguinal nerve pierces the lateral abdominal wall and runs medially at the level of the inguinal ligament. It supplies motor branches to both transversus abdominis and sensory branches (to the skin over the pubic symphysis and the lateral aspect of the labia majora or scrotum ).
The genital branch of the genitofemoral nerve courses differently in females and males.
Key Terms
lumbosacral plexus: The anterior divisions of the lumbar nerves, sacral nerves, and coccygeal nerve form this plexus, the first lumbar nerve being frequently joined by a branch from the twelfth thoracic nerve.
inguinal ligament: A band running from the pubic tubercle to the anterior superior iliac spine. Its anatomy is very important for operating on hernia patients.
subcostal nerve: The twelfth thoracic nerve, its anterior division is larger than the others; it runs along the lower border of the twelfth rib and often gives a communicating branch to the first lumbar nerve, and then passes under the lateral lumbocostal arch.
aponeurosis: Layers of flat, broad tendons that have a shiny, whitish-silvery color.
Structure and Distribution
The lumbar plexus is a nerve plexus in the lumbar region of the body that forms part of the lumbosacral plexus. It is formed by the ventral divisions of the first four lumbar nerves (L1–L4) and from contributions of the subcostal nerve (T12), which is the last thoracic nerve.
This plexus lies within the psoas major muscle. Nerves of the lumbar plexus serve the skin and the muscles of the lower abdominal wall, the thigh, and external genitals. The largest nerve of the plexus is the femoral nerve and it supplies the anterior muscles of the thigh and a part of skin distal to the inguinal ligament.
Lumbar plexus: An image of the lumbar plexus with its nerves highlighted in yellow.
Branches of the Lumbar Plexus
Iliohypogastric Nerve
Lumbar plexus: Schematic of the lumbar plexus.
Runs anterior to the psoas major on its proximal lateral border to run laterally and obliquely on the anterior side of the quadratus lumborum. Lateral to this muscle, it pierces the transversus abdominis to run above the iliac crest between that muscle and the abdominal internal oblique. It gives off several motor branches to these muscles and a sensory branch to the skin of the lateral hip. Its terminal branch then runs parallel to the inguinal ligament to exit the aponeurosis of the abdominal external oblique above the external inguinal ring, where it supplies the skin above the inguinal ligament (i.e., the hypogastric region) with the anterior cutaneous branch.
Ilioinguinal Nerve
This nerve closely follows the iliohypogastric nerve on the quadratus lumborum but then passes below it to run at the level of the iliac crest. It pierces the lateral abdominal wall and runs medially at the level of the inguinal ligament where it supplies motor branches to both the transversus abdominis and sensory branches through the external inguinal ring to the skin over the pubic symphysis and the lateral aspect of the labia majora in females, and in males, the scrotum.
Genitofemoral Nerve
Pierces the psoas major anteriorly, below the former two nerves to immediately split into two branches that run downward on the anterior side of the muscle. The lateral femoral branch is purely sensory and pierces the vascular lacuna near the saphenous hiatus and supplies the skin below the inguinal ligament. In males, the genital branch runs in the spermatic cord then sends sensory branches to the scrotal skin and supplies motor innervations to the cremaster muscle. In females, it runs in the inguinal canal together with the teres uteri ligament. It then sends sensory branches to the labia majora in females.
Lateral Cutaneous Femoral Nerve
Pierces the psoas major on its lateral side and runs obliquely downward below the iliac fascia. Medial to the anterior superior iliac spine, it leaves the pelvic area through the lateral muscular lacuna and enters the thigh by passing behind the lateral end of the inguinal ligament. In the thigh, it briefly passes under the fascia lata before it breaches the fascia and supplies the skin of the anterior thigh.
Obturator Nerve
Leaves the lumbar plexus and descends behind the psoas major on its medial side, follows the linea terminalis into the lesser pelvis, then finally leaves the pelvic area through the obturator canal. In the thigh, it sends motor branches to the obturator externus before dividing into an anterior and a posterior branch, both of which continue distally. These branches are separated by the adductor brevis and supply all thigh adductors with motor innervations. The anterior branch contributes a terminal, sensory branch that passes along the anterior border of gracilis and supplies the skin on the medial, distal part of the thigh.
Femoral Nerve
This is the largest and longest of the plexus’ nerves. It gives motor innervation to iliopsoas, pectineus, sartorius, and quadriceps femoris, and sensory innervation to the anterior thigh, posterior lower leg, and hindfoot. In the pelvic area, it runs in a groove between the psoas major and iliacus muscles and gives branches to both. It exits the pelvis through the medial aspect of the muscular lacuna. In the thigh, it divides into numerous sensory and muscular branches and the saphenous nerve, its long sensory terminal branch that continues down to the foot.
Sacral and Coccygeal Plexuses
The sacral plexus is the plexus of the three sacral spinal nerves (S2–S4) that arise from the lower back just above the sacrum.
Key Points
The sacral plexus, together with the lumbar plexus, forms the lumbosacral plexus.
The largest nerve in the sacral plexus is the sciatic nerve that innervates the thigh, lower leg, and the foot.
The coccygeal plexus consists of the coccygeal nerve and the fifth sacral nerve, which innervate the skin in the coccygeal region, around the tailbone (called the coccyx).
Key Terms
sacral plexus: A nerve plexus that provides motor and sensory nerves for the posterior thigh, most of the lower leg, the entire foot, and part of the pelvis.
coccygeal nerve: The spinal nerve that corresponds to the coccyx bone.
sciatic nerve: A large nerve that starts in the lower back and runs through the buttock and down the lower limb.
The sacral plexus is a nerve plexus that provides motor and sensory nerves for the posterior thigh, most of the lower leg, the entire foot, and part of the pelvis. It is part of the lumbosacral plexus and emerges from the sacral vertebrae (S2–S4).
The sacral plexus: The nerves of the sacral plexus are shown.
The largest and longest nerve of the human body, the sciatic nerve, is the main branch and gives rami to the motor innervation of the muscles of the foot, the leg, and the thigh.
The sacral plexus is formed by:
The lumbosacral trunk.
The anterior division of the first sacral nerve.
Portions of the anterior divisions of the second and third sacral nerves.
The nerves forming the sacral plexus converge toward the lower part of the greater sciatic foramen and unite to form a flattened band from the anterior and posterior surfaces, from which several branches arise.
The band itself is continued as the sciatic nerve, which splits on the back of the thigh into the tibial nerve and the common fibular nerve. These two nerves sometimes arise separately from the plexus and, in all cases, their independence can be shown by dissection.
Often, the sacral plexus and the lumbar plexus are considered to be one large nerve plexus, the lumbosacral plexus. The lumbosacral trunk connects the two plexuses.
The coccygeal plexus originates from the S4, S5, and Co1 spinal nerves. It is interconnected with the lower part of the sacral plexus. The only nerve in this plexus is the anococcygeal nerve, which serves sensory innervation of the skin in the coccygeal region.
Sacral plexus diagram: Diagram of the sacral plexus showing the various anterior and posterior nerve branches that arise from each lumbar and sacral nerve.
Sensory and Motor Tracts
The spinothalamic tract is a somatosensory tract and the corticospinal tract is a motor tract.
Key Points
The spinothalamic tract is split into the lateral spinothalamic tract that transmits pain and temperature sensation to the thalamus, and the anterior spinothalamic tract that transmits pressure and crude touch sensation to the thalamus.
The corticospinal tract is a motor tract comprised of mostly motor axons that carry motor information from the cerebral cortex and brainstem to the musculature for voluntary movement.
The corticospinal tract is split into the lateral and anterior corticospinal tracts, which decussate, or cross, in the medulla oblongata. Therefore, the right brain controls the left side of the body, and the left brain controls the right side of the body.
Betz cells, the largest pyramidal cells, are only found in the corticospinal tract.
Key Terms
spinothalamic tract: A sensory pathway originating in the spinal cord. It transmits information to the thalamus about pain, temperature, itch, and crude touch.
somatosensory tract: The system that reacts to diverse stimuli using thermoreceptors, nociceptors, mechanoreceptors, and chemoreceptors. The transmission of information from the receptors passes via sensory nerves through tracts in the spinal cord and into the brain.
Betz cell: Giant pyramidal cells (neurons) located within the fifth layer of the grey matter in the primary motor cortex. They have a rapid conduction rate of over 70m/sec, which is the fastest conduction of any signals from the brain to the spinal cord.
corticospinal tract: The nervous system tract that conducts impulses from the brain to the spinal cord. It contains mostly motor axons and is made up of two separate tracts in the spinal cord: the lateral corticospinal tract and the anterior corticospinal tract.
The Somatosensory Tract
The spinothalamic tract is a sensory pathway originating in the spinal cord. It transmits information to the thalamus about pain, temperature, itch, and crude touch. The pathway decussates at the level of the spinal cord.
The somatosensory organization is divided into the dorsal column–medial lemniscus tract (the touch, proprioception, vibration sensory pathway) and the anterolateral system, or ALS (the pain, temperature sensory pathway). Both sensory pathways use three different neurons to get information from sensory receptors at the periphery to the cerebral cortex.
These neurons are designated primary, secondary, and tertiary sensory neurons. In both pathways, primary sensory neuron cell bodies are found in the dorsal root ganglia, and their central axons project into the spinal cord.
Function
The types of sensory information transmitted via the spinothalamic tract are described as effective sensations. This means that the sensation is accompanied by a compulsion to act. For instance, an itch is accompanied by a need to scratch, and a painful stimulus makes us want to withdraw from the pain.
There are two subsystems:
Direct (for direct, conscious appreciation of pain).
Indirect (for affective and arousal impact of pain).
Indirect projections are further divided into
Spino-reticulo-thalamocortical (part of the ascending reticular arousal system, also known as ARAS).
Spino-mesencephalic-limbic (for the affective impact of pain).
The Corticospinal Tract
The corticospinal tract conducts impulses from the brain to the spinal cord. It contains mostly motor axons. The corticospinal tract is made up of two separate tracts in the spinal cord: the lateral corticospinal tract and the anterior corticospinal tract.
The corticospinal tract also contains the Betz cell (the largest pyramidal cells) that are not found in any other region of the body. An understanding of these tracts leads to an understanding of why one side of the body is controlled by the opposite side of the brain.
The corticospinal tract is concerned specifically with discrete, voluntary, skilled movements, such as the precise movement of fingers and toes. The brain sends impulses to the spinal cord that relay the message.
This is imperative in understanding that the left hemisphere of the brain controls the RIGHT side of the body, while the right hemisphere of the brain controls the LEFT side of the body. The signals cross in the medulla oblongata, and this process is also known as decussation.
Spinal cord tracts: Spinal cord tracts are identified.
Function
The primary purpose of the corticospinal tract is to maintain voluntary motor control of the body and limbs. However, connections to the somatosensory cortex suggest that the pyramidal tracts are also responsible for modulating sensory information from the body.
Some of these connections across the midline; therefore, each side of the brain is responsible for controlling muscles for the limbs on opposite sides of the body. However, control of trunk muscles is on the same side of the body.
After a patient’s pyramidal tracts are injured, the patient is paralyzed on the corresponding side of the body. Fortunately, they can re-learn some crude, basic motions, but not fine movements. This implies that the connections to these tracts are crucial for fine movement, and only partial recovery is possible if they are damaged.
Spinal nerves form from the dorsal nerve roots and the ventral nerve roots which branch from the dorsal and ventral horn of the spinal cord, respectively. The spinal nerves exit through the intervertebral foramina or neuroforamina and travel along with their respective dermatomal distributions from posterior to anterior, creating specific, observable dermatomal patterns.[rx]In total, there are 31 distinct spinal segments and thus 31 distinct spinal nerves bilaterally. These 31 spinal nerves are composed of 8 pairs of cervical nerves, 12 pairs of thoracic nerves, five pairs of lumbar nerves, five pairs of sacral nerves, and one pair of coccygeal nerves.[rx]
A spinal nerve is a mixed nerve, which carries motor, sensory, and autonomic signals between the spinal cord and the body. In the human body, there are 31 pairs of spinal nerves, one on each side of the vertebral column. These are grouped into the corresponding cervical, thoracic, lumbar, sacral, and coccygeal regions of the spine.[1] There are eight pairs of cervical nerves, twelve pairs of thoracic nerves, five pairs of lumbar nerves, five pairs of sacral nerves, and one pair of coccygeal nerves. The spinal nerves are part of the peripheral nervous system.
Before diving into the anatomy of the spinal nerves, let’s list the most common anatomical terms used in neuroanatomy in order to easily orientate in the matter.
Common terms in neuroanatomy
Ventral
Anterior, towards the front
Dorsal
Posterior, towards the back
Rostral
On the forward’s side (towards the nose)
Caudal
On the lowermost end (towards the tail)
Cranial
On the top side, towards the skull
Ipsilateral
On the same side
Contralateral
On the opposite side
Bilateral
On both sides
Overview of the Spinal Nerves
Each spinal nerve is a mixed nerve, formed from the combination of nerve fibers from its dorsal and ventral roots. The dorsal root is the afferent sensory root and carries sensory information to the brain. The ventral root is the efferent motor root and carries motor information from the brain. The spinal nerve emerges from the spinal column through an opening (intervertebral foramen) between adjacent vertebrae. This is true for all spinal nerves except for the first spinal nerve pair (C1), which emerges between the occipital bone and the atlas (the first vertebra). Thus the cervical nerves are numbered by the vertebra below, except spinal nerve C8, which exists below vertebra C7 and above vertebra T1. The thoracic, lumbar, and sacral nerves are then numbered by the vertebra above. In the case of a summarized S1 vertebra (aka L6) or a sacralized L5 vertebra, the nerves are typically still counted to L5 and the next nerve is S1.
Scheme showing structure of a typical spinal nerve
Somatic efferent.
2. Somatic afferent.
3,4,5. Sympathetic efferent.
6,7. Autonomic afferent.
Outside the vertebral column, the nerve divides into branches. The dorsal ramus contains nerves that serve the posterior portions of the trunk carrying visceral motor, somatic motor, and somatic sensory information to and from the skin and muscles of the back (epaxial muscles). The ventral ramus contains nerves that serve the remaining anterior parts of the trunk and the upper and lower limbs (hypaxial muscles) carrying visceral motor, somatic motor, and sensory information to and from the ventrolateral body surface, structures in the body wall, and the limbs. The meningeal branches (recurrent meningeal or sinuvertebral nerves) branch from the spinal nerve and re-enter the intervertebral foramen to serve the ligaments, dura, blood vessels, intervertebral discs, facet joints, and periosteum of the vertebrae. The rami communicantes contain autonomic nerves that serve visceral functions carrying visceral motor and sensory information to and from the visceral organs.
Some anterior rami merge with adjacent anterior rami to form a nerve plexus, a network of interconnecting nerves. Nerves emerging from a plexus contain fibers from various spinal nerves, which are now carried together to some target location. Major plexuses include the cervical, brachial, lumbar, and sacral plexuses.
Spinal nerves, a part of the peripheral nervous system (PNS), are mixed nerves that send motor, sensory, and autonomic signals between the CNS and the body.
Key Points
Afferent sensory axons bring sensory information from the body to the spinal cord and brain; they travel through the dorsal roots of the spinal cord.
Efferent motor axons bring motor information from the brain to the body; they travel through the ventral roots of the spinal cord.
All spinal nerves—except the first pair—emerge from the spinal column through an opening between vertebrae, called an intervertebral foramen.
The spinal nerves are typically labeled by their location in the body: thoracic, lumbar, or sacral.
Key Terms
ventral root: Also called the anterior root, it is the efferent motor root of a spinal nerve.
autonomic: Acting or occurring involuntarily, without conscious control.
dorsal root: Also known as the posterior root, the afferent sensory root of a spinal nerve.
intervertebral foramen: The foramen allows for the passage of the spinal nerve root, dorsal root ganglion, the spinal artery of the segmental artery, the communicating veins between the internal and external plexuses, recurrent meningeal (sinu-vertebral) nerves, and transforaminal ligaments.
Spinal Nerve Anatomy
The term spinal nerve generally refers to a mixed spinal nerve that carries motor, sensory, and autonomic signals between the spinal cord and the body.
Humans have 31 left-right pairs of spinal nerves, each roughly corresponding to a segment of the vertebral column: eight cervical spinal nerve pairs (C1–C8), 12 thoracic pairs (T1–T12), five lumbar pairs (L1–L5), five sacral pairs (S1–S5), and one coccygeal pair. The spinal nerves are part of the peripheral nervous system (PNS).
A spinal nerve: Spinal nerves arise from a combination of nerve fibers from the dorsal and ventral roots of the spinal cord.
Location
Intervertebral foramina: Intervertebral foramina are indicated by arrows.
Each spinal nerve is formed by the combination of nerve fibers from the dorsal and ventral roots of the spinal cord. The dorsal roots carry afferent sensory axons, while the ventral roots carry efferent motor axons.
The spinal nerve emerges from the spinal column through an opening (intervertebral foramen) between adjacent vertebrae.
This is true for all spinal nerves except for the first spinal nerve pair, which emerges between the occipital bone and the atlas (the first vertebra). Thus the cervical nerves are numbered by the vertebra below, except C8, which exists below C7 and above T1.
The thoracic, lumbar, and sacral nerves are then numbered by the vertebra above. In the case of a summarized S1 vertebra (i.e., L6) or a sacralized L5 vertebra, the nerves are typically still counted to L5 and the next nerve is S1.
Spinal Nerve Innervation
Outside the vertebral column, the nerve divides into branches. The dorsal ramus contains nerves that serve the dorsal portions of the trunk; it carries visceral motor, somatic motor, and somatic sensory information to and from the skin and muscles of the back (epaxial muscles).
The ventral ramus contains nerves that serve the remaining ventral parts of the trunk and the upper and lower limbs (hypaxial muscles); they carry the visceral motor, somatic motor, and sensory information to and from the ventrolateral body surface, structures in the body wall, and the limbs.
The meningeal branches (recurrent meningeal or sinuvertebral nerves) branch from the spinal nerve and re-enter the intervertebral foramen to serve the ligaments, dura, blood vessels, intervertebral discs, facet joints, and periosteum of the vertebrae.
The rami communicantes contain autonomic nerves that serve visceral functions, such as carrying visceral motor and sensory information to and from the visceral organs.
Cervical Nerves
The posterior distribution of the cervical nerves includes the suboccipital nerve (C1), the greater occipital nerve (C2), and the third occipital nerve (C3). The anterior distribution includes the cervical plexus (C1–C4) and brachial plexus (C5–T1).
The muscles innervated by the cervical nerves are the sternohyoid, sternothyroid, and omohyoid muscles.
A loop of nerves called ansa cervicalis is also part of the cervical plexus.
Thoracic Nerves
Thoracic nerve branches exit the spine and go directly to the paravertebral ganglia of the autonomic nervous system, where they are involved in the functions of organs and glands in the head, neck, thorax, and abdomen.
Anterior Divisions
The intercostal nerves come from thoracic nerves T1–T11 and run between the ribs. The subcostal nerve comes from nerve T12 and runs below the twelfth rib.
Posterior Divisions
The medial branches (ramus medialis) of the posterior branches of the upper six thoracic nerves run between the semispinalis dorsi and multifidus, which they supply.
They then pierce the rhomboid and trapezius muscles and reach the skin by the sides of the spinous processes. This branch is called the medial cutaneous ramus.
The medial branches of the lower six thoracic nerves are distributed chiefly to the multifidus and longissimus dorsi, occasionally they give off filaments to the skin near the middle line. This sensitive branch is called the posterior cutaneous ramus.
Lumbar Nerves
The lumbar nerves are divided into posterior and anterior divisions.
Posterior Divisions
The medial branches of the posterior divisions of the lumbar nerves run close to the articular processes of the vertebrae and end in the multifidus muscle. The lateral branches supply the erector spinae muscles.
Anterior Divisions
The anterior divisions of the lumbar nerves (rami anteriores) consist of long, slender branches that accompany the lumbar arteries around the sides of the vertebral bodies, beneath the psoas major.
The first and second, and sometimes the third and fourth, lumbar nerves are each connected with the lumbar part of the sympathetic trunk by a white ramus communicans.
The nerves pass obliquely outward behind the psoas major, or between its fasciculi, distributing filaments to it and the quadratus lumborum.
The first three and the greater part of the fourth are connected by anastomotic loops and form the lumbar plexus.
The smaller part of the fourth joins with the fifth to form the lumbosacral trunk, which assists in the formation of the sacral plexus. The fourth nerve is named the furcal nerve, from the fact that it is subdivided between the two plexuses.
Sacral Nerves
There are five paired sacral nerves, half of them arising through the sacrum on the left side and the other half on the right side. Each nerve emerges in two divisions: one division through the anterior sacral foramina and the other division through the posterior sacral foramina.
The sacral nerves have both afferent and efferent fibers, thus they are responsible for part of the sensory perception and the movements of the lower extremities of the human body.
The pudendal nerve and parasympathetic fibers arise from S2, S3, and S4. They supply the descending colon and rectum, urinary bladder, and genital organs. These pathways have both afferent and efferent fibers.
Coccygeal Nerve
The coccygeal nerve is the 31st pair of spinal nerves and arises from the conus medullaris. Its anterior root helps form the coccygeal plexus.
Function
Spinal nerve motor functions are summarized in the table below.
Actions of the spinal nerves
Level
Motor Function
C1–C6
Neck flexors
C1–T1
Neck extensors
C3, C4, C5
Supply diaphragm (mostly C4)
C5, C6
Move shoulder, raise arm (deltoid); flex elbow (biceps)
C6
Externally rotate (supinate) the arm
C6, C7
Extend the elbow and wrist (triceps and wrist extensors); pronate wrist
C7, C8
Flex wrist; supply small muscles of the hand
T1–T6
Intercostals and trunk above the waist
T7–L1
Abdominal muscles
L1–L4
Flex thigh
L2, L3, L4
Adduct thigh; extend leg at the knee (quadriceps femoris)
L4, L5, S1
Abduct thigh; flex leg at the knee (hamstrings); dorsiflex foot (tibialis anterior); extend toes
L5, S1, S2
Extend leg at the hip (gluteus maximus); plantarflex foot and flex toes
Branches of Spinal Nerves
The spinal nerves branch into the dorsal ramus, ventral ramus, the meningeal branches, and the rami communicantes.
Key Points
The dorsal and ventral rami contain nerves that provide visceral motor, somatic motor, and sensory information, with the dorsal ramus feeding the dorsal trunk (skin and muscles of the back), and the ventral ramus feeding the ventral trunk and limbs through the ventrolateral surface.
The meningeal branches supply nerve function to the vertebrae themselves, including the ligaments, dura, blood vessels, intervertebral discs, facet joints, and periosteum.
The rami communicantes contain autonomic nerves that carry visceral motor and sensory information to and from the visceral organs.
Key Terms
nerve plexus: A branching network of intersecting nerves.
dorsal ramus: The posterior (or dorsal) branches (or divisions) of the spinal nerves are, as a rule, smaller than the anterior divisions. They are also referred to as the dorsal rami. They are directed backwards and—with the exceptions of those of the first cervical, the fourth and fifth sacral, and the coccygeal—divide into medial and lateral branches for the supply of the muscles and skin of the posterior part of the trunk.
meningeal branches: Also known as recurrent meningeal nerves, sinuvertebral nerves, or recurrent nerves of Luschka, these are a number of small nerves that branch from the spinal nerve (or the posterior ramus) near the origin of the anterior and posterior rami. They then re-enter the intervertebral foramen, and innervate the facet joints, the annulus fibrosus of the intervertebral disk, and the ligaments and periosteum of the spinal canal, carrying pain sensation.
Course and branches of thoracic spinal nerve: This diagram depicts the course and branches of a typical thoracic spinal nerve. The posterior division (dorsal ramus) is labeled at the top right.
Outside the vertebral column, the spinal nerves divide into branches.
The dorsal ramus: Contains nerves that serve the dorsal portions of the trunk carrying visceral motor, somatic motor, and sensory information to and from the skin and muscles of the back.
The ventral ramus: Contains nerves that serve the remaining ventral parts of the trunk and the upper and lower limbs carrying visceral motor, somatic motor, and sensory information to and from the ventrolateral body surface, structures in the body wall, and the limbs. Some ventral rami merge with adjacent ventral rami to form a nerve plexus, a network of interconnecting nerves. Nerves emerging from a plexus contain fibers from various spinal nerves, which are now carried together to some target location. Major plexuses include the cervical, brachial, lumbar, and sacral plexuses.
The meningeal branches (recurrent meningeal or sinuvertebral nerves): These branch from the spinal nerve and re-enter the intervertebral foramen to serve the ligaments, dura, blood vessels, intervertebral discs, facet joints, and periosteum of the vertebrae.
The rami communicantes: Contain autonomic nerves that carry visceral motor and sensory information to and from the visceral organs.
Types of Spinal Nerve fibers
Somatic efferent fibers originate in the anterior/ventral column of central grey matter in the spinal cord. They pass through the anterior root of the spinal nerve. They are responsible for the motor innervation of the skeletal muscles.
Somatic afferent fibers carry sensory information from the skin, joints, and muscle to the posterior/dorsal column of grey matter in the spinal cord. These fibers pass through the dorsal root ganglion.
Visceral efferent fibers are autonomic fibers that supply the organs. They are divided into sympathetic and parasympathetic fibers. Sympathetic fibers originate from the thoracic spinal nerves as well as L1 and L2. Parasympathetic nerves come from the S2, S3, and S4 spinal nerves only to supply the pelvic and lower abdominal viscera. The remainder of the parasympathetic nerves come from extensions of the cranial nerves into the thoracic and abdominal cavities.
Visceral afferent fibers carry sensory information through the dorsal root ganglion and to the dorsal column of grey matter in the spinal cord.
Plexuses
A nerve plexus is a network of intersecting nerves that serve the same part of the body.
Key Points
Nerve plexuses throughout the body tend to be named after the area in which the plexus occurs and the organs, limbs, and tissues it serves. Examples include the cervical, brachial, lumbar, sacral, celiac, and coccygeal plexuses.
Auerbach’s plexus, which serves the gastrointestinal tract, is named after the first person to describe this plexus, Leopold Auerbach, rather than the area of the body it serves.
The brachial plexus serves the chest, shoulders, arms and hands and is formed by the ventral rami of C5, C8, and T1 spinal nerves, and the lower and upper halves of the C4 and T2 spinal nerves.
Key Terms
nerve plexus: A network of intersecting nerves.
brachial plexus: A network of nerve fibers, running from the spine, formed by the ventral rami of the lower four cervical and first thoracic nerve roots (C5–C8, T1). It proceeds through the neck, the axilla (armpit region), and into the arm. It also supplies the brachium, the antebrachium, and the hand.
coccygeal plexus: A plexus of nerves near the coccyx bone.
Autonomic: A division of the peripheral nervous system that influences the function of internal organs.
A nerve plexus is a network of intersecting nerves; multiple nerve plexuses exist in the body. Nerve plexuses are composed of afferent and efferent fibers that arise from the merging of the anterior rami of spinal nerves and blood vessels.
There are five spinal nerve plexuses—except in the thoracic region—as well as other forms of autonomic plexuses, many of which are a part of the enteric nervous system.
Spinal Plexuses
Cervical Plexus—Serves the Head, Neck, and Shoulders
The cervical plexus is formed by the ventral rami of the upper four cervical nerves and the upper part of the fifth cervical ventral ramus. The network of rami is located deep within the neck.
Brachial Plexus—Serves the Chest, Shoulders, Arms, and Hands
The brachial plexus is formed by the ventral rami of C5–C8 and the T1 spinal nerves, and lower and upper halves of the C4 and T2 spinal nerves. The plexus extends toward the armpit (axilla).
Lumbar Plexus—Serves the Back, Abdomen, Groin, Thighs, Knees, and Calves
The lumbar plexus is formed by the ventral rami of L1–L5 spinal nerves with a contribution of T12 form the lumbar plexus. This plexus lies within the psoas major muscle.
