Fibromyalgia is a common condition characterized by abnormal central nervous system sensitivity to external stimuli. It affects between 2 and 8% of the total population, with a strong female predominance. The most recognizable clinical feature associated with fibromyalgia is widespread pain and tenderness throughout multiple regions of the body, in the absence of pathology at the sites of pain. Patients may also experience a wide variety of other symptoms including fatigue and sleep disturbance, cognitive changes such as poor concentration and memory, and amplified sensory systems leading to an intolerance of loud noise, bright lights, and strong odors. Medication side effects are commonly exacerbated in this patient population and many drugs are poorly tolerated. Fibromyalgia is associated with several related medical conditions including irritable bowel syndrome, temporomandibular joint dysfunction, tension headaches, chronic fatigue syndrome, and restless leg syndrome.
Fibromyalgia is a syndrome characterized by chronic widespread pain at multiple tender points, joint stiffness, and systemic symptoms (e.g., mood disorders, fatigue, cognitive dysfunction, and insomnia) [rx–rx] without a well-defined underlying organic disease. Nevertheless, it can be associated with specific diseases such as rheumatic pathologies, psychiatric or neurological disorders, infections, and diabetes
The pathophysiology of fibromyalgia is complex, although understanding has increased substantially in recent years. The net effect of multiple factors leads to a sensitization of central pain and sensory processing centers such that patients become overly sensitive to external stimuli. Functional imaging studies have shown amplified responses in sensory regions of the brain when mechanical or painful stimuli are administered. There is also evidence of enhanced connections between brain centers that process pain and sensory input, such as the insular cortex, and parts of the brain associated with concentration and working memory, such as the frontoparietal executive attention network. This may provide some explanation for the cognitive symptoms many patients experience. Several abnormalities of neurotransmitters have also been identified in fibromyalgia patients, and relate to the modulation of descending sensory inhibitory pathways from the brain to the spinal cord. These are discussed in relation to specific pharmacological interventions in later sections
Fibromyalgia has a strong genetic predisposition — twin studies suggest the contribution is as high as 50%. In genetically susceptible individuals, symptoms tend to be triggered by a stressful event such as physical illness, trauma or psychological distress Symptoms of fibromyalgia wax and wane over time, and tend to be exacerbated by fluctuations in psychological or physical stress.
Diagnosis of fibromyalgia is based on the identification of characteristic clinical features. Validated diagnostic criteria are available and require the presence of widespread pain in conjunction with high levels of some of the above mentioned associated symptoms.
Causes of Fibromyalgia
Infections – Prior illnesses may trigger fibromyalgia or make symptoms of the condition worse.
Genetics – Fibromyalgia often runs in families. If you have a family member with this condition, your risk for developing it is higher. Researchers think certain genetic mutations may play a role in this condition. Those genes haven’t yet been identified.
Trauma – People who experience physical or emotional trauma may develop fibromyalgia. The condition has been linked with post-traumatic stress disorder.
Stress – Like trauma, stress can create long-reaching effects your body deals with for months and years. Stress has been linked to hormonal disturbances that could contribute to fibromyalgia.
Viral infection – Viral infections such as the herpes simplex -1 virus, commonly linked to cold sores, have been connected to the development of fibromyalgia.
Dysfunctional pain processing – Many researchers agree that one of the key causes of fibromyalgia is dysfunction in the central nervous system’s (CNS) pain processing.
Having a family history of fibromyalgia
Repetitive injuries
Rheumatoid arthritis or other autoimmune diseases
Central nervous system (CNS) problems
The way our genes regulate how we process painful stimuli
Being exposed to stressful or traumatic events, such as
Car accidents
Injuries to the body caused by performing the same action over and over again (called “repetitive” injuries)
Infections or illnesses
Being sent to war
Symptoms of Fibromyalgia
Common symptoms include
widespread body-wide pain
jaw pain and stiffness
pain and tiredness in the face muscles and adjacent fibrous tissues
stiff joints and muscles in the morning
headaches
irregular sleep patterns
irritable bowel syndrome (IBS)
painful menstrual periods
tingling and numbness in the hands and feet
restless leg syndrome (RLS)
sensitivity to cold or heat
difficulties with memory and concentration are known as “fibro-fog”
fatigue
The following are also possible:
problems with vision
nausea
pelvic and urinary problems
weight gain
dizziness
cold or flu-like symptoms
skin problems
chest symptoms
depression and anxiety
breathing problems
dizziness and clumsiness
feeling too hot or too cold – this is because you’re not able to regulate your body temperature properly
restless legs syndrome (an overwhelming urge to move your legs)
tingling, numbness, prickling or burning sensations in your hands and feet (pins and needles, also known as paraesthesia)
in women, unusually painful periods
anxiety
depression
Widespread muscle soreness
Muscle spasms
Tenderness
Headaches or migraines
Rebound pain
Irritable bowel syndrome
Nausea
Constipation
Excessive gas
Diarrhea
Painful bladder syndrome
Increased sensitivity to pain
Pins and needles sensations
Increased overall sensitivity to cold and touch
Forgetfulness
Inability to concentrate, or “fibro fog”
Problems with balance and coordination
Fatigue
Depression
Nervous energy
Anxiety
Emotional sensitivity
Increased stress response
Sleep disorders
Joint stiffness
Menstrual pain or changes
Increased chance of other health conditions
Diagnosis of Fibromyalgia
Differential diagnosis
This includes:
inflammatory arthritis (IA) and spondylo-arthropathies,
autoimmune connective tissue disease,
myositis,
myopathies,
primary generalized osteoarthritis,
polymyalgia rheumatica,
hypothyroidism,
malignancies.
Laboratory Investigations
Laboratory testing, such as complete blood count, erythrocyte sedimentation rate, rheumatoid factor, antinuclear antibody, thyroid-stimulating hormone, T3, T4, creatinine phosphokinase, a serum muscle enzyme, vitamin D, ESR, CRP, renal function, and liver function tests are necessary to rule out other disorders. X-rays, blood tests, specialized scans such as nuclear medicine and CT scan muscle biopsy are normal in cases of fibromyalgia.
Differential diagnoses for fibromyalgia and corresponding diagnostic testing options.
The location of the nine paired tender points that comprise the 1990 American College of Rheumatologycriteria for fibromyalgia.
There is no single test that can fully diagnose fibromyalgia and there is debate over what should be considered essential diagnostic criteria and whether an objective diagnosis is possible. In most cases, people with fibromyalgia symptoms may also have laboratory test results that appear normal and many of their symptoms may mimic those of other rheumatic conditions such as arthritis or osteoporosis. The most widely accepted set of classification criteria for research purposes was elaborated in 1990 by the Multicenter Criteria Committee of the American College of Rheumatology. These criteria, which are known informally as “the ACR 1990”, define fibromyalgia according to the presence of the following criteria:
A history of widespread pain lasting more than three months – affecting all four quadrants of the body, i.e., both sides, and above and below the waist.
Tender points – there are 18 designated possible tender points (although a person with the disorder may feel pain in other areas as well). Diagnosis is no longer based on the number of tender points.
The ACR criteria for the classification of patients were originally established as inclusion criteria for research purposes and were not intended for clinical diagnosis but have now become the de facto diagnostic criteria in the clinical setting. It should be noted that the number of tender points that may be active at any one time may vary with time and circumstance. A controversial study was done by a legal team looking to prove their client’s disability based primarily on tender points and their widespread presence in non-litigious communities prompted the lead author of the ACR criteria to question now the useful validity of tender points in diagnosis. Use of control points has been used to cast doubt on whether a person has fibromyalgia, and to claim the person is malingering; however, no research has been done for the use of control points to diagnose fibromyalgia, and such diagnostic tests have been advised against, and people complaining of pain all over should still have fibromyalgia considered as a diagnosis.
2010 provisional criteria
Widespread Pain Index (WPI) Areas
In 2010, the American College of Rheumatology approved provisional revised diagnostic criteria for fibromyalgia that eliminated the 1990 criteria’s reliance on tender point testing. The revised criteria use a widespread pain index (WPI) and symptom severity scale (SS) in place of tender point testing under the 1990 criteria. The WPI counts up to 19 general body areas in which the person has experienced pain in the preceding two weeks. The SS rates the severity of the person’s fatigue, unrefreshed waking, cognitive symptoms, and general somatic symptoms, each on a scale from 0 to 3, for a composite score ranging from 0 to 12. The revised criteria for diagnosis are:
WPI ≥ 7 and SS ≥ 5 OR WPI 3–6 and SS ≥ 9,
Symptoms have been present at a similar level for at least three months, and
No other diagnosable disorder otherwise explains the pain.
Multidimensional assessment
Some research has suggested not to categorize fibromyalgia as a somatic disease or a mental disorder, but to use a multidimensional approach taking into consideration somatic symptoms, psychological factors, psychosocial stressors and subjective belief regarding fibromyalgia. A review has looked at self-report questionnaires assessing fibromyalgia on multiple dimensions, including:
Revised Fibromyalgia Impact Questionnaire
Widespread Pain Index
Hospital Anxiety and Depression Scale
Multiple Ability Self-Report Questionnaire
Multidimensional Fatigue Inventory
Medical Outcomes Study Sleep Scale
Fibromyalgia survey questionnaire
I. Using the following scale, indicate for each item the level of severity over the past week by checking the appropriate box.
0: No problem
1: Slight or mild problems; generally mild or intermittent
2: Moderate; considerable problems; often present and/or at a moderate level
3: Severe; continuous, life-disturbing problems
Fatigue
□ 0 □ 1 □ 2 □ 3
Trouble thinking or remembering
□ 0 □ 1 □ 2 □ 3
Waking up tired (unrefreshed)
□ 0 □ 1 □ 2 □ 3
II. During the past 6 months have you had any of the following symptoms?
Pain or cramps in lower abdomen
□ Yes □ No
Depression
□ Yes □ No
Headache
□ Yes □ No
III. Joint/body pain
Please indicate below if you have had pain or tenderness over the past 7 days in each of the areas listed below. Please make an X in the box if you have had pain or tenderness. Be sure to mark both right side and left side separately.
□ Shoulder, left
□ Upper leg, left
□ Lower back
□ Shoulder, right
□ Upper leg, right
□ Upper back
□ Hip, left
□ Lower leg, left
□ Neck
□ Hip, right
□ Lower leg, right
□ Upper arm, left
□ Jaw, left
□ No pain in any of these areas
□ Upper arm, right
□ Jaw, right
□ Lower arm, left
□ Chest
□ Lower arm, right
□ Abdomen
IV. Overall, were the symptoms listed in I–III above generally present for at least 3 months? □ Yes □ No
Comparison between American Pain Society (APS) and Association of the Scientific Medical Societies in Germany (AWMF) with European League Against Rheumatism (EULAR).
Nonpharmacologic treatment
Medications
APS (American Pain Society) and AWMF (Association of the Scientific Medical Societies in Germany)
Antidepressants (amitriptyline, fluoxetine, duloxetine, milnacipran, moclobemide, pirlindol) (grade A)
Others: relaxation, rehabilitation, physiotherapy, and/or psychological support (grade C)
Tropisetron, pramipexole, pregabalin (grade A)
Fibromyalgia can have a substantial impact on both a patient’s mental and physical health. Low work participation, high rates of financial dependency and poor quality of life are all well described in this population Treatment of fibromyalgia is aimed at modulating central pain pathways to reduce sensitivity, which can be obtained via a range of treatment modalities. The most recently published guidelines are the 2016 European League Against Rheumatism (EULAR) fibromyalgia management guidelines, and the 2012 Canadian fibromyalgia diagnosis and management guidelines, and these are referred to and discussed in this article
The mainstay of treatment is non-pharmacological. Evidence-based treatment strategies with the highest efficacy include education in relation to the nature of the condition, graded exercise programmes, and psychological-based interventions. These may range from cognitive-based stress management therapy with a pain management psychologist to yoga, tai-chi or simple meditation strategies. These non-pharmacological interventions are recommended by EULAR as first-line treatments. More than 30 trials involving more than 2,000 fibromyalgia patients have been performed evaluating various forms of exercise, and a further 2,000 patients have been involved in trials of cognitive based therapy (CBT). Both aerobic and strengthening exercises have been shown to significantly reduce pain and increase function, with CBT also proving effective, albeit with lower quality evidence. The EULAR guidelines provide a thorough review of the evidence to support the various non-pharmacological strategies available.
However, many patients require the addition of pharmacological therapy for the management of their symptoms. It should be noted that medication is unlikely to be of benefit in isolation in the absence of the above-mentioned strategies.
Medications recommended for the treatment of fibromyalgia
Several medications have shown some efficacy in the management of fibromyalgia. Availability and condition-specific approval of medications vary across countries (see Table 1). There are currently no medications with fibromyalgia-specific approval under the European Medicines Agency, although many of the discussed agents are approved for other conditions. Many patients will respond to some degree to one or more of the discussed medications, although each individual medication is only effective in a minority of patients. Patients may need to trial several options before finding one that is both tolerable and helpful.
Table 1: Availability and approval of recommended medications for fibromyalgia
These include the antidepressant (tricyclic, selective serotonin-norepinephrine uptake inhibitor (SNRI), serotonin selective reuptake inhibitor (SSRI)] and anticonvulsant classes of medications. Amitriptyline has some evidence[rx] and is recommended in all the guidelines,[rx]and, therefore, is worthwhile considering particularly for patients with FM and sleep disturbance. The serotonin-norepinephrine uptake inhibitors (SNRIs) have better evidence than SSRIs,7 and may benefit from their effect on both serotonin and noradrenaline on the descending modulatory pathways. Gabapentin and pregabalin are also commonly used in FM and CWP.
Serotonin and noradrenergic reuptake inhibitors (SNRIs)
Serotonin and noradrenaline are neurotransmitters involved in pain-processing pathways via their action on descending inhibitory pathways in the brain and spinal cord, with the net effect of reducing sensory input from the periphery. Both neurotransmitters have an array of other functions including roles in the regulation of mood and emotion, with noradrenaline also involved in the regulation of attention and memory
The cerebrospinal fluid (CSF) of patients with fibromyalgia has been shown to have lower levels of biogenic amines, the metabolites of noradrenaline and serotonin, suggesting a deficiency of these neurotransmitters. Studies using murine models have shown that modulation of noradrenaline and serotonin in unison provides more effective analgesic effects than modulation of serotonin alone. However, there is no direct comparative study between SNRIs and selective serotonin reuptake inhibitors (SSRIs) in fibromyalgia. Two SNRI medications, duloxetine, and milnacipran are recommended for the treatment of fibromyalgia. Milnacipran is not approved by the European Medicines Agency, but it is approved in several European countries for indications other than fibromyalgia, such as depression (see Table 1).
Duloxetine – is an SNRI originally marketed for the treatment of depression, but several studies have since evaluated its benefit in fibromyalgia A meta-analysis of six randomized trials of duloxetine compared with placebo in more than 2,000 patients with fibromyalgia showed a significant improvement in a pain reduction at weeks 12 and 28. Overall, the number needed to treat was eight.
Doses can range from 30 to 120mg daily, however, many patients with fibromyalgia cannot tolerate doses above 60mg. Common side effects include a headache, palpitations, nausea, and flushing. Some patients find that duloxetine causes drowsiness and should take it before bed, while a smaller number of patients find it stimulating, and thus benefit more from taking it in early in the day.
Milnacipran – is another SNRI recommended for the management of fibromyalgia. Trial data suggest that milnacipran improved quality of life and patient reported pain in around 15% of participants above that of placebo. The usual marketed dose of milnacipran is 50mg twice daily. However, many patients only tolerate much smaller doses, such as 25mg once or twice daily. Patients should be initiated on a dose of 25mg daily and then titrated upwards by 25mg daily at a minimum of every few days. Milnacipran has a similar side effect profile to duloxetine but has stronger noradrenergic qualities than duloxetine and for this reason may be more stimulating.
Patients with prominent fatigue symptoms may benefit from SNRIs, in particular, milnacipran, but they may be less appropriate for those patients with significant insomnia. Concurrent depressive or anxiety symptoms may be another reason for the preference of these agents in individual patients.
Duloxetine is metabolized via the cytochrome (CY) P450 2D6 pathway, a system which metabolizes around 25% of clinically used drugs, and there is, therefore, a high risk of drug interactions Variations in the metabolism of duloxetine can occur due to polymorphisms of the 2D6 gene. By comparison, milnacipran is not metabolized via the CYP450 pathway and, as such, drug interactions are much less likely.
SNRIs can be combined with pregabalin and simple analgesics, however, caution should be taken when combining SNRIs with tricyclic antidepressants or tramadol due to the potential risk of serotonin syndrome. Low doses in combination may be considered with careful patient education and monitoring. The symptoms of serotonin syndrome are variable and include cognitive changes such as agitation, autonomic symptoms (e.g. flushing and sweating), and neuromuscular symptoms (e.g. tremor). The exact incidence of serotonin syndrome is unknown due to the lack of large studies and variations in diagnostic criteria, however, potent CYP450 2D6 inhibitors, increased age, and higher doses increase the risk of this complication Most cases are mild and self-limiting on drug cessation, however, rare severe cases can be life-threatening. SNRIs are recommended in both the EULAR and Canadian Guidelines
Selective serotonin reuptake inhibitors (SSRIs)
As discussed above, the modulation of serotonin alone is of less benefit than dual modulation of noradrenaline and serotonin together in the treatment of fibromyalgia. Several studies have evaluated the use of SSRIs in fibromyalgia with inconsistent results. A meta-analysis of seven studies demonstrated some benefit when compared with placebo, although the quality of the study overall was low and the authors reported that there was no unbiased high-quality data to support the use of SSRIs in the management of fibromyalgia The EULAR guidelines recommend against the use of SSRIs, while the Canadian guidelines suggest their use may be appropriate as an alternative to SNRIs. Common side effects associated with SSRIs include nausea, sexual dysfunction, dry mouth, drowsiness, and insomnia.
Gabapentinoids
Pregabalin – was originally marketed as an antiepileptic but is now commonly used for pain management. It mediates its effects by binding to voltage-gated calcium channels, reducing calcium influx at sensitized spinal cord neurons, thereby reducing the release of neuroactive molecules, including glutamate, substance P and noradrenaline, into the synapse. It has been shown that patients with fibromyalgia have increased levels of glutamate in their insula, an area of the brain involved in pain processing and that pregabalin can reduce this, leading to an associated decreased level of perceived pain. Several studies have evaluated its effectiveness in fibromyalgia, and a recent Cochrane Review reported pregabalin reduces pain with tolerable side effects in around 10% of patients above that of placebo.
The full dose of pregabalin given to patients can be as high as 300mg twice daily, but similarly, with many other medications, patients with fibromyalgia are poorly tolerant of such doses. Pregabalin can be initiated at a dose of 25–75mg daily, with the additional 25–75mg every one to two weeks as tolerated. Common side effects associated with pregabalin include dizziness, somnolence, and weight gain. If somnolence is prominent, patients may benefit from taking pregabalin only at night to enhance sleep and minimize daytime drowsiness. Drug interactions are uncommon and pregabalin can be safely added to SNRIs, tricyclic antidepressants (TCAs) and most analgesics. It may be best for patients with prominent pain and sleep disturbance and is less effective for fatigue. Pregabalin is recommended in both the EULAR and Canadian guidelines
Gabapentin – is another antiepileptic medication that is sometimes used to treat fibromyalgia. Gabapentin has a similar mechanism of action to pregabalin and exerts its effects via modulating neuronal voltage-gated calcium channels It has a shorter half-life than pregabalin, and is usually given three or more times daily, which may make dose titration easier, however, this does increase pill burden. Gabapentin is cheaper than pregabalin and may be prescribed for this reason. A small randomized trial of 150 patients reported that patients taking 1200-2400mg of gabapentin were more likely to have a 30% reduction in their pain at week 12, with a response rate around 20% higher in the treatment group compared with placebo , However, a recent Cochrane Review concluded that there is currently insufficient evidence to recommend gabapentin for routine use in fibromyalgia treatment The EULAR guidelines make no recommendation for or against gabapentin given limited data; however, the Canadian guidelines do not differentiate between pregabalin and gabapentin.
Like SNRIs, TCAs mediate their effects via modulation of noradrenaline and serotonin and were originally developed for the treatment of depression.
Amitriptyline – is a TCA commonly prescribed for the management of fibromyalgia and short-term studies have shown clinical improvements in 15-20% of patients taking amitriptyline above that of placebo. Nortriptyline is an alternative option; however, fewer studies have examined the use of this agent.
Side effects from amitriptyline are common and include dry mouth, constipation, daytime drowsiness, and mental clouding. Like pregabalin, patients may benefit from taking this medication in the evening to promote sleep and minimize daytime side effects. Typically, much smaller doses are used in fibromyalgia than in depression, with between 10mg and 25mg usually prescribed as an early evening dose, with doses above 50mg seldom being used for this indication. It can be co-prescribed with pregabalin, SSRIs and simple analgesics, and cautiously with SNRI medications as discussed above. It may be particularly helpful in patients in whom insomnia is a prominent clinical feature.
Cyclobenzaprine – is a medication with a similar tricyclic structure to amitriptyline, but is not known to have antidepressant effects. It is available in the United States but not in the UK. A meta-analysis of the use of this medication in patients with fibromyalgia reported that it leads to symptomatic improvement in one in five patients. The side effects commonly associated with the use of cyclobenzaprine are similar to amitriptyline. Doses of 1–4mg at night has been shown to improve sleep. Both amitriptyline and cyclobenzaprine are recommended in the EULAR and Canadian guidelines.
Tramadol is a weak opioid with mild serotonin-noradrenaline reuptake inhibition. A small study showed the benefit of tramadol in combination with paracetamol in patients with fibromyalgia compared with placebo. In this study, patients were given 37.5mg of tramadol four times per day. While difficult to confirm, it is likely that the positive effects of tramadol in fibromyalgia are due to their SNRI activity as opposed to their opioid effect. As discussed in the next section, opioids are unlikely to be beneficial in fibromyalgia, with side effects likely to include drowsiness, dizziness, and nausea. Tramadol is recommended in the EULAR fibromyalgia guidelines, however, in the Canadian guidelines, it is suggested that tramadol is reserved for those patients with significant symptoms not responding to the above-mentioned drug classes. It should be used with caution with SSRIs, SNRIs, and TCAs and, as it is metabolized by CYP450 2D6 and 3A4 pathways, medications that are potent inhibitors of this pathway, such as paroxetine or fluoxetine, should be avoided.
Contraindications, warning and precautions with regards to the most commonly used drugs in fibromyalgia syndrome (FMS) as per summary of product characteristic (SPC).
Drug
Contraindications
Warning and Precautions
Last Update
Amitriptyline
Prior Hypersensitivity
Concomitant use of MAOI
Acute recovery phase following myocardial infarction
Mania
Sever liver disease
Congestive heart failure
Suicidality
Hyponatraemia
QT interval prolongation on ECG
Blood dyscrasias
5 December 2016
Duloxetine
Serotonin syndrome and MAOIs.
Concomitant use of irreversible MOAi, fluvoxamine, ciprofloxacin or enoxacin
Liver disease resulting in hepatic impairment
Severe renal impairment
Known hypersensitivity to pregabalin (PGB) or any of its components
-Hypersensitivity reaction
-Dizziness, somnolence, loss of consciousness
-Vision-related effects
-Increase risk of suicidal thoughts and behaviours
-Encephalopathy
Reduced lower gastrointestinal tract function
14 November 2016
Tramadol Hydrochloride
Hypersensitivity to tramadol or other opioids
Severe hepatic/renal impairment
MOA or within 2 weeks of their withdrawal
Withdrawal symptoms
Dependence and abuse
Convulsive disorders
22 September 2015
Milnacipran
HypersensitivityConcomitant use to MAOI
Liver disease resulting in hepatic impairment
Uncontrolled hypertensionSevere renal impairment
As per Duloxetine
8 February 2017
SSRI (Fluoxetine)
Concomitant of metoprolol and irreversible non-selective MAO, hypersensitivity to the active substance
Suicidality
Rash and allergic reaction
Seizures
Mania
Hepatic/renal function
Prolonged QT
It should be noted that in many of the discussed trials, medications were administered as a single agent in the absence of concurrent non-pharmacological management strategies, which is not consistent with the typical way these medications are used in clinical practice. Although there are limited data to support this approach, many patients who do not respond to a single agent receive combination therapy. A retrospective study reported that patients receiving either milnacipran or duloxetine in conjunction with pregabalin had improved pain scores compared with any of the three agents alone A further study suggested that adding milnacipran to pregabalin resulted in higher response rates than pregabalin alone. However, not unexpectedly, there were also more side effects associated with dual therapy. Further studies are required to investigate the efficacy of combination therapy and drug interactions need careful consideration.
Medications that are not recommended in fibromyalgia
Medications not recommended for treatment of fibromyalgia. Where no recommendation for/against is offered, a grey box is used. LE: level of evidence.
Nonsteroidal anti-inflammatory drugs (NSAIDs) and glucocorticoids act peripherally to reduce inflammation at the site of tissue damage. Given that the pain experienced by patients with fibromyalgia is not nociceptive, it is not surprising that these medications are not of particular benefit. Small studies have evaluated the use of both NSAIDs and low-to-moderate dose glucocorticoids in fibromyalgia and have found no benefit over placebo. Any concurrent inflammatory or mechanical musculoskeletal condition should be treated appropriately, which may include the use of these medications in some patients.
Opioids
Despite their common use, there is no evidence to suggest opioid medication is beneficial in fibromyalgia and, to the contrary, these medications may be associated with significant harm. There are no randomized trials available; however, longitudinal observational studies have suggested that patients with fibromyalgia taking opioid medications have worse outcomes than those patients not taking opioids in terms of pain, function, and quality of life.
There is evidence to suggest that patients with fibromyalgia have abnormal endogenous opioidergic activity. Patients with fibromyalgia have been shown to have reduced μ-opioid receptor binding in several central nervous systems (CNS) centers that are involved in processing pain, including the amygdala, cingulate and nucleus accumbens This reduced binding potential is associated with increased perceived pain. Furthermore, endogenous opioids have been shown to be elevated in the CSF of fibromyalgia patients. Together, these findings may be suggestive of a chronically activated endogenous opioid system leading to downregulation of opioid receptors. This explanation provides a rationale for why fibromyalgia patients respond poorly to opioid medication. In line with this, it has been shown that patients with more fibromyalgia symptoms were likely to require significantly more opioid post joint replacement surgery than those patients with fewer fibromyalgia symptoms.
Beyond this, common opioid-related side effects such as drowsiness and mental clouding are likely to exacerbate symptoms of fibromyalgia. Enteral side effects of opioids may worsen irritable bowel syndrome which is commonly associated with fibromyalgia. A further concern is that of opioid hyperalgesia, which can occur with prolonged opioid use and causes a paradoxical increase in pain sensitivity. This phenomenon may be related to sensitization of pro-nociceptive pathways secondary to opioid induced toll like receptor 4 (TLR4) activation in glial cells. TLR4 activation leads to the release of neuroexcitatory and proinflammatory products. Opioids, excluding tramadol, are not recommended by any current guidelines for the management of fibromyalgia.
Medications requiring more study to assess efficacy in fibromyalgia
Low dose naltrexone
Interestingly, small studies have evaluated the use of low dose naltrexone, an opioid antagonist, in fibromyalgia on the basis that fibromyalgia patients may have a chronically activated endogenous opioid system. It is likely that low doses of naltrexone exert an analgesic effect via antagonism of TLR4 as opposed to the opioid receptor antagonism seen at higher doses. Small studies have suggested efficacy, reporting 20–30% of patients achieving a significant pain reduction above placebo. Larger studies are required before recommendations can be made in regard to the routine use of naltrexone in the management of fibromyalgia.
NMDAR inhibitors
The N-methyl-D-aspartate receptor (NMDAR) is involved in the spinal cord and brain sensory pathway neural transmission via interaction with the neurotransmitter glutamate. As previously discussed, fibromyalgia patients have been shown to have elevated levels of glutamate in their central nervous system and CSF.
Several small studies have evaluated intravenous low dose ketamine, a non-competitive NMDAR antagonist, in patients with fibromyalgia, with around half of patients experiencing a reduction in pain intensity of more than 50%. However, duration of follow up was brief and there are no long-term data for this medication.
Memantine, another noncompetitive NMDAR inhibitor, was evaluated in a small randomized trial in fibromyalgia and was found to be more successful than placebo at reducing pain intensity by 50%, with a number needed to treat of six. Further studies of NMDAR inhibitors in fibromyalgia are required before recommendations can be made.
Dopamine agonists
Dopamine is a neurotransmitter with multiple functions, including a central role in the modulation of pain via descending inhibitory pathways. Using functional imaging, it was shown that fibromyalgia patients have abnormal dopaminergic activity, with reduced CNS release of dopamine in response to painful stimuli In a small trial, 42% of patients with fibromyalgia receiving pramipexole, a dopamine agonist, reported a 50% improvement in pain compared with 14% in placebo. However, terguride, a partial dopamine agonist, did not show any benefit. Pramipexole may also be helpful for patients with symptomatic restless leg syndrome, which is a common comorbidity with fibromyalgia. Further studies are required.
Cannabinoids
Cannabinoids are discussed as an option for management in the Canadian treatment guidelines. A recent Cochrane Review evaluated the use of cannabinoid medication in the treatment of fibromyalgia. Two studies of nabilone, a synthetic cannabinoid, were examined. Both were of very low quality and the authors concluded that there is currently no quality evidence to suggest that cannabinoids are effective for fibromyalgia symptoms.
Other experimental agents
Stress Management – Many patients with fibromyalgia have increased levels of stress and feelings of depression, anxiety, and frustration. Several treatment options are available such as cognitive behavioral therapy; including relaxation training, group therapy, and biofeedback, which are some of the useful options.rx]
Alternative Therapies – Chinese herbal medications, Chinese herbal tea, acupuncture, Tai-chi are the different modalities available but more research is required in these fields.35rx]–[rx] It has also been suggested that acupuncture triggers the release of endorphins into the blood stream and are body’s natural pain relievers.]rx]
Flupirtine is a centrally acting agent that is thought to indirectly inhibit the NMDAR by activation of the G-protein regulated inwardly rectifying potassium (GIRK) ion channel. There is evidence to suggest efficacy in acute pain, with some efficacy in fibromyalgia reported in a small case series. Melatonin, an agent typically used for sleep disturbance, has also been shown to have analgesic properties, the mechanisms of which remain incompletely understood. In several small randomized trials, melatonin was shown to be superior to placebo when used either alone or in combination with other agents in treating fibromyalgia pain and sleep disturbance.
Exercise – Exercise is highly recommended even though people with fibromyalgia may be reluctant to exercise because of their pain. Exercise is important to prevent the muscles from losing strength due to lack of use. Other benefits of regular exercise include sleep promotion, aiding digestion, increasing blood flow and improving muscle tone. It is best to start with small amounts of low impact exercise (such as walking) on a daily basis, and gradually increase this as tolerated. Physical activity can be taken in many ways, including activities such as walking, jogging or sports.[rx] Exercise is a way of responding to stress which allows the discharge of the energy the body is anticipating.[rx]
Physical and occupational therapy may help to reduce the effects of fibromyalgia on everyday life. A physical therapist can teach exercises that will improve strength, flexibility, and stamina. An occupational therapist can help make adjustments to workstations or the way that certain tasks are performed to reduce the level of stress on the body.
Rest and sleep – Rest is also important in managing fibromyalgia. People with fibromyalgia often feel exhausted after only small amounts of activity. It is often helpful, therefore, to rest regularly during the day and even during activity if it is needed. Even 5-10 minute periods of rest can be helpful. Sleep is often inadequate in quality for people with fibromyalgia. It is not advisable to use sleeping tablets unless they are absolutely necessary, and then only for brief periods of time. Some methods that may help to gain more restful sleep include avoiding alcohol and coffee in the evening, using the bedroom only for sleep (ie: not for working or eating), ensuring the room is dark when trying to sleep and having a regular time for going to bed.
Stress reduction and relaxation – Stress reduction is important as increased stress can worsen fibromyalgia symptoms. Finding methods of relaxation (such as reading or listening to music) that suit the individual with fibromyalgia can be helpful in stress reduction. Talking about the condition with friends and family can also be helpful. Some people may find it helpful to work with a professional counselor or psychologist to develop relaxation techniques and strategies to cope with the pain. A psychological technique known as Cognitive Behavioural Therapy (CBT) has been shown to help people with fibromyalgia.
Alternative therapy
Alternative therapies such as acupuncture/acupressure, homeopathy, hot and cold packs, massage therapy, yoga and tai chi, nutritional supplements and dietary modifications, herbal.
Cognitive behavioral therapy
Non-pharmacological components include cognitive-behavioral therapy (CBT), exercise and psychoeducation (specifically, sleep hygiene). CBT and related psychological and behavioral therapies have a small to moderate effect in reducing symptoms of fibromyalgia. Effect sizes tend to be small when CBT is used as a stand-alone treatment for FM patients, but these improve significantly when CBT is part of a wider multidisciplinary treatment program. The greatest benefit occurs when CBT is used along with exercise.
A 2010 systematic review of 14 studies reported that CBT improves self-efficacy or coping with pain and reduces the number of physician visits at post-treatment, but has no significant effect on pain, fatigue, sleep or health-related quality of life at post-treatment or follow-up. Depressed mood was also improved but this could not be distinguished from some risks of bias.
Mind-body therapy
Mind-body therapies focus on interactions among the brain, mind, body, and behavior. The National Centre for Complementary and Alternative Medicine defines the treatments under the holistic principle that mind-body are interconnected and through treatment, there is an improvement in psychological and physical well-being, and allow patients to have an active role in their treatment. There are several therapies such as mindfulness, movement therapy (yoga, tai chi), psychological (including CBT) and biofeedback (use of technology to give audio/visual feedback on physiological processes like heart rate). There is only weak evidence that psychological intervention is effective in the treatment of fibromyalgia and no good evidence for the benefit of other mind-body therapies
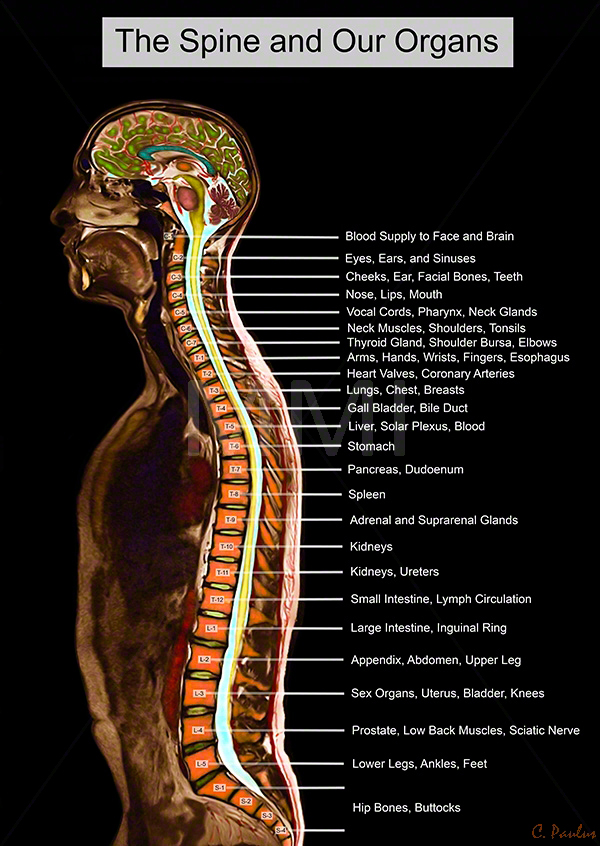
Cervical myelopathy occurs when the spinal cord is compressed. Spinal cord compression can cause neurologic symptoms – such as pain, numbness, or difficulty walking. Your spinal cord is the conduit that enables communication between your brain and body. The spinal cord begins at the base of the brain and ends at the first lumbar vertebra (L1). Below L1, the spinal cord becomes the cauda equina; a bundle of lumbar and sacral nerves.
Anatomy of Cervical Myelopathy
Your spine is made up of 24 bones, called vertebrae, that are stacked on top of one another.
The seven small vertebrae that begin at the base of the skull and form the neck comprise the cervical spine.
Other parts of your spine include
Spinal cord and nerves. The spinal cord extends from the skull to your lower back and travels through the middle part of each stacked vertebra, called the central canal. Nerves branch out from the spinal cord through openings in the vertebrae (foramen) and carry messages between the brain and muscles.
Intervertebral disks. In between your vertebrae are flexible intervertebral disks. They act as shock absorbers when you walk or run.
Intervertebral disks are flat and round and about a half inch thick. They are made up of two components:
Annulus fibrosus. This is the tough, flexible outer ring of the disk.
Nucleus pulposus. This is the soft, jelly-like center of the disk.
Animation courtesy Visual Health Solutions, Inc
About Myelopathy
More common in adults age 50 and older
Most often affects the cervical spine (neck)
Less common in the thoracic spine (mid back)
Sometimes affects the low back (eg, severe lumbar spinal stenosis)
Usually a gradual and progressive disorder
Can develop quickly (eg, trauma, injury)
Below is a lateral MRI of a patient’s cervical spine. The red arrow points to areas where the spinal cord is compressed—cervical myelopathy.
Symptoms of Cervical Myelopathy
Neck pain and stiffness
Tingling
Numbness
Weakness
Find yourself dropping things
Hand clumsiness (eg, buttoning a shirt)
Balance problems
Difficulty walking
Tingling or numbness in the arms, fingers, or hands
Weakness in the muscles of the arms, shoulders, or hands. You may have trouble grasping and holding on to items.
Imbalance and other coordination problems. You may have trouble walking or you may fall down. With myelopathy, there is no sensation of spinning, or “vertigo.” Rather, your head and eyes feel steady, but your body feels unable to follow through with what you are trying to do.
Loss of fine motor skills. You may have difficulty with handwriting, buttoning your clothes, picking up coins, or feeding yourself.
Pain or stiffness in the neck
Possible Causes
There are many different causes of myelopathy; several are listed below.
Cervical kyphosis
Cyst or tumor
Degenerative spondylosis (spinal arthritis)
Epidural abscess, infection
Herniated disc
Inflammatory diseases (eg, Rheumatoid Arthritis)
Osteophytes (bone spurs)
Spinal Stenosis
Spondylolisthesis
Vertebral body abnormality
Diagnosis of Cervical Myelopathy
The neurological exam is non-invasive and evaluates your sensory and motor functions. Sensory functions are related to your senses, such as sight, hearing, eye movement, and touch. Motor functions are related to your gait (how you walk), balance, coordination, reflexes, the range of motion, and muscle movement.
Physical Examination
After discussing your medical history and general health, your doctor will ask you about your symptoms. He or she will conduct a thorough examination of your neck, shoulders, arms, hands, and legs, looking for:
Changes in reflexes—including the presence of hyperreflexia, a condition in which reflexes are exaggerated or overactive
Numbness and weakness in the arms, hands, and fingers
Trouble walking, loss of balance, or weakness in the legs
Atrophy—a condition in which muscles deteriorate and shrink in size
Clinical Examination
The diagnosis of CSM is primarily based on the clinical signs found on physical examination and is supported by imaging findings. According to Cook et al, selected combinations of the following clinical findings are effective in ruling out and ruling in cervical spine myelopathy. Combinations of three of five or four of five of these tests enable the post-test probability of the condition to 94–99%:
gait deviation
+ve Hoffmann’s test
inverted supinator sign
+ve Babinski test
age 45 years or older
Other clinical examination tests often used for myelopathy include
Spurling’s test
Distraction test
+ve clonus/Babinski/Hoffman’s
Hyperreflexic biceps
Hyperreflexia quadriceps
Hyperreflexia achilles
Pain constancy
L’hermitte’s sign
Romberg test
Although these tests exhibit moderate to substantial reliability among skilled clinicians, they demonstrate low sensitivity and are not appropriate for ruling out myelopathy. One method used to improve the diagnostic accuracy of clinical testing is combining tests into clusters. These often overcome the inherent weakness of stand-alone tests.