Sacral Plexus—Serves the Pelvis, Buttocks, Genitals, Thighs, Calves, and Feet
The sacral plexus is formed by the ventral rami of L4-S3, with parts of the L4 and S4 spinal nerves. It is located on the posterior wall of the pelvic cavity.
Coccygeal Plexus—Serves a Small Region over the Coccyx
The coccygeal plexus serves a small region over the coccyx and originates from S4, S5, and Co1 spinal nerves. It is interconnected with the lower part of the sacral plexus.
In addition, the celiac plexus serves the internal organs, and Auerbach’s plexus serves the gastrointestinal tract.
Auerbach’s plexus—Serves the gastrointestinal tract.
Meissner’s plexus (submucosal plexus)—Serves the gastrointestinal tract.
Brachial plexus: Cervical (C5–C8) and thoracic (T1) nerves comprise the brachial plexus, which is a nerve plexus that provides sensory and motor function to the shoulders and upper limbs.
Lumbar plexus: The lumbar plexus is comprised of the ventral rami of the lumbar spinal nerves (L1–L5) and a contribution from the thoracic nerve (T12). The posterior (green) and anterior (yellow) divisions of the lumbar plexus are shown in the diagram.
Intercostal Nerves
The anterior divisions of the thoracic spinal nerves (T1–T11) are called the intercostal nerves.
Key Points
The intercostal nerves are part of the somatic nervous system. This enables them to control the contraction of muscles, as well as provide specific sensory information regarding the skin and parietal pleura.
Intercostal nerves connect to the appropriate ganglion in the sympathetic trunk through rami communicantes and serve the thoracic pleura and the abdominal peritoneum.
Unlike most other anterior divisions of spinal nerves, the intercostal nerves do not form a plexus.
Key Terms
thoracic spinal nerves: The spinal nerves emerging from the thoracic vertebrae. Branches also exit the spine and go directly to the sympathetic chain ganglia of the autonomic nervous system where they are involved in the functions of organs and glands in the head, neck, thorax, and abdomen.
sympathetic trunk: Also called the sympathetic chain or gangliated cord, these are a paired bundle of nerve fibers that run from the base of the skull to the coccyx.
abdominal peritoneum: The serous membrane that forms the lining of the abdominal cavity. It covers most of the intra-abdominal organs. It is composed of a layer of mesothelium supported by a thin layer of connective tissue. The peritoneum supports the abdominal organs and serves as a conduit for their blood and lymph vessels and nerves.
The intercostal nerves are part of the somatic nervous system and arise from anterior divisions (rami anterior, ventral divisions) of the thoracic spinal nerves T1 to T11. The intercostal nerves are distributed chiefly to the thoracic pleura and abdominal peritoneum.
Intercostal nerves: An image of the intercostal brachial nerves.
They differ from the anterior divisions of the other spinal nerves in that each pursues an independent course without plexus formation.
First Thoracic Nerve
The anterior division of the first thoracic nerve divides into two branches:
The larger branch leaves the thorax in front of the neck of the first rib and enters the brachial plexus.
The other smaller branch, the first intercostal nerve, runs along with the first intercostal space and ends on the front of the chest as the first anterior cutaneous branch of the thorax.
The Upper Thoracic Nerves (2nd–6th)
These are limited in their distribution to the parietes (wall) of the thorax. The anterior divisions of the second, third, fourth, fifth, and sixth thoracic nerves, and the small branch from the first thoracic are confined to the walls of the thorax and are named thoracic intercostal nerves.
Near the sternum, they cross in front of the internal mammary artery and transversus thoracic muscle, pierce the intercostales interni, the anterior intercostal membranes, and pectoralis major, and supply the integument of the front of the thorax and over the mamma, forming the anterior cutaneous branches of the thorax.
The branch from the second nerve unites with the anterior supraclavicular nerves of the cervical plexus.
The Lower Thoracic Nerves (7th–12th)
The seventh intercostal nerve terminates at the xiphoid process, at the lower end of the sternum.
The anterior divisions of the seventh, eighth, ninth, tenth, and eleventh thoracic intercostal nerves are continued anteriorly from the intercostal spaces into the abdominal wall; hence they are named thoracoabdominal nerves or thoracoabdominal intercostal nerves.
The tenth intercostal nerve terminates at the umbilicus.
The twelfth (subcostal) thoracic nerve is distributed to the abdominal wall and groin.
Unlike the nerves from the autonomic nervous system that innervate the visceral pleura of the thoracic cavity, the intercostal nerves arise from the somatic nervous system. This enables them to control the contraction of muscles, as well as provide specific sensory information regarding the skin and parietal pleura.
This explains why damage to the internal wall of the thoracic cavity can be felt as a sharp pain localized in the injured region. Damage to the visceral pleura is experienced as an unlocalized ache.
Dermatomes
A dermatome is an area of skin that is supplied by a single spinal nerve, and a myotome is a group of muscles that a single spinal nerve root innervates.
Key Points
There are eight cervical nerves, twelve thoracic nerves, five lumbar nerves and five sacral nerves. Each of these nerves relays sensation, including pain, from a particular region of skin to the brain.
Along the thorax and abdomen, the dermatomes are like a stack of discs, with each section supplied by a different spinal nerve. The pattern is different along the arms and the legs. The dermatomes run longitudinally along the limbs, so that each half of the limb has a different dermatome.
Dermatomes have clinical significance, especially in the diagnosis of certain diseases. Symptoms that follow a dermatome, such as pain or a rash, may indicate a pathology that involves the related nerve root. Examples include dysfunction of the spine or a viral infection.
Key Terms
shingles: Also known as herpes zoster, shingles is an acute viral inflammation of the sensory ganglia of spinal and cranial nerves associated with a vesicular eruption and neuralgic pains and caused by reactivation of the poxvirus causing chickenpox.
chickenpox: A common childhood disease caused by the varicella-zoster virus.
A dermatome is an area of skin that is supplied by a single spinal nerve. There are eight cervical nerves, twelve thoracic nerves, five lumbar nerves and five sacral nerves. Each of these nerves relays sensation, including pain, from a particular region of the skin to the brain.
Dermatomes: Dermatomes are areas of skin supplied by sensory neurons that arise from a spinal nerve ganglion. Dermatomes and the associated major cutaneous nerves are shown here in a ventral view.
Along the thorax and abdomen, the dermatomes are like a stack of discs, with each section supplied by a different spinal nerve. Along the arms and the legs, the pattern is different. The dermatomes run longitudinally along the limbs, so that each half of the limb has a different dermatome.
Although the general pattern is similar in all people, the precise areas of innervation are as unique to an individual as fingerprints.
Dermatomes have clinical significance, especially in the diagnosis of certain diseases. Symptoms that follow a dermatome, such as pain or a rash, may indicate a pathology that involves the related nerve root. Examples include dysfunction of the spine or a viral infection.
Viruses that remain dormant in nerve ganglia, such as the varicella zoster virus that causes both chickenpox and shingles, often cause either pain, rash, or both in a pattern defined by a dermatome.
Shingles rash: The shingles rash appears across a dermatome. In this patient, one of the dermatomes in the arm is affected, restricting the rash to the length of the back of the arm.
Shingles is one of the only diseases that cause a rash in a dermatomal pattern, and as such, this is its defining symptom. The rash of shingles is almost always restricted to a specific dermatome, such as on the chest, leg, or arm caused by the residual varicella-zoster virus infection of the nerve that supplies that area of skin. Shingles typically appear years or decades after recovery from chickenpox.
Myotome
A myotome is the group of muscles that a single spinal nerve root innervates. The myotome is the motor equivalent of a dermatome.
The myotome distributions of the upper and lower extremities are listed below:
The testing of myotomes provides the clinician with information about the level in the spine where a lesion may be present. During testing, the clinician looks for muscle weakness of a particular group of muscles. Results may indicate lesions to the spinal cord nerve root, or intervertebral disc herniation that presses on the spinal nerve roots.
Function and Physiology of the Spinal Nerves
Spinal nerves connect the brain and spinal cord to the limbs and organs of the body.
Key Points
Spinal nerves, considered part of the peripheral nervous system, generally refer to mixed spinal nerves, which carry the motor, sensory, and autonomic information between the brain and spinal cord and the rest of the body.
The cervical spinal nerves innervate the muscles and provide sensation for the head, neck, and diaphragm, as well as the upper limbs and back.
The lumbar, sacral, and coccygeal nerves combine to form the lumbosacral plexus.
The spinal cord can be divided into the lateral, posterior, and medial cord, each segment of which gives rise to specific nerves and serves specific areas of the body.
The somatic nervous system is responsible for voluntary body movements, receiving information from afferent fibers and contracting muscles with efferent fibers.
The autonomic nervous system involves the visceral organs and regulates involuntary movements or unconscious actions.
The sympathetic nervous system is responsible for the fight or flight reaction under stressful conditions, while the parasympathetic nervous system conserves energy after high-stress situations or during rest and digestion.
The primary neurotransmitters of the peripheral nervous system (PNS) are acetylcholine and noradrenaline, though other neurotransmitters are also present. Acetylcholine acts on two sets of receptors, muscarinic and nicotinic cholinergic receptors.
Key Terms
nicotinic: Excitatory acetylcholine receptors.
mixed spinal nerve: A nerve that carries motor, sensory, and autonomic signals between the spinal cord and the body.
peripheral nervous system: The nerves and ganglia outside of the brain and spinal cord.
muscarinic: Acetylcholine receptors
that can be both excitatory and inhibitory.
Review of Peripheral Nervous System Structure
The peripheral nervous system (PNS) consists of the nerves and ganglia outside of the brain and spinal cord. The main function of the PNS is to connect the central nervous system (CNS) to the limbs and organs.
Unlike the CNS, the PNS is not protected by the bones of the spine and skull, or by the blood –brain barrier, leaving it exposed to toxins and mechanical injuries. The peripheral nervous system is divided into the somatic nervous system and the autonomic nervous system.
Spinal nerve: This diagram indicates the formation of a typical spinal nerve from the dorsal and ventral roots. Numbers indicate the types of nerve fibers: 1 somatic efferent, 2 somatic afferent, 3–5 sympathetic efferent, 6–7 sympathetic afferent.
The peripheral nervous system includes 12 cranial nerves and 31 pairs of spinal nerves that provide communication from the CNS to the rest of the body by nerve impulses to regulate the functions of the human body. The term spinal nerve generally refers to a mixed spinal nerve, which carries motor, sensory, and autonomic signals between the spinal cord and the body.
Spinal Nerve Correspondences
Each pair of spinal nerves roughly correspond to a segment of the vertebral column: 8 cervical spinal nerve pairs (C1–C8), 12 thoracic pairs (T1–T12), 5 lumbar pairs (L1–L5), 5 sacral pairs (S1–S5), and 1 coccygeal pair.
The first 4 cervical spinal nerves, C1 through C4, split and recombine to produce a variety of nerves that subserve the neck and back of the head.
The spinal nerve C1 (suboccipital nerve) provides motor innervation to muscles at the base of the skull.
C2 and C3 form many of the nerves of the neck, and provides both sensory and motor control. These include the greater occipital nerve that provides sensation to the back of the head, the lesser occipital nerve that provides sensation to the area behind the ears, the greater auricular nerve, and the lesser auricular nerve.
The phrenic nerve arises from nerve roots C3, C4, and C5. It innervates the diaphragm to enable breathing. If the spinal cord is transected above C3, then spontaneous breathing is not possible.
The last four cervical spinal nerves, C5 through C8, and the first thoracic spinal nerve, T1, combine to form the brachial plexus, or plexus brachialis, a tangled array of nerves, splitting, combining and recombining to form the nerves that subserve the upper limb region and upper back. Although the brachial plexus may appear tangled, it is highly organized and predictable with little variation among people.
Lumbosacral Plexus
The anterior divisions of the lumbar, sacral, and coccygeal nerves form the lumbosacral plexus, the first lumbar nerve being frequently joined by a branch from the twelfth thoracic. For descriptive purposes, this plexus is usually divided into three parts: lumbar plexus, sacral plexus, and pudendal plexus.
Autonomic Nervous System Function (ANS)
The sympathetic division typically functions in actions that need quick responses. The parasympathetic division functions with actions that do not require immediate reaction.
The sympathetic system is often considered the fight or flight system, while the parasympathetic system is often considered the rest and digest or feed and breed system.
Some typical actions of the sympathetic and parasympathetic systems are listed below.
Sympathetic Nervous System
Diverts blood flow away from the gastrointestinal (GI) tract and skin via vasoconstriction.
Enhances blood flow to skeletal muscles and the lungs.
Dilates bronchioles of the lung by circulating epinephrine to allow for greater alveolar oxygen exchange.
Increases the heart rate and contractility of cardiac muscle for enhanced blood flow to skeletal muscles.
Dilates pupils and relaxes the ciliary muscle to the lens for far vision.
Provides vasodilation for the coronary vessels of the heart.
Constricts all the intestinal sphincters and the urinary sphincter.
Inhibits peristalsis.
Stimulates orgasm.
Parasympathetic Nervous System
Dilates blood vessels that lead to the GI tract to increase blood flow; this is important following food consumption due to the greater metabolic demands placed on the body by the gut.
Constricts the bronchiolar diameter when the need for oxygen has diminished.
Manages heart control via dedicated cardiac branches of the vagus and thoracic spinal accessory nerves.
Constricts the pupil and contracts the ciliary muscles to facilitate accommodation for closer vision.
Stimulates salivary gland secretion and accelerates peristalsis to mediate the digestion of food.
PNS nerves are involved in the erection of genital tissues via the pelvic splanchnic nerves 2–4. They are also responsible for stimulating sexual arousal.
Neurotransmitters
Acetylcholine is the preganglionic neurotransmitter for both divisions of the ANS, as well as the postganglionic neurotransmitter of parasympathetic neurons.
Nerves that release acetylcholine are said to be cholinergic. In the parasympathetic system, ganglionic neurons use acetylcholine as a neurotransmitter to stimulate muscarinic receptors.
At the adrenal medulla, there is no postsynaptic neuron. Instead, the presynaptic neuron releases acetylcholine to act on nicotinic receptors.
Stimulation of the adrenal medulla releases adrenaline (epinephrine) into the bloodstream, which acts on adrenoceptors, producing a widespread increase in sympathetic activity.
Autonomic nervous sytem: The functions of the parasympathetic and sympathetic nervous systems are detailed.
Somatic Nervous System Function (SoNS)
The somatic nervous system consists of afferent and efferent nerves and is associated with the voluntary control of skeletal muscle movements. The afferent nerves are responsible for relaying sensations from the body to the central nervous system (CNS), while the efferent nerves are responsible for sending out commands from the CNS to the body to stimulate muscle contraction.
Upper motor neurons release acetylcholine. Acetylcholine is released from the axon terminal knobs of alpha motor neurons and received by postsynaptic receptors (nicotinic acetylcholine receptors) of muscles, thereby relaying the stimulus to contract muscle fibers.
Blood Supply and Lymphatics
The spinal cord receives both longitudinal and segmental blood supply. The vasculature is highly complex and anastomotic which ensures adequate delivery to the entire structure. Longitudinally, the anterior spinal artery (ASA) and a pair of posterior spinal arteries (PSAs) are the predominant supply of the spinal cord. The three arteries branch from the distal vertebral arteries at the base of the skull. The three vessels connect circumferentially around the cord as the vaso-corona to supply the entire periphery of the cord.[rx] Numerous radicular arteries are also arranged segmentally which provide additional blood flow to the entire vertebral column. Many of these are branches of segmental intercostal and lumbar arteries.[rx][rx]
or
Three lumbar vertebral arteries surround each lumbar vertebral body. Lumbar vertebral arteries are direct branches off of the aorta. Spinal arterial branches differentiate into radicular and segmental arteries. Segmental branches supply vertebral bodies, and posterior arterial branches supply vertebral arches. Spinal branches enter the vertebral canal through intervertebral foramina to supply the bones, periosteum, ligaments, and meninges. Radicular and segmental arteries supply spinal nerve roots, spinal nerves, and the spinal cord. Venous drainage of the vertebral column parallels the arterial system. Additionally, there is an internal anterior lumbar venous plexus; and a posterior external venous plexus.[rx]
Diseases of the Cranial Nerves 12 mean the specific abnormality that is happening in cranial nerves are peripheral nerves except for the optic nerve which is a central nervous system tract. Disorders of particular note include the following: Olfactory (I) nerve—anosmia is most commonly encountered as a sequel to head injury.
Third, fourth, and sixth cranial nerves—complete lesions lead to the following deficits
(1) third nerve—a dilated and unreactive pupil, complete ptosis, and loss of upward, downward, and medial movement of the eye;
(2) fourth nerve—extorsion of the eye when the patient looks outwards, with diplopia when the gaze is directed downwards and medially;
(3) sixth nerve—convergent strabismus, with the inability to abduct the affected eye and diplopia maximal on lateral gaze to the affected side. The third, fourth, and sixth nerves may be affected singly or in combination: in older patients, the commonest cause is a vascular disease of the nerves themselves or their nuclei in the brainstem.
Other causes of lesions include (1) false localizing signs—third or sixth nerve palsies related to the displacement of the brainstem produced by supratentorial space-occupying lesions; (2) intracavernous aneurysm of the internal carotid artery—third, fourth, and sixth nerve lesions. Lesions of these nerves can be mimicked by myasthenia gravis
Diseases of the Cranial Nerves – Test and Examination
Facial nerve palsy is paresis of the muscles supplied by the facial nerve (VII) on 1 side of the face due to a lesion of the facial nerve. The paresis generally only occurs on 1 side, but it may also occur on both sides. Usually, it is temporary. Initially, the patient suffers from non-specific dragging pain in the region of the ear before the paresis develops over several hours or days.
This occurs in 10–35 cases/100,000 inhabitants. During pregnancy, the prevalence increases 3 times, especially in the 1st trimester. This condition has a universal distribution and has no predilection for ethnicity or age.
Possible causes for facial nerve paresis:
Viral and bacterial infections
Stroke/ischemic lesions
Basal skull fracture
Tumors in the petrous bone or the parotid gland
Intracranial injury
Toxic causes
Idiopathic causes
Chromosomal damage
Depending on the location of the lesion, one distinguishes between central and peripheral facial nerve palsy.
In both, rehabilitation must be started as soon as possible to avoid complications.
Peripheral facial nerve paresis
Peripheral facial nerve paresis involves lesions of the 2nd motor neuron, the anterior motor horn, the peripheral nerves, or the muscles outside the central nervous system. Peripheral facial nerve palsy is characterized by a weakened myotatic reflex, negative pyramidal tract signs, a slack tone, and atrophy of the affected muscles.
Idiopathic facial nerve palsy (Bell’s palsy) is the most frequent peripheral cranial nerve lesion, and it is accompanied by a single-sided and acute occurrence of peripheral facial nerve palsy. This disease can occur at any age, often between the ages of 10–20 and 30–40 years. Women seem to be affected more frequently than men.
Bell’s palsy heals in approx. 70% of cases without any consequences, but persistent defects after re-innervation may remain.
As a consequence of 1-sided peripheral facial palsy, the following actions are no longer possible:
Frowning
Raising eyebrows
Closing the eyes
Puffing out the cheeks
Whistling
Showing the teeth
These symptoms also suggest the failure of the nerve, and weakness or complete paresis of the mimic muscles may result. Symptoms include:
Bell’s phenomenon (incomplete closure of the eyelid)
Upward rotation of the eyeball becomes visible
Drooping of the labial angle and the lower eyelid
Elapsed nasolabial fold
Slackened platysma
Disorders of lacrimation, headache, gustatory disturbances in the anterior 3rd of the tongue, ear pain, and increased hearing sensation are other accompanying symptoms.
Causes of Bell’s palsy are:
Herpes zoster infections
Otitis media
Guillain-Barré syndrome
HIV infection tumor
Ischemic stroke
Autoimmune disease
Lyme disease
Among others.
Central facial palsy
Central facial palsy is due to a lesion of the 1st motor neuron in the region of the brain or its descending projections to the spinal cord.
Central facial palsy involves increased myotatic reflexes, weakened multisynaptic reflexes, and positive pyramidal tract signs; a cramp-like increase in the tone of the affected muscles also occurs, without any relevant atrophy. Frequently, central facial palsies are caused by cerebral circulatory impairments or brain tumors.
In contrast to peripheral facial palsy, a patient with central facial palsy can frown and close his eyelid since the peripheral nuclear areas (facial nucleus) lead to the fibers of the facial nerve and are interconnected to finally reach the forehead and the eye, which also receive fibers from the other side.
The musculature is no longer mobile – especially in the area of the mouth – and it is flaccid, as with peripheral facial palsy. Also, the labial angle droops are immobile and are partially open on the affected side.
Note: A distinguishing feature of peripheral and central facial palsy: with central facial palsy, the patient can frown and close his eyelid.
Trigeminal Neuralgia
Trigeminal neuralgia occurs in the innervation area of the trigeminal nerve in the form of a severe, acute, and recurrent attack-like facial pain that is generally single-sided. Three forms are distinguished:
Classic trigeminal neuralgia: in patients with compression of the trigeminal nerve by a presumed or demonstrated vascular loop
Secondary trigeminal neuralgia: associated with another disease such as multiple sclerosis and tumors
Idiopathic trigeminal neuralgia: when the cause is unknown
Other categories include several causes of facial pain such as painful trigeminal neuropathy due to herpes zoster virus, post-traumatic trigeminal neuropathy, painful trigeminal neuropathy attributed to other disorders, and idiopathic painful trigeminal neuropathy.
Classic trigeminal neuralgia
Previously called tic douloureux. The principal cause of this pain is the compression or mechanical irritation of the trigeminal nerve by blood vessel loops at the point where it exits the brainstem. The average age of onset is between 50–79 years.
Symptomatic trigeminal neuralgia
This form of trigeminal neuralgia accompanies demyelination diseases such as multiple sclerosis, which occurs as a consequence of either tumors or Costen’s syndrome (e.g., a facial pain that originates from the facial muscles due to malfunction of the mandibular joint). Inflammatory processes and, in rare cases, medical interventions can result in trigeminal neuralgia.
Symptomatic trigeminal neuralgia may be accompanied by hypoesthesia, i.e. reduced sensitivity towards tactile stimuli, in the form of numbness or tingling, in the region of the 1st trigeminal branch. Furthermore, the corneal reflex is weakened.
Patients with symptomatic trigeminal neuralgia are, on average, younger than patients with the classical form of the disease (tic doulourex). Double-sided facial pain often also occurs in such patients. The goal of therapy is to treat the underlying cause.
Symptoms of trigeminal neuralgia:
Attacks of shooting and severe pain, which occurs repeatedly, up to 100 times a day
Mostly, the supply area of the 2nd branch of the trigeminal nerve is affected
It can be triggered by touch, coldness, speaking, swallowing, chewing, combing hair, touching or washing the face, spicy food, vibration at walking, etc.
Due to the pain, patients are sad, powerless, anorexic, they sleep badly, and they feel weak
The patients try to avoid the trigger by reducing their mimic movement, not speaking, and not eating. Often, only fluid foods are taken in with a straw. In the cold seasons, most patients protect themselves from the cold and the wind with a scarf.
Eye muscle paresis
Oculomotor nerve palsy
The oculomotor nerve (the eye movement nerve) innervates several eye muscles and – along with the trochlear nerve (IV) and the abducens nerve (VI) – is responsible for the movement of the eyeball.
Roughly/3rd of all eye muscle pareses are caused by oculomotor nerve palsy, which is overall slightly rarer than abducens nerve palsy. In 60–70% of cases, oculomotor nerve palsy occurs as an isolated loss.
Lesions of this nerve can result in various types of paresis: complete (inner and outer) oculomotor nerve palsy.
Complete loss of the function of the nerve leads to the following clinical picture:
Ptosis (drooping of the upper eyelid)
The eyeball deviates to the outside and downwards
Widened pupil (mydriasis) and pupils unresponsive to light (totally unresponsive pupil)
Diplopia (double vision)
In cases of complete oculomotor nerve palsy, the consensual reaction of the opposite eye remains, i.e. a reflex-triggered concordant reaction occurs on the opposite side of the body. The opening of the eyelid may be possible through contraction of the frontal muscle since double vision only occurs following the elevation of the eyelid.
Causes of oculomotor nerve palsy are:
Tumor
Stroke
Infections of the central nervous system (meningitis or encephalitis)
Aneurysm
A local lesion in the base of the eye.
Ophthalmoplegia interna
Ophthalmoplegia interna involves completely unresponsive pupils accompanied by the free movement of the eyeball; the pupil does not react to either direct or indirect light nor convergence. As a result, the patient does not have a clear vision in the affected eye when looking at close objects. There is also paresis of accommodation.
Ophthalmoplegia externa
In cases of ophthalmoplegia externa, however, the motility of the eyeball is impaired, yet autonomous innervation of the pupil and the ciliary muscle is intact. If pupil function has been preserved, complete paresis of all the muscles innervated by the oculomotor nerve is quite rare.
Anisocoria
Another disease or deficit of the oculomotor nerve would be pupils of unequal width, which is referred to as anisocoria. Anisocoria is present in Claude-Bernard- Horner syndrome, which is characterized by constriction of the pupil (miosis), a drooping eyelid (ptosis), anhidrosis (decreased sweating), and posterior displacement of the eyeball (enophthalmos).
Anisocoria can also occur alongside intracranial pressure involving compression of the oculomotor nerve.
Trochlear Nerve Palsy
Trochlear nerve palsies are rarer than oculomotor or abducens nerve palsies. The most frequent cause of monosymptomatic trochlear nerve palsy is a traumatic brain injury.
Trochlear nerve palsy is characterized by isolated paresis of the superior oblique muscle. The function of this muscle is to depress the eyeball. In cases of paresis, the symptom increases during adduction and is virtually absent during abduction, i.e. the eye of the patient faces towards the nose and upwards, and the patient experiences double vision (diplopia), just as in cases of oculomotor nerve palsy.
Causes of trochlear nerve palsy are tumor, demyelination, meningitis, and other.
A distinction is made between double and single-sided trochlear nerve palsy.
Double-sided trochlear nerve palsy
In cases of double-sided trochlear nerve palsy, the Bielschowsky phenomenon is often positive on both sides. In this case, the diseased eye stands higher, is rotated outwards to the temple, and has a squint deviation to the nose, which creates oblique double vision. To compensate, the patient tries to rotate and lower the chin and to tilt the head to the healthy side.
Compensatory head-turning and tilting are usually not present, in contrast to 1-sided trochlear nerve palsy.
One-sided trochlear nerve palsy
One-sided trochlear nerve palsy is accompanied by a compensatory head posture with turning and tilting towards the healthy shoulder and lowering of the chin. The affected eye is in an abduction position and is rotated outwards. An annoying pathological rolling image is avoided since the slackened internal rotator is not utilized this way.
Abducens nerve palsy
The abducens nerve palsy is characterized by an isolated paresis of the rectus lateralis muscle (an externally turning muscle), which often occurs without identifiable intracranial lesions. In a high percentage of cases, the cause of these palsies remains idiopathic. However, trauma, a diabetic metabolic state, and increased intracranial pressure due to tumor or meningitis are some causes of abducens nerve palsy.
In cases of abducens nerve palsy, convergent paralytic strabismus occurs even in the primary position, i.e. the affected eye deviates towards the inside and the paralyzed eye is impaired or inhibited if it tries to turn to look to the side or to look up.
Furthermore, a slight adduction position can occur when looking up or down. Undisturbed binocular movement is, however, observed when looking to the healthy side.
Horizontally parallel double images (i.e. double vision) are usually perceived even in the primary position. The deviation of the images of objects on the retina increases on the paralyzed side, but when the affected eye is covered, the image corresponding to the respective side disappears.
However, the annoying phenomenon of double vision causes a compensatory head posture, which leads to the head being turned towards the side of the paralyzed muscle – a position that does not require the rectus lateralis muscle.
Lesions of the visual pathway
Each optic tract consists of ‘2 half, former’ optical nerves. They conduct the lateral part of the visual information coming from the same side and also the medial sensations of the opposite side.
The visual pathway crosses the whole brain. Very differing deficits in the visual field may arise depending on the location of the lesion. Therefore, when there is a lesion in the visual pathway, the visual field is examined, and pupil reaction and the appearance of the papilla are examined.
The following deficits in the visual field can occur as a result of nerve lesions:
If the optic nerve is severely damaged on 1 side, the patient is blind on the affected eye, and their sight is not impaired on the other side.
When there is a lesion of the medial part of the optic chiasm, it is mainly the fibers that cross to the other side that are damaged. The patient can suffer from a bitemporal (heteronymous) hemianopsia, i.e the patient does not get any visual information relating to what happens in his lateral field of vision. This is referred to as hemianopsia, or ‘blinker vision.’ The lateral section, which does not cross and leads to the optic tract, remains intact, meaning sight in this part of the visual field is not impaired.
Visual loss can also affect the optic tract. For example, the patient may have a lesion in the right optic tract which leads to a deficit in the left half of the visual field of both eyes. This failure is referred to as bilateral homonymous hemianopsia (left). A lesion of the left optic tract would lead to a corresponding opposite deficit in the right half of the visual field. Depending on where the optic tract is damaged, this may lead to a complete or an incomplete deficit. Once such deficits have arisen, they do not usually disappear.
Further lesions can arise in the realm of visual radiation, and such lesions have diverse consequences since visual radiation spreads a fan-like manner. Tumors and strokes are the most frequent triggers for this visual disorder.
Deficits in the visual field can be observed in the following form:
First: Pathology to the right part of the visual radiation produces left homonymous hemianopsia
Second: Pathology to the leftward side of the visual radiation produces right homonymous hemianopsia
Quadrantanopsia occurs whenever there is only partial damage to the visual radiation such that a quadrant of the visual field is missing rather than an entire half.
Deficits in the upper part of the visual radiation are more severe than in the lower part. Deficits in the area of the visual radiation likewise do not regress either.
Amaurosis
This term refers to a complete loss of vision without apparent lesions in the eye; it can occur in 1 or 2 eyes. Amaurosis can be congenital (Leber’s congenital amaurosis) or secondary. What this means for the optic nerve is that injury is commonly secondary to compression of the nerve by tumor (commonly from the pituitary), trauma, or ischemic events.
Summary of the Important Diseases of All 12 Pairs of Cranial Nerves
Olfactory nerve (I)
Anosmia (inability to smell)
Hyposmia (weakened ability to smell)
Optical nerve (II)
Anopsia or amaurosis (blindness in 1 or both eyes)
Hemianopsia
Quadrant anopsia
Blinker-phenomenon
Papilledema
Oculomotor nerve (III)
Anisocoria (unequally wide pupils)
Miosis (narrow pupils)
Mydriasis (wide pupils)
Gaze palsy
Diplopia (double vision)
Ptosis (drooping upper eyelid)
Trochlear nerve (IV)
Strabismus
Diplopia
Trigeminal nerve (V)
Trigeminal neuralgia/tic doulourex
Paresis of the muscles of mastication
Loss of the sensation of touch and temperature
Abducens nerve (VI)
Diplopia
Facial nerve (VII)
Bell’s palsy (paralysis of the the facial muscles)
Hyperacusis (sounds are perceived too loud)
Loss of gustatory sensation in the anterior tongue
Burning eye sensation due to dehydration of the conjunctiva/cornea
Vestibulocochlear nerve (VIII)
Hypacusis (hearing loss)
Deafness
Tinnitus (permanent aural noises)
Ataxia (instability regarding movement)
Rotatory vertigo
Nystagmus (eye twitching)
Glossopharyngeal nerve (IX)
Difficulty swallowing
Diminished salivation
Loss of gustatory sensation in the posterior part of the tongue
Loss of sensation in the throat
Vagus nerve (X)
Hoarseness
Difficulties with swallowing and at phonation
Posticus paralysis (severe respiratory distress when a particular muscle of the larynx fails)
Changes in heart rate (quicker or slower)
Less gastric acid and intestinal peristalsis
Accessory nerve (XI)
Inability to lift the shoulder
Weakness in turning the head
The hypoglossal nerve (XII)
Speech disorders
Difficulty swallowing
Cranial nerve examination frequently appears in OSCEs. You’ll be expected to assess a subset of the twelve cranial nerves and identify abnormalities using your clinical skills. This cranial nerve examination OSCE guide provides a clear step-by-step approach to examining the cranial nerves, with an included video demonstration.
Download the cranial nerve examination PDF OSCE checklist, or use our interactive OSCE checklist. If you want to learn more about the cranial nerves, check out our summary. You may also be interested in our guide to dermatomes and myotomes or our pediatric neurological examination guide.
Cranial Nerves – Test and Examination
Gather equipment
Gather the appropriate equipment to perform cranial nerve examination:
Pen torch
Snellen chart
Ishihara plates
Ophthalmoscope and mydriatic eye drops (if necessary)
Cotton wool
Neuro-tip
Tuning fork (512hz)
Glass of water
Introduction
Wash your hands and don PPE if appropriate.
Introduce yourself to the patient including your name and role.
Confirm the patient’s name and date of birth.
Briefly explain what the examination will involve using patient-friendlylanguage.
Gain consent to proceed with the examination.
Ask the patient to sitonachair, approximately one arm’s length away.
Ask the patient if they have any pain before proceeding with the clinical examination.
General inspection
Perform a brief general inspection of the patient, looking for clinical signs suggestive of underlying pathology:
Speech abnormalities: may indicate glossopharyngeal or vagus nerve pathology.
Facial asymmetry: suggestive of facial nerve palsy.
Eyelid abnormalities: ptosis may indicate oculomotor nerve pathology.
Pupillary abnormalities: mydriasis occurs in oculomotor nerve palsy.
Strabismus: may indicate oculomotor, trochlear or abducens nerve palsy.
Limbs: pay attention to the patient’s arms and legs as they enter the room and take a seat noting any abnormalities (e.g. spasticity, weakness, wasting, tremor, fasciculation) which may suggest the presence of a neurological syndrome).
Look for objects or equipment on or around the patient that may provide useful insights into their medical history and current clinical status:
Walking aids: gait issues are associated with a wide range of neurological pathology including Parkinson’s disease, stroke, cerebellar disease and myasthenia gravis.
Hearing aids: often worn by patients with vestibulocochlear nerve issues (e.g. Ménière’s disease).
Visual aids: the use of visual prisms or occluders may indicate underlying strabismus.
Prescriptions: prescribing charts or personal prescriptions can provide useful information about the patient’s recent medications.
Olfactory nerve (CN I)
The olfactory nerve (CN I) transmits sensory information about odors to the central nervous system where they are perceived as smell (olfaction). There is no motor component to the olfactory nerve.
Ask the patient if they have noticed any recent changes to their senseofsmell.
Olfaction can be tested more formally using different odors (e.g. lemon, peppermint), or most formally using the University of Pennsylvania smell identification test. However, this is unlikely to be required in an OSCE.
Causes of anosmia
There are many potential causes of anosmia including:
Mucous blockage of the nose: preventing odors from reaching the olfactory nerve receptors.
Head trauma: can result in shearing of the olfactory nerve fibers leading to anosmia.
Genetics: some individuals have congenital anosmia.
Parkinson’s disease: anosmia is an early feature of Parkinson’s disease.
COVID-19: transient anosmia is a common feature of COVID-19.
Optic nerve (CN II)
The optic nerve (CN II) transmits sensory visual information from the retina to the brain. There is no motor component to the optic nerve.
Inspect the pupils
The pupil is the hole in the centre of the iris that allows light to enter the eye and reach the retina.
Assess pupil size:
Normal pupil size varies between individuals and depends on lighting conditions (i.e. smaller in bright light, larger in the dark).
Pupils are usually smaller in infancy and larger in adolescence.
Assess pupil shape:
Pupils should be round, abnormal shapes can be congenital or due to pathology (e.g. posterior synechiae associated with uveitis).
Peaked pupils in the context of trauma are suggestive of globe injury.
Assess pupil symmetry:
Note any asymmetry in pupil size between the pupils (anisocoria). This may be longstanding and non-pathological or relate to actual pathology. If the pupil is more pronounced in bright light this would suggest that the larger pupil is the abnormal pupil, if more pronounced in dark this would suggest the smaller pupil is abnormal.
Examples of asymmetry include a large pupil in oculomotor nerve palsy and a small and reactive pupil in Horner’s syndrome.
Inspect the pupils
Visual acuity
Assessment of visual acuity (distance)
Begin by assessing the patient’s visualacuity using a Snellenchart. If the patient normally uses distanceglasses, ensure these are worn for the assessment.
1. Stand the patient at 6 metres from the Snellen chart.
2. Ask the patient to cover one eye and read the lowest line they are able to.
3. Record the lowest line the patient was able to read (e.g. 6/6 (metric) which is equivalent to 20/20 (imperial)).
4. You can have the patient read through a pinhole to see if this improves vision (if vision is improved with a pinhole, it suggests there is a refractive component to the patient’s poor vision).
5. Repeat the above steps with the other eye.
Recording visual acuity
Visual acuity is recorded as chart distance (numerator) over the number of the lowest line read (denominator).
If the patient reads the 6/6 line but gets 2 letters incorrect, you would record as 6/6 (-2).
If the patient gets more than 2 letters wrong, then the previous line should be recorded as their acuity.
When recording the vision it should state whether this vision was unaided (UA), with glasses or with pinhole (PH).
Further steps for patients with poor vision
If the patient is unable to read the topline of the Snellenchart at 6 metres (even with pinhole) move through the following steps as necessary:
1. Reduce the distance to 3 metres from the Snellen chart (the acuity would then be recorded as 3/denominator).
2. Reduce the distance to 1 metre from the Snellen chart (1/denominator).
3. Assess if they can count the number of fingers you’re holding up (recorded as “Counting Fingers” or “CF”).
4. Assess if they can see gross hand movements (recorded as “Hand Movements” or “HM”).
5. Assess if they can detect light from a pen torch shone into each eye (“Perception of Light”/”PL” or “No Perception of Light”/”NPL”).
Assess visual acuity using a Snellen chart
Re-assess visual acuity using a pinhole
Assess visual acuity using number of fingers
Assess visual acuity using hand movements
Causes of decreased visual acuity
Decreased visual acuity has many potential causes including:
Refractive errors
Amblyopia
Ocular media opacities such as cataract or corneal scarring
Retinal diseases such as age-related macular degeneration
Optic nerve (CN II) pathology such as optic neuritis
Lesions higher in the visual pathways
Optic nerve (CN II) pathology usually causes a decrease in acuity in the affected eye. In comparison, papilloedema (optic disc swelling from raised intracranial pressure), does not usually affect visual acuity until it is at a late stage.
Pupillary reflexes
With the patient seated, dim the lights in the assessment room to allow you to assess pupillaryreflexes effectively.
Direct pupillary reflex
Assess the direct pupillary reflex:
Shine the light from your pen torch into the patient’s pupil and observe for pupillary restriction in the ipsilateral eye.
A normal direct pupillary reflex involves constriction of the pupil that the light is being shone into.
Consensual pupillary reflex
Assess the consensual pupillary reflex:
Once again shine the light from your pen torch into the same pupil, but this time observe for pupillary restriction in the contralateral eye.
A normal consensual pupillary reflex involves the contralateral pupil constricting as a response to light entering the eye being tested.
Assess direct and consensual pupillary light reflexes
Assess consensual pupillary reflex
Swinging light test
Move the pen torch rapidly between the two pupils to check for a relative afferent pupillary defect (see more details below).
Perform the swinging light test
Perform the swinging light test
Relative afferent pupillary defect 15
Relative afferent pupillary defect 15
Accommodation reflex
1. Ask the patient to focus on a distant object (clock on the wall/light switch).
2. Place your finger approximately 20-30cm in front of their eyes (alternatively, use the patient’s own thumb).
3. Ask the patient to switch from looking at the distant object to the nearby finger/thumb.
4. Observe the pupils, you should see constriction and convergence bilaterally.
Assess the accommodation reflex
Assess the accommodation reflex
Pupillary light reflex
Each afferent limb of the pupillary reflex has two efferent limbs, one ipsilateral and one contralateral.
The afferent limb functions as follows:
Sensory input (e.g. light being shone into the eye) is transmitted from the retina, along the optic nerve to the ipsilateral pretectal nucleus in the midbrain.
The two efferent limbs function as follows:
Motor output is transmitted from the pretectal nucleus to the Edinger-Westphal nuclei on both sides of the brain (ipsilateral and contralateral).
Each Edinger-Westphal nucleus gives rise to efferent nerve fibres which travel in the oculomotor nerve to innervate the ciliary sphincter and enable pupillary constriction.
Normal pupillary light reflexes rely on the afferent and efferent pathways of the reflex arc being intact and therefore provide an indirect way of assessing their function:
The direct pupillary reflex assesses the ipsilateral afferent limb and the ipsilateral efferent limb of the pathway.
The consensual pupillary reflex assesses the contralateral efferent limb of the pathway.
The swinging light test is used to detect relative afferent limb defects.
Abnormal pupillary responses
Relative afferent pupillary defect (Marcus-Gunn pupil): normally light shone into either eye should constrict both pupils equally (due to the dual efferent pathways described above). When the afferent limb in one of the optic nerves is damaged, partially or completely, both pupils will constrict less when light is shone into the affected eye compared to the healthy eye. The pupils, therefore, appear to relatively dilate when swinging the torch from the healthy to the affected eye. This is termed a relative…. afferent… pupillary defect. This can be due to significant retinal damage in the affected eye secondary to central retinal artery or vein occlusion and large retinal detachment; or due to significant optic neuropathy such as optic neuritis, unilateral advanced glaucoma and compression secondary to tumour or abscess.
Unilateral efferent defect: commonly caused by extrinsic compression of the oculomotor nerve, resulting in the loss of the efferent limb of the ipsilateral pupillary reflexes. As a result, the ipsilateral pupil is dilated and non-responsive to light entering either eye (due to loss of ciliary sphincter function). The consensual light reflex in the unaffected eye would still be present as the afferent pathway (i.e. optic nerve) of the affected eye and the efferent pathway (i.e. oculomotor nerve) of the unaffected eye remain intact.
Relative afferent pupillary defect (RAPD) 1
Relative afferent pupillary defect (RAPD) 1
Colour vision assessment
Colour vision can be assessed using Ishihara plates, each of which contains a colored circle of dots. Within the pattern of each circle are dots that form a number or shape that is clearly visible to those with normal color vision and difficult or impossible to see for those with a red-green color vision defect.
How to use Ishihara plates
If the patient normally wears glasses for reading, ensure these are worn for the assessment.
1. Ask the patient to cover one of their eyes.
2. Then ask the patient to read the numbers on the Ishihara plates. The first page is usually the ‘test plate’ which does not test color vision and instead assesses contrast sensitivity. If the patient is unable to read the test plate, you should document this.
3. If the patient is able to read the test plate, you should move through all of the Ishihara plates, asking the patient to identify the number on each. Once the test is complete, you should document the number of plates the patient identified correctly, including the test plate (e.g. 13/13).
4. Repeat the assessment on the other eye.
Assess colour vision using an Ishihara chart at arms length
Ensure the patient can read the Ishihara test plate
Ask the patient to read the numbers on the Ishihara plates
Colour vision deficiencies
Colour vision deficiencies can be congenital or acquired. Some causes of acquired colour vision deficiency include:
Optic neuritis: results in a reduction of colour vision (typically red).
Vitamin A deficiency
Chronic solvent exposure
Visual neglect/inattention
Visualneglect (also known as visual inattention) is a condition in which an individual develops a deficit in their awareness of one side of their visualfield. This typically occurs in the context of parietal lobe injury after stroke, which results in an inability to perceive or process stimuli on one side of the body. The side of the visual field that is affected is contralateral to the location of the parietal lesion. It should be noted that visual neglect is not caused by optic nerve pathology and therefore this test is often not included in a cranial nerve exam.
Assessment
To assess for visualneglect:
1. Position yourself sitting opposite the patient approximately 1 metre away.
2. Ask the patient to remain focused on a fixed point on your face (e.g. nose) and to state if they see your left, right or both hands moving.
3. Hold your hands out laterally with each occupying one side of the patient’s visual field (i.e. left and right).
4. Take turns wiggling a finger on each hand to see if the patient is able to correctly identify which hand has moved.
5. Finally wiggle both fingers simultaneously to see if the patient is able to correctly identify this (often patients with visual neglect will only report the hand moving in the unaffected visual field – i.e. ipsilateral to the primary brain lesion).
Assess for visual inattention
Assess for visual inattention
Visual fields
This method of assessment relies on comparing the patient’s visual field with your own and therefore for it to work:
you need to position yourself, the patient and the target correctly (see details below).
you need to have normal visual fields and a normal-sized blindspot.
Visual field assessment
1. Sit directly opposite the patient, at a distance of around 1 metre.
2. Ask the patient to cover one eye with their hand.
3. If the patient covers their right eye, you should cover your left eye (mirroring the patient).
4. Ask the patient to focus on part of your face (e.g. nose) and not move their head or eyes during the assessment. You should do the same and focus your gaze on the patient’s face.
5. As a screen for central visual field loss or distortion, ask the patient if any part of your face is missing or distorted. A formal assessment can be completed with an Amsler chart.
6. Position the hatpin (or another visual target such as your finger) at an equal distance between you and the patient (this is essential for the assessment to work).
7. Assess the patient’s peripheral visual field by comparing to your own and using the target. Start from the periphery and slowly move the target towards the centre, asking the patient to report when they first see it. If you are able to see the target but the patient cannot, this would suggest the patient has a reduced visual field.
8. Repeat this process for each visual field quadrant, then repeat the entire process for the other eye.
9. Document your findings.
Assess the patient’s peripheral visual fields
Assess the patient’s peripheral visual fields
Types of visual field defects
Types of visual field defects
Bitemporal hemianopia: loss of the temporal visual field in both eyes resulting in central tunnel vision. Bitemporal hemianopia typically occurs as a result of optic chiasm compression by a tumour (e.g. pituitary adenoma, craniopharyngioma).
Homonymous field defects: affect the same side of the visual field in each eye and are commonly attributed to stroke, tumour, abscess (i.e. pathology affecting visual pathways posterior to the optic chiasm). These are deemed hemianopias if half the vision is affected and quadrantanopias if a quarter of the vision is affected.
Scotoma: an area of absent or reduced vision surrounded by areas of normal vision. There is a wide range of possible aetiologies including demyelinating disease (e.g. multiple sclerosis) and diabetic maculopathy.
Monocular vision loss: total loss of vision in one eye secondary to optic nerve pathology (e.g. anterior ischaemic optic neuropathy) or ocular diseases (e.g. central retinal artery occlusion, total retinal detachment).
Blind spot
A physiological blind spot exists in all healthy individuals as a result of the lack of photoreceptor cells in the area where the optic nerve passes through the optic disc. In day to day life, the brain does an excellent job of reducing our awareness of the blind spot by using information from other areas of the retina and the other eye to mask the defect.
Blind spot assessment
1. Sit directly opposite the patient, at a distance of around 1 metre.
2. Ask the patient to cover one eye with their hand.
3. If the patient covers their right eye, you should cover your left eye (mirroring the patient).
4. Ask the patient to focus on part of your face (e.g. nose) and not move their head or eyes during the assessment. You should do the same and focus your gaze on the patient’s face.
5. Using a red hatpin (or alternatively, a cotton bud stained with fluorescein/pen with a red base) start by identifying and assessing the patient’s blindspot in comparison to the size of your own. The red hatpin needs to be positioned at an equal distance between you and the patient for this to work.
6. Ask the patient to say when the red part of the hatpin disappears, whilst continuing to focus on the same point on your face.
7. With the red hatpin positioned equidistant between you and the patient, slowly move it laterally until the patient reports the disappearance of the top of the hatpin. The blind spot is normally found just temporal to central vision at eye level. The disappearance of the hatpin should occur at a similar point for you and the patient.
8. After the hatpin has disappeared for the patient, continue to move it laterally and ask the patient to let you know when they can see it again. The point at which the patient reports the hatpin re-appearing should be similar to the point at which it re-appears for you (presuming the patient and you have a normal blind spot).
9. You can further assess the superior and inferior borders of the blind spot using the same process.
Assess the patient’s blind spot
The blind spot is located just temporal to central vision at eye level
Fundoscopy
In the context of a cranial nerve examination, fundoscopy is performed to assess the opticdisc for signs of pathology (e.g. papilloedema). You should offer to perform fundoscopy in your OSCE, however, it may not be required. See our dedicated fundoscopy guide for more details.
The oculomotor (CN III), trochlear (CN IV) and abducens (CN VI) nerves transmit motor information to the extraocular muscles to control eye movement and eyelid function. The oculomotor nerve also carries parasympathetic fibres responsible for pupillary constriction.
Eyelids
Inspect the eyelids for evidence of ptosis which can be associated with:
Oculomotor nerve pathology
Horner’s syndrome
Neuromuscular pathology (e.g. myasthenia gravis)
Eye movements
Briefly assess for abnormalities of eyemovements which may be caused by underlying cranial nerve palsy (e.g. oculomotor, trochlear, abducens, vestibular nerve pathology).
1. Hold your finger (or a pin) approximately 30cm in front of the patient’s eyes and ask them to focus on it. Look at the eyes in the primary position for any deviation or abnormal movements.
2. Ask the patient to keep their head still whilst following your finger with their eyes. Ask them to let you know if they experience any double vision or pain.
3. Move your finger through the various axes of eye movement in a ‘H’ pattern.
4. Observe for any restriction of eye movement and note any nystagmus (which may suggest vestibular nerve pathology or stroke).
Assess eye movements
Assess eye movements
Actions of the extraocular muscles
Superior rectus: primary action is elevation, secondary actions include adduction and medial rotation of the eyeball.
Inferior rectus: primary action is depression, secondary actions include adduction and lateral rotation of the eyeball.
Medial rectus: adduction of the eyeball.
Lateral rectus: abduction of the eyeball.
Superior oblique: depresses, abducts and medially rotates the eyeball.
Inferior oblique: elevates, abducts and laterally rotates the eyeball.
Oculomotor, trochlear and abducens nerve palsy
Damage to any of the three cranial nerves innervating the extraocular muscles can result in paralysis of the corresponding muscles.
Oculomotor nerve palsy (CN III)
The oculomotor nerve supplies all extraocular muscles except the superior oblique (CNIV) and the lateralrectus (CNVI). Oculomotor palsy (a.k.a. ‘third nerve palsy’), therefore, results in the unopposed action of both the lateral rectus and superior oblique muscles, which pull the eye inferolateral. As a result, patients typically present with a ‘down and out’ appearance of the affected eye.
Oculomotor nerve palsy can also cause ptosis (due to a loss of innervation to levator palpebrae superioris) as well as mydriasis due to the loss of parasympathetic fibres responsible for innervating to the sphincter pupillae muscle.
Trochlear nerve palsy (CN IV)
The only muscle the trochlear nerve innervates is the superior oblique muscle. As a result, trochlear nerve palsy (‘fourth nerve palsy’) typically results in vertical diplopia when looking inferiorly, due to loss of the superior oblique’s action of pulling the eye downwards. Patients often try to compensate for this by tilting their heads forwards and tucking their chin in, which minimises vertical diplopia. Trochlear nerve palsy also causes torsional diplopia (as the superior oblique muscle assists with intorsion of the eye as the head tilts). To compensate for this, patients with trochlear nerve palsy tilt their head to the opposite side, in order to fuse the two images together.
Abducens nerve palsy (CN VI)
The abducens nerve (CN VI) innervates the lateral rectus muscle. Abducens nerve palsy (‘sixth nerve palsy’) results in unopposed adduction of the eye (by the medial rectus muscle), resulting in a convergent squint. Patients typically present with horizontal diplopia which is worsened when they attempt to look towards the affected side.
Assessment of strabismus
Strabismus is a condition in which the eyes do not properly align with each other when looking at an object. Pathology affecting the oculomotor, trochlear or abducens nerves can cause strabismus.
Light reflex test (a.k.a. corneal reflex test or Hirschberg test)
1. Ask the patient to focus on a target approximately half a metre away whilst you shine a pen torch towards both eyes.
2. Inspect the corneal reflex on each eye:
If the ocular alignment is normal, the light reflex will be positioned centrally and symmetrically in each pupil.
Deflection of the corneal light reflex in one eye suggests a misalignment.
Cover test
The cover test is used to determine if a heterotropia (i.e. manifest strabismus) is present.
1. Ask the patient to fixate on a target (e.g. light switch).
2. Occlude one of the patient’s eyes and observe the contralateral eye for a shift in fixation:
If there is no shift in fixation in the contralateral eye, while covering either eye, the patient is orthotropic (i.e. normal alignment).
If there is a shift in fixation in the contralateral eye, while covering the other eye, the patient has a heterotropia.
3. Repeat the cover test on the other eye.
The direction of the shift in fixation determines the type of tropia; the table below describes the appropriate interpretation.
Interpretation of the cover test
Direction of eye at rest
The direction of shift in fixation of the unoccluded eye when the opposite eye is occluded
Type of tropia present
Temporally (i.e. laterally or outwards)
Nasally (i.e. medially or inwards)
Exotropia
Nasally (i.e. medially or inwards)
Temporally (i.e. laterally or outwards)
Esotropia
Superiorly (i.e. upwards)
Inferiorly (i.e. downwards)
Hypertropia
Inferiorly (i.e. downwards)
Superiorly (i.e. upwards)
Hypotropia
Cover test interpretation
Trigeminal nerve (CN V)
The trigeminal nerve (CN V) transmits both sensory information about facial sensation and motor information to the muscles of mastication.
The trigeminal nerve has three sub-divisions, each of which has its own broad set of functions (not all are covered below):
Ophthalmic (V1): carries sensory information from the scalp and forehead, nose, upper eyelid as well as the conjunctiva and cornea of the eye.
Maxillary (V2): carries sensory information from the lower eyelid, cheek, nares, upper lip, upper teeth and gums.
Mandibular (V3): carries sensory information from the chin, jaw, lower lip, mouth, lower teeth and gums. Also carries motor information to the muscles of mastication (masseter, temporal muscle and the medial/lateral pterygoids) as well as the tensor tympani, tensor veli palatini, mylohyoid and digastric muscles.
Sensory assessment
First, explain the modalities of sensation you are going to assess (e.g. light touch/pinprick) to the patient by demonstrating on their sternum. This provides them with a reference of what the sensation should feel like (assuming they have no sensory deficits in the region overlying the sternum).
Ask the patient to close their eyes and say ‘yes’ each time they feel you touch their face.
Assess the sensory component of V1, V2 and V3 by testing lighttouch and pinpricksensation across regions of the face supplied by each branch:
Forehead (lateral aspect): ophthalmic (V1)
Cheek: maxillary (V2)
Lower jaw (avoid the angle of the mandible as it is supplied by C2/C3): mandibular branch (V3)
You should compare each region on both sides of the face to allow the patient to identify subtle differences in sensation.
Motor assessment
Use the muscles of mastication to assess the motorcomponent of V3:
1. Inspect the temporalis (located in the temple region) and masseter muscles (located at the posterior jaw) for evidence of wasting. This is typically most noticeable in the temporalis muscles, where a hollowing effect in the temple region is observed.
2. Palpate the masseter muscle (located at the posterior jaw) bilaterally whilst asking the patient to clench their teeth to allow you to assess and compare muscle bulk.