These provide images of dense structures, such as bone. An x-ray will show the alignment of the vertebrae in your neck.
Magnetic resonance imaging (MRI) scans
These studies create better images of the body’s soft tissues. An MRI can show spinal cord compression and help determine whether your symptoms are caused by damage to soft tissues—such as a bulging or herniated disk.
This MRI image shows herniated disks pressing on the spinal cord (red arrows).
Computed tomography (CT) scans – More detailed that a plain x-ray, a CT scan can show narrowing of the spinal canal and can help your doctor determine whether you have developed bone spurs in your cervical spine.
Myelogram –This is a special type of CT scan. In this procedure, a contrast dye is injected into the spinal column to make the spinal cord and nerve roots show up more clearly.
In some cases, doctors use nerve conduction studies to measure how well the cervical spinal nerves work and to help specify the site of compression. Doctors commonly use a test called a nerve conduction velocity (NCV) test. During the study, a nerve is stimulated in one place and the amount of time it takes for the message or impulse to travel to a second place is measured.
Somatosensory evoked potentials (SSEPs) or motor evoked potentials (MEPs) are used to test how the spinal cord transmits nerve signals about sensory or movement information. Your doctor will place sticky patch-like electrodes on your skin that covers a spinal nerve. The NCV test may feel uncomfortable while it is performed.
Electromyography (EMG) test is often done at the same time as the NCV test. An EMG measures the impulses in the muscles to identify damage or decay. Muscles need impulses to perform movements. Your doctor will place fine needles through your skin and into the muscles that the spinal nerve controls.
Treatment of Cervical Myelopathy
Your spine specialist may recommend spine surgery. The goals of spine surgery to treat myelopathy are: (1) remove pressure from the spinal cord, (2) prevent symptoms from becoming worse, and (3) improve your condition.
Nonsurgical Treatment
In milder cases, initial treatment for CSM may be nonsurgical. The goal of nonsurgical treatment is to decrease pain and improve the patient’s ability to perform daily activities. Nonsurgical treatment options include:
Soft cervical collar – This is a padded ring that wraps around the neck and is held in place with velcro. Your doctor may advise you to wear a soft cervical collar to allow the muscles of the neck to rest and limit neck motion. A soft collar should only be worn for a short period of time since long-term wear may decrease the strength of the muscles in your neck.
Physical therapy management of Cervical Myelopathy
Patients can be treated conservatively. Kadaňka et al. found no difference in long term outcomes (2 years after the intervention) between a patient who received conservative or surgical treatment. Even after 10 years, there were no differences found between the surgery and conservative group.F ouyas et al also confirmed these findings. The only prognostic factor in which surgery can be generally recommended is with a circumferential spinal cord compression seen on an axial MRI.
The goals of physiotherapy treatment are
pain relief
to improve function
to prevent neurological deterioration
to reverse or improve neurological deficits
Cervical myelopathy can be treated symptomatically. Possible therapies include:
Ice, heat, and other modalities – Your doctor may recommend careful use of ice, heat, massage, and other local therapies to help relieve symptoms. Applying a cold pack to the painful part of the back contracts inflamed muscle and relieves pain. This treatment helps a great deal when the disk has recently ruptured and swelling is at its greatest. A heating pad or warm pack helps with residual pain.
Cervical traction and manipulation of the thoracic spine – useful for the reduction of pain scores and level of disability in patients with mild cervical myelopathy. Other signs and symptoms, such as weakness, headache, dizziness, and hypoesthesia, can also be positively affected. Cervical traction can be combined with other treatments like electrotherapy and exercises. Joghataei et al. reported a significant increase in grip strength after 10 weeks of this combined treatment
Manual therapy techniques – used to reduce the neck pain with natural apophyseal glides and sustained natural apophyseal glides for cervical extension and rotation. Manipulation and mobilizations can be effective when they are combined with exercise therapy. When you use them without exercises, there is only poor evidence that it could be effective
Exercises – the effects of exercise therapy specifically on cervical myelopathy have not been studied, but there is evidence for exercises for mechanical neck pain. For example: stretching, strengthening exercises, active range of motion exercises, home exercise programmes.
Cervical stabilization exercises – when there is anteroposterior instability of the vertebral bodies of a degenerative nature, vertebral segment stabilization of the cervical spine can be performed with a pressure biofeedback unit (PBU),
Dynamic upper and lower limb exercises – (flexion and extension) with the use of the PBU on the neck.
Proprioceptive neuromuscular facilitation – for the upper and lower limbs.
Improve posture
Motor training programmes– may improve arm and hand functioning at a function and/or activity level in cervical spinal cord injured patients.
Mobility and proprioception exercises
Aerobic exercises
Balance training – e.g. standing on one leg with eyes open and evolving to eyes closed; standing on a stable platform and evolving to an unstable platform with a rocker board
Core stability exercises –In surgical cases, the physiotherapist still has an important role, both before and after the surgery. In the pre-operative phase, the physiotherapist needs to become thoroughly familiar with the patient’s history and about their activities of daily living that they are aiming to return to. The physiotherapist will inform the patient about the treatment program and the expectations after the surgery. There are different tests to develop a thorough picture of the patient’s baseline pre-operative status such as walking tolerance, Neck Pain and Disability Scale, the Neck Disability Index and lung function. Nomura et. al found that the maximum voluntary ventilation should significantly increase after surgery
Continued Physical Activity – Though pain or weakness seem like good reasons to rest the neck, excessive bed-rest worsens the symptoms of a slipped disc in neck. Moving around too little allows muscles to grow weaker and prevents the body from healing. Periods of rest interspersed with periods of normal activity throughout the day keep the back muscles in shape.
Physical Therapy – Physical therapists show slipped disc sufferers ways to move that do not cause pain. Occupational therapists teach skills that allow patients to return to a productive life.
Nutrition – In order to restore the disc we also are going to need to include different substances in our diet. There are a lot of supplements on the market, of course. If you wish to try them, that’s fine. I personally don’t like them. I have tried one with glucosamine and chondroitin, but I didn’t feel any different. So, if you have the opportunity to take these with the food or from more natural sources, it will be great. You can find these substances in seafood and animal cartilages and by digesting them we ensure the building blocks for the connecting tissue for our joints and spine. Also, we will need more
Omega 3 fatty acids– which can be supplied from cold pressed oils, fatty fish, flax seeds, chia and many more. Vitamins from the B group are very beneficial for people with herniated discs and all kinds of issues with the peripheral nervous system. Vitamins B1, B6 and B12 nourish the nerves and help them recover from the disk accident. Usually, doctors prescribe them as a part of the treatment, but it is worth mentioning anyway.
A good massage – A massage is one of the natural methods of relieving pain. Individuals who get a massage weekly for several months stand a better chance of alleviating neck pain. A good massage provides a person with many health benefits that lessen neck pain. A massage triggers the release of endorphins. Endorphins aid in decreasing anxiety and relieving pain. They offer a relaxation effect by softening muscles that are injured preventing cramping.
Undertaking yoga– Yoga is an applicable strategy for keeping the level of back pain at minimal levels. Taking yoga sessions often is very an effective method of dealing with neck pain. With yoga, there is a high likelihood of proper body functions. The use of pain prescriptions is also diminished. Patients suffering from neck pain related issues do not have to rely on these prescriptions to manage pain. Incorporating laughter in yoga is a good way of exercising. Yoga incorporates simple yet appropriate exercises that enhance the stretching of muscles. Laughter with yoga stimulates relieving of pain. It facilitates increased uptake of oxygen, little anxiety, and production of endorphins. All these variables play an essential role in diminishing neck pain.
Adjusting sleeping position – A simple sleeping mistake can immensely contribute to neck pain. A poor sleeping position can cause stress and tension on the muscles contributing to neck pain. Altering one’s sleeping position and adopting a style that does not exert a lot of stress on the back is a recommended tactic. Nurturing sleeping habits such as assuming a reclining position, using wedge-shaped cushions and getting adjustable beds from reputable medical institutions are easy techniques to endorse. If a reclining position does not suit an individual, the other two techniques can be embraced.
Heat therapy – Several considerations should be observed when using heat therapy. The right temperature ought to be set so as to ensure a patient does not face risks associated with too much exposure to heat. The key objective should be to ensure enough access to heat to the muscles to yield benefits for the patient. The adoption of heat therapy for easing neck pain is determined by the magnitude of pain a person is experiencing. In cases where relatively low back pain is encountered, short heat therapy sessions are recommended. On the other hand, if an individual is experiencing prolonged back pain, long heat therapy sessions are the most applicable.
Taking hot baths – This is a form of heat therapy that aims at relieving neck pain. It guarantees permeation of heat into the muscles leading to reduced pain. Many individuals opt for this method since they believe it achieves competent results. Hot baths initiate a fast process of blood supply to stiff neck muscles. When this happens, the muscles relax and stretch leading to decreased pain. To avoid interference with one’s sleeping patterns, a hot bath should be taken several hours before retiring to bed.
Aquatic therapy – This natural technique involves physical therapy in a pool. Individuals get the best out of this therapy by relying on the resistance of water. Consistency in undertaking this therapy is what ascertains getting back pain relief. Integrating aquatic therapy in an individual’s life for the better part of the week enhances the reduction of back pain quickly.
Enlighten others – Individuals have the power to devise their own natural strategies that aid them in coping with back pain. The strategies can also be a good remedy for others going through similar circumstances. An individual can use social media platforms to equip others with important tips on how to keep back pain at bay. Further, becoming a member of associations that address back pain issues enables better communication of the knowledge gained from personal experience.
Medications of Cervical Myelopathy
In some cases, medications can help improve your symptoms.
Analgesics – Prescription-strength drugs that relieve pain but not inflammation.
Antidepressants: A Drugs that block pain messages from your brain and boost the effects of endorphins (your body’s natural painkillers).
Corticosteroid injections – Your doctor will inject a steroid such as prednisone into your back or neck. Steroids make inflammation go down. However, because of side effects, they are used sparingly.
Anesthetics – Used with precision, an injection of a “nerve block” can stop the ain for a time.
Muscle Relaxants – These medications provide relief from spinal muscle spasms.
Skeletal muscle relaxers– may also be used. Their short term use has been shown to be effective in the relief of acute back pain. However, the evidence of this effect has been disputed, and these medications do have negative side-effects.
Antibiotic –to the management of bowel & bladders control and protect further infection. Infection causes should be treated with appropriate antibiotic therapy
Topical Medications – These prescription-strength creams, gels, ointments, patches, and sprays help relieve pain and inflammation through the skin.
Glucosamine & diacerine – can be used to tightening the loose tension and regenerate cartilage or inhabit the further degeneration of cartilage.
Corticosteroid – to healing the nerve inflammation and clotted blood in the joints.
Dietary supplement-to remove the general weakness & improved the health.
Amitriptyline – If pain persists for more than a month, and has not responded to the above painkillers, your GP may prescribe a medicine called amitriptyline. Amitriptyline was originally designed to treat depression, but doctors have found that a small dose is also useful in treating nerve pain. You may experience some side effects when taking amitriptyline.
Lesion debulking – is required for space-occupying lesions – eg, tumors, abscess.
If surgery cannot be performed – radiotherapy may relieve cord compression caused by malignant disease.
Radiation therapy and Chemotherapy – may have a role in treatment if the cauda equina syndrome is caused by a tumor.
Support or brace – A pelvic belt can be used to stabilize a joint that is too loose until the inflammation and pain subside.
Joint injections– Numbing injections into the sacroiliac joint are used diagnostically to help identify the cause of them but are also useful in providing immediate pain relief. Typically, an anesthetic is injected along with an anti-inflammatory medication.
Cervical epidural block – In this procedure, steroid and anesthetic medicine is injected into space next to the covering of the spinal cord (“epidural” space). This procedure is typically used for neck and/or arm pain that may be due to a cervical disk herniation, also known as radiculopathy or a “pinched nerve.”
Cervical facet joint block – In this procedure, steroid and anesthetic medicine is injected into the capsule of the facet joint. The facet joints are situated at the back of the neck and stability and movement. Arthritis may be formed and will play a part to neck pain.
Medial branch block and radiofrequency ablation – This procedure is usually done for some chronic neck pain It can be used for both diagnosis and treatment of a potentially painful joint.
Although people sometimes turn to chiropractic manipulation for neck and back pain, manipulation should never be used for spinal cord compression.
Other Treatment Options
Other treatment options – may be useful in certain patients, depending on the underlying cause of the CES
Patients with spinal neoplasms should be evaluated for chemotherapy and radiation therapy.
Weakness – Physiotherapy may be helpful if there is no inflammatory component such as that found in arachnoiditis where exercise might exacerbate the condition and cause flare-ups.
Sensory Loss – Little conventional treatment exists for sensory loss in cauda Equina syndrome, although in conditions such as Multiple Sclerosis use of vitamin B complex is considered to have potential beneficial effects.
Sore Feet – Loss of muscle tone and control over the movement of the foot may lead to foot pain. If foot drop is a notable issue, a brace to hold it in position may help. It is important; however, to attempt to maintain as much muscle tone as possible as well as the range of movement (ROM). Exercises might help.
Sexual Dysfunction –Sexual dysfunction is very hard for people to talk about at times. It might be best to pursue advice from specialists. If no physical treatment is feasible for improving function, the person and their sexual partner might pursue counseling which might help to lessen the impact of this disability on not only the person affected but their partner.
Depression– Depression is an understandable reaction to a form of debilitating illness. Antidepressant medication should be reserved for severe depression. Counseling and support are the preferred methods of managing depression. Sharing experiences may help people with Cauda equina syndrome to come to terms with the disabilities associated with Cauda Equina syndrome.
Poor Circulation – Poor circulation is a common issue in Cauda Equina syndrome. The person’s feet may be cold and turn white, then red when re-warmed (also known as, ‘Raynaud’s syndrome,) as well as chilblains. Some medications exist that can be taken, yet it is most likely best to use general measures such as avoiding getting cold feet and foot massage with warm oil to help improve the person’s circulation. Avoid extremely hot baths after the feet have been cold because it will most likely cause chilblains.
Postoperative care – includes addressing lifestyle issues (eg, obesity), and also physiotherapy and occupational therapy, depending on residual lower limb dysfunction.
Prolotherapy – the practice of injecting solutions into joints (or other areas) to cause inflammation and thereby stimulate the body’s healing response – has not been found to be effective by itself, although it may be helpful when added to another therapy.
Herbal medicines – as a whole, are poorly supported by evidence. The herbal treatments Devil’s claw and white willow may reduce the number of individuals reporting high levels of pain; however, for those taking pain relievers, this difference is not significant. Capsicum, in the form of either a gel or a plaster cast, has been found to reduce pain and increase function.
Behavioral therapy – may be useful for chronic pain. There are several types available, including operant conditioning, which uses reinforcement to reduce undesirable behaviors and increase desirable behaviors;
Cognitive behavioral therapy– which helps people identify and correct negative thinking and behavior; and respondent conditioning, which can modify an individual’s physiological response to pain. Medical providers may develop an integrated program of behavioral therapies. The evidence is inconclusive as to whether mindfulness-based stress reduction reduces chronic back pain intensity or associated disability, although it suggests that it may be useful in improving the acceptance of existing pain.
Tentative evidence supports neuroreflexotherapy (NRT) – in which small pieces of metal are placed just under the skin of the ear and back, for non-specific low back pain
Surgery of Cervical Myelopathy
If nonsurgical treatment does not relieve your symptoms, your doctor will talk with you about whether you would benefit from surgery. The majority of patients with symptoms and tests consistent with CSM are recommended to have surgery.There are several procedures that can be performed to help relieve pressure on the spinal cord. The procedure your doctor recommends will depend on many factors, including what symptoms you are experiencing and the levels of the spinal cord that are involved.
Scoliosis is a medical condition in which a person’s spine has a sideways curve. The curve is usually “S”or “C”-shaped. In some the degree of curve is stable while in others, it increases over time. Mild scoliosis does not typically cause problems, while severe cases can interfere with breathing. Typically, no pain is present. The cause of most cases is unknown, but is believed to involve a combination of genetic and environmental factors. Risk factors include other affected family members. It can also occur due to another condition such as muscles spasms, cerebral palsy, Marfan syndrome, and tumors such as neurofibromatosis.
According to the American Association of Neurological Surgeons (AANS), scoliosis affects between 2% and 3% of the American population, or about six to nine million people. It is characterized by an abnormal lateral curvature of the spine and there are many different forms. The various types of scoliosis are classified by cause and age of onset; the speed and mechanism of progression also plays a role in determining the specific type of scoliosis.
Though all forms of scoliosis involve some degree of spinal curvature, some are more severe than others.
Types of Scoliosis
Classification of scoliosis.
Congenital – Failure of formation,Failure of segmentation
Scoliosis is classified according to the patient’s age at the time of diagnosis, as follows:
infantile (under age 3),
juvenile (age 3 to 9), and
adolescent scoliosis (age 10 to 18).
There are a number of ways to differentiate between the various forms of scoliosis, but the most common method for classification is based on etiology, or the underlying cause for the condition. There are three categories into which the different forms of scoliosis fit: idiopathic, congenital, and neuromuscular.
www.rxharun.com
Most types of scoliosis are idiopathic, which means that the cause is unknown or that there is no single factor that contributes to the development of the disease.
Congenital – forms of scoliosis typically result from a spinal defect present at birth, and are therefore usually detected at an earlier age than idiopathic forms of scoliosis.
Neuromuscular – scoliosis is spinal curvature that develops secondary to some kind of neurological or muscular disease, such as muscular dystrophy or cerebral palsy. This form of scoliosis tends to progress much more quickly than others.
Knowing how spinal curvature disorders are classified provides a foundation of knowledge on which to build understanding of the specific types of scoliosis.
Congenital Scoliosis
Congenital scoliosis is fairly rare, affecting only 1 in 10,000 newborns, and it results from spinal abnormalities that develop in the womb. During fetal development, malformation of the vertebrae is one of the most common causes for congenital scoliosis. It may also result from partial formation of certain bones or the absence of one or more bones in the spine. Not only can congenital scoliosis lead to a sideways curvature of the spine, it can cause the child to develop additional curves in the opposite direction – the body’s attempt to compensate for the abnormality.Because congenital scoliosis is related to spinal defects present at birth, it is typically diagnosed much earlier than other forms of the disease.
Symptoms of congenital scoliosis include tilted shoulders, an uneven waistline, a prominence of the ribs on one side, head tilt, and an overall appearance of the body leaning to one side. When symptoms develop, diagnostic tests such as EOS imaging, x-rays, MRIs, and CT scans can be used to confirm the diagnosis.
Early Onset Scoliosis
www.rxharun.com
The most common age range at which scoliosis is diagnosed is during adolescence – which is why it is called adolescent scoliosis. When scoliosis is present prior to the age of 10, however, it is referred to as early onset scoliosis.
It is important to differentiate between adolescent and early onset scoliosis because children over the age of 10 have already completed most of their spinal growth while children under 10 are still growing. Because children under 10 are still growing, early onset scoliosis can affect more than just the spine – it can also lead to malformed ribs, which can affect lung development.
In many cases, children with early onset scoliosis do not show any outward signs of spinal problems, especially if the curve is mild. In order to detect early onset scoliosis, it is important to pay attention to the symmetry of the affected child’s body. Uneven shoulders, asymmetric contour of the waist, uneven hips, tilted head, and leaning can all be signs of scoliosis in children under the age of 10. Upon diagnosis, treatment for this form of scoliosis is more important than for other forms of scoliosis because the child is still developing. Lack of treatment can contribute to lung and heart problems and may even increase the risk of death due to lung and heart disease.
Adolescent Idiopathic Scoliosis
By far the most common form of scoliosis, adolescent idiopathic scoliosis affects as many as 4 out of 100 children between the ages of 10 and 18. The name for this condition comes from the age of onset (adolescence) and the fact that no single cause has been identified.
Idiopathic scoliosis is classified according to the age of the patient at the time of diagnosis. On the basis of the notion that three growth spurts correspond to the phases of highest risk for worsening of scoliosis, the condition is subdivided into three types:
infantile scoliosis (under age 3),
juvenile scoliosis (ages 3 to 9), and
adolescent scoliosis (ages 10 to 18).
By the age of 10, spinal growth has started to slow; if the child has already developed a significant degree of spinal curvature by this point, the curve may continue to progress into adulthood.
There are a number of theories regarding the cause of adolescent idiopathic scoliosis, which range from hormonal imbalances to asymmetric growth. About 30% of all adolescent idiopathic scoliosis patients have a family history of scoliosis, which suggests a genetic link. In most cases, adolescent idiopathic scoliosis patients do not experience any pain or neurologic abnormalities – they may even look normal when viewed from the side. When symptoms do develop, they typically take the form of uneven shoulders, a rib hump, or a leaning torso. This form of scoliosis is also sometimes correlated with lower back pain.
While curve progression may naturally slow as the child reaches skeletal maturity , ScoliSMART Clinics highly recommends muscle retraining through Early Stage Scoliosis Intervention (ESSI) as soon as a curve is detected.
www.rxharun.com
Degenerative Scoliosis (De Novo Scoliosis)
Also known as adult onset scoliosis, late onset scoliosis, or de novo scoliosis, degenerative scoliosis is characterized by a sideways curvature of the spine that develops slowly over time. One of the natural consequences of aging is degeneration of the joints and discs in the spine. (In younger individuals, facet joints function like hinges, helping the spine to bend in a smooth motion with intervertebral discs to cushion the individual bones.) Uneven degradation of these discs and joints can cause spinal curvature to become more pronounced on one side – a hallmark of scoliosis.
Degenerative scoliosis most commonly develops in the lumbar spine, or the lower back, and it forms a slight C-shape. When the degree of sideways curvature exceeds 10 degrees (as measured by the Cobb angle), it is diagnosed as scoliosis. Although many forms of scoliosis are not painful, degenerative scoliosis certainly can be. Common symptoms include a dull ache or stiffness in the lower back, a radiating pain that spreads to the legs, a tingling sensation that runs down the leg, or a sharp pain in the leg that occurs while walking but subsides during periods of rest.
A recent study suggests that more than 60% of the adult population over the age of 60 has some degree of degenerative scoliosis.
De novo scoliosis is directly caused by age-related degeneration of the spine and occurs in adult patients who have no prior history of scoliosis. It is most commonly diagnosed in people over the age of 50 and it can be diagnosed through physical examination and x-rays. Patients with de novo scoliosis frequently complain of muscle fatigue and lower back pain, as well as stiffness and leg symptoms such as numbness or weakness. Over time, patients often develop poor posture and loss of balance, but treatment is tricky because there are increased risks associated with surgery in older individuals.
Neuromuscular Scoliosis
Technically a type of idiopathic scoliosis, neuromuscular scoliosis develops secondary to various disorders of the spinal cord, brain, and muscular system. Spinal curvature occurs when the nerves and muscles are unable to maintain the proper alignment and balance of the spine and trunk. This curvature is likely to progress into adulthood and may become increasingly severe in patients who are unable to walk. Patients who are confined to wheelchairs may have trouble sitting upright and may have a tendency to slump to one side.
Some of the underlying conditions known to contribute to neuromuscular scoliosis include myelodysplasia, cerebral palsy, Duchenne muscular dystrophy, Freidrich ataxia, and spinal muscular atrophy. Symptoms associated with neuromuscular scoliosis are typically not painful unless the spinal curvature becomes very pronounced. In many cases, the first sign of scoliosis is a change in posture – either leaning forward or leaning to one side while standing or sitting. Diagnosis can be confirmed through clinical exam and full spinal x-rays, which typically show a long, C-shaped curvature that affects the entirety of the spine.
Spine Anatomy for Scoliosis
To understand scoliosis, you first need to know what a healthy spine looks like. There are four regions in your spine
Cervical spine – This is your neck, which begins at the base of your skull. It contains seven small spinal bones (called vertebrae), which doctors label C1 to C7 (the “C” means cervical). The numbers one to seven indicate the level of the vertebrae. C1 is closest to your skull, while C7 is closest to your chest.
Thoracic spine – Your mid-back has 12 vertebrae that are labeled T1 to T12 (the “T” means thoracic). Vertebrae in your thoracic spine connect to your ribs, making this part of your spine relatively stiff and stable. Your thoracic spine doesn’t move as much as the other regions of your spine.
Lumbar spine– In your low back, you have five vertebrae that are labeled L1 to L5 (the “L” means lumbar). These vertebrae are your largest and strongest vertebrae, responsible for carrying a lot of your body’s weight. The lumbar vertebrae are also your last “true” vertebrae; down from this region, your vertebrae are fused. In fact, L5 may even be fused with part of your sacrum.
Sacrum and coccyx – The sacrum has five vertebrae that usually fuse by adulthood to form one bone. The coccyx—commonly known as your tail bone—has four (but sometimes five) fused vertebrae.
Normal Spinal Curves of Scoliosis
Lordosis and Kyphosis – When viewed from the side, you can see the spine has both inward and outward curves. These curves help your back carry your weight and are also important for flexibility.
There are two types of normal curves in your spine, and they are called kyphosis and lordosis. Kyphosis means the spine curves inward, and lordosis means the spine curves outward. There are two kyphotic and two lordotic spinal curves in a normal spine. Your cervical and lumbar spines each have a lordotic curve. Your thoracic spine and sacrum have kyphotic curves. While kyphosis and lordosis refer to a healthy curvature in your spine, they also describe abnormal spinal curves that are different than scoliosis. Abnormal lordosis is an extreme inward spinal curve.
Scheuermann’s Kyphosis
Whereas scoliosis is defined as an abnormal curvature of the spine when viewed from the front, kyphosis is a forward rounding of the spine. Scoliosis most frequently affects the lower spine, or lumbar spine, while kyphosis usually affects the cervical spine and thoracic spine. Scheuermann’s kyphosis is one of three types of kyphosis and it is typically diagnosed during adolescence. It develops secondary to some structural deformity in the vertebrae and early symptoms include poor posture, back pain, muscle fatigue, and stiffness in the back. In most cases, these symptoms remain fairly consistent and they generally do not worsen over time except in severe cases.
Syndromic Scoliosis
As the name suggests, syndromic scoliosis is a form of scoliosis that develops secondary to some kind of syndrome. Some of the syndromes that are most commonly linked to syndromic scoliosis include Rett’s syndrome, Beale’s syndrome, muscular dystrophy, osteochondral dystrophy, and various connective tissue disorders. Because this condition can be linked to many different disorders, its symptoms are highly variable. Though symptoms are not typically painful, they can cause discomfort or pain with sitting when they are severe. Because the connection between various disorders and syndromic scoliosis is well-known, children who develop these disorders can be screened for scoliosis at an early age.
Causes of Scoliosis
Below are some of the possible causes of scoliosis
Congenital scoliosis (present at birth) – this is rare and occurs because the bones in the spine developed abnormally when the fetus was growing inside the mother.
Specific genes – at least one gene is thought to be involved in scoliosis.
Leg length – if one leg is longer than the other, the individual may develop scoliosis.
Syndromic scoliosis – scoliosis can develop as part of another disease, including neurofibromatosis and Marfan’s syndrome.
Osteoporosis – can cause secondary scoliosis due to bone degeneration.
Other causes – bad posture, carrying backpacks or satchels, connective tissue disorders, and some injuries.
Secondary causes of scoliosis and relevant symptoms.
Neuologic Disorders
Sign and Symptoms
Syringomyelia
Tethered cord syndrome
Spinal tumor
Weakness, sensory changes, problems of balance, gait and coordination, as well as bowel and bladder difficulties such as incontinence
Neurofibromatosis
café-au-lait spots or axillary freckles
Friedreich’s ataxia
Gait disturbance to speech problems. Heart disease and diabetes
Familial dysautonomia (Riley-Day syndrome)
Insensitivity to pain, instability to produce tears, poor growth and labile blood pressure
Werdnig-Hoffmann disease
Inefficiency of respiratory system – and pneumonia-induced respiratory failure
Duchenne muscular dystrophy
Progressive proximal muscle weakness of the legs and pelvis associated with a loss of muscle mass
Cerebral palsy
Spasticities, spasms, unsteady gait, problems with balance and decreased muscle mass
Poliomyelitis
Flaccid paralysis in one or more limbs with decreased or absent tendon reflexes, without sensory or cognitive loss.
Charcot-Marie-Tooth disease
High- arched or cavus feet
Connective Tissue Disorders
Ehlers-Danlos Syndrome
Marked ligamentous hyperlaxity and or skin elasticity
Marfan syndrome
Tall, long fingers, increased arm span to height ratio and cardiac abnormalities
Homocystinuria
Family history, seizures, Marfanoid habitus, seizures and mental retardation
Musculoskeletal
Leg length discrepancy
Previous injury/fractures
Developmental dysplasia of the hip
Family history, positive Ortolani and Barlow tests
Osteogenesis imperfecta
Family history, multiple fractures, loose joints and respiratiory problems
Klippel-Feil syndrome
Spina bifida, cleft palate, short stature and cardiorespiratory problems
Resulting from other conditions
Secondary scoliosis due to neuropathic and myopathic conditions can lead to a loss of muscular support for the spinal column so that the spinal column is pulled in abnormal directions. Some conditions which may cause secondary scoliosis include muscular dystrophy, spinal muscular atrophy, poliomyelitis, cerebral palsy, spinal cord trauma, and myotonia. Scoliosis often presents itself, or worsens, during an adolescent’s growth spurt and is more often diagnosed in females than males.
Scoliosis associated with known syndromes is often subclassified as “syndromic scoliosis”. Scoliosis can be associated with amniotic band syndrome,
A 20th-century illustration of a severe case of a “S” shaped scoliosis
Symptoms associated with scoliosis can include:
Pain in the back, shoulders, and neck and buttock pain nearest the bottom of the back
Respiratory and/or cardiac problems in severe cases
Constipation due to curvature causing “tightening” of stomach, intestines, etc.
Limited mobility secondary to pain or functional limitation in adults
Painful menstruation
Uneven musculature on one side of the spine
Rib prominence or a prominent shoulder blade, caused by rotation of the rib cage in thoracic scoliosis
Uneven hips, arms, or leg lengths
Slow nerve action
Heart and lung problems in severe cases
Calcium deposits in the cartilage endplate and sometimes in the disc itself
Recent longitudinal studies reveal that the most common form of the condition, late-onset idiopathic scoliosis, causes little physical impairment other than back pain and cosmetic concerns, even when untreated, with mortality rates similar to the general population. Older beliefs that untreated idiopathic scoliosis necessarily progresses into severe (cardiopulmonary) disability by old age have been refuted by later studies.
Diagnosis of Scoliosis
Physical Examination
The standard screening test for scoliosis is the “Adam’s forward bend test.” During the test, your child will bend forward with feet together, knees straight and arms hanging free. Your doctor will observe your child from the back, looking for a difference in the shape of the ribs on each side. A spinal deformity is most noticeable in this position.
The person’s gait is assessed, with an exam for signs of other abnormalities (e.g., spina bifida as evidenced by a dimple, hairy patch, lipoma, or hemangioma). A thorough neurological examination is also performed, the skin for café au lait spots, indicative of neurofibromatosis, the feet for cavovarus deformity, abdominal reflexes and muscle tone for spasticity.
When a person can cooperate, he or she is asked to bend forward as far as possible. This is known as the Adams forward bend test and is often performed on school students. If a prominence is noted, then scoliosis is a possibility and an X-ray may be done to confirm the diagnosis.
A medical history – in which you answer questions about your health, symptoms, and activity.
A physical exam to assess your strength – reflexes, sensation, stability, alignment, and motion. You may also need blood tests.
A myelogram – an X-ray of the spinal canal after injection of contrast material which can pinpoint pressure on the spinal cord or nerves.
X-rays – will provide clear images of the bones in your child’s spine. They allow your doctor to see the exact location of the curve and to measure how severe it is. In general, curves greater than 25° are considered serious enough to require treatment.
Urodynamic studies – may be required to monitor recovery of bladder function following decompression surgery.
Imaging scans– If there are further symptoms, such as back pain, or if symptoms are severe, an MRI or CT scan may be ordered.
As an alternative, a scoliometer may be used to diagnose the condition – When scoliosis is suspected, weight-bearing, full-spine AP/coronal (front-back view) and lateral/sagittal (side view) X-rays are usually taken to assess the scoliosis curves and the kyphosis and lordosis, as these can also be affected in individuals with scoliosis. Full-length standing spine X-rays are the standard method for evaluating the severity and progression of scoliosis, and whether it is congenital or idiopathic in nature. In growing individuals, serial radiographs are obtained at 3- to 12-month intervals to follow curve progression, and, in some instances, MRI investigation is warranted to look at the spinal cord.
The standard method for assessing the curvature quantitatively is measuring the Cobb angle, which is the angle between two lines, drawn perpendicular to the upper endplate of the uppermost vertebra involved and the lower endplate of the lowest vertebra involved. For people with two curves, Cobb angles are followed for both curves. In some people, lateral-bending X-rays are obtained to assess the flexibility of the curves or the primary and compensatory curves.
Treatment of Scoliosis
Treatment options for idiopathic scoliosis could include
Observation – Typically, a doctor will advise observation for a scoliosis curve that has not yet reached 25 degrees. Every 4 to 6 months, the doctor will take another X-ray of the spine to see if the scoliosis is progressing or not.
Bracing – If scoliosis has progressed past 20 or 25 degrees, a back brace could be prescribed to be worn until the adolescent has reached full skeletal maturity. The goal of bracing is to prevent the curve from getting worse and to avoid surgery.
Thoracolumbosacral orthosis (TLSO) – the TLSO is made of plastic and designed to fit neatly around the body’s curves. It is not usually visible under clothing.
Milwaukee brace – this is a full-torso brace and has a neck ring with rests for the chin and the back of the head. This type of brace is only used when the TLSO is not possible or not effective
If the curve continues to progress despite bracing, surgery could be considered. The most common surgical option for scoliosis today is a posterior spinal fusion, which can offer better corrections with fewer fusion levels (preserving more back mobility) than what was done in years past.
Braces used for scoliosis
Bracing – For curves between 25 and 45 degrees below the level of T8 in general, and there is a risk of curve progression. Bracing should be considered so that the curve does not progress with time. In past braces were uncomfortable and embarrassing. Now thoracolumbar braces come in a variety of shapes, size, and padding (Milwaukee brace, Boston brace and the Charleston brace). A meta-analysis by Row et al. [rx] has shown a 93% success rate for bracing 23 hours per day. Although bracing has been shown to be effective, compliance is poor and it is associated with psychological stress [rx]. It is important to counsel adolescents and their parents that bracing does not correct scoliosis but may prevent significant progression of the spinal curvature. Use of a brace is continued until the patient reaches Risser grade 4 or 5. Although bracing is moderately successful, its efficacy is not fully proven due to lack of strong evidence [rx].
Actually, 25 papers were found on this topic. It should be emphasized that the aim of this article was only to introduce the orthoses not to compare their performances. As can be seen from [rx], the spinal orthoses can be divided into rigid and soft orthoses based on the structure of the orthosis.
Milwaukee brace
One of the commonly used high profile orthoses is Milwaukee orthosis. This is the first modern orthosis designed to treat spinal deformities. It was developed by Blount and Schmidt for postoperative treatment of postpolio scoliosis.[rx]
This orthosis consists of pelvic section (which is mainly made from plastic), anterior and posterior uprights, and neck ring with throat mold anteriorly and occipital pads posteriorly. It is used mostly for the patients with apex of curve above T8.[rx] Another types of braces used for scoliosis are TLSOs which were first applied by Watts team for the patients with progressive AIS and curve apex below T8.[rx]
Boston brace
Actually, it is the most common used braces in North America, which was developed by John Hall and William Miller at Boston children Hospital in 1972.
Now, this brace is produced commercially in six different sizes to reduce manufacturing time and cost. This is a posterior opening TLSO which passively correct the scoliotic curve.[rx]
Cheneau brace
This brace was introduced by Dr. Jacques Chenean in the sixth decade. However, officially was presented in 1979 in Bratislava. It has been shown that this orthosis has two mechanisms of actions including active and passive.
Although the aim of orthotic treatment of scoliosis is curve progression control, Cheneau brace seems to correct the curvatures in some cases.[rx]
Rigo Cheneau brace
This brace was developed by Rigo Manuel in the early 90s. This brace is mostly recommended for the patients with mild to moderate juvenile scoliosis. It is based on concept of equilibrium at L4/L5 level.[rx]
The Cobb angle correction of the main curvature is considered to be set at 53.7%. However, in the patients with a single long dorsal curvature, the curve correction is set at 76.7% and 55% in axial rotation cases.[rx]
Cheneau light brace
This brace was developed by Hans-Rudolf Weiss in 2005 to solve the problems of the previous designs.[rx] The design of this orthosis was based to make the orthosis available immediately and to make its adjustment and modifications very easily.[rx]
Gensingen brace
This brace was also developed by Weiss, which is based on Cheneau light brace.[rx] It is based on computer-aided design/computer-aided manufacturing technology (CAD-CAM).
This is used mostly for the curvature exceeding 50°, which cannot be managed by other orthoses.[rx]
Cheneau-Toulouse-Munster brace
This brace is actually a TLSO with front opening. It applies specific pressure on torso to modify scoliotic curve and to prevent curve progression. It is recommended to use this orthosis particularly at night for low curvature (Cobb angle <30).[rx]
Triac brace
In contrast to other previous orthoses, this brace provides a dynamic correction force to correct scoliosis. Due to the location of the hinge section of the orthosis, this orthosis can be only used for curve below T11.[rx]
The name of Triac comes from three C’s including comfort, control, and cosmesis. The main point of the design of this orthosis was that the brace follows the motion of the patients. The interesting point regarding this orthosis is that the immediate correction of 22% can be achieved for primary curve and 35% for the secondary curve.[rx]
C-brace
Actually, this brace acts on single curve deformity and the design of the brace allows trunk movement, and hence, patients have more comfort while wearing the brace.[rx]
Scoliosis Lycra orthosis
This orthosis is used for the patients with neurological scoliosis. In this orthosis, a simple panel was added on the convex side of the brace to decrease the progression of the curve. Use of this orthosis is mostly recommended for the patients with cerebral palsy.[rx]
SpineCor orthosis
Actually, this is a dynamic orthosis which was developed in 1992–1993. The design of this orthosis is based on active biofeedback mechanism. The effectiveness of the SpineCor brace has been recommended for mild and moderate curves.[rx]
Charleston brace
This is a custom-molded spinal orthosis which holds the patients in overcorrected position. This brace seems to alter the natural history in retrospective studies with 5–10 h wearing time.[rx]
Long lever scoliosis brace
This orthosis was designed to treat large translational displacement associated with idiopathic scoliosis. The amount of the force required to stabilize the scoliosis curve decreases follow the use of long lever arm system.[rx]
Providence brace
This is also an orthosis which can be used during night. This brace puts the spine in an overcorrected position by application of the opposing forces. It is designed especially for curvature abnormalities.[rx]
Sforzesco brace
This brace was named in honor of the Medieval Sferza family in 2004 to avoid casting procedure, especially for the worst patients based on SPoRT (symmetric patient-oriented, rigid three-dimensional, active) concept of bracing.
It is constructed from polycarbonate in two pieces which connected in anterior and posterior sides by a closure and a vertical aluminum bar, respectively.[rx]
Lapadula brace
This has the same structure as Sforzesco brace which is made from polycarbonate. The only difference was that Lapadula brace does not have the upper plastic part over the breast. It is also recommended to be used for the patients with hyperkyphosis and scoliosis.[rx]
Sibilla brace
This orthosis has the same structure as Lapadula brace and also made from polycarbonate sheet.[rx]
Dynamic derotational brace
This orthosis was designed and used by surgeon and spine unit of KAT orthopedic Hospital in Athens, with collaboration of Mr Nikolas Vastatzidis of Athen.[rx] Actually, this is a modification of Boston limited pressure, with addition of a system of light and slightly flexible blades made of aluminum. The results of the study of this brace showed that the brace not only restrict the progression of the curve but also correct it. It can be produced based on traditional cast method or use of CAD/CAM technology.[rx]
Progressive Action Short Brace
It is a custom-made TLSO introduced by Dr. Lorenzo Aulisa at Institute of orthopedic Catholic University. The brace is based on principle that constrained spines can achieve the correction through the use of inverting the abnormal loads distribution during growth.[rx]
Spinealite soft brace
This orthosis is also called CMCR brace (Correct Monocoque Carbone respectant la Respiration). This monoshell brace was developed by Lecanto society at the center des Massues in Lyon, in 1997. The pads of the brace in contrast to the pads of Lyon are mobile and more comfortable. This is a light brace reinforced by carbon blades and implemented without prior casting.[rx]
ART brace
Actually, after the development of CAD/CAM modeling, most of the braces have been developed by use of this system. In 2013, the new generation software (OrthenShape) allowed the overlay of different CAD/CAM modulus.
The brace which was produced by the use of this technology, based on Lyon approach, is called ART brace. ART is the acronym for asymmetrical, rigid, torsion brace. The name was created by Stefano Negrini, the inventor of Sforzesco brace.[rx]
Lyon brace
Actually, Lyon brace created in 1947 by Pierre Stagnara to be adjustable, active, decompressive, symmetrical, stable, and transparent. It is possible to adjust the orthosis up to 7 cm of growth. It was made of polymethyl methacrylate which is transparent to monitor the skin conditions.[rx]
The design of this brace is based on stretching of the ligaments of the spine to a certain point for a prolonged period by the use of plaster cast for 4 weeks. After that, the brace can be used especially during night to maintain viscoelastic level of the structure.
The indication of use of this orthosis is the same as other orthoses. However, it is recommended to not be used for juvenile and infantile scoliosis to avoid a tubular thorax and also for those with sever thoracic lordosis for whom the treatment is mostly surgical.[rx] It is also recommended to not be used for those with major psychological reactions and those with nonacceptation of the plaster cast.
Wilmington brace
This brace was designed by G Dean Mac Even to improve patients’ compliance by making the brace less bulky and light weight compared to other braces. Actually, it is a custom-made TLSO orthosis from orthoplast.
The design of this orthosis is the same as body jacket with an anterior opening. There are some adjustable straps to secure the orthosis. It is recommended to wear the orthosis as full time (23 h per day).[rx]
It should also be emphasized that the scoliotic brace can be categorized into soft and rigid orthoses. Figure [rx] shows the classification of the braces based on structure. It is also possible to classify the scoliosis brace based on the time of wear.
Exercise
Another type of conservative treatment which is recommended for scoliotic patients is exercise. Beside of the routinely used exercise for scoliosis, some especial approaches have prescript for the patients with scoliosis which can be mentioned as following.
Functional individual therapy of scoliosis
It is based on inclusion of many elements selected from variety of therapeutic approaches that have been adapted from a different treatment concepts.[rx] This method was created in Poland, which was aimed to improve postural problems and scoliosis.
Actually, this is a method of diagnosis and therapy for idiopathic scoliosis. It can be used to correct scoliosis, a supportive therapy to bracing, preparation of children for surgery, and may be used after surgery to correct shoulder and pelvic girdles.[rx]
SpineCore method
It is a postural reeducation method which consists of combinations of corrective movement and global muscles rebalance exercise.[rx]
The Lyon approach
Lyon approach is a method of physical therapy which is used in combination with Lyon brace. Three main parameters are considered with this approach including patient age, postural imbalance, and Cobb angle.[rx]
Dobomed physical therapy approach
It should be emphasized that this method was also developed in Poland that addresses both trunk deformity as well as respiratory function impairment. This method requires a high degree of patient cooperation. Therefore, it is not recommended for children.[rx]
Barcelona scoliosis physical therapy
This method of treatment is based on this assumption that scoliosis posture and soft tissue imbalance promote curve progression. Actually this is physical therapy method which can be defined as a therapy plane of cognitive, sensory motor, and kinesthetic training.[rx]
Scientific exercise approach to scoliosis
As can be understood from the title, this approach is based on scientific principles. This is an extension of Lyon approach which is based on four principles including improving the patient’s awareness of their deformity, autonomous correction by the patients, use of exercise to stimulate a balanced reaction, and use of in brace scoliosis specific exercise.[rx]
Schroth method
Actually, this method was developed in Germany in 1927 by Katrina Schroth. This is a method to correct the scoliosis in three dimensions. It was aimed to reduce the incidence of scoliosis progression, reduce postural rotation, improve mobility, improve postural stability, reduce pain, and improve cardiopulmonatory function in scoliosis.[Rx]
There are some evidences in the literature regarding the effects of these exercises on scoliosis correction. Footwear, wedge, and insoles are the other conservative approaches used for the patients with scoliosis. This is based on this theory that incongruity of pelvis, especially sacroiliac joint, can induce deformation of lower extremity which finally lead to scoliosis.[rx] However, there is no evidence regarding the effectiveness of this method.
Functional electrical stimulation
Although the development of this method returned to around 1980, it seems to be ineffective in treatment of scoliosis. At present, the results of some studies showed that if FES combine with other exercise or brace, it may be more effective.[rx]
Acupuncture
Actually, sharp and sensitive needles are used to stimulate a certain part of body. It used most often in Chinese medicine also for scoliosis and to reduce the pain associated with low back pain. Based on the available literature, it is too difficult to reach a strong conclusion regarding the effects of acupuncture on scoliosis.[rx]
Scoliosis surgery (spinal fusion)
In severe cases, scoliosis can progress over time. In these cases, the physician may recommend spinal fusion. This surgery reduces the curve of the spine and stops it from getting worse.
Scoliosis surgery involves the following
Bone grafts – two or more vertebrae (spine bones) are connected with new bone grafts. Sometimes, metal rods, hooks, screws, or wires are used to hold a part of the spine straight while the bone heals.
Intensive care – the operation lasts 4-8 hours. After surgery, the child is transferred to an ICU (intensive care unit) where they will be given intravenous fluid and pain relief. In most cases, the child will leave the ICU within 24 hours but may have to remain in the hospital for a week to 10 days.
Recovery – Children can usually go back to school after 4-6 weeks, and can take part in sports roughly 1 year after surgery. In some cases, a back brace is needed to support the spine for about 6 months.
The patient will need to return to the hospital every 6 months to have the rods lengthened – this is usually an outpatient procedure, so the patient does not spend the night. The rods will be surgically removed when the spine has grown.
A doctor will only recommend spinal fusion if the benefits are thought to outweigh the risks. The risks include:
Rod displacement – a rod may move from its correct position. Although not uncomfortable, the patient may need further surgery.
Pseudarthrosis – one of the bones used to fuse the spine into place does not stick properly. Some patients may experience mild discomfort, and the spine will not be corrected as successfully. Further surgery may be needed.
Infection – this is usually treated with antibiotics medication.
Nerve damage – damage occurs to the nerves of the spine. Results can range from mild, with numbness in one or both legs, to paraplegia (loss of all lower bodily functions). A neurosurgeon may be present for scoliosis surgery.
Foot drop is a gait abnormality in which the dropping of the forefoot happens due to weakness, irritation or damage to the common fibular nerve including the sciatic nerve, or paralysis of the muscles in the anterior portion of the lower leg. It is usually a symptom of a greater problem, not a disease in itself.
Foot drop is defined as a weakness of the anterior tibialis and is frequently accompanied by weakness of the extensor hallucis longus and extensor digitorum longus [Rx]. It is usually caused by LMN pathology, commonly disruption of conduction from the deep peroneal nerve (L4-L5). L4-L5 radiculopathy is the most common recognized cause of foot drop, usually caused by herniated nucleus pulposus or foraminal stenosis [rx]. Peripheral peroneal neuropathy is the next most common and is brought on by neurogenic and nonneurogenic causes such as nerve entrapment, diabetes mellitus, inflammatory neuropathy, trauma, masses or pressure near the fibular head, intraneural tumors, and vascular pathology [Rx]. Central or UMN causes are extremely rare but must be considered.
Foot drop is defined as a weak anterior tibialis muscle (on foot extension) and is usually caused by lower motor neuron (LMN) disease. Common causes are L4-L5 radiculopathy, caused by either a herniated nucleus pulposus or foraminal stenosis, and peroneal peripheral neuropathy. Other causes include any axonal or demyelinating damage along the whole peripheral nervous system: conus medullaris, cauda equina, nerve plexus, and peripheral mixed nerve. Central nervous system pathology can also cause foot drop. Foot drop has been reported to occur in 52% to 67% of patients with spinal upper motor neuron (UMN) pathology [rx][Rx]. Central causes tend to occur where nerve fibers are highly condensed along the UMN tracts: interhemispheric motor cortex homunculus (mass lesion, anterior cerebral artery stroke), corona radiata, internal capsule (lacune), cerebral peduncle (lacune), medulla, and spinal cord pyramidal tract (myelopathy).[rx]
Anatomy of Foot Drop
Fibers from the dorsal branches of the ventral rami of L4-S1 are found in the peroneal nerve, which is paired with the tibial nerve to constitute the sciatic nerve. The sciatic nerve leaves the pelvic cavity at the greater sciatic foramen, just inferior to the piriformis. It bifurcates to form the peroneal and tibial nerves either in the distal third of the thigh or at the midthigh level.
The peroneal nerve crosses laterally to curve over the posterior rim of the fibular neck to the anterior compartment of the lower leg, dividing into superficial and deep branches. The superficial branch travels between the two heads of the peronei and continues down the lower leg to lie between the peroneal tendon and the lateral edge of the gastrocnemius. It then branches to the ankle anterolaterally to supply sensation to the dorsum of the foot .
Common and superficial peroneal nerves, branches, and cutaneous innervation.
The deep branch divides just after rounding the fibular neck. Its initial branch supplies the tibialis anterior, and the remaining branches supply the EDL, the EHL, and a small sensory patch at the first dorsal web space .
www.rxharun.com
Deep peroneal nerve, branches, and cutaneous innervation.
The peroneal nerve is susceptible to injury all along its course. In that it is part of the sciatic nerve, its funiculi are relatively isolated from those of the tibial nerve. Therefore, trauma to the sciatic nerve may affect only one of its divisions. The funiculi of the peroneal nerve also are larger and have less protective connective tissue than those of the tibial nerve, making the peroneal nerve more susceptible to trauma. In addition, the peroneal nerve has fewer autonomic fibers; thus, in any injury, motor and sensory fibers bear the brunt of the trauma.
Causes of Foot Drop
There are gradations of weakness that can be seen with foot drop, as follows: 0=complete paralysis, 1=flicker of contraction, 2=contraction with gravity eliminated alone, 3=contraction against gravity alone, 4=contraction against gravity and some resistance, and 5=contraction against powerful resistance (normal power). Foot drop is different from foot slap, which is the audible slapping of the foot to the floor with each step that occurs when the foot first hits the floor on each step, although they often are concurrent.
Following surgery (such as knee replacement). This may be due to a haematoma causing compression or irritation of the nerve which is temporary, or nerve damage during surgery.
Habitual crossing of the legs when sitting – compresses the peroneal nerve.
If the L5 nerve root is involved, the most common cause is a herniated disc. Other causes of foot drop are diabetes (due to generalized peripheral neuropathy), trauma, motor neuron disease (MND), adverse reaction to a drug or alcohol, and multiple sclerosis.
Symptoms of peroneal nerve injury (foot drop)
Symptoms of peroneal nerve injury (foot drop) may include:
Inability to point toes toward the body (dorsi flexion)
Imaging tests can help pinpoint these types of problems.
X-rays –Plain X-rays use a low level of radiation to visualize a soft tissue mass or a bone lesion that may be causing your symptoms.
Ultrasound – This technology uses sound waves to create images of internal structures. It may be used to check for cysts or tumors that may be pressing on the nerve.
Computerized tomography (CT) scan – Computerized tomography combines X-ray images taken from many different angles to form cross-sectional views of structures within the body.
Magnetic resonance imaging (MRI) – This test uses radio waves and a strong magnetic field to create detailed images. MRI is particularly useful in visualizing soft tissue lesions that may be compressing a nerve.
Nerve tests
Electromyography (EMG) and nerve conduction studies measure electrical activity in the muscles and nerves. These tests can be uncomfortable, but they’re very useful in determining the location of the damage along the affected nerve.
Treatment of Foot Drop
In case of severe pain, medications may include:
Analgesics-Prescription-strength drugs that relieve pain but not inflammation.
Non-steroidal anti-inflammatory drugs – (NSAIDs – such as aspirin, ibuprofen or naproxen, COX-2 inhibitors (celecoxib)Pain medicines and anti-inflammatory drugs help to relieve pain and stiffness, allowing for increased mobility and exercise. There are many common over-the-counter medicines called non-steroidal anti-inflammatory drugs (NSAIDs). They include aspirin,ibuprofen (Motrin, Advil), and naproxen (Naprosyn, Aleve).
Muscle Relaxants– These medications provide relief from spinal muscle spasms, spasticity & increase muscle tone by increaseing blood flood to the cell.
Prednisone – 20-30 mg/day with a progressive taper over 7-10 days.
Nonpharmacological treatment for foot drop may include
Braces or splints. A brace on your ankle and foot or splint that fits into your shoe can help hold your foot in a normal position.
Physical therapy. Exercises that strengthen your leg muscles and help you maintain the range of motion in your knee and ankle may improve gait problems associated with foot drop. Stretching exercises are particularly important to prevent the development of stiffness in the heel.
Nerve stimulation. Sometimes stimulating the nerve that lifts the foot improves foot drop.
Surgery. Depending upon the cause, and if your foot drop is relatively new, nerve surgery may be helpful. If foot drop is long-standing, your doctor may suggest surgery that fuses ankle or foot bones or a procedure that transfers a functioning tendon to a different position.
Exercise
Physical therapy can help strengthen your muscles, improving your gait (your pattern of walking) and your walking ability. According to Rohrig, your physical therapist will identify whether weakness, spasticity, or both are causing the foot drop, and will then prescribe specific exercises for you. The therapist will also determine how foot drop is impacting your functioning and will investigate whether an assistive device might help you get around better.
Toe-to-Heel Rock
Osteopathclinic.com says to stand with your hands on a table or the wall for support and rise up on your toes. Hold this position for about 5 seconds then lower your heels and rock back on them so your toes are in the air and you feel a stretch in your calf muscles. Hold this position for 6 seconds then repeat the entire sequence six times.
Toe Co-ordination Test
Fitness magazine, says to place a few marbles on the floor and try to pick them up with your toes. This will help to improve your dexterity and the strength of the small muscles in your feet.
Sit on the floor with your legs straight out in front of you then flex your foot so your toes move towards your body and your heels lift off the ground.Hold for about 5 seconds then stretch your foot in the opposite direction and curl tour toes under as tightly as you can. Hold for another 5 seconds and repeat the full range of movement as many times as you can.
Rehabilitation Exercises for Foot Drop
Specific exercises that strengthen the muscles in the foot, ankle and lower leg can help improve the symptoms of foot drop in some cases. Exercises are important for improving range of motion, preventing injury, improving balance and gait, and preventing muscle stiffness.
When treating foot drop, you may work with a physical therapist who will help you get started strengthening your foot, leg and ankle muscles. Rehabilitation for foot drop can be a slow process, so your physical therapist will likely recommend that you continue to do strengthening exercises at home on your own.
By being consistent about your exercises at home, you can maximize your chances of making a successful recovery from foot drop. Strengthening the weakened muscles will allow you to restore normal function and hopefully start walking normally again.
Like any exercise program, please consult your healthcare professional before you begin. Please stop immediately if any of the following exercises cause pain or harm to your body. It’s best to work with a trained professional for guidance and safety.
Towel Stretch
Sit on the floor with both legs straight out in front of you. Loop a towel or exercise band around the affected foot and hold onto the ends with your hands. Pull the towel or band towards your body. Hold for 30 seconds. Then relax for 30 seconds. Repeat 3 times.
Toe to Heel Rocks
Stand in front of a table, chair, wall, or another sturdy object you can hold onto for support. Rock your weight forward and rise up onto your toes. Hold this position for 5 seconds. Next, rock your weight backward onto your heels and lift your toes off the ground. Hold for 5 seconds. Repeat the sequence 6 times.
Marble Pickup
Sit in a chair with both feet flat on the floor. Place 20 marbles and a bowl on the floor in front of you. Using the toes of your affected foot, pick up each marble and place it in the bowl. Repeat until you have picked up all the marbles.
Ankle Dorsiflexion
Sit on the floor with both legs straight out in front of you. Take a resistance band and anchor it to a stable chair or table leg. Wrap the loop of the band around the top of your affected foot. Slowly pull your toes towards you then return to your starting position. Repeat 10 times.
Plantar Flexion
Sit on the floor with both legs straight out in front of you. Take a resistance band and wrap it around the bottom of your foot. Hold both ends in your hands. Slowly point your toes then return to your starting position. Repeat 10 times.
Ball Lift
Sit in a chair with both feet flat on the floor. Place a small round object on the floor in front of you (about the size of a tennis ball). Hold the object between your feet and slowly lift it by extending your legs. Hold for 5 seconds then slowly lower. Repeat 10 times.
How can I manage foot drop myself?
There are some options you can try to help you reduce the risks of trips or falls if you have foot drop, which you can use in conjunction with one of the treatments.
Footwear
suitable and well fitting footwear can help support your foot and lessen the dragging along the floor
shoes with laces or with Velcro fastenings that can be adjusted, may be safer than slip-ons that can become loose with wear
boots can be helpful as they provide ankle support
avoid cumbersome or heavy shoes that quickly tire your muscles.
Awareness
be aware of your surroundings when moving about, concentrate and be ALERT: Assess your Location and Environment for the Risk of Trips
plan your movement, consider which route offers the least potential risk or fewest obstacles. If an obstacle does exist, can this be either safely moved or negotiated?
Remove hazards
a certain degree of clutter is an inevitable part of day to day life, but try to keep your main routes around the house free from obstacles
tape down or use non-slip mats under rugs particularly in the bathroom and bedroom, or consider removing them completely
with electrical items, try to keep wires and cables covered or taped down in walking areas to prevent them being tripped over. An extension lead can help to reroute cables away from places where they might be a tripping hazard.
Multiple joints pain or polyarthralgia is defined as aches in the joints, joint pains, arthralgia of multiple joints, and multiple joint pain. Polyarthritis is the word usually used to describe pain affecting five or more joints, while a patient with 2 to 4 joints involved would be said to have the oligoarticular disease.
Polyarthralgia is more common in women and even more so with increasing age.
Types of Multiple Joint Pain
Multiple Joint pain (arthralgia) can be categorized as
Inflammatory or non-inflammatory – Swelling of the joint, along with redness of the overlying skin and warmth of the area, are signs of an inflamed joint (arthritis). The absence of swelling, redness, and warmth of the affected joint, despite the pain, is an indication of non-inflammatory joint pain.
Mono-, oligo-, polyarticular – Monoarticular refers to one joint, whereas oligoarticular refers to two to four joints and polyarticular is more than four joints (five or more). This approach is often adopted for arthritis.
Generalized or localized – Generalized joint pain refers to diffuse pain, often with a regular change in the location of the joint pain (flitting) and may affect multiple joints simultaneously. Localized joint pain refers to pain within a specific joint or joints.
Causes of Multiple Joints Pain
Peripheral oligoarticular arthritis and polyarticular arthritis are more commonly associated with a systemic infection (eg, viral) or systemic inflammatory disorder (eg, RA) than is monoarticular arthritis. A specific cause can usually be determined (see Table: Some Causes of Pain in ≥ 5 Joints* and Some Causes of Pain in ≤ 4 Joints); however, sometimes the arthritis is transient and resolves before a diagnosis can be clearly established. Axial involvement suggests a seronegative spondyloarthropathy (also called spondyloarthritis—see Overview of Seronegative Spondyloarthropathies) but can also occur in RA (affecting the cervical spine but not the lumbar spine).
Chronic polyarticular arthralgia in children is most often due to the following:
Chronic polyarthralgia in adults is caused most often by RA and osteoarthritis.
Noninflammatory polyarticular pain in adults is most often due to the following:
Chronic polyarticular arthritis in adults is most often due to the following:
Acute polyarticular arthritis is most often due to the following:
Some Causes of Pain in ≤ 4 Joints
Cause
Suggestive Findings
Diagnostic Approach*
Cause
Suggestive Findings
Diagnostic Approach*
Ankylosing spondylitis
Usually axial pain and stiffness, worse in the morning and relieved with activity
Sometimes effusions in large peripheral joints
Sometimes extra-articular manifestations (eg, uveitis, enthesitis, aortic insufficiency)
More common among young adult males
Lumbosacral spine x-ray
Sometimes MRI or CT, blood tests (ESR, C-reactive protein, and CBC), and/or specific (modified New York) clinical criteria
Behçet syndrome
Arthralgia or arthritis
Extra-articular manifestations, such as recurrent oral and/or genital lesions, or uveitis
Usually begins during a person’s 20s
Specific (international) clinical criteria
Crystal-induced arthritis‡, typically caused by uric acid crystals (gout), Ca pyrophosphate crystals (pseudogout), or Ca hydroxyapatite crystals
Acute onset of arthritis with joint warmth and swelling
May be clinically indistinguishable from infectious bacterial (septic) arthritis
Sometimes fever
Arthrocentesis
Infective endocarditis
Arthralgia or arthritis
Systemic symptoms, such as fever, night sweats, rash, weight loss, heart murmur
Blood cultures
Echocardiography
Osteoarthritis
Chronic pain more commonly affecting the base of the thumbs, PIP and DIP joints, knees, and hips
Sometimes Heberden nodes
X-rays
Reactive arthritis and enteropathic arthritis
Arthritis that is asymmetric and more common in large lower extremity joints
Reactive arthritis: GI or GU infection 1–3 wk before onset of acute arthritis
Enteropathic arthritis: Coexisting GI condition (eg, inflammatory bowel disease, intestinal bypass surgery) with a chronic arthritis
Clinical evaluation
Testing for STDs as clinically indicated
*Patients with joint effusion or inflammation should have arthrocentesis (with cell counts, Gram stain, cultures, and crystal examination), and usually ESR and C-reactive protein. X-rays are often not helpful early in the disease course.
†These disorders can manifest with axial involvement.
‡Crystal-induced arthritis is most often monoarticular but sometimes oligoarticular.
Joint pain and swelling usually less severe than infectious bacterial arthritis
Other systemic symptoms depending on virus (eg, jaundice with hepatitis B, often generalized lymphadenopathy with HIV)
Arthrocentesis
Viral serology testing as clinically indicated (eg, hepatitis B surface antigen and IgM antibody to hepatitis B core for suspected hepatitis B)
Juvenile idiopathic arthritis
Childhood onset of joint symptoms
Manifestation with oligoarthritis plus uveitis, or with systemic symptoms (Still disease—fever, rash, adenopathy, splenomegaly, pleural and/or pericardial effusions)
Disease-specific manifestations including specific dermatologic manifestations (dermatomyositis), dysphagia (systemic sclerosis), muscle soreness (polymyalgia rheumatica), or dry eyes and dry mouth (Sjögren syndrome)
Clinical evaluation
Sometimes x-rays and/or serologic testing (eg, anti-SSA and anti-SSB in Sjögren syndrome, anti-Scl-70 in systemic sclerosis)
Sometimes skin or muscle biopsy
Psoriatic arthritis
One of five patterns of joint involvement, which include polyarthritis similar to RA and oligoarthritis
Extra-articular manifestations, such as psoriasis, onychodystrophy, uveitis, tendinitis, and dactylitis (sausage digits)
Clinical evaluation
Sometimes x-rays
RA
Symmetric arthritis of small and large joints
Sometimes initially monoarticular or oligoarticular
More common among young adults but can manifest at any age
Sometimes joint deformities at late stages
Clinical evaluation
RF and anti-CCP testing
X-rays
Serum sickness
Arthralgia more often than arthritis
Fever, lymphadenopathy, and rash
Exposure to blood products within 21 days of symptom onset
Clinical evaluation
SLE
Arthralgia more often than arthritis
Systemic manifestations, such as rash (eg, malar rash), mucosal lesions (eg, oral ulcers), serositis (eg, pleuritis, pericarditis), manifestations of glomerulonephritis
More common among women
Clinical evaluation
ANA, anti-dsDNA, CBC, urinalysis, chemistry profile with renal and liver enzymes
Systemic vasculitides (eg, immunoglobulin A–associated vasculitis [formerly called Henoch-Schönlein purpura], polyarteritis nodosa, granulomatosis with polyangiitis)
Arthralgias, particularly with immunoglobulin A–associated vasculitis
Extra-articular symptoms, often involving multiple organ systems (eg, abdominal pain, renal failure, manifestations of pneumonitis, sinonasal symptoms, skin lesions that may include rash, purpura, nodules, and ulcers)
Serologic testing as clinically indicated (eg, ANCA testing with suspected granulomatosis with polyangiitis)
Biopsy as indicated (eg, of kidney, skin, or lung)
*These disorders may also manifest as oligoarticular (involving ≤ 4 joints).
†Patients with joint effusion or inflammation should have arthrocentesis (with cell counts, Gram stain, cultures, and crystal examination), and usually ESR and C-reactive protein. X-rays are often unnecessary.
The following are the most common symptoms of multiple joints pain or poliarthritis arthritis. However, each individual may experience symptoms differently. Symptoms may include
Inflamed, painful joints
Stiff joints
Enlarged and/or deformed joints (such as fingers bent toward the little finger and/or swollen wrists)
Frozen joints (joints that freeze in one position)
Cysts behind the knees that may rupture, causing lower leg swelling and pain
Hard nodules (bumps) under the skin near affected joints
Low-grade fever
Inflamed blood vessels (vasculitis) may occur occasionally, leading to nerve damage and leg sores
Inflamed membranes around the lungs (pleurisy), the sac around the heart (pericarditis), or inflammation and scarring of the lungs themselves, that may lead to chest pain, difficulty breathing, and abnormal heart function
Swollen lymph nodes
Sjögren’s syndrome (dry eyes and mouth)
Eye inflammation
If a person has four or more of the following symptoms, he/she may be diagnosed with multiple joints pain
Morning stiffness that lasts longer than one hour for at least six weeks
Three or more joints that are inflamed for at least six weeks
Presence of arthritis in the hand, wrist, or finger joints for at least six weeks
Blood tests that reveal rheumatoid factor
X-rays that show characteristic changes in the joints
Diagnosis of Multiple Joints Pain
Selected Extra-Articular Manifestations Associated with Conditions That Result in Polyarticular Joint Pain*
PHYSICAL FINDING
DIAGNOSES TO CONSIDER
Skin and mucous membranes
Rash
Erythema infectiosum
Reticulated (lacy) rash
Human parvovirus B19 infection
Facial exanthema (slapped cheek)
Human parvovirus B19 infection
Malar rash
SLE, human parvovirus B19 infection, Lyme disease, rosacea, seborrhea, dermatomyositis
Non-pharmacologic therapies include treatments other than medications and are the foundation of treatment for all people with rheumatoid arthritis.
Rest
When joints are inflamed, the risk of injury of the joint itself and the adjacent soft tissue structures (such as tendons and ligaments) is high. This is why inflamed joints should be rested. However, physical fitness should be maintained as much as possible. At the same time, maintaining a good range of motion in your joints and good fitness overall are important in coping with the systemic features of the disease.
Exercise
Pain and stiffness often prompt people with rheumatoid arthritis to become inactive. However, inactivity can lead to a loss of joint motion, contractions, and a loss of muscle strength. These, in turn, decrease joint stability and further increase fatigue.
Regular exercise, especially in a controlled fashion with the help of physical therapists and occupational therapists, can help prevent and reverse these effects. Types of exercises that have been shown to be beneficial include range-of-motion exercises to preserve and restore joint motion, exercises to increase strength and exercises to increase endurance (walking, swimming, and cycling).
Physical and Occupational Therapy
Physical and occupational therapy can relieve pain, reduce inflammation, and help preserve joint structure and function for patients with rheumatoid arthritis.
Specific types of therapy are used to address the specific effects of rheumatoid arthritis:
The application of heat or cold can relieve pain or stiffness.
Use of ultrasound to help reduce inflammation of the sheaths surrounding tendons (tenosynovitis)
Passive and active exercises to improve and maintain the range of motion of the joints
Rest and splinting to reduce joint pain and improve joint function
Finger-splinting and other assistive devices to prevent deformities and improve hand function.
Relaxation techniques to relieve secondary muscle spasm
Occupational therapists also focus on helping people with rheumatoid arthritis to be able to continue to actively participate in work and recreational activity with special attention to maintaining good function of the hands and arms.
Nutrition and Dietary Therapy
Weight loss may be recommended for overweight and obese people to reduce stress on inflamed joints.
People with rheumatoid arthritis have a higher risk of developing coronary artery disease. High blood cholesterol is one risk factor for coronary disease that can respond to changes in diet. A nutritionist can recommend specific foods to eat or avoid in order to achieve a desirable cholesterol level.
Changes in diet have been investigated as treatments for rheumatoid arthritis, but there is no diet that is proven to cure rheumatoid arthritis. No herbal or nutritional supplements, such as cartilage or collagen, can cure rheumatoid arthritis. These treatments can be dangerous and are not usually recommended.
Smoking and Alcohol
Smoking is a risk factor for rheumatoid arthritis and it has been shown that quitting smoking can improve the condition. People who smoke need to quit completely. Assistance in quitting should be obtained if needed.
Moderate alcohol consumption is not harmful to rheumatoid arthritis, although it may increase the risk of liver damage from some drugs such as methotrexate. People should discuss the safety of alcohol use with a doctor because recommendations depend on the medications a person is taking and on their other medical conditions.
Measures to Reduce Bone Loss
Inflammatory conditions such as rheumatoid arthritis can cause bone loss, which can lead to osteoporosis. The use of prednisone further increases the risk of bone loss, especially in postmenopausal women. It is important to do a risk assessment and address risk factors that can be changed in order to help prevent bone loss.
Patients may do the following to help minimize the bone loss associated with steroid therapy:
Use the lowest possible dose of glucocorticoids for the shortest possible time, when possible, to minimize bone loss.
Consume an adequate amount of calcium and vitamin D, either in the diet or by taking supplements.
Use medications that can reduce bone loss, including that which is caused by glucocorticoids.
Control the disease itself with appropriate medications prescribed by your doctor.
Medical Management of Acute Polyarthritis
Hospitalize the patient in the presence of any of the following
Significant, concomitant internal organ involvement
Signs of bacteremia, including vesiculopustular skin lesions, Roth spots, shaking chills, or splinter hemorrhages
Systemic vasculitis
Severe pain
Severe constitutional symptoms
Purulent (group III) synovial fluid in 1 or more joints
Immunosuppression
Medications
There are many medications available to decrease joint pain, swelling and inflammation and hopefully, prevent or minimize the progression of the disease. The type of drugs that your doctor recommends will depend on how severe your arthritis is and how well you respond to the medications. These medications include:
Analgesics – Prescription-strength drugs that relieve pain but not inflammation.
Non-steroidal anti-inflammatory drugs (NSAIDs – such as aspirin, ibuprofen or naproxen, COX-2 inhibitors (celecoxib))Pain medicines and anti-inflammatory drugs help to relieve pain and stiffness, allowing for increased mobility and exercise. There are many common over-the-counter medicines called non-steroidal anti-inflammatory drugs (NSAIDs). They include aspirin, ibuprofen (Motrin, Advil), and naproxen (Naprosyn, Aleve).
Antidepressants – Drugs that block pain messages from your brain and boost the effects of endorphins (your body’s natural painkillers).
Antibiotic therapy – is indicated for septic polyarthritis or bacteremia with joint involvement (eg, disseminated gonococcemia). Systemic antibiotics are used after appropriate cultures are taken. Prolonged treatment of Chlamydia-induced reactive arthritis with antibiotics may be of benefit; this is not true for other forms of reactive arthritis.
Indomethacin – is highly effective, but adverse effects in some patients limit its utility. Other NSAIDs with short half-lives (eg, ibuprofen and diclofenac) can also be used.
Corticosteroids – Corticosteroid to healing the nerve inflammation and clotted blood in the joints. It is an effective alternative to NSAIDs and colchicine for patients in whom these drugs may be contraindicated or hazardous (eg, patients with advanced age, renal insufficiency, congestive heart failure, inability to take oral medications). Regimens include the following:
Intramuscular – (IM) injection of a long-acting crystalline preparation (eg, triamcinolone acetonide 60-80 mg), with an option to repeat once after 24-48 hours
Muscle Relaxants- These medications provide relief from spinal muscle spasms, spasticity & increase muscle tone by increasing blood flood to the cell.
Neuropathic Agents- Drugs(pregabalin & gabapentin) that address neuropathic—or nerve-related—pain. This includes burning, numbness, and tingling.
Opioids – Also known as narcotics, these medications are intense pain relievers that should only be used under a doctor’s careful supervision.
Topical Medications- These prescription-strength creams, gels, ointments, patches, and sprays help relieve pain and inflammation through the skin.
Calcium & vitamin D3 – to improve bones health and healing fracture.
Prednisone – 20-30 mg/day with a progressive taper over 7-10 days.
Dietary supplement -to remove the general weakness & improved the health.
Disease-modifying anti-rheumatic drugs – (DMARDs) such as hydroxychloroquine, methotrexate, sulfasalazine, and leflunomide improvement in symptoms may require four to six weeks of treatment with methotrexate. Improvement may require one to two months of treatment with sulfasalazine and two to three months of treatment with hydroxychloroquine.
Biologic agents – (such as infliximab, etanercept, adalimumab, certolizumab and golimumab, tocilizumab, rituximab, abatacept, anakinra, tofacitinib) Biologics tend to work rapidly, within two weeks for some medications and within four to six weeks for others. Biologics may be used alone or in combination with other DMARDs. Usually, they are reserved for patients who do not adequately respond to DMARDs, or if adverse prognostic factors are present.
When choosing DMARDs, the following principles should be considered
Combinations of DMARDs may be more effective than single drugs. For example, hydroxychloroquine, sulfasalazine, and methotrexate together are more effective than methotrexate alone or the other two together.
Combining a DMARD – with another drug, such as methotrexate plus a TNF-α antagonist or an IL-1 receptor antagonist, or a rapidly tapered corticosteroid, may be more effective than using DMARDs alone.
Methotrexate – is a folate antagonist with immunosuppressive effects at the high dose. It is anti-inflammatory at doses used in RA. It is very effective and has a relatively rapid onset (a clinical benefit often within 3 to 4 wk). Methotrexate should be used with caution, if at all, in patients with hepatic dysfunction or renal failure. Alcohol should be avoided. Supplemental folate, 1 mg po once/day, reduces the likelihood of adverse effects. CBC, AST, ALT, and albumin and creatinine level should be determined about every 8 wk. When used early in the course of RA, efficacy may equal the biologic agents. Rarely, a liver biopsy is needed if liver function test findings are persistently twice the upper limit of normal or more and the patient needs to continue to use methotrexate. Severe relapses of arthritis can occur after withdrawal of methotrexate. Paradoxically, rheumatoid nodules may enlarge with methotrexate therapy.
Hydroxychloroquine – can also control symptoms of mild RA. Funduscopic examination should be done and visual fields should be assessed before and every 12 mo during treatment. The drug should be stopped if no improvement occurs after 9 mo.
Leflunomide – interferes with an enzyme involved with pyrimidine metabolism. It is about as effective as methotrexate but is less likely to suppress bone marrow, cause abnormal liver function, or cause pneumonitis. Alopecia and diarrhea are fairly common at the onset of therapy but may resolve with a continuation of therapy.
Sulfasalazine – Sulfasalazine (Azulfidine, generic) works best when the disease is confined to the joints. Symptom relief occurs within 1 – 3 months. Side effects are common, particularly stomach and intestinal distress, which usually occur early in the course of treatment. (However, serious gastrointestinal side effects, such as stomach ulcers, occur less frequently with sulfasalazine than with NSAIDs.) A coated-tablet form may help reduce side effects. Other side effects include skin rash and headache. Sulfasalazine increases sensitivity to sunlight. Be sure to wear sunscreen (SPF 15 or higher) while taking this drug. People with intestinal or urinary obstructions or who have allergies to sulfa drugs or salicylates should not take sulfasalazine.
Minocycline – Minocycline (Minocin, generic) is a tetracycline antibiotic that is generally reserved for patients with mild RA. It can take 2 – 3 months before symptoms begin to improve and up to a year for full benefit. Side effects include upset stomach, dizziness, and skin rash. Long-term use of minocycline can cause changes in skin color, but this side effect usually disappears once the medication is stopped. Minocycline can cause yeast infections in women. It should not be used by women who are pregnant or planning on becoming pregnant. Minocycline increases sensitivity to sunlight and patients should be sure to wear sunscreen. In rare cases, minocycline can affect the kidneys and liver.
Tofacitinib- Tofacitinib (Xeljanz) is the newest DMARD. Approved in 2012, tofacitinib is the first in a new class of drugs. It works by blocking “Janus kinase” molecules involved in joint inflammation. There is hope that DMARD might be an alternative to biologic DMARDs and a new option for patients with moderate-to-severe RA who have not been helped by methotrexate. Tofacitinib, which is taken as a twice-daily pill, can be used alone or in combination with methotrexate. Tofacitinib may increase the risk of serious infections. Because it is new a drug, long-term side effects are still unknown.
Gold- Gold used to be a time-honored DMARD for rheumatoid arthritis but its use has decreased with the development of newer DMARDs and biologic drugs. Gold is usually administered in an injected form because the oral form, auranofin (Ridaura, generic), is much less effective. There are two injectable forms of gold: Gold sodium thiomalate (Myochrysine, generic) and aurothioglucose (Solganal, generic). It can take 3 – 6 months before injections have an effect on RA symptoms. Gold injections can cause a number of side effects including mouth sores and skin rash and in rare cases more serious problems such as kidney damage.