3. Ask the patient to open their mouth whilst you apply resistance underneath the jaw to assess the lateral pterygoid muscles. An inability to open the jaw against resistance or deviation of the jaw (typically to the side of the lesion) may occur in trigeminal nerve palsy.
Reflexes
Jaw jerk reflex
The jaw jerk reflex is a stretch reflex that involves the slight jerking of the jaw upwards in response to a downward tap. This response is exaggerated in patients with an upper motor neuron lesion. Both afferent and efferent pathways of the jaw jerk reflex involve the trigeminal nerve.
To assess the jaw jerk reflex:
1. Clearly explain what the procedure will involve to the patient and gain consent to proceed.
2. Ask the patient to open their mouth.
3. Place your finger horizontally across the patient’s chin.
4. Tap your finger gently with the tendon hammer.
5. In healthy individuals, this should trigger a slight closure of the mouth. In patients with upper motor neuron lesions, the jaw may briskly move upwards causing the mouth to close completely.
Corneal reflex
The corneal reflex involves involuntary blinking of both eyelids in response to unilateral corneal stimulation (direct and consensual blinking). The afferent branch of the corneal reflex involves V1 of the trigeminal nerve whereas the efferent branch is mediated by the temporal and zygomatic branches of the facial nerve.
To assess the cornealreflex:
1. Clearly explain what the procedure will involve to the patient and gain consent to proceed.
2. Gently touch the edge of the cornea using a wisp of cotton wool.
3. In healthy individuals, you should observe both direct and consensual blinking. The absence of a blinking response suggests pathology involving either the trigeminal or facial nerve.
The corneal reflex is not usually assessed in an OSCE scenario, however, you should offer to test it and understand the purpose behind the test.
Assess light touch sensation (V1)
Assess light touch sensation (V2)
Assess light touch sensation (V3)
Assess pinprick sensation (V1, V2, V3)
Assess masseter muscle bulk
Mouth opening against resistance
Assess jaw jerk reflex
Assess corneal reflex
Facial nerve (CN VII)
The facial nerve (CN VII) transmits motor information to the muscles of facial expression and the stapedius muscle (involved in the regulation of hearing). The facial nerve also has a sensory component responsible for the conveyance of taste from the anterior two-thirds of the tongue.
Sensory assessment
Ask the patient if they have noticed any recent changes in their sense of taste.
Motor assessment
Hearing changes
Ask the patient if they have noticed any changes to their hearing (paralysis of the stapedius muscle can result in hyperacusis).
Inspection
Inspect the patient’s face at rest for asymmetry, paying particular attention to:
Forehead wrinkles
Nasolabial folds
Angles of the mouth
Facial movement
Ask the patient to carry out a sequence of facialexpressions whilst again observing for asymmetry:
Raised eyebrows: assesses frontalis – “Raise your eyebrows as if you’re surprised.”
Closed eyes: assesses orbicular oculi – “Scrunch up your eyes and don’t let me open them.”
Blown out cheeks: assesses orbicularis oris – “Blow out your cheeks and don’t let me deflate them.”
Smiling: assesses levator anguli oris and zygomaticus major – “Can you do a big smile for me?”
Pursed lips: assesses orbicularis oris and buccinator – “Can you try to whistle?”
“Raise your eyebrows”
“Tightly close your eyes and don’t let me open them”
“Blow out your cheeks”
“Purse your lips”
“Smile for me”
Facial nerve palsy
Facial nerve palsy presents with unilateral weakness of the muscles of facial expression and can be caused by both upper and lower motor neuron lesions.
Facial nerve palsy caused by a lower motor neuron lesion presents with weakness of all ipsilateral muscles of facial expression, due to the loss of innervation to all muscles on the affected side. The most common cause of lower motor neuron facial palsy is Bell’s palsy.
Facial nerve palsy caused by an upper motor neuron lesion also presents with unilateral facial muscle weakness, however, the upper facial muscles are partially spared because of bilateral cortical representation (resulting in forehead/frontalis function being somewhat maintained). The most common cause of upper motor neuron facial palsy is stroke.
Bell’s palsy 2, 3
Vestibulocochlear nerve (CN VIII)
The vestibulocochlear nerve (CN VIII) transmits sensory information about sound and balance from the inner ear to the brain. The vestibulocochlear nerve has no motor component.
Gross hearing assessment
Preparation
Ask the patient if they have noticed any change in their hearing recently.
Explain that you’re going to say 3 words or 3 numbers and you’d like the patient to repeat them back to you (choose two-syllable words or bi-digit numbers).
Assessment
1. Position yourself approximately 60cm from the ear and then whisper a number or word.
2. Mask the ear not being tested by rubbing the tragus. Do not place your arm across the face of the patient when rubbing the tragus, it is far nicer to occlude the ear from behind the head. If possible shield the patient’s eyes to prevent any visual stimulus.
3. Ask the patient to repeat the number or word back to you. If they get two-thirds or more correct then their hearing level is 12db or better. If there is no response use a conversational voice (48db or worse) or loud voice (76db or worse).
4. If there is no response you can move closer and repeat the test at 15cm. Here the thresholds are 34db for a whisper and 56db for a conversational voice.
5. Assess the other ear in the same way.
Whisper a number 60cm from the ear
Mask the ear not being tested by rubbing the tragus
Rinne’s test
1. Place a vibrating 512 Hz tuning fork firmly on the mastoid process (apply pressure to the opposite side of the head to make sure the contact is firm). This tests bone conduction.
2. Confirm the patient can hear the sound of the tuning fork and then ask them to tell you when they can no longer hear it.
3. When the patient can no longer hear the sound, move the tuning fork in front of the external auditory meatus to test air conduction.
4. Ask the patient if they can now hear the sound again. If they can hear the sound, it suggests air conduction is better than bone conduction, which is what would be expected in a healthy individual (this is often confusingly referred to as a “Rinne’s positive” result).
Summary of Rinne’s test results
These results should be assessed in context with the results of Weber’s test before any diagnostic assumptions are made:
Normal result: air conduction > bone conduction (Rinne’s positive)
Sensorineural deafness: air conduction > bone conduction (Rinne’s positive) – due to both air and bone conduction being reduced equally
Conductive deafness: bone conduction > air conduction (Rinne’s negative)
Place a 512 Hz tuning fork on the mastoid process
Ask the patient to tell you when they can no longer hear it
When the patient can no longer hear the sound, moving the tuning fork in front of the external auditory meatus to test air conduction
Weber’s test
1. Tap a 512Hz tuning fork and place in the midline of the forehead. The tuning fork should be set in motion by striking it on your knee (not the patient’s knee or a table).
2. Ask the patient “Where do you hear the sound?”
These results should be assessed in context with the results of Rinne’s test before any diagnostic assumptions are made:
Normal: sound is heard equally in both ears.
Sensorineural deafness: sound is heard louder on the side of the intact ear.
Conductive deafness: sound is heard louder on the side of the affected ear.
A 512Hz tuning fork is used as it gives the best balance between time of decay and tactile vibration. Ideally, you want a tuning fork that has a long period of decay and cannot be detected by vibration sensation.
Tap a 512Hz tuning fork and place in the midline of the forehead
Conductive vs sensorineural hearing loss
Conductive hearing loss occurs when sound is unable to effectively transfer at any point between the outer ear, external auditory canal, tympanic membrane and middle ear (ossicles). Causes of conductive hearing loss include excessive ear wax, otitis externa, otitis media, perforated tympanic membrane and otosclerosis.
Sensorineural hearing loss occurs due to dysfunction of the cochlea and/or vestibulocochlearnerve. Causes of sensorineural hearing loss include increasing age (presbycusis), excessive noise exposure, genetic mutations, viral infections (e.g. cytomegalovirus) and ototoxic agents (e.g. gentamicin).
Vestibular testing – “Unterberger” or “Turning test”
Ask the patient to march on the spot with their arms outstretched and their eyes closed:
Normal result: the patient remains in the same position.
Vestibular lesion: the patient will turn towards the side of the lesion
Vestibular testing – “Head thrust test” or “Vestibular-ocular reflex”
Before performing this test you need to check if the patient has any neck problems and if so you should not proceed.
1. Explain to the patient that the test will involve briskly turning their head and then gain consent to proceed.
2. Sit facing the patient and ask them to fixate on your nose at all times during the test.
3. Hold their head in your hands (one hand covering each ear) and rotate it rapidly to the left, at a medium amplitude.
4. Repeat this process, but this time turn the head to the right.
The normal response is that ocularfixation is maintained. In a patient with loss of vestibular function on one side, the eyes will first move in the direction of the head (losing fixation), before a corrective refixation saccade occurs towards your nose.
Turning test
Glossopharyngeal (CN IX) and vagus (CN X) nerves
The glossopharyngeal nerve transmits motor information to the stylopharyngeusmuscle which elevates the pharynx during swallowing and speech. The glossopharyngeal nerve also transmits sensory information that conveys taste from the posterior third of the tongue. Visceral sensory fibres of CN IX also mediate the afferent limb of the gag reflex.
The vagus nerve transmits motor information to several muscles of the mouth which are involved in the production of speech and the efferent limb of the gag reflex.
The glossopharyngeal and vagus nerves are assessed together because of their closely related functions.
Assessment
Ask the patient if they have experienced any issues with swallowing, as well as any changes to their voice or cough.
Inspection
Ask the patient to open their mouth and inspect the softpalate and uvula:
Note the position of the uvula. Vagus nerve lesions result in deviation of the uvula towards the unaffected side.
Ask the patient to say “ahh“:
Inspect the palate and uvula which should elevate symmetrically, with the uvula remaining in the midline. A vagus nerve lesion will cause asymmetrical elevation of the palate and uvula deviation away from the lesion.
Ask the patient to cough:
Vagus nerve lesions can result in the presence of a weak, non-explosive sounding bovine cough caused by an inability to close the glottis.
Swallow assessment
Ask the patient to take a small sip of water (approximately 3 teaspoons) and observe the patient swallow. The presence of a cough or a change to the quality of their voice suggests an ineffective swallow which can be caused by both glossopharyngeal (afferent) and vagus (efferent) nerve pathology.
Gag reflex
The gag reflex involves both the glossopharyngeal nerve (afferent) and the vagus nerve (efferent). This test is highly unpleasant for patients and therefore the swallow test mentioned previously is preferred as an alternative. You should not perform this test in an OSCE, although you may be expected to have an understanding of what cranial nerves are involved in the reflex.
To perform the gagreflex:
1. Stimulate the posterior aspect of the tongue and oropharynx which in healthy individuals should trigger a gag reflex. The absence of a gag reflex can be caused by both glossopharyngeal and vagus nerve pathology.
Assess soft palate and uvula
Assess cough
Assess swallow
Accessory nerve (CN XI)
The accessory nerve (CN XI) transmits motor information to the sternocleidomastoid and trapezius muscles. It does not have a sensory component.
Assessment
To assess the accessorynerve:
1. First, inspect for evidence sternocleidomastoid or trapezius muscle wasting.
2. Ask the patient to raise their shoulders and resist you pushing them downwards: this assesses the trapezius muscle (accessory nerve palsy will result in weakness).
3. Ask the patient to turn their head left whilst you resist the movement and then repeat with the patient turning their head to the right: this assesses the sternocleidomastoid muscle (accessory nerve palsy will result in weakness).
Assess trapezius strength
Assess sternocleidomastoid strength
Hypoglossal nerve (CN XII)
The hypoglossal nerve (CN XII) transmits motor information to the extrinsicmuscles of the tongue (except for palatoglossus which is innervated by the vagus nerve). It does not have a sensory component.
Assessment
To assess the hypoglossalnerve:
1. Ask the patient to opentheirmouth and inspect the tongue for wasting and fasciculations at rest (minor fasciculations can be normal).
2. Ask the patient to protrudetheirtongue and observe for any deviation (which occurs towards the side of a hypoglossal lesion).
3. Place your finger on the patient’scheek and ask them to push their tongueagainstit. Repeat this on each cheek to assess and compare power (weakness would be present on the side of the lesion).
Inspect the tongue at rest
Inspect protruded tongue
Assess tongue power
Hypoglossal nerve palsy
Hypoglossal nerve palsy causes atrophy of the ipsilateral tongue and deviation of the tongue when protruded towards the side of the lesion. This occurs due to the overaction of the functioning genioglossus muscle on the unaffected side of the tongue.
Left hypoglossal nerve palsy 4
To complete the examination…
Explain to the patient that the examination is now finished.
Cranial nerve examination frequently appears in OSCEs. You’ll be expected to assess a subset of the twelve cranial nerves and identify abnormalities using your clinical skills. This cranial nerve examination OSCE guide provides a clear step-by-step approach to examining the cranial nerves, with an included video demonstration.
Examination of the 12 Pairs of Cranial Nerves
The diagnosis of a simple neurological disorder without EEG, CT or MRT scans is clear,manageable and cost-effective.
It consists of a light source, a neurological reflex hammer, a tuning fork and resources such as brushes, cotton swabs, and blunt pins with which a patient’s sensitivity can be examined. Test tubes filled with cold and warm water can be used to determine a patient’s sensation of cold and warm temperatures.
Anamnesis is an essential component of anysuspected diagnosis, especially in neurology. Using specifically targeted questions, the physician establishes solid medical basis for the patient for further case history and subsequent examination.
Examination of the N. Olfactorius
The olfactory nerve (n. olfactorius) is responsible for the sense of smell and is a complete sensory nerve.
The olfactory test entails individual examination of each nostril and closure of the patient’s eyes because olfactory memory leads to odor recognition. Using scented sticks with characteristic odors such as coffee, cinnamon, or aniseed, the patient is asked to smell and identify them individually, using each nostril.
According to the patient’s age and the number of odors detected, a distinction is drawn between anosmia, hyposmia and normosmia. Loss of smell (anosmia) may be attributed to:
Severe cranial cerebral trauma caused by an accident
Altered and abnormal sensory perception
Infections
Tumors, especially olfactory meningioma
Inflammation of the nasopharyngeal space, with infection of olfactory mucosa
Note: Testing with acetic acid or ammonia as a pure trigeminal irritant is useful in distinguishing sensitive and sensory disorders, especially when simulating olfactory dysfunction, such as anosmia induced organically. Despite the loss of olfactory ability, these materials are perceived as nasal irritation. A psychogenic disorder or simulation is established in the absence of any patient response.
In case of gustatory sensation (lat. gustare = taste), especially due to suspected simulation, the patient is explicitly requested to taste pure olfactory irritants (e.g., cinnamon) or mixed irritants comprising smell and taste components (e.g., cocoa with nuts). Upon taste recognition, the patient identifies the odor component, suggesting simulation.
Examination of the N. Opticus
The optic nerve (n.opticus) is the second cranial nerve, which transmits visual information to the occipital visual cortex. It is a complete sensory nerve. Visual acuity and visual fields are important aspects of the optic nerve.
Neurological examination of the optic nerve entails:
Indicative examination of visual acuity
Indicative examination of visual fields by confrontation (perimetry)
Simultaneous examination of the visual fields
Inspection of the pupils and examination of the pupil size
Indicative examination of visual acuity
Visual acuity testing is an integral component of any ophthalmological examination determining the best possible visual acuity.
Visual acuity test is used to evaluate the optical integrity of the eyes, retinal health, and the interpretation of retinal images by the brain.
Basically, the test is carried out monocularly at an approx. distance of 5 m, with the unexamined eye fully but loosely covered. The vision reading charts contain various eye test characters (optotypes) such as numbers, letters, children´s images, landolt rings and e-hooks (for patients where verbal communication is not possible). The process is repeated for both the eyes, with and without distance glasses. Another vision reading chart to determine visual acuity is the “Snellen Chart”:
The visual acuity for proximity is tested using reading samples at a reading distance of about 30 cm.
Indicative examination of visual fields by confrontation (perimetry)
The patient covers one eye while fixing their gaze on the opposite eye of the examiner with the other eye. The examiner moves an extended forefinger in different directions, from the periphery and into the patient’s visual field. The patient signals upon detection of the examiner’s finger.
The examiner should note: The examiner’s own field of vision should be used for comparison. Peripheral visual field of each eye is tested individually.
Simultaneous examination of visual fields
The patient looks at the examiner with both eyes, without covering an eye. The examiner holds his hands peripherally in the right and left visual fields, and moves his fingers randomly on one side, or simultaneously bilaterally. The patient then indicates the side or sides, in which the fingers were moved.
Inspection of the pupils and examination of the pupil size
Before testing pupillary constriction, the examiner should inspect and evaluate the function of the musculus sphincter pupillae. The examiner also tests the sympathetic fibers, which innervate the musculus dilator pupillae, and the afferent (lat. affere = to bring, to lead) pathways related to pupillary function, the retina, the optic nerve and the optic tract (tractus opticus).
When examining pupil size, pupillary constriction is tested under direct lighting using a small light source. This test is used to determine the shape, symmetry and reactivity as well as the size of the pupils. Using a semi-darkened room, the patient looks into the distance, thereby avoiding initiation of a short-range adaptation miosis (Greek miosis = reduction).
The examiner then separates the eyes from each other by placing a flat hand on the bridge of the nose. He/she then illuminates one eye with bright light at a time from a position below the pupil. The reaction of the illuminated eye is initially observed, followed by the reaction of the non-illuminated eye.
A normal result with respect to the pupil suggests symmetrical size and shape, and prompt constriction of the pupil in response to light without any side-related difference.
Examination of the N. Oculomotorius, N. Trochlearis and N. Abducens
The oculomotor (n. oculomotorius), trochlear (n. trochlearis) and abducens (n. abducens) nerves are cranial nerves with predominantly motor function, which coordinate movement of the eyeball via control of external ocular muscles. The position of the eyeball allows the examiner to determine the damaged nerve.
Each eye is controlled by six external ocular muscles, which control the full range of movement of the eyeball.
The nervus oculomotorius
The oculomotor nerve is the nerve which controls the movement of the eye and innervates the musculus rectus superior (superior rectus muscle), the musculus rectus medialis (medial rectus muscle), the musculus rectus inferior (inferior rectus muscle), and the musculus obliquus inferior (inferior oblique muscle).
To test the eye movement, the patient focuses and follows the examiner’s fingers while maintaining the head stationary in a dark room, followed by bright and dim light to study sympathetic or parasympathetic tone.
Normal finding: The patient can easily follow the examiner’s fingers in six directions, with respect to all three nerves without the eyeball lagging behind. Moreover, the patient must be able to lift their eyelids and change the ocular lens such that things that are close in front of the eye (approx. 20-30 cm) can be seen in sharp focus (visual accommodation).
Nervus trochlearis
The trochlear nerve is responsible for rotation of the eye; it innervates the superior oblique muscle and can be checked by convergence or tested using a ‘squint test’. The patient is asked to fix their gaze on the index finger of the examiner while moving the finger from a position (approx. 30–50 cm) below the patient’s face, towards the tip of the patient’s nose.
Normal finding: There should not be any side-related differences with respect to the pupils.
Nervus abducens
The abducens nerve (n. abducens) supplies the lateral rectus muscle. The patient is asked to follow an object or a lamp.
Normal finding: The patient is able to follow the object or the lamp medially or laterally, with both eyes pointing in the same direction.
Examination of the N. Trigeminus
The trigeminal nerve (n. trigeminus) is the largest cranial nerve, and has both sensory and motor functions. It provides sensory innervation to the skin of the face, to the facial mucosa, including the teeth, and also to the dura mater (part of the hard cerebral membrane). It also provides motor control to the muscles of mastication (chewing).
Examination of the trigeminal nerve is based on:
sensory function test
examination of the nerve exit points
the corneal reflex
the masseter reflex
Testing sensory functions
The skin on the patient’s face is touched gently, using a wisp of cotton wool, to test the sense of touch. The pain is evaluated with a blunt object (e.g. a wooden stick). Normal findings are symmetrical touch, and sensation of pain.
Examination of the nerve exit points
The rough tenderness of the three peripheral branches of the nerves can be assessed at their exit points: the supraorbital foramen, the infraorbital foramen and the mental foramen. The examiner presses the foramen using the thumb or middle finger. Slight tenderness is a normal finding.
The corneal reflex
The cornea is touched on one side, using a cotton swab. A normal finding is represented by normal closing of the eyelid (the blink reflex), with respect to each eye. It determines the sensation nerve V and VII.
The masseter reflex
The examiner places the index finger across a slightly open lower jaw, and taps it with a tendon hammer, which should elicit bilateral contraction of the jaw by contracting temporalis. It can be felt as an upward phasic movement of the lower jaw by pterygoids.
Examination of the N. Facialis
The facial nerve (n. facialis) is a mixed cranial nerve. It is responsible for the movement of most of the facial muscles, except the masticatory muscles, and also for the movement of platysma and the stapedius muscle in the middle ear.
Examination of the seventh cranial nerve is based on the patient’s facial expression, whether or not the nasolabial grooves carry equal depth bilaterally, depending on the symmetry of the eyelids in terms of width, and pronounced furrows of the forehead. In addition, the patient is asked to activate the facial muscles innervated by the facial nerve, for example by means of:
a frown,
puffing out the cheeks,
closing the eyes, against resistance,
firmly shutting of the eyes,
revealing the teeth or
whistling
Note: Any visible difference in terms of unilateral paresis (paralysis), arbitrary innervation, and involuntary movements relating to emotional expression (e.g., laughing). These differences may be attributed to lesions in the lower or upper motor neurons, and are not normal findings.
Examination of the N. Vestibulocochlearis
The vestibulocochlear nerve (n. vestibulocochlear) is a cranial nerve with a mainly sensory function, and comprises the vestibular and the cochlear nerves. The vestibular nerve is responsible for innervation of the organ of equilibrium (balance) and the cochlear nerve is responsible for hearing (audition).
Indicative hearing examination
With decreasing distance, and starting at 6 m, words or numbers of four syllables are directed at the patient alternating with natural and whispered speech. The test ear is inclined towards the examiner during the examination.
Normal finding: Natural language and whispering from a distance of 6 m is audible.
Note: Whispering or high-frequency tuning fork can be used in this test. The properties of tuning fork can be used to determine nerve deafness or conductive deafness.
Examination of balance
When examining the vestibular nerve, Romberg’s Test and Unterberger’s Stepping Test are two important options available. However, when it comes to testing the auditory nerve, a variety tuning fork tests are used.
With Romberg’s test, the patient stands with feet together, arms stretched forwards and eyes closed. Vestibular disease is indicated by the reproducible tendency to fall towards one side. However, a tendency for the patient to fall towards the front, towards the back or to both sides excludes neurological factors underlying the loss of motor coordination.
Unterberger’s stepping test is similar to Romberg’s test, except that the patient is additionally asked to walk on the spot with eyes closed. A vestibular disorder is present if the patient reproducibly turns more than 60º to one side. This test is used to determine peripheral labyrinthine dysfunction.
In addition to coordination of movement, the examiner evaluates nystagmus (eye movement).
Examination of the N. Glossopharyngeus and the N. Vagus
The glossopharyngeal nerve (n. glossopharyngeus) is a mixed cranial nerve containing both sensory and motor components. It provides sensitivity-related and sensory innervation to the palate and the throat, and also to the back of the tongue, especially with respect to the sensation of bitter tastes.
Examination
When examining the ninth cranial nerve, any hoarseness in the patient is evaluated. The soft palate and the uvula are also inspected. The examiner determines whether or not the soft palate is uniform in height and the uvula appears in the midline.
When clear phonation is used – ask the patient to say “Aaah” – and the finding is normal if the soft palate elevates symmetrically, and the uvula remains in the midline.
The pharyngeal reflex (the gag reflex)
The swallowing reflex is initiated through the respective motor fibers. Using the tip of a cotton swab or a sharp object usually a tongue depressor, the sense of touch is examined. It triggers reflexive elevation of the soft palate or the gag reflex.
The vagus nerve (n. vagus) provides autonomous parasympathetic innervation of the internal organs and innervates the muscles of the larynx and the upper digestive tract triggering the swallow or gag reflex.
If the reflex fails, then both the ninth and the tenth cranial nerves may be damaged, as both cerebral nerves are involved in the gag reflex. The examiner should look for any indications of swallowing disorders or cardiac arrhythmias during the examination of the pharyngeal reflex.
Examination of the N. Accessories
The accessory nerve (n. accessories) is a cranial nerve with predominantly motor function, and it innervates the sternocleidomastoid and the trapezius muscle.
The testing function of the two muscles
This examination tests the strength of the two muscles, on separate sides. The sternocleidomastoid muscle is evaluated by asking the patient to rotate their head to the side, against resistance, or by asking them to raise or shrug their shoulders against resistance, by pressing on the trapezius, using the hands.
Normal finding: Symmetrical, full strength in the innervated muscle. Lower motor nerves induce weakness in both the muscles and the upper motor nerve lesion triggers ipsilateral weakness in the sternomastoid and contralateral weakness in the trapezius muscle.
Examination of the N. Hypoglossus
The hypoglossal nerve (n. hypoglossus) is a cranial nerve with motor function, which innervates the tongue.
While examining the tongue, the examiner should pay attention to:
the symmetry of the protruded tongue
any deviation from the paralyzed side
any atrophy
The patients are also asked to move their protruded tongue back and forth quickly and to lick their lips.
Alternatively, the examiner can ask the patients to press their tongue against the inside of their cheek with all their strength. The examiner applies counter-pressure externally to assess the degree of force on both sides.
In this test, if the protruded tongue is deviated to one side, it indicates hypoglossal lesions.
12 Cranial nerves are the nerves that emerge directly from the brain (including the brainstem), of which there are conventionally considered twelve pairs. Cranial nerves relay information between the brain and parts of the body, primarily to and from regions of the head and neck, including the special senses of vision, taste, smell, and hearing.[rx]
The cranial nerves emerge from the central nervous system above the level of the first vertebrae of the vertebral column.[rx] Each cranial nerve is paired and is present on both sides. There are conventionally twelve pairs of cranial nerves, which are described with Roman numerals I–XII. Some considered there to be thirteen pairs of cranial nerves, including cranial nerve zero. The numbering of the cranial nerves is based on the order in which they emerge from the brain and brainstem, from front to back.[rx]
Brief Overview of Cranial Nerves
The characteristics of this nerve are presented in the table.
CRANIAL NERVE
NERVE TYPE
FUNCTIONS
1. Olfactory Nerve
Sensory
Smell
2. Optic Nerve
Sensory
Vision
3. Oculomotor Nerve
Motor
Eye Movement
4. Trochlear Nerve
Motor
Eyeball Movement
5. Trigeminal Nerve – Ophthalmic Branch
Sensory
Facial Muscle Movement, Chewing, Sense Temperature, touch and Pain on the Face
5. Trigeminal Nerve – Maxillary Branch
Sensory
Same as Above
5. Trigeminal Nerve – Mandibular Branch
Mixed
Same as Above
6. Abducens Nerve
Motor
Eyeball Movement
7. Facial Nerve
Mixed
Sense of Taste, Saliva and Tear Secretion, Movement of Facial Muscles
Swallowing and Secretion of Saliva, Monitors Blood Pressure, Levels of Oxygen and Carbon Dioxide in Blood
10. Vagus Nerve
Mixed
Parasympathetic Sensation, Control of Smooth Muscles of Lungs, Heart, Viscera and Secretion of Digestive Enzymes
11. Accessory Nerve
Motor
Swallowing and Movement of Head & Shoulders
12. Hypoglossal Nerve
Motor
Tongue Movement, Speech and Swallowing
The peripheral nervous system has 12 pairs of cranial nerves that control much of the motor and sensory functions of the head and neck.
Key Points
The cranial nerves serve functions such as smell, sight, eye movement, and feeling in the face. The cranial nerves also control balance, hearing, and swallowing.
The twelve cranial nerves, in order from I to XII are: olfactory nerve, optic nerve, oculomotor nerve, trochlear nerve, trigeminal nerve, abducens nerve, facial nerve, vestibulocochlear nerve, glossopharyngeal nerve, vagus nerve, spinal accessory nerve, and hypoglossal nerve.
The vagus nerve (X) has many branches and is responsible for tasks including heart rate, gastrointestinal peristalsis, sweating, and muscle movements in the mouth, including speech and keeping the larynx open for breathing.
Key Terms
innervate: To supply an organ or other body part with nerves.
peripheral nervous system: The nerves and ganglia outside of the brain and spinal cord.
peristalsis: A radially symmetrical contraction and relaxation of muscles that propagates in a wave down a tube (such as the gastrointestinal tract) in an anterograde direction.
Cranial nerves are the nerves that emerge directly from the brain (including the brainstem). In contrast, spinal nerves emerge from segments of the spinal cord. Cranial nerves relay information between the brain and parts of the body, primarily to and from regions of the head and neck.
Cranial Nerve Anatomy and Terminology
Spinal nerves emerge sequentially from the spinal cord with the spinal nerve closest to the head (C1) emerging in the space above the first cervical vertebra. The cranial nerves emerge from the central nervous system above this level.
Each cranial nerve is paired and is present on both sides. The numbering of the cranial nerves is based on the order in which they emerge from the brain, front to back (brainstem).
The terminal nerves, olfactory nerves (I) and optic nerves (II) emerge from the cerebrum or forebrain, and the remaining ten pairs arise from the brainstem, which is the lower part of the brain. The cranial nerves are considered components of the peripheral nervous system.
However, on a structural level, the olfactory, optic, and terminal nerves are more accurately considered part of the central nervous system.
The twelve cranial nerves are shown in the figure below followed by brief descriptions.
The cranial nerves: The locations of the cranial nerves within the brain.
The olfactory nerve (I): This is instrumental for the sense of smell, it is one of the few nerves that are capable of regeneration.
The optic nerve (II): This nerve carries visual information from the retina of the eye to the brain.
The oculomotor nerve (III): This controls most of the eye’s movements, the constriction of the pupil, and maintains an open eyelid.
The trochlear nerve (IV): A motor nerve that innervates the superior oblique muscle of the eye, which controls rotational movement.
The trigeminal nerve (V): This is responsible for sensation and motor function in the face and mouth.
The abducens nerve (VI): A motor nerve that innervates the lateral rectus muscle of the eye, which controls lateral movement.
The facial nerve (VII): This controls the muscles of facial expression, and functions in the conveyance of taste sensations from the anterior two-thirds of the tongue and oral cavity.
The vestibulocochlear nerve (VIII): This is responsible for transmitting sound and equilibrium (balance) information from the inner ear to the brain.
The glossopharyngeal nerve (IX): This nerve receives sensory information from the tonsils, the pharynx, the middle ear, and the rest of the tongue.
The vagus nerve (X): This is responsible for many tasks, including heart rate, gastrointestinal peristalsis, sweating, and muscle movements in the mouth, including speech and keeping the larynx open for breathing.
The spinal accessory (XI): This nerve controls specific muscles of the shoulder and neck.
The hypoglossal nerve (XII): This nerve controls the tongue movements of speech, food manipulation, and swallowing.
There are many mnemonic devices to remember the cranial nerves. One that may be helpful is: Old Opie Occasionally Tries Trigonometry And Feels Very Gloomy, Vague And Hypoactive.
Olfactory (I) Nerve
The olfactory nerve, or cranial nerve I, is the first of 12 cranial nerves and is responsible for the sense of smell.
Key Points
The olfactory nerve consists of a collection of many sensory nerve fibers that extend from the olfactory epithelium to the olfactory bulb.
Olfactory receptors within the olfactory mucosa in the nasal cavity receive information about smells that travel to the brain through the cranial nerve that extends from the olfactory epithelium to the olfactory bulb.
Olfactory receptor neurons continue to emerge throughout life and extend new axons to the olfactory bulb.
The olfactory nerve is the shortest of the 12 cranial nerves and only one of two cranial nerves (the other being the optic nerve) that do not join with the brainstem.
Key Terms
olfactory receptors: Expressed in the cell membranes of olfactory receptor neurons, these are responsible for the detection of odor molecules. Activated olfactory receptors are the initial player in a signal transduction cascade that ultimately produces a nerve impulse that is transmitted to the brain. The olfactory receptors form a multigene family consisting of over 900 genes in humans and 1,500 genes in mice.
cribriform plate: A sieve-like structure of the ethmoid bone that supports the olfactory bulb.
olfactory tract: A narrow white band made of a bundle of axons connecting the olfactory bulb to several brain regions.
ethmoid bone: An unpaired bone in the skull that separates the nasal cavity from the brain.
olfactory mucosa: Located in the upper region of the nasal cavity, this is made up of the olfactory epithelium and the underlying lamina propria, connective tissue containing fibroblasts, blood vessels, Bowman’s glands, and bundles of fine axons from the olfactory neurons.
Olfactory bulb: Sagittal section of human head showing the olfactory bulb.
The olfactory nerve, or cranial nerve I, is the first of the 12 cranial nerves. It is instrumental in the sense of smell. The olfactory nerve is the shortest of the 12 cranial nerves and only one of two cranial nerves (the other being the optic nerve) that do not join with the brainstem.
The specialized olfactory receptor neurons of the olfactory nerve are located in the olfactory mucosa of the upper parts of the nasal cavity. The olfactory nerves consist of a collection of many sensory nerve fibers that extend from the olfactory epithelium to the olfactory bulb, passing through the many openings of the cribriform plate of the ethmoid bone.
Olfactory receptor neurons continue to emerge throughout life and extend new axons to the olfactory bulb. Olfactory-ensheathing glia wrap bundles of these axons and are thought to facilitate their passage into the central nervous system.
The sense of smell (olfaction) arises from the stimulation of olfactory (or odorant) receptors by small molecules of different spatial, chemical, and electrical properties that pass over the nasal epithelium in the nasal cavity during inhalation. These interactions are transduced into electrical activity in the olfactory bulb, which then transmits the electrical activity to other parts of the olfactory system and the rest of the central nervous system via the olfactory tract.
Optic (II) Nerve
The optic nerve (cranial nerve II) receives visual information from photoreceptors in the retina and transmits it to the brain.
Key Points
The optic nerve is considered part of the central nervous system. The myelin on the optic nerve is produced by oligodendrocytes rather than Schwann cells and it is encased in the meningeal layers instead of the standard endoneurium, perineurium, and epineurium of the peripheral nervous system.
The optic nerve travels through the optic canal, partially decussates in the optic chiasm, and terminates in the lateral geniculate nucleus where information is transmitted to the visual cortex.
The axons responsible for reflexive eye movements terminate in the pretectal nucleus.
Key Terms
oligodendrocyte: A type of neuroglia that provides support and insulation to axons in the central nervous system.
retina: The thin layer of cells at the back of the eyeball where light is converted into neural signals sent to the brain.
optic nerve: Either of a pair of nerves that carry visual information from the retina to the brain.
visual cortex: The visual cortex of the brain is the part of the cerebral cortex responsible for processing visual information. It is located in the occipital lobe, in the back of the brain.
pretectal nucleus: This mediates behavioral responses to acute changes in ambient light, such as the pupillary light reflex and the optokinetic reflex.
The optic nerve is also known as cranial nerve II. It transmits visual information from the retina to the brain.
Each human optic nerve contains between 770,000 and 1.7 million nerve fibers. The eye’s blind spot is a result of the absence of photoreceptors in the area of the retina where the optic nerve leaves the eye.
Optic nerve: An illustration of the brain highlighting the optic nerve and optic tract.
The optic nerve is the second of twelve paired cranial nerves. It is considered by physiologists to be part of the central nervous system, as it is derived from an outpouching of the diencephalon during embryonic development.
As a consequence, the fibers are covered with myelin produced by oligodendrocytes, rather than Schwann cells that are found in the peripheral nervous system. The optic nerve is ensheathed in all three meningeal layers (dura, arachnoid, and pia mater) rather than the epineurium, perineurium, and endoneurium found in the peripheral nerves.
The fiber tracks of the mammalian central nervous system are incapable of regeneration. As a consequence, optic nerve damage produces irreversible blindness.
The optic nerve leaves the orbit, which is also known as an eye socket, via the optic canal, running posteromedially toward the optic chiasm, where there is a partial decussation (crossing) of fibers from the nasal visual fields of both eyes.
Most of the axons of the optic nerve terminate in the lateral geniculate nucleus (where information is relayed to the visual cortex), while other axons terminate in the pretectal nucleus and are involved in reflexive eye movements.
The optic nerve transmits all visual information including brightness perception, color perception, and contrast. It also conducts the visual impulses that are responsible for two important neurological reflexes: the light reflex and the accommodation reflex.
The light reflex refers to the constriction of both pupils that occurs when light is shone into either eye; the accommodation reflex refers to the swelling of the lens of the eye that occurs when one looks at a near object, as in reading.
Oculomotor (III) Nerve
The oculomoter nerve (cranial nerve III) controls eye movement, such as constriction of the pupil and open eyelids.
Key Points
The oculomotor nerve is the third paired cranial nerve.
The oculomotor nerve contains two nuclei, including the Edinger-Westphal nucleus that supplies parasympathetic nerve fibers to the eye to control pupil constriction and accommodation.
The oculomotor nerve originates at the superior colliculus and enters through the superior orbital fissure to control the levator palpebrae superioris muscles that hold the eyelids open.
Key Terms
levator palpebrae superioris: A muscle that elevates the upper eyelid.
superior colliculus: The primary integrating center for eye movements.
cavernous sinus: A venous channel found between layers of dura mater in the brain.
tentorium cerebelli: An extension of the dura mater that separates the cerebellum from the inferior portion of the occipital lobes.
superior orbital fissure: The superior orbital fissure is a foramen in the skull, although strictly it is more of a cleft, lying between the lesser and greater wings of the sphenoid bone.
plexus: A network or interwoven mass, especially of nerves, blood vessels, or lymphatic vessels.
The oculomotor nerve is the third paired cranial nerve. It enters the orbit via the superior orbital fissure and controls most of the eye’s movements, including constriction of the pupil and maintaining an open eyelid by innervating the levator palpebrae superiors muscle.
The oculomotor nerve is derived from the basal plate of the embryonic midbrain. Cranial nerves IV and VI also participate in the control of eye movement.
There are two nuclei for the oculomotor nerve:
The oculomotor nucleus originates at the level of the superior colliculus. The muscles it controls are the striated muscle in the levator palpebrae superioris and all extraocular muscles, except for the superior oblique muscle and the lateral rectus muscle.
The Edinger-Westphal nucleus supplies parasympathetic fibers to the eye via the ciliary ganglion and controls the pupillae muscle (affecting pupil constriction) and the ciliary muscle (affecting accommodation).
Sympathetic postganglionic fibers also join the nerve from the plexus on the internal carotid artery in the wall of the cavernous sinus and are distributed through the nerve, for example, to the smooth muscle of the levator palpebrae superioris.
Emergence from Brain
On emerging from the brain, the oculomotor nerve is invested with a sheath of pia mater and enclosed in a prolongation from the arachnoid mater. It passes between the superior cerebellar and posterior cerebral arteries, and then pierces the dura mater anterior and lateral to the posterior clinoid process (to give attachment to the tectorium cerebella), passing between the free and attached borders of the tentorium cerebelli.
It then runs along the lateral wall of the cavernous sinus, above the other orbital nerves, receiving in its course one or two filaments from the cavernous plexus of the sympathetic nervous system, and a communicating branch from the ophthalmic division of the trigeminal nerve.
It then divides into two branches that enter the orbit through the superior orbital fissure, between the two heads of the lateral rectus (a muscle on the lateral side of the eyeball in the orbit). Here the nerve is placed below the trochlear nerve and the frontal and lacrimal branches of the ophthalmic nerve, while the nasociliary nerve is placed between its two rami (the superior and inferior branch of oculomotor nerve).
Cranial nerves: Image of cranial nerves showing the position of the oculomotor nerve.
Trochlear (IV) Nerve
The trochlear nerve (cranial nerve IV) is a motor nerve that innervates a single muscle: the superior oblique muscle of the eye.
Key Points
The trochlear nerve innervates the superior oblique muscle of the eye.
The trochlear nerve contains the smallest number of axons of all the cranial nerves and has the greatest intracranial length.
The two major clinical syndromes that can arise from damage to the trochlear nerve are vertical and torsional diplopia.
Key Terms
contralateral: On the opposite side of the body.
cerebral aqueduct: The channel in the brain that connects the third ventricle to the fourth ventricle. Also called the aqueduct of Sylvius, it is surrounded by periaqueductal gray matter.
The trochlear nerve (cranial nerve IV) is a motor nerve that innervates a single muscle: the superior oblique muscle of the eye.
The trochlear nerve: The trocheal nerve and where it innervates.
The trochlear nerve is unique among the cranial nerves in several respects.
It is the smallest nerve in terms of the number of axons it contains and it has the greatest intracranial length.
Other than the optic nerve (cranial nerve II), it is the only cranial nerve that decussates (crosses to the other side) before innervating its target.
It is the only cranial nerve that exits from the dorsal aspect of the brainstem.
The nucleus of the trochlear nerve is located in the caudal mesencephalon beneath the cerebral aqueduct. It is immediately below the nucleus of the oculomotor nerve (III) in the rostral mesencephalon.
The trochlear nucleus is unique in that its axons run dorsally and cross the midline before emerging from the brainstem—so a lesion of the trochlear nucleus affects the contralateral eye. Lesions of all other cranial nuclei affect the ipsilateral side (except of course the optic nerve, cranial nerve II, which innervates both eyes).
Homologous trochlear nerves are found in all jawed vertebrates. The unique features of the trochlear nerve, including its dorsal exit from the brainstem and its contralateral innervation, are seen in the primitive brains of sharks.
The human trochlear nerve is derived from the basal plate of the embryonic midbrain.
Clinical Syndromes
There are two major clinical syndromes that can manifest through damage to the trochlear nerve:
Vertical diplopia: Injury to the trochlear nerve causes weakness of downward eye movement with consequent vertical diplopia (double vision).
Torsional diplopia: Weakness of intorsion results in torsional diplopia, in which two different visual fields, tilted with respect to each other, are seen at the same time. To compensate for this, patients with trochlear nerve palsies tilt their heads to the opposite side, in order to fuse the two images into a single visual field.
The clinical syndromes can originate from both peripheral and central lesions. A peripheral lesion is damage to the bundle of nerves, in contrast to a central lesion, which is damage to the trochlear nucleus.
Trigeminal (V) Nerve
The trigeminal nerve is the fifth cranial nerve and it is responsible for sensation and motor function in the face and mouth.
Key Points
The sensory function of the trigeminal nerve is to provide tactile, motion, position, and pain sensations for the face and mouth; its motor function activates the muscles of the jaw, mouth, and inner ear.
The trigeminal nerve has three major branches on each side—the opthalmic nerve, maxillary nerve, and mandibular nerve—that converge on the trigeminal ganglion.
The trigeminal ganglion is analogous to the dorsal root ganglia of the spinal cord, which contain the cell bodies of incoming sensory fibers from the rest of the body.
Key Terms
trigeminal ganglion: The trigeminal ganglion (also called the Gasserian ganglion, semilunar ganglion, or Gasser’s ganglion) is a sensory ganglion of the trigeminal nerve (cranial nerve V) that occupies a cavity (Meckel’s cave) in the dura mater, covering the trigeminal impression near the apex of the petrous part of the temporal bone.
trigeminal nerve: The nerve responsible for sensation and motor function in the face and mouth.
The trigeminal nerve (cranial nerve V), and it contains both sensory and motor fibers. It is responsible for sensation in the face and certain motor functions such as biting, chewing, and swallowing.
Trigeminal nerve: Schematic illustration of the trigeminal nerve (labeled Sensory root above) and the structures it innervates in the face and mouth.
The sensory function of the trigeminal nerve is to provide the tactile, motion, position, and pain sensations of the face and mouth. The motor function activates the muscles of the jaw, mouth, and inner ear.
Structure
The trigeminal nerve is the largest of the cranial nerves. Its name, trigeminal, means three twins. It is derived from the fact that each nerve, one on each side of the pons, has three major branches: the ophthalmic nerve (V1 in the illustration below), the maxillary nerve (V2), and the mandibular nerve (V3).
The ophthalmic and maxillary nerves are purely sensory. The mandibular nerve has both sensory and motor functions.
The three branches converge on the trigeminal ganglion that is located within the trigeminal cave in the brain; it contains the cell bodies of incoming sensory nerve fibers. The trigeminal ganglion is analogous to the dorsal root ganglia of the spinal cord, which contain the cell bodies of incoming sensory fibers from the rest of the body.
Areas of the face innervated by the trigeminal nerve: The ophthalmic nerve branch (V1) innervates the bright red area, the maxillary nerve branch (V2) innervates the light red area, and the mandibular nerve branch (V3) innervates the yellow area.
From the trigeminal ganglion, a single large sensory root enters the brainstem at the level of the pons. Immediately adjacent to the sensory root, a smaller motor root emerges from the pons at the same level.
Motor fibers pass through the trigeminal ganglion on their way to peripheral muscles, but their cell bodies are located in the nucleus of the trigeminal nerve, deep within the pons.
Function
The sensory function of the trigeminal nerve is to provide tactile, proprioceptive, and nociceptive afferents to the face and mouth. The motor component of the mandibular division (V3) of the trigeminal nerve controls the movement of eight muscles, including the four muscles of mastication: the masseter, the temporal, and the medial and lateral pterygoids.
The other four muscles are the tensor veli palatini, the mylohyoid, the anterior belly of the digastric, and the tensor tympani. With the exception of the tensor tympani, all of these muscles are involved in biting, chewing and swallowing, and all have bilateral cortical representation.
The function of the trigeminal nerve
The sensory functions of the trigeminal nerve are the transmission of impulses for touch, pain, temperature, proprioception,andthe somatomotor function with mandibular movement.
The ophthalmic nerve (V1) has mainly sensory fibers and has the following functions:
Sensory innervation of the skin of the forehead, the eyes, the nose, and the nasal mucosa
Innervation of the iris, the cornea, the conjunctiva, and the lacrimal gland
Supply of the skin of the forehead and transmission of pressure pain at the exit point of the supraorbital foramen
The maxillary nerve (V2) innervates the facial skin with sensory fibers and a parasympathetic part and has the following tasks:
Supply of the lower eyelid, its conjunctiva, and the upper lip
Supply of the teeth (upper molar, incisor, and canine), nasal cavity gums of the upper jaw and the palate mucosa (including the uvula), and tonsils
Supply of the lacrimal gland and nasal glands by the parasympathetic part
In addition to the sensory fibers, the mandibular nerve also contains motor fibers of the trigeminal nerve. It has the following tasks:
Innervation of all the muscles of mastication (e.g., masseter muscle) and the suprahyoid muscles by the motor fibers
Supply of the teeth (lower molar, incisor, and canine teeth), the gums of the lower jaw, the buccal mucosa, the dorsum of the tongue, and the external acoustic meatus, including the eardrum, by the sensory fibers
Abducens (VI) Nerve
The abducens nerve (cranial nerve VI) controls the lateral movement of the eye through innervation of the lateral rectus muscle.
Key Points
The abducens nerve exits the brainstem at the junction of the pons and the medulla and runs upward to reach the eye, traveling between the dura and the skull.
The long course of the abducens nerve between the brainstem and the eye makes it vulnerable to injury at many levels.
In most mammals besides humans, it also innervates the musculus retractor bulbi, which can retract the eye for protection.
Key Terms
abducens nerve: A nerve that controls the lateral rectus muscle in the eye.
clivus: A part of the cranium at the base of the skull. It forms a gradual sloping process at the anterior-most portion of the basilar occipital bone at its junction with the sphenoid bone.
petrous temporal bone: A pyramid-shaped bone that is wedged in at the base of the skull between the sphenoid and occipital bones and is part of the endocranium.
lateral rectus muscle: A muscle in the orbit. It is one of six extraocular muscles that control the movements of the eye (abduction in this case) and the only muscle innervated by the abducens nerve, cranial nerve VI, functioning to bring the pupil away from the midline of the body.
The abducens nerve (cranial nerve VI) is a somatic efferent nerve that, in humans, controls the movement of a single muscle: the lateral rectus muscle of the eye that moves the eye horizontally. In most other mammals it also innervates the musculus retractor bulbi, which can retract the eye for protection. Homologous abducens nerves are found in all vertebrates except lampreys and hagfishes.
Abducens nerve: Schematic of cranial nerves showing cranial nerve VI, the abducens nerve.
The abducens nerve leaves the brainstem at the junction of the pons and the medulla, medial to the facial nerve. In order to reach the eye, it runs upward (superiorly) and then bends forward (anteriorly).
The nerve enters the subarachnoid space when it emerges from the brainstem. It runs upward between the pons and the clivus, and then pierces the dura mater to run between the dura and the skull.
At the tip of the petrous temporal bone, it makes a sharp turn forward to enter the cavernous sinus. In the cavernous sinus it runs alongside the internal carotid artery. It then enters the orbit through the superior orbital fissure and innervates the lateral rectus muscle of the eye.
The long course of the abducens nerve between the brainstem and the eye makes it vulnerable to injury at many levels. For example, fractures of the petrous temporal bone can selectively damage the nerve, as can aneurysms of the intracavernous carotid artery.
Mass lesions that push the brainstem downward can damage the nerve by stretching it between the point where it emerges from the pons and the point where it hooks over the petrous temporal bone.
Facial (VII) Nerve
The facial nerve (cranial nerve VII) determines facial expressions and the taste sensations of the tongue.
Key Points
The facial nerve (cranial nerve VII) is responsible for the muscles that determine facial expression, as well as the sensation of taste in the front of the tongue and oral cavity.
The facial nerve’s motor component begins in the facial nerve nucleus in the pons, and the sensory component begins in the nervus intermedius. The nerve then runs through the facial canal, passes through the parotid gland, and divides into five branches.
Voluntary facial movements, such as wrinkling the brow, showing teeth, frowning, closing the eyes tightly (inability to do so is called lagophthalmos), pursing the lips, and puffing out the cheeks, all test the facial nerve.
Key Terms
nervus intermedius: A part of the facial nerve (cranial nerve VII) located between the motor component of the facial nerve and the vestibulocochlear nerve (cranial nerve VIII). It contains the sensory and parasympathetic fibers of the facial nerve.
Bell’s Palsy: Bell’s palsy is a form of facial paralysis resulting from a dysfunction of the cranial nerve VII (the facial nerve) that results in the inability to control facial muscles on the affected side.
The facial nerve: Illustration of the facial nerve and its branches.
The facial nerve is the seventh (cranial nerve VII) of the 12, paired cranial nerves. It emerges from the brainstem between the pons and the medulla and controls the muscles of facial expression.
It also functions in the conveyance of taste sensations from the anterior two-thirds of the tongue and oral cavity, and it supplies preganglionic parasympathetic fibers to several head and neck ganglia.
Location
The motor part of the facial nerve arises from the facial nerve nucleus in the pons, while the sensory part of the facial nerve arises from the nervus intermedius. The motor and sensory parts of the facial nerve enter the petrous temporal bone into the internal auditory meatus (intimately close to the inner ear), then runs a tortuous course (including two tight turns) through the facial canal, emerges from the stylomastoid foramen, and passes through the parotid gland, where it divides into five major branches.
Although it passes through the parotid gland, it does not innervate the gland (this is the responsibility of cranial nerve IX, the glossopharyngeal nerve). The facial nerve forms the geniculate ganglion prior to entering the facial canal.
The path of the facial nerve can be divided into six segments.
The intracranial (cisternal) segment.
The meatal segment (brainstem to the internal auditory canal).
The labyrinthine segment (internal auditory canal to geniculate ganglion),
The tympanic segment (from geniculate ganglion to pyramidal eminence).
The mastoid segment (from pyramidal eminence to stylomastoid foramen).
The extratemporal segment (from stylomastoid foramen to post parotid branches).
Function
Bell’s Palsy: A person attempting to show his teeth and raise his eyebrows with Bell’s palsy on his right side (left side of the image).
Motor functions include the following:
Innervation of the entire mimic facial musculature (platysma and muscles of the auricle)
Eyelid movement and closing of the eye by the orbicularis oculi muscle
Movement and closing of the mouth by the orbicularis oris muscle
Precise adjustment of the auditory ossicles by the stapedius muscle
Movement of the mandible by the mentalis muscle
Sensory and parasympathetic functions include the following:
Sense of taste in the anterior two-thirds of the tongue
Innervation of the three large salivary glands, the lacrimal glands, and the nasal glands
External acoustic meatus
Voluntary facial movements, such as wrinkling the brow, showing teeth, frowning, closing the eyes tightly (inability to do so is called lagophthalmos), pursing the lips, and puffing out the cheeks, all test the facial nerve. There should be no noticeable asymmetry.
In an upper motor neuron lesion, called central seven (central facial palsy ), only the lower part of the face on the contralateral side will be affected due to the bilateral control to the upper facial muscles (frontalis and orbicularis oculi).
Lower motor neuron lesions can result in cranial nerve VII palsy (Bell’s palsy is the idiopathic form of facial nerve palsy), manifested as both upper and lower facial weakness on the same side of the lesion.
Taste can be tested on the anterior 2/3 of the tongue. This can be tested with a swab dipped in a flavored solution, or with electronic stimulation (similar to putting your tongue on a battery).
In regards to the corneal reflex, the afferent arc is mediated by the general sensory afferents of the trigeminal nerve. The efferent arc occurs via the facial nerve.
The reflex involves the consensual blinking of both eyes in response to stimulation of one eye. This is due to the facial nerve’s innervation of the muscles of facial expression, namely the orbicularis oculi, responsible for blinking. Thus, the corneal reflex effectively tests the proper functioning of both cranial nerves V and VII.
Vestibulocochlear (VIII) Nerve
The vestibulocochlear nerve (cranial nerve VIII) carries information about hearing and balance.
Key Points
The vestibulocochlear nerve comprises the cochlear nerve that transmits hearing information, and the vestibular nerve that transmits balance information.
The cochlear nerve travels away from the cochlea of the inner ear where it starts as the spiral ganglia.
The vestibular nerve travels from the vestibular system of the inner ear.
Key Terms
cochlear nerve: A sensory nerve that conducts information about the environment to the brain, in this case acoustic energy impinging on the tympanic membrane (sound waves reaching the ear drum). The cochlear nerve arises from within the cochlea and extends to the brainstem where its fibers make contact with the cochlear nucleus, the next stage of neural processing in the auditory system.
vestibulocochlear nerve: Also known as the auditory vestibular nerve, this is the eighth of twelve cranial nerves, and it is responsible for transmitting sound and equilibrium (balance) information from the inner ear to the brain.
vestibular nerve: One of the two branches of the vestibulocochlear nerve (the cochlear nerve being the other). It connects to the semicircular canals via the vestibular ganglion and receives positional information.
The vestibulocochlear nerve (also known as the auditory vestibular nerve and cranial nerve VIII) has axons that carry the modalities of hearing and equilibrium.
It consists of the cochlear nerve that carries information about hearing, and the vestibular nerve that carries information about balance.
This is the nerve along which the sensory cells (the hair cells) of the inner ear transmit information to the brain. It emerges from the pons and exits the inner skull via the internal acoustic meatus (or internal auditory meatus) in the temporal bone.
Vestibular system’s semicircular canal: An illustration of the inner ear showing its semicircular canal, hair cells, ampulla, cupula, vestibular nerve, and fluid.
The vestibulocochlear nerve consists mostly of bipolar neurons and splits into two large divisions: the cochlear nerve and the vestibular nerve. The cochlear nerve travels away from the cochlea of the inner ear where it starts as the spiral ganglia.
Processes from the organ of Corti (the receptor organ for hearing) conduct afferent transmission to the spiral ganglia. It is the inner hair cells of the organ of Corti that are responsible for activating the afferent receptors in response to pressure waves reaching the basilar membrane through the transduction of sound.