Azathioprine-Azathioprine (Imuran, generic) suppresses immune system activity. It takes 6 – 8 weeks for early symptom improvement and up to 12 weeks for full benefit. Azathioprine can cause serious problems with the gastrointestinal tract including nausea and vomiting, often accompanied by stomach pain and diarrhea. Azathioprine can also cause problems with liver function and pancreas gland inflammation and can reduce white blood cell count.
Cyclosporine – Like azathioprine, cyclosporine (Sandimmune, Neoral, generic) is an immunosuppressant. It is used for people with RA who have not responded to other drugs. It can take a week before symptoms improve and up to 3 months for full benefit. The most serious and common side effects of cyclosporine are high blood pressure and kidney function problems. While kidney function usually improves once the drug is stopped, mild-to-moderate high blood pressure may continue. Swelling of the gums is also common. Patients should practice good dental hygiene, including regular brushing and flossing.
Corticosteroids – Systemic corticosteroids decrease inflammation and other symptoms more rapidly and to a greater degree than other drugs. They also seem to slow bone erosion. However, they may not prevent joint destruction, and their clinical benefit often diminishes with time. Furthermore, rebound often follows the withdrawal of corticosteroids in active disease. Because of their long-term adverse effects, some doctors recommend that corticosteroids are given to maintain function only until another DMARD has taken effect. Corticosteroids may be used for severe joint or systemic manifestations of RA (eg, vasculitis, pleurisy, pericarditis). Relative contraindications include peptic ulcer disease, hypertension, untreated infections, diabetes mellitus, and glaucoma. The risk of latent TB should be considered before corticosteroid therapy is begun.
Intra-articular injections or Intra-articular corticosteroid therapy – of depot corticosteroids may temporarily help control pain and swelling in particularly painful joints. Triamcinolone hexacetonide may suppress inflammation for the longest time. Triamcinolone acetonide and methylprednisolone acetate are also effective. No single joint should be injected with a corticosteroid more than 3 to 4 times a year, as too-frequent injections may accelerate joint destruction (although there are no specific data from humans to support this effect). Because injectable corticosteroid esters are crystalline, local inflammation transiently increases within a few hours in < 2% of patients receiving injections. Although infection occurs in only < 1:40,000 patients, it must be considered if pain occurs > 24 h after injection.
Immunomodulatory, cytotoxic, and immunosuppressive drugs – Treatment with azathioprine or cyclosporine (an immunomodulatory drug) provides efficacy similar to DMARDs. However, these drugs are more toxic. Thus, they are used only for patients in whom treatment with DMARDs has failed or to decrease the need for corticosteroids. They are used infrequently unless there are extra-articular complications. For maintenance therapy with azathioprine, the lowest effective dose should be used. Low-dose cyclosporine may be effective alone or when combined with methotrexate. It may be less toxic than azathioprine. Cyclophosphamide is no longer recommended due to its toxicity.
Biologic agents – Biologic response modifiers other than TNF-α antagonists can be used to target B cells or T cells. These agents are typically not combined with each other.
Rituximab – is an anti-CD 20 antibody that depletes B cells. It can be used in refractory patients. The response is often delayed but may last 6 mo. The course can be repeated after 6 mo. Mild adverse effects are common, and analgesia, corticosteroids, diphenhydramine, or a combination may need to be given concomitantly. Rituximab is usually restricted to patients who have not improved after using a TNF-α inhibitor and methotrexate. Rituximab therapy has been associated with progressive multifocal leukoencephalopathy, mucocutaneous reactions, delayed leukopenia, and hepatitis B reactivation.
Abatacept – a soluble fusion cytotoxic T lymphocyte-associated antigen 4 (CTLA-4) Ig, is indicated for patients with RA with an inadequate response to other DMARDs.
Other agents
Anakinra – is a recombinant IL-1 receptor antagonist. IL-1 is heavily involved in the pathogenesis of RA. Infection and leukopenia can be problems.
TNF-α antagonists – (eg, adalimumab, etanercept, golimumab, certolizumab pegol, and infliximab) reduce the progression of erosions and reduce the number of new erosions. Although not all patients respond, many have a prompt, dramatic feeling of well being, sometimes with the first injection. Inflammation is often dramatically reduced. These drugs are often added to methotrexate therapy to increase the effect and possibly prevent the development of drug-neutralizing antibodies.
Tocilizumab – blocks the effect of IL-6 and has clinical efficacy in patients who have responded incompletely to other biologic agents.
Tofacitinib – is a Janus kinase (JAK) inhibitor that is given orally with or without concomitant methotrexate to patients who do not respond to methotrexate alone or other biologic agents. Although there are some differences among agents, the most serious problem is an infection, particularly with reactivated TB. Patients should be screened for TB with PPD or an interferon-gamma release assay. TNF-α antagonists should probably be stopped before major surgery. Etanercept, infliximab, and adalimumab can and probably should be used with methotrexate. High-dose infliximab should not be used in patients with severe heart failure. However, the risk of side effects from treatment must be weighed against the benefits on an individual basis.
Other Strategies to Manage Multiple Joints Pain
Other important strategies that can help you manage rheumatoid arthritis include
Self-management courses – can help people with rheumatoid arthritis and other chronic (ongoing) conditions to build skills and confidence in becoming more actively involved in your healthcare and in managing rheumatoid arthritis day to day.
Aids and equipment – supports such as walking aids and specialized cooking utensils reduce joint strain and can help you to manage pain and fatigue. An occupational therapist can give you advice on aids. You can also phone the Independent Living Centre for advice.
Relaxation techniques – muscle relaxation, distraction, guided imagery, and other techniques can help you manage pain and difficult emotions such as anxiety.
If exercise is causing sharp pain, stop immediately.
If lesser aches and pains continue for more than 2 hours afterward, try a lighter exercise program for a while.
Using large joints instead of small ones for ordinary tasks can help relieve pressure, for instance, closing a door with the hip or pushing buttons with the palm of the hand.
Start with the easiest exercises, stretching and tensing of the joints without movement.
Next, attempt mild strength training.
The next step is to try aerobic exercises. These include walking, dancing, or swimming, particularly in heated pools. Avoid heavy impact exercises, such as running, downhill skiing, and jumping.
Tai chi, which uses graceful slow sweeping movements, is an excellent method for combining stretching and range-of-motion exercises with relaxation techniques. It may be of particular value for elderly patients with RA.
Exercise –It is important for patients with RA to maintain a balance between rest (which will reduce inflammation) and moderate exercise (which will relieve stiffness and weakness). Studies have suggested that even as little as 3 hours of physical therapy over 6 weeks can help people with RA and that these benefits are sustained. The goal of the exercise is to In general, doctors recommend the following approaches, Maintain a wide range of motion
Promote well-being
Improve general health
Increase strength, endurance, and mobility
A Common-Sense Approach to Exercise is The Best Guide
Rest – can help you to manage fatigue and is particularly important when your joints are swollen.
Nutrition – while there is no specific ‘diet’ for people with rheumatoid arthritis, it is important to have a healthy, balanced diet to maintain general health and, prevent weight gain and other medical problems, such as diabetes and heart disease.
Support – a peer support group can provide understanding, advice, support and information from others in a similar situation. Contact MOVE muscle, bone & joint health for more information.
Complementary therapies – such as massage or acupuncture may be helpful. Consult your doctor or rheumatologist before commencing any treatment. Fish oil supplements may also be helpful as they contain a certain type of fat called omega-3. Current research suggests omega-3 fats can help reduce inflammation in rheumatoid arthritis.
Omega-3 fatty acids – There are lots of natural anti-inflammatories, but the best studied by far are omega-3 fatty acids. These heart-healthy, brain-boosting fats are especially prevalent in seafood, especially fatty fish such as salmon, sardines, and tuna. Studies have found that adding omega-3s to the diet can reduce joint pain and morning stiffness in people with RA, says Chaim Putterman, M.D., chief of rheumatology at Montefiore Medical Center and Albert Einstein College of Medicine in New York City. Not a fan of fish? Fish oil capsules can give you the same benefits. But beware: High concentrations of omega-3s can thin the blood, so consult your doctor for the right dose
Gamma linolenic acid (GLA)- is another fatty acid with anti-inflammatory properties, says Robert Zurier, M.D., who has studied the effects of GLA in rheumatoid arthritis patients at the University of Massachusetts Medical School. GLA is found mostly in botanical oils—evening primrose, black currant seed and especially borage oil, its richest source. The patients in Dr. Zurier’s studies took three 1,000-milliliter capsules of borage oil every day for six months and reported less joint pain and stiffness than patients who took placebo capsules, and they also reduced their dose of nonsteroidal anti-inflammatory drugs.
Joint surgery – may be necessary in some cases if the joint is very painful or there is a risk of losing overall function. Any medication or treatment for arthritis must be discussed with and monitored by your doctor or rheumatologist. They will take into account the condition being treated, any other health issues and identifiable risk factors.
Diet – Many patients with RA try dietary approaches, such as fasting, vegan diets, or eliminating specific foods that seem to worsen RA symptoms. There is little scientific evidence to support these approaches but some patients report anecdotally that they are helpful.
In recent years – a number of studies have suggested that the omega-3 fatty acids contained in fish oil may have anti-inflammatory properties useful for RA joint pain relief. The best source of fish oil is through increased consumption of fatty fish such as salmon, mackerel, and herring. Fish oil supplements are another option, but they may interact with certain medications. If you are thinking of trying fish oil supplements, talk to your doctor first.
Pain with Stress Management – Patients can learn strategies to cope with the stress and frustration of living with chronic pain. Relaxation and stress management techniques such as guided imagery, breathing exercises, hypnosis, or biofeedback can be helpful. Although there is no definitive evidence to support their efficacy, some patients report relief with modalities such as acupuncture, massage, and mineral baths.
Assistive Devices – There are many different types of assisted devices that can help make life easier in the home. Kitchen gadgets, such as jar openers, can assist with gripping and grabbing. Door-knob extenders and key turners are helpful for patients who have trouble turning their wrists. Bathrooms can be fitted with shower benches, grip bars, and raised toilet seats. An occupational therapist can advise you on choosing the right kinds of assistive devices.
Miscellaneous Supportive Treatments – Various ointments, including Ben Gay and capsaicin (a cream that use the active ingredient in chili peppers), may help soothe painful joints. Orthotic devices are specialized braces and splints that support and help align joints. Many such devices made from a variety of light materials are available and can be very helpful when worn properly.
Herbal Remedies
Massage
This is the first out of the most efficient home remedies for rheumatoid arthritis in the body that I want to reveal in this entire writing.
When being applied properly, massage can help to relieve the pain caused rheumatoid arthritis as it can relax your stiff muscles. Massage will help to boost your blood circulation, which is essential for alleviating the discomfort due to the symptoms of rheumatoid arthritis.
Evening Primrose Oil
Evening primrose oil is one kind of plant oil which can help to relieve morning stiffness and pain effectively. This plant oil has the gamma-linolenic acid properties – an essential fatty acid which can help to relieve the intensity of numerous symptoms caused by rheumatoid arthritis.
Take 540 mg to 2.8 g of evening primrose oil in divided doses every day. Remember to consult an expert to get proper dosage because this oil may interfere with some medications.
Epsom Salt
Epsom salt is also a great and highly effective natural remedy which can help to soothe the pain and swelling due to rheumatoid arthritis. Epsom salt is an abundant source of magnesium, so it can help to regulate the pH levels in your body effectively as well. In turn, it can help to reduce rheumatoid arthritis, stiffness, and pain in the joints. In addition, it can help to mineralize bone well.
Add 2 cups of Epsom salt to a bathtub full of warm water.
Soak in the bathtub within about half an hour.
Apply this method up to 3 times weekly.
In fact, this is also one of the best home remedies for rheumatoid arthritis in the body that people should make use for good!
Ginger
In naturopathy and Ayurvedic as well, ginger has been used for people at all ages to deal with inflammatory conditions, including rheumatoid arthritis. Ginger contains a compound named gingerol – a powerful agent with natural anti-inflammatory properties, helping to relieve swelling and pain due to rheumatoid arthritis effectively.
You can add ginger to daily food dishes or drink two or three cups of ginger tea every day.
Alternatively, you can chew some fresh ginger slices every day.
Use ginger oil to rub onto your affected area. Then expose that area to sunlight for five to ten minutes to generate heat and warmth. Apply this tip on a regular basis.
In brief, making use of ginger is one of the most effective home remedies for rheumatoid arthritis pain that people should never look down and should apply for good!
Garlic
Thanks to its powerful anti-inflammatory properties, garlic is also advisable for dealing with rheumatoid arthritis. Garlic can help to inhibit the pro-inflammatory substances (also called “cytokines”) production, helping to relieve swelling and pain efficiently and fast.
You can take garlic capsules. For correct dosage, remember to consult experts.
You can also eat one or two raw garlic cloves every day
Apple Cider Vinegar
Apple cider vinegar is considered very useful in helping people relieve several symptoms caused by rheumatoid arthritis. Being rich in minerals, such as phosphorus, potassium, magnesium, and calcium, apple cider vinegar can help to relieve rheumatoid arthritis pain effectively.
You should use some apple cider vinegar to directly apply to the affected area of your body. Then, use warm castor oil to massage your painful area. Finally, use a cotton cloth to wrap that area and use plastic to cover it. Apply this method every day before bedtime for good results as desired.
Mix one teaspoon of honey with one tablespoon of raw, unfiltered apple cider vinegar and add them to 1/2 cup of warm water. Consume this solution once every day.
Turmeric
Turmeric can help to reduce the risk of joint rheumatoid arthritis by blocking certain cytokines and enzymes causing rheumatoid arthritis.
You can add turmeric powder to your daily meals to benefit from this natural ingredient.
Alternatively, you can take turmeric in form of capsules by 500 – 1,000 mg three times daily. Remember to consult experts initially.
Bring 1 quart of water to a boil. Add 1 tablespoon of turmeric powder and boil it for another 10 minutes. Allow it to cool and drink it once or twice daily.
Do not consume high doses of turmeric because it can act as a blood thinner as well as leading to a stomach upset.
This is actually one of the best home remedies for rheumatoid arthritis pain that I would like to reveal in this entire article and want my readers to make use for good!
Fish Oil
Fish oil contains omega-3 fatty acids – DHA and EPA – that have a powerful anti-inflammatory ability and can help to relieve pain as well. In addition, fish oil can help to prevent the risks of heart disease, which rheumatoid arthritis sufferers are usually at high risks.
Add cold-water fish like salmon and tuna to your daily diet
Take up to 2.6 grams of fish oil (containing 30% DHA/EPA at least) 2 times every day.
Before taking fish oil supplements, remember to consult your doctor because the supplements could interfere with some types of medications you are taking.
Hot And Cold Compresses
Alternating hot and cold compresses is also a great way to reduce the symptoms caused by rheumatoid arthritis. While a cold compress can dull the pain and relieve rheumatoid arthritis and joint swelling, a hot compress can help to relieve pain by relaxing sore joints and muscles.
For the cold compress, use a thin towel to wrap some ice cubes.
For the hot compress, use a towel to wrap a hot water bag.
Put the hot compress right onto the affected area and let it stay within just three minutes.
Remove the hot compress and place the cold compress immediately in its place within just one minute.
Repeat these steps for fifteen to twenty minutes 2 – 3 times every day until your pain is relieved.
Parsley – In a research conducted by JNR (Journal of Natural Remedies) on rats, it was found that extract made of fresh leaves of parsley had reduced inflammation in their paws. Therefore, using it as a home remedy to relieve you from your arthritis pain can have a positive impact.
Carrots –Carrots have an abundance amount of Vitamin C and beta carotene. Beta-carotene and Vitamin C both have antioxidant properties that kill free radicals which are responsible for arthritis inflammation.
Rosemary – Rosemary has a polyphenol called rosmarinic acid which is a potent antioxidant and inflammation reliever.
Kale –Kale is a vegetable that is a rich source of anti-oxidants, Vitamin C, Vitamin K, and beta-carotene that can reverse arthritis inflammation.
Coriander – According to medical research conducted by All India Institute of Medical Sciences, the coriander powder has the potential to reduce swelling and inflammation. It can also be digested as green leaves.
Olive Oil – Olive oil, especially raw ice-pressed, has many health benefits starting from reducing your blood cholesterol to diabetes and inflammation. It can be used as cooking oil that could not only make your dish tastier but also loads with various health benefits. The anti-inflammatory properties of olive oil relieve you from arthritis joints pain.
Greentea – Green tea is a wonder drink that is loaded with antioxidants that have anti-inflammatory properties. Along with relieving you from severe arthritis pain, green tea has many health benefits from lowering your LDL cholesterol to minimizing the risk of bladder cancer.
Pineapple – The stems of pineapples are rich in a protein called bromelain. It acts as a digestive enzyme that relieves from arthritis inflammation.
Blueberries – Blueberries are rich in various minerals and they are considered to be the potential sources of antioxidants. However, always go for organically grown berries because they have higher amounts of polyphenols than the non-organically grown. These polyphenols and antioxidants prevent cell damage and reduce inflammation.
Homeopathic Treatment For Multiple Joints Pain
The treatment for Rheumatoid Arthritis may vary from cases to the case – some requiring short-term whereas others requiring long term treatment. The duration of treatment depends on various factors such as the severity, duration, and extent of the illness, the nature of treatment taken for the same and general health of the patient.
Common Homeopathy medicines for Rheumatoid Arthritis are
Arnica – Useful for chronic arthritis with a feeling of bruising and soreness. The painful parts feel worse from being moved or touched.
Bryonia – Helpful for stiffness and inflammation with tearing or throbbing pain, made worse by motion. The condition may have developed gradually and is worse in cold dry weather. Discomfort is aggravated by being touched or bumped, or from any movement. Relief can be had from pressure and from rest. The person may want to stay completely still and not be interfered with.
Calcarea carbonica- Helpful for deeply aching arthritis involving node formation around the joints. Inflammation and soreness are worse from cold and dampness, and problems may be focused on the knees and hands. Common symptoms are: weakness in the muscles, easy fatigue from exertion, and a feeling of chilliness or sluggishness. The person who benefits from Calcarea is often solid and responsible, but tends to become extremely anxious and overwhelmed when ill or overworked.
Aurum metallicum- This remedy is often prescribed for wandering pains in the muscles and joints that are better from motion and warmth, and worse at night. The person may experience deep pain in the limbs when trying to sleep.
Causticum – Useful when deformities develop in the joints, in a person with tendon problems, muscle weakness, and contractures. The hands and fingers may be most affected. Stiffness and pain are worse from being cold, and relief may come with warmth. The person often feels best in rainy weather and worse when the days are clear and dry.
Calcarea fluorica – Helpful when arthritic pains improve with heat and motion. Joints become enlarged and hard, and nodes or deformities develop. Arthritis after a chronic injury to joints also responds to Calcarea fluorica.
Dulcamara – Indicated if arthritis flares up during cold damp weather. The person gets chilled and wet. They are often stout, with a tendency toward back pain, chronic stiffness in the muscles, and allergies.
Kali bichromicum – This is useful when arthritic pains alternate with asthma or stomach symptoms. Pains may suddenly come and go, or shift around. Discomfort and inflammation are aggravated by heat and worse when the weather is warm.
Kali carbonicum – Arthritis with great stiffness and stitching pains, worse in the early morning hours and worse from cold and dampness, may respond to Kali carbonicum. The joints may be becoming thickened or deformed.
Kalmia latiflora – Useful for intense arthritic pain that flares up suddenly. The problems start in higher joints and extend to lower ones. Pain and inflammation may begin in the elbows, spreading down to the wrists and hands. Discomfort is worse from motion and often worse at night.
Ledum palustre – Arthritis that starts in lower joints and extends to higher ones are a candidate for this remedy. Pain and inflammation often begin in the toes and spread upward to the ankles and knees. The joints may also make cracking sounds. Ledum is strongly indicated when swelling is significant and relieved by cold applications.
Pulsatilla – Applicable when rheumatoid arthritis pain is changeable in quality, or when the flare-ups move from place to place. The symptoms (and the person) feel worse from warmth, and better from fresh air and cold applications. Can benefit people who are emotional and affectionate, sometimes having teary moods.
Rhododendron – Strongly indicated if swelling and soreness flare up before a storm, continuing until the weather clears. Cold and dampness aggravate the symptoms. Discomfort is often worse toward early morning, or after staying still too long.
Rhus Toxicodendron – Useful for rheumatoid arthritis, with pain and stiffness that is worse in the morning and worse on the first motion, but better from continued movement. Hot baths or showers, and warm applications improve the stiffness and relieve the pain. The condition is worse in cold, wet weather. The person may feel extremely restless, unable to find a comfortable position, and need to keep moving constantly. The continued motion also helps to relieve anxiety.
Ruta graveolens – Arthritis with a feeling of great stiffness and lameness, worse from cold and damp and worse from exertion, may be helped by Ruta graveolens. Tendons and capsules of the joints can be deeply affected or damaged. Arthritis may have developed after overuse, from repeated wear and tear.
Rheumatic Diseases is an umbrella term for conditions causing chronic, often intermittent pain affecting the joints and/or connective tissue. The study of, and therapeutic interventions in, such disorders is called rheumatology. The term “rheumatism”, however, does not designate any specific disorder but covers at least 200 different conditions.
Sources dealing with rheumatism tend to focus on arthritis, but “rheumatism” may also refer to other conditions causing chronic pain, grouped as “non-articular rheumatism”, also known as “regional pain syndrome” or “soft tissue rheumatism”. The term “Rheumatic Diseases” is used in MeSH to refer to connective tissue disorders.
Types of Rheumatic Diseases
Many rheumatic disorders of chronic, intermittent joint pain have historically been caused by infectious diseases. Their etiology was unknown until the 20th century and not treatable, like Lyme disease (in the Northern and Northeastern US), coccidiomycosis or Valley fever (in the Western US), and Chikungunya in India and a myriad of causes for postinfectious arthritis also known as reactive arthritis like, for example, the once very common rheumatic fever after Group A Streptococcus infection up to the rare Whipple’s disease.
Major rheumatic disorders currently recognized include
Palindromic rheumatism has been theorized to be a form of rheumatoid arthritis.
Although these disorders probably have little in common in terms of their epidemiology, they do share three characteristics: they cause chronic, often intermittent pain, they are difficult to treat and are collectively very common.
Rheumatic diseases caused by autoimmunity include:
In a 2013 review article, researchers provided a deeper understanding of pain mechanisms in osteoarthritis, systemic lupus erythematosus, and rheumatoid arthritis. Their research suggests that disease-modifying antirheumatic drugs and surgery are unlikely to be effective as sole therapies when central pain versus peripheral pain is suspected in these patients.
The review appears in the January 28, 2013 online issue of Arthritis and Rheumatism.
In many rheumatologic conditions, chronic pain is an ongoing concern that results from the complex interaction of both central and peripheral nervous system signaling. Chronic pain in patients may involve pathology of the peripheral nerves, joints, muscles or skin. Currently, the selection of safe and effective pain therapies remains challenge for rheumatologists, as many of them have not received formal training on pain processing or management.
Led Kristine Phillips, M.D., of the University of Michigan, the goal of this review paper is provide an overview of central pain in the context of rheumatic diseases and to propose future directions for research. Lessons learned from this research will provide a better understanding of pain mechanisms and potentially lead to more personalized approaches to pain managements.
Concept of Centralized Pain
The phrase “central pain” was historically used to describe the condition resulting from individuals who developed pain following a stroke or spinal cord lesion. In these patients, “central” referred to the fact that the lesion leading to pain occurred within the central nervous system or CNS. More recently, the term central pain has expanded to describe any central nervous dysfunction or pathologic condition that contributes to the development or persistence of chronic pain. This new definition also encompasses the patient’s psychosocial aspects of pain perception. Moreover, the concept of centralized pain was originally thought to only apply to people with rare structural causes of pain or idiopathic pain syndromes such as fibromyalgia.
Central Pain Prone Phenotype
Various factors contribute to the development of central pain including, but not limited to:
genetics
early life trauma
the family history of mood disturbances
family history of chronic pain
a personal history of chronic centrally-mediated symptoms such as fatigue or sleep disturbance
cognition
low pain threshold
female sex
Centralized Pain in Rheumatic Diseases
It is estimated that 15-30% patients with rheumatic diseases also have fibromyalgia, which is much higher than the rate of fibromyalgia in the general population (~2%). This suggests that chronic rheumatoid arthritis may be a trigger for fibromyalgia.
Regarding osteoarthritis, the condition causes damage to bones and cartilage. This damage and inflammation of related structures is thought to predict pain symptoms. It is hypothesized that central factors (vs. peripheral factors) may play a critical role in the development of pain in osteoarthritis patients, which is further exacerbated by somatic symptoms such as poor sleep.
Fibromyalgia is suspected to be comorbid with systemic lupus erythematosus, a relationship that confounds the treatment and timely diagnosis of lupus. Surprisingly, the inflammation and damage from lupus are not the main culprits of pain in these patients, but rather the presence or absence of fibromyalgia. Fibromyalgia tends to occur in about 20% of patients with systemic lupus erythematosus.
Finally, in contrast to osteoarthritis and fibromyalgia, rheumatoid arthritis is characterized by systemic inflammation. Pain management in rheumatoid arthritis patients does not necessarily improve with disease-modifying antirheumatic drugs, as these drugs target peripheral pathways. To the contrary, some evidence suggests that there are deficits in central pain processing in rheumatoid arthritis patients, which has implications for proper pain management.
“Centrally targeted therapies have the potential to change the treatment of chronic pain in many diseases. Several classes of centrally acting agents (e.g., tricyclics, SSNRIs, gabapentinoids) may prove to be more effective in individuals with rheumatic disorders who have a central pain overlay than classes of drugs that are typically more effective for peripherally based nociceptive pain states (e.g., NSAIDs), but additional studies are needed to prove this. Newly developed pain cohort studies should identify these subsets of RA, SLE, and OA patients who are preferentially predisposed to respond to these centrally, in addition to peripherally acting treatments, including nonpharmacologic therapy,” wrote Phillips and colleagues.
Strategies for prevention of CVD in patients with rheumatic diseases
Preventive strategy
Suggested interventions
References
Achieve target levels for traditional risk factors including blood pressure, glucose, and lipids
Regular screening, counseling and pharmacotherapy according to guidelines
Autonomic nervous system (ANS), formerly the vegetative nervous system, is a division of the peripheral nervous system that supplies smooth muscle and glands, and thus influences the function of internal organs. The autonomic nervous system is a control system that acts largely unconsciously and regulates bodily functions such as the heart rate, digestion, respiratory rate, pupillary response, urination, and sexual arousal. This system is the primary mechanism in control of the fight-or-flight response.
Within the brain, the autonomic nervous system is regulated by the hypothalamus. Autonomic functions include control of respiration, cardiac regulation (the cardiac control center), vasomotor activity (the vasomotor center), and certain reflex actions such as coughing, sneezing, swallowing and vomiting. Those are then subdivided into other areas and are also linked to ANS subsystems and nervous systems external to the brain. The hypothalamus, just above the brain stem, acts as an integrator for autonomic functions, receiving ANS regulatory input from the limbic system to do so.
Specific learning objectives for the discussion of the autonomic nervous system include the following:
Explain how various regions of the central nervous system regulate autonomic nervous system function;
Explain how autonomic reflexes contribute to homeostasis;
Describe how the neuroeffector junction in the autonomic nervous system differs from that of a neuron-to-neuron synapse;
Compare and contrast the anatomical features of the sympathetic and parasympathetic systems;
For each neurotransmitter in the autonomic nervous system, list the neurons that release them and the type and location of receptors that bind with them;
Describe the mechanism by which neurotransmitters are removed;
Distinguish between cholinergic and adrenergic receptors;
Describe the overall and specific functions of the sympathetic system;
Describe the overall and specific functions of the parasympathetic system; and
Explain how the effects of the catecholamines differ from those of direct sympathetic stimulation.
Autonomic Nervous System
Up until now we’ve covered everything in this organizational chart below except for the ANS and visceral sensory system, which are highlighted in yellow.
The autonomic nervous system (ANS) is a system of motor neurons that innervate smooth muscle, cardiac muscle and glands.
The autonomic nervous system has two divisions:
Sympathetic and Parasympathetic. They mostly innervate the same structures but cause opposite effects. The sympathetic division mobilizes the body during extreme situations such as exercise, excitement and emergencies. Colloquially known as “fight or flight.” The parasympathetic division controls routine maintenance functions such as to conserve body energy and is colloquially called as “rest and digest.”
To make sense of the picture above, note the following…
A neuron found in the parasympathetic nervous system has:
LONG myelinated axon –> ganglion –> SHORT unmyelinated axon.
A neuron found in the sympathetic nervous system has:
SHORT myelinated axon –> ganglion –> LONG unmyelinated axon.
Now is a good time to make sure we differentiate that the ganglion we are talking about is not the same as the dorsal root ganglia. The “ganglia” in the ANS are motor ganglia made up of cell bodies of motor neurons. The “dorsal root ganglia” is in the sensory-somatic part of the peripheral nervous system and are sensory ganglia made up of cell bodies of sensory neurons. Review the location of the dorsal root ganglia here: CNS:
The Parasympathetic Division
The sacral outflow comes from spinal nerves S2 – S4 and innervates:
2nd half of large intestine (smooth muscle)
Urinary bladder and ureters (smooth muscle)
Reproductive organs/erectile tissues of external genitalia (smooth muscle)
This is what points the penis.
The cranial outflow is made up of CN and this is what they innervate:
III (Oculomotor) – constriction of pupils. The pupil is really just a hole; the absence of light. The iris itself has a smooth muscle inside of it. These muscles are circular. There’s other smooth muscle fibers that run like spoke wheels that dilate the pupils.
IX (Glossopharyngeal) – parotid gland (which is a salivary gland)
X (Vagus) – heart (cardiac muscle), lungs (bronchi smooth muscle), liver/gallbladder (glands), stomach (smooth muscle and secretions), pancreas (gland), small intestine and 1st half of large intestine (smooth muscle and secretions)
The Sympathetic Division (T1 – L2)
Note it does the opposite of parasympathetic :
Pupil dilation
Inhibit tear, nasal mucus, saliva production
Skin blood vessel constriction (shunt blood away from skin and to vital organs)
Sweat
Increase heartrate and bloodflow to heart muscle
Bronchodilation
Liver/gallbladder – release glucose
Inhibit rest of digestive system
Inhibit defecation and urination
Ejaculation
Adrenal Medulla
The adrenal medulla is GIGANTIC. It’s the largest sympathetic ganglia. The cells are made of modified neurons that have short axons and no nerve processes. The adrenal cortex is an endocrine organ and the outer layer is the adrenal cortex while the inner layer is the medulla. When stimulated by preganglionic sympathetic fibers from T8-L1, they secrete large quantities of the excitatory hormones norepinephrine and epinephrine (adrenaline) into nearby capillaries. When these two hormones are released in the blood they amplify all of this fight or flight stuff to give you more energy.
courtesy by Rx
Function
Sympathetic and parasympathetic divisions typically function in opposition to each other. But this opposition is better termed complementary in nature rather than antagonistic. For an analogy, one may think of the sympathetic division as the accelerator and the parasympathetic division as the brake. The sympathetic division typically functions in actions requiring quick responses. The parasympathetic division functions with actions that do not require immediate reaction. The sympathetic system is often considered the “fight or flight” system, while the parasympathetic system is often considered the “rest and digest” or “feed and breed” system.
However, many instances of sympathetic and parasympathetic activity cannot be ascribed to “fight” or “rest” situations. For example, standing up from a reclining or sitting position would entail an unsustainable drop in blood pressure if not for a compensatory increase in the arterial sympathetic tonus. Another example is the constant, second-to-second, modulation of heart rate by sympathetic and parasympathetic influences, as a function of the respiratory cycles. In general, these two systems should be seen as permanently modulating vital functions, in usually antagonistic fashion, to achieve homeostasis. Some typical actions of the sympathetic and parasympathetic systems are listed below.
Sympathetic nervous system
Promotes a fight-or-flight response, corresponds with arousal and energy generation, and inhibits digestion
Diverts blood flow away from the gastro-intestinal (GI) tract and skin via vasoconstriction
Blood flow to skeletal muscles and the lungs is enhanced (by as much as 1200% in the case of skeletal muscles)
Dilates bronchioles of the lung through circulating epinephrine, which allows for greater alveolar oxygen exchange
Increases heart rate and the contractility of cardiac cells (myocytes), thereby providing a mechanism for enhanced blood flow to skeletal muscles
Dilates pupils and relaxes the ciliary muscle to the lens, allowing more light to enter the eye and enhances far vision
Provides vasodilation for the coronary vessels of the heart
Constricts all the intestinal sphincters and the urinary sphincter
Inhibits peristalsis
Stimulates orgasm
Parasympathetic nervous system
The parasympathetic nervous system has been said to promote a “rest and digest” response, promotes calming of the nerves return to regular function, and enhancing digestion. Functions of nerves within the parasympathetic nervous system include
Dilating blood vessels leading to the GI tract, increasing the blood flow.
Constricting the bronchiolar diameter when the need for oxygen has diminished
Dedicated cardiac branches of the vagus and thoracic spinal accessory nerves impart parasympathetic control of the heart (myocardium)
Constriction of the pupil and contraction of the ciliary muscles, facilitating accommodation and allowing for closer vision
Stimulating salivary gland secretion, and accelerates peristalsis, mediating digestion of food and, indirectly, the absorption of nutrients
Sexual. Nerves of the peripheral nervous system are involved in the erection of genital tissues via the pelvic splanchnic nerves 2–4. They are also responsible for stimulating sexual arousal.
Enteric nervous system
The enteric nervous system is the intrinsic nervous system of the gastrointestinal system. It has been described as “the Second Brain of the Human Body”. Its functions include:
Sensing chemical and mechanical changes in the gut
Regulating secretions in the gut
Controlling peristalsis and some other movements
Neurotransmitters
A flow diagram showing the process of stimulation of adrenal medulla that makes it release adrenaline, that further acts on adrenoreceptors, indirectly mediating or mimicking sympathetic activity.
At the effector organs, sympathetic ganglionic neurons release noradrenaline (norepinephrine), along with other cotransmitters such as ATP, to act on adrenergic receptors, with the exception of the sweat glands and the adrenal medulla:
Acetylcholine is the preganglionic neurotransmitter for both divisions of the ANS, as well as the postganglionic neurotransmitter of parasympathetic neurons. Nerves that release acetylcholine are said to be cholinergic. In the parasympathetic system, ganglionic neurons use acetylcholine as a neurotransmitter to stimulate muscarinic receptors.
At the adrenal medulla, there is no postsynaptic neuron. Instead the presynaptic neuron releases acetylcholine to act on nicotinic receptors. Stimulation of the adrenal medulla releases adrenaline (epinephrine) into the bloodstream, which acts on adrenoceptors, thereby indirectly mediating or mimicking sympathetic activity.
Sever’s Disease another name known as calcaneal apophysitis is an inflammation of the growth plate in the heel of growing children, typically adolescents. The condition presents as pain in the heel and is caused by repetitive stress to the heel and is thus particularly common inactive children.
Sever’s Disease or calcaneal apophysitis, is a common cause of heel pain in the skeletally immature athlete due to overuse. The overuse injury to the secondary ossification center is thought to be caused by a traction apophysitis at the heel, correlating with the Achilles tendon insertion site. Thus, the condition often coincides with the onset of a pediatric/adolescent patient’s rapid growth spurt or a sudden increase in sports-related activity. The latter is appreciated in sports requiring repetitive running and/or jumping.[rx][rx]
Pathophysiology
www.rxharun.com
The calcaneal apophysis develops as an independent center of ossification (possibly multiple). It appears in boys aged 9-10 years and fuses by age 17 years; it appears in girls at slightly younger ages. During the rapid growth surrounding puberty, the apophyseal line appears to be weakened further because of increased fragile calcified cartilage.
Microfractures are believed to occur because of shear stress leading to the normal progression of fracture healing. This theory explains the clinical picture and the radiographic appearance of resorption, fragmentation, and increased sclerosis leading to eventual union. The radiographs showing fragmentation of the apophysis are not diagnostic, because multiple centers of ossification may exist in the normal apophysis, as noted. However, the degree of involvement in children displaying the clinical symptoms of Sever disease appears to be more pronounced.
In a study of 56 male students from a soccer academy, of whom 28 had Sever disease and 28 were healthy control subjects, findings suggested that higher heel plantar pressures under dynamic and static conditions were associated with Sever disease, though it was not established whether the elevated pressures predisposed to or resulted from the disease.Gastrocnemius ankle equinus also appeared to be a predisposing factor.
Who Gets Sever’s Disease?
Sever’s disease is common and typically occurs during a child’s growth spurt, which can occur between the ages of 10 and 15 in boys and between the ages of 8 and 13 in girls. Feet tend to grow more quickly than other parts of the body, and in most kids, the heel has finished growing by the age of 15. Being active in sports or participating in an activity that requires standing for long periods can increase the risk of developing Sever’s disease. In some cases, Sever’s disease first becomes apparent after a child begins a new sport, or when a new sports season starts. Sports that are commonly associated with Sever’s disease include track, basketball, soccer, and gymnastics.
Children who are overweight or obese are also at a greater risk of developing this condition. Certain foot problems can also increase the risk, including:
Overpronating – Kids who overpronate (roll the foot inward) when walking may develop Sever’s disease.
Flat foot or high arch – An arch that is too high or too low can put more stress on the foot and the heel, and increase the risk of Sever’s disease.
Short leg – Children who have one leg that is shorter than the other may experience Sever’s disease in the foot of the shorter leg because that foot is under more stress when walking.
Presentation
Heel pain, usually in young physically active individuals, which is
Gradual in onset and worse on exercise, especially running or jumping.
Relieved by rest.
Often bilateral.
Ask specifically about
The nature of the pain.
Aggravating or relieving factors.
History of trauma.
Physical activities – sports, dance, etc
How often do you train?
How often do you compete?
At what level?
Type of shoes normally worn.
Any other medical conditions or medications.
On examination, the typical signs are
Tenderness on palpation of the heel – particularly on deep palpation at the Achilles tendon insertion.
Pain on dorsiflexion of the ankle – particularly when doing active toe raises; forced dorsiflexion of the ankle is also uncomfortable.
Swelling of the heel – usually mild.
Calcaneal enlargement – in long-standing cases.
Carefully examine the whole foot and ankle because Sever’s disease may be associated with other foot abnormalities such as flat feet or high arches.
Factors That Contribute
Tight calf muscles
High levels of sports participation (Involving ballistic movements e.g. Jumping, sprinting etc.).
The diagnosis is clinical and investigations are not routinely required. However, investigation to look for other causes is suggested if
Pain is persistent or significant at rest.
Pain disturbs sleep.
There is significant swelling.
There is a reduction of subtalar movement (suggests tarsal coalition).
Possible tests
X-ray of the heel may show increased sclerosis and fragmentation of the calcaneal apophysis – but these features are nonspecific and it may be normal.T he value of X-ray is to exclude a fracture or a rare tumor. The diagnosis is clinical, not radiological.
Radiographs
diagnosis is clinical as there is no established diagnostic criteria
sclerosis can be present in both patients with and without calcaneal apophysitis
fragmentation is more frequently seen in patients with Sever’s disease
helpful to rule out other causes of heel pain (osteomyelitis, calcaneal bone cysts)
MRI
can help localize inflammation to the apophysis
can rule out disorders of the body of the os calcis (stress fracture, lytic lesion, osteomyelitis)
Other
a bone scan can show increased uptake at the apophysis but is typically not helpful in diagnosis symptoms of Sever’s disease
A few signs and symptoms point to Sever’s disease, which may affect one or both heels. These include:
Pain at the heel or around the Achilles tendon
Heel pain during physical exercise, especially activities that require running or jumping
Worsening of pain after exercise
A tender swelling or bulge on the heel that is sore to touch
Calf muscle stiffness first thing in the morning
Limping
A tendency to tiptoe.