The vestibular nerve travels from the vestibular system of the inner ear. The vestibular ganglion houses the cell bodies of the bipolar neurons and extends processes to five sensory organs.
Three of these are the cristae, located in the ampullae of the semicircular canals. Hair cells of the cristae activate afferent receptors in response to rotational acceleration.
The other two sensory organs supplied by the vestibular neurons are the maculae of the saccule and utricle. Hair cells of the maculae activate afferent receptors in response to linear acceleration.
The vestibulocochlear nerve has axons that carry the modalities of hearing and equilibrium. Damage to the vestibulocochlear nerve may cause hearing loss, vertigo, a false sense of motion, loss of equilibrium in dark places, nystagmus, motion sickness, and gaze-evoked tinnitus.
A benign primary intracranial tumor of the vestibulocochlear nerve is called a vestibular schwannoma (also called acoustic neuroma).
Functions of the vestibular nerve include the following:
Regulation of the hair cells of the organ of Corti for the adjustment of sensitivity (spatial position)
Transmission of impulses for the sense of balance, maintaining equilibrium
Functions of the cochlear nerve include the following:
Regulation of the hair cells of the organ of Corti for the adjustment of sensitivity (regarding sound waves)
Transmission of impulses for hearing
Glossopharyngeal (IX) Nerve
The glossopharyngeal nerve (cranial nerve IX) serves many distinct functions, including providing sensory innervation to various head and neck structures.
Key Points
The glossopharyngeal nerve (cranial nerve IX) is responsible for swallowing and the gag reflex, along with other functions.
The glossopharyngeal nerve receives input from the general and special sensory fibers in the back of the throat.
The glossopharyngeal nerve has five components: branchial motor, visceral motor, visceral sensory, general sensory, and special sensory components.
Key Terms
otic ganglion: A small parasympathetic ganglion located immediately below the foramen ovale in the infratemporal fossa that is associated with the glossopharyngeal nerve.
medulla: The lower half of the brainstem that contains the cardiac, respiratory, vomiting, and vasomotor centers and is associated with autonomic, involuntary functions such as breathing, heart rate, and blood pressure.
stylopharyngeus muscle: A muscle in the head that stretches between the temporal styloid process and the pharynx.
Structure
The glossopharyngeal nerve is the ninth of 12 pairs of cranial nerves. It exits the brainstem out from the sides of the upper medulla, just rostral (closer to the nose) to the vagus nerve.
Glossopharyngeal nerve: Image of head structures including the glossopharyngeal nerve.
The motor division of the glossopharyngeal nerve is derived from the basal plate of the embryonic medulla oblongata, while the sensory division originates from the cranial neural crest.
Function
There are a number of functions of the glossopharyngeal nerve. It controls muscles in the oral cavity and upper throat, as well as part of the sense of taste and the production of saliva.
Along with taste, the glossopharyngeal nerve relays general sensations from the pharyngeal walls. The various functions of the glossopharyngeal nerve are that:
It receives general sensory fibers (ventral trigeminothalamic tract) from the tonsils, the pharynx, the middle ear, and the posterior 1/3 of the tongue.
It receives special sensory fibers (taste) from the posterior 1/3 of the tongue.
It receives visceral sensory fibers from the carotid bodies, carotid sinus.
It supplies parasympathetic fibers to the parotid gland via the otic ganglion.
It supplies motor fibers to the stylopharyngeus muscle.
It contributes to the pharyngeal plexus.
Motor functions include the following:
Innervation of the palate muscles and the muscles of the pharynx by the vagus nerve
Dilatation of the pharynx during swallowing and speaking
Sensory functions include the following:
Innervation of the mucosa of the middle ear, the mastoid, and the eardrum
Supply of the velum, including the palatine tonsil and the posterior third of the tongue
Taste and somatic perception (touch, pain, and temperature) of the posterior third of the tongue
Proprioception in the swallowing musculature
Blood pressure regulation
Regulation of the oxygen and carbon dioxide content of the blood for the control of ventilation
Parasympathetic functions include the following:
Stimulation of salivation
Carotid glomus—contains chemoreceptors responsible for the oxygen content, as well as pressure receptors that are important for the regulation of blood pressure
Five Functional Components
The glossopharyngeal nerve consists of five components with distinct functions:
Branchial motor (special visceral efferent): Supplies the stylopharyngeus muscle.
Visceral motor (general visceral efferent): Provides parasympathetic innervation of the parotid gland.
Visceral sensory (general visceral afferent): Carries visceral sensory information from the carotid sinus and body.
General sensory (general somatic afferent): Provides general sensory information from the skin of the external ear, the internal surface of the tympanic membrane, upper pharynx, and the posterior 1/3 of the tongue.
Special sensory (special afferent): Provides taste sensation from the posterior 1/3 of the tongue.
Vagus (X) Nerve
The vagus nerve (cranial nerve X) is responsible for parasympathetic output to the heart and visceral organs.
Key Points
The vagus nerve (cranial nerve X) sends information about the body’s organs to the brain and carries some motor information back to the organs.
The vagus nerve has axons that originate from or enter the dorsal nucleus of the vagus nerve, the nucleus ambiguus, the solitary nucleus in the medulla, and the spinal trigeminal nucleus.
The vagus nerve is responsible for heart rate, gastrointestinal peristalsis, and sweating, to name a few.
Key Terms
nucleus ambiguus: A region of histologically disparate cells located just dorsal (posterior) to the inferior olivary nucleus in the lateral portion of the upper (rostral) medulla. It receives upper motor neuron innervation directly via the corticobulbar tract.
Valsalva maneuver: Performed by making a moderately forceful attempt to exhale against a closed airway; this is usually done by closing one’s mouth and pinching one’s nose shut while pressing out as if blowing up a balloon.
solitary nucleus: Structures in the brainstem that carry and receive visceral sensation and taste from the facial (VII), glossopharyngeal (IX), and vagus (X) cranial nerves.
dorsal nucleus of the vagus nerve: Also called the posterior motor nucleus of the vagus, this is a cranial nerve nucleus for the vagus nerve in the medulla that lies under the floor of the fourth ventricle. It mostly serves parasympathetic vagal functions in the gastrointestinal tract, lungs, and other thoracic and abdominal vagal innervations.
spinal trigeminal nucleus: A nucleus in the medulla that receives information about deep/crude touch, pain, and temperature from the ipsilateral face.
Vagus Nerve Anatomy
The vagus nerve, also known as the pneumogastric nerve or cranial nerve X, is the tenth of twelve paired cranial nerves. Upon leaving the medulla between the medullary pyramid and the inferior cerebellar peduncle, it extends through the jugular foramen, then passes into the carotid sheath between the internal carotid artery and the internal jugular vein below the head, to the neck, chest and abdomen, where it contributes to the innervation of the viscera.
Vagus nerve: Diagram demonstrating the course of the vagus nerve.
Besides output to the various organs in the body, the vagus nerve conveys sensory information about the state of the body’s organs to the central nervous system. Eighty to 90% of the nerve fibers in the vagus nerve are afferent (sensory) nerves that communicate the state of the viscera to the brain.
The vagus nerve includes axons that emerge from or converge onto four nuclei of the medulla.
The dorsal nucleus of vagus nerve: Sends parasympathetic output to the viscera, especially the intestines.
The nucleus ambiguus: Sends parasympathetic output to the heart (slowing it down).
The solitary nucleus: Receives afferent taste information and primary afferents from visceral organs.
The spinal trigeminal nucleus: Receives information about deep/crude touch, pain, and temperature of the outer ear, the dura of the posterior cranial fossa, and the mucosa of the larynx.
Function
The vagus nerve supplies motor parasympathetic fibers to all the organs, except the suprarenal (adrenal) glands, from the neck down to the second segment of the transverse colon. The vagus also controls a few skeletal muscles, most notably:
Cricothyroid muscle.
Levator veli palatini muscle.
Salpingopharyngeus muscle.
Palatoglossus muscle.
Palatopharyngeus muscle.
Superior, middle, and inferior pharyngeal constrictors.
Muscles of the larynx (speech).
Sensory functions include the following:
Taste and sensation (touch, pain, temperature, etc.) in the epiglottis and the pharynx
Blood pressure regulation
Regulation of the oxygen and carbon dioxide content in the blood for the control of ventilation
Sensation in visceral, thoracic, and abdominal organs
Somatomotor functions include the following:
Swallowing
Coughing
Voice production
Parasympathetic functions include the following:
Contraction and relaxation of the smooth musculature of the gastrointestinal tract
Reduction of the heart rate
Secretion of digestive juices
This means that the vagus nerve is responsible for such varied tasks as heart rate, gastrointestinal peristalsis, sweating, and quite a few muscle movements in the mouth, including speech (via the recurrent laryngeal nerve), swallowing, and keeping the larynx open for breathing (via action of the posterior cricoarytenoid muscle, the only abductor of the vocal folds).
It also has some afferent fibers that innervate the inner (canal) portion of the outer ear, via the auricular branch (also known as Alderman’s nerve) and part of the meninges. This explains why a person may cough when tickled on the ear (such as when trying to remove ear wax with a cotton swab).
Afferent vagus nerve fibers that innervate the pharynx and back of the throat are responsible for the gag reflex. In addition, 5-HT3 receptor-mediated afferent vagus stimulation in the gut due to gastroenteritis and other insults is a cause of vomiting.
Cardiovascular Influence
Parasympathetic innervation of the heart is partially controlled by the vagus nerve and is shared by the thoracic ganglia. Activation of the vagus nerve typically leads to a reduction in heart rate and/or blood pressure.
This occurs commonly in cases of viral gastroenteritis, acute cholecystitis, or in response to stimuli such as the Valsalva maneuver or pain. Excessive activation of the vagal nerve during emotional stress can also cause vasovagal syncope due to a sudden drop in cardiac output, causing cerebral hypoperfusion.
Accessory (XI) Nerve
The accessory nerve (cranial nerve XI) controls the muscles of the shoulder and neck.
Key Points
Cranial nerve XI is responsible for tilting and rotating the head, elevating the shoulders, and adducting the scapula.
Most of the fibers of the accessory nerve originate in neurons situated in the upper spinal cord. The fibers that make up the accessory nerve enter the skull through the foramen magnum and proceed to exit the jugular foramen with cranial nerves IX and X.
Due to its unusual course, the accessory nerve is the only nerve that enters and exits the skull.
Key Terms
sternocleidomastoid: A paired muscle in the superficial layers of the side of the neck. Its actions of the muscle are rotation of the head to the opposite side and flexion of the neck.
trapezius: A large vertebrate skeletal muscle divided into an ascending, descending, and transverse portion, attaching the neck and central spine to the outer extremity of the scapula; it functions in scapular elevation, adduction, and depression.
accessory nerve: The 11th cranial nerve of higher vertebrates, it controls the pharynx and the muscles of the upper chest and shoulders.
foramen: An opening, an orifice, or a short passage.
Anatomic Description
The accessory nerve (cranial nerve XI) controls the sternocleidomastoid and trapezius muscles of the shoulder and neck. It begins in the central nervous system (CNS) and exits the cranium through a foramen.
Unlike the other 11 cranial nerves, the accessory nerve begins outside the skull. In fact, most of the fibers of the nerve originate in neurons situated in the upper spinal cord.
The accessory nerve: Upon exiting the skull via the jugular foramen, the spinal accessory nerve pierces the sternocleidomastoid muscle before terminating on the trapezius muscle.
The fibers that make up the accessory nerve enter the skull through the foramen magnum and proceed to exit the jugular foramen with cranial nerves IX and X. Due to its unusual course, the accessory nerve is the only nerve that enters and exits the skull.
Traditional descriptions of the accessory nerve divide it into two components: a spinal component and a cranial component. However, more modern characterizations of the nerve regard the cranial component as separate and part of the vagus nerve.
Therefore, in contemporary discussions of the accessory nerve, it is common to disregard the cranial component when referencing the accessory nerve and assume reference to the spinal accessory nerve.
Accessory Nerve Function
The accessory nerve provides motor innervation from the CNS to the sternocleidomastoid and trapezius muscles of the neck. The sternocleidomastoid muscle tilts and rotates the head, while the trapezius muscle has several actions on the scapula, including shoulder elevation and adduction of the scapula.
During neurological examinations, the function of the spinal accessory nerve is often measured by testing the range of motion and strength of the aforementioned muscles. Limited range of motion or diminished muscle strength often indicates injury of the accessory nerve.
Patients with spinal accessory nerve palsy may exhibit signs of lower motor neuron disease, such as atrophy and fasciculations of both the sternocleidomastoid and trapezius muscles.
Hypoglossal (XII) Nerve
The hypoglossal nerve (cranial nerve XII) controls the muscles of the tongue.
Key Points
It controls tongue movements of speech, food manipulation, and swallowing.
While the hypoglossal nerve controls the tongue’s involuntary activities of swallowing to clear the mouth of saliva, most of the functions it controls are voluntary, meaning that the execution of these activities requires conscious thought.
Proper function of the hypoglossal nerve is important for executing tongue movements associated with speech. Many languages require specific uses of the nerve to create unique speech sounds, which may contribute to the difficulties some adults encounter when learning a new language.
Key Terms
digastric muscle: A small muscle located under the jaw.
hypoglossal nerve: The twelfth cranial nerve (XII) controls the muscles of the tongue.
olivary body: Located on the anterior surface of the medulla, lateral to the pyramid.
medullary pyramid: Paired white matter structures of the brainstem’s medulla oblongata that contain motor fibers of the corticospinal and corticobulbar tracts.
Structure and Location
The hypoglossal nerve is the twelfth cranial nerve (XII) and innervates all extrinsic and intrinsic muscles of the tongue, except for the palatoglossus. The hypoglossal nerve emerges from the medulla oblongata in the preolivary sulcus where it separates the olive (olivary body) and the pyramid (medullary pyramid).
It goes on to traverse the hypoglossal canal and, upon emerging, it branches and merges with a branch from the anterior ramus of C1. It passes behind the vagus nerve and between the internal carotid artery and internal jugular vein which lies on the carotid sheath. After passing deep to the posterior belly of the digastric muscle it proceeds to the submandibular region to enter the tongue.
Sensory functions include the following:
Proprioception
Somatomotor functions include the following:
Innervation of the sternocleidomastoid muscle and the trapezius muscle to control the movement of the head and the shoulders
Swallowing movement
Hypoglossal nerve: Schematic image of the hypoglossal nerve and the structures it innervates.
Function
The hypoglossal nerve controls tongue movements of speech, food manipulation, and swallowing. It supplies motor fibers to all of the muscles of the tongue, with the exception of the palatoglossus muscle, which is innervated by the vagus nerve (cranial nerve X) or, according to some classifications, by fibers from the glossopharyngeal nerve (cranial nerve IX) that hitchhike within the vagus.
While the hypoglossal nerve controls the tongue’s involuntary activities of swallowing to clear the mouth of saliva, most of the functions it controls are voluntary, meaning that the execution of these activities requires conscious thought.
Proper function of the hypoglossal nerve is important for executing the tongue movements associated with speech. Many languages require specific and sometimes unusual uses of the nerve to create unique speech sounds, which may contribute to the difficulties some adults encounter when learning a new language. Several corticonuclear-originating fibers supply innervation and aid in the unconscious movements required upon engaging in speech and articulation.
Progressive bulbar palsy is neuromuscular atrophy associated with the combined lesions of the hypoglossal nucleus and the nucleus ambiguous, upon the atrophy of the motor nerves of the pons and medulla. This condition causes dysfunctional tongue movements that lead to speech and chewing impairments and swallowing difficulties. Tongue muscle atrophy may also occur.
Somatomotor functions include the following:
Innervation of tongue muscles
Transmission of impulses for speaking and swallowing
Sensory functions include the following:
Proprioception
Associated Conditions
The possible conditions associated with the cranial nerves are as follows:
Abducens Nerve Diseases – Also known as sixth cranial disorders, this palsy kind of disease results in diabetics, mostly. This condition is a part of Mononeuritis Multiplex, which may result in ischemia, hypertension (sometimes), or compression of the nerve by lesions in the cavernous sinus (eg, nasopharyngeal tumors), orbit, or base of the skull.
Accessory Nerve Diseases Of Cranial Nerves – Weakness in these muscles may result to a general disease process such as amyotrophic lateral sclerosis, Guillain-Barre syndrome or poliomyelitis. Injuries in these nerves can result in neck dissection and lymph node excision.
Glossopharyngeal Nerve Diseases – Glossopharyngeal neuralgia is a state wherein one can experience unbearable, frequent pain in the throat, ears, tongue, and tonsils. However, this pain can stay around a few minutes.
Cranial Nerve Injuries – These are commonly traumatic injuries.
Cranial Nerve Malignant Neoplasm – Malignant cranial nerve sheath tumors are uncommon and deals with weak prognosis as those of spinal nerves at other places.
Facial Nerve Diseases – This conditions pull down your facial expressions and cause weakness on your face. Bell’s palsy, Ramsay Hunt syndrome, Lyme disease are the conditions associated with facial nerve disorders.
Hypoglossal Nerve Diseases – This condition results in tight oral musculature, making it difficult for the person to chew or eat.
Ocular Motility Disorders – This causes impairment of eye movements.
Olfactory Nerve Diseases – This is a result of a physical blockage in the nose and this can cause loss of smell.
Optic Nerve Diseases – These disorders are related to loss of vision.
Trochlear Nerve Diseases – Injuries in the nucleus of the midbrain can be counted within this.
Vagus Nerve Diseases – These are caused by the damage of stomach muscles.
Vestibulocochlear Nerve Diseases – Disorders related to this affects the inner ear and weaken the functions related to it.
Cranial nerves are the nerves that emerge directly from the brain (including the brainstem), of which there are conventionally considered twelve pairs. Cranial nerves relay information between the brain and parts of the body, primarily to and from regions of the head and neck, including the special senses of vision, taste, smell, and hearing.[rx]
The cranial nerves emerge from the central nervous system above the level of the first vertebrae of the vertebral column.[rx] Each cranial nerve is paired and is present on both sides. There are conventionally twelve pairs of cranial nerves, which are described with Roman numerals I–XII. Some considered there to be thirteen pairs of cranial nerves, including cranial nerve zero. The numbering of the cranial nerves is based on the order in which they emerge from the brain and brainstem, from front to back.[rx]
Brief Overview of Cranial Nerves
The characteristics of this nerve are presented in the table.
CRANIAL NERVE
NERVE TYPE
FUNCTIONS
1. Olfactory Nerve
Sensory
Smell
2. Optic Nerve
Sensory
Vision
3. Oculomotor Nerve
Motor
Eye Movement
4. Trochlear Nerve
Motor
Eyeball Movement
5. Trigeminal Nerve – Ophthalmic Branch
Sensory
Facial Muscle Movement, Chewing, Sense Temperature, touch and Pain on the Face
5. Trigeminal Nerve – Maxillary Branch
Sensory
Same as Above
5. Trigeminal Nerve – Mandibular Branch
Mixed
Same as Above
6. Abducens Nerve
Motor
Eyeball Movement
7. Facial Nerve
Mixed
Sense of Taste, Saliva and Tear Secretion, Movement of Facial Muscles
Swallowing and Secretion of Saliva, Monitors Blood Pressure, Levels of Oxygen and Carbon Dioxide in Blood
10. Vagus Nerve
Mixed
Parasympathetic Sensation, Control of Smooth Muscles of Lungs, Heart, Viscera and Secretion of Digestive Enzymes
11. Accessory Nerve
Motor
Swallowing and Movement of Head & Shoulders
12. Hypoglossal Nerve
Motor
Tongue Movement, Speech and Swallowing
The peripheral nervous system has 12 pairs of cranial nerves that control much of the motor and sensory functions of the head and neck.
Key Points
The cranial nerves serve functions such as smell, sight, eye movement, and feeling in the face. The cranial nerves also control balance, hearing, and swallowing.
The twelve cranial nerves, in order from I to XII are: olfactory nerve, optic nerve, oculomotor nerve, trochlear nerve, trigeminal nerve, abducens nerve, facial nerve, vestibulocochlear nerve, glossopharyngeal nerve, vagus nerve, spinal accessory nerve, and hypoglossal nerve.
The vagus nerve (X) has many branches and is responsible for tasks including heart rate, gastrointestinal peristalsis, sweating, and muscle movements in the mouth, including speech and keeping the larynx open for breathing.
Key Terms
innervate: To supply an organ or other body part with nerves.
peripheral nervous system: The nerves and ganglia outside of the brain and spinal cord.
peristalsis: A radially symmetrical contraction and relaxation of muscles that propagates in a wave down a tube (such as the gastrointestinal tract) in an anterograde direction.
Cranial nerves are the nerves that emerge directly from the brain (including the brainstem). In contrast, spinal nerves emerge from segments of the spinal cord. Cranial nerves relay information between the brain and parts of the body, primarily to and from regions of the head and neck.
Cranial Nerve Anatomy and Terminology
Spinal nerves emerge sequentially from the spinal cord with the spinal nerve closest to the head (C1) emerging in the space above the first cervical vertebra. The cranial nerves emerge from the central nervous system above this level.
Each cranial nerve is paired and is present on both sides. The numbering of the cranial nerves is based on the order in which they emerge from the brain, front to back (brainstem).
The terminal nerves, olfactory nerves (I) and optic nerves (II) emerge from the cerebrum or forebrain, and the remaining ten pairs arise from the brainstem, which is the lower part of the brain. The cranial nerves are considered components of the peripheral nervous system.
However, on a structural level, the olfactory, optic, and terminal nerves are more accurately considered part of the central nervous system.
The twelve cranial nerves are shown in the figure below followed by brief descriptions.
The cranial nerves: The locations of the cranial nerves within the brain.
The olfactory nerve (I): This is instrumental for the sense of smell, it is one of the few nerves that are capable of regeneration.
The optic nerve (II): This nerve carries visual information from the retina of the eye to the brain.
The oculomotor nerve (III): This controls most of the eye’s movements, the constriction of the pupil, and maintains an open eyelid.
The trochlear nerve (IV): A motor nerve that innervates the superior oblique muscle of the eye, which controls rotational movement.
The trigeminal nerve (V): This is responsible for sensation and motor function in the face and mouth.
The abducens nerve (VI): A motor nerve that innervates the lateral rectus muscle of the eye, which controls lateral movement.
The facial nerve (VII): This controls the muscles of facial expression, and functions in the conveyance of taste sensations from the anterior two-thirds of the tongue and oral cavity.
The vestibulocochlear nerve (VIII): This is responsible for transmitting sound and equilibrium (balance) information from the inner ear to the brain.
The glossopharyngeal nerve (IX): This nerve receives sensory information from the tonsils, the pharynx, the middle ear, and the rest of the tongue.
The vagus nerve (X): This is responsible for many tasks, including heart rate, gastrointestinal peristalsis, sweating, and muscle movements in the mouth, including speech and keeping the larynx open for breathing.
The spinal accessory (XI): This nerve controls specific muscles of the shoulder and neck.
The hypoglossal nerve (XII): This nerve controls the tongue movements of speech, food manipulation, and swallowing.
There are many mnemonic devices to remember the cranial nerves. One that may be helpful is: Old Opie Occasionally Tries Trigonometry And Feels Very Gloomy, Vague And Hypoactive.
Olfactory (I) Nerve
The olfactory nerve, or cranial nerve I, is the first of 12 cranial nerves and is responsible for the sense of smell.
Key Points
The olfactory nerve consists of a collection of many sensory nerve fibers that extend from the olfactory epithelium to the olfactory bulb.
Olfactory receptors within the olfactory mucosa in the nasal cavity receive information about smells that travel to the brain through the cranial nerve that extends from the olfactory epithelium to the olfactory bulb.
Olfactory receptor neurons continue to emerge throughout life and extend new axons to the olfactory bulb.
The olfactory nerve is the shortest of the 12 cranial nerves and only one of two cranial nerves (the other being the optic nerve) that do not join with the brainstem.
Key Terms
olfactory receptors: Expressed in the cell membranes of olfactory receptor neurons, these are responsible for the detection of odor molecules. Activated olfactory receptors are the initial player in a signal transduction cascade that ultimately produces a nerve impulse that is transmitted to the brain. The olfactory receptors form a multigene family consisting of over 900 genes in humans and 1,500 genes in mice.
cribriform plate: A sieve-like structure of the ethmoid bone that supports the olfactory bulb.
olfactory tract: A narrow white band made of a bundle of axons connecting the olfactory bulb to several brain regions.
ethmoid bone: An unpaired bone in the skull that separates the nasal cavity from the brain.
olfactory mucosa: Located in the upper region of the nasal cavity, this is made up of the olfactory epithelium and the underlying lamina propria, connective tissue containing fibroblasts, blood vessels, Bowman’s glands, and bundles of fine axons from the olfactory neurons.
Olfactory bulb: Sagittal section of human head showing the olfactory bulb.
The olfactory nerve, or cranial nerve I, is the first of the 12 cranial nerves. It is instrumental in the sense of smell. The olfactory nerve is the shortest of the 12 cranial nerves and only one of two cranial nerves (the other being the optic nerve) that do not join with the brainstem.
The specialized olfactory receptor neurons of the olfactory nerve are located in the olfactory mucosa of the upper parts of the nasal cavity. The olfactory nerves consist of a collection of many sensory nerve fibers that extend from the olfactory epithelium to the olfactory bulb, passing through the many openings of the cribriform plate of the ethmoid bone.
Olfactory receptor neurons continue to emerge throughout life and extend new axons to the olfactory bulb. Olfactory-ensheathing glia wrap bundles of these axons and are thought to facilitate their passage into the central nervous system.
The sense of smell (olfaction) arises from the stimulation of olfactory (or odorant) receptors by small molecules of different spatial, chemical, and electrical properties that pass over the nasal epithelium in the nasal cavity during inhalation. These interactions are transduced into electrical activity in the olfactory bulb, which then transmits the electrical activity to other parts of the olfactory system and the rest of the central nervous system via the olfactory tract.
Optic (II) Nerve
The optic nerve (cranial nerve II) receives visual information from photoreceptors in the retina and transmits it to the brain.
Key Points
The optic nerve is considered part of the central nervous system. The myelin on the optic nerve is produced by oligodendrocytes rather than Schwann cells and it is encased in the meningeal layers instead of the standard endoneurium, perineurium, and epineurium of the peripheral nervous system.
The optic nerve travels through the optic canal, partially decussates in the optic chiasm, and terminates in the lateral geniculate nucleus where information is transmitted to the visual cortex.
The axons responsible for reflexive eye movements terminate in the pretectal nucleus.
Key Terms
oligodendrocyte: A type of neuroglia that provides support and insulation to axons in the central nervous system.
retina: The thin layer of cells at the back of the eyeball where light is converted into neural signals sent to the brain.
optic nerve: Either of a pair of nerves that carry visual information from the retina to the brain.
visual cortex: The visual cortex of the brain is the part of the cerebral cortex responsible for processing visual information. It is located in the occipital lobe, in the back of the brain.
pretectal nucleus: This mediates behavioral responses to acute changes in ambient light, such as the pupillary light reflex and the optokinetic reflex.
The optic nerve is also known as cranial nerve II. It transmits visual information from the retina to the brain.
Each human optic nerve contains between 770,000 and 1.7 million nerve fibers. The eye’s blind spot is a result of the absence of photoreceptors in the area of the retina where the optic nerve leaves the eye.
Optic nerve: An illustration of the brain highlighting the optic nerve and optic tract.
The optic nerve is the second of twelve paired cranial nerves. It is considered by physiologists to be part of the central nervous system, as it is derived from an outpouching of the diencephalon during embryonic development.
As a consequence, the fibers are covered with myelin produced by oligodendrocytes, rather than Schwann cells that are found in the peripheral nervous system. The optic nerve is ensheathed in all three meningeal layers (dura, arachnoid, and pia mater) rather than the epineurium, perineurium, and endoneurium found in the peripheral nerves.
The fiber tracks of the mammalian central nervous system are incapable of regeneration. As a consequence, optic nerve damage produces irreversible blindness.
The optic nerve leaves the orbit, which is also known as an eye socket, via the optic canal, running posteromedially toward the optic chiasm, where there is a partial decussation (crossing) of fibers from the nasal visual fields of both eyes.
Most of the axons of the optic nerve terminate in the lateral geniculate nucleus (where information is relayed to the visual cortex), while other axons terminate in the pretectal nucleus and are involved in reflexive eye movements.
The optic nerve transmits all visual information including brightness perception, color perception, and contrast. It also conducts the visual impulses that are responsible for two important neurological reflexes: the light reflex and the accommodation reflex.
The light reflex refers to the constriction of both pupils that occurs when light is shone into either eye; the accommodation reflex refers to the swelling of the lens of the eye that occurs when one looks at a near object, as in reading.
Oculomotor (III) Nerve
The oculomoter nerve (cranial nerve III) controls eye movement, such as constriction of the pupil and open eyelids.
Key Points
The oculomotor nerve is the third paired cranial nerve.
The oculomotor nerve contains two nuclei, including the Edinger-Westphal nucleus that supplies parasympathetic nerve fibers to the eye to control pupil constriction and accommodation.
The oculomotor nerve originates at the superior colliculus and enters through the superior orbital fissure to control the levator palpebrae superioris muscles that hold the eyelids open.
Key Terms
levator palpebrae superioris: A muscle that elevates the upper eyelid.
superior colliculus: The primary integrating center for eye movements.
cavernous sinus: A venous channel found between layers of dura mater in the brain.
tentorium cerebelli: An extension of the dura mater that separates the cerebellum from the inferior portion of the occipital lobes.
superior orbital fissure: The superior orbital fissure is a foramen in the skull, although strictly it is more of a cleft, lying between the lesser and greater wings of the sphenoid bone.
plexus: A network or interwoven mass, especially of nerves, blood vessels, or lymphatic vessels.
The oculomotor nerve is the third paired cranial nerve. It enters the orbit via the superior orbital fissure and controls most of the eye’s movements, including constriction of the pupil and maintaining an open eyelid by innervating the levator palpebrae superiors muscle.
The oculomotor nerve is derived from the basal plate of the embryonic midbrain. Cranial nerves IV and VI also participate in the control of eye movement.
There are two nuclei for the oculomotor nerve:
The oculomotor nucleus originates at the level of the superior colliculus. The muscles it controls are the striated muscle in the levator palpebrae superioris and all extraocular muscles, except for the superior oblique muscle and the lateral rectus muscle.
The Edinger-Westphal nucleus supplies parasympathetic fibers to the eye via the ciliary ganglion and controls the pupillae muscle (affecting pupil constriction) and the ciliary muscle (affecting accommodation).
Sympathetic postganglionic fibers also join the nerve from the plexus on the internal carotid artery in the wall of the cavernous sinus and are distributed through the nerve, for example, to the smooth muscle of the levator palpebrae superioris.
Emergence from Brain
On emerging from the brain, the oculomotor nerve is invested with a sheath of pia mater and enclosed in a prolongation from the arachnoid mater. It passes between the superior cerebellar and posterior cerebral arteries, and then pierces the dura mater anterior and lateral to the posterior clinoid process (to give attachment to the tectorium cerebella), passing between the free and attached borders of the tentorium cerebelli.
It then runs along the lateral wall of the cavernous sinus, above the other orbital nerves, receiving in its course one or two filaments from the cavernous plexus of the sympathetic nervous system, and a communicating branch from the ophthalmic division of the trigeminal nerve.
It then divides into two branches that enter the orbit through the superior orbital fissure, between the two heads of the lateral rectus (a muscle on the lateral side of the eyeball in the orbit). Here the nerve is placed below the trochlear nerve and the frontal and lacrimal branches of the ophthalmic nerve, while the nasociliary nerve is placed between its two rami (the superior and inferior branch of oculomotor nerve).
Cranial nerves: Image of cranial nerves showing the position of the oculomotor nerve.
Trochlear (IV) Nerve
The trochlear nerve (cranial nerve IV) is a motor nerve that innervates a single muscle: the superior oblique muscle of the eye.
Key Points
The trochlear nerve innervates the superior oblique muscle of the eye.
The trochlear nerve contains the smallest number of axons of all the cranial nerves and has the greatest intracranial length.
The two major clinical syndromes that can arise from damage to the trochlear nerve are vertical and torsional diplopia.
Key Terms
contralateral: On the opposite side of the body.
cerebral aqueduct: The channel in the brain that connects the third ventricle to the fourth ventricle. Also called the aqueduct of Sylvius, it is surrounded by periaqueductal gray matter.
The trochlear nerve (cranial nerve IV) is a motor nerve that innervates a single muscle: the superior oblique muscle of the eye.
The trochlear nerve: The trocheal nerve and where it innervates.
The trochlear nerve is unique among the cranial nerves in several respects.
It is the smallest nerve in terms of the number of axons it contains and it has the greatest intracranial length.
Other than the optic nerve (cranial nerve II), it is the only cranial nerve that decussates (crosses to the other side) before innervating its target.
It is the only cranial nerve that exits from the dorsal aspect of the brainstem.
The nucleus of the trochlear nerve is located in the caudal mesencephalon beneath the cerebral aqueduct. It is immediately below the nucleus of the oculomotor nerve (III) in the rostral mesencephalon.
The trochlear nucleus is unique in that its axons run dorsally and cross the midline before emerging from the brainstem—so a lesion of the trochlear nucleus affects the contralateral eye. Lesions of all other cranial nuclei affect the ipsilateral side (except of course the optic nerve, cranial nerve II, which innervates both eyes).
Homologous trochlear nerves are found in all jawed vertebrates. The unique features of the trochlear nerve, including its dorsal exit from the brainstem and its contralateral innervation, are seen in the primitive brains of sharks.
The human trochlear nerve is derived from the basal plate of the embryonic midbrain.
Clinical Syndromes
There are two major clinical syndromes that can manifest through damage to the trochlear nerve:
Vertical diplopia: Injury to the trochlear nerve causes weakness of downward eye movement with consequent vertical diplopia (double vision).
Torsional diplopia: Weakness of intorsion results in torsional diplopia, in which two different visual fields, tilted with respect to each other, are seen at the same time. To compensate for this, patients with trochlear nerve palsies tilt their heads to the opposite side, in order to fuse the two images into a single visual field.
The clinical syndromes can originate from both peripheral and central lesions. A peripheral lesion is damage to the bundle of nerves, in contrast to a central lesion, which is damage to the trochlear nucleus.
Trigeminal (V) Nerve
The trigeminal nerve is the fifth cranial nerve and it is responsible for sensation and motor function in the face and mouth.
Key Points
The sensory function of the trigeminal nerve is to provide tactile, motion, position, and pain sensations for the face and mouth; its motor function activates the muscles of the jaw, mouth, and inner ear.
The trigeminal nerve has three major branches on each side—the opthalmic nerve, maxillary nerve, and mandibular nerve—that converge on the trigeminal ganglion.
The trigeminal ganglion is analogous to the dorsal root ganglia of the spinal cord, which contain the cell bodies of incoming sensory fibers from the rest of the body.
Key Terms
trigeminal ganglion: The trigeminal ganglion (also called the Gasserian ganglion, semilunar ganglion, or Gasser’s ganglion) is a sensory ganglion of the trigeminal nerve (cranial nerve V) that occupies a cavity (Meckel’s cave) in the dura mater, covering the trigeminal impression near the apex of the petrous part of the temporal bone.
trigeminal nerve: The nerve responsible for sensation and motor function in the face and mouth.
The trigeminal nerve (cranial nerve V), and it contains both sensory and motor fibers. It is responsible for sensation in the face and certain motor functions such as biting, chewing, and swallowing.
Trigeminal nerve: Schematic illustration of the trigeminal nerve (labeled Sensory root above) and the structures it innervates in the face and mouth.
The sensory function of the trigeminal nerve is to provide the tactile, motion, position, and pain sensations of the face and mouth. The motor function activates the muscles of the jaw, mouth, and inner ear.
Structure
The trigeminal nerve is the largest of the cranial nerves. Its name, trigeminal, means three twins. It is derived from the fact that each nerve, one on each side of the pons, has three major branches: the ophthalmic nerve (V1 in the illustration below), the maxillary nerve (V2), and the mandibular nerve (V3).
The ophthalmic and maxillary nerves are purely sensory. The mandibular nerve has both sensory and motor functions.
The three branches converge on the trigeminal ganglion that is located within the trigeminal cave in the brain; it contains the cell bodies of incoming sensory nerve fibers. The trigeminal ganglion is analogous to the dorsal root ganglia of the spinal cord, which contain the cell bodies of incoming sensory fibers from the rest of the body.
Areas of the face innervated by the trigeminal nerve: The ophthalmic nerve branch (V1) innervates the bright red area, the maxillary nerve branch (V2) innervates the light red area, and the mandibular nerve branch (V3) innervates the yellow area.
From the trigeminal ganglion, a single large sensory root enters the brainstem at the level of the pons. Immediately adjacent to the sensory root, a smaller motor root emerges from the pons at the same level.
Motor fibers pass through the trigeminal ganglion on their way to peripheral muscles, but their cell bodies are located in the nucleus of the trigeminal nerve, deep within the pons.
Function
The sensory function of the trigeminal nerve is to provide tactile, proprioceptive, and nociceptive afferents to the face and mouth. The motor component of the mandibular division (V3) of the trigeminal nerve controls the movement of eight muscles, including the four muscles of mastication: the masseter, the temporal, and the medial and lateral pterygoids.
The other four muscles are the tensor veli palatini, the mylohyoid, the anterior belly of the digastric, and the tensor tympani. With the exception of the tensor tympani, all of these muscles are involved in biting, chewing and swallowing, and all have bilateral cortical representation.
The function of the trigeminal nerve
The sensory functions of the trigeminal nerve are the transmission of impulses for touch, pain, temperature, proprioception,andthe somatomotor function with mandibular movement.
The ophthalmic nerve (V1) has mainly sensory fibers and has the following functions:
Sensory innervation of the skin of the forehead, the eyes, the nose, and the nasal mucosa
Innervation of the iris, the cornea, the conjunctiva, and the lacrimal gland
Supply of the skin of the forehead and transmission of pressure pain at the exit point of the supraorbital foramen
The maxillary nerve (V2) innervates the facial skin with sensory fibers and a parasympathetic part and has the following tasks:
Supply of the lower eyelid, its conjunctiva, and the upper lip
Supply of the teeth (upper molar, incisor, and canine), nasal cavity gums of the upper jaw and the palate mucosa (including the uvula), and tonsils
Supply of the lacrimal gland and nasal glands by the parasympathetic part
In addition to the sensory fibers, the mandibular nerve also contains motor fibers of the trigeminal nerve. It has the following tasks:
Innervation of all the muscles of mastication (e.g., masseter muscle) and the suprahyoid muscles by the motor fibers
Supply of the teeth (lower molar, incisor, and canine teeth), the gums of the lower jaw, the buccal mucosa, the dorsum of the tongue, and the external acoustic meatus, including the eardrum, by the sensory fibers
Abducens (VI) Nerve
The abducens nerve (cranial nerve VI) controls the lateral movement of the eye through innervation of the lateral rectus muscle.
Key Points
The abducens nerve exits the brainstem at the junction of the pons and the medulla and runs upward to reach the eye, traveling between the dura and the skull.
The long course of the abducens nerve between the brainstem and the eye makes it vulnerable to injury at many levels.
In most mammals besides humans, it also innervates the musculus retractor bulbi, which can retract the eye for protection.
Key Terms
abducens nerve: A nerve that controls the lateral rectus muscle in the eye.
clivus: A part of the cranium at the base of the skull. It forms a gradual sloping process at the anterior-most portion of the basilar occipital bone at its junction with the sphenoid bone.
petrous temporal bone: A pyramid-shaped bone that is wedged in at the base of the skull between the sphenoid and occipital bones and is part of the endocranium.
lateral rectus muscle: A muscle in the orbit. It is one of six extraocular muscles that control the movements of the eye (abduction in this case) and the only muscle innervated by the abducens nerve, cranial nerve VI, functioning to bring the pupil away from the midline of the body.
The abducens nerve (cranial nerve VI) is a somatic efferent nerve that, in humans, controls the movement of a single muscle: the lateral rectus muscle of the eye that moves the eye horizontally. In most other mammals it also innervates the musculus retractor bulbi, which can retract the eye for protection. Homologous abducens nerves are found in all vertebrates except lampreys and hagfishes.
Abducens nerve: Schematic of cranial nerves showing cranial nerve VI, the abducens nerve.
The abducens nerve leaves the brainstem at the junction of the pons and the medulla, medial to the facial nerve. In order to reach the eye, it runs upward (superiorly) and then bends forward (anteriorly).
The nerve enters the subarachnoid space when it emerges from the brainstem. It runs upward between the pons and the clivus, and then pierces the dura mater to run between the dura and the skull.
At the tip of the petrous temporal bone, it makes a sharp turn forward to enter the cavernous sinus. In the cavernous sinus it runs alongside the internal carotid artery. It then enters the orbit through the superior orbital fissure and innervates the lateral rectus muscle of the eye.
The long course of the abducens nerve between the brainstem and the eye makes it vulnerable to injury at many levels. For example, fractures of the petrous temporal bone can selectively damage the nerve, as can aneurysms of the intracavernous carotid artery.
Mass lesions that push the brainstem downward can damage the nerve by stretching it between the point where it emerges from the pons and the point where it hooks over the petrous temporal bone.
Facial (VII) Nerve
The facial nerve (cranial nerve VII) determines facial expressions and the taste sensations of the tongue.
Key Points
The facial nerve (cranial nerve VII) is responsible for the muscles that determine facial expression, as well as the sensation of taste in the front of the tongue and oral cavity.
The facial nerve’s motor component begins in the facial nerve nucleus in the pons, and the sensory component begins in the nervus intermedius. The nerve then runs through the facial canal, passes through the parotid gland, and divides into five branches.
Voluntary facial movements, such as wrinkling the brow, showing teeth, frowning, closing the eyes tightly (inability to do so is called lagophthalmos), pursing the lips, and puffing out the cheeks, all test the facial nerve.
Key Terms
nervus intermedius: A part of the facial nerve (cranial nerve VII) located between the motor component of the facial nerve and the vestibulocochlear nerve (cranial nerve VIII). It contains the sensory and parasympathetic fibers of the facial nerve.
Bell’s Palsy: Bell’s palsy is a form of facial paralysis resulting from a dysfunction of the cranial nerve VII (the facial nerve) that results in the inability to control facial muscles on the affected side.
The facial nerve: Illustration of the facial nerve and its branches.
The facial nerve is the seventh (cranial nerve VII) of the 12, paired cranial nerves. It emerges from the brainstem between the pons and the medulla and controls the muscles of facial expression.
It also functions in the conveyance of taste sensations from the anterior two-thirds of the tongue and oral cavity, and it supplies preganglionic parasympathetic fibers to several head and neck ganglia.
Location
The motor part of the facial nerve arises from the facial nerve nucleus in the pons, while the sensory part of the facial nerve arises from the nervus intermedius. The motor and sensory parts of the facial nerve enter the petrous temporal bone into the internal auditory meatus (intimately close to the inner ear), then runs a tortuous course (including two tight turns) through the facial canal, emerges from the stylomastoid foramen, and passes through the parotid gland, where it divides into five major branches.
Although it passes through the parotid gland, it does not innervate the gland (this is the responsibility of cranial nerve IX, the glossopharyngeal nerve). The facial nerve forms the geniculate ganglion prior to entering the facial canal.
The path of the facial nerve can be divided into six segments.
The intracranial (cisternal) segment.
The meatal segment (brainstem to the internal auditory canal).
The labyrinthine segment (internal auditory canal to geniculate ganglion),
The tympanic segment (from geniculate ganglion to pyramidal eminence).
The mastoid segment (from pyramidal eminence to stylomastoid foramen).
The extratemporal segment (from stylomastoid foramen to post parotid branches).
Function
Bell’s Palsy: A person attempting to show his teeth and raise his eyebrows with Bell’s palsy on his right side (left side of the image).
Motor functions include the following:
Innervation of the entire mimic facial musculature (platysma and muscles of the auricle)
Eyelid movement and closing of the eye by the orbicularis oculi muscle
Movement and closing of the mouth by the orbicularis oris muscle
Precise adjustment of the auditory ossicles by the stapedius muscle
Movement of the mandible by the mentalis muscle
Sensory and parasympathetic functions include the following:
Sense of taste in the anterior two-thirds of the tongue
Innervation of the three large salivary glands, the lacrimal glands, and the nasal glands
External acoustic meatus
Voluntary facial movements, such as wrinkling the brow, showing teeth, frowning, closing the eyes tightly (inability to do so is called lagophthalmos), pursing the lips, and puffing out the cheeks, all test the facial nerve. There should be no noticeable asymmetry.
In an upper motor neuron lesion, called central seven (central facial palsy ), only the lower part of the face on the contralateral side will be affected due to the bilateral control to the upper facial muscles (frontalis and orbicularis oculi).
Lower motor neuron lesions can result in cranial nerve VII palsy (Bell’s palsy is the idiopathic form of facial nerve palsy), manifested as both upper and lower facial weakness on the same side of the lesion.
Taste can be tested on the anterior 2/3 of the tongue. This can be tested with a swab dipped in a flavored solution, or with electronic stimulation (similar to putting your tongue on a battery).
In regards to the corneal reflex, the afferent arc is mediated by the general sensory afferents of the trigeminal nerve. The efferent arc occurs via the facial nerve.
The reflex involves the consensual blinking of both eyes in response to stimulation of one eye. This is due to the facial nerve’s innervation of the muscles of facial expression, namely the orbicularis oculi, responsible for blinking. Thus, the corneal reflex effectively tests the proper functioning of both cranial nerves V and VII.
Vestibulocochlear (VIII) Nerve
The vestibulocochlear nerve (cranial nerve VIII) carries information about hearing and balance.
Key Points
The vestibulocochlear nerve comprises the cochlear nerve that transmits hearing information, and the vestibular nerve that transmits balance information.
The cochlear nerve travels away from the cochlea of the inner ear where it starts as the spiral ganglia.
The vestibular nerve travels from the vestibular system of the inner ear.
Key Terms
cochlear nerve: A sensory nerve that conducts information about the environment to the brain, in this case acoustic energy impinging on the tympanic membrane (sound waves reaching the ear drum). The cochlear nerve arises from within the cochlea and extends to the brainstem where its fibers make contact with the cochlear nucleus, the next stage of neural processing in the auditory system.
vestibulocochlear nerve: Also known as the auditory vestibular nerve, this is the eighth of twelve cranial nerves, and it is responsible for transmitting sound and equilibrium (balance) information from the inner ear to the brain.
vestibular nerve: One of the two branches of the vestibulocochlear nerve (the cochlear nerve being the other). It connects to the semicircular canals via the vestibular ganglion and receives positional information.
The vestibulocochlear nerve (also known as the auditory vestibular nerve and cranial nerve VIII) has axons that carry the modalities of hearing and equilibrium.
It consists of the cochlear nerve that carries information about hearing, and the vestibular nerve that carries information about balance.
This is the nerve along which the sensory cells (the hair cells) of the inner ear transmit information to the brain. It emerges from the pons and exits the inner skull via the internal acoustic meatus (or internal auditory meatus) in the temporal bone.
Vestibular system’s semicircular canal: An illustration of the inner ear showing its semicircular canal, hair cells, ampulla, cupula, vestibular nerve, and fluid.
The vestibulocochlear nerve consists mostly of bipolar neurons and splits into two large divisions: the cochlear nerve and the vestibular nerve. The cochlear nerve travels away from the cochlea of the inner ear where it starts as the spiral ganglia.
Processes from the organ of Corti (the receptor organ for hearing) conduct afferent transmission to the spiral ganglia. It is the inner hair cells of the organ of Corti that are responsible for activating the afferent receptors in response to pressure waves reaching the basilar membrane through the transduction of sound.
The vestibular nerve travels from the vestibular system of the inner ear. The vestibular ganglion houses the cell bodies of the bipolar neurons and extends processes to five sensory organs.
Three of these are the cristae, located in the ampullae of the semicircular canals. Hair cells of the cristae activate afferent receptors in response to rotational acceleration.
The other two sensory organs supplied by the vestibular neurons are the maculae of the saccule and utricle. Hair cells of the maculae activate afferent receptors in response to linear acceleration.
The vestibulocochlear nerve has axons that carry the modalities of hearing and equilibrium. Damage to the vestibulocochlear nerve may cause hearing loss, vertigo, a false sense of motion, loss of equilibrium in dark places, nystagmus, motion sickness, and gaze-evoked tinnitus.
A benign primary intracranial tumor of the vestibulocochlear nerve is called a vestibular schwannoma (also called acoustic neuroma).
Functions of the vestibular nerve include the following:
Regulation of the hair cells of the organ of Corti for the adjustment of sensitivity (spatial position)
Transmission of impulses for the sense of balance, maintaining equilibrium
Functions of the cochlear nerve include the following:
Regulation of the hair cells of the organ of Corti for the adjustment of sensitivity (regarding sound waves)
Transmission of impulses for hearing
Glossopharyngeal (IX) Nerve
The glossopharyngeal nerve (cranial nerve IX) serves many distinct functions, including providing sensory innervation to various head and neck structures.
Key Points
The glossopharyngeal nerve (cranial nerve IX) is responsible for swallowing and the gag reflex, along with other functions.
The glossopharyngeal nerve receives input from the general and special sensory fibers in the back of the throat.
The glossopharyngeal nerve has five components: branchial motor, visceral motor, visceral sensory, general sensory, and special sensory components.
Key Terms
otic ganglion: A small parasympathetic ganglion located immediately below the foramen ovale in the infratemporal fossa that is associated with the glossopharyngeal nerve.
medulla: The lower half of the brainstem that contains the cardiac, respiratory, vomiting, and vasomotor centers and is associated with autonomic, involuntary functions such as breathing, heart rate, and blood pressure.
stylopharyngeus muscle: A muscle in the head that stretches between the temporal styloid process and the pharynx.
Structure
The glossopharyngeal nerve is the ninth of 12 pairs of cranial nerves. It exits the brainstem out from the sides of the upper medulla, just rostral (closer to the nose) to the vagus nerve.
Glossopharyngeal nerve: Image of head structures including the glossopharyngeal nerve.
The motor division of the glossopharyngeal nerve is derived from the basal plate of the embryonic medulla oblongata, while the sensory division originates from the cranial neural crest.
Function
There are a number of functions of the glossopharyngeal nerve. It controls muscles in the oral cavity and upper throat, as well as part of the sense of taste and the production of saliva.
Along with taste, the glossopharyngeal nerve relays general sensations from the pharyngeal walls. The various functions of the glossopharyngeal nerve are that:
It receives general sensory fibers (ventral trigeminothalamic tract) from the tonsils, the pharynx, the middle ear, and the posterior 1/3 of the tongue.
It receives special sensory fibers (taste) from the posterior 1/3 of the tongue.
It receives visceral sensory fibers from the carotid bodies, carotid sinus.
It supplies parasympathetic fibers to the parotid gland via the otic ganglion.
It supplies motor fibers to the stylopharyngeus muscle.
It contributes to the pharyngeal plexus.
Motor functions include the following:
Innervation of the palate muscles and the muscles of the pharynx by the vagus nerve
Dilatation of the pharynx during swallowing and speaking
Sensory functions include the following:
Innervation of the mucosa of the middle ear, the mastoid, and the eardrum
Supply of the velum, including the palatine tonsil and the posterior third of the tongue
Taste and somatic perception (touch, pain, and temperature) of the posterior third of the tongue
Proprioception in the swallowing musculature
Blood pressure regulation
Regulation of the oxygen and carbon dioxide content of the blood for the control of ventilation
Parasympathetic functions include the following:
Stimulation of salivation
Carotid glomus—contains chemoreceptors responsible for the oxygen content, as well as pressure receptors that are important for the regulation of blood pressure
Five Functional Components
The glossopharyngeal nerve consists of five components with distinct functions:
Branchial motor (special visceral efferent): Supplies the stylopharyngeus muscle.
Visceral motor (general visceral efferent): Provides parasympathetic innervation of the parotid gland.
Visceral sensory (general visceral afferent): Carries visceral sensory information from the carotid sinus and body.
General sensory (general somatic afferent): Provides general sensory information from the skin of the external ear, the internal surface of the tympanic membrane, upper pharynx, and the posterior 1/3 of the tongue.
Special sensory (special afferent): Provides taste sensation from the posterior 1/3 of the tongue.
Vagus (X) Nerve
The vagus nerve (cranial nerve X) is responsible for parasympathetic output to the heart and visceral organs.
Key Points
The vagus nerve (cranial nerve X) sends information about the body’s organs to the brain and carries some motor information back to the organs.
The vagus nerve has axons that originate from or enter the dorsal nucleus of the vagus nerve, the nucleus ambiguus, the solitary nucleus in the medulla, and the spinal trigeminal nucleus.
The vagus nerve is responsible for heart rate, gastrointestinal peristalsis, and sweating, to name a few.
Key Terms
nucleus ambiguus: A region of histologically disparate cells located just dorsal (posterior) to the inferior olivary nucleus in the lateral portion of the upper (rostral) medulla. It receives upper motor neuron innervation directly via the corticobulbar tract.
Valsalva maneuver: Performed by making a moderately forceful attempt to exhale against a closed airway; this is usually done by closing one’s mouth and pinching one’s nose shut while pressing out as if blowing up a balloon.
solitary nucleus: Structures in the brainstem that carry and receive visceral sensation and taste from the facial (VII), glossopharyngeal (IX), and vagus (X) cranial nerves.
dorsal nucleus of the vagus nerve: Also called the posterior motor nucleus of the vagus, this is a cranial nerve nucleus for the vagus nerve in the medulla that lies under the floor of the fourth ventricle. It mostly serves parasympathetic vagal functions in the gastrointestinal tract, lungs, and other thoracic and abdominal vagal innervations.
spinal trigeminal nucleus: A nucleus in the medulla that receives information about deep/crude touch, pain, and temperature from the ipsilateral face.
Vagus Nerve Anatomy
The vagus nerve, also known as the pneumogastric nerve or cranial nerve X, is the tenth of twelve paired cranial nerves. Upon leaving the medulla between the medullary pyramid and the inferior cerebellar peduncle, it extends through the jugular foramen, then passes into the carotid sheath between the internal carotid artery and the internal jugular vein below the head, to the neck, chest and abdomen, where it contributes to the innervation of the viscera.
Vagus nerve: Diagram demonstrating the course of the vagus nerve.
Besides output to the various organs in the body, the vagus nerve conveys sensory information about the state of the body’s organs to the central nervous system. Eighty to 90% of the nerve fibers in the vagus nerve are afferent (sensory) nerves that communicate the state of the viscera to the brain.
The vagus nerve includes axons that emerge from or converge onto four nuclei of the medulla.
The dorsal nucleus of vagus nerve: Sends parasympathetic output to the viscera, especially the intestines.
The nucleus ambiguus: Sends parasympathetic output to the heart (slowing it down).
The solitary nucleus: Receives afferent taste information and primary afferents from visceral organs.
The spinal trigeminal nucleus: Receives information about deep/crude touch, pain, and temperature of the outer ear, the dura of the posterior cranial fossa, and the mucosa of the larynx.
Function
The vagus nerve supplies motor parasympathetic fibers to all the organs, except the suprarenal (adrenal) glands, from the neck down to the second segment of the transverse colon. The vagus also controls a few skeletal muscles, most notably:
Cricothyroid muscle.
Levator veli palatini muscle.
Salpingopharyngeus muscle.
Palatoglossus muscle.
Palatopharyngeus muscle.