Swelling in the heel
Redness in the heel
Antalgic gait (such as limping)
Foot pain or stiffness first thing in the morning or while walking
Pain that is worsened by squeezing the heel
Treatment of Sever’s Disease
Treatment for Sever’s disease is mainly supportive, to stop inflammation and reduce pain. The condition will resolve on its own when the growth in the growth plate is complete, but until then, measures can be taken to resolve pain and discomfort.
Rest – Resting the foot and discontinuing sports and other activities until the pain and stiffness are resolved may be recommended. In extreme cases, a walking boot or a cast might be used to completely immobilize the foot.
Icing – Applying ice to the painful or swollen areas on the foot may provide some short-term relief from pain and prevent further inflammation. Ice can be applied for about 20 minutes two or three times a day. This may also include holding out of sport/practice until symptoms subside. Orthotic use/casting Patient-specific treatment protocols should be dictated as necessary by the treating clinician. Immobilization including periods of casting or use of a CAM boot may be necessary depending on symptom severity. Heel cups or heel pads
Supportive footwear – Footwear that is too big, too small, or does not provide proper support can exacerbate the symptoms of Sever’s disease. Supportive footwear is important to prevent discomfort, especially in children who participate in sports and activities that take place on a hard surface (such as pavement or a basketball court). Shoes should also have adequate padding and not rub against the heel. In some cases, shoes that do not have heels (such as sandals) may be more comfortable to wear while the heel is healing, but care should be taken that the shoe provides proper support to the rest of the foot. Children with Sever’s disease should avoid going barefoot.
Treating foot conditions – Children with flat feet, high arches, or over-pronation may need treatment to resolve these underlying conditions. In many cases, an orthotic worn inside the shoe can help put the foot into better alignment and provide relief to the foot or the arch.
Losing weight – Children who are overweight or obese may be counseled to lose weight. Being overweight can contribute to the development of several conditions, including Sever’s disease.
Stretching – A physical therapist may recommend stretching exercises for the muscles in the calf and the Achilles tendon. A stretching routine is usually done several times a day. Stretching these muscles can help improve strength and decrease the stress on the heel plate.
Changing footwear – Cleats are a major source of pain. Avoiding cleats or getting a more supportive or cushioned pair can be helpful. People with flat feet should consider certain types of shoes for pronation control and people with high arches should look into those designed for neutral distribution.
Orthotics and inserts – Gel heel pads can help with the symptoms. In most cases, commercially available arch supports can be helpful. For more extreme conditions, such as severe flatfoot or high arches, a custom orthotic is recommended. Orthotics and inserts are about comfort and often there is some trial and error required to find the right one.
Compression stockings – are often supportive and help with the pain.
Cross-training and activity reduction – Limiting organized athletics to 3-4 hours per week can make a huge difference, even if it means cutting back on the schedule of weekly physical activities. Cross-training – participating in activities that use different muscle groups and physical motions can also help decrease the risk of pain.
Anti-inflammatory medications – Some physicians may recommend over-the-counter pain relievers such as ibuprofen or acetaminophen. Care must be taken when administering these medications to children, especially with acetaminophen, as overdoses are possible when using more than one medication containing acetaminophen. Aspirin should never be given to children. The utility of pain relievers in children must be weighed against their possible side effects.
Correcting unequal leg length – For small variations—less than an inch or so—shoe lifts can help equalize the length of the legs. In cases with more variation between legs, surgical solutions may be considered.
Taping – The use of taping alone [rx] was only reported in one pre-post intervention, (n = 10) case series. This modality was reported by the authors to be effective in the acute and immediate (no time frame was reported) relief of pain with p = 001. The measurement of pain was by an 11-point ordinal scale with 0 representing ‘absolutely no pain’ and 10 representing ‘worst imaginable pain’. The wording of the pain question was not provided so it is unclear which domain within the construct of pain was being measured. The use of padding and strapping was utilized [rx] in one case series, (n = 11) where n = 5 had a diagnosis of calcaneal apophysitis. The authors reported this modality to be effective in decreasing pain during and post-activity across a time period of 1 month with p = <0.01. As this study also included adults who had posterior heel pain, the resultant pain relief from this treatment should be cautiously regarded.
Concurrently applied therapies – Many authors also incorporated strategies to both minimize inflammation i.e. icing and active rest, together with the minimization of the proposed biomechanical contributing factors i.e. gastrocnemius and soleus static stretch as standard, usual care treatments. No studies were identified that examined these modalities as isolated treatment entities. It is not known whether the concurrent application of these treatment approaches when investigating other treatment modalities introduces treatment effect-diluting or moderating (interaction) effects.
Heel lifts – The use of heel lifts was reported in many of the studies [rx]. All of the studies reported that heel lifts decreased pain, though many of them used these concurrently with other treatment modalities such as stretching and ice [rx] and were unable to provide results regarding the heel raises’ efficacy alone.
Sever’s disease is ultimately a self-limiting condition that resolves with maturation and closure of the apophysis.
Footwear should be well-maintained and up-to-date. A rehabilitation regimen is essential and should include heel cord stretching in addition to dorsiflexor strengthening. If the pain does not respond to conservative measures, a walking boot or short leg cast may be used for short-term immobilization. Symptoms are usually self-limited with improvement within 6 to 12 months and a complete resolution with apophyseal closure. There is no role for injection therapy or surgical intervention in the treatment of Sever’s disease. There are no long-term complications, and the prognosis is excellent.[rx]
Physical Therapy Management for Sever’s Disease
The practitioner should inform the patient and the patient’s parents that this is not a dangerous disorder and that it will resolve spontaneously as the patient matures (16-18 years old). Treatment depends on the severity of the child’s symptoms. The condition is self-limiting, thus the patient’s activity level should be limited only by pain. Treatment is quite varied.
Treatment
Relative Rest/ Modified rest or cessation of sports.
Cryotherapy.
Stretching Triceps Surae and strengthen extensors.
Nighttime dorsiflexion splints (often used for plantar fasciitis, relieve the symptoms and help to maintain flexibility).
Plantar fascial stretching
Gentle mobilizations to the subtalar joint and forefoot area.
Heel lifts, Orthoses (all types, heel cups, heel foam), padding for shock absorption or strapping of heel: to decrease impact shock.
Electrical stimulation in the form of Russian stimulation sine wave modulated at 2500 Hz with a 12 second on time and an 8 second off time with a 3-second ramp.
Advise wearing supportive shoes.
Ultrasound, nonsteroidal anti-inflammatory drugs.
Casting (2-4 weeks) or Crutches (sever cases): symptom control.
Corticosteroid injections are not recommended.
Ketoprofen Gel as an addition to treatment.
Symptoms usually resolve in a few weeks to 2 months after therapy is initiated.
In order to prevent calcaneal apophysitis when returning to sports (after successful treatment and full recovery), icing and stretching after activity are most indicated.
Respectable opinion and poorly conducted retrospective case series make up the majority of evidence on this condition. The level of evidence for most of what we purport to know about Sever’s disease is at such a level that prospective, well-designed studies are a necessity to allow any confidence in describing this condition and its treatment.
Prevention
Maintain good flexibility through stretching exercises
Avoid excessive running on hard surfaces
Use quality, well-fitting shoes with firm support and a shock-absorbent sole
Elevating the heel
By stretching hamstring and calf muscles 2–3 times daily
Ankylosing spondylitis (Bechterew’s disease or Marie Struempell disease as it is also known) (AS) is a chronic progressive inflammatory arthropathy or seronegative spondyloarthropathy or inflammatory form of arthritis that causes vertebrae in the spine to fuse together. This limits flexibility in the spine and may cause a person to have a hunched-forward posture. It is a form of chronic, degenerative arthritis that affects the spine and sacroiliac joints and often other joints of the body.
Ankylosing spondylitis is a chronic inflammatory rheumatic disorder that primarily affects the axial skeleton. Sacroiliitis is its hallmark, accompanied by inflammation of the entheses (points of union between tendon, ligament, or capsule and bone) and formation of syndesmophytes, leading to spinal ankylosis in later stages. The pathogenesis of AS is poorly understood. [Rx]However, immune-mediated mechanisms involving human leucocyte antigen (HLA)-B27, inflammatory cellular infiltrates, cytokines (for example, tumor necrosis factor α and interleukin 10), and genetic and environmental factors are thought to have key roles. The detection of sacroiliitis by radiography, magnetic resonance imaging, or computed tomography in the presence of clinical manifestations is diagnostic for AS, although the presence of inflammatory back pain plus at least two other typical features of spondyloarthropathy (for example, enthesitis and uveitis) is highly predictive of early AS. Non-steroidal anti-inflammatory drugs (NSAIDs) effectively relieve inflammatory symptoms and are presently first line drug treatment.[Rx]
Ankylosing Spondylitis Meaning
The word ankylosing means fusion and the word spondylitis means inflammation of the joints of the spine. Inflammation within the spine and sacroiliac joints develops which also triggers the development of bony growths which often fuse the vertebrae causing pain and stiffness. It is a form of chronic, degenerative arthritis that affects the spine and sacroiliac joints and often other joints of the body. The cause is currently unknown although there is a hereditary factor.
Ankylosing Spondylitis is one of a group of arthritis conditions known as spondyloarthritides, including psoriatic, colitic and reactive arthritis. AS can occur in isolation or in conjunction with any of these conditions, as well as Crohn’s disease, psoriasis, and osteoporosis.
No two cases of AS are exactly the same. Variations occur in the distribution of pain, stiffness, inflammation and in the length of flare-ups and course of the disease. In some cases, the disease becomes less active and pain may cease altogether.
Anatomy of Ankylosing Spondylitis
Ankylosing spondylitis is a systemic disease, meaning it can affect the entire body in some people. It can cause fever, loss of appetite, and fatigue, and it can damage other organs besides the joints, such as the lungs, heart, and eyes. Most often though, only the low back is involved.
The articulation mechanisms between any two vertebrae and the connecting soft tissues form what is called the motion segment. The anterior and posterior longitudinal ligaments connect the vertebral bodies. The intervertebral disc consists of an external fibrous ring, the annulus fibrosus, and a gelatinous core, the nucleus pulposus. On each side of the vertebral arch, the laminae of the upper and lower vertebrae are joined by a ligament flavum. There is a spinous process at the junction of the two laminae. The interspinous ligament joins the spinous processes of the upper and lower vertebrae, and the supraspinous ligament connects their tips. The zygapophyseal joints (facet joints) form between the superior articular process of the lower vertebra and the inferior articular process of the upper vertebrae[Rx].
Anatomy of sacroiliac joints
The sacroiliac (SI) joint is a strong diarthrodial weight-bearing compound joint. It consists of an anterior synovial joint (between the articular surfaces of the sacrum and ilium), whose irregular interlocking surfaces are covered with articular cartilage as well as a posterior syndesmosis located between the tuberosities of these bones. The SI joint has unique characteristics not typically found in other diarthrodial joints. These characteristics include the presence of fibrocartilage in addition to hyaline cartilage, discontinuity of the posterior capsule, many ridges and depressions in the articular surfaces, and limited range of mobility compared to other synovial joints. Three main ligaments stabilize the SI joint: The thin anterior SI ligament, the thick interosseous ligament lying deep between the tuberosities of the sacrum and ilium, which is critically involved in transmitting weight from the sacrum to the iliac bones, and the posterior SI ligament, which is the external continuation of the same mass of fibrous tissue[2,Rx]. Histological examination reveals rich innervation of the SI joint as well as the presence of free nerve fibers within the joint capsule and the adjoining ligaments[Rx].
Ankylosing Spondylitis is usually diagnosed during the second to fourth decade of life. It is more common in first degree relatives of those with Ankylosing Spondylitis. While a strong affiliation with the HLA-B27 antigen supports a genetic predisposition, the evidence suggests that other factors also play a role in susceptibility to Ankylosing Spondylitis. The HLA-B27 antigen is a generic maker found in 8% of North Americans of European (white) heritage. Of those who are HLA-B27 positive, the actual risk of developing Ankylosing Spondylitis is estimated to be 1 to 2 %. Only 20% of HLA-B27 positive first degree relatives of individuals with Ankylosing Spondylitis and who are positive for HLA-B27 will develop the disease.
Causes of Ankylosing Spondylitis
The exact cause of ankylosing spondylitis is unclear. It is thought to be an autoimmune disease – where the body’s own immune system attacks the body’s tissues causing inflammation and tissue damage.
Genetic (inherited) factors appear to influence the development of AS. Approximately 90% of people diagnosed with AS have a gene called HLA-B27. However, only about 10 – 15% of people with the gene will go on to develop AS. Approximately one in five individuals with AS also has a relative with the condition.
Causes And / Or Aggravation
The information cited below is not binding. Each case should be adjudicated on the evidence provided and its own merits.
Idiopathic
The precise etiology is unclear.
Genetic
Although the precise cause of Ankylosing Spondylitis is unknown, there is a strong genetic component, i.e. HLA-B27.
Significant physical trauma – aggravation only
Significant physical trauma will produce aggravation only on the site that is affected by significant physical trauma.
For significant physical trauma to produce aggravation of Ankylosing Spondylitis, the following should be evident
Significant physical trauma must occur in an area of the body where Ankylosing Spondylitis is active;
Increased signs/symptoms of Ankylosing Spondylitis must be present on a continuous or recurrent basis for at least 6 months.
Significant physical trauma is a discrete injury that causes, within 24 hours of the injury being sustained, the development of acute symptoms and signs for which medical attention would normally or reasonably be sought.
Inability to obtain appropriate clinical management
Medical conditions which are to be included in entitlement / Assessment
Symptoms of ankylosing spondylitis may initially be limited to lower back or joint aching, which is often just put down to ‘aches and pains’ and ‘growing pains’ in young people. Symptoms come and go and will usually progress to include the following:
Stiffness and pain in the morning affecting the sacroiliac joint area and spine.
Early diagnosis of AS is important if fusion of the joints and permanent stiffening of the spine are to be avoided. It can be difficult to diagnose in the early stages as symptoms may be attributed to more common causes of back pain. A doctor will evaluate the following when diagnosing the condition
A full medical history, including any family history of AS
Discussion of current symptoms including a history of back pain
The age of the patient when the pain started
Physical assessment
Bamboo spine- Bamboo spine is a radiographic feature seen in ankylosing spondylitis that occurs as a result of vertebral body fusion. It is often accompanied by fusion of the posterior vertebral elements as well and resembles a bamboo stem…therefore the term bamboo spine.
Schober’s test – The Schober’s test is a useful clinical measure of flexion of the lumbar spine performed during the physical examination.
A number of imaging abnormalities, especially those affecting the spine and sacroiliac joints, are characteristic of AS. In fact, according to the Assessment of Spondyloarthritis International Society (ASAS) 2009 axial SpA criteria, evidence of sacroiliitis on imaging (radiographic or MRI) is a major inclusion criteria for AS. A standardized plain radiographic grading scale exists for sacroiliitis, which ranges from normal (0) to most severe (IV), as detailed below.
0: Normal SI joint width, sharp joint margins
I: Suspicious
II: Sclerosis, some erosions
III: Severe erosions, pseudo dilation of the joint space, partial ankylosis
IV: Complete ankylosis
In the first few years of AS, plain radiographic changes in the SI joints can be very subtle, but within the first decade will usually become more obvious. Subchondral erosions, sclerosis, and joint fusion are the most obvious abnormalities, and these radiographic changes are typically symmetric.
These diagnostic criteria include
Inflammatory Back Pain
Chronic, inflammatory back pain is defined when at least four out of five of the following parameters are present-
Age of onset below 40 years old,
Insidious onset,
Improvement with exercise, or not?
no improvement with rest
pain at night (with improvement upon getting up)
Past history of inflammation in the joints, heels, or tendon-bone attachments
A drawback of X-ray– diagnosis is the signs and symptoms of AS have usually been established as long as 8–10 years prior to X-ray-evident changes occurring on a plain film X-ray, which means a delay of as long as 10 years before adequate therapies can be introduced. Options for earlier diagnosis are tomography and MRI of the sacroiliac joints, but the reliability of these tests is still unclear.
Genetic testing – Variations of the HLA-B gene increase the risk of developing ankylosing spondylitis, although it is not a diagnostic test. Those with the HLA-B27 variant are at a higher risk than the general population of developing the disorder. HLA-B27, demonstrated in a blood test, can occasionally help with diagnosis, but in itself is not diagnostic of AS in a person with back pain. Over 90% of people that have been diagnosed with AS are HLA-B27 positive, although this ratio varies from population to population (about 50% of African Americans with AS possess HLA-B27 in contrast to the figure of 80% among those with AS who are of Mediterranean descent
In order for a diagnosis of AS to be made, a referral to a rheumatologist – who specializes in treating arthritis – may be recommended.
Treatment of Ankylosing Spondylitis
Non-Surgical Treatment
Bed rest for first 24 hours. Additional bed rest will be determined by the severity of the problem. Recent medical studies indicate that staying more active is better for back disorders than prolonged bed rest.
Use a firm mattress (place a bed board under the mattress if needed).
Massage may help. Be sure the person is well-trained or massage could cause more harm than help.
Wear a special back support device.
Other options are available depending on the degree of injury, such as surgery (if disk damaged), electrical nerve stimulation, acupuncture, special shoes, etc.
Stress reduction techniques, if needed.
Non-Prescription Pain Relievers – Naproxen, acetaminophen, and ibuprofen each reduce inflammation and pain. Though these drugs are available over-the-counter, they are potent and taking more than the recommended dose can harm health. A doctor can help with advice about the right kind of non-prescription pain reliever to take.
Cold and Heat – Applying a cold pack to the painful part of the back contracts inflamed muscle and relieves pain. This treatment helps a great deal when the disk has recently ruptured and swelling is at its greatest. A heating pad or warm pack helps with residual pain.
Continued Physical Activity – Though pain or weakness seem like good reasons to rest the back, excessive bed-rest worsens the symptoms of a slipped disc. Moving around too little allows muscles to grow weaker and prevents the body from healing. Periods of rest interspersed with periods of normal activity throughout the day keep the back muscles in shape.
Prescription Remedies – If over-the-counter drugs fail to ease slipped disc pain, the doctor will turn to prescription medications. These can include narcotics, such as hydrocodone or codeine. While they can do away with pain, narcotics are very addictive and induce a mental fogginess that can itself be dangerous. More narrowly-focused medicines designed to target damaged nerves that create chronic pain may be a better choice, as they have fewer undesirable side effects. Gabapentin and Cymbalta are two drugs that act in different ways to minimize nerve pain. These drugs are less addictive than narcotics.
Nutrition – In order to restore the disc we also are going to need to include different substances in our diet. There are a lot of supplements on the market, of course. If you wish to try them, that’s fine. I personally don’t like them. I have tried one with glucosamine and chondroitin, but I didn’t feel any different. So, if you have the opportunity to take these with the food or from more natural sources, it will be great. You can find these substances in seafood and animal cartilages and by digesting them we ensure the building blocks for the connecting tissue for our joints and spine. Also, we will need more Omega 3 fatty acids, which can be supplied from cold pressed oils, fatty fish, flax seeds, chia and many more. Vitamins from the B group are very beneficial for people with herniated discs and all kinds of issues with the peripheral nervous system. Vitamins B1, B6 and B12 nourish the nerves and help them recover from the disk accident. Usually, doctors prescribe them as a part of the treatment, but it is worth mentioning anyway.
A good massage – A massage is one of the natural methods of relieving pain. Individuals who get a massage weekly for several months stand a better chance of alleviating back pain. A good massage provides a person with many health benefits that lessen back pain. A massage triggers the release of endorphins. Endorphins aid in decreasing anxiety and relieving pain. They offer a relaxation effect by softening muscles that are injured preventing cramping.
Undertaking yoga – Yoga is an applicable strategy for keeping the level of back pain at minimal levels. Taking yoga sessions often is very an effective method of dealing with back pain. With yoga, there is a high likelihood of proper body functions. The use of pain prescriptions is also diminished. Patients suffering from back pain related issues do not have to rely on these prescriptions to manage pain. Incorporating laughter in yoga is a good way of exercising. Yoga incorporates simple yet appropriate exercises that enhance the stretching of muscles. Laughter with yoga stimulates relieving of pain. It facilitates increased uptake of oxygen, little anxiety, and production of endorphins. All these variables play an essential role in diminishing back pain.
Adjusting sleeping position – A simple sleeping mistake can immensely contribute to back pain. A poor sleeping position can cause stress and tension on the muscles contributing to back pain. Altering one’s sleeping position and adopting a style that does not exert a lot of stress on the back is a recommended tactic. Nurturing sleeping habits such as assuming a reclining position, using wedge-shaped cushions and getting adjustable beds from reputable medical institutions are easy techniques to endorse. If a reclining position does not suit an individual, the other two techniques can be embraced.
Heat therapy – Several considerations should be observed when using heat therapy. The right temperature ought to be set so as to ensure a patient does not face risks associated with too much exposure to heat. The key objective should be to ensure enough access to heat to the muscles to yield benefits for the patient. The adoption of heat therapy for easing back pain is determined by the magnitude of pain a person is experiencing. In cases where relatively low back pain is encountered, short heat therapy sessions are recommended. On the other hand, if an individual is experiencing prolonged back pain, long heat therapy sessions are the most applicable.
Taking hot baths – This is a form of heat therapy that aims at relieving back pain. It guarantees permeation of heat into the muscles leading to reduced pain. Many individuals opt for this method since they believe it achieves competent results. Hot baths initiate a fast process of blood supply to stiff neck and back muscles. When this happens, the muscles relax and stretch leading to decreased back pain. To avoid interference with one’s sleeping patterns, a hot bath should be taken several hours before retiring to bed.
Aquatic therapy – This natural technique involves physical therapy in a pool. Individuals get the best out of this therapy by relying on the resistance of water. Consistency in undertaking this therapy is what ascertains getting back pain relief. Integrating aquatic therapy in an individual’s life for the better part of the week enhances the reduction of back pain quickly.
Enlighten others – Individuals have the power to devise their own natural strategies that aid them in coping with back pain. The strategies can also be a good remedy for others going through similar circumstances. An individual can use social media platforms to equip others with important tips on how to keep back pain at bay. Further, becoming a member of associations that address back pain issues enables better communication of the knowledge gained from personal experience.
The major types of medications used to treat ankylosing spondylitis are pain-relievers and drugs aimed at stopping or slowing the progression of the disease. All of these have potentially serious side effects. Pain-relieving drugs come in two major classes:
Nonsteroidal anti-inflammatory drugs (NSAIDs) – NSAIDs including the Coxib class are the first-line drugs for ankylosing spondylitis. A recent study reported that ankylosing spondylitis is associated with the prostaglandin E receptor 4 (PTGER4) gene. This receptor is associated with bone absorption; NSAIDs inhibit prostaglandin production, thus reducing the absorption12). The mainstay of therapy in all seronegative spondyloarthropathies are anti-inflammatory drugs, which include NSAIDs such as ibuprofen, phenylbutazone, diclofenac,indomethacin,naproxen and COX-2 inhibitors, which reduce inflammation and pain. Indomethacin is a drug of choice. 2012 research showed that those with AS and elevated levels of acute phase reactants seem to benefit most from continuous treatment with NSAIDs.
Analgesics – Acetaminophen and opioid-(like) agents are often used 1) for patients who complain of pain even after administration of NSAIDs and TNF-α inhibitors or 2) when other therapeutic options are not available.
Glucocorticoids – Although local glucocorticoid injection can be considered for skeletal muscle inflammation such as enthesitis, systematic administration of steroids is not generally recommended6)
Antidepressants – such as tricyclics and serotonin and norepinephrine reuptake inhibitors have been commonly prescribed for chronic low back pain, but their benefit for nonspecific low back pain is unproven, according to a review of studies assessing their benefit.
Glucosamine & Diacerein – can be used to tightening the loose tension and regenerate cartilage or inhabit the further degeneration of cartilage.
Corticosteroid- to healing the nerve inflammation and clotted blood in the joints.
Dietary supplement-to remove the general weakness & improved the health.
Muscle Relaxants – If the muscles around the slipped disc experience painful spasms, a muscle relaxant such as Valium may be useful. The drawback to drugs like these is that they do not limit their power to the affected nerve. Instead, they have a generally relaxing effect and will interfere with daily activities. Such as cyclobenzaprine (Flexeril), might be prescribed to relieve the discomfort associated with muscle spasms. However, these medicines might cause confusion in older people. Depending on the level of pain, prescription pain medicines might be used in the initial period of treatment.
Steroids – If inflammation is severe, a doctor may also prescribe a steroid. Steroids, such as cortisone, reduce swelling quickly. A cortisone shot directly in the affected area will have an immediate effect on the displaced disc.
Counter-irritants – such as creams or sprays applied topically stimulate the nerves in the skin to provide feelings of warmth or cold in order to dull the sensation of pain. Topical analgesics reduce inflammation and stimulate blood flow.
Nerve Relaxant — Pregabalin or gabapentin and anti-inflammatory drugs help to relieve pain and stiffness, allowing for increased mobility and exercise. There are many common over-the-counter medicines called non-steroidal anti-inflammatory drugs (NSAIDs). They include aspirin, ibuprofen, and naproxen.
Disease-modifying anti-rheumatic drugs (DMARDs) – Although the administration of DMARDs (e.g., sulfasalazine and methotrexate) is not recommended for axial diseases such as back pain, sulfasalazine is worth considering for treatment of peripheral arthritis Rx. Disease-modifying antirheumatic drugs (DMARDs) such as sulfasalazine can be used in people with peripheral arthritis. For axial involvement, the evidence does not support sulfasalazine.Other DMARDs, such as methotrexate, did not have enough evidence to prove their effectiveness. Generally, systemic corticosteroids were not used due to lack of evidence. Local injection with a corticosteroid can be used for certain people with peripheral arthritis.
TNF-α inhibitors – In 1995, Braun and coworkersrx) isolated TNF-α from ankylosing spondylitis patients via sacroiliac arthrocentesis. Thus, it was recognized that TNF-α is an important inflammatory mediator in this disease, which dramatically facilitated the development of biological agents.
Infliximab (Remicade) – Infliximab is a chimeric monoclonal antibody against TNF-α and is the first developed biological agent, consisting of 75% of human and 25% of mouse sequences rx). This antibody directly binds to TNF-α and neutralizes it. It is administered by intravenous injections at 5 mg/kg body weight. For the first administration, the same dose of infliximab is injected twice with an interval of 2 weeks and then the drug is administered every 6 weeks. Baraliakos et al.Rx reported a drug survival rate (patients who completed 8 years of treatment) of 48% and 88% of partial remission or low disease activity after 8-year follow-up. It was also reported that the potency was similar when the treatment was interrupted for 3 years and then resumed.
Etanercept (Enbrel) – Etanercept is a soluble blocker of TNF-α. This fusion protein binds TNF-α, which hinders interactions between TNF-α and TNF-α receptor located on other cells. Etanercept is generally administered by subcutaneous injection of 25 mg twice a week Rx. Martĺn-Mola et al.Rxreported that 63% of the enrolled patients completed 5 years of etanercept administration without any serious complications, while Baraliakos reported a drug survival rate of 62%, partial remission in 31% of patients, and complete remission in 44% of patients in a 7-year follow-up study. Similar to infliximab, etanercept was effective when the medication was interrupted and then resumed; the drug survival rate was slightly higher in the etanercept group than in the infliximab group.
Adalimumab (Humira) – Like infliximab, adalimumab is a monoclonal antibody against TNF-α but its sequence is 100% human. Adalimumab is administered by subcutaneous injections of 40 mg once per 2 weeks. Sieper et al.Rx reported a drug survival rate of 65%, partial remission according to Ankylosing Spondylitis Disease Activity Score (ASDAS) in 51% of patients, and ASDAS inactive disease in 61% of patients in a 5-years follow-up study. Similar to the long-term follow-up results for infliximab, favorable outcomes of long-term follow-up were demonstrated with remission achieved after 12 weeks of administration.
Anti-tumor necrosis factor therapy —A group of medicines known as anti-tumor necrosis factor agents (anti-TNF agents or TNF inhibitors) are often effective in the treatment of AS. Examples of anti-TNF medications include infliximab, etanercept, adalimumab, certolizumab pegol, and golimumab. People who do not respond to one anti-TNF treatment may respond to another. Improvement in symptoms is common and may occur within a few weeks of starting the drugs.
Who should use anti-TNF therapy? – Not every patient with AS needs anti-TNF therapy. In general, people with the active disease in the spine who have not responded fully to NSAIDs may be candidates (see ‘How do I know how active my ankylosing spondylitis is?’ above). Your clinician may also recommend a glucocorticoid (cortisone-like drug) injection into painful or swollen joints before starting an anti-TNF drug if these areas continue to bother you despite using NSAIDs (see ‘Glucocorticoids (steroids)’ below). The decision to use anti-TNF therapy depends upon several factors that should be discussed with your clinician.
Secukinumab— Secukinumab (brand name: Cosentyx) may be an alternative treatment option for some people who do not respond adequately to anti-TNF therapy.
Glucocorticoids (steroids)— Some clinicians may also recommend a glucocorticoid injection into particularly painful or swollen joints, especially if only one or two areas are causing the most pain. In some cases, a glucocorticoid injection into the sacroiliac joint may help provide relief in patients who have sacroiliac pain that has not responded to other therapies.
Bisphosphonates – Oral bisphosphonates are commonly used for fracture prevention in ankylosing spondylitis. Bisphosphonates also have an anti-inflammatory action and may have an effect on disease activity. Intravenous pulses of the bisphosphonate pamidronate have been investigated in several studies and have produced significant clinical improvements in some but not all studies.rx
Other Medications to Stop Inflammation and Save Your Joints: Biological Drugs
If NSAIDs or DMARDs do not control your AS, your doctor may prescribe drugs called biologics. These drugs aim to address the problems with your immune system. They target your body’s production of specific proteins that cause inflammation.
Biologic drugs slow your immune system to help ease AS symptoms (pain, swelling, tenderness, and stiffness) as well as inflammation. These drugs may also help protect your joints from damage.
You are at higher risk of infections like tuberculosis when you take biologics. If you have signs of an infection, such as a fever or congestion, you should tell your doctor. Your doctor will test you for tuberculosis before you start a biologic drug and while you take it. These drugs also may raise your risk of getting certain types of cancer, but this is rare.
Doctors and scientists are constantly coming up with new ways to treat diseases, and they always need patients to test the efficacy of a proposed intervention. Below, you will find a current list of trials for ankylosing spondylitis and related conditions, as well as a link to enroll. You should speak with your doctor to decide if enrolling in a clinical trial is a good option for you.
Study Title
Description
Link
A Study to Evaluate the Efficacy and Safety of Ustekinumab in the Treatment of A … Show More
A Study Treating Participants With Early Axial Spondyloarthritis (axSpA) Taking … Show More
Condition: Axial Spondyloarthritis Intervention: Biological: Adalimumab; Other: Standard of Care (SOC) Sponsor: AbbVie; Improvement by Movement GmbH, Germany; Hannover Medical School; IST GmbH, Germany Recruiting – verified October 2016
An Efficacy and Safety Study of Ustekinumab in Participants With Active Nonradio … Show More
Condition: Nonradiographic Axial Spondylitis, Ankylosing Intervention: Drug: Group 1: Placebo; Drug: Group 2: Ustekinumab 45 mg; Drug: Group 3: Ustekinumab 90 m
Physical therapy
Though physical therapy remedies have been scarcely documented, some therapeutic exercises are used to help manage lower back, neck, knee, and shoulder pain. Some therapeutic exercises include
Moderate-to-high impact exercises like jogging are generally not recommended or recommended with restrictions due to the jarring of affected vertebrae that can worsen pain and stiffness in some with AS.
Physical therapy and education – The most important component of non-drug treatments of ankylosing spondylitis is the education of patients and regular exercise. Although home exercise is known to be effective, group physical therapy under appropriate supervision is more efficient than individual exercise6). It is important to educate patients that proper exercise not only alleviates pain but also relaxes the joints so that daily life activities are not affected.
Stretching – Stretching helps build flexibility and may reduce pain. Consider adding the spine stretch or the low-back rotation stretch to your daily routine.
Heat therapy – Apply a hot water bottle or heating pad to the affected area to reduce stiffness and pain. You may also use moist or dry heat. A warm bath may also help, especially before exercise. Don’t use heat therapy without consulting your doctor if you have diabetes, deep vein thrombosis, vascular disease, an open wound, or a skin condition such as dermatitis.
Cold therapy – Applying an ice pack, cold gel pack, or a bag of frozen vegetables to painful joints can help reduce swelling. After exercise, cold therapy may help reduce inflammation. Don’t apply ice for more than 20 minutes at a time. Don’t use cold therapy without consulting your doctor if you have circulation problems.
Acupuncture – Acupuncture is an ancient remedy for pain. It involves inserting thin needles into specific points in your skin. This is thought to activate your body’s pain-relieving hormones. Some people report acupuncture relieves AS pain.
Massage therapy – Massage helps you relax. It may also help you feel more flexible or “loose” so that you can exercise or stretch. Massage may cause pain at tender points around your spine. If this happens, avoid those areas and only use light massage techniques until the pain improves.
Movement – The more you sit, the stiffer you’re likely to feel. Get up, move around, and stretch regularly. If you have a desk job, take a “get up and move” break every hour.
Exercise – Gentle exercise programs such as yoga and Pilates are great for AS because they incorporate stretching. Swimming may also be beneficial because it’s easy on your joints. Strengthening exercises with weights can help build muscle, which supports joints affected by AS.
Alexander Technique – AS often leaves you hunched over. Practicing good posture is critical. The Alexander Technique teaches you to be aware of your posture throughout your day. It also teaches you how to correct poor posture and may be helpful for people with AS.
TENS Therapy – TENS stands for transcutaneous electrical nerve stimulation. This therapy uses electrical current to stimulate nerves through the body for pain control. Electrodes are usually applied at the pain site and connected to a TENS machine. It’s thought that when TENS stimulates nerves, it overrides pain signals. The TENS technique is usually taught by a physical therapist and may be continued at home.
Stop smoking – Smokers, especially men, are at risk for greater spine damage from AS than non-smokers. Quitting smoking not only helps reduce AS damage but also improves your overall health.
Physiotherapy – In spondylosis (spinal osteoarthritis), your spinal joints don’t move as well as they used to because of age-related changes in your spine, similar to arthritis. This can make it very painful to move because of decreased mobility within the spine itself. Your doctor may recommend physical therapy as part of your treatment plan because a physical therapist can help you maintain and increase mobility, learn ways to reduce pain, strengthen your spinal muscles so that they better support your spine, and stretch muscles that may be increasing nerve compression in your spine.
Physical therapy involves three main components: education, passive treatments, and active treatments. A physical therapist uses passive treatments to relax you and your body and to decrease acute pain or inflammation. They’re called passive because you don’t have to actively participate. If you’re experiencing acute pain, you’ll most likely start with passive treatments as your body heals and/or adjusts to the pain. However, the goal of physical therapy is to get into active treatments. These are therapeutic exercises that strengthen your body so that your spine has better support.
Passive Treatments for Ankylosing Spondylitis
Your physical therapist may give you passive treatments such as:
Deep Tissue Massage – This technique targets spasms and chronic muscle tension that perhaps builds up through daily life stress. You could also have spasms or muscle tension because of strains or sprains. The therapist uses direct pressure and friction to try to release the tension in your soft tissues (ligaments, tendons, muscles).
Hot and Cold Therapies – Your physical therapist will alternate between hot and cold therapies. By using heat, the physical therapist seeks to get more blood to the target area because an increased blood flow brings more oxygen and nutrients to that area. Blood is also needed to remove waste byproducts created by muscle spasms, and it also helps to heal. Cold therapy, also called cryotherapy, slows circulation, helping to reduce inflammation, muscle spasms, and pain. You may have a cold pack placed upon the target area, or even be given an ice massage. Another cryotherapy option is a spray called fluoromethane that cools the tissues. After cold therapy, your therapist may work with you to stretch the affected muscles.
Electrical stimulation – This can be performed within the clinic and if extremely successful, a TENS unit can be issued to a patient for home use. E-stim stimulates your muscles through variable (but safe) intensities of electrical current. It helps to reduce muscle spasms, and it may increase your body’s production of endorphins, your natural pain killers. It may also drive out inflammation, bring in healing properties, relax, and re-educate the muscles involved. The e-stim unit in the clinic is of a professional standard; the equipment is relatively large. However, a smaller machine for at “at home” use is also available. Electrical stimulation is a helpful therapy.
Yoga – Yoga is a great natural pain reliever for ankylosing spondylitis,” Ostrowski says. “You need to start with very basic poses and be patient, but if you work with an instructor who can modify the yoga positions for you, you can really benefit from this form of exercise.” A review of studies published in January 2016 in the Journal of Orthopedics & Rheumatology examined the impact of yoga on low back pain and found that it was safe and can help reduce both disability and pain.
Omega-3 fats and inflammation – Foods that contain omega-3 fats have been found to help reduce the inflammation associated with some forms of arthritis. These effects are modest compared with medication.
Omega-3 fats have few side effects and may have other health benefits, such as reduced heart disease. Foods rich in omega-3 fats include
fish – the oily fish such as salmon and sardines have greater amounts of omega-3 fats
linseeds and linseed (flaxseed) oil
canola (rapeseed) oil
walnuts
foods fortified with omega-3, such as margarine and eggs
some fish oil supplements.
Potassium Rich Foods
Potassium is known to decrease inflammation if it is present in the body in adequate amounts. Foods that contain potassium in high amounts are bananas, almonds, apricots, and broccoli.
Vitamin D – You must correct the vitamin D deficiency in your body if you are suffering from ankylosis. Bones need Vitamin D in greater amounts when they are affected by a disease.
Home Remedies For Ankylosing Spondylitis
Use Ginger, Black Pepper or any good digestive with your meals. It will help detoxify your body.
1 tablespoonful of Turmeric should be consumed once every day, after boiling it in milk for half an hour.
Constipation must be avoided at all costs. Constipation may increase pain in Ankylosing spondylitis.
Herbs have divine healing powers and they have the ability to cure any disease of the root. They were gifted to us by God when he created life. So believe in God if you want to get rid of your problems!
Ayurvedic herbs are unique natural remedies for Ankylosing spondylitis. Ayurvedic principles are different in many ways From modern medicine for example – Drinking water From a copper pan after keeping it overnight is also very useful in Rheumatoid arthritis and Ankylosing spondylitis.
Consuming castor oil at night with milk or alone is a very useful herbal remedy for arthritis, especially rheumatoid arthritis and ankylosing spondylitis.
Improve your nutrition as the first step. It plays an important role to fight diseases. When nothing works, nutrition works a lot !
Use herbal juices like Aloe vera juice (Kumari Saar) and Amla Juice ( Amla Saar) in routine. Amla is the richest source of natural Vitamin C. Vitamin C improves the natural immunity of the body. 100 gm of Amla juice contains 30 times more vitamin C than 100 gm of oranges.
Homeopathic treatment for Ankylosing Spondylitis
Homeopathy treats the person as a whole. A Remedy is selected after full individualizing examination and case analysis which includes a medical history of the patient, physical and mental constitution etc.
Phosphorus – The rigidity of nape of the neck. Pressure on shoulders. Swelling of the neck. Engorgement of axillary glands and of those of nape of the neck and of the neck. Paralyzes sensation in the upper sacrum and lower lumbar vertebrae. Contusive pain in loins and back (as if the back were broken), especially after having been seated a long time Sensitiveness of spinous processes of dorsal vertebrae to pressure.
Silicea –The stiffness of nape, with a headache. Swelling of glands of nape, in the neck, and under the axillae (with suppuration), sometimes with indurations…Stitches between the hips.Coccyx painful, as after a long carriage ride.- Stinging in os coccyx on rising, painful to pressure. -Scabby elevation on the coccyx, above fissure of nates- Inflammatory abscess in the lumbar region (on the psoas muscle).- Weakness and paralytic stiffness in back, loins, and nape.
Aurum Metallicum – Serious or advanced rheumatism with marked stiffness. Rheumatism with stiffness or spasms of the chest wall. Severe spasm or tearing pains. Pains also described as “paralytic.” An important remedy in ankylosing spondylitis. Wandering arthritis; moving spot to spot from one week to next. Worse: Night. Morning in bed. Hip pain worse rising from a seat or from walking.
Sulfur – The stiffness of the neck, in nape, with a paralytic, sprained pain. A child cannot hold head up neck muscles so weak. Tetters on nape. Swelling and inflammation of glands of nape and of the neck. Swelling and suppuration of axillary glands. Cracking in vertebrae of the neck, especially on bending backward.
Maintain a healthy weight– If you are overweight or obese, the extra load on your joints may be exacerbating your symptoms, especially if your affected joints include those of the hip, knee or spine. There is also a clear link between being overweight and an increased risk of developing osteoarthritis.
Dietary recommendations for ankylosing spondylitis
General dietary recommendations for a person with ankylosing spondylitis:
eat a well-balanced diet, including fruit and vegetables, protein foods, dairy, cereals, and grains. This will help to maintain general good health and a healthy weight
avoid crash dieting or fasting
increase dietary calcium to reduce the risk of osteoporosis in later life
drink plenty of non-alcoholic fluids, especially water
keep your weight within the normal range. Excess body weight increases stress on joints, especially weight-bearing joints like knees and hips.
What can the athlete do?
Keep themselves fit and healthy
Maintain an optimum weight to place as little strain on the spine as possible
Have a good diet
Maintain a good posture and mobility
Avoid sudden twisting and turning movements
Use a heat pack or warm bath to reduce pain and stiffness
Exercise such as swimming can be great for ankylosing spondylitis as it places very little strain on the spine and joints.
Other exercises for mobility and back strength can also be beneficial.
Lumbago is a common disorder involving the muscles, nerves, and bones of the back. Pain can vary from a dull constant ache to a sudden sharp feeling. Low back pain may be classified by duration as acute (pain lasting less than 6 weeks), sub-chronic (6 to 12 weeks), or chronic (more than 12 weeks). The condition may be further classified by the underlying cause as either mechanical, non-mechanical, or referred pain. The symptoms of low back pain usually improve within a few weeks from the time they start, with 40-90% of people completely better by six weeks.
Acute low-back pain without sciatica, with some spread of discomfort to the region of the sacroiliac joint, to the outer part of the buttock as well as to the lateral and the back part of the thigh, is a unifying symptom of a very common clinical syndrome whose exact underlying cause remains often uncertain. Most patients fall then into the category of non-specific low-back pain. Probably the pathogenesis is not uniform, and the pain can arise from a variety of structures (muscles, ligament, spine). Pain which persists after 3 to 4 days should warn the clinician that a serious pathological condition may be present which requires a new approach to diagnosis and treatment.
Pain in the lower part of the back is commonly referred to as Lumbago. It can be defined as mild to severe pain or discomfort in the area of the lower back. The pain can be acute (sudden and severe) or chronic if it has lasted more than three months.
Most people will experience lumbago at some point in their life. It is one of the most common reasons people miss work and visit the doctor. It can occur at any age but is a particular problem in younger people whose work involves physical effort and much later in life, in the elderly.
www.rxharun.com
Anatomy of the Low Back
The lumbar spine consists of five vertebrae (L1–L5). The complex anatomy of the lumbar spine is a combination of these strong vertebrae, linked by joint capsules, ligaments, tendons, and muscles, with extensive innervation. The spine is designed to be strong since it has to protect the spinal cord and spinal nerve roots. At the same time, it is highly flexible, providing for mobility in many different planes.
The mobility of the vertebral column is provided by the symphyseal joints between the vertebral bodies, with an IVD in between. The facet joints are located between and behind adjacent vertebrae, contributing to spine stability. They are found at every spinal level and provide about 20% of the torsional (twisting) stability in the neck and low back segments [rx]. Ligaments aid in joint stability during rest and movement, preventing injury from hyperextension and hyperflexion. The three main ligaments are the anterior longitudinal ligament (ALL), posterior longitudinal ligament (PLL), and ligament flavum (LF). The canal is bordered by vertebral bodies and discs anteriorly and by laminae and LF posteriorly. Both the ALL and PLL run the entire length of the spine, anteriorly and posteriorly, respectively. Laterally, spinal nerves and vessels come out from the intervertebral foramen. Beneath each lumbar vertebra, there is the corresponding foramen, from which spinal nerve roots exit. For example, the L1 neural foramina are located just below the L1 vertebra, from where the L1 nerve root exits.
IVDs are located between vertebrae. They are compressible structures able to distribute compressive loads through osmotic pressurization. In the IVD, the annulus fibrosus (AF), a concentric ring structure of organized lamellar collagen, surrounds the proteoglycan-rich inner nucleus pulposus (NP). Discs are avascular in adulthood, except for the periphery. At birth, the human disc has some vascular supply but these vessels soon recede, leaving the disc with little direct blood supply in the healthy adult [rx]. Hence, metabolic support of much of the IVD is dependent on the cartilaginous endplates adjacent to the vertebral body. A meningeal branch of the spinal nerve, better known as the recurrent sinuvertebral nerve, innervates the area around the disc space [rx].
The lumbar spine is governed by four functional groups of muscles, split into extensors, flexors, lateral flexors, and rotators. The lumbar vertebrae are vascularized by lumbar arteries that originate in the aorta. Spinal branches of the lumbar arteries enter the intervertebral foramen at each level, dividing themselves into smaller anterior and posterior branches [rx]. The venous drainage parallels the arterial supply [rx].
Typically, the end of the spinal cord forms the conus medullaris within the lumbar spinal canal at the lower margin of the L2 vertebra [rx]. All lumbar spinal nerve roots stem from the connection between the dorsal or posterior (somatic sensory) root from the posterolateral aspect of the spinal cord and the ventral or anterior (somatic motor) root from the anterolateral aspect of the cord [rx]. The roots then flow down through the spinal canal, developing into the cauda equina, before exiting as a single pair of spinal nerves at their respective intervertebral foramina. Cell bodies of the motor nerve fibers can be found in the ventral or anterior horns of the spinal cord, whereas those of the sensory nerve fibers are in the dorsal root ganglion (DRG) at each level. One or more recurrent meningeal branches, known as the sinuvertebral nerves, run out from the lumbar spinal nerves. The sinuvertebral nerve, or Luschka’s nerve, is a recurrent branch created from the merging of the grey ramus communicans (GRC) with a small branch coming from the proximal end of the anterior primary ramus of the spinal nerve. This polisegmentary mixed nerve directly re-enters the spinal canal and gives off ascending and descending anastomosing branches comprising both somatic and autonomic fibers for the posterolateral annulus, the posterior vertebral body and the periosteum, and the ventral meninges [rx, rx]. The sinuvertebral nerves connect with branches from radicular levels both above and below the point of entry, in addition to the contralateral side, meaning that localizing pain from the involvement of these nerves is challenging [rx]. Also, the facet joints receive two-level innervation comprising somatic and autonomic components. The former convey a well-defined local pain, while the autonomic afferents transmit referred pain.
www.rxharun.com
Causes of Lumbago
The human back is composed of a complex structure of muscles, ligaments, tendons, disks and bones – the segments of our spine are cushioned with cartilage-like pads called disks. Problems with any of these components can lead to back pain. In some cases of back pain, its cause is never found.
Problems with the spine such as osteoporosis can lead to back pain.
Strain – the most common causes of back pain are
Strained muscles
Strained ligaments
A muscle spasm
Things that can lead to strains or spasms include
Lifting something improperly
Lifting something that is too heavy
The result of an abrupt and awkward movement
Structural problems –
Sprains and strains – account for most acute back pain. Sprains are caused by overstretching or tearing ligaments, and strains are tears in tendon or muscle. Both can occur from twisting or lifting something improperly, lifting something too heavy, or overstretching. Such movements may also trigger spasms in back muscles, which can also be painful.
Intervertebral disc degeneration – is one of the most common mechanical causes of low back pain, and it occurs when the usually rubbery discs lose integrity as a normal process of aging. In a healthy back, intervertebral discs provide height and allow bending, flexion, and torsion of the lower back. As the discs deteriorate, they lose their cushioning ability.
Herniated or ruptured discs – can occur when the intervertebral discs become compressed and bulge outward (herniation) or rupture, causing low back pain.
Radiculopathy – is a condition caused by compression, inflammation and/or injury to a spinal nerve root. Pressure on the nerve root results in pain, numbness, or a tingling sensation that travels or radiates to other areas of the body that are served by that nerve. Radiculopathy may occur when spinal stenosis or a herniated or ruptured disc compresses the nerve root.
Sciatica – is a form of radiculopathy caused by compression of the sciatic nerve, the large nerve that travels through the buttocks and extends down the back of the leg. This compression causes shock-like or burning low back pain combined with pain through the buttocks and down one leg, occasionally reaching the foot. In the most extreme cases, when the nerve is pinched between the disc and the adjacent bone, the symptoms may involve not only pain, but numbness and muscle weakness in the leg because of interrupted nerve signaling. The condition may also be caused by a tumor or cyst that presses on the sciatic nerve or its roots.
Spondylolisthesis – is a condition in which a vertebra of the lower spine slips out of place, pinching the nerves exiting the spinal column.
A traumatic injury – such as from playing sports, car accidents, or a fall can injure tendons, ligaments or muscle resulting in low back pain. Traumatic injury may also cause the spine to become overly compressed, which in turn can cause an intervertebral disc to rupture or herniate, exerting pressure on any of the nerves rooted to the spinal cord. When spinal nerves become compressed and irritated, back pain and sciatica may result.
Ruptured disks – each vertebra in our spine is cushioned by disks. If the disk ruptures there will be more pressure on a nerve, resulting in back pain.
Bulging disks – in much the same way as ruptured disks, a bulging disk can result in more pressure on a nerve.
Sciatica – a sharp and shooting pain that travels through the buttock and down the back of the leg, caused by a bulging or herniated disk pressing on a nerve.
Arthritis – patients with osteoarthritis commonly experience problems with the joints in the hips, lower back, knees, and hands. In some cases, spinal stenosis can develop, which is the term used to describe when the space around the spinal cord narrows.
Abnormal curvature of the spine – if the spine curves in an unusual way the patient is more likely to experience back pain. An example is scoliosis, a condition in which the spine curves to the side.
Osteoporosis– bones, including the vertebrae of the spine, become brittle and porous, making compression fractures more likely.
Spinal stenosis – is a narrowing of the spinal column that puts pressure on the spinal cord and nerves that can cause pain or numbness with walking and over time leads to leg weakness and sensory loss.
Skeletal irregularities – include scoliosis, a curvature of the spine that does not usually cause pain until middle age; lordosis, an abnormally accentuated arch in the lower back; and other congenital anomalies of the spine.
Abdominal aortic aneurysms – occur when the large blood vessel that supplies blood to the abdomen, pelvis, and legs becomes abnormally enlarged. Back pain can be a sign that an aneurysm is becoming larger and that the risk of rupture should be assessed.
Kidney stones – can cause sharp pain in the lower back, usually on one side.
Below are some other causes of back pain
Cauda equina syndrome – the cauda equine is a bundle of spinal nerve roots that arise from the lower end of the spinal cord. People with cauda equine syndrome feel a dull pain in the lower back and upper buttocks, as well as analgesia (lack of feeling) in the buttocks, genitalia, and thigh. There are sometimes bowel and bladder function disturbances.
Cancer of the spine – a tumor located on the spine may press against a nerve, resulting in back pain.
Infection of the spine – if the patient has an elevated body temperature (fever) as well as a tender warm area on the back, it could be caused by an infection of the spine.
Other infections – pelvic inflammatory disease (females), bladder, or kidney infections may also lead to back pain.
Endometriosis – is the buildup of uterine tissue in places outside the uterus.
Fibromyalgia – a chronic pain syndrome involving widespread muscle pain and fatigue.
Sleep disorders – individuals with sleep disorders are more likely to experience back pain, compared to others.
Shingles – an infection that can affect the nerves may lead to back pain, depending on the nerves affected.
Bad mattress – if a mattress does not support specific parts of the body and keep the spine straight, there is a greater risk of developing back pain.
Everyday activities or poor posture
Back pain can also be the result of some everyday activity or poor posture. Examples include:
Adopting a very hunched sitting position when using computers can result in increased back and shoulder problems over time.
Bending awkwardly
Pushing something
Pulling something
Carrying something
Lifting something
Standing for long periods
Bending down for long periods
Twisting
Coughing
Sneezing
Muscle tension
Over-stretching
Straining the neck forward, such as when driving or using a computer
Long driving sessions without a break, even when not hunched
Exertion or lifting.
Severe blow or fall.
Back disorders.
Infections.
Ruptured lumbar disk.
Nerve dysfunction.
Osteoporosis.
Spondylosis (hardening and stiffening of the spinal column).
The main symptom of back pain is, as the name suggests, an ache or pain anywhere on
Pain in the back, and sometimes all the way down to the buttocks and legs. Some back issuescan cause pain in other parts of the body, depending on the nerves affected.
In most cases, signs, and symptoms clear up on their own within a short period. If any of the following signs or symptoms accompany back pain, people should see their doctor:
Pain. It may be continuous, or only occur when you are in a certain position. The pain may be aggravated by coughing or sneezing, bending or twisting.
Patients who have been taking steroids for a few months
Drug abusers
Patients with cancer
Patients who have had cancer
Patients with depressed immune systems
Stiffness.
According to the British National Health Service (NHS), the following groups of people should seek medical advice if they experience back pain:
Weight loss
Elevated body temperature (fever)
Inflammation (swelling) on the back
Persistent back pain – lying down or resting does not help
Pain down the legs
Pain reaches below the knees
A recent injury, blow or trauma to your back
Urinary incontinence – you pee unintentionally (even small amounts)
Difficulty urinating – passing urine is hard
Fecal incontinence – you lose your bowel control (you poo unintentionally)
Numbness around the genitals
Numbness around the anus
Numbness around the buttocks
dull ache,
numbness,
tingling,
sharp pain,
pulsating pain,
pain with movement of the spine,
pins and needles sensation,
muscle spasm,
tenderness,
sciatica with shooting pain down one or both lower extremities
People aged less than 20 and more than 55 years
Additionally, people who experience pain symptoms after a major trauma (such as a car accident) are advised to see a doctor. If low back pain interferes with daily activities, mobility, sleep, or if there are other troubling symptoms, medical attention should be sought.
Risk increases with
Biomechanical risk factors.
Sedentary occupations.
Gardening and other yard work.
Sports and exercise participation, especially if infrequent.
Obesity.
Preventive measures
Exercises to strengthen lower back muscles.
Learn how to lift heavy objects.
Sit properly.
Back support in bed.
Lose weight, if obese.
Choose proper footwear.
Wear special back support devices.
Red flag conditions indicating possible underlying spinal pathology or nerve root problemsw9
Red flags
Onset age < 20 or > 55 years
Non-mechanical pain (unrelated to time or activity)
Thoracic pain
Previous history of carcinoma, steroids, HIV
Feeling unwell
Weight loss
Widespread neurological symptoms
Structural spinal deformity
Indicators for nerve root problems
Unilateral leg pain > low back pain
Radiates to foot or toes
Numbness and paraesthesia in same distribution
Straight leg raising test induces more leg pain
Localized neurology (limited to one nerve root)
Diagnosis of Lumbago /Backache
Suspected disk, nerve, tendon, and other problems – X-rays or some other imaging scan, such as a CT (computerized tomography) or MRI (magnetic resonance imaging) scan may be used to get a better view of the state of the soft tissues in the patient’s back.
X-rays – can show the alignment of the bones and whether the patient has arthritis or broken bones. They are not ideal for detecting problems with muscles, the spinal cord, nerves or disks.
MRI or CT scans – these are good for revealing herniated disks or problems with tissue, tendons, nerves, ligaments, blood vessels, muscles, and bones.
Bone scan – a bone scan may be used for detecting bone tumors or compression fractures caused by brittle bones (osteoporosis). The patient receives an injection of a tracer (a radioactive substance) into a vein. The tracer collects in the bones and helps the doctor detect bone problems with the aid of a special camera.
Electromyography or EMG – the electrical impulses produced by nerves in response to muscles is measured. This study can confirm nerve compression which may occur with a herniated disk or spinal stenosis (narrowing of the spinal canal).
[stextbox id=’alert’]
Types of low back pain associated with physical findings of no clear pathoanatomical significance
Syndrome
Findings
Assessment/Plan
Facet syndrome
History and physical examination:
local and pseudoradicular symptoms and signs
pain on movement
facet tenderness
pain on reclination
positive injection test
joint dysfunction on manual diagnosis
Radiological findings (not indicated on initial evaluation):
differentiation from high-grade or activated spondylarthrosis (possibly, juxtaforaminal cyst) or
The differential diagnosis for back pain is very broad, especially when considering the pediatric population. Below is a review of the more common diagnoses along with history or physical exam features that may increase your index of suspicion. This list is not comprehensive but represents the more likely and more concerning conditions that make up the differential.
Presentation: follows traumatic incident or repetitive overuse, pain worse with movement, better with rest, restricted range of motion, tenderness to palpation of muscles
Lumbar spondylosis
Presentation: patient typically is greater than 40years old, pain may be present or radiate from hips, pain with extension or rotation, neurologic exam is usually normal
Disk herniation
Presentation: usually involves the L4 to S1 segments, may include paresthesia, sensory change, loss of strength or reflexes depending on severity and nerve root involved
Spondylolysis, Spondylolisthesis
Presentation: similar to pediatrics, spondylolisthesis may present back pain with radiation to buttock and posterior thighs, neuro deficits are usually in the L5 distribution
Vertebral compression fracture
Presentation: localized back pain worse with flexion, point tenderness on palpation, may be acute or occur insidiously over time, age, chronic steroid use, and osteoporosis are risk factors
Spinal stenosis
Presentation: back pain which can be accompanied with sensory loss or weakness in legs relieved with rest (neurologic claudication), neuro exam normal.
Tumor
Presentation: a history of metastatic cancer, unexplained weight loss, focal tenderness to palpation in the setting of risk factors
Clinical note: 97% of spinal tumors are metastatic disease; however, the provider should keep multiple myeloma in the differential
Presentation: Spinal procedure within the last 12 months, Intravenous drug use, Immunosuppression, prior lumbar spine surgery, fever, wound in spinal region, localized pain, and tenderness
Clinical note: Granulomatous disease may represent as high as one-third of cases in developing countries.
Fracture
Presentation: Significant trauma (relative to age), Prolonged corticosteroid use, osteoporosis, and age greater than 70 years, Contusions, abrasions, tenderness to palpation over spinous processes
Clinical note: Osteoid osteoma is the most common tumor that presents with back pain – classically, the pain is promptly relieved with anti-inflammatory drugs such as NSAIDS
Clinical notes: Epidural abscess should be a consideration with the presence of fever, spinal pain, and neurologic deficits or radicular pain; discitis may present with a patient refusing to walk or crawl
Herniated disk, slipped apophysis
Presentation: Acute pain, radicular pain, positive straight leg raise test, pain with spinal forward flexion, recent onset scoliosis
Spondylolysis, spondylolisthesis, lesion or injury to the posterior arch
Presentation: Acute pain, radicular pain, positive straight leg raise test, pain with spinal extension, tight hamstrings
Vertebral fracture
Presentation: acute pain, other injuries, traumatic mechanism of injury, neurologic loss
Muscle strain
Presentation: acute pain, muscle tenderness without radiation
Presentation: normal evaluation but persistent subjective pain
Idiopathic Scoliosis:
Presentation: positive Adam’s test (for larger angle curvature), most commonly asymptomatic
Clinical note: Of note, no definitive evidence that scoliosis causes pain, but patients with scoliosis have more frequently reported pain; therefore provider should rule out other causes before attributing pain to scoliosis
Treatment of Lumbago /Backache
General measures
Bed rest for the first 24 hours. Additional bed rest will be determined by the severity of the problem. Recent medical studies indicate that staying more active is better for back disorders than prolonged bed rest.
Use a firm mattress (place a bed board under the mattress if needed).
An ice pack or cold massage or heat applied to the affected area with a heating pad or hot water bottle.
Physical therapy.
Massage may help. Be sure the person is well-trained or massage could cause more harm than help.
Wear a special back support device.
Other options are available depending on the degree of injury, such as surgery (if disk damaged), electrical nerve stimulation, acupuncture, special shoes, etc.
Stress reduction techniques, if needed.
Non-Prescription Pain Relievers – Naproxen, acetaminophen, and ibuprofen each reduce inflammation and pain. Though these drugs are available over-the-counter, they are potent and taking more than the recommended dose can harm health. A doctor can help with advice about the right kind of non-prescription pain reliever to take.
Cold and Heat – Applying a cold pack to the painful part of the back contracts inflamed muscle and relieves pain. This treatment helps a great deal when the disk has recently ruptured and swelling is at its greatest. A heating pad or warm pack helps with residual pain.
Continued Physical Activity – Though pain or weakness seem like good reasons to rest the back, excessive bed-rest worsens the symptoms of a slipped disc. Moving around too little allows muscles to grow weaker and prevents the body from healing. Periods of rest interspersed with periods of normal activity throughout the day keep the back muscles in shape.
Prescription Remedies – If over-the-counter drugs fail to ease slipped disc pain, the doctor will turn to prescription medications. These can include narcotics, such as hydrocodone or codeine. While they can do away with pain, narcotics are very addictive and induce a mental fogginess that can itself be dangerous. More narrowly-focused medicines designed to target damaged nerves that create chronic pain may be a better choice, as they have fewer undesirable side effects. Gabapentin and Cymbalta are two drugs that act in different ways to minimize nerve pain. These drugs are less addictive than narcotics.
Physical Therapy – Physical therapists show slipped disc sufferers ways to move that do not cause pain. Occupational therapists teach skills that allow patients to return to a productive life.
Nutrition – In order to restore the disc we also are going to need to include different substances in our diet. There are a lot of supplements on the market, of course. If you wish to try them, that’s fine. I personally don’t like them. I have tried one with glucosamine and chondroitin, but I didn’t feel any different. So, if you have the opportunity to take these with the food or from more natural sources, it will be great. You can find these substances in seafood and animal cartilages and by digesting them we ensure the building blocks for the connecting tissue for our joints and spine. Also, we will need more Omega 3 fatty acids, which can be supplied from cold-pressed oils, fatty fish, flax seeds, chia and many more. Vitamins from the B group are very beneficial for people with herniated discs and all kinds of issues with the peripheral nervous system. Vitamins B1, B6 and B12 nourish the nerves and help them recover from the disk accident. Usually, doctors prescribe them as a part of the treatment, but it is worth mentioning anyway.
A good massage – A massage is one of the natural methods of relieving pain. Individuals who get a massage weekly for several months stand a better chance of alleviating back pain. A good massage provides a person with many health benefits that lessen back pain. A massage triggers the release of endorphins. Endorphins aid in decreasing anxiety and relieving pain. They offer a relaxation effect by softening muscles that are injured preventing cramping.
Undertaking yoga – Yoga is an applicable strategy for keeping the level of back pain at minimal levels. Taking yoga sessions often is very effective method of dealing with back pain. With yoga, there is a high likelihood of proper body functions. The use of pain prescriptions is also diminished. Patients suffering from back pain related issues do not have to rely on these prescriptions to manage pain. Incorporating laughter in yoga is a good way of exercising. Yoga incorporates simple yet appropriate exercises that enhance the stretching of muscles. Laughter with yoga stimulates relieving of pain. It facilitates increased uptake of oxygen, little anxiety, and production of endorphins. All these variables play an essential role in diminishing back pain.
Adjusting sleeping position – A simple sleeping mistake can immensely contribute to back pain. A poor sleeping position can cause stress and tension on the muscles contributing to back pain. Altering one’s sleeping position and adopting a style that does not exert a lot of stress on the back is a recommended tactic. Nurturing sleeping habits such as assuming a reclining position, using wedge-shaped cushions and getting adjustable beds from reputable medical institutions are easy techniques to endorse. If a reclining position does not suit an individual, the other two techniques can be embraced.
Heat therapy – Several considerations should be observed when using heat therapy. The right temperature ought to be set so as to ensure a patient does not face risks associated with too much exposure to heat. The key objective should be to ensure enough access of heat to the muscles to yield benefits for the patient. The adoption of heat therapy for easing back pain is determined by the magnitude of pain a person is experiencing. In cases where relatively low back pain is encountered, short heat therapy sessions are recommended. On the other hand, if an individual is experiencing prolonged back pain, long heat therapy sessions are the most applicable.
Taking hot baths – This is a form of heat therapy that aims at relieving back pain. It guarantees permeation of heat into the muscles leading to reduced pain. Many individuals opt for this method since they believe it achieves competent results. Hot baths initiate a fast process of blood supply to stiff neck and back muscles. When this happens, the muscles relax and stretch leading to decreased back pain. To avoid interference with one’s sleeping patterns, a hot bath should be taken several hours before retiring to bed.
Aquatic therapy – This natural technique involves physical therapy in a pool. Individuals get the best out of this therapy by relying on the resistance of water. Consistency in undertaking this therapy is what ascertains getting back pain relief. Integrating aquatic therapy in an individual’s life for the better part of the week enhances the reduction of back pain quickly.
Enlighten others – Individuals have the power to devise their own natural strategies that aid them in coping with back pain. The strategies can also be a good remedy for others going through similar circumstances. An individual can use social media platforms to equip others with important tips on how to keep back pain at bay. Further, becoming a member of associations that address back pain issues enables better communication of the knowledge gained from personal experience.
[stextbox id=’alert’]
Treatments for acute and chronic low back pain Rx
Effectiveness
Acute low back pain
Chronic low back pain
Beneficial
Advice to stay active, non-steroidal anti-inflammatory drugs (NSAIDs)
A wide range of medications is used to treat acute and chronic low back pain. Some are available over the counter (OTC); others require a physician’s prescription. Certain drugs, even those available OTC, may be unsafe during pregnancy, may interact with other medications, cause side effects, or lead to serious adverse effects such as liver damage or gastrointestinal ulcers and bleeding. Consultation with a health care provider is advised before use. The following are the main types of medications used for low back pain:
Analgesic medications – are specifically designed to relieve pain. They include OTC acetaminophen and aspirin, as well as prescription opioids such as codeine, oxycodone, hydrocodone, and morphine. Opioids should be used only for a short period of time and under a physician’s supervision. People can develop a tolerance to opioids and require increasingly higher dosages to achieve the same effect. Opioids can also be addictive. Their side effects can include drowsiness, constipation, decreased reaction time, and impaired judgment. Some specialists are concerned that chronic use of opioids is detrimental to people with back pain because they can aggravate depression, leading to a worsening of the pain.
Nonsteroidal anti-inflammatory drugs(NSAIDS) – relieve pain and inflammation and include OTC formulations (ibuprofen, ketoprofen, and naproxen sodium). Several others, including a type of NSAID called COX-2 inhibitors, are available only by prescription. Long-term use of NSAIDs has been associated with stomach irritation, ulcers, heartburn, diarrhea, fluid retention, and in rare cases, kidney dysfunction and cardiovascular disease. The longer a person uses NSAIDs the more likely they are to develop side effects. Many other drugs cannot be taken at the same time a person is treated with NSAIDs because they alter the way the body processes or eliminates other medications.
Anticonvulsants—drugs primarily used to treat seizures—may be useful in treating people with radiculopathy and radicular pain.
Antidepressants – such as tricyclics and serotonin and norepinephrine reuptake inhibitors have been commonly prescribed for chronic low back pain, but their benefit for nonspecific low back pain is unproven, according to a review of studies assessing their benefit.
Muscle Relaxants – If the muscles around the slipped disc experience painful spasms, a muscle relaxant such as Valium may be useful. The drawback to drugs like these is that they do not limit their power to the affected nerve. Instead, they have a generally relaxing effect and will interfere with daily activities. Such as cyclobenzaprine (Flexeril), might be prescribed to relieve the discomfort associated with muscle spasms. However, these medicines might cause confusion in older people. Depending on the level of pain, prescription pain medicines might be used in the initial period of treatment.
Steroids – If inflammation is severe, a doctor may also prescribe a steroid. Steroids, such as cortisone, reduce swelling quickly. A cortisone shot directly in the affected area will have an immediate effect on the displaced disc.
Counter-irritants – such as creams or sprays applied topically stimulate the nerves in the skin to provide feelings of warmth or cold in order to dull the sensation of pain. Topical analgesics reduce inflammation and stimulate blood flow.
Nerve Relaxant — Pregabalin or gabapentin and anti-inflammatory drugs help to relieve pain and stiffness, allowing for increased mobility and exercise. There are many common over-the-counter medicines called non-steroidal anti-inflammatory drugs (NSAIDs). They include aspirin, ibuprofen (Motrin, Advil), and naproxen (Naprosyn, Aleve).
Carisoprodol – This muscle relaxant was investigated in two high-quality studies on acute low back pain. The first study compared carisoprodol with diazepam [rx]. Carisoprodol was superior in performance on all the outcome parameters measured. A comparison of carisoprodol with cyclobenzaprine‐hydrochloride in the second study revealed no statistically significant differences between the two treatments [rx].
Chlorzoxazone – This muscle relaxant was compared with tizanidine in one high-quality study in a very small sample of patients with degenerative lumbar disc disease [rx]. No differences were found between the treatments.
Cyclobenzaprine‐hydrochloride – Cyclobenzaprine was compared with diazepam in a low-quality trial on chronic low back pain, but no significant differences between the treatments were identified [rx]. There was also no significant difference between cyclobenzaprine and carisoprodol in one high-quality study on acute low back pain [rx].
Diazepam – In comparison with carisoprodol, diazepam was found to be inferior in performance on muscle spasm, global efficacy and functional status in a high-quality trial on acute low back pain [rx]. In a very small high-quality trial (30 people) comparing diazepam with tizanidine, there were no differences in pain, functional status and muscle spasm after seven days [rx].
Tizanidine – This muscle relaxant was compared with chlorzoxazone and diazepam in two very small high quality [rx]. Both trials did not find any differences in pain, functional status and muscle spasm after 7 days.
Pridinol mesylate – One low-quality trial showed no differences between this muscle relaxant and thiocolchicoside on pain relief and global efficacy.
Advanced Treatment of
Spinal manipulation and spinal mobilization – Are approaches in which professionally licensed specialists (doctors of chiropractic care) use their hands to mobilize, adjust, massage, or stimulate the spine and the surrounding tissues. Manipulation involves a rapid movement over which the individual has no control; mobilization involves slower adjustment movements. The techniques have been shown to provide small to moderate short-term benefits in people with chronic low back pain. Evidence supporting their use for acute or subacute low back pain is generally of low quality. Neither technique is appropriate when a person has an underlying medical cause for back pain such as osteoporosis, spinal cord compression, or arthritis.
Traction – involves the use of weights and pulleys to apply constant or intermittent force to gradually “pull” the skeletal structure into better alignment. Some people experience pain relief while in traction, but that relief is usually temporary. Once traction is released the back pain tends to return. There is no evidence that traction provides any longterm benefits for people with low back pain.
Spinal injections — An injection of a cortisone-like anti-inflammatory medicine into the lower back might help reduce swelling and inflammation of the nerve roots, allowing for increased mobility.
Biofeedback – It is used to treat many acute pain problems, most notably back pain and headache. The therapy involves the attachment of electrodes to the skin and the use of an electromyography machine that allows people to become aware of and self-regulate their breathing, muscle tension, heart rate, and skin temperature. People regulate their response to pain by using relaxation techniques. Biofeedback is often used in combination with other treatment methods, generally without side effects. The evidence is lacking that biofeedback provides a clear benefit for low back pain.
Nerve block therapies – aim to relieve chronic pain by blocking nerve conduction from specific areas of the body. Nerve block approaches range from injections of local anesthetics, botulinum toxin, or steroids into affected soft tissues or joints to more complex nerve root blocks and spinal cord stimulation. When extreme pain is involved, low doses of drugs may be administered by catheter directly into the spinal cord. The success of a nerve block approach depends on the ability of a practitioner to locate and inject precisely the correct nerve. Chronic use of steroid injections may lead to increased functional impairment.
Surgery Lumbago
When other therapies fail, surgery may be considered an option to relieve pain caused by serious musculoskeletal injuries or nerve compression. It may be months following surgery before the patient is fully healed, and he or she may suffer permanent loss of flexibility.
Vertebroplasty and kyphoplasty – are minimally invasive treatments to repair compression fractures of the vertebrae caused by osteoporosis. Vertebroplasty uses three-dimensional imaging to assist in guiding a fine needle through the skin into the vertebral body, the largest part of the vertebrae. Glue-like bone cement is then injected into the vertebral body space, which quickly hardens to stabilize and strengthen the bone and provide pain relief. In kyphoplasty, prior to injecting the bone cement, a special balloon is inserted and gently inflated to restore height to the vertebral structure and reduce spinal deformity.
Spinal laminectomy – (also known as spinal decompression) is performed when spinal stenosis causes a narrowing of the spinal canal that causes pain, numbness, or weakness. During the procedure, the lamina or bony walls of the vertebrae, along with any bone spurs, are removed. The aim of the procedure is to open up the spinal column to remove pressure on the nerves.
Discectomy or microdiscectomy – may be recommended to remove a disc, in cases where it has herniated and presses on a nerve root or the spinal cord, which may cause intense and enduring pain. Microdiscectomy is similar to a conventional discectomy; however, this procedure involves removing the herniated disc through a much smaller incision in the back and a more rapid recovery. Laminectomy and discectomy are frequently performed together and the combination is one of the more common ways to remove pressure on a nerve root from a herniated disc or bone spur.
Foraminotomy – is an operation that “cleans out” or enlarges the bony hole (foramen) where a nerve root exits the spinal canal. Bulging discs or joints thickened with age can cause narrowing of the space through which the spinal nerve exits and can press on the nerve, resulting in pain, numbness, and weakness in an arm or leg. Small pieces of bone over the nerve are removed through a small slit, allowing the surgeon to cut away the blockage and relieve pressure on the nerve.
Intradiscal electrothermal therapy (IDET) – is a treatment for discs that are cracked or bulging as a result of degenerative disc disease. The procedure involves inserting a catheter through a small incision at the site of the disc in the back. A special wire is passed through the catheter and an electrical current is applied to heat the disc, which helps strengthen the collagen fibers of the disc wall, reducing the bulging and the related irritation of the spinal nerve. IDET is of questionable benefit.
Nucleoplasty also called plasma disc decompression (PDD) – is a type of laser surgery that uses radiofrequency energy to treat people with low back pain associated with mildly herniated discs. Under x-ray guidance, a needle is inserted into the disc. A plasma laser device is then inserted into the needle and the tip is heated to 40-70 degrees Celsius, creating a field that vaporizes the tissue in the disc, reducing its size and relieving pressure on the nerves. Several channels may be made depending on how tissue needs to be removed to decompress the disc and nerve root.
Radiofrequency denervation – is a procedure using electrical impulses to interrupt nerve conduction (including the conduction of pain signals). Using x-ray guidance, a needle is inserted into a target area of nerves and a local anesthetic is introduced as a way of confirming the involvement of the nerves in the person’s back pain. Next, the region is heated, resulting in localized destruction of the target nerves. Pain relief associated with the technique is temporary and the evidence supporting this technique is limited.
Spinal fusion – is used to strengthen the spine and prevent painful movements in people with degenerative disc disease or spondylolisthesis (following laminectomy). The spinal disc between two or more vertebrae is removed and the adjacent vertebrae are “fused” by bone grafts and/or metal devices secured by screws. The fusion can be performed through the abdomen, a procedure known as an anterior lumbar interbody fusion, or through the back, called posterior fusion. Spinal fusion may result in some loss of flexibility in the spine and requires a long recovery period to allow the bone grafts to grow and fuse the vertebrae together. Spinal fusion has been associated with an acceleration of disc degeneration at adjacent levels of the spine.
Artificial disc replacement – is considered an alternative to spinal fusion for the treatment of people with severely damaged discs. The procedure involves removal of the disc and its replacement by a synthetic disc that helps restore height and movement between the vertebrae.
Other Rx of Lumbago /Backache
Chiropractic Care
Sixty percent of people with sciatica who didn’t get relief from other therapies and then tried spinal manipulation experienced the same degree of pain relief as patients who eventually had surgery, found a 2010 study in the Journal of Manipulative and Physiological Therapeutics. The 120 people in the study saw a chiropractor about 3 times a week for 4 weeks and then continued weekly visits, tapering off treatment as they felt better. In people who responded to chiropractic care, benefits lasted up to a year. “Spinal manipulation may create a response in the nervous system that relieves pain and restores normal mobility to the injured area,” says study researcher Gordon McMorland, DC, of National Spine Care in Calgary, Alberta. “It also reduces inflammation, creating an environment that promotes the body’s natural healing mechanisms.”
Acupuncture
You can get relief as soon as the first session, though it takes about 12 sessions to see improvement,” says Jingduan Yang, MD, assistant professor at the Jefferson Myrna Brind Center of Integrative Medicine at Thomas Jefferson University. A small study in the Journal of Traditional Chinese Medicine found that of 30 people with sciatica, 17 got complete relief and 10 saw symptoms improve with warming acupuncture, in which the needles are heated.
Yoga
A study in the journal Pain reported that people with chronic back pain who practiced Iyengar yoga for 16 weeks saw pain reduced by 64% and disability by 77%. Although yoga’s effects on sciatica are less clear, gentle forms may be beneficial. By strengthening muscles and improving flexibility, a yoga practice can help sciatica sufferers “move and function better so they don’t fall into a posture that aggravates sciatica,” says James W. Carson, Ph.D., a psychologist at the Comprehensive Pain Center at Oregon Health & Science University. For extra grip and stability, try these grip socks from Natural Fitness.
Massage
Don’t expect a chilled-out spa massage if you have sciatica. In this instance, trigger-point therapy is best, says Jeff Smoot, vice president of the American Massage Therapy Association. The sciatic nerve sits underneath a muscle called the piriformis, which is located beneath the glutes. “When the piriformis muscle gets tight, it pinches the sciatic nerve, causing tingling and numbness down into the leg,” says Smoot. He applies pressure to irritated and inflamed areas, or trigger points, in the piriformis muscle, as well as in muscles in the lower back and glutes. Typically, Smoot schedules treatments 7 to 10 days apart. If patients don’t see progress by the fourth visit, “they need to try another form of therapy,” he says.