Superior, middle, and inferior pharyngeal constrictors.
Muscles of the larynx (speech).
Sensory functions include the following:
Taste and sensation (touch, pain, temperature, etc.) in the epiglottis and the pharynx
Blood pressure regulation
Regulation of the oxygen and carbon dioxide content in the blood for the control of ventilation
Sensation in visceral, thoracic, and abdominal organs
Somatomotor functions include the following:
Swallowing
Coughing
Voice production
Parasympathetic functions include the following:
Contraction and relaxation of the smooth musculature of the gastrointestinal tract
Reduction of the heart rate
Secretion of digestive juices
This means that the vagus nerve is responsible for such varied tasks as heart rate, gastrointestinal peristalsis, sweating, and quite a few muscle movements in the mouth, including speech (via the recurrent laryngeal nerve), swallowing, and keeping the larynx open for breathing (via action of the posterior cricoarytenoid muscle, the only abductor of the vocal folds).
It also has some afferent fibers that innervate the inner (canal) portion of the outer ear, via the auricular branch (also known as Alderman’s nerve) and part of the meninges. This explains why a person may cough when tickled on the ear (such as when trying to remove ear wax with a cotton swab).
Afferent vagus nerve fibers that innervate the pharynx and back of the throat are responsible for the gag reflex. In addition, 5-HT3 receptor-mediated afferent vagus stimulation in the gut due to gastroenteritis and other insults is a cause of vomiting.
Cardiovascular Influence
Parasympathetic innervation of the heart is partially controlled by the vagus nerve and is shared by the thoracic ganglia. Activation of the vagus nerve typically leads to a reduction in heart rate and/or blood pressure.
This occurs commonly in cases of viral gastroenteritis, acute cholecystitis, or in response to stimuli such as the Valsalva maneuver or pain. Excessive activation of the vagal nerve during emotional stress can also cause vasovagal syncope due to a sudden drop in cardiac output, causing cerebral hypoperfusion.
Accessory (XI) Nerve
The accessory nerve (cranial nerve XI) controls the muscles of the shoulder and neck.
Key Points
Cranial nerve XI is responsible for tilting and rotating the head, elevating the shoulders, and adducting the scapula.
Most of the fibers of the accessory nerve originate in neurons situated in the upper spinal cord. The fibers that make up the accessory nerve enter the skull through the foramen magnum and proceed to exit the jugular foramen with cranial nerves IX and X.
Due to its unusual course, the accessory nerve is the only nerve that enters and exits the skull.
Key Terms
sternocleidomastoid: A paired muscle in the superficial layers of the side of the neck. Its actions of the muscle are rotation of the head to the opposite side and flexion of the neck.
trapezius: A large vertebrate skeletal muscle divided into an ascending, descending, and transverse portion, attaching the neck and central spine to the outer extremity of the scapula; it functions in scapular elevation, adduction, and depression.
accessory nerve: The 11th cranial nerve of higher vertebrates, it controls the pharynx and the muscles of the upper chest and shoulders.
foramen: An opening, an orifice, or a short passage.
Anatomic Description
The accessory nerve (cranial nerve XI) controls the sternocleidomastoid and trapezius muscles of the shoulder and neck. It begins in the central nervous system (CNS) and exits the cranium through a foramen.
Unlike the other 11 cranial nerves, the accessory nerve begins outside the skull. In fact, most of the fibers of the nerve originate in neurons situated in the upper spinal cord.
The accessory nerve: Upon exiting the skull via the jugular foramen, the spinal accessory nerve pierces the sternocleidomastoid muscle before terminating on the trapezius muscle.
The fibers that make up the accessory nerve enter the skull through the foramen magnum and proceed to exit the jugular foramen with cranial nerves IX and X. Due to its unusual course, the accessory nerve is the only nerve that enters and exits the skull.
Traditional descriptions of the accessory nerve divide it into two components: a spinal component and a cranial component. However, more modern characterizations of the nerve regard the cranial component as separate and part of the vagus nerve.
Therefore, in contemporary discussions of the accessory nerve, it is common to disregard the cranial component when referencing the accessory nerve and assume reference to the spinal accessory nerve.
Accessory Nerve Function
The accessory nerve provides motor innervation from the CNS to the sternocleidomastoid and trapezius muscles of the neck. The sternocleidomastoid muscle tilts and rotates the head, while the trapezius muscle has several actions on the scapula, including shoulder elevation and adduction of the scapula.
During neurological examinations, the function of the spinal accessory nerve is often measured by testing the range of motion and strength of the aforementioned muscles. Limited range of motion or diminished muscle strength often indicates injury of the accessory nerve.
Patients with spinal accessory nerve palsy may exhibit signs of lower motor neuron disease, such as atrophy and fasciculations of both the sternocleidomastoid and trapezius muscles.
Hypoglossal (XII) Nerve
The hypoglossal nerve (cranial nerve XII) controls the muscles of the tongue.
Key Points
It controls tongue movements of speech, food manipulation, and swallowing.
While the hypoglossal nerve controls the tongue’s involuntary activities of swallowing to clear the mouth of saliva, most of the functions it controls are voluntary, meaning that the execution of these activities requires conscious thought.
Proper function of the hypoglossal nerve is important for executing tongue movements associated with speech. Many languages require specific uses of the nerve to create unique speech sounds, which may contribute to the difficulties some adults encounter when learning a new language.
Key Terms
digastric muscle: A small muscle located under the jaw.
hypoglossal nerve: The twelfth cranial nerve (XII) controls the muscles of the tongue.
olivary body: Located on the anterior surface of the medulla, lateral to the pyramid.
medullary pyramid: Paired white matter structures of the brainstem’s medulla oblongata that contain motor fibers of the corticospinal and corticobulbar tracts.
Structure and Location
The hypoglossal nerve is the twelfth cranial nerve (XII) and innervates all extrinsic and intrinsic muscles of the tongue, except for the palatoglossus. The hypoglossal nerve emerges from the medulla oblongata in the preolivary sulcus where it separates the olive (olivary body) and the pyramid (medullary pyramid).
It goes on to traverse the hypoglossal canal and, upon emerging, it branches and merges with a branch from the anterior ramus of C1. It passes behind the vagus nerve and between the internal carotid artery and internal jugular vein which lies on the carotid sheath. After passing deep to the posterior belly of the digastric muscle it proceeds to the submandibular region to enter the tongue.
Sensory functions include the following:
Proprioception
Somatomotor functions include the following:
Innervation of the sternocleidomastoid muscle and the trapezius muscle to control the movement of the head and the shoulders
Swallowing movement
Hypoglossal nerve: Schematic image of the hypoglossal nerve and the structures it innervates.
Function
The hypoglossal nerve controls tongue movements of speech, food manipulation, and swallowing. It supplies motor fibers to all of the muscles of the tongue, with the exception of the palatoglossus muscle, which is innervated by the vagus nerve (cranial nerve X) or, according to some classifications, by fibers from the glossopharyngeal nerve (cranial nerve IX) that hitchhike within the vagus.
While the hypoglossal nerve controls the tongue’s involuntary activities of swallowing to clear the mouth of saliva, most of the functions it controls are voluntary, meaning that the execution of these activities requires conscious thought.
Proper function of the hypoglossal nerve is important for executing the tongue movements associated with speech. Many languages require specific and sometimes unusual uses of the nerve to create unique speech sounds, which may contribute to the difficulties some adults encounter when learning a new language. Several corticonuclear-originating fibers supply innervation and aid in the unconscious movements required upon engaging in speech and articulation.
Progressive bulbar palsy is neuromuscular atrophy associated with the combined lesions of the hypoglossal nucleus and the nucleus ambiguous, upon the atrophy of the motor nerves of the pons and medulla. This condition causes dysfunctional tongue movements that lead to speech and chewing impairments and swallowing difficulties. Tongue muscle atrophy may also occur.
Somatomotor functions include the following:
Innervation of tongue muscles
Transmission of impulses for speaking and swallowing
Sensory functions include the following:
Proprioception
Associated Conditions
The possible conditions associated with the cranial nerves are as follows:
Abducens Nerve Diseases – Also known as sixth cranial disorders, this palsy kind of disease results in diabetics, mostly. This condition is a part of Mononeuritis Multiplex, which may result in ischemia, hypertension (sometimes), or compression of the nerve by lesions in the cavernous sinus (eg, nasopharyngeal tumors), orbit, or base of the skull.
Accessory Nerve Diseases Of Cranial Nerves – Weakness in these muscles may result to a general disease process such as amyotrophic lateral sclerosis, Guillain-Barre syndrome or poliomyelitis. Injuries in these nerves can result in neck dissection and lymph node excision.
Glossopharyngeal Nerve Diseases – Glossopharyngeal neuralgia is a state wherein one can experience unbearable, frequent pain in the throat, ears, tongue, and tonsils. However, this pain can stay around a few minutes.
Cranial Nerve Injuries – These are commonly traumatic injuries.
Cranial Nerve Malignant Neoplasm – Malignant cranial nerve sheath tumors are uncommon and deals with weak prognosis as those of spinal nerves at other places.
Facial Nerve Diseases – This conditions pull down your facial expressions and cause weakness on your face. Bell’s palsy, Ramsay Hunt syndrome, Lyme disease are the conditions associated with facial nerve disorders.
Hypoglossal Nerve Diseases – This condition results in tight oral musculature, making it difficult for the person to chew or eat.
Ocular Motility Disorders – This causes impairment of eye movements.
Olfactory Nerve Diseases – This is a result of a physical blockage in the nose and this can cause loss of smell.
Optic Nerve Diseases – These disorders are related to loss of vision.
Trochlear Nerve Diseases – Injuries in the nucleus of the midbrain can be counted within this.
Vagus Nerve Diseases – These are caused by the damage of stomach muscles.
Vestibulocochlear Nerve Diseases – Disorders related to this affects the inner ear and weaken the functions related to it.
Nerves is an enclosed, cable-like bundle of nerve fibers called axons, in the peripheral nervous system. A nerve transmits electrical impulses and is the basic unit of the peripheral nervous system. A nerve provides a common pathway for the electrochemical nerve impulses called action potentials that are transmitted along each of the axons to peripheral organs or, in the case of sensory nerves, from the periphery back to the central nervous system. Each axon within the nerve is an extension of an individual neuron, along with other supportive cells such as some Schwann cells that coat the axons in myelin.
Nerves are a part of the nervous system. They are primarily involved in the control and coordination of all the parts of the body. The nervous system not only sends and receives messages but also processes them into chemical signals called impulses in the human body.
Types of Nerves
There are three types of nerves in the human body which are classified based on their functions. These are the sensory nerves, motor nerves, and mixed nerves.
Sensory Nerves
These are the nerves that send messages to the brain or the spinal cord from the sense organs. These are enclosed in the form of bundle structures or nerve fibers in the peripheral nervous system. They carry information from the PNS to the CNS( Central Nervous System).
Motor Nerves
Motor nerves are those nerves that carry the messages in the form of a response from the brain or the spinal cord to other parts of the body such as the muscles and glands. They are responsible for carrying the information from the CNS to the PNS.
Mixed Nerves
Mixed nerves are the nerves that perform both the action of sensory nerves as well as motor nerves. They transform electrical impulses from the central nervous system to the muscles of the body. Generally, the mixed nerves transmit impulses at the rate of 120 meters per second or 432 kilometers per hour.
Structure of a Nerve
A nerve is the primary structure of the peripheral nervous system and is composed of bundles of axons.
Nerves are the organs that make up the peripheral nervous system. It consists of a cord-like structure with multiple nerve fibers (also called axons) wrapped in layers of tissue and fat. This axon has layers of connective tissue around it. This connective tissue is called the endoneurium. This entire nerve is further enclosed in another layer of connective tissue called the epineurium.
Neuron Structure
The structure of a nerve is explained below:
A group of neurons is organized into bundles inside the nerves. This bundle is known as fascicles.
The perineurium surrounds and holds together each fascicle.
The perineurium is concentrically laminated and composed of flattened cells collagen fibers and basement membranes.
Neurons and blood vessels are held inside the fascicles by a loose connective tissue known as endoneurium. It covers and holds the outer surface of the nerves together.
Arteries and veins are present between the fascicles. These blood vessels supply nutrients and gases to the neurons inside the fascicles.
Key Points
A nerve is the primary structure of the peripheral nervous system (PNS) that encloses the axons of peripheral neurons.
A nerve provides a structured pathway that supports neuron function.
A nerve consists of many structures including axons, glycocalyx, endoneurial fluid, endoneurium, perineurium, and epineurium.
The axons are bundled together into groups called fascicles, and each fascicle is wrapped in a layer of connective tissue called the perineurium.
Magnetic resonance neurography is a technology used to detect nerve damage.
Key Terms
endoneurial fluid: A low protein liquid that is the peripheral nervous system equivalent to cerebrospinal fluid in the central nervous system.
perineurium: A protective sheath covering nerve fascicles.
glycocalyx: A glycoprotein-polysaccharide covering that surrounds cell membranes.
endoneurium: A layer of connective tissue that surrounds axons.
fascicles: A small bundle of nerve fibers enclosed by the perineurium.
epineurium: The outermost layer of dense, irregular connective tissue surrounding a peripheral nerve.
Nerve Anatomy
Nerves: An illustration of the main nerves of the arm.
A nerve is an enclosed, cable-like bundle of axons (the projections of neurons) in the peripheral nervous system (PNS). A nerve provides a structured pathway that supports the electrochemical nerve impulses transmitted along each of the axons.
In the central nervous system, the analogous structures are known as tracts. Neurons are sometimes referred to as nerve cells, although this term is misleading since many neurons do not occupy nerves, and nerves also include non-neuronal support cells (glial cells) that contribute to the health of enclosed neurons.
Each nerve contains many axons that are sometimes referred to as fibers. Within a nerve, each axon is surrounded by a layer of connective tissue called the endoneurium. The axons are bundled together into groups called fascicles. Each fascicle is wrapped in a layer of connective tissue called the perineurium.
Finally, the entire nerve is wrapped in a layer of connective tissue called the epineurium. See the following illustrations of these structures.
The endoneurium consists of an inner sleeve of material called the glycocalyx and a mesh of collagen. Nerves are bundled along with blood vessels, which provide essential nutrients and energy to the enclosed and metabolically demanding, neurons.
Within the endoneurium, individual nerve fibers are surrounded by a liquid called the endoneurial fluid. The endoneurium has properties analogous to the blood-brain barrier. It prevents certain molecules from crossing from the blood into the endoneurial fluid.
In this respect, endoneurial fluid is similar to cerebrospinal fluid in the central nervous system. During nerve irritation or injury, the amount of endoneurial fluid may increase at the site of damage. This increase in fluid can be visualized using magnetic resonance neurography to diagnose nerve damage.
(a) Anatomy of a nerve and (b) Cross-section of a nerve: The primary structures of a nerve. An illustration of a cross-section of a nerve highlighting the epineurium and perineurium. Individual axons can also be seen as tiny circles within each perineurium.
Basic Function
A nerve conveys information in the form of electrochemical impulses (known as nerve impulses or action potentials) carried by the individual neurons that make up the nerve. These impulses are extremely fast, with some myelinated neurons conducting at speeds up to 120 m/s. The impulses travel from one neuron to another by crossing a synapse, and the message is converted from electrical to chemical and then back to electrical.
Nerves can be categorized into two groups based on function:
Sensory nerves conduct sensory information from their receptors to the central nervous system, where the information is then processed. Thus they are synonymous with afferent nerves.
Motor nerves conduct signals from the central nervous system to muscles. Thus they are synonymous with efferent nerves.
Neurologists usually diagnose disorders of the nerves by a physical examination, including the testing of reflexes, walking and other directed movements, muscle weakness, proprioception, and the sense of touch. This initial exam can be followed with tests such as nerve conduction study, electromyography, or computed tomography.
Classification of Nerves
Nerves are primarily classified based on their direction of travel to or from the CNS, but they are also subclassified by other nerve characteristics.
Key Points
Nerves can be categorized as afferent, efferent, and mixed based on the direction of signal transmission within the nervous system. Nerves can be further categorized as spinal nerves or cranial nerves based on where they connect to the central nervous system.
Individual peripheral nerve fibers are classified based on the diameter, signal conduction velocity, and myelination state of the axons, as well as by the type of information transmitted and the organs they innervate.
Key Terms
mixed nerve: Nerves that contain both afferent and efferent axons, and thus conduct both incoming sensory information and outgoing muscle commands in the same bundle.
Afferent nerve: Carries nerve impulses from sensory receptors or sense organs toward the central nervous system.
Schwann cell: The principal glia of the peripheral nervous system.
efferent nerve: Nerves that conduct signals from the central nervous system along motor neurons to their target muscles and glands.
spinal nerve: The term generally refers to a mixed nerve that carries motor, sensory, and autonomic signals between the spinal cord and the body.
Nerve Classifications
The direction of Signal Transmission
Nerves are categorized into three, primary groups based on the direction of signal transmission within the nervous system.
Afferent nerves conduct signals from sensory neurons to the central nervous system, for example from mechanoreceptors in skin.
Efferent nerves conduct signals away from the central nervous system to target muscles and glands.
Mixed nerves contain both afferent and efferent axons, and thus conduct both incoming sensory information and outgoing muscle commands in the same nerve bundle.
Afferent and efferent nerve transmission: Schematic of efferent and afferent nerve transmission to and from peripheral tissue and spinal cord.
Central Nervous System Connection
Nerves can be further categorized based on where they connect to the central nervous system. Spinal nerves innervate much of the body and connect through the spinal column to the spinal cord. Spinal nerves are assigned letter-number designations according to the vertebra where they connect to the spinal column. Cranial nerves innervate parts of the head and connect directly to the brain. Cranial nerves are typically assigned Roman numerals from 0 to 12.
Diameter, Conduction Velocity, Myelination State
Peripheral nerve fibers are grouped based on the diameter, signal conduction velocity, and myelination state of the axons. These classifications apply to both sensory and motor fibers. Fibers of the A group have a large diameter, high conduction velocity, and are myelinated.
The A group is further subdivided into four types (A-alpha, A-beta, A-delta, and A-gamma fibers) based on the information carried by the fibers and the tissues they innervate.
A-alpha fibers are the primary receptors of the muscle spindle and golgi tendon organ.
A-beta fibers act as secondary receptors of the muscle spindle and contribute to cutaneous mechanoreceptors.
A-delta fibers are free nerve endings that conduct painful stimuli related to pressure and temperature.
A-gamma fibers are typically motor neurons that control the intrinsic activation of the muscle spindle.
Fibers of the B group are myelinated with a small diameter and have a low conduction velocity. The primary role of B fibers is to transmit autonomic information. Fibers of the C group are unmyelinated, have a small diameter, and low conduction velocity. The lack of myelination in the C group is the primary cause of their slow conduction velocity.
Saltatory conduction: Demonstrates the faster propagation of an action potential in myelinated neurons than that of unmyelinated neurons.
C fiber axons are grouped together into what is known as Remak bundles. These occur when an unmyelinated Schwann cell bundles the axons close together by surrounding them. The Schwann cell keeps them from touching each other by squeezing its cytoplasm between the axons.
C fibers are considered polymodal because they can often respond to combinations of thermal, mechanical, and chemical stimuli.
A-delta and C fibers both contribute to the detection of diverse painful stimuli. Because of their higher conduction velocity, A-delta fibers are responsible for the sensation of sharp, initial pain and respond to a weaker intensity of the stimulus.
These nerve fibers are associated with acute pain and therefore constitute the afferent portion of the reflex arc that results in pulling away from noxious stimuli. An example is a retraction or your hand from a hot stove. Slowly conducting, unmyelinated C fibers, by contrast, carry slow, longer-lasting pain sensations.
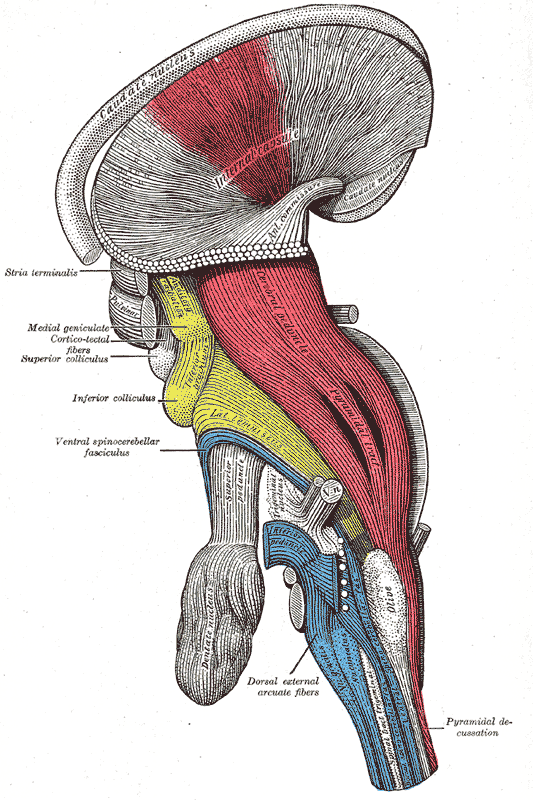
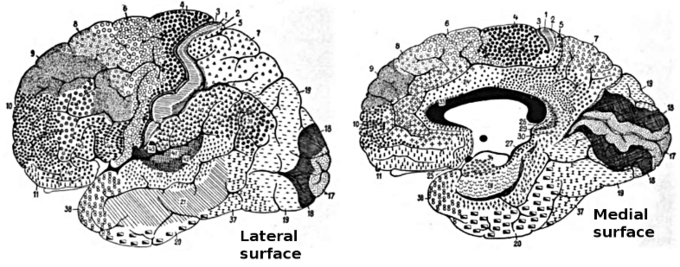

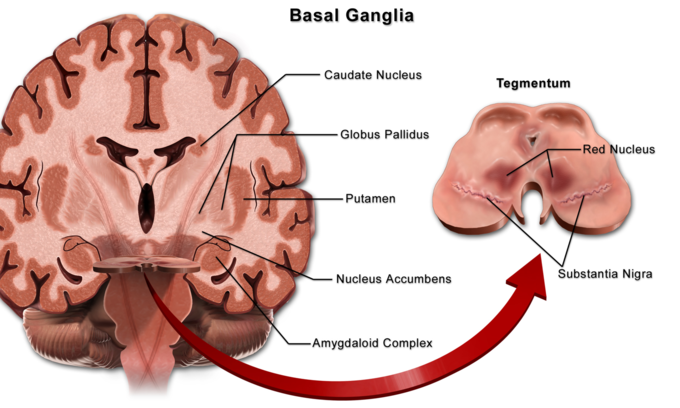

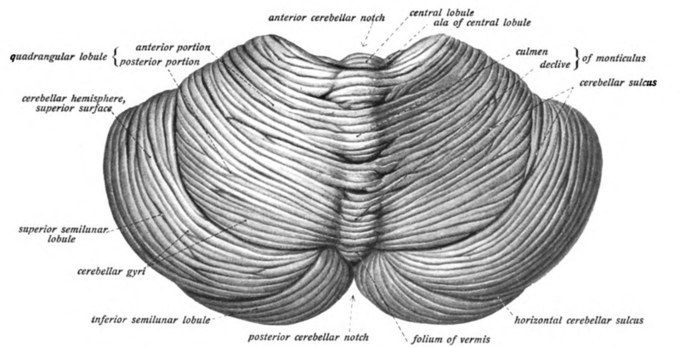
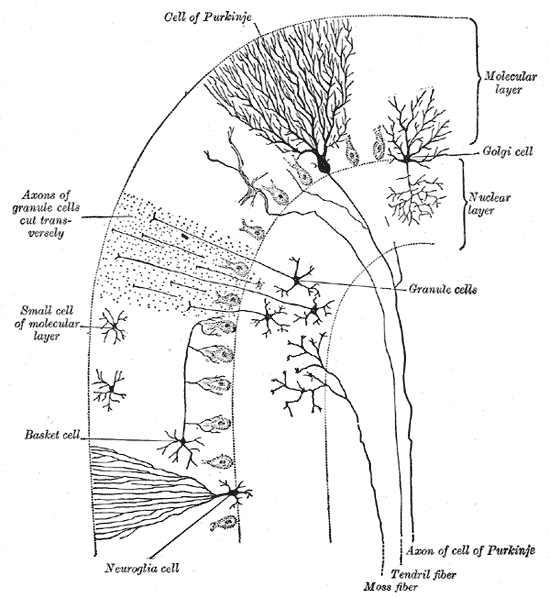
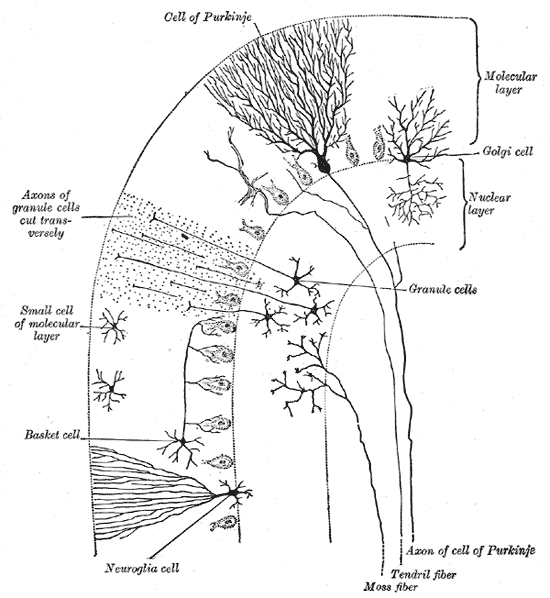





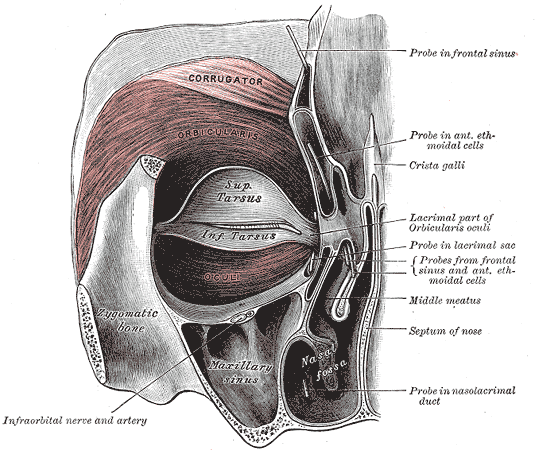




















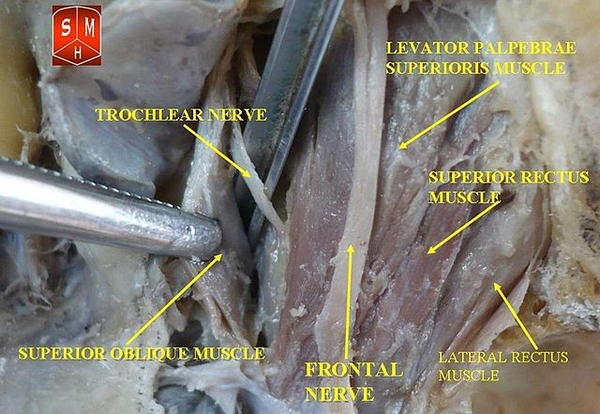
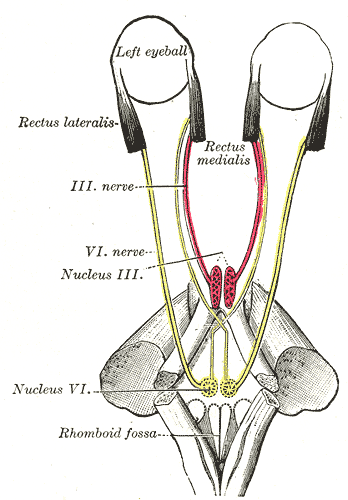















")
")