Shiatsu,
Also known as finger pressure therapy, is a type of massage where pressure is applied along energy lines in the body. The shiatsu therapist applies pressure with his/her fingers, thumbs and elbows.
Topical Preparations
St. John’s wort oil, a liniment, is “one of my favorites for nerve pain,” says Tieraona Low Dog, MD, director of the fellowship at the Arizona Center for Integrative Medicine. Apply the anti-inflammatory oil two or three times a day where there’s a pain. Another option: an OTC cayenne pepper plaster or cream; capsaicin, found in chiles, hinders the release of pain-causing compounds from nerves. For severe cases, Low Dog uses the prescription chile patch Qutenza, designed for shingles pain. “One application is effective for weeks,” says Low Dog.
Ice or Heat
Because the sciatic nerve is buried deep within the buttock and leg, ice or heat on the surface of the body won’t ease that inner inflammation. But the time-honored treatments can act as counterirritants—that is, “they give your body other input in the painful area, and that brings the pain down a notch,” says Ruppert. Apply an ice pack or a heating pad as needed for 15 minutes.
Devil’s Claw
The herbal medication devil’s claw is “quite a potent anti-inflammatory, working like ibuprofen and similar drugs to inhibit substances that drive inflammation,” says Low Dog. She generally starts patients on 1,500 to 2,000 mg twice a day. Look for a brand that has a standardized extract of roughly 50 mg of harpagoside, the active compound. Safety reviews show that the supplement is well tolerated by most people but should be avoided by patients with peptic ulcers or on blood-thinning medications.
CBT (cognitive behavioral therapy)
CBT can help patients manage chronic back pain. The therapy is based on the principle that the way a person feels is, in part, dependent on the way they think about things. People who can be taught to train themselves to react in a different way to pain may experience less perceived pain. CBT may use relaxation techniques as well as strategies to maintain a positive attitude. Studies have found that patients with CBT tend to become more active and do exercise, resulting in a lower risk of back pain recurrence.
Exercise and Physical Therapy
Moving is usually the last thing people dogged by sciatica want to do, but it’s important to be physically active. Lying in bed makes it more likely that the pain will last longer, says Ruppert. Exercise increases blood flow to the disk and the nerve, helping to get rid of the chemicals causing the inflammation. Take 15- to 20-minute walks. If that hurts too much, give swimming or water aerobics a try; there’s not as much pressure on the back when you’re in the water, says Ruppert. It may also be worth seeing a physical therapist, who can prescribe stretching exercises to restore flexibility to the back or moves that strengthen core muscles, helping to stabilize the spine and reduce the likelihood of a similar injury.
Here are six exercises for Lumbago /Backache
Pigeon pose
Pigeon Pose is a common yoga pose. It works to broadly open the hips. There are multiple versions of this stretch. The first is a starting version of the pigeon pose, known as the reclining pigeon pose. If you are just starting your treatment, you should try the reclining pose first. Once you can do the reclining version without pain, work with your physical therapist on the sitting and forward versions.
Reclining pose
While on the back, bring your right leg up to a right angle and grasp it with both hands behind the thigh, locking your fingers.
Take your left leg and place your ankle against the knee. Hold the position for a moment before changing legs. This helps stretch the tiny piriformis muscle, which sometimes becomes inflamed and presses against the sciatic nerve causing pain.
Repeat by switching sides and doing the same exercise with the other leg.
Sitting pose
Sit on the floor with your legs stretched out straight in front of you. Then bend your right leg, putting your right ankle on top of the left knee.
Lean forward and allow your upper body to lean toward your thigh. Hold for 15 to 30 seconds and then switch sides. This stretches the glutes and lowers back.
Forward pose
Kneel on the floor on all fours.
Pick up your right leg and move it forward so that your lower leg is on the ground, horizontal to the body. Your right foot should be in front of your right knee while your right knee stays to the right.
Stretch the left leg out all the way behind you on the floor, with the top of the foot on the ground and toes pointing back.
Shift your body weight gradually from your arms to your legs so that your legs are supporting your weight. Sit up straight with your hands on either side of your legs.
Take a deep breath. While exhaling, lean your upper body forward over your lower leg. Support your weight with your arms as much as possible.
Knee to the opposite shoulder
This simple stretch helps relieve sciatica pain by loosening your gluteal and piriformis muscles, which can become inflamed and press against the sciatic nerve.
Lie on your back with your legs extended outward and your feet flexed upward.
Clasp your hands around your knee and gently pull your right leg across your body toward your left shoulder. Hold it there for 30 seconds and then push your knee so your leg returns to its starting position.
Repeat for a total of 3 reps, and then switch legs. Remember to only pull your knee as far as it will comfortably go. You should feel a relieving stretch in your muscles, not pain.
Sitting spinal stretch
Sciatica pain is triggered when vertebrae in the spine compress. This stretch helps create space in the spine to relieve pressure from the sciatic nerve.
Sit on the ground with your legs extended straight out with your feet flexed upward.
Bend your right knee and place your foot flat on the floor on the outside of your opposite knee.
Place your left elbow on the outside of your right knee to help you gently turn your body toward the right. Hold for 30 seconds and repeat three times, then perform this stretch with your left leg bent and body turned to the left side.
Standing hamstring stretch
This stretch can help ease pain and tightness in the hamstring caused by sciatica.
Place your right foot on an elevated surface at or below your hip level. This could be a chair, ottoman, or step on a staircase. Flex your foot so your toes and leg are straight. If your knee tends to hyperextend, keep a slight bend in it.
Bend your body forward slightly toward your foot. The further you go, the deeper the stretch. Do not push so far that you feel pain.
Release the hip of your raised leg downward as opposed to it lifting up. If you need help easing your hip down, loop a yoga strap or long exercise band over your right thigh and under your left foot. Hold for at least 30 seconds, and then repeat on the other side.
Exercise with care
Kovacs emphasizes that you should not assume that you will be able to be as flexible as the exercises ideally call for. Don’t think that because of what you see on YouTube or TV that you can get into these positions, he said. Most people who demonstrate the exercises have great flexibility and have been doing it for years. If you have any kind of pain, you should stop.”
Corina Martinez – a physical therapist at Duke Sports Medicine Center and a member of the American Medical Society for Sports Medicine, says that there is no one-size-fits-all exercise for people suffering from sciatic nerve pain. “Do you feel better when you bring your knees to the chest, or when they extend back a little more? If one feels better, that is the treatment you want to pursue.”
Martinez – says that anyone experiencing even mild sciatic nerve pain symptoms for more than a month should see a doctor or physical therapist. They may find relief with an in-home exercise program tailored specifically to how their pain presents itself.
What complications are associated with – Chronic (ongoing and lasting) pain is a complication of untreated sciatica. If the “pinched nerve” is seriously injured, chronic muscle weakness, such as a “drop foot,” might occur.
What is the outlook for people with – Sciatic pain usually goes away with time and rest. Most people with sciatica (80 percent to 90 percent) will get better without surgery. About half of affected individuals recover from an episode within six weeks.
Can sciatica be prevented?
Some sources of sciatica are not preventable, such as degenerative disc disease, back strain due to pregnancy, and accidental falls.
Although it might not be possible to prevent all cases of sciatica, you can take steps to protect your back and reduce your risk.
Practice proper lifting techniques. Lift with your back straight, bringing yourself up with your hips and legs, and holding the object close to your chest. Use this technique for lifting everything, no matter how light.
Avoid/ stop cigarette smoking, which promotes disc degeneration.
Exercise regularly to strengthen the muscles of your back and abdomen, which work to
support your spine
Use good posture when sitting, standing, and sleeping. Good posture helps to relieve the pressure on your lower back.
Avoid sitting for long periods.
Preventing Lumbago /Backache
Steps to lower the risk of developing back pain consist mainly of addressing some of the risk factors.
Exercise – Regular exercise helps build strength as well as keeping your body weight down. Experts say that low-impact aerobic activities are best; activities that do not strain or jerk the back. Before starting any exercise program, talk to a health care professional. There are two main types of exercise that people can do to reduce the risk of back pain
Core-strengthening exercises– exercises that work the abdominal and back muscles, helping to strengthen muscles that protect the back.
Flexibility – exercises aimed at improving flexibility in your core, including your spine, hips, and upper legs, may help too.
Smoking – a significantly higher percentage of smokers have back pain incidences compared to non-smokers of the same age, height, and weight.
Bodyweight – the number of weight people carry, as well as where they carry it, affects the risk of developing back pain. The difference in back pain risk between obese and normal-weight individuals is considerable. People who carry their weight in the abdominal area versus the buttocks and hip area are also at greater risk.
Posture when standing – make sure you have a neutral pelvic position. Stand upright, head facing forward, back straight, and balance your weight evenly on both feet – keep your legs straight and your head in line with your spine.
If you regularly use a computer, it is important to ensure that you have a chair with good back support and adopt a good posture and head position.
Posture when sitting – a good seat should have good back support, armrests and a swivel base (for working). When sitting try to keep your knees and hips level and keep your feet flat on the floor – if you can’t, use a footstool. You should ideally be able to sit upright with support in the small of your back. If you are using a keyboard, make sure your elbows are at right-angles and that your forearms are horizontal.
Lifting things – the secret for protecting your back when lifting things is to think “legs not back”. In other words, use your legs to do the lifting, more than your back. Keep your back as straight as you can, keeping your feet apart with one leg slightly forward so you can maintain balance. Bend only at the knees, hold the weight close to your body, and straighten the legs while changing the position of your back as little as possible. Bending your back initially is unavoidable, but when you bend your back try not to stoop or squat, and be sure to tighten your stomach muscles so that your pelvis is pulled in. Most importantly, do not straighten your legs before lifting; otherwise, you will be using your back for most of the work.
Do not lift and twist at the same time. If something is particularly heavy, see if you can lift it with someone else. While you are lifting keep looking straight ahead, not up nor down, so that the back of your neck is like a continuous straight line from your spine.
Moving things – remember that it is better for your back to push things across the floor, using your leg strength, rather than pulling them.
Shoes – flat shoes place less of a strain on the back.
Driving – it is important to have proper support for your back. Make sure the wing mirrors are properly positioned so you do not need to twist. The pedals should be squarely in front of your feet. If you are on a long journey, have plenty of breaks – get out of the car and walk around.
Your bed – you should have a mattress that keeps your spine straight, while at the same time supporting the weight of your shoulders and buttocks. Use a pillow, but not one that forces your neck into a steep angle.
Home Remedies for Lumbago /Backache
Ice and Heat
Ice works wonders on lower back pain. Wrap some ice cubes in a plastic bag to prepare an ice pack. Then cover it with a towel and apply it to the painful area for 20 minutes. Repeat the same process several times a day. Then after 48 hours, you can switch to heat method. Dip a towel in warm water. Flatten and fold it on to the affected area. Place a heating pad on it with a plastic cover between towel and heating pad. Leave it for 20 minutes. Do it several times a day. It reduces swelling and relaxes the nerves that are responsible for sending pain signals to the brain.
Rest
Get sufficient rest. Don’t exhaust yourself physically and mentally. When sleeping, keep changing your positions. When you lie on back, put a pillow under your knees. Similarly, if you lie on your side, draw your knees near your chest and keep a pillow between your knees.
Right Posture
Your sitting and standing posture is very important to keep back pain at bay. One should not be in a bending position for a long time whether sitting or standing. Sitting on the edge of the chair and slouching should be avoided. The angle of the chair in office should be 110 degrees.
Lemon Juice
Lemon juice is an effective home remedy for back pain. Drink lemon juice twice a day for better results.
Poppy Seeds
Prepare a mixture of poppy seeds and rock candy by grinding together 100 gm of each. Take this mixture twice a day with a glass of milk. You will get relief from back pain.
Massage with Olive Oil
Massage with olive oil to reduce stress by relaxing tensed muscles. It also helps release stiffness in joints and relieves upper back pain.
Stretching
Stretching is the easiest back pain treatment. If your job demands sitting or standing for long hours, just take a break of 5 minutes every hour and walk or simply stretch your body to avoid back pain.
Wheat
Wheat has pain minimizing component in it. Mix cuscus grass and coriander with overnight soaked wheat. Add 1 cup of milk and bring it to boil. Consume this mixture twice a day
Garlic
Eat 2-3 garlic cloves on an empty stomach every morning to get relief from back pain. You can also use garlic oil. Massage your back with this oil, cover it with a warm blanket and lie on your back. Bathe using warm water after 20 minutes. This is a wonderful home remedy to treat back pain.
Ginger
The anti-inflammatory properties of ginger make it an ideal home remedy to get rid of back pain. Add ½ teaspoon of black peppercorns, ½ teaspoon of cloves and 1 teaspoon of ginger powder in a cup of boiling water to prepare herbal tea. Drink it 2-3 times a day.
Alternatively, grate some ginger to prepare a paste. Apply it on the affected area. Then massage with eucalyptus oil.
Put thin ginger slices in a pan of boiling water. Simmer it for 10-15 minutes. Strain and allow it to cool down at room temperature. Add honey to sweeten it. Drink it twice or thrice a day.
Milk
Since milk is a great source of calcium, it is extremely beneficial for strong bones and preventing back pain. People of every age group should consume milk. For quick relief, add a few drops of honey and a pinch of turmeric in the milk.
Epsom Salt
A natural healer, Epsom salt reduces swelling in the back. It contains magnesium and sulfate which help muscles function properly, thus, provide relief from pain. Add 2 cups of Epsom salt to a tub of warm water. Let it soak for 30 minutes. Take bath with this water.
Rice
Rice is easily available in every household. It’s an effective home remedy for back pain. Put 1 cup uncooked rice in a thick sock and place it in the microwave for ½ – 1 minute. Now apply it onto the back.
Oats
Mash cooked whole oats with vinegar. Apply it on the back when hot. It soothes the aching back.
Potatoes
Mash the peeled and boiled potatoes. Let them cool and then apply on back. You will experience relief from back pain.
Coconut Oil
Take some coconut oil. Mix camphor in it and boil for 5-7 minutes. Allow it to cool. Store it in a bottle. Massage with this oil two times a day to cure back pain.
Capsaicin Cream
Capsaicin is an important ingredient of chilies. Apply capsaicin cream on the back. It will reduce the production of chemicals that transmit signals of pain to your brain.
Herbal Remedies for Lumbago /Backache
Willow Bark
White willow tree’s bark is considered an excellent herbal remedy for treating back pain. It has pain-relieving properties the same as aspirin. So it will help reduce your back pain.
Basil Leaves
Basil leaves are very famous for their medicinal benefits. They aid in curing lower back pain. Boil 10-12 fresh basil leaves in a cup of water until it becomes half. Add a pinch of salt to it. Drink it once or twice a day depending on the severity of your pain.
Herbal Oils
Herbal oils like almond oil, eucalyptus oil, coconut oil or olive oil are very effective in alleviating back pain. Massage with warm oils on the painful area to relax the nerves causing pain.
Chamomile
Take some chamomile flowers. Steep them in a cup of boiling water for 15-20 minutes. Drink it 2-3 times a day. It will relax the tense muscles, thereby cure a backache.
Note: – Pregnant ladies and those allergic to chamomile flowers should first consult doctor before taking this.
Ginger
Though more studies are needed, says Dr. Kiefer, ginger extract may help with joint and muscle pain because it contains phytochemicals, which help stop inflammation. Few side effects have been linked to ginger when taken in small doses.
Feverfew
Feverfew has been used for centuries to treat headaches, stomachaches, and toothaches. Nowadays it’s also used for migraines and rheumatoid arthritis. More studies are required to confirm whether feverfew is actually effective, but the herb may be worth trying since it hasn’t been associated with serious side effects. Mild side effects include canker sores and irritation of the tongue and lips. Pregnant women should avoid this remedy.
Turmeric
This spice has been used to relieve arthritis pain and heartburn, and to reduce inflammation. It’s unclear how turmeric works against pain or inflammation, but its activity may be due to a chemical called curcumin, which has anti-inflammatory properties. Turmeric is usually safe to use, but high doses or long-term use may cause indigestion. Also, people with gallbladder disease should avoid using turmeric.
Homeopathic Medicines for Lumbago /Backache
Rhus Tox
Rhus Tox tops the list of Homeopathic medicines for back pain. I have seen magnificent results in back pain from the use of Rhus Tox. Rhus Tox is indicated for both upper and lower back pain, especially where the back pain is accompanied by intense stiffness. The back pain that arises from muscle strain also recovers wonderfully well with Rhus Tox. Persons suffering from back pain as a result of exertion or lifting heavy weights have found complete relief when prescribed Rhus Tox, making it one of the most reliable Homeopathic medicines for back pain. A prominent symptom to look out for while prescribing Rhus Tox is that the back pain gets worse with rest while walking or hard pressure brings relief from pain.
Bryonia
In my clinical practice, Bryonia has shown marvelous results in lower back pain that worsens with the slightest of movements. Apart from motion, this pain also gets worse with standing or from turning in the bed, a key sign that Bryonia will work best. The pain may be accompanied by marked stiffness in such cases, for which Bryonia would rate among the best Homeopathic medicines for back pain. Lying down and taking rest brings relief from pain.
Aesculus
Aesculus is one of the most effective Homeopathic medicines for lower back pain that gets worse from stooping. In this case, the pain is most marked in the sacrum and hip region. The lower back feels as if it would break. Stiffness in the lower back is also intense. Aesculus is also one of the best Homeopathic medicines for back pain which gets worse when rising from a sitting position. Here it takes the person repeated efforts to rise from a chair or another sitting position.
Kali Carb
I would rank Kali Carb as one of the top grade Homeopathic medicines for back pain that arises after childbirth. The most prominent symptoms indicative of Kali Carb as the best suited Homeopathic medicines for back pain in such instances are stiffness and weakness in the lower back. The pain is very severe, with a feeling that the back might break. The back pain makes it difficult to walk. Women feel the need to lie down to get relief from the pain which may radiate to the upper back or down to the thigh and hips. Where these symptoms exist, Kali Carb comes highly recommended as one of the best Homeopathic medicines for back pain. Apart from a post-partum backache, Kali Carb is also useful for backache in women before or during menses and after a miscarriage.
Cobalt
Cobalt ranks on top of the list of Homeopathic medicines for back pain that worsens from sitting. In such cases, the person feels better while walking or lying down. The back pain may radiate down the legs and feet in some cases, but the person will surely feel a weakness in the legs, a sure sign that Cobaltum will provide sustained relief.
Colocynth & Magnesium Phos
I have successfully treated several cases of back pain radiating down the legs and/or feet with two main Homeopathic medicines. These top-rated Homeopathic medicines for back pain are Colocynth and Magnesium Phos. Among these, Colocynth is most effective Homeopathic medicine for back pain when the lower back pain radiates to the left leg and foot. Magnesium Phos brings relief when the lower back pain radiates down the right leg. The pain, in both cases, can be of a shooting, cramping or tearing nature. However, both the medicines have proven their ability to bring lasting relief from pain and established themselves as the best Homeopathic medicines for back pain.
Cimicifuga & Kalmia
Two highly recommended Homeopathic medicines for back pain in the cervical region are Cimicifuga and Kalmia. I have seen remarkable results with the use of Cimicifuga in cervical back pain accompanied by stiffness, contraction, and sensitiveness in the neck. If pressure worsens the neck pain, Cimicifuga will offer effective treatment. However, in cases where the cervical pain radiates down the arm or hands, Kalmia has proved to be one of the most helpful Homeopathic medicines for back pain treatment. Persons feeling a weakness, numbness or tingling sensation in the arms and hands along with neck pain also recover fully well with the use of Homeopathic medicine Kalmia.
Ruta & Hypericum
Ruta and Hypericum are highly suitable Homeopathic medicines for back pain resulting from the injury. Ruta is prescribed for a back that is sore and bruised from injury. The pain is most marked over the sacrum and coccyx region. The injured person may feel a weakness in the lower back. Where such symptoms are noted, Ruta is the most prominent among Homeopathic medicines for back pain and has shown effective results. Homeopathic medicine Hypericum is recommended when the pain from the tailbone radiates up the spine and down the limbs after injury. The pain is very sharp and intense. Motion, walking and stooping all make the pain worse. The spine is very tender and sensitive to touch in such cases where Hypericum has shown the best results.
Carpal tunnel syndrome (CTS) is a common median nerve compression syndrome and the most common peripheral mononeuropathy. The clinical syndrome is diagnosed by history and physical examination. Electrodiagnostic testing is the objective method used to measure median nerve dysfunction at the wrist and confirm the clinical diagnosis of CTS. Neuromuscular ultrasound imaging of the carpal tunnel provides supportive diagnostic information by revealing pathologic nerve swelling in CTS, and other anatomic anomalies that compress the median nerve. These tests cannot be used to make the diagnosis in the absence of history that includes CTS symptom criteria and excludes other causes.
Carpal tunnel syndrome is a painful disorder of the hand caused by pressure on nerves that run through the wrist. Symptoms include numbness, pins and needles, and pain (particularly at night). Anything that causes swelling inside the wrist can cause carpal tunnel syndrome, including repetitive hand movements, pregnancy, and arthritis. Possible treatments include rest, splinting, cortisone injections, and surgery.
Anatomy of Carpal Tunnel Syndrome
The carpal tunnel is composed of a bony canal, consisting of carpal bones, the roof of which is the fibrous but rigid transverse carpal ligament. The carpal tunnel contains the nine flexor tendons and the median [rx], which enters the tunnel in the midline or slightly radial to it [rx]. Atypical presentations could be explained by anatomical variations in the median nerve itself [rx].
Sensory branches from the median nerve supply the 3 radial digits and the radial half fourth digit – hence why CTS symptoms are felt in these fingers. The palmar sensory cutaneous branch of the median nerve supplies the cutaneous skin of the palm, and arises, on average, 6 cm proximal to the transverse carpal ligament (TLC). Therefore, the palm is generally not affected in CTS [rx].
The carpal tunnel is a narrow passageway in the wrist, which opens into the hand. It is surrounded by the bones of the wrist (underneath) and the transverse carpal ligament (across the top). The median nerve runs through the carpal tunnel and gives feeling to the thumb, forefinger, middle finger, and half of the ring finger.
Flexor tendons run through the carpal tunnel into the hand. These tendons are covered by a smooth membrane called the tenosynovium and allow hand movement. Any thickening from inflamed tendons or other causes of swelling can reduce the amount of space inside the carpal tunnel. If left unchecked, the median nerve is squashed against the transverse carpal ligament until the nerve cannot function properly. Numbness and pain are the results. It can affect one or both hands.
The muscles of the thumb are also serviced by the median nerve. A person with advanced carpal tunnel syndrome may find they cannot properly use or move their thumb anymore and may find it difficult to grasp an object.
Causes of Carpal Tunnel Syndrome
In some cases, the cause cannot be found. Sometimes there is a combination of factors such as
Pregnancy– the hormones associated with pregnancy cause general fluid retention, which can compress the nerve. Carpal tunnel syndrome triggered by pregnancy usually goes away soon after birth
Wrist fractures – bone fragments can irritate the tenosynovium or reduce the amount of space in the carpal tunnel
Congenital factors – some people have a smaller carpal tunnel than others
Overuse injury – the tendons in the carpal tunnel can become irritated and inflamed by awkward postures or repetitive hand movements.
*According to the American Academy of Neurology’s guidelines
Conditions that may be confused with carpal tunnel syndrome
Cervical radiculopathy (especially C6/7)—look for local neck pain on movement and neurological signs outside the territory of the distal median nerve
Ulnar neuropathy—this can also produce nocturnal paraesthesias; the distribution will usually be to the medial side of the hand.
Raynaud’s phenomenon—this should be recognizable from a history of symptoms related to cold exposure
Vibration white finger—suspect this if the patient uses vibrating hand tools at work
Osteoarthritis of the metacarpophalangeal joint of the thumb—this can produce a spurious appearance of thenar wasting but not true weakness or sensory deficit
Tendonitis—specific tests may help in diagnosis, such as Finkelstein’s test for De Quervain’s tenosynovitis
Generalized peripheral neuropathies—these should be recognized from the wider distribution of symptoms and reflex changes
Motor neuron disease—this can present with wasting in one hand but does not produce sensory symptoms
Syringomyelia—features such as prominent loss of temperature sensation in the hands should give a clue
Multiple sclerosis—this should be recognized from the presence of neurological abnormalities disseminated in location and time
Cervical radiculopathy – especially C6 or C7 radiculopathy, which commonly results in numbness of the thumb, index finger, or middle finger. Sensory symptoms or signs above the wrist, unilateral radicular pain exacerbated by neck movements, segmental weakness in the arm and forearm, or myotatic reflex asymmetry favors radiculopathy.
Neurogenic thoracic outlet syndrome – which frequently is associated with thenar atrophy. However, the pain and sensory manifestations in neurogenic thoracic outlet syndrome are in a C8/T1 distribution (ring and little fingers and medial aspect of the forearm).
Peripheral polyneuropathy – which may be associated with hand numbness. However, there are often sensory manifestations and motor weakness in the legs. Also, there usually is hyporeflexia or areflexia, especially at the ankles.
High median mononeuropathy – including the pronator syndrome, and compression at the ligament of Struthers in the distal arm. Both are rare syndromes and usually are associated with weakness of the long finger flexors.
Cervical myelopathy– In this condition, the numbness is not restricted to the median nerve, and there are frequently other pyramidal manifestations.
Risk factors of Carpal Tunnel Syndrome
Some people are at higher risk of developing carpal tunnel syndrome, including
People who use their hands repetitively in their day-to-day activities, such as typists or assembly line workers.
Symptoms of Carpal Tunnel Syndrome
Abnormal sensations – Parts of the hand feel numb or may tingle (also called “pins and needles”). Usually, the thumb and the middle three fingers are affected (these appear red in the illustration). Your hand falling asleep at night could be a typical early sign of carpal tunnel syndrome.
Pain in your fingers – Sometimes the entire hand might also hurt, or the pain may radiate into your arm.
The little finger and half of the ring finger are unaffected.
Standard symptoms of carpal tunnel syndrome*
Dull, aching discomfort in the hand, forearm, or upper arm
Paraesthesias in the hand
Weakness or clumsiness of the hand
Dry skin, swelling, or color changes in the hand
The occurrence of any of the above in the median distribution
Provocation of symptoms by sleep
Provocation of symptoms by sustained hand or arm positions
Provocation of symptoms by repetitive actions of the hand or wrist
Mitigation of symptoms by changing hand posture or shaking the wrist
Diagnosis of Carpal Tunnel Syndrome
Physical Assessment Tests for Carpal Tunnel Syndrome
The best of these include the carpal compression test. This is done by applying firm pressure directly over the carpal tunnel for 30 seconds. The test is positive when paresthesias, pain, or other symptoms are reproduced.
Flick Signal – One important and simple test of carpal tunnel is the “flick” signal. The patient is asked, “What do you do when your symptoms are worse?” If the patient responds with a motion that resembles shaking a thermometer, the doctor can strongly suspect carpal tunnel.
Testing for Thumb Weakness – Two questions are useful in determining thumb weakness, Can the thumb rise up from the plane of the palm? Can the thumb stretch so that its pad rests on the little finger pad?
Phalen’s Test – In Phalen’s test, the patient rests the elbows on a table and lets the wrists dangle with fingers pointing down and the backs of the hands pressed together. If symptoms develop within a minute, CTS is indicated. (If the test lasts for more than a minute, even patients without CTS may develop symptoms.) This test may be particularly important in determining the severity of CTS and assessing the results of treatment.
Tinel’s Sign – In the Tinel’s sign test, the doctor taps over the median nerve to produce a tingling or mild shock sensation.
Pressure Provocation Test – The doctor presses over the carpal tunnel for 30 seconds to produce tingling or shock in the median nerve.
Tourniquet Test – This test uses an inflatable cuff that applies pressure over the median nerve to produce tingling or small shocks.
Hand Elevation Test – The patient raises his or her hand overhead for 2 minutes to produce symptoms of CTS. The test was has been proven to be accurate and may provide useful information when combined with the Tinel’s and Phalen’s tests.
The reverse Phalen’s, or ‘prayer test,’ – is done by having the patient extend both of their wrists by placing palmar surfaces of both hands together for 1 minute (as if praying). Again a positive test is with the reproduction of symptoms.
The reverses prayer Test – is performed by having the patient fully flex their wrists by placing dorsal surfaces of both hands for one minute. A positive test is when symptoms (numbness, tingling, pain) are reproduced.
The square sign test – is an evaluation to determine the risk of developing carpal tunnel syndrome. The test is positive if the ratio of the thickness of the wrist divided by the width of the wrist is great than 0.7.
Imaging Test
X-rays – X-rays of the affected extremity at the elbow and wrist should be obtained to rule out any osseous deformity that may cause nerve entrapment, as well as cervical spine radiographs that may reveal sources of radiculopathy or first rib involvement. Finally, a chest x-ray should be obtained to rule out compression of the medial chord by an apical lung or Pancoast tumor, particularly in a patient with a positive history for smoking.
Plain radiographs – May be useful during instances where there is a history of trauma, or there is suspicion of a fracture. It can also help to identify cases of osteoarthritis, bony prominences or osteophytes, and the presence of orthopedic hardware that could compress nerves.
Ultrasound – of the nerve at the elbow and wrist can be used to measure the size of the radial nerve compared to controls, as well as to identify a thrombosis of the radial artery that can lead to ulnar nerve symptoms originating in Guyon’s canal.[rx]
Electrodiagnostic studies – Electromyography and nerve conduction studies help to localize the nerve involved as well as where along the course of the nerve it is affected. Additionally, testing can serve as a baseline for comparison with future studies during the course of treatment. It is important to note that normal electrodiagnostic studies do not rule out disease, and clinical correlation should include the patient’s history and physical examination findings.
Magnetic Resonance Imaging (MRI) – Can be useful in the identification of ganglion cysts, synovial or muscular hypertrophy, edema, vascular disease, as well as nerve changes. The cross-sectional area and space available for the nerve can also be measured and compared to accepted normal values.
Nerve ultrasonography – The use of nerve ultrasonography has increased recently. It can measure the cross-sectional area and the longitudinal diameter of the nerve. It can also identify compressive lesions. Ultrasound may also evaluate the presence of local edema. Additionally, ultrasound may help distinguish between different causes of wrist pain that can include tendonitis or osteoarthritis.
Serologicstudies – There are no blood tests used to specifically support the diagnosis of nerve compression, but the use of these tests may be necessary for medical conditions that can either promote nerve compression or can mimic their symptoms. Some of the most frequently encountered conditions include diabetes and hypothyroidism. The assessment of a patient’s fasting blood glucose, hemoglobin A1c, or thyroid function tests may be helpful in the general management of the patient. Other conditions that could mimic nerve compression include deficiency of vitamin B12 or folate, vasculitides, and fibromyalgia.
Electromyography – is also commonly used in the diagnosis of compression neuropathy with muscle denervation. Compressive neuropathies result in increased distal latency and decreased conduction velocity. Thus in patients with cubital tunnel syndrome, one is likely to identify a slowing of conduction in the ulnar nerve segment crossing the elbow.[rx][rx]
Both ultrasonic scanning (USS) – and magnetic resonance imaging (MRI) have sensitivity and specificity over 80% in diagnosis. MRI and USS are also helpful to identify other causes of compression, which may not be picked up on plain radiograph films such as soft tissue swelling and lesions such as neuroma, ganglions, aneurysms, etc.[rx]
Electromyographic and nerve conduction velocity – studies are used to evaluate the ulnar nerve pathology and to rule out other diagnoses.[rx][rx]
Electrodiagnostic tests – analyze the electric waves of nerves and muscles. These tests can help detect median nerve compression in the carpal tunnel.
Electrodiagnostic tests – should be used if clinical or provocative tests are positive and the patient is considering surgery. These tests are the best methods for confirming a diagnosis of CTS. Doctors who perform these tests should be certified by the American Board of Electrodiagnostic Medicine, which uses rigorous standards in qualifying doctors. Specific electrodiagnostic tests called nerve conduction studies and electromyography, are the most common ones performed. Nerve conduction tests can also detect other problems that cause CTS symptoms, such as pinched nerves in the neck or elbow, or thoracic outlet syndrome.
Nerve Conduction Studies – To perform nerve conduction studies, surface electrodes are first fastened to the hand and wrist. Small electric shocks are then applied to the nerves in the fingers, wrist, and forearm to measure how fast a signal travels through the nerves that control movement and sensation. Nerve conduction tests are fairly accurate when done on patients with more clear-cut symptoms of carpal tunnel syndrome. They are less accurate in identifying mild CTS, however. Patients should be sure their practitioners perform tests that compare a number of internal responses, not just the responses of muscles located in the palm at the base of the thumb. They should also make sure the tests measure responses on the second or third fingers.
Electromyography – To perform electromyography, a thin, sterile wire electrode is inserted briefly into a muscle, and the electrical activity is displayed on a viewing screen. Electromyography can be painful and is less accurate than nerve conduction. Some experts question whether it adds any valuable diagnostic information. They suggest that its use is limited to unusual cases, or when other tests indicate that the condition is aggressive and may increase the risk for rapid, significant injury.
Portable electrodiagnostic testing – Portable electronic devices are being evaluated for measuring nerve conductivity. They are relatively quick and easy to use on a large scale in an industrial facility. However, these devices have not been not well studied in clinical trials.
Limitations
Electrodiagnostic studies are not well standardized, and certain conditions can skew the results of either test:
Women and the elderly normally have slower conduction times than younger adult men.
A diagnosis of carpal tunnel syndrome may follow testing the affected hand for numbness, tingling, weakness or pain in specific areas. Muscle and nerve conduction tests may also help affirm or rule out carpal tunnel syndrome.
Treatment of Carpal Tunnel Syndrome
The improvements last for more than 6 months. Even among patients with mild CTS, there is a high risk of relapse. Some researchers are reporting better results when specific exercises for carpal tunnel syndrome are added to the program of treatments.
Ice – Ice may help with acute pain. Some patients have reported that alternating warm and cold soaks is beneficial. (If hot applications relieve pain, most likely the problem is not caused by CTS but by another condition that produces similar symptoms.)
Limiting Movement – If possible, the patient should avoid activities at work or home that may aggravate the syndrome. The affected hand and wrist should be rested for 2 – 6 weeks. This allows the swollen, inflamed tissues to shrink and relieves pressure on the median nerve. If the injury is work-related, the worker should ask to see if other jobs are available that will not involve the same hand or wrist actions. Few studies have been conducted on ergonomically designed furniture or equipment, or on frequent rest breaks. However, it is reasonable to ask for these if other work is not available.
Physiotherapy – It is one of the most common and effective non-pharmacological treatments in the world. It has a variety of treatment modules to erase acute and chronic pain. It is especially helpful in muscle spasticity, spasms related to carpal tunnel syndrome. Inflammatory and noninflammatory pain is treated by ultrasound, MRI, Shortwave, microwave, wax therapy, IRR, laser therapy, interferential current therapy, iontophoresis. Some studies have reported good outcomes with physiotherapy regimes of stretching and strengthening, with more favorable results than rest and reduced activity at short-term follow-up.[rx]
Deep transverse friction massage – It is a special type of massage technique called transverse friction massage is often used to treat carpal tunnel syndrome patients. It is applied to the tendons and the muscles, using the tips of one or two fingers to heal carpal tunnel syndrome.
Transcutaneous electrical nerve stimulation (TENS) – It is called TENS devices that help to transfer electrical impulses that are helpful for the treatment of carpal tunnel syndrome to the nervous system through the skin. These are supposed to keep the pain signals from reaching the brain by blocking pain message signals.
Extracorporeal shockwave therapy (ESWT) – It is a physiotherapy device that generates shock or pressure waves that are transferred to the tissue through the skin for healing carpal tunnel syndrome. This is assumed that to improve the circulation of blood in the tissue and speed up the healing process
Wrist Splints – Wrist splints can keep the wrist from bending. They are not as beneficial as surgery for patients with moderate-to-severe CTS, but they appear to be helpful in specific patients, such as those with mild-to-moderate nighttime symptoms that have lasted for less than a year. Typically the splint is worn at night or during sports. The splint is used for several weeks or months, depending on the severity of the problem, and it may be combined with hand and finger exercises. Benefits may last even after the patient stops wearing the splint.
Ultrasound – Ultrasound uses high-frequency sound waves directed toward the inflamed area. The sound waves are converted into heat in the deep tissues of the hand, opening the blood vessels and allowing oxygen to be delivered to the injured tissue. Ultrasound is often performed along with nerve and tendon exercises. Ultrasound treatment appears to be effective in the short term, but its long-term benefit remains unknown.
Yoga – Very limited evidence suggests that yoga practice may provide some benefit for patients with carpal tunnel syndrome. Yoga postures are designed to stretch, strengthen, and balance upper body joints.
General Exercise Program – Some experts have reported that people who are physically fit, including athletes, joggers, and swimmers, have a lower risk for cumulative trauma disorders. Although there is no evidence that exercise can directly improve CTS, a regular exercise regimen using a combination of aerobic and resistance training techniques strengthens the muscles in the shoulders, arms, and back; helps reduce weight, and improves overall health and well-being.
Low-Level Laser Therapy – Some investigators are working with low-level laser therapy (LLLT), which generates extremely pure light in a single wavelength. The procedure is painless. However, two trials comparing laser therapy to conservative treatment or a placebo laser treatment found no real benefit from this therapy.
Alternative Therapies – Many alternative therapies are offered to people with carpal tunnel syndrome and other repetitive stress disorders. Few of these therapies have any proven benefit, however. People should learn how alternative therapies may interact with other medications they are taking, or impact other medical conditions they have, and they should check with their doctor before trying any of these therapies.
Acupuncture – Acupuncture is often used to relieve CTS symptoms. Although the treatment looks promising for symptom relief, there isn’t enough solid research at this point to recommend it for CTS. More studies are needed to evaluate its benefit.
Chiropractic Therapies – Chiropractic techniques may be helpful for some people whose problems are caused by pinched nerves. There is little evidence, however, to support the use of chiropractic therapies for carpal tunnel syndrome.
Magnets – Magnets are a popular but unproven therapy for pain relief.
Medication
Over-the-counter drugs – In special circumstances, various medications can reduce the pain, the pain and swelling associated with carpal tunnel syndrome. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as aspirin, ibuprofen, naproxen, aceclofenac, and other nonprescription pain relievers, may provide some short-term relief from discomfort.
Prescription medicines – The corticosteroids (such as prednisone) or the drug lidocaine can be injected directly into the wrist to healing and remove overpressure in the median nerve or taken by mouth (in the case of prednisone) to relieve pressure on the median nerve in people with mild or intermittent symptoms.
Vitamin B1, B6, and B12 – It is essential for neuropathic pain management, pernicious anemia, tennis elbow, with vitamin b complex deficiency pain, paresthesia, numbness, itching with diabetic neuropathy pain, myalgia, etc. A side effect may be nausea- vomiting, abdominal pain, cramping
Nerve relaxant – It is basically used to reduce neuropathic pain, inflammation, nerve root entrapment, myalgia, neuralgia, and fibromyalgia, and carpal tunnel syndrome. Your doctor may prescribe gabapentin, pregabalin, vitamin B1, B6, B12, etc. Major side effects are abdominal pain, nausea- vomiting.
Lidoderm patches – It is a prescription medicine that is used to reduce pain, swelling, tenderness, paresthesia, itching, numbness, and carpal tunnel syndrome. It has the anesthetic power that is helpful in carpal tunnel syndrome.
Corticosteroid Injections – Corticosteroids (also called steroids) reduce inflammation. If restricting activities and using painkillers are unsuccessful, the doctor may inject a corticosteroid into the carpal tunnel. In CTS, steroid injections (such as cortisone or prednisolone) shrink the swollen tissues and relieve pressure on the nerve. There is good evidence that they offer short-term symptom relief in a majority of CTS patients. However, in about half of cases, symptoms return within 12 months. Generally, a second injection does not provide any added benefit. Another concern with the use of these injections in moderate or severe diseases is that nerve damage may occur even while symptoms are improving. Most doctors limit steroid injections to about three per year because they can cause complications, such as weakened or ruptured tendons, nerve irritation, or more widespread side effects.
Low-Dose Oral Corticosteroids – A short course (1 – 2 weeks) of oral corticosteroid medicines may provide relief for some people, but the relief does not usually last. Long-term use of these medications can cause serious side effects.
Botulinum toxin type A – Intracarpal injections of botulinum toxin type A (Botox) have not been well studied.
Surgery
Carpal tunnel release surgery is among the most common surgeries performed in the United States. In various trials, 70 – 90% of patients who underwent surgery were free from nighttime pain afterward. Studies have found that surgery provides a greater benefit over the long term compared with splinting or anti-inflammatory drugs plus hand therapy.
Candidates for Surgery
Although evidence strongly suggests that surgery is more effective than conservative approaches (at least in patients with moderate-to-severe CTS), the decision about whether to have surgery to correct CTS and when to have it, is not always clear. Electrodiagnostic and other tests used to confirm CTS are not always perfect or useful in determining the best candidates for surgery.
As a result, surgery does not cure all patients. A number of experts believe that release surgery is performed too often. Some recommend a full trial of conservative treatment (such as splints, anti-inflammatory agents, and physical therapy) before choosing surgery. Others warn that CTS is often progressive and will worsen over time without surgery and that surgery is better than splints and conservative measures for pain relief in cases where carpal tunnel syndrome is likely to present.
Factors that may increase the chances of a successful surgery
Having surgery performed within 3 years of being diagnosed with the disorder
Being in good general health
Having very slow nerve conduction results, but also having reasonably good muscle strength before surgery
Having symptoms that are worse at night than during the day
Factors that may reduce the chances for success
Having very severe symptoms before surgery, such as:
Symptoms that have been present for more than 10 months
Being over 50 years old
Performing heavy manual labor, particularly working with vibrating tools. Only slightly more than half of people who use vibrating hand-held tools are symptom-free 3 years after a CTS operation.
Patients who are on hemodialysis have good initial success, but the condition deteriorates in about half of these patients after around a year and a half.
Patients with diabetes and high blood pressure may be more likely to require a second operation.
Standard Release Surgical Procedures
CTS surgery can be performed through a standard open release, a mini-open technique, or endoscopy. There is no clear evidence to suggest that one surgical technique is much better than another over the long term.
Open Release Surgery – Traditionally, surgery for CTS has involved an open surgical procedure performed in an outpatient facility. In this procedure, the carpal ligament is cut free (released) from the median nerve. This relieves pressure on the median nerve. The surgery is straightforward. In treating carpal tunnel syndrome, surgery may be required to release the compressed median nerve. The open release procedure involves simply cutting the transverse carpal ligament.
The Mini-Open Approach – In recent years, more surgeons have adopted a “mini” open also called short-incision procedure. This surgery requires only a 1-inch incision, but it still allows a direct view of the area (unlike endoscopy, which is viewed on a monitor). The mini-open approach seems to reduce recovery time, pain, and recurrence rate compared to an open approach. However, over the long term, there doesn’t seem to be any significant difference between the mini-open approach and the standard open release.
Endoscopy.
Endoscopy for carpal tunnel syndrome is a less invasive procedure than standard open release.
A surgeon makes one or two 1/2-inch incisions in the wrist and palm and inserts one or two endoscopes (pencil-thin tubes).
The surgeon then inserts a tiny camera and a knife through the lighted tubes.
While looking at the underside of the carpal ligament on a screen, the surgeon cuts the ligament to free the compressed median nerve.
Patients who have endoscopic surgery report less pain than those who have the open release procedure, and they return to normal activities in about half the time. Nevertheless, at this time the best evidence available does not show any significant long-term advantages of endoscopy over open release in terms of muscle, grip strength, or dexterity. The endoscopic approach may even carry a slightly higher risk of pain afterward. This may be due to a more limited view of the hand with endoscopy. (In the open release procedure, the surgeon has a full view of the structures in the hand.) Because of this reduced visibility, there are more concerns about irreversible nerve injury with endoscopic carpal tunnel release than with open carpal tunnel release. However, larger studies have shown an extremely low number of complications when the procedure is performed by experienced physicians.
Recovery after Surgery
Timing of Recovery
For some patients, release surgery relieves symptoms of numbness and tingling immediately.
People who have the operation on both hands will need someone to help them at home for about 2 weeks.
Returning to strenuous work right after surgery may cause the symptoms to return. Patients who work in strenuous jobs generally stay out of work for at least a month and often much longer, depending upon the type of surgery and the severity of the condition. Recovery time appears to be faster with endoscopy or a mini-open release than with open release.
People who perform light office work will return to work much sooner, although possibly with some limitations.
Immediately after surgery, patients usually experience a decline in grip strength and dexterity. Studies have reported a wide range of recovery in this area. The scar may remain tender for up to a year.
Peak improvement (the best level of improvement a patient can reach) may take a long time (up to 10 months).
Physical Therapy. Physical therapy following surgery has not been shown to speed up recovery or affect the final outcome of CTS surgery.
Complications and Long-Term Outcome
Treatment failure and complication rates of CTS surgery vary.
Complications after surgery may include the following:
Loss of some wrist strength is a complication that affects 10 – 30% of patients. Some patients who have jobs requiring significant hand and wrist strength may not be able to perform them after surgery. These workers may also have problems in other parts of the upper body, including the elbows and shoulders. These problems do not go away with surgery and can persist. Studies indicate that 10 – 15% of patients change jobs after a CTS operation.
If pain and symptoms return, the release procedure may be repeated.
Reasons for procedure failure include
Incomplete release of the ligament
Extensive scarring
Recurrence of the disorder due to underlying medical conditions
Patients who had open release surgery appear more likely to require repeat operations compared with those who have had endoscopic surgery.
Immediately after surgery for carpal tunnel syndrome
You should exercise your hand and wrist as soon as possible, following your doctor’s advice.
Self-care after surgery for carpal tunnel syndrome
Follow your doctor’s advice, but general suggestions include:
If you go home within a day or two of surgery, you will probably need some help around the house.
Continue your medication as ordered by your doctor.
Cold packs applied at regular intervals can help reduce post-operative swelling.
Rest the hand as much as you can for at least four weeks following surgery.
Long-term outlook after surgery for carpal tunnel syndrome
Your symptoms should ease dramatically after surgery. However, pain around the surgery site may linger for some months. See your doctor if you are concerned about the amount of pain or discomfort. If you have non-absorbable sutures, your doctor will need to remove these about two weeks after the operation. If you have any increased swelling, redness or heat, see your doctor immediately, since these symptoms could indicate infection.
Exercises for Carpal Tunnel Syndrome
Wrists
Exercise 1
Make a loose right fist, palm up, and use your left hand to press gently down against the clenched hand.
Resist the force with the closed right hand for 5 seconds. Be sure to keep your wrist straight.
Turn your right fist palm down, and press the knuckles against the left open palm for 5 seconds.
Finally, turn your right palm so the thumb-side of the fist is up, and press down again for 5 seconds.
Repeat with your left hand.
Exercise 2
Hold one hand straight up shoulder-high with your fingers together and palm facing outward. (The position looks like a shoulder-high salute.)
With the other hand, bend the hand you are exercising backward with the fingers still held together and hold for 5 seconds.
Spread your fingers and thumb open while your hand is still bent back and hold for 5 seconds.
Repeat five times with each hand.
Exercise 3 (Wrist Circle)
Hold your second and third fingers up, and close the others.
Draw five clockwise circles in the air with the two fingertips.
Draw five more counterclockwise circles.
Repeat with your other hand.
Fingers and Hand
Exercise 1
Clench the fingers of one hand into a tight fist.
Release, fanning out your fingers.
Do this five times. Repeat with the other hand.
Exercise 2
To exercise your thumb, bend it against the palm beneath the little finger, and hold for 5 seconds.
Spread the fingers apart, palm up, and hold for 5 seconds.
Repeat five to 10 times with each hand.
Exercise 3
Gently pull your thumb out and back and hold for 5 seconds.
Repeat five to 10 times with each hand.
Forearms (stretching these muscles will reduce tension in the wrist)
Place your hands together in front of your chest, fingers pointed upward in a prayer-like position.
Keeping your palms flat together, raise your elbows to stretch your forearm muscles.
Stretch for 10 seconds.
Gently shake your hands limp for a few seconds to loosen them.
Repeat frequently when your hands or arms tire from activity.
Neck and Shoulders
Exercise 1
Sit upright and place your right hand on top of your left shoulder.
Hold that shoulder down, and slowly tip your head down toward the right.
Keep your face pointed forward, or even turned slightly toward the right.
Hold this stretch gently for 5 seconds.
Repeat on the other side.
Exercise 2
Stand in a relaxed position with your arms at your sides.
Shrug your shoulders up, then squeeze your shoulders back, then stretch your shoulders down, and then press them forward.
Tennis elbow is also known as lateral epicondylalgia (LE) and often referred to as epicondylitis or tendinopathy clinically,[rx] has complex underlying pathophysiology which is not well understood but is characterized by uncomplicated signs of localized pain over the lateral epicondyle which is made worse with resisted wrist extension and grip.[rx] The term epicondylitis has recently been considered a misnomer because of a lack of inflammatory signs. The pain may also extend into the back of the forearm and grip strength may be weak.[rx][rx] Onset of symptoms is generally gradual.[rx] Golfer’s elbow is a similar condition that affects the inside of the elbow.[rx]
Lateral epicondylitis also is known as tenniselbow, is a common condition that is estimated to affect 1% to 3% of the population. The word epicondylitis suggests inflammation, although histological analysis on the tissue fails to show any inflammatory process. The structure most commonly affected is the origin of the tendon of the extensor carpi radialis brevis and the mechanism of injury is associated with overloading. Nonsurgical treatment is the preferred method, and this includes rest, physiotherapy, cortisone infiltration, platelet-rich plasma injections and use of specific immobilization. Surgical treatment is recommended when functional disability and pain persist. Both the open and the arthroscopic surgical technique with resection of the degenerated tendon tissue present good results in the literature.
Tennis Elbow
Obviously, this condition earned its name because whacking tennis balls around a lot was the original main cause, but these days it is much more commonly caused by computer usage. And heavy computer users outnumber serious tennis players at least a thousand to one.
Today, this condition would be better-called computer elbow.
(1) Electrohydraulic – electromagnetic, or piezoelectric devices are used to translate energy into acoustic waves during extracorporeal shock wave treatment (ESWT) for chronic lateral epicondylitis (CLE) of the elbow (elbow tendonitis or tenniselbow). These waves may help to accelerate the healing process via an unknown mechanism.
(2) Results from randomized – controlled trials have been conflicting. Half of the studies showed statistically significant improvement in pain in the treatment group, and half of the studies had data showing no benefit over placebo for any measured outcomes.
(3) Limited evidence shows that ESWT – is cheaper than arthroscopic surgery, open surgery, and other conservative therapies, such as steroid infiltrations and physiotherapy, that continue for more than six weeks.
(4) The lack of convincing evidence – regarding its effectiveness does not support the use of ESWT for CLE.
Causes of Tennis Elbow
Overuse – This can be both non-work and work-related. Overuse can happen from “repetitive” gripping and grasping activities such as meat cutting, plumbing, painting, auto-mechanic work, etc.
Trauma – Although less common, a direct blow to the elbow may result in swelling of the tendon that can lead to degeneration. This can make the elbow more susceptible to an overuse injury.
Tennis elbow is a type of repetitive strain injury – resulting from tendon overuse and failed healing of the tendon. In addition, the extensor carpi radialis brevis muscle plays a key role.[rx][rx] Example of repetitive movement that may cause tennis elbow
Early experiments suggested that tennis elbow – was primarily caused by overexertion. However, studies show that trauma such as direct blows to the epicondyle, a sudden forceful pull, or forceful extension cause more than half of these injuries.[rx] Repeatedly mis-hitting a tennis ball in the early stages of learning the sport causes shock to the elbow joint and may contribute to contracting the condition.[rx]
Tendons and joints are made of flexible – string-like tissues that connect muscles to bones. Repeatedly using tendons and joints can lead to strains, tears or inflammation because the tissue forming them becomes degenerated and worn-down over time (meaning the tissue experiences microtears)
An injury to a tendon is called “tendinopathy – In the case of tennis elbow, the tendon that is injured is the extensor carpi radiaslis reavis (or the ECRB). The ECRB tendon controls the movement of the wrists when the elbow is straight. If the elbow is straightened and bent over and over again, the tendon can become overworked. This is why tennis elbow is really a form of injury.
Inflammation – then develops around the outer elbow muscle and tendon as your body’s way of attempting to heal these tiny tissue tears. The damaged tendon sometimes starts leaking fluid and even collagen, increasing inflammation. Sometimes the area forms hardened tissue to fix the damage.
Tennis elbow is most common – in people who use their elbows in the same manner day after day, for many weeks or months on end.
Adults with professions – that require consistent use of the upper arms and repetitive movements are especially prone to developing tennis elbow. This includes athletes, personal trainers, gardeners, painters, auto workers, landscapers, carpenters, cooks or butchers and plumbers
Even if your job – doesn’t require much use of your elbows or arms, if you spend a lot of time typing on the computer, knitting, cooking, painting or playing an instrument, it’s still possible to suffer from tennis elbow.
Playing racquet sports – such as tennis, badminton or squash (see below)
Throwing sports – such as the javelin or discus
Using shears while gardening
Using a paintbrush or roller while decorating
Manual work such as plumbing or bricklaying
Activities that involve fine, repetitive hand and wrist movements – such as using scissors or typing
Other activities that involve repeatedly bending the elbow – such as playing the violin
Sports like tennis, rowing or strength training
Manual labor like painting, carpentry or turning screws
Heavy lifting
Playing musical instruments, such as the piano
Working at a computer or a supermarket cash register
Using plumbing tools
Painting
Driving screws
Cutting up cooking ingredients, particularly meat
Repetitive computer mouse use
Symptoms of Tennis Elbow & Diagnosis
A symptom of tennis elbow commonly include
Pain, tenderness and swelling – around the elbow. Some people find that pain is the first in the morning after getting up
Shooting or intense pain – that carries over to other parts of the forearm, especially when moving the arm
Trouble moving the wrist normally and stretching the hand
Pain on the outside of your upper forearm, just below your elbow – the pain may also travel down your forearm towards your wrist
Pain when lifting or bending your arm
Pain when writing or gripping small objects – for example, when holding a pen
Pain when twisting your forearm – for example, when turning a door handle or opening a jar
Pain and stiffness when fully extending your arm
Pain when picking things up – gripping objects, typing on a computer and putting pressure on the lower arms in other ways
Tennis elbow will develop slowly – as more micro tears develop in the elbow’s tendon. At first, you might not notice this process happening, but at some point, you’ll feel tenderness, especially when repeatedly moving the elbow.
Tennis elbow experience – a weakening in their grip (like when they are holding a tennis racket or golf club); others have trouble picking up everyday things, like a toothbrush or phone.
Diagnosis of Tennis Elbow
Physical examination
To diagnose tennis elbow, physicians perform a battery of tests in which they place pressure on the affected area while asking the patient to move the elbow, wrist, and fingers. Diagnosis is made by clinical signs and symptoms that are discrete and characteristic.
For example, when the elbow fully extended, the patient feels points of tenderness over the affected point on the elbow. The most common location of tenderness is at the origin of the extensor carpi radialis brevis muscle from the lateral epicondyle (extensor carpi radialis brevis origin), 1 cm distal and slightly anterior to the lateral epicondyle.[rx] There is also pain with passive wrist flexion and resistive wrist extension (Cozen’s test).[rx]
Medical imaging
X-rays – These tests provide clear images of dense structures like bone. They may be taken to rule out arthritis of the elbow. X-rays can confirm and distinguish possibilities of existing causes of pain that are unrelated to tennis elbows, such as fracture or arthritis. Rarely, calcification can be found where the extensor muscles attach to the lateral epicondyle.[rx]
Medical ultrasonography – are other valuable tools for diagnosis but are frequently avoided due to the high cost.[rx] MRI screening can confirm excess fluid and swell in the affected region in the elbow, such as the connecting point between the forearm bone and the extensor carpi radialis brevis muscle.
Magnetic resonance imaging (MRI) scan – If your doctor thinks your symptoms are related to a neck problem, an MRI scan may be ordered. MRIs scans show details of soft tissues and will help your doctor see if you have a possible herniated disk or arthritis in your neck. Both of these conditions often produce arm pain.
Electromyography (EMG) – Your doctor may order an EMG to rule out nerve compression. Many nerves travel around the elbow, and the symptoms of nerve compression are similar to those of tennis elbow.
Cervical radiculopathy with pain in the elbow and forearm.[rx]
Elbow overuse to compensate for disease in an adjacent joint (frozen shoulder for example).
Posterior interosseous nerve (PIN) entrapment (also known as ‘radial tunnel syndrome’). Nerve compression produces neuropathic pain in the lateral forearm. However, pain is not reproduced by wrist extension. Resisted supination can produce pain as the supinator is one of the possible areas of PIN compression.
An anesthetic block of the PIN can be diagnostic, but injection should be performed selectively to avoid diffusion of the local anesthetic to the lateral epicondyle area.[rx] The middle finger extension test, resisted supination of the forearm and nerve conduction studies have all been described to assist in the diagnosis of radial tunnel syndrome.[rx]
Degenerative changes and OCD of the capitellum. It has been observed that 59% of cases of lateral elbow pain refractory to conservative treatment have some chondral changes in the radiocapitellar joint.[rx] OCD typically affects young individuals involved in sports and physical activities who have mild grinding and pain when performing a moving valgus test.
Inflammation and edema of the anconeus muscle. Some studies have reported a relatively high incidence of anconeus edema, shown in MRI of patients complaining of lateral elbow pain.[rx]Fasciotomy of the muscle can solve that problem.[rx]
Posterolateral elbow instability should definitely be ruled out in every patient suffering from lateral elbow pain. The association between instability and epicondylitis has been established, following excessive use of steroids or the local pathogenic insult. The presentation is low-grade and may require examination of the patient under anesthesia to test it properly. The presence of cubitus varus, previous surgery or dislocations of the elbow should be assessed.
Other causes of pain include low-grade infection (Propionibacterium acnes)[rx] or other inflammatory diseases such as rheumatoid arthritis.[rx]
Treatment of tennis elbow
In the acute stage
Give advice on the self-limiting nature of the pathology if adequate steps to avoid the aggravation of symptoms are taken.
Give advice on the modification of aggravating activities: • Avoid lifting, especially heavyweights,
Lift objects close to the body, with elbow bent and palm facing upwards
Avoid repetitive gripping and twisting activities,
Take regular breaks from all activities involving the upper limb,
Suggest the patient seek “light duties” which avoid tasks aggravating the condition at work if possible.
Offer analgesia or NSAID medication if clinically appropriate. Although evidence for analgesia and NSAID are inconclusive, patients may opt to try pain-relieving medication.
If symptoms persist beyond 12 weeks but are less than 26 weeks, discuss other options including
Referral to physiotherapy for supervised and home exercise programs and manual therapy.
Laser therapy (of the correct dose) could be considered.
For short-term relief of severe pain consider corticosteroid injections. However, consideration of long-term relapses and the likelihood of adverse effects should be discussed with the patient.
Non-operative treatment
Non-operative treatment includes a wide array of possibilities with a rate of improvement in 90% of cases. Several new techniques have been developed in last decade including percutaneous radiofrequency treatment and injections with different preparations of growth factors. It is wise to involve the patient and gain their commitment to the management programme as it may be months before improvement is observed:
Rest
Rest is your first line of defense against this condition. People find it persistent mainly because they don’t take the problem seriously enough. Even a minor injury like this will not just magically go away if you keep doing whatever irritated the forearm muscles and tendons in the first place. A week of resting the arm as much as possible is often enough to make a significant difference.
Exercise
Although resting is initially critical, a careful balance of rest and a variety of exercise is the basic formula for recovery from most RSIs. Nothing in biology seems to recover without a little stimulation — you just have to beware of overdoing it. Gradually and progressively train the flexor muscles and tendons to tolerate exercise again.
Chances are good that you will need to go more slowly than you think; these conditions rarely change quickly. Mobilizations and stretching (next up) are good examples of easy, intermediate exercises — ways to start exercising without over-stimulating.
But eventually, you want to work up to working out with, say, spring-loaded hand grips … and then tennis, of course (even if you’re not a tennis player). At all stages, though, you start with small doses, and the need to give plenty of rest (recovery time) is crucial throughout. It’s never just exercise, and never just rest, but a long term balancing act between them.
Stretching and mobilizing
Although stretching is over-rated as a general tonic (see Quite a Stretch), it can be useful for specific therapy like this. Muscle trigger points (muscle knots) occasionally respond well to stretch (see Stretching for Trigger Points), and in my experience, it’s a little more likely to work out in this muscle group.
Since trigger points are almost always a factor in tennis elbow, I always recommend stretching for this condition. It is tricky to fully stretch the muscles involved in tennis elbow, but you can do it like this – while standing, with your arm in front of you, place the back of your hand against a wall with the fingers pointed out to the side, straighten your elbow, and then press into the wall so that your wrist is flexed sharply. Hold for a minute. Be cautious: do not stretch too hard, and release the stretch gradually, over several seconds at least.
Isometric contraction for pain relief
A small 2015 test showed a surprisingly robust pain-relief effect from briefly “clenching”:7 tensing the muscles on the back of the forearm without the wrist, basically just putting the tendon under strong tension for about a minute. The pain reduction was substantial and lasted for at least 45 minutes.
It may be one of the best pain-control strategies, and a good alternative to medication. For tennis elbow, you want to pull on the common extensor tendon of the forearm. Probably the easiest way to do that is just to hold the hand firmly in a neutral position (with the other hand), and then attempted to extend the hand (bend the wrist backward). Start with moderate intensity for about one minute, and tinker with the intensity and duration to see what works best for you.
Icing
Tendinitis supposedly hurts because of the “inflammation,” but as explained above inflammation is actually limited or missing entirely in chronic cases. In acute (fresh) cases, or serious flare-ups of a chronic condition, ice might actually control inflammation and potentially retard the progression of the condition — a genuine biological benefit, as opposed to just a bit of pain control — but unfortunately, no one knows if it actually works.
Contrast Hydrotherapy
Contrasting is the alternating application of heat and cold to the area. This dramatically increases circulation to the entire arm and hand. Like icing, this is stressless tissue stimulation, but with a much greater impact on circulation in particular.
Like icing, there’s no direct evidence that this actually works, but it’s a solid theory — and, done right, it is actually extremely pleasant! Obviously, please don’t burn yourself with too-hot water. By far the most convenient method of doing this is in a double-sink: one filled with cold water, the other with hot water. For more information about contrasting, see Contrast Hydrotherapy.
Self-massage
Your forearm is an easy body part to reach for self-massage! Tennis elbow is probably always aggravated by muscle tension in the forearms, regardless of whether muscle strain is part of the condition or not. It is often helpful to do some simple massage: firm, long, lubricated strokes from hand to elbow on the back of the arm.
Be firm but not brutal. Visualize the muscles like a sponge full of dirty water that you are squeezing out! See Massage Therapy for Tennis Elbow and Wrist Pain, which explains exactly where the worst trigger points in the arm usually form.
Friction Massage
Like all tendinitises, tennis elbow may respond well to a specific massage technique called “friction massage.” Rub back and forth over the tendon (across it) gently with your thumb or finger pads until the sensitivity fades, which should take no more than a minute or two, and then increase the intensity slightly and repeat. If the intensity doesn’t ease, discontinue. Deep Friction Massage Therapy for Tendonitis.
Ergonomic Adjustments
If you use a computer heavily, you may wish to invest in some improvements to your computer workstation to aid in healing from computer elbow. Keyboards are straightforward, as there is really only one important thing to know: don’t lift the back of your keyboard. This is a bizarre anachronism that exists only because early keyboard manufacturers wanted computer keyboards to seem more like typewriter keyboards (i.e. steep). However, the ergonomic problem with this is significant. An elevated keyboard forces you to keep the wrists “cocked” into extension, holding all of the extensor muscles of the forearm in contraction. This is Very, Very Bad, and severely aggravates computer elbow situations. Avoid it at all costs. Mitigate it with a gel wrist pad (to lift the heel of the hand).
Shock wave Therapy
Extracorporeal shock wave therapy (ESWT) is the more expensive, intense, and high-tech and over-hyped cousin of regular ultrasound. ESWT uses much stronger sound waves — shock waves! Treatment is painfully intense and painfully pricey, though it would probably be worthwhile if it worked.
On the one hand, ESWT is just a “more is better” version of standard ultrasound because it is often used with the same imprecise clinical intention to stimulate/provoke tissues. On the other hand, because it was originally developed for smashing gall stones, ESWT is strong enough to actually disrupt tissue, such as, say, calcifications in tendons — which is a nice precise clinical goal and a whole different kettle of fish. And there is evidence that it can be effective in exactly that circumstance: if your tendons are calcifying.
One woman’s ergonomic mouse is another’s hand torture device!
And we even fail to adjust when the cord outright snags! We get focussed on our work and simply put up with the cord being caught under a book or the corner of the keyboard. It’s not that the mouse is necessarily stuck in a “bad” position, but we aren’t free to move it to a better one. By contrast, wireless mice are surprisingly liberating. If your arm is getting uncomfortable using the mouse in one position, you can simply adjust.
For the same reason, I recommend basically the best quality mouse, which is laser these days. Mouse shape and button design are pretty trivial factors. Basically, comfort is all you’re looking for, and people’s hand shapes and usage patterns are so different that one woman’s “ergonomic” mouse is another’s hand torture device.
Physiotherapy
It is another alternative. Some studies have reported good outcomes with physiotherapy regimes of stretching and strengthening, with more favorable results than rest and reduced activity at short-term follow-up.[rx] No standard regime has been established as superior to any other method.
The fundamental principle is to load the tendon as close as possible to its limit but without surpassing it. Eccentric exercises and partial load-favoring tendon healing are the mainstays of physiotherapy regimes. A stable shoulder and scapula are necessary for correct elbow function; strengthening exercises of the scapular stabilizers including the lower trapezius, serratus anterior and rotator cuff muscles is mandatory.
Epicondylar Counterforce Braces
Work by reducing tension in the wrist extensors. Elbow straps, clasps or sleeve orthoses have been demonstrated as superior for pain relief and grip strength when compared with placebo orthoses.[rx] However, no differences between races were shown in a systematic review[rx] and we do not use them in our practice. We have seen patients with secondary nerve problems due to prolonged use of a counterforce brace.
Percutaneous Radiofrequency thermal Treatment
A radiofrequency electrode is introduced percutaneously under ultrasound guidance which produces a thermal injury when activated, inducing a microtenotomy and removing all pathological tissue. Good outcomes have been reported, and no reduction of tendon size has been observed.[rx]
Extracorporeal Shock-wave Therapy
A device generates shock or pressure waves that are transferred to the tissue through the skin. This is supposed to improve the circulation of blood in the tissue and speed up the healing process. (ECSW) has been proposed as an alternative to non-operative management. The mechanism of action is not fully known. A generator of specific frequency sound waves is applied directly onto the overlying skin of the ECRB tendon. It has not been demonstrated to be more beneficial than other treatment modalities.[rx]
The Use of Low-Level Laser Therapy
It has been proposed due to the stimulating effect of laser on collagen production in tendons. Although laser was not initially viewed as particularly useful among LE therapies, a recent study has demonstrated some short-term benefits when using an adequate dose and wavelength.39
Acupuncture
It has demonstrated good outcomes on short-term follow-up.[rx] However, long-term results remain unclear. The acupuncture needles are inserted into certain points on the surface of the arm. Here, too, the aim is to minimize the perception of pain.
Laser Therapy
The tissue is treated with concentrated beams of light. This is supposed to stimulate the circulation of blood and the body’s cell metabolism.
TENS devices transfer electrical impulses to the nervous system through the skin. These are supposed to keep the pain signals from reaching the brain.
Activity Modification
Initially, the activity causing the condition should be limited. Modifying grips or techniques, such as use of a different size racket in tennis, may relieve the problem.
Equipment Check
If you participate in a racquet sport, your doctor may encourage you to have your equipment checked for proper fit. Stiffer racquets and looser-strung racquets often can reduce the stress on the forearm, which means that the forearm muscles do not have to work as hard. If you use an oversized racquet, changing to a smaller head may help prevent symptoms from recurring.
Medication
Non-steroidal anti-inflammatory drugs – (NSAIDs) can be useful for the short-term relief of symptoms. Even if their use is superior to a placebo, no differences between oral and topical NSAIDs have been established.[rx]
Corticosteroid injections – are commonly used to treat LE. The way in which they work is currently unknown; they probably help to control local inflammatory response and pain medication.[Rx]Corticosteroid injections seem to be superior to NSAIDs at four weeks, but no differences are observed at a later stage. Cortisone injections should be avoided in all cases, unless a short-term good result is advisable (such as a professional tennis player in mid-season), as most patients improve without corticosteroids and better long-term results can be achieved without them.[rx]Patients should be advised of potential side-effects including changes in coloration of the skin, fat atrophy and muscle wasting.
Hyaluronic acid – A substance made by the body, found in tissue and joints. It is typically used to treat osteoarthritis. One study suggests that hyaluronic acid might be effective in the treatment of tennis elbow. But further research is needed to assess its pros and cons.
Autologous blood injections – are thought to work by stimulating an inflammatory response which will bring in the necessary nutrients to promote healing. Short-term good results have been reported recently;[rx,rx] however, no benefit in the long-term follow-up has been found and its use is only recommended for those recalcitrant cases when other modalities of treatment have failed.
Platelet-rich plasma injections (PRP) – These preparations are thought to contain high concentrations of growth factors, which could theoretically enhance tendon healing. The general technique involves patient-blood extraction, centrifugation and re-injection of the plasma into the lateral epicondyle. Good outcomes have been reported.[rx,rx] However, no differences were seen between PRP and whole blood injections.[rx] Moreover, significant differences among available commercial systems and variations in the technique make it difficult to draw clear conclusions about the use of PRP in this pathology. New legal regulations could slow down the adoption of these last techniques.
Botulinum toxin A injections – act by diminishing muscle tone. Reducing the tension on the ECRB insertion could be beneficial for pain relief. Good short-term results have been published,[rx] but as yet there is no consensus on its use and the effects may be conditioned by the technique, the operator and the dose.
[stextbox id=’info’]
Randomized controlled trials published subsequent to the latest systematic reviews on injection therapy
Significant improvement in PRP group over steroid group for pain and DASH.
Corticosteroid group better initially and then declined
PRP group progressively improved
Corticosteroid injection significantly better for all outcomes at 4 weeks
Autologous blood injection and ECSWT gave significantly better Thomsen provocative test results and upper extremity functional scores at 52 weeks
The success rate of corticosteroid injection was 50%, which was significantly lower than the success rates for autologous blood injection (83.3%) and ECSWT (89.9%)
[/stextbox]
Surgery
In recalcitrant cases, surgery may be an option. Surgical methods include
Lengthening, release, debridement, or repair of the origin of the extrinsic extensor muscles of the hand at the lateral epicondyle
Rotation of the anconeus muscle
Denervation of the lateral epicondyle
Decompression of the posterior interosseous nerve
Surgical techniques for lateral epicondylitis can be done by open surgery, percutaneous surgery or arthroscopic surgery, with no evidence that any particular type is better or worse than another.[rx] Side effects include infection, damage to nerves and inability to straighten the arm.[rx]
Exercise Protocol For Rehabilitations
Eccentric exercises
Muscle-strengthening exercises can generally be divided up into concentric and eccentric exercises. In concentric exercises, the muscle contracts (tightens) – and in eccentric exercises, the muscle relaxes. One example of a concentric exercise is holding a weight in your hand and pulling it up towards your body. Gradually lowering the weight again is an eccentric exercise. Slowly working against gravity like this strengthens the muscles.
Eccentric strengthening exercises
Hold a weight in your hand.
Rest the affected arm on a table with your palm facing down, allowing your hand to hang off the edge of the table.
Use your free hand to bend the affected wrist back as far as you can while lifting the weight.
Gradually lower the hand with the weight in it.
Repeat about 10 to 15 times.
After a short break, repeat this set of exercises two more times.
Strengthening exercise for tennis elbow. It’s important not to use heavy weights. The weight should be about 30% of the maximum weight you can hold. Slight pain is okay, but you shouldn’t put too much strain on the arm.
Eccentric strengthening exercises
Rest the elbow of the affected arm on a table, with your forearm upright. Turn your forearm so that the palm of your hand is facing away from you.
Hold a full bottle in the affected hand.
Gradually lower the arm with the bottle, making sure not to bend your wrist.
Allow the bottle to fall into your free hand and move the affected arm back to the upright starting position.
Pass the bottle from the free hand back up to the affected hand.
Repeat about 10 to 15 times.
After a short break, repeat this set of exercises two more times.
It’s best to do strengthening exercises three times a day. Strengthening exercise for tennis elbow
Stretching
The aim of stretching exercises is to stretch the wrist extensor muscles in the forearm. These exercises are recommended in order to improve the mobility (range of movement) of the arm and wrist. They can either be done actively or passively. By “actively,” we mean you do them yourself. In passive exercises, a physiotherapist or training partner stretches that part of the body for you.
Example:
Stretch the affected arm out in front of you, with your palm facing downwards.
Relax your wrist, allowing your hand to dangle down.
Using your other hand, push the affected hand down and pull it towards your body.
Hold the stretch for about 30 to 45 seconds.
Have a break (about 30 seconds).
Repeat three times.
People are advised to do these stretching exercises about twice a day.
Stretching exercise for tennis elbow
Wrist turn
To perform a wrist turn:
bend the elbow at a right angle
extend the hand outwards, palm facing up
twist the wrist around gradually, until the palm is facing down
hold the position for 5 seconds
repeat nine more times
do two more sets of 10 repetitions
Wrist turn with weight
The wrist turn with weight is the same as the wrist turn above. But, in this version, the person also grips a light weight, such as a small dumbbell or a tin of food.
Wrist lift, palm up
To perform a wrist lift, palm up:
grip a light weight, such as a small dumbbell or a tin of food
bend the elbow at a right angle
extend the hand outwards, palm facing up
bend the wrist up towards the body
hold this position for 5 seconds, then release slowly
repeat nine more times
do two more sets of 10 repetitions
Elbow Bend
To perform the elbow bend:
stand straight
lower the arm to one side
slowly bend the arm upwards until the hand touches the shoulder
hold this position for 15 to 30 seconds
repeat nine more times
Wrist extensor stretch
To perform the wrist extensor stretch:
raise the arm straight out in front of the body
with the palm facing down, slowly bend the wrist downwards
using the other hand, gently pull the stretching hand back towards the body
hold this position for 15 to 30 seconds
straighten the wrist again
repeat twice
do two more sets of 3 repetitions
Wrist extensor flex
To perform the wrist extensor flex:
raise the arm straight out in front of the body
with the palm facing down, slowly bend the wrist upwards
using the other hand, gently pull the fingers back towards the body
hold this position for 15 to 30 seconds
straighten the wrist again
repeat twice
do two more sets of 3 repetitions
Fist squeeze
To perform the fist squeeze:
use a rolled-up towel, sock, or tennis ball and place in the palm
grip the ball or towel with the fingers to form a fist
squeeze tightly for 10 seconds
repeat nine more times
Towel twist
To perform the towel twist:
hold a loosely rolled-up towel lengthways, with one hand at each end
keep the shoulders relaxed
twist the towel by moving the hands in opposite directions, as if wringing out water
repeat nine more times
then repeat ten more times twisting the towel in the reverse direction
Complications
Failing to address concomitant pathology
Patients report inferior outcomes and lack of improvement if the primary cause of symptoms is not addressed; patients should be educated regarding the risks and benefits of surgery — the former include but are not limited to infection, blood loss, neurovascular injury, continued pain, stiffness, or continued or worsening overall dysfunction
Radial nerve entrapment can be missed or not addressed clinically in up to 5% of patients being managed for lateral epicondylitis.
Iatrogenic LUCL injury
Occurs iatrogenically with increased risk if the surgical dissection extends beyond the radial head equator
Postoperative iatrogenic posterolateral rotatory instability (PLRI) can develop if the extension or LUCL compromise is significant
Iatrogenic neurovascular injury
Radial nerve injury
Heterotopic ossification to decrease risk with via copious saline irrigation following decortication and debridement
Infection
Prevention
Other ways to prevent tennis elbow:
Warming up: Warming up before playing a sport that involves repetitive arm movements, such as tennis or squash, is essential. Gently stretching the arm muscles will help to avoid injury.
Using lightweight tools: Lighter sports equipment or racquets with a larger grip size will help reduce strain on the tendons. Damp tennis balls and older balls load the arm with unnecessary force.
Increasing the strength of forearm muscles: This can help support arm movement and prevent tennis elbow.
Decrease the amount of playing time if already injured or feeling pain in the outside part of the elbow.
Stay in overall good physical shape.
Strengthen the muscles of the forearm: (pronator quadratus, pronator teres, and supinator muscle)—the upper arm: (biceps, triceps)—and the shoulder (deltoid muscle) and upper back (trapezius). Increased muscular strength increases the stability of joints such as the elbow.
Like other sports, use equipment appropriate to your ability, body size, and muscular strength.[8]
Avoid any repetitive lifting or pulling of heavy objects (especially over your head) [21]
Vibration dampers (otherwise known as “gummies”) are not believed to be a reliable preventative measure. Rather, proper weight distribution in the racket is thought to be a more viable option in negating shock.[22]









































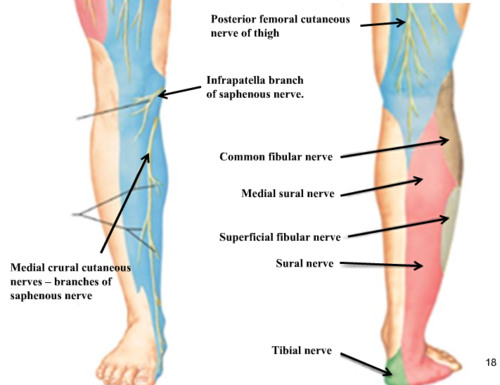





































 The autonomic nervous system (ANS) is a system of motor neurons that innervate smooth muscle, cardiac muscle and glands.
The autonomic nervous system (ANS) is a system of motor neurons that innervate smooth muscle, cardiac muscle and glands.